
Submitted:
05 January 2024
Posted:
08 January 2024
You are already at the latest version
Abstract
Mandibular third molar is the most frequently impacted tooth. Mandibular third molar impaction bears consequences on the adjacent mandibular second molar (MSM) like bone loss. It can be identified initially using orthopantomography (OPG). The objective is to compare the changes in the bone level distal to MSM between patients with extracted and non-extracted impacted man-dibular third molars (IMTM) using OPG. In this retrospective case-control study, 160 archived (OPGs) of 80 patients visiting the Dental Hospital of the University of Barcelona (HOUB) were randomly selected. The participants were stratified into two groups. The study group involved measuring the bone level distal to the mandibular second molar before and after the extraction of the IMTM. The control group, on the other hand, had bone levels measured twice within 3–6-month period without the extraction of the IMTM. The mean ages of patients in study and control groups were 35.5 ± 15.45 and 33 ± 16.49, respectively. Study group demonstrated signifi-cant (p < 0.05) bone gain after extraction, whereas control group demonstrated significant bone loss (p < 0.0001) after follow-up. Bone improvements were observed distal to the mandibular second molar after the extraction of the IMTM compared to those in control group.
Keywords:
impacted mandibular third molar
; bone loss
; mandibular second molar
; panoramic radiography
1. Introduction
The term “erumpere,” which means “to erupt,” refers to the movement of a developing tooth from its non-functional position to its corresponding functional and anatomical position in the dental arch [1]. However, for several reasons, some teeth fail to undergo this physiological process, leading to partial or complete tooth impaction [1]. An unerupted tooth is defined as one that remains embedded within the jawbone, is covered by gingival tissue, and may be partially or entirely covered by bone. Nevertheless, the tooth is expected to erupt and come into occlusion based on the clinical and radiographic findings [2]. A partially erupted tooth is defined as one that does not fully erupt into its normal position but can still be seen in the oral cavity. The term tooth impaction signifies that the tooth is obstructed from fully erupting into the oral cavity due to the blockage of the eruption path or a lack of space [3]. Third molars, followed by maxillary canines, are the most frequently impacted teeth routinely encountered in dental practice [3]. The frequency of a mandibular third molar impaction is influenced by factors such as facial skeleton, gender, age, and ethnic group [4]. Breik and Grupor [4] reported a higher incidence of mandibular third molar impaction in individuals with a dolichofacial pattern (vertical growth; facial axis angle, <87) and in females (43%) compared to males (45%). On the contrary, Padhye et al. [5] observed a higher prevalence of third molar impaction in males (51.77%) than in females (48.33%). In the study KalaiSelvan et al. [6], they reported a prevalence of 45.8% in the Tamil population while Prajapati et al. [7] reported a higher prevalence of impacted mandibular third molars (IMTM) among females aged 21–30. The worldwide prevalence of impacted third molars is 24% [11].
Several reasons, both systemic and local, contribute to tooth impaction. Systemic conditions, such as nutritional deficiencies, vitamin D insufficiency, anemia, rickets, Down’s syndrome, genetic factors, endocrine disturbances, various syndromes, and infectious diseases, play a significant role in tooth impaction [8]. Local factors that can hinder eruption and lead to impaction include premature loss of deciduous teeth, traumatic conditions, ankylosed teeth, inflammatory and pathological conditions, and insufficient space in the dental arch [1,8].
Different imaging modalities, including conventional radiography and advanced three-dimensional imaging, are used in dental practice. The initial screening of the oral cavity-related abnormalities is done using periapical and panoramic radiography. Intraoral periapical radiography is used whenever it is possible to position the radiographic sensor inside the oral cavity. This technique provides a sharp and detailed image of the impacted tooth and its relation to the inferior alveolar canal [9]. The tube shift technique can be used to determine the relationship of the tooth to the inferior mandibular nerve [9]. However, due to difficulties in positioning the device, panoramic radiography is more convenient to use [10]. The orthopantomogram (OPG) provides the advantage of viewing the structures of the mandible, maxilla, and facial bone in a single broad image. It is beneficial for identifying different pathological conditions, assessing carious and fractured teeth, detecting dental anomalies, and determining the presence of impacted teeth and pathologies [2]. However, there are several drawbacks linked to the panoramic radiography technique, including overlapping, magnification, blurred images, metal artifacts, and errors related to patient positioning and image acquisition [10]. Therefore, the need for more accurate three-dimensional diagnosis has led to the introduction of cone-beam computed tomography (CBCT). CBCT is considered superior to conventional panoramic radiography because it portrays structures in a three-dimensional view [11]. However, the routine use of CBCT in dental practice is controversial and limited to the patient’s needs due to the higher radiation doses than conventional dental radiography [11]. The radiation doses resulting from a full field-of-view dental CBCT scan are reported to be 4–42 times higher than the dose from an OPG [12]. Thus, it is necessary to implement the ALADA (as low as diagnostically acceptable) concept, which has replaced the previous ALARA (as low as reasonably acceptable) concept, to control the use of CBCT [13].
Hence, this study aims to compare the changes in bone level between patients who underwent extraction of the IMTM and those who did not. The findings were also analyzed in relation to the gender and age of the patients. Additionally, the pattern of impaction in the study sample has been described.
2. Materials and Methods
2.1. Study Description
This retrospective case-control study utilized archived panoramic radiography images of patients who visited the Dental Hospital of the University of Barcelona (HOUB) from June 2018 to December 2022. A total of 1000 OPGs were randomly selected. Among them, 400 are deemed error-free and suitable for analysis. Based on the study characteristics, 160 OPGs were selected to perform the measurements, with 40 patients representing the study group and 40 patients representing the control group. Ethical approval for the study was obtained from the ethics committee of HOUB (protocol number: 2022-032-1).
2.2. Study Description
The patients were selected using the simple random sampling technique, and the sample size was calculated using Cohen’s concept, as described in the study conducted by Faria et al. [14]. The minimum determined sample size for each group was 24; however, 80 patients (40 in each group) were included in the study for validity. The patients were divided into two groups based on whether they underwent extraction (study group) or non-extraction (control group) of the IMTM. The patients in the study group involved individuals who came to extract their impacted lower third molar, with two X-rays taken. One before the extraction, and the other taken at least 3–6 months later for evaluation, considering the time necessary for bone healing and remodeling, is three months. It is considered the cut-off period for periodontal healing [15]. Measurement of bone loss is performed on both radiographs, and the mean difference is compared.
The control group consists of patients who visit the dental clinic for various dental issues and undergo an OPG that shows the presence of either partial or complete impaction of the lower third molar. However, in this group, the impacted tooth is not extracted. A control panoramic image is performed to assess the oral condition and the evolution of this non-extracted third molar at least 3–6 months later. Since our goal is to examine bone changes in patients with and without extractions, those who do not undergo extraction should have a follow-up panoramic radiograph 3–6 months after their visit. This will help evaluate their oral status, history, and the condition of the bone distal to the second molar.
2.3. Inclusion and Exclusion Criteria
The inclusion criteria for the study were as follows: patients older than 18 years; availability of images depicting the presence of an IMTM; availability of undistorted panoramic images without errors or overlapping; availability of radiographs taken before and after the extraction of the IMTM with a clearly documented history for the study group; the presence of a second molar adjacent to the impacted mandibular third molar. The exclusion criteria included images demonstrating an absent or extracted mandibular third molar, patients who had undergone chemotherapy, radiotherapy, or bisphosphonate treatment for head and neck tumors, individuals with incomplete records, and those with incomplete formation of the third molar roots.
2.4. Inclusion and Exclusion Criteria
The panoramic images were obtained using the Planmeca ProMax® X-ray unit (Planmeca Oy, 00880 Helsinki, Finland), which was equipped with a digital sensor called Planmeca Dimax 3. The measurement was performed using the Planmeca Romexis® software. Images were taken based on the manufacturer’s recommendations at 64–70 kV and 7–14 mA, depending on the patient’s gender and age. The recommended settings varied for adult females, small males, adult males, and large adult males. Well-trained doctoral students from the Oral Radiology Department conducted the investigation twice, with a two-month interval between each session. The intra-examiner reliability was calculated using the Kappa test [16]. On OPGs, the level of the bone was measured from the cementoenamel junction of the second molar to the level of the alveolar crest for the study group before (Figure 1A) and extraction and after extraction. (Figure 1B).
2.5. Statistical Analysis
The data were imported into an Excel sheet (Microsoft® Excel® for Microsoft 365 MSO, Version 2307) for the descriptive analysis. All statistical analysis was performed using IBM SPSS Statistics for Windows, version 26 (IBM Corp., Armonk, NY, USA). A chi-square test was performed to identify the differences between the variables. Quantitative variables are expressed as the mean and standard deviation. Since the sample with respect to age and gender is not normally distributed, a Wilcoxon test was performed to determine the statistical difference in the numerical value of bone level changes between the two groups. A one-way analysis of variance (ANOVA) was used to investigate differences regarding gender and age in both groups. A p-value of <0.05 was considered statistically significant.
3. Results
The mean ages of the patients in the study and control groups were 35.5 ± 15.45 and 33 ± 16.49, respectively. Females and males accounted for 62% and 37.5%, respectively, of the patients in the study group and 55% and 45%, respectively, of those in the control group. Furthermore, the patients were divided into four subgroups based on age: 18–28, 29–39, 40–50, and ≥51.
3.1. Comparison of Bone Levels among the Groups
The bone level measurements, regardless of the side, were calculated and reported as the mean and standard deviation in both the study and control groups. The values in the study group before and after extraction were 3.00 ± 1.68 and 2.63 ± 1.75, respectively, indicating a statistically significant difference in favor of bone gain in the study group (p < 0.0001). In the control group, the value at the baseline radiography was 2.73 ± 1.75, whereas that after the second radiography was 3.01 ± 1.98, revealing a statistically significant difference in favor of bone loss (p < 0.001) (Table 1). The Kappa values are interpreted as follows: low agreement (<0), very slight agreement (0–0.19), slight agreement (0.2–0.39), moderate agreement (04–0.59), substantial agreement (0.6–0.70), and almost perfect agreement (0.8–1) (27). (Table 1):
3.2. Comparison of Bone Levels among the Groups
Both males and females experienced bone gain in the study group and bone loss in the control group. However, the difference in bone level change was not statistically significant with respect gender in both groups (Table 2).
3.3. Bone Changes among the Two Groups Based on the Age Groups
In the study group, patients between the ages of 29 and 39 appeared to have witnessed the highest bone gain after extraction compared to those in the other age groups (Table 3). On the other hand, only those aged 40–50 experienced bone loss after extraction (-1.20 ± 0.14 mm). A significant difference in bone changes was observed among the age subgroups after extraction in the study group (p < 0.05; Table 3).
In the control group, all the age subgroups were presented with bone loss at the follow-up evaluation; however, the difference among the age subgroups was not statistically significant (p-value 0.07) (Table 3).
3.4. Pattern of Impaction
The number of IMTMs in this study, based on Winter’s classification, was 139 out of a total sample of 160. It accounts for 82.28%. Vertical impaction was the most prevalent (41.24%), followed by mesioangular impaction (28.75%) and horizontal impaction (16.62%). No statistically significant difference in the occurrence of the different types of impactions was observed in the current study (p-value 0.539) (Table 4).
3.5. Impaction Side
Most of the patients in both groups demonstrated bilateral impaction, which accounted for 73.8% of the total sample. In the study group, the unilateral impaction on the right side was more prevalent than the unilateral impaction of the left side (15%) and (12.5%) respectively. On the contrary, the unilateral impaction of the left side preceded the unilateral right impaction in the control group (17.5%) and (7.5%) respectively. Statistically, no significant difference regarding the side of impaction was observed between the two groups (p-value 0.509). (Table 5).
4. Discussion
In the present study, the bone level changes in the mandibular second molar (MSM) were compared between patients who underwent extraction of the IMTM and those who did not. The bone level was measured from the cementoenamel junction to the level of the bone crest, as described by Faria et al. [14].In dental practice, identifying bone loss in the presence of an IMTM is essential to assessing the overall prognosis and planning the appropriate treatment strategy. Despite the possible limitations of the OPG, clinicians continue to rely on it for interventional decisions [17]. In the current study, the second OPG was available for patients from both groups because they had revisited the hospital and taken the OPGs for other dental needs. No significant differences in bone loss were observed among patients in the different age groups, although it appeared to be more pronounced in those aged ≥51 years in the control group. This finding differs from those reported by Dias et al. [18]; wherein statistically significant differences in the severity of bone loss were seen among participants <50 years old. Interestingly, our findings demonstrated bone loss in the 40–50 age group among the patients in the study group. Furthermore, our results agreed with those in the study by Fernandes et al. [19]; which indicated an association between age and the change in the status of the alveolar crest. In the current study, a higher degree of bone loss was observed among males than females, but the difference was not statistically significant. Similar findings were reported by Dias et al. [18]; wherein no significant difference in the severity of bone loss distal to the MSM was noted between males and females using panoramic radiography. It should be emphasized that several factors, such as smoking habits, impacted positioning, and maintenance of proper oral hygiene, can potentially worsen periodontal conditions on the distal aspect of the MSM [20,21]. Therefore, if the impaction is not managed, bone changes in the form of bone loss may occur. Despite variations in the IMTM inclination type and other contributing risk factors among individuals, our findings revealed bone loss in patients who did not undergo extraction of the IMTM after evaluating their follow-up OPGs. Bone improvement and gain distal to the MSM were observed after the extraction of the IMTM in the study group. These findings agree with those reported by Passarelli et al. [22]; wherein an overall improvement in the periodontal status was observed following surgical extraction of the IMTM. The removal of such teeth provides better access for cleaning, leading to overall improvement. Similarly, Krausz et al. [17] reported significant improvements in the bone on the distal aspect of the MSM after the extraction of an IMTM. These improvements were evaluated clinically and radiographically using an OPG. Additionally, they noticed mild bone loss in the control group despite variations in contributing factors, such as the degree of oral hygiene maintenance, which aligns with our findings in the control group. Furthermore, Montero et al. [23] indicated an overall improvement in the periodontal health status adjacent to the MSM after the removal of the IMTM. On the contrary, Kan et al. (24) pointed out the formation of periodontal defects on the distal aspect of the MSM after removing the IMTM. Several studies have investigated the different patterns of IMTM in various demographic samples [25,26]. In the present study, the vertical type of impaction was found to be the most prevalent, followed by the mesioangular type. Alsaegh et al. [27] reported a higher prevalence of mesioangular impaction than other types in the Arab Emirati population. Similarly, Eshghpour et al. [28] claimed a higher predominance of mesioangular impaction in the Iranian population. Prajapati et al. [7] conducted investigations on the Indian population and reported that the mesioangular inclination dominated the other patterns, such as vertical, horizontal, and distoangular. Awareness of the different inclination patterns would indicate the need to remove the IMTM and aid in determining the necessary surgical method. The current study revealed a higher number of individuals with bilateral impaction, which is different from the study conducted by Alsaegh et al. [27]; wherein a comparable distribution of unilateral and bilateral impaction was reported. However, several studies have shown considerable variations in the occurrence of bilateral and unilateral events among different populations, including Saudi Arabian, Singaporean, Chinese, and Libyan populations [29,30]. Bilateral impaction was predominant in these studies. It should be highlighted that the intra-examiner agreement was used instead of the inter-examiner agreement when assessing the OPGs. This decision was made because the assessment was performed concurrently between the observers, resulting in only one single outcome. Thus, the intra-examiner calculation was considered sufficient. To investigate the reproducibility of the OPG in estimating bone loss on the distal aspect of the MSM, a Kappa test was calculated. Based on the outcome mean, we assigned descriptive categories for the status of bone change, whether it is bone loss, bone gain, or no change of bone, to report the intra-examiner agreement. These descriptive categories were assigned to translate the quantitative measurements on panoramic radiography because of difficulties in reproducing the quantitative measures. Consequently, our Kappa results indicated a substantial agreement of 0.68. This study has some limitations. The reproducibility of a panoramic radiograph in terms of quantitative measures is questionable due to inherited limitations. However, we used this method to assess the bone loss distal to the MSM in cases of an IMTM owing to its routine use in clinical practice and the expected occurrence of such pathologic conditions. Furthermore, our study solely focused on the radiographic findings without considering the clinical parameters that may contribute to the periodontal status of the patients. Thus, further studies using alternative radiographic techniques and a larger sample size are required to validate the findings of the current study.
5. Conclusions
An increase and improvement in the bone distal to the mandibular second molar were observed after the extraction of the IMTM, as compared to the control group. Furthermore, the findings of this study suggest that considering the routine use, affordability, and convenience of the OPG, it may be beneficial for visualizing the bone status after extracting an impacted molar.
Author Contributions
H.A. contributed to the collection of the data. J.L.-L. reviewed the manuscript, guided the necessary corrections, and approved the final manuscript. S.E.-M. contributed to the writing of the manuscript. X.R.-L. contributed to the following research process. M.H. revised the manuscript structure. A.E.-D. contributed to the follow-up of the manuscript preparation and correction of possible encountered errors. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
“The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the dental hospital of the University of Barcelona (HOUB) (2022-032-1) on the date 28/09/2022.
Informed Consent Statement
“Patient consent was waived because we reviewed only the radiographic images of the patients anonymously and there was no intervention or studies on humans directly.
Data Availability Statement
All relevant data are provided within the article.
Acknowledgments
We acknowledge the personnel staff of the Dental Hospital of the University of Barcelona for their contribution.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Alfadil L, Almajed E. Prevalence of impacted third molars and the reason for extraction in Saudi Arabia. Saudi Dent J. 2020 Jul;32(5):262-268. [CrossRef]
- Gupta S, Bhowate RR, Nigam N, Saxena S. Evaluation of Impacted Mandibular Third Molars by Panoramic Radiography. ISRN Dent. 2011 Sep; 2011:1–8. [CrossRef]
- Pedro FLM, Bandéca MC, Volpato LER, Marques ATC, Borba AM, Musis CR de, et al. Prevalence of impacted teeth in a Brazilian subpopulation. J Contemp Dent Pract. 2014 Mar;15(2):209–13. [CrossRef]
- Breik O, Grubor D. The incidence of mandibular third molar impactions in different skeletal face types. Aust Dent J. 2008 Dec;53(4):320–4. [CrossRef]
- Padhye MN, Dabir A V., Girotra CS, Pandhi VH. Pattern of mandibular third molar impaction in the Indian population: a retrospective clinico-radiographic survey. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013 Sep;116(3):e161–6. [CrossRef]
- KalaiSelvan S, Ganesh SKN, Natesh P, Moorthy MS, Niazi TM, Babu SS. Prevalence and Pattern of Impacted Mandibular Third Molar: An Institution-based Retrospective Study. J Pharm Bioallied Sci. 2020 Aug;12(Suppl 1):S462–7. [CrossRef]
- Prajapati VK, Mitra R, Vinayak KM. Pattern of mandibular third molar impaction and its association to caries in mandibular second molar: A clinical variant. Dent Res J (Isfahan). 2017;14(2):137–42. [CrossRef]
- Hassan AH. Pattern of third molar impaction in a Saudi population. Clin Cosmet Investig Dent. 2010 Oct 11;2:109-13. [CrossRef]
- Arora A, Patil BA, Sodhi A. Validity of the vertical tube-shift method in determining the relationship between the mandibular third molar roots and the inferior alveolar nerve canal. J Korean Assoc Oral Maxillofac Surg. 2015 Apr;41(2):66-73. [CrossRef]
- Cederhag J, Truedsson A, Alstergren P, Shi XQ, Hellén-Halme K. Radiographic imaging in relation to the mandibular third molar: a survey among oral surgeons in Sweden. Clin Oral Investig. 2022 Feb;26(2):2073-2083. [CrossRef]
- Shukla S, Chug A, Afrashtehfar KI. Role of Cone Beam Computed Tomography in Diagnosis and Treatment Planning in Dentistry: An Update. J Int Soc Prev Community Dent. 2017 Nov;7(Suppl 3):S125-S136. [CrossRef]
- Ariizumi D, Sakamoto T, Yamamoto M, Nishii Y. External Root Resorption of Second Molars Due to Impacted Mandibular Third Molars during Orthodontic Retention. Bull Tokyo Dent Coll. 2022 Sep;63(3):129-138. [CrossRef]
- Jaju PP, Jaju SP. Cone-beam computed tomography: Time to move from ALARA to ALADA. Imaging Sci Dent. 2015 Dec;45(4):263-5. [CrossRef]
- Faria AI, Gallas-Torreira M, López-Ratón M. Mandibular second molar periodontal healing after impacted third molar extraction in young adults. J Oral Maxillofac Surg. 2012 Dec;70(12):2732-41. [CrossRef]
- Pham TAV, Nguyen NH. Periodontal Status of the Adjacent Second Molar after Impacted Mandibular Third Molar Surgical Extraction. Contemp Clin Dent. 2019 Apr-Jun;10(2):311-318. [CrossRef]
- McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb). 2012;22(3):276–82. [CrossRef]
- Krausz AA, Machtei EE, Peled M. Effects of lower third molar extraction on attachment level and alveolar bone height of the adjacent second molar. Int J Oral Maxillofac Surg. 2005 Oct;34(7):756-60. [CrossRef]
- Dias MJ, Franco A, Junqueira JL, Fayad FT, Pereira PH, Oenning AC. Marginal bone loss in the second molar related to impacted mandibular third molars: comparison between panoramic images and cone beam computed tomography. Med Oral Patol Oral Cir Bucal. 2020 May;25(3):e395-e402. [CrossRef]
- Fernandes IA, Galvão EL, Gonçalves PF, Falci SGM. Impact of the presence of partially erupted third molars on the local radiographic bone condition. Sci Rep. 2022 May;12(1):8683. [CrossRef]
- Tai S, Zhou Y, Pathak JL, Piao Z, Zhou L. The association of mandibular third molar impaction with the dental and periodontal lesions in the adjacent second molars. J Periodontol. 2021 Oct;92(10):1392-1401. [CrossRef]
- Tolentino PHMP, Rodrigues LG, Miranda de Torres É, Franco A, Silva RF. Extractions in Patients with Periodontal Diseases and Clinical Decision-Making Process. Acta Stomatol Croat. 2019 Jun;53(2):141-149. [CrossRef]
- Passarelli PC, Lajolo C, Pasquantonio G, D'Amato G, Docimo R, Verdugo F, D'Addona A. Influence of mandibular third molar surgical extraction on the periodontal status of adjacent second molars. J Periodontol. 2019 Aug;90(8):847-855. [CrossRef]
- Montero J, Mazzaglia G. Effect of removing an impacted mandibular third molar on the periodontal status of the mandibular second molar. J Oral Maxillofac Surg. 2011 Nov;69(11):2691-7. [CrossRef]
- Kan KW, Liu JK, Lo EC, Corbet EF, Leung WK. Residual periodontal defects distal to the mandibular second molar 6-36 months after impacted third molar extraction. J Clin Periodontol. 2002 Nov;29(11):1004-11. [CrossRef]
- Al-Dajani M, Abouonq AO, Almohammadi TA, Alruwaili MK, Alswilem RO, Alzoubi IA. A Cohort Study of the Patterns of Third Molar Impaction in Panoramic Radiographs in Saudi Population. Open Dent J. 2017 Dec 26;11:648-660. [CrossRef]
- Yilmaz S, Adisen MZ, Misirlioglu M, Yorubulut S. Assessment of Third Molar Impaction Pattern and Associated Clinical Symptoms in a Central Anatolian Turkish Population. Med Princ Pract. 2016;25(2):169-75. [CrossRef]
- Alsaegh MA, Abushweme DA, Ahmed KO, Ahmed SO. The pattern of mandibular third molar impaction and its relationship with the development of distal caries in adjacent second molars among Emiratis: a retrospective study. BMC Oral Health. 2022 Jul;22(1):306. [CrossRef]
- Eshghpour M, Nezadi A, Moradi A, Shamsabadi RM, Rezaei NM, Nejat A. Pattern of mandibular third molar impaction: A cross-sectional study in northeast of Iran. Niger J Clin Pract. 2014 Nov-Dec;17(6):673-7. [CrossRef]
- Zaman MU, Almutairi NS, Abdulrahman Alnashwan M, Albogami SM, Alkhammash NM, Alam MK. Pattern of Mandibular Third Molar Impaction in Nonsyndromic 17760 Patients: A Retrospective Study among Saudi Population in Central Region, Saudi Arabia. Biomed Res Int. 2021 Aug;2021:1880750. [CrossRef]
- Quek SL, Tay CK, Tay KH, Toh SL, Lim KC. Pattern of third molar impaction in a Singapore Chinese population: a retrospective radiographic survey. Int J Oral Maxillofac Surg. 2003 Oct;32(5):548–52. [CrossRef]
Figure 1.
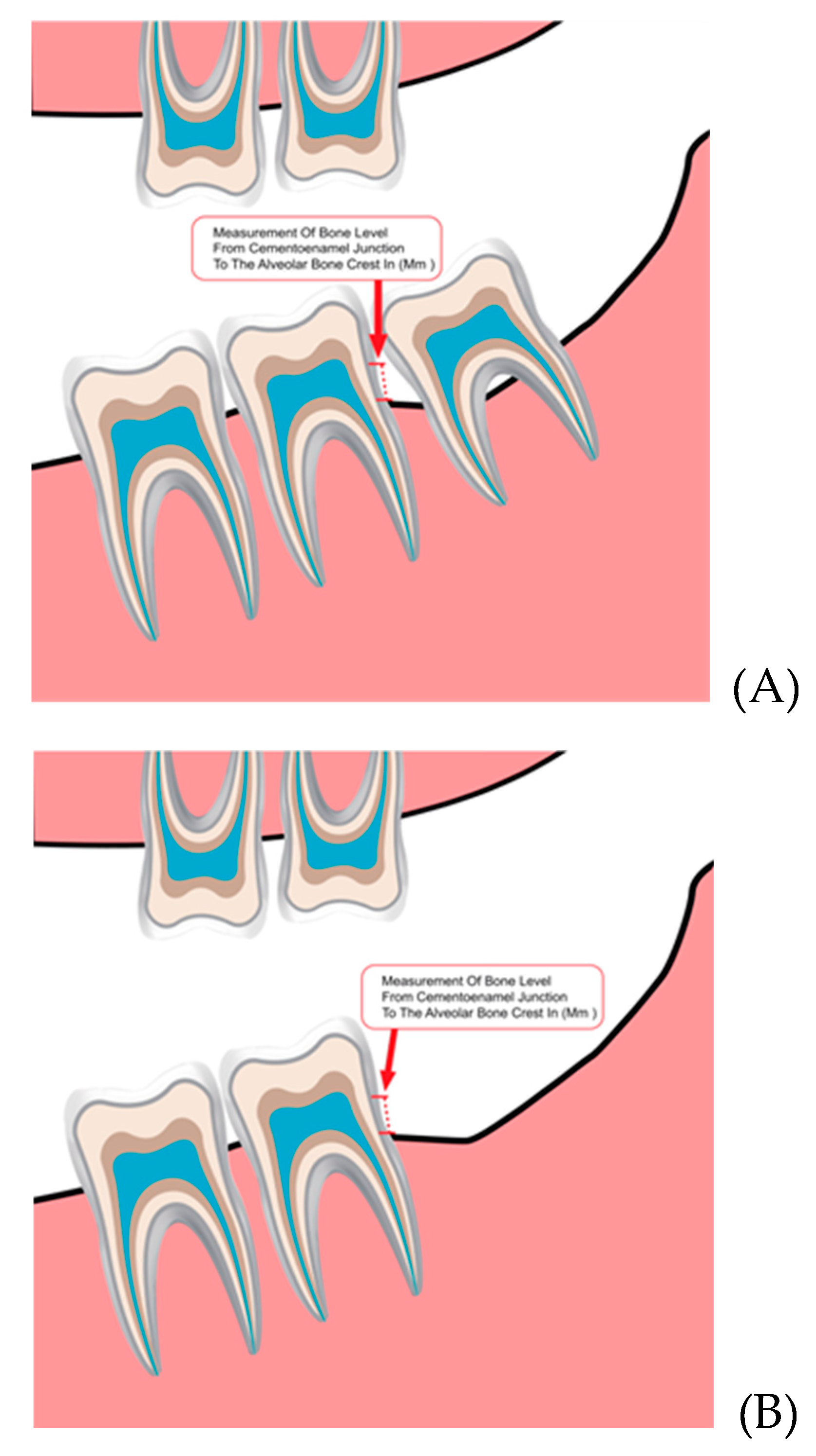
Figure 2.
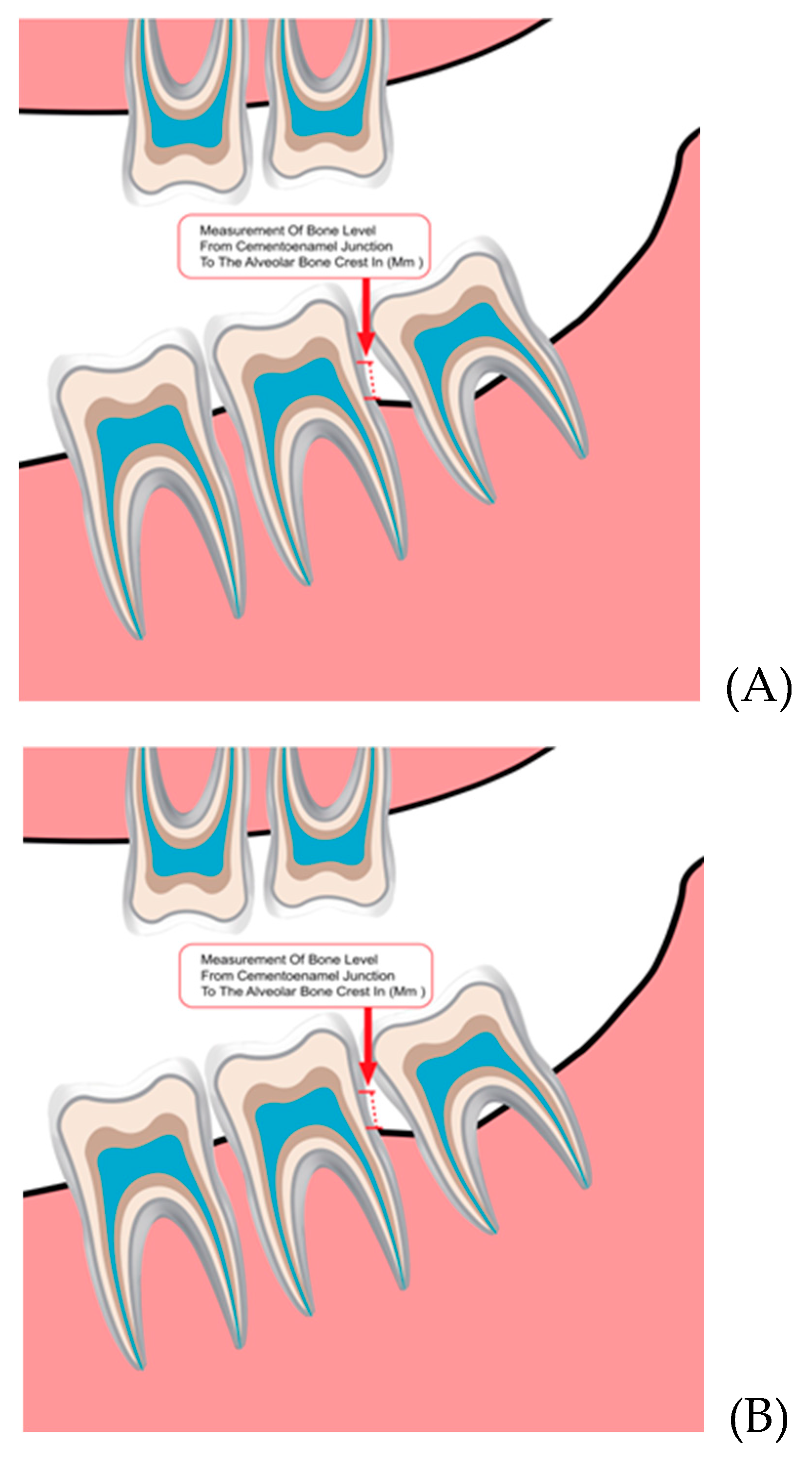

Table 1.
Comparison of bone changes between study group and control group.
| Group | Baseline Bone Level Mean SD* |
Bone Level after Extraction/Follow-up Mean SD |
p-Value |
|---|---|---|---|
| Study group | 3.00 ± 1.68 | 2.63 ± 1.75 | 0.0001 |
| Control group | 2.73 ± 1.75 | 3.01 ± 1.98 | 0.001 |
*SD, standard deviation.
Table 2.
Bone level changes in the two groups based on gender.
| Groups | Gender | Baseline BL1 | Follow up BL2 | Bone Change df (mm)3 | p-Value |
|---|---|---|---|---|---|
| Study | Male | 3.51 ± 1.89 | 3.27 ± 2.17 | 0.24 ± 1.29 | 0.190 |
| Female | 2.73 ± 1.35 | 2.29 ± 1.41 | 0.44 ± 1.13 | ||
| Control | Male | 3.64 ± 1.79 | 4.12 ± 2.11 | -0.48 ± 0.66 | 0.734 |
| Female | 1.97 ± 1.32 | 2.11 ± 1.3 | -0.13 ± 0.31 |
1= bone loss measured before extraction in study group and at baseline in control group (non-extraction group); 2= bone loss measured after extraction in study group and after following up in the control group; 3= bone level difference between the two times measurements.
Table 3.
Bone level changes in relation to the different age groups.
| Groups | Age Groups | Baseline BL | Follow up BL | Bone Change df (mm) | p-Value |
|---|---|---|---|---|---|
| Study | 18–28 | 2.48 ± 1.51 | 2.18 ± 1.57 | 0.29 ± 1.07 | 0.05 |
| 29–39 | 3.25 ± 1.69 | 2.29 ± 1.51 | 0.96 ± 1.05 | ||
| 40–50 | 4.30 ± 3.53 | 5.50 ± 3.39 | -1.20 ± 0.14 | ||
| ≥51 | 3.51 ± 1.53 | 3.45 ± 1.44 | 0.05 ± 1.34 | ||
| Control | 18–28 | 2.93 ± 1.94 | 3.19 ± 2.13 | -0.26 ± 0.53 | 0.07 |
| 29–39 | 2.28 ± 1.32 | 2.45 ± 1.50 | -0.17 ± 0.25 | ||
| 40–50 | 2.20 ± 0.71 | 2.38 ± 0.46 | -0.17 ± 0.25 | ||
| ≥51 | 2.58 ± 1.72 | 3.16 ± 2.35 | -0.57 ± 0.69 |
Table 4.
Distribution of the impaction pattern according to Winter’s classification.
| Classification | Inclination | Study Group (N) (F) |
Control Group (N) (F) |
Total Sample (N) (F) |
P-Value | |||
|---|---|---|---|---|---|---|---|---|
| Winter’s classification | Vertical | 31 | 44.9% | 35 | 50% | 66 | 41.25% | 0.539 |
| Mesioangular | 26 | 37.7% | 20 | 28.6% | 46 | 28.75% | ||
| Distoangular | 1 | 1.4% | 0 | 0% | 1 | 1.25% | ||
| Horizontal | 10 | 14.5% | 15 | 21.4% | 25 | 16.62% | ||
| Buccally tilted | 1 | 1.4% | 0 | 0% | 1 | 1.25% | ||
| Total | 69 | 86.25% | 70 | 87.5% | 139 | 82.28% | ||
Table 5.
the occurrence of the impact among the two groups in relation to the sides.
| Impaction Side | Occurrence |
Study Group (N) (F) |
Control Group (N) (F) |
Total Sample (N) (F) |
P-Value | |||
| Right | 6 | 15% | 3 | 7.5% | 9 | 11.3% | 0.509 | |
| Left | 5 | 12.5% | 7 | 17.5% | 12 | 15% | ||
| Bilateral | 29 | 72.5% | 30 | 75% | 59 | 73.8% | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



