Submitted:
05 January 2024
Posted:
08 January 2024
You are already at the latest version
Abstract
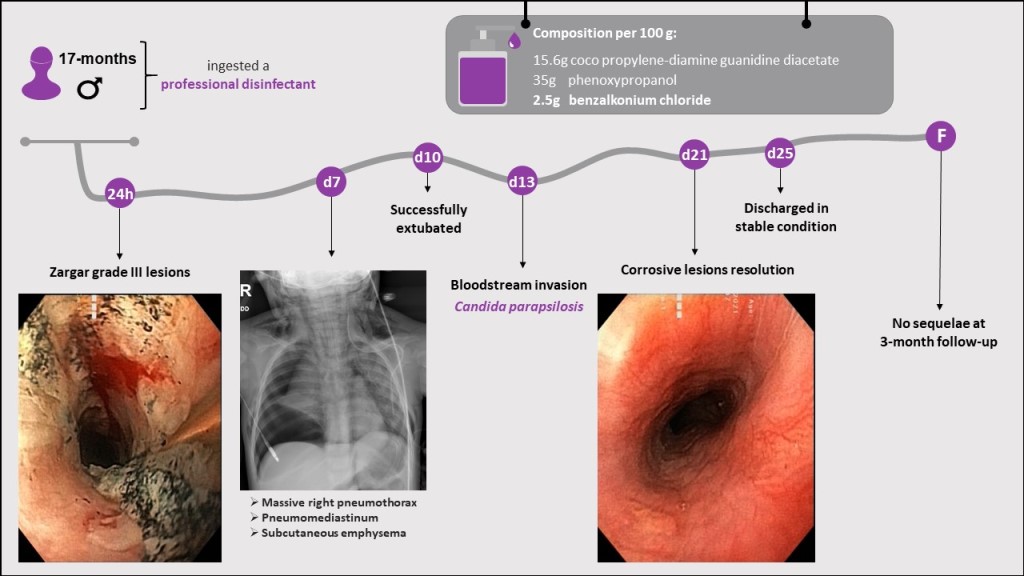
The use of disinfectants, particularly those containing quaternary ammonium compounds (QUACs), has dramatically escalated globally since the coronavirus disease 2019 pandemic. We report a case that highlights the risks associated with the ingestion of a low-concentration QUACs solution and emphasizes the importance of effective management in resolving severe lesions without sequelae. A 17-month-old boy experienced severe respiratory failure after ingesting a disinfectant containing benzalkonium chloride (BAC). The child was initially treated in a local emergency department and was subsequently transferred to a pediatric poison center. Upon evaluation, the child was found to have grade III-A corrosive esophageal lesions and chemical pneumonitis. Several complications, including massive pneumothorax and candidemia, occurred during the clinical course of the disease. However, with timely medical intervention and appropriate supportive care, the patient completely recovered without any long-term sequelae. The properties of BAC and a comprehensive management approach may have been responsible for the patient's full recovery despite the potential life-threatening effects of the ingestion of disinfectants.
Keywords:
disinfectants
; quaternary ammonium compounds
; benzalkonium compounds
; poisoning
; child
; aspiration
; pneumonia
; pneumothorax
; corrosion
1. Introduction
The global spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has led to a substantial increase in the use of disinfectants [1,2,3]. The United States Environmental Protection Agency has published a list of disinfectants proven to be effective against SARS-CoV-2 [4]. Approximately half of these products contain quaternary ammonium compounds (QUACs) as active ingredients [5,6]. Although QUACs have been used as disinfectants and sanitizers since 1930 [6], their use by the general population has significantly increased due to public awareness regarding their efficacy against SARS-CoV-2 [2,5].
Benzalkonium chloride (BAC), a cationic surfactant with well-documented antimicrobial properties [4,6], is a QUAC. BAC can displace divalent cations from the lipid bilayers of bacterial cell membranes, including those of human cells [6,7,8].
It was initially believed that the toxicological profile of BAC was limited to local effects due to its high elimination via feces, which was assumed to be related to an absorption rate from the gastrointestinal tract <10% [4]. However, Seguin et al. [10] characterized the metabolic pathways of BAC via hepatic CYP enzymes, providing an alternative explanation for its high elimination in the stool. The presence of BAC in blood samples serves as evidence of systemic exposure [2,9].
The manifestations of BAC largely overlap with those of alkali compounds, with corrosive tissue damage being the predominant characteristic [10,11]. However, BC toxicological profiles reveal specific effects of BAC, including apoptosis-induced lung injury [7,10], bronchoconstriction [12], and hypersensitivity reactions [13,14,15,16].
The clinical and biological features of BAC poisoning are derived from sporadic case reports and case series as observational studies regarding QUAC exposure are lacking. Herein, we report a case to contribute to the accumulation of knowledge regarding the hazards of disinfectant ingestion in children, focusing on the risks associated with the use of QUACs.
2. Case Description
A 17-month-old boy ingested an unknown quantity of disinfectant while riding in a car seat. The disinfectant was stored in a sippy-cap water bottle within the child's reach and was intended for the disinfection of objects. Upon ingestion, the mother promptly induced vomiting and rushed the child to the nearest emergency department. Fortunately, the original bottle was retained by the mother, allowing for the identification of the chemical composition and properties of the disinfectant (Table 1).
The patient’s condition rapidly deteriorated at the local emergency department, resulting in severe respiratory failure due to glottic edema. The patient required intubation and mechanical ventilation to ensure adequate respiration. Following clinical stabilization, our poison center was contacted, and the child was subsequently transferred to our clinic via air ambulance.
The patient was admitted to our intensive care unit five hours after ingestion. On physical examination, the patient was comatose, intubated, and mechanically ventilated. The patient was febrile (38.4°C), with a heart rate of 150 beats per minute, normal blood pressure of 94/54 mmHg, and normal urinary output. The chest was clear on auscultation and no adventitious sounds were heard. Cardiac examination revealed normal heart sounds. The abdominal wall palpatory examination results were normal, including the limits of the liver and spleen. However, an oral cavity examination revealed intense oropharyngeal edema, hyperemia, and massive swelling of the uvula. No pathological dermatologic changes were observed.
The patient's initial blood test results indicated metabolic acidosis (pH 7.25; base excess: -7.7 mmol/l), an increased white blood cell count (17,190 cells/mm3 - reference range: 4,000–12,000 cells/mm3) with a predominance of neutrophils (84%), and an elevated creatine kinase concentration (238 U/L - reference range: 0–171 U/L). Bacterial cultures obtained at admission were negative, except for positive results for coagulase-negative Staphylococcus on auricular and cutaneous swabs and Streptococcus pneumoniae on nasal swabs. The initial chest radiograph revealed bilateral perihilar alveolar infiltration (Figure 1A).
The severity of the lesions was assumed to be significant due to the hazardous nature of the substance [18,19,20] and the presence of clinical and laboratory risk factors [21,22,23,24]. Therefore, the treatment was initiated immediately (Figure 2). A nasogastric tube was inserted and partial parenteral nutrition was started, including amino acids, glucose, and lipid emulsion. According to established guidelines [25,26], the patient was administered 2 mg/kg/day of pantoprazole intravenously (IV), 10 mg/kg/day of methylprednisolone IV, and a broad-spectrum antibiotic regimen consisting of meropenem at 50 mg/kg/day IV and gentamicin at 4 mg/kg/day IV.
The use of corticosteroids has been debated in several studies [25,26,27]. Currently, the European Society of Gastrointestinal Endoscopy and European Society for Pediatric Gastroenterology Hepatology and Nutrition guidelines endorse their use for grade IIB lesions and suggest their possible implementation for grade III lesions [28].
Based on state-of-the-art practices [25,26], an endoscopic procedure was performed 16 h after ingestion, revealing the presence of grade III-A lesions according to the Zargar classification [29]. The patient’s mucosal edema diminished, exposing extensive areas of sloughing lesions in the oral cavity, pharynx, and vocal cords and bleeding spots on the tonsils. The esophagus exhibited patchy necrosis, ulceration, and sloughing (Figure 3A–D). The gastric mucosa displayed prominent hyperemia and bleeding marks (Figure 3E,F).
Biological samples were collected on a periodic basis for the purpose of monitoring patient progress and modifying treatment plans as necessary. The laboratory test results are presented kinetically in Figure 4. Notable increases in inflammatory markers were detected four days after ingestion.
The patient’s lung damage progressively worsened, ultimately resulting in the development of subcutaneous emphysema, pneumomediastinum, and massive right pneumothorax on hospital day seven (Figure 2B), necessitating urgent drainage tube implantation. Subsequently, the patient’s lung damage gradually improved, as confirmed by blood tests and chest radiography on hospital day 10. The patient was then successfully extubated. Thoracic angio-computed tomography revealed improvements in the patient’s lung status with only a small condensation in the right upper lobe. On hospital day 12, the patient was transferred to the toxicology department.
During the initial 24 h in the toxicology department, the patient’s status deteriorated, with fever and sleepiness. The central venous catheter (CVC) was removed, and microbiological CVC cultures (negative) and blood cultures (positive for Candida parapsilosis) were performed. Based on these findings, 40 mg/kg/day IV vancomycin was administered for 10 days, followed by five days each of 100 mg/kg/day IV ceftriaxone and 7 mg/kg/day IV fluconazole (Figure 3).
The patient's response to treatment was favorable. On hospital day 18, the nasogastric tube was successfully removed and the patient was able to resume oral alimentation, which was initiated as clear liquids and progressed to double-mixed alimentation.
Follow-up endoscopy conducted on hospital day 21 revealed a significant improvement in the patient's condition, with small ulcerations on the tongue, an edematous pharynx, ulcerations (< 0.5 cm), punctiform necrosis in the esophagus, and hyperemic mucosa in the stomach (Figure 5).
On hospital day 25, the patient was discharged in stable condition. The patient had a normal appetite, normal swallowing function, and normal laboratory values, with the exception of iron-deficiency anemia. At home, the child received semiliquid nourishment, oral iron therapy, and vitamin B supplementation.
Three months after ingestion, physical examination, blood test, and chest radiography results were within the normal ranges. A barium meal examination revealed normal swallowing function without any signs of gastroesophageal reflux. Endoscopy revealed a complete recovery without complications.
3. Discussion
3.1. General considerations
The exposure characteristics of our patient were similar to those in most reported cases of unintentional disinfectant poisoning [18,30]. The primary contributing factors towards disinfectant poisoning in this patient were the inappropriate storage of the hazardous chemical and its accessibility to the child [31,32]. Several studies have highlighted the significance of the absence of parental awareness regarding the hazards of corrosive substances, coupled with the absence of preventive measures, as a significant issue [33,34,35]. The tasteless and odorless properties of alkaline liquid solutions, which can lead the ingestion of a significant volume before protective reflexes intervene, were additional contributing factors in this case [21].
Severe clinical presentations of BAC poisoning have been reported, and most include patients who ingested concentrations ≥ 10% [10,36]. One report regarding BAC poisoning at a concentration < 10% was identified in a brief literature search [37]. Therefore, this report indicates that low BAC concentrations can cause severe manifestations.
3.2. Gastrointestinal tract involvement
The patient presented in this report had severe corrosive lesions in the esophagus, necessitating prompt multidisciplinary management to ensure favorable outcomes [12,34,38]. The resolution of the mucosal lesions was consistent with the expected timeframe for BAC poisoning [9]. Despite the serious nature of esophageal lesions, the current patient had a favorable outcome that did not include the development of strictures, which is noteworthy due to the abundance of risk factors typically observed in patients with alkali poisoning [21,25,38].
A literature search regarding the prevalence of strictures in patients with BAC poisoning was conducted to identify factors that may have contributed to a favorable outcome. One observational study reported the rates of stricture development in patients with BAC poisoning. This study included 11 children who had ingested BAC among 968 cases of corrosive poisoning and none of the patients developed strictures [11]. However, the previous study did not report the burn severity.
In a review of the reported cases in both adults [39] and children [37,40,41,42,43] who survived the ingestion of BAC solutions, strictures were described in few neonatal cases [42]. Therefore, the positive outcome in our patient and the management or nature of the substance involved are likely not directly and causally related.
3.3. Respiratory tract involvement
The rapid development of acute respiratory distress in this patient may be related to laryngeal edema and BAC-induced bronchoconstriction through the release of mediators from mast cells and stimulation of cholinergic receptors [10]. The mechanisms of lung toxicity have been extensively studied via animal models [12], cell culture investigations [7], and forensic reports [10], resulting in the characterization of BAC-induced lung injury. Based on these data and previously reported cases [39,40,41,42,43], we concluded that our patient developed chemical pneumonitis due to aspiration of the BAC solution.
The worsening of our patient’s condition that occurred on hospital day seven had not been previously reported in cases of QUAC-related poisoning. This may be due to the occurrence of a delayed toxic event facilitated by apoptosis, which is the primary mechanism underlying BAC-induced lung injury [12]. However, it is more likely that the incident was related to prolonged mechanical ventilation, as demonstrated by Amigoni et al. [44] who reported that chemical injury in one lung may lead to mechanical ventilation-induced injury in the contralateral lung.
3.4. Other complications
The patient in this case report experienced candidemia as an indirect consequence of BAC poisoning. According to Chirica et al. [45], bloodstream microbial invasion and elevated inflammatory markers are indicative of tardive esophageal rupture. However, this was not observed in the current patient. Candidemia may have resulted from prolonged hospitalization in the intensive care unit.
4. Conclusions
The ingestion of disinfectants is a significant public health concern that can result in severe and potentially life-threatening effects. The current patient had acute symptoms and a severe clinical course, though he ultimately recovered without any long-term impairment. This favorable outcome may be attributed to the properties of BAC or the comprehensive management approach used in this patient. It is essential that clinical toxicologists be aware of the potential, yet rare, hazards posed by low-concentration QUAC solutions and exercise caution in managing such cases.
Author Contributions
Conceptualization, V.N. and C.U.; methodology, V.N., A.L., D.B., and C.U.; formal analysis, V.N. and A.L.; investigation, V.N., A.L., D.B., and C.U.; resources, V.N..; data curation, A.L.; writing—original draft preparation, A.L. and D.B.; writing—review and editing, V.N. and C.U..; visualization, A.L..; supervision, C.U.; project administration, V.N.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the hospital’s ethics committee.
Informed Consent Statement
Written informed consent was obtained from the patient’s legal representative in accordance with the hospital protocol for publication of this case report. The following data were removed to ensure patient de-identification: name, address, contact information, birth date, admission date, discharge date, and medical record number.
Data Availability Statement
All data are available in the article body.
Acknowledgments
The authors extend their gratitude to Dr. Viorel Dănilă and his team for conducting the endoscopy and providing the video endoscopy images.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Rosenman, K. D.; Reilly, M. J.; Wang, L. Calls to a State Poison Center Concerning Cleaners and Disinfectants From the Onset of the COVID-19 Pandemic Through April 2020; 2021; Vol. 136. [CrossRef]
- Hrubec, T. C.; Seguin, R. P.; Xu, L.; Cortopassi, G. A.; Datta, S.; Hanlon, A. L.; Lozano, A. J.; McDonald, V. A.; Healy, C. A.; Anderson, T. C.; Musse, N. A.; Williams, R. T. Altered Toxicological Endpoints in Humans from Common Quaternary Ammonium Compound Disinfectant Exposure. Toxicol Rep 2021, 8, 646–656. [CrossRef]
- Li, D.; Sangion, A.; Li, L. Evaluating Consumer Exposure to Disinfecting Chemicals against Coronavirus Disease 2019 (COVID-19) and Associated Health Risks. Environ Int 2020, 145, 106108. [CrossRef]
- Osimitz, T. G.; Droege, W. Quaternary Ammonium Compounds: Perspectives on Benefits, Hazards, and Risk. Toxicology Research and Application 2021, 5, 239784732110490. [CrossRef]
- Mai, Y.; Wang, Z.; Zhou, Y.; Wang, G.; Chen, J.; Lin, Y.; Ji, P.; Zhang, W.; Jing, Q.; Chen, L.; Chen, Z.; Lin, H.; Jiang, L.; Yuan, C.; Xu, P.; Huang, M. From Disinfectants to Antibiotics: Enhanced Biosafety of Quaternary Ammonium Compounds by Chemical Modification. J Hazard Mater 2023, 460, 132454. [CrossRef]
- Sapozhnikov, S. V.; Sabirova, A. E.; Shtyrlin, N. V.; Druk, A. Y.; Agafonova, M. N.; Chirkova, M. N.; Kazakova, R. R.; Grishaev, D. Y.; Nikishova, T. V.; Krylova, E. S.; Nikitina, E. V.; Kayumov, A. R.; Shtyrlin, Y. G. Design, Synthesis, Antibacterial Activity and Toxicity of Novel Quaternary Ammonium Compounds Based on Pyridoxine and Fatty Acids. Eur J Med Chem 2021, 211. [CrossRef]
- Kim, S. H.; Kwon, D.; Lee, S.; Son, S. W.; Kwon, J. T.; Kim, P. J.; Lee, Y. H.; Jung, Y. S. Concentration-and Time-Dependent Effects of Benzalkonium Chloride in Human Lung Epithelial Cells: Necrosis, Apoptosis, or Epithelial Mesenchymal Transition. Toxics 2020, 8 (1). [CrossRef]
- Pereira, B. M. P.; Tagkopoulos, I. Benzalkonium Chlorides: Uses, Regulatory Status, and Microbial Resistance. Applied and Environmental Microbiology. American Society for Microbiology 2019. [CrossRef]
- Mishima-Kimura, S.; Yonemitsu, K.; Ohtsu, Y.; Sasao, A.; Tsutsumi, H.; Furukawa, S.; Nishitani, Y. Liquid Chromatography-Tandem Mass Spectrometry Detection of Benzalkonium Chloride (BZK) in a Forensic Autopsy Case with Survival for 18 days Post BZK Ingestion. Leg Med 2018, 32, 48–51. [CrossRef]
- Tambuzzi, S.; Gentile, G.; Andreola, S.; Migliorini, A. S.; Zoja, R. Visceral Microscopic Pattern From Suicidal Ingestion of Professional Lysoform® With Delayed Death. Acad Forensic Pathol 2022, 12 (3), 118–125. [CrossRef]
- Karaman, I.; Koç, O.; Karaman, A.; Erdogan, D.; Çavusoglu, Y. H.; Afsarlar, Ç. E.; Yilmaz, E.; Ertürk, A.; Balci, Ö.; Özgüner, I. F. Evaluation of 968 Children with Corrosive Substance Ingestion. Indian Journal of Critical Care Medicine 2015, 19 (12), 714–718. [CrossRef]
- Lee, H.; Park, K. Acute Toxicity of Benzalkonium Chloride in Balb/c Mice Following Intratracheal Instillation and Oral Administration. Environ Anal Health Toxicol 2019, 34 (3), e2019009. [CrossRef]
- Wentworth, A. B.; Yiannias, J. A.; Davis, M. D. P.; Killian, J. M. Benzalkonium Chloride: A Known Irritant and Novel Allergen. Dermatitis 2016, 27 (1), 14–20. [CrossRef]
- Peyneau, M.; de Chaisemartin, L.; Gigant, N.; Chollet-Martin, S.; Kerdine-Römer, S. Quaternary Ammonium Compounds in Hypersensitivity Reactions. Frontiers in Toxicology 2022, 4. [CrossRef]
- Migueres, N.; Debaille, C.; Walusiak-Skorupa, J.; Lipińska-Ojrzanowska, A.; Munoz, X.; van Kampen, V.; Suojalehto, H.; Suuronen, K.; Seed, M.; Lee, S.; Rifflart, C.; Godet, J.; de Blay, F.; Vandenplas, O. Occupational Asthma Caused by Quaternary Ammonium Compounds: A Multicenter Cohort Study. J Allergy Clin Immunol Pract 2021, 9 (9), 3387–3395. [CrossRef]
- Lechien, J. R.; Costa De Araujo, P.; De Marrez, L. G.; Halloy, J.-L.; Khalife, M.; Saussez, S. Contact Allergy to Benzalkonium Chloride in Patients Using a Steroid Nasal Spray: A Report of 3 Cases; 2018. https://www.entjournal.com/print/article/contact-allergy-benzalkonium-chloride-patients-using-steroid-nasal-spray-report-3-cases.
- Gigasept® instru AF Product Information Sheet. Available online: https://www.schuelke.com/media/products/docs/en/PRI_gigasept_instru_AF_664_EN_062023_06.pdf (first accessed on November 26, 2021, most recent date of access was December 27, 2023).
- Obarski, P.; Włodarczyk, J. Diagnosis and Management of Gastrointestinal Chemical Burns and Post-Burn Oesophageal Stenosis. Kardiochirurgia i Torakochirurgia Polska. Termedia Publishing House Ltd. 2021, pp 252–259. [CrossRef]
- Chen, Y. J.; Seak, C. J.; Kang, S. C.; Chen, T. H.; Chen, C. C.; Ng, C. J.; Lee, C. W.; Su, M. Y.; Huang, H. C.; Chen, P. C.; Ooyang, C. H.; Hsieh, S. Y.; Cheng, H. T. A New Perspective of the Risk of Caustic Substance Ingestion: The Outcomes of 468 Patients in One North Taiwan Medical Center within 20 Years. Clin Toxicol 2021, 59 (5), 409–417. [CrossRef]
- Rossi, A. Acute Caustic Ingestion: State of Art and New Trends. J Gastroenterol Hepatol Res 2015, 4 (3), 1501–1506. [CrossRef]
- Meena, B. L.; Narayan, K. S.; Goyal, G.; Sultania, S.; Nijhawan, S. Corrosive Injuries of the Upper Gastrointestinal Tract. Journal of Digestive Endoscopy 2017, 08 (04), 165–169. [CrossRef]
- Chirica, M.; Bonavina, L.; Kelly, M. D.; Sarfati, E.; Cattan, P. Caustic Ingestion. The Lancet. Lancet Publishing Group May 20, 2017, pp 2041–2052. [CrossRef]
- Caganova, B.; Foltanova, T.; Plackova, S.; Placha, K.; Bibza, J.; Puchon, E.; Ondriasova, E.; Batora, I. Caustic Effects of Chemicals: Risk Factors for Complications and Mortality in Acute Poisoning. Monatsh Chem 2017, 148 (3), 497–503. [CrossRef]
- Sharif, A. F.; Gameel, D. E. G. El; Abdo, S. A. E.-F.; Elgebally, E. I.; Fayed, M. M. Evaluation of Pediatric Early Warning System and Drooling Reluctance Oropharynx Others Leukocytosis Scores as Prognostic Tools for Pediatric Caustic Ingestion: A Two-Center, Cross-Sectional Study. Environmental Science and Pollution Research 2022, 29 (4), 5378–5395. [CrossRef]
- Hall, A. H.; Jacquemin, D.; Henny, D.; Mathieu, L.; Josset, P.; Meyer, B. Corrosive Substances Ingestion: A Review. Critical Reviews in Toxicology. Taylor and Francis Ltd September 14, 2019, pp 637–669. [CrossRef]
- Oliva, S.; Romano, C.; De Angelis, P.; Isoldi, S.; Mantegazza, C.; Felici, E.; Dabizzi, E.; Fava, G.; Renzo, S.; Strisciuglio, C.; Quitadamo, P.; Saccomani, M. D.; Bramuzzo, M.; Orizio, P.; Nardo, G. Di; Bortoluzzi, F.; Pellegrino, M.; Illiceto, M. T.; Torroni, F.; Cisarò, F.; Zullo, A.; Macchini, F.; Gaiani, F.; Raffaele, A.; Bizzarri, B.; Arrigo, S.; de’ Angelis, G. L.; Martinelli, M.; Norsa, L. Foreign Body and Caustic Ingestions in Children: A Clinical Practice Guideline: Foreign Bodies and Caustic Ingestions in Children. Digestive and Liver Disease 2020, 52 (11), 1266–1281. [CrossRef]
- Usta, M.; Erkan, T.; Cokugras, F. C.; Urganci, N.; Onal, Z.; Gulcan, M.; Kutlu, T. High Doses of Methylprednisolone in the Management of Caustic Esophageal Burns. Pediatrics 2014, 133 (6). [CrossRef]
- Tringali, A.; Thomson, M.; Dumonceau, J. M.; Tavares, M.; Tabbers, M. M.; Furlano, R.; Spaander, M.; Hassan, C.; Tzvinikos, C.; Ijsselstijn, H.; Viala, J.; Dall’Oglio, L.; Benninga, M.; Orel, R.; Vandenplas, Y.; Keil, R.; Romano, C.; Brownstone, E.; Hlava, Š.; Gerner, P.; Dolak, W.; Landi, R.; Huber, W. D.; Everett, S.; Vecsei, A.; Aabakken, L.; Amil-Dias, J.; Zambelli, A. Pediatric Gastrointestinal Endoscopy: European Society of Gastrointestinal Endoscopy (ESGE) and European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) Guideline Executive Summary. Endoscopy. Georg Thieme Verlag January 1, 2017, pp 83–91. [CrossRef]
- Ali Zargar, S.; Kochhar, R.; Mehta, S.; Kumar Mehta, S. The Role of Fiberoptic Endoscopy in the Management of Corrosive Ingestion and Modified Endoscopic Classification of Burns. Gastrointest Endosc 1991, 37 (2), 165–169. [CrossRef]
- Mantho, P.; Engbang, J. P.; Ndzana Awono, C. D.; Essola, B.; Kamguep, T.; Noah Noah, D.; Ngowe Ngowe, M. Caustic Esophageal Strictures in Children: Diagnosis, Treatment and Evolution in the City of Douala. J Surg Res (Houst) 2022, 05 (03). [CrossRef]
- Demirören, K.; Kocamaz, H.; Doğan, Y. Gastrointestinal System Lesions in Children Due to the Ingestion of Alkali and Acid Corrosive Substances. Turk J Med Sci 2015, 45 (1), 184–190. [CrossRef]
- Ollandzobo, L. C. A.-I. I.; Ahoui-Apendi, C.; Mimiesse-Monamou, J. F.; Babela, J. R. M.; D.-G.; Ibara, B. I. A.; Ibara, J.-R. Ingestion of Caustics by Children in Brazzaville (CONGO). Open J Pediatr 2018, 08 (03), 283–291. [CrossRef]
- Alser, O.; Hamouri, S.; Novotny, N. M. Esophageal Caustic Injuries in Pediatrics: A Sobering Global Health Issue. Asian Cardiovascular and Thoracic Annals. SAGE Publications Inc. July 1, 2019, pp 431–435. [CrossRef]
- Niedzielski, A.; Schwartz, S. G.; Partycka-Pietrzyk, K.; Mielnik-Niedzielska, G. Caustic Agents Ingestion in Children: A 51-Year Retrospective Cohort Study. Ear Nose Throat J 2020, 99 (1), 52–57. [CrossRef]
- Nardo, G. Di; Betalli, P.; Illiceto, M. T.; Giulia, G.; Martemucci, L.; Caruso, F.; Lisi, G.; Romano, G.; Villa, M. P.; Ziparo, C.; Pensabene, L.; Vassallo, F.; Quitadamo, P. Caustic Ingestion in Children: 1 Year Experience in 3 Italian Referral Centers. J Pediatr Gastroenterol Nutr 2020, 71 (1), 19–22. [CrossRef]
- Spiller, H. A. A Case of Fatal Ingestion of a 10% Benzalkonium Chloride Solution. Journal of Forensic Toxicology and Pharmacology 2014, 03 (01). [CrossRef]
- Wilson, J. T. Benzalkonium Chloride Poisoning in Infant Twins. Arch Pediatr Adolesc Med 1975, 129 (10), 1208. [CrossRef]
- Elkaramany, M. An Overview of Corrosive Injury of the Upper Gastrointestinal Tract: Discussion of Types, Clinical Evaluation, and Management Procedures. Advances in Digestive Medicine 2018, 5 (4), 115–120. [CrossRef]
- Amit Kumar; Rajesh Chetiwal; Priyank Rastogi; Shweta Tanwar; Saurabh Gupta; Rajesh Patnaik; Maduri Vankayalapati; Sudhish Gupta; Alok Arya. Severe Esophagitis and Chemical Pneumonitis as a Consequence of Dilute Benzalkonium Chloride Ingestion: A Case Report. International Journal of Medical Students 2021. [CrossRef]
- Bekdas, M.; Ozturk, S.; Kara, B.; Acar, S.; Ozturk, H. An Unpleasant Result of Imprecision: Esophageal Corrosive Injury Due to the Oral Intake of 10% Benzalkonium Chloride. Br J Med Med Res 2016, 14 (4), 1–4. [CrossRef]
- Civan, H. A.; Gulcu, D.; Erkan, T. Corrosive Esophagitis with Benzalkonium Chloride in a Two Days Old Neonate. Pediatr Gastroenterol Hepatol Nutr 2016, 19 (3), 207–209. [CrossRef]
- Turan, C.; Özkan, U.; Özokutan, B. H.; Özdemir, M.; Okur, H.; Küçükayd&#x, M. Corrosive Injuries of the Esophagus in Newborns. Pediatr Surg Int 2000, 16 (7), 483–484. [CrossRef]
- Okan, F.; Coban, A.; Ince, Z.; Can, G. A Rare and Preventable Cause of Respiratory Insufficiency Ingestion of Benzalkonium Chloride; 2007. [CrossRef]
- Amigoni, M.; Bellani, G.; Zambelli, V.; Scanziani, M.; Farina, F.; Fagnani, L.; Latini, R.; Fumagalli, R.; Pesenti, A. Unilateral Acid Aspiration Augments the Effects of Ventilator Lung Injury in the Contralateral Lung. Anesthesiology 2013, 119 (3), 642–651. [CrossRef]
- Chirica, M.; Kelly, M. D.; Siboni, S.; Aiolfi, A.; Riva, C. G.; Asti, E.; Ferrari, D.; Leppäniemi, A.; Ten Broek, R. P. G.; Brichon, P. Y.; Kluger, Y.; Fraga, G. P.; Frey, G.; Andreollo, N. A.; Coccolini, F.; Frattini, C.; Moore, E. E.; Chiara, O.; Di Saverio, S.; Sartelli, M.; Weber, D.; Ansaloni, L.; Biffl, W.; Corte, H.; Wani, I.; Baiocchi, G.; Cattan, P.; Catena, F.; Bonavina, L. Esophageal Emergencies: WSES Guidelines. World Journal of Emergency Surgery. BioMed Central Ltd. May 31, 2019. [CrossRef]
Figure 1.
Chest radiographs: (A) Upon admission, a chest radiograph depicted bilateral perihilar alveolar infiltration; (B) Chest radiograph performed on hospital day seven showed subcutaneous emphysema, pneumomediastinum, and massive right pneumothorax; (C) At discharge, the chest radiograph displayed a normal aspect.
Figure 1.
Chest radiographs: (A) Upon admission, a chest radiograph depicted bilateral perihilar alveolar infiltration; (B) Chest radiograph performed on hospital day seven showed subcutaneous emphysema, pneumomediastinum, and massive right pneumothorax; (C) At discharge, the chest radiograph displayed a normal aspect.
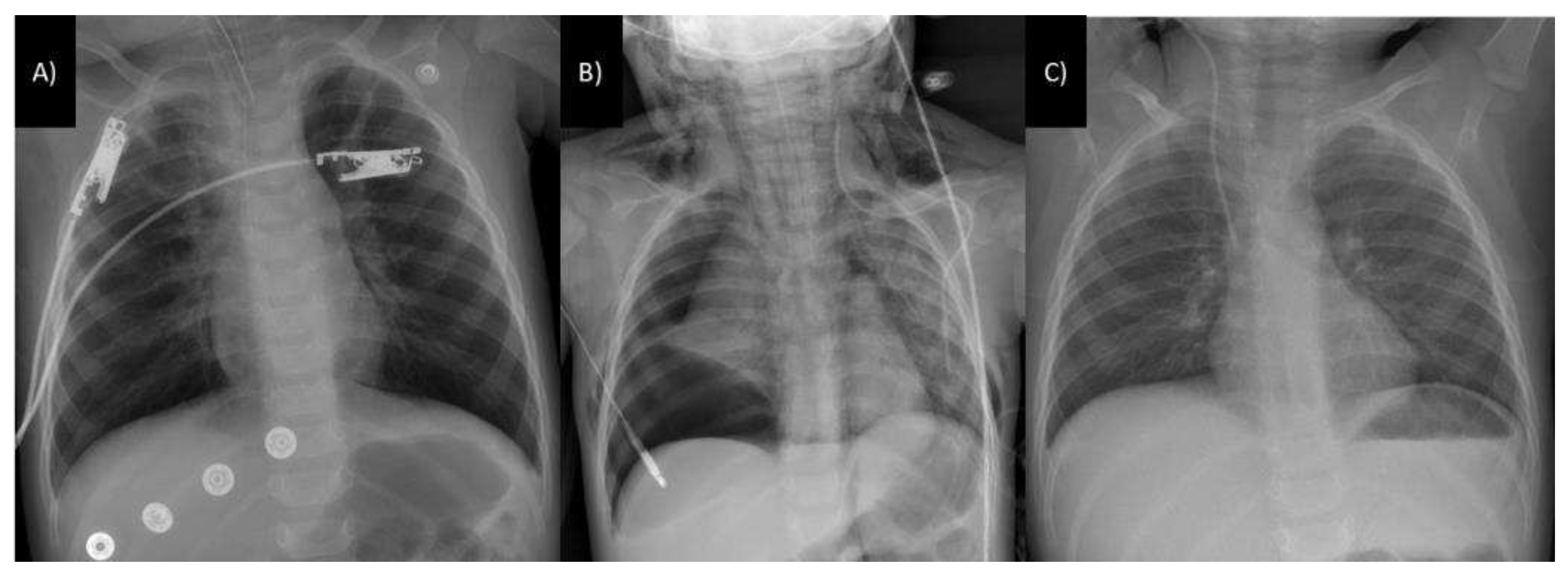
Figure 2.
Treatment during hospitalization. The patient’s treatment was complex and included partial parenteral nutrition, broad-spectrum antibiotics, and corticosteroids. A specific treatment was added for Candida bloodstream invasion. Abbreviations: IV, intravenous; mg, milligram; kg, kilogram. initiated.
Figure 2.
Treatment during hospitalization. The patient’s treatment was complex and included partial parenteral nutrition, broad-spectrum antibiotics, and corticosteroids. A specific treatment was added for Candida bloodstream invasion. Abbreviations: IV, intravenous; mg, milligram; kg, kilogram. initiated.
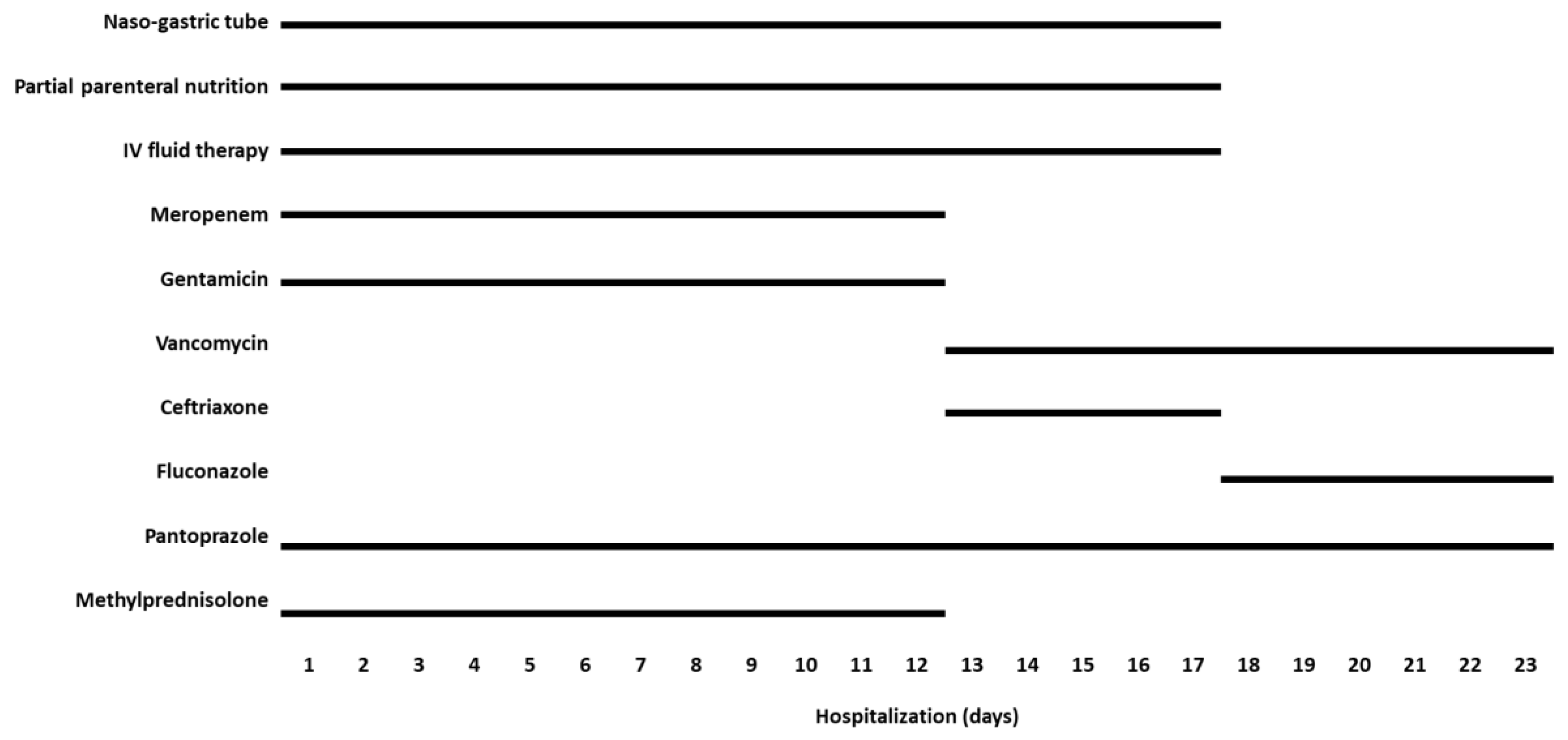
Figure 3.
Superior digestive endoscopy performed at 16 h after ingestion: (A-D) The esophagus exhibited patchy necrosis, ulceration, and sloughing; (E-F) The gastric mucosa displayed prominent hyperemia and bleeding marks.
Figure 3.
Superior digestive endoscopy performed at 16 h after ingestion: (A-D) The esophagus exhibited patchy necrosis, ulceration, and sloughing; (E-F) The gastric mucosa displayed prominent hyperemia and bleeding marks.
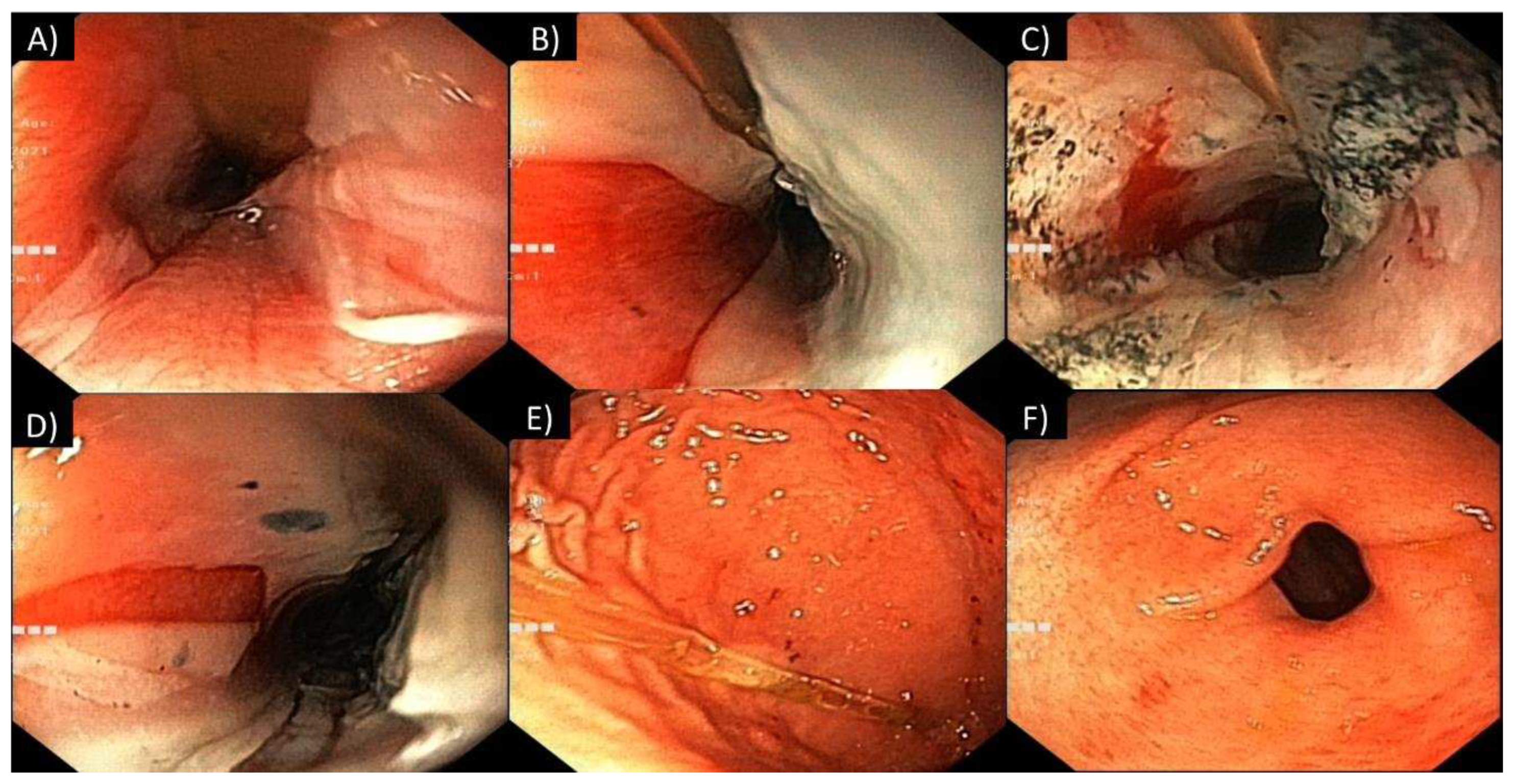
Figure 4.
Laboratory test results during the clinical course: (A) venous blood gas (VBG) analysis; (B) leukocyte count and inflammatory markers; and (C) creatine kinase level. Note: The VBG and creatine kinase levels are illustrated for the initial 12 days, up until the point of normalization. Abbreviations: BE, base excess; WBC, white blood cell count; CRP, C-reactive protein; CK, creatine kinase.
Figure 4.
Laboratory test results during the clinical course: (A) venous blood gas (VBG) analysis; (B) leukocyte count and inflammatory markers; and (C) creatine kinase level. Note: The VBG and creatine kinase levels are illustrated for the initial 12 days, up until the point of normalization. Abbreviations: BE, base excess; WBC, white blood cell count; CRP, C-reactive protein; CK, creatine kinase.
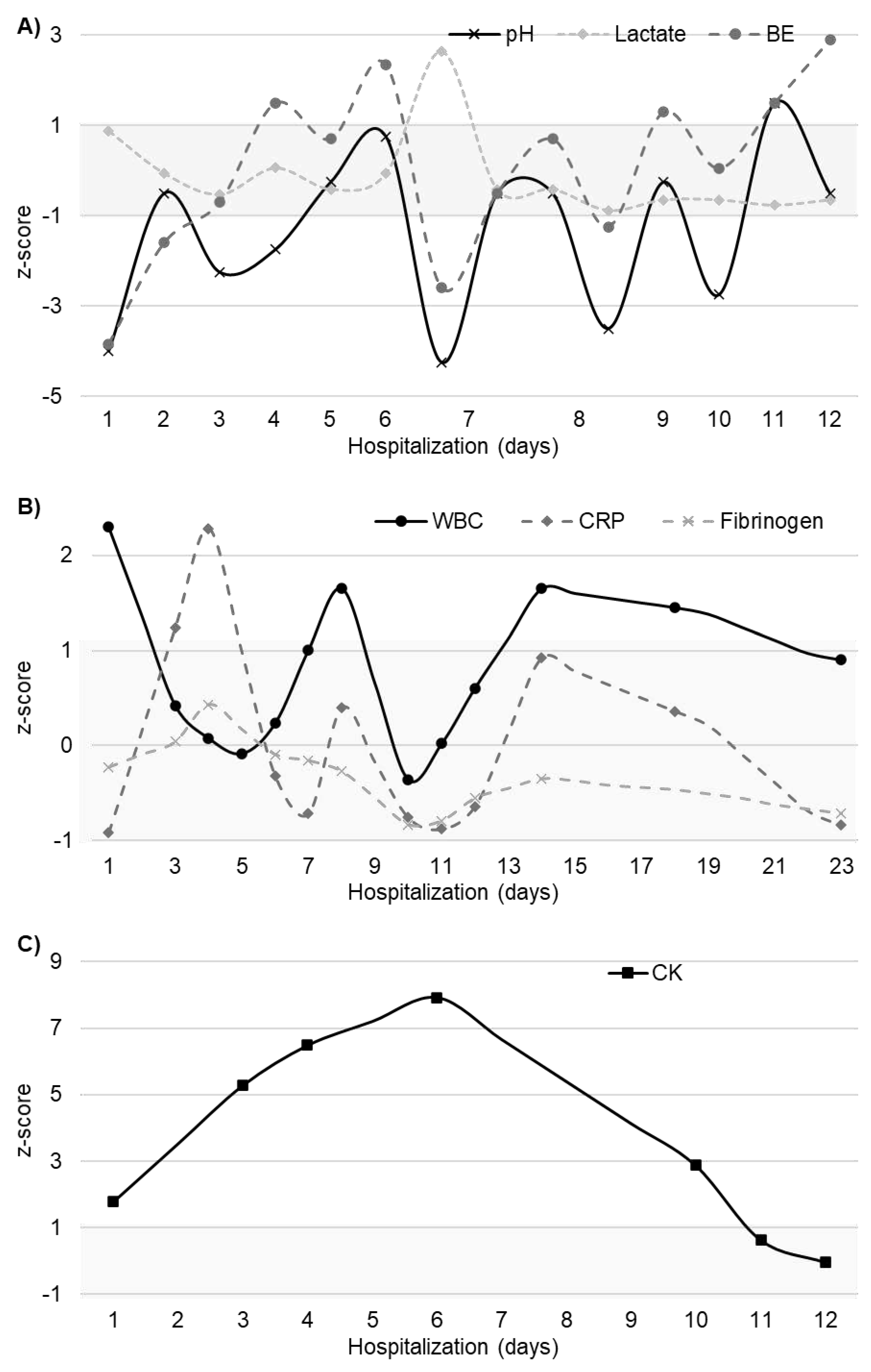
Figure 5.
Superior digestive endoscopy performed 21 days after ingestion showed resolution of corrosive lesions with persistence of (A) punctiform necrosis in the esophagus and (B-C) hyperemic gastric mucosa.
Figure 5.
Superior digestive endoscopy performed 21 days after ingestion showed resolution of corrosive lesions with persistence of (A) punctiform necrosis in the esophagus and (B-C) hyperemic gastric mucosa.


Table 1.
The composition and chemical-physical properties of the disinfectant at 20°C [17].
Table 1.
The composition and chemical-physical properties of the disinfectant at 20°C [17].
| Activeingredients: | 15.6% Cocos propylene diamine-guanidine diacetate |
| 35% Phenoxypropanols | |
| 2.5% Benzalkonium chloride | |
| pH: | 9.1—9.5 |
| Density: | 0.99 g/cm3 |
| Viscosity: | 30 mPa*s |
Abbreviations: °C, degree Celsius; g, gram; cm3, cubic centimeter; mPa, millipascal; s, second.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



