
Submitted:
29 December 2023
Posted:
03 January 2024
You are already at the latest version
Abstract
Patients with low back pain often have deficits in trunk stability. For this reason, many patients receive physiotherapy treatment, which represents an enormous socio-economic burden. Training at home could reduce these costs. The prob-lem here is the lack of correction of the exercise execution. This feasibility study therefore investigates the applicability of a vibrotactile-controlled feedback system for trunk stabilization exercises.
A sample of 13 healthy adults performed three trunk stabilization exercises. Exercise performance was corrected by physiotherapists using vibrotactile feedback. The NASA TLX questionnaire was used to assess the practicability of the vibrotactile feedback.
The Nasa TLX questionnaire show a very low global workload M = 37.96 (SD =11.63). The quality of feedback perception was perceived as good by the subjects, varying between 76.9 % and 92.3 % depending on the body part. 80.8 % rated the feedback as helpful for their training. On the expert side, the results show a high rating of movement quality.
The positive evaluations of the physiotherapists and the participants on the use of the vibrotactile feedback system indi-cate that such a system can reduce the trainees fear of independent training and support the users in their training. This could increase training adherence and long-term success.
Keywords:
vibrotactile feedback system
; trunk stability.
; Nasa TLX questionnaire
1. Introduction
With a lifetime prevalence of 80 to 85 %, low back pain is one of the most common musculoskeletal disorders worldwide (1–3). The cost burden on the healthcare system is expected to continue to increase in the coming decades (4,5). To counteract this trend, early identification of patients at risk for back pain is of general importance, as is the use of effective primary preventive measures to avoid LBP (1,6). It has been shown that well-developed trunk stability is crucial for this purpose, both in elite sport and in the general population (7–10). Recent studies show that trunk stabilising sensorimotor training performed twice a week for twelve weeks can reduce the rates of recurring in LBP patients by 80 % (11,12). To this end, most patients with LBP are treated in physiotherapy practices (13,14). Most people use an outpatient rehabilitation facility for this purpose. However, physiotherapy treatment is one of the most staff-intensive areas of medical care. Home-based training, on the other hand, is an alternative form of treatment that can take place in the rehabilitant's familiar surroundings and facilitates the transfer of treatment into everyday life. In this context, independent home practice is becoming increasingly important. The costs for the same rehabilitation success can be reduced by about 50 % through independent intensive practice at home (15).
Theory
Home training in physiotherapeutic contexts. According to recent studies in the field of the post-operation treatments, an independent but also significantly intensified home practice achieves the same rehabilitation success as guided physiotherapy (16). The patient must integrate the rehabilitation measure into his or her daily routine. The success of home training depends decisively on individual discipline, self-motivation and the correct execution of the exercises by the patient. The key to success lies in the combination of professional treatment by the physiotherapist and independent intensification of therapy at home. A high quality of movement is essential for a successful rehabilitation. In professional treatments, this can be achieved by feedback given by therapists directly to patients through touch or verbal communication. For home-based trainings however, no physiotherapists are present. Therefore, a different approach must be applied to ensure the necessary movement quality.
Vibrotactile feedback / tactile internet.
The tactile internet opens up technical possibilities for providing feedback. The almost latency-free data transmission allows data to be measured and real-time feedback to be transmitted (17). A vibrotactile-controlled feedback system is a promising variant that enables autonomous training, but also monitors training quality and supports the trainee in performing exercises correctly (Islam & Lim, 2022). The tactile feedback is perceived via the skin. The information can be generated by pressure or vibration, with the latter being referred to as vibrotactile feedback (18).
Tactile feedback can be given directly to patients by therapists. In a hands-off context, a human-machine interface is required to provide tactile feedback.
Feedback is usually provided by small, lightweight, vibrating transducers called actuators.
Vibrotactile feedback can be positioned in different locations on the body and in different ways to respond to the stimulus (19–22). Users are usually instructed to move in the direction of the stimulus (attractive cue) (19,23). However, when using vibrotactile feedback on the lower back of healthy older adults, moving in the opposite direction of the stimulus (repulsive cue) leads to better movement performance (20,22). In a comparative study between attractive or reimpulsive feedback, Kinnaird et al. 2016 showed that reimpulsive feedback was superior to attractive feedback in healthy older adults on the lower back. However, further studies show that the use of attractive feedback can be just as effective in correcting motor tasks.
In this context, it should also be borne in mind that attractive feedback may be cognitively associated with a reward and therefore has a more positive connotation in the user's evaluation and could therefore increase the trainee's motivation and ultimately training compliance. In contrast, reimpulsive feedback could be interpreted as an alarm, which could be associated with negative emotions, as it suggests to the exerciser that they are not performing the exercise correctly. In addition, Lee et al. were able to show that attractive stimulation, without further instructions, causes the subjects to align their body position with the attractive stimuli. Lee et al. conclude that an improved internal proprioceptive representation and orientation is responsible for this. By utilizing this natural tendency, the attractive feedback could be used just as well as the stimulus-plus feedback.
However, research as well as the use of vibrotactile feedback devices in a therapeutic context is still insufficient, so that little can be said about the design of technical feedback systems (24). The aim of this research project is therefore to derive requirements for the design of a tactile feedback strategy, especially for the implementation of trunk-stabilizing exercises. To this end, this study examines the feedback behavior of healthy people and analyzes their use of technical tactile feedback.
Form this point of view the following questions arise.
RQ1: “Is it possible to use vibrotactile feedback to support people in correctly performing physiotherapeutic exercises?”
RQ2: “What requirements do users have for vibro-tactile technology-based feedback to accept it?”.
2. Materials and Methods
Sample
The sample consisted of 9 women and 4 men with an average age of 46.5 years (SD ± 9.6), an average height of 173.4 cm (SD ± 10.0), an average weight of 72.7 kg (SD ± 8.4) and a BMI of 24.0 (SD ± 1.8). The recruitment and examination of the subjects took place at a DOSB-licensed sports medicine facility. Subjects who had not experienced back pain in the last three months and were between 40 and 60 years old were included. Subjects who had an ankle, knee or hip injury in the last three months or who could not support themselves on their hand or knee joints were excluded.
To enable vibrotactile feedback for the test subjects, they wore a tight-fitting long-sleeved top with twelve vibration modules that generated vibrations in the frequency range of 10-400 Hz using ERM vibration motors. The prototype also includes three circuit boards and the cabling for the components.
All components are shielded from the test subject by housings. All electronic components are insulated and the applied voltage of 5V and a current of 0.9A pose no danger to healthy test subjects in the event of a defect. Power was supplied via a USB cable connected to a laptop. The ERM vibration motors were attached to the following body parts (Figure 1).
Materials
The applicability of vibrotactile feedback as a tool for correcting exercise performance was evaluated by both the physiotherapist and the subjects. The movement quality as well as the assessment of the feedback quality of the subjects regarding the vibro-tactile feedback, are carried out by means of standardised questionnaires.
Physiotherapist questionnaire. The feedback giving physio therapists gave a third-party assessment on different variables. In order to assess the specific functionality of the vibrotactile feedback to support a correct execution of trunk stabilising exercises, the correction behaviour by physiotherapists was evaluated on a 4-point Likert scale (poles: not at all, a little, moderately, very):
1) Ability to implement the vibro-tactile feedback
2) Level of difficulty for the subject to perform the exercises
3) Accuracy of axis and thus the quality of movement of the subjects
Subject questionnaire. The subject questionnaire focused on capturing subjective user perceptions and eliciting potential users' requirements for vibrotactile technology-based feedback. The NASA TLX was used for this purpose, (25) which can be used to assess psychological workload. It provides a global rating of subjective workload. In addition to the global rating, six subscales can be calculated (mental, physical and temporal demand, effort, performance, frustration level).
The mental demand scale refers to the mental and perceptual activity a user needs to complete a task. This measure includes mental activities such as thinking, decision making, remembering, looking and similar aspects. High levels indicate that a task was demanding, complex, whereas low levels are indicators for simple and easy tasks.
Physical demand refers to actual physical efforts needed by users for task completion. It includes for example activities like pushing, pulling and such. High levels on this subscale indicate that a task was demanding, brisk or laborious. Low levels indicate an easier and slack task with possibilities for slow execution or even resting.
Effort means the amount of work users put into the completion of a task. It combines the ratings of physical and mental activities during the task execution and therefore refers to a rating of overall strain or struggle.
The scale temporal demand measures the subjective time pressure users feel during a task execution. It depends on the pace of task elements. In this case high outcome refers to frantic or rapid pace, whereas low outcomes indicate the subjective time perception as more slow and leisurely.
The rating of performance indicates a self-rating on task success by the users in terms of goal completion. It includes the users satisfaction with the accomplishment.
Frustration Level refers to certain feelings an user may have while performing a task. High levels indicate that they are insecure, discouraged, irritated, stressed or annoyed during a task while low levels indicate opposite aspects such as feeling gratified, content, relaxed and complacent.
Besides NASA TLX, subjects were asked to rate the intensity of the feedback related to the location of the feedback indicator in different areas of the body. This measure was imposed to find out whether users are able to feel the vibro-tactile at all while performing physically demanding tasks. Feedback intensity was rated on a 4-point Likert scale (anchors: not noticeable at all, weak, good, too strong). To ascertain whether the feedback can be associated with an intended purpose, subjects were asked about their subjective degree of approval on six potential purpose associations (alarming, warning, indicative, leading, supportive, meaningless) using a 2-point Likert Scale (anchors: does apply, does not apply). To rule out, that future users have negative associations regarding the new system, a range of feedback-associated emotions were rated by the participants on the same scale as purpose. These included positive associated emotions (calming, pleasing, relaxing, motivating, exciting) as well as negative ones (dangerous, irritating, frustrating, meaningless) (26).
Study procedure.
To provide vibrotactile feedback for the test subjects, they wore a tight-fitting long-sleeved top with twelve vibration modules. Three different types of exercises were used during the study, on the one hand to exclude effects regarding specific kinds of exercises, on the other hand to ensure that subjects can encounter the need for a correction. The exercise portfolio consisted of the quadruped stand with diagonal arm-leg coordination. The second exercise was to train the shoulder blade fixators while leaning against a wall in a two-legged stand by moving the arms up and down. The third exercise was to present a lateral support with pelvic raise and lowering (see Figure 2). All exercises were performed on an unstable surface in order to particularly stress the neuromuscular control function. The three basic exercises were practised with the subjects. Correct execution and error patterns were shown to them in detail by a physiotherapist and described verbally before they began to perform the exercises independently. Basically, the subjects were asked to move in the opposite direction of the stimulus from the feedback (repulsive cue). Only in the scapula fixator exercise were the subjects asked to move in the direction of the stimulus (attractive stimulus) when lowering the shoulders: M. (trapecius pars ascendens). The same applied when tensing the arms backwards (middle third Os humeri /Humerus). The subjects were asked to perform ten repetitions of each of the three exercises. The exercise performance was corrected by a physiotherapist using vibrotactile feedback. As the exercise quality was to be assessed independently by two physiotherapists, the subjects completed two rounds, meaning each exercise was performed two times.
3. Results
Research question 1.
The first research question was related to the general functionality of the feedback: "Is it possible to use vibrotactile feedback to help people perform physiotherapeutic exercises correctly?" To answer the question, the subjects' quality of movement after correction and feasibility of feedback by physiotherapists, as well as the workload during exercise performance by the subjects were collected.
Quality of movement and feasibility
As a general starting point, it was important to determine whether the vibrotactile technology-assisted feedback can have a general and positive effect on the execution of an exercise, as well as whether the subjects can implement the feedback. Mean values for the quality of exercise execution were calculated. The results showed an overall high evaluation of the quality of movement in the corrected subjects (M = 3.27; SD = 0.56; range between 1-4, with 4 being the best quality). This indicates the general functionality as well as the quality of the feedback technique in a physiotherapeutic setting. None of the physiotherapists chose the anchor "not at all". Furthermore, the physiotherapists were asked whether the subjects were able to implement the feedback in their exercises during the study. The results on implementability indicate an overall good rating of the variable (M = 3.27; SD = 0.72). No physiotherapist chose the option "not at all". In general, the subjects were able to integrate the feedback into their movements.
Workload
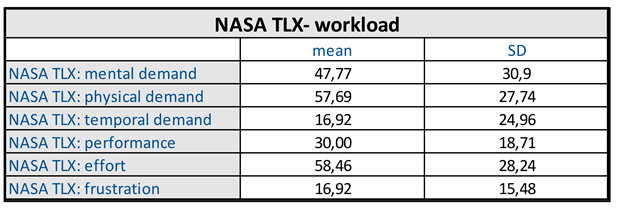
To determine whether the cognitive processing of the technology-assisted vibrotactile feedback interferes with users performing the exercises, the unweighted NASA TLX was evaluated. The global workload was M = 37.96 (SD =11.63), indicating a very low workload. It was interpreted using the benchmarks for global workload associated with physical activity summarised by Grier (2015) using meta-analysis (Min = 40.83; Max = 75.19). To examine the distribution of mental workload in more detail, scores were calculated for each of the NASA TLX subscales; the results are shown in table 1. The result on mental workload, can be classified as a medium value: M = 47.77; SD = 30.89. The highest scores were obtained for physical demand (M = 57.69; SD = 27.74) and effort (M = 58.46; SD = 28.24). The result for temporal demand is very low (M = 16.92; SD = 24.96). Frustration also reached a low level (M = 16.92; SD = 15.48). The score for achievement (30.00; SD = 18.71) is in the middle range of values.

Table 1.
subscales of global workload of the NASA TLX questionnaire.
 |
In view of these results, research question 1 can be answered. It is indeed possible to initiate postural correction through technology-based vibrotactile feedback. Not only does it work in general, but it also leads to good results in postural correction with regard to exercise performance from an expert's point of view. The amount of work required to process the feedback is not so high that the subjects are prevented from actually performing the exercises tested.
Research question 2.
The second research question was related to technology acceptance: "What requirements do users have for vibrotactile technology-based feedback to be acceptable?". To answer this question, the subjective evaluations of the feedback in terms of intensity, purpose and the associated positive or negative feelings from the users' perspective were surveyed.
Intensity of the vibration. An essential question in connection with this second research question is whether the vibrotactile feedback during the execution of an exercise is strong enough to be perceived by the user. To answer this question, the subjects gave subjective assessments of the intensity of the vibration in relation to the different areas of the body where feedback could be given. The anchors "not noticeable at all" and "weak" were combined into one category to represent the area identified as “needing improvement”. The anchor "too strong" was not selected by any of the participants. Overall, the strength of the vibration was perceived well in all areas of the body. The area, which was perceived least good, was the abdominal area with 23.10 % of subjects rating it as “weak” or “not noticeable at all”. The upper body areas were only rated as “to weak” by 7.70 % to 15.40 % of the subjects.
Perceived purpose of the feedback
Apart from the basic perception of the feedback, the purpose that the user associates with it is crucial. If the feedback is interpreted differently than intended by the designers and physiotherapists, this can lead to serious discrepancies between the intention of the feedback and the user's actions after correction. The feedback was not perceived as meaningless (0 %). A large proportion of subjects assigned the purposes indicative (84.60 %) and supportive (69.20 %). However, it was perceived as indicative by only a small proportion of respondents (30.80 %). Moreover, it was not perceived as alarming (0 %), a mediated purpose that can lead to negative emotions.
Feedback-associated emotions
As indicated earlier, the purpose of feedback can evoke emotions with feedback technology. To further investigate the feelings conveyed by vibrotactile feedback in exercise situations, subjects rated a variety of possible feedback-associated emotions. These included feelings with positive connotations, such as "motivating" or "relaxing", as well as feelings with more negative connotations, such as "irritating" or "dangerous". Figure 3 show the percentage values of the ratings. In general, the feelings with positive connotations were rated "does not apply" in the majority of cases (between 54 % and 100 %). The feedback does not seem to trigger many positive feelings. Nevertheless, about 50 % of the respondents rated the feedback as motivating and about 30 % as pleasant. This is related to the results regarding the negatively connoted feelings, which were rated as almost completely absent. The feelings "dangerous" and "irritating" received 7.7 % approval, while "frustrating" (0 %) was completely absent from the subjective evaluation.
To summarise the results presented for research question 2, it can be said that the acceptance is quite good for a first evaluation. The vibrotactile feedback perception is already at a very good level and there are very low ratings for negative emotions. However, improvements in all aspects are desirable for the future. The main aspect that needs improvement in the current situation is the directional content that the feedback can provide.
4. Discussion
The purpose of this feasibility study was to investigate whether this technology-based feedback approach is suitable as a correction tool for the execution of trunk-stabilising exercises and how it is perceived. In this context it was examined, to which extend the subjects were able to correct their execution in real time in response to given vibrotactile impulse. The vast majority of the test persons rated the feedback as helpful for the implementation of the exercises. The physiotherapists also rated independently of each other that the test persons were able to implement the vibrotactile feedback instructions initiated by them well to very well and were accordingly able to correct the exercise execution in real time without interrupting the flow.
Quality of movement and feasibility
As a general starting point, it was important to determine whether vibrotactile technology-assisted feedback can have a general and positive effect on the exercise execution. The results showed the general functionality as well as the quality of the feedback technique in a physiotherapy setting.
The results for practicability showed good ratings. The subjects were able to integrate the feedback into their movements. Both the best and worst perceptions were attributed to reimpulsive feedback points (under back/ 92.3 %; hip ventral 69.2 %), which is consistent with previous studies (20,22). In contrast, attractive feedback was used for the activation exercise of the trapezius pars transversa / trapezius pars ascendens muscle. In this case, 84.6 % of the subjects rated the intensity of the feedback as easily noticeable. Although this study focuses on the recording of subjective user sensations and not on measurements of vibrotactile detection, the results suggest that it is possible to use both reimpulsive and attractive feedback in vibrotactile feedback training of trunk stabilising exercises. It might be interesting to collect ratings on the users subjective preference regarding the two feedback strategies in future research.
Workload
The result for mental demand can be classified as a medium value (mean 47.7). It is in an absolutely acceptable range for the task and indicates that the required mental capacities are not too loaded by the processing of the vibrotactile feedback. Users should therefore be able to use the system without too much workload. The highest scores were obtained for physical demand and effort. Both describe aspects strongly associated with physical activity, with a higher score being acceptable due to the characteristics of the exercises. Nevertheless, the results for physical demand and effort are acceptable as long as they do not prevent the subjects from completing their tasks. The result for time demand is very low, indicating that the subjects did not feel much time pressure during the exercises. Frustration also reached a low level, which shows indicating that the subjects did not feel very frustrated or insecure during the implementation. These results are consistent with the subjective rating of the negatively connoted feedback-associated feelings listed under associated feelings in Research Question 2, with frustration at 0 %, being not chosen by any participant. The value for performance is located in the middle range of values. It was expected that the expression for achievement would be between medium and high values, since getting feedback obviously means that the subject is doing something wrong that needs to be corrected. Any correction can of course be attributed to poor performance. This may diminish the rating of the degree of success on this variable. So the results show a desirable result because the score is still relatively low. This is a very positive result, because the subjects do not seem to interpret the receipt of feedback as failure, which can lead to negative emotions.
Intensity of the vibration
An essential question related to this second research question is whether the vibrotactile feedback during the execution of an exercise is strong enough to be perceived by the user. The analysed data show that the quality of feedback perception was generally perceived as good. However, the perception varied depending on the body part addressed. The vibrotactile feedback is perceived less well at positions far from the head than at positions close to the head. For example, perception at the hips and stomach is less good than at the upper body areas. This is largely in line with the results of Bao et al. 2019 who used a similar approach in their study and found shorter reaction times for healthy adults at feedback points close to the head compared to feedback points far away. This could be due to the fact that the receptor density and the size of the receptive fields are related to the cortical representation and therefore the tactile spatial acuity of the skin and the density of the mechanoreceptors in different areas of the body vary greatly (27). This means that both the perception and the neuromuscular response to vibrotactile stimuli are favoured in densely populated body regions, which are particularly close to the head (22). Therefore, it is recommended to vary the intensity of the vibrations depending on the body region in future studies in order to achieve a similar perception for all body areas. To further optimise the feedback, it could be helpful to adjust the frequency of the feedback in addition to varying the intensity depending on body region. In this regard, the results of Stuart et al. 2003 can be interpreted, who were able to determine different detection thresholds between different body regions in healthy individuals (28). They substantiate their results with the fact that vibrotactile sensitivity depends on different groups of peripheral receptors, which can be differentiated into four different channels. These have the ability to perceive both high-frequency (60-1000 Hz) vibrations and, due to their fast-adapting afferent fibres also low-frequencies (0.4-100 Hz). Depending on the size of the receptive fields and the density of the receptors, there are clear differences between bald skin areas and hairy skin areas with regard to vibrotactile sensitivity (28). In addition, Morioka et al. 2005 were able to observe a correlation in the perception of threshold values of vibration depending on size and location of the actuator. The effect varied with regard to proximal or distal positioning (29). The aspect of different perceptual sensitivity depending on the location of the actuators on the body should also be taken into account when deciding whether to use attractive or reimpulsive feedback (30). An additional interesting aspect of the results is that no subject chose the anchor "too strong" as an option for vibration intensity. It would be interesting for future research to generally test at what intensity a vibration is perceived as "too strong" in a realistic context and whether "too strong" even exists in certain or all areas. If this is not the case, the vibration intensity for embodied feedback technology can be further increased. This can reduce the risk of users perceiving it as too weak to almost zero. This has the potential to minimise the system's susceptibility to error.
Perceived purpose of the feedback
Apart from the basic perception of the feedback, the purpose that the user associates with it is crucial. If the feedback is interpreted differently than intended by the designers and physiotherapists, this can lead to serious discrepancies between the intention of the feedback and the user's actions after correction. The feedback was not perceived as meaningless at all (0 %), which indicates that it conveys information to the subjects. The majority of respondents classified the feedback as indicative (84.60 %) and supportive (69.20 %). Here it would be desirable to achieve even higher values in the future. However, it is not possible to deduce from the quantitative data how the implementation of instructions for action can be improved. A possible starting point for future research could be the design of the vibration pattern. However, it was only perceived as guiding by a small proportion of respondents (30.80 %). It can therefore be assumed that directional instructions cannot yet be optimally implemented. Again, it cannot be deduced from the quantitative data how the implementation of directional instructions can be improved. Moreover, it was not perceived as alarming (0 %), a mediated purpose that can lead to negative emotions. The purpose of warning, which could also trigger negative emotions, was assigned to feedback at 23.10 %, indicating a more urgent interpretation compared to the other assigned adjectives. Both warn and alert imply urgency, more so than support, point out or similar. In this respect, the low approval rate for feedback with these connotations is positive, as the negative emotions associated with urgency (e.g. panic, fear, etc.) are avoided. For future application purposes, it would be interesting to test the effect on subjects of vibrotactile patterns associated with a warning. In the long term, a gradation of feedback patterns between "pointing out/supporting" for minor error behaviour over a short period of time and "warning" for potentially harmful and/or long-lasting error behaviour could be realised.
Feedback-associated affective emotions
In general, the emotions with positive connotations were rated "does not apply" in the majority of cases (between 54 % and 100 %). About 50 % of the respondents rated the feedback as motivating and about 30 % as pleasant. This is related to the results regarding the negatively connoted feelings, which were rated as almost completely absent. The feelings "dangerous" and "irritating" received only 7.7 % approval, while "frustrating" (0 %) was completely absent from the subjective evaluation. The absence of frustration is nevertheless very positive for the proposed vibrotactile feedback method. In particular, the absence of "irritating" and "frustrating" is an important result here. If the system were irritating, it would most likely lead to less good or even worse posture correction. It may also lead to higher frustration scores because the user would not know what to do when feedback is given. In the absence of these issues, it can be concluded that the feedback technology, derived from the data, is generally functional, with some room for improvement in identified areas. Overall, it can be assumed that subjects tend to rate feedback as neutral due to the absence of negative emotions and the relative absence of positive emotions. This is a landmark finding for the future of technology. It may not be necessary for the system to be associated with positive emotions; rather, it is necessary not to arouse negative emotions through further developments.
5. Conclusions
In this feasibility study, we investigated for the first time the practicability of a vibrotactile feedback system for motion guidance in the context of physiotherapy. We did not only proof the technological and clinical feasibility but also the user experience and acceptance of such a system at the same time. By that, we can show that the use of real-time feedback via a haptic waistcoat could be a promising approach to correct trunk-stabilising exercises. The results of the expert evaluation indicate a significant improvement of quality of movement trough the vibrotactile feedback and can be compared with the effect of the “real” haptic feedback of a physiotherapist. On top, the physiotherapists rated the ability of implementation as high. That results in the overall assessment of the experts that such a system has a high practicability for remote active motion guidance. The results of the NASA TLX questionnaire suggest that the use of such a system can reduce the trainees' fear of independent training and support the users instead. In order to increase the trainees' motivation, it could be considered in the future to underpin the vibrotactile feedback with an acoustic feedback which motivates the user with positive statements when the movement is performed more correctly. Thus, in the setting of a home-based training, this system could increase the training fidelity and the long-term success. In addition, follow-up work should investigate whether the perception of body parts such as the abdomen or hips can be improved in healthy people by adjusting the vibrotactile parameters as intensity or frequency. Furthermore, it should be tested whether back pain patients react similarly to healthy persons to the vibrotactile feedback or whether the feedback must be fundamentally changed in this cohort. This also concerns the positioning of the sensors in pain patients. Here, it must be checked which distance from the pain point must be maintained in order not to increase the pain due to the haptic feedback but nevertheless to achieve the desired movement correction.
Author Contributions
Conceptualization, P.F. and L.M.L.; methodology, P.F. and J.S.; software, L.M.L.; data curation, P.F. and L.ML.; writing—original draft preparation, P.F. and J.S.; writing—review and editing, L.M.L., N.P., J.F., F.K., D.L., J.K., U.P. and A.C.D.; visualization, P.F.; supervision, J.K. and A.C.D.; project administration, P.F. and L.M.L. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
The study was performed in accordance with the Declaration of Helsinki and was approved by the Ethics Committee at TU Dresden (protocol code: BO-EK-215052022) on 07 June 2023.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest
References
- Aboagye E, Lilje S, Bengtsson C, Peterson A, Persson U, Skillgate E. Manual therapy versus advice to stay active for nonspecific back and/or neck pain: a cost-effectiveness analysis. Chiropr \& Man Ther. 2022;30(1):1–10. [CrossRef]
- Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non-specific low back pain. Lancet. 2012;379(9814):482–91.
- Apeldoorn AT, Ostelo RW, van Helvoirt H, Fritz JM, de Vet HCW, van Tulder MW. The cost-effectiveness of a treatment-based classification system for low back pain: design of a randomised controlled trial and economic evaluation. BMC Musculoskelet Disord. 2010 Mar;11:58. [CrossRef]
- Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356–67. [CrossRef]
- Harris SA, Rampersaud YR. The importance of identifying and modifying unemployment predictor variables in the evolution of a novel model of care for low back pain in the general population. Spine J. 2016;16(1):16–22. [CrossRef]
- Abdelraouf OR, Abdel-aziem AA. The relationship between core endurance and back dysfunction in collegiate male athletes with and without nonspecific low back pain. Int J Sports Phys Ther. 2016;11(3):337.
- Ferreira PH, Ferreira ML, Maher CG, Refshauge K, Herbert RD, Hodges PW. Changes in recruitment of transversus abdominis correlate with disability in people with chronic low back pain. Br J Sports Med. 2010 Dec;44(16):1166–72. [CrossRef]
- Lemos LFC, Teixeira CS, Mota CB. Low back pain and corporal balance of female brazilian selection canoeing flatwater athletes. Brazilian J Kinanthropometry Hum Perform. 2010;12(6):457–63.
- Mueller J, Mueller S, Stoll J, Baur H, Mayer F. Trunk extensor and flexor strength capacity in healthy young elite athletes aged 11--15 years. J Strength Cond Res. 2014;28(5):1328–34. [CrossRef]
- Engel T, Arampatzis A, Català MM, Kopinski S, Mayer F. Perturbations in Prevention and Therapy of Low Back Pain: a New Approach. Ger J Sport Med Zeitschrift fur Sport. 2018;69. [CrossRef]
- Fleckenstein J, Floessel P, Engel T, Klewinghaus L, Stoll J, Behrens Ma, et al. Individualised exercise in chronic non-specific low back pain: a systematic review with meta-analysis on the effects of exercise alone or in combination with psychological interventions on pain and disability. medRxiv. 2021;
- Ogbeivor C, Elsabbagh L. Management approach combining prognostic screening and targeted treatment for patients with low back pain compared with standard physiotherapy: A systematic review & meta-analysis. Musculoskeletal Care. 2021 Mar; [CrossRef]
- Sowden G, Hill JC, Morso L, Louw Q, Foster NE. Advancing practice for back pain through stratified care (STarT Back). Brazilian J Phys Ther. 2018;22(4):255–64.
- Salkeld G, Cumming RG, Thomas M, Szonyi G, Westbury C, O’Neill E. The cost effectiveness of a home hazard reduction program to reduce falls among older persons. Aust N Z J Public Health. 2000;24(3):265–71. [CrossRef]
- Hohmann E, Tetsworth K, Bryant A. Physiotherapy-guided versus home-based, unsupervised rehabilitation in isolated anterior cruciate injuries following surgical reconstruction. Knee surgery, Sport Traumatol Arthrosc. 2011;19:1158–67. [CrossRef]
- Szabo D, Gulyas A, Fitzek FHP, Lucani DE. Towards the tactile internet: Decreasing communication latency with network coding and software defined networking. In: Proceedings of European Wireless 2015; 21th European Wireless Conference. 2015. p. 1–6.
- Sigrist R, Rauter G, Riener R, Wolf P. Augmented visual, auditory, haptic, and multimodal feedback in motor learning: a review. Psychon Bull \& Rev. 2013;20(1):21–53. [CrossRef]
- Asseman F, Bronstein AM, Gresty MA. Using vibrotactile feedback of instability to trigger a forward compensatory stepping response. J Neurol. 2007;254(11):1555–61. [CrossRef]
- Kinnaird C, Lee J, Carender WJ, Kabeto M, Martin B, Sienko KH. The effects of attractive vs. repulsive instructional cuing on balance performance. J Neuroeng Rehabil. 2016;13(1):1–5.
- Ma CZ-H, Lee WC-C. A wearable vibrotactile biofeedback system improves balance control of healthy young adults following perturbations from quiet stance. Hum Mov Sci. 2017;55:54–60. [CrossRef]
- Nanhoe-Mahabier W, Allum JH, Pasman EP, Overeem S, Bloem BR. The effects of vibrotactile biofeedback training on trunk sway in Parkinson’s disease patients. Park \& Relat Disord. 2012;18(9):1017–21.
- Ballardini G, Florio V, Canessa A, Carlini G, Morasso P, Casadio M. Vibrotactile feedback for improving standing balance. Front Bioeng Biotechnol. 2020;8:94. [CrossRef]
- Islam MS, Lim S. Vibrotactile feedback in virtual motor learning: A systematic review. Appl Ergon. 2022;101:103694.
- Galy E, Paxion J, Berthelon C. Measuring mental workload with the NASA-TLX needs to examine each dimension rather than relying on the global score: an example with driving. Ergonomics [Internet]. 2018;61(4):517–27. Available from: http://doi.org/10.1080/00140139.2017.1369583.
- Kim E, Schneider O. Defining haptic experience: Foundations for understanding, communicating, and evaluating HX. In: Proceedings of the 2020 CHI conference on human factors in computing systems. 2020. p. 1–13.
- Bao T, Su L, Kinnaird C, Kabeto M, Shull PB, Sienko KH. Vibrotactile display design: Quantifying the importance of age and various factors on reaction times. PLoS One. 2019;14(8):e0219737. [CrossRef]
- Stuart M, Turman AB, Shaw J, Walsh N, Nguyen V. Effects of aging on vibration detection thresholds at various body regions. BMC Geriatr. 2003;3:1–10. [CrossRef]
- Morioka M, Griffin MJ. Thresholds for the perception of hand-transmitted vibration: Dependence on contact area and contact location. Somatosens \& Mot Res. 2005;22(4):281–97. [CrossRef]
- Tannert I, Schulleri KH, Michel Y, Villa S, Johannsen L, Hermsdörfer J, et al. Immediate effects of vibrotactile biofeedback instructions on human postural control. In: 2021 43rd Annual International Conference of the IEEE Engineering in Medicine \& Biology Society (EMBC). 2021. p. 7426–32.
Figure 1.
Actuator fixation of vibrotactile feedback.
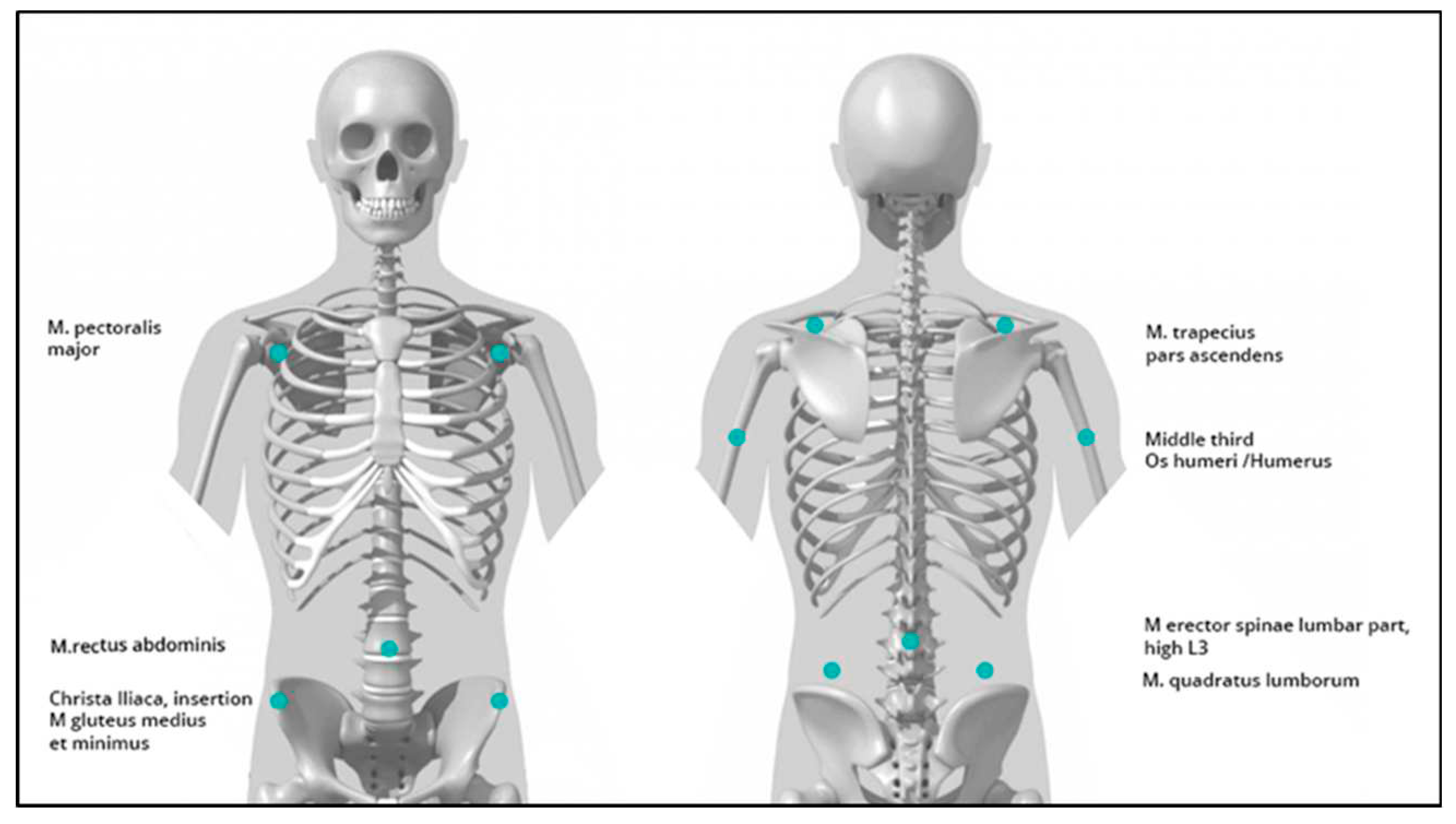
Figure 2.
trunk train exercise portfolio.

Figure 3.
subscales of emotional feedbacks of the NASA TLX questionnaire.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



