
Submitted:
27 December 2023
Posted:
28 December 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
PURPOSE: Our research interrogates Professor Peter Doherty’s warning to Australians in April 2020 that ‘COVID-19 is just as lethal as the Spanish flu’.
METHODS: We identified the epicentres of both pandemics, namely metropolitan Sydney in 1919 and metropolitan Melbourne in 2020. Using original sources, we compared the lethality of COVID-19 in these two cities. Lethality was measured by the number and rate of hospitalisations and deaths per 100,000 of population. Using these two measures, we diagnosed the waves of infection, their severity at various points in time and the cumulative impact of the viruses by the end of our in-depth study period, i.e. 30 September in 1919 and 2020.
RESULTS: Spanish Flu in 1919 was more than 30 times more lethal than COVID-19 in 2020. The hospital admission and death rates of COVID-19 in Melbourne in 2020 constituted a small fraction of the devastation wrought by the Spanish Flu in Sydney in 1919. The patterns and lethality of the pandemic waves were also strikingly different.
DISCUSSION AND CONCLUSION: Both pandemics broke out with the arrival of unknown pathogens against which vaccines and antivirals did not exist. Professor Doherty’s warning was perhaps taken seriously and that partly explains the findings of this study. Containing infection in 1919 and 2020 threw the burden on nonpharmaceutical interventions (NPIs) such as ‘protective sequestration’ (quarantine), contact tracing, lockdowns and masks. We discuss the effectiveness of these. Despite the failures of genomic analysis and the weaknesses of the contact tracing system due to mismanagement, it was persistent and detailed contact tracing that provided the best explanation for why NPIs in 2020 were more effective than in 1919 and therefore contributed to the lower lethality of the COVID-19 pandemic in its first year.
Keywords:
Covid-19
; Spanish Flu
; lethality
; hospital admissions
; death rate
; nonpharmaceutical interventions (NPIs)
; pandemic response
; quarantine
; lockdowns
1. Introduction
Professor Peter Doherty, a Nobel-prize laureate and world authority on viruses, warned Australians in April 2020 that ‘COVID-19 is just as lethal as the Spanish flu’ (1). The speed with which COVID-19 spread in Melbourne and the many personal stories of loss and suffering that defined 2020, the first year of the pandemic, make it hard to reject Professor Doherty’s statement. At the same time, we were curious to discover how the COVID-19 pandemic of 2020 in Australia compared with our experience of the Spanish Flu in 1919. What did the waves of infection look like, how quickly did the pandemics spread, and most important of all does the evidence for 1919 and 2020 show that both pandemics were equally lethal as Professor Doherty suggested? This comparative study employs original data for the Spanish Flu and COVID-19 from the first confirmed case of infection in 1919 and 2020. At the start, we identified the epicentres of both pandemics, namely metropolitan Sydney in 1919 and metropolitan Melbourne in 2020 using data for the calendar years. Using two measures of lethality – the number and rate of hospitalisations and deaths, we then diagnosed the waves of infection and compared their severity at various points in time and the cumulative impact of the viruses. For this in-depth analysis of the pandemics, we defined our study period as 25 January to 30 September 1919 and 2020. Our research began in 2020 on the assumption that the pandemic would burn out in the following year. That has not happened.
We did not know in 2020 that the COVID-19 pandemic would be with us for many years and that the third year, namely 2022, marked a dramatic change in trends compared to the events of the first year. This comparison alone justifies the importance of understanding Year 1 of the pandemic in Australia and its value in comparing it with the Spanish Flu. More importantly, Australians had no access to pharmaceuticals to address the virus in 2020 – this makes year one of the COVID-19 pandemic comparable with 1919. We therefore assessed the efficacy of nonpharmaceutical interventions (NPIs) in the general community. While it is important to acknowledge the essential roles of NPIs in the case of healthcare workers in hospitals, other clinical settings and aged care/disability facilities their contributions to preventing transmission of the virus in these settings are discussed elsewhere (2).
On his retirement in late 2022 as the long serving director of the National Institute of Allergy and Infectious Diseases (NIAID) in the US, Fauci expressed his concerns about the next pandemic saying that ‘we may not necessarily prevent the emergence of a new infection, but hopefully we can prevent it from becoming a pandemic’. Controlling new pathogens in the first phase can only be done by changing state policies and individual behaviour by using NPIs. Fauci also validated the importance of comparative studies against the Spanish Flu benchmark because ‘…the last time a pandemic of this magnitude occurred (i.e. the Spanish Flu) was well over 100 years ago’ (3). Remembering and understanding pandemics is especially important when there has been a long history of forgetting them because they are relatively ‘silent’ once the crisis has passed. Australia, for example, has less than a dozen monuments to those who died from influenza in 1919 compared with 62,000 for soldiers who were killed during the First World War (4), although the death toll from the pandemic was about a fifth of the war dead. Moreover, public perceptions of pandemics are quirky- according to one report the pandemic that generated the greatest amount of fear in Australian history was not the Spanish Flu, with the highest recorded mortality up until 2022, but polio (4).
The diagnostic value of documenting and understanding the pandemic pattern in 2020, its first year, is based on several premises. The strongest justification is that in 2020 Australia (and the world) found itself without vaccines or antivirals for fighting infection. In 2020 we learnt how to slow down and reduce the lethality of COVID-19 using NPIs while we waited for medical science to catch up with our needs by inventing new drugs and vaccines. Many of the tools we used had been known to humankind for thousands of years – in particular putting the sick into quarantine. For example, the Torah (Old Testament) warns us: ‘He shall be unclean as long as the disease is on him. Being unclean, he shall dwell apart; his dwelling shall be outside the camp’ (Book of Leviticus 13-14) (5).
During the Spanish Flu the strict quarantine measures introduced into all Australian ports in October 1918 kept out the most virulent strains of the influenza virus for some four months. When influenza gripped the Australian mainland in late January 1919, swift controls were introduced by central and state governments, including the mandatory isolation of the sick and their close contacts. The New South Wales (NSW) state government introduced the ‘compulsory wearing of masks on trains, trams and ferries and in public streets, places and buildings’ (6). However, policy flip-flops in 1919 acted as constraints on attempts to change how individuals behaved. For example, at the end of February 1919, all laws about masking were removed only to be reintroduced in late-March/early April and then again removed in mid-May never to be introduced again despite the massive upswing in infections (6). Policy flip-flops also occurred in Melbourne in 2020 but they were driven by the rise and fall of infections: as infections rose wearing masks in public became mandatory on 19 July 2020 (7), and when they fell, mandatory mask wearing was limited to indoors, public transport and crowded outdoor areas. This easing was announced on 22 November 2020 but even then, a casual walk in your own neighbourhood, required people to carry a mask in case a crowded situation arose (8). This five-month period of mandatory mask wearing from 19 July to 22 November 2020 contrasted with the much shorter duration of inconsistent mandates in Sydney in 1919 (6).
The value of wearing of masks as a guard against infection was highly controversial in 1919 and also in 2020 (see Discussion). Despite debates, the standout feature of our response to the pandemic of 2020 was that Australians had the benefit of scientific knowledge to establish contact tracing when pharmaceutical interventions were not possible. The Australian and global scenario changed dramatically in February-March 2021 when vaccines against COVID-19 became available. Diagnosing the effectiveness of nonpharmaceutical interventions in 2020 is, therefore critical, given many studies suggesting that we can expect unknown pathogens in the future. As one US Defence Department Study (9) asked, how are we going to protect citizens until our scientific institutions develop pharmaceutical responses to viruses that we have no knowledge of.
2. Materials and Methods
We took the following four steps for our data analysis.
Step 1: Identifying the epicentres of the two pandemics
Estimates of the total deaths caused by the Spanish Flu in Australia range up to 15,000 in the single year of 1919 (10). In this report we have cited the figure given in the Commonwealth Official Year-Book 1901-1919 (11) because its more conservative figure of 11,552 allows us to be cautious. For the capital cities we have used the local state reports because it was the states that reported their estimates to the Commonwealth Government. Using state-based sources also gave us access to time series data. Hence for Sydney we used Smith’s estimate of 3,902 deaths (12) because he also provided a breakdown of the weekly deaths that we needed for our in-depth study of the waves of infection. HA Smith was the government statistician who assisted WG Armstrong the Director General of Health for NSW in 1919; Smith was the author of Part II of the 1919 report which focussed on the mortality aspect of influenza during the epidemic in New South Wales. For Melbourne we used the Victorian Year-Book 1919-20 for the Spanish Flu (13) and the Australian Government Department of Health report on COVID-19 for 2020 (Table 1).
The estimates given in Table 1 differ from those in other parts of this paper because we sought to generate comparisons for the calendar years 1919 and 2020. In reality, the figure of 3,902 deaths for Sydney in 1919 covered the period up to 30 September not 31 December 1919. Using this proxy number, however, is reasonable for two reasons: (a) by the end of September 1919 deaths from Spanish Flu in Sydney were down to single figures and did not rise again; (b) the deaths reported for Melbourne in 1919 were for the whole calendar year but the pandemic was officially declared to have ended in that city on the 8 September 1919 (13) suggesting that as with Sydney, the pandemic had reached single figures. In other words, after 30 September 1919, it is reasonable to assume that the differential impact of the Spanish Flu on the two cities did not change beyond what is stated in Table 1.
Another data problem we faced was the lack of publicly accessible information on the total COVID-19 deaths in Australian capital cities at the end of December 2020. However, it has been reported that deaths in the major cities of Australia accounted for about 87% of total deaths (17). We have therefore decided to use the total COVID-19 deaths for each of the states in the calendar year 2020, i.e. 54 deaths in NSW and 820 in Victoria, as proxies for Sydney and Melbourne (Table 1). The very small number of COVID-19 deaths in NSW demonstrates that Victoria carried the burden of COVID-19 lethality in 2020 (820 out of the national total of 909). Given that 75.8% of population in Victoria resided in Melbourne (Table 1), it is reasonable to assume that Melbourne was Victoria’s epicentre for the pandemic.
Step 2: The prevalence of infection in the general community
The second step in our comparison of lethality in Sydney and Melbourne during the two pandemics, focuses on the incidence or prevalence of infection in the general community. Detailed data about the weekly number of COVID-19 cases in the community in 2020 were available from Victoria’s Department of Health and Human Services (hereafter DHHS); however, we were unable to use them in our comparisons because there were no matching data for the 1919 Spanish Flu. Attempts to keep track of daily infections in 1919 were abandoned in the early stages of the pandemic. Moreover, we have no scientific way of knowing the actual prevalence of infection because the Spanish Flu virus was not identified until 1933 and the genome of the H1N1 virus was only reconstructed in 1997-2005 (18). Armstrong, the NSW Director General of Public Health at the time, concluded in his 1920 report that the Spanish Flu had infected about 290,000 or 36.6% of Sydney residents (19). This estimate was based on a sample of the proportion of employees who were absent from their workplaces from 1 January to 30 September 1919 because of influenza. The survey was based on over 600 ‘establishments, including government departments, banks, insurance offices, merchants’ offices shops and factories’; together they accounted for 106,923 employees of whom 39,195 had been too sick to work during that period (19). Given that about half of these sick workers were women and that the proportion of children who caught the flu were thought to be roughly the same as in the adult cohorts, this percentage was applied to the whole of the Sydney metropolitan population. With the circumstances facing the Sydney health authorities in 1919, their estimates of the extent of infection in the metropolitan area were reasonable. At the same time, this aggregated estimate is no substitute for the time series that we need in order to fully understand the waves of infection. We have, therefore, accepted Armstrong’s calculation that the cumulative number of infections in Sydney in 1919 was 290,000 (19).
Step 3: Hospitalisations as a proxy for the analysis of the waves of infection
As previously noted, no data exists for analysing the weekly trends in community infections in Sydney in 1919. However, weekly data about hospital admissions in metropolitan Sydney were given by Armstrong (the Director General of Public Health) in his Report on the Influenza Epidemic in New South Wales in 1919 (19). Hence we have used this information as a proxy for the waves of community infection and compared that with hospital admissions for Melbourne in 2020. Armstrong’s report for Sydney I919 ran from the week before 1st February (i.e. 25 January) to 30 September, a total of 35.5 weeks. The start of the time series, reflected the dates for the first Spanish Flu infections in Sydney. Fortuitously, the 25 January was also the date of the first confirmed infection by COVID-19 in Melbourne in 2020. Information about hospital admissions in metropolitan Melbourne was provided by DHHS in response to our request for a detailed breakdown of data by each week of the study period and by all the ‘Local Government Areas’ (LGA) for metropolitan Melbourne (20). We collated this data into the estimates we discuss in our report.
Using these sources about hospital admissions as proxies for trends in community infections during the pandemics of 1919 and 2020, made it possible to analyse the weekly fluctuations in infections and the cumulative infections at the end of our in-depth study period 30 September 1919 and 2020.
Step 4: Analysis of the trends in weekly death rates
The Director General of Public Health’s Report on the Influenza Epidemic in New South Wales in 1919 also gave us information about the weekly deaths in Sydney in 1919 (12) while DHHS provided us with data about the weekly COVID-19 deaths in Melbourne (20). Using these sources, we interrogate the Crude Death Rates reported in Table 1 by considering the patterns of weekly and cumulative mortality rates (per 100,000 population) in 1919 and 2020.
Having located the data for analysing the weekly and cumulative pandemic deaths and hospitalisations in 1919 and 2020, some minor data adjustment was needed. While the Report on the Influenza Epidemic in New South Wales in 1919 (12, 19), was comprehensive and detailed for our study period (25 January to 30 September 1919 and 2020), the reporting dates of hospitalisations and deaths were slightly different: weekly hospital admission reports began on Saturday 1 February but weekly death rates began on Tuesday 4 February. Given that we were not investigating the time lag between hospitalisation and deaths, we adjusted the reporting date for deaths in line with the reporting date for hospitalisations: i.e. the first reporting date for deaths in our comparative analysis is now given as Saturday 1 February instead of Tuesday 4 February. The adjusted dates facilitated the comparisons between the weekly hospital and death rates in Sydney in 1919 and Melbourne in 2020. However, the adjusted data is only referred to when we compare the pandemic in Sydney and Melbourne; in other instances where we refer to Sydney deaths in 1919 we cite the unadjusted, original dates given in the Report on the Influenza Epidemic in New South Wales in 1919 (12).
Given the unique nature of the Sydney data and the absence of alternative or more disaggregated sources, we took these adjusted data sets as our starting point and matched the Melbourne data for 2020 with them. The matching time series that we created for COVID-19 in 2020 was based on disaggregated data by Local Government Areas (LGAs) for both hospitalisations and crude death rates from Victorian DHHS (20). Data for the week ending 1 February means that our study period captures trends in the week before for both hospitalisations and crude deaths in Sydney and Melbourne. During the 7 day-period up to that reporting day, there were 23 hospital admissions in Sydney and 3 in Melbourne and no deaths were registered in either city. In both 1919 and 2020, the 1 February was a Saturday, a coincidence that ensures that our weekly timeframes are comparable. In summary: the comparisons between the pandemic in Sydney and Melbourne both cover the in-depth study period 25 January to 30 September, some 35.5 weeks and the weekly reporting dates in both cases begin with Saturday 1 February for preceding week.
3. Results
3.1. Crude Death Rates per 100,000 population in the epicentres of Sydney (1919) and Melbourne (2020)
Using the percentage of national deaths, Table 1 shows metropolitan Sydney as the epicentre of the Spanish Flu in 1919 and metropolitan Melbourne of COVID-19 in 2020: 3,902 deaths representing 33.8% of Australian deaths caused by Spanish Flu in 1919 occurred in Sydney and 820 deaths or 90.2% of Australian deaths caused by COVID-19 were recorded in Melbourne in 2020. The table also yields estimates of the Crude Death Rates per 100,000 population in these two cities: 471 for Sydney in 1919 and 16.1 for Melbourne in 2020. In other words, the death rate in Melbourne from COVID-19 was only 3.4% of that in Sydney from Spanish Flu. Another way to express this is to say that mortality from Spanish Flu in Sydney in 1919 was almost 30 times higher or more lethal than COVID-19 in Melbourne in 2020. These results do not support the notion that COVID-19 pandemic in 2020 was as lethal as the Spanish Flu in 1919. Professor Doherty’s statement does not appear to hold.
3.2. Contrasting patterns of hospitalisations as a proxy for infections
Armstrong estimated that about 36% of Sydney residents had been infected with influenza in 1919: in other words that cumulative infections in Sydney with a population of 828,700 in 1919 came to about 290,000 (19) or 34,995 cases per 100,000 population. This compares with 20,368 cumulative cases of COVID-19, using the State of Victoria’s figure as a proxy (16), or 401 cases per 100,000 population, for metropolitan Melbourne with population of about 5.1 million. The comparison suggests that the infection rate in the general community in Sydney in 1919 was about 87 times greater than that in Melbourne in 2020. The trends behind these annual figures are discussed below; in that analysis we focus on the in-depth study period 25 January - 30 September 2020.
The NSW Department of Health reported that by 30 September 1919, some 14,164 people had been hospitalised in Sydney compared with 2,518 hospitalisations in Melbourne (Figure 1A). Cumulative Melbourne hospitalisations were only 18% of those in Sydney in 1919. The great stress on Sydney’s hospitals is revealed by Figure 1A,B showing that hospitalisations in Sydney exceeded those in Melbourne 5.6 times. Cumulative hospital admissions per 100,000 shows an even greater disparity between Sydney and Melbourne in 1919 and 2020: 1,709 relative to 50 (Figure 2). Sydney admissions were 34 time higher than those in Melbourne. Had Melbourne hospitals been confronted by the same number of hospitalisations as Sydney in 1919, the health system would have been overwhelmed.
Actual hospitalisations fell far short of what was needed in 1919. A total of 25 metropolitan hospitals in Sydney struggled to manage the crisis with only 2,000 beds and 1,488 doctors, nurses and wardsmen (19). Over half of these 1,488 professionals (i.e. 814) eventually caught influenza, making it impossible to operationalise a new 500 bed hospital that had been set up in the Randwick Racecourse (19).
The vast majority of the sick, however, were nursed at home and in some suburbs infection raged in ‘almost every house in every street’.
During the last 100 years, the Australian economy has been totally transformed, with the burden of professional care for the old and sick being spread more widely across multiple institutions. The Health Care and Social Assistance sector has emerged as the largest industry by employment: the estimated Australian workforce of 1.7 million people represents 1 in 7 workers, 30% of them based in hospitals (21). In the state of Victoria (Melbourne is the capital) there were 30,311 registered medical practitioners in 2020, 105,113 nurses and 7,438 nurses and midwives (22). Roughly a third of these were based in hospitals, namely 10,100, 35,037, and 2,479 respectively; supposing that half of these healthcare workers were based in metropolitan Melbourne, it is obvious that the burden on Sydney hospital staff of 1,488 professionals was overwhelming in 1919. In Melbourne, the pressure on professional hospital staff was even less than this because of the 3,519 cases of COVID-19 amongst Victoria’s healthcare workers, only a third (c.1,073) occurred amongst hospital professionals; the bulk of the cases (about 1,714 or 49%) affected professional staff in the aged care homes (23). This statement is not intended to minimise the pressure on the staff of Melbourne’s metropolitan hospitals. In fact, their experience of extra workloads, great exhaustion and stress of correctly donning personal protective (24) all serve as indicators of the unrelenting trauma experienced by the relatively tiny Sydney hospital workforce in 1919.
Figure 1A,B show that the Sydney pandemic was characterised by two very high and distinctive peaks while Melbourne’s crisis took the form of one major wave from mid-July to mid-September with only one peak. The weekly hospital admissions in Sydney first peaked at the week ending 11 April with 1,025 admissions and then again at the week ending 20 June with 1,315 admissions while in Melbourne they peaked at the week ending 8 August with 419 admissions. Given the much larger population of Melbourne in 2020 relative to Sydney in 1919, Figure 1B shows that the dramatic differences between the two pandemics was even greater than the crude numbers suggest: per 100,000 population, the highest weekly hospital admission rates in Sydney were 124 and 159 per 100,000 population for each peak compared with Melbourne’s peak on 8 August at about 8.
Figure 2 shows the cumulative hospital admission rates (per 100,000 population) at any point in time for Sydney in 1919 and Melbourne in 2020 – that is the number of new admissions in week X plus all admissions in the weeks previous to that point. Cumulative weekly admission rates in Sydney in 1919 started at a higher point than Melbourne in 2020 and continued to be higher for the rest of the study period. At the end of September, the cumulative hospital admission rates in Sydney were 1,709 compared with Melbourne’s of 50. The multiple problems of handling the COVID-19 pandemic in Melbourne’s hospitals in 2020 allows us to imagine the extreme stress experienced in Sydney given that the cumulative hospital admissions rate was 34 times higher. Once again, Professor Doherty’s statement does not appear to hold.
3.3. Contrasting patterns of death
The current ‘pandemic era’ which began around 1900 has taught us to anticipate ‘inconsistent behaviour’ in the number, nature and duration of waves of infection and mortality (25, 26). Strict maritime quarantine protected Australia from Europe’s terrible pandemic waves in late 1918, with the result that Australia had only two waves (27). Our analysis so far has addressed the question of hospital admissions in 1919 and 2020. We now consider mortality as the other measure of lethality.
Figure 3 depicts the pandemic waves for Sydney and Melbourne using the weekly cumulative deaths per 100,000 population at the end of each week as reported from 1 February to 30 September. Figure 3 and Table 2 suggest that the speed with which the Spanish Flu pandemic unfolded in Sydney contributed to the high cumulative death rate of 471 per 100,000 population by the end of September 1919. This cumulative death rate was about 30.4 times higher than that of Melbourne (15.5 per 100,000 population) for the same period from week ending 1 February to 30 September in 2020.
The first death from Spanish Flu was recorded in Sydney for the week ending 4 February 1919, while the Melbourne weekly deaths began during the week ending 21 March 2020. Although the first confirmed case of COVID-19 in Melbourne was recorded on the 25 January 2020, there were no deaths for the first seven weeks since the start of the pandemic. In the following 17 weeks there were either no deaths or single-digit deaths (Table 2), with total cumulative deaths coming to only 32 by week 24 ending on 11 July. In other words, during the first six months of the pandemic, total deaths in Melbourne from COVID-19 were exceptionally low. Once more, Professor Doherty’s statement does not appear to hold.
Using a log scale for cumulative death rates ranging from 0.1 to 1,000 deaths per 100,000 population allows us to capture the relatively much higher death rates in Sydney during the Spanish Flu. Figure 3 shows that from week ending 21 March onwards COVID-19 cumulative death rates per 100,000 population in Melbourne took off from a very low starting point but a plateau was quickly reached and maintained for some 17 weeks until mid-July. After that there was a considerable surge that lasted some three weeks in the cumulative death rates after which another plateau was reached lasting till the end of September.
Using weekly death rates per 100,000 population, it is hard to say that Melbourne had two waves of COVID-19. From the onset of the pandemic up to the week ending 11 July there was only a low tide of cumulative death rates ranging from zero up to 0.64 per 100,000 population. Then Melbourne experienced a single wave of cumulative mortality over a period of 12.5 weeks starting in the week ending 11 July when it rose from less than one death to 15.5 deaths per 100,000 population on 30 September 2020.
Figure 3 shows the dramatic contrast between pandemic mortality in Sydney and Melbourne. Instead of plateauing as in the case of COVID-19 in Melbourne in 2020. There was no death reported in the first week of the Spanish Flu pandemic, but there was a surge involving 767 total deaths during the following 11 weeks. This represents a jump in the cumulative death rates from 0.1 to 92.5 per 100,000 population. After that, within 8 weeks the cumulative weekly death rate doubled to 201 and doubled again in the following 4 weeks to 420. Then slowly the cumulative death rate reached 471 on 30 September 1919.
The sheer numbers who were dying in Sydney struck terror in the hearts of all citizens. Table 2 captures some of the desperation that Sydney experienced in 1919. In this analysis, the stages of each pandemic were defined by whether the total deaths per week were reported as single-, double- or triple-digit numbers for a total of 35.5 weeks. The results confirm the high lethality of Spanish Flu in Sydney. The first death had been reported on 4 February 1919 and weekly deaths in single digit numbers were reported for the following 7 weeks. After a week of double-digit weekly deaths (Stage 2) mortality surged to weekly triple-digits for 6 weeks (Stage 3) followed by a decline into double-digit figures for 5 weeks (Stage 4). However, instead of continuing to fall to single digits, mortality surged again to triple-digits for another 5 weeks (Stage 5) before dropping to double-digit numbers and eventually to single numbers by 30 Sep 1919. The total of 11 weeks of triple-digit deaths defined the Spanish Flu for 31% of the pandemic’s duration in Sydney.
By contrast, Melbourne experienced much lower levels of triple-digit deaths for only a single period of 3 weeks (Stage 4 in Table 2), some 27% of the length of elevated mortality levels in Sydney. Even more markedly, despite recording the first confirmed positive case of COVID-19 on 25 January, Melbourne’s rising case numbers (infections) did not generate any deaths for a total of 15 weeks (Stages 1 and 2 in Table 2) or 42% of the duration of the COVID-19 pandemic. Taking all the 24 weeks in Stages 1 and 2 together, when weekly deaths were either zero or single digits, we can say that these 24 weeks of the pandemic up to 11 July demonstrated the low impact of the virus by causing only 32 deaths.
Figure 4 shows the total number of weekly COVID-19 cases in Melbourne from the first confirmed case on 25 January to 30 September 2020 relative to hospital admissions, ICU admissions and deaths. Although we lack comparative data on cases for Sydney, we have included Figure 4 here because it was the fluctuations in total cases that drove government interventions in Melbourne in 2020. Moreover, the trend in weekly COVID-19 cases is the only evidence we have to show that the Melbourne pandemic in fact involved two waves of infection if we take the crude numbers rather than the rate of infection per 100,000 of population. At any point along the top line representing weekly positive COVID-19 cases the public health experts could see how the pandemic trend was developing and advise the government about appropriate actions to take before things became worse. Thanks to the Victoria State Government’s testing and contact tracing regimes, we knew that infection started spreading in Melbourne in mid-March and again in mid-June. Authorities were able to pinpoint specific locations in which COVID-19 was concentrated and where the infectious clusters were moving. Public health interventions brought down not only the cases of infection but also the hospital and ICU admissions and deaths. However, these options were not available for the Spanish Flu; moreover, attempts to keep track of daily infections in 1919 were abandoned in the early stages of the pandemic.
3.4. Summary of the results
The results reported above show that Professor Doherty’s statement does not appear to hold for any measures of lethality using either the calendar years 1919 and 2020 or our in-depth study period of 25 January to 30 September. Instead of being ‘just as lethal as the Spanish Flu’, we found that the COVID-19 pandemic in Melbourne in 2020 was less lethal based on the following evidence:
- The cumulative death rate per 100,000 from Spanish Flu in Sydney in 1919 was about 30 times higher than the death rate from COVID-19 in Melbourne in 2020.
- Per 100,000 the rate of infection in the general community in 1919 was about 87 times higher than in 2020.
- The cumulative hospital admission rate per 100,000 was 34 times higher in 1919 than in 2020.
- The weekly patterns of mortality in 1919 and 2020 were significantly different – Sydney experienced 11 weeks of triple-digit deaths in two distinctive waves compared with Melbourne’s single wave of only three weeks with triple-figure deaths. In other words, the greater lethality of the Spanish Flu in Sydney in 1919 was linked to the elevated levels of mortality in 1919 that were more persistent and lasted longer than was true of Melbourne in 2020.
- From the start of our study period in Melbourne up to 11 July 2020, there were 15 weeks when no deaths occurred (7 weeks in Stage 1 and 8 weeks in Stage 2) compared with the persistent increase in mortality from the start of the pandemic in Sydney. Up to the week ending 11 July there were only 32 cumulative deaths in Melbourne in 2020 compared with 3,477 in Sydney in 1919.
4. Discussion
In this part of our paper we reflect on the severity of the Spanish Flu in 1919 relative to COVID-19 in 2020 and the efficacy of NPIs in containing infections. Much can be learned about how changing human behaviour can dampen the impact of pandemics (28), despite the current public scepticism in Australia about masks, for example. That discussion is followed by an explanation of why our study of COVID-19 in 2020 is dependable given the reliability of the data that was collected in 2020, relative to 2021-2023.
4.1. The critical role of non-pharmaceutical interventions (NPIs) in 1919 and 2020
Our estimates showed that the Spanish Flu death rate in 1919 was more than 30 times the COVID-19 death rate and hospitalisation rates in 2020. This dramatic difference is not unique to Australia: for example, in Switzerland Spanish Flu cases were 40 times greater than confirmed COVID-19 cases in 2020 (29). These estimates are counterintuitive given that relative to the Spanish Flu, COVID-19 appears to have a greater propensity to mutate, resulting in greater infectiveness, and greater longevity because of the ongoing cycle of mutations (30, 31). Of course, without any genomic data for 1918-1919 we can only speculate about the nature of the influenza virus and its various strains at that time. In 2020 the high infectiveness of COVID-19 was identified as being linked to its longer incubation period of between four and 12 days relative to SARS in 2002 (2-7 days) and pandemic influenza in 2009 (2 days) (32). The incubation period of the Spanish Flu virus was very much shorter at a few hours up to one or two days (29, 33), but there is insufficient explanation of the true characteristics of the virus that caused the 1918-1919 pandemic.
The severity of Spanish Flu has never been fully explained despite the research by Tumpey and colleagues on the virulence of the reconstructed Spanish Flu H1N1 virus in 2005 (34). Moreover, the influenza virus appears not to have been the primary driver of mortality: rather it was secondary infections from a range of ‘bacterial pneumopathogens’. These worked in tandem with the H1N1 virus amongst a population that had no experience of or access to antibiotics which did not yet exist (25). Coming on top of the deprivations experienced by all sections of society during the First World War, the immunity of Australians was also very low making them susceptible to viral and bacterial pathogens. The age specific nature of the Spanish Flu may have been another factor driving the severity of the 1919 pandemic. It affected mainly those of working age and many more men than women died. Workforce participation rates (67.7% for men and 22% for women) may have been a factor together with the pub-drinking habits of men that threw them close together after working in crowded blue-collar jobs. Again, there is no certainty about these socioeconomic drivers of the Spanish Flu (6). The many measures that were taken to reduce the spread and severity of Spanish Flu, including the closure of international borders, the lockdown of schools and other public facilities, the wearing of face masks and health measures including public inhalations and inoculations with the Commonwealth Serum Laboratory vaccine and the distribution of aid, were useful but insufficient aids to reducing the high levels of mortality and morbidity that were experienced (35, 36). On the other hand, we suggest in the following section that without NPIs the lethality of Spanish Flu in 1919 would have been even higher.
4.1.1. Protective sequestration as an NPI
Despite the imperfections of NPIs, we should not dismiss the importance of early and timely nonpharmaceutical interventions and realise that without any changes in human behaviour the outcomes of the Spanish Flu in Sydney might have been much worse.
Detailed studies for Australian cities in 1919 do not exist, but we have much to learn from research about the American experience where special attention has been paid to assessing the benefits of quarantine and masks. The US Defence Department wanted to know what could be done to protect America in the event of a sudden pandemic for which pharmaceutical responses such as vaccines or antivirals would take many months to develop. The commissioned study by the University of Michigan Medical School located seven communities that during the second wave of the Spanish Flu pandemic in America (September-December 1918) experienced low rates of infection and no more than one death each (9). The study concluded that the most dramatic example of infection control occurred at the US Navy Yerba Buena Island Training Base (in San Francisco Bay) that was subjected to ‘protective sequestration’ imposed under strict naval command. The base’s island location made that possible. While draconian quarantine of this kind was not workable in most American situations, protective sequestration could be useful in shielding small, contained communities in emergency situations – for example military installations.
The benefits of non-pharmaceutical interventions in more typical situations were demonstrated by two other studies. Research on San Francisco compared with 15 other American cities suggested that a 25% reduction in mortality had occurred thanks to the use of masks and bans on large public gatherings (37). Unfortunately, the city authorities did not persist with their interventions. Had the San Francisco authorities been stricter for longer, the authors suggested that the transmission of flu could have been stopped completely and its mortality rate reduced by about 95%. By extension, had the Sydney metropolitan authorities been more persistent in their interventions instead of engaging in policy flip-flops in their mask mandates, the Spanish Flu might have killed fewer in 1919. The same applies to containing COVID-19 infections in Australia during 2022, the third year of the pandemic; that year was characterised by very high levels of excess mortality from COVID-19 despite the availability of vaccines and antivirals.
A second study of 43 American cities (from 8 September 1918 to 22 February 1919), showed that closing schools and cancelling public gatherings were effective in flattening the impact of the pandemic. About 79% of these 43 cities implemented these two restrictions for a median period of four weeks and this was ‘significantly associated with reductions in weekly EDR’ (Excess Death Rates’) (38). The cities that introduced these NPI strategies earlier experienced statistically significant ‘greater delays in reaching peak mortality’, had ‘lower peak mortality rates’ and ‘lower total mortality’.
As in America, ‘protective sequestration’ or quarantine was highly successful in keeping the Spanish Flu virus at bay in Australia. As an isolated island continent, stringent port regulations made that possible with the result that the most savage influenza strains of 1918 did not enter and Australia escaped the first global waves of the pandemic. By late January 1919 the situation changed with the outbreak of the Spanish Flu in Melbourne and Sydney, the detailed circumstances of which have not yet been fully explained. Once the pandemic burnt itself out, memory of the Spanish Flu dimmed quickly despite the huge number of deaths. The debates about how to control the pandemic, the protests against masks and the policy changes that defined the responses of other countries to influenza became features of the Australian experience in 1919. There has been no study of the Australian experience, comparable to the American research by Markel and others (9, 38) yet there is no reason to think that quarantine in Australia during the Spanish Flu did not make an equally important contribution to dampening the waves of infection.
In 2020 Australia’s quarantine system needed to respond to a much more complex international economy compared to 1919 with frequent arrivals from many global destinations at many entry points. On 1 February 2020 the first ban was introduced preventing all foreign nationals who had left mainland China from landing in Australia until 14 days had passed since they left the People’s Republic of China (39). It was widely assumed that COVID-19 originated in Wuhan, mainland China, as a result of either natural or unnatural causes (40).
Prior to that, arrivals were met at the airport where various degrees of screening for COVID-19 were undertaken. Australians were advised not to travel to Wuhan and then not to travel to China. In early February Australian citizens and permanent residents were evacuated from Wuhan to Christmas Island that had been opened up as a quarantine station. Then on 9 February 2020, the Howard Springs quarantine centre received their first group of many hundreds of evacuees (39). Gradually travel restrictions and then bans were extended to other countries and by mid-March 2020 domestic restrictions were placed on visitors to aged care homes in an effort to protect the vulnerable aged. On the 20 March 2020 Australia closed its international borders to all but Australian citizens, permanent residents and returning family members (39). Two days later, bans were introduced in Melbourne ordering the closure of pubs and bars, entertainment venues, religious gatherings, cafes and restaurants – only a few exceptions were permissible such as takeaway food and drink and very small groups at funerals and some religious events where the ‘1 person per 4 square meters applied’ (39). By the end of March 2020 Australia became one of 12 countries to introduce quarantine hotels as a way of detaining all international arrivals for 14 days surveillance and testing for COVID-19: 14 days was the upper limit of the incubation period for the virus. Arrivals were transported from their arrival points to hotels for 14 days mandatory detention. At first the hotels had ‘red floors’ for only COVID-19 positive arrivals but later these were replaced by dedicated COVID-19 positive hotels or ‘hot hotels’ for arrivals who had tested positive tests for the virus and their close contacts (41).
The system was flawed with 20 known breaches of quarantine, complaints by international arrivals of the poor condition of many of the hotels and how they felt at risk of catching COVID-19 and other infections. Reports were received by authorities about the inadequate protective equipment and procedures in airports, ports, buses and hotels, and the casual attitudes of hotel staff, airline and transport staff, police, defence force personnel, and security personnel (42). The effectiveness of Australia’s quarantine system in 2020 has yet to be systematically assessed but it is reasonable to suggest that despite the inadequacies, the system was a great advance on what was possible in 1919 because testing for the SARS-CoV-2 virus was possible. Given the millions of people affected by the above-mentioned quarantine measures, the breaches were relatively few although, 90% of COVID fatalities in 2020 were linked to quarantine breaches at the Rydges Hotel in Carlton, Melbourne and the other 10% to the Stamford Hotel in Melbourne’s central business district. In other words, the virus escaped from the international arrivals in these two ‘hot hotels’ into the general Melbourne community, mainly via the aged care sector. Paradoxically, our certainty about these transmission routes has been generated by one of our most powerful NPIs against the pandemic in 2020, namely, genomic tracing which was developed to cut the transmission networks.
4.1.2. Contemporary, scientific ‘protective sequestration’ via contact tracing and genomic sequencing
In 2020 ‘protective sequestration’ was placed onto a scientific basis thanks to our capacity to test for the presence of SARS-Cov-2. That led to contact tracing and genomic sequencing of the SARS-CoV-2 virus that enabled governments in Australia to generate detailed maps of outbreaks of infection and the geographical directions in which it had moved. Contact tracing began on the 25 January 2020, the same day that the first Australian case of COVID-19 was confirmed in a patient from Wuhan who had flown to Melbourne via Guangdong six days earlier. Details about outbreaks of infections in public spaces such as shops, cafes and bars appeared daily in Victorian news bulletins, the DHHS website, and social media. The Chief Medical Officer and his staff in Melbourne gave daily press conferences to convey the latest details about the pandemic and provide advice on interventions. Information about the suburb, name of the site, address and the date and time that a COVID-19 positive customer or member of staff was confirmed to have been at that site was widely disseminated. As a consequence, Melbournians had the choice of avoiding specific locations in particular neighbourhoods. Mass communication systems ensured that once the testing results had been released by the laboratories, this information became widely known very quickly. In 1919, by contrast, Sydney residents only knew about the spread of infection in limited areas because the authorities lacked the methods of modern contact tracing or mass communication to generate a wider picture of the emerging trends in the pandemic.
On the other hand, the benefits of imposing ‘protective sequestration’ in Melbourne through targeted lockdowns were partially compromised by the feeling amongst some communities that they were under attack. For example, when high-rise residential towers in North Melbourne and Flemington were identified as clusters of infection on 29 June 2020, movements into and out of the apartments and buildings were stopped without warning or any community consultations involving residents. At any one time, about 500 police were asked to ‘ring- fence’ all the towers including those that had not had a confirmed case of infection (43, 44). No effort was made to explain to residents why stopping the spread of infections needed to involve towers that had not yet succumbed to COVID-19. Nor did the residents have ready access to media releases about the progression of the pandemic, because these were typically in English and many locals were migrants from non-English backgrounds. They were, therefore, poorly prepared for any state intervention – especially of the draconian type. The residential population included refugees from countries where they had suffered police oppression, and many were unemployed or poorly paid, casual workers. The lockdown was supposed to protect the residents by containing the existing infections but in doing this through culturally insensitive means it further reduced the trust that they had in the authorities. Many of the employed residents in these towers were indeed at higher risk of COVID-19 infection because of their lower socio-economic status and willingness to work as casual labourers juggling numerous poorly paid jobs at the same time. The Victorian Chief Medical Officer’s reason for more rather than less intervention was that given the lack of vaccines and antivirals, ‘an abundance of caution’ was necessary to ensure that the risks of cross-infection be minimised in facilities with high population densities. This rationale was totally logical but the lockdowns could have been implemented in better ways and with communications and ‘outreach to multicultural communities’ (45). Even the police complained about the unplanned manner in which this particular ‘protective sequestration’ was implemented.
Contact tracing was an important tool that allowed the Victorian government to re-reinvent the ancient system of ‘quarantine’. When that information required interventions beyond voluntary avoidance practices by individuals, the state used that data to ensure public compliance with stringent public health measures. The majority of these interventions did not lead to the public outrage that defined the quarantine cordon around the high-rise towers of North Melbourne and Flemington. Metropolitan Melbourne experienced a cascading series of mini-sequestrations that peaked with the introduction of city-wide lockdowns and curfews, the latter being unfamiliar to all who did not live through the Second World War. Six lockdowns were implemented during the first two years of the pandemic- the longest lasted 111 days from 9 July to 27 October 2020 (46). On 2 August 2020 the Victorian government declared a ‘state of disaster’ and also imposed a curfew from 8pm to 5am. Six weeks later, on 14 September, the curfew was eased to 9pm to 5am and then removed on 28 September (47).
Notably, Melbourne became the most locked down city in the world (48), at an estimated weekly cost of about AUD$1 billion. Preceding the metropolitan-wide lockdowns, there were lockdowns of particular facilities where infectious clusters had been identified: for example, as reported on 1 August 2020 there were hundreds of active cases including 823 in aged care homes, 377 in public housing towers, 286 meatworkers, 184 in the Al-Taqwa College and several cases in retail outlets (49). Regular monitoring for infection was introduced for residents and essential visitors in aged care homes and public housing towers and special arrangements were made for the delivery of food and medical supplies. Through these means the Victorian government sought to contain the spread of infection at a time when little was known about the virus and when pharmaceutical solutions were not available. Government intervention did not waiver despite many justifiable complaints about the imperfect implementation of these policies. Mini-sequestrations often gave way to lockdowns of whole suburbs or local government areas where numerous infectious clusters had been identified. Travel into and out of these areas was highly restricted and fines were imposed for breaches of the rules – for example, driving beyond one’s residential suburb to another suburb required a good reason such as medical treatment that could not be provided locally.
Genomic tracing had the capacity to enhance the contact tracing system by providing authorities with information about specific strains of the COVID-19 virus and matching that information with data about the clusters of infection. The corona virus has RNA, a genetic code similar to human DNA. Minute changes in RNA are identified by laboratory analysis and then linked to epidemiological information collected from known sites of infection. In this manner, genomic sequencing can help to identify the origins of infections and the sequence of transmission to other localities. The infectious materials analysed came from individuals who had tested positive for COVID-19 and also their symptomless contacts – the latter, in 2020, represented about 18% of all infections (50). In bringing together epidemiological clusters with genomic clusters, a powerful diagnostic tool was invented for tracing the movement of the virus amongst the population. This tool sought to gather a large volume of systematic information to break the networks of viral transmission (50).
Unfortunately, the analysis of genomic clusters came too late in 2020 to prevent infected workers at the Rydges and Stamford Hotels from carrying the virus into the general community and ultimately into aged care homes that suffered the highest lethality. The preliminary results of genomic analysis were not known until mid-June 2020 and the final reports to the DHHS arrived on 31 July 2020 for the Rydges Hotel and on the 4 August for the Stamford Hotel (41). Nor could specific events of transmission be pinpointed and the mode of transmission also remained open to speculation i.e. whether it was the result of contact with inanimate objects in the hotels, poor environmental conditions such as inadequate ventilation or person to person contact. As the Royal Commission inquiry into hotel quarantine noted, the results of contact tracing and genomic sequencing within the ‘hot hotels’ could only be improved and made more timely by placing into each quarantine facility specialised units to prevent and control infection and undertake hotel specific contact tracing (41). This imperfect tracing system may have contributed to the double- and triple-digit weekly deaths recorded in Stages 3, 4 and 5 (Table 2).
While genomic sequencing arrived too late in 2020, its potential to break networks of transmission was eloquently explained to the inquiry into Melbourne’s hot hotels and their failure to secure the ‘protective sequestration’ that had been expected of them. This new knowledge, including the failures to prevent quarantine breaches, stands ready to be mobilised as a powerful NPI in future pandemics caused by the arrival of exotic pathogens. Nor was the more routine contact tracing system without its flaws, even after it was accompanied by the introduction in late August 2020 of wastewater testing for viral fragments (51, 52). Yet, despite being slow and cumbersome, as an NPI, the contact tracing approach provided essential information at a time when genomic sequencing was not an established practice and Australia lacked a Centre for Diseases Control (CDC) or any other system of surveillance comparable to that which existed in the UK and USA (53). Authorities were able to justify the many mini-sequestrations and lockdowns in a way that ensured a high degree of public compliance with the restrictions. Even breaches of the curfews in Melbourne were rare, as dog owners will testify - late night walks for dogs are essential given the confines of apartment living in modern cities but except for dog owners and their pets the streets in Melbourne were empty. Even homeless people were tested for the virus and moved off the streets into hotel accommodation to ensure that the poorest Australians did not become sick and pass on infections.
The lower lethality of COVID-19 in Melbourne in 2020 relative to the Spanish Flu in Sydney in 1919 was achieved largely because of the persistence of the contact tracing system, the detailed information that it generated and the high public awareness of the risks of infection that it created. Thanks to this NPI, the public’s risk appetite in Melbourne was very low in 2020. Other NPIs such as the wearing of masks and physical distancing were, in our view, less effective because they allowed a wider degree of discretion on the part of the individual user. In the worst-case scenarios, contact tracing allowed the Victorian government to justify requisitioning the use of public and private hospitals for providing the residents of aged care housing priority access to treatment. Driven by media images of the horrors experienced by the citizens of Lombardy (Italy), fears of the possible collapse of Melbourne’s hospital system were palpable by March 2020 (54). On 28 July 2020, the state government announced that all elective surgery (except for emergencies in Categories I and II) in public and private hospitals was suspended to make room for the relocation of aged care residents; provision was also made to ensure that there were extra hospital staff to look after them (55).
4.1.3. Cloth masks as NPIs
Despite the lax use of masks even when authorities mandated their use, masks played an important role in containing infection both in 1919 and 2020. Had they been used more systematically and continuously, the outcomes for the communities would have been even better, given the research that increasingly points to the considerable benefits of even cloth masks as an NPI. New research in China suggests that masks are important not only in crowded indoor settings but also in crowded outdoor markets where the SARS-CoV-2 can survive in the air for more than an hour and a half (56).
Again, given the lack of research about the value of masks in the case of Sydney’s Spanish Flu in 1919 we cite American examples that are compelling. Despite the violent resistance to mask wearing in many quarters, many citizens in San Francisco made masks from all kinds of cloth. Medical professionals, however, preferred gauze masks over others. In 1920 Kellogg imitated human mask wearing by covering laboratory dishes with various layers of gauze and pumping the airtight dishes with B. prodigiosus- a common bacillus, also known as Serratia marcescens. The ‘possible reduction in dosage of infection [was] not more than 50% effective’ and in his view did not justify mandatory mask wearing (57). With hindsight we can now appreciate that the widespread wearing of 50% effective cloth masks could have made a big difference to reducing the rate at which infection spread in any location by lowering the viral load to which people were exposed.
A much later laboratory experiment in 1949 involved tests on rabbits wearing gauze masks. It concluded that between 90% and 95% of ‘virulent bovine tubercle’ could be screened out (58). The scientists measured the thread diameters and interthread spaces in gauze and reported that three to six layers of this material ‘occluded practically all of the spaces’ and this accounted for the effective barrier that the gauze had created to the dissemination of the bacterium. In laboratory conditions, high levels of protection were easier to achieve than amongst active citizens. The masks were tight fitting and the rabbits virtually inert. Despite the problem of how to ensure that a face mask provides a proper seal when worn by humans, a recent literature review by Clase et al. supports the value of using a wide range of cloths (including gauze) as barriers against infection on the basis of their review of 25 articles that summarise ‘a century of evidence on the efficiency of cloth and cloth masks to reduce transmission of droplets and aerosols’ (59). Despite the enormous variety of materials, methods and tests, the cumulative evidence showed ‘that even at low thread counts and layers, and for aerosols, some kinds of cloth block substantial percentages of transmission’. The size of the virions (a virion is a complete infectious particle including its genome) of H1N1 and SARS-CoV-2 are similar: 80nm-120nm (0.08mm-0.12mm) in the former case and 100 nm (0.1mm) in the case of SARS-CoV-2 (60, 61). However, neither the size of the virions nor the thread counts of the cloth appear to be the determining factors in screening out viruses. Additional considerations come into play, for at the microscopic level the thread is thick and deep so that the gaps between the threads take the form of tunnels into which small filaments of broken and irregular threads intrude. This means that when a virus particle impacts on a thread it acts ‘like a ball hitting a wall’. It bounces off and cannot ‘redirect itself to avoid obstacles’ (60). If the cloth mask has numerous layers, these add further obstacles that the virion must pass through before it completely escapes from the mask. In short, ‘the point is not that some particles may penetrate the cloth, but that some are blocked’. At a more basic level, masking greatly reduces the distance travelled by the jet stream of air emanating from a sick person: one study reported that without a mask the average distance travelled by a jet stream was 8 feet compared with less than half of that in the case of a bandana elastic T-shirt material mask and as little as 2.5 inches in the case of a stitched mask made from quilting cotton (62). Personal observations over the last three years of the COVID-19 pandemic in Melbourne also showed that masks promote physical distancing on the street by signalling to passers-by that the mask wearer might be infected and needs to be avoided. The mere sight of a person wearing a mask can also trigger memories of the purposes of masks and the risks of contracting an infection during a pandemic if you do nothing. When distancing is not possible masks are even more important as the barrier between the sick and non-sick.
On balance, the evidence shows that cloth masks have always been and remain a useful non-pharmaceutical intervention for citizens trapped in pandemic conditions: they are effective barriers to spreading infection, though imperfect because of difficulties in firmly sealing the edge of the mask against the human face. By the best standards of air filtration in developed countries today they have been superseded by the use of N95 masks which provide the most reliable protection (63) – provided that they are fitted properly. Surgical masks are also useful but significantly inferior to N95s (64).
Despite these technological advances, the day of the cloth mask is far from over given that in 2020 ‘nearly half the world—over 3 billion people—lived on less than US$ 6.85 per day’ (65) and a single N95 mask in Australia costs about US$ 2.60.
Without vaccines or antivirals, the evidence about NPIs discussed above suggests that in 1919 and 2020 the wearing of masks helped to contain the spread and severity of infection in the general community. Combined with contact tracing in the case of Melbourne, masks probably had a greater impact than was true of 1919. As in China, deploying multiple non-pharmaceutical interventions in Melbourne had the additional benefit of reducing the incidence of seasonal flu (66). ‘Year to Date’ comparisons between 2020 (on 8 August) and the previous three years show that Victoria only had 4,722 flu cases relative to an annual average of 20,286 for 2017-2019, a decline of 77% (67). NPIs not only flattened the curve of infections for SARS-CoV-2 but also for influenza. Once the NPIs were rolled back influenza cases in Victoria began to rise dramatically; Australia’s Department of Health and Aged Care reported 35,136 cases between 1 January and 9 October 2022 (68). The data is unequivocal: ‘Australia hasn’t made the most of the lessons of Covid-19 about masks, ventilation, and optimal vaccination to inform public health strategies to reduce the impact of seasonal flu’ (69).
4.1.4. NPIs in Melbourne in 2020 and 2022
We acknowledge that the warnings by Professor Doherty and other scientists, probably helped to galvanise the community to change its behaviour in dealing with the challenges of 2020. That behavioural change happened despite insufficient knowledge in the community about the spread of infection via aerosols rather than droplets (70). The relatively low lethality of COVID-19 in 2020 suggests that Australians responded appropriately during the first year of the new pathogen’s arrival. Only 909 Australian deaths were registered in 2020 relative to 11,552 for the Spanish Flu in 1919, comparing the two calendar years (Table 1). In 2021, there was a small increase in mortality to 1,351 but in 2022 annual deaths soared to 10,095 (71). Using these Australian Bureau of Statistics (hereafter ABS) figures, total mortality ‘due’ to COVID-19 in the three years 2020 to 2022 came to 12,352 (71). These ABS figures refer to people who had died because COVID-19 was the ‘underlying cause of death’ (i.e. due to COVID-19). This figure is almost the same as the total mortality from Spanish Flu in 1919 i.e. 11,552. In other words, Professor Doherty’s predictions in 2020 did not apply to the first year of the COVID-19 pandemic in Australia but they became increasingly relevant over time. Total COVID-19 deaths in 2022 accounted for 81.7% of all Australian deaths since the start of the pandemic in early 2020 despite the multiple benefits of both pharmaceutical interventions (vaccines and antivirals) and the NPIs that were available by then.
The ABS also noted that in addition to deaths ‘due’ to COVID-19 more Australians had died than would normally have been the case because COVID-19 contributed to their death from other underlying causes. The number of national deaths registered under this heading were 9, 60 and 2,901 in 2020, 2021 and 2022 respectively (71). Taking these two categories of deaths (12,352+2,970) the total COVID-19 related deaths in Australia from 2020 to 2022 came to 15,322: 85% of these occurred in 2022 compared with only 6% in 2020. The ABS estimates for the second category of deaths ‘related to COVID-19’ are lower than, for example, the figures given by the Actuaries Institute of Australia. According to that source, in 2022 alone, there were 7,000 ‘incidental COVID-19 deaths’ defied as cases where ‘the person was COVID-19 positive at the time of death, but COVID-19 was not recorded on the death certificate’ (72).
Thanks to the worsening COVID-19 pandemic in 2022, in that year COVID-19 emerged as Australia’s ‘third leading cause of death… behind ischaemic heart disease and dementia’ (72). This shocking outcome for 2022 was predicted in late September 2022 by Professor Crabb (the CEO and Director of the Burnet Institute, Melbourne) (73) who responded to the Australian National Cabinet decision of 30 September 2022 by arguing against the idea that Australia needed to move away from ‘COVID exceptionalism’ and treat it like any other disease by ending ‘mandatory isolation requirements for COVID-19 effective 14 October’ (74, 75). Professor Crabb certainly knew what he was talking about: influenza deaths in 2022 demonstrated that COVID-19 was indeed ‘exceptional’: about 300 people died from flu but deaths from COVID-19 were 40 to 50 times higher. Hospitalisations from influenza up to early December 2022 numbered 1,700 about equal to the total number of people in hospital for COVID-19 on the day of the National Cabinet decision of 30 September 2022. In hearing of the latter’s decision, Professor Crabb, ‘collapsed with disbelief’ (73). For the first time since the end of World War Two, excess deaths in Australia increased in 2022, reversing the long term trend of improving longevity in Australia during the last 78 years.
Another reason for his shock was the growing evidence since 2020 of the extensive, negative impact of long-COVID on the human body. Cabinet’s decision at the end of September cut across a parliamentary inquiry into Long COVID, submitted on 12 November 2022 (76). The report identified between two kinds of ‘long COVID’: firstly, a situation where the symptoms of infection persisted beyond three months after catching the virus and secondly, a situation where the virus ‘caused or triggered’ a chronic or non-communicable disease affecting different organs, the blood and nervous systems. This second circumstance is called Post-acute COVID Sequelae (PACS). In this case a person can recover from the acute phase of COVID-19 but suffer a pre-mature death from these other conditions. The parliamentary inquiry called for more government intervention to curtail deaths and illness – the usual NPIs were named including mandatory masking and the isolation of the sick (76). Their advice was based on not only Australian mortality rates exceeding most of the OECD countries but also the estimated 370,000 Australians with severe long COVID on 31 October 2022. The latter group represented about 6% of people who had ‘symptomatic COVID’ – their seriously compromised health conditions prevented them from resuming their daily routines and jobs (76). Given the rising rates of reinfection and the proliferation of COVID-19 strains, mandatory measures were recommended to ‘manage the unfolding public health-social-economic crisis that will exist for years to come’ (76). The report stressed that to avoid long COVID the best thing was to avoid COVID, yet the estimates suggest that about 11.2% of those infected had had COVID twice and a further 5.4% had had it three times or more (77). The health costs of the COVID-19 pandemic are now contributing to Australia’s fiscal crisis, made evident by questions about the affordability of the National Disability Insurance Scheme (that covers some 500,000 citizens) and the recent purchase of nuclear submarines. More and more international studies have confirmed the devastating impact of Post-acute COVID Sequelae (PACS): if 10% of acute infections lead to persistent symptoms, it could be predicted that about 400 million individuals globally are in need of support for long COVID (78). Altman and colleagues discussed the multiple mechanisms that can lead to such serious long COVID. Another study reported that about a third of 34 patients who died from non-COVID-related causes in 2021 and 2022 had spike protein in their skulls – confirming the view that SARS-CoV-2 contributed to their ill health and possible death in ways that we still do not fully understand (79).
Despite easy access to pharmaceutical and nonpharmaceutical aids, Australia’s appalling death rate from COVID-19 in 2022 (the third year of the pandemic) tells us that we still have much to learn from our experience during the first year of the pandemic. In 2020, the spread of infection was reasonably manageable and contained even with the lack of vaccines or antivirals. The lethality of COVID-19 was relatively low by historical standards and the experience of Australia in 2022. Our public health system did not collapse; nor did we face the serious fiscal crisis that now looms before us. As discussed in the next section, the abandonment of NPIs in 2022, together with the unrelenting propensity of the virus to mutate and assume highly infectious form, make the US Defence Department’s warnings of 2006 relevant today:
“If vaccine and antivirals are not effective, we have to resort to NPIs and we need to know this before the pandemic hits because NPI is costly and socially disruptive; so we need to have a plan and rationale for using them”.(9)
4.2. Transparency and data reliability were better in 2020 than in 2021-2022
The diagnostic value of documenting the contours of the COVID-19 pandemic in 2020, the first year of the pandemic, also arises from the better quality of the data we have for that year. This is especially important because the epidemiology and aetiology of pandemics is an indispensable tool for appropriate public health measures in the short term and pandemic planning in the long run. Such documentation, however, is only as good as the reliability of the data and the access that the public has to it. What emerged with growing clarity in 2022, the third year of the pandemic in Australia, is that over the course of the pandemic, Australian data has become less complete, less reliable and less accessible. These developments are counter-intuitive given that by early 2022 the scientific basis of our response to the pandemic had improved greatly thanks to the arrival and widespread use of vaccines and antivirals and better ways of monitoring the spread of infection using contact tracing and genome analysis. At the end of 2022, stringent complaints were voiced by a number of Australian experts about the lack of public and media understandings of the pandemic caused by federal and state governments refusing to share the data that they did have and the special studies that they themselves had commissioned. A good example of the dire state of public information about COVID-19 in Australia has been given by Hyndman, a member of an inter-university research team set up in March 2020 under Professor McCaw to provide weekly assessments of the progress of the pandemic to the Australian Health Protection Principal Committee or AHPPC (that includes all State Chief Health Officers and the national Chief Medical Officer). The committee regularly provided ‘a relatively good data set of case numbers for all states’. Despite this high-quality research, officially appointed teams such as this ‘were explicitly forbidden to make the data publicly available, even though our data was more accurate than what was appearing in the media’ (80). The secrecy of Australian governments compares poorly with the approach to information sharing in the USA where ‘an official repository of data [was] set up early in the pandemic, and anyone could download it and produce forecasts, and submit those forecasts to the Centre for Disease Control for inclusion in their analysis’ (80). Professor McCaw, head of the taskforce that generates the weekly ‘Situational assessment of COVID-19 in Australia’ for the AHPPC, has also expressed his disappointment with the failure of Australian governments to acknowledge to information provided to them. In particular, he has been concerned about how the Australian public has been misinformed about their own, sensible behavioural responses to the risks of infection. His ‘situational awareness’ data showed that the Australian public was ‘highly compliant’ with government restrictions despite ‘bitter argument … through the media that people weren't taking things seriously’ (81).
MacIntrye, an epidemiologist and one of the world’s foremost experts on biosecurity and bioterrorism, has gone beyond these critiques and documented a much wider practice of government censorship and its impact on medical practitioners who have been silenced from expressing opinions that diverge from the official authorities, including the Therapeutic Goods Administration (TGA), the Australian Health Practitioner Regulation Agency and state based medical councils (82).
On 16 August 2021 she and two colleagues set up ‘OzSAGE’ which is an independent research/advisory association to widen the debate about how best to respond to the COVID-19 pandemic and include a broader range of experts (https://ozsage.org/). However, this was ‘perceived with hostility’ and she was asked to choose between serving on a government committee or working with OzSAGE (83). She and her two colleagues left the health policy committee to devote their energies to OzSAGE. Despite this the government remained unconcerned about their shrinking access to scientists specialising on infections.
Complaints about the lack of transparency in Australia’s pandemic response began well before the complaints described above. In early 2021 widespread criticisms emerged about the delays and confusion surrounding Australia’s vaccine rollout, with the Commonwealth Government hiding behind the screen of saying that full public disclosure was not possible owing to ‘commercial in confidence’ agreements with vaccine suppliers. Official secrecy and its corrosive effect on public trust were contrasted with the New Zealand government’s openness about their vaccine rollout and warnings about possible adverse side-effects (84). A year later in January 2022, Professor McLaws, one of Australia’s leading epidemiologists, was still calling for the release of timely data to show whether the c. 300% increase in hospitalisations in NSW were caused mainly by the Delta or Omicron strain of COVID-19 (85). Such details mattered because they affected public health policies at a time when the Omicron strain was overtaking Delta: the former was milder than Delta but 36% more transmissible than Delta which was 60% more transmissible than the earlier Alpha strain. Professor McLaws’ sense of urgency was driven by the Commonwealth Government’s decision on 30 December 2021 to restrict testing to ‘close contacts’ redefined as ‘a person who spent four hours or more with a confirmed case in a household or ‘household-like’ setting’ (86). Given the growing transmissibility of successive strains of SARS-CoV-2, hardly any time was needed to risk exposure, let alone four hours. McLaws called for more rather than less testing and other ways of containing the costs of running public testing hubs that were groaning under the burden of meeting public demand for tests (85).
Another reason for the reliability of data for 2020 is that self-testing for infection was not yet an option. The Therapeutic Goods Administration (the TGA is the Australian government regulator) only approved the home use of Rapid Antigen Tests (RATs) in mid-October 2021 and made them available from 1 November 2021 onwards (87). In 2020 all testing was carried using RTPCR tests administered by health professionals at government approved centres and clinics. This testing method remains the ‘gold standard’ against which RATs are less accurate, but in a rapidly escalating health crisis RATs play a range of important functions (88). Despite this, the new RATs based reporting system is full of loopholes that did not exist in 2020 (89). In the newly introduced RATS system after 1 November 2021, many people lacked the motivation to test, or thought that they had the flu or if they tested themselves they could not be bothered to report their test results. The roll out of RAT kits to the public was also insufficient and unreliable (90), and acted as a further disincentive to their use by the public if and when supplies became more accessible. As RATs took over and the government data collection system began to crumble, data about the cases of infection and their geographical locus became less and less comprehensive and dependable.
The data limitations for the Spanish Flu pandemic were of a completely different order and could never have been fully rectified by government intervention because the very existence of viruses was yet to be discovered. That did not happen until 1933. As a result, although the sick and their contacts were quarantined in 1919, no assessment could be made of how effective the system of isolation was or the direction in which sickness was moving (6). This meant that quarantine arrangements were working within a knowledge void. The very idea that something called ‘viruses’ was creating sickness was unimaginable, let alone that these viruses could change their genetic features and generate accelerated risks of continuous infection from mutations. It follows that locking down specific high-risk localities beyond large venues where the public gathered (schools for example) remained inconceivable.
Comparative historical studies always suffer from data problems and the Spanish Flu epidemic generated many of these. Information about deaths from flu in 1919 are hampered by the widely reported phenomenon of the large number of people who died in their own homes where ‘whole families had been ill at once’ (91). Reliable figures on those domestic deaths do not exist but anecdotal and other information speaks to the importance of this aspect of the pandemic. In Sydney the Metropolitan Citizen’s Influenza Administrative Committee ran about 100 relief centres to distribute aid to needy households but these provisions were difficult to access. Families wanting food aid, for example, had to request help and send a family member to a depot to fill in an application which was then scrutinised on Saturdays to ensure compliance with the rules that prevented fraud (92). Meat, bread, milk, groceries and vegetables were named in the committee’s report, but not fruit- and it was fruit which the sick preferred to eat (93). Moreover, given the prevailing economic philosophy of the times that treated inequality as a ‘natural’ state of the social order, it is likely that Sydney’s working poor received less than their fair share of domestic assistance despite mortality amongst male labourers being three times higher than amongst middle class professionals (6).
Over time, self-isolation at home became more common given the limited capacity of Sydney hospitals to take everyone. Shortages of doctors, nurses and other staff also emerged as medical professionals caught the virus. On 23 June 1919, it was reported that Sydney hospitals would now only take the most serious cases (94). Of course, even less serious cases on one day might suddenly turn lethal on the next. Temporary ‘influenza hospitals’ were opened in every accessible public facility including ‘schools, showground buildings, churches, gaols, bowling clubs, tearooms, drill halls and courthouses’ (6). The general chaos that characterised life in 1919 was exacerbated by the speed with which the Spanish Flu claimed lives even within a 24- hour window- although the modal time from onset of the flu to death was 7 days (95).
The available evidence suggests that the collection of data was hardly uppermost in the minds of citizens or medical professionals and their volunteer helpers. Moreover, many victims of the Spanish Flu, just like the government officials who reported on sickness and mortality, had no way of separating the symptoms of the pandemic virus from other kinds of influenza or respiratory diseases. ‘Flu-like’ symptoms continue to confuse medical practitioners and researchers to this day (96). The government statistician’s report of 1920 sought to distinguish between pneumonial influenza, influenza with pneumonia and influenza ‘for what they were worth’ and despite ‘differences of opinion between medical men’ about the appropriateness of these distinctions (12). Most dramatically, Cumpston, Australia’s Director of Quarantine, insisted that Australia’s 1919 epidemic was unrelated to the Spanish Flu that had devastated the rest of the world: ‘it is legitimate to say that the evidence available points more directly to a slow evolution of an established local infection than to the introduction of fresh sources of infection from outside’ (97). Perhaps Cumpston was too eager to claim that his control over Australian ports and the arrival of ships with returning soldiers, passengers and cargo had secured Australia against any migration of the disease from the quarantine stations to the domestic population? More realistically, The Medical Journal of Australia noted that ‘Confidence [about the specific nature of the flu] can only be attained if the medical profession admits frankly and without reserve the extent of its ignorance of the causation of influenza and the limitations of its powers to gain a mastery of the disease’ (36). As noted under ‘Materials and Methods’, we have used conservative estimates for the total deaths during the Spanish Flu and data that was presented in its original weekly summary form for Sydney.
During the first year of the COVID-19 pandemic, Melbourne’s victims of infection also largely dealt with their own sickness in home isolation. At the end of our in-depth study period, 30 September 2020, this ‘hidden health crisis’ meant that of the 305 active cases in Victoria only 44 (about 15%) were in hospital including six in intensive care (98). The remaining 85% of active COVID-19 cases were nursing themselves at home or via telehealth with health professionals. Thousands more of symptomatic and asymptomatic Australians also suffered the physical and psychological effects of COVID-19 alone. Throughout the year, health professionals were being called upon to become directly involved in home-based or clinic based primary health care of COVID-19 patients (99), despite official policies that placed the management of the pandemic in the hands of hospitals and clinics.
The difference between home nursing in 1919 and 2020 is that Melbourne’s ‘hidden health crisis’ in 2020 did not distort the data we have about COVID-19 deaths or hospitalisations. This is because mortality from COVID-19 was concentrated in aged care homes where many of the oldest and most vulnerable Australians lived. On 19 September 2020, about 74% of deaths from SARS-CoV-2 had occurred amongst those ‘living in aged care homes at the time of their deaths, although many died in hospital’ (100). Cases of infection in the ten worst affected aged care homes in Victoria on 31 July 2020 came to 49% of residents and 38% of staff (101, 102). The concentration of deaths in older persons and particular facilities, means that the data on hospitalisations and deaths is relatively complete and accurate. Moreover, the newly introduced telehealth system placed high risk patients into regular contact with their GPs who, in turn, would arrange for the evacuation of their clients to hospitals in emergency cases.
At another level of analysis, we learn from investigations into the aged care sector about the inadequacy of NPIs – not because appropriate technology was lacking but because there were insufficient supplies of protective masks and gloves provided to aged care homes (41). Other evidence pointed to the casualisation of labour with some 70% of part time aged care workers struggling to manage COVID-19 with six weeks training as part of their Certificate 3 courses (103). Many casual staff also worked at numerous aged care facilities in order to earn decent incomes and this allowed corridors of infection to develop between aged care homes, family residences and the workplaces of other family members. By the end of July, the Australian government banned aged care staff from working at more than one site in Victoria (104) and paid ‘pandemic leave’ for casual workers was introduced in the hope of encouraging staff with symptoms to stay away from their workplaces. Yet the system was not applied universally and only staff who had been employed on a ‘regular and systemic basis’ were eligible (105). Many casual workers did not qualify and continued to work at numerous part-time jobs. As happened during the Spanish Flu in 1919, Melbourne’s working poor in 2020 were compelled to take greater health risks than the general workforce because they needed multiple income sources to make up for low wages (106, 107).
It is salutary to remind ourselves that inequality in developed countries today, including Australia, has reached the old levels of the pre-Keynesian revolution of the 1940s (108). This is reflected in the studies about the COVID-19 pandemic showing a correlation between a higher incidence of COVID-19 infection in metropolitan Melbourne in 2020 and ‘larger proportions of people who were unemployed, without paid leave benefits, or experiencing mortgage or rent stress, and in areas with higher population and housing density or larger proportions of people who speak languages other than English at home’ (109). The report of the Parliamentary Inquiry of 2021 confirmed this: in metropolitan Melbourne ‘The five councils that had the most active COVID-19 cases as at 1 December 2020 are amongst the 10 most disadvantaged councils in Victoria’ (107).
The data limitations associated with the Spanish Flu in Australia cannot be fixed – we are stuck with the sources that we have used in this analysis. Yet the benefits of comparative studies overwhelm these constraints, especially when the data for COVID-19 in 2020, the first year of the ongoing pandemic, are relatively complete and reliable. Our confidence in this statement is based on recognising the data limitations which emerged in Australia towards the end of 2021, the second year of the pandemic, and how by 2022 serious concerns about these data problems were being expressed by many of Australia’s leading scientists.
5. Conclusion
Our analysis in this paper is based on comparing metropolitan Sydney and metropolitan Melbourne, the two Australian epicentres for the Spanish Flu and COVID-19 pandemics, in 1919 and 2020 respectively. Our findings show that by various measures the Spanish Flu in 1919 was significantly more lethal than COVID-19 in 2020 (see 3.4 Summary of the Results). However, over time, Professor Doherty’s warning in April 2020 that ‘‘COVID-19 is just as lethal as the Spanish flu’ has become increasingly pertinent. The year of great lethality in Australia was 2022, the third year of the COVID-19 pandemic (See section 4.1.4 NPIs in Melbourne in 2020 and 2022). The critical difference between the first and third year of the pandemic was that in 2020 our first and only line of defence against COVID-19 was the use of NPIs. In the third year of the pandemic, we had the additional benefit of a second line of defence against infection and death in the form of vaccines and antivirals. The great paradox of Australia’s experience of the pandemic is that our second line of defence using pharmaceuticals displaced NPIs as our first line of defence. We then went one step further: lead by Australian governments, the general public decided that pharmaceuticals were now our only line of defence and NPIs were no longer needed. In 2020, lacking all other options, we choose to use NPIs but then, as the benefits of scientific knowledge arrived in the form of pharmaceutical intervention, we choose to abandon contact tracing and face masks and only use RATs when compelled to do so i.e. rarely. We have also discouraged residents from undertaking RTPRC tests by, amongst other things, the recent decision to close down the single, remaining drive-in testing centre in Melbourne. As we abandoned NPIs the lethality of COVID-19 surged in 2022 and first equalled and then overtook the lethality of the Spanish Flu in 1919 when measured by the crude death figures. Reflecting on the trends that had emerged by the end of 2022, Professor Crabb declared that Australia had created the ‘worst public health disaster in living memory’ (110).
The lessons of 2020 and the inestimable value of NPIs remain highly relevant today, especially if we take pandemic planning seriously. We need to imagine what might happen if new unknown pathogens or mutations of SARS-CoV-2 arrive and these have a special appetite for killing mainly people of working age as happened during the Spanish Flu? This, economically productive demographic cohort in contemporary Australia is far larger than the aged cohorts that have been the main victims of COVID-19 thus far. The only way to prevent elevated mortality at the start of any pandemic, is to use NPIs, our first and only line of defence, as was true of 2020. Then as the miracle drugs arrive, we will be able to add a second line of defence to our public health strategies. At that stage, it is critical for government, professional and community leaders to prevent citizens from developing the false expectation that miracle drugs lead to miracle cures. If we have learnt anything from the elevated lethality of COVID-19 in the third year of the pandemic in Australia, it is that pharmaceutical interventions are a necessary but insufficient response to an ongoing pandemic. Based on our experience in 2020, the first year of the pandemic in Australia, NPIs should remain our first line of defence because even after the miracle drugs have been invented, the roll-out of pharmaceutical options is typically delayed or interrupted by the many management issues that confront health and supply systems under stress. Moreover, the time and effort that is needed to get vaccinated or obtain supplies of antivirals puts off many people who are then tempted to rationalise their sickness by assuming that they have caught the flu or a cold, not COVID-19. By contrast, wearing a mask and avoiding crowded indoor and outdoor spaces requires much less individual effort: all one has to do is always carry a mask when leaving home and avoid crowds or wear a properly sealed mask if attending a mass event. The relatively small amount of behavioural change required by NPIs is a worthy investment by all citizens in their own future.
Author Contributions
MV and LP contributed to the concept of the research, literature review and revised the manuscript critically for important intellectual content. MV and NW contributed to acquisition of data, analysis and interpretation of results. MV drafted the manuscript, and all authors read and approved the final manuscript.
Funding
This research received no external funding.
Acknowledgments
We are grateful for the provision of COVID-19 datasheets in response to our requests to the Government of Victoria Department of Health and Human Services (DHHS), Public Health Events Surveillance System, Notifiable Conditions. We thank Dr Serajul Hoque (DHHS) for his help in sourcing this information. We have also benefited from the support provided in sourcing documents by the Monash University Library Document Delivery system and Dr Deborah Bennett, Parliamentary Librarian, NSW Parliamentary Library, Sydney, Australia.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Walker, J. Chilling evidence of COVID-19’s potency. The Weekend Australian. 4 April 2020. Available at: www.theaustralian.com.au/science/coronavirus-is-just-as-lethal-as-spanish-flu-nobel-laureate-peter-doherty-warns/news-story/351d7fc88c012d7f4a4b2d1659f12942 (Accessed 18 October 2020).
- Utzet M, Benavides FG, Villar R, Burón A, Sala M, López L-E, et al. Non-Pharmacological Preventive Measures Had an Impact on COVID-19 in Healthcare Workers before the Vaccination Effect: A Cohort Study. Int J Environ Res Public Health (2022) 19(6):3628. [CrossRef]
- Young, S. Fauci Q&A: On masking, vaccines, and what keeps him up at night. WebMD Health News. 30 January 2023. Available at: https://www.medscape.com/viewarticle/987658?src=WNL_trdalrt_pos1_ous_230202&uac=398377DN&impID=5133523%20-%20vp_4 (Accessed 3 February 2023).
- Huf B, Mclean H. Epidemics and pandemics in Victoria: Historical perspectives. Melbourne, Victoria, Australia: Department of Parliamentary Services, Parliament of Victoria (2020). Available at: https://apo.org.au/sites/default/files/resource-files/2020-05/apo-nid303897.pdf (Accessed 1 April 2023).
- Piterman L, Vicziany M, Yang H. Questioning quarantine: There is a better way to do this: Medical Republic (2020). Available at: https://www.medicalrepublic.com.au/questioning-quarantine-there-is-a-better-way-to-do-this/33884 (Accessed 30 March 2023).
- McCracken K, Curson P. “Flu downunder: A demographic and geographic analysis of the 1919 epidemic in Sydney, Australia”. In: Killingray D, Oxford JS, Phillips H, Ranger T, editors. The Spanish Influenza Pandemic of 1918-1919: New Perspectives. 1st ed. London, UK: Routledge, Taylor and Francis Group (2003). p. 110-3.
- State Government of Victoria Department of Health and Human Services. Face coverings mandatory for Melbourne and Mitchell Shire. Melbourne, Victoria, Australia: State Government of Victoria (2020). Available at: https://www.dhhs.vic.gov.au/updates/coronavirus-covid-19/face-coverings-mandatory-melbourne-and-mitchell-shire (Accessed 6 June 2023).
- State Government of Victoria Department of Health and Human Services. Statement from the Premier - 22 November 2020. Melbourne, Victoria, Australia: State Government of Victoria (2020). Available at: https://www.dhhs.vic.gov.au/updates/coronavirus-covid-19/statement-premier-22-november-2020 (Accessed 6 June 2023).
- Markel H, Stern AM, Navarro JA, Michalsen JR. A historical assessment of nonpharmaceutical disease containment strategies employed by selected U.S. communities during the second wave of the 1918-1920 influenza pandemic: Final report. Defense Threat Reduction Agency, Advanced Systems and Concepts Office (2006). Available at: https://hdl.handle.net/2027/mdp.39015064102463 (Accessed 6 March 2023).
- Hobbins P, McWhinney G, Wishart A. An intimate pandemic: Creating community histories of the 1918–19 influenza pandemic. Sydney, NSW, Australia: Royal Australian Historical Society (2019). Available at: https://www.rahs.org.au/wp-content/uploads/2019/01/Research-guide-final-version.pdf (Accessed 8 February 2023).
- Commonwealth Government of Australia. Official Year Book, 1901-1919. Melbourne, Victoria, Australia: Commonwealth Government of Australia (1920). Available at: https://www.ausstats.abs.gov.au/ausstats/free.nsf/0/74934FD052EE5A3BCA257AEF001938FF/$File/13010_1901_1919_bk13.pdf (Accessed 7 August 2023).
- Smith, HA. “Part II.- Mortality statistics”. In: Report on the influenza epidemic in New South Wales in 1919. Report of Director-General of Public Health: NSW Department of Health (1920). p. 173-80. Available at: http://pandora.nla.gov.au/pan/83132/20080410-1521/influenza_report_full_36-44.pdf (Accessed 7 August 2023).
- Australian Bureau of Statistics (ABS). Victorian Year-Book 1919-20. Melbourne, Victoria, Australia: Australian Bureau of Statistics (1921). Available at: www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/1301.21919-20?OpenDocument (Accessed 7 August 2023).
- Australian Bureau of Statistics (ABS). Australian Demographic Statistics, June 2019. Estimated resident population. Australian Bureau of Statistics (2019). Available at: https://www.abs.gov.au/AUSSTATS/abs@.nsf/Lookup/3101.0Main+Features1Jun%202019?OpenDocument (Accessed 7 August 2023).
- Australian Bureau of Statistics (ABS). Regional population, 2018-2019. Canberra, ACT, Australia: Australian Bureau of Statistics (2020). Available at: www.abs.gov.au/statistics/people/population/regional-population/2018-19 (Accessed 7 August 2023).
- Australian Government Department of Health. Coronavirus (COVID-19) at a glance – 31 December 2020. (2020). Available at: https://www.health.gov.au/resources/publications/coronavirus-covid-19-at-a-glance-31-december-2020 (Accessed 7 August 2023).
- Australian Institute of Health and Welfare. “The impact of a new disease: COVID-19 from 2020, 2021 and into 2022”. In: Australia’s health 2022: Data insights. catalogue number AUS 240, Australia’s health series number 18. Canberra, ACT, Australia AIHW, Australian Government (2022). p. 1-60. [CrossRef]
- Jordan, D. The deadliest flu: The complete story of the discovery and reconstruction of the 1918 pandemic virus: Centers for Disease Control and Prevention, US Department of Health and Human Services (2019). Available at: www.cdc.gov/flu/pandemic-resources/reconstruction-1918-virus.html (Accessed 17 June 2023).
- Armstrong, WG.; “Part I. - Epidemiology and Administration”. In: Report on the influenza epidemic in New South Wales in 1919. Report of Director-General of Public Health: NSW Department of Health (1920). p. 144-72. Available at: http://pandora.nla.gov.au/pan/83132/20080410-1521/influenza_report_full_6-35.pdf (Accessed 7 August 2023).
- State Government of Victoria Department of Health and Human Services. Public Health Events Surveillance System, Notifiable Conditions dataset for COVID-19 [Unpublished data received]. 1 October 2020.
- Australian Bureau of Statistics (ABS). A caring nation – 15 per cent of Australia’s workforce in Health Care and Social Assistance industry. Canberra, ACT, Australia: Australian Bureau of Statistics. 12 October 2022. Available at: https://www.abs.gov.au/media-centre/media-releases/caring-nation-15-cent-australias-workforce-health-care-and-social-assistance-industry (Accessed 12 July 2023).
- MacKinnon, K.; Healthcare worker infections dashboard. Analytics: Health Care Workers Australia (2021). Available at: https://healthcareworkersaustralia.com/analytics/ (Accessed 20 July 2023).
- State Government of Victoria Department of Health and Human Services. Victorian Healthcare Worker Coronavirus (COVID-19) Data, 30 September 2020. Melbourne, Victoria, Australia: State Government of Victoria (2020). Available at: https://www.dhhs.vic.gov.au/victorian-healthcare-worker-covid-19-data (Accessed 30 September 2020).
- Buising KL, Williamson D, Cowie BC, MacLachlan J, Orr E, MacIsaac C, et al. A hospital-wide response to multiple outbreaks of COVID-19 in health care workers: lessons learned from the field. Med J Aust (2021) 214(3):101-4.e1. [CrossRef]
- Morens DM, Taubenberger JK. Understanding Influenza Backward. JAMA (2009) 302(6):679-80. [CrossRef]
- Taubenberger JK, Morens DM. Pandemic influenza—including a risk assessment of H5N1. Rev Sci Tech (2009) 28(1):187-202. [CrossRef]
- Short KR, Kedzierska K, Van de Sandt CE. Back to the future: Lessons learned from the 1918 influenza pandemic. Front Cell Infect Microbiol (2018) 8:343. [CrossRef]
- Lacombe K, Bhagani S. COVID-19 prevention strategies from real-world data. Medscape. 27 June 2023. Available at: https://reference.medscape.com/recap/989356 (Accessed 25 August 2023).
- Standl F, Jöckel K-H, Brune B, Schmidt B, Stang A. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect Dis (2021) 21(4):e77. [CrossRef]
- Zhao LP, Lybrand TP, Gilbert PB, Payne TH, Pyo C-W, Geraghty DE, et al. Rapidly identifying new coronavirus mutations of potential concern in the Omicron variant using an unsupervised learning strategy. Sci Rep (2022) 12(1):19089. 1908. [CrossRef]
- State Government of Victoria Department of Health. Chief Health Officer Update - 12 May 2023. Melbourne, Victoria, Australia: State Government of Victoria (2023). Available at: https://www.health.vic.gov.au/media-releases/chief-health-officer-update-12-may-2023 (Accessed 1 June 2023).
- Petersen E, Koopmans M, Go U, Hamer DH, Petrosillo N, Castelli F, et al. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect Dis (2020) 20(9):e238-e44. [CrossRef]
- Nuzum JW, Pilot I, Stangl FH, Bonar BE. Pandemic influenza and pneumonia in a large civil hospital. JAMA (1918) 71(19):1562-5. [CrossRef]
- Tumpey TM, Basler CF, Aguilar PV, Zeng H, Solórzano A, Swayne DE, et al. Characterization of the reconstructed 1918 Spanish influenza pandemic virus. Science (2005) 310(5745):77-80. [CrossRef]
- Hyslop, A. “Forewarned, forearmed: Australia and the Spanish influenza pandemic, 1918–1919”. In: Lack J, editor. 1919: The Year Things Fell Apart? Melbourne, Victoria, Australia: Australian Scholarly Publishing (2019). p. 31-4.
- McQueen, H.; “The ‘Spanish’ Influenza Pandemic in Australia, 1912-19”. In: Roe J, editor. Social Policy in Australia - Some Perspectives 1901-1975. Stanmore, NSW, Australia: Cassell Australia (1976). p. 131-48. Available at: https://labourhistorycanberra.org/2018/06/the-spanish-influenza-pandemic-in-australia-1912-19/ (Accessed 7 February 2023).
- Bootsma MCJ, Ferguson NM. The effect of public health measures on the 1918 influenza pandemic in U.S. cities. Proc Natl Acad Sci U S A (2007) 104(18):7588-93. [CrossRef]
- Markel H, Lipman HB, Navarro JA, Sloan A, Michalsen JR, Stern AM, et al. Nonpharmaceutical interventions implemented by US cities during the 1918-1919 influenza pandemic. JAMA (2007) 298(6):644-54. [CrossRef]
- Campbell K, Vines E. COVID-19: A chronology of Australian Government announcements (up until 30 June 2020). Parliamentary Library Research Paper Series (2021). Available at: https://parlinfo.aph.gov.au/parlInfo/download/library/prspub/8027137/upload_binary/8027137.pdf (Accessed 26 March 2023).
- MacIntyre, R. “Jurassic Park for viruses”. In: Dark Winter. An insider’s guide to pandemics and biosecurity. Sydney, NSW, Australia: UNSW Press (2022). p. 65-80.
- COVID-19 Hotel Quarantine Inquiry. Final Report and Recommendations. Volume 2, Chapter 9 (2020). Available at: https://content.royalcommission.vic.gov.au/sites/default/files/2020-12/0387_RC_Covid-19%20Final%20Report_Volume%201%2B2_Digital.pdf (Accessed 1 March 2023).
- Haire B, Gilbert GL, Kaldor JM, Hendrickx D, Dawson A, Williams JH. Experiences of risk in Australian hotel quarantine: a qualitative study. BMC Public Health (2022) 22(1):953. [CrossRef]
- Fowler M, Booker C. Anger at hard lockdown for towers without confirmed virus cases. The Age. 5 July 2020. Available at: https://www.theage.com.au/national/victoria/covid-public-housing-wrap-20200705-p5596z.html (Accessed 28 June 2023).
- Kelaita P, Pienaar K, Keaney J, Murphy D, Vally H, Bennett CM. Pandemic policing and the construction of publics: an analysis of COVID-19 lockdowns in public housing. Health Sociol Rev (2023):1-16. [CrossRef]
- Parliament of Victoria Public Accounts and Estimates Committee. Inquiry into the Victorian Government’s response to the COVID-19 pandemic. Findings and recommendations. Melbourne, Victoria, Australia: Victorian Government Printer (2021). p. xxiii-xlvii. Available at: https://new.parliament.vic.gov.au/49706e/contentassets/9c4e489fe9834121826347ad523e87d2/paec_59-08_vic_gov_response_to_covid-19_pandemic.pdf (Accessed 28 June 2023).
- Wikipedia contributors. COVID-19 lockdowns: Wikipedia, The Free Encyclopedia (2023). Available at: https://en.wikipedia.org/w/index.php?title=COVID-19_lockdowns&oldid=1146756105 (Accessed 4 April 2023).
- Fair Work Commission. Information note – COVID-19 situation update 28 September 2020. COVID-19 information notes and updates. Canberra, ACT, Australia: Commonwealth of Australia (2020). Available at: https://www.fwc.gov.au/documents/resources/covid-19-information/information-note-covid-19-situation-update-2020-09-28.pdf (Accessed 2 June 2023).
- Kelly, L.; Melbourne to ease world’s longest COVID-19 lockdowns as vaccinations rise. Reuters. 17 October 2021. Available at: https://www.reuters.com/world/asia-pacific/melbourne-ease-worlds-longest-covid-19-lockdowns-vaccinations-rise-2021-10-17/ (Accessed 3 February 2023).
- State Government of Victoria Department of Health and Human Services. Coronavirus update for Victoria - 1 August 2020. Melbourne, Victoria, Australia: State Government of Victoria (2020). Available at: https://www.dhhs.vic.gov.au/coronavirus-update-victoria-1-august-2020 (Accessed 9 July 2023).
- COVID-19 Hotel Quarantine Inquiry. Final Report and Recommendations. Volume 1, Chapter 2 (2020). Available at: https://content.royalcommission.vic.gov.au/sites/default/files/2020-12/0387_RC_Covid-19%20Final%20Report_Volume%201%2B2_Digital.pdf (Accessed 1 March 2023).
- Parliament of Victoria Legislative Council Legal and Social Issues Committee. Inquiry into the Victorian Government’s COVID–19 contact tracing system and testing regime. Melbourne, Victoria, Australia: Victorian Government (2020). Available at: https://www.parliament.vic.gov.au/images/stories/committees/SCLSI/Inquiry_into_the_Victorian_Governments_COVID19_Contact_Tracing_System_and_Testing_Regime_/report/LCLSIC_59-05_Vic_Gov_COVID-19_contact_tracing_testing.pdf (Accessed 18 February 2023).
- State Government of Victoria. Wastewater testing. Melbourne, Victoria, Australia: State Government of Victoria (2020). Available at: https://www.coronavirus.vic.gov.au/wastewater-testing (Accessed 19 February 2023).
- Breadon P, Fox L, Emslie O. The Australian Centre for Disease Control (ACDC): Highway to Health. Melbourne, Victoria, Australia: Grattan Institute (2023). Available at: https://grattan.edu.au/report/acdc-highway-to-health/ (Accessed 13 February 2023).
- Blau A, Martino M. Coronavirus could flood our hospital ICUs with COVID-19 patients, so do we have enough beds? ABC News. 27 March 2020. Available at: https://www.abc.net.au/news/2020-03-27/coronavirus-australia-covid-19-icu-beds-ventilators-hospitals/12090420 (Accessed 17 June 2023).
- ABC News. Victorian elective surgeries suspended as coronavirus cases grow by 384 with six more deaths. ABC News. 28 July 2020. Available at: www.abc.net.au/news/2020-07-28/coronavirus-case-numbers-victoria-rise-384-with-six-new-deaths/12498024 (Accessed 17 June 2023).
- Mingyu L, Shelan L, Liebo Z, Fengying W, Kunyang W, Hanqing H, et al. Analysis of a super-transmission of SARS-CoV-2 omicron variant BA. 5.2 in the outdoor night market. Front Public Health (2023) 11:1153303. 3303. [CrossRef]
- Kellogg WH, MacMillan G. An experimental study of the efficacy of gauze face masks. Am J Public Health (1920) 10(1):34-42. [CrossRef]
- Lurie MB, Abramson S. The efficiency of gauze masks in the protection of rabbits against the inhalation of droplet nuclei of tubercle bacilli. Am Rev Tuberc (1949) 59(1):1-9. [CrossRef]
- Clase CM, Fu EL, Ashur A, Beale RCL, Clase IA, Dolovich MB, et al. Forgotten Technology in the COVID-19 Pandemic: Filtration Properties of Cloth and Cloth Masks—A Narrative Review. Mayo Clin Proc (2020) 95(10):2204-24. 2204. [CrossRef]
- Clase C, Fu E, Carrero JJ. COVID-19 masks FAQs: How can cloth stop a tiny virus? What’s the best fabric? Do they protect the wearer? The Conversation. 12 October 2020. Available at: https://theconversation.com/covid-19-masks-faqs-how-can-cloth-stop-a-tiny-virus-whats-the-best-fabric-do-they-protect-the-wearer-146822 (Accessed 7 March 2023).
- Saxena SK, Kotikalapudi R, Tiwari S, Muvva C. Influenza A(H1N1)pdm09 virus: Therapeutics and challenges. Future Virology (2012) 7(10):947-50. [CrossRef]
- Verma S, Dhanak M, Frankenfield J. Visualizing the effectiveness of face masks in obstructing respiratory jets. Phys Fluids (2020) 32(6):061708. [CrossRef]
- L’Orange, C.; What’s the best mask for COVID-19? A mechanical engineer explains the science after two years of testing in his lab. The Conversation (2022). Available at: https://theconversation.com/what-is-the-best-mask-for-covid-19-a-mechanical-engineer-explains-the-science-after-2-years-of-testing-masks-in-his-lab-175481 (Accessed 15 February 2023).
- MacIntyre, R. “The fuss about facemasks”. In: Dark Winter. An insider’s guide to pandemics and biosecurity. Sydney, NSW, Australia: UNSW Press (2022). p. 170-88.
- World Bank. Poverty and Shared Prosperity 2022: Correcting Course. Washington, DC, USA: World Bank (2022). [CrossRef]
- Lei H, Xu M, Wang X, Xie Y, Du X, Chen T, et al. Nonpharmaceutical interventions used to control COVID-19 reduced seasonal influenza transmission in China. J Infect Dis (2020) 222(11):1780-3. [CrossRef]
- State Government of Victoria Department of Health and Human Services. Victorian Weekly Influenza Report Week ending: 8 August 2020. Melbourne, Victoria, Australia: State Government of Victoria (2020). Available at: https://content.health.vic.gov.au/sites/default/files/migrated/files/collections/research-and-reports/s/seasonal-influenza-reports/2020/2020-weekly-influenza-surveillance-report-week-ending-8-august.pdf (Accessed 13 February 2023).
- Australian Government Department of Health and Aged Care. Australian Influenza Surveillance Report, No 14, 9 October, Reporting fortnight: 26 September to 09 October 2022. Canberra, ACT, Australia: Government of Australia, (2022). Available at: https://www.health.gov.au/sites/default/files/documents/2022/10/aisr-fortnightly-report-no-14-26-september-to-9-october-2022.pdf (Accessed 22 March 2023).
- Trent MJ, Moa A, MacIntyre CR. “I’ll be back”: Australia’s experience of flu in 2022. BMJ (2022) 379:o2998. [CrossRef]
- Morawska L, Milton DK. It is time to address airborne transmission of coronavirus disease 2019 (COVID-19). Clin Infect Dis (2020) 71(9):2311-3. [CrossRef]
- Australian Bureau of Statistics (ABS). COVID-19 Mortality in Australia: Deaths registered until 28 February 2023. Australian Bureau of Statistics (2023). Available at: https://www.abs.gov.au/articles/covid-19-mortality-australia-deaths-registered-until-28-february-2023 (Accessed 15 June 2023).
- COVID-19 Actuaries Institute Mortality Working Group. COVID-19 Mortality Working Group Confirmation of 20,000 excess deaths for 2022 in Australia (2023). Available at: https://www.actuaries.digital/2023/04/06/covid-19-mortality-working-group-confirmation-of-20000-excess-deaths-for-2022-in-australia/ (Accessed 15 June 2023).
- Mullins A, host. The scientific reality of COVID-19 for all Australians. Uncommon Sense Podcast. 6 December 2022. Available at: https://www.rrr.org.au/explore/podcasts/uncommon-sense/episodes/6333-professor-brendan-crabb-on-the-scientific-reality-of-covid-19-for-all-australians (Accessed 13 February 2023).
- Burnet Institute. COVID isolation rule change ‘disappointing’. Burnet Institute News. Melbourne, Victoria, Australia: Burnet Institute (2022). Available at: https://burnet.edu.au/news/1677_covid_isolation_rule_change_disappointing (Accessed 13 February 2023).
- Office of the Prime Minister of Australia. Media Release on National Cabinet Meeting of 30 September 2022: COVID-19. Canberra, ACT, Australia: Commonwealth Government of Australia. 30 September 2022. Available at: https://www.pm.gov.au/media/meeting-national-cabinet-1 (Accessed 13 February 2023).
- Grafton RQ, Chu L, Kompas T, McLaws M-L, Suan D. Long COVID in Australia: Evidence and Key Findings, Inquiry into Long COVID and Repeated COVID Infections. Inquiry into Long COVID and Repeated COVID Infections. Submission 208: Australian Parliament House (2022). Available at: https://www.aph.gov.au/DocumentStore.ashx?id=17f15f1d-a2f0-4fae-bd9d-85a0918ee6ac&subId=725489 (Accessed 26 January 2023).
- Biddle N, Korda R. The experience of COVID-19 in Australia, including long-COVID – Evidence from the COVID-19 Impact Monitoring Survey Series. Centre for Social Research & Methods, ANU College of Arts & Social Sciences, Australian National University, (2022). Available at: https://csrm.cass.anu.edu.au/research/publications/experience-covid-19-australia-including-long-covid-evidence-covid-19-impact (Accessed 28 January 2023).
- Altmann DM, Whettlock EM, Liu S, Arachchillage DJ, Boyton RJ. The immunology of long COVID. Nat Rev Immunol (2023). [CrossRef]
- Rong Z, Mai H, Kapoor S, Puelles V, Czogalla J, Schädler J, et al. SARS-CoV-2 spike protein accumulation in the skull-meninges-brain axis: Potential implications for long-term neurological complications in post-COVID-19. bioRxiv (2023):2023.04.04.535604. [CrossRef]
- Hyndman, RJ. We need more open data in Australia (2022). Available at: https://robjhyndman.com/hyndsight/open-data.html (Accessed 1 March 2023).
- Briggs, C.; Australian governments have kept much of their COVID research and modelling secret. Why? ABC News. 7 January 2023. Available at: https://www.abc.net.au/news/2023-01-07/covid-data-government-secrecy/101827548 (Accessed 29 January 2023).
- MacIntyre, R. “Trust me, I’m a doctor”. In: Dark Winter. An insider’s guide to pandemics and biosecurity. Sydney, NSW, Australia: UNSW Press (2022). p. 138-51.
- MacIntyre, R. “Information warfare”. In: Dark Winter. An insider’s guide to pandemics and biosecurity. Sydney, NSW, Australia: UNSW Press (2022). p. 117-37.
- Mullins A, host. Listen to Epidemiologist Mary-Louise McLaws on how to fix Australia’s vaccine rollout. Uncommon Sense Podcast. 20 April 2021. Available at: https://www.rrr.org.au/explore/podcasts/uncommon-sense/episodes/5107-epidemiologist-mary-louise-mclaws-on-how-to-fix-australias-vaccine-rollout-wild-mushrooming-with-alison-pouliot-the-rediscovery-of-a-rare-cloaked-bee (Accessed 2 July 2023).
- ABC News. Epidemiologist says COVID-19 testing is an ‘enormous problem’. ABC News. 2 January 2022. Available at: https://www.youtube.com/watch?v=GV3i7vN8vXM&ab_channel=ABCNews(Australia) (Accessed 2 July 2023).
- Hayes, P. What is the new national definition of a COVID close contact? News GP: The Royal Australian College of General Practitioners (RACGP) (2021). Available at: https://www1.racgp.org.au/newsgp/clinical/new-national-definition-of-covid-close-contact (Accessed 2 July 2023).
- Therapeutic Goods Administration (TGA). COVID-19 rapid antigen self-tests that are approved in Australia. Australian Government, Department of Health and Aged Care (2023) [updated 17 March 2023]. Available at: https://www.tga.gov.au/products/covid-19/covid-19-tests/covid-19-rapid-antigen-self-tests-home-use/covid-19-rapid-antigen-self-tests-are-approved-australia (Accessed 26 March 2023).
- Vicziany M, Hardikar J. Can self-administered rapid antigen tests (RATs) help rural India? An evaluation of the CoviSelf kit as a response to the 2019-2022 COVID-19 pandemic. Diagnostics (2022) 12(3):644. [CrossRef]
- Royal College of Pathologists of Australia (RCPA). Position Statement: COVID-19 antigen and point of care testing. Surry Hills, New South Wales, Australia: Royal College of Pathologists of Australia. July 2022. Available at: https://www.rcpa.edu.au/getattachment/dde91525-d128-4f0a-ba47-ddea400c061b/COVID-19-Antigen-and-Point-of-Care-Testing.aspx (Accessed 27 February 2023).
- MacIntyre, R. “Epidemic detectives”. In: Dark Winter. An insider’s guide to pandemics and biosecurity. Sydney, NSW, Australia: UNSW Press (2022). p. 152-69.
- The Sydney Morning Herald. Effects of the Epidemic. The Sydney Morning Herald. 25 June 1919. Available at: https://www.newspapers.com/clip/59130451/para-4-of-25619-p-12/ (Accessed 2 April 2023).
- New South Wales Metropolitan Citizens’ Influenza Administrative Committee & New South Wales Parliament Legislative Assembly. Outbreak of pneumonic influenza in New South Wales in 1919: Report. Sydney, New South Wales, Australia: Legislative Assembly (1920). Available at: https://nla.gov.au/nla.cat-vn2062179 (Accessed 4 April 2023).
- The Sydney Morning Herald. Effects of the Epidemic. The Sydney Morning Herald. 25 June 1919. p. 12 para.5. Available at: https://www.newspapers.com/clip/59130483/para-5-of-25619-p-12/ (Accessed 2 April 2023).
- The Sydney Morning Herald. Page 1 Summary. The Sydney Morning Herald. 23 June 1919. p. 1. Available at: https://www.newspapers.com/clip/59170828/from-page-1-summary-not-picked-up-in/ (Accessed 2 April 2023).
- Caley P, Philp DJ, McCracken K. Quantifying social distancing arising from pandemic influenza. J R Soc Interface (2008) 5(23):631-9. [CrossRef]
- Foley, PB. Encephalitis lethargica and the influenza virus. II. The influenza pandemic of 1918/19 and encephalitis lethargica: epidemiology and symptoms. J Neural Transm (2009) 116(10):1295-308. 1295. [Google Scholar] [CrossRef]
- Cumpston JHL. Influenza and maritime quarantine in Australia. Commonwealth of Australia Quarantine Service Publication. Melbourne, Victoria, Australia: Commonwealth of Australia Quarantine Service (1919). Available at: https://nla.gov.au/nla.obj-192064587 (Accessed 17 June 2023).
- State Government of Victoria Department of Health and Human Services. Coronavirus update for Victoria - 30 September 2020. Melbourne, Victoria, Australia: State Government of Victoria (2020). Available at: https://www.dhhs.vic.gov.au/coronavirus-update-victoria-30-september-2020 (Accessed 17 June 2023).
- South Eastern Melbourne Primary Health Network (SEMPHN). South Eastern Melbourne COVID-19 primary care management. Heatherton, Victoria, Australia: South Eastern Melbourne PHN (2020). Available at: www.semphn.org.au/SEMPHN_GP_managment_of_COVID_ve_patients_Pathways_14092020_.pdf (Accessed 9 September 2020).
- Royal Commission into Aged Care Quality and Safety. Aged care and COVID-19: A special report: Commonwealth of Australia (2020). Available at: https://agedcare.royalcommission.gov.au/sites/default/files/2020-12/aged-care-and-covid-19-a-special-report.pdf (Accessed 4 February 2023).
- ABC News. Victorian coronavirus outbreaks in aged care homes swell as St Basil’s in Melbourne evacuated. ABC News. 31 July 2020. Available at: https://www.abc.net.au/news/2020-07-31/victorian-coronavirus-outbreaks-aged-care-homes-st-basils/12513668 (Accessed 28 February 2023).
- Handley, E. Why are there are more COVID-19 cases in private aged care than the public sector? ABC News. 1 August 2020. Available at: https://www.abc.net.au/news/2020-08-01/why-more-covid-19-cases-in-private-aged-care-than-public-sector/12503212 (Accessed 1 August 2020).
- Lunn S, Baxendale RL. Grim toll as unskilled staff put aged-aged homes at risk. The Australian. 24 July 2020. Available at: https://www.theaustralian.com.au/nation/politics/grim-toll-as-unskilled-staff-put-melbourne-agedcare-homes-at-risk/news-story/863182db7610ba22d304f82fec3cd30a (Accessed 30 March 2023).
- The Weekly Source. Department of Health extends Victorian ban on aged care staff working across multiple sites until October – but DHHS says some workers still at more than one facility. The Weekly Source. 20 September 2020. Available at: https://www.theweeklysource.com.au/department-of-health-extends-victorian-ban-on-aged-care-staff-working-across-multiple-sites-until-october-but-dhhs-says-some-workers-still-at-more-than-one-facility/ (Accessed 28 February 2023).
- Clayton R, Murray-Atfield Y. Fair Work Commission awards paid pandemic leave to aged care workers to stop staff going to work sick. ABC News. 27 July 2020. Available at: https://www.abc.net.au/news/2020-07-27/aged-care-workers-get-paid-pandemic-leave-fair-work-commission/12496342 (Accessed 28 February 2023).
- Davern M, McLaws M-L, Gudes O. Mapping COVID-19 spread in Melbourne shows link to job types and ability to stay home. The Conversation (2020). Available at: https://theconversation.com/mapping-covid-19-spread-in-melbourne-shows-link-to-job-types-and-ability-to-stay-home-143610 (Accessed 9 July 2023).
- Parliament of Victoria Public Accounts and Estimates Committee. Inquiry into the Victorian Government’s response to the COVID-19 pandemic. Chapter 6: Jobs and industry. Melbourne, Victoria, Australia: Victorian Government Printer (2021). p. 115-36. Available at: https://new.parliament.vic.gov.au/49706e/contentassets/9c4e489fe9834121826347ad523e87d2/paec_59-08_vic_gov_response_to_covid-19_pandemic.pdf (Accessed 28 June 2023).
- Piketty, T. Capital in the Twenty-First Century. Cambridge, MA, USA & London, England: Harvard University Press (2014). [CrossRef]
- Roder C, Maggs C, McNamara BJ, O’Brien D, Wade AJ, Bennett C, et al. Area-level social and economic factors and the local incidence of SARS-CoV-2 infections in Victoria during 2020. Med J Aust (2022) 216(7):349-56. [CrossRef]
- Belling N, host. The worst public health disaster in living memory... Why we need to talk about COVID. Australia Today’s Morning Agenda with Natarsha Belling Podcast. 19 December 2022. Available at: https://omny.fm/shows/your-morning-agenda-with-natarsha-belling-1/the-worst-public-health-disaster-in-living-memory (Accessed 1 January 2023).
Figure 1.
(A) Weekly hospital admissions and deaths in Sydney (1919) and Melbourne (2020) for weeks ending 1 February to 30 September Sources: NSW Department of Health, Report on the Influenza Epidemic in New South Wales in 1919, Government Printer, Sydney, 1920, Table 1 on hospital admissions p.147 and table on deaths p.174; Datasheets from Victoria’s DHHS, Melbourne Public Health Events Surveillance System, Notifiable Conditions dataset for COVID-19, received 1 October 2020. (B)Weekly hospital admissions and deaths per 100,000 population in Sydney (1919) and Melbourne (2020) for weeks ending 1 February to 30 September. Sources: NSW Department of Health, Report on the Influenza Epidemic in New South Wales in 1919, Government Printer, Sydney, 1920, Table 1 on Admissions p.147 and table on deaths p.174; Datasheets from Victoria’s DHHS, Melbourne Public Health Events Surveillance System, Notifiable Conditions dataset for COVID-19, received 1 October 2020.
Figure 1.
(A) Weekly hospital admissions and deaths in Sydney (1919) and Melbourne (2020) for weeks ending 1 February to 30 September Sources: NSW Department of Health, Report on the Influenza Epidemic in New South Wales in 1919, Government Printer, Sydney, 1920, Table 1 on hospital admissions p.147 and table on deaths p.174; Datasheets from Victoria’s DHHS, Melbourne Public Health Events Surveillance System, Notifiable Conditions dataset for COVID-19, received 1 October 2020. (B)Weekly hospital admissions and deaths per 100,000 population in Sydney (1919) and Melbourne (2020) for weeks ending 1 February to 30 September. Sources: NSW Department of Health, Report on the Influenza Epidemic in New South Wales in 1919, Government Printer, Sydney, 1920, Table 1 on Admissions p.147 and table on deaths p.174; Datasheets from Victoria’s DHHS, Melbourne Public Health Events Surveillance System, Notifiable Conditions dataset for COVID-19, received 1 October 2020.
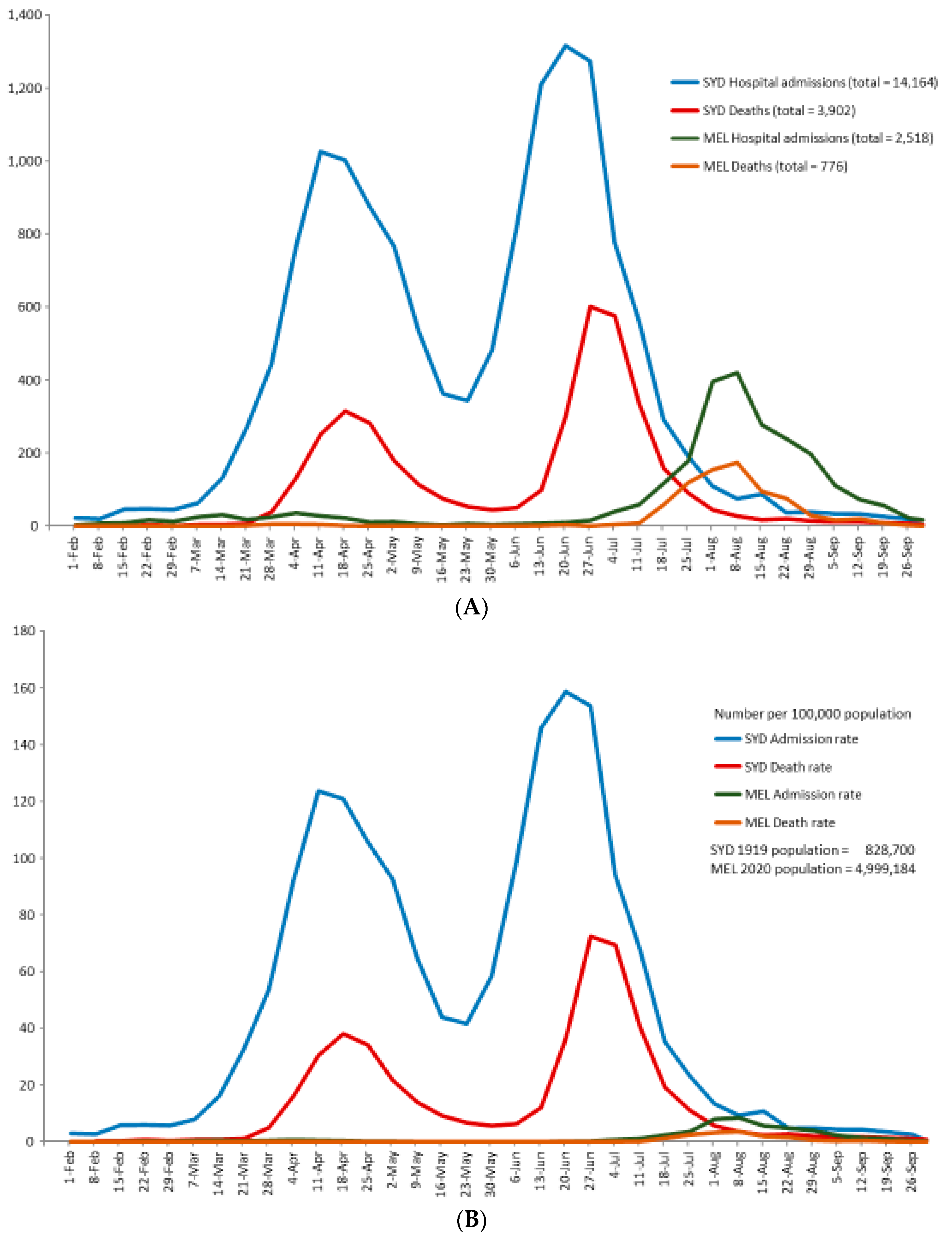
Figure 2.
Cumulative weekly hospital admissions per 100,000 population (log scale) in Sydney (1919) and Melbourne (2020) for weeks ending 1 February to 30 September. Sources: NSW Department of Health, Report on the Influenza Epidemic in New South Wales in 1919, Government Printer, Sydney, 1920, Table 1 on hospital admissions p.147; Datasheets from Victoria’s DHHS, Melbourne Public Health Events Surveillance System, Notifiable Conditions dataset for COVID-19, received 1 October 2020.
Figure 2.
Cumulative weekly hospital admissions per 100,000 population (log scale) in Sydney (1919) and Melbourne (2020) for weeks ending 1 February to 30 September. Sources: NSW Department of Health, Report on the Influenza Epidemic in New South Wales in 1919, Government Printer, Sydney, 1920, Table 1 on hospital admissions p.147; Datasheets from Victoria’s DHHS, Melbourne Public Health Events Surveillance System, Notifiable Conditions dataset for COVID-19, received 1 October 2020.
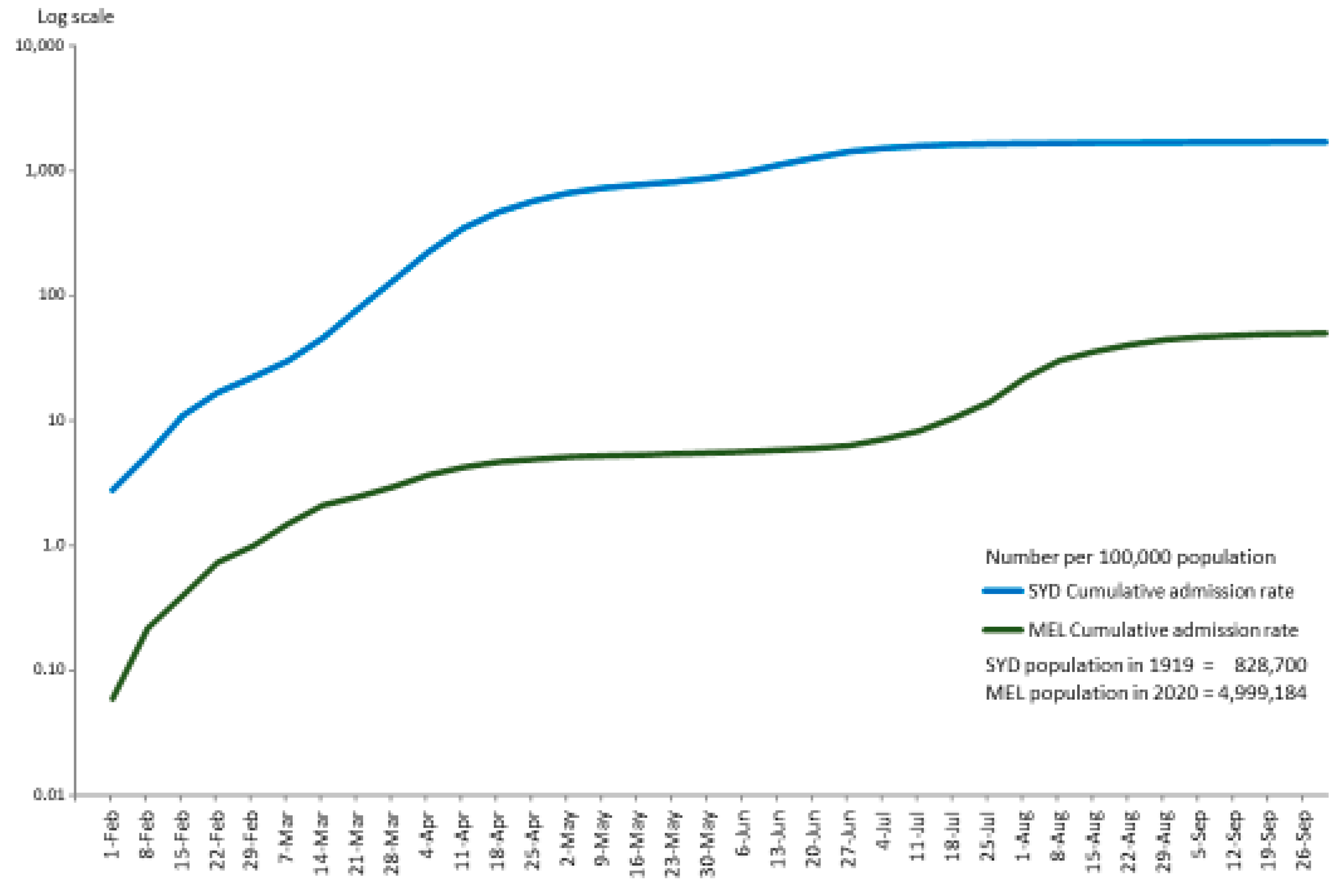
Figure 3.
Cumulative weekly deaths per 100,000 population (log scale) in Sydney (1919) and Melbourne (2020) for weeks ending 1 February to 30 September. Sources: NSW Department of Health, Report on the Influenza Epidemic in New South Wales in 1919, Government Printer, Sydney, 1920, table p.174 on deaths; Datasheets from Victoria’s DHHS, Melbourne Public Health Events Surveillance System, Notifiable Conditions dataset for COVID-19, received 1 October 2020.
Figure 3.
Cumulative weekly deaths per 100,000 population (log scale) in Sydney (1919) and Melbourne (2020) for weeks ending 1 February to 30 September. Sources: NSW Department of Health, Report on the Influenza Epidemic in New South Wales in 1919, Government Printer, Sydney, 1920, table p.174 on deaths; Datasheets from Victoria’s DHHS, Melbourne Public Health Events Surveillance System, Notifiable Conditions dataset for COVID-19, received 1 October 2020.
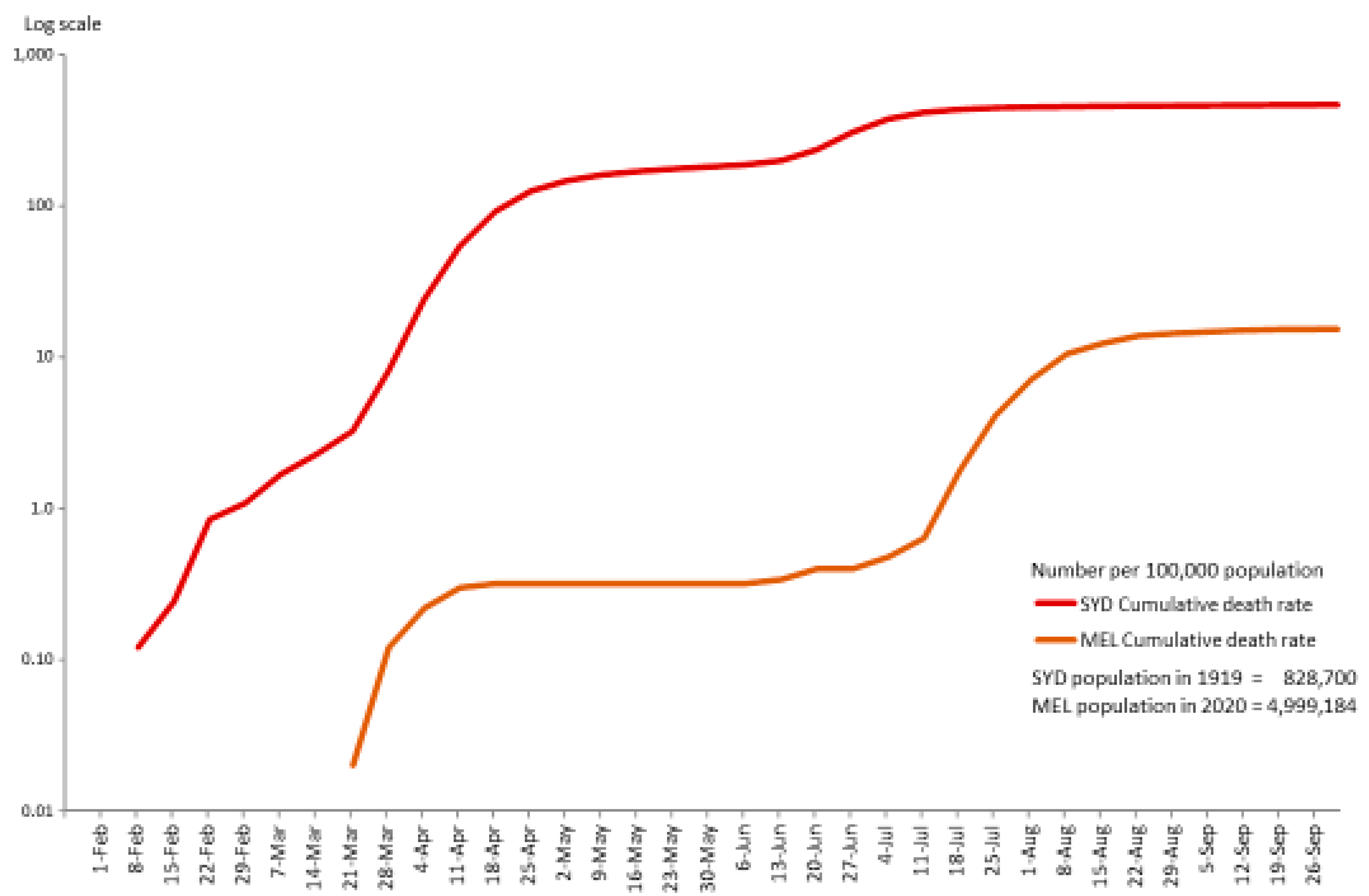
Figure 4.
Weekly number of COVID-19 cases, hospital and ICU admissions and deaths in Melbourne for weeks ending 1 February to 30 September 2020. Source: Datasheets from Victoria’s DHHS, Melbourne Public Health Events Surveillance System, Notifiable Conditions dataset for COVID-19, received 1 October 2020.
Figure 4.
Weekly number of COVID-19 cases, hospital and ICU admissions and deaths in Melbourne for weeks ending 1 February to 30 September 2020. Source: Datasheets from Victoria’s DHHS, Melbourne Public Health Events Surveillance System, Notifiable Conditions dataset for COVID-19, received 1 October 2020.
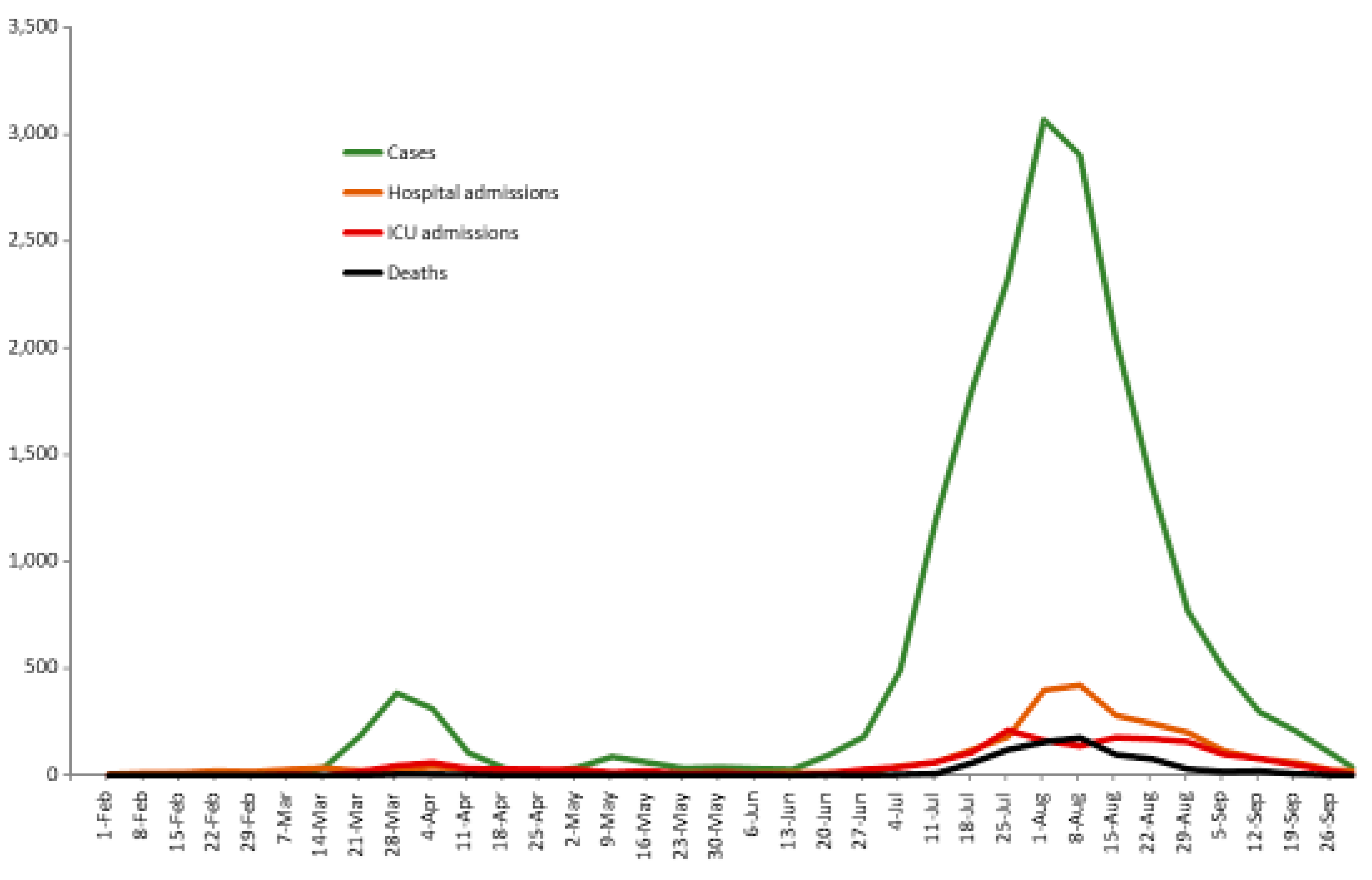

Table 1.
Identifying the epicentres in Australia for the Spanish Flu in 1919 and COVID-19 in 2020.
| Spanish Flu 1919 | COVID-19 2020 | |||||
|---|---|---|---|---|---|---|
| Australia | Sydney | Melbourne | Australia | Sydney | Melbourne | |
| Population (11,14,15) | 5,217,019 | 828,700 | 743,000 | 25,364,300. | 5,312,163 | 5,078,193 |
| % Capital city population in national population | 100 | 15.9 | 14.2 | 100 | 20.9 | 20.0 |
| % Capital city population in total state population | 41.4 | 49.7 | 65.7 | 77.0 | ||
| Number of deaths (11,12,16) | 11,552 a | 3,902 b | 2,391 a | 909 a | 54 ac | 820 ac |
| % of national deaths | 100 | 33.8 | 20.7 | 100 | 5.9 | 90.2 |
| Crude Death Rate per 100,000 population | 221 | 471 | 322 | 3.6 | 1.0 | 16.1 |
a total number of deaths for the whole calendar year. b number of deaths for the period from 1 January to 30 September 1919. C number of deaths in New South Wales and Victoria as proxies for Sydney and Melbourne respectively.
Table 2.
Stages of the 1919 and 2020 pandemics based on the frequency of zero, single-, double- and triple-digit weekly deaths from weeks ending 1 February to 30 September a (12, 20).
Table 2.
Stages of the 1919 and 2020 pandemics based on the frequency of zero, single-, double- and triple-digit weekly deaths from weeks ending 1 February to 30 September a (12, 20).
| SYDNEY | MELBOURNE | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Stages | Weekly deaths | Number of weeks | Week ending dates | % of 35.5 weeks | Stages | Weekly deaths | Number of weeks | Week ending dates | % of 35.5 weeks |
| Stage 1 | Zero & Single digits | 8 | 1 Feb – 21 Mar | 23% | Stage 1 | Zero | 7 | 1 Feb – 14 Mar | 20% |
| Stage 2 | Double digits | 1 | 28 Mar | 3% | Stage 2 | Zero & single digits | 17[including 8 zero weeks] | 21 Mar – 11 Jul | 48% [22%] |
| Stage 3 | Triple digits | 6 | 4 Apr – 9 May | 17% | Stage 3 | Double digits | 1 | 18 Jul | 3% |
| Stage 4 | Double digits | 5 | 16 May – 13 Jun | 14% | Stage 4 | Triple digits | 3 | 25 Jul – 8 Aug | 8% |
| Stage 5 | Triple digits | 5 | 20 Jun – 18 Jul | 14% | Stage 5 | Double digits | 5 | 15 Aug – 12 Sep | 14% |
| Stage 6 | Double digits | 9 | 25 Jul – 19 Sep | 25% | Stage 6 | Single digits | 2.5 | 19 Sep – 30 Sep | 7% |
| Stage 7 | Single digits | 1.5 | 26 Sep – 30 Sep | 4% | |||||
| TOTAL 35.5 weeks | 100% | TOTAL 35.5 weeks | 100% | ||||||
a The week ending dates are adjusted reporting dates for deaths (see explanation in ‘Materials and Methods’).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



