
Submitted:
25 December 2023
Posted:
26 December 2023
You are already at the latest version
Abstract
Reactive attachment disorder (RAD) and disinhibited social engagement disorder (DSED) manifest in individuals facing attachment system chal-lenges, particularly observed in minors under protective measures. The lack of standardized tools for assessing these difficulties and uncertainty about the most effective instruments from a psychometric perspective prompted this study. Using the COSMIN checklist, we systematically reviewed instruments assessing RAD, adhering to PRISMA and COSMIN guidelines. Examined tools included the Disturbance Attachment Inter-view, Preschool Age Psychiatric Assessment, Relationship Patterns Questionnaire, Assessment of RAD and DSED, Development and Well-Being Assessment, and Reactive Attachment Disorder Question-naire. Of the 11 articles analyzed, results highlight a research emphasis on internal consistency, structural and construct validity, sidelining other properties. While the instruments demonstrate strong structural validity, excellent internal consistency, and generally satisfactory error measurement results, the study concludes a dearth of investigations into psychometric properties for children and adolescents under protective measures.
Keywords:
reactive attachment disorder
; children
; adolescents
; psychometric proprieties
; COSMIN
; systematic review
1. Introduction
The inclusion of attachment disorders in the DSM-III marked a significant milestone, encompassing manifestations of Reactive Attachment Disorder (RAD) and Disinhibited Social Engagement Disorder (DSED) [1]. In the DSM-5-TR, these challenges are categorized separately [2,3]. Key features of RAD in young children include: (a) absence of attachment behaviors directed toward the primary caregiver, (b) failure to seek and respond to comfort in distressing situations, (c) diminished social and emotional reciprocity, and (d) disruptions in emotional regulation. Notable characteristics of DSED include: (a) little caution in approaching unfamiliar adults, (b) willingness to be with strangers, (c) lack of appropriate social and physical boundaries, evidenced by overly close interaction with unfamiliar adults, and (d) seeking close physical contact [3].
Observing attachment disorders in children involves examining the shallowness and conflict in their relationships, stemming from a lack of trust due to negative experiences with primary caregivers. Children with RAD struggle to trust others, even when encountering kindness. In contrast, those with DSED exhibit indiscriminate trust, placing them at a higher risk of physical, sexual, and emotional harm [4].
RAD and DSED relate to a failure in the normative attachment system that a baby should develop with their primary caregiver, experiencing a lack of access to the protection and security the caregiver should provide [5]. Certain risk factors, particularly adverse childhood experiences, contribute to the development of RAD or DSED. These include psychological maltreatment, sexual abuse, neglect, parental alcoholism, familial drug use, caregiver mental health issues, or the absence of a consistent primary caregiver, potentially due to institutionalization, recurring protective measures changes, parental incarceration, or parental abandonment [6]. Younger children are more susceptible to negligent or abusive behaviors from caregivers, leading to situations of neglect and an increased risk of removal from their biological family and institutionalization [7].
Furthermore, DSED and RAD are frequently diagnosed in children who have been institutionalized, post-institutionalized, or placed in foster homes. These children often display self-soothing behaviors, discomfort in social interactions, and aggression towards peers [8]. Additionally, they commonly exhibit other associated personal, developmental, emotional, social, and behavioral difficulties [9,10]. Despite an initial improvement in symptoms when transferred to a protective institution, this improvement tends to be temporary. Inhibitory behaviors remain stable, while disinhibited behaviors worsen with prolonged stay, suggesting that institutionalization can exacerbate attachment disorders, particularly disinhibited behaviors [11,12,13,14]. Despite the relevance and prevalence of RAD and DAI, there are few designed instruments that assess these disorders.
1.1. Instruments Assessing Attachment Disorders
- Disturbance Attachment Interview (DAI): The DAI, developed by Smyke and Zeanah in 1999 [15], is a semi-structured interview consisting of 12 items administered to a primary caregiver or someone well-acquainted with the child. It aims to assess signs related to disordered attachment and symptoms of both RAD and DSED. The items cover inhibited behaviors for RAD diagnosis, such as the absence of a preferred adult, lack of comfort-seeking, and limited social reciprocity. For DAI diagnosis, disinhibited behaviors are evaluated, including a lack of caution with strangers and a willingness to go with unknown adults. Scoring for the DAI ranges from 0 to 10 for RAD and 0 to 8 for DSED [16].
- The Preschool Age Psychiatric Assessment (PAPA): Seim (2019) [17] developed the PAPA, a caregiver-reported questionnaire designed for preschoolers aged 2-8 years. This assessment evaluates RAD and DSED based on DSM-5 criteria. RAD classification requires meeting RAD criteria A1 and one or more criteria B. For DSED, participants must meet at least two DSED criteria [18].
- Reactive Attachment Disorder and Disinhibited Social Engagement Disorder Assessment (RADA): Developed by Lehmann et al. in 2018 [21], the RADA assessment follows DSM-5 criteria. It features 11 items for RAD and 9 for DSED. TAR includes two factors: incapacity to seek/accept comfort and low socioemotional responsiveness/emotional dysregulation, while DSED has one factor related to indiscriminate behaviors [22].
- Development and Well-Being Assessment RAD/DSED (DAWBA RAD/DSED): A section within the DAWBA interview [23] comprises 14 items derived from the Child and Adolescent Psychiatric Assessment for RAD/DSED. These items assess social behaviors of concern to caregivers, scoring from 0 to 10 for TAR and 0 to 18 for DSED [24].
- RAD Questionnaire (Questionnaire Disorder Attachment Reactive): The RAD Questionnaire, developed by Minnis in 2002 [25], consists of 17 items evaluating both reactive and disinhibited attachment disorders concurrently. Scores on this questionnaire range from 0 to 51, with higher scores indicating more severe attachment disorder symptoms [26].
1.2. The current study
The aim of the present study was to assess the psychometric properties of instruments evaluating attachment disorders in samples of minors under protective measures. To achieve this, a systematic review was conducted, adhering to PRISMA standards and utilizing the Consensus based Standards for the selection of health status Measurement Instruments (COSMIN) checklist for systematic reviews of Patient-Reported Outcome Measures (PROMs) [27]. Information was gathered for each analyzed instrument, including authors, sample characteristics, country, design quality of the studies, and measurement properties as indicated in the studies.
2. Materials and Methods
2.1. Search Strategy
A systematic review of the scientific literature related to RAD was conducted according to the guidelines established by the PRISMA statement [28]. The search was carried out in March 2023 in the Web of Science. The names of the assessment instruments were combined using Boolean terms along with words related to the evaluation of psychometric properties and terms referring to the protective care system. The combination of these Boolean terms can be observed in Table 1.
2.2. Eligibility Criteria
Inclusion This review included articles analyzing the psychometric properties of instruments assessing RAD and DSED in minors within the protective care system. To ensure data comprehensiveness, articles meeting the criteria described below were included: 1) Original articles published in English or Spanish, 2) published between 2000 and 2022, 3) with samples of minors in adoption or residential/foster care, and 4) addressing the study of psychometric properties of instruments evaluating RAD or DSED.
Exclusions comprised: 1) Gray literature (doctoral theses, conference communications, or press articles), 2) articles using questionnaires but lacking psychometric information, and 3) systematic reviews of articles.
2.3. Procedure
All records were screened in a blinded by two authors (FG-S and MS) and when there was disagreement, a third reviewer interceded (LL-T). After reviewing the title and abstract to identify articles that analyzed the psychometric properties of instruments, works that did not meet the inclusion criteria were excluded (n = 189).
From the selected articles (n = 25), the full text was consulted, and once again, those that did not address the study of any instrument property were eliminated, resulting in a total of 10 articles. Among these, four focused on the DAI, one on the PAPA, two on the RPQ, one on the RADA, one on the DAWBA RAD/DSED, and two on the RAD Questionnaire. The entire process is outlined in Figure 1.
2.4. COSMIN Checklist for Systematic Reviews of PROMs
In order to thoroughly assess the methodological quality of the studies, the COSMIN checklist for systematic reviews of Patient-Reported Outcome Measures (PROMs) was utilized. This checklist distinguishes between "standards" and "criteria," with the former referring to the requirements set by each research study, indicating the quality of the study itself. Meanwhile, the latter, the "criteria," pertain to what would constitute good measurement (the quality of the PROM) [27]. The objective of this checklist is to evaluate the methodological quality of assessment instruments.
The checklist is divided into three parts and 10 boxes. The first part includes contributions from procedures aimed at conducting a systematic review according to guidelines such as PRISMA [28]. The second part encompasses the criteria used to assess the measurement quality of PROM instruments. The third and final part corresponds to the evaluation of the interpretability and feasibility of the PROM, as well as the formulation and reporting of the systematic review. For optimal use of the COSMIN guide, the authors recommend employing the checklist as a modular tool, filling in the relevant boxes [27].
3. Results
In the following section, the psychometric properties of each of the instruments selected for this study will be presented in detail.
3.1. Characteristics of the samples of the studies analyzed
Four articles analyzed the psychometric properties of the Disturbance Attachment Interview (DAI). These works included samples of between 55 and 853 people, all of whom were children aged between 4 months (Smyke et al., 2002) and 15 years (Elovainio et al., 2015) who were in protective measures. On the other hand, only one work analyzed the psychometric properties of The Preschool Age Psychiatric Assessment (PAPA). It had a sample of 400 adolescent and young-adult participants of both sexes from residential centers. In this case, although the instrument is for younger children, it was applied to adolescents.
On the other hand, an article psychometrically analyzed the Relationship Patterns Questionnaire (RPQ). It had a sample of 135 children with an average age of around 7 years. This work compared normal population, foster children, and hospitalized children (Schröder et al., 2019). The Reactive Attachment Disorder and Disinhibited Social Engagement Disorder Assessment (RADA), on the other hand, had one study that analyzed its properties with sample of over 300 children aged between 11 and 18 in foster care (Lehhmann et al.; 2020).
The Development and Well-Being Assessment RAD/DSED (DAWBA) was evaluated in a study that included 122 children adopted from birth to 10 years of age (Lehhmann et al.; 2015). Finally, the Questionnaire Disorder Attachment Reactive (RAD-Questionnaire) is analyzed in two studies with samples of 55 children (Kliewer Neumann, et al., 2018) and 182 children (Minnis et al., 2002) in protective situations, between 12 months (Kliewer Neumann, et al., 2018) and 16 years (Minnis et al., 2002), all of whom had experienced various changes within the foster care resource, both residential and family. More detailed information on these aspects can be found in Table 2.
3.2. Methodological and measurement quality of the results of the instruments
In general terms, none of the works that evaluate the psychometric properties of the instruments present the eight relevant items indicated in the COSMIN Guide. None of the manuscript’s present cross-cultural validity indices, relation or comparison with the gold standard or responsiveness. The methodological quality of the chosen studies is summarized in Table 3.
- Disturbance Attachment Interview (DAI): In most cases, the focus is on structural validity and internal consistency. In this regard, two out of the four studies conducted structural validity analyses, with both employing confirmatory factor analysis. However, one of them (Kliewer-Neumann, et al., 2015) had a small sample size (< 5 times the number of items). Regarding criterion validity, one study examined it (Kliewer Neumann, et al., 2015). Concerning hypothesis testing and construct validity, various tests were conducted, but without establishing a priori hypotheses.
In terms of reliability (Test-Retest) and measurement error, only one study provided information (Kliewer Neumann, et al., 2015). As for consistency, two out of the four studies estimated Cronbach's alpha and inter-rater reliability (Kliewer Neumann et al., 2018; Smyke et al., 2002). Both studies achieved adequate inter-rater reliability. Regarding the internal consistency of the instrument, Smyke et al. (2002), the authors who developed the interview, obtained satisfactory internal consistency values.
In the case of the study by Kliewer-Neuman et al. (2018), it was not acceptable even after relevant statistical modifications. Thus, after removing item 5, an α= .72 was obtained on the DSED subscale, and on the secure base disturbance scale, α= 0.42 was obtained, which is insufficient. This study also assessed consistency over time with weighted kappa, although it was only performed in 30% of the interviews, yielding substantial results (0.61 to 0.80) (McHugh, 2012). Sufficient data were also provided to calculate the Limits of Agreement (LoA) for measurement error and information on concurrent validity, considering the relationship between DAI and the SDQ questionnaire that assesses emotional, behavioral, and hyperactive symptoms (Kliewer-Neumann et al., 2015).
The study by Kliewer Neumann et al. (2018) assessed the association between DAI and RAD, demonstrating concurrent validity with the inhibition subscale of DAI but not with disinhibition. In the case of the disinhibition scale, an association was found with tests related to the strange situation.
No study evaluated the transcultural validity of the instruments, nor responsiveness (Area under the Curve), and there were not enough studies testing hypotheses to calculate the percentage of agreement as established in the COSMIN criteria.
- The Preschool Age Psychiatric Assesment (PAPA): A study conducted by Seim et al. (2020) assessed the psychometric properties of the PAPA, focusing on criterion validity, measurement error, and discriminant validity. The study yielded favorable results regarding the two-factor factorial structure (inhibited and disinhibited) as well as discriminant validity. It was observed that RAD and DSED were distinct constructs from each other and from other mental health issues.
- Relationship Patterns Questionnaire (RPQ): A study conducted by Schöder et al. (2019) assessed the internal consistency and measurement error of the RPQ. The study reported adequate values for internal consistency (overall scale α = .82; inhibition subscale α = .75; disinhibition subscale α = .81). In terms of criterion validity analysis and responsiveness, calculations were performed in the study by Schröder et al. (2019). Significant Area Under the Curve (AUC) values were obtained, indicating diagnostic accuracy, with lower accuracy observed in boys compared to girls. The study also proposed diagnostic cut-off points.
- Reactive Attachment Disorder and Deshinhibited Social Engagement Disorder Assessment (RADA): One study assessed the psychometric properties of the RADA (Lehmann, Monette et al., 2020). It was focused on analyzing its factorial structure by proposing a three-construct factorial solution (DSED: indiscriminate behaviors with strangers; RAD1: inability to seek/accept comfort; RAD2: withdrawal/hypervigilance). The study also examined internal consistency and criterion and construct validity.
- Developmental and Well-Being Assessment RAD/DSED (DAWBA RAD/DSED): Lehmann et al. (2016) examines structural validity through a confirmatory factor analysis with two factors, consistent with the DSM-5 definition. Regarding construct validity, the study aimed to differentiate difficulties between SDQ, DSED, and RAD.
- RAD Questionnarie: Minnis et al. (2002) assessed structural validity, internal consistency, temporal consistency, measurement error, and criterion validity. Adequate indicators were obtained in all cases. Therefore, satisfactory internal consistency for the tool's use in research settings (α= 0.7) was achieved. The relationship between the questionnaire and the SDQ was tested, yielding very high correlations, which, in general terms, may not necessarily be positive.
On the other hand, the study by Kliewer Neumann et al. (2018) only examined hypothesis testing for construct validity without proposing an a priori hypothesis. Moderate relationships were observed between the RAD Questionnaire and the DAI.
3.3. Criteria measurement: quality of the instruments
The quality of the assessment measures was evaluated taking into account the updated criteria for good measurement properties outlined in the COSMIN manual [27].

Table 4.
COSMIN results of the criteria of measurement (quality of the PROM).
| Study and Instrument | Structural validity | Internal consistency | Crosscultural validity Measurement invariance |
Reliability | Measurement error | Criterion validity | Hypothesis testing for content validity |
Responsiveness |
|---|---|---|---|---|---|---|---|---|
| Kliewer Neumann, et al. (2018) – DAI | ? | ? | ? | + | ? | ? | + | ? |
| Kliewer Neumann, et al. (2015) – DAI | ? | + | - | ? | ? | + | ? | ? |
| Smyke et al. (2002) - DAI | ? | + | ? | + | ? | ? | ? | ? |
| Elovainio et al. (2015) - DAI | + | ? | ? | ? | ? | + | ? | ? |
| Seim et al. (2019) - PAPA | + | + | ? | ? | ? | + | ? | ? |
| Schröder et al. (2019) - RPQ | + | ? | ? | ? | + | ? | ? | |
| Lehhmann et al. (2020) – RADA | + | + | ? | ? | ? | + | ? | ? |
| Lehmann et al. (2015) - DAWBA | + | ? | ? | ? | ? | ? | ? | ? |
| Kliewer-Neumann, et al. (2018) – RAD | ? | ? | ? | ? | ? | ? | + | ? |
| Minnis et al. (2002) - RAD | + | ? | ? | ? | ? | + | ? | ? |
| Note: | ||||||||
 | ||||||||
3.4. Strength of evidence
Referring to Table 5, it can be observed that none of the studies provided information for all nine criteria in the COSMIN checklist. According to the modified GRADE criteria (Prinsen et al., 2018), most instruments exhibited low to moderate evidence.
4. Discussion
The main objective of this systematic review was to evaluate the psychometric properties of assessment instruments for Reactive Attachment Disorder (RAD) and Disinhibited Social Engagement Disorder (DSED) in minors under protective measures through a systematic review following the COSMIN checklist (Mokkink et al., 2010). As a primary finding, we note that the general trend in the examined studies is to report on internal consistency and structural validity. Additionally, the majority conducted hypothesis testing for construct validity, but without a priori hypotheses. Overall, there is a lack of evidence regarding reliability, cross-cultural validity, measurement error, and responsiveness. Therefore, we conduct an exhaustive analysis of the instruments, though it may be limited due to the nature of the studies.
To date, this is the first study evaluating the psychometric properties of instruments assessing RAD and DSED in under protective measures minors. Consequently, our results are challenging to compare with previous works. However, the study by Wright et al. (2015), which conducted a systematic review and meta-analysis on instruments assessing and/or diagnosing attachment problems, concluded that assessments of the psychometric properties of these instruments often neglect cross-cultural validity or longitudinal reliability. Therefore, more high-quality scientific research is needed to examine the validity of available instruments and provide sufficient evidence for their consideration in clinical diagnosis.
As far as we know, the reliability indices of different instruments, while mostly adequate (alpha between .70 and .82), are not sufficient to use the tools as diagnostic instruments for RAD/DSED. Most studies support the two-factor RAD and DSED factorial structure, but some authors suggest the existence of three factors (DSED: indiscriminate behaviors with strangers; RAD1: inability to seek/accept comfort; RAD2: withdrawal/hypervigilance) (Lehmann, Monette et al., 2020; Lehmann, Breivik et al., 2020), in line with the proposals of the DSM-5-TR and opening avenues for further research into a potential new diagnostic category associated with RAD. However, much more evidence and research are needed in this regard.
Furthermore, it is necessary for studies to conduct cross-cultural investigations testing the functioning of instruments in different countries. Despite studies being conducted in various countries such as Germany (Kliewer Neumann, et al., 2018; Kliewer Neumann, et al., 2015; Schröder et al., 2019), Norway (Seim et al., 2019; Lehhmann et al., 2018; Lehmann et al., 2020; Lehmann et al., 2015), Scotland (Minnis et al., 2002), Romania (Smyke et al., 2002), Belgium (Vervoot et al., 2013), and Finland (Elovainio et al., 2015), there is a lack of evidence for cross-cultural construct validity through multigroup structural equation modeling. Additionally, some studies focus on assessment interviews for these disorders, providing only evidence of inter-rater reliability (Kliewer et al., 2018). Therefore, future research should assess internal consistency over time, content and construct validity, cross-cultural validity, and the structure, efficacy, and efficiency of interviews.
Despite the significant contributions of this work, evaluating key RAD/DSED detection measures in protective minors, it is essential to acknowledge limitations. Strict selection criteria may have limited the scope of the review, as only works published in Spanish and English were considered. The COSMIN checklist (Mokkink et al., 2010), while enhancing the structure and quality of our work, leaves room for subjectivity in data interpretation and quality assessment. Future research should replicate the search in other databases to provide additional information. For example, in criteria where evaluation is based on a time period, it depends on the construct being assessed and what the researcher deems appropriate. Furthermore, even with adequate reliability, a high Cronbach's alpha does not guarantee that the desired construct is being measured or that no essential concepts are missing. Similarly, having high test-retest reliability or responsiveness does not imply that all items are important or that central concepts have not been overlooked. This highlights the possibility of assessing an incomplete or incorrect construct reliably when following the checklist.
On the other hand, research on reactive attachment disorder is limited, resulting in few studies delving into its assessment and even fewer evaluating the psychometric properties of assessment instruments. This limitation is particularly pronounced when considering studies focused on minors under protection, who, as we know, are more susceptible to experiencing RAD/DSED than minors outside the protection system (Talmon-Knuser et al., 2023). Finally, it is important to note that the search was conducted solely in one database, the one that aggregates a greater number of impactful publications. Nevertheless, future studies should replicate this search in other databases to contribute additional information on the subject.
However, this work contributes to expanding knowledge about assessment instruments for reactive attachment disorder in the context of child protection, laying the groundwork for future assessments of the psychometric properties of these instruments. Having identified areas for improvement in assessing the psychometric properties of these instruments, future studies could be designed with a cross-cultural and longitudinal approach to gather more scientific evidence in line with COSMIN checklist criteria, including measurement error, cross-cultural validity, test-retest reliability, responsiveness, criterion validity, and construct validity (Mokkink et al., 2010). In this way, progress can be made in understanding, assessing, and treating RAD/DSED. In conclusion, we note that this is the first study to examine and assess the psychometric properties of six instruments that assess RAD/DSED in a sample of adopted or foster children and adolescents. Regarding the evaluated measures, it can be concluded that all of them exhibit good structural validity, adequate internal consistency, and generally positive results with respect to measurement error.
Author Contributions
Conceptualization, M.S. and F.G-S..; methodology, M.S., L.L-T. and F.G-S; software, M.S., L.L-T. and F.G-S; investigation, M.S., L.L-T., F.G-S P.S-G; writing—original draft preparation, L.L-T. and F.G-S; writing—review and editing, F.G-S, L.L-T., P.S-G., supervision, F.G-S, L.L-T., P.S-G.; project administration, F.G-S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bowlby, J. The Diagnosis and Treatment of Psychological Disorders in Childhood. Health Education Journal 1954, 12, 59–68. [Google Scholar] [CrossRef]
- Zeanah CH, Gleason, MM. Annual Research Review: Attachment disorders in early childhood - clinical presentation, causes, correlates, and treatment. J Child Psychol Psychiatry 2015, 56, 207–222. [Google Scholar] [CrossRef] [PubMed]
- Main, M. Introduction to the special section on attachment and psychopathology: 2. Overview of the field of attachment. J Consult Clin Psychol 1996, 64, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Fresno, A.; Spencer, R.; Retamal, T. Maltrato infantil y representaciones de apego: defensas, memoria y estrategias, una revisión. Universitas Psychologica 2012, 11, 829–838. [Google Scholar]
- Ellis, E. E.; Yilanli, M.;Saadabadi, A. Reactive Attachment Disorder. In StatPearls. StatPearls Publishing, 2023.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders(5-TR ed.). Washington, DC: American Psychiatric Association, 2022.
- Moran K, Dyas R, Kelly C; et al. Reactive Attachment Disorder, Disinhibited Social Engagement Disorder, adverse childhood experiences, and mental health in an imprisoned young offender population. Psychiatry Research 2023, 115597. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, S; Breivik, K; Monette, S; Minnis, H. Potentially traumatic events in foster youth, and association with DSM-5 trauma- and stressor related symptoms. Child Abuse Negl 2020, 101, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Turner, M; Beckwith, H; Duschinsky, R; Forslund, T; Foster, SL.; Coughlan, B.; Pal, S.; Schuengel, C. Attachment difficulties and disorders. InnovAiT 2019, 12, 173–179. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (4th ed.). American Psychiatric Publishing, 1994.
- Jorjadze N, Bovenschen I, Spangler G. Attachment Representations, and Symptoms of Reactive Attachment Disorder and Disinhibited Social Engagement Disorder in Foster Children With Different Preplacement Experiences. Devel child welf 2023, 5, 138–157. [Google Scholar] [CrossRef]
- Zilberstein, K. Clarifying core characteristics of attachment disorders. Am J Orthopsychiatry 2006, 76, 55–64. [Google Scholar] [CrossRef]
- Gleason, MM.; Fox, NA.; Drury, S.; Smyke, A.; Egger, HL.; Nelson, CA.; Gregas, MC.; Zeanah, CH. Validity of evidence-derived criteria for Reactive Attachment Disorder: Indiscriminately Social/Disinhibited and Emotionally Withdrawn/Inhibited types. J Am Aca Child Adol Psychiatry 2011, 50, 216–231. [Google Scholar] [CrossRef]
- Lehmann, S.; Breivik, K.; Heiervang, ER.; Havik, T.; Havik, OE. Reactive Attachment Disorder and Disinhibited Social Engagement Disorder in school-aged foster children - a confirmatory approach to dimensional measures. J Abnorm Child Psychol 2016, 44, 445–457. [Google Scholar] [CrossRef]
- Zilberstein, K. One piece of the puzzle: Treatment of fostered and adopted children with RAD and DSED. Adoption & Fostering 2023, 47, 40–57. [Google Scholar]
- Kay, C.; Green, J.; Sharma, K. Disinhibited Attachment Disorder in UK adopted children during middle childhood: Prevalence, validity and possible developmental rigin. J Abnorm Child Psychol 2016, 44, 1375–1386. [Google Scholar] [CrossRef]
- Coughlan B, Woolgar M, Van Ijzendoorn M.H, Duschinsky R. Socioemotional profiles of autism spectrum disorders, attention deficit hyperactivity disorder, and disinhibited and reactive attachment disorders: A symptom comparison and network approach. Development and psychopathology 2023, 35, 1026-1035. [CrossRef]
- Kroupina MG, Dahl C.M, Nakitende AJ, Elison KC. Reactive attachment disorder (RAD) and disinhibited social engagement disorder (DSED) symptomatology in a high-risk clinical sample. Clinical pediatrics 2023, 62, 760-768. [CrossRef]
- Muzi S, Pace CS. Attachment and alexithymia predict emotional–behavioural problems of institutionalized, late-adopted and community adolescents: An explorative multi-informant mixed-method study. Clinical Psychology & Psychotherapy 2023. [Google Scholar]
- Davies, J; Glinn, L; Osborne, LA; Reed, P. Exploratory study of parenting differences for autism spectrum disorder and attachment disorder. Journal of Autism and Developmental Disorders 2023, 53, 2143–2152. [Google Scholar] [CrossRef]
- Oliveira PS, Fearon P, Belsky J; et al. Neural correlates of face familiarity in institutionalised children and links to attachment disordered behaviour. Journal of child psychology and psychiatry 2023, 64, 736–746. [Google Scholar] [CrossRef]
- Page, MJ.; Moher, D.; Bossuyt, PM.; Boutron, I.; Hoffmann, TC.; Mulrow, CD.; Shamseer, L.; Tetzlaff, JM.; Akl, EA.; Brennan, SE.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Santos, CM.; Pimenta, CA.; Nobre, MR. The PICO strategy for the research question construction and evidence search. Rev Latino-am Enfermagem 2007, 15, 508–11. [Google Scholar] [CrossRef]
- Covidence systematic review software. Veritas Health Innovation, Melbourne, Australia. https://www.covidence.org. Accessed 22 Feb 2023.
- Ogrinc G, Davies L, Goodman D, Batalden P, Davidoff F, Stevens D. SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence): Revised Publication Guidelines From a Detailed Consensus Process. J Nurs Care Qual 2016, 31, 1-8. [CrossRef]
- Orwin, R. G. Evaluating coding decisions. In The handbook of research synthesis; Russell Sage Foundation, EEUU, 2018. pp. 95-107.
- Hernández-Nieto, RA. Contributions to Statistical Analysis: The Coefficients of Proportional Variance, Content Validity and Kappa. CreateSpace Independent Publishing Platform, 2002.
- Smyke AT, Zeanah CH. Disturbances of attachment interview. New Orleans: Tulane University; 1999 (Unpublished Manual).
- Angold, A.; Prendergast, M.; Cox, A.; Harrington, R.; Simonoff, E.; Rutter, M. The child and adolescent psychiatric assessment (CAPA). Psychol Med 1995, 25, 739–753. [Google Scholar] [CrossRef]
- Minnis, H.; Green, J.; O’Connor, T.; Liew, A.; Glaser, D.; Taylor, E.; Follan, M.; Young, D.; Barnes, J.; Gillberg, C.; Pelosi, A.; Arthur, J.; Burston, A.; Connolly, B.; Sadiq, F.A. An exploratory study of the association between reactive attachment disorder and attachment narratives in early school-age children. J Child Psychol Psychiatry 2009, 50, 931–942. [Google Scholar] [CrossRef]
- Lehmann, S.; Monette, S.; Egger, H.; Breivik, K.; Young, D.; Davidson, C.; Minnis, H. Development and examination of the reactive attachment disorder and disinhibited social engagement disorder assessment interview. Assessment 2020, 27, 749–765. [Google Scholar] [CrossRef]
- Kurth, R.A.; Körner, A.; Geyer, M.; Pokorny, D. Relationship Patterns Questionnaire (RPQ): Psychometric properties and clinical applications. Psychotherapy Research 2004, 14, 418–434. [Google Scholar] [CrossRef]
- Corval, R.; Baptista, J.; Fachada, I.; Soares, I. Rating of inhibited attachment disordered behavior. Unpublished manuscript, Universidade do Minho, 2016.
- Elovainio, M.; Raaska, H.; Sinkkonen, J.; Makipaa, S.; Lapinleimu, H. Associations between attachment-related symptoms and later psychological problems among international adoptees: results from the FinAdo study. Scand J Psychol 2015, 56, 53–61. [Google Scholar] [CrossRef]
- Coughlan, B.; Woolgar, M.; Van Ijzendoorn, MH.; Duschinsky, R. Socioemotional profiles of autism spectrum disorders, attention deficit hyperactivity disorder, and disinhibited and reactive attachment disorders: a symptom comparison and network approach. Dev Psychopathol 2021, 35, 1026–1035. [Google Scholar] [CrossRef]
- Giltaij, HP.; Sterkenburg, PS.; Schuengel, C. Psychiatric diagnostic screening of social maladaptive behaviour in children with mild intellectual disability: differentiating disordered attachment and pervasive developmental disorder behaviour. J Intellec Disabil Res 2015, 59, 138–149. [Google Scholar] [CrossRef]
- Hong, M.; Moon, DS.; Chang, H.; Lee, SY.; Cho, SW.; Lee, K.; Bahn, GH. Incidence and comorbidity of Reactive Attachment Disorder: Based on national health insurance claims data, 2010–2012 in Korea. Psychiatry Investig 2018, 15, 118–123. [Google Scholar] [CrossRef]
- Sadiq, FA.; Slator, L.; Skuse, D.; Law, J.; Gillberg, C.; Minnis, H. Social use of language in children with reactive attachment disorder and autism spectrum disorders. Eur Child Adolesc Psychiatry 2012, 21, 267–276. [Google Scholar] [CrossRef]
- Bosmans, G.; Spilt, J.; Vervoort, E.; Verschueren, K. Inhibited symptoms of Reactive Attachment Disorder: links with working models of significant others and the self. Attach Hum Dev 2019, 21, 190–204. [Google Scholar] [CrossRef]
- Bruce, M.; Young, D.; Turnbull, S.; Rooksby, M.; Chadwick, G.; Oates, C.; et al. Reactive Attachment Disorder in maltreated young children in foster care. Attach Hum Dev 2019, 21, 152–169. [Google Scholar] [CrossRef]
- Davidson, C.; O’Hare, A.; Mactaggart, F.; Green, J.; Young, D.; Gillberg, C.; et al. Social relationship difficulties in autism and reactive attachment disorder: Improving diagnostic validity through structured assessment. Res Dev Disabil 2015, 40, 63–72. [Google Scholar] [CrossRef]
- Guyon-Harris, KL.; Humphreys, KL.; Fox, NA.; Nelson, CA.; Zeanah, CH. Signs of attachment disorders and social functioning among early adolescents with a history of institutional care. Child Abuse Negl 2019, 88, 96–106. [Google Scholar] [CrossRef]
- Jonkman, CS.; Oosterman, M.; Schuengel, C.; Bolle, EA.; Boer, F.; Lindauer, RJ. Disturbances in attachment: inhibited and disinhibited symptoms in foster children. Child Adolesc Psychiatry Ment Health 2014, 15, 1–7. [Google Scholar] [CrossRef]
- Kocovska, E.; Puckering, C.; Follan, M.; Smillie, M.; Gorski, C.; Lidstone, E.; Pritchett, R.; Hockaday, H.; Minnis, H. Neurodevelopmental problems in maltreated children referred with indiscriminate friendliness. Res Dev Disabil 2012, 33, 1560–1565. [Google Scholar] [CrossRef]
- Mayes, SD.; Calhoun, SL.; Waschbusch, DA.; Breaux, RP.; Baweja, R. Reactive attachment/disinhibited social engagement disorders: Callous-unemotional traits and comorbid disorders. Res Dev Disabil 2017, 63, 28–37. [Google Scholar] [CrossRef]
- Moran, K.; McDonald, J.; Jackson, A.; Turnbull, S.; Minnis, H. A study of Attachment Disorders of young offenders attending specialist services. Child Abuse Negl 2017, 65, 77–87. [Google Scholar] [CrossRef]
- Raaska, H.; Lapinleimu, H.; Sinkkonen, J.; Salmivalli, C.; Matomäki, J.; Mäkipää, S.; et al. Experiences of School Bullying Among Internationally Adopted Children: Results from the Finnish Adoption (FINADO) Study. Child Psychiatry Hum Dev 2012, 43, 592–611. [Google Scholar] [CrossRef]
- Seim, AR.; Jozefiak, T.; Wichstrøm, L.; Lydersen, S.; Kayed, NS. Self-esteem in adolescents with reactive attachment disorder or disinhibited social engagement disorder. Child Abuse Negl 2021, 118, 1–13. [Google Scholar] [CrossRef]
- Seim, AR.; Jozefiak, T.; Wichstrøm, L.; Lydersen, S.; Kayed, NS. Reactive attachment disorder and disinhibited social engagement disorder in adolescence: co-occurring psychopathology and psychosocial problems. Eur Child Adolesc Psychiatry 2022, 31, 85–98. [Google Scholar] [CrossRef]
- Shimada, K.; Takiguchi, S.; Mizushima, S.; Fujisawa, TX.; Saito, DN.; Kosaka, H.; et al. Reduced visual cortex grey matter volume in children and adolescents with reactive attachment disorder. NeuroImage Clinical 2015, 9, 13–19. [Google Scholar] [CrossRef]
- Zimmermann, P.; Iwanski, A. Attachment Disorder behavior in early and middle childhood: associations with children's self-concept and observed signs of negative internal working models. Attach Hum Dev 2019, 21, 170–189. [Google Scholar] [CrossRef]
- Pritchett, R.; Pritchett, J.; Marshall, E.; Davidson, C.; Minnis, H. Reactive Attachment Disorder in the general population: A hidden ESSENCE disorder. Scientific World Journal 2013, 2013, 1–6. [Google Scholar] [CrossRef]
- Vervoort, T.; Trost, Z.; Van Ryckeghem, D. M. L. Children’s selective attention to pain and avoidance behaviour: The role of child and parental catastrophizing about pain. Pain 2013, 154, 1979–1988. [Google Scholar] [CrossRef]
- Vervoort, E.; Bosmans, G.; Doumen, S.; Minnis, H.; Verschueren, K. Perceptions of self, significant others, and teacher–child relationships in indiscriminately friendly children. Res Dev Disabil 2014, 35, 2802–2811. [Google Scholar] [CrossRef]
- Egger, HL.; Erkanli, A.; Keeler, G.; Potts, E.; Walter, BK.; Angold, A. Test-Retest Reliability of the Preschool Age Psychiatric Assessment (PAPA). J Am Acad Child Adolesc Psychiatry 2006, 45, 538–549. [Google Scholar] [CrossRef]
- World Health Organization. The ICD-10: Version 2010. Classification of Mental and Behavioral Disorders: Diagnostic Criteria for Research. Geneva. 2010.
- World Health Organization. The ICD-10 Classification of Mental and Behavioral Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva, Switzerland: World Health Organization, 1992.
- World Health Organisation. The ICD-10 classification of mental and behavioural disorders: diagnostic criteria for research. World Health Organisation, Geneva. 1993.
- Vasquez, M.; Miller, N. Aggression in Children With Reactive Attachment Disorder: A sign of deficits in emotional regulatory processes? J Aggress, Maltreat Trauma 2018, 27, 347–366. [Google Scholar] [CrossRef]
- Corbin, J. Reactive Attachment Disorder: A biopsychosocial Disturbance of Attachment. Child Adolesc Soc Work J 2007, 24, 539–552. [Google Scholar] [CrossRef]
- Schore, JR.; Schore, AN. Modern attachment theory: The central role of affect regulation in development and treatment. Clin Soc Work J 2008, 36, 9–20. [Google Scholar] [CrossRef]
Figure 1.
Flow of information through the different phases of a systematic review.
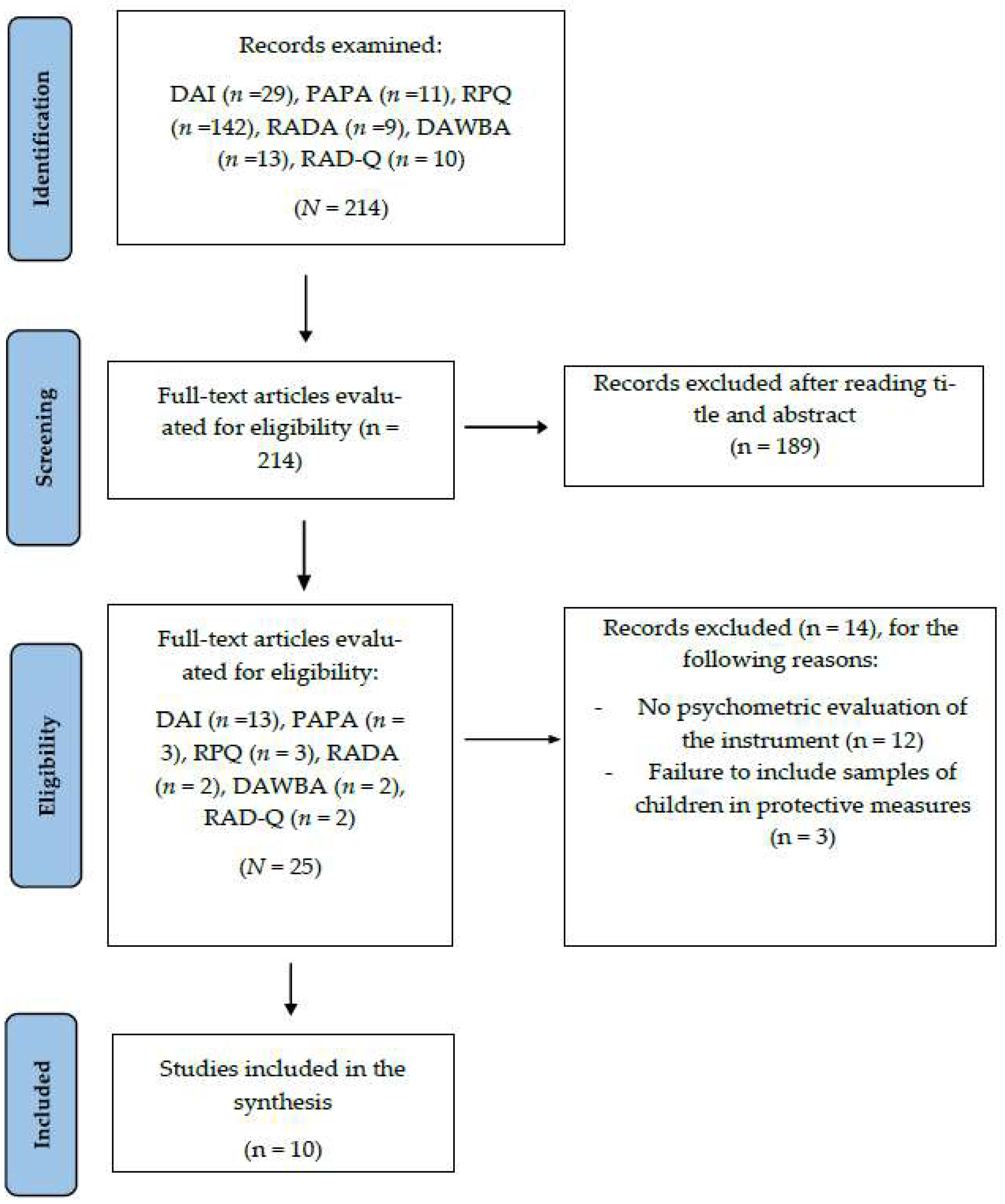
Table 1.
Keywords used for the Boolean search.
| Questionnaires | Psychometric Properties | Samples | ||
|---|---|---|---|---|
| Disturbance Attachment Interview OR DAI The Preschool Age Psychiatric Assessment OR PAPA Relationship Patterns Questionnaire OR RPQ Reactive Attachment Disorder and Disinhibited Social Engagement Disorder Assessment OR RADA Developmental and Well-Being Assessment RAD/DSED OR DAWBA RAD/DSED Questionnaire Disorder Attachment Reactive OR RAD Questionnaire |
AND | validity OR measurement error OR reliability OR invariance OR cross OR retest OR consistence OR responsive |
AND | foster* OR adopt* OR residential foster care |
Table 2.
Characteristics of samples used in published scientific articles on psychometric properties of questionnaires assessing RAD and DSED.
Table 2.
Characteristics of samples used in published scientific articles on psychometric properties of questionnaires assessing RAD and DSED.
| Article & Instrument | N | Characteristics of samples |
| Kliewer et al. (2018) – DAI | 55 | Foster children from German youth welfare programs. The children ranged in age from 12 to 82 months (M=35.87; SD=18.37), with 50.9% being female (n=28). These children had been in foster care for an average of 78 days, and some of them had experienced up to 5 changes in placement or families. |
| Kliewer et al. (2015) – DAI | 50 | Foster children aged between 34 and 104 months (M=68.32; SD=19.29), with 48% being female (n=24). The children had been living with their foster families for an average of 45.36 months. |
| Smyke et al. (2002) – DAI | 94 | Children residing in a large institution in Bucharest (n=32), young children residing in the same institution but in a pilot unit (n=29), and young children living in foster care who had never been institutionalized (n=33). All children ranged in age from 4 months to 68 months. |
| Elovainio et al. (2015) - DAI | 853 | Boys and girls adopted as part of a Finnish adoption study (FinAdo), involving international adoption. The participants' ages ranged from 6 to 15 years (M=8.5; SD=2.9), and they had been adopted for an average of 2.4 years (SD=1.3). Prior to adoption, they had experienced various placement resources, including foster care, residential care, among others. An adapted version of the DAI was administered. |
| Seim et al. (2020) - PAPA | 400 | Adolescents aged between 12 and 23 years, residing in Norwegian residential centers. The participants had a mean age of M=16.7 (SD=3.9), an average of 3.3 out-of-home placements (SD=2.4), and the mean age of their first out-of-home placement was 12.5 years (SD=3.9). |
| Schröder et al. (2019) – RPQ | 135 | The sample comprised a total of 135 children, with a mean age of 7.17 years (SD=1.40). The sample divided participants into three groups: general population (n=34), with a mean age of 6.36 years (SD=1.06); hospitalized and outpatient patients (n=69), with a mean age of 7.39 years (SD=1.42); and the foster care group (n=32), with a mean age of 7.52 years (SD=1.42). |
| Lehhmann, Monette et al. (2020) - RADA | 320 | Youth living in foster care for an average of 6.6 years (SD=4.3), aged between 11 and 17 years (M=14.8, SD=2.0), with 56.8% being boys. |
| Lehmann et al. (2015) - DAWBA | 122 | Adopted children aged between 0 and 10 years in Norway, of which 57% were girls. |
| Kliewer et al. (2018) – RAD Questionnaire | 55 | Foster children from German youth welfare programs. The children ranged in age from 12 to 82 months (M=35.87; SD=18.37), with 50.9% being female (n=28). These children had been with their foster families for an average of 78 days, and some of them had experienced up to 5 changes in placement or families. |
| Minnis et al. (2002) – RAD Questionnaire | 182 | Scottish children residing in foster homes aged between five and sixteen years (M=11) and had spent an average of 2.5 years with their current foster caregivers. |
Table 3.
Psychometric properties and methodological quality of the instruments according to the COSMIN guidelines.
Table 3.
Psychometric properties and methodological quality of the instruments according to the COSMIN guidelines.
| Psychometric property | Articles | Psychometric property | Articles |
|---|---|---|---|
| Structural validity | Measurement error | ||
| Excellent | 4,5,7,8,10 | Excellent | |
| Good | Good | ||
| Fair | Fair | ||
| Poor | Poor | ||
| Unknown/NA | 1,3,10 | Unknown/NA | 1,2,3,4,6,7,8,9,10 |
| Internal consistency | Criterion validity | ||
| Excellent | 2,3,5,6,7,10 | Excellent | 2,4,5,6,7,10 |
| Good | Good | ||
| Fair | Fair | ||
| Poor | Poor | ||
| Unknown/NA | 1,4,8 | Unknown/NA | 1,3,8,11 |
|
Cross-cultural validity/ measurement invariance |
Hypothesis testing for construct validity | ||
| Excellent | Excellent | 1 | |
| Good | Good | 9 | |
| Fair | Fair | ||
| Poor | Poor | ||
| Unknown/NA | 1,2,3,4,5,6,7,8,9,10 | Unknown/NA | 2,3,4,5,6,7,8,9,10 |
| Reliability | Responsiveness | ||
| Excellent | 1,3,10 | Excellent | |
| Good | Good | ||
| Fair | Fair | ||
| Poor | Poor | ||
| Unknown/NA | 1,3,4,5,6,7,8,9 | Unknown/NA | 1,2,3,4,5,6,7,8,9,10 |
Note: DAI: (1): Kliewer Neumann, et al. (2018); (2): Kliewer Neumann, et al. (2015); (3): Smyke et al. (2002); (4) Elovaino et al. (2015); PAPA (5) Seim et al. (2020); RPQ: (6) Schröder et al. (2019); RADA: (7) Lehmann et al. (2020); DAWBA: (8) Lehmann et al. (2016); RAD Questionnaire: (9) Kliewer Neumann et al. (2018); (10) Minnis et al. (2002). NA: Not applicable.
Table 5.
Strength of evidence of each study.
| Study and Instrument | Structural validity | Internal consistency | Crosscultural validity/ Measurement invariance |
Reliability | Measurement error | Criterion validity | Hypothesis testing for content validity |
Responsi veness |
% strong- moderate evidence |
Average percentage evidence of instruments |
|---|---|---|---|---|---|---|---|---|---|---|
| Kliewer Neumann, et al. (2018) – DAI | U | U | U | S | U | U | S | U | 25% | 28.13% |
| Kliewer Neumann, et al. (2015) – DAI | U | S | M | U | U | S | U | U | 37.5% | |
| Smyke et al. (2002) - DAI | U | S | U | S | U | U | U | U | 25% | |
| Elovainio et al. (2015) - DAI | S | U | U | U | U | S | U | U | 25% | |
| Seim et al. (2019) - PAPA | S | S | U | U | U | S | U | U | 37.5% | 37.5% |
| Schröder et al. (2019) - RPQ | U | S | U | U | U | S | U | U | 25% | 25% |
| Lehmann, Breivik et al. (2020) – RADA | S | S | U | U | U | S | U | U | 37.5% | 37.5% |
| Lehmann et al. (2015) - DAWBA | S | U | U | U | U | U | U | U | 12.5% | 12.5% |
| Kliewer Neumann, et al. (2018) – RAD | U | U | U | U | U | U | S | U | 12.5% | 18.7% |
| Minnis et al. (2002) - RAD | S | U | U | U | U | S | U | U | 25% | |
| % strong-moderate evidence |
40% | 50% | 0% | 20% | 0% | 60% | 20% | 0% | ||
| % limited conflicting evidence |
0% | 0% | 0% | 80% | 0% | 0% | 0% | 0% | ||
| % unknown evidence | 50% | 50% | 90% | 80% | 100% | 40% | 80% | 100% | ||
 | ||||||||||
Note: Right hand column represents the % of strong-moderate evidence for each article, bottom row indicated the strength of evidence for each psychometric characteristic evaluated by COSMIN.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



