Submitted:
28 December 2023
Posted:
03 January 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
COVID-19 affected health and wellbeing globally. Graduating nursing students face a variety of stressors and entering the nursing profession during the pandemic added additional stress. Mood, perceived stress, resilience, and coping were assessed in an Australian sample of 112 graduating nursing students, who completed the Brunel Mood Scale (BRUMS), Perceived Stress Scale (PSS-4), and Brief Resilient Coping Scale (BRCS). Mean BRUMS scores for tension, fatigue, and confusion were significantly above population norms, and vigour scores significantly below. Mean PSS-4 scores were reflective of population norms, but showed higher levels of stress for younger and on-campus students compared to those who were older or who studied externally. BRCS data showed that 82.1% of the graduating nursing students were medium or high resilient copers. Mood profiles suggested that 19.6% of participants had elevated mental health risk, 23.2% showed potential risk of burnout, and only 17.9% reported mood profiles associated with positive mental health. High mean tension scores reported by the graduating nursing students indicated apprehension about joining the profession, although stress, resilience and coping scores suggested they were adequately managing the additional stressors generated by a global pandemic.
Keywords:
Affect
; coping
; COVID
; emotion
; feeling
; mood
; nurse
; stress
1. Introduction
Nurses form the largest body of health care professionals in Australia and, while the nursing workforce continues to grow annually, the profession still experiences a chronic shortage of registered nurses [1]. Alarmingly, survey data from the Australian Primary Health Care Nurses Association (APNA) showed that 86.7% of more than 1,000 of its members felt stressed at work, 78.8% felt burnt out, and 28.7% planned to leave their current job within the next 2 to 5 years [2], leaving the long-term sustainability of the nursing profession in Australia under threat. Further, a large-scale study of more than 46,000 full-time clinical nurses in Taiwan found that perceived job stress and depressed mood were significant predictors of nurses’ intention to leave the profession [3], indicating that the sustainability challenge extends internationally.
The advent of the COVID-19 pandemic in 2020 exacerbated the stress on nursing professionals and negatively impacted mental health globally, triggering a 25% increase in the prevalence of anxiety and depression worldwide [4]. There is no reason to assume that nursing students, who represent a critical pipeline of new nursing professionals to sustain an adequate workforce, would be immune to such effects. Indeed, an investigation into the effects of the pandemic on the mental wellbeing of 305 final-year nursing students at three Spanish universities found that risk of mental health issues had more than doubled from pre-pandemic levels [5]. The authors highlighted the need to prepare students for pandemic situations due to their impact “on the mental health of both the members of the public who will be treated by these future nursing professionals and the students themselves” (p. 694).
Nursing students not only have to cope with the usual stressors associated with university study, such as academic pressure, financial stress, and poor self-care [6] but typically also experience anxiety about entering the clinical workforce [7]. When additional stressors related to the pandemic, which have been shown to increase the risk of mental ill-health [8] are added to the equation, coping becomes more challenging. It has even been suggested that the pandemic caused some nursing students to feel they had to choose between pursuing a nursing career and safeguarding the health of their homes and loved ones [9].
Further, a meta-analysis of 27 cross-sectional studies [7] showed a high prevalence of depression (34%) among nursing students generally, with younger nursing students (< 25 yr.) showing a significantly higher prevalence (41%) than their older counterparts (18%), and Asian nursing students showing the highest prevalence of depression (43%) among geographical groups. Evidence from Portugal related to the transition to professional life of senior nursing students during the pandemic [10] showed that COVID-19 created diverse stressors ranging from “general social risks and fears of the unknown to the more concrete situations related to class interruptions that can postpone the course completion” (p. 5). However, students were equally concerned about non-pandemic issues related to applying their theoretical knowledge in professional practice contexts, particularly in areas such as safe medication administration, communication with multidisciplinary teams, and the fear of making mistakes that could harm patients. Given that nursing students are the nursing professionals of the future, the mental health of graduating nursing students is of particular interest to those concerned about the sustainability of health systems internationally [7].
Mood profiling is a common method for monitoring mental health status in a wide variety of contexts [11,12,13,14]. Within medical settings, mood profiling has been used, for example, to monitor the psychological wellbeing of cardiac rehabilitation patients [15] and those recovering from prostate surgery [16]. Among nurses, mood profiling has been used previously to assess the effects of shift work on mood states [17,18]. Collectively, previous findings suggest that the moods of nursing students, particularly scores on the tension and depression subscales, may not only indicate risk of mental health issues but also flag risk of poorer clinical care. To assess whether the alarming rates of mental health concerns found among nurses and nursing students in other parts of the world were replicated in Australia, the primary aim of the present study was to assess mood, stress, resilience, and coping among graduating nursing students entering the profession during a global pandemic. A secondary aim was to test whether mood, stress, resilience, and coping scores varied according to the demographic characteristics of the sample. Given that mood scores have previously been shown to vary according to the gender, age, residency status, and study mode of students in the Australian higher education sector during the pandemic [19], the group analyses in the present study included those demographic variables. Finally, employment status among graduating nursing students in Australia has been shown to be a predictor of mental health status [20] and therefore a comparison of participants who had secured employment and those who had not was included in the analyses.
2. Materials and Methods
2.1. Participants
Purposive sampling was used to recruit nursing students due to graduate from an undergraduate nursing program in Queensland, Australia and enter the profession as registered nurses. Nursing students at an earlier stage of their program were excluded from the study. A total of 112 graduating nursing students completed the survey (female = 98, 87.5%; male = 14, 12.5%) ranging in age from 20 to 69 yr. (M = 33.3, SD = 11.4 yr.). A total of 88 were domestic students (78.6%) and 24 were international students (21.4%); 56 studied on-campus (50%) and 56 studied externally (50%); 81 studied full-time (72.3%) and 31 studied part-time (27.7%). Fifty-one participants (45.5%) had already secured employment as a nurse pending their graduation, whereas 61 (54.5%) had yet to find employment.
2.2. Measures
2.3.1. Mood
Mood was assessed using the Brunel Mood Scale (BRUMS) [21,22], a 24-item scale to assess the six mood dimensions of tension, depression, anger, vigour, fatigue, and confusion (four items each). Respondents rated how they were feeling “right now” (e.g., panicky, miserable, bad-tempered, alert, tired, uncertain) on a 5-point scale from 0 = “not at all” to 4 = “extremely.” Possible scores on each mood dimension ranged from 0–16. The measurement model of the BRUMS has been evaluated using multi-sample confirmatory factor analysis that supported its configural, metric, scalar, and residual invariance [21,22,23]. In the present study, internal consistency coefficients of the six subscales ranged from 0.80–0.86, exceeding the 0.70 benchmark of acceptability [24]. To aid the interpretation of mood scores, raw scores were transformed into standard T-scores using tables of normative scores for the BRUMS [13].
2.3.2. Perceived stress
Perceived stress was assessed using the 4-item version of the Perceived Stress Scale (PSS-4) [25,26]. Respondents rated their feelings and thoughts during the “last month” (e.g., “unable to control the important things in your life”) on a 5-point scale from 0 = “never” to 4 = “very often.” Questions 2 and 3 were reverse scored and higher scores denoted higher levels of perceived stress, with possible total scores ranging from 0–16. Adequate psychometric characteristics have been reported for the PSS-4, including internal consistency (α = 0.77). In the present study, internal consistency (α = 0.60) fell below the 0.70 benchmark of acceptability [24]. PSS-4 scores were interpreted with reference to the norms produced by Warttig et al. [26] and descriptive statistics for the original validation study of the PSS-4 [25].
2.3.3. Resilience and coping
Resilience and coping skills were assessed using the 4-item Brief Resilient Coping Scale (BRCS) [27]. Respondents rated their behaviours and actions to questions such as “I believe I can grow in positive ways by dealing with difficult situations” on a 5-point scale ranging from 1 = “does not describe me” to 5 = “describes me very well”. Possible total scores ranged from 4–20. Adequate internal consistency, test-retest reliability, and convergent validity has been reported for the BRCS [27]. In the present study internal consistency (Cronbach α = 0.56) fell below the 0.70 benchmark of acceptability [24]. Total scores ranging from 4–13, 14–16, and 17–20, were interpreted as low, medium, and high resilient copers, respectively [27].
2.3. Procedure
An online survey was created using LimeSurvey [28] and data collection occurred during the period November 2021 to November 2022. The survey captured a range of demographic information described above, plus measures of mood, perceived stress, and resilience and coping. Students were invited to participate via electronic communications and completion time was approximately 10 minutes. Ethical approval was granted by the Human Research Ethics Committee of the University of Southern Queensland (approval number: H21REA266, date of approval 2 November 2021). The study conformed to the “Statement on Human Experimentation” by the National Health and Medical Research Council of Australia. All participants provided informed consent and anonymity was preserved.
2.4. Data Analysis
The IBM Statistical Package for the Social Sciences (SPSS) program version 28.0 [29] was used for all analyses. Descriptive statistics were calculated for all dependent variables and score distributions were checked for non-normality. Multivariate analysis of variance (MANOVA) was used to compare BRUMS, PSS-4, and BRCS scores among participants grouped by demographic characteristics, where group sizes were viable. Group comparisons were made for age (≤ 30 years vs. 31+ years), residency (international vs. domestic students), mode of study (on-campus vs external; full-time vs part-time), and employment status (employment secured vs. employment not secured). Effect sizes were assessed using Cohen’s d [30], where 0.20, 0.50, and 0.80 represent small, moderate, and large effects, respectively. No group comparison was conducted for gender due to the very large proportion of participants (87.5%) who identified as female. Pearson correlation analysis was used to identify relationships among measured variables and seeded k-means cluster analysis was used to classify participants into mood clusters. A power analysis indicated that, given the number of groups and response variables, a minimum sample size of 51 would be required to detect a predicted effect size of 0.20 at p < .05 with 80% power [30].
3. Results
3.1. Data Screening and Descriptive Statistics
Data were screened for missing or out-of-range values and non-normal distributions. No missing values were detected and all responses were within range. Descriptive statistics are shown in Table 1. Except for BRUMS anger scores, and to a lesser extent depression and confusion scores which were positively skewed and leptokurtic, no univariate non-normality was evident [31]. The non-normality for anger, depression, and confusion scores was due to a small number of participants scoring towards the upper end of the 0–16 scale. Such participants are of particular interest when screening for mental health issues and therefore they were retained in the data set. The Mahalanobis distances statistic was calculated to identify multivariate outliers at p < .001 [32] but none were found. Therefore all cases were retained and 112 participants were included in the analyses.
3.2. Mood scores
3.2.1. Comparison with population norms.
As explained above, raw mood scores were transformed into standardized T-scores and then compared with test norms [13], which by definition have a mean of 50 and standard deviation of 10. Significant deviations from test norms were found for tension, vigour, fatigue, and confusion scores, with effect sizes ranging from medium-to-large for tension (d = 0.70), and small-to-medium for the remaining three subscales (d = 0.22–0.38; Table 2). Subscale means are compared graphically to test norms in Figure 1, which also includes comparison with mean BRUMS scores derived from the general population during the pandemic [8].
3.2.2. Between-group comparisons of mood
A significant between-group difference was found for residency status (Wilks’Ʌ = .765, F(6, 105) = 5.368, p < .001, partial η² = .235), explaining 23.5% of variance. Univariate tests showed that international students reported higher vigour scores (M = 59.21, SD = 9.26) than domestic students (M = 50.11, SD = 8.17; p < .001, d = 0.99).
A comparison of graduating nursing students who had secured employment and those who had not showed a significant multivariate effect (Wilks’Ʌ = .802, F(6, 105) = 4.330, p < .001, partial η² = .198), explaining 19.8% of variance. Univariate tests showed that students who had not yet secured employment reported higher vigour scores (M = 54.26, SD = 9.09) than domestic students (M = 49.43, SD = 8.64; p = .005, d = 0.53).
A significant result (p = .04) was also identified for study location (on-campus vs. external), although none of the univariate analyses reached significance once a Bonferroni adjusted alpha value of p < .008 was applied to account for the six dependent variables. No significant differences in mood scores were found for age (≤ 30 years vs. 31+ years) or mode of study (full-time vs. part-time).
3.3. Perceived stress
PSS-4 scores for the group overall (M = 6.17, SD = 2.06) were lower than norms based on females in a UK sample (M = 6.38, SD = 3.15) [26], although the difference was not significant [Welch t(175) = 0.96, p = .339]. Compared to the scores for females (M = 4.7, SD = 3.1) reported in the original validation study of the PSS-4 by Cohen et al. [25], the graduating nurses in the present studies reported significantly higher perceived stress [Welch t(144) = 7.07, p < .001].
Significant between-group differences were found in PSS-4 scores for study location [t(111) = -2.098, p = .038] in that on-campus students (M = 6.57, SD = 1.84) reported higher perceived stress than those who studied externally (M = 5.77, SD = 2.20). No significant differences for perceived stress were found for gender, residency status, mode of study, or employment status, although a significant inverse relationship was shown for PSS-4 scores and age [r(111) = -.353, p < .001] indicating that younger students tended to report higher perceived stress than their older counterparts.
Pearson correlations showed positive relationships between scores for PSS-4 and BRUMS tension [r(111) = .185, p = .05]; depression [r(111) = .248, p = .008]; fatigue [r(111) = .260, p = .006]; and confusion [r(111) = .195, p = .039], and an inverse relationship between scores for PSS-4 and vigour [r(111) = -.225, p = .017].
3.4. Resilience and coping
Using the Brief Resilient Coping Scale (BRCS) classification cut-offs [27], 17.9% of nursing graduates were classified as low resilient copers (M = 11.85, SD = 1.27), 56.3% as medium resilient copers (M = 15.10, SD = 0.84), and 25.9% as high resilient copers (M = 17.90, SD = 1.05). No significant differences for resilience and coping were found for gender, residency status, mode of study, or employment status. A positive correlation was found between BRCS scores and BRUMS vigour scores [r(112) = .210, p = .026]. No other significant relationships between mood and resilience were found.
3.5. Cluster analysis of mood scores
A seeded k-means cluster analysis was used to classify participants into distinct mood clusters to identify participants who reported mood profiles shown previously to be associated with increased risk of mental health issues. Cluster analysis identified the six distinct mood profiles found in the literature, referred to as the iceberg, inverse Everest, inverse iceberg, shark fin, submerged, and surface profiles, with similar but not identical prevalence rates to those previously reported (Figure 2) [8,19,33,34]. A total of 22 participants (19.6%) reported mood profiles (inverse Everest and inverse iceberg) previously shown to associate with increased risk of mental health issues [11,12,13,14,35]. A further 26 nursing graduates (23.2%) reported a shark fin mood profile, characterised by high levels of fatigue and low levels of vigour, which has been linked to poor adherence to safety procedures [36] and may therefore pose a risk to patient safety.
4. Discussion
Concern for the sustainability of the health system in Australia prompted this cross-sectional study of final year nursing students. The primary aim of the study was to assess mood, stress, resilience, and coping among graduating students entering the nursing profession during a global pandemic. A secondary aim was to test whether mood, stress, resilience, and coping scores varied according to the demographic characteristics of the sample.
The average mood of the graduating nursing students was more negative than population norms, with tension, fatigue, and confusion scores all significantly elevated [13]. It should be noted, however, that the average mood of the graduating nursing students remained more positive than the typical mood reported among the general population during the height of the pandemic, using the same assessment methods [8]. The most notable characteristic of the group mood profile was the significantly elevated levels of tension compared to population norms, which represented a moderate-to-large effect.
Although the overall negativity of mood was relatively modest, it should be noted that 22 nursing graduates (19.6%) reported mood profiles (i.e., inverse Everest and inverse iceberg) associated with elevated risk of mental health issues [11,12,13,14]. The inverse Everest profile, which is characterised by very high scores for tension, depression, anger, fatigue, and confusion, is clearly not reflective of positive mental health nor is it an optimal mood for graduating nursing students to enter the profession. The prevalence of the inverse Everest profile in the present study (8%) is higher than reported among a large sample (N = 15,692) of the general population (4.6%)[34], but lower than samples of the general population (12.2%)[8] and students (9.5%)[16] during the pandemic.
The inverse iceberg profile, which is characterised by high scores for tension, depression, anger, fatigue and confusion, and low scores for vigour, has been used for decades as signalling potential burnout among athletes [12,35] and is also indicative of risk of mental health issues in military [11] and youth groups [14]. The prevalence of the inverse iceberg profile in the present sample (11.6%) is almost identical to population norms (11.8%)[34], and lower than COVID-specific samples (13%)[16], (21.2%)[8]. A further 26 nursing graduates (23.2%) reported a shark fin mood profile, characterised primarily by very high levels of fatigue and low levels of vigour. This prevalence is much higher than population norms (15.5%)[34], and other groups assessed during COVID (15.6%)[16], (12.9%)[8]. The behavioural consequences of a shark fin mood profile are not well understood, although it has been linked to poor adherence to safety procedures in high-risk vocations [36]. As such, nurses who report such high levels of fatigue may pose an elevated risk of them making medication errors, which represents a critical threat to patient safety. Fatigue among nurses has frequently been implicated as a cause of medication errors in health facilities [37,38,39,40].
A striking feature of the mood profiles was the low prevalence among the graduating nursing students of the iceberg profile, which has been associated with positive mental health and superior performance for several decades [41,42]. The prevalence of the iceberg profile in the present study (17.9%) was much lower than reported in the general population (28.5%)[34] and lower even than among other COVID samples (20.2%)[8], (20.3%)[16]. A relatively small number of between-group differences in mood scores were found. These were restricted to higher levels of vigour reported by international students compared to domestic students, and by those still seeking employment compared to those who had already secured a job post-graduation. Previous research [16] has shown more extensive differences in mood scores by residency status, with international students reporting higher tension, depression, anger, and confusion, as well as vigour, compared to domestic students. The greater consistency of mood scores within the current sample may be explained by the fact that they were all nursing students, whereas previous research [16] surveyed students across a very wide range of academic disciplines. Regarding employment status, it has been shown that being employed significantly reduces the risk of mental ill-health among pre-registration nursing students [20]. It is perhaps surprising that graduating nursing students in the present study who had not yet secured employment did not report higher scores on negative mood dimensions, nor on stress scores, compared to those who already had a job to start after graduating.
Results for perceived stress showed that the cohort of graduating nursing students in the present study reported PSS-4 scores that were high compared to the mean scores reported in the original validation study [25] but comparable with population norms for the measure derived from a UK sample [26]. On-campus students reported higher perceived stress than those who studied externally. This finding is consistent with a previous study of Australian students [16], which found that on-campus students reported higher scores for depression, anger, and confusion, which was explained by “the greater flexibility afforded by online study may alleviate rather than exacerbate the stressors involved” [16, p.11]. The inverse correlation between age and perceived stress is consistent with the findings of a study that investigated generational differences in psychological wellbeing among a sample of 631 Australian pre-registration nursing students [43], findings of which showed higher anxiety scores among the younger nurses compared to their older counterparts. Other studies of age differences on psychological wellbeing beyond the realm of nursing have shown older adults to have more highly developed skills for managing stress and to use more adaptive stress management strategies [44].
Regarding resilience and coping, 82.1% of the graduating nursing students in the present study reported BRCS scores that placed them in the categories of medium or high resilient copers. This finding mirrors the results of a systematic review of research into resilience and coping among health care workers during the COVID-19 pandemic [45], in which most studies showed health care workers to have high or moderate levels of psychological resilience. With respect to coping, most studies have shown high scores for positive (adaptive) rather than negative (maladaptive) coping among health care workers [45]. Communication with family, friends, and colleagues appears to have been the primary way in which healthcare workers managed to cope with the adverse mental health consequences of the pandemic [45]. Overall, findings from the present investigation suggest that most graduating students entering the nursing profession during the pandemic do not feel overly stressed, as assessed by the PSS-4, and tend to report positive appraisals of their psychological resilience and ability to cope with demands of the pandemic, as assessed by the BRCS. These results are encouraging for those seeking to maintain a sustainable pipeline of new graduates into the nursing profession. Nevertheless, focus should be maintained on promoting strategies to support those coming into the profession and to encourage those more experienced nurses to remain in the profession. In a study of 720 nurses conducted in Turkey during the pandemic [46], the level of social support provided to nurses by family, friends and significant others was shown to be significantly related to nurses’ psychological resilience.
4.1. Future research
There is a need for future research to address the projected shortfall of nurses domestically [1,47] and globally [3]. Bakker and colleagues [48] conducted a systematic review of 21 studies that evaluated interventions designed to improve the mental health of student and novice nurses and/or prevent nurses leaving the profession. Interventions were focused on managing stress, facilitating the transition to nursing practice, or a combination of both. Only five studies showed a significant effect on dropout-related outcomes and generally study quality was judged to be low with a high overall risk of bias. The authors concluded that, although a wide range of interventions are available, compelling evidence of their effectiveness is limited. Therefore, for the long-term sustainability of the nursing workforce in Australia and internationally, future research should seek to develop effective ways to support nurses in training and once they are working in the profession, to prevent dropout rate.
To address this need, a systematic review of factors influencing retention among undergraduate nursing students in regional, rural, and remote areas of Australia was conducted by Liu and colleagues [49], the findings of which emphasized the importance of academic and personal support, and highlighted several internal factors (such as stress, personal qualities, ability to engage with classes and institutions, time management, lack of confidence, cultural well-being, and Indigenous identity), and external factors (such as technical difficulties, casual tutors, different competing demands, study facilities, and financial and logistical barriers), all of which were shown to influence retention. Further research to develop evidence-based strategies to address these issues is urgently required.
A study by Grundy and Lum [50] reported that patient expectations evolved during the pandemic, with the traditional expectations of safe, reliable, and compassionate care being augmented by an additional expectation of specific COVID-19 related safety procedures. Universities Australia has predicted a national shortfall of 85,000 nurses by 2025 [47], requiring a significant expansion of clinical placements for nursing students, especially in the growth areas of aged care, primary care, mental health care, and disability services. Given the likely outbreaks of future pandemics, it would be prudent for student nurses to receive clinical training in pandemic-specific care as a part of their university training. University academics should consider this recommendation when designing future iterations of nursing program curricula.
4.2. Strengths and limitations
It is a strength of the present study that participation was restricted to students who were about to graduate from a nursing degree program and enter the workforce as this cohort becomes the much-needed new recruits into the nursing profession. Limitations of the present study are acknowledged. Firstly, data were collected at one university among students who participated voluntarily. Therefore, results may not generalise to graduating nursing students in other parts of Australia and beyond. Secondly, given that some of the measures used in the present study (PSS-4, BRCS) had reliability coefficients below the standard benchmark of acceptability, results related to those measures should be viewed with caution.
5. Conclusions
It is concluded that nursing students eligible to graduate from a university program and enter the nursing profession during a pandemic reported a range of mood profiles. Mood profiles indicated that 19.6% of participants had elevated mental health risk, 23.2% showed potential risk of burnout, and only 17.9% reported mood profiles associated with positive mental health. Regarding perceived stress, resilience, and coping, participants generally reported normal levels of stress (UK norms) and 82.1% of the graduating nursing students were classified as medium or high resilient copers. Group differences across the measured variables were limited.
Author Contributions
Victoria R. Terry: Conceptualization, Data Curation, Investigation, Methodology, Supervision, Writing – original draft, review & editing. Renée L. Parsons-Smith: Data Curation, Formal analysis, Methodology, Visualization, Writing – original draft, review & editing. Jessica Elliott: Methodology, Writing – original draft, review & editing. Geraldine Roderick: Methodology, Writing – original draft, review & editing. Patricia Luyke: Methodology, Writing – original draft, review & editing. Peter C. Terry: Conceptualization, Formal analysis, Methodology, Supervision, Visualization, Writing – original draft, review, & editing.
Funding
No funding sources were used in writing this manuscript.
Institutional Review Board Statement
This study was reviewed and approved by the Human Research Ethics Committee (HREC) of the University of Southern Queensland (approval number: H21REA266, date of approval 2 November 2021).
Informed Consent Statement
All participants provided written informed consent.
Data Availability Statement
Data are available from the corresponding author upon request.
Conflicts of Interest
None.
References
- Department of Health and Aged Care. Nurses and midwives in Australia. Canberra, ACT: Australian Government, 2023. Available online: https://www.health.gov.au/topics/nurses-and-midwives/in-australia (accessed on 1 November 2023).
- Australian Primary Health Care Nurses Association. One in four primary health care nurses plans to quit. 2022. Available online: https://www.apna.asn.au/about/media/one-in-four-primary-health-care-nurses-plans-to-quit (accessed on 2 November 2023).
- Lo, W.Y.; Chien, L.Y.; Hwang, F.M.; Huang, N.; Chiou, S.T. From job stress to intention to leave among hospital nurses: A structural equation modelling approach. J. Advanc. Nurs. 2018, 74, 677–688. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 pandemic triggers 25% increase in prevalence of anxiety and depression worldwide. 2022. Available online: https://www.who.int/news/item/02-03-2022-covid-19-pandemic-triggers-25-increase-in-prevalence-of-anxiety-and-depression-worldwide (accessed on 2 November 2023).
- Reverté-Villarroya, S.; Ortega, L.; Lavedán, A.; Masot, O.; Burjalés-Martí, M.D.; Ballester-Ferrando, D.; Fuentes-Pumarola, C.; Botigué, T. The influence of COVID-19 on the mental health of final-year nursing students: comparing the situation before and during the pandemic. Int. J. Ment. Health. Nurs. 2021, 30, 694–702. [Google Scholar] [CrossRef]
- The National Centre of Excellence in Youth Mental Health. Under the radar: The mental health of Australian university students. Orygen: Melbourne, VIC, Australia, 2017. Available online: https://www.orygen.org.au/About/News-And-Events/Mental-health-of-Australian-university-students-fl (accessed on 15 December 2023).
- Tung, Y.J.; Lo, K.K.H.; Ho, R.C.M.; Tam, W.S.W. Prevalence of depression among nursing students: A systematic review and meta-analysis. Nurs. Educ. Today 2018, 63, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Terry, P.C.; Parsons-Smith, R.L.; Terry, V.R. Mood responses associated with COVID-19 restrictions. Front. Psychol. 2020, 11, e589598. [Google Scholar] [CrossRef] [PubMed]
- Fowler, K.; Wholeben, M. COVID-19: Outcomes for trauma-impacted nurses and nursing students. Nurs. Educ. Today 2020, 93, e104525. [Google Scholar] [CrossRef]
- Castro, C.; Antunes, R.; Fernandes, J.B.; Reisinho, J.; Rodrigues, R.; Sardinha, J.; Vaz, C.; Miranda, L.; Simões, A. Perceptions and representations of senior nursing students about the transition to professional life during the COVID-19 pandemic. Int. J. Environ. Res. Publ. Health 2022, 19, e4466. [Google Scholar] [CrossRef] [PubMed]
- Gould, M.S.; Marrocco, F.A.; Kleinman, M.; Thomas, J.G.; Mostkoff, K.; Côté, J.; Davies, M. Evaluating iatrogenic risk of youth suicide screening. JAMA 2005, 293, 1635–1643. [Google Scholar] [CrossRef]
- Morgan, W.P.; Brown, D.R.; Raglin, J.S.; O’Connor, P.J.; Ellickson, K. Psychological monitoring of overtraining and staleness. Br. J. Sports Med. 1987, 21, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Terry, P.C.; Parsons-Smith, R.L. Mood profiling for sustainable mental health among athletes. Sustain. 2021, 13, e6116. [Google Scholar] [CrossRef]
- van Wijk, C.H.; Martin, J.H.; Hans-Arendse, C. Clinical utility of the Brunel Mood Scale in screening for post-traumatic stress risk in a military population. Mil. Med. 2013, 178, 372–376. [Google Scholar] [CrossRef]
- Sties, S.W.; Gonzáles, A.I.; Netto, A.S.; Wittkopf, P.G.; Lima, D.P.; De Carvalho, T. Validation of the Brunel Mood Scale for Cardiac Rehabilitation Program. Rev. Bras. Med. Esporte, 2014, 20, 281–284. [Google Scholar] [CrossRef]
- Braslis, K.G.; Santa-Cruz, C.; Brickman, A.L.; Soloway, M.S. Quality of life 12 months after radical prostatectomy. Brit. J. Urol. 1995, 75, 48–53. [Google Scholar] [CrossRef]
- Bueno, J.L.; De Martino, M.M.; Figueiredo, T.H. Present mood states in Brazilian night nurses. Psychol. Rep. 2003, 93, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, T.S.; Moreira, C.Z.; Guo, J.; Noce, F. Effects of a 12-hour shift on mood states and sleepiness of neonatal intensive care unit nurses. J. School Nurs. Univ. São Paulo 2017, 51, e7. [Google Scholar] [CrossRef]
- Brownlow, C.; Eacersall, D.; Nelson, C.W.; Parsons-Smith, R.L.; Terry, P.C. Risks to mental health of higher degree by research (HDR) students during a global pandemic. PLOS ONE 2022, 17, e0279698. [Google Scholar] [CrossRef] [PubMed]
- Moxham, L.J.; Fernandez, R.; Kim, B.; Lapkin, S.; Ten Ham-Baloyi, W.; Al Mutair, A. Employment as a predictor of mental health, psychological distress, anxiety, and depression in Australian pre-registration nursing students. J. Prof. Nurs. 2018, 34, 502–506. [Google Scholar] [CrossRef] [PubMed]
- Terry, P.C.; Lane, A.; Lane, H.J.; Keohane, L. Development and validation of a mood measure for adolescents. J. Sports Sci. 1999, 17, 861–872. [Google Scholar] [CrossRef]
- Terry, P.C.; Lane, A.; Fogarty, G. Construct validity of the Profile of Mood States—Adolescents for use with adults. Psychol. Sport Exerc. 2003, 4, 125–139. [Google Scholar] [CrossRef]
- Terry, P.C.; Skurvydas, A.; Lisinskiene, A.; Majauskiene, D.; Valanciene, D.; Cooper, S.; Lochbaum, M. Validation of a Lithuanian-language version of the Brunel Mood Scale: The BRUMS-LTU. Int. J. Environ. Res. Public Health 2022, 19, e4867. [Google Scholar] [CrossRef]
- Nunnally, J.C. Psychometric theory, 2nd ed.; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Warttig, S.L.; Forshaw, M.J.; South, J.; White, A.K. New, normative, English-sample data for the Short Form Perceived Stress Scale (PSS-4). J. Health Psychol. 2013, 18, 1617–1628. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, V.G.; Wallston, K.A. The development and psychometric evaluation of the Brief Resilient Coping Scale. Assess. 2004, 11, 94–101. [Google Scholar] [CrossRef]
- Engard, N.C. LimeSurvey http://limesurvey.org. Publ. Serv. Quart. 2009, 5, 272–273. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows; Version 28.0; IBM Corp.: Armonk, NY, USA, 2021. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences. New York, NY, USA: Routledge Academic, 1988.
- Field, A. Discovering statistics using SPSS. Sage: London, UK, 2009. [Google Scholar]
- Tabachnick, B.L.; Fidell, L.S. Using Multivariate Statistics (7th ed.). Boston, MA, USA: Pearson Education, 2017.
- Parsons-Smith, R. L., Terry, P. C., & Machin, M. A. (2017). Identification and description of novel mood profile clusters. Frontiers in Psychology, 8, e1958. [CrossRef]
- Terry, P. C., Parsons-Smith, R. L., King, R., & Terry, V. R. (2021). Influence of sex, age, and education on mood profile clusters. PLOS ONE, 16, e245341. [CrossRef]
- Budgett, R. Fatigue and underperformance in athletes: The overtraining syndrome. Br. J. Sports Med. 1988, 32, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Parsons-Smith, R.L. In the mood: Online mood profiling, mood response clusters, and mood-performance relationships in high-risk vocations. Available online: https://research.usq.edu.au/item/q3941/in-the-mood-online-mood-profiling-mood-response-clusters-and-mood-performance-relationships-in-high-risk-vocations (accessed on 2 November 2023).
- Bell, T.; Sprajcer, M.; Flenady, T.; Sahay, A. Fatigue in nurses and medication administration errors: A scoping review. J. Clin. Nurs. 2023, 32, 5445–5460. [Google Scholar] [CrossRef] [PubMed]
- Castaldo, A.; Ferrentino, M.; Ferrario, E.; Papini, M.; Lusignami, M. Factors contributing to medication errors: A descriptive qualitative study of Italian nursing students. Nurs. Educ. Tod. 2022, 118, e105511. [Google Scholar] [CrossRef]
- Schroers, G.; Ross, J.G.; Moriarty, H. Nurses’ perceived causes of medication administration errors: A qualitative systematic review. Joint Commis. J. Qual. Patient Safe. 2021, 47, 38–53. [Google Scholar] [CrossRef]
- Stolic, S.; Ng, L.; Southern, J.; Sheridan, G. Medication errors by nursing students on clinical practice: An integrative review. Nurs. Educ. Tod. 2022, 112, e105325. [Google Scholar] [CrossRef]
- Morgan, W.P. Selected psychological factors limiting performance: a mental health model. In Limits of Human Performance, eds D.H. Clarke; H.M. Eckert. Champaign, IL, USA: Human Kinetics, 1985, 70–80.
- Raglin, J.S. Psychological factors in sport performance. Sports Med. 2001, 31, 875–890. [Google Scholar] [CrossRef]
- Middleton, R.; Fernandez, R.; Moxham, L.; Tapsell, A.; Halcomb, E.; Lord, H.; Alomari, A.; Hunt, L. Generational differences in psychological wellbeing and preventative behaviours among nursing students during COVID-19: a cross-sectional study. Contemp. Nurs. 2021, 57, 213–223. [Google Scholar] [CrossRef]
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clin. Psychol. Rev. 2010, 30, 217–237. [Google Scholar] [CrossRef]
- Labrague, L.J. Psychological resilience, coping behaviours and social support among health care workers during the COVID-19 pandemic: A systematic review of quantitative studies. J. Nurs. Manage. 2021, 29, 1893–1905. [Google Scholar] [CrossRef]
- Kilinç, T.; Sis Çelik, A. Relationship between the social support and psychological resilience levels perceived by nurses during the COVID-19 pandemic: A study from Turkey. Perspect. Psychiatr. Care 2021, 57, 1000–1008. [Google Scholar] [CrossRef] [PubMed]
- Universities Australia. More clinical placements needed to grow nursing workforce [media release]. Deakin, ACT, Australia: Universities Australia. Available online: https://universitiesaustralia.edu.au/media-item/more-clinical-placements-need-to-grow-nursing-workforce (accessed on 19 December 2023).
- Bakker, E.J.M.; Kox, J.H.A.M.; Boot, C.R.L.; Francke, A.L.; van der Beek, A.J.; Roelofs, P.D.D.M. Improving mental health of student and novice nurses to prevent dropout: A systematic review. J. Advance. Nurs. 2020, 76, 2494–2509. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.-L.; Wang, T.; Bressington, D.; Nic Giolla Easpaig, B.; Wikander, L.; Tan, J.-Y. Factors influencing retention among regional, rural, and remote undergraduate nursing students in Australia: A systematic review of current research evidence. Int. J. Environ. Res. Public Health 2023, 20, e3983. [Google Scholar] [CrossRef] [PubMed]
- Grundy, T.J.; Lum, C. Impact of COVID-19 Pandemic on Patient Experience in the Asian Region. Melbourne, Australia: Insync-Press-Ganey, 2023. Available online: https://insync.com.au/insights/covid-impact-patient-experience-asia/ (accessed on 19 December 2023).
Figure 1.
Comparison of mean mood for 112 graduating nurses, compared to test norms [13] and mood during COVID-19 lockdowns [8].
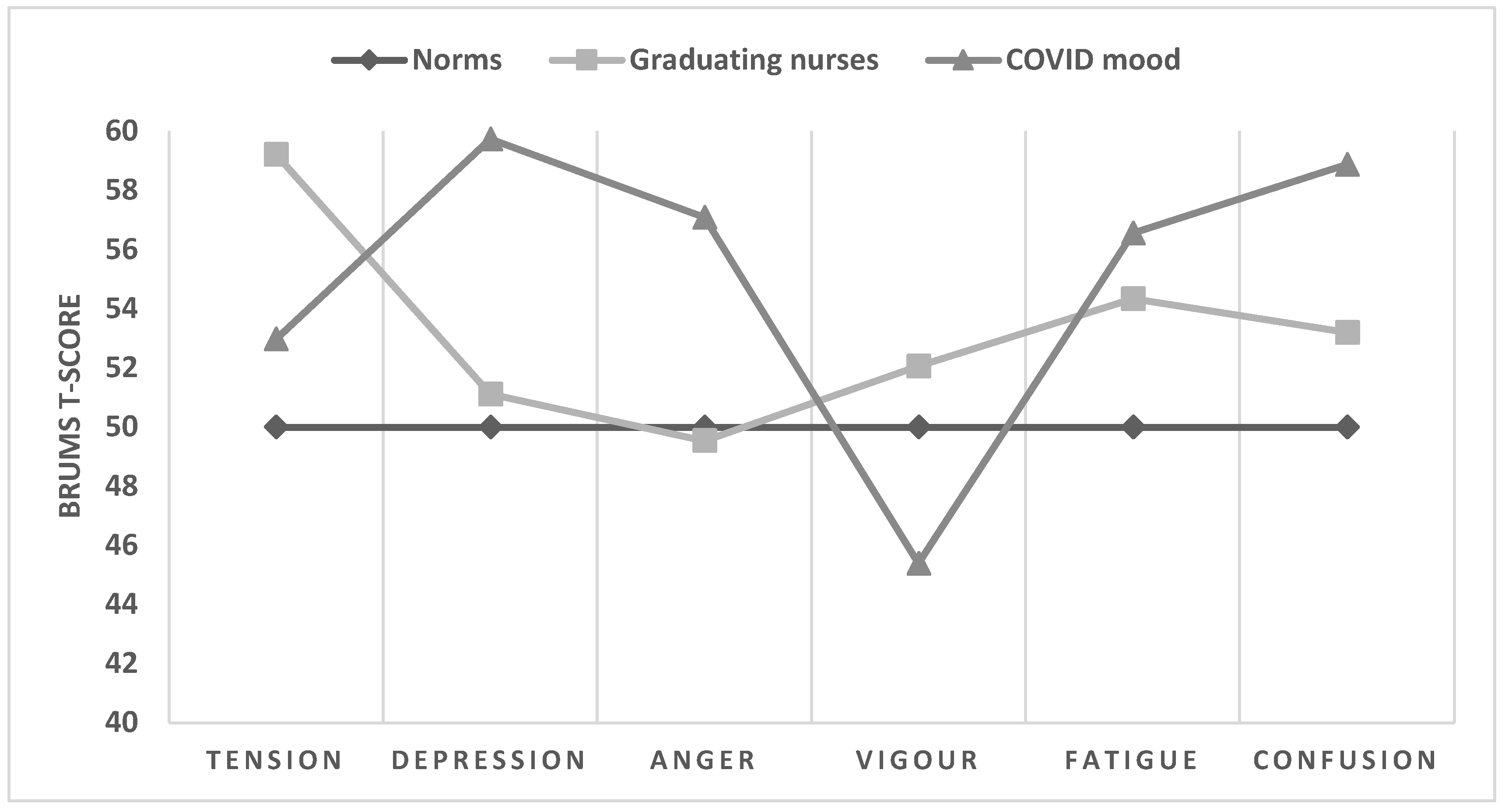
Figure 2.
Graphical representation of the 6-cluster solution for 112 graduating nurses.
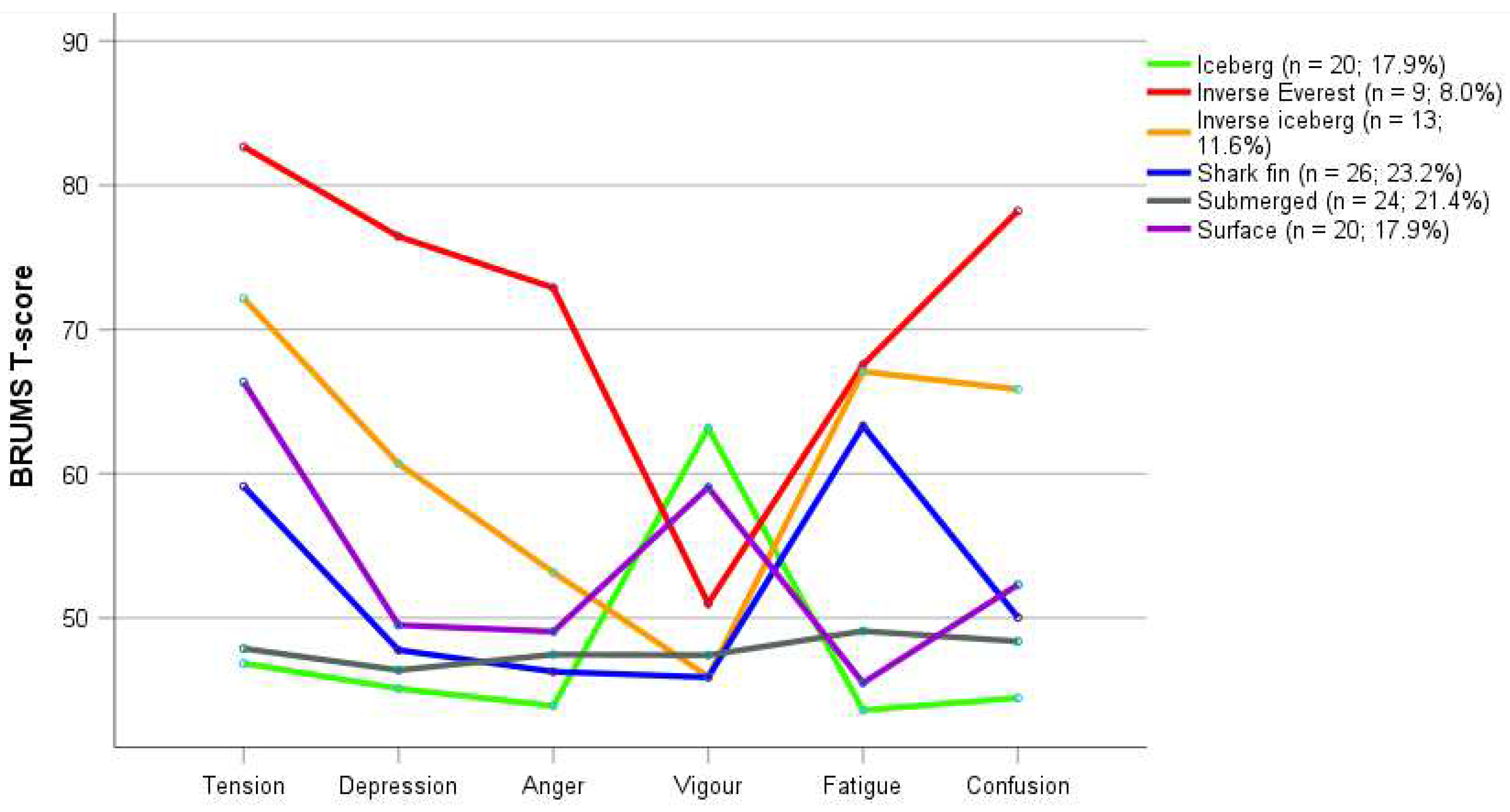

Table 1.
Descriptive statistics for PSS-4, BRCS, and BRUMS scores for 112 graduating nurses.
| Source | M | SD | Minimum | Maximum | Skewness | Kurtosis |
| PSS-4 | 6.17 | 2.06 | 1 | 12 | 0.22 | 0.31 |
| BRCS | 15.24 | 2.21 | 9 | 20 | -0.29 | 0.34 |
| BRUMS-Ten | 6.07 | 4.39 | 0 | 16 | 0.64 | -0.43 |
| BRUMS-Dep | 2.52 | 3.34 | 0 | 14 | 1.59 | 2.07 |
| BRUMS-Ang | 2.05 | 3.00 | 0 | 14 | 2.19 | 5.35 |
| BRUMS-Vig | 8.09 | 3.65 | 0 | 16 | 0.16 | -0.48 |
| BRUMS-Fat | 6.99 | 4.47 | 0 | 16 | 0.39 | -0.84 |
| BRUMS-Con | 3.51 | 3.44 | 0 | 15 | 1.20 | 0.86 |
Note. Ten = tension, Dep = depression, Ang = anger, Vig = vigour, Fat = fatigue, Con = confusion.
Table 2.
Mean BRUMS scores for 112 graduating nurses vs. population norms.
| Subscale | M | SD | 95% CI | t | g |
| Tension | 59.21 | 13.16 | [56.75, 61.68] | 7.41† | 0.70 |
| Depression | 51.11 | 10.69 | [49.11, 53.11] | 1.10 | - |
| Anger | 49.54 | 9.64 | [47.73, 51.34] | -0.51 | - |
| Vigour | 52.06 | 9.17 | [50.35, 53.78] | 2.38* | 0.22 |
| Fatigue | 54.34 | 11.34 | [52.22, 56.46] | 4.05† | 0.38 |
| Confusion | 53.19 | 11.06 | [51.12, 55.26] | 3.05§ | 0.29 |
Note. All scores are T-scores; t = 2-tailed t-test between observed mean and normative mean of 50 (SD = 10); g = effect size; *p < .05, §p < .01., †p < .001.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



