
Submitted:
06 January 2024
Posted:
08 January 2024
You are already at the latest version
Abstract
It is currently believed that the cause of superior mesenteric artery syndrome (SMAS) is compression of the duodenum in the angle between the aorta and superior mesenteric artery (SMA). It is recognized that a decrease in aortomesenteric angle (AMA) <25° and intervascular distance < 8 mm, caused by fat loss, is characteristic of SMAS. Based on these statements, surgeons operate on patients with symptoms of dyspepsia only based on a reduction of AMA. This study is devoted to the analysis of the literature, including four own studies on this issue. Results: Measurement of the length of the constriction in the third part of the duodenum on radiograms from available sources showed that its true length ranged from 2.5 to 4.2 (3.30±0.15) cm and began a few centimeters cranial to the AMA. Therefore, it could not have been caused by compression in the AMA. In terms of length (3.20±0.15 cm) and location, this constriction corresponded to Ochsner’s sphincter, which normally short-term contracts to prevent the penetration of an acid bolus into the jejunum. Conscientious studies have shown that AMA is proportional to BMI, i.e., a decrease in AMA is observed in all thin people. An analysis of 211 cases of SMAS made it possible to differentiate two types of diseases. In 101 patients, the disease occurred acutely 1–53 (8.2 ± 1.9) days after stressful situations, accompanied by a catabolic reaction and hypersecretion of hydrochloric acid. In 110 patients, SMAS developed 3-72 (17.2±3.2) months after the diagnosis of acid-dependent diseases. Conclusion: The analysis of the literature led to the conclusion that hypersecretion of hydrochloric acid causes damage to the upper level of the digestive system, including duodenal dyskinesia. One of the manifestations of duodenal dyskinesia is an increase in tone and hypertrophy of the Ochsner’s sphincter. The clinic of the disease depends on the varying degree of Ochsner’s sphincter dyskinesia. In severe cases, partial or complete intestinal obstruction. New ideas about the etiology and pathogenesis of the so-called SMAS have made it possible to propose a tactic for the diagnosis and treatment of Ochsner’s sphincter dyskinesia, where there is no place for surgical treatment.
Keywords:
Duodenal physiology
; superior mesenteric artery syndrome
; Ochsner's sphincter dyskinesia
; hydrochloric acid hypersecretion
; pathophysiology
1. Introduction
Currently, all authors of articles adhere to the hypothesis Professor Carl von Rokitansky (1842) that explains the presence of clinical and radiological symptoms of obstruction in the 3rd part of the duodenum, by its compression in the aortomesenteric angle (AMA). Therefore, this syndrome has received the name “Superior mesenteric artery syndrome” (SMAS). There are many contradictory statements in this hypothesis, which will be discussed below. To understand the pathological physiology of SMAS, it is necessary to focus on the normal physiology of the duodenum [1].
- Duodenal motility
In the duodenum, from the pyloric sphincter (PS) of the stomach to the duodenojejunal junction, four sphincters function, which protects the small intestine from the aggressive effects of hydrochloric acid. If the bolus would pass through the duodenum as quickly as through the esophagus, then an extremely low pH bolus would cause irritation of the jejunum or, at best, a dumping syndrome [2].
The post bulbar sphincter (PBS), together with the pyloric sphincter (PS), provides evacuation of the chyme from the stomach as portions of a certain volume (Figure 1A). When the acid bolus reaches the Ochsner’s sphincter, which is in the 3rd part of the duodenum, it causes of its contraction, which prevents entering aggressive chyme to the jejunum (Figure 1B). As a result of the Ochsner’s sphincter contraction, the bolus is thrown cranially, but Kapanji’s sphincter contraction, it is again thrown to the Ochsner’s sphincter. This pendulum movement of the bolus between the Ochsner and Kapanji sphincters occurs several times. During this time, the chyme mixes with bile and pancreatic juice, which raise the pH of the chyme. When the pH reaches a level that is safe for the jejunum, Ochsner’s sphincter opens, and bolus passes into the jejunum [1,3].
The motility of the Ochsner’s sphincter is a periodic change of contraction and relaxation, depending on the pH of the bolus. Normally, radiologists cannot see a contraction of the Ochsner Sphincter works because they use an acid-free contrast agent. I have done research adding 3g Vitamin C to 200 ml of barium. The acid caused Ochsner’s sphincter to contract and this made possible to determine and measure of its length. It turned out that in length (3.20 ± 0.15 cm) and location it corresponds to the length (3.30 ± 0.15 cm) (P > 0.2) and location of the narrowing of the duodenum in the so-called SMAS [3].
Ochsner described in detail the functional sphincter in the 3rd part of the duodenum in 1906. During gallbladder and stomach operations he found “in many cases, the duodenum is distended with gas to a point just below the entrance of the common duct, while below this it is contracted, and upon raising the transverse colon and finding the origin of the jejunum, this portion of the intestine will also be found in a contracted condition. In all these specimens, there is also a marked thickening of the intestinal wall at a point 2 to 4 centimeters below the entrance of the common duct, and a careful study of this thickening demonstrated the presence of a marked increase in the circular muscle fibers. These facts pointed towards the presence of a sphincter at this point whose physiological function would consist in providing for a means of retaining the chyme in the upper portion of the duodenum sufficiently long to provide for thorough mixing with bile and pancreatic fluid”. Ochsner believed that “under certain forms of irritation or inflammation of the gallbladder or ducts, this duodenal sphincter had taken up an action” [4]. The 12 out of 14 patients described by Ochsner were diagnosed with gastric ulcer (4), duodenal ulcer (2), cholecystitis (7), chronic appendicitis (5), pancreatitis (7). All patients had a dilated duodenum, and 6 of them had a gastric dilatation [4]. Kapanji’s sphincter and Ochsner’s sphincter are widely known in the scientific literature in French and Russian [5]. Oddi’s sphincter this is the only sphincter of the duodenum, which is described in the English-language literature. The pathology of this sphincter is closely related to the pathology of the bile and pancreatic ducts.
2. Analysis of the Vascular Hypothesis of the Pathogenesis of Smas
- 1.
- Analysis of radiological studies in the so-called SMAS
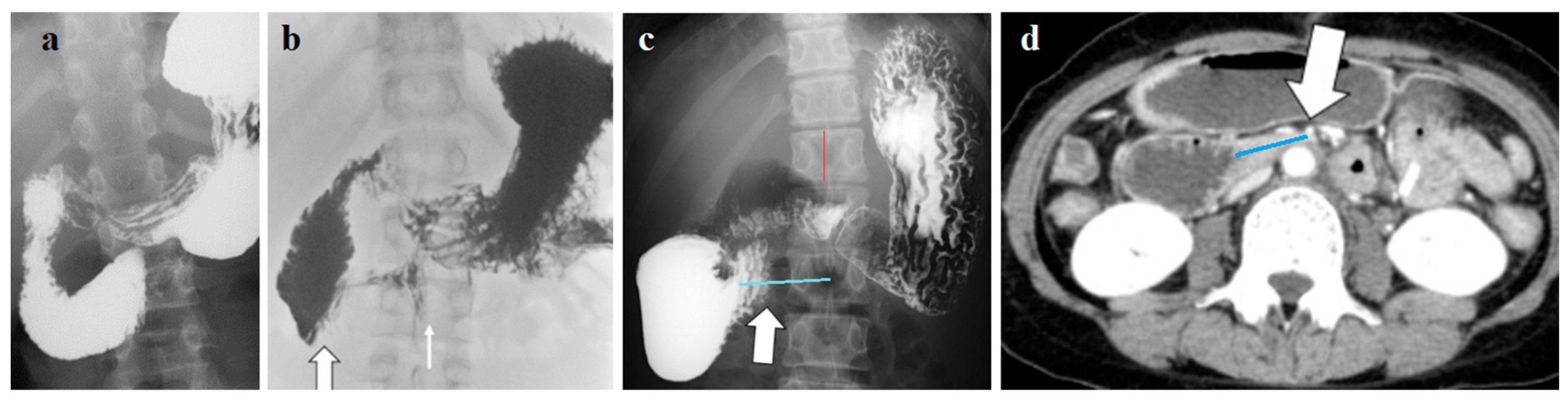
Ever since Professor Carl von Rokitansky (1842) advanced the vascular hypothesis it is believed that obstruction of the 3rd part of the duodenum is caused by intestinal compression in the aortomesenteric angle (AMA). The abdominal aorta is located near the middle of the vertebra (Figure 2a-b) Its width is approximately 2 cm, and the width of the superior mesenteric artery (SMA) is 0.5 cm. The length of the constriction that these vessels can create cannot exceed 1 cm. I measured the distance from proximal points the sharp contraction in the 3rd part of the duodenum to the location of the SMA, i.e., up to the middle of the 3rd lumbar vertebra (L-3) on 35 radiographs, CT, and MRI, published in PubMed and PMC. On radiographs, all the values are greater than the real ones. We calculated the true value by multiplying the value measured on the radiograph by the projection increase factor. It is equal to the ratio of the true height of the first lumbar vertebra (2.2 cm in adults) to the value of its image on the radiograph. When analyzing CT and MRI, the coefficient is equal to the ratio of the true diameter of the abdominal aorta (2 cm) to the value of its image on the scan. In 29 (83%) cases on X-ray examination or on CT and MRI, the length of the narrowed segment of the duodenum ranged from 2.5 to 4.6 cm (3.30 ± 0.15 cm) and always started a few centimeters to the right of L-3 (Figure 2a-d) [1,3,6,7].
Only in 6 (17%) of 35 cases where the length of the narrowed segment of the could be measured, it looked short, since the place of obstruction was near the midline of the vertebra and its length was within 1 cm. However, as seen in Figure 2 e, the narrowed segment of the duodenum can be located to the left of the midline of the vertebra, which is confirmed by Ochsner’s observations during surgery. Secondly, the X-ray can show the moment opening of the Ochsner’s sphincter, which happens when there is high pressure above it (Figure 3).
From the analysis of radiological studies, it follows that in all cases, the contraction of the Ochsner sphincter, and not the compression of the duodenum in the AMA, is the cause of the so called SMAS.
- 2.
- On the pathogenesis of the so-called SMAS
It is argued that the cause of the compression of the duodenum in the AMA is rapid weight loss and the disappearance of adipose tissue, which normally supposedly push the SMA away from the aorta [8]. This statement is hypothetical in nature, since, firstly, no evidence is provided to support this thesis. On the contrary, analysis of the literature does not support this claim. For example:
A) In a significant percentage of patients with SMAS, the mean body mass index (BMI) was within normal limits. In a series of 14 children, it was 21.3 kg/m² (range 13.3-30.4 kg/m²). The mean weight loss before diagnosis was 3.8 kg (range 0-20 kg). No weight loss was found in 50% of the patients [8].
B) Among patients with acute development of the disease, i.e., within 1 - 53 (8.2 ± 1.9) days, conservative treatment was successful after 2-59 (13.4 ± 2.9) days in 88.9% of patients. First, it is obvious that during this time the volume of adipose tissue in the AMA could not change significantly. Second, repeated CT after resolution of clinical symptoms did not reveal any changes in AMA [9].
С) If soft adipose tissue appears between the aorta and the SMA, then how does it can push forward the tense vessel and does not push away and squeeze more compliant duodenum?
- 3
- What does the AMA value indicate?
А) All authors, referring to the article by Neri et al. [10], believe that the AMA value less than 25 ° is an important diagnostic feature of SMAS. However, the study, to which everyone refers, was carried out with numerous violations that do not allow us to consider its results reliable, that is, scientific. Studies with the AMA <25 ° were initially selected. No justification for the choice of this figure is provided. There are no characteristics of 50 healthy subjects (control group). The authors did not measure AMA for persons with different BMIs. Therefore, they had no reason to report normal boundaries at all. «The US detected reduced angles <25 ° in 29 of the 950 subjects (3.05%). X-ray with barium (Figure 4a) revealed compression on the third segment of the duodenum in 28 of 29 patients during the symptomatic period and in nine of 29 during the symptom-free interval» [10]. On the radiograph (Figure 4a), which Neri et al presented as the most demonstrative of 29, there are no signs of obstruction because neither the stomach nor the duodenum is dilated. Therefore, this case does not have the main features of SMAS. Secondly, the narrowing on this x-ray, that begins to the right of the vertebra has nothing to do with AMA. It corresponds to the contraction of the Ochsner sphincter. This is confirmed by a similar observation by Eisenberg [11] (Figure 4b-c). Thus, this radiograph does not correspond to the concept of SMAS and as well as all the conclusions of the article by Neri et al it is a falsification of the facts for confirming the invented limit of the AMA norm - 25°. So, for example, it states: “The aortomesenteric angle is normally 25–60° {[2,3,6,7,10-12]} and the mean aortomesenteric distance of 10–28 mm {[1-3,6,7,10-12]}. Subjects presenting an angle <25° and aortomesenteric distance <8-10 mm may be affected by SMA syndrome” [10]. However, none of these references, AMA studies in healthy patients with different BMIs, like in the article by Neri et al., Moreover, most of the links are descriptions of isolated cases. It is an indicator of the quality of the article. This lie had to confirm the reliability of the proposed parameters of the norm.
B). Bhagirath Desai et al. did a prospective study of 100 patients who had undergone CT scans for various other complaints. A strong positive correlation was found between BMI and the angle between the aorta and SMA. With BMI increase, the angle also increases. In 25% of patients, these rates were less than the norm [12]. In third world countries, there are hundreds of millions of people with low BMI which does not increase the SMAS frequency. Thus, the AMA value depends only on the amount of fat in the body.
From the above it follows that: - (1) No one has researched the AMA value in healthy people of different ages and weights. (2) The value of AMA is proportional to BMI. 3) The statement that in AMA is <25° should be suspected of SMA, is the result of not conscientious research.
3. Clinical Analysis of 227 Cases of Smas
I have analyzed 79 articles from PubMed and PMC describing 227 cases of SMAS from 1990 to 2015. Based on clinical data, all patients were divided into 2 groups. The 1st group consisted of 101 patients aged 3 – 81 (25.8 ± 3.4) years. The obstruction of the duodenum appeared in them 1–53 (8.2±1.9) days after severe stressful events: complicated surgeries, burns, trauma, chemotherapy, etc. In 126 patients of the second group aged 17– 86 (36.7±2.2) years, including 8 patients with anorexia nervosa, the duodenal obstruction occurred after 3 -72 (17.2±3.2) months of the chronic diseases. Almost all these patients had acid related upper gastrointestinal tract diseases. It became apparent that two different processes can lead to the appearance of duodenal obstruction (Table 1).
1st group: Acute development of symptoms was in the stressful conditions, which in the catabolic stage are accompanied by significant weight loss. This is especially often observed in adolescents after surgery on the spine [6,7]. It is known that stress states are accompanied by a decrease in the pH of gastric 10 contents. In such cases, even high doses of proton pump inhibitors do not have an effect in improving gastric pH [13]. Conservative treatment in conditions of partial obstruction of the duodenum was successful in 89% of patients after 2-59 (13.4±2.9) days. Obviously, during this time, neither intravenous hyperalimentation, nor tube introduction of food into the small intestine could change either the total weight of patients or the volume of adipose tissue in the AMA. Moreover, after the restoration of patency in the duodenum, the distance between the vessels does not change [9]. Therefore, the positive effect of conservative treatment is not associated with an increase in adipose tissue in the AMA, which does not support the hypothesis of the role of AMA in the pathogenesis of SMAS.
2nd group: In patients of the 2nd group with functional dyspepsia, postprandial syndrome, and other peptic syndromes, the pathology is due to the hypersecretions of hydrochloric acid. They, in contrast to the patients in the 1st group, had a long history of the disease. Disturbance of the duodenal patency increased gradually: from slight disruption to complete obstruction. In these patients, as Ochsner showed, hypertrophy of the circular muscle layer of the third part of the duodenum distal to the sphincter of Oddi occurs. This may be the reason for the lower effectiveness of the short-term conservative treatment in patients of the 2nd group. As can be seen from Table 1, surgeons operated the patients of the 2nd group, only based on a decrease in AMA (<25), or the distance between the aorta and SMA (< 8 mm). In 47% of cases, the operation was performed without attempting conservative treatment. Conservative treatment was successful in 39% of cases, and in 14% of cases conservative treatment was short-term and ineffective. These patients were operated on. Thus, 61% of patients with peptic problems accompanied by duodenal dyskinesia were operated on only because they were thin or had no effect after short-term non-pathogenic conservative treatment.
4. What does the AMA angle depend on?
This question is very important, since another, even more improbable hypothesis about the role of adipose tissue in AMA has been proposed to support the vascular hypothesis. The diagram (Figure 5c,d) shows the principle of this hypothesis. SMAS supposedly arises from the loss of adipose tissue in the AMA, which leads to compression of the duodenum, which passes through this angle. From this follows the principle of SMAS treatment, i.e., hyperalimentation, to increase the volume of adipose tissue and push the SMA anteriorly and thus make room for the duodenum. This hypothesis is rejected by the following evidence. 1) An increase in soft adipose tissue in the AMA cannot push back a tense vessel. 2) An additional volume of adipose tissue competes with the duodenum for space in the AMA, i.e., it can increase its compression. 3) Hyperalimentation can lead to an increase in adipose tissue only with a simultaneous increase in fat throughout the body. This means that for enough fat to appear in the AMA, the patient must gain tens of kilograms. This cannot be done not only in a few days, but also in many months, especially since we are talking about a violation of the patency of the duodenum. Figure 5a,b,E provides further evidence that “when BMI of a patient decreases, there is a corresponding reduction in SMA angle and distance» [14,12].
5. Etiology, pathogenesis, diagnosis, and treatment of Ochsner`s sphincter dyskinesia.
The above evidence leads to the following conclusions:
1. The zone of contraction in the 3rd part of the duodenum with a length of 2.5-4.6 (3.30 ± 0.15) cm cannot be caused by compression of the intestine in the AMA, firstly, because between the aorta with a diameter of 2 cm and the SMA with a diameter of 0.5 cm, the length of the compressed intestine cannot be more than 1 cm. Secondly, the beginning of the contracted segment of the duodenum is a few centimeters cranial to the AMA. In length (3.2 ± 0.15 cm) and localization, the contracted segment of the duodenum corresponds to the sphincter Ochsner, which normally contracts to prevent an aggressive low pH bolus from entering the small intestine. A prolonged contraction of the sphincter Ochsner, which disrupts the passage into the jejunum, indicates its dyskinesia.
2. Article 8. Neri et al. [8], identifying AMA < 25° and distance between aorta and SMA < 8 mm as proof of SMAS is based on false information and is untrue. These parameters are proportional to BMI. Surgeons relying on these parameters operate on patients with dyspepsia, duodenitis or duodenal ulcer without signs of obstruction. They produce a bypass duodenojejunostomy, because of which the aggressive chyme immediately from the stomach enters the jejunum, which inevitably leads to chronic enteritis.
3. The notion that the cause of SMAS is the loss of adipose tissue in the AMA and hyperalimentation over several weeks can lead to fat accumulation in AMA and to recovery does not withstand scientific scrutiny.
- Etiology
Hypersecretion of hydrochloric acid provokes by the food ingredients. These provocateurs or stimuli includes delayed-onset diseases, that can be mediated by intestinal mucosal mechanisms involving not only IgE but also T cells, mast cells and eosinophils that produce proinflammatory mediators. Belong of this kind of disease: atopic dermatitis, celiac disease, or eosinophilic GI diseases, such as esophagitis, gastritis, gastroenteritis, enterocolitis and proctitis” [15]. It turned out that under stress “mast cells (MC) are important effectors of brain-gut axis that translate the stress signals into the release of a wide range of neurotransmitters and proinflammatory cytokines, which may profoundly affect the gastrointestinal physiology” [16]. In both cases, one of the end products is acid hypersecretion. The lactose is the most common provocateur of hydrochloric acid hypersecretion [17]. It causes the release of histamine from mast cells, which, through a chain of mediators, leads to the hypersecretion of hydrochloric acid. There are patients with histamine intolerance [18] and others. Probably, in most cases, the hypersecretion of hydrochloric acid can be the cause of all acid-dependent diseases (esophagitis, GERD, stomach ulcer and gastritis, duodenal ulcer and duodenitis, sphincter of Oddi dyskinesia and cholecystitis, as well as SMAS). As a rule, one of these problems, to a greater or lesser extent, are present in every patient with Ochsner’s sphincter dyskinesia.
- 2.
- Pathogenesis
Prolonged duodenal irritation with low pH hydrochloric acid causes an increase in the tone of Ochsner’s sphincter, which gradually leads to wall hypertrophy, as Ochsner saw during the operation. If normally a fleeting contraction of the sphincter Ochsner is recorded as a pendulum movement of the bolus, then with dyskinesia, a narrowing of the intestine is clearly recorded. However, it is necessary to distinguish between the contraction of the sphincter Ochsner without disturbing the bolus evacuation into the jejunum with obstruction of the duodenum, which is characterized by the expansion of the stomach and duodenum and is accompanied by vomiting.
- 3.
- Diagnosis
As shown above, the magnitude of the AMA and the distance between the aorta and the SMA are proportional to the BMI. This means that a decrease in these parameters only indicates the thinness of patients. Therefore, their definition on CT, MRI and US does not make any sense. Two clinical conditions must be distinguished: (a) For symptoms of intestinal obstruction that are accompanied by recurring vomiting, a radiography is shown to determine the size of the stomach and duodenum. (b) Abdominal pain, weight loss, and other symptoms of acid-related disease require a barium x-ray. If sphincter Ochsner dyskinesia is detected, gastroscopy should be the next step to rule out tumor, peptic stenosis, and other acid-related disorders.
- 4.
- Treatment
Based on our hypothesis, dyskinesia of the sphincter Ochsner is caused by hypersecretion of hydrochloric acid and the pathogenetic treatment should be aimed at the reducing of the hydrochloric acid release and removing it from the duodenum. As the literature analysis has shown, the most effective are nasogastric decompression with nasojejunal feeding. In patients without obstruction of the duodenum, the use of PPI 40 mg twice a day for 4 weeks is justified. In patients with obstruction of the duodenum the high-dose PPI therapy (intravenous loading dose followed by continuous infusion) [19,20] until the sphincter Ochsner is fully opened, followed by a transition to oral PPI reception. The duodenal irrigation with alkaline solution is theoretically justified. In the absence of the effect of drug treatment to relieve spasm of the sphincter Ochsner, the use of Botox injections is justified. With sphincter Ochsner dyskinesia, there is no place for surgical treatment.
6. Discussion
New things in science begin with an assumption that does not contradict reliable scientific facts. If subsequent scientific research confirms a hypothesis, it becomes a theory. But if at least one irrefutable scientific fact contradicts the hypothesis, it should be rejected as untenable. In 1842 Prof. Carl von Rokitansky suggested that acquired duodenal obstruction occurs because of compression of the intestine in the AMA. Numerous scientific facts presented in this article prove the fallacy of this hypothesis. Based on an analysis of the literature, we propose two hypotheses. Firstly, the clinical picture and pathogenesis of the disease are the result of duodenal dyskinesia. Secondly, duodenal dyskinesia occurs because of hypersecretion of hydrochloric acid.
Kim et al did not use CT and MRI to diagnose SMAS. They performed UGI series or hypotonic duodenography to confirm SMAS. Based on radiography, all cases were divided into 2 groups: with SMAS and without SMAS. The three most common presenting symptoms were abdominal pain, postprandial discomfort, and early satiety. Weight loss was noted in 38.9 and 18.2% in group I and II, respectively. Less common were vomiting and nausea, which occurred with equal frequency in both groups. The endoscopic suspicion of SMAS was a constellation of three findings: (1) pulsating vertical or oblique band or slit like luminal narrowing of the third part of the duodenum with luminal expansion no more than one third during air insufflation over 15 s, (2) proximal duodenal over distension during air insufflation, (3) bile lakes in the stomach. The authors diagnosed SMAS based on the following radiological signs: (1) gastroduodenal dilatation with delayed gastric and duodenal emptying, (2) abrupt vertical or oblique cutoff of contrast shadow at the third part of the duodenum (3) 'to and fro' flow of contrast from the proximal to the obstruction [21].
The clinical picture in both groups is fully consistent with peptic disease, which is caused by hypersecretion of hydrochloric acid. Endoscopic symptoms correspond to duodenal dyskinesia. Firstly, because each of these signs was found in the group without SMAS. Secondly, the pulsating vertical or oblique band is clearly visible in thin children, because the duodenum passes between the pulsating vessels. The Ochsner sphincter cannot be visualized during endoscopy, since endoscope is easily passed through the sphincter, which opens when insufflated with air. Proximal duodenal over distension during air insufflation, as shown above and described by Ochsner, is a sign of duodenal dyskinesia. Bile lakes in the stomach are the result of duodenogastric reflux [22] due to dyskinesia of the duodenal sphincters. The radiological criteria of the SMAS, described by the authors are typical signs of duodenal dyskinesia: 1) gastroduodenal dilatation with delayed gastric and duodenal emptying is absent in the typical example of SMAS presented by the authors (Figure 6a), (2) abrupt vertical or oblique cutoff of contrast shadow at the third part of the duodenum is due to contraction Ochsner's sphincter, (3) 'to and fro' flow of contrast between Ochsner's and Kapandji's sphincters is also known as pendulum-like movement of contrast agent, is normal reaction to acid. In none of the described observations was there a sharp dilation of the stomach and duodenum with a clinical picture of intestinal obstruction. An analysis of the article by Kim et al shows that the authors examined patients with hypersecretion of hydrochloric acid with special attention to the condition of the duodenum. Ignoring the clinical symptoms, in mild cases they called them “without SMAS”, and in more severe cases of duodenum dyskinesia they called them “with SMAS”.
Caterine et al retrospectively evaluated radiographs of patients with weight loss, reflux, and dysphagia. They believed that a radiological conclusion about SMAS is possible with a combination of three criteria (1) dilation of the first and second parts of the duodenum; (2) abrupt vertical or oblique mid-to-left of midline compression of the third part of the duodenum; and (3) “to-and-fro” flow of contrast proximal to the compression. The authors believe that radiological signs are often incorrectly assessed due to an anatomic impression by the inferior vena cava to the right-of-midline. There were 5 patients who had a clinical diagnosis of SMAS which was identified in their patient notes. None of the patients with a clinical diagnosis of SMAS radiological criteria for SMAS. All five patients had a right-of midline duodenal impression, and not where the superior mesenteric artery is located (Figure 6b).
On radiographs of four patients with peptic symptoms, signs were found that do not occur normally: (1) dilation of the first and second parts of the duodenum; (2) abrupt vertical or oblique narrowing of the third part of the duodenum; and (3) “to-and-fro” flow of contrast proximal to the narrowing. These signs indicate prolonged exposure to hydrochloric acid. Normally, a contrast agent without acid does not cause these symptoms. The authors call this picture normal, despite other typical symptoms of gastritis, duodenitis and gastroesophageal reflux. If there is no SMAS, this does not mean that you can neglect the obvious signs of the disease. The above radiological signs are evidence of peptic pathology, i.e., hypersecretion of hydrochloric acid. Caterine et al [23], as well as Dross et al [24], believe that a diagnosis of SMAS is not supported by impression found to the right of the vertebral bodies. They suggest calling such cases “superior mesentery artery-like syndrome,” which is supposedly caused by compression by other vessels. They diagnose SMAS only when there is a compression of the intestine to the mid-to-left of the spine. These statements require detailed analysis. It is an obvious fact that the narrowing of the duodenum, which begins on the right at a considerable distance from the location of the AMA, cannot be caused by compression of the intestine in the AMA. Therefore, in such cases, narrowing of the aortomesenteric space has no significance, as evidenced by the refusal of these authors to use CT and MRI as diagnostic procedures. Therefore, according to the same principle, narrowing of the intestine near other vessels has the same negative diagnostic value. Secondly, the length of the narrowing in the intestine to the right of the spine is on average 3.30 ± 0.15 cm, which cannot be caused by any vessel. Thirdly, if the clinic appears over the age of 80 [24], then it is obvious that other reasons caused these symptoms. On the other hand, the claim that the presence of a narrowing in the center of L-3 or to the left of it is evidence of SMAS is not supported by research. The narrowing of the intestine may begin to the right of the vertebra and end to the left of it (see Figure 2d,c,e and Figure 4a). Its length cannot in any way be caused by compression in the AMA. Ochsner's observations also showed that the narrowing of the intestine, which had all the signs of a sphincter, was sometimes located to the left of the vertebra [2]. Unfortunately, despite the obvious facts that the distance between the beginning of the narrowing of the duodenum and the AMA is not related to SMAS, some authors continue to diagnose and operate on patients based on false hypotheses. An example is the article by Oka et al [25] (Figure 6c,d).
Figure 6.
Radiographs of the stomach and duodenum in patients with peptic symptoms. (a). X-ray from the article by Kim et al with a conclusion about SMAS [21]. Although the proximal part of the contracted Ochsner sphincter is in the middle of L-3, the stomach and proximal part of the duodenum are not dilated, indicating sufficient cross-country ability of the duodenum. (b). X-ray from an article by Caterine et al with a clinical diagnosis of SMAS [23]. However, the long, narrow section of bowel to the right of the spine cannot be caused by compression of the SMA. The stomach and duodenum are not dilated and there are typical radiological signs of gastritis and duodenitis. (c-d). Studies from the article by Oka et al [25] supposedly confirm the diagnosis of SMAS. (с). On the radiograph, the intestine begins to contract 3.5 cm to the right of the AMA (blue line). (d). In the axial view of CT, the length of the contracted portion of the duodenum is 4.5 cm (blue line) to the right of the AMA.
Figure 6.
Radiographs of the stomach and duodenum in patients with peptic symptoms. (a). X-ray from the article by Kim et al with a conclusion about SMAS [21]. Although the proximal part of the contracted Ochsner sphincter is in the middle of L-3, the stomach and proximal part of the duodenum are not dilated, indicating sufficient cross-country ability of the duodenum. (b). X-ray from an article by Caterine et al with a clinical diagnosis of SMAS [23]. However, the long, narrow section of bowel to the right of the spine cannot be caused by compression of the SMA. The stomach and duodenum are not dilated and there are typical radiological signs of gastritis and duodenitis. (c-d). Studies from the article by Oka et al [25] supposedly confirm the diagnosis of SMAS. (с). On the radiograph, the intestine begins to contract 3.5 cm to the right of the AMA (blue line). (d). In the axial view of CT, the length of the contracted portion of the duodenum is 4.5 cm (blue line) to the right of the AMA.
7. Conclusions
The analysis of the literature led to the conclusion that hypersecretion of hydrochloric acid causes damage to the upper level of the digestive system, including duodenal dyskinesia. One of the manifestations of duodenal dyskinesia is an increase in tone and hypertrophy of the Ochsner’s sphincter. The clinic of the disease depends on the varying degree of Ochsner’s sphincter dyskinesia. In severe cases, partial or complete intestinal obstruction. New ideas about the etiology and pathogenesis of the so-called SMAS have made it possible to propose a tactic for the diagnosis and treatment of Ochsner’s sphincter dyskinesia, where there is no place for surgical treatment.
References
- van Beek, A.P.; Emous, M.; Laville, M.; JTack, J. Dumping syndrome after esophageal, gastric or bariatric surgery: pathophysiology, diagnosis, and management. Obes Rev. 2017, 18, 68–85. [Google Scholar] [CrossRef]
- Ochsner, A.J., VIII. Construction of the Duodenum Below the Entrance of the Common Duct and Its Relation to Disease. Ann Surg. 1906, 43, 80–87. [Google Scholar] [CrossRef]
- Aldot, G.; Kapandji, M.; Ringendach, J. Physiology of timed duodenal intubation. II. Role of Ochsner's sphincter in the mechanism of normal duodenal intubation and in that of certain prolongations of so-called 13 Oddi's closed time. Arch Mal Appar Dig Mal Nutr. 1956, 45, 449–457. [Google Scholar]
- Levin, M.D.; Korshun, Z.; Mendelson, G. [Duodenal motility in norm and in some diseases. Hypothesis]. Ter Arkh. 2016, 88, 68–74. [Google Scholar] [CrossRef]
- Levin, M.D. Ochsner's Sphincter Dyskinesia Is the Cause of Superior Mesenteric Artery Syndrome. J Gastrointest Surg. 2019, 23, 1714–1716. [Google Scholar] [CrossRef]
- Levin, M.D. Sphincter Ochsner dyskinesia as a cause of superior mesenteric artery syndrome. Review. Vestn Rentgenol Radiol. 2016, 97, 110–117. [Google Scholar] [CrossRef]
- Levin, M.D. PATHOGENETIC SIGNIFICANCE OF DYSKINESIA OF THE SPHINCTER OF OKSNER IN THE DEVELOPMENT OF THE SYNDROME OF THE SUPERIOR MESENTERIC ARTERY. Review. Eksp Klin Gastroenterol. 2016, 12, 67–72. [Google Scholar]
- Biank, V.; Werlin, S. Superior mesenteric artery syndrome in children: a 20- year experience. J Pediatr Gastroenterol Nutr. 2006, 42, 522–525. [Google Scholar] [CrossRef]
- Santer, R.; CYoung, C.; Rossi, T.; Riddlesberger, M.M. Computed tomography in superior mesenteric artery syndrome. Pediatr Radiol. 1991, 21, 154–155. [Google Scholar] [CrossRef] [PubMed]
- Neri, S.; Signorelli, S.S.; Mondati, E.; et al. Ultrasound imaging in diagnosis of superior mesenteric artery syndrome. J Intern Med. 2005, 257, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Diagnostic imaging in internal medicine. By R.L. Eisenberg. Copyright © 1985 by McGraw-Hill, Inc. p.694.
- Bhagirath Desai, A.; Sandeep Shah, D.; Jagat Bhatt, C.; et al. Measurement of the Distance and Angle Between the Aorta and Superior Mesenteric Artery on CTScan: Values in Indian Population in Different B MI Categories. Indian J Surg. 2015, 77 (Suppl 2), 614–617. [Google Scholar] [CrossRef] [PubMed]
- Alzerwi, N.A.N. Predictors of Superior Mesenteric Artery Syndrome: Evidence from a Case-Control Study. Cureus. 2020, 12, e9715. [Google Scholar] [CrossRef] [PubMed]
- Lenz, K.1.; Buder, R.; Firlinger, F.; Lohr, G.; Voglmayr, M. Effect of proton pump inhibitors on gastric pH in patients exposed to severe stress. Wien Klin Wochenschr. 2014, 127, 51–56. [Google Scholar] [CrossRef]
- Cuomo, R.; Andreozzi, P.; Zito, F.P.; et al. Irritable bowel syndrome and food interaction. World J Gastroenterol. 2014, 20, 8837–8845. [Google Scholar] [CrossRef] [PubMed]
- Konturek, P.C.; Brzozowski, T.; Konturek, S.J. Stress and the gut: pathophysiology, clinical consequences, diagnostic approach and treatment options. J Physiol Pharmacol. 2011, 62, 591–599. [Google Scholar]
- Minenna, M.F.; Palieri, A.; Panella, C.; Ierardi, E. Gastro-oesophageal reflux disease and lactose malabsorption: Casual comorbidity or neglected association? Dig Liver Dis. 2006, 38, 437–438. [Google Scholar] [CrossRef]
- Comas-Basté, O.; Sánchez-Pérez, S.; Veciana-Nogués, M.T.; et al. Histamine Intolerance: The Current State of the Art. Biomolecules. 2020, 10, 1181. [Google Scholar] [CrossRef] [PubMed]
- Barkun, A.N.; Almadi, M.; Kuipers, E.J.; et al. Management of Nonvariceal Upper Gastrointestinal Bleeding: Guideline Recommendations From the International Consensus Group. Ann Intern Med. 2019, 171, 805–822. [Google Scholar] [CrossRef] [PubMed]
- Pang, S.H.; Graham, D.Y. A clinical guide to using intravenous proton-pump inhibitors in reflux and peptic ulcers. Therap Adv Gastroenterol. 2010, 3, 11–22. [Google Scholar] [CrossRef]
- Kim, J.Y.; Shin, M.S.; Lee, S. Endoscopic features for early decision to evaluate superior mesenteric artery syndrome in children. BMC Pediatr. 2021, 21, 392. [Google Scholar] [CrossRef]
- Livzan, M.A.; Mozgovoi, S.I.; Gaus, O.V.; Bordin, D.S.; Kononov, A.V. Diagnostic Principles for Chronic Gastritis Associated with Duodenogastric Reflux. Diagnostics (Basel). 2023, 13, 186. [Google Scholar] [CrossRef] [PubMed]
- Caterine, S.; Patil, N.S.; Takrouri, H.; Issenman, R.M.; Stein, N.R.; Donnellan, J.; Yikilmaz, A. Understanding the diagnosis of superior mesenteric artery syndrome: analysis of the location of duodenal impression on upper gastrointestinal studies. Pediatr Radiol. 2023, 53, 2633–2641. [Google Scholar] [CrossRef] [PubMed]
- Dross, P.E.; Shawdon Molavi, S.; Alex Chan, A.; Latshaw, R.; Chhabra, P. Unusual Etiologies for Vascular Duodenal Compression Mimicking the Superior Mesenteric Artery (SMA) Syndrome: The SMA-Like Syndrome. J Gastrointestinal Abdominal Radiol ISGAR 2019, 2, 140–146. [Google Scholar] [CrossRef]
- Oka, A.; Awoniyi, M.; Hasegawa, N.; Yoshida, Y.; Tobita, H.; Ishimura, N.; Ishihara, S. Superior mesenteric artery syndrome: Diagnosis and management. World J Clin Cases. 2023, 11, 3369–3384. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
X-ray demonstration of the duodenal sphincters. (A). During antral contraction, the duodenal bulb fills to the limit, after which the pyloric sphincter (PS) contracts, stopping the flow of barium from the stomach into the bulb. Then, during the peristaltic contraction of the bulb between the PS and PBS, the pressure rises, which causes the PBS to relax, and the bolus penetrates the 2nd part of the duodenum. (B) In elderly patient with duodenal dyskinesia the white arrow shows PBS location. An expansion of the duodenum is determined between the Kapanji’s sphincter (pink arrow) and the Ochsner’s sphincter (blue arrow). (C) The duodenum was emptied, but the barium remained in deep folds because the barium-filled bowel was very wide. Two zones of contraction with longitudinal folds are visible: (a) the Kapanji’s sphincter, and (b) the Ochsner’s sphincter. The juxtapapillary diverticulum (d) is located between them. These diverticula result from the extrusion of the mucosa between the muscular fibers. Thus, this diverticulum is evidence of high pressure that occurs between contracted sphincters Kipunji and Ochsner.
Figure 1.
X-ray demonstration of the duodenal sphincters. (A). During antral contraction, the duodenal bulb fills to the limit, after which the pyloric sphincter (PS) contracts, stopping the flow of barium from the stomach into the bulb. Then, during the peristaltic contraction of the bulb between the PS and PBS, the pressure rises, which causes the PBS to relax, and the bolus penetrates the 2nd part of the duodenum. (B) In elderly patient with duodenal dyskinesia the white arrow shows PBS location. An expansion of the duodenum is determined between the Kapanji’s sphincter (pink arrow) and the Ochsner’s sphincter (blue arrow). (C) The duodenum was emptied, but the barium remained in deep folds because the barium-filled bowel was very wide. Two zones of contraction with longitudinal folds are visible: (a) the Kapanji’s sphincter, and (b) the Ochsner’s sphincter. The juxtapapillary diverticulum (d) is located between them. These diverticula result from the extrusion of the mucosa between the muscular fibers. Thus, this diverticulum is evidence of high pressure that occurs between contracted sphincters Kipunji and Ochsner.
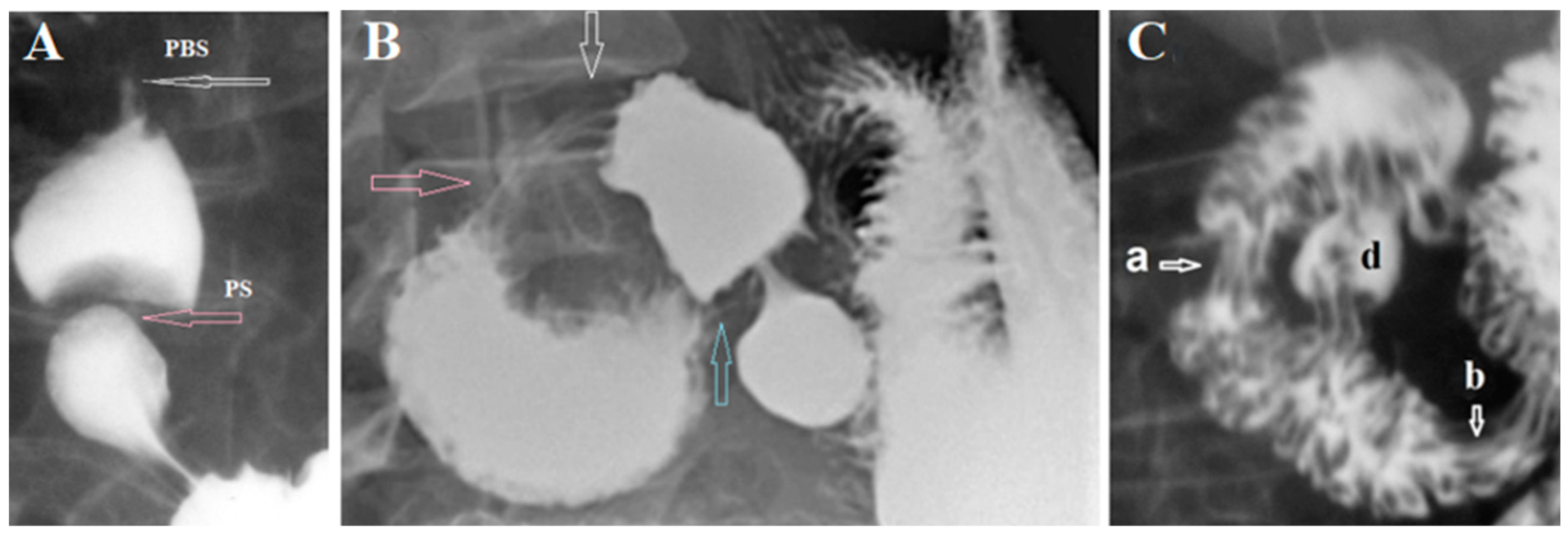
Figure 2.
X-ray examinations of patients with a “diagnosis” of SMAS. (a) A patient after laparotomy. The beginning of the narrowed segment of the duodenum (blue line) is located 3.2 cm from the midline L-3. His CT (b) shows that the narrowed segment is located far from the AMA (red line). (c) In a patient with a bulb ulcer (black arrow), the narrowed segment of the duodenum begins to the right of L-3 (white arrow) and ends to the left of L-3. Its length is 4.6 cm. (d) The distance from the duodenum to the jejunum is 6.5 cm. (e) In this patient the narrowed segment of the duodenum begins to the right of L-4 and ends to the left of the midline of L-3. Its length is 4.9 cm.
Figure 2.
X-ray examinations of patients with a “diagnosis” of SMAS. (a) A patient after laparotomy. The beginning of the narrowed segment of the duodenum (blue line) is located 3.2 cm from the midline L-3. His CT (b) shows that the narrowed segment is located far from the AMA (red line). (c) In a patient with a bulb ulcer (black arrow), the narrowed segment of the duodenum begins to the right of L-3 (white arrow) and ends to the left of L-3. Its length is 4.6 cm. (d) The distance from the duodenum to the jejunum is 6.5 cm. (e) In this patient the narrowed segment of the duodenum begins to the right of L-4 and ends to the left of the midline of L-3. Its length is 4.9 cm.
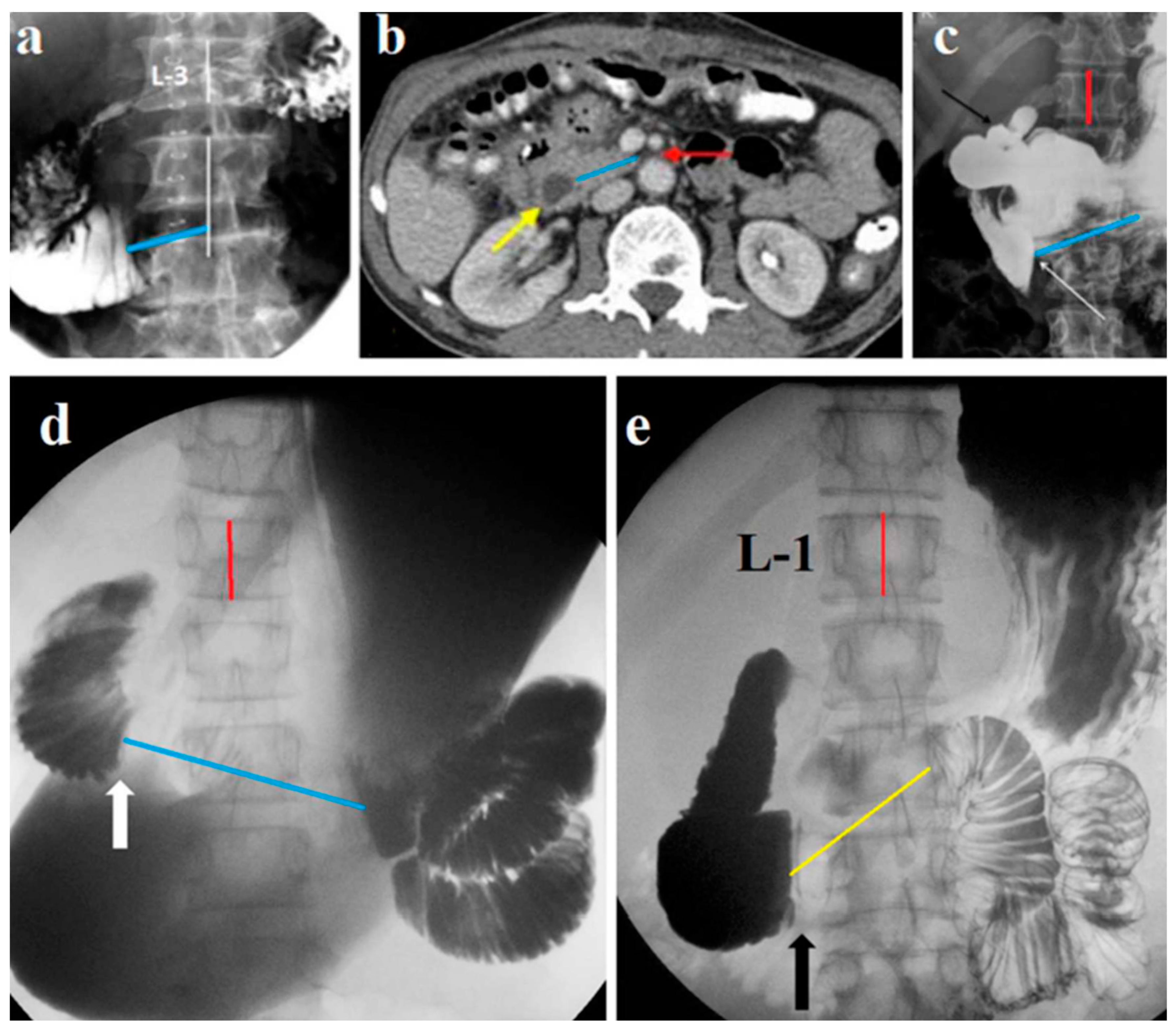
Figure 3.
MRI of a patient with SMAS and its scheme. The second part of the rectum is expanded to 4 cm. Deep fixed folds in the third part of the duodenum indicate rigid duodenitis. This picture, resembling a hedgehog, was the same in three patients. The moment of opening of Ochsner’s sphincter was probably recorded at high pressure in the expanded duodenum above it.
Figure 3.
MRI of a patient with SMAS and its scheme. The second part of the rectum is expanded to 4 cm. Deep fixed folds in the third part of the duodenum indicate rigid duodenitis. This picture, resembling a hedgehog, was the same in three patients. The moment of opening of Ochsner’s sphincter was probably recorded at high pressure in the expanded duodenum above it.
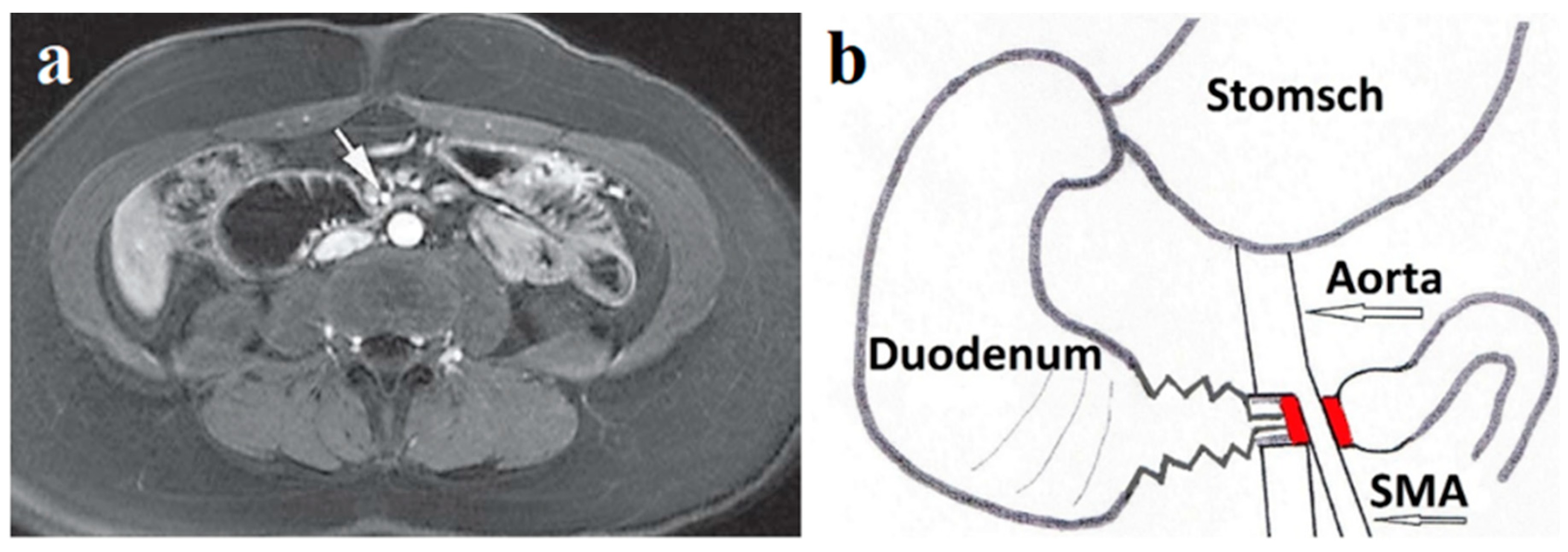
Figure 4.
(a) Radiograph from the article Neri et al [10]. There is no enlargement of the stomach and duodenum. Temporary stop in the passage of barium arose to the right of the spine. Contraction of the Ochsner sphincter (o) and Kapandji sphincter (white arrow) indicates duodenal dyskinesia. (b, c) Radiographs from the textbook. Signed: “Normal patient with transient proximal duodenal dilatation (b) Radiograph shows apparent obstruction third portion of the duodenum (arrow) suggesting the SMAS. (c) The view obtained slightly later shows the duodenal sweep to be entirely normal” [11].
Figure 4.
(a) Radiograph from the article Neri et al [10]. There is no enlargement of the stomach and duodenum. Temporary stop in the passage of barium arose to the right of the spine. Contraction of the Ochsner sphincter (o) and Kapandji sphincter (white arrow) indicates duodenal dyskinesia. (b, c) Radiographs from the textbook. Signed: “Normal patient with transient proximal duodenal dilatation (b) Radiograph shows apparent obstruction third portion of the duodenum (arrow) suggesting the SMAS. (c) The view obtained slightly later shows the duodenal sweep to be entirely normal” [11].
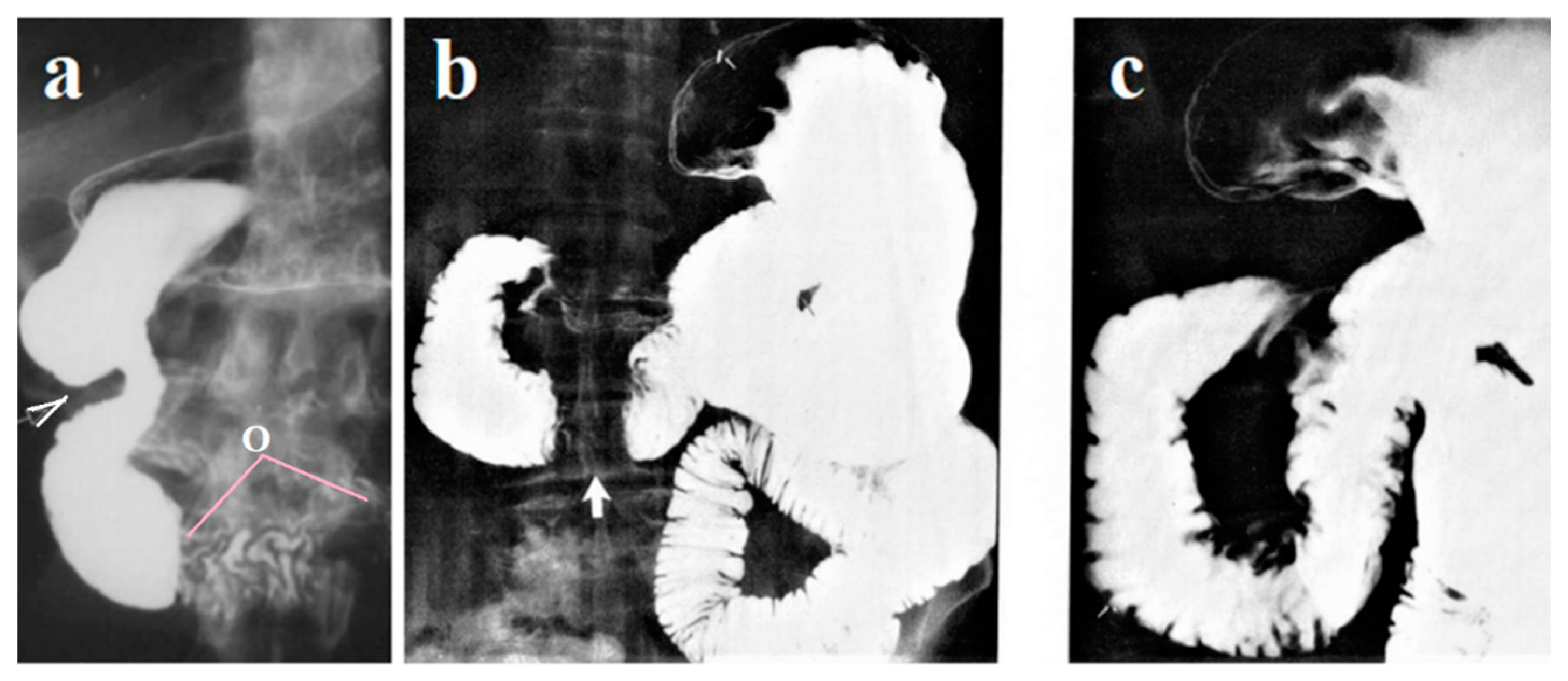
Figure 5.
Central sagittal scans (CT). The true height of the 1st lumbar vertebra (red line) is 2.2 cm. (a) In a patient with SMAS, the greatest distance from the anterior abdominal wall to the spine is 8 cm (blue). (b) A patient with SMA thrombosis (red arrow) has a large volume of adipose tissue pushed the anterior wall and colon forward to 13.2 cm (8 cm- blue +5, 2 cm- white). The SMA that supplies blood to the colon together with the colon and mesentery is pushed forward, which leads to an increase in AMA (yellow angle). (c, d) Scheme of the generally accepted hypothesis of the pathogenesis of SMAS, which contradicts physical laws. (E) Scheme of the increase in AMA because of the forward displacement of the SMA along with the intestine and its mesentery due to the large volume of fat in the abdominal cavity.
Figure 5.
Central sagittal scans (CT). The true height of the 1st lumbar vertebra (red line) is 2.2 cm. (a) In a patient with SMAS, the greatest distance from the anterior abdominal wall to the spine is 8 cm (blue). (b) A patient with SMA thrombosis (red arrow) has a large volume of adipose tissue pushed the anterior wall and colon forward to 13.2 cm (8 cm- blue +5, 2 cm- white). The SMA that supplies blood to the colon together with the colon and mesentery is pushed forward, which leads to an increase in AMA (yellow angle). (c, d) Scheme of the generally accepted hypothesis of the pathogenesis of SMAS, which contradicts physical laws. (E) Scheme of the increase in AMA because of the forward displacement of the SMA along with the intestine and its mesentery due to the large volume of fat in the abdominal cavity.
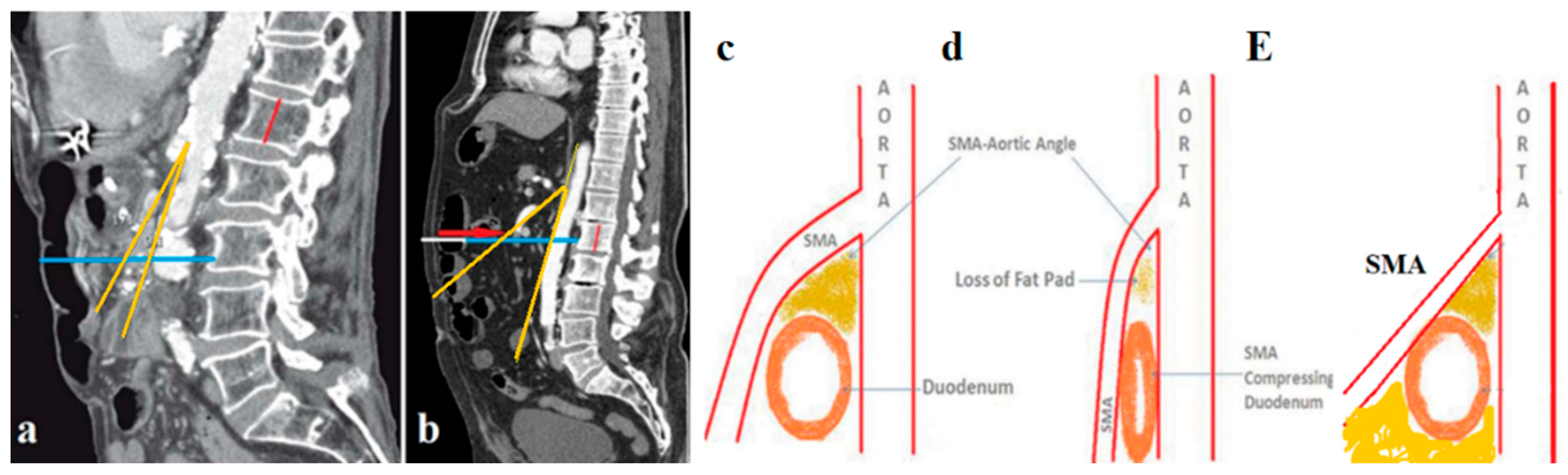

Table 1.
Distribution of the patients with SMAS depending on the duration of the disease. .
| Groups | Number of patients | Age (years) |
M/W | Duration of The disease |
Weight loss (kg) | BMI | Conservative treatment |
Treatment time (days) | Surgery without Conservative treatment |
|---|---|---|---|---|---|---|---|---|---|
| 1st group | 101 | 3-81 25.8±3.4 |
44/56 | 1-53 days 8,2±1.9 |
3-17 13.6±3.6 |
14-21 18.9±0.9 |
88.9% | 2-59 13.4±2.9 |
4% |
| 2nd group | 110 | 17-86 36.7±2.2 |
52/58 | 3-72 months 17.2±3.2 |
3-29 18.0±4.3 |
15 – 28 16.0±3.6 |
39% | ? | 47% |
| 211 | p<0.001 | p<0.001 | p>0.2 | p>0.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



