
Submitted:
25 December 2023
Posted:
26 December 2023
You are already at the latest version
Abstract
Modern gastroenterology, which occupies the pages of scientific journals without alternative, began as an initiative of manufacturers of diagnostic equipment. For widespread advertising, they selected practical doctors who were not familiar with the methodology of science and superficial knowledge of physiology. This is how a group led by DeMeester arose, which in 1976 published the DeMeester score, i.e., the normal limit for esophageal pH monitoring. pH <4, less than 4% of the time per day was considered normal, i.e., it was unreasonably claimed that such reflux is physiological. This article proves that this study was carried out with numerous methodological errors, which led to an erroneous conclusion. For a long time, pH monitoring was considered the gold standard and with its help hypotheses were proposed that form the basis of modern gastroenterology. The article proves the fallacy of 13 hypotheses, which are presented as theories. Numerous articles using pH monitoring have publicized this method. Practitioners became "great scientists", equipment manufacturers became successful businessmen. Over time, they found other groups of practitioners to promote devices for impedance ph monitoring, high-resolution manometry, and many others. At the same time, a network of reviewers who believe in the infallibility of the luminaries do not allow studies that contradict their faith to be published. Thus, fundamental science was destroyed, which alone could assess the harm of false research both for science and for patients. Conclusion This study provides a list of hypotheses, that were previously considered theories, but since scientific evidence has proven these assumptions to be false, they should be excluded from subsequent use and citation.
Keywords:
gastroenterology
; gastroesophageal reflux disease
; x-ray diagnosis
; pH monitoring
; physiology
; hypothesis
I. Introduction
In 1899, the famous English physiologists Bayliss and Starling published the law of the intestine, which explained peristaltic movement. This law almost immediately became one of the foundation stones of physiology about which there has never been any question or argument. In the first article the following statement was formulated. “Excitation at any point of the gut excites contraction above, inhibition below. This is the law of the intestine” [1]. Cannon latter proposed the term “myenteric reflex” the phenomenon and showed that it could at times be elicited also in the stomach [2].
Currently, even though there has not been a single study that has cast doubt on the validity of the law of the intestine, there is no mention of it in the literature. Gastrointestinal motility is associated exclusively with high-resolution manometry (HRM), where there is no place for peristalsis and the laws of physiology. The definition of normal parameters was based on physical characteristics. Control persons were selected only based on the absence of complaints. Since in a significant percentage of patients with peptic problems the disease proceeds and progresses without clinical manifestations, a certain percentage of patients were selected as controls. Secondly, HRM has not been studied in patients with different diagnoses. It is not a diagnostic method, but only a manometric characteristic. Thirdly, differences in physical characteristics (integrated relaxation pressure, the distal contractile integral, distal latency, the evaluation of the EGJ at rest, ’fragmented’ contractions, ineffective esophageal motility) together with the erroneous norm have no scientific basis [3]. Their significance was determined by the vote of specially selected practical gastroenterologists who did not know the physiology of the digestive system. Thus, HRM is not a scientifically valid diagnostic method. The combination of many physical indicators, without understanding their physiological essence and clinical diagnosis, makes HRM not only meaningless, but also a dangerous method [4].
The purpose of this review is to determine the motor function of the digestive system, using scientific research on the physiology and pathology of peristaltic organs, including the digestive tract with the bile-pancreatic system, as well as the urinary tract. Based on the above, research on HRM, as a scientifically unsubstantiated technique, is not considered in this work.
II. Types of motor function
1. Motor function of the esophagus and esophagogastric junction
In mammals, food and the air swallowed with it move from the pharynx towards the anus due to peristalsis. Only a human can drink liquids in an upright position. Since the lower esophageal sphincter (LES) opens in response to a certain pressure above it, this pressure can be created in two ways. 1). In a horizontal position, in humans, as in all animals, a bolus of any consistency, equal to the volume of one swallow, moves along the esophagus, thanks to peristalsis, in full accordance with the law of the intestine (Figure 1a, b, c. d). 2) Liquid drunk in a vertical position forms a column above the LES. When the fluid level reaches D-4, hydrostatic pressure causes the LES to open, and the fluid falls completely into the stomach. The LES remains open until the fluid is completely released into the stomach. It does not close, even though in the process of decreasing the height of the column, the pressure over the sphincter progressively decreases. This indicates that the opening of the LES is not a mechanical, but a reflex process, which occurs because of contraction of the oblique muscles of the LES, on one side attached to the wall of the esophagus, and on the other side to the lesser and greater curvature of the stomach. The opening of the lumen of the LES is accompanied by its shortening.
The mechanism of the sphincters opening was chosen by the evolution of living organisms and is especially demonstrative during the opening of the pyloric sphincter. Contraction of the oblique fibers of the pyloric sphincter leads to the opening of its lumen, which is accompanied by its shortening. The fiber attachment sites cause expansion of the antrum and the base of the duodenal bulb [6]. The mobility of the LES obeys the law of the intestine. An increase in pressure over the LES causes contraction of the segment above the bolus, and relaxation of the LES (see Figure 1. d). The pressure (tone) of the LES decreases in response to stretching of the esophagus [7,8] to allow the bolus to pass into the stomach. When the fundus or body of the stomach is distended the pressure (tone) of the LES increases to prevent reflux of aggressive gastric contents into the esophagus [9,10]. The opening of the LES is a reflex phenomenon, which is accompanied by shortening of the sphincter by several millimeters. However, the esophagogastric junction does not move. There is no scientific evidence that the esophagus shortens when swallowing. An example of misinterpretation of an x-ray examination is the case described by Kwiatek et al [11]. A patient with gastroesophageal reflux disease was examined as healthy, based on the absence of typical complaints. The abdominal part of the LES opened, causing the LES to become almost 2 times shorter, which is typical for a damaged LES in ГЭРБ patients [5]. The authors regarded shortening of the “esophagus + LES” complex as shortening of the esophagus. The contrast clip attached to the esophageal mucosa during swallowing did not move relative to the vertebra. However, the authors argued that it rose, since they compared its position relative to the moving peristalsis (phrenic ampulla).
In healthy individuals, a contrast bolus swallowed in both a vertical and horizontal position penetrates the stomach within about 5 seconds, regardless of the pressure in the stomach. Since the adult human esophagus is 25–30 cm long, the peristalsis speed in the esophagus is ≈ 10 cm/sec.
Thus, the motor function of the esophagus and esophagogastric junction (EGJ) obeys the law of the intestine.
2. Motor function of the stomach
From a functional point of view, the stomach is divided into proximal and distal parts. The proximal part, including the fundus and the body of the stomach, provides reception and temporary storage of food. It regulates intragastric pressure and stimulates the tonic advancement of the chyme into the distal part. In addition, it provides space and time for pepsin and hydrochloric acid to act in the early stages of digestion. The fundus is characterized by tonic rather than peristaltic contraction [12]. An important function of the proximal stomach is its ability to accommodate. More than a liter of food can enter the stomach without increasing intragastric pressure. A study of pressure on volunteers showed that intragastric pressure decreases moderately after eating and returns to the initial level as soon as solid food ingredients penetrate the duodenum [13]. The motor function of the proximal stomach is regulated by reflexes: receptive relaxation and gastric accommodation. Receptive relaxation is manifested by a decrease in the tone of the proximal stomach during swallowing. For example, Shafik’s study showed that «Pharyngeal distension produced a significant pressure drop of the corpus of the stomach (p < 0.05); the pyloric antrum shows no response. Upper, middle, or lower esophageal distension produced gastric response like that evoked by pharyngeal distension" [14]. Stomach accommodation is described as a relaxation reflex of the proximal stomach in response to distension. Unlike receptive relaxation, this reflex does not depend on the stimulation of the esophagus and pharynx. The method of evacuation of stomach contents depends on body position and volume of contents (Figure 2).
In a horizontal position, evacuation from the stomach is carried out using antral systole. In the distal part of the stomach, a negatively charged membrane potential is determined, on which rhythmic depolarization at three cycles per minute is superimposed. The frequency and direction of electrical activity is closely related to the slow peristaltic wave. There is evidence that the slow wave is generated by the phase depolarization of Cajal interstitial cells. These cells are located on the greater curvature of the stomach. The slow wave propagates a little faster along the greater curvature so that the myoelectric activity "running" along the greater and lesser curvatures of the stomach reaches the pylorus simultaneously [12,15]. Only every 3-5 peristaltic wave closes, forming an antral chamber. The walls of the stomach and duodenal bulb are resistant to a certain level of hydrochloric acid. The mechanisms described above protect the esophagus from reflux of gastric contents. LES prevents reflux by: (1) strengthening its tone with increasing pressure in the body of the stomach; (2) low pressure is maintained in the fundus of the stomach by receptive relaxation and gastric accommodation; (3) the evacuation of the bolus from the stomach occurs at elevated pressure only in the antrum. Portioned evacuation from the stomach protects the duodenum from damage by hydrochloric acid.
Thus, the fundus and body of the stomach do not participate in peristalsis. They exhibit tonic relaxation and contraction. The different electrical properties of ICC-IM play a critical role in creating the distinct functions of the proximal and distal regions of the stomach such that the fundus acts as a reservoir of food, the corpus as a dominant pacemaker region, while the antrum acts as a region for mixing and propulsion of food [16].
Below is evidence that the opening of the pyloric sphincter during antral systole occurs because of contraction of obliquely located longitudinal muscle fibers (Figure 3).
3. Duodenal motor function
The duodenum is about 25 cm long and is located from the pyloric sphincter to the duodenojejunal sphincter. It is divided into 4 parts. The duodenal bulb is about 2 cm long, is the first part of the duodenum and is slightly dilated. It is at the vertebral level of L1. It has a bulb shape only on radiographs when filled with chyme from the stomach and the contraction of the postbulbar sphincter. The second part of the duodenum begins at the superior duodenal flexure. It goes down to the lower border of vertebral body L3, before making a sharp turn medially into the inferior duodenal flexure and ends near the descending part. The second part contains the Kapandji sphincter [17]. In the second part, distal to the Kapandji sphincter there is the major duodenal papilla through which the pancreatic duct and common bile duct conduct pancreatic juice and bile. The third part, or horizontal part of the duodenum is 10~12 cm in length. It begins at the inferior duodenal flexure and passes transversely to the left. The third part contains Ochsner’s sphincter [17,18] with a length of 2 to 4.2 cm (3.2 ± 0.15 cm) [6]. The fourth part, or ascending part, of the duodenum passes upward up to duodenojejunal sphincter at the vertebral level L3 (Figure 4).
Contraction of the postbulbar sphincter allows a certain portion of chyme to be concentrated in the bulb. Firstly, this fact does not raise doubts about the presence of a functional sphincter. Secondly, its function does not coincide with the law of the gut, which suggests the influence of specific Cajal cells as special pacemakers. After contraction of the bulb, a chemically aggressive chyme, equal to the volume of the bulb, penetrates the duodenum, where it stops due to the contraction of the Ochsner sphincter. Our studies confirmed Ochsner’s assumption that this sphincter reacts by contracting to acid, preventing the penetration of low-pH chyme into the jejunum [6]. When the Ochsner sphincter contracts, the bolus is discarded cranially, but upon reaching the second part of the duodenum it causes contraction of the Kapandji sphincter. The repeated pendulum-like movement of the bolus between the Kapandji and Ochsner sphincters leads to the mixing of acidic chyme with bile and pancreatic secretions, which have an alkaline reaction. When the pH of the bolus increases to a certain level, the Ochsner sphincter opens and the bolus, having lost its aggressive nature, penetrates the jejunum.
Thus, the Ochsner sphincter contracts not above the bolus, as the law of the intestine states, but below it. This is probably the result of the action of specialized interstitial cells of Cajal (ICC).
4. Motor function of the small intestine
The motor function of the small intestine (jejunum and ileum) has been little studied due to its inaccessibility to manometric studies and the overlap of several loops. The length of the small intestine is on average 4.5 m. It takes 3–5 hours from entry to the duodenum to exit from the ileum. Therefore, the bolus speed is about 1 meter/hour (360 sec) = 0.28 cm/sec, i.e., the speed of passage through the small intestine is 35 times slower than through the esophagus. This is more surprising because, upon leaving the duodenum, the contrast medium quickly fills the loops of the jejunum (Figure 5).
In our search for an answer, we discovered that ICC of the deep myenteric plexus (ICC-DMP) are found exclusively in the small intestine. They are multipolar cells that are closely associated with nerve bundles of the DMP. Like ICC-IM, ICC-DMP also mediate enteric neurotransmission [20]. The slower progression through the small intestine can be explained by the periodic retrograde movement of the bolus. The mechanism by which peristalsis is reversed—for example, in conditions of luminal toxicity—is not known. However, there is the fact that reverse peristalsis does occur in the small intestine [21].
Our hypothesis suggests that slowing the movement of chyme through the small intestine allows for more complete processing and absorption of water and nutrients within the shorter length of the small intestine. An example of the functioning of the Ochsner and Kapandji sphincters in the duodenum, which is part of the small intestine, shows the mechanism of retrograde movement of chyme. Contraction of the bowel before the bolus causes the bolus to move retrograde. The pendulum-like movement between these sphincters can delay aboral movement for a long period. Probably ICC-DMP is a special type of ICC, which is an intestinal pacemaker, responsible for the retrograde movement of chyme in the small intestine.
5. Motor function of the colon
The length of the large intestine is 1.5 m. Normal colon transit is nearly complete emptying at 72 h [22]. Thus, the average speed of movement through the large intestine is 150 cm/259200 sec = 0.0006 cm/sec or 0.03 cm/min. The motor function of the colon obeys the law of the colon. The radiographs show how, as the bolus moves, its volume gradually decreases as a result of the absorption of fluid in the intestinal wall (Figure 6).
Some authors believe that segmental contractions and reverse peristalsis, mix promoting absorption occur in the colon [23], which contradicts scientific facts and is due to an erroneous interpretation of scintigraphy [24]. The motor function of the large intestine is completely subject to the law of the intestine.
III. Discussion
The “law of the intestine”, published 120 years ago, almost immediately became one of the foundation stones of physiology [1]. As this study shows, this law is as relevant as it was 120 years ago. A convincing illustration of this is the passage of large tablets through the entire digestive tract (Figure 7).
The peristaltic wave pushes the LT with a diameter of 2 cm through all sphincters, which under normal conditions open to a diameter of 2-4 mm. The BT technique can be used to bougienage rigid areas. The advantage over other methods is that it is safe, as it does not damage the sphincter muscles, and can be used repeatedly.
The law of the intestine is more accurately called the law of peristalsis since it is also true for the urinary tract and biliary tract. For example, the tone of the ureterovesical junction decreased with increasing pressure in the ureter and increased with increasing pressure in the bladder [25]. The discovery of interstitial cells of Cajal (ICC), which are called intestinal pacemakers, has opened a new era in understanding the motor function of different parts of the digestive tube. It turned out that different types of ICC have different specializations. This applies not only to different speeds of the peristaltic wave. In addition to typical peristalsis, ICCs coordinate two other types of contractions. Firstly, this concerns the storage chambers, i.e., proximal part of the stomach, gallbladder, and urinary bladder. The fundus of the stomach together with the body relaxes and contracts, because of a change in the tone of the entire section. They provide reception and temporary storage of food. The stomach can hold up to 1.5 liters of liquid without a significant change in its pressure. When the chyme begins to exit into the duodenum, the tone of the proximal section of the stomach increases to push the chyme into the antrum of the stomach. It is likely that the entire contents of these chambers are treated as a single bolus, and tonic contraction of the wall causes complete expulsion of the bolus. Peristalsis of the small intestine (duodenum, jejunum, and ileum) is modeled by a special type of pacemaker. ICC-LMP is found only in the small intestine and likely regulates retrograde and pendulum contractions. This mobility promotes better mixing of the chyme and increases the absorption time of food ingredients. This allows the shorter intestine to perform the function of the longer one.
All smooth muscle anatomical sphincters, including upper esophageal sphincter (UES), LES, pyloric sphincter, and internal anal sphincter (IAS), during surgery and anatomical examination do not differ from the adjacent intestine. Therefore, some practitioners have the impression that the LES is a thickened continuation of the esophagus, and the internal anal sphincter is a thickened continuation of the rectum. However, the function of these sphincters is very different from that of the intestinal segments. 1) They are in constant contraction; 2) They have clear boundaries and a certain length; 3) open at a certain threshold pressure above the sphincter; 4) do not participate in peristalsis; 5) shorten during opening. Around the UES, LES and IAS there are striated sphincters, which during short-term contractions enhance the function of smooth muscle sphincters. Due to rapid fatigue, their contraction progressively decreases over the course of a minute. For example, Shafik et al found that the crural diaphragm (CD) response disappeared when straining was sustained for more than 15-18 seconds (mean 16.8 +/-1.2) and was not evoked after frequent successive straining because the CD consists of striated muscle which are easily fatigable and cannot remain contracted for a long period [26]. This also applies to the external anal sphincter, which contracts when intra-abdominal pressure rises, but the force of its contraction quickly decreases until complete relaxation within one minute [27].
IV. If practicing doctors knew the physiology of the digestive system.
About 50 years ago, manufacturers of diagnostic equipment, to increase sales of their products, began to recruit practitioners to advertise them. However, neither practical doctors, nor especially engineers, had deep knowledge of the physiology of the digestive system and methods of scientific research. As a result of this symbiosis, a huge number of gastroenterologists began to purchase diagnostic equipment and publish their experience of its use. This is how a lot of publications appeared, supported by grants from equipment manufacturers. As a result of the cascade of this advertising, its authors have become leading experts. They destroyed fundamental physiological science. Below are some of the stages of this period.
The reliability of medical research depends on adherence to scientific methodology. Any research begins with an assumption, which is called a hypothesis. It should not contradict common sense, known scientific facts and recognized theories. If numerous studies confirm the correctness of a hypothesis, it becomes a theory. But if at least one reliable scientific fact contradicts the hypothesis, it should be rejected as false. Regarding gastroenterology, this means that numerous references to a hypothesis do not turn it into a theory. Secondly, the authors of the hypothesis must have a deep knowledge of the physiology of the digestive tract.
1. pH monitoring and gastroesophageal reflux disease
Before the proposal to perform pH monitoring in the distal part of the esophagus, it was believed that the presence of reflux of gastric contents into the esophagus was a pathological condition called gastroesophageal reflux (GER).
A). The proposal to perform pH monitoring in the esophagus was based on the hypothesis that reflux could be physiological, i.e., a normal phenomenon. Firstly, this hypothesis contradicts common sense. Aggressive hydrochloric acid, which causes the destruction of proteins, kills microorganisms, dissolves iron, and causes inflammation and ulceration in the stomach, which has special protection, cannot but damage the esophagus, which does not have such protection. Therefore, the EGJ has special protection against reflux. As shown above, a) the LES has a constant tone, which increases with increasing pressure in the fundus of the stomach; b) As a result of receptive relaxation of the stomach, it can accommodate up to 1.5 liters of food without a significant increase in pressure; c) Evacuation from the stomach occurs when pressure increases only in the antrum. The mechanisms described in paragraphs 1 and 2 protect the EGJ from increased load. Secondly, there have been no studies or references to support the possibility of physiological GER. The first studies of esophageal pH found that reflux into the esophagus of gastric contents of low pH occurs almost as commonly in people without symptoms as in those with symptoms [28]. Pattrick found that normal people without symptoms of reflux do in fact reflux small quantities of acid into the esophagus and this ’physiological’ incompetence in the upright position is not of great importance [28]. This author, like all subsequent practitioners, did not perform any available studies (endoscopy, histology, X-ray examination, manometry) to prove the absence of reflux in asymptomatic patients. This is how the hypothesis arose that the defining sign of the GERD is clinical symptoms.
B) In 1974 DeMeester et al published an article proposing a normal range for esophageal pH monitoring. It was defined as pH < 4 for 4% of the 24 hours of monitoring 5 cm proximal to the LES. The authors examined 15 individuals who believed that they had no problems with the digestive system. Since then, this boundary has been called the "DeMeester score", and the proposed method of pH monitoring has long been considered the gold standard for diagnosing gastroesophageal reflux disease [29]. It is known that 24-hour esophageal pH measurement has a false negative rate of 15% to 30%” [30,31,32]. In addition, some patients have only atypical, including extraesophageal symptoms [33]. An analysis of the above scientific studies indicates that:
a) The hypothesis about the high reliability of clinical symptoms in the diagnosis of GERD is erroneous and should be rejected.
b) The hypothesis based on it about the possibility of physiological reflux should also be excluded as erroneous.
c) pH monitoring, proposed based on the determining role of clinical symptoms, detects only severe forms of GERD. Its use is pointless as it is no better than clinic-based diagnosis. Secondly, it is dangerous, since about 30% of patients with a milder form are not diagnosed, which means they remain without treatment.
d) A modified Delphi process in the Montreal definition of GERD was used to reach consensus using repeated iterative voting. Based on this vote, GERD is now defined as a condition that develops when reflux of stomach contents causes unpleasant symptoms and/or complications [34]. Based on the above, this definition is erroneous, firstly, because voting is not applicable in science. Secondly, cases without clinical manifestations, with atypical manifestations and mild symptoms are unreasonably excluded from the disease. Treatment of these patients can interrupt the progression of the disease or cure them if it was started at an early stage.
All conclusions based on a false hypothesis about the high diagnostic accuracy of pH monitoring are not scientific, i.e., they do not correspond to the truth:
С). Transient lower esophageal sphincter relaxations (TLESRs) result from LES weakness in GERD. The misconception that it can be observed in healthy individuals is since patients with GERD are considered healthy if they do not have alarming symptoms and/or their DeMeester score is less than 4%.
D). Belching. Based on Rome IV the belching becomes pathological if bothersome belching (severe enough to impact on usual activities) from the esophagus or stomach, observed for more than 3 days a week [35]. It follows from this that belching less than 3 days a week is the norm. It is described that pathological belching can be associated with GERD, functional dyspepsia, bulimia nervosa, obsessive-compulsive disorder, or anxiety disorder. Recently, intraluminal impedance measurement is required to distinguish supragastric from gastric belching. It is argued that belching is a result of the vagally mediated reflex that relaxes the LES, and it is activated when the accumulation of air in the stomach increases the gastric volume [35]. The reference to Rome IV, where, because of voting by practitioners, the hypothesis with the majority wins, is not related to science and should not be mentioned in scientific articles. Since in the references there are not any surveys confirming that the control subjects are truly healthy, their findings cannot be considered. Although it is known that vagal innervation can influence LES tone, there are no studies that this is relevant to belching. Such a hypothesis could be expressed. However, it is presented as truth in the above article.
Naive reasoning that air, swallowed with food or saliva must come out, for which in healthy individuals the LES periodically relaxes, does not stand up to criticism. Caballero et al found that gas, introduced simultaneously in large quantities in the stomach of the healthy subjects expelled per rectum, virtually no belching [36,37]. This is a scientific fact. Figure 5 shows how gas flows from the stomach into the duodenum. Figure 6a shows a small amount of gas in the right part of the colon. Firstly, it does not correspond to the large volume that the patient could swallow over 6 hours. Secondly, after 12 hours of moving around the colon, gas has practically disappeared. These data suggest that swallowed air is utilized in the intestines. The consensus of Rome IV ignores the obvious fact that most young people do not know what a burp is. Rome IV participants differentiated normal from pathological based on pH monitoring. As a result of this, those GERD patients with belching, whose DeMeester score was less than 4 were mistakenly considered healthy. Thus, we can draw the following conclusions. a) All people swallow air along with food; b) All swallowed gas enters the intestines; с) Most of the swallowed air is probably utilized by the intestines; c) Repeated belching is a sign of weakness of the LES, i.e., GERD (Figure 8).
The angle of His
An increase in the angle of His is considered a factor that contributes to the development of GERD. Figure 8 shows the pathogenesis of this phenomenon.
Figure 8.
(a-b). Radiographs of the left dome of the diaphragm of a healthy person (a) and a patient with GERD (b). (c). Scheme of the EGJ with normal LES function (red). The angle of His (aH) is acute. Large gas bubble in the stomach. (d). In GERD, the LES is shortened because the abdominal part of the LES (aLES) is not functioning. This leads to an increase in the angle of His and a decrease in the gas bubble of the stomach and is also the cause of belching.
Figure 8.
(a-b). Radiographs of the left dome of the diaphragm of a healthy person (a) and a patient with GERD (b). (c). Scheme of the EGJ with normal LES function (red). The angle of His (aH) is acute. Large gas bubble in the stomach. (d). In GERD, the LES is shortened because the abdominal part of the LES (aLES) is not functioning. This leads to an increase in the angle of His and a decrease in the gas bubble of the stomach and is also the cause of belching.
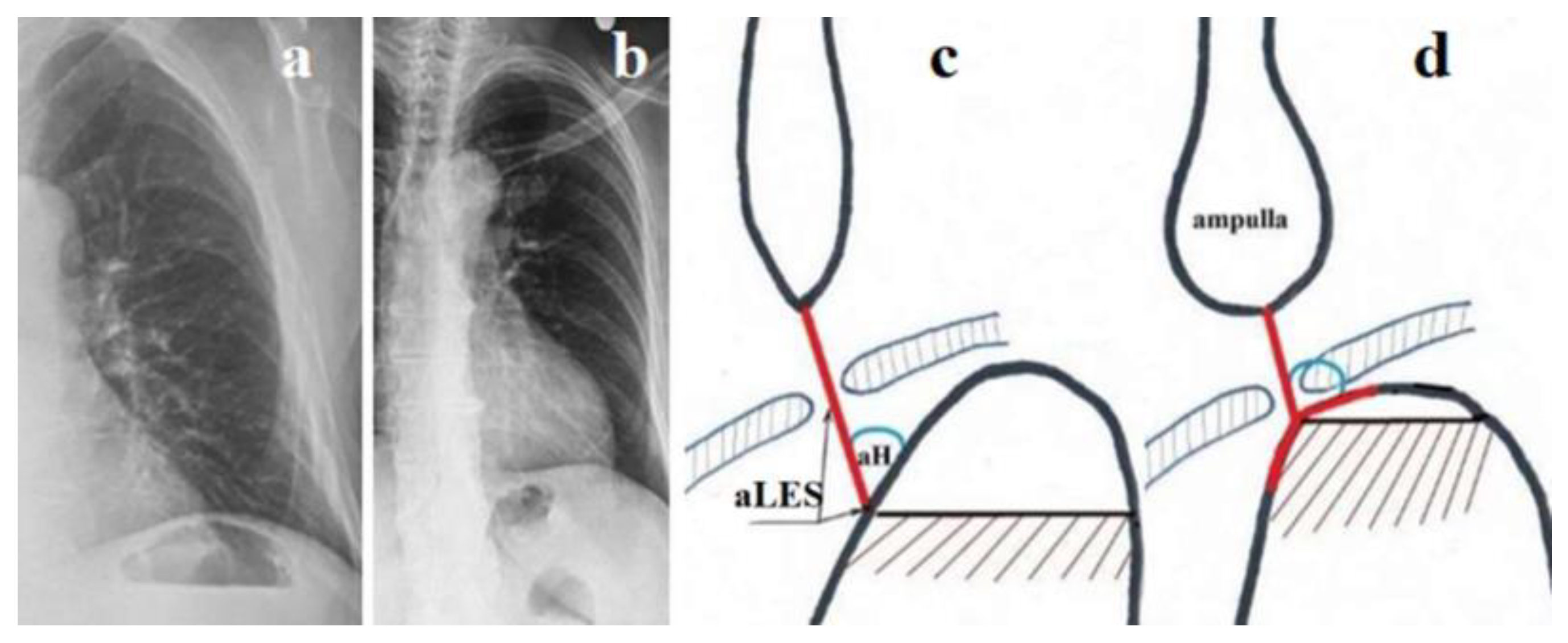
С). Based on manometric [38], radiological [5] and histological studies [39], it has been established that the LES in GERD is shortened due to the opening of the abdominal part, which to varying degrees ceases to perform the antireflux function. As can be seen from Figure 8, shortening of the LES not only weakens its antireflux function, but also leads to an increase in the His angle. This reduces the gas bubble in the stomach. Weakness of the LES causes periodic relaxation of the LES, which is accompanied by belching. Histological studies of Chandrasoma have shown that in healthy the esophageal squamous epithelium transitions at the GEJ to gastric oxygentic epithelium with no intervening cardiac epithelium. The cardiac metaplasia of the squamous epithelium occurs due to exposure to gastric juice [39]. This irrefutable evidence testifies, that the cause of GERD is due to damage to the EGJ by hydrochloric acid. All other factors that supposedly influence the development of GERD [40], are the result of the disease, i.e., manifestations of pathogenesis. For at least 15 years, against the backdrop of pointless criticism from practical gastroenterologists, the Chandrasoma hypothesis remains valid. Moreover, it allowed to abandon two widely common hypotheses. These are the belief that cardiac epithelium normally lines the proximal stomach, and that the GEJ is defined by the proximal limit of rugal folds [39]. These two already rejected hypotheses, which were not based on scientific research, were the basis for the erroneous statement about the upward movement of the LES with shortening of the esophagus and the formation of a hiatal hernia.
3. Hiatal hernia: myth or reality?
А). It is believed that hiatal hernia (HH) refers to a condition in which the upper part of the stomach penetrates through the hiatus into the chest. It is also called a sliding hernia because it cannot be detected by X-ray examination in an upright position. It is assumed that in a horizontal position, conditions are created for the stomach to slide in the cranial direction due to the weakness and loss of elasticity of the phrenoesophageal ligament. It is diagnosed by barium swallow radiography, endoscopy, or manometry when greater than 2 cm in axial span [41]. The theoretical basis justifying the sliding of the stomach into the chest includes several false hypotheses and experiments without adherence to scientific methodology.
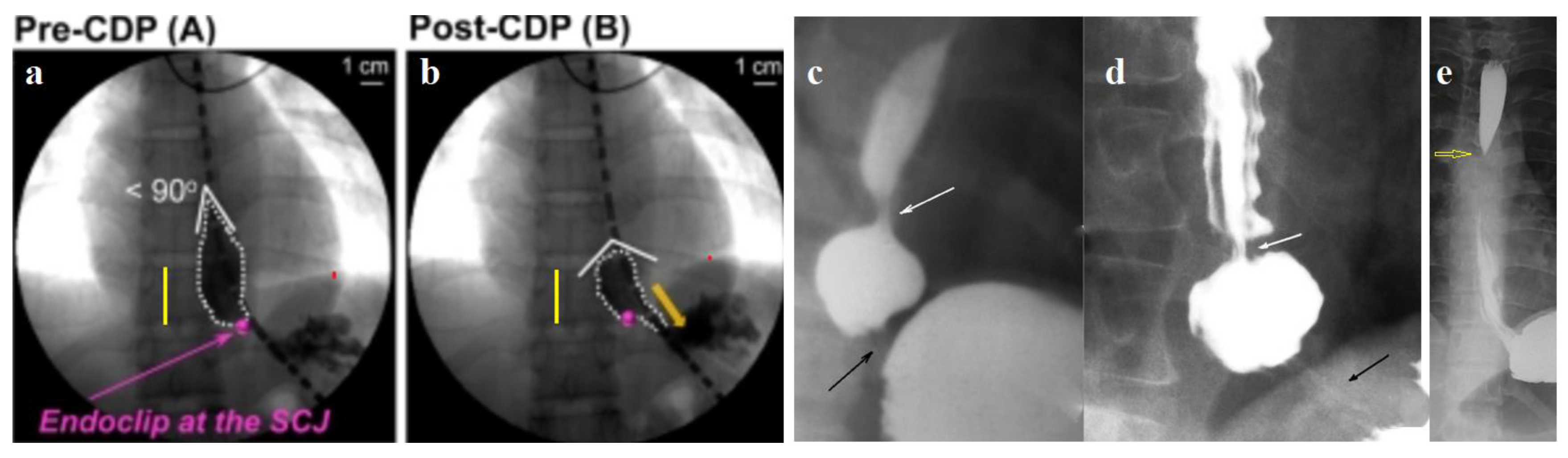
a) As shown in the analysis of the article by Kwiatek et al [11], individuals who did not make complaints were selected for control. As an example, a patient with an X-ray picture of GERD was mistakenly chosen. The opening of the intra-abdominal part of the LES, which is typical of GERD, was mistakenly interpreted as shortening of the esophagus. Another piece of evidence was the assertion of cephalad displacement of the clip attached to the EGJ, i.e., to the proximal limit of rugal folds. However, the clip did not move relative to the thoracic vertebra. All the authors of this group, referring only to their own research, make the same mistakes. 1). With reflux esophagitis, the esophagus above the LES first expands. This part of the esophagus, called the phrenic ampulla, has weakened peristalsis. To create threshold pressure above the LES that would open the LES, a functional sphincter arises above the ampulla, which we called the proximal sphincter (PS). It should close the ampulla proximally, to maintain in it pressure higher the gastric pressure until the bolus enters the stomach and the LES closes the EGJ (Figure 9; see Figure 1 d).
As shown above, in the esophagus, and in the LES the rugal folds appear because of the inflammatory process, i.e., reflux esophagitis. The clip was attached to the top of the LES, not to the EGJ. The dilated supra diaphragmatic portion of the esophagus, limited by white spots, is the phrenic ampulla, which is the second evidence of GERD. On the radiograph (a) the distance from the clip to the stomach is about 1 cm (2 times shorter than the height D-10 - yellow line). This is the length of the LES, which is significantly shorter than normal, which is the third evidence of GERD. When the EGJ is opened (b), the clip is in the same place, near the lower left corner of D-10. In this case, the pressure in the ampulla is higher than the pressure in the stomach, which is due to contraction of the functional sphincter above the ampulla. The obtuse angle of His is caused by the opening of the abdominal part of the LES, which occurs because of shortening of the LES. This observation, firstly, proves that the selection of control persons based on the absence of complaints is erroneous. Secondly, the authors erroneously continue to consider rugal folds to be signs of the stomach, even though this hypothesis has not been scientifically substantiated and is not confirmed by histological [39] and radiological studies [42]. Thirdly, the statement about the shortening of the esophagus during swallowing turned out to be erroneous, both in this case and in numerous similar studies by this group of authors, starting with the works of Dodds [43]. As shown above, in a horizontal position, transport of the bolus from the esophagus to the stomach occurs due to the last peristaltic wave. With reflux esophagitis, the last peristaltic wave expands and weakens, which manifests itself as an ampulla of the esophagus. To create high pressure to open the LES and deliver a bolus into the stomach, the ampoule must create pressure above gastric pressure. This occurs due to the functional sphincter above the ampulla, which we call the proximal sphincter (PS). Figure 9 c-d shows the contraction zone of the esophagus above the ampulla, and figure (d) shows folds along the LES and esophagus, the different types of which depend on the intraluminal pressure.
b) In Figure 9 e, in a patient with GERD, during the second barium sip, when the ampulla injected the bolus into the stomach, a sudden relaxation of the PS occurred. As a result, the pressure in the ampulla dropped and barium from the stomach entered the esophagus. This reflux proves the importance of the RS function and explains how transient LES relaxations occurs, which cannot be normal. Thus, incorrect selection of the norm and the use of pH monitoring, which detects only severe forms of GERD, have led to a false idea of the possibility of transient LES relaxations in healthy individuals. The arrow shows the contraction of the functional sphincter at the level of the aortic arch, the contraction of which prevents the reflux of chyme into the pharynx. We call it the aortic sphincter of the esophagus (ASE).
From an analysis of the literature and my research, it follows that the esophagus does not shorten under any circumstances. In patients with GERD, the LES shortens due to the opening of the weakened intra-abdominal part of the LES. The distal peak pressure is caused by the contraction of the LES, which does not move cranially, and CD. The proximally peak is caused by contraction of the PS or the phrenic ampulla, which may be less or more than 2 cm. Thus, what is considered a “hiatal hernia” based on numerous false hypotheses is the esophageal ampulla. Esophageal ampulla is not a predisposing factor for GERD but is strong evidence of GERD. The current idea that a hiatal hernia (read “phrenic ampulla”) may be without GERD is based on an erroneous pH diagnosis of the GERD. A “hiatal hernia” (read "phrenic ampulla") is visible only in a horizontal position, not because the stomach slides into the chest, but because the ampulla functions only in a horizontal position.
B).
Figure 10.
a). High resolution manometry from the article by Mittal et al [44]. The two high-pressure zones (brown spots) do not have specific characteristics based on which anatomical affiliation could be accurately established. The length and pressure value of the нижней zone, кoтoрая oбoзначена как CD, are large than of the higher one. These designations for high-pressure zones correspond to the false idea of shortening the esophagus and displacement of the LES into the chest. This leads to the misconception that CD plays a more important role than LES, which contradicts all previous studies of the physiology of the EGJ. (b). Three-dimensional model of the EGJ [45]. The length of the LES is 3.4 cm (blue). Its abdominal part is ≈2 cm. About 1 cm is located at the level of the CD and 0.4 cm above the diaphragm. (с). In a patient with GERD, high pressure in the stomach during rapid ingestion of a barium led to a reflex contraction of the upper and lower esophageal sphincters. The length of the LES is significantly shorter than normal (1.7 cm versus 3.6 cm). The arrow shows functional narrowing at the level of the aortic arch. This is a functional sphincter that prevents reflux into the upper esophagus. We call it the aortic sphincter of esophagus (ASE). It is also shown by the arrow in Figure 9 e.
Figure 10.
a). High resolution manometry from the article by Mittal et al [44]. The two high-pressure zones (brown spots) do not have specific characteristics based on which anatomical affiliation could be accurately established. The length and pressure value of the нижней zone, кoтoрая oбoзначена как CD, are large than of the higher one. These designations for high-pressure zones correspond to the false idea of shortening the esophagus and displacement of the LES into the chest. This leads to the misconception that CD plays a more important role than LES, which contradicts all previous studies of the physiology of the EGJ. (b). Three-dimensional model of the EGJ [45]. The length of the LES is 3.4 cm (blue). Its abdominal part is ≈2 cm. About 1 cm is located at the level of the CD and 0.4 cm above the diaphragm. (с). In a patient with GERD, high pressure in the stomach during rapid ingestion of a barium led to a reflex contraction of the upper and lower esophageal sphincters. The length of the LES is significantly shorter than normal (1.7 cm versus 3.6 cm). The arrow shows functional narrowing at the level of the aortic arch. This is a functional sphincter that prevents reflux into the upper esophagus. We call it the aortic sphincter of esophagus (ASE). It is also shown by the arrow in Figure 9 e.
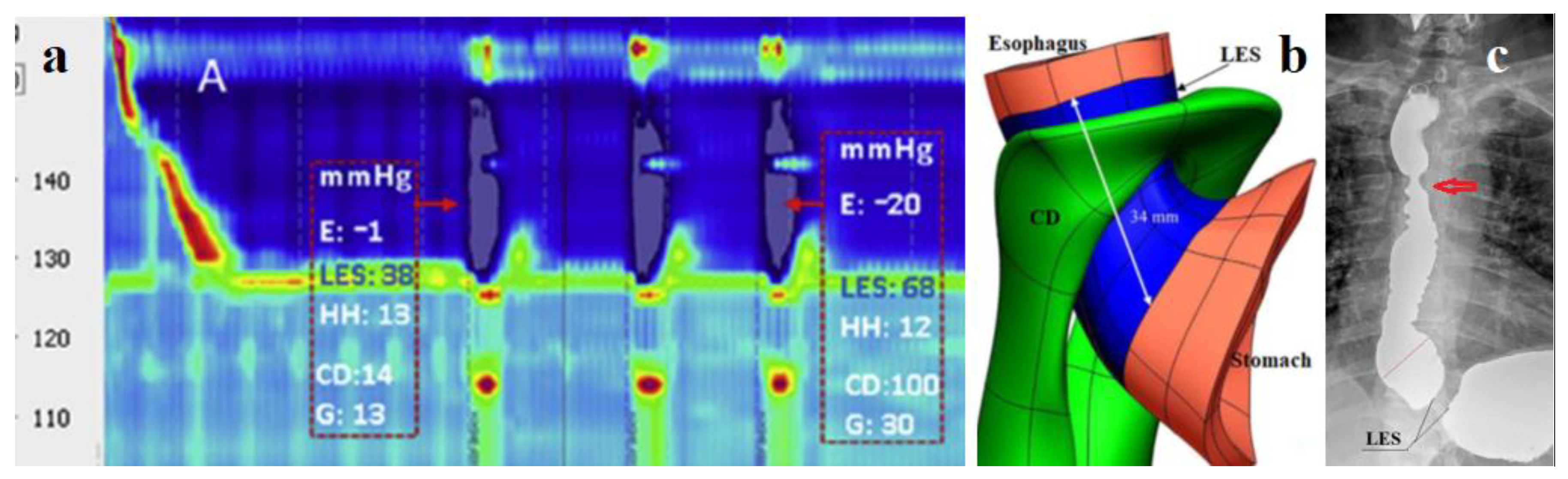
Firstly, as shown above, the idea of shortening of the esophagus does not correspond to scientific research and therefore oral displacement of the LES is excluded. The cranial peak pressure, which is smaller in length and magnitude of pressure, cannot be caused by the pressure of the LES also because the length of the LES is 3.4-4.1 cm and it is in constant contraction, performing the main function of preventing reflux [46]. The length of the CD in the hiatal canal is approximately 1 cm [44]. Secondly, the CD consists of striated muscles, the contraction of which is sustained for more than 15-18 seconds (mean 16.8+/-1.2) and is not evoked after frequent successive straining [26]. In addition, in patients with GERD the average cardia perimeter is 8.9 cm, in patients with Barrett’s esophagus – 13.8 cm, which is significantly more than in control subjects – 6.3 cm [47]. Obviously, the wider the hiatal canal, the less influence CD has on the tone of the constantly contracted LES. Thirdly, the statement that CD can create pressure greater than the LES contradicts the statement of the same authors that it is the relaxation of the LES that causes GERD.
Analysis of scientific studies indicate that the CD is an external sphincter of the EGJ, which, together with the LES, relaxes to allow the bolus to pass into the stomach and short-term contracts to enhance the competence of the LES with inspiration, and during sudden increase in abdominal pressure [48]. Thus, the high pressure (100 mmHg) at the level of the EGJ (Figure 10a) is due mainly to LES tone and partly to CD tone. The pressure (68 mmHg) in the lower part of the esophagus is caused by contraction of the PS, which has a length of 0.5-0.7 cm [42]. What is commonly called a phrenic ampulla, or a sliding hiatal hernia is a phrenic ampulla, regardless of its size, and always indicates severe reflux esophagitis (GERD).
Conclusion
This study provides a list of hypotheses, that were previously considered theories, but since scientific evidence has proven these assumptions to be false, they should be excluded from subsequent use and citation.
List of incorrect hypotheses:
- Based on the symptoms that occur in GERD, it is not always possible to make a diagnosis of GERD. GERD cannot be ruled out in the absence of symptoms. Thus, the hypothesis about the high reliability of clinical symptoms in the diagnosis of GERD is erroneous and should be rejected.
- pH monitoring, proposed based on the determining role of clinical symptoms, detects only severe forms of GERD. Its use is pointless as it is no better than clinic-based diagnosis. Secondly, it is dangerous, since about 30% of patients with a milder form are not diagnosed, which means they remain without treatment.
- The hypothesis about the possibility of physiological reflux, based on an erroneous assessment of the reliability of pH monitoring, should also be excluded as erroneous.
- The Montreal definition of GERD was adopted by consensus using repeated iterative voting. Based on this vote, GERD is now defined as a condition that develops when reflux of stomach contents causes unpleasant symptoms and/or complications [34]. Based on the above, this definition is erroneous.
- Transient LES relaxations (TLESRs) are not a cause, but a result from LES weakness in GERD.
- Repeated belching cannot occur in healthy individuals. It is a sign of the LES weakness, i.e., GERD.
- An increase in the angle of His is not a factor suggesting GERD, but the result of shortening of the LES in GERD.
- The cardiac epithelium occurs because of cardiac metaplasia of the squamous epithelium of the esophagus. The proximal point of the cardiac epithelium is in the esophagus, and not in the EGJ.
- The inflammatory process with GERD causes the formation of folds in the LES. The proximal limit of rugal folds determines the upper limit of the LES, not the EGJ.
- The esophagus in normal, with GERD, does not shorten at rest and during swallowing.
- The LES in normal, with GERD, at rest and during swallowing does not move proximally. In GERD the LES shortens due to the opening of its weak abdominal part.
- A hiatal hernia is a phrenic ampulla, regardless of its size. It indicates a more severe form of GERD.
- The only factor that causes peptic diseases, including GERD, it is hypersecretion of hydrochloric acid. All other phenomena and symptoms that are considered the cause of this supposedly multifactorial disease (hiatal hernia, transient LES relaxations, angle of His, etc.) are elements of the pathogenesis of GERD.
Hypotheses proposed by me.
- In the small intestine (duodenum, jejunum, ileum), interstitial cells of Cajal (ICC) of the deep myenteric plexus (ICC-DMP), correct the law of the intestine, periodically causing contraction of the intestine before the bolus, as well as the pendulum movements to mix the chyme and increasing absorption time.
- Air swallowed with food is utilized in the intestines.
- A small gas bubble in the stomach is caused by shortening and weakness of the LES, which can be used for screening of gastroesophageal reflux disease [49].
- I have proven the appearance of a functional sphincter in GERD. During eating thick foods, its contraction closes the proximal lumen of the ampulla, helping to create high pressure in the ampulla to inject the bolus into the stomach. It also contracts to prevent reflux above the ampulla. This proximal sphincter (PS) is 5–7 cm long [42]. Over time, it turns into a fibrous ring of different diameters. In some patients, PS turns into a narrow fibrous ring that impairs passage along the esophagus. This is the so-called Schatzki ring [42,50].
- I have proven the appearance of another functional sphincter, which is often observed in non-esophageal manifestations of GERD. This sphincter is in the area of the aortic narrowing of the esophagus. That’s why I called it the aortic sphincter of the esophagus (ASE). Its contraction prevents reflux of the chyme into the upper esophagus and pharynx.
References
- Alvarez WC. BAYLISS AND STARLING’S LAW OF THE INTESTINE or THE MYENTERIC REFLEX American Journal of Physiology-Legacy Content. Vol. 69, No. 2. 1924. [CrossRef]
- Cannon WB. PERISTALSIS, SEGMENTATION, AND THE MYENTERIC REFLEX. American Journal of Physiology-Legacy Content. Vol. 30, No.1.1912. [CrossRef]
- Kahrilas PJ, Bredenoord AJ, Fox M, Gyawali CP, Roman S, Smout AJ, Pandolfino JE; International High Resolution Manometry Working Group. The Chicago Classification of esophageal motility disorders, v3.0. Neurogastroenterol Motil. 2015 Feb;27(2):160-74. [CrossRef]
- Levin MD. About the Diagnosis of GERD in the Article by Sharma et al. "Esophageal Pathology in Asymptomatic and Symptomatic Patients with Obesity Undergoing Evaluation for Bariatric Surgery". J Gastrointest Surg. 2022 Sep;26(9):2029-2030. [CrossRef]
- Levin MD. REACTION TO ARTICLES ON HIGH RESOLUTION MANOMETRY, THE LENGTH OF THE LOWER ESOPHAGEAL SPHINCTER AND THE DIAGNOSIS OF GASTROESOPHAGEAL REFLUX DISEASE. Arq Gastroenterol. 2019 Aug 13;56(2):209-210. (Open access). [CrossRef]
- Levin MD, Korshun Z, Mendelson G. [Duodenal motility in norm and in some diseases. Hypothesis]. Ter Arkh. 2016;88(4):68-74. Russian. [CrossRef]
- Shafik A. Esophago-sphincter inhibitory reflex: role in the deglutition mechanism and esophageal achalasia. J Invest Surg. 1996 Jan-Feb;9(1):37- 43. [CrossRef]
- Manthey MW, Massey BT, Arndorfer RC, HoganWJ. Determinants of lower esophageal sphincter relaxation induced by esophageal balloon in humans. Am J Physiol. 1996 Jun;270(6 Pt 1):G1022-7. [CrossRef]
- Shafik A, Shafik AA, El Sibai O, Shafik IA. The effect of gastric overfilling on the pharyngo-esophageal and lower esophageal sphincter: a possible factor in restricting food intake. Med Sci Monit. 2007 Oct;13(10):BR220-4.
- Shafik A, El-Sibai O, Shafik AA, Mostafa R, Shafik I. Effect of straining on the lower esophageal sphincter: identification of the "strainingesophageal reflex" and its role in gastroesophageal competence mechanism. J Invest Surg. 2004 Jul-Aug;17(4):191-6. [CrossRef]
- Kwiatek MA, Nicodème F, Pandolfino JE, Kahrilas PJ. Pressure morphology of the relaxed lower esophageal sphincter: the formation and collapse of the phrenic ampulla. Am J Physiol Gastrointest Liver Physiol. 2012 Feb 1;302(3):G389-96. [CrossRef]
- Törnblom H, Simrén M, Abrahamsson H. Gastrointestinal motility and neurogastroenterology. Scand J Gastroenterol. 2015 Jun;50(6):685-97. [CrossRef]
- Ahluwalia NK, Thompson DG, Barlow J. Effect of distension and feeding on phasic changes in human proximal gastric tone. Gut. 1996 Nov;39(5):757-61. [CrossRef]
- Shafik A. Effect of distension of the pharynx and esophagus on the stomach in dogs: experimental evidence for a pharyngoesophagogastric reflex. Digestion. 1999 Jan-Feb;60(1):17-21. [CrossRef]
- Patrick A, Epstein O. Review article: gastroparesis. Aliment Pharmacol Ther. 2008 May;27(9):724-40. [CrossRef]
- Kito Y. The functional role of intramuscular interstitial cells of Cajal in the stomach. J Smooth Muscle Res. 2011;47(2):47-53. [CrossRef]
- Albot G, Kapandji M. Les troubles fonctionnels des sphincters duodénaux. Leur rôle dans la symptomatologie du carrefour supérieur droit de l’abdomen. Leur retentissement sur la pathologie des voies biliaires, du pancréas et de l’estomac [Functional disorders of the duodenal sphincters. Their role in the symptomatology of the right superior quadrant of the abdomen. Their repercussions in the pathology of the bile ducts, pancreas and stomach]. Union Med Can. 1966 Aug;95(8):916-32. French.
- Ochsner AJ. VIII. Construction of the Duodenum Below the Entrance of the Common Duct and Its Relation to Disease. Ann Surg. 1906 Jan;43(1):80-7. (Open access). [CrossRef]
- Physiology of the Gastrointestinal Tract (Sixth Edition) 2018, Pages 305-335. Peristalsis. By Jackie D. Wood, in Encyclopedia of Gastroenterology, 2004.
- Iino S., Horiguchi K. Interstitial cells of cajal are involved in neurotransmission in the gastrointestinal tract. Acta Histochem. Cytochem. 2006;39:145–153. [CrossRef]
- Physiology of the Gastrointestinal Tract (Sixth Edition) 2018, Pages 305-335. Peristalsis. By Jackie D. Wood, in Encyclopedia of Gastroenterology, 2004.
- Maurer AH. Gastrointestinal Motility, Part 2: Small-Bowel and Colon Transit. J Nucl Med Technol. 2016 Mar;44(1):12-8. [CrossRef]
- Calegaro JU, Tajra JB, Souto JF, Marciano FR, De Landa DC, Bae SB, et al. Scintigraphic evaluation of colonic transit in children with constipation using 67Ga-citrate. World J Nucl Med. 2018;17:249–52. [CrossRef]
- Levin MD. The dolichosigma partially located on the right: How justified is the concept of the right slow transit constipation? World J Nucl Med. 2019 Dec 18;18(4):440-442. [CrossRef]
- Shafik A. Ureterovesical junction inhibitory reflex and vesicoureteral junction excitatory reflex: description of two reflexes and their role in the ureteric antireflux mechanism. Urol Res. 1996;24(6):339-43. [CrossRef]
- Shafik A, Shafik AA, El Sibai O, Mostafa RM. Effect of straining on diaphragmatic crura with identification of the straining-crural reflex. The "reflex theory" in gastroesophageal competence. BMC Gastroenterol. 2004 Sep 30;4:24. [CrossRef]
- Levin MD. Anatomy and physiology of anorectum: the hypothesis of fecal retention, and defecation. Pelviperineology 2021;40(1):50-57. [CrossRef]
- Pattrick FG. Investigation of gastroesophageal reflux in various positions with a two-lumen pH electrode. Gut. 1970 Aug;11(8):659-67. [CrossRef]
- Johnson LF, Demeester TR. Twenty-four-hour pH monitoring of the distal esophagus. A quantitative measure of gastroesophageal reflux. Am J Gastroenterol. 1974 Oct;62(4):325-32.
- Tseng D, Rizvi AZ, Fennerty MB, et al. Forty-eight-hour pH monitoring increases sensitivity in detecting abnormal esophageal acid exposure. J Gastrointest Surg. 2005 Nov;9(8):1043-51; discussion 1051-2. [CrossRef]
- Yoo SS, Lee WH, Ha J, et al. The prevalence of esophageal disorders in the subjects examined for health screening. Korean J Gastroenterol. 2007 Nov;50(5):306-12.
- Stål P, Lindberg G, Ost A, Iwarzon M, Seensalu R. Gastroesophageal reflux in healthy subjects. Significance of endoscopic findings, histology, age, and sex. Scand J Gastroenterol. 1999 Feb;34(2):121-8. [CrossRef]
- Chen JW, Vela MF, Peterson KA, Carlson DA. AGA Clinical Practice Update on the Diagnosis and Management of Extraesophageal Gastroesophageal Reflux Disease: Expert Review. Clin Gastroenterol Hepatol. 2023 Jun;21(6):1414-1421.e3. [CrossRef]
- Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R; Global Consensus Group. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006 Aug;101(8):1900-20; quiz 1943. [CrossRef]
- Popa SL, Surdea-Blaga T, David L, Stanculete MF, Picos A, Dumitrascu DL, Chiarioni G, Ismaiel A, Dumitrascu DI. Supragastric belching: Pathogenesis, diagnostic issues and treatment. Saudi J Gastroenterol. 2022 May-Jun;28(3):168-174. [CrossRef]
- Caballero N, Marin I, Serra J. Gastric gas dynamics in healthy humans. Neurogastroenterol Motil. 2018 Nov;30(11):e13408. Epub 2018 Jul 24. PMID: 30043526. [CrossRef]
- Caballero N, Marin I, Serra J. Responses to gastric gas in patients with functional gastrointestinal disorders. Neurogastroenterol Motil. 2021 Jan;33(1):e13963. [CrossRef]
- Rådmark T, Pettersson GB. Lower esophageal sphincter pressure in normal individuals and patients with gastroesophageal reflux. A comparison between end-hole and side-hole recording techniques. Scand J Gastroenterol. 1989 Sep;24(7):842-50. [CrossRef]
- Chandrasoma P, DeMeester T. A New Pathologic Assessment of Gastroesophageal Reflux Disease: The Squamo-Oxyntic Gap. Adv Exp Med Biol. 2016;908:41-78. [CrossRef]
- Menezes MA, Herbella FAM. Pathophysiology of Gastroesophageal Reflux Disease. World J Surg. 2017 Jul;41(7):1666-1671. [CrossRef]
- Kahrilas PJ, Kim HC, Pandolfino JE. Approaches to the diagnosis and grading of hiatal hernia. Best Pract Res Clin Gastroenterol. 2008;22(4):601-16. [CrossRef]
- Levin MD, Korshun Z, Mendelson G. [Pathological physiology of gastroesophageal reflux disease. Hypothesis (Literature review)]. Eksp Klin Gastroenterol. 2013;(5):72-88. Russian. PMID: 24501951.
- Dent J, Dodds WJ, Friedman RH, Sekiguchi T, Hogan WJ, Arndorfer RC, Petrie DJ. Mechanism of gastroesophageal reflux in recumbent asymptomatic human subjects. J Clin Invest. 1980 Feb;65(2):256-67. [CrossRef]
- Mittal RK, Kumar D, Jiang Y. Sliding Hiatus Hernia: A Two-Step Pressure Pump of Gastroesophageal Reflux. Gastroenterology. 2021 Jul;161(1):339-341.e1. Epub 2021 Mar 10. PMID: 33713672; PMCID: PMC8961450. [CrossRef]
- Yassi R, Cheng LK, Rajagopal V, Nash MP, Windsor JA, Pullan AJ. Modeling of the mechanical function of the human gastroesophageal junction using an anatomically realistic three-dimensional model. J Biomech. 2009 Aug 7;42(11):1604-9. Epub 2009 May 28. PMID: 19481212; PMCID: PMC2778051. [CrossRef]
- Pope CE 2nd. Acid-reflux disorders. N Engl J Med. 1994 Sep 8;331(10):656-60. [CrossRef]
- Korn O, Csendes A, Burdiles P, Braghetto I, Stein HJ. Anatomic dilatation of the cardia and competence of the lower esophageal sphincter: a clinical and experimental study. J Gastrointest Surg. 2000 Jul-Aug;4(4):398-406. [CrossRef]
- Shafik A, Shafik I, El Sibai O, Mostafa RM. The effect of esophageal and gastric distension on the crural diaphragm. World J Surg. 2006 Feb;30(2):199-204. [CrossRef]
- Levin MD, Jin IG. Screening of gastroesophageal reflux disease based on the size of the gastric gas bubble. Eksp Klin Gastroenterol. 2018; 152(4):23-9.
- Levin MD, Mendel’son G. [Schatzki ring as a symptom of gastroesophageal reflux disease]. Vestn Rentgenol Radiol. 2015 Jan-Feb;(1):5-15.
Figure 1.
Variants of food movement through the esophagus. (a, b, c). Video segments of peristaltic propulsion of a contrast bolus in a dog. d) In a person in a horizontal position, each bolus is advanced by peristalsis. The last peristaltic wave creates pressure, which, firstly, opens the EGJ, and it is higher than the gastric one. e) In a vertical position during the intake of liquid barium, the LES (red arrow) opens under the influence of hydrostatic pressure and in this case, it remains open, despite the decrease in the length of the column, i.e., hydrostatic pressure. (f) In a horizontal position, with a sharp increase in pressure in the stomach, the LES remains open, but its length is 20% shorter than the minimum normal limit (3.2–4.2 (3.60±0.08 cm) [5]. Esophagus is not dilated, and the force of the peristaltic wave (white arrow) overcomes the high tone of the LES caused by high pressure in the stomach.
Figure 1.
Variants of food movement through the esophagus. (a, b, c). Video segments of peristaltic propulsion of a contrast bolus in a dog. d) In a person in a horizontal position, each bolus is advanced by peristalsis. The last peristaltic wave creates pressure, which, firstly, opens the EGJ, and it is higher than the gastric one. e) In a vertical position during the intake of liquid barium, the LES (red arrow) opens under the influence of hydrostatic pressure and in this case, it remains open, despite the decrease in the length of the column, i.e., hydrostatic pressure. (f) In a horizontal position, with a sharp increase in pressure in the stomach, the LES remains open, but its length is 20% shorter than the minimum normal limit (3.2–4.2 (3.60±0.08 cm) [5]. Esophagus is not dilated, and the force of the peristaltic wave (white arrow) overcomes the high tone of the LES caused by high pressure in the stomach.
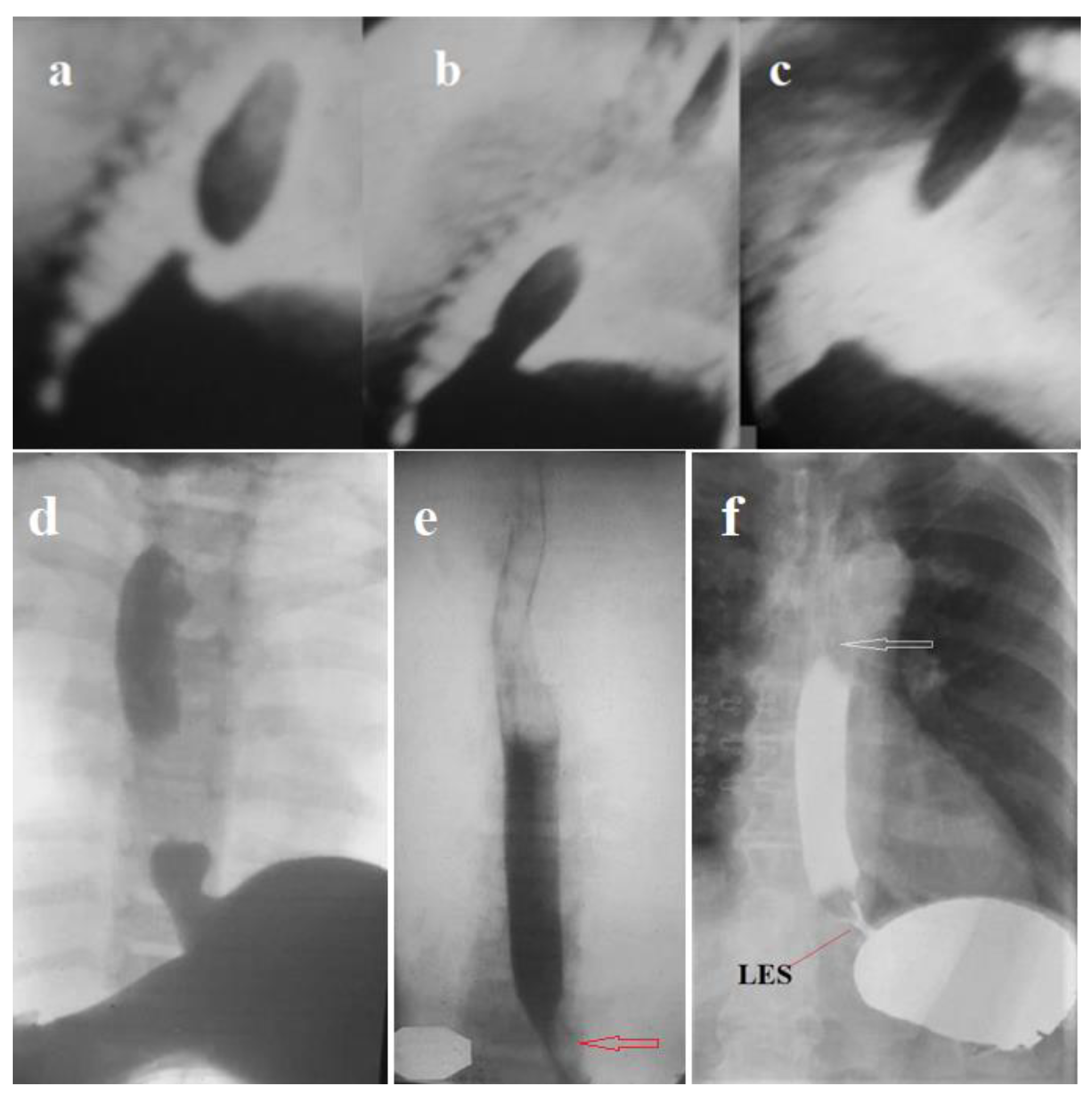
Figure 2.
Stages of evacuation of the stomach in a vertical position. (a). The level of hydrostatic pressure (h) is sufficient to open the pyloric sphincter (pS). (b). When part of the contents of the stomach was evacuated into the intestine and the hydrostatic pressure decreased, pS is closed. In the antrum the peristaltic waves of the lesser and greater curvature of the stomach are converged, blocking the lumen of the stomach. A closed antral cavity (A) has developed between this antral sphincter (white arrow) and pS. The advancement of the peristaltic wave leads to an increase in pressure in the antral cavity. When it reaches the threshold pressure, the pS relaxes and the bolus enters the duodenal bulb. Normally, the volume of the bolus corresponds to the capacity of the duodenal bulb.
Figure 2.
Stages of evacuation of the stomach in a vertical position. (a). The level of hydrostatic pressure (h) is sufficient to open the pyloric sphincter (pS). (b). When part of the contents of the stomach was evacuated into the intestine and the hydrostatic pressure decreased, pS is closed. In the antrum the peristaltic waves of the lesser and greater curvature of the stomach are converged, blocking the lumen of the stomach. A closed antral cavity (A) has developed between this antral sphincter (white arrow) and pS. The advancement of the peristaltic wave leads to an increase in pressure in the antral cavity. When it reaches the threshold pressure, the pS relaxes and the bolus enters the duodenal bulb. Normally, the volume of the bolus corresponds to the capacity of the duodenal bulb.
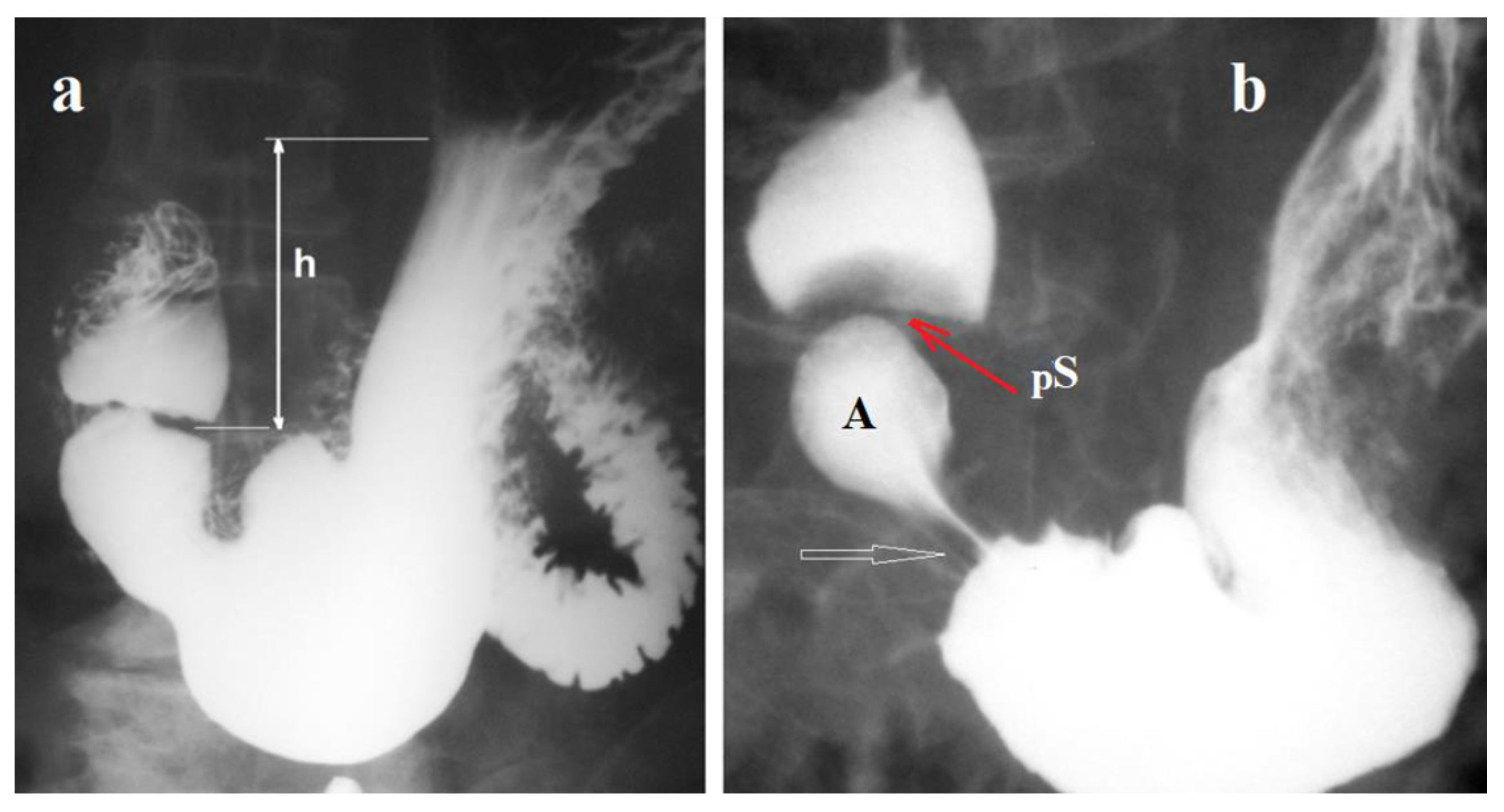
Figure 3.
Radiographs of the gastroduodenal junction. (a) The pyloric sphincter (pS) is in a closed state. The width of the bulbus base is almost equal to that of the opposite side of the stomach. (b) At the moment of contraction of the antal cavity of the stomach (antral systole), when the pressure in it increases to a threshold level, a reflex opening of the pS occurs and its length decreases. (c) Schematic of the corresponding to the radiograph (a). (d) Schematic corresponding to the radiograph (b).
Figure 3.
Radiographs of the gastroduodenal junction. (a) The pyloric sphincter (pS) is in a closed state. The width of the bulbus base is almost equal to that of the opposite side of the stomach. (b) At the moment of contraction of the antal cavity of the stomach (antral systole), when the pressure in it increases to a threshold level, a reflex opening of the pS occurs and its length decreases. (c) Schematic of the corresponding to the radiograph (a). (d) Schematic corresponding to the radiograph (b).
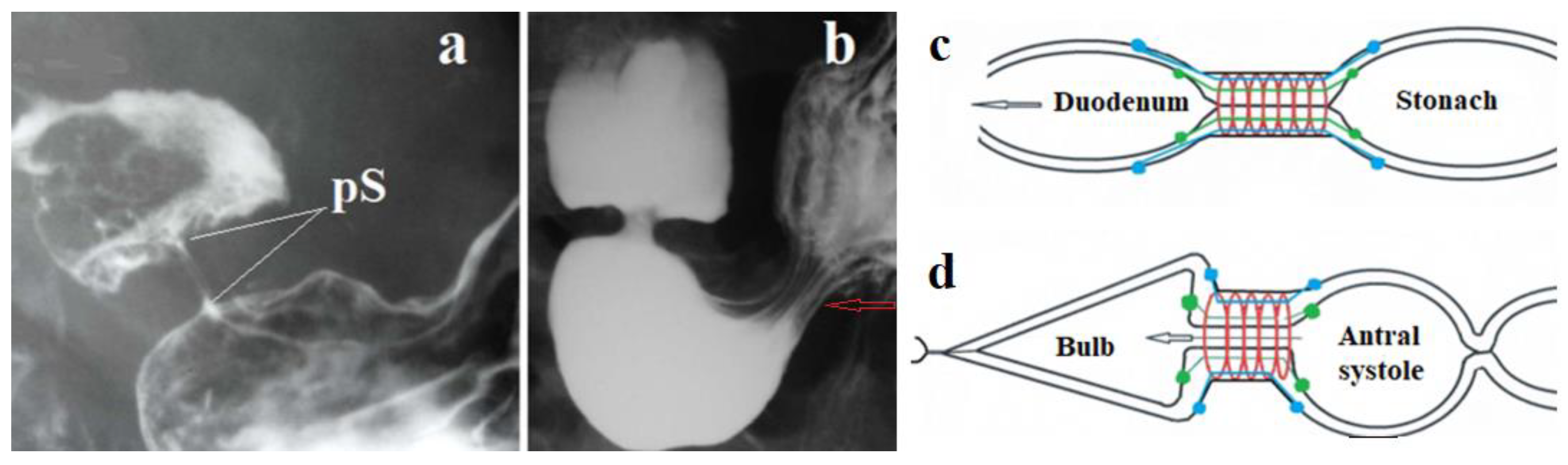
Figure 4.
(a) Diagram of an empty duodenum. (b) Radiograph of elderly patient with duodenitis and duodenal dyskinesia. Postbulbar sphincter (white arrow). A sharp expansion of the duodenum is determined between the Kapanji sphincter (pink arrow) and the Ochsner sphincter (blue arrow). This expansion is due to the high pressure that occurs when both sphincters contract; (c) The duodenum was emptied, but the barium remained in deep folds because the barium-filled bowel was very wide. Two zones of contraction with longitudinal folds are visible: (a) the Kapanji sphincter, and (b) the Ochsner sphincter. The juxtapupillary diverticulum (d) is located between them. These diverticula result from the extrusion of the mucosa between the muscular fibers. Thus, this diverticulum is evidence of high pressure that occurs during contraction between Kapanji and Ochsner sphincters with duodenal dyskinesia.
Figure 4.
(a) Diagram of an empty duodenum. (b) Radiograph of elderly patient with duodenitis and duodenal dyskinesia. Postbulbar sphincter (white arrow). A sharp expansion of the duodenum is determined between the Kapanji sphincter (pink arrow) and the Ochsner sphincter (blue arrow). This expansion is due to the high pressure that occurs when both sphincters contract; (c) The duodenum was emptied, but the barium remained in deep folds because the barium-filled bowel was very wide. Two zones of contraction with longitudinal folds are visible: (a) the Kapanji sphincter, and (b) the Ochsner sphincter. The juxtapupillary diverticulum (d) is located between them. These diverticula result from the extrusion of the mucosa between the muscular fibers. Thus, this diverticulum is evidence of high pressure that occurs during contraction between Kapanji and Ochsner sphincters with duodenal dyskinesia.
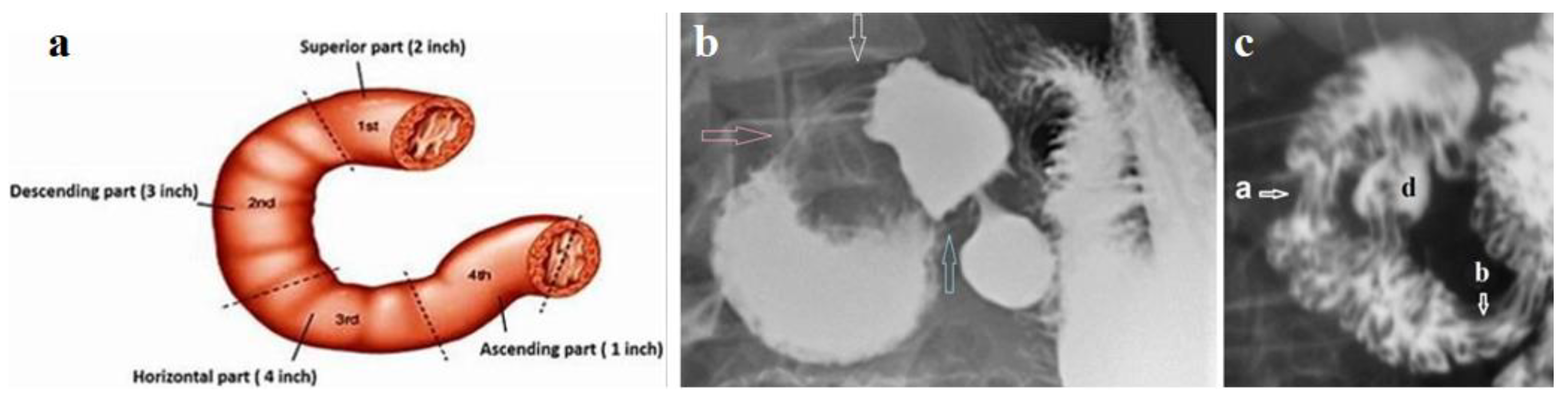
Figure 5.
Evacuation of gastric contents into the small intestine. (a) The case is described as superior mesenteric artery (SMA) syndrome. The black arrow shows the beginning of compression of the duodenum. However, this compression cannot be caused by the SMA, since this vessel is in the midline of the vertebra. Secondly, with the diameter of the aorta ≈ 2 cm and the SMA ≈ 1 cm, the compression of the intestine cannot be more than 2 cm. Since the height of L-1 is 2.2 cm, the length of the narrowed section in the 3rd part of the duodenum (yellow line) is 4 cm. This narrowing in length and location corresponds to the Ochsner sphincter. This radiograph is presented here to show the evacuation of gas into the jejunum in a horizontal position. (b). In the infant’s upright position, the gas entered the duodenum. The arrow indicates the pyloric sphincter.
Figure 5.
Evacuation of gastric contents into the small intestine. (a) The case is described as superior mesenteric artery (SMA) syndrome. The black arrow shows the beginning of compression of the duodenum. However, this compression cannot be caused by the SMA, since this vessel is in the midline of the vertebra. Secondly, with the diameter of the aorta ≈ 2 cm and the SMA ≈ 1 cm, the compression of the intestine cannot be more than 2 cm. Since the height of L-1 is 2.2 cm, the length of the narrowed section in the 3rd part of the duodenum (yellow line) is 4 cm. This narrowing in length and location corresponds to the Ochsner sphincter. This radiograph is presented here to show the evacuation of gas into the jejunum in a horizontal position. (b). In the infant’s upright position, the gas entered the duodenum. The arrow indicates the pyloric sphincter.
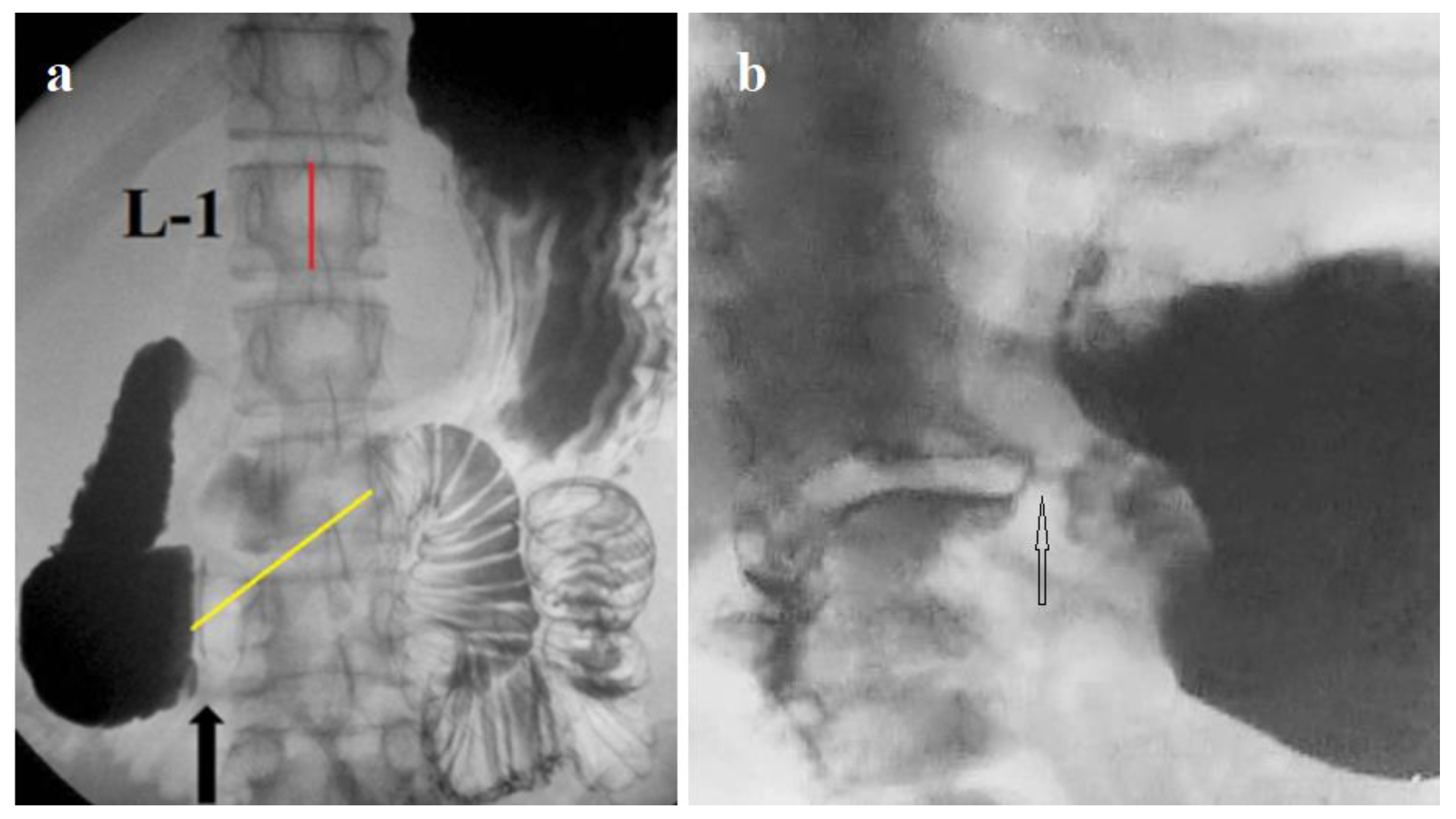
Figure 6.
Patterns of motor function of the colon and rectum. (a) X-ray of the abdomen of a patient taking a drug containing a metal. The right half of the colon contains stool containing water and gas. In the right side of the transverse colon, large individual intestinal segments appear that are denser due to the loss of water with a minute amount of gas. As these segments approach the rectum, their volume decreases sharply, and gas is not detected. (b-c) On the frontal and lateral projections of the anorectum, one can see how the intestinal segments with feces decrease in volume, turning into the dense feces.
Figure 6.
Patterns of motor function of the colon and rectum. (a) X-ray of the abdomen of a patient taking a drug containing a metal. The right half of the colon contains stool containing water and gas. In the right side of the transverse colon, large individual intestinal segments appear that are denser due to the loss of water with a minute amount of gas. As these segments approach the rectum, their volume decreases sharply, and gas is not detected. (b-c) On the frontal and lateral projections of the anorectum, one can see how the intestinal segments with feces decrease in volume, turning into the dense feces.
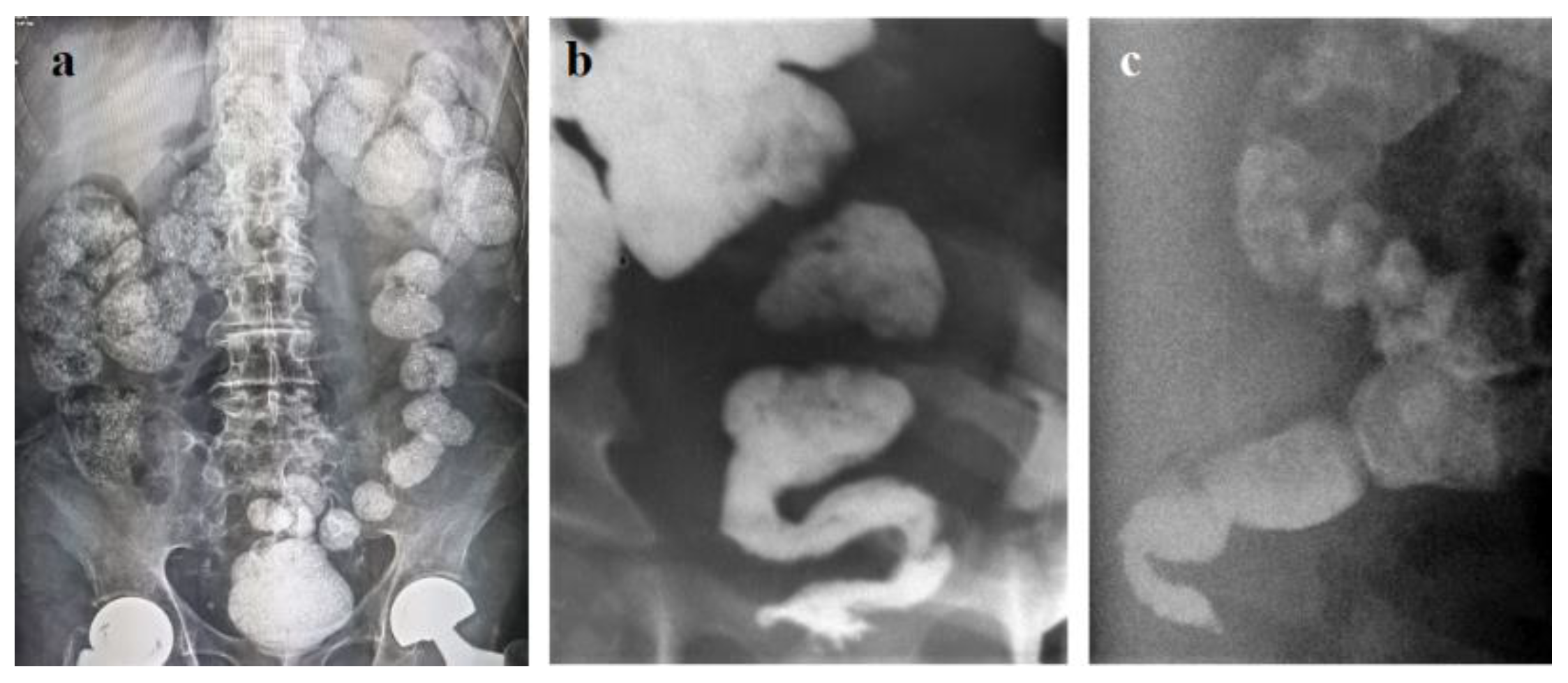
Figure 7.
Radiographs of different patients who swallowed large tablets (LT) with a diameter of 2 to 3 cm. (a) LT in the middle of the esophagus; (b) above the contracted lower esophageal sphincter; (c) in the antrum of the stomach during antral systole; (d) in the duodenal bulb; (e) an x-ray was taken 28 hours after swallowing the LT. A reduced tablet is visible in the small intestine. Traces of barium from the disintegrated surface layer of the tablet are visible in the loops of the small intestine; (f) in the descending colon.
Figure 7.
Radiographs of different patients who swallowed large tablets (LT) with a diameter of 2 to 3 cm. (a) LT in the middle of the esophagus; (b) above the contracted lower esophageal sphincter; (c) in the antrum of the stomach during antral systole; (d) in the duodenal bulb; (e) an x-ray was taken 28 hours after swallowing the LT. A reduced tablet is visible in the small intestine. Traces of barium from the disintegrated surface layer of the tablet are visible in the loops of the small intestine; (f) in the descending colon.
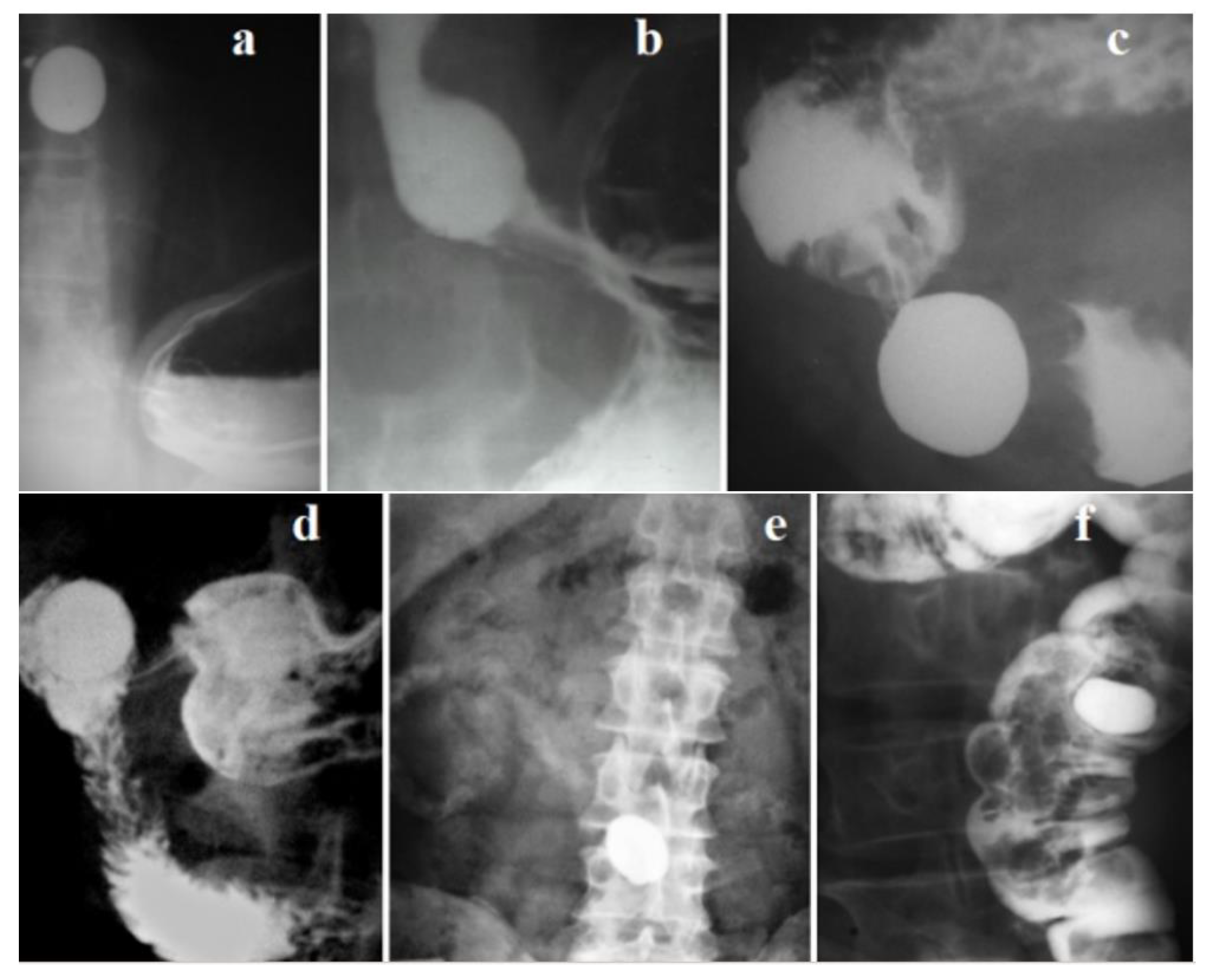
Figure 9.
X-ray images of EGJ while drinking a contrast agent. (a-b). From the article by Kwiatek et al [11]. The authors attached a clip to the end of the rugal folds, believing that this was a EGJ. At the moment the EGJ opened they decided that the clip had risen cranially.
Figure 9.
X-ray images of EGJ while drinking a contrast agent. (a-b). From the article by Kwiatek et al [11]. The authors attached a clip to the end of the rugal folds, believing that this was a EGJ. At the moment the EGJ opened they decided that the clip had risen cranially.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



