
Submitted:
27 December 2023
Posted:
28 December 2023
You are already at the latest version
Abstract
Breast and prostate cancer lead incidence rankings in Chile, with obesity and overweight as important risk factors involved in prognosis. Nutritional interventions have shown to be beneficial therapies in patients with cancer, improving anthropometric and biochemical measurements. This study investigates the feasibility and effectiveness of Calorie Restriction and Time-Restricted Feeding in overweight or obese patients undergoing curative radiotherapy for breast and prostate cancer. The research was conducted as a prospective, interventional, non-randomized clinical trial, involving 27 participants, of whom 23 completed the study. Findings indicate that both interventions are feasible and effective. Notably, Time-Restricted Feeding demonstrated superior adherence and more significant improvements in weight loss and metabolic parameters. A mean weight reduction of 3.6 kg and waist circumference decrease of 4.9 cm was observed across participants. Serum levels of glucose, insulin, LDL, HDL and TG showed an average reduction, indicating positive metabolic changes. Results suggest that Time-Restricted Feeding could be a superior beneficial dietary intervention for cancer patients undergoing radiotherapy, due to its ease of adherence and positive impact on metabolic health. This research contributes to the growing evidence on the role of nutritional interventions in cancer treatment and underscores the need for more extensive studies to validate these findings.
Keywords:
Intermittent Fasting
; Cancer
; Curative
; Radiotherapy
; Calorie Restriction
; Time-Restricted Feeding
; Diet
; Nutrition
; Overweight
; Obese
1. Introduction
In the last decade, cancer and cardiovascular diseases have established themselves as the first cause of morbidity and mortality collectively, with over 18 million new cases of cancer being registered only in 2020 [1]. These pathologies share common risk factors such as sedentary lifestyle, poor diet, obesity, tobacco and alcohol consumption [2]. Notably, overweight and obesity are modifiable risk factors present in 74.2% of the Chilean population [3], and are particularly impactful due to their implication in the origin of various types of cancer [4]. Breast cancer and prostate cancer are of significant interest as they lead the incidence of new cancer cases among Chilean women and men, respectively [1].
Due to the implication of weight and nutrition in incidence and prognosis in cancer [5,6,7], numerous nutritional interventions such as Calorie Restriction (CR), Ketogenic Diet (KD) [8] and Intermittent Fasting (IF) (defined in Table 1), have been investigated to elucidate their impact as beneficial therapies in cancer [9]. IF is one of the most frequently cited diet patterns in 2023 among Americans aged 18 to 80 years according to the International Food Information Council survey [10]. CR is frequently applied in overweight people and, despite showing great results when applied in short-term duration (< 6 months), it tends to have a lot of difficulties with adherence when following it for extended periods of time [11].
The pathophysiological reasoning behind the effectiveness of these nutritional interventions has long been researched and explained [16,17,18]. There are preclinical studies that establish the impact from IF and CR on glucose regulation, resistance to stress and inflammation suppression [19]. Despite showing promising results in regression of tumor volume and radiosensitivity of tumors in mice preclinical models [20,21,22,23], clinical trials are a must to determine the effect of these interventions on patients with cancer [24]. Unfortunately, available evidence on this matter is lacking and even international guidelines (ACS, NCCN, ESPEN or ASCO) don’t have a conclusive stance on their application [25,26,27,28].
The recommendations from these guidelines on breast and prostate cancer were reviewed and summarized in Table 2.
A 2020 literature review [29] found 9 clinical trials which focused on radiotherapy and a KD. These studies suggested that KD may have a beneficial effect, but the small numbers of patients in these cohorts, absence of control groups, and in 3 studies KD not being the only variable associated with response to RT, prevented them from drawing definitive conclusions.
A recent paper from June 2023 by Kalam et al. [30] synthesized results from 23 studies dating 2020 onwards where various methods of IF were used. Studies involving IF found rates of severe toxicity decreased. Those combining fasting and KD found it was well tolerated and decreased toxicity. Others investigating Fasting-mimicking Diets, a low-calorie diet that is low in protein and carbohydrates but high in unsaturated fat, found it increased ketone bodies and improved plasma glucose, but had variable compliance and conflict of interest. Lastly, TRF showed the highest degree of adherence, and helped decrease fatigue, improved visceral adipose tissue, whole-body fat mass, cardiometabolic outcomes, anxiety, and depression.
A systematic review on the impact of IF on breast cancer from January 2023 by Anemoulis et al. [31] which included studies from 2009 to 2021, failed to conclude there were beneficial effects from IF on Quality of Life (QoL), response after chemotherapy or an improvement on symptoms. They did, however, find that there could be a beneficial effect on chemotherapy related adverse effects based on markers of DNA and leukocyte damage but require further validation.
The lack of evidence in this area of research and variety of nutritional interventions make it so that it is often overseen and difficult to gauge their real impact. Important international guidelines published in 2021 and 2022, such as ACS and NCCN, have no dedicated space for IF, TRF or CR in the entirety of their guidelines, whereas ESPEN or ASCO group it together with other recommendations that, while they may have in common the modification of food intake, have different objectives and ways to implement.
In practice, many patients show interest in a dietary modification that could increase their chances of success in treatment. A recent study evaluating CR and radiotherapy in breast cancer patients found that up to 75% would be part of a CR study [32]. However, adherence to dietary interventions is variable, and can be explained by several reasons such as: depression, stress, previous weight loss attempts or negative perceptions of diet and exercise [33,34]. On the other hand, regular and frequent attendance at nutritional controls, physical exercise, educational materials and feeling control over what they eat are factors that favor adherence [35,36].
A prospective, interventional, non-randomized clinical trial was built. It assesses the feasibility and effectiveness of CR and TRF in patients with breast or prostate cancer, overweight or obese, undergoing curative radiotherapy. CR and TRF were chosen due to their history, ease of application and as previously exposed, supporting evidence in their favor.
The main objective of this clinical trial is to evaluate the feasibility and effectiveness of either CR or TRF in prostate and breast cancer patients who are under curative radiotherapy treatment.
In this novelty clinical trial we seek to establish guidelines for future works in this area which can be easily reproducible and improved upon, and thus build the foundations for effective and efficient interventions such as TRF or CR.
To our knowledge it is the first published work of this kind in developing countries, and showed consistent results in favor of the intervention.
2. Materials and Methods
We defined a prospective, interventional, non-randomized clinical trial that assesses the feasibility and effectiveness of CR and TRF in patients with breast or prostate cancer, body mass index (BMI) >25 and treated with curative radiotherapy. A summary of the main characteristics of the cohort can be found in Table 3.
Inclusion criteria:
- ≥18 years old
- Breast cancer or hormone-sensitive prostate cancer diagnosed by biopsy
- Overweight or obesity defined as BMI ≥ 25 kg/m2 and 30 kg/m2 respectively
- Indication of radiotherapy with a curative intent.
Exclusion criteria:
- BMI < 25 kg/m2
- Patients undergoing nutritional treatment or malnutrition
- Patients with diabetes mellitus using insulin
- Diagnosis of vascular ischemia, uncontrolled thyroid disease, mental illness without medical supervision, liver disease or malabsorption syndromes (inflammatory bowel disease, celiac disease)
- Patients with gastric by-pass or gastric sleeve
- Use of corticosteroids or anti-depressants
- Moderate or high level of physical activity.
If the patient was a suitable candidate, during the initial consultation the details of the study along with its risks and benefits were explained. Patients who accepted to be part of the study signed an informed consent and were distributed between CR and IF according to their preferences.
The following steps were taken with each patient to ensure a thorough procedure:
Step 1: Initial Evaluation
- A.
- Nutritional evaluation: baseline measurement of weight, BMI, waist circumference, along with serum levels of glucose, basal insulin and lipid were performed.
- B.
- Quality of life (QoL): QoL was assessed through the EORTC-c30 questionnaire with all patients, and additionally the EORTC QLQ - BR23 questionnaire in breast cancer and the Expanded Prostate Cancer Index Composite (EPIC 2.0) in prostate cancer, if appropriate, which were taken at the same time as the EORTC-30.
- C.
- Physical activity: international physical activity questionnaire (IPAQ) from the World Health Organization (WHO).
- D.
- Eating habits: a 24-hour food survey and consumption trend was used to determine the patient’s eating habits (Supplementary Material, “Supplementary Spreadsheet 1”).
Step 2: Intervention
Each intervention was defined to start 2 weeks before the patient’s oncologic treatment, and last for 12 weeks.
Once nutritional evaluation was done, participants were then assigned to TRF or CR according to their preferences. Patient distribution can be seen in Figure 1.
Nutritional guidelines were made and personalized for each patient according to their group, following certain rules:
- A.
- The TRF group had a sugar and saturated fat free diet with caloric intake according to the patient's total energy expenditure, distributed in 8 hours of food intake and 16-hour daily fast.
- B.
- The CR group was based on the Obesity Society guidelines, with a total caloric intake 25% less than total energy expenditure. This was distributed in 4 meals and 1 snack according to the following proportions: 55% for carbohydrates, 15% protein and 30% fat, without sugar or saturated fat.
- C.
- Every patient, independent of their group, was tasked with a dairy registry of what they ate.
Step 3: Monitoring
Throughout the investigation, the following parameters were closely monitored:
- A.
- Treatment adherence: patients were called once a week and their dairy diet registry was evaluated according to their corresponding group, where important concepts related to their intervention were reinforced.
- B.
- Anthropometric changes: every 4 weeks every patient’s weight and waist circumference were measured.
- C.
- Toxicity: once a week during their consultation with radiation oncology, acute toxicity was assessed using the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE).
Step 4: Final Evaluation
12 weeks after having started the intervention, and at least 4 weeks after finishing oncologic treatment, the following were measured:
- A.
- Acute Toxicity
- B.
- Weight and waist circumference
- C.
- Fasting glucose, basal insulin and lipid profile.
- D.
- QoL with EORTC-c30, EORTC QLQ - BR23 (for breast cancer) and the EPIC 2.0 (for prostate cancer)
3. Hypothesis
CR or TRF are feasible and effective interventions in overweight and obese patients with breast or prostate cancer undergoing curative radiotherapy.
4. Primary objectives
Evaluate feasibility and effectiveness of CR and TRF in overweight and obese patients with cancer under curative radiotherapy.
5. Secondary Objectives
- A.
- Assess adherence, defined as a reduction in body weight of at least 5% compared to baseline and in at least 50% of the recruited patients.
- B.
- Establish which intervention (CR or TRF) has better adherence.
- C.
- Assess the impact on quality of life in patients under nutritional interventions
- D.
- Assess differences in weight and waist circumference in patients under nutritional interventions
- E.
- Assess differences in serum levels of fasting glucose, basal insulin and lipid profile in patients under nutritional interventions
- F.
- Assess acute toxicity grade ≥2 in patients under nutritional interventions
6. Results
27 patients were recruited from April 2021 to May 2023. Two patients withdrew from the trial before treatment and one patient did not receive radiotherapy (as seen in Figure 2). At the end of May 2023, 23 patients had completed 12 weeks of follow up of which 21 were women and 2 were men.
Of the 24 patients available for analysis, 22 were women with breast cancer with luminal ductal carcinoma being the most common histologic subtype. From the 22 women with breast cancer, 14 received some kind of chemotherapy (neoadjuvant, adjuvant or both), and 19 received endocrine therapy. All 22 patients underwent whole breast radiotherapy (+-regional nodal irradiation) and 11 received simultaneous integrated boost to the tumor bed up to 45,75 Gy.
Of the 24 patients available for analysis, 2 were men with prostate cancer and a Gleason score of 6 and 7. Both of them underwent surgery and had initiated androgen deprivation therapy. They received a dose of 51 Gy in 17 fractions to the prostate bed or equivalent EQD2.
Table 4 provides detailed clinical characteristics of patients separated by intervention, along with changes in biochemical and anthropometric measures before and after the intervention.
Notable results before and after the intervention are as following:
- A.
- There was a reported loss of 5% or more of the initial weight in 52,1% of patients (12/23).
- B.
- Within the patients with breast cancer, 100% of those who chose TRF showed true adherence (5 out of 5), whereas only 43.75% (7 out of 16) showed true adherence in the CR group.
- C.
- Within the patients with prostate cancer, 0% showed true adherence in the TRF group (0 out of 2).
- D.
- There was a mean reduction in weight of 3.6 kg and waist circumference of 4.9 cm.
- E.
- Serum levels of glucose, insulin, LDL, HDL and TG showed a mean reduction of 0.6 mg/dL, 2.0 uU/mL, 8.1 mg/dL, 0.4 mg/dL and 12.4 mg/dL respectively (Figure 3).
Differences between interventions are as following (as seen in Table 5, and better visualized in Figure 4):
- A.
- Anthropometric measures: patients in the TRF group lost 61.8 % more weight and reduced their waist circumference by 49.5% more in comparison to those in the CR group (6.50% and 6.52% vs 3.87% and 4.26%, respectively).
- B.
- Glucose and insulin: TRF showed a reduction 38% smaller than the CR group in mean serum glucose levels (0.57 vs 0.92), but a 270% bigger decrease in their mean serum insulin level, in comparison to the CR group (3.65 vs 0.99).
- C.
- LDL and HDL: in mean serum levels of LDL, the TRF group showed an increase of 3.9%, whereas the CR group showed a decrease of 11.14%. On the other hand, the TRF group showed an increase of 0.88% in their mean serum levels of HDL, whereas the CR group showed a reduction of 2.57%.
- D.
- TG: the TRF group showed a decrease in their TG mean serum levels 1900% higher than those in the CR group (21.16% vs 0.97% reduction, respectively).
- E.
- Adherence: of the 12 patients who showed true adherence, all 12 were women. 5 were on the TRF group (5 out of 7 patients in the TRF group) and 7 were on the CR group (7 out of 16 patients in the CR group). None of the men showed true adherence.
7. Discussion
Our findings show that 52.1% of patients lost 5% or more of the initial weight, which shows that a nutrition intervention of these characteristics is not only feasible and attains true adherence from participants, but is also effective in reducing metabolic parameters in a short period of time (12 weeks).
Compared with other publications, our results are consistent with the available literature. TRF showed similar results to existing articles [30]: high degree of adherence, decrease in weight, and improvement of blood glucose and insulin levels. Our differences in the result of blood glucose levels may be explained by the low adherence of both men in the TRF group. The differences with the study from Harvie [37] may be explained due to the fact they used another approach of IF which focuses on the amount of calories consumed (2 days of 650-1000 kcal/day before chemotherapy infusion) rather than the window of time they are consumed within.
Of interest is the differences of findings with the systematic review from Anemoulis et al. [31]. This could be explained due to the type of IF approaches utilized in the studies considered, where only one of them specified the use of TRF, and the others were variations of calorie restricting approaches of IF: one included Ramadan-fasting patients, one used a FMD, while the others employed varied hours of fasting before and after chemotherapy. This reinforces the need for clear and established definitions of IF and its different approaches, and also an urgent necessity of evidence in this field.
Our findings are similar in adherence, weight loss and insulin levels in both interventions. We found that both TRF and CR managed to improve mean serum glucose, insulin, and TG levels. We also found that TRF was a vastly superior intervention in comparison to CR when it came to improving insulin and TG levels, but more research is required to further cement these findings in international literature.
Not only did these interventions as a group achieve true adherence, but 100% of the patients with breast cancer in the TRF group showed true adherence in comparison to only 43.75% adhering in the CR group, despite previous literature indicating breast cancer patients favored a CR approach [30].
We believe these findings to be due to how TRF does not restrict the amount of calories in a certain day, but rather restricts the timing of meals to 4 - 12 hours a day (8 hours in this study) and thus may be easier to carry on in cancer patients busy with the whole therapeutic process. Further research is needed on this aspect.
Despite both interventions showing positive results, it seems TRF as a nutritional intervention has both better adherence, improved anthropometric values and metabolic serum levels.
In this novel clinical trial, we propose a straightforward and easy to replicate method with which to reclute patients and further study nutritional interventions besides TRF or CR, which we believe can provide the base for future nutritional intervention studies and open a window into other aspects of nutritional interventions such as impact on toxicity reduction which, although seen in animals [38,39], has yet to be reproduced and further explored in human participants.
To our knowledge it is the first published work of this intervention in developing countries and showed consistent efficacy of the intervention.
Limitations of our work include but aren’t limited to: limited number of participants, a relatively short period of surveillance, adherence of patients to the guidelines given, the low number of prostate cancer patients in our cohort and the lack of prostate patients in the CR group, only evaluating the TRF approach of IF, and the absence of a control group.
This work could be improved by an increase in the number of participants and specifically the number of prostate patients, an increase in the time of surveillance, employing other nutritional interventions, recruiting more types of cancer patients, measuring blood levels of inflammatory response markers, recruiting only patients with cancer in early stages, having a more homogeneous cohort, the inclusion of a control group, or the incorporation of feedback from participants.
8. Conclusions
Cardiovascular diseases and cancer lead incidence and mortality rates worldwide, sharing common risk factors such as overweight and obesity. These play an important role in the origin of breast and prostate cancer, and thus different interventions have been investigated to establish a faithful and reproducible way to improve weight in cancer patients.
The theory behind the benefit of diet and weight loss in cancer has been largely studied and established in preclinical studies, but clinical studies that show these results in practice are few in between and limited in their approach. This could be attributed to the numerous interventions in existence and a lack of agreement on definitions, establishing which ones are best, and also a lack of patients on which these interventions have been measured thoroughly.
Two of these interventions are TRF and CR. These nutritional interventions were chosen due to their historical relevance and evidence supporting them. Our findings are consistent with the literature, with TRF displaying better results in terms of adherence, weight loss and metabolic parameters, whereas CR still proves to be beneficial but has worse adherence and glucose, insulin and lipid profile levels in comparison to TRF.
Differences with literature can be explained due to heterogeneity on application of IF and its different approaches, lacking a formal definition. This leads to large differences in fasting hours, number of fasting days and the existence or not of a caloric restriction.
QoL and acute toxicity were also evaluated, but are currently under analysis and will be published in another manuscript.
We propose a series of steps through which metabolic parameters, anthropometry and quality of life can be measured. These steps are simple to apply and reproducible. We hope this helps establish concrete and well established definitions of the various fasting regimes, and motivates other researchers to further investigate and build the foundation of what we believe is a low-cost and effective way to lose weight and improve metabolic parameters.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Supplementary Spreadsheet 1: 24- hour Reminder Survey.
Author Contributions
Conceptualization, Carmen Vega and Tomás Merino; Data curation, Esteban Barnafi and Nicolás Rivas; Funding acquisition, Carmen Vega; Investigation, Carmen Vega, Alejandra Parada and Nicolás Rivas; Methodology, Carmen Vega and Tomás Merino; Project administration, Carmen Vega; Resources, César Sánchez, Francisco Acevedo, Benjamin Walbaum and Tomás Merino; Supervision, Carmen Vega and Francisco Acevedo; Validation, Tomás Merino; Visualization, Esteban Barnafi; Writing – original draft, Esteban Barnafi; Writing – review & editing, Carmen Vega, Esteban Barnafi and Tomás Merino.
Funding
This research was funded by CONCURSO DE INVESTIGACIÓN PARA RESIDENTES DE POSGRADO, ESCUELA DE MEDICINA, FACULTAD DE MEDICINA, PONTIFICIA UNIVERSIDAD CATÓLICA DE CHILE.
Institutional Review Board Statement
This study was conducted with the approval of the Comité Ético Científico de Ciencias de la Salud UC (CEC-Salud UC). This Committee adheres to the ethical principles of Pontificia Universidad Católica de Chile, which considers respect for the dignity of the human person in any condition as a fundamental axis. This Committee also complies with the Good Clinical Practice Guidelines defined by the International Conference on Harmonization (GCP-ICH); and with Chilean laws 19.628; 20.120; 20.584 and 20.850 that modify the Health Code.
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study after the procedure and the steps involved were explained.
Data Availability Statement
All statements and conclusions made within this article have been made with the data and information contained within the provided supplements (tables and figures). No other data was used.
Acknowledgments
We kindly thank N.B for his relentless revisions and support during the manufacturing of this manuscript.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- The International Agency for Research on Cancer (IARC). Global Cancer Observatory. Retrieved August 10, 2023, from https://gco.iarc.fr/today/home.
- World Health Organization. (2020, December 9). The top 10 causes of death. Retrieved August 10, 2023, from https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
- Margozzini, P.; Passi, A. Encuesta Nacional de Salud, ENS 2016-2017: Un aporte a la planificación sanitaria y políticas públicas en Chile.
- World Cancer Research Fund/American Institute For Cancer Research, «Continuous Update Project Report Summary. Food, Nutrition, Physical Activity, And The Prevention Of Colorectal Cancer». 2011.
- Rock, C.L.; Thomson, C.; Gansler, T.; Gapstur, S.M.; McCullough, M.L.; Patel, A.V.; Bandrews, K.S.; Bandera, E.V.; Spees, C.K.; Robien, K.; et al. American Cancer Society guideline for diet and physical activity for cancer prevention. CA A Cancer J. Clin. 2020, 70, 245–271. [Google Scholar] [CrossRef] [PubMed]
- Protani, M.; Coory, M.; Martin, J.H. Effect of obesity on survival of women with breast cancer: Systematic review and meta-analysis. Breast Cancer Res. Treat. 2010, 123, 627–635. [Google Scholar] [CrossRef] [PubMed]
- De Cabo, R.; Mattson, M.P. Effects of intermittent fasting on health, aging, and disease. N. Engl. J. Med. 2019, 381, 2541–2551. [Google Scholar] [CrossRef] [PubMed]
- Nebeling, L.C.; Miraldi, F.; Shurin, S.B. Effects of a ketogenic diet on tumor metabolism and nutritional status in pediatric oncology patients: Two case reports. J. Am. Coll. Nutr. 1995, 14, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Tagde, P.; Tagde, S.; Bhattacharya, T.; Tagde, P.; Akter, R.; Rahman, M.H. Multifaceted effects of intermittent fasting on the treatment and prevention of diabetes, cancer, obesity or other chronic diseases. Curr. Diabetes Rev. 2022, 18, 33–49. [Google Scholar] [CrossRef] [PubMed]
- International Food Information Council. 2023 Food & Health Survey. 23 May 2023. [https://foodinsight.org/2023-food-health-survey/].
- Vasim, I.; Majeed, C.N.; DeBoer, M.D. Intermittent Fasting and Metabolic Health. Nutrients 2022, 14, 631. [Google Scholar] [CrossRef]
- Most, J.; Tosti, V.; Redman, L.M.; Fontana, L. Calorie restriction in humans: An update. Ageing Res. Rev. 2017, 39, 36–45. [Google Scholar] [CrossRef]
- Flanagan, E.W.; Most, J.; Mey, J.T.; Redman, L.M. Calorie Restriction and Aging in Humans. Annu. Rev. Nutr. 2020, 40, 105–133. [Google Scholar] [CrossRef] [PubMed]
- Simone, B. The design and implementation of caloric restriction for oncology research (CaReFOR): Is starving cancer cells in the clinical realm feasible? Hematol. Med. Oncol. 2017, 2, 1–6. [Google Scholar] [CrossRef]
- Masood W, Annamaraju P, Khan Suheb MZ; et al. Ketogenic Diet. [Updated 2023 Jun 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499830/.
- Madeo, F.; Carmona-Gutierrez, D.; Hofer, S.J.; Kroemer, G. Caloric Restriction Mimetics against Age-Associated Disease: Targets, Mechanisms, and Therapeutic Potential. Cell Metab. 2019, 29, 592–610. [Google Scholar] [CrossRef]
- Alidadi, M.; Banach, M.; Guest, P.C.; Bo, S.; Jamialahmadi, T.; Sahebkar, A. The effect of caloric restriction and fasting on cancer. Semin. Cancer Biol. 2020, 73, 30–44. [Google Scholar] [CrossRef] [PubMed]
- Klement, R.J.; Champ, C.E. Calories, carbohydrates, and cancer therapy with radiation: Exploiting the five R’s through dietary manipulation. Cancer Metastasis Rev. 2014, 33, 217–229. [Google Scholar] [CrossRef] [PubMed]
- Trepanowski, J.F.; Kroeger, C.M.; Barnosky, A.; Klempel, M.; Bhutani, S.; Hoddy, K.K.; Rood, J.; Ravussin, E.; Varady, K.A. Effects of alternate-day fasting or daily calorie restriction on body composition, fat distribution, and circulating adipokines: Secondary analysis of a randomized controlled trial. Clin. Nutr. 2017, 37, 1871–1878. [Google Scholar] [CrossRef] [PubMed]
- Kharazi, A.; James, S.; Taylor, J.; Lubinski, J.; Nakamura, L.; Makinodan, T. Combined chronic low dose radiation-caloric restriction: A model for regression of spontaneous mammary tumor. Endocrine 1994, 28, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Safdie, F.; Brandhorst, S.; Wei, M.; Wang, W.; Lee, C.; Hwang, S.; Conti, P.S.; Chen, T.C.; Longo, V.D. Fasting Enhances the Response of Glioma to Chemo- and Radiotherapy. PLoS ONE 2012, 7, e44603. [Google Scholar] [CrossRef] [PubMed]
- Saleh, A.; Simone, B.; Palazzo, J.; Savage, J.E.; Sano, Y.; Dan, T.; Jin, L.; Champ, C.; Zhao, S.; Lim, M.; et al. Caloric restriction augments radiation efficacy in breast cancer. Cell Cycle 2013, 12, 1955–1963. [Google Scholar] [CrossRef] [PubMed]
- Simone, B.A.; Dan, T.; Palagani, A.; Jin, L.; Han, S.Y.; Wright, C.; Savage, J.E.; Gitman, R.; Lim, M.K.; Palazzo, J.; et al. Caloric restriction coupled with radiation decreases metastatic burden in triple negative breast cancer. Cell Cycle 2016, 15, 2265–2274. [Google Scholar] [CrossRef] [PubMed]
- Mercier, B.D.; Tizpa, E.; Philip, E.J.; Feng, Q.; Huang, Z.; Thomas, R.M.; Pal, S.K.; Dorff, T.B.; Li, Y.R. Dietary Interventions in Cancer Treatment and Response: A Comprehensive Review. Cancers 2022, 14, 5149. [Google Scholar] [CrossRef]
- Rock, C.L.; Thomson, C.A.; Sullivan, K.R.; Howe, C.L.; Kushi, L.H.; Caan, B.J.; Neuhouser, M.L.; Bandera, E.V.; Wang, Y.; Robien, K.; et al. American Cancer Society nutrition and physical activity guideline for cancer survivors. CA A Cancer J. Clin. 2022, 72, 230–262. [Google Scholar] [CrossRef]
- Sanft, T.; Day, A.; Peterson, L.; Rodriguez, M.A.; Ansbaugh, S.; Armenian, S.; Baker, K.S.; Ballinger, T.; Broderick, G.; Demark-Wahnefried, W.; et al. NCCN Guidelines® Insights: Survivorship, Version 1.2022. J. Natl. Compr. Cancer Netw. 2022, 20, 1080–1090. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef] [PubMed]
- Ligibel, J.A.; Bohlke, K.; May, A.M.; Clinton, S.K.; Demark-Wahnefried, W.; Gilchrist, S.C.; Irwin, M.L.; Late, M.; Mansfield, S.; Marshall, T.F.; et al. Exercise, Diet, and Weight Management During Cancer Treatment: ASCO Guideline. J. Clin. Oncol. 2022, 40, 2491–2507. [Google Scholar] [CrossRef] [PubMed]
- Icard, P.; Ollivier, L.; Forgez, P.; Otz, J.; Alifano, M.; Fournel, L.; Loi, M.; Thariat, J. Perspective: Do Fasting, Caloric Restriction, and Diets Increase Sensitivity to Radiotherapy? A Literature Review. Adv. Nutr. Int. Rev. J. 2020, 11, 1089–1101. [Google Scholar] [CrossRef] [PubMed]
- Kalam, F.; James, D.L.; Li, Y.R.; Coleman, M.F.; A Kiesel, V.; Feliciano, E.M.C.; Hursting, S.D.; Sears, D.D.; Kleckner, A.S. Intermittent fasting interventions to leverage metabolic and circadian mechanisms for cancer treatment and supportive care outcomes. JNCI Monogr. 2023, 2023, 84–103. [Google Scholar] [CrossRef] [PubMed]
- Anemoulis, M.; Vlastos, A.; Kachtsidis, V.; Karras, S.N. Intermittent Fasting in Breast Cancer: A Systematic Review and Critical Update of Available Studies. Nutrients 2023, 15, 532. [Google Scholar] [CrossRef] [PubMed]
- Vega, C.; Merino, T. Radiotherapy and Oncology, 2022-05-01, Volume 170, Pages S1028–S1029.
- Leung, A.W.Y.; Chan, R.S.M.; Sea, M.M.M.; Woo, J. An Overview of Factors Associated with Adherence to Lifestyle Modification Programs for Weight Management in Adults. Int. J. Environ. Res. Public Health 2017, 14, 922. [Google Scholar] [CrossRef] [PubMed]
- Aycinena, A.C.; Valdovinos, C.; Crew, K.D.; Tsai, W.Y.; Mata, J.M.; Sandoval, R.; Hershman, D.; Greenlee, H. Barriers to Recruitment and Adherence in a Randomized Controlled Diet and Exercise Weight Loss Intervention Among Minority Breast Cancer Survivors. J. Immigr. Minor. Health 2017, 19, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Dent, R.; McPherson, R.; Harper, M.-E. Factors affecting weight loss variability in obesity. Metabolism 2020, 113, 154388. [Google Scholar] [CrossRef]
- Harvey, B.I.; Youngblood, S.M.; Kleckner, A.S. Barriers and Facilitators to Adherence to a Mediterranean Diet Intervention during Chemotherapy Treatment: A Qualitative Analysis. Nutr. Cancer 2023, 75, 1349–1360. [Google Scholar] [CrossRef]
- Harvie, M.; Pegington, M.; Howell, S.J.; Bundred, N.; Foden, P.; Adams, J.; Graves, L.; Greystoke, A.; Mattson, M.P.; Cutler, R.G.; et al. Randomised controlled trial of intermittent vs continuous energy restriction during chemotherapy for early breast cancer. Br. J. Cancer 2022, 126, 1157–1167. [Google Scholar] [CrossRef]
- Cortellino, S.; Quagliariello, V.; Delfanti, G.; Blaževitš, O.; Chiodoni, C.; Maurea, N.; Di Mauro, A.; Tatangelo, F.; Pisati, F.; Shmahala, A.; et al. Fasting mimicking diet in mice delays cancer growth and reduces immunotherapy-associated cardiovascular and systemic side effects. Nat. Commun. 2023, 14, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, M.d.l.C.; Stemler, K.M.; Jeter-Jones, S.; Fujimoto, T.N.; Molkentine, J.; Torres, G.M.A.; Zhang, X.; Broaddus, R.R.; Taniguchi, C.M.; Piwnica-Worms, H. Fasting Reduces Intestinal Radiotoxicity, Enabling Dose-Escalated Radiation Therapy for Pancreatic Cancer. Endocrine 2019, 105, 537–547. [Google Scholar] [CrossRef]
Figure 1.
Patient distribution according to sex (Male and Female) and chosen nutritional intervention (TRF or CR).
Figure 1.
Patient distribution according to sex (Male and Female) and chosen nutritional intervention (TRF or CR).
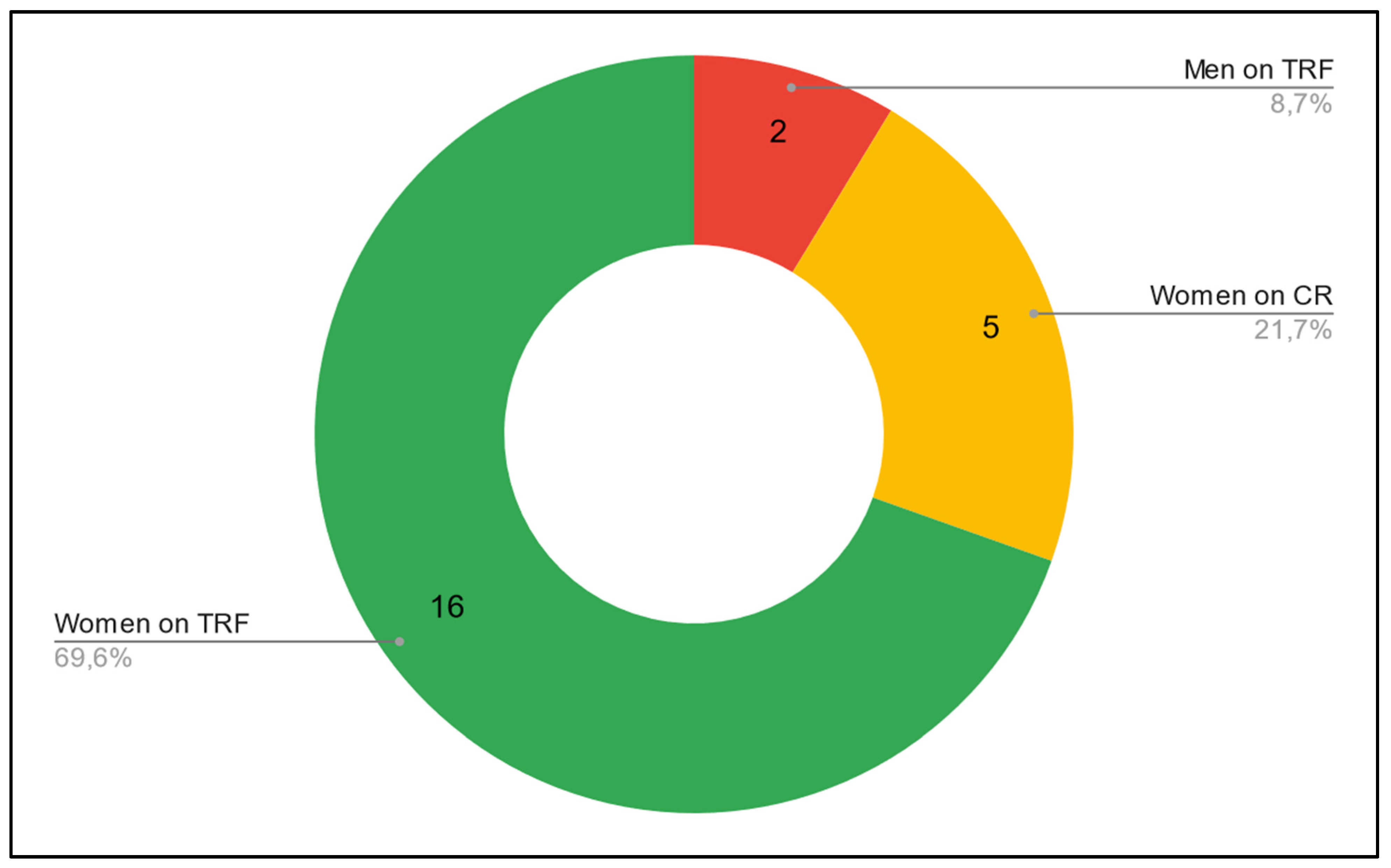
Figure 2.
General outline of the study. Figure showing an easier to visualize representation of the cohort of the study and the steps taken to ensure the intervention was a thorough and replicable success.
Figure 2.
General outline of the study. Figure showing an easier to visualize representation of the cohort of the study and the steps taken to ensure the intervention was a thorough and replicable success.
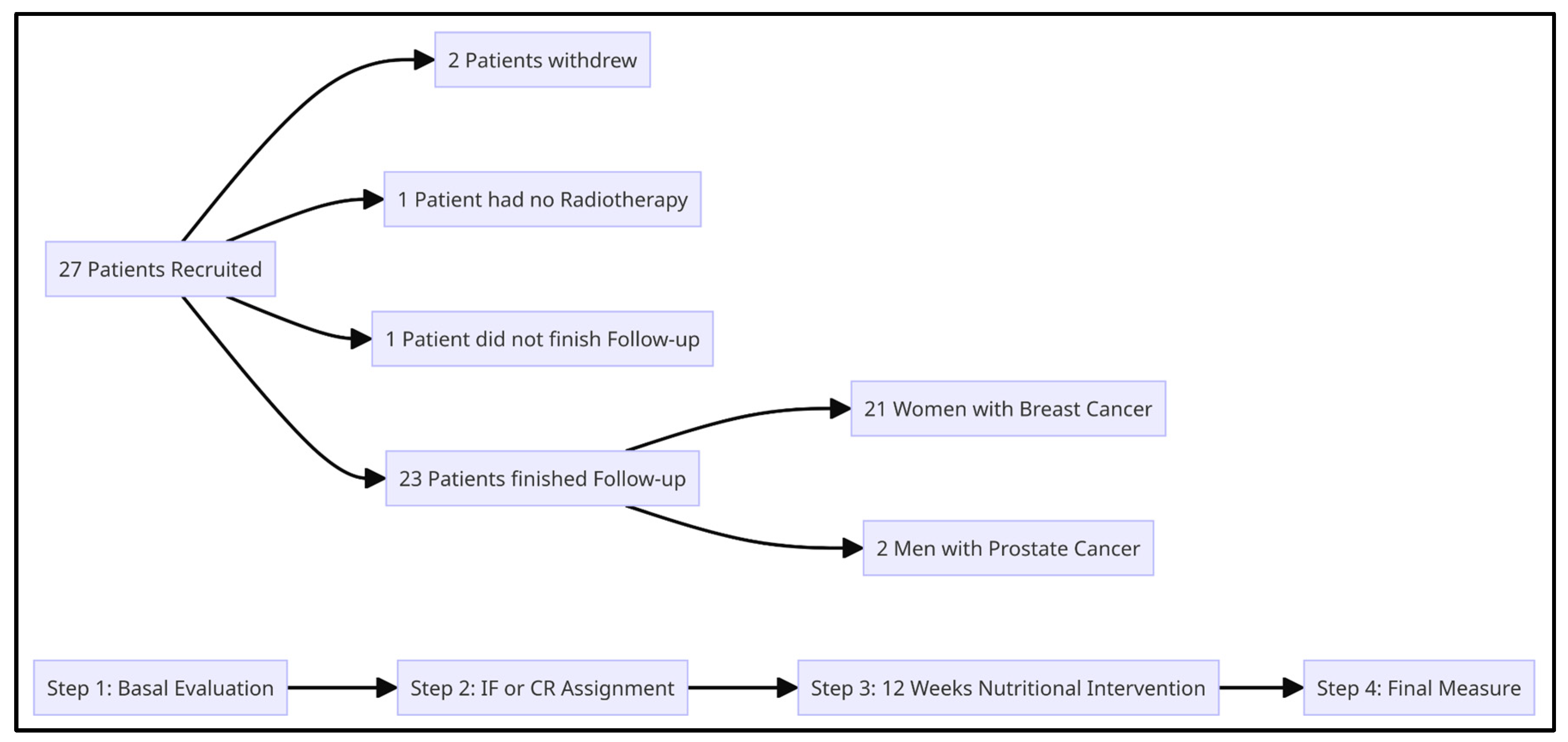
Figure 3.
Differences in biochemical measurements before and after the intervention. Shows changes in all our patients, independent of their clinical characteristics and chosen intervention. All measurements show a decrease after this study’s intervention was implemented.
Figure 3.
Differences in biochemical measurements before and after the intervention. Shows changes in all our patients, independent of their clinical characteristics and chosen intervention. All measurements show a decrease after this study’s intervention was implemented.
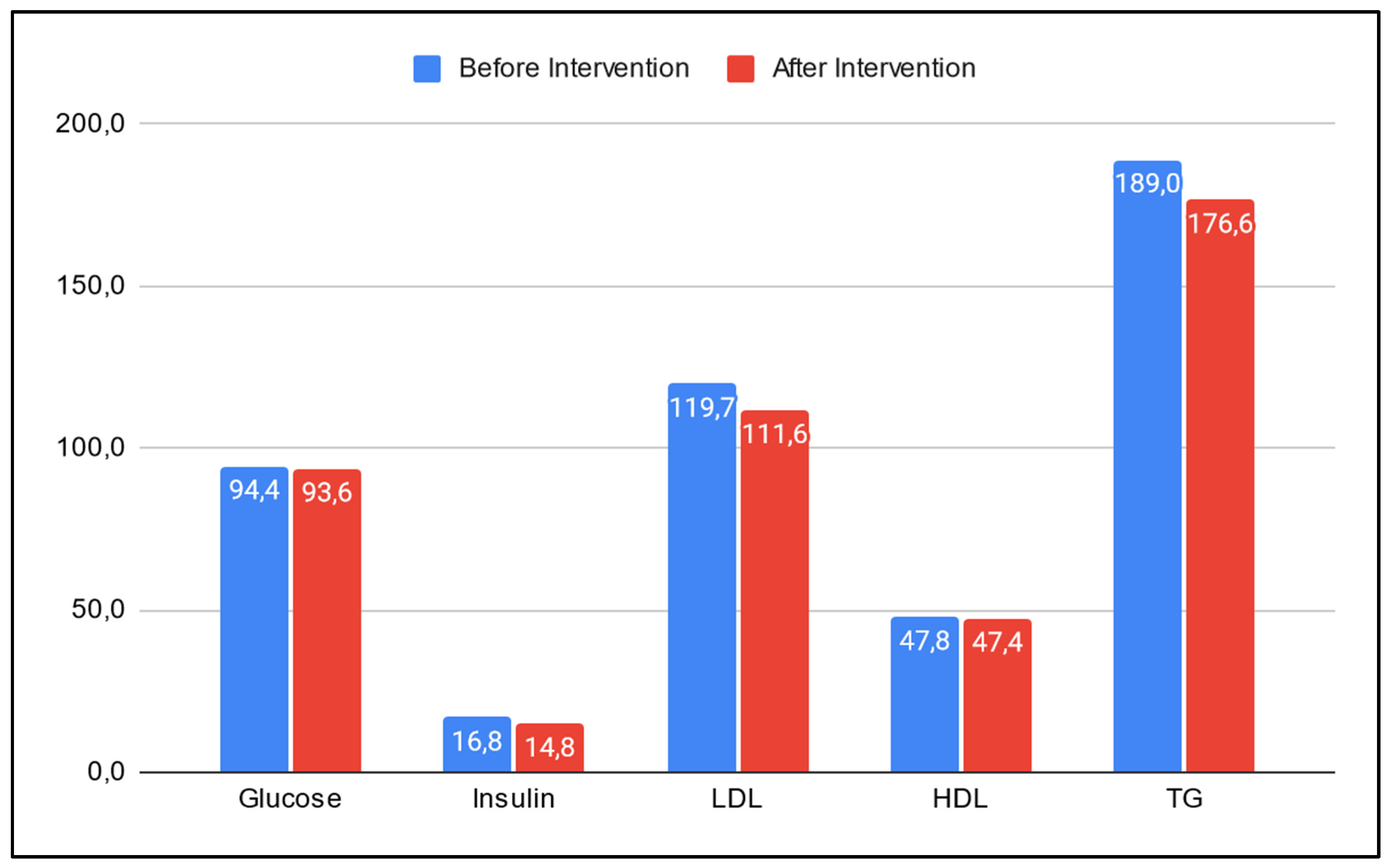
Figure 4.
Differences in anthropometric and biochemical measurements between interventions. Both TRF and CR show a decrease in the measure of glucose, insulin, TG, waist circumference and weight. TRF had a bigger drop than CR on waist circumference, weight, and levels of insulin and TG; while CR shows a larger drop in glucose level than TRF. On the other hand, TRF led to an increase in LDL and CR decreased it, while CR led to a decrease in HDL while TRF increased it.
Figure 4.
Differences in anthropometric and biochemical measurements between interventions. Both TRF and CR show a decrease in the measure of glucose, insulin, TG, waist circumference and weight. TRF had a bigger drop than CR on waist circumference, weight, and levels of insulin and TG; while CR shows a larger drop in glucose level than TRF. On the other hand, TRF led to an increase in LDL and CR decreased it, while CR led to a decrease in HDL while TRF increased it.
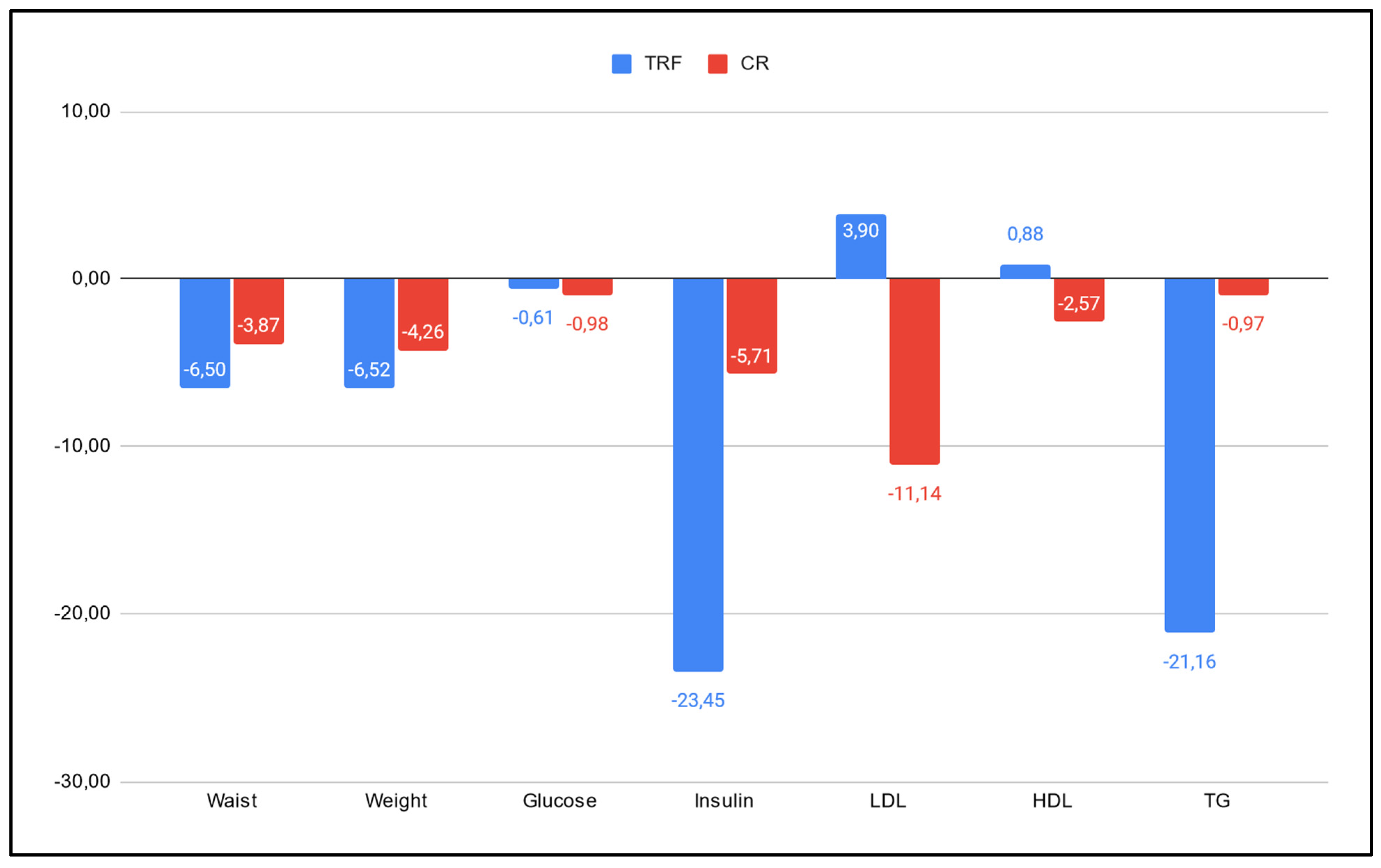

Table 1.
Nutritional interventions definitions and different approaches to IF [11]. In this study we analyzed CR and IF. Specifically, the Time Restricted Feeding (TRF) approach. We also define other approaches so the reader understands crucial differences between nutritional interventions and key aspects of the various approaches of IF.
Table 1.
Nutritional interventions definitions and different approaches to IF [11]. In this study we analyzed CR and IF. Specifically, the Time Restricted Feeding (TRF) approach. We also define other approaches so the reader understands crucial differences between nutritional interventions and key aspects of the various approaches of IF.
| Intervention | Approach | Definition |
|---|---|---|
| Intermittent Fasting | Periods of voluntary abstinence from food and drink [11]. There are various ways to approach IF. Most of them have no caloric restriction associated, or have caloric restriction for short periods of time. | |
| TRF | Fasting that requires limiting the consumption of calories to a window of time, typically between 4 and 12 h daily | |
| 5:2 | Two days per week, 24 hours each day, a very low calorie diet is applied. | |
| B2 | Two large meals are eaten per day: breakfast between 06:00 a.m. and 10:00 a.m., and lunch between 12:00 p.m. and 04:00 p.m. No dinner. | |
| Calorie Restriction | Nutritional intervention where the focus is in reducing energy intake, but keeping adequate nutrition [12]. In general, 10 - 30% of restriction is accepted as having beneficial effects and being tolerable [13,14]. | |
| Ketogenic Diet | Diet primarily consists of high fat intake, moderate protein consumption, and low carbohydrate intake. The macronutrient distribution typically ranges from approximately 55% to 60% fat, 30% to 35% protein, and 5% to 10% carbohydrates [15]. |
Table 2.
Summary of recommendations from international guidelines. ACS (American Cancer Society). NCCN (National Comprehensive Cancer Network). ESPEN (The European Society for Clinical Nutrition and Metabolism). ASCO (American Society of Clinical Oncology).
Table 2.
Summary of recommendations from international guidelines. ACS (American Cancer Society). NCCN (National Comprehensive Cancer Network). ESPEN (The European Society for Clinical Nutrition and Metabolism). ASCO (American Society of Clinical Oncology).
| ACS | Published in 2022. Focuses mostly on BMI, dietary patterns, specific food avoidance and physical activity. |
| NCCN | Published in 2022. Similar to ACS, it focuses mostly on BMI, dietary patterns, specific food avoidance and physical activity. No mention of intermittent fasting or caloric restriction at all in their guidelines. |
| ESPEN | Published in 2021. Does not recommend fasting unless there is evidence of a benefit. |
| ASCO | Published in 2022. Mentions intermittent fasting as an intervention, but refrains from recommending it as there is insufficient evidence and points to 5 systematic reviews. These reviews revised 177 articles, where only 7 talk about any kind of weight loss intervention and of these, 5 of them investigated short term fasting finding it to be well tolerated and having beneficial effects. |
Table 3.
Summary of main characteristics of patient cohort. Clinical characteristics of patients along the staging of their cancer. Number of people in each intervention. Changes in biochemical and anthropometric values before and after intervention in the complete cohort.
Table 3.
Summary of main characteristics of patient cohort. Clinical characteristics of patients along the staging of their cancer. Number of people in each intervention. Changes in biochemical and anthropometric values before and after intervention in the complete cohort.
| General | |||
| Male patients | 2 | ||
| Female patients | 21 | ||
| Mean Age (y) | 53,1 | ||
| Mean Height (m) | 1,57 | ||
| Cancer | |||
| Breast | 21 | ||
| Prostate | 2 | ||
| Stage | |||
| Breast Cancer | 0 | 1 | |
| I | 13 | ||
| II | 2 | ||
| III | 2 | ||
| N/A | 3 | ||
| Prostate Cancer | Recurrence | 2 | |
| Intervention | |||
| TRF | 7 | ||
| CR | 16 | ||
| Mean serum levels | Before | After | |
| Glucose | 94,4 | 93,6 | |
| Insulin | 16,8 | 14,8 | |
| LDL | 119,7 | 111,6 | |
| HDL | 47,8 | 47,4 | |
| TG | 189,0 | 176,6 | |
| Mean Anthropometry | Before | After | |
| Weight (kg) | 77,2 | 73,6 | |
| Waist Circ. (cm) | 95,8 | 90,9 |
Table 4.
Expanded table of the cohort of patients. Shows characteristics of the cohort and results from the study, differentiated by intervention type (TRF or CR). Clinical characteristics of patients and their cancer (sex, cancer type and molecular subtype), differences in measures before and after the intervention, and percentage of adherence in both breast and prostate cancer.
Table 4.
Expanded table of the cohort of patients. Shows characteristics of the cohort and results from the study, differentiated by intervention type (TRF or CR). Clinical characteristics of patients and their cancer (sex, cancer type and molecular subtype), differences in measures before and after the intervention, and percentage of adherence in both breast and prostate cancer.
| General | ||||
| Male | 2 | |||
| TRF | 2 | |||
| CR | 0 | |||
| Female | 21 | |||
| TRF | 5 | |||
| CR | 16 | |||
| Type | ||||
| Breast | ||||
| DCIS | 1 | |||
| CDI | 18 | |||
| CLI | 3 | |||
| Poorly Differentiated | 1 | |||
| Prostate | ||||
| Adenocarcinoma | Gleason 3 + 3 | 1 | ||
| Gleason 3 + 4 | 1 | |||
| Molecular Subtypes | ||||
| Breast | Luminal | 18 | ||
| Triple Negative | 3 | |||
| Mean Serum Levels by Intervention | Before | After | Difference (%) | |
| TRF | ||||
| Glucose | 94,43 | 93,86 | -0,61 | |
| Insulin | 15,58 | 11,93 | -23,45 | |
| LDL | 122,23 | 127,00 | 3,90 | |
| HDL | 48,43 | 48,86 | 0,88 | |
| TG | 180,29 | 142,14 | -21,16 | |
| CR | ||||
| Glucose | 94,38 | 93,45 | -0,98 | |
| Insulin | 17,26 | 16,28 | -5,71 | |
| LDL | 116,93 | 103,90 | -11,14 | |
| HDL | 47,88 | 46,64 | -2,57 | |
| TG | 195,75 | 193,86 | -0,97 | |
| Mean Anthropometry by Intervention | Before | After | Difference (%) | |
| TRF | ||||
| Weight (kg) | 75,11 | 70,23 | -6,50 | |
| Waist Circ. (cm) | 94,21 | 88,07 | -6,52 | |
| CR | ||||
| Weight (kg) | 78,09 | 75,07 | -3,87 | |
| Waist Circ. (cm) | 96,47 | 92,36 | -4,26 | |
| Loss of 5% or more of initial weight (True adherence) | Yes | No | ||
| Breast Cancer | ||||
| TRF (n = 5) | 5 | 0 | ||
| CR (n = 16) | 7 | 9 | ||
| Prostate Cancer | ||||
| TRF (n = 2) | 0 | 2 | ||
| CR (n = 0) | 0 | 0 |
Table 5.
Changes in anthropometric and biochemical measurements post intervention. Differences before and after treatment quantified in quantity (QD) and in percentage (PD) relative to each intervention’s average levels.
Table 5.
Changes in anthropometric and biochemical measurements post intervention. Differences before and after treatment quantified in quantity (QD) and in percentage (PD) relative to each intervention’s average levels.
| TRF | CR | ||||
| QD | PD (%) | QD | PD (%) | TRF:CR | |
| Glucose | -0,57 | -0,61 | -0,92 | -0,98 | - 38,0 |
| Insulin | -3,65 | -23,45 | -0,99 | -5,71 | 270,8 |
| LDL | 4,77 | 3,90 | -13,03 | -11,14 | - |
| HDL | 0,43 | 0,88 | -1,23 | -2,57 | - |
| TG | -38,14 | -21,16 | -1,89 | -0,97 | 1915,1 |
| Weight (kg) | -4,89 | -6,50 | -3,02 | -3,87 | 61,8 |
| Waist Circ. (cm) | -6,14 | -6,52 | -4,11 | -4,26 | 49,5 |
*On column TRF:CR, by using the following formula:
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



