
Submitted:
05 January 2024
Posted:
05 January 2024
You are already at the latest version
Abstract
Workplace exercise programs are imperative for improving employee health and wellbeing. Employee cognition and productivity can also benefit from such programs; however, the practical application of interventions to influence these outcomes is poorly understood. This research aimed to assess the suitability of a university Staff Fitness Program for improving employee productivity and cognition. Forty-seven participants were included in the study, comprising 27 Staff Fitness participants and 20 control group participants. A two (groups) x three (time-points) between-subjects/within-subjects design was employed over 14 weeks, comprising ten weeks of once-weekly exercise intervention for Staff Fitness participants. All participants completed the Victoria Stroop Colour and Word Test and the Health and Work Questionnaire at each time-point, to assess cognition and productivity, respectively. Participants also completed the International Physical Activity Questionnaire (short form) at time-point one, three and during training weeks (excluding week one) to measure physical activity. Appropriate T-tests and non-parametric equivalents were used to assess group differences in outcome measures and across time-points. There were no significant between group or longitudinal differences indicative of improved productivity or cognition. The Staff Fitness group demonstrated a non-significant improvement (Z = 73.00, p = .055) in physical activity from time-point one (M = 1540.93 MET-min-week, SD = 1083.74) to three (M = 2077.32 MET-min-week, SD = 1401.48) with a large effect size (d = 0.97), while control group physical activity significantly decreased (Z = 10.00, p = .013). The present Staff Fitness Program benefited employees by improving physical activity, despite no improvements in productivity or cognition. Future research should further explore the application of workplace exercise programs and the manipulation of exercise parameters to show improvements in employee productivity and cognition.
Keywords:
Cognition
; productivity
; employee health and wellbeing
; exercise
; workplace exercise program
1. Introduction
In 2022, 5.5 million years of healthy life were lost in Australia from fatal and non-fatal burden of disease, with 62% of this burden being comprised of five major disease groups including cancer, musculoskeletal diseases, mental health conditions, neurological conditions and substance use disorders [1]. Australian health is worsening, with two thirds of the adult population classified as obese and 40% estimated to experience a mental disorder during their life [2]. Lifestyle behaviours greatly contribute to this poor health, as modifiable risk factors account for one third of disability adjusted life years (DALY’s) [2]. One modifiable risk factor is physical inactivity, yet currently 75% of the population aged 18-64 do not meet the national aerobic and resistance training guidelines [3]. This physical inactivity epidemic requires novel solutions, one of which may include the integration of exercise programs at work for improved accessibility and convenience. Such programs have demonstrated the ability to improve employee physical activity, cardiovascular and musculoskeletal disease risk, respiratory function and body composition [4]. These programs are also proposed to enhance cognition, an additional component of wellbeing [4,5]. Specifically, cognition is critical to all voluntary actions, including occupational success and functional independence [6]. Our cognitive abilities also mediate how we interact with the world and have been linked to psychosocial functioning and the attainment of goals, which fosters a greater sense of life satisfaction [6,7]. Improved cognition and other associated benefits of exercise can also benefit workplace productivity [6,8]. However, more research is needed to evaluate the relationship between exercise with productivity and cognitive outcomes to optimise the implementation of workplace wellness programs for employees and corporations [5,9].
Productivity describes the amount of work output by an individual or corporation, the loss of which can be categorised as absenteeism or presenteeism [9]. Absenteeism is simple to measure and describes lost productivity due to employees being absent from work [9]. Presenteeism can be perceived as the loss of productivity where employees are present at work, but not fully productive due to health problems or other events that might normally compel absence [10]. In this context, exercise can reduce absenteeism and presenteeism by improving physical health [4,8]. Exercise can also reduce presenteeism by increasing work capacity through cognitive and physical enhancement, while additioanlly mitigating against wellbeing implications of the modern-day work environment such as mental and emotional exhaustion [11,12]. Workplaces commonly seek to increase employee physical activity through environmental modifications and incidental activity incentives, therefore, improving productivity [8]. These interventions including sit to stand desks, step count challenges and the introduction of exercise facilities, all have mixed productivity and physical activity outcomes [10,13,14,15,16,17,18,19]. Intentional aerobic and resistance based exercise can also be incorporated into workplaces through individaul and group exercise classes at home and in the workplace. These types of interventions achieve mixed productivity and physical activity outcomes, but are more likely to have positive effects compared to interventions targeting environmental modification and incidental activity such as step count challenges [8,10,20]. Consistent parameters that improve the likelihood of positive outcomes are unclear, due to the heterogeneity of exercise interventions [8]. However, longer and multifaceted programs appear more successful than shorter and unidimensional ones [8,21]. Despite a lack of consensus surrounding best practice and less than half of implemented interventions being successful, workplace exercise programs are still encouraged by governments and corporations as a part of general occupational health promotion [10,22]. For this reason, it is critical to further explore what types of exercise interventions are optimal in terms of employee health and wellbeing outcomes, including cognition and productivity [10].
Improved employee cognition from exercise benefits individual and corporate wellbeing, however, further research is also required to elucidate how this can be practically achieved [23]. Exercise can improve global cognitive abilities as well as narrow abilities in all demographics, which are both important for overall wellbeing and job performance [6,7,24,25]. Specific narrow abilities improved through exercise include inhibitory control, working memory and cognitive flexibility, which all comprise ‘executive function’, a subset of capacities involved in the cognitive control of behaviour [26]. Other narrow abilities, such as attention, are malleable with exercise as well, however, those comprising executive function are most responsive [27,28]. Exercise can improve cognition through acute and chronic increases in cerebral perfusion, which enhances the delivery of oxygen and glucose to the brain [28,29,30]. Other acute and longitudinal neurophysiological changes include increased P3 wave amplitude and decreased latency, diminished beta-amyloid accumulation and increased homocysteine concentrations [31,32]. Exercise can also improve cognition through the upregulation of hormones such as brain-derived neurotrophic factor (BDNF) and insulin growth factor one (IGF-1), which increase neuroplastic processes such as synaptogenesis and long-term potentiation [30,31]. These neuroplastic processes lead to long-term neuroanatomical adaptations such as increased gray and white matter volume [30,31]. Cognitive improvement through neural adaptation is evident via exercise [31]. However, the practical delivery of workplace exercise intervention to fulfill this capacity is not well understood [23].
Research demonstrates a precise dose-response relationship and minimal effective dose between physical activity and cognitive adaptation for elderly individuals [25]. However, studies investigating the impact of exercise on cognitive abilities in younger demographics, including working adults, are scarce. This is because there is little motivation for researchers to examine younger populations as they are at their lifetime peak of cognitive health [33]. Targeting cognition with exercise in all age-groups is imperative, as cognitive decline begins at 20 years of age, with memory function declining by 8% and executive function declining by 7% with each decade of age onwards [34,35]. Additionally, with sedentary behaviour increasing and the importance of cognitive function for work performance and general wellbeing, it is necessary to develop and identify suitable intervention to improve cognitive functioning in all demographics [23]. Therefore, the purpose of this study was to examine the impact of a university workplace exercise intervention on employee productivity and cognition. It was hypothesised that the program would have a significant positive effect on both productivity and cognitive outcomes.
2. Materials and Methods
2.1. Ethics and consent
This project received ethical approval by the Human Research Ethics Committee at the University of Notre Dame Australia (UNDA), Fremantle, on 25/06/2019 (HREC number: 019014F). A further ethics amendment was submitted to include various methodologies and approved on 01/02/2023. All participants were provided an information sheet and fully informed of the nature and possible risks of procedures before providing written informed consent.
2.2. Participants
Forty-seven staff members volunteered to participate in this study from the UNDA, Fremantle Campus. Twenty-seven participants took part in the Staff Fitness Program, while 20 participants composed the control group. Staff Fitness sample size was limited due to the availablity of student trainers (final-year Exercise & Sport Science students), and a maximum amount of volunteer control participants were recruited. Exclusion criteria included changes to medications throughout the intervention that may have interfered with cognition. Staff Fitness participants also completed the ESSA Adult Pre-Exercise Screening system (APSS) [36] prior to training, and were excluded if not medically fit to partake in exercise. Control participants weren’t required to complete the APSS as they didn’t receive any exercise delivery from the Staff Fitness Program.
2.3. Study Design
The present study used a two (groups) x three (time-points) between-subjects/within-subjects design, with a total duration of 14 weeks, comprising ten weeks of exercise intervention (Staff Fitness participants only) and the completion of all testing procedures. A visual depiction of the experimental design and timeline for this intervention is provided in Figure 1. Staff Fitness participants (n=27) completed a once-weekly personalised and goal-oriented exercise training program, prescribed and delivered by a final-year Exercise and Sport Science student trainer, within the UNDA Human Performance Lab. While the volume of face-to-face exercise training was one hour per week, students could prescribe independent exercise for participants to complete externally and generally promoted the importance of physical activity to their staff participant. The student trainers were required to prescribe exercise tailored to the unique fitness goals of each participant, with 20 participants requesting to focus on health and wellbeing outcomes, and six participants requesting to focus on performance outcomes. The control group (n=20) were instructed to maintain their typical exercise and physical activity habits throughout the study period. To note, the Staff Fitness Program serves as a formal teaching and learning program among the final-year Exercise and Sport Science student cohort, with their exercise prescription and other professional qualities assessed in accordance with Exercise and Sport Science Australia’s (ESSA) professional standards for accreditation [37].
2.4. International Physical Activity Questionnaire – Short Form
The International Physical Activity Questionnare – Short Form (IPAQ-SF) was used to evaluate physical activity behaviour across the study and was completed through the online survey platform Qualtrics [38]. The IPAQ-SF is a valid and reliable (r = 0.66-0.88) measure of total activity, measured through metabolic equivalent of tasks per week (MET-min-week) and hours spent sitting per week (r = 0.71-0.95) [39]. Participants completed the IPAQ-SF during each training week (not including week 1) as well as at time-points one and three, which totalled ten measurements throughout the intervention.
2.5. Health and Work Questionnaire
The Health and Work Questionnaire (HWQ) was completed by participants via Qualtrics at time-points one, two and three [38]. This questionnaire was used to measure subjective ratings of workplace productivity via 30 questions on a 10 point Likert scale, that were grouped into subscales [40]. The HWQ is validated against objective measures of workplace productivity and all subscales demonstrate excellent internal consistency reliability (α0.84–0.96), apart from the ‘irritability/impatience’ subscale which has adequate reliability (α0.72) [40]. Averages were calculated for the HWQ subscales: concentration/focus, impatience/irritability, supervisor relationships, work satisfaction, non-work satisfaction, total productivity, supervisor perceived productivity, self-rated productivity and overall score. A higher score is indicative of greater performance in that subscale and therefore, greater productivity.
2.6. Victoria Stroop Colour and Word Test
The Victoria Stroop Colour and Word Test (VSCWT) is a common measure of executive function and inhibitory control [41]. The VSCWT was selected due to its greater reliability for the dot, word and colour sections (r = 0.90, r = 0.83, r = 0.91) than the more popular Golden version (r = 0.89, r = 0.84, r = 0.73) [41,42,43]. The VSCWT is also preferable due to its shorter subsections, as shorter tasks have been evidenced to be more successful at identifying individuals with poor cognitive function [44]. A computerised version of the VSCWT [45] was administered through the Psychology Experiment Building Language (PEBL), a free testing battery [46]. No settings were augmented and testing was completed on a university laptop running Windows 10 [47]. This computerised version of the VSCWT has been used in other studies and was selected due to its ability to measure reaction time more accurately [48,49]. Participants completed one practice run of the VSCWT at each time-point, as suggested in other studies to account for learning effects [50,51]. Numbers one to four on the number pad were used to respond to stimuli, with these keys coloured to mitigate against added cognitive interference for participants. Participants were asked to refrain from consuming caffeine within 12 hours of testing, alcohol within 24 hours and to refrain from intentional exercise 48 hours prior to testing.
The VSCWT consists of three parts, each with 24 stimuli, presented in Figure 2. Participants were not permitted to move past a stimuli until it was answered correctly and the total time taken to complete each stage alongside accuracy was recorded. The first stage of the VSCWT (Dot) involves the presentation of coloured dots, requiring participants to respond to the ink colour of each stimuli presented. The second stage of the test (Word) involves the presentation of common words in coloured ink, where participants are once again required to respond to the ink colour of each stimuli presented. The third stage (Colour) contains the names of colours printed in non-congruent ink. In this stage, participants are required to respond to the ink colour of each stimuli and ignore the semantic meaning of the word. Two interference scores are calculated to measure executive function through the VSCWT by comparing the time taken to complete the stages with added cognitive interference to the time taken to complete the simple ‘Dot’ task. The two interference scores are calculated as below:
Word/Dot interference = Word (seconds)/Dot (seconds)
Colour/Dot interference = Colour (seconds)/Dot (seconds)
2.7. Confounding factors
Confounding factors including perceived hydration, hours fasted, hours of sleep, quality of sleep, subjective health (illness), and medications, were measured prior to each cognitive testing session through Qualtrics [38]. Subjective stress was also measured at each testing time-point via the Perceived Stress Scale (PSS), which is a valid and reliable measure of stress (ICC > 0.70) [53]. Violation of exercise, caffeine and alcohol controls were also measured through qualtrics prior to cognitive testing. Participant demographics including profession, age and gender were collected at the beginning of the study.
2.8. Statistical analysis
All measures were scored and recorded according to methodological instructions and then entered into Microsoft Excel [54]. Missing data was excluded from analysis. Data cleaning and checking was undertaken in Microsoft Excel before data was imported into IBM SPSS (version 28.0.1.0) for statistical analysis [55].
Data for outcome measures were described using means (M) and standard deviations (SD) while participant characteristics and responses were described using frequencies (N). Scored measures were assessed for normality using shapiro-wilks tests, skewness, kurtosis and normality plots. Between group (control / intervention) differences were assessed using Independent T, Mann-Whitney U, Chi-Square or Fishers exact tests as appropriate. Intragroup differences over time were assessed using paired T and Wilcoxon Signed Rank Tests. Effect sizes were calculated for the IPAQ-SF using an augmented Cohens d calculation from Hedges and Olkin [56] to account for differing sample sizes. Effect sizes for the HWQ and VSCWT were calculated using the method from Morris [57], which allows for the comparison of mean differences of unequal sample sizes within a pre-post control design. Effect sizes were categorised as being small (< 0.2), moderate (< 0.50) or large (> 0.80) for both methods.
Generalised estimating equations were used to explore differences in outcome measures for the VSCWT and HWQ. The group of participants (control / intervention), test occasion and confounding factors including profession, mean MET-min-week and the number of days between testing were treated as fixed effects. Age was also included as a confounding factor for the VSCWT outcome measures. Participant code was included as a repeated measure. Tests of model effects and statistical significance were examined along with Bonferroni post hoc comparisons and parameter estimates.
3. Results
3.1. Participant characteristics
Three participants were excluded from the study due to changes in medication, therefore data from 26 Staff Fitness participants and 18 control participants was used for statistical analysis. No participants were excluded after completion of the APSS. Sample sizes differ between measurements and time points due to illness, non-compliance and absence from work. Demographic details for Staff Fitness and control participants are presented in Table 1.
3.2. Confounding factors
There were no significant between group differences detected in age, or sex, however, there was a significant difference for profession (p = .028), with more full-time professional staff in the Staff Fitness group, and more full-time academics in the control group. Prior to cognitive testing, there were no significant differences in the time of day tested, hours fasted, hours of sleep, quality of sleep, perceived hydration, illness, stress or violation of alcohol, caffeine, and exercise controls. Staff Fitness participants were tested later (M + 5.75 days, SD = 5.46, p=.020) at time-point three than control participants. This occurred due to the logistics of testing 47 participants and the necessary time to complete the relevant procedures at a similar time of day to the other testing time-points.
3.3. International Physical Activity Questionnaire – Short Form
Results for the IPAQ-SF are presented in Table 2. The Staff Fitness group were significantly less active (M = 1540.93 MET-min-week, SD = 1083.74) than the control group (M = 2368.80 MET-min-week, SD = 1377.70) at time-point one (week one) (Z = 88.00, p = .039). The Staff Fitness group were more active (M = 2077.32 MET-min-week, SD = 1401.48) than the control group (M = 1699.50 MET-min-week, SD = 1359.31) at time-point three (week 13), with a non-significant between group difference (Z = 88.00, p = .370) and small effect size (d = 0.27). Physical activity levels at time-point three (M = 1699.50 MET-min-week, SD = 1359.31) were significantly lower than time-point one (M = 2368.80 MET-min-week, SD = 1377.70) for the control group (Z = 10.00, p = .013). The Staff Fitness group showed a non-significant improvement with a large effect (d = 0.97) in physical activity from time-point one (M = 1540.93 MET-min-week, SD = 1083.74) to three (M = 2077.32 MET-min-week, SD = 1401.48) (Z = 73.00, p = .055). Data for the IPAQ-SF is represented visually in Figure 3, which shows the Staff Fitness group becoming more active from week seven of the study onwards. No significant differences in time spent sitting per week were detected, nor any meaningful associated effect sizes.
3.4. Health and Work Questionaire
Results for the HWQ are presented in Table 3. There was no significant difference at time-point three between the Staff Fitness (M = 7.14, SD = 0.88) and control group (M = 7.18, SD = 0.89) for overall HWQ score (t(29) = 0.109, p = .914). There was a small effect size (d = 0.08) from the start to the end of the intervention for the Staff Fitness group in comparison to the control group. The control group did experience a significant decrease in concentration/focus score from time-point one (M = 7.31, SD = 2.37) to two (M = 6.28, SD = 2.23) (Z = 16.00, p = 0.039) with a moderate effect size in comparison to the Staff Fitness group (d = 0.55). No significant difference was detected between the Staff Fitness (M = 6.92 , SD = 1.71) and control group (M = 6.61 , SD = 1.76) at the end of the intervention in concentration and focus (Z = 146.00, p = .725). Concentration and focus increased more for the Staff Fitness group with a small effect (d = 0.44) in comparison to the control group from time-point one to three.
Mean subscale scores were higher midway through the intervention compared to baseline for Staff Fitness participants, however these were not statistically significant and effect sizes small (d = 0.20-0.36). The exception was concentration/focus, which reported a moderate effect size (d = 0.55).
3.5. Victoria Stroop Colour and Word Test
The results for the VSCWT can be seen in Table 4. The control group had a significantly higher Word/Dot interference score (M = 1.10, SD = 0.11) than the Staff Fitness group (M = 1.03, SD = 0.11) at time-point one (t(40) = 2.05, p = .047). However, at time-point three, no significant group difference was detected (Z = 217.00, p = .774). The control group had a significant improvement in Word/Dot interference score from time-point one (M = 1.10, SD = 0.11) to two (M = 0.99, SD = 0.18) (Z = 30.00, p = .049), with a large effect size (d = 0.89) in comparison to the Staff Fitness group. However, this improvement was non-significant from time-point one (M = 1.10, SD = 0.11) to three (M = 1.03, SD = 0.14) (t(15) = 1.88 , p = .080), with a moderate effect size (d = 0.71).
No significant group differences in Colour/Dot interference score were detected at time-point one (Z = 188.00, p = .530) or three (t(38) = -1.231, p = .226) respectively. There was a non-significant improvement for the control group with a small magnitude of effect (d = 0.26) in comparison to the Staff Fitness group from time-point one (M = 1.21, SD = 0.13) to three (1.16, SD = 0.16) (t(15) = 1.28, p = .220).
The Staff Fitness group experienced a significant improvement in time taken to complete the ‘Dot’ task from time-point one (M = 19.93, SD = 5.43) to three (M = 18.77, SD = 4.63) (Z = 65.00, p =.026). The Staff Fitness group also experienced a significant improvement in time taken to complete the ‘Word’ part of the test from time-point one (M = 20.26, SD = 4.47) to three (M = 19.20, SD = 4.18) (Z = 203.00, p = .048).
3.6. Longitudinal changes over time
Generalised estimating equations were explored to examine the changes in outcome measures over time, between control and intervention groups while accounting for identified confounding variables. Unfortunately, the large variability in IPAQ-SF scores and the relatively small sample size did not allow convergence to a model solution. Hence, no results are able to be reported.
4. Discussion
This study evaluated the impact of the UNDA, Fremantle, Staff Fitness Program on employee productivity and cognition. There were no statistically significant longitudinal or between group differences indicative of improved performance for the Staff Fitness group. Therefore, these results support the null hypothesis, that the intervention was ineffective at improving employee productivity or cognition. Exercise can improve cognition through neurophysiological and neuroanatomical adaptation [31]. Exercise can also benefit objective and subjective productivity by improving employee health and work efficiency [8]. The absence of significant outcomes in this study suggests that the Staff Fitness Program exercise parameters (frequency, intensity, type and time), which included ten weeks of once-weekly, mixed modality, moderate to high-intensity exercise, were insufficient [58]. Despite this, the Staff Fitness group started the intervention significantly less active than the control group and experienced a non-significant improvement in physical activity from time-point one to three, with a large effect size. Meanwhile, the control group experienced a significant decrease in physical activity engagement. This finding suggests that the Staff Fitness Program may mitigate against increasing sedentary behaviour in university staff across semester. This is significant, as greater physical activity engagement is associated with improved employee health and wellbeing [59,60]
The lack of significant productivity outcomes from the Staff Fitness Program may suggest that improvements in productivity from workplace exercise are dose-dependent. Combined modality exercise programs, similar to the intervention in this study, can improve productivity outcomes [61,62,63,64]. However, due to the heterogeneity in design and assessment of these interventions, there is no guidance on the amount of exercise that should be delivered or any relevant parameters [8,10]. Studies with positive productivity outcomes involve a higher amount of exercise than implemented in the Staff Fitness Program, with training incorporated on 2 to 4 days of the week from 9 weeks to a year in duration [61,62,63]. Once-weekly intervention has shown significant improvements in productivity over the course of a year [64]. Another study incorporating once-weekly exercise over a six month period showed no significant outcomes, however, this program had poor compliance (<50%) and was low intensity in nature [65]. This suggests that a minimal effective dose does exist to yield exercise induced productivity improvements and that Staff Fitness Program parameters were insufficient. However, results from Justesen et al. and Dalager et al. [61,64] who achieved significant productivity improvements with the same weekly dose of exercise suggests that the Staff Fitness Program may be suitable with augmentation. To emulate these results, spreading exercise across multiple weekdays or increasing program duration may be required [61,64].
The lack of significant cognitive outcomes from the Staff Fitness Program may suggest that improvements in cognition from workplace exercise are also dose-dependent. The Staff Fitness group experienced a significant improvement in time taken to complete the ‘Dot’ and ‘Word’ parts of the VSCWT from time-point one to three. However, interference scores alone are typically used to assess inhibitory control and executive function; which did not significantly improve across the intervention [41]. Staff Fitness group performance in the ‘Dot’ task was also accompanied by a small effect size in comparison to the control group, suggesting that improvements may be due to learning effects or potential cognitive enhancement [41]. Finally, the significant improvement for the control group in Word/Dot interference score from time-point one to two is thought to be attributed to the increase in time taken to complete the ‘Dot’ task in relation to the Staff Fitness group. The only other study to examine the impact of intentional exercise on workplace cognition incorporated a lower weekly dose of exercise than the Staff Fitness Program [52]. This intervention by da Silva et al. [52] showed no significant changes in executive function from a 3-month flexibility intervention, with participants training for 10-15 minutes, three days of the week. In controlled environments, there is a lack of research looking into the impact of exercise on cognition in middle-aged adults, which further restricts the relevant contextualization of this study’s findings [33]. However, chronic exercise induced cognitive improvement is evident in both young adult and elderly populations [33,66,67,68]. Older adults respond to minimalisitc intervention, similar to the Staff Fitness Program, whereas young adults respond to intervention implemented 2 to 3 times a week for 8 weeks to 4 months [33,66,67,68]. These results suggest that the exercise parameters of the Staff Fitness Program were insufficient or too minimal to improve cognition, despite improvements in physical activity engagement.
Findings from this study showed that Staff Fitness physical activity levels improved non-significantly from time point one to three with a large effect size, while physical activity participation decreased significantly for the control group. Improving physical activity engagement is an important outcome of intervention, however, just over half of workplace wellness programs achieve significant difference in comparison to a control group [69]. Increasing physical activity engagement indicates improved quality of life and decreased risk of all-cause mortality [59,60]. Improvements in IPAQ-SF scores are inversely correlated with adverse health outcomes such as obesity, mental illness risk and blood pressure [70,71]. Greater physical activity has also been linked to better emotional health and psychosocial functioning [60,72]. Therefore, this intervention can be seen to have a positive impact on university staff by mitigating against increasing sedentary behaviour across semester, despite no evident improvements in productivity or cognition.
The UNDA, Fremantle, Staff Fitness Program therefore potentially benefits employee wellbeing and provides a workplace exercise intervention that addresses many common barriers for corporations and participants, including return on investment and a ‘one size fits all’ approach to training [8,73,74]. This program also presents an initiative with the potential to be implemented for free in all universities with a suitable Bachelor of Exercise and Sport Science (BESS) program. Results from this study advocate for this implementation, as improvements in physical activity were evident. The implementation of similar programs in other workplaces may require novel solutions, for example, telehealth to connect staff with student trainers. Future research should look at further modifying parameters of exercise to create interventions that can improve employee productivity and cognition. Research should also seek to further the Staff Fitness Program design, due to its applicability in most university settings and its evidenced success at improving employee physical activity engagement.
It must be acknowledged that the results attained from this study are only generalisable to the sample population, being middle aged university employees. There are also limitations to this study, including the self-report nature of the HWQ and IPAQ-SF, which may have encouraged self-reporting bias. Data analysis was also limited by the small sample size and large variability of various outcome measures, which prevented the use of linear models to evaluate longitudinal change while controlling for confounding factors. However, paired T and Wilcoxon signed rank tests were used to evaluate longitudinal change and independent T and Mann Whitney tests were used to evaluate between group differences at various time-points. During the intervention, there was an error in data collection for the HWQ. Therefore, one question pertaining to peer-perceived productivity was excluded, which resulted in the peer-perceived productivity subscale being excluded from further data analysis. All other questions from the peer-perceived productivity subscale were included in the total HWQ score but not the total productivity score. Finally, despite the practical benefit from the individualised structure of the Staff Fitness program, the inability to standardise activity parameters prevented the precise quantification of exercise and comparison to other interventions, thus demonstrating a limitation.
5. Conclusion
The Staff Fitness Program had a positive impact on employees through increasing physical activity levels, despite no improvements in productivity or cognition. This program provided a unique and practical intervention opportunity, where free and individualised training could be delivered to university staff across a semester. The individualised structure was a functional benefit of the program. However, this design was also a weakness, as the non-standardised training prevented the precise measurement and comparison of training parameters to other studies. Findings suggest that improvements in productivity and cognition are dose-dependent and that a higher dose of exercise than implemented in this intervention is required to see significant change in these variables. Despite this, universities with BESS programs and other workplaces should look to improve employee physical activity through implementing interventions similar to the Staff Fitness Program. Future research should further manipulate intervention design and exercise parameters to examine effects on employee productivity and cognition.
Author Contributions
Conceptualisation, A.C. and J.C.; methodology, A.C., J.P. and J.C.; software, J.P.; validation, J.P.; formal analysis, P.C. and J.P.; investigation, J.P.; resources, A.C., J.P. and J.C.; data curation, J.P.; writing—original draft preparation, J.P.; writing—review and editing, A.C., J.P., P.C. and J.C.; visualisation, J.P.; supervision, A.C. and J.C.; project administration, J.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This project received ethical approval by the Human Research Ethics Committee at the University of Notre Dame Australia (UNDA), Fremantle, on 25/06/2019 (HREC number: 019014F). A further ethics amendment was submitted to include various methodologies and approved on 01/02/2023.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data for this study is unavailable due to ethical considerations.
Acknowledgments
The authors thank the participants for their contribution to this research and would like to acknowledge the University of Notre Dame Australia for supporting this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Australian Institute of Health and Welfare (AIHW). Australian Burden of Disease Study 2022. BOD 37; Australian Government; Canberra, AUS, 2022; 12.
- Australian Institute of Health and Welfare (AIHW). Overweight and Obesity. Available online: https://www.aihw.gov.au/reports/overweight-obesity/overweight-and-obesity/contents/overweight-and-obesity (accessed on 19 March 2023).
- Australian Institute of Health and Welfare (AIHW). Physical Activity. Available online: https://www.aihw.gov.au/reports/physical-activity/physical-activity (accessed on 19 March 2023).
- Dabkowski, E.; Porter, J.E.; Barbagallo, M.; Prokopiv, V.; Snell, C.; Missen, K. A Systematic Literature Review of Workplace Physical Activity Programs: An Exploration of Barriers and Enabling Factors. Cogent Psychol 2023, 10, 2186327: 1- 2186327: 21. [CrossRef]
- Toyoshima, K.; Ichiki, M.; Inoue, T.; Shimura, A.; Masuya, J.; Fujimura, Y.; Higashi, S.; Kusumi, I. Subjective Cognitive Impairment and Presenteeism Mediate the Associations of Rumination with Subjective Well-Being and Ill-Being in Japanese Adult Workers From the Community. Biopsychosoc Med 2021, 15, 15: 1-15: 10. [CrossRef]
- Nye, C.D.; Ma, J.; Wee, S. Cognitive Ability and Job Performance: Meta-Analytic Evidence for the Validity of Narrow Cognitive Abilities. J Bus Psychol 2022, 37, 1119-1139. [CrossRef]
- Toh, W.X.; Yang, H.; Hartanto, A. Executive function and Subjective Well-Being in Middle and Late Adulthood. J Gerontol B Psychol Sci Soc Sci 2020, 75, 69-77. [CrossRef]
- Marin-Farrona, M.; Wipfli, B.; Thosar, S.S.; Colino, E.; Garcia-Unanue, J.; Gallardo, L.; Felipe, J.L.; López-Fernández, J. Effectiveness of worksite wellness programs based on physical activity to improve workers’ health and productivity: a systematic review. Systematic Reviews 2023, 12, 87: 1-87: 13. [CrossRef]
- Grimani, A.; Aboagye, E.; Kwak, L. The Effectiveness of Workplace Nutrition and Physical Activity Interventions in Improving Productivity, Work Performance and Workability: A Systematic Review. BMC Public Health 2019, 19, 1676: 1-1676: 12. [CrossRef]
- Hervieux, V.; Biron, C.; Dima, J. Investigating Associations Between Physical Activity and Presenteeism – A Scoping Review. Am J Health Promot 2023, 0, e04074015: e1-e04074015: 15. [CrossRef]
- Gil-Beltrán, E.; Llorens, S.; Salanova, M. Employees’ Physical Exercise, Resources, Engagement, and Performance: A Cross-Sectional Study from HERO Model. J work org sych 2020, 36, 39-47. [CrossRef]
- Naczenski, L.M.; De Vries, J.D.; Van Hooff, M.L.M.; Kompier, M.A.J. Systematic Review of the Association Between Physical Activity and Burnout. J Occup Health 2017, 59, 477-494. [CrossRef]
- Pedersen, M.T.; Blangsted, A.K.; Andersen, L.L.; Jørgensen, M.B.; Hansen, E.A.; Sjøgaard, G. The Effect of Worksite Physical Activity Intervention on Physical Capacity, Health, and Productivity: A 1-Year Randomized Controlled Trial. J Occup Environ Med 2009, 51, 759-770. [CrossRef]
- Martland, R.; Gaughran, F.; Stubbs, B.; Onwumere, J. Perspectives on Implementing Exercise Bikes for Use by Inpatient Mental Health Staff in the Workplace: A Qualitative Study Investigating Staff Attitudes. J Psychiatr Ment Health Nurs 2023, 30, 1027-1039. [CrossRef]
- Hunter, J.R.; Gordon, B.A.; Lythgo, N.; Bird, S.R.; Benson, A.C. Exercise at an Onsite Facility With or Without Direct Exercise Supervision Improves Health-Related Physical Fitness and Exercise Participation: An 8-Week Randomised Controlled Trial With 15-Month Follow-Up. Health Promot J Austr 2018, 29, 84-92. [CrossRef]
- Hergenroeder, A.; Quinn, T.D.; Perdomo, S.J.; Kline, C.E.; Gibbs, B.B. Effect of a 6-Month Sedentary Behavior Reduction Intervention on Well-Being and Workplace Health in Desk Workers With Low Back Pain. Work 2022, 71, 1145-1155. [CrossRef]
- Chau, J.Y.; Sukala, W.; Fedel, K.; Do, A.; Engelen, L.; Kingham, M.; Sainsbury, A.; Bauman, A.E. More Standing and Just As Productive: Effects of a Sit-Stand Desk Intervention on Call Center Workers’ Sitting, Standing, and Productivity at Work in the Opt to Stand Pilot Study. Prev Med Rep 2016, 3, 68-74. [CrossRef]
- Niven, A.; Ryde, G.C.; Wilkinson, G.; Greenwood, C.; Gorely, T. The Effectiveness of an Annual Nationally Delivered Workplace Step Count Challenge on Changing Step Counts: Findings from Four Years of Delivery. Int J Environ Res Public Health 2021, 18, 5140: 1-5140: 11. [CrossRef]
- Ryde, G.C.; Tomaz, S.A.; Sandison, K.; Greenwood, C.; Kelly, P. Measuring Productivity, Perceived Stress and Work Engagement of a Nationally Delivered Workplace Step Count Challenge. Int J Environ Res Public Health 2022, 19, 1843: 1-1843: 14. [CrossRef]
- Lock, M.; Post, D.; Dollman, J.; Parfitt, G. Efficacy of Theory-Informed Workplace Physical Activity Interventions: A Systematic Literature Review With Meta-Analyses. Health Psychol Rev 2021, 15, 483-507. [CrossRef]
- Murphy, B.; Parekh, N.; Vieira, D.L.; O’Connor, J.A. A Systematic Review of Randomized Controlled Trials Examining Workplace Wellness Interventions. Nutrition and Health 2022, 28, 111-122. [CrossRef]
- Sköld, M.B.; Bayattork, M.; Andersen, L.L.; Schlünssen, V. Psychosocial Effects of Workplace Exercise – A Systematic Review. Scand J Work Environ Health 2019, 45, 533-545. [CrossRef]
- Guiney, H.; Lucas, S.J.; Cotter, J.D.; Machado, L. Evidence Cerebral Blood-Flow Regulation Mediates Exercise-Cognition Links in Healthy Young Adults. Neuropsychology 2015, 29, 1-9. [CrossRef]
- Haverkamp, B.F.; Wiersma, R.; Vertessen, K.; van Ewijk, H.; Oosterlaan, J.; Hartman, E. Effects of Physical Activity Interventions on Cognitive Outcomes and Academic Performance in Adolescents and Young Adults: A Meta-Analysis J Sports Sci 2020, 38, 2637-2660. [CrossRef]
- Gallardo-Gómez, D.; del Pozo-Cruz, J.; Noetel, M.; Álvarez-Barbosa, F.; Alfonso-Rosa, R.M.; del Pozo Cruz, B. Optimal Dose and Type of Exercise to Improve Cognitive Function in Older Adults: A Systematic Review and Bayesian Model-Based Network Meta-Analysis of RCTs. Ageing Res Rev 2022, 76, 101591: 1-101591: 11. [CrossRef]
- Xiong, J.; Ye, M.; Wang, L.; Zheng, G. Effects of Physical Exercise on Executive Function in Cognitively Healthy Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials: Physical Exercise for Executive Function Int J Nurs Stud 2021, 114, 103810: 1-103810. [CrossRef]
- Basso, J.C.; Suzuki, W.A. The Effects of Acute Exercise on Mood, Cognition, Neurophysiology, and Neurochemical Pathways: A Review. Brain Plast 2017, 2, 127-152. [CrossRef]
- Wilke, J.; Giesche, F.; Klier, K.; Vogt, L.; Herrmann, E.; Banzer, W. Acute Effects of Resistance Exercise on Cognitive Function in Healthy Adults: A Systematic Review with Multilevel Meta-Analysis. Sports Med 2019, 49, 905-916. [CrossRef]
- Stoner, L.; Willey, Q.; Evans, W.S.; Burnet, K.; Credeur, D.P.; Fryer, S.; Hanson, E.D. Effects of Acute Prolonged Sitting on Cerebral Perfusion and Executive Function in Young Adults: A Randomized Cross-Over Trial. Psychophysiology 2019, 56, e13457: e1- e13457: 29. [CrossRef]
- Heijnen, S.; Hommel, B.; Kibele, A.; Colzato, L.S. Neuromodulation of Aerobic Exercise-A Review. Front Psychol 2016, 6, 1890: 1-1890: 6. [CrossRef]
- Herold, F.; Törpel, A.; Schega, L.; Müller, N.G. Functional and/or Structural Brain Changes in Response to Resistance Exercises and Resistance Training Lead to Cognitive Improvements – A Systematic Review. Eur Rev Aging Phys Act 2019, 16, 10: 1-10: 33. [CrossRef]
- Landrigan, J.-F.; Bell, T.; Crowe, M.; Clay, O.J.; Mirman, D. Lifting Cognition: A Meta-Analysis of Effects of Resistance Exercise on Cognition. Psychol Res 2020, 84, 1167-1183. [CrossRef]
- Chow, Z.-S.; Moreland, A.T.; Macpherson, H.; Teo, W.-P. The Central Mechanisms of Resistance Training and Its Effects on Cognitive Function. Sports Med 2021, 51, 2483-2506. [CrossRef]
- Wechsler, D. Wechsler Adult Intelligence Scale. Administration and Scoring Manual, 3rd ed.; The Psychological Corporation, Harcourt Brace: San Antonio, TX, USA, 1997; ISBN: 0158981030.
- Wechsler, D. Wechsler Memory Scale. Administrationand Scoring Manual, 3rd ed.; The Psychological Corporation, Harcourt Brace: San Antonio, TX, USA, 1997.
- Norton, K. New Australian Standard for Adult Pre-Exercise Screening. Sport health 2012, 30, 12-16. https://search.informit.org/doi/10.3316/informit.808362433833839.
- Exercise and Sports Science Australia (ESSA). Accredited Exercise Scientist Professional Standards for Accreditation; Queensland, AUS, 2020.
- Qualtrics, 18.9; Qualtrics: Utah, USA, 2005.
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med Sci Sports Exerc 2003, 35, 1381-1395. [CrossRef]
- Shikiar, R.; Halpern, M.T.; Rentz, A.M.; Khan, Z.M. Development of the Health and Work Questionnaire (HWQ): An Instrument for Assessing Workplace Productivity in Relation to Worker Health. Work 2004, 22, 219-229. https://pubmed.ncbi.nlm.nih.gov/15156087/.
- Scarpina, F.; Tagini, S. The Stroop Color and Word Test. Front Psychol 2017, 8, 557: 1-557: 8, doi:10.3389/fpsyg.2017.00557.Golden, C.J. Stroop Color and Word Test: A Manual for Clinical and Experimental Uses; Stoelting Co.: Chicago, IL, USA, 1978. [CrossRef]
- Golden, C.J. Stroop Color and Word Test: A Manual for Clinical and Experimental Uses; Stoelting Co.: Chicago, IL, USA, 1978.43.
- Strauss, E.; Sherman, E.M.S.; Spreen, O. A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary, 3rd ed.; Oxford University Press: New York, NY, USA, 2006. ISBN: 0195159578.
- Klein, M.; Ponds, R.W.H.M.; Houx, P.J.; Jolles, J. Effect of Test Duration on Age-Related Differences in Stroop Interference. J Clin Exp Neuropsychol 1997, 19, 77-82. [CrossRef]
- The Psychology Experiment Building Language (PEBL), 2.1; Mueller, S.T: Michigan, USA, 2013.
- Mueller, S.T.; Piper, B.J. The Psychology Experiment Building Language (PEBL) and PEBL Test Battery. Journal of Neuroscience Methods 2014, 222, 250-259. [CrossRef]
- Microsoft Windows 10, 22H2; Microsoft: Washington, USA, 2015.
- Lim, L.W.; Aquili, L. GABA Supplementation Negatively Affects Cognitive Flexibility Independent of Tyrosine. J Clin Med 2021, 10, 2028: 1-2028: 10. [CrossRef]
- Pilli, R.; Mur, N.; Pingali, U.R.; Shobha, J.C.; Reddy, A.P. A Computerized Stroop Test for the Evaluation of Psychotropic Drugs in Healthy Participants. Indian J Psychol Med 2013, 35, 180-189. [CrossRef]
- Ferris, L.T.; Williams, J.S.; Shen, C.-L. The Effect of Acute Exercise on Serum Brain-Derived Neurotrophic Factor Levels and Cognitive Function. Med Sci Sports Exerc 2007, 39, 728-734. [CrossRef]
- Coetsee, C.; Terblanche, E. The Effect of Three Different Exercise Training Modalities on Cognitive and Physical Function in a Healthy Older Population. Eur Rev Aging Phys Act 2017, 14, 13: 1-13: 10. [CrossRef]
- da Silva, D.N.F.B.; Faro, H.K.C.; Tavares, M.P.M.; do Nascimento Neto, L.I.; Agrícola, P.M.D.; da Silva Machado, D.G. Influence of Workplace Exercise on Workers’ Cognitive Performance. Rev Bras Med Trab 2021, 19, 157-164. [CrossRef]
- Lee, E.-H. Review of the Psychometric Evidence of the Perceived Stress Scale. Asian Nurs Res 2012, 6, 121-127. [CrossRef]
- Microsoft Excel, 16.77.1; Microsoft Office: Washington, USA, 1985.
- IBM SPSS, 28.0.1.0; IBM Corp: New York, USA 1968.
- Hedges, L.V.; Olkin, I. Statistical Methods for Meta-Analysis, 1st ed.; Academic Press: New York, NY, USA, 1985. ISBN: 0080570658.
- Morris, S.B. Estimating Effect Sizes From Pretest-Posttest-Control Group Designs. Organ Res Methods 2008, 11, 364-386. [CrossRef]
- Weinberg, L.; Hasni, A.; Shinohara, M.; Duarte, A. A Single Bout of Resistance Exercise Can Enhance Episodic Memory Performance. Acta Psychologica 2014, 153, 13-19. [CrossRef]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-Response Associations Between Accelerometry Measured Physical Activity and Sedentary Time and All Cause Mortality: Systematic Review and Harmonised Meta-Analysis. BMJ 2019, 366, 4570: 1-4570: 10. [CrossRef]
- Gill, D.L.; Hammond, C.C.; Reifsteck, E.J.; Jehu, C.M.; Williams, R.A.; Adams, M.M.; Lange, E.H.; Becofsky, K.; Rodriguez, E.; Shang, Y.T. Physical Activity and Quality of Life. J Prev Med Public Health 2013, 46, 28-34. [CrossRef]
- Justesen, J.B.; Søgaard, K.; Dalager, T.; Christensen, J.R.; Sjøgaard, G. The Effect of Intelligent Physical Exercise Training on Sickness Presenteeism and Absenteeism Among Office Workers. J Occup Environ Med 2017, 59, 942-948. [CrossRef]
- Eather, N.; Babic, M.; Riley, N.; Harris, N.; Jung, M.; Jeffs, M.; Barclay, B.; Lubans, D.R. Integrating High-Intensity Interval Training Into the Workplace: The Work-HIIT Pilot RCT. Scand J Med Sci Sports 2020, 30, 2445-2455. [CrossRef]
- Michishita, R.; Jiang, Y.; Ariyoshi, D.; Yoshida, M.; Moriyama, H.; Obata, Y.; Nagata, M.; Nagata, T.; Mori, K.; Yamato, H. The Introduction of an Active Rest Program by Workplace Units Improved the Workplace Vigor and Presenteeism Among Workers: A Randomized Controlled Trial. J Occup Environ Med 2017, 59, 1140-1147. [CrossRef]
- Dalager, T.; Justesen, J.B.; Murray, M.; Boyle, E.; Sjøgaard, G. Implementing Intelligent Physical Exercise Training at the Workplace: Health Effects Among Office Workers—A Randomized Controlled Trial. Eur J Appl Physiol 2016, 116, 1433-1442. [CrossRef]
- Brox, J.I.; Frøystein, O. Health-Related Quality of Life and Sickness Absence in Community Nursing Home Employees: Randomized Controlled Trial of Physical Exercise. Occup Med 2005, 55, 558-563. [CrossRef]
- Madinabeitia-Cabrera, I.; Alarcón-López, F.; Chirosa-Ríos, L.J.; Pelayo-Tejo, I.; Cárdenas-Vélez, D. The Cognitive Benefits of Basketball Training Compared to a Combined Endurance and Resistance Training Regimen: A Four-Month Intervention Study. Sci Rep 2023, 13, 11132: 1-11132: 11. [CrossRef]
- Fortes, L.d.S.; Costa, M.d.C.; Perrier-Melo, R.J.; Brito-Gomes, J.L.; Nascimento-Júnior, J.R.A.; de Lima-Júnior, D.R.A.A.; Cyrino, E.S. Effect of Volume in Resistance Training on Inhibitory Control in Young Adults: A Randomized and Crossover Investigation. Front Psychol 2018, 9, 2028: 1-2028: 10. [CrossRef]
- Peig-Chiello, P.; Perrig, W.J.; Ehrsam, R.; Staehelin, H.B.; Krings, F. The Effects of Resistance Training on Well-Being and Memory in Elderly Volunteers. Age Ageing 1998, 27, 469-475. [CrossRef]
- Malik, S.H.; Blake, H.; Suggs, L.S. A Systematic Review of Workplace Health Promotion Interventions for Increasing Physical Activity. Br J Health Psychol 2014, 19, 149-180. [CrossRef]
- Alomari, M.A.; Keewan, E.F.; Qhatan, R.; Amer, A.; Khabour, O.F.; Maayah, M.F.; Hurtig-Wennlöf, A. Blood Pressure and Circulatory Relationships with Physical Activity Level in Young Normotensive Individuals: IPAQ Validity and Reliability Considerations. Clin Exp Hypertens 2011, 33, 345-353. [CrossRef]
- Encarnação, S.G.A.d.; Moreira, O.C.; de Castro Pinto, B.W.F.; de Miranda, C.N.; Araújo, D.P.d.S.; Pereira, F.S.T.; Fazolo, S.L.; Carneiro-Júnior, M.A. Physical Activity Levels and Mental Illness Risk in Elderly Women During COVID-19. Motricidade 2022, 18, 225-229. [CrossRef]
- Cooper, K.; Barton, G.C. An Exploration of Physical Activity and Wellbeing in University Employees. Perspect Public Health 2015, 136, 152-160. [CrossRef]
- Thonon, F.; Godon-Rensonnet, A.-S.; Perozziello, A.; Garsi, J.-P.; Dab, W.; Emsalem, P. Return on Investment of Workplace-Based Prevention Interventions: A Systematic Review. Eur J Public Health 2023, 33, 612-618. [CrossRef]
- SantaBarbara, N.J.; Rezai, R.; Soetenga, S.; Terry, E.; Carpenter, C.L.; Comulada, W.S. Exercise Preferences for a Workplace Wellness Program to Reduce Cardiovascular Risk and Increase Work Productivity. J Occup Environ Med 2022, 64, 545-549. [CrossRef]
Figure 1.
Structure and Timeline of the Staff Fitness Program. Each arrow represents a single week of the program. IPAQ-SF (international physical activity Questionnaire), VSCWT (Victoria Stroop Colour and Word Test) and the HWQ (Health and Work Questionnaire) where the testing metrics used at respective time-points.
Figure 1.
Structure and Timeline of the Staff Fitness Program. Each arrow represents a single week of the program. IPAQ-SF (international physical activity Questionnaire), VSCWT (Victoria Stroop Colour and Word Test) and the HWQ (Health and Work Questionnaire) where the testing metrics used at respective time-points.
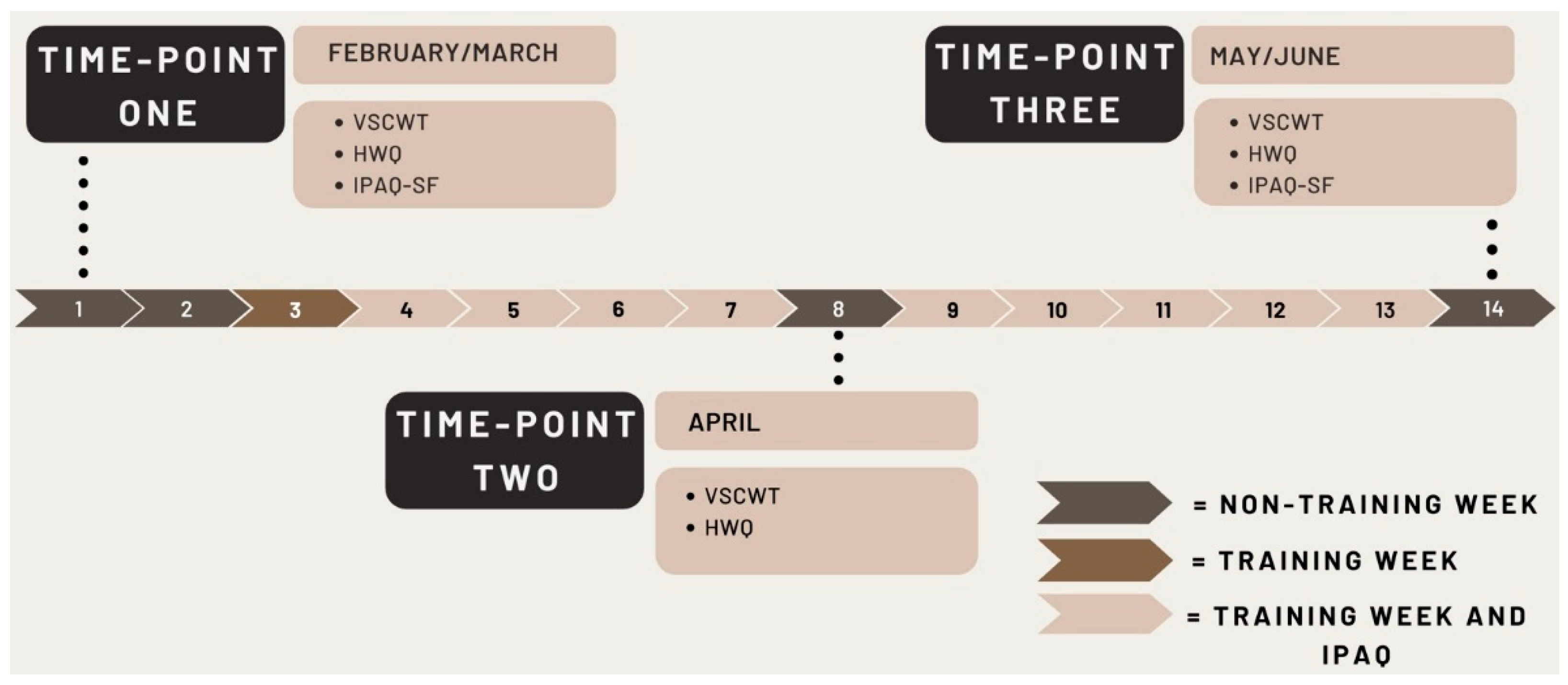
Figure 2.
Stages of the Victoria Stroop Colour and Word Test, administered through PEBL. (a) part one (Dot); (b) part two (Word); (c) part three (Colour). Augmented figure design from da Silva et al. [52].
Figure 2.
Stages of the Victoria Stroop Colour and Word Test, administered through PEBL. (a) part one (Dot); (b) part two (Word); (c) part three (Colour). Augmented figure design from da Silva et al. [52].
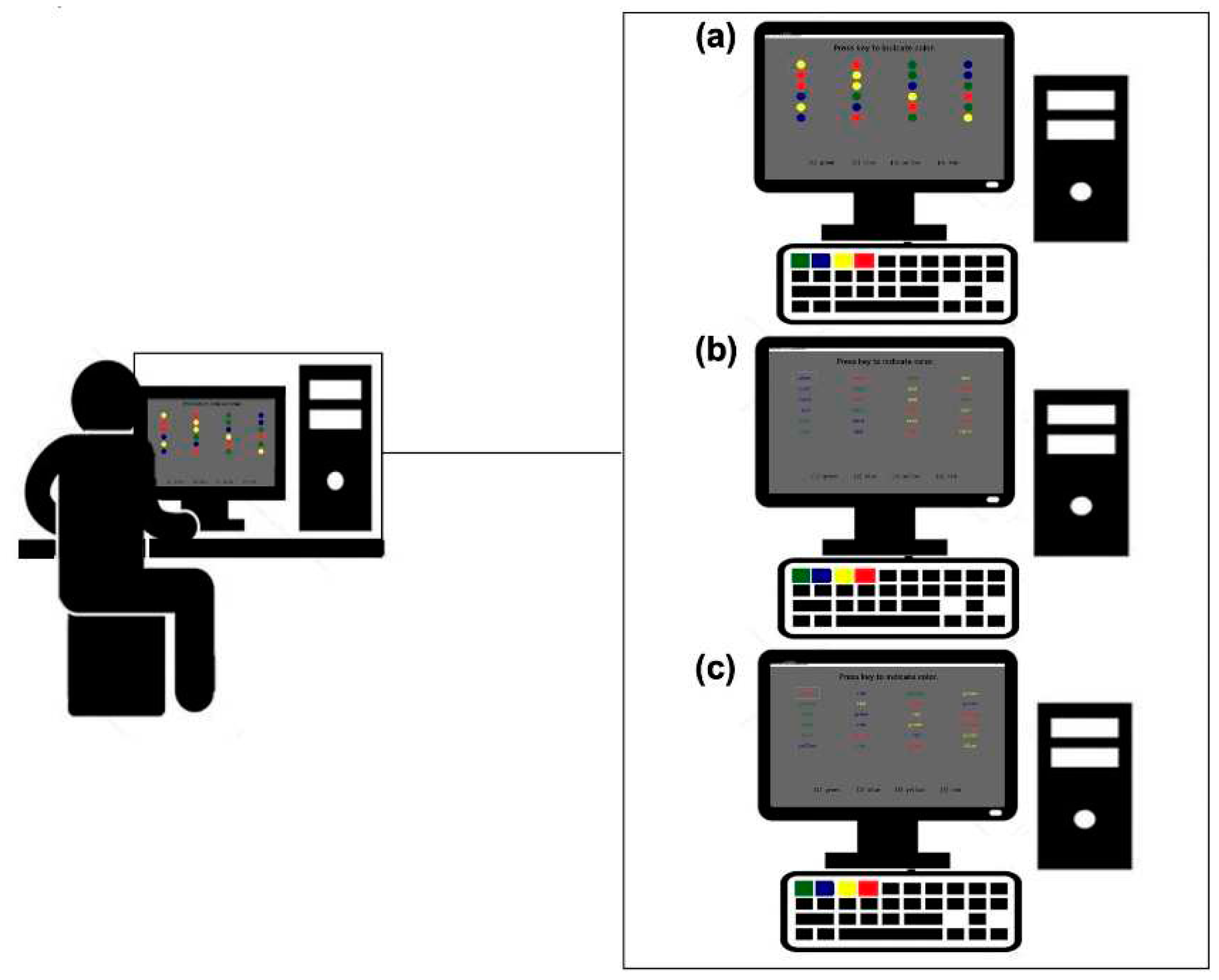
Figure 3.
Mean MET-min-week Across Weeks of the Intervention. * Significant difference between values (p < .05), Error bars: 95% CI.
Figure 3.
Mean MET-min-week Across Weeks of the Intervention. * Significant difference between values (p < .05), Error bars: 95% CI.
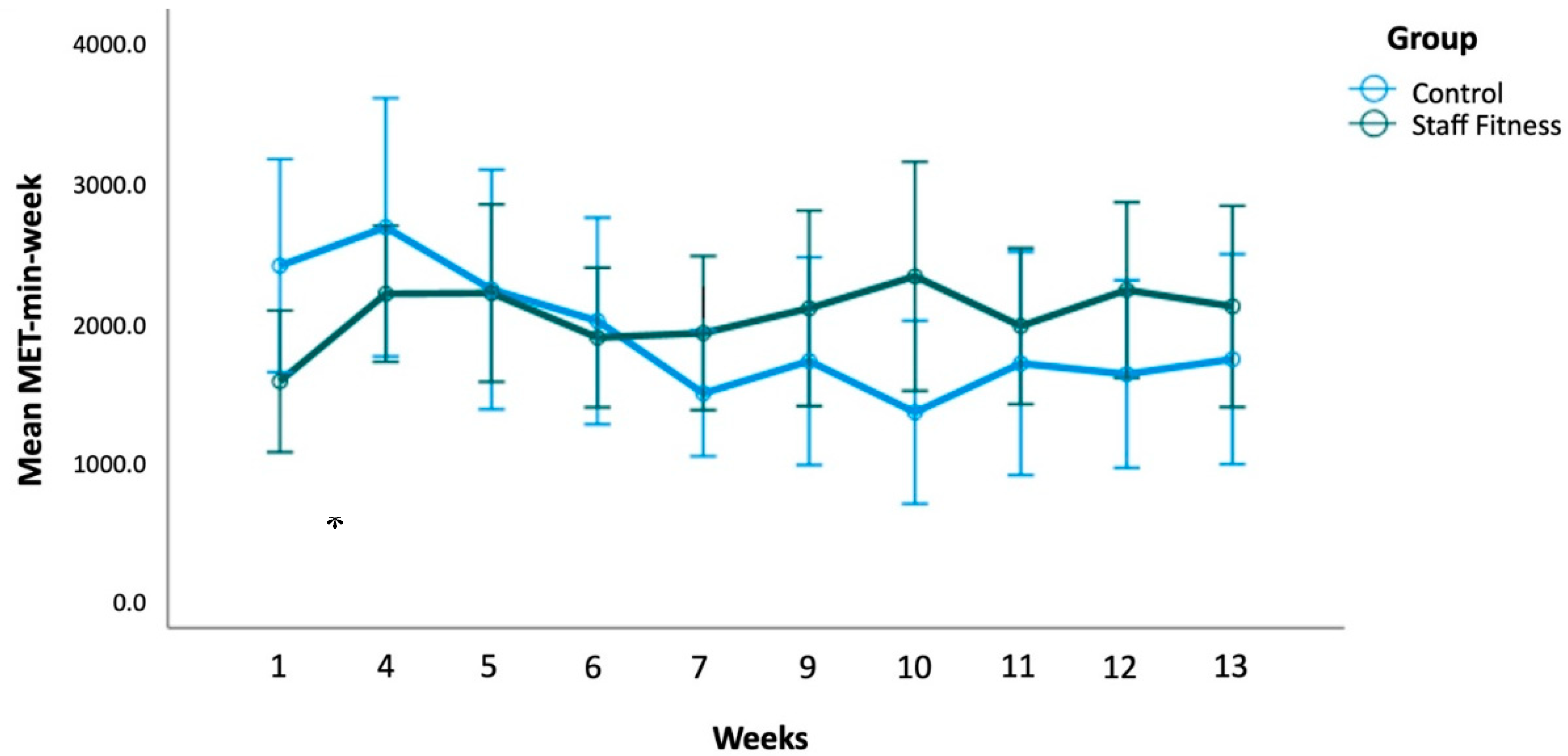

Table 1.
Demographic Details for Control and Test Participants.
| Variable | All participants (n = 44) | Staff Fitness (n = 26) | Control (n = 18) |
|---|---|---|---|
| Age | 42.30 ± 11.68 | 43.12 ± 11.83 | 41.11 ± 11.69 |
| Women: Men | 24: 20 | 17: 9 | 7: 11 |
| Occupation | |||
| Casual/sessional academic staff | 2 | 2 | 0 |
| Full-time academic staff | 9 | 2 | 7 |
| Full-time professional staff | 17 | 14 | 3 |
| Part-time academic staff | 11 | 5 | 6 |
| Part-time professional staff | 5 | 4 | 2 |
Note. Age presented as mean +/- standard deviations.
Table 2.
Physical Activity Levels Measured in Metabolic Equivalent of Tasks per Week (MET-min-week) across weeks of the Staff Fitness Program.
Table 2.
Physical Activity Levels Measured in Metabolic Equivalent of Tasks per Week (MET-min-week) across weeks of the Staff Fitness Program.
| Staff Fitness group (26) | Control Group (18) | ||||||
|---|---|---|---|---|---|---|---|
| MET-min-week | N | Mean | SD | N | Mean | SD | Effect Size dCohen resp. gHedges |
| Week 1 | 20 | 1540.93* | 1083.74 | 15 | 2368.80* | 1377.70 | -0.68 |
| Week 4 | 25 | 2167.58 | 1180.41 | 14 | 2643.96 | 1601.89 | -0.36 |
| Week 5 | 22 | 2173.02 | 1433.30 | 13 | 2198.46 | 1418.88 | -0.02 |
| Week 6 | 20 | 1854.40 | 1069.78 | 15 | 1973.90 | 1335.54 | -0.10 |
| Week 7 | 20 | 1886.63 | 1177.34 | 15 | 1455.12 | 814.72 | 0.42 |
| Week 9 | 19 | 2063.50 | 1452.80 | 11 | 1686.00 | 1107.13 | 0.28 |
| Week 10 | 17 | 2292.82 | 1594.43 | 13 | 1319.27 | 1084.48 | 0.70 |
| Week 11 | 15 | 1936.60 | 1010.11 | 14 | 1668.89 | 1384.36 | 0.22 |
| Week 12 | 23 | 2194.83 | 1454.72 | 12 | 1592.50 | 1057.62 | 0.45 |
| Week 13 | 17 | 2077.32 | 1401.48 | 15 | 1699.50 | 1359.31 | 0.27 |
Note. *Significant difference (p < .05).
Table 3.
Subscale and Total Outcomes for the Health and Work Questionnaire (HWQ) at the Start, Middle and End of the Intervention.
Table 3.
Subscale and Total Outcomes for the Health and Work Questionnaire (HWQ) at the Start, Middle and End of the Intervention.
| Staff Fitness Group (26) | Control Group (18) | Effect size dppc2 sensu Morris (2008) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Subscale | Start (25) | Mid-point (21) | End (20) | Start (15) | Mid-point (15) | End (11) | Start-end | Start-middle | Middle-end |
| Productivity | 7.33 ± 0.97 | 7.09 ± 1.09 | 7.10 ± 0.92 | 7.28 ± 1.10 | 6.85 ± 1.21 | 6.97 ± 0.84 | 0.08 | 0.18 | -0.09 |
| Supervisor perceived | 7.68 ± 1.44 | 7.32 ± 1.45 | 7.38 ± 1.41 | 7.84 ± 1.05 | 7.21 ± 1.54 | 7.58 ± 1.22 | -0.03 | 0.20 | -0.20 |
| Self-rated | 7.12 ± 0.85 | 6.95 ± 0.94 | 6.93 ± 0.71 | 6.93 ± 1.29 | 6.76 ± 1.08 | 6.62 ± 0.76 | 0.11 | 0.00 | 0.12 |
| Concentration/Focus | 6.68 ± 1.88 | 6.82 ± 1.75 | 6.92 ± 1.71 | 7.31 ± 2.37 | 6.28 ± 2.23a | 6.61 ± 1.76 | 0.44 | 0.55 | -0.12 |
| Impatience/Irritability | 7.63 ± 1.94 | 8.03 ± 1.51 | 7.98 ± 1.66 | 7.93 ± 1.64 | 7.91 ± 1.77 | 8.58 ± 1.29 | -0.16 | 0.22 | -0.43 |
| Work satisfaction | 6.89 ± 1.67 | 6.73 ± 1.89 | 6.88 ± 1.53 | 6.88 ± 1.34 | 6.22 ± 1.73 | 6.57 ± 1.53 | 0.19 | 0.32 | -0.11 |
| Non-work satisfaction | 7.32 ± 1.53 | 7.71 ± 1.35 | 7.43 ± 1.43 | 7.36 ± 2.09 | 7.44 ± 1.90 | 8.00 ± 1.24 | -0.30 | 0.17 | -0.51 |
| Supervisor relationships | 7.46 ± 2.52 | 6.98 ± 2.91 | 7.67 ± 1.92 | 8.30 ± 1.72 | 7.63 ± 2.33 | 7.45 ± 2.14 | 0.46 | 0.08 | 0.32 |
| Total HWQ score | 7.18 ± 1.17 | 7.18 ± 0.97 | 7.14 ± 0.88 | 7.32 ± 1.21 | 6.89 ± 1.18 | 7.18 ± 0.89 | 0.08 | 0.36 | -0.30 |
Note. Data presented as mean + standard deviations. (n); * Significant difference (p < .05); a Significant difference from start to mid-point (p < .05); b Significant difference from start to end (p < .05).
Table 4.
Victoria Stroop Colour and Word Test Scores at the Start, Middle and End of the Intervention.
Table 4.
Victoria Stroop Colour and Word Test Scores at the Start, Middle and End of the Intervention.
| Variable | Staff Fitness group (26) | Control Group (18) | Effect size dppc2 sensu Morris (2008) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Start (25) | Mid-point (25) | End (24) | Start (17) | Mid-point (16) | End (16) | Start-end | Start-middle | Middle-end | |
| Dot (seconds) | 19.93 ± 5.43 | 19.26 ± 3.96 | 18.77 ± 4.63 b | 19.51 ± 4.53 | 22.28 ± 10.04 | 19.78 ± 4.15 | -0.28 | -0.66 | 0.28 |
| Accuracy (%) | 98.50 ± 1.64 | 98.50 ± 3.15 | 97.92 ± 4.08 | 99.26 ± 1.64 | 97.40 ± 3.36 a | 97.92 ± 3.40 | 0.46 | 1.11 | -0.33 |
| Word (seconds) | 20.26 ± 4.47 | 19.64 ± 4.29 | 19.20 ± 4.18 b | 21.42 ± 5.25 | 20.69 ± 3.35 | 20.16 ± 4.14 | 0.04 | 0.02 | 0.02 |
| Accuracy (%) | 99.00 ± 2.53 | 98.67 ± 2.88 | 98.96 ± 2.22 | 98.53 ± 2.53 | 97.92 ± 3.40 | 97.66 ± 4.56 | 0.32 | 0.11 | 0.16 |
| Colour (seconds) | 24.76 ± 11.96 | 23.02 ± 8.41 | 23.43 ± 8.96 | 23.58 ± 6.33 | 23.07 ± 5.36 | 22.63 ± 5.17 | -0.04 | -0.12 | 0.11 |
| Accuracy (%) | 97.33 ± 5.63 | 98.00 ± 5.12 | 96.70 ± 5.35 | 98.77 ± 2.45 | 98.44 ± 2.58 | 98.18 ± 3.72 | -0.01 | 0.21 | -0.24 |
| Colour/Dot | 1.23 ± 0.27 | 1.18 ± 0.24 | 1.24 ± 0.22 | 1.21 ± 0.13 | 1.10 ± 0.22 | 1.16 ± 0.16 | 0.26 | 0.26 | 0.00 |
| Word/Dot | 1.03 ± 0.11* | 1.02 ± 0.12 | 1.04 ± 0.11 | 1.10 ± 0.11* | 0.99 ± 0.18 a | 1.03 ± 0.14 | 0.71 | 0.89 | -0.13 |
Note. Scores presented as mean + standard deviations. Sample sizes are displayed as: (n). ‘Dot’, ‘Word’ and ‘Colour’ are part 1, 2 and 3 of the VSCWT respectively. * Significant between group difference (p < 0.05); a Significant difference from start to mid-point (p < 0.05); b Significant difference from start to end (p < 0.05).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



