
Submitted:
28 December 2023
Posted:
29 December 2023
You are already at the latest version
Abstract
Currently, the use of medications during pregnancy in Latin America is common; studies with Latin American samples find that nearly 90% of pregnant women use some medication at least once during pregnancy. Furthermore, approximately 21% of the respondents self-medicated. Worldwide, the prevalence of this disease is 32%. The most common medications are nonsteroidal anti-inflammatory drugs and analgesics. Many of these drugs are available over the counter without a prescription. For this reason, a systematic review of the literature on the adverse effects on the woman and the fetus was performed.
Objective: To determine the adverse effects associated with the use of nonsteroidal anti-inflammatory drugs (NSAIDs) on pregnant women and fetuses during pregnancy.
Methods: Systematic literature review. The following search strategy was used for the databases: Science Direct, PubMed, Scopus and Web of Science, through September 3, 2022. The population of pregnant women without previous comorbidities was defined. The intervention of interest was the use of NSAIDs during pregnancy. The outcomes of interest were adverse effects for the mother or fetus (weight of the newborn, congenital malformations present in the fetus, systemic effects in the pregnant woman during her gestation period). The types of studies included clinical trials, cohort studies and case‒control studies.
Results: 1 study included 2,985 pregnant women without previous comorbidities. The use of aspirin more frequently during pregnancy stands out. The adverse effects on the fetus were preterm birth <37 weeks, low birth weight < 2500 g and increased admission to the neonatal intensive care unit. No adverse effects were found for the mother.
Conclusions: There are not enough data indicating that the use of NSAIDs during pregnancy is safe. Some studies show that the use of NSAIDs during pregnancy could be related to problems in the development and growth of the fetus and health effects for the mother during pregnancy, so it is advisable to use these drugs under medical prescription and for the shortest possible time. in the gestation stage.
Keywords:
Nonsteroidal anti-inflammatory drugs
; pregnancy
; adverse effects
; analgesics
; self-medication
Introduction
Currently, the use of medications during pregnancy is common for women in relation to symptom management, and many of these medications are not prescribed regularly, which creates a problem because these medications require treatment. aKnowledge of the contraindications of each medication, as well as its mechanism of action, spectrum, half-life, absorption, availability and excretion. Most pregnant mothers are unaware of this situation, according to Doering and Stewart (1978), who observed that, on average, pregnant women take eleven different medications during the nine months of the prenatal period and take seven different medications during labor (1). However, this concern remains.
During the pregnancy stage, the woman experiences physiological changes to adapt her body to the embryonic period, which consists of three trimesters of full-term pregnancy. These changes alter the pharmacokinetics and pharmacodynamics of drugs and have a significant impact on their absorption, distribution, and excretion. For this reason, the Food and Drug Administration (FDA) created five categories with the letters A, B, C, and D. As a result, maternal drug use can have effects on the fetus, as many drugs can pass through the placenta and come into direct contact with the fetus, possibly leading to adverse effects (2).
It should be noted that the use of drugs in pregnant women follows FDA guidelines on adverse effects at each stage of gestation and even allows the use of some drugs at certain stages; that is, depending on the trimester of gestation, the risk of adverse effects increases. adverse to the fetus.
The existence of adverse effects in clinical practice, despite government regulations regarding the prevention of such adverse effects, is still an area of interest for the scientific community. The authorities recognize that this control over unwanted pharmacological effects can reduce the number of articles that report this type of adverse event. However, the growing interest in the transparency and quality of research in the medical sciences, in addition to the lack of systematization of the scientific literature proven in the Cochrane and Prospero repositories of systematic reviews on the adverse effects of medications in young pregnant women and adults, encourages this research.
For this reason, the objective of the review was to describe the adverse effects associated with the use of nonsteroidal anti-inflammatory drugs (NSAIDs) in pregnant women and fetuses.
Materials and methods
Type of study:
Systematic literature review The PRISMA protocol for systematic reviews of the literature on clinical trials on the adverse effects associated with the use of drugs in pregnant women during pregnancy was used. Answering the guiding question: What are the adverse effects associated with the use of NSAIDs (nonsteroidal anti-inflammatory drugs) in pregnant women during pregnancy? Since this review evaluates the damage caused to the health of pregnant women and fetuses, only evidence from clinical trials, cohort studies, and case‒control studies was included as appropriate evidence to evaluate the harm of the use of these drugs.
Inclusion criteria:
Young and adult pregnant women who consumed nonsteroidal anti-inflammatory drugs during pregnancy without exposure to other drugs were included, and associated adverse, secondary and/or unwanted effects were identified (reported in public and private pharmacological surveillance mechanisms, scientific literature). to nonsteroidal agents during pregnancy for the fetus and the mother, the search was carried out in clinical trials, cohort studies and case‒control studies.
Exclusion criteria:
Systematic reviews or meta-analyses were not performed because a review of reviews was not performed. Additionally, observational or qualitative studies were not included because they are not adequate sources of evidence for evaluating the harmful effects of drugs on pregnancy (mothers and fetuses).
Selected databases
The following databases were searched for publication in all years, from all languages until September 3, 2022: ScienceDirect, PubMed/Medline, Scopus and Web of Science. Scientific information related to the criteria set out in the PICOT question was obtained.
The search strategy for the Science Direct, PubMed, Scopus and Web of Science databases was as follows: (("Pharmacology, Clinical"[Mesh]) AND "adverse effects" [Subheading]) AND "Pregnancy"[Mesh] OR "Pharmacology, Clinical " AND "adverse effects" AND Pregnancy”.
Data analysis and synthesis process
This systematic literature review was carried out through the Rayyan collaborative search server, in which articles that reported adverse effects of nonsteroidal anti-inflammatory drugs (NSAIDs) on pregnant women and fetuses were identified. The authors independently reviewed the titles and abstracts and subsequently extracted the synthesized evidence from the full-text articles that met the inclusion criteria.
Clinical characteristics of the mothers, sociodemographic data about the sample, treatment characteristics (dose, type of drug), and outcome of interest (what adverse effect is reported in the mother and/or the fetus) were extracted. Since more than one article was not found, it was not possible to perform a meta-analysis. The process is detailed in the PRISMA flowchart (Figure 1).
Results:
The search results are detailed in Table 1. Finally, 1 multicenter trial was included in which 2,985 pregnant women were observed. Patients ranging between 13 and 25 weeks of gestation without previous comorbidities were included. (3) The list of excluded articles, as well as the reasons for exclusion, are detailed in Figure 1.
Main results of the multicenter trial:
Adverse effects were observed for the fetus but not for the mother. It should be noted that it was ruled out that the effects differ from those of smoking since there were no significant differences in patients randomly assigned to aspirin versus placebo among smokers and nonsmokers.
The studies were of high quality, while the bias assessment was low for most of the bias assessment criteria used.
Discussion
Pregnancy is a biological process in which women are responsible for the development of a human being and starts at the time of gestation and childbirth. During this period, the woman's body experiences a series of drastic physiological and hormonal changes that allow it to provide the necessary environment for the growth and development of the fetus, generating the experience of pain or inflammation, which is often also associated with the preexisting medical conditions of the pregnant woman.
In this context, a high population of pregnant mothers has shown that they are looking for pharmacological options that allow them to reduce the symptoms generated by pregnancy without truly understanding the components and implications that it can have on their body or the fetus. Among these options are nonsteroidal anti-inflammatory drugs (NSAIDs), drugs that are frequently used during pregnancy due to the symptoms that can develop during this stage. However, the information available on its effects during pregnancy is limited and, for the most part, inconclusive. An examination of the potential risks for pregnant women and fetuses derived from self-medication with NSAIDs through a review of the literature revealed that the use of NSAIDs in the first trimester does not appear to be a significant risk factor. However, in subsequent trimesters, teratogenic effects on the fetus have been reported (4).
Consequently, these findings support the Food and Drug Administration (FDA) recommendation to avoid the use of NSAID medications during pregnancy, especially after 20 weeks, due to the risk of placental hypoperfusion and fetal kidney damage. This warning highlights the prevailing need to perform constant pharmacological surveillance on nonsteroidal anti-inflammatory drugs (NSAIDs), which, as mentioned above, are widely consumed due to their over-the-counter availability and easy access to the market. (5)
The remarkable ability of NSAIDs to relieve pain and reduce inflammation by inhibiting prostaglandin synthesis at the peripheral level exposes the paradox of their popularity and the need for caution in their use, especially during pregnancy. Additional research evidence suggests that the use of these drugs during pregnancy may be related to a slight increase in the frequency of cardiac and orofacial malformations in fetuses. These findings reinforce the importance of using these medications both moderately and under medical supervision, highlighting the complexity of balancing the need for pain relief with the precaution necessary to safeguard the health of the fetus and the pregnant woman. In this context, informed decision-making and appropriate medical advice are essential to ensure the safety of both the mother and the future baby during the gestational period (6).
On the other hand, the wide availability of NSAIDs and their attractive analgesic and anti-inflammatory action make their unrestricted use common, but the potential risk for fetal development highlights the need for careful and controlled administration of these medications, especially in pregnant women. Constant care and pharmacological monitoring are essential to ensure the safety of both expectant mothers and their babies during this crucial stage of life. Therefore, in this study, an exhaustive analysis of adverse effects during the gestation period was performed through a systematic review of the literature. The central purpose is to enrich the scientific evidence available in this field.
Abramovici's study revealed significant findings. Among the 2985 women without serious illnesses, with a gestation period between 13 and 25 weeks, the impact of the administration of analgesic drugs was observed. The initial results indicated premature birth, defined as birth before 37 weeks of gestation. This event results in a greater risk of hemorrhage, ovarian damage, and systemic or intestinal effects at the time of delivery. It should be noted that these aforementioned risks are not produced by NSAIDs but by premature birth, which is an effect of them. low birth weight <2,500 gr. In addition, an increase in the admission of newborns to neonatal intensive care units (NICUs) was observed. These results highlight the importance of carefully considering the administration of analgesics during pregnancy since it is related not only to neonatal risks but also to adverse consequences for maternal health (3).
These results, derived from specific research, underline the importance of understanding the possible adverse effects that may arise during pregnancy. Preterm birth has significant implications for maternal and fetal health. The increase in NICU admissions highlights the need for more rigorous medical care and monitoring during pregnancy to reduce the risks associated with these unfavorable outcomes. Thus, pregnant women may not be fully aware of the risks that certain medications may represent for them and their babies since they often rely on knowledge from popular culture to administer drugs since the suggestion is given by acquaintances who speak from their own experience without recognizing the effects that could be caused. Additionally, one of the main problems that is evident is that many pregnant women avoid medical advice and normalize pain treatment with the medications they normally consume but are unaware of the adverse effects that could develop during pregnancy. body or in the formation of the fetus, the body has changed, and with this change, the body processes what it consumes. Therefore, pregnant women should be regularly monitored by health professionals to guarantee a healthy pregnancy, in which the risks for the mother and her fetus are minimized.
Likewise, it is interesting to note that some of the public policies that regulate the supply of medications and care for pregnant mothers have not had adequate systematization that shows the potential impact of the use of NSAIDs and that therefore allows regulation to be carried out. through pedagogical and legislative means that restrict the risk of pregnancy for mothers. For example, through Statutory Law 1751 of 2015, which determines the regulation of the fundamental right to health, pregnant mothers were considered subjects of special constitutional protection, prioritizing the fundamental principles for them (availability, acceptability, accessibility and quality). professional:
Therefore, in the case of pregnant women, measures will be adopted to guarantee access to the health services they require during pregnancy and after pregnancy and to guarantee that they can exercise their fundamental rights within the framework of access to health services. (Congress of Colombia, 2015, Law 1751, Article 11) (7). Law 1751 addresses the prioritization that should be given to pregnant mothers and the care that should be implemented from health services, but it does not regulate public policies regarding pharmacological regulation for pregnant women and, therefore, pedagogical processes for understanding possible risks from their supply. It is interesting to see greater pharmacological regulation in contraception and safe abortion processes than in what is linked to pregnancy (7).
Another implication of this process is the easy access of pregnant women to NSAID drugs. This is related to the widespread availability of NSAIDs on the market, their sale without a prescription, and the common perception that they are low-risk medications. Easy access to these drugs may lead to greater self-medication by pregnant women, as they may consider them quick and convenient options for relieving pain or inflammation during pregnancy. However, such accessibility raises important concerns since NSAIDs can have the previously mentioned adverse effects. Furthermore, in populations with health difficulties such as arthritis, spontaneous abortions could occur, although the findings of Rojas and Cabrera are inconclusive. (8).
Ramírez et al. noted that there is a significant propensity for the use of NSAIDs for possible congenital diseases in children due to problems during pregnancy resulting from placental abruption or other difficulties during pregnancy. (8) A study by Bohórquez et al. revealed the prevalence of self-medication in pregnant women in Colombia over a period of 10 years and revealed that analgesics and nonsteroidal anti-inflammatory drugs (NSAIDs) are the drugs most commonly self-administered by these women, although they are not recommended for use in the last trimester of pregnancy (9). Arellano et al. focused on the pharmacological management of common disorders during pregnancy in primary care and noted that some NSAIDs are classified as risk category B during the first or second trimester but become category D in the last trimester, which indicates a significant risk for the fetus. The importance of avoiding its use after the third trimester is emphasized due to potential adverse effects on maternal and fetal health (10).
Although all the studies suggest the use of NSAIDs in pregnant women is alarming, the lack of definitive conclusions is due to the difficulty in generalizing the results. Different studies can yield different conclusions, especially when considering populations with particular conditions. The variability in findings highlights the complexity of the impact of nonsteroidal anti-inflammatory drugs (NSAIDs) on pregnancy. However, although adverse effects were identified in the present study, continuing to investigate the effects of NSAIDs on pregnancy is crucial. Therefore, persistent research is vital to guarantee the safety of pregnancy and fetal development, as this research could lead to the establishment of pharmacological control measures from a legislative basis. It is essential to specifically address the reasons underlying the lack of conclusive approaches in studies, considering the variables that may influence the results. Additionally, understanding the risks and benefits of these medications can play a critical role in medical decision-making and prenatal care. By taking into account the complexity of factors affecting the relationship between NSAIDs and pregnancy, the ability to guide informed decisions can be improved, thereby contributing to the health and well-being of both expectant mothers and their babies. This approach may help reduce the risks associated with the use of NSAIDs during pregnancy.
Understanding the risks associated with the use of nonsteroidal anti-inflammatory drugs (NSAIDs) is vital for a pregnant mother, as this understanding can reveal the difference between a healthy pregnancy and one with unnecessary complications. First, a pregnant mother who understands the risks of NSAIDs is therefore more prepared to make informed decisions about her health and that of her baby, resorting to a much more careful medical protocol. Knowing that some NSAIDs, such as ibuprofen, are linked to an increased risk of complications, such as premature closure of the ductus arteriosus or pulmonary hypertension in the baby, allows the mother to take preventative measures by avoiding these medications (9).
Furthermore, understanding the risks of NSAIDs can encourage open and effective communication with health professionals who supervise pregnancy and who reject self-diagnoses or those given by people in the community since ignorance often puts people at risk. the well-being of mothers and fetuses. This communication is essential for proper medical care, as it allows the doctor and mother to make decisions together based on a complete evaluation of the risks and benefits of any necessary treatment.
On the other hand, knowledge of the risks of NSAIDs may motivate pregnant women to seek safer alternatives to relieve pain or inflammation; nonpharmacological therapies, such as physical therapy, rest, physical therapy, and other approaches, may be helpful. adequate options, mainly supported by health entities that privilege the mother and fetus as subjects of special protection. By helping mothers make decisions that minimize exposure to NSAIDs, reduce unnecessary risks and protect the health of both mothers and fetuses, this knowledge empowers future mothers and contributes to healthier pregnancies without unnecessary complications.
As health professionals, we must have extensive knowledge of medical studies and the possible implications that can develop in different populations, observing patient variables in each context. In the case of pregnant mothers, the particularities of each patient must be recognized, and aggravations that may develop during the period of gestation until delivery must be understood. The pregnancy process and the transformation of the body must be recognized, and the possible implications that could affect the baby based on the mother's health particularities must be understood. In the case of NSAIDs, the effects of the gestation period must be recognized since medical treatment varies significantly from the first trimester to the last (which becomes more risky for the fetus).
The study of the effects of nonsteroidal anti-inflammatory drugs (NSAIDs) on pregnancy in young and adult women, as well as on the fetus, is a field of research with significant challenges facing the medical sector. Many of these limitations are related to medical and moral ethics, data availability, and variability of results. In the case of ethical implications, there is a confrontation with carrying out controlled clinical studies in pregnant women because many sectors do not agree with exposing pregnant women and fetuses to possible risks since the systematization of data from the observation that takes a human being as an object of testing. As a result, most studies in this area are based on retrospective observations and analyses of existing data rather than controlled experiments. The present work collected literature on the effects of nonsteroidal inflammatory agents on pregnancy in women.
The variability of the results from different studies is a common limitation in research into the effects of NSAIDs on pregnancy. This is because the effects may depend on the dose supplied, the duration of exposure during pregnancy, the presence of congenital diseases, and the context in which the mother is exposed, among other factors, which makes it difficult to draw definitive conclusions. Some repetitive patterns can be rectified, but due to the lack of further experimentation in this field, it is not possible to determine precepts.
It is relevant to note that, unlike other studies where the data depend on objective measurements such as physiological and clinical indicators, in the study of the adverse effects of NSAIDs during pregnancy, the information is often based on the truthfulness of the patients. This dependence on self-reports can introduce biases and errors in the information since there is no complete monitoring process of the mother, in part due to the ethical considerations previously stated. The lack of objective measures may affect the accuracy of the results, highlighting the need to address these limitations in future research to improve the reliability of the data and strengthen the knowledge base in this field.
Gaps in the data on population groups and diseases were noted, as was the need for specific information for children, adolescents, and pregnant and lactating women, according to the WHO. Including detailed data for these groups is essential for ensuring that they receive the necessary interventions. Although pregnancy is exclusively associated with the female sex, the importance of comprehensively addressing the different dimensions of health that can vary between genders is highlighted beyond the biological issues associated with pregnancy (11).
Due to ethical and implementation limitations, the lack of controlled clinical trials in this field leaves gaps in solid scientific evidence. This means that much of the available information is derived from observational studies and retrospective analyses, which prevents detailed implementation of the care and pedagogy of pregnant mothers. The World Health Organization (11) has sought to expand the field of application of strategies that enable clinical trials in prioritized populations and that allow more conclusive results to be determined.
Recognizing that “well-designed and well-executed clinical trials are indispensable for evaluating the safety and effectiveness of health interventions” and recognizing “the importance of promoting equity in clinical trial capacity”, the Health Assembly set out to improve the quality of the evidence generated in clinical trials and its coordination. [...] "Clinical trials of new health interventions are likely to produce a clearer result when carried out in diverse settings, especially in all the main population groups that the intervention is intended to benefit, with particular attention given to underrepresented populations"; These populations may include women, especially pregnant and breastfeeding women, children, and other groups underrepresented in such trials, such as vulnerable and marginalized people.
To advance research on the effects of nonsteroidal anti-inflammatory drugs (NSAIDs) in pregnancy, both in young and adult women and in fetuses, and to address the previously mentioned limitations, different recommendations have been derived from the present discussion.
It is essential to develop production processes for large-scale observational studies, which should be encouraged through comprehensive policies that allow the execution of the study with the protection of the health and well-being of the mother and fetus. Therefore, conducting larger-scale studies would provide more solid and generalizable data on the effects of NSAIDs during pregnancy, allowing them to be compared at local and international levels. Likewise, long-term follow-up of pregnant women exposed to NSAIDs and their babies should be performed. This approach allows us to evaluate the impact of these changes during gestation and the possible variants that may arise during a child's growth, providing crucial information on the possible long-term effects on the development of the child and the mother.
On the other hand, investigating the relationship between the dose and duration of NSAID use during pregnancy and the resulting effects on the mother and fetus is essential since understanding the stage of development of both drugs and the effects generated would help determine safer use guidelines, promoting more rigorous regulation of the sale of these drugs to pregnant women. In addition, it is necessary to encourage research into safer alternatives for the treatment of pain and inflammation in pregnant women, which could include nonpharmacological therapies, such as physiotherapy, homeopathy and analgesics, which are considered safer during pregnancy. Likewise, promoting collaboration between researchers and health professionals at an international level is crucial, as this not only seeks to compile findings but also inform the affected public.
Another important measure is to develop educational programs and awareness campaigns aimed at both health professionals and pregnant women, with a social approach based on responsibility toward others, where these initiatives must address the risks of NSAIDs and promote safe practices during pregnancy for pain management. Therefore, medical and regulatory organizations should regularly review and update clinical guidelines related to the use of NSAIDs during pregnancy. This should be based on the most recent evidence available, as well as seeking to establish the basis for general legislation.
Finally, given their importance in maternal and fetal health, state and international research funding agencies should prioritize the allocation of resources for studies related to the use of NSAIDs during pregnancy. These joint steps will significantly contribute to advancing the understanding and safe management of NSAIDs during pregnancy.
Conclusions:
There is not enough data to say that the use of NSAIDs is unsafe, the information available on their effects during pregnancy is limited, and, for the most part, the data are inconclusive. When examining the potential risks for pregnant women and fetuses derived from self-medication with NSAIDs through a review of the literature and systematic and descriptive research, it has been confirmed that the use of NSAIDs in the first trimester does not seem to represent a factor of significant risk. However, in the second and third trimesters, teratogenic effects on the fetus, such as the risk of placental hypoperfusion, fetal kidney damage, and cardiac and facial malformations, as well as an increased risk of preeclampsia and premature birth, have been reported, among others already mentioned herein. Thus, the potential risk for fetal development and maternal well-being should be increased, so it is advisable to avoid the use of these drugs with caution during pregnancy, especially in the second and third trimesters.
However, the effects may depend on the dose consumed, the duration of exposure during pregnancy, the comorbidities of the pregnant woman and the context in which the mother is exposed, among other factors, which makes it difficult to establish definitive conclusions. Some repetitive patterns can be seen, but because there is still a lack of additional experimentation in this field, it is not possible to have conclusive precepts. In addition, the research data mostly depend on the veracity of the patients, so we can be faced with biases and errors in the information since there is no complete follow-up and monitoring process for the mother, thus leaving us with biases that can generate information errors.
References
- DOERING, Paul L.; STEWART, Ronald B. The extent and character of drug consumption during pregnancy. Jama, 1978, vol. 239, no. 9, p. 843-846.
- FDA recommends avoiding use of NSAIDs in pregnancy at 20 weeks or later because they can result in low amniotic fluid [Internet]. US Food and Drug Administration . FDA; 2022 [cited 6 Nov 2023]. Available at: https://www.fda.gov/drugs/fda-drug-safety-podcasts/fda-recommends-avoiding-use-nsaids-pregnancy-20-weeks-or-later-because-they-can-result -low-amniotic.
- Jauk V, Wetta L, Cantu J, Edwards R, Biggio J, Tita A, et al. Low-dose aspirin, smoking status, and the risk of spontaneous preterm birth. Am J Perinatol [Internet]. 2014 [cited 2023 Nov 6];32(05):445–50. Available at: https://pubmed.ncbi.nlm.nih.gov/25261702/.
- Vera, O. (2018). USE OF DRUGS IN PREGNANCY. La Paz Medical Journal, 21(2), 60-76. Retrieved on May 30, 2023, from http://www.scielo.org.bo/scielo.php?script=sci_arttext&pid=S1726-89582015000200010&lng=es&tlng=es .
- Pola CS, Guillén E, Martín CA. Use of nonsteroidal anti-inflammatory drugs during pregnancy. Med Clin (Barc) [Internet]. 2021 [cited 2023 Nov 6];156(11):568–72. Available at: https://dialnet.unirioja.es/servlet/articulo?codigo=7934475.
- Gov.co. [cited Nov 6, 2023]. Available at: https://www.minsalud.gov.co/Normatividad_Nuevo/Ley%201751%20de%202015.pdf.
- Rojas, E. Cabrera, S. (2020). Rheumatoid arthritis and pregnancy. Update. Paraguayan Journal of Rheumatology, 6(1), 36-47. Epub . Pp. 36-47. http://scielo.iics.una.py/scielo.php?pid=S2413-43412020000100036&script=sci_arttext\.
- Ramírez, E., Acuña, A., Azofeifa, M. (2021). Pharmacological management of chronic pain in pregnancy. Sinergia Medical Magazine, 6 (8). https://www.medigraphic.com/pdfs/sinergia/rms-2021/rms218h.pdf.
- EdU.co. [cited Nov 6, 2023]. Available at: https://www.unipamplona.edu.co/unipamplona/portalIG/home_253/recursos/general/16062022/vol_10-ii_rev.pdf.
- View of Respiratory, painful and gastrointestinal disorders: Pharmacological management in Primary Care of common pathologies during pregnancy [Internet]. Uaca.ac.cr. [cited Nov 3, 2023]. Available at: http://revista.uaca.ac.cr/index.php/actas/article/view/1341/1705.
- the Argentina P of RPP, the North the P and. the UK of GB e. I. Strengthening clinical trials to provide high-quality evidence on health interventions and improve the quality and coordination of research [Internet]. Who.int. [cited Nov 6, 2023]. Available at: https://apps.who.int/gb/ebwha/pdf_files/WHA75/A75_ACONF9-sp.pdf.
Figure 1.
Prism flow chart for study selection.
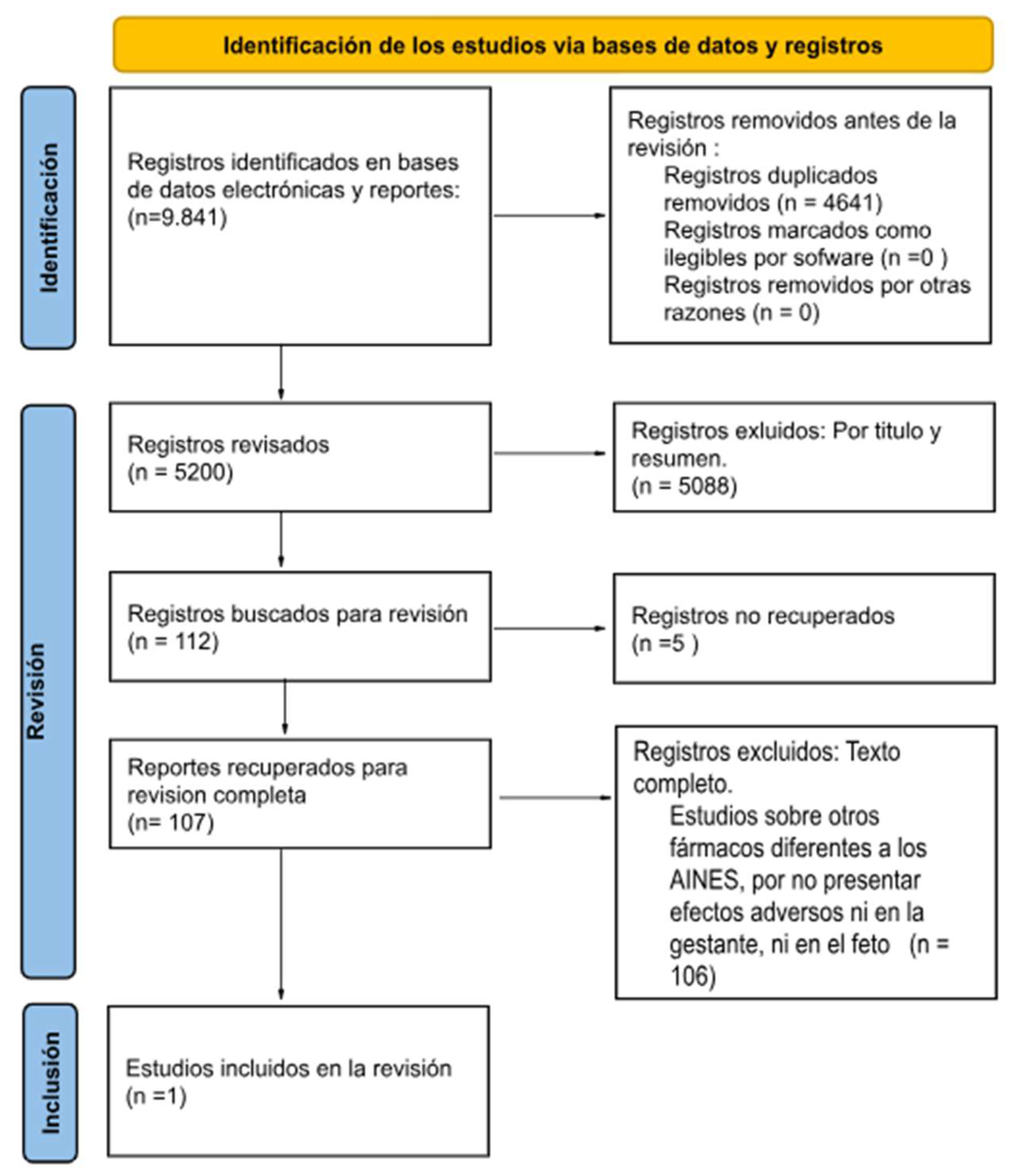

Table 1.
Characteristics of the included studies.
| Author, year, type of study. | Sample characteristics | Drug classification | Adverse effect in pregnant women | Adverse effect on the fetus. |
|---|---|---|---|---|
| 1. Abramovici (2015), Multicenter trials | Single gestation between 13 and 25 weeks at the time of randomization, in total 2,985 pregnant women. Women were excluded if: preexisting hypertension, kidney disease, diabetes mellitus and other comorbidities . | NSAID (Aspirin) | There was no difference between aspirin and placebo. | Premature birth <37 weeks Low birth weight (birth weight < 2,500 g and increased admission to the neonatal intensive care unit. |
Table 2.
Evaluation of bias in the included studies according to the Cochrane Library.
| Author year | Random sequence generation | Concealment of the randomization sequence | Blinding of participants and staff | Blinding of outcome assessment | Lost data | Selective reporting of results | Other biases |
| 1. Abramovici A (2015), Secondary analysis of 2 multicenter trials | R.B. | R.B. | R.B. | R.B. | R.B. | R.B. | RM |
RA: High; RM: Medium; RB: Low
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



