
Submitted:
25 December 2023
Posted:
26 December 2023
You are already at the latest version
Abstract
Chronic hepatitis B virus (HBV) infection is the largest global cause of hepatocellular carcinoma (HCC). Current HBV treatment options include pegylated interferon-alpha and nucleos(t)ide analogues (NAs), which have been shown to be effective in reducing HBV DNA levels to become undetectable. However, literature has shown that some patients have persistent risk of developing HCC. The mechanism in which this occurs is not fully elucidated, however it has been discovered that HBV covalently closed circular DNA (cccDNA) integrates into critical HCC driver genes in hepatocytes upon initial infection and are not targets of current NA therapy. Some studies suggest that HBV undergoes compartmentalization in peripheral blood mononuclear cells that serve as a sanctuary for replication during antiviral therapy. The aim of this review is to expand on how patients with HBV may develop HCC despite years of HBV viral suppression and carry worse prognosis than treatment-naive HBV patients who develop HCC. Furthermore, HCC recurrence after initial surgical or locoregional treatment in this setting may cause carcinogenic cells to be-have more aggressively in the treatment experienced. Curative novel therapies targeting the life cycle of HBV, modulating the host immune response, and inhibiting HBV RNA translation are being investigated.
Keywords:
Hepatitis B virus
; Hepatocellular Carcinoma
; nucleoside analog
; antiviral therapy
; hepatitis cure
; cccDNA
1. Introduction
Hepatitis B virus (HBV) is a global public health problem with an estimated 350 million chronic hepatitis B carriers and causing 820,000 deaths in 2019 alone [1-3]. HBV is endemic in many parts of the world, including Southeast Asia, China, and Africa [4]. It belongs to a family of DNA viruses called hepadnaviruses which is composed of at least ten genotypes, A-J [2,5,6]. The virion is an enveloped nucleocapsid that delivers an incomplete circular DNA genome into the host cell, initiating viral replication [7]. HBV is a dynamic, hepatotropic virus and its infection has a wide spectrum of clinical manifestations [7]. Fifteen to forty percent of HBV-infected patients develop cirrhosis, liver failure, or hepatocellular carcinoma (HCC) [1,8]. In fact, HBV is the most common hepatocarcinogen, being accountable for 25% of HCC in developed countries and 60% in developing countries [9,10,11,12]. There is a limited understanding of the pathogenesis, prognosis, and treatment strategies for HBV-associated HCC which we will highlight in this review paper.
2. HBV Pathophysiology and Hepatocarcinogenesis
HBV is transmitted by percutaneous inoculation or transmission of infectious bodily fluids. In high-prevalence areas, mother-to-child transmission is the predominant mode of transmission while unprotected sex and injection drug use are the common modes of transmission in low prevalence areas [13,14]. The incubation period of HBV is between 30 and 180 days. During infection, complete and incomplete viral particles are released into the serum of the host, facilitating viral replication [15].
HBV is a non-cytopathic virus, and the liver damage associated with HBV is caused by the host immune response [16,17]. During acute infection, host immune cells, most prominently CD8 T cells, kill infected cells, inducing hepatic inflammation [4,18]. Around 70% of patients with acute HBV have subclinical or anicteric hepatitis, while 30% have icteric hepatitis [19]. The clearance of HBV is mediated by the adaptive immune system and HBV utilizes multiple strategies to evade this line of defense [19-21]. Hypo-responsiveness of HBV-specific T cells may also contribute to persistent HBV infection [21]. While recovery commonly occurs in immunocompetent individuals, a small proportion of those infected can progress to chronic HBV, which is defined as the presence of HBsAg for greater than six months [22].
There are four phases of chronic hepatitis B (CHB) infection: immune tolerance, immune clearance, immune control, and immune escape/reactivation [23]. In the immune tolerance phase, ALT levels are still low, viral DNA levels are high (usually at least 2,000,000 IU/mL), and there is minimal or no inflammation on liver biopsy [4,18,23-26]. This phase may last for a few years to around 30 years [27,28]. In the immune clearance phase, hepatitis B e antigen (HBeAg) is positive, there is intermittent or persistent elevation of ALT levels, elevated HBV DNA levels (at least 2000 IU/mL), and some degree of inflammation or fibrosis on liver biopsy [23,28]. In this phase, HBV-specific CD8 T cells directly attack infected hepatocytes and recruit other immune cells to the liver, which further exacerbate hepatic injury [4,17,18,26,29]. During immune clearance, patients may present with flares which although are often asymptomatic, may be characterized by signs of acute hepatitis. During flares, ALT levels may be elevated to greater than 5-times the upper limit of normal [23,30]. The end of the immune clearance phase and beginning of immune control is marked by seroconversion, which is the loss of HBeAg and development of antibodies to hepatitis B e antigen (HBeAb). Intriguingly, the duration of the immune clearance phase has a critical association with the development of complications; those who seroconvert after the age of 40 have a significantly higher risk of cirrhosis, HCC, and CHB compared to those who seroconverted before the age of 30 [23,31]. In addition, HBeAg positivity is a known risk factor for HCC [26,32]. The immune control phase is characterized by lower levels of HBV DNA (usually < 2000 IU/mL) and ALT, although HBsAg remains [4,18,23]. Some patients, even after seroconversion, may continue to have moderate levels of viral replication with associated abnormal ALT, leading to eventual reactivation of the immune active phase; this phenomenon is known as immune escape [23,28,33,34]. Resolution of infection is indicated by disappearance of HBsAg [4,18].
In CHB, there are crucial changes in immune cell activity and function involving both the innate and adaptive immune systems that lead to hepatic inflammation and hepatocyte killing [17]. Chronic infection may progress to liver fibrosis, cirrhosis, and HCC [17,35]. HBV-mediated carcinogenesis is a complex process that involves viral DNA integration into the host genome, ultimately leading to viral manipulation of cell-signaling and proliferation. This leads to a cascade of events which converts normal hepatocytes into malignant cells [36-39]. Oxidative stress associated with viral hepatitis changes the cellular environment in such a way that promotes carcinogenesis. Overproduction of free radicals and reactive oxidative species leads to the upregulation of inflammatory pathways that result in hepatocyte release of cytokines and chemokines that recruit neutrophils, monocytes, and lymphocytes [18,37,40,41]. As inflammation persists, immune cells, including macrophages and myeloid-derived suppressor cells, become dysfunctional, further amplifying the pro-inflammatory environment. The chronic inflammatory state leads to compensatory hepatocyte proliferation, which leads to accumulation of mutations that promote cell growth and proliferation which predisposes the host to developing HCC (Figure 1) [40,42].
Moreover, it was found that the incidence of HCC is fivefold higher among HBV-infected patients with cirrhosis compared to asymptomatic carriers, indicating that cirrhosis may be a pre-malignant condition [38]. Indeed, fibrosis of the liver disrupts the normal architecture which leads to modification of cell-cell interactions and ultimately, loss of regulation over cell proliferation [38].
Furthermore, it is important to note that numerous factors including host characteristics, HBV genotype, viral mutations, viral load and HBsAg levels all influence the clinical manifestations of HBV infection [6]. Research has shown that there are differences between the various genotypes of HBV in tendency of chronicity, primary mode of transmission, timing of seroconversion, timing of HBsAg clearance, and clinical outcomes [6]. For example, multiple studies have shown that genotype C tends to cause more severe liver disease, including cirrhosis and HCC, compared to other genotypes [6,43,44]. Genotype C also has higher serum HBV levels and was shown to cause DNA mutations more frequently than Genotype B [6,45]. Further research investigating the utility of routine HBV genotyping is needed before implementation into clinical practice.
3. HCC Risk Factors and Surveillance
HCC is one of the major malignant diseases in the world today and ranks fifth in overall frequency. Its incidence is high in Eastern Asia, sub-Saharan Africa and increasing in many parts of the Western world [46]. Unfortunately, the annual mortality from HCC is close to its incidence because of its rapid progression and poor prognosis. Additionally, the therapeutic interventions available at time of diagnosis are generally ineffective. Thus, the focus has been on early screening and treatment of known causes, including chronic hepatitis B which is the most frequent underlying cause of HCC. There are several major risk factors for development of HCC in chronic HBV infection. While having a first-degree relative with HCC, metabolic syndrome, type 2 diabetes, and central obesity are all host factors that have been linked to HCC development in HBV-infected patients or carriers, it appears that liver cirrhosis has been consistently identified to be the most significant risk factor for development of HCC during nucleos(t)ide therapy [47-51]. Studies indicate that the presence of male gender, increasing age, higher HBV DNA level, and core promoter mutations are also independently associated with HCC risk [52,53]. It is postulated that androgens may play a role in the observed difference in incidence of HCC based on gender [54]. While less investigated, concurrent HCV or HIV infection has also been identified to have an association with increased incidence of HCC [55,56]. Surveillance with ultrasound imaging and measurement of alpha-fetoprotein levels has been directed towards these populations to help with early detection of HCC. Guidelines suggest surveillance for HCC in high-risk groups including patients with cirrhosis, noncirrhotic patients with HBV and any of the following characteristics: active hepatitis, family history of HCC, Africans and African Americans, Asian males over 40 years of age, and Asian females over 50 years of age [57-60]. Other populations that undergo surveillance include patients with chronic hepatitis C virus and advanced liver fibrosis in absence of cirrhosis although this is not a consistent recommendation across all societies and the cost effectiveness has not been verified [58].
Currently a knowledge gap remains regarding host factors that contribute to the vagaries of HBV infection outcomes. A group of researchers attempted to explore this by investigating the diverse manifestations of CHB in three families that were observed over decades. Block et al. showed how only one case of HBV-related HCC occurred within every family cluster despite each having the same virus given perinatal transmission from mother to offspring [61]. Furthermore, one of the families had monozygotic twins in which only one sibling developed HBV-related HCC, while the other remained a chronic HBV carrier. The same finding is presenting in a case series by Noverati et al., which presented four family clusters in which patients had very variable courses, some with indolent chronic HBV infection, some requiring treatment, and others who developed HCC or cirrhosis [62]. It is postulated that inheritable immuno-genetic alleles that affect CHB differ from those that influence HBV-related HCC development, which may explain the discrepancy in manifestations in this case series [63]. The study was limited by lack of host and viral genomic analysis as previous studies have shown certain host polymorphisms and HBV mutations are associated with HBV-related HCC. Nonetheless, this highlights that there are genetic and non-genetic host factors that play a role in development of HCC.
Exogenous, non-genetic factors such as chronic stress have been implicated in the incidence and outcomes of HCC, which may also have contributed to the differing presentations in the case outlined above [18]. One of the first published studies highlighting the significance of stress was by Russ et al., in which the group found in a large UK meta-analysis that those with higher scores on a general health questionnaire measuring psychological distress had a higher mortality from liver disease [64]. Joung et al. outlined how stress can increase inflammatory, oxidative reactions including hypoxia-reoxygenation, overactivation of Kupffer cells, influx of gut-derived lipopolysaccharide and norepinephrine, and overproduction of stress hormones in the sympathetic drive, which cause hepatocellular damage and promote mutagenesis [65]. Studies have shown how the tumor milieu of existing HCC undergoes changes that make it immunosuppressive. Specifically, He et al. discovered how chronic stress transitions cytokines to those that are T helper 2 cell-mediated, a tumor microenvironment that carries a poorer prognosis [66]. Similar studies show how this is exacerbated by the presence of T regulatory cells that suppress pro-inflammatory cytokines [67,68].
4. Incidence of HCC in Response to Treatment of HBV
Chronic inflammation and necrosis are key factors which predispose patients to developing HCC. In HBV infection, viral load generally correlates with the severity of disease. NA therapies aimed at decreasing viral load including lamivudine, entecavir, and tenofovir have provided a breakthrough in the treatment of HBV infection as they have demonstrated a reduction in incidence of HCC [69-71] and are now standard of care. Results of prior systematic reviews demonstrate that the risk of HCC is significantly lower in CHB patients receiving oral antiviral therapy. One of the first data to demonstrate efficacy of anti-HBV therapy in HCC risk reduction came from a randomized controlled trial by Liaw et al. which compared lamivudine vs placebo in treatment-naive patients with cirrhosis or advanced fibrosis and active liver disease. Lamivudine treatment for 3 years reduced the risk of HCC by 51% compared to placebo [71]. According to Papatheodoridis et al., across three studies including untreated controls, HCC developed in 2.8% of treated and in 6.4% of untreated CHB patients (p=0.003). A similar study by Singal et al. pooled data from six other studies and showed that the incidence of HCC among lamivudine-treated patients was significantly lower than that of untreated patients (3.4% vs 9.6%, p<0.0001) [72]. This data also demonstrated that HCC occurred more frequently among CHB patients receiving therapy who were older, had cirrhosis, or had detectable HBV-DNA at the end of treatment.
Over time it was discovered that several patients on lamivudine therapy did not attain virological response in the setting of resistance. This did not come without consequence. Alarmingly, Papatheodoridis et al. demonstrated that the rate of HCC was significantly higher in lamivudine resistance than in nucleos(t)ide naive patients (7.1% vs 3.8%, p=0.001), even after correcting for those with cirrhosis (18% vs 11%, p=0.015). It is believed that mutations including changes at position 181 of the reverse transcriptase domain of HBV polymerase have oncologic potential. This led to the advent of newer nucleos(t)ide analog therapies such as tenofovir and entecavir, which proved to be effective. Kim et al. observed that the incidence of HCC in patients with CHB and cirrhosis was decreased compared to the predicted incidence for untreated CHB patients after treatment with tenofovir disoproxil fumerate (TDF) for 3 years [70]. Lim et al. elaborated on this finding and showed that the difference in observed versus predicted HCC risk is more pronounced with tenofovir alafenamide (TAF) than TDF treatment [73]. In a study of entecavir-treated patients, the cumulative incidences of HCC were lower with achievement of a virologic response in both non-cirrhotic and cirrhotic patients [74]. In another study which included cirrhotic CHB patients treated with entecavir, those with undetectable HBV DNA levels were associated with a lower probability of developing HCC [75]. A separate study sought to identify the long-term clinical impact of low-level viremia (<2,000 IU/mL) in patients on entecavir monotherapy. Kim et al. observed that among patients with cirrhosis, those with low-level viremia exhibited a significantly higher HCC risk than those with maintained virological response [76]. These findings support the current recommendation for indefinite therapy in chronic HBV patients, and that inability to achieve undetectable viral load can be consequential.
5. Persistent Risk of HCC in HBV Infection
Maintenance of viral suppression is necessary to reduce HCC risk as demonstrated above. Unfortunately, recent evidence shows that there remains a persistent risk of HCC despite successful HBV therapy resulting in viral suppression [46,77-81]. While spontaneous or treatment-induced seroclearance of HBsAg is also associated with lower risk of liver-related complications, there remains persistent risk of HCC development in these patients as well. Ahn et al. showed a significant reduction of necroinflammation on liver biopsy of patients before and after seroclearance, however all the patients demonstrated presence of HBV DNA without a change in the fibrosis score [82]. Additionally, Gounder et al. showed that seroclearance was not associated with reduced HCC risk compared to a matched control group [83]. The proposed mechanisms in which HCC develops despite adequate treatment are described here.
It has been discovered that HBV covalently closed circular DNA (cccDNA) integrates into the hepatocytes upon initial infection and can be detected even after antiviral treatment. This integration may occur at critical HCC driver genes which may give rise to malignant HBV-infected hepatocytes. Li et al. found that the common location of integration included the TERT, CCNEI1, and MLL4 genes, and that virus-host chimera DNA circulates in 97.7% of CHB patients with HCC [84,85]. Interestingly, the group demonstrated how viral-host chimera DNA could be used as a biomarker for detecting tumor load in this patient population, and how it may aid in monitoring recurrence after tumor resection [84]. In the first detailed molecular evaluation completed by Coffin et al., despite undetectable HBV DNA in plasma via clinical assays, patients treated with oral anti-HBV therapy undergoing liver transplant were found to have low levels of HBV genome in the liver, circulating lymphoid cells, as well as plasma using ultrasensitive PCR/nucleic acid hybridization assay. Their data promotes the idea of HBV compartmentalization where despite adequate suppression, the liver supports replication and extrahepatic HBV can be detected, particularly in peripheral blood mononuclear cells (PBMC) that may serve as a sanctuary for wild type virus during antiviral therapy [86].
Other possible mechanisms that have been postulated include progression of cirrhosis, necroinflammation caused by HBV infection, and the oncogenic effect of HBV genome integration into the hepatocyte chromosomes. HBV DNA may remain detectable in the serum or liver cells, which is referred to as occult HBV infection [87]. Wong et al. found that 69% of 90 HBsAg-negative patients with HCC had occult infection and that of these patients, 47% had detectable cccDNA in hepatocytes and 53% had integration of HBV DNA near hepatic oncogenes [88]. In fact, the HBV genome has been detected in tumor tissue of HBsAg negative patients with HCC in a prevalence ranging from 30% to 80% [89,90]. Therefore, these patients continue to undergo surveillance per the AASLD guidelines [91]. Michalak et al. showed that traces of the HBV genome persist for years following recovery from hepatitis B (characterized by seronegativity) and that they can lead to HCC development in a woodchuck model [92].
HBV infection has an inhibitory effect on the innate and adaptive immune cells which may aggravate chronic inflammation and lead to carcinogenesis. These effects are thought to persist despite antiviral treatment as the microenvironment is altered upon initial infection. It has been shown that the virus may decrease the expression of STAT3 in NK cells, ultimately inhibiting their ability to clear HBV [93]. Studies demonstrate that HBV may promote polarization of cells from M1 to M2 and inhibit secretion of antiviral cytokines by macrophages [94]. Immune tolerance to HBV infection plays a key role in the acceleration of progression of HBV to HCC.
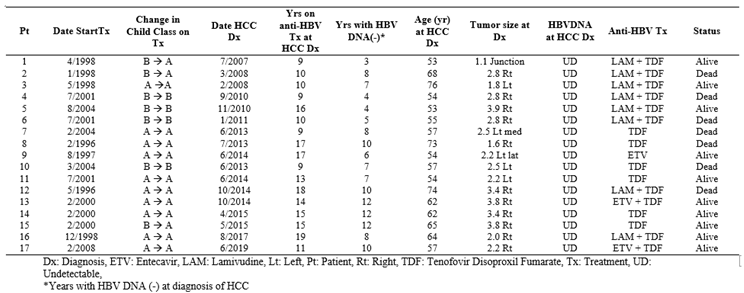
Most reported cases of HBV-HCC in literature are within the first five years of NA therapy, but data on long-term risk of HCC while on treatment is lacking. The Liver Disease Prevention Center, Division of Gastroenterology and Hepatology at Thomas Jefferson University Hospital has observed several HBV positive patients develop HCC even after 10 or more years of successful viral suppression [95]. Specifically, in our observational cohort, 17 patients developed HCC despite having noted undetectable HBV DNA for up to 12 years and on treatment for up to 19 years (Table 1) [96]. Currently this is among the longest known follow-up studies on development of HCC in patients on HBV treatment.
Our center has observed six patients who developed new or recurrent HCC after undergoing curative therapy for HCC and achieving adequate HBV suppression for 5-11 years on antivirals [95]. Unfortunately, recent studies have shown that the patients who develop HCC after years of viral suppression, in fact, carry worse prognosis than those who develop HCC without prior treatment of HBV [97,98]. A case series of 26 patients, 13 antiviral-naive and 13 antiviral-treated, assessed clinical outcomes after HCC diagnosis. Garrido et al. showed that after the first HBV-HCC event, death was observed more frequently among the antiviral-treated cohort at 46.2% compared to 15.4% in the antiviral-naive cohort [99]. Li et al. compared patients who received NA therapy after hepatectomy for HCC and those who did not receive treatment and discovered that there was no difference in the recurrence rate of HCC [100]. The suggested mechanism by which this occurs is that halting HBV replication at the reverse transcription phase for a prolonged time may prime the infected hepatocytes to increasingly turnover HBV DNA integration which can cause insertional mutagenesis and genomic instability [99]. This additionally results in the accumulation of incompletely transcribed mRNAs which may lead to further integration.
It is believed that HCC inoculation in this setting of disorganized products and instability may also cause cancerous cells to be primed to behave more aggressively. Chowdhury et al. described two cases of HBV treatment-naive HCC where despite radiofrequency tumor ablation (RFA) and subsequent undetectable HBV viral load on NA therapy, the patients developed recurrent, more aggressive cancer [98]. The first case described an elderly female who underwent RFA and trans-arterial embolization (TACE) of a 2.1 x 5 cm mass suggestive of HCC. She started NA therapy and became HBV DNA negative, however developed recurrence 5 years later and required repeat TACE. Ten years after the recurrence, MRI demonstrated another LI-RADS 4 5 mm lesion in segment 2 which was monitored with evidence of regression. Unfortunately, this tumor had grown to 1.2 cm two years later, which marked 28 years after the development of her initial HCC. The second case described a male who was found to have cirrhosis with 1.0 cm HCC at age 68. He underwent NA therapy with undetectable HBV DNA and RFA, however at age 79, was found to have two new lesions on abdominal MRI (3 x 2.8 cm and 2 x 1.7 cm) in segment 5 adjacent to gallbladder, and segment 7/8 respectively. He received cholecystectomy and tumor ablation but four years later was found to have a new 4.8 cm lesion in segment 4 on MRI. This illustrates the complexity of the relationship between HBV and HCC, as there is accelerated progression and recurrence of tumor in patients after becoming treatment experienced.
NAs have been critical in decreasing HBV-associated mortality worldwide, however we demonstrate in this review that they do not eradicate the risk of HCC development. There is persistent risk of hepatocarcinogenesis despite adequate treatment marked by undetectable HBV DNA. Thus, there remains a public health threat as currently there is no cure for HBV infection. Achievement of a cure would require therapies which eliminate cccDNA and integrated HBV DNA as well as help restore the impaired innate and adaptive immune responses against HBV.
6. The Road to HBV Cure
The AASLD defines two different types of “cures” of HBV. First, it defines “immunological cure” as HBsAg loss and sustained HBV DNA suppression. Second, it defines “virological cure” as eradication of the virus, including cccDNA, which is not achievable with current therapies which, with current therapies, is not achievable.
The next generation of drugs in development to treat Hepatitis B can be divided into the following classes: drugs targeting the life cycle of the hepatitis B virus; drugs aiming to modulate the host’s immune response to CHB infection; monoclonal antibodies aiming to directly inhibit translation of HBV RNA; and therapeutic vaccines (Figure 2) [101]. A detailed discussion of the progress of these drugs’ development is beyond the scope of this paper; for further reading, the excellent review by Yardeni et al. is highly recommended [102].
Drugs targeting the life cycle of the hepatitis B virus can be classified into entry inhibitors, capsid assembly modulators, post-transcriptional control inhibitors, and Hepatitis B surface antigen release inhibitors.
Novel drugs aiming to modulate the host’s immune response to the HBV are comprised of innate immune activators – specifically, toll-like receptor (TLR) agonists and RIG-1 agonists, and checkpoint inhibitors.
Monoclonal antibodies designed to inhibit the life cycle of HBV have been investigated. One such neutralizing monoclonal antibody, VIR-3434, enhances HBsAg uptake by dendritic cells to promote its presentation to naive T cells thereby stimulating a HBV-specific immune response [103].
Finally, there has been interest in using therapeutic vaccines in effort to stimulate the host’s immune response against CHB infection. However, early studies in humans showed only modest declines in HBsAg [104]. With that said, several new therapeutic vaccines are in development which may be tested in combination with drugs of other mechanisms of action, including siRNAs [105]. However, these therapies have not yet been tested in humans.
In summary, the emerging landscape for novel CHB treatments is composed of vast and varied mechanisms of action, but further clinical testing is still required to establish superiority in efficacy compared to the current standard of care.
7. Conclusion and Future Directions
HBV is a global health threat worldwide as infection can lead to HCC. Available treatment options do not fully eradicate the risk of hepatocarcinogenesis as initial integration of cccDNA into the host genome is not prevented. Continued transcription creates a milieu of genomic instability which can make recurrence of HCC even more aggressive. The phenomenon of worse prognosis in treatment-experienced HCC versus treatment-naive HCC is observed. While there remains a persistent risk of HBV-associated HCC despite viral suppression, recent studies show promising novel approaches to HBV cure.
Author Contributions
Conceptualization, H.H.; Resources, H.H., N.V., A.M., S.N.; Writing – N.V., A.M., S.N. Original Draft Preparation, N.V., A.M., S.N.; Writing – Review & Editing, H.H., D.H., N.V., A.M., S.N., T.B.; Visualization, H.H., D.H., N.V., T.B.; Supervision, H.H., D.H., T.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data was created or analyzed in this study. Data sharing does not apply to this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hou, J.; Liu, Z.; Gu, F. Epidemiology and Prevention of Hepatitis B Virus Infection. Int J Med Sci 2005, 2, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Bashir Hamidu, R.; Hann, R.R.; Hann, H.-W. Chronicles of HBV and the Road to HBV Cure. Livers 2023, 3, 232–239. [Google Scholar] [CrossRef]
- Hepatitis, B. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 21 December 2023).
- Pithawa, A.K. Sleisenger and Fordtran's Gastrointestinal and Liver Disease: pathophysiology, diagnosis, management. Medical Journal Armed Forces India 2007, 63, 205. [Google Scholar] [CrossRef]
- Kao, J.H.; Chen, P.J.; Lai, M.Y.; Chen, D.S. Hepatitis B genotypes correlate with clinical outcomes in patients with chronic hepatitis B. Gastroenterology 2000, 118, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Sunbul, M. Hepatitis B virus genotypes: global distribution and clinical importance. World J Gastroenterol 2014, 20, 5427–5434. [Google Scholar] [CrossRef] [PubMed]
- Guidotti, L.G.; Chisari, F.V. Immunobiology and pathogenesis of viral hepatitis. Annu Rev Pathol 2006, 1, 23–61. [Google Scholar] [CrossRef]
- Lok, A.S. Chronic hepatitis B. N Engl J Med 2002, 346, 1682–1683. [Google Scholar] [CrossRef] [PubMed]
- Parkin, D.M.; Pisani, P.; Ferlay, J. Global cancer statistics. CA Cancer J Clin 1999, 49, 33-64, 31. [CrossRef]
- Fattovich, G. Natural history and prognosis of hepatitis B. Semin Liver Dis 2003, 23, 47–58. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Rudolph, K.L. Hepatocellular carcinoma: epidemiology and molecular carcinogenesis. Gastroenterology 2007, 132, 2557–2576. [Google Scholar] [CrossRef] [PubMed]
- MacLachlan, J.H.; Cowie, B.C. Hepatitis B virus epidemiology. Cold Spring Harb Perspect Med 2015, 5, a021410. [Google Scholar] [CrossRef]
- Beasley, R.P.; Hwang, L.Y.; Lin, C.C.; Leu, M.L.; Stevens, C.E.; Szmuness, W.; Chen, K.P. Incidence of hepatitis B virus infections in preschool children in Taiwan. J Infect Dis 1982, 146, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Alter, M.J.; Hadler, S.C.; Margolis, H.S.; Alexander, W.J.; Hu, P.Y.; Judson, F.N.; Mares, A.; Miller, J.K.; Moyer, L.A. The changing epidemiology of hepatitis B in the United States. Need for alternative vaccination strategies. JAMA 1990, 263, 1218–1222. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.C.; Tsai, K.N.; Ou, J.J. Pathogenicity and virulence of Hepatitis B virus. Virulence 2022, 13, 258–296. [Google Scholar] [CrossRef]
- Ganem, D.; Prince, A.M. Hepatitis B virus infection--natural history and clinical consequences. N Engl J Med 2004, 350, 1118–1129. [Google Scholar] [CrossRef] [PubMed]
- Khanam, A.; Chua, J.V.; Kottilil, S. Immunopathology of Chronic Hepatitis B Infection: Role of Innate and Adaptive Immune Response in Disease Progression. Int J Mol Sci 2021, 22. [Google Scholar] [CrossRef] [PubMed]
- Noverati, N.; Bashir-Hamidu, R.; Halegoua-DeMarzio, D.; Hann, H.W. Hepatitis B Virus-Associated Hepatocellular Carcinoma and Chronic Stress. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- Liaw, Y.F.; Tsai, S.L.; Sheen, I.S.; Chao, M.; Yeh, C.T.; Hsieh, S.Y.; Chu, C.M. Clinical and virological course of chronic hepatitis B virus infection with hepatitis C and D virus markers. Am J Gastroenterol 1998, 93, 354–359. [Google Scholar] [CrossRef]
- Wieland, S.; Thimme, R.; Purcell, R.H.; Chisari, F.V. Genomic analysis of the host response to hepatitis B virus infection. Proc Natl Acad Sci U S A 2004, 101, 6669–6674. [Google Scholar] [CrossRef] [PubMed]
- Chisari, F.V.; Isogawa, M.; Wieland, S.F. Pathogenesis of hepatitis B virus infection. Pathol Biol (Paris) 2010, 58, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, N.; Mousa, O.Y. Hepatitis B. In StatPearls; Treasure Island (FL), 2023.
- Croagh, C.M.; Lubel, J.S. Natural history of chronic hepatitis B: phases in a complex relationship. World J Gastroenterol 2014, 20, 10395–10404. [Google Scholar] [CrossRef] [PubMed]
- Takashima, H.; Araki, K.; Miyazaki, J.; Yamamura, K.; Kimoto, M. Characterization of T-cell tolerance to hepatitis B virus (HBV) antigen in transgenic mice. Immunology 1992, 75, 398–405. [Google Scholar] [PubMed]
- Shi, Y.H.; Shi, C.H. Molecular characteristics and stages of chronic hepatitis B virus infection. World J Gastroenterol 2009, 15, 3099–3105. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.L. Management of chronic hepatitis B patients in immunetolerant phase: what latest guidelines recommend. Clin Mol Hepatol 2018, 24, 108–113. [Google Scholar] [CrossRef]
- Hui, C.K.; Leung, N.; Yuen, S.T.; Zhang, H.Y.; Leung, K.W.; Lu, L.; Cheung, S.K.; Wong, W.M.; Lau, G.K.; Hong Kong Liver Fibrosis Study, G. Natural history and disease progression in Chinese chronic hepatitis B patients in immune-tolerant phase. Hepatology 2007, 46, 395–401. [Google Scholar] [CrossRef] [PubMed]
- McMahon, B.J. The natural history of chronic hepatitis B virus infection. Hepatology 2009, 49, S45–55. [Google Scholar] [CrossRef] [PubMed]
- Thimme, R.; Wieland, S.; Steiger, C.; Ghrayeb, J.; Reimann, K.A.; Purcell, R.H.; Chisari, F.V. CD8(+) T cells mediate viral clearance and disease pathogenesis during acute hepatitis B virus infection. J Virol 2003, 77, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Jeng, W.J.; Sheen, I.S.; Liaw, Y.F. Hepatitis B virus DNA level predicts hepatic decompensation in patients with acute exacerbation of chronic hepatitis B. Clin Gastroenterol Hepatol 2010, 8, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Chu, C.M.; Liaw, Y.F. Age-specific prognosis following spontaneous hepatitis B e antigen seroconversion in chronic hepatitis B. Hepatology 2010, 51, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.I.; Lu, S.N.; Liaw, Y.F.; You, S.L.; Sun, C.A.; Wang, L.Y.; Hsiao, C.K.; Chen, P.J.; Chen, D.S.; Chen, C.J.; et al. Hepatitis B e antigen and the risk of hepatocellular carcinoma. N Engl J Med 2002, 347, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Bonino, F.; Rosina, F.; Rizzetto, M.; Rizzi, R.; Chiaberge, E.; Tardanico, R.; Callea, F.; Verme, G. Chronic hepatitis in HBsAg carriers with serum HBV-DNA and anti-HBe. Gastroenterology 1986, 90, 1268–1273. [Google Scholar] [CrossRef] [PubMed]
- Lok, A.S.; Hadziyannis, S.J.; Weller, I.V.; Karvountzis, M.G.; Monjardino, J.; Karayiannis, P.; Montano, L.; Thomas, H.C. Contribution of low level HBV replication to continuing inflammatory activity in patients with anti-HBe positive chronic hepatitis B virus infection. Gut 1984, 25, 1283–1287. [Google Scholar] [CrossRef] [PubMed]
- Bixler, D.; Zhong, Y.; Ly, K.N.; Moorman, A.C.; Spradling, P.R.; Teshale, E.H.; Rupp, L.B.; Gordon, S.C.; Boscarino, J.A.; Schmidt, M.A.; et al. Mortality Among Patients With Chronic Hepatitis B Infection: The Chronic Hepatitis Cohort Study (CHeCS). Clin Infect Dis 2019, 68, 956–963. [Google Scholar] [CrossRef]
- Brechot, C.; Pourcel, C.; Louise, A.; Rain, B.; Tiollais, P. Presence of integrated hepatitis B virus DNA sequences in cellular DNA of human hepatocellular carcinoma. Nature 1980, 286, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Chemin, I.; Zoulim, F. Hepatitis B virus induced hepatocellular carcinoma. Cancer Lett 2009, 286, 52–59. [Google Scholar] [CrossRef]
- De Mitri, M.S.; Cassini, R.; Bernardi, M. Hepatitis B virus-related hepatocarcinogenesis: molecular oncogenic potential of clear or occult infections. Eur J Cancer 2010, 46, 2178–2186. [Google Scholar] [CrossRef] [PubMed]
- Neuveut, C.; Wei, Y.; Buendia, M.A. Mechanisms of HBV-related hepatocarcinogenesis. J Hepatol 2010, 52, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Block, P.D.; Shinn, B.; Kim, J.H.; Hann, H.W. Hepatitis B-related hepatocellular carcinoma and stress: untangling the host immune response from clinical outcomes. Hepat Oncol 2020, 8, HEP35. [Google Scholar] [CrossRef]
- Li, S.; Hong, M.; Tan, H.Y.; Wang, N.; Feng, Y. Insights into the Role and Interdependence of Oxidative Stress and Inflammation in Liver Diseases. Oxid Med Cell Longev 2016, 2016, 4234061. [Google Scholar] [CrossRef] [PubMed]
- Peneau, C.; Zucman-Rossi, J.; Nault, J.C. Genomics of Viral Hepatitis-Associated Liver Tumors. J Clin Med 2021, 10. [Google Scholar] [CrossRef]
- Wong, G.L.; Chan, H.L.; Yiu, K.K.; Lai, J.W.; Chan, V.K.; Cheung, K.K.; Wong, E.W.; Wong, V.W. Meta-analysis: The association of hepatitis B virus genotypes and hepatocellular carcinoma. Aliment Pharmacol Ther 2013, 37, 517–526. [Google Scholar] [CrossRef]
- Yang, H.I.; Yeh, S.H.; Chen, P.J.; Iloeje, U.H.; Jen, C.L.; Su, J.; Wang, L.Y.; Lu, S.N.; You, S.L.; Chen, D.S.; et al. Associations between hepatitis B virus genotype and mutants and the risk of hepatocellular carcinoma. J Natl Cancer Inst 2008, 100, 1134–1143. [Google Scholar] [CrossRef] [PubMed]
- Kao, J.H.; Chen, P.J.; Lai, M.Y.; Chen, D.S. Clinical and virological aspects of blood donors infected with hepatitis B virus genotypes B and C. J Clin Microbiol 2002, 40, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Papatheodoridis, G.V.; Lampertico, P.; Manolakopoulos, S.; Lok, A. Incidence of hepatocellular carcinoma in chronic hepatitis B patients receiving nucleos(t)ide therapy: a systematic review. J Hepatol 2010, 53, 348–356. [Google Scholar] [CrossRef]
- Chen, C.L.; Yang, H.I.; Yang, W.S.; Liu, C.J.; Chen, P.J.; You, S.L.; Wang, L.Y.; Sun, C.A.; Lu, S.N.; Chen, D.S.; et al. Metabolic factors and risk of hepatocellular carcinoma by chronic hepatitis B/C infection: a follow-up study in Taiwan. Gastroenterology 2008, 135, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Cheuk-Fung Yip, T.; Wai-Sun Wong, V.; Lik-Yuen Chan, H.; Tse, Y.K.; Pik-Shan Kong, A.; Long-Yan Lam, K.; Chung-Yan Lui, G.; Lai-Hung Wong, G. Effects of Diabetes and Glycemic Control on Risk of Hepatocellular Carcinoma After Seroclearance of Hepatitis B Surface Antigen. Clin Gastroenterol Hepatol 2018, 16, 765–773 e762. [Google Scholar] [CrossRef] [PubMed]
- Orito, E.; Hasebe, C.; Kurosaki, M.; Osaki, Y.; Joko, K.; Watanabe, H.; Kimura, H.; Nishijima, N.; Kusakabe, A.; Izumi, N.; et al. Risk of hepatocellular carcinoma in cirrhotic hepatitis B virus patients during nucleoside/nucleotide analog therapy. Hepatol Res 2015, 45, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Zhu, J.; Ge, Z.; Yu, C.; Tian, T.; Wang, H.; Han, J.; Shen, H.; Dai, J.; Lu, J.; et al. Spontaneous Seroclearance of Hepatitis B Surface Antigen and Risk of Hepatocellular Carcinoma. Clin Gastroenterol Hepatol 2019, 17, 1204–1206. [Google Scholar] [CrossRef]
- Tan, Y.; Zhang, X.; Zhang, W.; Tang, L.; Yang, H.; Yan, K.; Jiang, L.; Yang, J.; Li, C.; Yang, J.; et al. The Influence of Metabolic Syndrome on the Risk of Hepatocellular Carcinoma in Patients with Chronic Hepatitis B Infection in Mainland China. Cancer Epidemiol Biomarkers Prev 2019, 28, 2038–2046. [Google Scholar] [CrossRef] [PubMed]
- Yeung, P.; Wong, D.K.; Lai, C.L.; Fung, J.; Seto, W.K.; Yuen, M.F. Association of hepatitis B virus pre-S deletions with the development of hepatocellular carcinoma in chronic hepatitis B. J Infect Dis 2011, 203, 646–654. [Google Scholar] [CrossRef] [PubMed]
- Yuen, M.F.; Tanaka, Y.; Shinkai, N.; Poon, R.T.; But, D.Y.; Fong, D.Y.; Fung, J.; Wong, D.K.; Yuen, J.C.; Mizokami, M.; et al. Risk for hepatocellular carcinoma with respect to hepatitis B virus genotypes B/C, specific mutations of enhancer II/core promoter/precore regions and HBV DNA levels. Gut 2008, 57, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Keng, V.W.; Largaespada, D.A.; Villanueva, A. Why men are at higher risk for hepatocellular carcinoma? J Hepatol 2012, 57, 453–454. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Liu, K.; Luo, J. HIV-HBV and HIV-HCV Coinfection and Liver Cancer Development. Cancer Treat Res 2019, 177, 231–250. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.T.; Wu, L.W.; Tseng, T.C.; Chen, C.L.; Yang, H.C.; Su, T.H.; Wang, C.C.; Kuo, S.F.; Liu, C.H.; Chen, P.J.; et al. Hepatitis B Surface Antigen Loss and Hepatocellular Carcinoma Development in Patients With Dual Hepatitis B and C Infection. Medicine (Baltimore) 2016, 95, e2995. [Google Scholar] [CrossRef] [PubMed]
- Clinical Practice Guidelines for Hepatocellular Carcinoma - The Japan Society of Hepatology 2009 update. Hepatol Res 2010, 40 Suppl 1, 2–144. [CrossRef]
- European Association for the Study of the Liver. Electronic address, e.e.e.; European Association for the Study of the, L. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Kanwal, F.; Singal, A.G. Surveillance for Hepatocellular Carcinoma: Current Best Practice and Future Direction. Gastroenterology 2019, 157, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef]
- Block, P.; Shinn, B.; Roth, C.; Needleman, L.; Rosato, E.; Hann, H.-W. Vagaries of the Host Response in the Development of Hepatitis B-related Hepatocellular Carcinoma: A Case Series. Current Cancer Therapy Reviews 2020, 16, 253–258. [Google Scholar] [CrossRef]
- Noverati, N.; Nguyen, A.; Chalikonda, D.; Halegoua-DeMarzio, D.; Hann, H.W. The Role of Host in the Spectrum of Outcomes in Family Clusters of Hepatitis Infection: From Asymptomatic to Hepatocellular Carcinoma. Case Rep Gastroenterol 2023, 17, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Akcay, I.M.; Katrinli, S.; Ozdil, K.; Doganay, G.D.; Doganay, L. Host genetic factors affecting hepatitis B infection outcomes: Insights from genome-wide association studies. World J Gastroenterol 2018, 24, 3347–3360. [Google Scholar] [CrossRef] [PubMed]
- Russ, T.C.; Kivimäki, M.; Morling, J.R.; Starr, J.M.; Stamatakis, E.; Batty, G.D. Association Between Psychological Distress and Liver Disease Mortality: A Meta-analysis of Individual Study Participants. Gastroenterology 2015, 148, 958–966.e954. [Google Scholar] [CrossRef] [PubMed]
- Joung, J.Y.; Cho, J.H.; Kim, Y.H.; Choi, S.H.; Son, C.G. A literature review for the mechanisms of stress-induced liver injury. Brain Behav 2019, 9, e01235. [Google Scholar] [CrossRef]
- He, Y.; Gao, H.; Li, X.; Zhao, Y. Psychological stress exerts effects on pathogenesis of hepatitis B via type-1/type-2 cytokines shift toward type-2 cytokine response. PLoS One 2014, 9, e105530. [Google Scholar] [CrossRef] [PubMed]
- Granito, A.; Muratori, L.; Lalanne, C.; Quarneti, C.; Ferri, S.; Guidi, M.; Lenzi, M.; Muratori, P. Hepatocellular carcinoma in viral and autoimmune liver diseases: Role of CD4+ CD25+ Foxp3+ regulatory T cells in the immune microenvironment. World J Gastroenterol 2021, 27, 2994–3009. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.F.; Zhao, J.; Ma, L.Y.; Yin, J.H.; Chang, W.J.; Zhang, H.W.; Cao, G.W. Factors predicting occurrence and prognosis of hepatitis-B-virus-related hepatocellular carcinoma. World J Gastroenterol 2011, 17, 4258–4270. [Google Scholar] [CrossRef] [PubMed]
- Hosaka, T.; Suzuki, F.; Kobayashi, M.; Seko, Y.; Kawamura, Y.; Sezaki, H.; Akuta, N.; Suzuki, Y.; Saitoh, S.; Arase, Y.; et al. Long-term entecavir treatment reduces hepatocellular carcinoma incidence in patients with hepatitis B virus infection. Hepatology 2013, 58, 98–107. [Google Scholar] [CrossRef]
- Kim, W.R.; Loomba, R.; Berg, T.; Aguilar Schall, R.E.; Yee, L.J.; Dinh, P.V.; Flaherty, J.F.; Martins, E.B.; Therneau, T.M.; Jacobson, I.; et al. Impact of long-term tenofovir disoproxil fumarate on incidence of hepatocellular carcinoma in patients with chronic hepatitis B. Cancer 2015, 121, 3631–3638. [Google Scholar] [CrossRef]
- Papatheodoridis, G.V.; Chan, H.L.; Hansen, B.E.; Janssen, H.L.; Lampertico, P. Risk of hepatocellular carcinoma in chronic hepatitis B: assessment and modification with current antiviral therapy. J Hepatol 2015, 62, 956–967. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.K.; Salameh, H.; Kuo, Y.F.; Fontana, R.J. Meta-analysis: the impact of oral anti-viral agents on the incidence of hepatocellular carcinoma in chronic hepatitis B. Aliment Pharmacol Ther 2013, 38, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.S.; Chan, H.L.Y.; Ahn, S.H.; Seto, W.K.; Ning, Q.; Agarwal, K.; Janssen, H.L.A.; Pan, C.Q.; Chuang, W.L.; Izumi, N.; et al. Tenofovir alafenamide and tenofovir disoproxil fumarate reduce incidence of hepatocellular carcinoma in patients with chronic hepatitis B. JHEP Rep 2023, 5, 100847. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.C.; Lee, C.M.; Hu, T.H.; Wang, J.H.; Lu, S.N.; Hung, C.H.; Changchien, C.S.; Chen, C.H. Virological response to entecavir reduces the risk of liver disease progression in nucleos(t)ide analogue-experienced HBV-infected patients with prior resistant mutants. J Antimicrob Chemother 2013, 68, 2154–2163. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.S.; Ahn, S.J.; Park, S.Y.; Song, G.W.; Cheong, J.Y.; Cho, S.W. 652 VIROLOGICAL RESPONSE TO ENTECAVIR IS ASSOCIATED WITH LOW PROBABILITY OF DEVELOPING HEPATOCELLULAR CARCINOMA IN CHRONIC HEPATITIS B PATIENTS WITH CIRRHOSIS. Journal of Hepatology 2013, 58, S265. [Google Scholar] [CrossRef]
- Kim, J.H.; Sinn, D.H.; Kang, W.; Gwak, G.Y.; Paik, Y.H.; Choi, M.S.; Lee, J.H.; Koh, K.C.; Paik, S.W. Low-level viremia and the increased risk of hepatocellular carcinoma in patients receiving entecavir treatment. Hepatology 2017, 66, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Dargan, A.; Wong, S.Y.; Coben, R.; Conn, M.; Dimarino, A.J.; Hann, H.W. Persistent risk for hepatocellular carcinoma after more than a decade of successful hepatitis B virus suppression. Minerva Gastroenterol Dietol 2017, 63, 74–76. [Google Scholar] [CrossRef]
- Papatheodoridis, G.V.; Manolakopoulos, S.; Touloumi, G.; Vourli, G.; Raptopoulou-Gigi, M.; Vafiadis-Zoumbouli, I.; Vasiliadis, T.; Mimidis, K.; Gogos, C.; Ketikoglou, I.; et al. Virological suppression does not prevent the development of hepatocellular carcinoma in HBeAg-negative chronic hepatitis B patients with cirrhosis receiving oral antiviral(s) starting with lamivudine monotherapy: results of the nationwide HEPNET. Greece cohort study. Gut 2011, 60, 1109–1116. [Google Scholar] [CrossRef]
- Shinn, B.J.; Martin, A.; Coben, R.M.; Conn, M.I.; Prieto, J.; Kroop, H.; DiMarino, A.J.; Hann, H.W. Persistent risk for new, subsequent new and recurrent hepatocellular carcinoma despite successful anti-hepatitis B virus therapy and tumor ablation: The need for hepatitis B virus cure. World J Hepatol 2019, 11, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Vlachogiannakos, J.; Papatheodoridis, G. Hepatocellular carcinoma in chronic hepatitis B patients under antiviral therapy. World J Gastroenterol 2013, 19, 8822–8830. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.; Hann, H.W.; Coben, R.; Conn, M.; DiMarino, A.J. Update Treatment for HBV Infection and Persistent Risk for Hepatocellular Carcinoma: Prospect for an HBV Cure. Diseases 2018, 6. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.H.; Park, Y.N.; Park, J.Y.; Chang, H.Y.; Lee, J.M.; Shin, J.E.; Han, K.H.; Park, C.; Moon, Y.M.; Chon, C.Y. Long-term clinical and histological outcomes in patients with spontaneous hepatitis B surface antigen seroclearance. J Hepatol 2005, 42, 188–194. [Google Scholar] [CrossRef]
- Gounder, P.P.; Bulkow, L.R.; Snowball, M.; Negus, S.; Spradling, P.R.; Simons, B.C.; McMahon, B.J. Nested case-control study: hepatocellular carcinoma risk after hepatitis B surface antigen seroclearance. Aliment Pharmacol Ther 2016, 43, 1197–1207. [Google Scholar] [CrossRef] [PubMed]
- Li, C.L.; Ho, M.C.; Lin, Y.Y.; Tzeng, S.T.; Chen, Y.J.; Pai, H.Y.; Wang, Y.C.; Chen, C.L.; Lee, Y.H.; Chen, D.S.; et al. Cell-Free Virus-Host Chimera DNA From Hepatitis B Virus Integration Sites as a Circulating Biomarker of Hepatocellular Cancer. Hepatology 2020, 72, 2063–2076. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.L.; Kao, J.H. Development of hepatocellular carcinoma in treated and untreated patients with chronic hepatitis B virus infection. Clin Mol Hepatol 2023, 29, 605–622. [Google Scholar] [CrossRef] [PubMed]
- Coffin, C.S.; Mulrooney-Cousins, P.M.; Peters, M.G.; van Marle, G.; Roberts, J.P.; Michalak, T.I.; Terrault, N.A. Molecular characterization of intrahepatic and extrahepatic hepatitis B virus (HBV) reservoirs in patients on suppressive antiviral therapy. J Viral Hepat 2011, 18, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Mak, L.Y.; Wong, D.K.; Pollicino, T.; Raimondo, G.; Hollinger, F.B.; Yuen, M.F. Occult hepatitis B infection and hepatocellular carcinoma: Epidemiology, virology, hepatocarcinogenesis and clinical significance. J Hepatol 2020, 73, 952–964. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.K.; Cheng, S.C.Y.; Mak, L.L.; To, E.W.; Lo, R.C.; Cheung, T.T.; Seto, W.K.; Fung, J.; Man, K.; Lai, C.L.; et al. Among Patients with Undetectable Hepatitis B Surface Antigen and Hepatocellular Carcinoma, a High Proportion Has Integration of HBV DNA into Hepatocyte DNA and No Cirrhosis. Clin Gastroenterol Hepatol 2020, 18, 449–456. [Google Scholar] [CrossRef]
- Paterlini, P.; Driss, F.; Nalpas, B.; Pisi, E.; Franco, D.; Berthelot, P.; Brechot, C. Persistence of hepatitis B and hepatitis C viral genomes in primary liver cancers from HBsAg-negative patients: a study of a low-endemic area. Hepatology 1993, 17, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Pollicino, T.; Squadrito, G.; Cerenzia, G.; Cacciola, I.; Raffa, G.; Craxi, A.; Farinati, F.; Missale, G.; Smedile, A.; Tiribelli, C.; et al. Hepatitis B virus maintains its pro-oncogenic properties in the case of occult HBV infection. Gastroenterology 2004, 126, 102–110. [Google Scholar] [CrossRef]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef]
- Michalak, T.I.; Pardoe, I.U.; Coffin, C.S.; Churchill, N.D.; Freake, D.S.; Smith, P.; Trelegan, C.L. Occult lifelong persistence of infectious hepadnavirus and residual liver inflammation in woodchucks convalescent from acute viral hepatitis. Hepatology 1999, 29, 928–938. [Google Scholar] [CrossRef]
- Zheng, B.; Yang, Y.; Han, Q.; Yin, C.; Pan, Z.; Zhang, J. STAT3 directly regulates NKp46 transcription in NK cells of HBeAg-negative CHB patients. J Leukoc Biol 2019, 106, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Faure-Dupuy, S.; Delphin, M.; Aillot, L.; Dimier, L.; Lebosse, F.; Fresquet, J.; Parent, R.; Matter, M.S.; Rivoire, M.; Bendriss-Vermare, N.; et al. Hepatitis B virus-induced modulation of liver macrophage function promotes hepatocyte infection. J Hepatol 2019, 71, 1086–1098. [Google Scholar] [CrossRef] [PubMed]
- Boortalary T, S.B. , Coben RM, Conn MI, Prieto J, Kroop H, et al. Are We Close to Achieving a HBV Cure? Risk for Hepatocellular Carcinoma Persists Despite Long-term HBV Suppression: An Update on Our Experience. Arch Gastroenterol Res. 2020; 1(4): 105-110.
- Boortalary T, S.B. Halegoua-DeMarzio D, et al. Achieving a Cure: The Next Frontier in Hepatitis B Treatment. In: Sergi CM, editor. Liver Cancer [Internet]. Brisbane (AU): Exon Publications; 2021 Apr 6. Chapter 6. Available from: https://www.ncbi.nlm.nih.gov/books/NBK569795/. [CrossRef]
- Garrido D, B.P. , Lin S, Halegoua-DeMarzio D, Hann HW. Survival Disparity Between Antiviral-Treated and Antiviral-Nai¨ve Patients Who Develop Their First HBV-Associated Hepatocellular Carcinoma. Arch Gastroenterol Res. 2021;2(3):86-94.
- Chowdhury S, Garrido D, Halegoua-DeMarzio D, Roth C, Hann HW. Poor Prognosis in HBV-associated Hepatocellular Carcinoma After Successful Viral Suppression: A Case 1Series Highlighting a Need for a Cure. J Immunological Sci. (2023); 7(4):1-8.
- Lin, S.Y.; Zhang, A.; Lian, J.; Wang, J.; Chang, T.T.; Lin, Y.J.; Song, W.; Su, Y.H. Recurrent HBV Integration Targets as Potential Drivers in Hepatocellular Carcinoma. Cells 2021, 10. [Google Scholar] [CrossRef]
- Li, N.; Lai, E.C.; Shi, J.; Guo, W.X.; Xue, J.; Huang, B.; Lau, W.Y.; Wu, M.C.; Cheng, S.Q. A comparative study of antiviral therapy after resection of hepatocellular carcinoma in the immune-active phase of hepatitis B virus infection. Ann Surg Oncol 2010, 17, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Levrero, M.; Testoni, B.; Zoulim, F. HBV cure: why, how, when? Curr Opin Virol 2016, 18, 135–143. [Google Scholar] [CrossRef]
- Yardeni, D.; Chang, K.M.; Ghany, M.G. Current Best Practice in Hepatitis B Management and Understanding Long-term Prospects for Cure. Gastroenterology 2023, 164, 42–60 e46. [Google Scholar] [CrossRef] [PubMed]
- Feld, J.J.; Lok, A.S.; Zoulim, F. New Perspectives on Development of Curative Strategies for Chronic Hepatitis B. Clin Gastroenterol Hepatol 2023, 21, 2040–2050. [Google Scholar] [CrossRef]
- Lok, A.S.; Pan, C.Q.; Han, S.H.; Trinh, H.N.; Fessel, W.J.; Rodell, T.; Massetto, B.; Lin, L.; Gaggar, A.; Subramanian, G.M.; et al. Randomized phase II study of GS-4774 as a therapeutic vaccine in virally suppressed patients with chronic hepatitis B. J Hepatol 2016, 65, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Michler, T.; Kosinska, A.D.; Festag, J.; Bunse, T.; Su, J.; Ringelhan, M.; Imhof, H.; Grimm, D.; Steiger, K.; Mogler, C.; et al. Knockdown of Virus Antigen Expression Increases Therapeutic Vaccine Efficacy in High-Titer Hepatitis B Virus Carrier Mice. Gastroenterology 2020, 158, 1762–1775 e1769. [Google Scholar] [CrossRef]
Figure 1.
Mechanisms of hepatocarcinogenesis from chronic hepatitis B infection. Sourced from Péneau et al. [42].
Figure 1.
Mechanisms of hepatocarcinogenesis from chronic hepatitis B infection. Sourced from Péneau et al. [42].
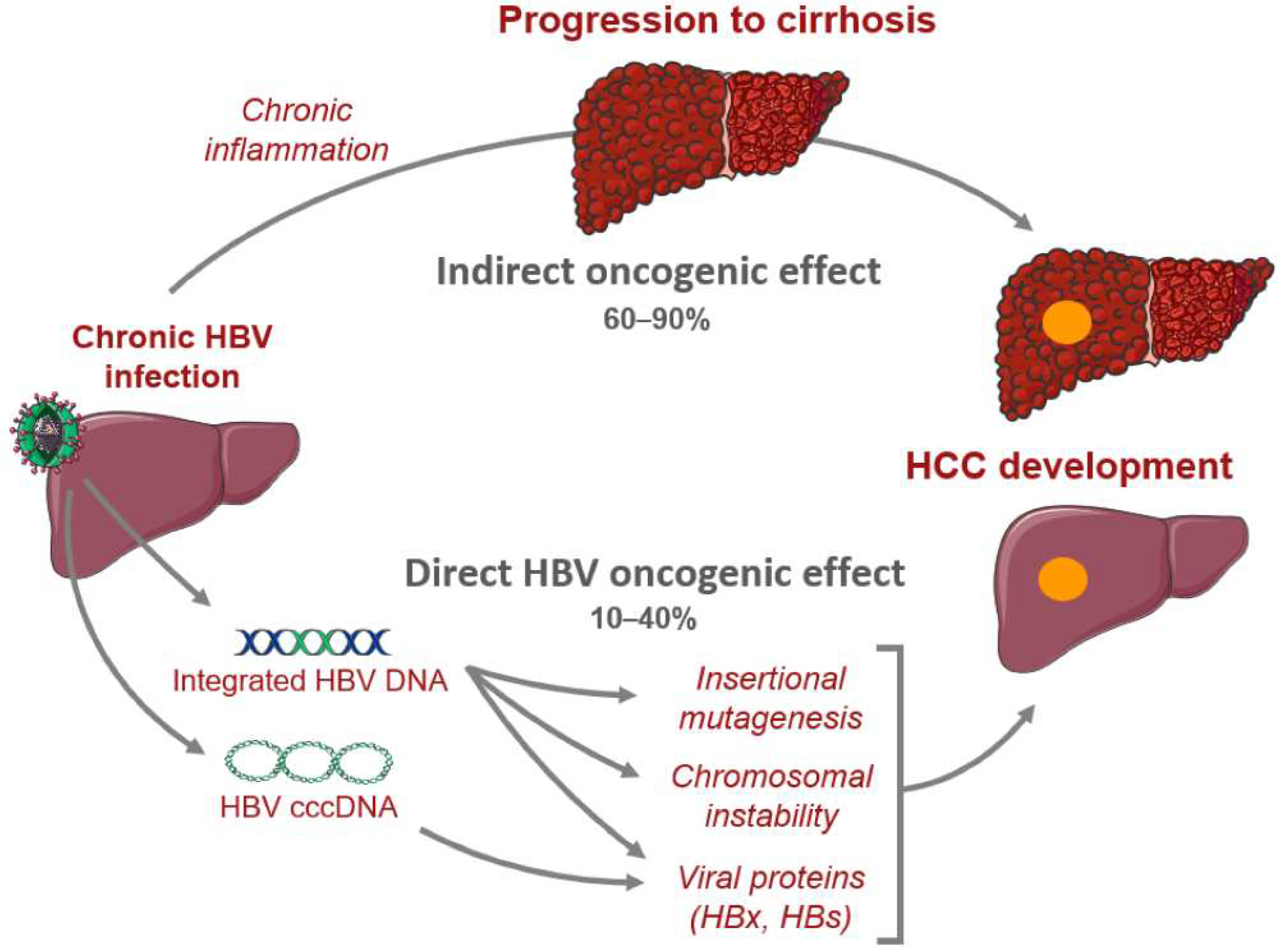
Figure 2.
Therapeutic drug targets of hepatitis B virus replication. Sourced from Levrero et al. [101]. Used with permission from original copyright holder.
Figure 2.
Therapeutic drug targets of hepatitis B virus replication. Sourced from Levrero et al. [101]. Used with permission from original copyright holder.
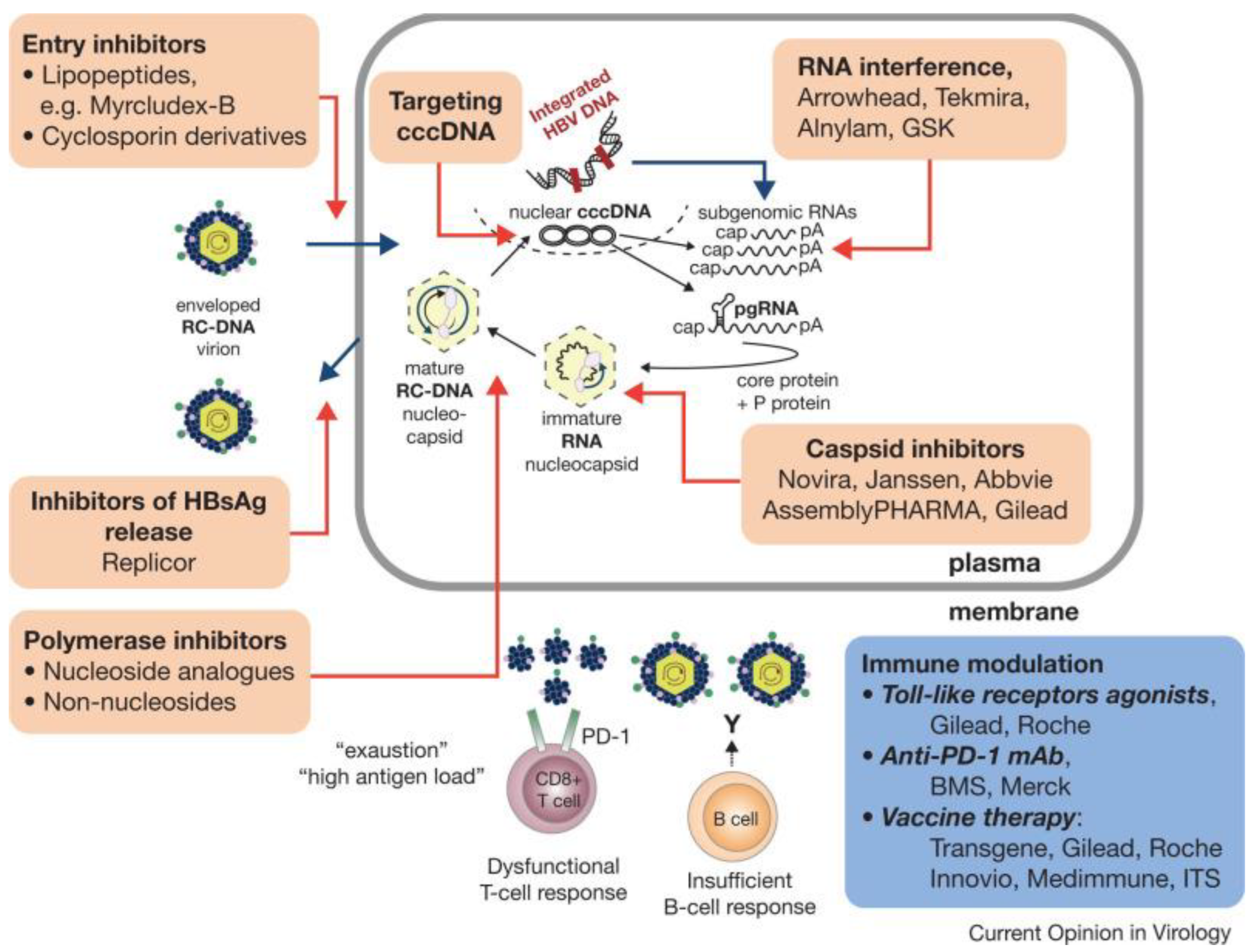

Table 1.
Development of HCC in patients with cirrhosis on long-term antiviral therapy. Sourced from Boortalary et al. [96].
Table 1.
Development of HCC in patients with cirrhosis on long-term antiviral therapy. Sourced from Boortalary et al. [96].
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



