
Submitted:
25 December 2023
Posted:
28 December 2023
You are already at the latest version
Abstract
Background and Objectives: Rheumatic diseases often exhibit a complex pattern of comorbidities, including the increased occurrence of emotional disorders like anxiety and depression, which are closely related to the presence of chronic pain. Therefore, a multimodal approach is necessary for treatment, targeting both the physical and psychological functioning. Due to the increased burden within the healthcare context that emerged during the post-pandemic period, the need to adjust the content and length of psychological interventions became ubiquitous. In this way, the main objective of this study was to investigate the efficiency of a single-session, process-based psychological intervention for patients with rheumatic conditions and emotional comorbidities in a naturalistic, in-patient setting. Materials and Methods: After the screening, a total of 31 participants (Mage = 58.9, SD = 12.03) completed the single session intervention. The therapeutic protocol relied on a process-based cognitive-behavioural therapy framework aiming to improve cognitive, emotional and behavioural functioning. Assessments were conducted prior to the intervention, post-intervention and one month following the hospitalization. Results: Immediately after the intervention, significant reductions in dysfunctional cognitive and emotional processes, along with the improvement of behavioural strategies were observed. At the one-month telephonic evaluation, participants reported decreased pain, state anxiety and state depression levels. Conclusions: The single-session, process-based approach represents a promising intervention in healthcare contexts, targeting important psychopathological mechanisms in patients with rheumatic conditions. Future studies could clarify the extent to which these outcomes persist over time and their specific associations with anxiety and depressive symptoms, by using more controlled and rigorous trial designs.
Keywords:
rheumatic conditions
; chronic pain
; anxiety
; depression
; psychological intervention
; process-based cognitive-behavioural therapy
; single-session intervention
1. Introduction
Rheumatic conditions are highly associated with a poor quality of life, given their increased comorbidity with emotional disorders like anxiety and/or depression, which occur in approximatively 20% of patients or more [1,2,3]. Specifically, one of the main mechanisms contributing to the onset of psychiatric disorders in association with rheumatic conditions is the presence of chronic pain, involving significant medical and economic challenges [4,5]. Besides the innate biological aspects, the clinical picture of these cases is strongly influenced by aversive life events, such as interpersonal problems, grave, psychological abuse, financial difficulties, as well as health-related concerns [6,7]. Particularly, the COVID-19 pandemic was correlated with increased psychological distress and healthcare challenges in patients with rheumatic conditions, requiring the adjustment of therapeutic protocols and methods [8]. Also, this period was repeatedly correlated with a raise of unhealthy cooping strategies in diverse populations, emphasizing the role of targeted interventions for promoting positive lifestyle changes [9,10].
Moreover, the bidirectional relationship between emotional and physical symptoms generates a complex network defined by multimorbidity, which involves various functional difficulties [11]. Therefore, a multidisciplinary and integrative approach is recommended for the management of common rheumatic conditions, especially when emotional disorders are also present [12]. The first-line treatment involves the medical management, including disease-modifying antirheumatic drugs (DMARDs), glucocorticoids and topical nonsteroidal anti-inflammatory drugs, as well as psychiatric treatment like anxiolytics and antidepressants [13,14,15].
Besides the medical treatment, the psychological intervention in these cases is highly recommended. In this regard, the efficiency of cognitive-behavioural therapies (CBT) is widely recognized in the management of chronic pain and associated emotional difficulties [16,17,18]. This approach outlines the role of pain-related thoughts in the occurrence of psychological distress, aiming to modify dysfunctional thoughts and correct specific cognitive distortions by promoting a healthier and realistic thinking style [19,20].
Therefore, symptoms within the anxious-depressive comorbidity, along with other disorders from the psychopathological spectrum, are interrelated, and potentiate each other, sharing common roots and dysfunctional processes [21]. Starting from this premise, the transdiagnostic psychological treatment protocols led to the emergence of a new model, which describes psychopathological mechanisms as a network in which each process influences the others [22]. In this way, process-based cognitive-behavioural therapy (CBT) can be considered a new CBT branch that aims to change dysfunctional processes related to psychopathology with their functional counterparts, relying on the assumption that these mechanisms are modifiable and dynamic characteristics [23]. The process-based CBT is grounded in the evolutionary theory, aiming to facilitate adaptation to various life contexts at the level of variation, selection and retention of strategies that operate at multiple dimensions of psychological functioning, including affectivity, cognition, attention, motivation and behaviour [24].
Psychological interventions adapted for chronic pain were delivered in a variety of formats, including face-to-face, online, individual and group programs, with a typical duration between 4 and 12 sessions [25]. However, the integration of medical and complementary treatments, along with the multiple medical appointments and time pressure inherent to the clinical environment are associated with high withdrawal from psychotherapy in patients with chronic pain, which points to an imperious need to adjust these interventions to enhance benefits, while reducing drop-out rates [26,27]. So far, process-based CBT proved to be efficacious for alleviating anxiety and depression levels among both the general and chronic pain population, with very good acceptability [28,29,30].
This approach targets psychological inflexibility as a common process involved in the onset of psychological disorders associated with chronic pain, including cognitive fusion, emotional suppression, experiential and behavioural avoidance [31,32,33]. These processes result in the patient’s incapacity to adapt to various life circumstances, including the aversive experience of pain [32,34]. Cognitive fusion refers to the idea that thoughts are appraised as general rules of functioning and not merely a perception of reality, so that the person takes decisions and acts according to the contents of their dysfunctional thoughts [32,35]. In contrast, cognitive defusion helps separating thoughts from facts and enables a more detached perspective on them, decreasing their potential to generate distress [36]. At the level of emotions, experiential avoidance is characterized as the patient’s tendency to withdraw from distressing internal experiences, despite physical and psychological costs [32,37]. The healthier variant is represented by acceptance, or the willingness to fully experience emotions or sensations, whether pleasant or not, without attempts to control them, facilitating adaptation in the case of chronic pain [38,39]. From a behavioural point of view, difficulties are linked to the use of unhealthy coping strategies, inconsistent with the patient’s aspirations, especially in the context of a chronic health condition [30,33]. On the other hand, increasing values-based action was associated with less disability and elevated motivation in chronic pain [40].
Against this background, as an alternative to the CBT short or medium-term intervention protocols, Single-Session Interventions (SSI) represent condensed treatments that can be considered useful ways to achieve the optimal results in a way that maximizes time resources [41,42]. In chronic health conditions, the application of SSI using a transdiagnostic framework was associated with moderate improvements related to functional measures, anxiety, depression and psychological flexibility processes [43]. For example, comparing SSI with a standard 8-session CBT protocol, Darnall and colleagues (2021) showed that emotional symptoms, pain-related distress and catastrophizing equivalently reduced among the treatment arms in patients with chronic low back pain [44].
Although these results are promising, further studies to investigate the benefits and feasibility of such brief interventions in clinical contexts are necessary. Based on the previous research literature, the main objective of the present study was to analyse the effects of an in-patient process-based SSI for patients with rheumatic diseases presenting chronic pain. First, starting from the process-based CBT model, we anticipated to find correlations between baseline measures of symptoms and psychological inflexibility processes in patients with chronic pain. Second, we expected that cognitive fusion, experiential avoidance and dysfunctional behavioural processes will reduce after the SSI, while the functional coping strategies will improve for those patients.
2. Materials and Methods
Participants. The sample size was calculated using the G-Power software version 3.1 [45] for a moderate effect size, expected power of 0.80 and alpha error probability of 0.05. A total number of 31 participants (Mage = 58.9, SD = 12.03) that presented a musculoskeletal condition diagnosed by a rheumatologist and were hospitalized for at least 1 week within the Rheumatology section of the Targu Mures County Emergency Clinical Hospital participated in this study. Further inclusion criteria were: 1) age over 18 years old; 2) the presence of a chronic pain condition for at least 3 months; 3) the fulfilment of psychodiagnosis criteria for generalized anxiety disorder and/or major depressive disorder according tothe Structured Clinical Interview for the DSM-5—Clinician Version. Exclusion criteria were: 1) age under 18 years old; 2) the existence of severe cognitive impairment; 3) the presence of severe psychiatric disorders; 4) not being able to understand Romanian language properly.
Ethical considerations. This study was approved by the Institutional Ethics Committee of the Targu Mures County Emergency Clinical Hospital from 27.07.2023 under the number 19622. Before enrolling in the study, participants were informed regarding the objectives and procedures of the research and signed the informed consent.
Measures
The DECAS Personality Inventory [46] was developed and validated on the Romanian population, based on the Five Factor Model of Personality [47], providing accurate estimates of important personality dimensions in relation to clinically relevant variables such as emotional distress. Particularly, the Emotional Stability subscale measures neuroticism, which is defined as the tendency to experience negative emotions more easily, encounter difficulties when confronted with stressful situations and rely on unhealthy coping strategies. At higher levels, there is a high overlap between this personality dimension and the occurrence of emotional disorders [48]. The subscale includes 19 items that asks responders to decide whether a specific affirmation is true or false in their case most of the time. The internal consistency demonstrated in the original study was good, as reflected by the obtained Cronbach’s alpha coefficient of .75 [49].
The Structured Clinical Interview for the DSM-5—Clinician Version (SCID-5-CV) [50] refers to a semi-structured clinician-rated tool based on the diagnosis criteria listed in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) [51]. Using a series of guiding questions, the interviewer decides whether key psychopathological symptoms are present or not in the case of a particular person, the instrument proving good discriminative properties. Specifically, for anxiety disorders, sensitivity and specificity were estimated at 0.94 and 0.78, respectively. At the same time, for depressive disorders, both sensitivity and specificity were 0.84. Also, the SCID-5-CV demonstrated moderate, albeit reasonable inter-rater agreement rates, with Kappa coefficients of 0.34 for anxiety disorders and 0.69 for depressive disorders [52]. However, other investigations estimated a Kappa coefficient of 0.73, along with a positive agreement rate of 73% for any anxiety disorder [53]. Therefore, it was concluded that the interview can reliably be used for screening purposes in both in-patient and out-patient settings.
The Visual Analogue Scale (VAS) is a single-item measure applied in the assessment of both physical and psychological variables [54]. Given their practical utility and high feasibility, such scales were traditionally implemented for evaluating the subjective pain intensity in various medical contexts. Typically, the VAS requires respondents to rate the severity of the symptom on a 10 cm scale, from 0= not present to 10 = worst imaginable intensity of the symptom [55]. Also, fatigue ratings were evaluated with the VAS in patients with rheumatoid arthritis, indicating similar properties to alternative fatigue measures in terms of sensitivity and association to clinical outcomes [56]. More recently, this approach was also used for evaluating psychological dimensions, like depressive mood, showing proper convergent and divergent validity [54]. Indeed, the VAS for depression proved a correlation of 0.61 with the total score of other validated and widely employed measures of depression, like the Patient Health Questionnaire-9 (PHQ-9) [57]. Finally, the same approach tested for anxiety led to equivalent results in terms of validity, as indicated by the correlations between VAS and other renowned tools, such as the Hamilton Rating Scale for Anxiety (r = 0.60), or the Hospital Anxiety and Depression Scale - Anxiety subscale (r = 0.74) [58].
The Process-Based Assessment Tool (PBAT) [59] is grounded in the evolution theory, using a behavioural approach to evaluate processes of change, which are highly cited especially in the context of process-based CBT [60]. Unlike most evaluation scales, this instrument is defined as an “item pool”, integrating 18 individual items that depict positive and negative behavioural responses. In this way, there are two items corresponding to the evolutionary dimension of variation, namely the ability to change one’s behaviour when it is beneficial (positive; item 1) and the opposite, incapacity to change and being stuck (negative; item 12). Retention is also reflected in two items, indicating one’s struggle to continue engaging in important action (positive; item 4), along with remaining stuck to previous strategies that are currently inefficient (negative; item 10). Finally, most contents are related to the evolutionary dimension of selection. On the one hand, positive selection mechanisms are presented in 8 items, as follows: the ability to experience a wide range of emotions (affective component; item 3), the choice of actions that may improve one’s physical health (item 6), paying attention to important goals and actions (motivation component; item 8), finding personally relevant ways for challenging oneself (need for competence; item 11), using one’s thinking to improve life (cognitive component; item 13), attempts to connect with meaningful moments (attention component; item 14) and significant people (social connection; item 15), along with choosing to do things that are personally important (item 16). On the other hand, negative selection mechanisms are included in the next 5 items: doing actions that hinder one’s connection to other people (social connection; item 2), failing to find a meaningful way to challenge oneself (need for competence; item 5), thinking in an inefficient way (cognitive component; item 7), performing various actions as a result of social desirability (motivation component; item 9), engaging in actions that are detrimental to one’s health (item 17), as well as facing difficulties in expressing emotions (affective component; item 18). Items are typically rated using a digital-analogue scale from 0 = strongly disagree to 100 = strongly agree. However, due to the setting of this study, we applied a classical pen-and-paper approach, using the same ordinal range. The original research on PBAT criterion validity showed that positive items predict good health and vitality, whereas negative processes are linked to sadness, anxiety, stress, anger and lack of social support [59].
The Acceptance and Action Questionnaire (AAQ-II) [61] refers to a self-report 7-item scale for measuring experiential avoidance, defined as the tendency to ward off difficult internal experiences, especially negative emotions (e.g., “I worry about not being able to control my worries and feelings” or “Emotions cause problems in my life”). Responses are rated using a 7-point Likert scale (starting from 1 = never true to 7 = always true). Total scores represent the sum of individual items, higher values indicating heightened experiential avoidance, with a higher possible score of 49. The mean Cronbach’s alpha coefficient obtained in the original validation study was 0.84, which suggests a very good reliability, along with the criterion and predictive validity established through comparisons with other symptom-oriented scales for assessing emotional disorders [61]. The Romanian validation of the scale resembled these findings, with a reliability coefficient of 0.80 [62]. In the present study, the Cronbach’s alpha coefficient values ranged from 0.65 to 0.76.
The Cognitive Fusion Questionnaire (CFQ) [63] is a 7-item scale that measures the tendency to consider thoughts as general rules and rely on them when making behavioural decisions, which amplifies the individual’s adjustment difficulties. As reflected in the content of the questionnaire (e.g., “I get so caught up in my thoughts that I am unable to do the things that I most want to do” or “It’s such a struggle to let go of upsetting thoughts even when I know that letting go would be helpful”), this mechanism is effortful, limiting personal coping resources. A 7-point Likert scale (starting from 1 = never true to 7 = always true) is employed for rating, adding up to a maximum final score of 49. From the perspective of psychometric properties, the CFQ demonstrated very good internal consistency, with Cronbach’s alpha coefficients ranging from 0.88 to 0.93 in the original validation study, depending on the participants’ characteristics. Also, the scale has proper criterion validity, as shown by the correlations with other instruments measuring psychological processes and clinical manifestations of various psychopathologies [63]. By using the Romanian translation of CFQ, we obtained similar reliability, with Cronbach’s alpha levels of 0.83 and 0.84 at pre- and post-test measures, respectively.
Design and procedure. The present study is an uncontrolled trial, involving an intervention group with no control arm. The participant flow is depicted in Figure 1. The screening involved using the DECAS Personality Inventory. More specifically, the composite T scores for the Emotional Stability (Neuroticism) subscale were extracted for each participant by using the DECAS online platform [46]. This initial assessment was doubled by the application of the SCID-5-CV - generalized anxiety disorder and major depressive disorder sections. Participants who met the criteria for one or both diagnoses were included in the study. A total number of 31 participants were enrolled and completed the SSI, based on established techniques and protocols of process-based CBT for chronic pain [64,65,66]. The intervention was carried out at the bedside, in an individual format, within 2 days after the hospital admission and lasted between 70 and 80 minutes. The detailed single-session protocol is presented in Figure 2. The pre-test involved the administration of a brief demographic questionnaire, the VAS scales for pain, fatigue, anxiety and depression, as well as the evaluation of psychological flexibility processes with the AAQ, CFQ and PBAT, respectively. The post-test at T1 was conducted after 3-5 days following the intervention, including the use of AAQ and CFQ scales. The post-test at T2 was conducted telephonically at one month after the hospital admission, asking participants to evaluate the intensities of pain, fatigue, anxiety and depression during the previous two weeks using the VAS scales.
Statistical analyses. Outcomes of the present study were analysed using the IBM SPSS software, version 29.0.1. First, Pearson’s correlations were performed for investigating the relations between different sets of variables at baseline, including subjectively evaluated health and mood components (pain, fatigue, anxiety and depression), as well as psychological inflexibility and behavioural processes. Second, the paired samples T test was used for analysing the intervention effects on the levels of experiential avoidance and cognitive fusion at T1, along with the impact on the subjective ratings of pain, fatigue, anxiety and depression at T2.
3. Results
3.1. Descriptive characteristics
Table 1 comprises the demographic particularities of our sample, along with the average baseline VAS scores regarding the major physical and mood components. The average participant was a female, around 59 years old, married, currently retired and graduated a form of secondary education (professional or high school). The intake/ admission screening/ assessment indicated an average extreme severity of subjectively reported pain and fatigue, along with moderate to high anxiety and depression ratings.
3.2. Baseline measures
The results of the correlation analyses performed on baseline measures including health components, psychological flexibility and behavioural processes are depicted in Table 2. Pain scores were significantly correlated with subjective anxiety levels (r = .40), along with the processes of cognitive fusion (r = .43) and the PBAT item Hurt Connection (r = .40). Also, fatigue was moderately and positively associated to depression scores (r = .41), as well as several behavioural processes, including PBAT items Important Challenges (r = .49), Connect to People and Personal Importance (r = .41), while negatively associated to PBAT item Stuck, unable to change (r = -.37). In addition, anxiety was positively correlated with experiential avoidance (r = .37) and the PBAT item Thinking Got In the Way (r = .42). Regarding the relation between psychological flexibility and behavioural processes, the PBAT item Hurt Health was positively and strongly associated to cognitive fusion (r = .60) and experiential avoidance (r = .45), respectively. In contrast, negative correlations emerged between experiential avoidance and the PBAT items Thinking Helped Life (r = -.41) and Struggle Connect Moments (r = -.35). In a similar way, the PBAT item Experience Range Emotions was inversely correlated with both experiential avoidance (r = -.39) and cognitive fusion (r = -.36). As expected, we also found a strong positive association between experiential avoidance and cognitive fusion (r = .60).
3.3. Intervention outcomes
3.2.1. Results at T1
The results are summarized in Table 1, showing significant beneficial effects of the intervention on psychological inflexibility dimensions. Both cognitive fusion and experiential avoidance were significantly reduced after the intervention, as compared to baseline. As regards to the behavioral strategies, a statistically significant difference was observed in relation to five processes. First, participants showed an improved ability to change their behaviour,and behaviours that helped physical health increased. Also, a reduced proneness to comply with other’s wishes without taking own needs into account, along with, as a lower tendency to feel stuck to unproductive working strategies and a decreased likelihood to behave in ways that would damage health were observed after the psychological intervention.

Table 1.
Summary of primary outcomes at T1 after the single-session treatment.
| Outcome measure | Mean (SD) | t(30) | p value | |
|---|---|---|---|---|
| Pre-test | Post-test T1 | |||
| Cognitive Fusion | 28.19 (17.77) | 17.77 (6.58) | 9.96 | <0.001 |
| Experiential avoidance | 28.06 (6.86) | 19.84 (6.38) | 7.79 | <0.001 |
| Able To Change Behaviour (PBAT_1) | 64.84 (22.19) | 81.61 (20.67) | -4.37 | <0.001 |
| Helped Health (PBAT_6) | 60.00 (24.76) | 79.68 (19.40) | -4.32 | <0.001 |
| Complying (PBAT_9) | 61.61 (27.21) | 41.94 (22.12) | 3.86 | <0.001 |
| Stuck To Working Strategies (PBAT_10) | 45.81 (29.18) | 28.39 (25.04) | 3.27 | 0.003 |
| Hurt Health (PBAT_17) | 45.16 (25.41) | 25.48 (22.03) | 4.05 | <0.001 |
3.2.2. Results at T2
The assessment conducted one month after the intervention indicated a statistically significant decrease of pain ratings from pre-test (M = 8.26, SD = 1.65) to the T2 post-test (M = 5.70, SD = 2.52), t(26) = 6.43, p < 0.001. In addition, state anxiety scores were lower at the T2 post-test (M = 4.96, SD = 2.68), in contrast to pre-test (M = 7.11, SD = 2.57), t(26) = 4.45, p < 0.001. State depression levels also dropped from pre-test (M = 6.26, SD = 2.56) to the T2 post-test (M = 4.15, SD = 2.69), t(26) = 3.43, p = 0.002. However, we did not observe a statistically significant reduction of fatigue scores at the T2 post-test.
4. Discussions
First, the correlational analysis indicated a pattern of associations between psychological inflexibility processes and reported physical or emotional symptoms at baseline in the expected direction. This finding supports the idea that several interdependent mechanisms could underpin the comorbidity between rheumatic diseases and emotional disorders [67]. Specifically, in our study, experiential avoidance and cognitive fusion were positively associated with the tendency to behave in ways that would damage one’s health. This could point to the existence of an indirect pathway explaining the link between psychological inflexibility and health-related problems through unhealthy behavioural choices [68]. Moreover, the negative associations between psychological inflexibility processes and the existence of a broad emotional repertoire, along with the ability to change thoughts to improve one’s mood outlined the connection between beliefs, feelings and behaviours that ultimately marks the boundary between psychopathology and healthy psychological functioning [69,70]. Also, perceived pain intensity was positively correlated to the tendency to engage in behaviours that damaged meaningful interpersonal relationships, which is in line with previous studies showing a link between interpersonal processes and pain adjustment [71]. In addition, the experience of fatigue was associated with perceived lack of meaningful reinforcements and incapacity to change inefficient strategies, similarly to other research showing a connection between perceived energy level and motivational features in chronic pain [72].
Second, our results showed that a brief and compacted intervention can promptly improve psychological flexibility in patients with rheumatic diseases and emotional comorbidities. This is in line with previous findings indicating that a single workshop based on process-based CBT can reduce psychological distress in patients with chronic pain [73]. In our study, participants proved to be less prone to engage in experiential avoidance and more willing to experience uncomfortable emotions and sensations immediately after the intervention. This is concordant to a large body of research that demonstrated the benefits of process-based therapies to increase acceptance, especially in relation to chronic pain [74,75,76]. Second, the level of cognitive fusion decreased shortly after the intervention. In a similar light, it has been proven that a single-session treatment is effective for modifying common cognitive features which are associated with emotional distress in chronic pain patients [77,78,79]. Third, at the behavioural level, the general direction was related to factual changes that promoted health-related activities. As expected, during the hospitalization, participants had a higher probability to engage in activities supporting physical health. Along with the inclusion of the intervention component focused on values and committed action, involving a concrete action plan with specific objectives for facilitating a balanced lifestyle, we believe this behavioural change could be strongly correlated to the inpatient context, defined by a multimodal approach in the treatment of rheumatic conditions [80]. This aligns with previous studies concluding that patients’ motivation and treatment adherence are correlated with a good quality medical care, using an integrative framework for targeting multiple areas of functioning [81,82,83]. Similarly, several investigations proved that encouraging values-based living is linked to a better functioning that includes personalized action plans facilitating the attainment of meaningful goals, despite the presence of chronic pain and potential physical constraints [84,85,86,87]. Interestingly, the likelihood to comply with others’ wishes without considering own needs also reduced, which points to an increased autonomy in the face of long-lasting health challenges [86]. Indeed, previous research indicated that promoting self-determination in patients with chronic medical conditions is related to benefits in terms of disease-related behaviours [89,90,91,92].
Moreover, one month after the intervention, participants reported improvements related to the symptom components. Namely, as anticipated following the hospitalization, significant changes were observed regarding the pain perception. In addition, we could assume that this outcome is also concordant with other research showing that process-based psychological treatments have a positive impact on the pain intensity and associated disability [93,94,95,96]. Furthermore, subjective anxiety and depression levels decreased after the in-patient treatment, compared to the baseline assessment. Multiple investigations resembled these findings, proving that working on dysfunctional cognitive and emotional mechanisms may notably alleviate emotional distress in patients with chronic pain [97,98,99,100,101].
Nonetheless, several limitations could impede the results interpretation in the present study. There are methodological constraints that hinder the generalizability of our findings. First and foremost, since our study did not include a control group, the effects of the intervention couldn’t be differentiated from other factors influencing the subjective experience of participants. While an uncontrolled design may provide the framework for more naturalistic research and resemble real-life circumstances, we acknowledge that a less rigorous trial generates a series of shortcomings regarding the validity and fidelity of results. In this way, an important limitation of our study is the incapacity to rule out the possibility of confounds that could influence the final outcomes. For example, other components of the treatment like administered medication or physical therapy could involve benefits that extend beyond somatic components, improving the psychological adjustment in patients with rheumatic diseases. Also, the benefits observed after the hospitalization could be linked more to the context, especially the fact that participants returned home and spent more time with their families. Second, our research included self-report measures, meaning that the results could be influenced by social desirability. This concern is particularly valid given the institutionalized environment, in which the psychological approach was integrated among various treatment components and the psychotherapist was perceived as part of the healthcare team. Third, another limitation assumed by authors is related to the measurement of anxiety and depressive symptoms. Fourth, we did not include longitudinal assessments for observing the evolution of these outcomes over time. Therefore, we believe future analyses could overcome these limitations by including passive and active control groups, additional instruments for assessing the intensity of clinical symptoms at different time points and follow-up intervals.
Clinical implications. The outcomes of the present study may inform the development of targeted protocols aiming to reduce emotional distress in patients with chronic pain, as part of interdisciplinary treatment packages [102,103,104]. The utility of the SSI format lies in the ability to achieve meaningful improvements in very short time, which transforms it in an efficient tool to match the challenges of delivering psychotherapeutic interventions within in-patient contexts [43,105]. Also, by encouraging health-related action, these interventions could successfully prevent the various side effects of medication misuse in patients with physical and/ or mental health difficulties [106,107]. In addition, such approaches can be easily integrated in the routine care of patients with rheumatic conditions, being easily applicable by medical professionals for increasing patients’ motivation and treatment compliance, above and beyond the hospitalization period [108,109,110]. In this way, we believe that the adoption of these treatment practices could have a positive impact on the burden of multimorbidity for the healthcare system as a whole in the long run.
5. Conclusions
This study showed that a brief process-based psychological intervention was associated with immediate improvements related to the cognitive, emotional and behavioral functioning in patients with rheumatic diseases and comorbid emotional disorders. Also, this approach could positively impact the experience of pain, anxiety and depression, outside of the in-patient context. However, further studies are required for drawing firm conclusions regarding the benefits of single-session approaches using a process-based framework with the medical milieu.
Author Contributions
Conceptualization, C.M.C., C.P., and A.S.; methodology, C.P., Z.J., B.A.S., and S.S.; software, B.A.S., and P.O.; validation, C.M.C., C.P., A.S., B.A.S., and H.P.; formal analysis, C.P., B.A.S., and P.O.; investigation, C.M.C., A.S., and S.S.; resources P.O., H.P., and S.S.; data curation, C.M.C., A.S., and S.S.; writing—original draft preparation, C.M.C., C.P., and A.S.; writing—review and editing, C.M.C., C.P., A.S., and Z.J.; visualization, Z.J., B.A.S., and H.P.; supervision, C.P. and B.A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Ethics Committee of the Targu Mures County Emergency Clinical Hospital from 27.07.2023 under the number 19622.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author (cosmin.popa@umfst.ro).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Anyfanti, P.; Gavriilaki, E.; Pyrpasopoulou, A.; Triantafyllou, G.; Triantafyllou, A.; Chatzimichailidou, S.; Gkaliagkousi, E.; Aslanidis, S.; Douma, S. Depression, anxiety, and quality of life in a large cohort of patients with rheumatic diseases: common, yet undertreated. Clin Rheumatol 2016, 35, 733–739. [CrossRef]
- Marchi, L.; Marzetti, F.; Orrù, G.; Lemmetti, S.; Miccoli, M.; Ciacchini, R.; Hitchcott, P.K.; Bazzicchi, L.; Gemignani, A.; Conversano, C. Alexithymia and Psychological Distress in Patients With Fibromyalgia and Rheumatic Disease. Front Psychol 2019, 10, 1735. [CrossRef]
- Matcham, F.; Rayner, L.; Steer, S.; Hotopf, M. The prevalence of depression in rheumatoid arthritis: a systematic review and me-ta-analysis. Rheumatology 2013, 52(12), 2136–2148. [CrossRef]
- Sarzi-Puttini, P.; Atzeni, F.; Clauw, D.J.; Perrot, S. The impact of pain on systemic rheumatic diseases. Best Pract Res Clin Rheumatol 2015, 29(1), 1–5. [CrossRef]
- Cohen, S.; Vase, L.; Hooten, W. Chronic pain: an update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [CrossRef]
- Parks, C.G.; Pettinger, M.; de Roos, A.J.; Tindle, H.A.; Walitt, B.T.; Howard, B.V. Life Events, Caregiving, and Risk of Autoimmune Rheumatic Diseases in the Women’s Health Initiative Observational Study. Arthritis Care Res 2023, 75(12), 2519-2528. [CrossRef]
- Luo, G.; Boelle, P.Y.; Turbelin, C.; Costantino, F.; Kerneis, S.; Said Nahal, R.; Breban, M.; Hanslik, T. Abrupt and unexpected stressful life events are followed with increased disease activity in spondyloarthritis: A two years web-based cohort study. Joint Bone Spine 2019, 86(2), 203–209. [CrossRef]
- Adnine, A.; Nadiri, K.; Soussan, I.; Coulibaly, S.; Berrada, K.; Najdi, A.; Abourazzak, F.E. Mental Health Problems Experienced by Patients with Rheumatic Diseases During COVID-19 Pandemic. Curr Rheumatol Rev 2021, 17(3), 303–311. [CrossRef]
- Nasui, B.A.; Toth, A.; Popescu, C.A.; Penes, O.N.; Varlas, V.N.; Ungur, R.A.; Ciuciuc, N.; Silaghi, C.A.; Silaghi, H.; Pop, A.L Comparative Study on Nutrition and Lifestyle of Information Technology Workers from Romania before and during COVID-19 Pandemic. Nutrients 2022, 14(6), 1202. [CrossRef]
- Nasui, B.A.; Ungur, R.A.; Nasui, G.A.; Popescu, C.A.; Hofer, A.M.; Dersidan, S.; Popa, M.; Silaghi, H.; Silaghi, C.A. Adolescents’ Lifestyle Determinants in Relation to Their Nutritional Status during COVID-19 Pandemic Distance Learning in the North-Western Part of Romania—A Cross-Sectional Study. Children 2023, 10, 922. [CrossRef]
- Daïen, C.I.; Tubery, A.; Beurai-Weber, M.; du Cailar, G.; Picot, M.C.; Jaussent, A.; Roubille, F.; Cohen, J.D.; Morel, J.; Bousquet, J.; Fesler, P.; Combe, B. Relevance and feasibility of a systematic screening of multimorbidities in patients with chronic inflammatory rheumatic diseases. Joint Bone Spine 2019, 86(1), 49–54. [CrossRef]
- Golenbiewski, J.T.; Pisetsky, D.S. A Holistic Approach to Pain Management in the Rheumatic Diseases. Curr Treat Options Rheumatol 2019, 5(1), 1–10. [CrossRef]
- Fraenkel, L.; Bathon, J.M.; England, B.R.; St Clair, E.W.; Arayssi, T.; Carandang, K.; Deane, K.D.; Genovese, M.; Huston, K.K.; Kerr, G.; et al. 2021 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis Care Res 2021, 73(7), 924-939. [CrossRef]
- Kolasinski, S.L.; Neogi, T., Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felsonet, D.; al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee [published correction appears in Arthritis Care Res 2021, 73(5), 764]. Arthritis Care Res 2020, 72(2), 149-162. [CrossRef]
- Fashler, S.R.; Cooper, L.K.; Oosenbrug, E.D.; Burns, L.C.; Razavi, S.; Goldberg, L.; Katz, J. Systematic Review of Multidisciplinary Chronic Pain Treatment Facilities. Pain Res Manag 2016, 2016, 5960987. [CrossRef]
- APA Division 12. Psychological treatment of chronic or persistent pain. Society of Clinical Psychology. 2012. Available at: http://www.psychologicaltreatments.org (accessed on 25 October 2023).
- Scott, A.J.; Bisby, M.A.; Heriseanu, A.I.; Salameh, Y.; Karin, E.; Fogliati, R.; Dudeney, J.; Gandy, M.; McLellan, L.F.; Wootton, B.; et al. Cognitive behavioral therapies for depression and anxiety in people with chronic disease: A systematic review and meta-analysis. Clin Psychol Rev 2023, 106, 102353. [CrossRef]
- Geenen, R.; Newman, S.; Bossema, E.R.; Vriezekolk, J.E.; Boelen, P.A. Psychological interventions for patients with rheumatic diseases and anxiety or depression. Best Pract Res Clin Rheumatol 2012, 26(3), 305–319. [CrossRef]
- Ehde, D.M.; Dillworth, T.M.; Turner, J.A. Cognitive-behavioral therapy for individuals with chronic pain: Efficacy, innovations, and directions for research. Am Psychol 2014, 69(2), 153–166. [CrossRef]
- Butler, A.C.; Chapman, J.E.; Forman, E.M.; Beck, A.T. The empirical status of cognitive-behavioral therapy: A review of meta-analyses. Clin Psychol Rev 2006, 26(1), 17–31. [CrossRef]
- Beard, C.; Millner, A.J.; Forgeard, M.J.; Fried, E.I.; Hsu, K.J.; Treadway, M.T.; Leonard, C.V.; Kertz, S.J.; Björgvinsson, T. Network analysis of depression and anxiety symptom relationships in a psychiatric sample. Psychol Med 2016, 46(16), 3359-3369. [CrossRef]
- Hofmann, S.G. Psychotherapeutic Interventions and Processes. Cogn Behav Pract 2022, 29(3), 581–584. [CrossRef]
- Sanford, B.; Ciarrochi, J.; Hofmann, S.; Chin, F.; Gates, K.; Hayes, S. Toward empirical process-based case conceptualization: An idionomic network examination of the process-based assessment tool. J Contextual Behav Sci 2022, 25(4). [CrossRef]
- Hayes, S.C.; Hofmann, S.G.; Ciarrochi, J. A process-based approach to psychological diagnosis and treatment: The conceptual and treatment utility of an extended evolutionary meta model. Clin Psychol Rev 2020, 82, 101908. [CrossRef]
- Du, S.; Dong, J.; Jin, S.; Zhang, H.; Zhang, Y. Acceptance and Commitment Therapy for chronic pain on functioning: A systematic review of randomized controlled trials. Neurosci Biobehav Rev 2021, 131, 59–76. [CrossRef]
- Godfrey, E.; Wileman, V.; Galea Holmes, M.; McCracken, L.M.; Norton, S.; Moss-Morris, R.; Noonan, S.; Barcellona, M.; Critchley, D. Physical Therapy Informed by Acceptance and Commitment Therapy (PACT) Versus Usual Care Physical Therapy for Adults With Chronic Low Back Pain: A Randomized Controlled Trial. J Pain 2020, 21(1-2), 71-81. [CrossRef]
- Malins, S.; Biswas, S.; Rathbone, J., Vogt, W.; Pye, N.; Levene, J.; Moghaddam, N.; Russell, J. Reducing dropout in acceptance and commitment therapy, mindfulness-based cognitive therapy, and problem-solving therapy for chronic pain and cancer patients using motivational interviewing. Br J Clin Psychol 2020, 59(3), 424-438. [CrossRef]
- Twohig, M.P.; Levin, M.E. Acceptance and Commitment Therapy as a Treatment for Anxiety and Depression: A Review. Psy-chiatr Clin North Am 2017, 40(4), 751-770. [CrossRef]
- Hughes, L.S.; Clark, J.; Colclough, J.A.; Dale, E.; McMillan, D. Acceptance and Commitment Therapy (ACT) for Chronic Pain: A Systematic Review and Meta-Analyses. Clin J Pain 2017, 33(6), 552-568. [CrossRef]
- Wetherell, J.L.; Afari, N.; Rutledge, T.; Sorrell, J.T.; Stoddard, J.A.; Petkus, A.J.; Solomon, B.C.; Lehman, D.H.; Liu, L.; Lang, A.J.; Atkinson, H.J. A randomized, controlled trial of acceptance and commitment therapy and cognitive-behavioral therapy for chronic pain. Pain. 2011, 152(9), 2098-2107. [CrossRef]
- Levin, M.E.; MacLane, C.; Daflos, S.; Seeley, J.R; Hayes, S.C.; Biglan, A.; Pistorello, J. Examining psychological inflexibility as a transdiagnostic process across psychological disorders. J Contextual Behav Sci 2014, 3(3), 155–163. [CrossRef]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and commitment therapy: The process and practice of mindful change. New York, NY: Guilford Press, USA, 2011.
- Popa, C.O.; Rus, A.V.; Lee, W.C.; Cojocaru, C.; Schenk, A.; Văcăraș, V.; Olah, P.; Mureșan, S.; Szasz, S.; Bredicean, C. The Relation between Negative Automatic Thoughts and Psychological Inflexibility in Schizophrenia. J Clin Med 2022, 11, 871. [CrossRef]
- Faustino, B.; Vasco, A.B.; Farinha-Fernandes, A.; Delgado, J. Psychological inflexibility as a transdiagnostic construct: relationships between cognitive fusion, psychological well-being and symptomatology. Curr Psychol 2023, 42(8), 6056–6061. [CrossRef]
- Harris, R. ACT made simple: An easy-to-read primer on acceptance and commitment therapy, 2nd ed. Oakland, CA: New Harbinger Publications, USA, 2019.
- Larsson, A.; Hooper, N.; Osborne, L.A.; Bennett, P.; McHugh, L. Using brief cognitive restructuring and cognitive defusion tech-niques to cope with negative thoughts. Behav Modif 2016, 40(3), 452–482. [CrossRef]
- Chawla, N.; Ostafin, B. Experiential avoidance as a functional dimensional approach to psychopathology: An empirical review. J Clin Psychol 2007, 63(9), 871-890. [CrossRef]
- Kratz, A.L.; Ehde, D.M.; Bombardier, C.H.; Kalpakjian, C.Z.; Hanks, R.A. Pain acceptance decouples the momentary associations between pain, pain interference, and physical activity in the daily lives of people with chronic pain and spinal cord injury. J Pain. 2017, 18(3), 319-331. [CrossRef]
- Wright, M.A.; Wren, A.A.; Somers, T.J.; Goetz, M.C.; Fras, A.M.; Huh, B.K.; Rogers, L.L.; Keefe, F.J. Pain acceptance, hope, and optimism: relationships to pain and adjustment in patients with chronic musculoskeletal pain. J Pain 2011, 12(11), 1155-1162. [CrossRef]
- Branstetter-Rost, A.; Cushing, C.; Douleh, T. Personal values and pain tolerance: Does a values intervention add to acceptance? J Pain. 2009, 10(8), 887-892. [CrossRef]
- Dryden W. Single-Session One-At-A-Time Therapy: A Personal Approach. Aust N Z J Fam Ther 2020, 41, 283-301. [CrossRef]
- Campbell A. Single-Session Approaches to Therapy: Time to Review. Aust N Z J Fam Ther 2012, 33(1), 15–26. [CrossRef]
- Dochat, C.; Wooldridge, J.S.; Herbert, M.S.; Lee, M.W.; Afari, N. Single-Session Acceptance and Commitment Therapy (ACT) Interventions for Patients with Chronic Health Conditions: A Systematic Review and Meta-Analysis. J Contextual Behav Sci 2021, 20, 52-69. [CrossRef]
- Darnall, B.D.; Roy, A.; Chen, A.L., Ziadni, M.S.; Keane, R.T.; You, D.S.; Slater, K.; Poupore-King, H.; Mackey, I.; Kao, M.C.; et al. Comparison of a Single-Session Pain Management Skills Intervention With a Single-Session Health Education Intervention and 8 Sessions of Cognitive Behavioral Therapy in Adults With Chronic Low Back Pain: A Randomized Clinical Trial [published correction appears in JAMA Netw Open 2022, 5(4), e229739]. JAMA Netw Open 2021, 4(8), e2113401. [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Res Methods 2007, 39(2), 175-191. [CrossRef]
- Sava, F. Inventarul de Personalitate DECAS. Timişoara: ArtPress, Romania, 2008.
- McCrae, R.R.; Costa, P.T. Validation of the five-factor model of personality across instruments and observers. J Pers Social Psychol 1987, 52(1), 81–90. [CrossRef]
- Barlow, D.H.; Curreri, A.J.; Woodard, L.S. Neuroticism and Disorders of Emotion: A New Synthesis. Curr Dir Psychol Sci 2021, 30(5), 410–417. [CrossRef]
- Sava, F.A.; Popa, R.I. Personality types based on the Big Five model. A cluster analysis over the Romanian population. Cogn Brain Behav 2011, 15(3), 359-384.
- First, M.B.; Williams, J.B.; Karg, R.S.; Spitzer, R.L. SCID-5-CV: Structured Clinical Interview for DSM-5 Disorders: Clinician Version. Washington, DC: American Psychiatric Association Publishing, USA, 2016.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM) 5th ed. Washington, DC: American Psychiatric Association, USA, 2013.
- Shabani, A.; Masoumian, S.; Zamirinejad, S.; Hejri, M.; Pirmorad, T.; Yaghmaeezadeh, H. Psychometric properties of Structured Clinical Interview for DSM-5 Disorders-Clinician Version (SCID-5-CV). Brain Behav 2021, 11(5), e01894. [CrossRef]
- Osório, F.L.; Loureiro, S.R.; Hallak, J.E.C.; Machado-de-Sousa, J.P.; Ushirohira, J.M.; Baes, C.V.W.; Apolinario, T.D.; Donadon, M.F.; Bolsoni, L.M.; Guimarães, T.; et al. Clinical validity and intrarater and test-retest reliability of the Structured Clinical Interview for DSM-5 - Clinician Version (SCID-5-CV). Psychiatry Clin Neurosci 2019, 73(12), 754-760. [CrossRef]
- Jollant, F.; Voegeli, G.; Kordsmeier, N.C.; Carbajal, J.M.; Richard-Devantoy, S.; Turecki, G.; Cáceda, R. A visual analog scale to measure psychological and physical pain: A preliminary validation of the PPP-VAS in two independent samples of depressed patients. Prog Neuropsychopharmacol Biol Psychiatry 2019, 90, 55–61. [CrossRef]
- Williamson, A.; Hoggart, B. Pain: a review of three commonly used pain rating scales. J Clin Nurs 2005, 14(7), 798–804. [CrossRef]
- Wolfe F. Fatigue assessments in rheumatoid arthritis: comparative performance of visual analog scales and longer fatigue questionnaires in 7760 patients. J Rheumatol 2004, 31(10), 1896–1902.
- Huang, Z.; Kohler, I.V.; Kämpfen, F. A Single-Item Visual Analogue Scale (VAS) Measure for Assessing Depression Among College Students. Community Ment. Health J 2020, 56(2), 355–367. [CrossRef]
- Williams, V.S.; Morlock, R.J.; Feltner, D. Psychometric evaluation of a visual analog scale for the assessment of anxiety. Health Qual Life Outcomes 2010, 8, 57. [CrossRef]
- Ciarrochi, J.; Sahdra, B.; Hofmann, S.G.; Hayes, S.C. Developing an item pool to assess processes of change in psychological interventions: The Process-Based Assessment Tool (PBAT). J Contextual Behav Sci 2022, 23, 200-213. [CrossRef]
- Hayes, S.C.; Hofmann, S.G.; Ciarrochi, J. A process-based approach to psychological diagnosis and treatment: The conceptual and treatment utility of an extended evolutionary meta model. Clinical Psychol Rev 2020, 82, 101908. [CrossRef]
- Bond, F.W.; Hayes, S.C.; Baer, R.A.; Carpenter, K.M.; Guenole, N.; Orcutt, H.K.; Waltz, T.; Zettle, R.D. Preliminary Psychometric Properties of the Acceptance and Action Questionnaire–II: A Revised Measure of Psychological Inflexibility and Experiential Avoidance. Behav Ther 2011, 42, 676–688. [CrossRef]
- Szabó, K.G.; Vargha, J.L.; Balázsi, R.; Bartalus, J.; Bogdan V. Measuring Psychological Flexibility: Preliminary Data on the Psychometric Properties of the Romanian Version of the Acceptance and Action Questionnaire (AAQ-II) J Cogn Behav Psychother 2011, 11, 67–82.
- Gillanders, D.; Bolderston, H.; Bond, F.W.; Dempster, M.; Flaxman, P.E.; Campbell, L.; Remington, B. The development and initial validation of the Cognitive Fusion Questionnaire. Behav Ther 2014, 45, 83–101. [CrossRef]
- Vowles, K.E.; McCracken, L.M. Acceptance and values-based action in chronic pain: A study of treatment effectiveness and process. J Consult Clin Psychol 2008, 76(3), 397–407. [CrossRef]
- Dahl, J.C.; Lundgren, T.L. Living beyond your pain: Using Acceptance and Commitment Therapy to ease chronic pain. Oakland, CA: New Harbinger Publications, USA, 2006.
- Hayes, S.C.; Strosahl, K.; Wilson, K.G. Acceptance and commitment therapy: An experiential approach to behavior change. New York, NY: Guilford Press, USA, 1999.
- Sturgeon, J.A.; Finan, P.H.; Zautra, A.J. Affective disturbance in rheumatoid arthritis: psychological and disease-related pathways. Nat Rev Rheumatol 2016, 12, 532–542. [CrossRef]
- Usubini, A.G.; Varallo, G.; Giusti, E.M.; Cattivelli, R.; Granese, V.; Consoli, S.; Bastoni, I.; Volpi, C.; Castelnuovo, G. The mediating role of psychological inflexibility in the relationship between anxiety, depression, and emotional eating in adult individuals with obesity. Front Psychol 2022, 13, 861341. [CrossRef]
- Crocker, L.D.; Heller, W.; Warren, S.L.; O'Hare, A.J.; Infantolino, Z.P.; Miller, G.A. Relationships among cognition, emotion, and motivation: implications for intervention and neuroplasticity in psychopathology. Front Hum Neurosci 2013, 11, 7:261. [CrossRef]
- Beck, A.T.; Haigh, E.A. Advances in cognitive theory and therapy: The generic cognitive model. Annu Rev Clin Psychol 2014, 10, 1-24. [CrossRef]
- Leonard, M.T.; Chatkoff, D.K.; Maier, K.J. Couples' Relationship Satisfaction and Its Association with Depression and Spouse Responses Within the Context of Chronic Pain Adjustment. Pain Manag Nurs 2019, 19(4), 400-407. [CrossRef]
- Van Damme, S.; Becker, S.; Van der Linden, D. Tired of pain? Toward a better understanding of fatigue in chronic pain. Pain 2018, 159(1), 7-10. [CrossRef]
- Dindo, L.; Zimmerman, M.B.; Hadlandsmyth K, StMarie, B.; Embree, J.; Marchman, J.; Tripp-Reimer, T.; Rakel, B. Acceptance and Commitment Therapy for Prevention of Chronic Postsurgical Pain and Opioid Use in At-Risk Veterans: A Pilot Randomized Controlled Study. J Pain 2018, 19(10), 1211-1221. [CrossRef]
- Åkerblom, S.; Perrin, S.; Rivano Fischer, M.; McCracken, L.M. The Mediating Role of Acceptance in Multidisciplinary Cognitive-Behavioral Therapy for Chronic Pain [published correction appears in J Pain 2016, 17(10), 1135-1136]. J Pain 2015, 16(7), 606-615. [CrossRef]
- Simister, H.D.; Tkachuk, G.A.; Shay, B.L.; Vincent, N.; Pear, J.J.; Skrabek, R.Q. Randomized controlled trial of online acceptance and commitment therapy for fibromyalgia. J Pain 2018, 19(7), 741-753. [CrossRef]
- Alda, M.; Luciano, J.V.; Andrés, E.; Serrano-Blanco, A.; Rodero, B.; del Hoyo, Y.L.; Roca, M.; Moreno, S.; Magallón, R.; García-Campayo, J. Effectiveness of cognitive behaviour therapy for the treatment of catastrophisation in patients with fibromyalgia: a randomised controlled trial. Arthritis Res Ther 2011, 13(5), R173. [CrossRef]
- Darnall, B.D.; Sturgeon, J.A.; Kao, M.C.; Hah, J.M.; Mackey, S.C. From catastrophizing to recovery: a pilot study of a single-session treatment for pain catastrophizing. J Pain Res 2014, 7, 219-226. [CrossRef]
- Gilliam, W.P.; Schumann, M.E.; Cunningham, J.L.; Evans, M.M.; Luedtke, C.A.; Morrison, E.J.; Sperry, J.A.; Vowles, K.E. Pain catastrophizing as a treatment process variable in cognitive behavioural therapy for adults with chronic pain. Eur J Pain 2021, 25(2), 339-347. [CrossRef]
- Nasiri, A.; Kazemi-Zahrani, H. The Effectiveness of Group Acceptance and Commitment Therapy on Pain Intensity, Pain Catastrophizing and Pain-Associated Anxiety in Patients with Chronic Pain. Asian Soc Sci 2015, 11(26). [CrossRef]
- Nijs, J.; D’Hondt, E.; Clarys, P.; Deliens, T.; Polli, A.; Malfliet, A.; Coppieters, I.; Willaert, W.; Tumkaya Yilmaz, S.; Elma, Ö.; Ickmans, K. Lifestyle and Chronic Pain across the Lifespan: An Inconvenient Truth? PM R 2020, 12(4), 410–419. [CrossRef]
- Znidarsic, J.; Kirksey, K.N.; Dombrowski, S.M.; Tang, A.; Lopez, R.; Blonsky, H.; Todorov, I.; Schneeberger, D.; Doyle, J.; Libertiniet, L.; et al. “Living Well with Chronic Pain”: Integrative Pain Management via Shared Medical Appointments. Pain Med 2021, 22(1), 181–190. [CrossRef]
- Will, K.K.; Johnson, M.L.; Lamb, G. Team-Based Care and Patient Satisfaction in the Hospital Setting: A Systematic Review. J Patient Cent Res Rev 2019, 6(2), 158-171. [CrossRef]
- Moore, A.J.; Holden, M.A.; Foster, N.E.; Jinks C. Therapeutic alliance facilitates adherence to physiotherapy-led exercise and physical activity for older adults with knee pain: a longitudinal qualitative study. J Physiother 2020, 66(1), 45–53. [CrossRef]
- Vowles, K.E.; Sowden, G.; Hickman, J.; Ashworth, J. An analysis of within-treatment change trajectories in valued activity in relation to treatment outcomes following interdisciplinary Acceptance and Commitment Therapy for adults with chronic pain. Behav Res Ther 2019, 115, 46–54. [CrossRef]
- Jensen, M.P.; Vowles, K.E.; Johnson, L.E.; Gertz, K.J. Living Well with Pain: Development and Preliminary Evaluation of the Valued Living Scale. Pain Med 2015, 16(11), 2109–2120. [CrossRef]
- McCracken, L.M.; Gutiérrez-Martínez, O. Processes of change in psychological flexibility in an interdisciplinary group-based treatment for chronic pain based on Acceptance and Commitment Therapy. Behav Res Ther 2011, 49(4), 267–274. [CrossRef]
- Kanzler, K.E.; Robinson, P.J.; McGeary, D.D.; Mintz, J.; Kilpela, L.S.; Finley, E.P.; McGeary, C.; Lopez, E.J.; Velligan, D.; Munante, M.; et al. Addressing chronic pain with Focused Acceptance and Commitment Therapy in integrated primary care: findings from a mixed methods pilot randomized controlled trial. BMC Prim Care 2022, 23(1), 77. [CrossRef]
- Ntoumanis, N.; Ng, J.Y.Y.; Prestwich, A.; Quested, E.; Hancox, J.E.; Thøgersen-Ntoumani, C.; Deci, E.L.; Ryan, R.M.; Lonsdale, C.; Williams, G.C. A meta-analysis of self-determination theory-informed intervention studies in the health domain: effects on motivation, health behavior, physical, and psychological health. Health Psychol Rev 2021, 15(2), 214–244. [CrossRef]
- Sheeran, P.; Wright, C.E.; Avishai, A.; Villegas, M.E.; Rothman, A.J.; Klein, W.M.P. Does increasing autonomous motivation or perceived competence lead to health behavior change? A meta-analysis. Health Psychol 2021, 40(10), 706–716. [CrossRef]
- Brooks, J.M.; Huck, G.; Iwanaga, K.; Chan, F.; Wu, J.R.; Finnicum, C.A., Brinck, E.A.; Estala-Gutierrez, V.Y.Towards an inte-gration of the health promotion models of self-determination theory and theory of planned behavior among people with chronic pain. Rehabil Psychol 2018, 63(4), 553–62. [CrossRef]
- Uysal, A.; Ascigil, E.; Turunc, G. Spousal autonomy support, need satisfaction, and well-being in individuals with chronic pain: A longitudinal study. J Behav Med 2017, 40(2), 81–92. [CrossRef]
- Vriezekolk, J.E.; Geenen, R.; van den Ende, C.H.M.; Slot, H.; van Lankveld, W.G.J.M.; van Helmond, T. Behavior change, acceptance, and coping flexibility in highly distressed patients with rheumatic diseases: Feasibility of a cognitive-behavioral therapy in multimodal rehabilitation. Patient Educ Couns 2012, 87(2), 171–7. [CrossRef]
- Hajihasani, A.; Rouhani, M.; Salavati, M.; Hedayati, R.; Kahlaee, A.H. The influence of cognitive behavioral therapy on pain, quality of life, and depression in patients receiving physical therapy for chronic low back pain: a systematic review. PM R 2019, 11(2), 167-76. [CrossRef]
- Ma, T.W.; Yuen, A.S.; Yang, Z.The efficacy of acceptance and commitment therapy for chronic pain: A systematic review and meta-analysis. Clin J Pain 2023, 39(3), 147-57. [CrossRef]
- Burns, J.W.; Jense, M.P.; Thorn, B.; Lillis, T.A.; Carmody, J.; Newman, A.K.; Keefe, F. Cognitive therapy, mindfulness-based stress reduction, and behavior therapy for the treatment of chronic pain: randomized controlled trial. Pain 2022, 163(2), 376-389. [CrossRef]
- Alonso-Fernández, M.; López-López, A.; Losada, A.; González, J.L.; Wetherell, J.L. Acceptance and Commitment Therapy and Selective Optimization with Compensation for Institutionalized Older People with Chronic Pain. Pain Med 2016, 17(2), 264-277. [CrossRef]
- Ólason, M.; Andrason, R.H.; Jónsdóttir, I.H.; Kristbergsdóttir, H.; Jensen, M.P. Cognitive Behavioral Therapy for Depression and Anxiety in an Interdisciplinary Rehabilitation Program for Chronic Pain: a Randomized Controlled Trial with a 3-Year Fol-low-up. Int J Behav Med 2018, 25(1), 55–66. [CrossRef]
- Clarke, S.P.; Poulis, N.; Moreton, B.J.; Walsh, D.A.; Lincoln, N.B. Evaluation of a group acceptance commitment therapy intervention for people with knee or hip osteoarthritis: A pilot randomized controlled trial. Disabil Rehabil 2017, 39(7), 663–670. [CrossRef]
- Trompetter, H.R.; Bohlmeijer, E.T.; Veehof, M.M; Schreurs, K.M. Internet-based guided self-help intervention for chronic pain based on Acceptance and Commitment Therapy: a randomized controlled trial. J Behav Med 2015, 38, 66-80. [CrossRef]
- Luciano, J.V.; Guallar, J.A.; Aguado, J.; López-Del-Hoyo,Y.; Olivan, B.; Magallón, R.; Alda, M.; Serrano-Blanco, A.; Gili, M.; Garcia-Campayo, J. Effectiveness of group acceptance and commitment therapy for fibromyalgia: a 6-month randomized con-trolled trial (EFFIGACT study). Pain 2013, 155(4), 693–702. [CrossRef]
- Garnefski, N.; Kraaij, V.; Benoist, M.; Bout, Z.; Karels, E.; Smit A. Effect of a Cognitive Behavioral Self-Help Intervention on Depression, Anxiety, and Coping Self-Efficacy in People With Rheumatic Disease. Arthritis Care Res (Hoboken) 2013, 65(7), 1077–84. [CrossRef]
- Joypaul, S.; Kelly, F.S.; King, M.A. Turning pain into gain: evaluation of a multidisciplinary chronic pain management pro-gram in primary care. Pain Med. 2019, 20(5), 925-33. [CrossRef]
- Casey, M.; Smart, K.; Segurado, R.; Doody C. Multidisciplinary-based Rehabilitation (MBR) Compared With Active Physical Interventions for Pain and Disability in Adults With Chronic Pain A Systematic Review and Meta-analysis. Clin J Pain 2020, 36(11), 874–86. [CrossRef]
- Fashler, S.R.; Cooper, L.K.; Oosenbrug, E.D.; Burns, L.C.; Razavi, S.; Goldberg, L.; Katz, J. Systematic Review of Multidisci-plinary Chronic Pain Treatment Facilities. Pain Res Manag 2016, 2016, 5960987. [CrossRef]
- Sumner, L.A.; IsHak, W.W.; Dang, J., Vanle, B.; Mahtani, N.; Danovitch, I. Psychological interventions in inpatient medical settings: A brief review. Int J Healthc Med Sci 2018, 4, 73-83.
- Davis, J.P.; Prindle, J.J.; Eddie, D.; Pedersen, E.R.; Dumas, T.M.; Christie, N.C. Addressing the opioid epidemic with be-havioral interventions for adolescents and young adults: A quasi-experimental design. J Consult Clin Psychol 2019, 87(10), 941–951. [CrossRef]
- Vassilopoulou, E.; Efthymiou, D.; Papatriantafyllou, E.; Markopoulou, M.; Sakellariou, E.M.; Popescu, A.C. Long Term Metabolic and Inflammatory Effects of Second-Generation Antipsychotics: A Study in Mentally Disordered Offenders. J Pers Med 2021, 11(11), 1189. [CrossRef]
- Tagliaferri, S.D.; Miller, C.T.; Owen, P.J.; Mitchell, U.H.; Brisby, H.; Fitzgibbon, B.; Masse-Alarie, H.; Van Oosterwijck, J.; Belavy D.L. Domains of chronic low back pain and assessing treatment effectiveness: a clinical perspective. Pain Pract 2020, 20(2), 211-25. [CrossRef]
- Jack, K.; McLean, S.M.; Moffett, J.K.; Gardiner E. Barriers to treatment adherence in physiotherapy outpatient clinics: a sys-tematic review. Man Ther 2010, 15, 220–228. [CrossRef]
- Li, J.; Li, X.; Jiang, J.; Xu, X.; Wu, J.; Xu, Y.; Lin, X.; Hall, J., Xu, H.; Xu, J.; Xu, X. The effect of cognitive behavioral therapy on depression, anxiety, and stress in patients with COVID-19: a randomized controlled trial. Front Psychiatry 2020, 11, 580827. [CrossRef]
Figure 1.
The flow diagram of the study procedure.
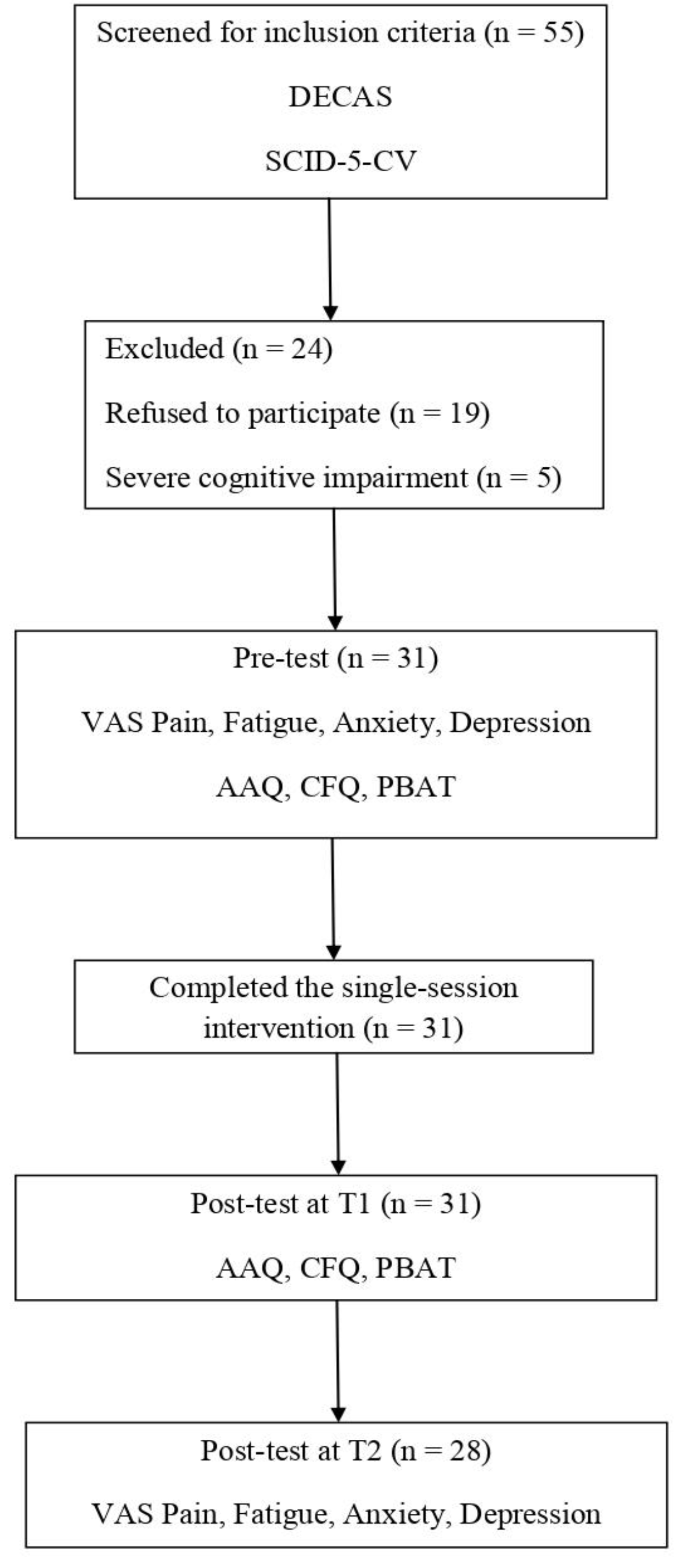
Figure 2.
The single-session protocol implemented in the study.
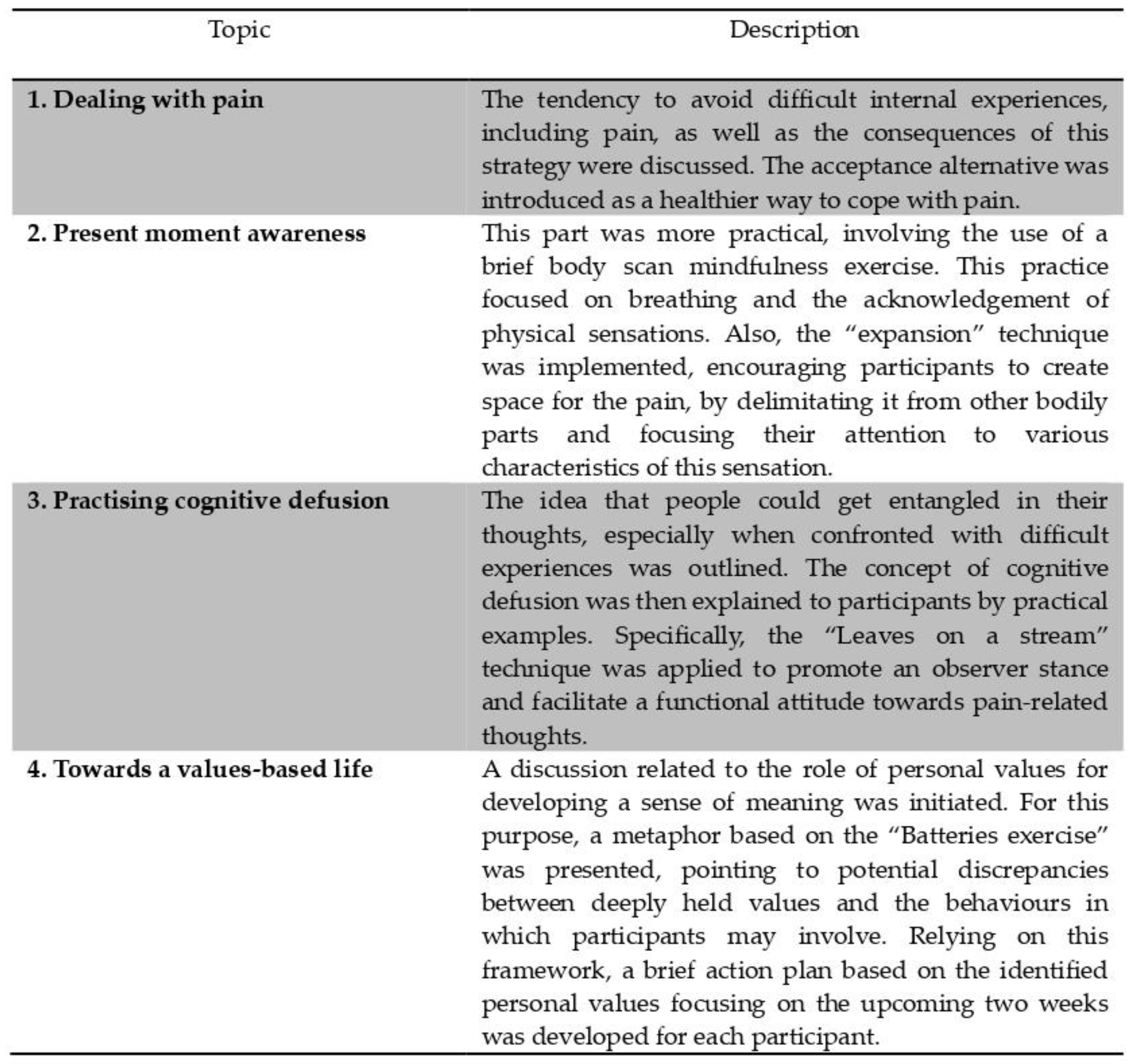
Table 1.
Descriptive characteristics of the study sample.
| Age (M, SD) | 58.9 (12.03) |
| Gender (N,%) | |
| Female | 29 (94) |
| Male | 2 (6) |
| Marital status | |
| Married | 25 (81) |
| Single | 1 (3) |
| Widowed | 5 (16) |
| Occupational status | |
| Employed | 4 (13) |
| Unemployed | 8 (26) |
| Retired | 19 (61) |
| Main diagnosis | |
| Ankylosing spondylitis | 1 (3) |
| Chronic post-surgical pain | 2 (7) |
| Coxarthrosis/ Gonarthrosis | 2 (7) |
| Osteoarthritis | 9 (29) |
| Psoriatic arthritis | 1 (3) |
| Rheumatoid arthritis | 10 (32) |
| Spondylosis (cervical/ lumbar)Psychodiagnosis | 6 (19) |
| GAD1 | 16 |
| MDD2 | 3 |
| GAD1 + MDD2 | 12 |
| Pain intensity (M, SD) | 8.12 (1.78) |
| Fatigue | 8.09 (2) |
| State_Anxiety | 6.54 (2.89) |
| State_Depression | 6.35 (2.52) |
Abbrreviations: 1. Generalized Anxiety Disorder; 2. Major Depressive Disorder.
Table 2.
Correlations between baseline measures.
| Dimension | Pain | Fatigue | Anxiety | Depression | Experiential Avoidance | Cognitive Fusion |
|---|---|---|---|---|---|---|
| Hurt Connect | .40* | -.07 | .07 | -.04 | .24 | .31 |
| Experience Range Emotions | -.31 | .06 | -.17 | -.17 | -.39* | -.36* |
| Thinking Got In Way | .22 | .09 | .42* | .13 | .33 | .30 |
| Important Challenge | -.08 | .49** | .01 | .23 | -.10 | -.10 |
| Stuck Unable Change | -.08 | -.37* | -.08 | -.21 | -.11 | -.10 |
| Thinking Helped Life | -.29 | .18 | -.13 | .04 | -.41* | -.35* |
| Struggle Connect Moments | -.23 | .27 | -.20 | -.06 | -.35* | -.30 |
| Connect To People | -.12 | .41* | -.10 | -.06 | -.29 | -.33 |
| Personal Impor | -.09 | .41* | -.09 | .13 | -.22 | -.16 |
| Hurt Health | .17 | -.01 | .11 | .11 | .45** | .60** |
| Pain | - | .34 | .40* | .24 | .29 | .43* |
| Fatigue | - | .23 | .41* | .07 | .02 | |
| State Anxiety | - | .14 | .37* | .28 | ||
| State Depression | - | .16 | .18 | |||
| Experiential Avoidance | - | .60** |
* p < .05; ** p < .01 (2-tailed).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



