
Submitted:
29 December 2023
Posted:
29 December 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The current context has proved unequivocally that public health is one of the pillars of society, playing a determining role and being a balancing factor. This study aimed to provide additional evidence supporting the use of geographic information systems in and from public health. For the study, the authors use public data from the Transparency COVID-19 data set at the Romanian level, which they process with the QGIS application, to effectively determine the influence of the location of the vaccination centers, respectively the impact on the incidence of COVID 19. The research carried out, which generated 153 maps, allows the statement, that reports based on the geographical location of data collected from the public health system are easier to analyze and to evaluate the effectiveness of the decisions taken. By analyzing the evolution of some public health indicators, that are difficult to correlate through analytical relationships, this study offers, as the main finding, an additional argument for the use of geographic information systems in public health management. As the limitations of research in the simulation component are relevant, further research is needed to provide the necessary evidence to convince about the effectiveness of using geographic information systems to optimize outcomes in the public health system. For this reason, it is necessary that the data structures in the public system, to be built and collected in a comprehensive way, with an optimal level of granularity.
Keywords:
GIS
; COVID19
; public health
; emergencies
1. Introduction and similar literature
Public health is a field of great interest for society, a statement that should not normally be justified, as it is axiomatic in nature. This statement can be made starting from the decision taken in 1945 by diplomats of the United Nations to establish the World Health Organization, followed in 1946 by the creation of the Constitution of the World Health Organization [1]. Probably as a result of this state of affairs many researchers have tried to approach issues in this field from various perspectives, seeking to find and propose solutions to improve the level of public health. In this regard, researchers have provided evidence of the relationship between public health and other domains in two ways, directly [2], when public health directly affects these other domains, or indirectly [3], when the other domains are affected by high resource consumption at the expense of others.
Thus, the concerns of researchers, but also of professionals involved in multidisciplinary fields can be grouped in several ways. The authors of this research use principles of the health care system, grouping the analysis carried out in two segments, the prevention of diseases, which in the case of this research can be understood as the analysis of the effects of problems in the public health system and the treatment of diseases, understood in this research as decision support for increasing the efficiency of the public health system. In the following two subsections, some of the research in this field are presented, grouped in the mentioned form.
1.1. Prevention - analysis of effects
Duarte et al. starting from the existing situation in Portugal managed to prove with the help of two GIS applications, opensource, and publicly available health data, that the processing of these data provides relevant results on the health situation of the population, implicitly on the effects of decisions in the public health system in Portugal. [4] Research of Duarte et al. proves the need for spatial analysis of health system data, also indicating some limitations in their approach.
Zhou et al. in their study on GIS and Big Data proved the importance of aggregating data from multiple sources for the purpose of spatial tracking of endemic domain information, an idea that arose following the outbreak of the COVID-19 pandemic. [5] A challenge for Zhou et al.’s research was data acquisition, as it is well known that timeliness and accuracy of data is one of the important requirements of a GIS.
One research demonstrating the usefulness of using epidemiological maps to analyze the effects of arboviral diseases in Honduras was conducted by Lysien et al. [6] In addition, through this research the authors presented the possibility of integrating public health policies with disease prevention and control strategies.
Nearly six months after the start of the COVID-19 pandemic Franch-Pardo et al. conducted an assessment of the extent to which the pandemic had spread geographically. [7] The assessment aimed to understand the socio-geographical implications of COVID-19 and implicitly represented another argument in favor of the use of GIS, of spatial analysis in the field of health.
1.2. Treatment – decision support
Pesaresi et al. used spatial analysis of data indicating a risk to public health from the effects of electromagnetic radiation, using data collected in northeast of Rome, to provide a contribution to the development of a system capable of supporting decision making in the public system. [8] The applications proposed by Pesaresi et al. eloquently complete the research circumscribed to medical geography and justify the need to use interdisciplinary analyses in the sense of using spatial analysis and risk analysis to support decisions that impact public health.
The finding regarding the increase in the number of Lyme disease cases and the potential correlation between this increase and natural factors of the fauna in eastern Ontario led Chen et al. to conduct GIS-based research to evaluate and then obtain results useful for public health management to prevent Lyme disease outbreaks. [9] The results of Chen et al.’s research succeed in clarifying to a good extend the correlation between deer habitat, the presence of ticks and the high rate of Lyme disease, a fact that increases the number of arguments in favor of using spatial analysis for better public health management.
Sarwar et al. used spatial analysis to analyze COVID-19 outbreak areas in Pakistan, with the aim of creating models used to simulate spread in early outbreaks for better countering virus spread. The result was to obtain realistic distributions of the virus using GIS simulation. [10]
Because surveillance and voluntary data collection represent essential elements in the strategy for shaping infectious disease management Saran et al. examined the importance of Geo surveillance for this aspect of public health. [11] Even if the other options available in developing such a strategy have led to reliable results, the authors managed to present the benefits of using geospatial technology, particularly in being able to link the appropriate disease environment to the disease itself.
2. Materials and Methods
2.1. Objective of the study
The objective of this study is to join other similar research, some of them presented in papers in Special issue GIS and Public Health Journal [12], the research of Geyer, N. R. et al. [13] or the conclusions of Xu, M. et al. [14], by adding additional elements to demonstrate the benefits of using spatial data analysis in public health. The main motivation for carrying out this study is given by reduced use of the tools offered by GIS for the management of the public health system, an opinion also supported by other researchers, as can be seen in Luan, H. et al. research. [15], but especially for the management of exceptional situations, such as the COVID-19 pandemic, which makes its presence felt even today. In addition, there are papers where researchers have presented with strong evidence the benefits of using GIS technology for assessing issues during the COVID-19 pandemic [16,17,18]. The development of a platform built on the principles of GIS technology, which can become the foundation of a digital Atlas of health services at the level of a country, circumscribes the objective of this study. This statement can be made even if the idea of a platform that includes resources and tools capable of allowing an increase in the performance of the public health system has not been stated in this way and as a result of the results obtained by other researchers, such as Xu, D. et al. [19] or Adibhesami, M.A. et al. [20]. In the study the authors use spatial analysis of data on SARS-CoV-2 infection and vaccination against COVID-19 to assess the effects and effectiveness of decisions in the COVID-19 pandemic management campaign in Romania, by comparing the evolution of a set of indicators, in order to observe whether the location of vaccination centers had a real effect in localized areas. In this respect the authors chose to divide the study objective issue into the following sub-objectives:
SO1 Analyzing the effects of public health decisions using GIS
SO2 Using GIS to support public health management.
2.2. Hypotheses of the study
The authors start from the premise that the existing data structures in cases of this kind, where the comparative tracking of the evolution of various parameters and their influence is difficult to do if the data are presented in tabular form. Usually, because the data used are part of multidimensional matrices, in such cases customized IT solutions are used, which unfortunately bring limitations, such as high price, high customization, and others. In this case such software solutions are more difficult to use because they aim at comparing different data sets, which need an aggregator to draw conclusions. Translating tabular data collections into graphs is a step forward in easing the analysis of the evolution of the data, from the sets that are used, but which in turn are limited by the same issue, the comparison of different data sets.
The study presented in this paper is substantiated by the researchers on two hypotheses, which correlate with the philosophy used by the authors in conducting the research presented in the introductory chapter.
H1 The correlation of the data collected from the public health system with the geographical location allows obtaining reports that are easier to analyze in order to evaluate the effectiveness of the decisions taken.
H2 The use of models based on geographic location allows management structures in the public health system to optimize system outcomes.
2.3. Methods of investigation
For the study, the authors use public data available on the data.gov.ro portal, maintained by the Romanian Government, namely the COVID-19 Transparency dataset at the Romanian level. [21] Within this dataset, general information entitled Transparency and COVID-19 vaccination information entitled Vaccination Transparency are made available to the public. The indicators found in these datasets and used in the investigation are: incidence of COVID-19, PCR tests, admissions to ICU (Intensive Care Unit) wards, deaths, and vaccinations. Due to the fact that on the government portal data for the above mentioned indicators are available every month starting from March 2021, but about vaccinations only for two months, March and April 2021 from which only March 2021 is complete, the analysis in this research is performed only for this month, March 2021. The existing data on the government portal is provided in xlsx format, the default format for Microsoft Excel since version 2007, a format based on the XML (Extensible Markup Language) database model [22]. Consequently, the authors, using a Microsoft Excel spreadsheet editor, extracted data on the incidence of COVID-19, PCR tests, admissions to ICU wards, deaths, and vaccinations, for the period 1 March 2021 - 31 March 2021, producing the information package required for the investigation. From this package, using the same tabular calculation editor, tables with data and charts showing the evolution by day and county of the five indicators were obtained. As for the GIS project, it was realized using QGIS 3.26 [23] and geospatial data structures related to Romania, border, administrative territorial units, counties, and localities, available in the public space, most of them found in geo-spatial.org archives. [24] The authors use all these data to build maps that graphically highlight the daily evolution of the five indicators at national level, the 14-day incidence at territorial administrative unit level, the number of vaccinations, deaths, PCR tests and the number of people admitted to ICU wards at county level. The maps created by the authors are heatmaps [25] for the mentioned indicators and include, with a discrete representation in the form of dots, the location of vaccination centers at national level, in order to assess the evolution of the indicators as accurately as possible. It is important to mention that the GIS project is configured for a reference system EPSG:31700 – (Dealul Piscului 1970/Stereo 70).
3. Results and Discussions
As mentioned in subchapter 2.3, the data processing allowed to obtain collections of tables, charts and maps.
Regarding the collection of tables, the existing information in the source data structures on the governmental portal data.gov.ro, related to the indicators used for the investigation, allowed the creation of five tables, which can be consulted in detail in Appendix 1. These tables are: Incidence by counties between March 1-31, 2021. (Cases per one thousand inhabitants in the last 14 days.), Tests conducted by counties between March 1-31, 2021, Deaths reported by counties between March 1-31, 2021, Persons hospitalized at ICU by counties between March 1-31, 2021, and Vaccinations by counties between March 1-31, 2021. The tables are in the format found in Table 1 or Table 2.
In order to obtain graphical reports based on spatial analysis, the processing of data collected from the governmental portal data.gov.ro allowed the creation of 153 maps, meaning 5 sets of maps with the evolution of the indicators monitored in the 31 days. The process of processing the available data involved two stages. As a result of the fact that vaccination information was provided at the level of vaccination centers, which in the vast majority were more than one at the level of administrative territorial units, in the first phase it was necessary to cumulate vaccination data by day at the level of administrative units. After this stage, all the data structures were added to the QGIS project [26], resulting in 153 maps. The analysis proposed in this case is based on the philosophy of tracking the simultaneous evolution of the 5 indicators, presented in heatmap maps. For this comparison to be effective, it is considered that public health specialists, in their analysis for the calculation of the incidence of infections, used the 14-day interval. At the same time, several product datasheets for COVID-19 vaccines, published on the European Medicines Agency [27] portal, were consulted and it was found that the general rule is that vaccinated persons are not fully protected until 14 days after the second dose of vaccination. As a result of this, the graphical charts for the analysis were built for the interval March 15 2021 - March 31 2021 for all indicators except the vaccination indicator, which was delayed by 14 days, it being included in the chart for the interval March 1 - 14 2021.All the maps displayed in the comparative diagram show a value gradient with the minimum and maximum limits of the monitored indicator, in order to provide a correlation between image and value. The evolution of the monitored indicators over the whole mentioned time interval can be seen in full in Appendix 2, Figure 1, Figure 2 and Figure 3 showing the beginning, middle and end of the time interval. In the complete collection of information related to this research, published in the GitHub digital repository [26], you can also find an animation showing the evolution of the 5 indicators per day.
The diagram-type reports, obtained by processing the data related to the 5 indicators, are equal in number to the monitored indicators and allow the observation of the evolution of these indicators at the level of each county in the interval 1 - 31 March 2021. The evolution of the incidence by county is presented in Figure 4, and the rest of the diagrams can be seen in Appendix 3.
From the analysis of the obtained reports, it can be seen that the tabular form of data presentation is capable of providing a good picture of the evolution compared by day, at county level or even compared between counties, as a result of the fact that the figures presented in the table are eloquent for the intended purpose. The diagram-type reports are superior to tabular reports, although the values are not explicitly displayed, but because the evolution per day, at county level, is easy to compare visually. Both types of reports have the weakness caused by the difficulty in comparing the simultaneous evolution of the five indicators.
The reports that are presented in the form of heatmaps maps are the most capable of providing a clear picture of how the five indicators change their values simultaneously over time, so that it can be understood whether the evolution of the values at the level of one of the indicators has an echo in the evolutions at the level of the other indicators. It is found that areas with a large number of vaccination centers, which are in fact also important territorial administrative units, have favorable developments of the indicators, in the sense that the incidence increases moderately, simultaneously with the number of PCR tests, the number of deaths is decreasing and the number of persons hospitalized at ICU remains low. Examples can be seen in Appendix 2, in the western part of Romania, where there are two important counties, Timis and Arad, or in the central-western part of Romania, where Cluj County is located.
As a result of the fact that the volume of data is limited to one month, as shown in this paper, the possibilities to determine the influential inter-indicators are limited and practically difficult to apply. Consequently, in order to verify the possibilities of using the analysis based on the use of a geographic information system in the simulation process, the authors identified a way in which by changing one indicator a result is obtained that influences another indicator. The authors introduced, through simulation, an increase in the number of daily vaccinations with a total of 30,000 vaccinations at the level of each county. This total was distributed at the level of territorial administrative units in proportion to the number of vaccinations carried out in real terms, obtaining a new total of vaccinations at the level of territorial administrative unit, which is used in the proposed simulation.
It is considered that at the level of territorial administrative units, the conditions that lead to illness remain the same. The newly created situation by increasing the number of vaccinations leads to a reduction in the number of residents susceptible to being infected with COVID-19, as a result of the fact that vaccinated people become immune after 14 days, as mentioned in this paper.
As a result of the described framework for the simulation, the authors determined the relationship between the calculated incidence (i) and the number of people likely to get sick (l) from COVID-19. This number (l) is determined by excluding vaccinated persons (v), already infected persons (e) and deceased persons (d) from the total population (p) at the level of the territorial administrative unit (2). Theoretically, only these people can get sick with COVID-19. Using this principle, the authors determined the ratio between the incidence and the number of people likely to get sick with COVID-19 (3). This ratio is used to determine the new incidence, which could be achieved by increasing the number of vaccinations (v1) and implicitly by decreasing the number of people susceptible to the disease. Another incidence value (i1) is determined in this way (4).
s = p x i/1000
l = p – (s + v + d)
i = ((p – l – v – d) x 1000)/p
i1 = ((p – l – v1 – d) x 1000)/p
Which are: s – sick; i – incidence; p – population; l – susceptible to illness; d - deceased; v – vaccinated; v1 – increased vaccination; i1 – incidence after increase vaccination
For example, you can see the new values in Table 3.
In the QGIS project, the values obtained at the level of all territorial administrative units were used and the "Incidence with simulated increase of vaccination maps" maps were obtained.
Figure 5, Figure 6 and Figure 7 show in parallel the maps obtained with the actual incidence and the maps with the incidence obtained by increasing the number of vaccinations. It can be seen that the high incidence areas are smaller in size, the positive impact on the number of illnesses being obvious. Unfortunately, the lack of a larger volume of data limited the ability to determine interdependencies that can be used for further simulations.
Basically, in accordance with the objectives of the study and starting from the hypotheses on which the research is based, two results emerge that validate these hypotheses to a good extent:
R1 The maps obtained by assigning geographical characteristics to the data collected from the public health system allow the simultaneous observation of the effects and impact over the whole country, at one-day intervals, with the possibility of assessing the situation for the indicators used, direct comparison and monitoring of the daily evolution.
R2 The evolution of the indicators used generates a picture of the trend which, together with the proposed model, constitutes the support for making the forecast. Using this model, by modifying various parameters, such as increasing the number of tests, increasing, or decreasing the number of vaccinations, possibly opening, or closing vaccination centers decision-making efficiency can be improved.
4. Conclusions, further research
The research explicitly provides the image of the monitoring efficiency based on geographic information systems, for five sets of indicators, without a determinable correlation and regarding the influence of the location of vaccination centers on Romanian territory. As a result, it can be stated that the public health system, which must always complete its set of analysis tools, must also include GIS among them. Regarding the use of this mode of analysis to perform simulations on the establishment or abolition of vaccination centers, the research does not provide an indisputable answer due to the limited possibility of creating a potential model of influencing the indicators on each other. The conducted study presents a limitation as a result of the fact that on the data.gov.ro portal only the month of March 2021 is complete with regard to the information related to vaccinations at the national level. This limitation affects R2 to a greater extent because it limits the amount of forecast capability. Even so, one can extract a trend and use the obtained result. It is obvious that a research using a dataset that covers a longer time span would provide results with a higher conclusiveness. In future research, it is considered that the proposed model will be applied by supplementing this type of information with information about residence, type of professional activity, but also with a greater granularity of data. This information has a relevant impact considering the contagiousness of the disease. It is not without importance that, if one or more additional indicators or with a greater granularity would appear in the research, which would provide additional elements on the treatments carried out, on the consumption of resources necessary for the cure, possibly on the effects that follow. hospital discharges, could lead to much more eloquent images for a better management of situations such as the one created by the COVID-19 pandemic. This is the direction of future research that the authors wish to continue, to demonstrate the undeniable ability of GIS technology to support applied management in the public health system and implicitly to perform simulations and forecasts, by using more extensive and accurate, complex tools, able to remove the limitation present in this research. In this way, the authors intend to strengthen the idea that the development of a Geographical Information System applied in Public Health can and must lead to the realization of a Digital Atlas of Health Services.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Appendix 1, Appendix 2, Appendix 3.
Author Contributions
Conceptualization, L.D.L.; methodology, L.D.L.; software, L.D.L.; validation, L.D.L. and E.E.; formal analysis, L.D.L.; investigation, L.D.L.; resources, L.D.L.; data curation, L.D.L.; writing—original draft preparation, L.D.L.; writing—review and editing, L.D.L.; visualization, E.E.; supervision, L.D.L.; project administration, L.D.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The authors have created a repository that can be found at: https://github.com/lucianlupu/digital_atlas_health. In this repository, which is openly accessible, all data downloaded from the Open Datasets of the Romanian government, geospatial datasets, intermediate data structures necessary for final processing and the QGIS project are available. In the same warehouse, the animation in which the evolution of the five indicators can be followed is made available to the public. This animation is accessible at: https://github.com/lucianlupu/digital_atlas_health/blob/main/evolution%20animation%2015-31.gif.
Acknowledgments
The authors thank the geo-spatial.org community for their constant and ongoing concern to advance GIS technology.
Conflicts of Interest
The authors declare no conflict of interest.
References
- ***, https://www.who.int/about/history, History of World Health Organization, accessed on 21 august 2022.
- Osypuk TL, Joshi P, Geronimo K, Acevedo-Garcia D. Do Social and Economic Policies Influence Health? A Review. Curr Epidemiol Rep. 2014 Sep 1;1(3):149-164. [CrossRef]
- Marc Suhrcke, Martin McKee, Regina Sauto Arce, Svetla Tsolova, Jørgen Mortensen, The contribution of health to the economy in the European Union, Luxembourg: Office for Official Publications of the European Communities, 2005, ISBN 92-894-9829-3, https://ec.europa.eu/health/archive/ph_overview/documents/health_economy_en.pdf, accessed on 31 august 2022.
- Duarte, L.; Teodoro, A.C.; Lobo, M.; Viana, J.; Pinheiro, V.; Freitas, A. An Open Source GIS Application for Spatial Assessment of Health Care Quality Indicators. ISPRS Int. J. Geo-Inf. 2021, 10, 264. [Google Scholar] [CrossRef]
- Chenghu Zhou; Fenzhen Su; Tao Pei; An Zhang; Yunyan Du, Bin Luo; Zhidong Cao; Juanle Wang; Wen Yuan; Yunqiang Zhu; Ci Song; Jie Chen; Jun Xu; Fujia Li; Ting Ma; Lili Jiang; Fengqin Yan; Jiawei Yi; Yunfeng Hu; Yilan Liao; Han Xiao, COVID-19: Challenges to GIS with Big Data, Geography and Sustainability, Volume 1, Issue 1, 2020. [CrossRef]
- Lysien I. Zambrano; Manuel Sierra; Bredy Lara; Iván Rodríguez-Núñez; Marco T. Medina; Carlos O. Lozada-Riascos; Alfonso J. Rodríguez-Morales, Estimating and mapping the incidence of dengue and chikungunya in Honduras during 2015 using Geographic Information Systems (GIS), Journal of Infection and Public Health, Volume 10, Issue 4, 2017. [CrossRef]
- Ivan Franch-Pardo; Brian M. Napoletano; Fernando Rosete-Verges; Lawal Billa, Spatial analysis and GIS in the study of COVID-19. A review, Science of The Total Environment, 2020. [CrossRef]
- Pesaresi, C.; Pavia, D. Radio Base Stations and Electromagnetic Fields: GIS Applications and Models for Identifying Possible Risk Factors and Areas Exposed. Some Exemplifications in Rome. ISPRS Int. J. Geo-Inf. 2021, 10, 3. [Google Scholar] [CrossRef]
- Chen, D.; Wong, H.; Belanger, P.; Moore, K.; Peterson, M.; Cunningham, J. Analyzing the Correlation between Deer Habitat and the Component of the Risk for Lyme Disease in Eastern Ontario, Canada: A GIS-Based Approach. ISPRS Int. J. Geo-Inf. 2015, 4, 105–123. [Google Scholar] [CrossRef]
- Suleman Sarwar; Rida Waheed; Sahar Sarwar; Aisha Khan, COVID-19 challenges to Pakistan: Is GIS analysis useful to draw solutions?, Science of The Total Environment, Vol. 730, 2020, 139089. [CrossRef]
- Saran, S., Singh, P., Kumar, V. et al. Review of Geospatial Technology for Infectious Disease Surveillance: Use Case on COVID-19. J Indian Soc Remote Sens 48, 1121–1138 (2020). [CrossRef]
- Bertazzon, S. GIS and Public Health. ISPRS Int. J. Geo-Inf. 2014, 3, 868–870. [Google Scholar] [CrossRef]
- Geyer, N.R.; Lengerich, E.J. LionVu: A Data-Driven Geographical Web-GIS Tool for Community Health and Decision-Making in a Catchment Area. Geographies 2023, 3, 286–302. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Cao, C.; Wang, D.; Kan, B. Identifying Environmental Risk Factors of Cholera in a Coastal Area with Geospatial Technologies. Int. J. Environ. Res. Public Health 2015, 12, 354–370. [Google Scholar] [CrossRef]
- Luan, H.; Law, J. Web GIS-Based Public Health Surveillance Systems: A Systematic Review. ISPRS Int. J. Geo-Inf. 2014, 3, 481–506. [Google Scholar] [CrossRef]
- Fernandez, G.; Maione, C.; Yang, H.; Zaballa, K.; Bonnici, N.; Carter, J.; Tsou, M.-H. COVID-19 Societal Effects and Perceptions: A Case Study of Italy. Med. Sci. Forum 2023, 19, 10. [Google Scholar] [CrossRef]
- Oluyomi, A.O.; Gunter, S.M.; Leining, L.M.; Murray, K.O.; Amos, C. COVID-19 Community Incidence and Associated Neighborhood-Level Characteristics in Houston, Texas, USA. Int. J. Environ. Res. Public Health 2021, 18, 1495. [Google Scholar] [CrossRef] [PubMed]
- Faisal, K.; Alshammari, S.; Alotaibi, R.; Alhothali, A.; Bamasag, O.; Alghanmi, N.; Bin Yamin, M. Spatial Analysis of COVID-19 Vaccine Centers Distribution: A Case Study of the City of Jeddah, Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 3526. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Wu, Q.; Feng, Y.; Wu, S. COVID-19: Evaluation of Fever Clinic and Fever Sentinel Configuration—A Case Study of Harbin, China. Sustainability 2022, 14, 9117. [Google Scholar] [CrossRef]
- Adibhesami, M.A.; Karimi, H.; Sharifi, A.; Sepehri, B.; Bazazzadeh, H.; Berardi, U. Optimization of Urban-Scale Sustainable Energy Strategies to Improve Citizens’ Health. Energies 2023, 16, 119. [Google Scholar] [CrossRef]
- Seturi de date deschise, https://data.gov.ro/dataset/transparenta-covid, accesed on 12 july 2022.
- ***, File formats that are supported in Excel, https://support.microsoft.com/en-au/office/file-formats-that-are-supported-in-excel-0943ff2c-6014-4e8d-aaea-b83d51d46247, accesed on 21 july 2022.
- ***, QGIS, https://qgis.org/en/site/forusers/download.html, accesed on 24 july 2022.
- ***, https:// geo-spatial.org, , accesed on 15 july 2022.
- Leland Wilkinson & Michael Friendly The History of the Cluster Heat Map, The American Statistician, 63:2, 179-184, (2009). [CrossRef]
- https://github.com/lucianlupu/digital_atlas_health.
- ***, COVID-19 Vaccine – COVID-19 Vaccine - SUMMARY OF PRODUCT CHARACTERISTICS (European Medicines Agency), https://www.ema.europa.eu/en/documents/product-information/covid-19-vaccine-inactivated-adjuvanted-valneva-epar-product-information_en.pdf, accesed on 22 july 2022.
Figure 1.
Vaccination map on March 1, 2021, Deaths, Admissions, Incidence, PCR tests on March 15, 2021.
Figure 1.
Vaccination map on March 1, 2021, Deaths, Admissions, Incidence, PCR tests on March 15, 2021.
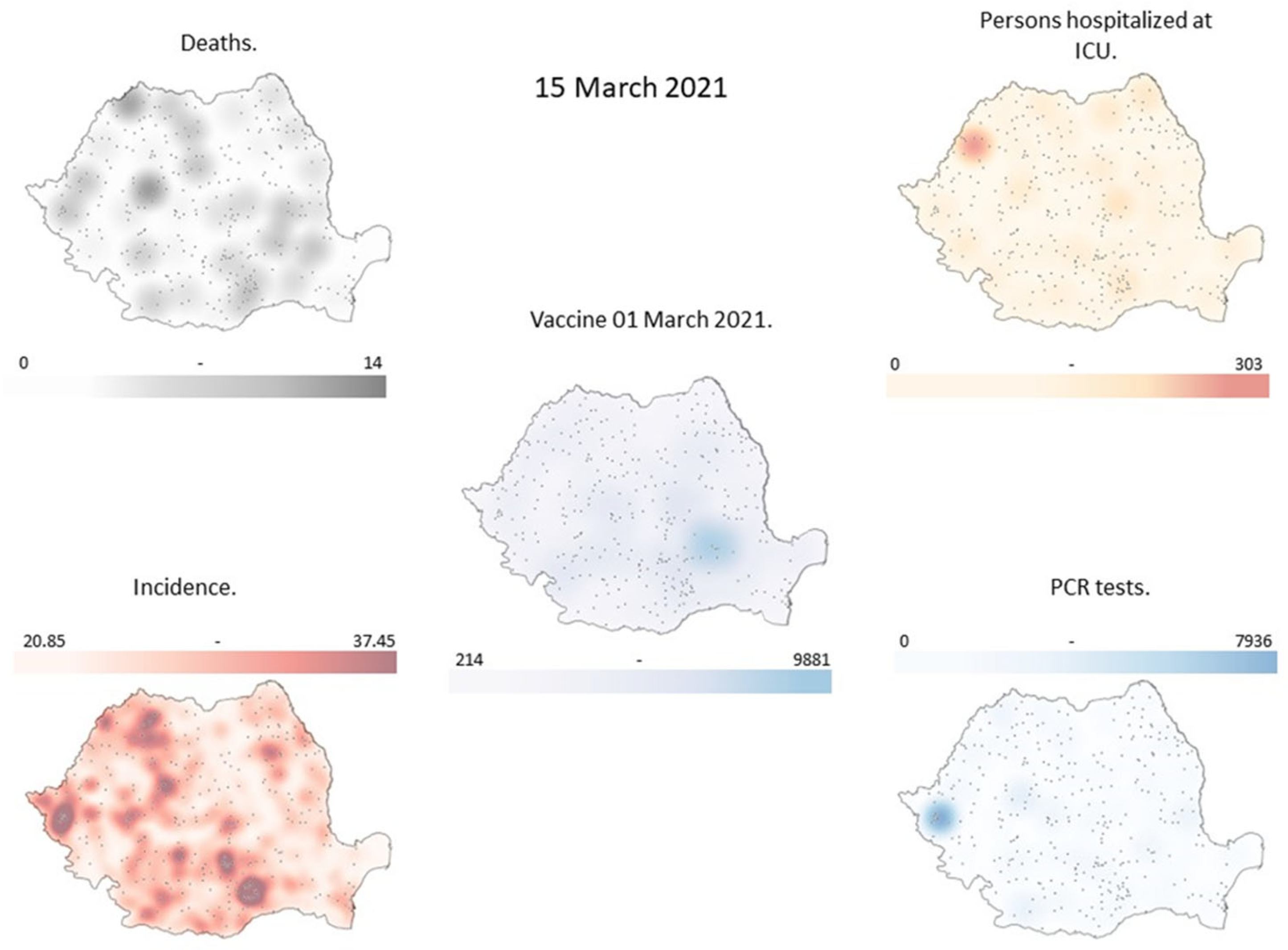
Figure 2.
Vaccination map on March 9, 2021, Deaths, Hospitalizations, Incidence, PCR tests on March 23, 2021.
Figure 2.
Vaccination map on March 9, 2021, Deaths, Hospitalizations, Incidence, PCR tests on March 23, 2021.
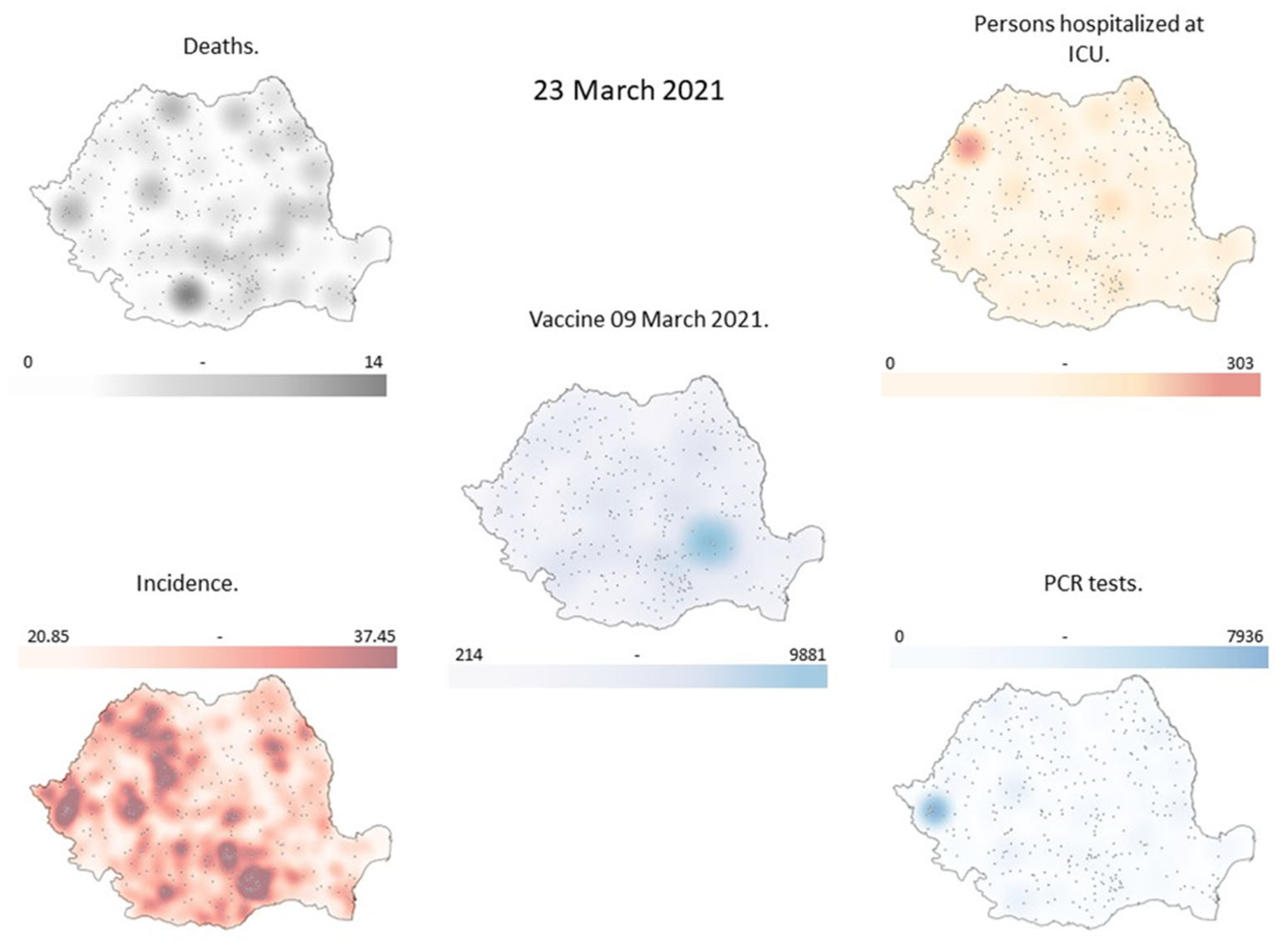
Figure 3.
Vaccination map on March 17, 2021, Deaths, Hospitalizations, Incidence, PCR tests on March 31, 2021.
Figure 3.
Vaccination map on March 17, 2021, Deaths, Hospitalizations, Incidence, PCR tests on March 31, 2021.
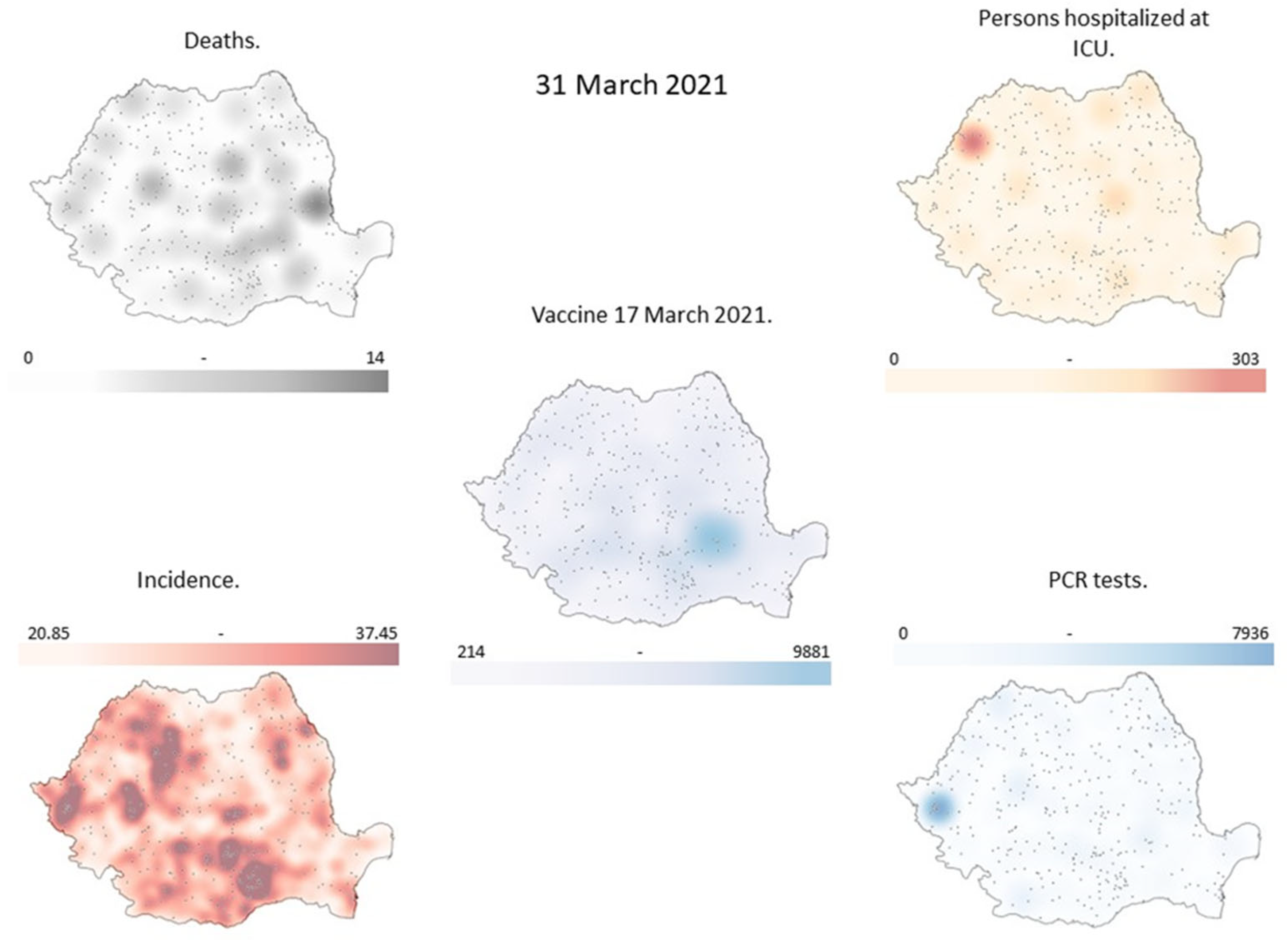
Figure 4.
The incidence of COVID-19 in March 2021 by county.
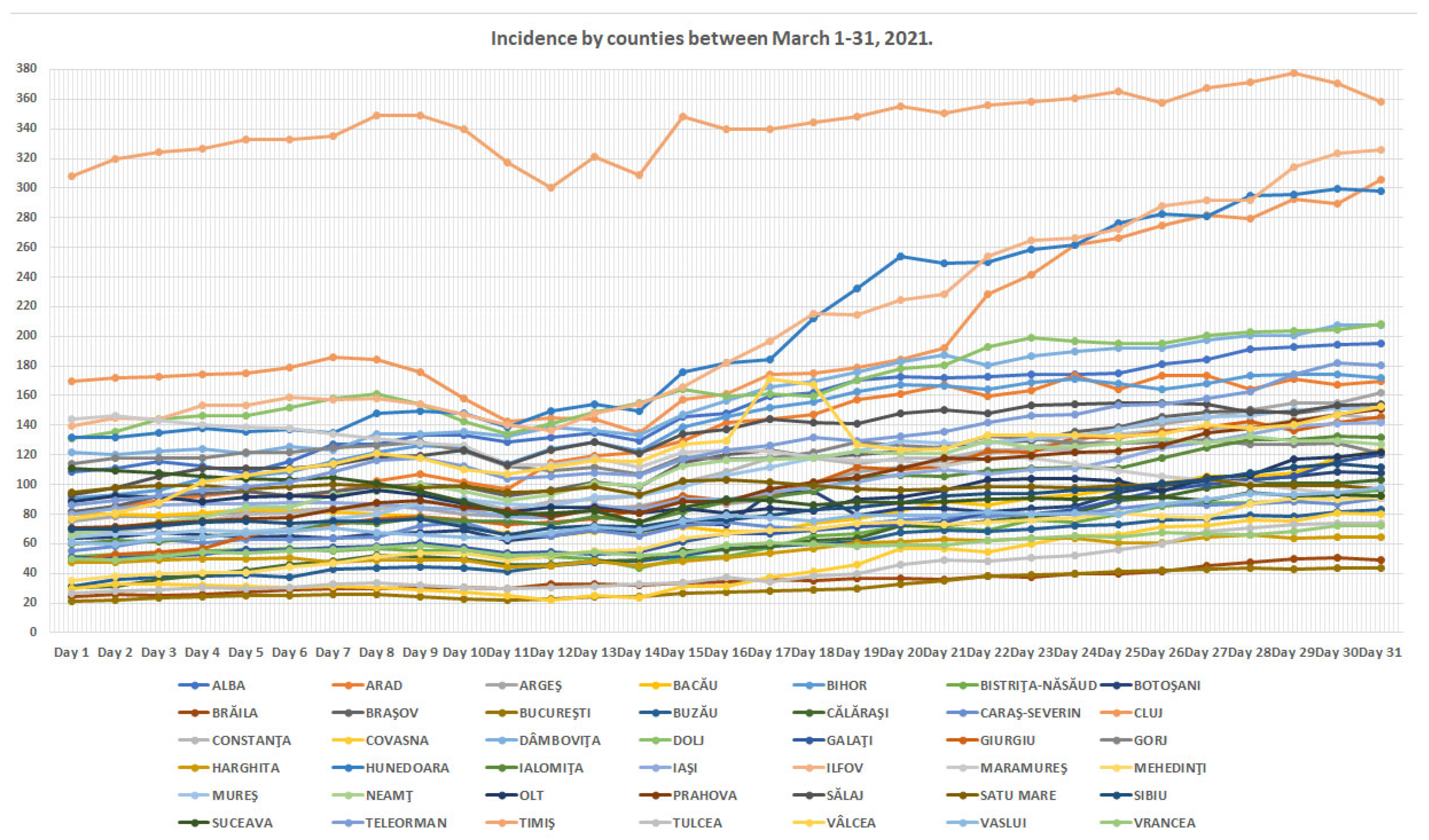
Figure 5.
Incident map for March 15, 2021 with actual values and values used in the simulation.
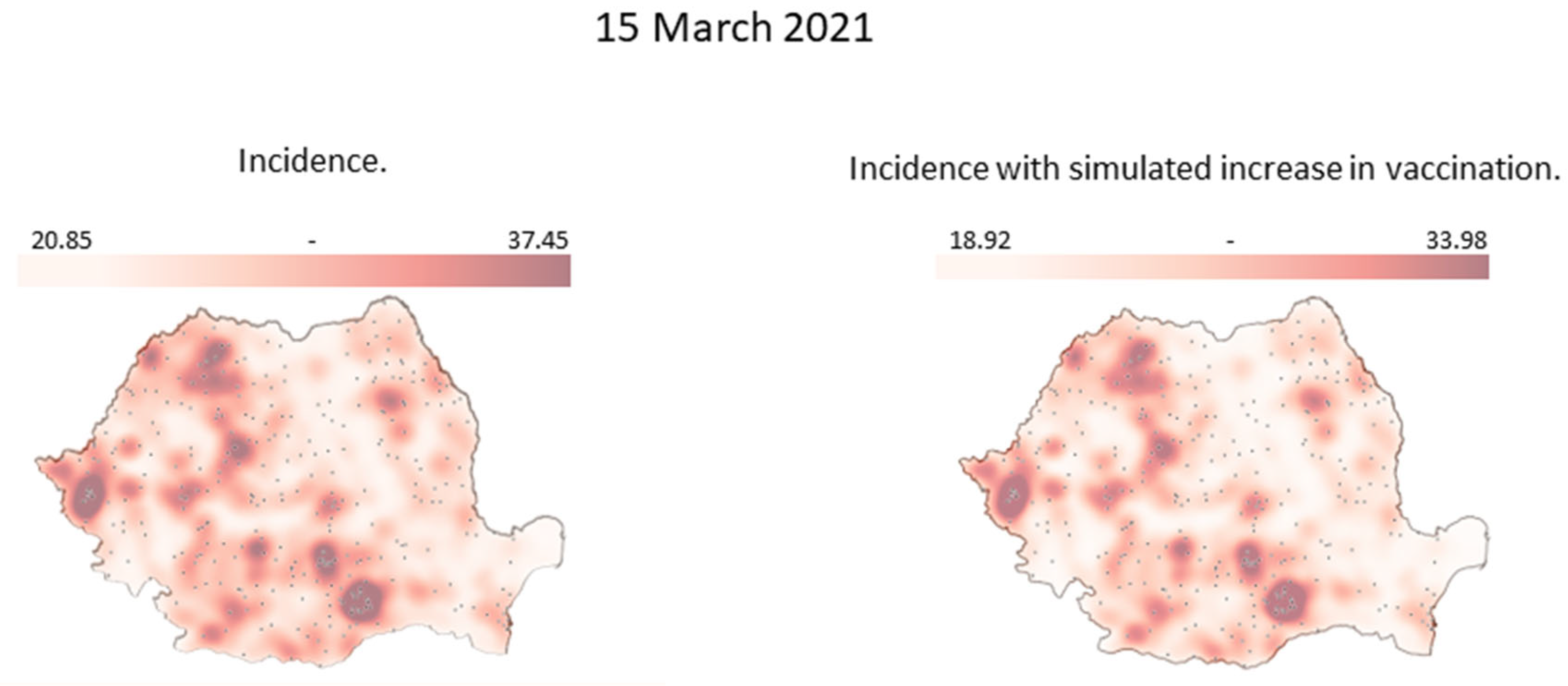
Figure 6.
Incident map for March 23, 2021 with actual values and values used in the simulation.
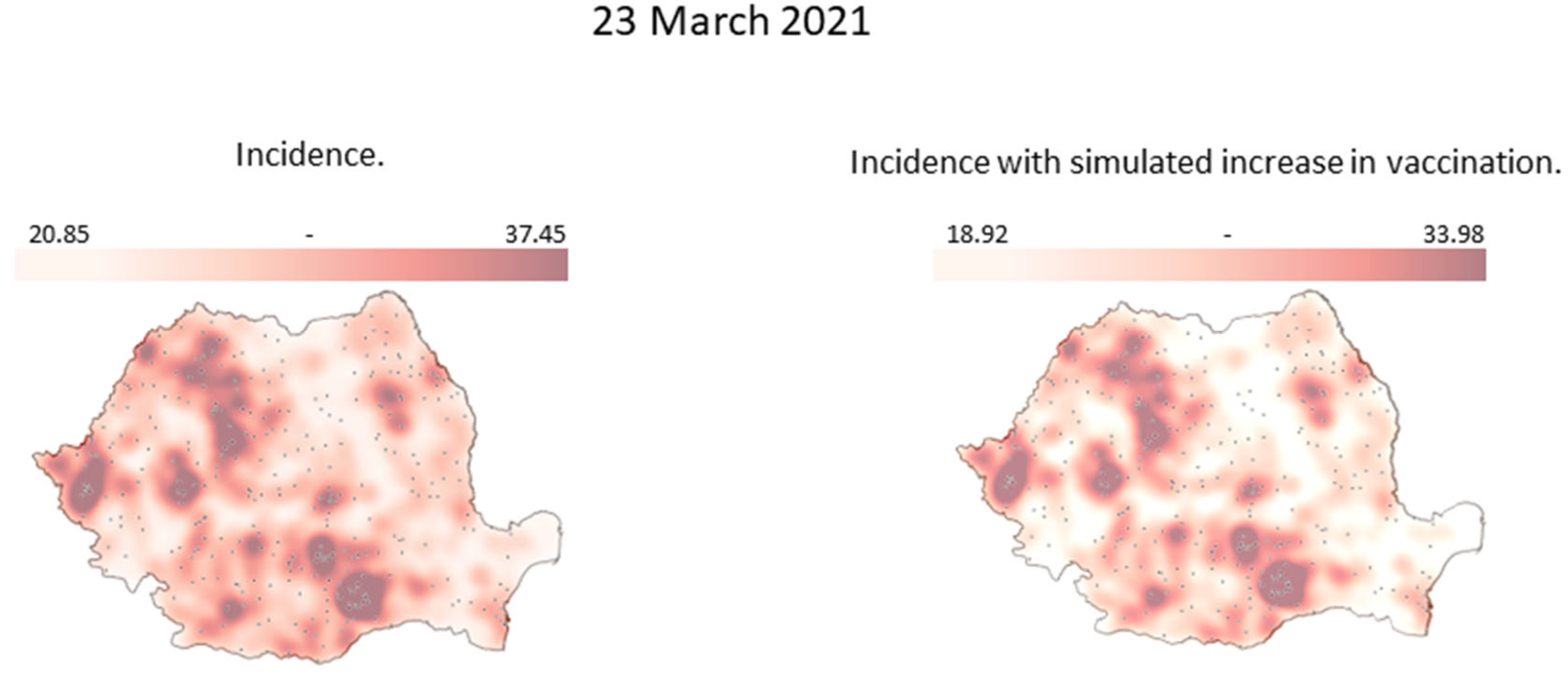
Figure 7.
Incident map for March 31, 2021 with actual values and values used in the simulation.
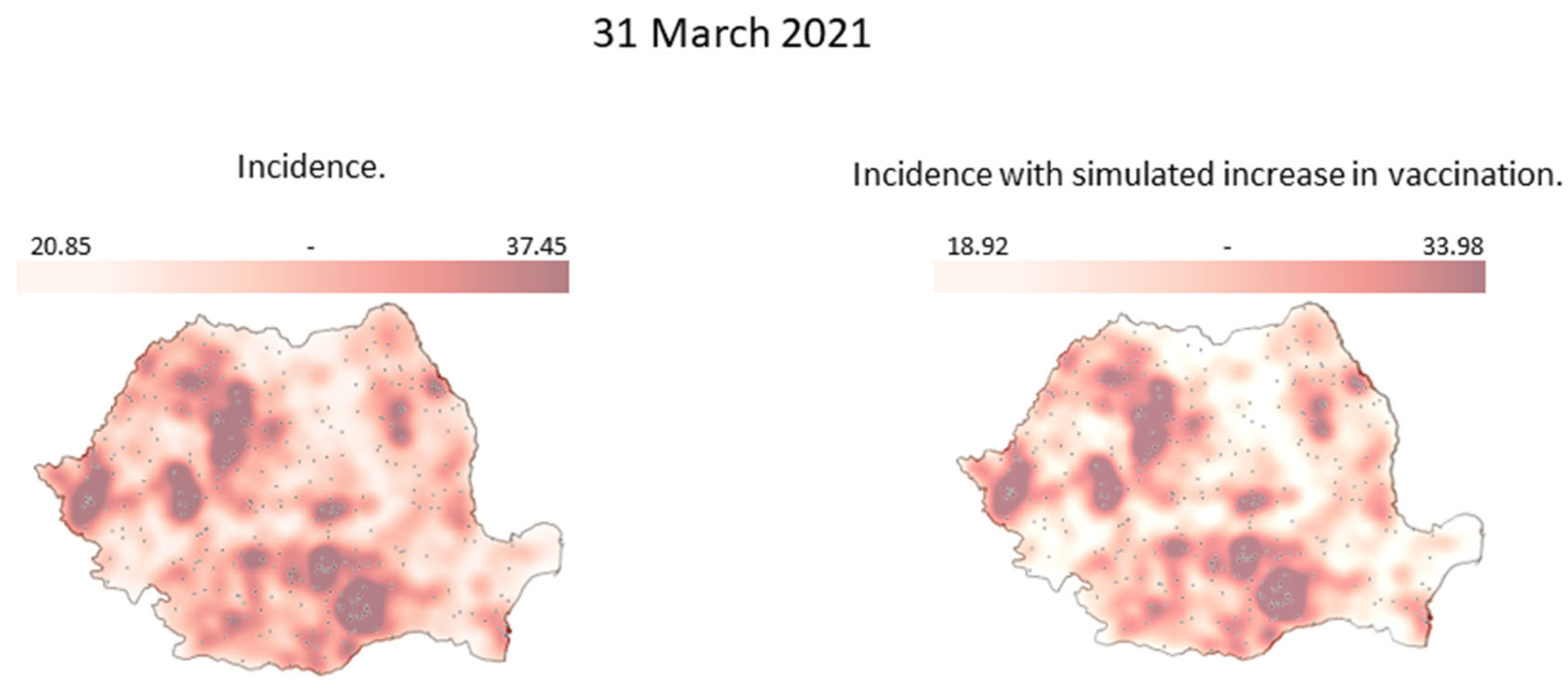

Table 1.
Incidence by counties between March 1-31, 2021. (Cases per 1000 inhabitants in the last 14 days.)
Table 1.
Incidence by counties between March 1-31, 2021. (Cases per 1000 inhabitants in the last 14 days.)
| COUNTY | Day 1 | Day 2 | Day … | Day 31 |
|---|---|---|---|---|
| ALBA | 108.6217157 | 110.9866 | … | 194.9185 |
| ARAD | 81.81863005 | 84.23531 | … | 169.8906 |
| … | … | … | … | … |
| VRANCEA | 49.9770577 | 48.66565 | … | 72.30731 |
Table 2.
Vaccinations by counties between March 1-31, 2021.
| COUNTY | Day 1 | Day 2 | Day … | Day 31 |
|---|---|---|---|---|
| ALBA | 851 | 819 | … | 961 |
| ARAD | 734 | 732 | … | 1568 |
| … | … | … | … | … |
| VRANCEA | 459 | 504 | … | 852 |
Table 3.
The new incidence obtained from the simulated increase in vaccinations per county between March 15-31, 2021. (Cases per 1000 inhabitants in the last 14 days.)
Table 3.
The new incidence obtained from the simulated increase in vaccinations per county between March 15-31, 2021. (Cases per 1000 inhabitants in the last 14 days.)
| COUNTY | Day 15 | Day 23 | Day … | Day 31 | |
| ALBA | 129,9929236 | 154,4271419 | … | 170,9672358 | |
| ARAD | 118,5443343 | 148,7452991 | … | 154,2532665 | |
| … | … | … | … | … | |
| VRANCEA | 48,73829657 | 57,24509257 | … | 65,06476179 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



