
Submitted:
08 January 2024
Posted:
08 January 2024
You are already at the latest version
Abstract
This study addresses the influence of working conditions on Work-Related Quality of Life (WRQOL) among Spanish healthcare professionals. The research seeks to elucidate the mediating roles of job engagement and burnout, and the moderating effects of resilience and self-efficacy, in this relationship. Methods: The study included 374 healthcare workers from Spain, encompassing physicians, nurses, and nursing assistants. It employed a methodological approach using validated instruments to assess psychosocial risks, work-life quality, job engagement, burnout, and resilience. Data were gathered through self-reported questionnaires. Results: Key findings indicate a negative association between working conditions and WRQOL. Job engagement and burnout significantly mediated this relationship, accounting for 19% to 33% of the variance in WRQOL. Notably, lack of support emerged as a strong negative factor for work-related quality of life. Additionally, resilience moderated the relationship between lack of support and burnout. Conclusions: The study concludes that improving working conditions could increase WRQOL. Interventions aimed at enhancing engagement and addressing burnout may be effective. The moderating role of resilience suggests that strategies to enhance resilience could also be beneficial. These findings hold significant implications for policy formulation and human resources planning in healthcare, emphasizing the need for enhanced workplace support and the development of resilience among health workers.
Keywords:
Healthcare Professionals
; Work Conditions
; Burnout
; Job Engagement
; Psychosocial Risks
; Social Support
; Resilience
; Job Satisfaction
; Work-Related Quality of Life (WRQoL)
; Occupational Health
1. Introduction
The quality of work life of healthcare professionals is an area of growing interest, particularly in a context where healthcare systems worldwide are facing increasing pressures due to an aging population, the rise of chronic diseases, and expectations for high quality healthcare services. In this demanding environment, the occupational health and well-being of healthcare workers are not only crucial to their own well-being, but also to the effectiveness and quality of the healthcare they provide [1]. Recent studies have begun to unravel the complex factors that contribute to work-related quality of life (WRQoL) in this sector, including the impact of burnout and work engagement [2,3,4]. The current pandemic of COVID-19 has further exacerbated these issues, highlighting the urgent need to investigate and improve the working conditions of these essential professionals [5].
The study of work conditions among healthcare professionals is pivotal, given that their well-being directly influences patient care quality, healthcare delivery efficiency, and the overall functioning of health systems. Occupational stress and burnout can lead to high turnover rates, staffing shortages, and increased costs due to absenteeism and decreased productivity [6]. Moreover, healthcare workers' job dissatisfaction can compromise patient safety, increase the likelihood of medical errors, and negatively impact patient satisfaction [7,8]. By understanding and improving the working conditions of healthcare professionals, the resilience and sustainability of healthcare systems can be enhanced, especially in the face of global health crises that demand optimal performance and retention of healthcare staff [9,10,11].
The main purpose of this research is to investigate the relationship between the working conditions of healthcare professionals in Spain and their work-related quality of life (WRQoL). Specifically, we seek to understand the extent to which work engagement and burnout mediate this relationship, and to explore the role of resilience and self-efficacy in buffering the potential negative impacts of adverse working conditions. This study aims to provide empirical evidence that can inform strategies to improve WRQoL among healthcare workers, with the goal of improving both employee well-being and patient care outcomes.
Work-related quality of life (WRQoL) in healthcare professionals is essential to their ability to deliver high-quality services. Positive WRQoL improves satisfaction and reduces absenteeism [12,13], whereas poor WRQoL can lead to burnout and affect patient care and health system efficiency [14,15]. This study aims to provide evidence for improving WRQoL in healthcare workers by analyzing how working conditions, engagement, and burnout, along with resilience and self-efficacy, influence it. Work stress in healthcare workers, its relationship with burnout and the importance of work engagement as a buffer are key issues in current research [16,17,18].
Recent research has expanded to include the concept of resilience as a critical factor in mitigating the effects of stressful work environments [19,20,21,22,23,24,25,26]. Resilience, understood as the ability to cope with adversity, is a valuable strength within the so-called psychological capital [27,28]. To enhance and improve it, it is recommended to implement specific training in this capacity, without forgetting the continuous improvement of working conditions and the work environment [29,30,31,32,33].
In addition to resilience, the role of self-efficacy in the well-being of healthcare professionals is increasingly recognized as a vital area of research. Self-efficacy, defined as an individual's belief in his or her ability to execute the behaviors necessary to produce specific performance achievements [34], has been shown to significantly influence how healthcare workers perceive and respond to their work environment. For example, self-efficacy has been found to predict less stressful perceptions of situations that healthcare workers must face in their work, such as emotional stress from patients and demands from family members [35]. Complementarily, other studies have found that burnout is positively associated with perceived stress and negatively associated with self-efficacy [36,37,38]. Self-efficacy has even been shown to predict reductions in burnout [39,40], especially when self-efficacy is specific to a domain that compromises the pressure of certain working conditions, as in the case of communication skills, so necessary for coordinating with colleagues and interviewing the sick [41]. Finally, the results of these studies highlight the protective role of self-efficacy and justify the implementation of programs to promote and maintain it.
The influence of self-efficacy on stress and burnout is not always direct. It may act as a mediator between stress and psychological well-being, where higher self-efficacy helps to mitigate the negative effects of job stress [42]. Furthermore, it has been found that both job burnout and job engagement can be influenced by self-efficacy, highlighting its role in moderating the impact of job stress and enhancing resilience in the face of job stress [43,44].
Attention to positive qualities such as resilience and self-efficacy aligns with the Council of Europe's recommendation to adopt an integrative approach based on 'well-being at work' [45], pointing to the importance of understanding how certain mechanisms influence the relationship between working conditions and WRQoL.
Starting from a broad conception of working conditions, which include the physical environment, workload, autonomy, and interpersonal relationships, and WRQoL, which integrates both work and nonwork factors and their interaction [46], our study focuses on exploring how psychosocial factors in the work environment affect the emotional and professional well-being of healthcare workers in hospitals. We have been interested in why burnout and engagement may explain the influence of working conditions on workers' well-being, and we consider the possibility that some factors, such as resilience or self-efficacy, function as moderators of these interactions.
Burnout is understood in our study as a manifestation of chronic work stress, evidenced by emotional exhaustion, depersonalization, and reduced self-fulfillment. In parallel, engagement is presented as a state of vigor, dedication, and absorption at work, which can act as a counterbalance to burnout [47]. Therefore, we test mediation models to reveal how burnout and engagement may mediate between working conditions and WRQoL, which can provide detailed insight into how these affective psychological states affect the perception and experience of work.
In addition, our study examines the role of resilience and self-efficacy, considered as personal resources that can soften the negative impacts of unfavorable work conditions, including lack of social support. These personal qualities not only directly influence WRQoL, but also differentially modulate the incidence of burnout in response to such conditions.
In the area of the mediating effect of burnout and engagement on the relationship between working conditions and quality of work life in healthcare professionals, the relevance of these conditions has been investigated. For example, the effects of job stress, exacerbated by COVID-19, on affective well-being through compassion fatigue in nursing were studied, which validated the model [48].
From the perspective of the demands-resources model [49], the effects of organizational factors such as nurse-patient ratio [50], interprofessional teamwork [51], and work environment and social support [52] on intention to quit have been analyzed, as well as their mediation by burnout. The impact of psychological capital [53] and self-efficacy [54] on turnover anxiety or turnover intention, with burnout as a mediator, has also been confirmed.
In addition, commitment and compassion satisfaction were shown to mediate the positive relationship between personal resources and health, well-being, safety, and quality of care [55,56], and their negative relationship with psychosocial risks [57].
These studies have deepened the understanding of the role of burnout and engagement in relation to working conditions and key aspects such as performance, safety and, especially, workers' mental health. However, WRQoL, which is vital for a comprehensive view of well-being at work, has been less studied. Its importance lies in encompassing both the impact of working conditions on the mental and physical health of employees and their influence on productivity, satisfaction, and organizational effectiveness [52,58,59].
Our study broadens the field by examining both personal and organizational predictor variables more broadly and deeply. Unlike previous research [54], we analyze how burnout and engagement, considered in part as mediators, interact and affect WRQoL, an innovative approach in the field [60,61]. We included a diverse sample of healthcare professionals, extending beyond the common focus on nursing staff [62,63].
By considering resilience and self-efficacy as moderators, we enrich the analysis of how personal attributes influence the relationship between job support and burnout. This approach broadens the understanding of work dynamics and has practical implications for the development of work support and well-being strategies. Our study highlights the use of advanced measurement models, which allow for a comprehensive exploration of the interactions between various psychosocial variables. Our rigorous and transparent methodology addresses in detail the normality, linearity, multicollinearity, and homoscedasticity of variables, overcoming the methodological limitations of previous studies [51].
In conclusion, our study provides a comprehensive and detailed interpretation of the data, offering a holistic view of psychosocial factors impacting quality of work life in the healthcare sector. We contribute significantly to existing knowledge and highlight key areas for future interventions in quality of work life in healthcare.
In the context of increasing pressures on healthcare systems and needs identified in the literature, this study seeks to fill a crucial gap in the understanding of factors influencing the WRQoL of healthcare professionals in Spain, focusing on unraveling the complex interactions between working conditions and their psychosocial impact.
The main objectives are to (1) Investigate the relationship between working conditions and WRQoL of health professionals. (2) To examine the mediating role of burnout and engagement in this relationship. (3) To explore how resilience and self-efficacy act as moderators. We seek to understand how these personal qualities may influence the intensity or direction of these relationships.
To achieve these objectives, we test the following hypotheses:
- Mediation Hypothesis. We postulate that both burnout and engagement significantly mediate the relationship between working conditions and WRQoL, providing a deeper understanding of how work dynamics affect the well-being of health care workers.
- Moderation Hypothesis: We propose that resilience and self-efficacy will moderate the relationship between working conditions and WRQoL, as well as mediate it through burnout and engagement, suggesting that these personal factors may reinforce or attenuate the effects of working conditions on WRQoL.
With these objectives and hypotheses, our study seeks to contribute significantly to the field of occupational health, offering a comprehensive perspective on how to improve the quality of work life of health professionals. By unraveling the complex relationships between working conditions, psychological well-being, and personal resources, we aim to provide empirical evidence to inform the development of more effective interventions and policies aimed at promoting a healthy and resilient work environment in the healthcare sector.
2. Materials and Methods
2.1. Participants
A total of 374 health professionals participated voluntarily and anonymously and were selected by random-incidental sampling according to sex and profession quotas [64]. According to the sampling technique, we invited 700 employees from a large hospital to participate in the study. Therefore, the response rate was approximately 53.43%. The sample size was a sampling error of 4.86% at a confidence interval of 95%, for a response of equiprobable interest. The composition of the sample was 63 physicians, 209 nurses, and 102 nursing assistants. The 74.3% of the sample were women, and 71.4% had a permanent employment contract.
2.2. Measures
2.2.1. Psychosocial Risks
Working conditions were assessed using a 30-item Psychosocial Risk Inventory (PRI), based on Karasek's [65] model of job stress, distributed in three dimensions: demand (16 items), control (10 items) and support (46 items). An example of an item from the demand scale is: "My job requires meeting strict deadlines for legal or procedural reasons" (item 4). For the control dimension, an example would be: 'I can control and schedule my work pace' (item 18). For support, the following stands out: 'I have smooth communication with immediate supervisors.' (item 28). The items are answered on a true/false dichotomous scale. The content validity of the scale was confirmed by means of inter-rater agreement (three senior occupational risk prevention technicians), obtaining a Kappa coefficient equal to 0.92, indicating almost perfect agreement. Reliability was obtained through the Alpha coefficient, whose values were 0.83 for the general scale and 0.73, 0.74 and 0.79 respectively for each of the subscales. In addition to the continuous scores, dichotomous qualitative ratings were obtained for each subscale. High demand is identified if two or more items of this subscale are answered affirmatively, or item 13, which states, "My work involves direct contact with users whose personal problems are serious or whose behavior is an obstacle to the provision of the service." Control is considered insufficient if two or more items of this subscale are answered negatively. Insufficient support is established if one responds negatively to items 27 and 28, or to item 29 or 30, which address fluid communication with superiors and a cordial and collaborative work environment, respectively.
2.2.2. Work-Related Quality of Life
Experienced quality of life at work was assessed through the work-related quality of life instrument [46], which consists of a self-administered 24-item scale, specially built for healthcare working population. They collected items from numerous previous well-being instruments [66,67], that reported work and non-work aspects of quality of work life, as well as work-related stress. In this sense, the instrument covers a broad theoretical scope. Although we used the overall scale score, the original version comprised six factors: job and career satisfaction (α=0.86), stress at work (α=0.82), working conditions (α=0.82), control at work (α=0.81), home-work interface (α=0.81) and general well-being (α=0.75). An example of item is “I have a clear set of goals and aims to enable me to do my job”.
2.2.3. Engagement.
Commitment was measured with the Spanish version of the Utrecht Work Engagement Scale (UWES) [68,69]. It consists of 17 self-administered 7-point Likert scale items, with responses ranging from 0 “never” to 6 “always”. Engagement is defined by its authors as “a positive, fulfilling, and work-related state of mind that is characterized by vigor, dedication, and absorption” [69] (p. 465). Factorial analysis showed a three-factor structure, with vigor (with 6 items, α=0.79), dedication (with 5 items, α=0.85) and absorption (with 6 items, α=0.65) as subscales. An example of the vigor subscale is “At my work, I feel bursting with energy”. An example of dedication subscale is “I find the work that I do full of meaning and purpose”. An example of absorption subscale is “Time flies when I am working”. However, for our study purposes we also took the overall engagement score, which also has shown to adequately fit the data.
2.2.4. Burnout.
Burnout was measured with the Shirom-Melamed Burnout Questionnaire [70,71], which is a specific instrument to measure stress-related exhaustion among healthcare working population [72]. Its theoretical foundations are the Conservation of Resources (COR) theory [73] and the idea that burnout is only related to energy resources [74,75].
The self-administered questionnaire consists of 12 items taping two subscales (of 6 items each), physical fatigue (α=0.92) and cognitive weariness (α=0.87-0.89). An example of item for physical fatigue is “I feel tired”, and for cognitive weariness “I’m too tired to think clearly”. However, for the study purposes we took the overall score.
2.2.5. Resilience.
To measure resilience, we used the generalized Connor-Davidson resilience scale (CD-RISC) [76]. It consists of a 25-item self-administered questionnaire, with a 5-point Likert scale response format, ranging from 0 "strongly disagree" to 4 "strongly agree". In its original version it covers 5 dimensions: personal competence, intrinsic tolerance of negative affect, positive acceptance of change, control, and spiritual influence. For our purposes we will stick to the general factor (resilience). In its original version, the entire scale had an internal consistency index of 0.89 (Cronbach's alpha). An example item is "When things seem hopeless, I don't give up.".
2.2.6. Workplace Self-efficacy
Instrument developed for this purpose according to the guidelines established by Bandura [77] for the construction of self-efficacy scales. It evaluates the degree of confidence or security that a professional has in being able to do his or her job under various adverse circumstances, considered as psychosocial risk situations (e.g., "If the facilities or the furniture are uncomfortable", "If I am assigned an important job in which any mistake would be serious", "If I have no possibility to participate in the decision-making process", "When I have to deal with difficult people"). It consists of 18 items to which the subjects must respond, assigning each one a score between 1 (Unable to do it) and 10 (Sure of being able to do it). The higher the score, the greater the perception of self-efficacy. The alpha reliability coefficient was 0.91 for the general scale.
2.3. Analysis
First, descriptive analysis (mean, standard deviation and Pearson correlation) was performed with IBM’s statistical program SPSS. We also reported frequencies for our qualitative demographic variables and for the qualitative transformation we performed on quality-of-life scores.
Second, we performed several multiple linear regression analyses with both the free access software RStudio V1.1.383 and the PROCESS macro for SPSS [78]. We examined normality in our quantitative variables by inspecting Q-Q plots, and skewness and kurtosis indexes. Linearity was assessed through the inspection of scatter plots. Multicollinearity was assessed by inspecting the residuals and correlation matrix. Our first aim was to fix two mediation models with burnout and engagement as respective single mediators. Later, we tried to fix moderated mediation models, by exploring well known potential moderators, as self-efficacy, or resilience. We examined both direct and indirect effects, and we estimated adjusted R square and partial eta square for every model and predictor within our models. Nevertheless, through these models, our intention was just to describe how our variables were associated following the proposed models. Thus, we didn’t seek causation since we didn’t manipulate our study variables in a fully controlled situation.
3. Results
3.1. Descriptives
Table 1 shows the frequencies and percentages of the qualitative variables of the study, which define, to a large extent, the demographic and professional profile of the participants. Analysis of the gender composition reveals a marked female predominance, with 74.3% of the responses coming from women, compared to 25.7% from men. This distribution is in line with the trends observed globally in the healthcare workforce, where the female presence is notably high.
Regarding the type of contract, it is observed that most professionals (71.4%) have permanent contracts, suggesting considerable job stability within the sample. On the other hand, 28.6% of the participants indicated having temporary contracts, reflecting a significant fraction of the workforce in more unstable employment conditions.
Regarding the presence of disability among the respondents, only 3.5% claimed to have a disability, which represents a minority within the sample studied.
Regarding employment position, the largest group was found to be nurses, who constituted 55.9% of the total, followed by clinical assistants with 27.3%, and physicians with 16.8%. This distribution pattern reflects the typical structure of health care teams, where nurses tend to be the most numerous.
The sample also shows diversity in terms of service areas, with higher representation in Critical Care and Emergency (29.7%), General and Internal Medicine (16.8%), and Surgery (16.6%). These data suggest a wide range of work settings and specializations within the healthcare sector.
Finally, in relation to occupational risk factors, a large majority of respondents reported high demand in their work (95.5%) and low control (86.4%), which may be indicative of a stressful work environment. However, only 19.5% of participants reported low support at work, suggesting that, despite conditions of high demand and low control, many health professionals perceive an adequate level of support in their work environments.
These findings provide valuable context for understanding the working conditions and demographics of health professionals, facilitating a deeper interpretation of their Work-Related Quality of Life (WRQoL) and other aspects related to their well-being and professional efficacy.

Table 1.
Distribution of qualitative variables.
| Variable | Categories | Frequency | Percentages |
|---|---|---|---|
| Sex | Woman | 278 | 74,3% |
| Male | 96 | 25,7% | |
| Contract | Temporary | 107 | 28,6% |
| Permanent | 267 | 71,4% | |
| Disability | No | 361 | 96,5% |
| Yes | 13 | 3,5% | |
| Job Position | Clinic Assistant | 102 | 27,3% |
| Nurse | 209 | 55,9% | |
| Physician | 63 | 16,8% | |
| Service Area | General & Internal Medicine | 63 | 16,8% |
| Surgical | 62 | 16,6% | |
| Critical Care and Emergency | 111 | 29,7% | |
| Pediatric | 27 | 7,2% | |
| Diagnostic and Support | 18 | 4,8% | |
| Oncology & Palliative Med. | 33 | 8,8% | |
| Health Mental | 16 | 4,3% | |
| Women | 27 | 7,2% | |
| Other | 17 | 4,5% | |
| Risks | High Demand | 357 | 95,5% |
| Low Control | 323 | 86,4% | |
| Low Support | 73 | 19,5% |
Table 2, which presents the means, standard deviations and skewness and kurtosis values of our quantitative variables, provides a revealing insight into the characteristics of the healthcare professionals. The mean age of 44.52 years suggests a workforce with considerable experience. The data on tenure and hours of work reflect a stable employment picture, with variations indicating diverse career paths and work schedules.
Analysis of days off work, the only variable showing serious violations of normality, highlights an interesting pattern of absence, in part due to high variability and many subjects reporting zero days off work. This aspect highlights unique facets of the work culture in healthcare settings.
In terms of psychosocial risks and burnout, the results suggest moderate challenges faced by staff. Despite these challenges, the data reveal a relatively high level of work engagement among healthcare professionals, indicating a strong commitment to their roles. In addition, positive work-related quality of life (WRQoL) scores highlight a generally favorable perception of their work environment.
Overall, the perceptions in Table 2 depicts a picture of an experienced and stable healthcare workforce, facing moderate psychosocial challenges but maintaining a high level of engagement and a positive perception of their work life. This balanced view is critical to understanding the dynamics within healthcare settings and informs strategies to improve staff well-being and efficiency.
Table 2.
Quantitative variables: descriptive parameters.
| Variable | Mean | Std. Deviation | Skewness | Kurtosis |
|---|---|---|---|---|
| Age | 44,52 | 9,836 | -,156 | -,576 |
| Tenure | 15,22 | 11,023 | ,481 | -,770 |
| Working hours | 37,29 | 7,830 | ,996 | 5,943 |
| Work leaves days | 4,64 | 13,690 | 5,102 | 33,011 |
| Psychosocial Risks | 11,3503 | 4,96991 | ,578 | ,339 |
| Demand | 6,63369 | 2,969377 | ,289 | -,265 |
| Control | 5,76471 | 2,460026 | -,370 | -,604 |
| Support | 3,51872 | ,895878 | -2,114 | 4,199 |
| Burnout | 2,5033 | 1,17167 | ,998 | ,926 |
| Engagement | 4,2550 | ,89996 | -,832 | 1,067 |
| Workplace Self-efficacy | 6,2686 | 1,45508 | -,087 | -,035 |
| Resilience | 2,9556 | ,50308 | -,335 | -,021 |
| WRQoL | 3,5189 | ,57523 | -,248 | -,114 |
3.2. Mediation tests
First, preliminary analyses were performed to test for linearity, normality, multicollinearity, and homoscedasticity of our variables. No serious violations of the regression assumptions were found, which allowed us to explore our mediation models.
The aim of our mediation models was to explore whether working conditions or their dimensions were related to work-related quality of life (WRQoL), through burnout, engagement, or both (double mediation). We used qualitative coding for general work conditions (with three items, showing whether individuals have one, two, or three risk factors) and their dimensions (coded as binary variables, meaning that individuals have or do not have that risk factor). As a first step, we explored the relationship between our predictor (PRI) and the outcome (WRQoL). We performed a regression model controlling for sex, age, seniority, days off work, hours of work, type of contract, service area and job position. We observed that working conditions were negatively related to work-related quality of life (β= -0.382; SE=0.0454; p<0.001), and that the overall model explained 14% of the variance (adjusted Rsq=0.144). However, when we introduced the dimensions of working conditions or psychosocial risks as predictors, we found that only support was significantly associated with WRQoL (β= -0.427; SE=0.053; p<0.001), with the model explaining 13% of the variance (adjusted Rsq = 0.1309). Thus, we decided to build our model with the overall PRI score.
As a second step, we performed several mediation tests with the Process macro for SPSS [78], with the intention of testing whether engagement or burnout were significant mediators of the relationship between working conditions and WRQoL. We entered all our demographic controls and created two dummy variables for our qualitative predictor (2-3 risk factors vs. 1, or 3 risk factors vs. 1-2). For the model with engagement as a mediator, we observed that: a) the second PRI dummy variable (having 3 risk factors vs. 1 or 2 was significantly negatively related to engagement (β= -0.408; SE=0.106; p<.001), b) engagement was significantly positively related to WRQoL (β= 0.253; SE=0. 024; p<.001), c) both PRI dummy variables were significantly negatively related to WRQoL (p<.01 for 2-3 risk factors vs. 1, and p<.0.001 for 3 risk factors vs. 1-2) after introducing the mediator, and d) the indirect effect for the second PRI dummy variable was different from zero (CI= -0.166 / -0.049). Overall, the model has an adjusted R-squared of 0.329 (almost 33% variance explained).
For the model with burnout as mediator, we observed that: a) the second dummy variable PRI was positively related to burnout (β= 0.688; SE=0.138; p<.001), b) burnout was negatively related to WRQoL (β= -0.097; SE=0.02; p<. 001), c) both PRI dummy variables were negatively related to WRQoL after introducing the mediator (p<.05 and p<.001, respectively), and d) indirect effects were different from zero for the second PRI dummy variable (CI= -0.126 / -0.028). The adjusted R-squared was 0.19 (19% variance explained).
Finally, we tested a double mediation model, but it was not significant. Even so, the two single-mediated effects were still present. In summary, we obtained two partially mediated models, explaining 33% (engagement) and 19% (burnout) of the variance, respectively.
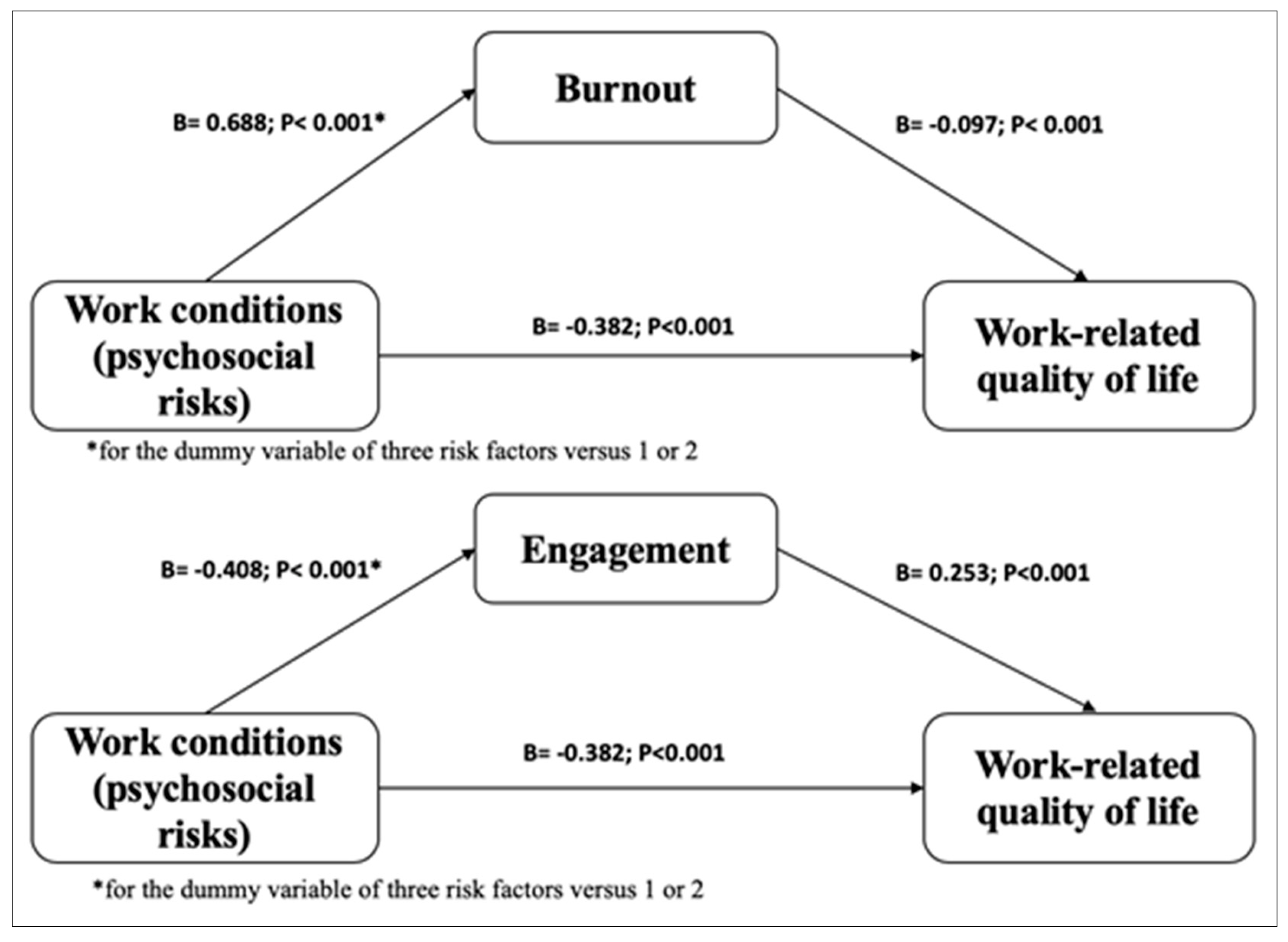
Figure 1.
Representation of the dual-mediation model.
Table 3.
Eta square values for engagement and burnout mediation models.
| Variable | Engagement: partial η2 | Burnout: partial η2 |
|---|---|---|
| Sex | 0.001 | 0.001 |
| Age | 0.001 | 0.001 |
| Tenure | 0.001 | 0.001 |
| Contract | 0.001 | 0.001 |
| Working hours | 0.001 | 0.001 |
| Work leaves days | 0.001 | 0.001 |
| Disability | 0.001 | 0.001 |
| Job position | 0.016 | 0.017 |
| Service area | 0.001 | 0.001 |
| PRI | 0.150 | 0.150 |
Outcome variable WRQoL. N = 374.
3.3. Moderated Mediation Tests.
We then sought to explore which variables might act as moderators in the mediation models described. We replicated our analyses with process, including resilience and self-efficacy as possible moderators. First, none of the moderated mediation models (with engagement or burnout as mediators) for the overall PRI score was significant, nor were the models with PRI dimensions as predictors and engagement as a mediator. However, for the PRI support risk dimension with burnout as mediator, we found a slight moderation effect for the relationship between PRI and burnout. Table 4 and Table 5 show the simple direct and indirect moderation effects. In summary, the simple conditional direct moderator effects were all significant, with the effect of lack of support being more negative on WRQoL as resilience decreases. Conditional indirect effects (effect of lack of support on WRQoL through burnout) were only significant for mean resilience values, or one standard deviation below the mean, also being more negative as resilience decreases. The adjusted R-squared for the moderated mediation model with PRI support was 0.356 (approximately 35% variance explained).
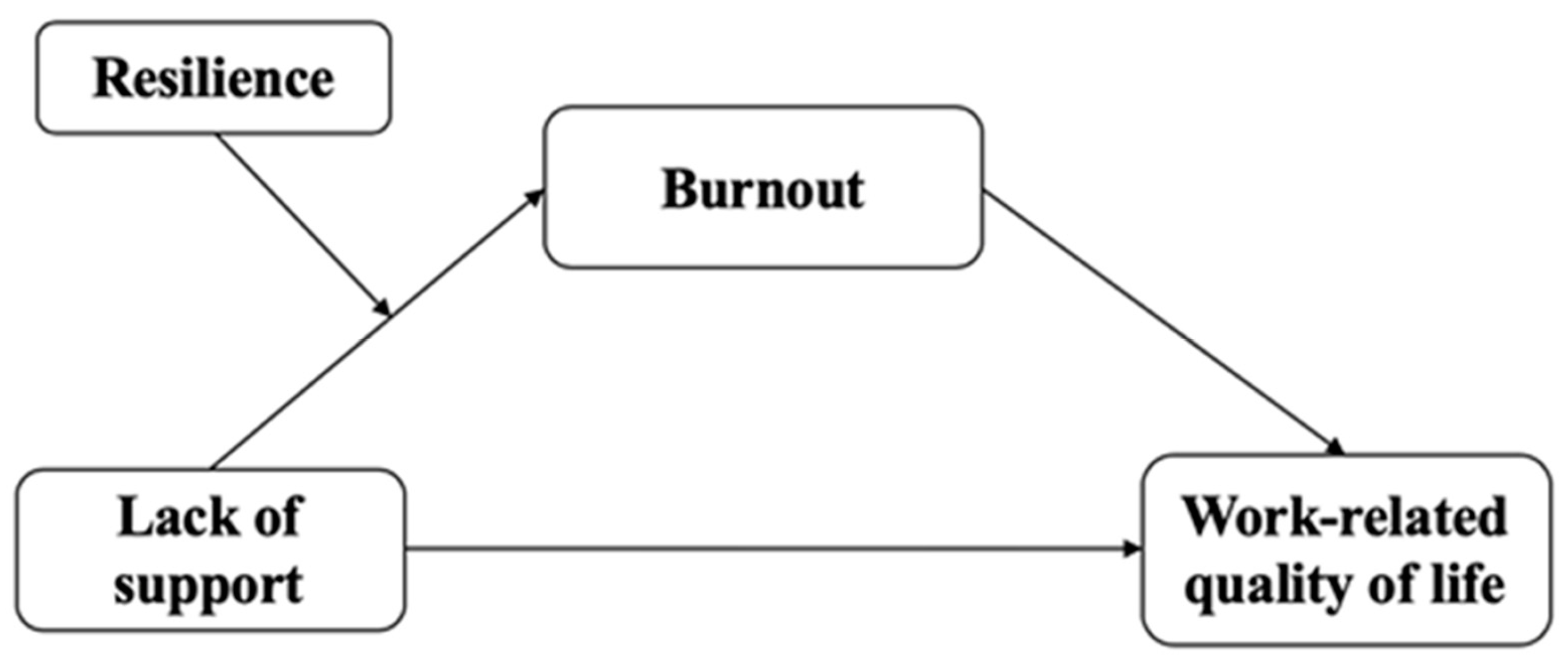
Figure 2.
Moderated mediation model for PRI support with resilience (moderator) and burnout (mediator).
Figure 2.
Moderated mediation model for PRI support with resilience (moderator) and burnout (mediator).
Table 4.
Direct simple moderation effects for PRI support with resilience.
| Resilience | Effect | SE | t | p value | CI |
|---|---|---|---|---|---|
| + 1 SD | -0.307 | 0.063 | -4.858 | .001 | (-0.431 - -0.182) ** |
| mean value | -0.322 | 0.048 | -6.644 | .001 | (-0.417 - -0.226) ** |
| - 1 SD | -0.337 | 0.07 | -4.768 | .001 | (-0.476 - -0.198) ** |
N=374; **CI does not comprise 0.
Table 5.
Indirect simple moderation effects for PRI support with resilience (moderator) and burnout (moderator).
Table 5.
Indirect simple moderation effects for PRI support with resilience (moderator) and burnout (moderator).
| Sex value | Effect | Boot SE** | Boot CI |
|---|---|---|---|
| + 1 SD | -0.011 | 0.012 | (-0.047 - 0.002) |
| mean value | -0.024 | 0.014 | (-0.058 - -0.001) *** |
| - 1 SD | -0.036 | 0.02 | (-0.086 - -0.003) *** |
*Mediator: Burnout; N=374; **Standard Error values and Confidence. Intervals obtained by Bootstrapping procedure; ***CI does not comprise 0.
4. Discussion
The present study comprehensively and novelty addresses the relationship between working conditions and Work-Related Quality of Life (WRQoL) among healthcare professionals in Spain. While our findings confirm the negative association between working conditions and WRQoL, aligning with previous research on the impact of work stress and burnout [6,7,8], this study goes further by exploring and evidencing the mediating role of work engagement and burnout in this relationship. In addition, we introduce an innovative approach by examining the moderating effect of resilience and self-efficacy, thereby expanding the understanding of how these psychological factors may influence and modify the work experience and WRQoL of healthcare professionals. This unique approach allows for a deeper and more nuanced understanding of work dynamics in the healthcare sector, highlighting the importance of addressing both organizational and psychological aspects to improve WRQoL.
Positive WRQoL has been observed to improve satisfaction and reduce absenteeism, whereas poor WRQoL can lead to burnout and affect patient care and health system efficiency [12,13,14,15]. Furthermore, studies have shown that commitment and compassion satisfaction mediate the positive relationship between personal resources and health, well-being, safety, and quality of care, as well as their negative relationship with psychosocial risks [55,56,57].
These aspects underscore the importance of understanding and improving the working conditions of health professionals to enhance the resilience and sustainability of health systems, especially in times of global health crises that demand optimal performance and retention of the health workforce [9,10,11].
The significant mediation of work engagement and burnout in the relationship between working conditions and WRQoL is a key finding of our study. These results not only align with the existing literature, which identifies both burnout and work engagement as critical indicators of workplace well-being [16,17,18,48,49,50,51,52,53,54,55,56,57], but also expand this knowledge. For example, the study by Gillen et al [16] on healthcare professionals in the UK during the COVID-19 pandemic highlights the impact of burnout on quality of work life, which corresponds with our observations on the importance of burnout as a mediating factor. Similarly, research by Yang et al [18], examining Chinese nurses in Japan, reinforces the idea that work engagement is foundational to well-being at work. Our findings support and extend these perspectives, suggesting that work engagement not only influences quality of life, but also acts as a key mediator in the specific context of health professionals in Spain. In this way, our study contributes to a deeper and more contextualized understanding of how these psychological factors operate in diverse work environments in the health sector.
Our study highlights the positive influence of adequate Work-Related Quality of Life (WRQoL) on satisfaction and reduced absenteeism, and how poor WRQoL can lead to burnout, affecting patient care and the efficiency of the healthcare system [12,13,14,15]. For example, the study [12] reveals that technological progress in healthcare not only benefits patients, but also healthcare professionals, which aligns with our findings on the importance of a positive WRQoL. In addition, research [13] highlights the impact of burnout and satisfaction on hospital staff during the pandemic, which reinforces our understanding of how poor WRQoL can adversely affect healthcare professionals. Similarly, the study [14] in Portugal demonstrates the relationship between burnout, WRQoL and mental health symptoms, supporting our conclusions about the importance of WRQoL in the mental health and general well-being of workers. Finally, research [15] on palliative care shows the complexity of burnout in different care settings, underscoring the need for tailored support policies and the relevance of our focus on improving working conditions to enhance the resilience and sustainability of health systems.
Consistent with our mediation hypothesis, our findings confirm that both burnout and work engagement play significant mediating roles in the relationship between working conditions and Work-Related Quality of Life (WRQoL). Our model showed that burnout mediated this relationship, with a significant indirect effect (CI= -0.126 / -0.028) and explaining 19% of the variance in WRQoL. Similarly, work engagement also acted as a significant mediator, with an indirect effect (CI= -0.166 / -0.049) and explaining approximately 33% of the variance in WRQoL. This observation aligns with our initial prediction, evidencing how these psychological factors affect the perception of the work environment and, consequently, WRQoL. The results corroborate the existing literature that identifies burnout and work engagement as crucial elements for workplace well-being [16,17,18,48,49,50,51,52,53,54,55,56,57].
Continuing with the analysis of our hypotheses, the results also support the moderation hypothesis by identifying resilience and self-efficacy as key moderators in the relationship between working conditions and WRQoL. In our study, we found that resilience moderates the relationship between lack of support and WRQoL through burnout. Direct moderation effects were significant, showing that the negative effect of lack of support on WRQoL was more pronounced as resilience decreased (effect of -0.337 for low resilience, -0.322 for medium value, and -0.307 for high resilience, p<0.001). Indirect moderation effects were also significant, particularly for lower resilience values or one standard deviation below the mean, being more negative as resilience decreases (effect of -0.036 for low resilience, -0.024 for the mean value, and -0.011 for high resilience). These findings underscore the need to improve working conditions and supportive policies, with the aim of strengthening the resilience and well-being of health professionals.
In summary, the findings of our study not only confirm our initial hypotheses, but also provide new insights into the complexity of work relationships in the health sector. We have shown that burnout and work engagement are key mediators in the relationship between working conditions and Work-Related Quality of Life (WRQoL). Furthermore, we have identified that resilience and self-efficacy act as significant moderators of this relationship, influencing how health professionals experience their work environment and work-related quality of life. This enriched understanding of work dynamics in the health care setting offers clear directions for future interventions and policies aimed at improving WRQoL. These findings underscore the importance of addressing both psychological and organizational aspects to strengthen health workers' resilience and well-being, which is crucial for the effectiveness and sustainability of health systems.
The moderation of resilience in the relationship between lack of support and burnout is particularly relevant, suggesting that strengthening resilience may be an effective strategy to mitigate the effects of burnout under unfavorable working conditions. This is consistent with research emphasizing resilience as a key factor in adaptation to stressful work environments [19,20,21,22,23,24,25,26,27,28,29,30,31,32,33]. Resilience, understood as the ability to cope with adversity, has been identified as a valuable strength within psychological capital, and its enhancement through specific training and continuous improvement of working conditions are recommendations supported by the literature.
The results also emphasize the importance of self-efficacy as a personal re-course in the healthcare work environment. Our study revealed that self-efficacy significantly mediated the relationship between working conditions and WRQoL. For example, we found that when self-efficacy was introduced as a mediator in our model, the negative effect of working conditions on WRQoL was attenuated. Specifically, self-efficacy was significantly related to higher WRQoL (β= 0.253, p<.001), while working conditions continued to have a negative impact on WRQoL (β= -0.382, p<.001). This suggests that self-efficacy acts not only as a moderator of the impact of work stress, but also as a mediator in the relationship between stress and psychological well-being. Furthermore, it has been shown that self-efficacy can predict a reduction in burnout, especially in specific domains that affect the pressure of working conditions, such as communication skills. These findings underscore the im-portance of self-efficacy in maintaining a high work-related quality of life, which is critical to both the well-being of the workforce and the efficacy of the health care system [34,35,36,37,38,39,40,41,42,43,44].
This study has important limitations that must be considered for a proper evaluation of the findings. First, although the sample size is adequate, its representativeness may not be optimal for all health professionals in Spain, as participants were selected by random incidental sampling, focusing mainly on hospital staff. This could affect the generalizability of the results to other geographical or cultural contexts.
Second, reliable instruments were used to assess the relevant variables, but some, such as the Psychosocial Risk Inventory and the Work-Related Life Quality Scale, have been little used in previous research. This limits the comparability of the results with other studies and raises questions about the cross-validation and applicability of these instruments in different work and cultural contexts.
Furthermore, being a cross-sectional study, causal relationships between variables cannot be established. The use of self-administered questionnaires could also introduce subjective biases in the responses. Future research should consider these aspects for a broader and more robust understanding of how occupational conditions and psychosocial factors affect work-related quality of life in different health settings.
Finally, although a wide range of psychosocial factors were addressed, other relevant variables such as organizational culture or economic factors were not considered. These elements could significantly influence quality of work life and should be the subject of future research.
To overcome these limitations, it will be necessary in the future to conduct longitudinal studies to establish causal relationships and evaluate the long-term effects of interventions. Expand research to different geographical contexts and to a wider variety of roles in the health sector and consider the impact of organizational culture and other structural factors on quality of work life.
It should also highlight the need for future research, especially in the development and implementation of interventions aimed at improving WRQoL in the healthcare sector. Future research could explore in greater detail how specific strategies to increase resilience and self-efficacy can be implemented and what their effectiveness is in different contexts and populations within the health sector.
In addition, it would be valuable to examine how interventions that simultaneously address personal and organizational factors may have a more significant impact on improving WRQoL. This would include the evaluation of resilience training programs, psychosocial support initiatives, and strategies to improve autonomy and physical conditions in the workplace.
5. Conclusions
This study confirmed the hypothesis of a negative relationship between working conditions and Work-Related Quality of Life (WRQoL) among health professionals in Spain. Significantly, it highlighted the mediating roles of work engagement and burnout, and the moderating effects of resilience and self-efficacy in this relationship. These findings highlight the importance of improving working conditions to optimize WRQoL, reduce absenteeism and prevent burnout, positively impacting patient care and health system efficiency.
The study suggests the need for future research, including longitudinal studies and in broader contexts, to better understand WRQoL in the healthcare setting. Furthermore, it highlights the relevance of developing and implementing interventions aimed at strengthening resilience and self-efficacy among healthcare professionals.
Author Contributions
Conceptualization, JM.L.R. and JI.V.N.; methodology, JM.LR., JI.V.N.; validation, JM.L.P., P.R.B. and FJ.C.S..; formal analysis, P.R.B.; investigation, JI.V.N., J.M.LR., FJ.C.S., and A.F.C..; resources, JM.LR., JM.L.P.; data curation, JM.L.R.; writing—original draft preparation, JM.L.R., JI.V.N.; writing—review and editing, FJ.C.S., JM.L.P. A.F.C.; visualization, FJ.C.S., A.F.C.; supervision, JM.L.P.; project administration, JM.L.R.; funding acquisition, JM.L.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the European Union (“Fondo Europeo de Desarrollo Regional (FEDER)”) and the Andalusian Government (“Consejería de Economía, Conocimiento, Empresas y Universidad de la Junta de Andalucía, dentro del Programa Operativo FEDER 2014-2020”). Project ref. US-1381664.
Institutional Review Board Statement
According to the Andalusian Ethics Committee, anonymous self-reported survey research does not need formal approval as writing informed consent is implicit in answering the survey. The study was conducted in accordance with the Declaration of Helsinki and the general data protection regulations.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study by ticking a box in the instructions survey.
Data Availability Statement
The data presented in this study are available upon request from the corresponding authors. The data are publicly available in the University of Seville Research Repository (https://idus.us.es/).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ortega-Galán, Á.M.; Ruiz-Fernández, M.D.; Lirola, M.-J.; Ramos-Pichardo, J.D.; Ibáñez-Masero, O.; Cabrera-Troya, J.; Salinas-Pérez, V.; Gómez-Beltrán, P.A.; Fernández-Martínez, E. Professional Quality of Life and Perceived Stress in Health Professionals before COVID-19 in Spain: Primary and Hospital Care. Healthcare 2020, 8, 484. [Google Scholar] [CrossRef] [PubMed]
- Nuriye, C.; Mustafa, M. The Effect of Stress, Anxiety and Burnout Levels of Healthcare Professionals Caring for COVID-19 Patients on Their Quality of Life. Frontiers in Psychology 2020, 11. [Google Scholar] [CrossRef]
- Permarupan, P. Y., Al Mamun, A., Samy, N. K., Saufi, R. A., & Hayat, N. Predicting Nurses Burnout through Quality of Work Life and Psychological Empowerment: A Study Towards Sustainable Healthcare Services in Malaysia. Sustainability 2019, 12(1), 388. [CrossRef]
- Scheepers, R.A., van den Broek, T., Cramm, J.M. et al. Changes in work conditions and well-being among healthcare professionals in long-term care settings in the Netherlands during the COVID-19 pandemic: a longitudinal study. Hum Resource Health 2023, 21, 59. [CrossRef]
- Kandula UR, Wake AD. Assessment of Quality of Life Among Health Professionals During COVID-19: Review. J Multidiscip Healthc. 2021; 14:3571-3585. [CrossRef]
- oshi K, Modi B, Singhal S, Gupta S. Occupational Stress among Health Care Workers [Internet]. Identifying Occupational Stress and Coping Strategies. IntechOpen; 2023. [CrossRef]
- Barili, E., Bertoli, P., Grembi, V., & Rattini, V. Job satisfaction among healthcare workers in the aftermath of the COVID-19 pandemic. Plos One 2022. 17(10), e0275334. [CrossRef]
- Ge, J., He, J., Liu, Y. et al. Effects of effort-reward imbalance, job satisfaction, and work engagement on self-rated health among healthcare workers. BMC Public Health 2021, 21, 195. [CrossRef]
- Rieckert A, Schuit E, Bleijenberg N, et alHow can we build and maintain the resilience of our health care professionals during COVID-19? Recommendations based on a scoping review. BMJ Open 2021;11: e043718. [CrossRef]
- WHO, Building health systems resilience for universal health coverage and health security during the COVID-19 pandemic and beyond: WHO position paper. Geneva: World Health Organization; 2021 (WHO/UHL/PHCSP/2021.01). Licence: CC BY-NC-SA 3.0 IGO.
- OECD, Ready for the Next Crisis? Investing in Health System Resilience, OECD Health Policy Studies, OECD Publishing, Paris, 2023. [CrossRef]
- Ezura, M., Sawada, K., Takushi, Y., Matsui, H., Fukuda, Y., Nomura, K., & Asai, A. A systematic review of the characteristics of resilience training programs designed to improve resilience and mental health outcomes in physicians and nurses: What are we missing? Journal of Market Access & Health Policy 2023, 11(1), 2234139. [CrossRef]
- Schroeder, S., Kelly, D., & Leighton, K. Influence of years of experience and age on hospital workforce retention. Psychology, Health & Medicine 2023, 28(7), 1741-1754. [CrossRef]
- Pereira, H., Feher, G., Tibold, A., & Martins, C. Mediating Effect of Burnout on the Association Between Psychological Morbidity and Quality of Work Life Among Portuguese Medical Doctors. Brain Sciences 2021, 11(6), 813. 6. [CrossRef]
- Cohen, J. B., Reiser, V. L., Adelman, A. D., Carpenter, K. M., Hoerger, M., & Trevino, K. M. Burnout Among Oncology Nurses: The Effects of Palliative Care Education and Support. Clinical Journal of Oncology Nursing 2022, 26(4), 391-398. [CrossRef]
- Gillen, P., Neill, R. D., Mallett, J., McFetridge, B., Moriarty, J., Mairs, A., ..., & McKenna, H. Wellbeing and coping of UK nurses, midwives and allied health professionals during COVID-19. PloS One 2022, 17(9), e0274036. [CrossRef]
- Martins, M. V., Valente, V. A., Simões, A. D., & Gama, J. A. Death is a sensitive topic when you are surrounded by it: End-of-life care in obstetrics. Sexual & Reproductive Healthcare 2023, 35, 100817. [CrossRef]
- Yang Y, Hatanaka K, Takahashi K, Shimizu Y. Working Conditions Among Chinese Nurses Employed in Japan: A Cross-Sectional Survey-Based Study. SAGE Open Nursing. 2023;9. [CrossRef]
- Manzanares, I., Guerra, S. S., Mencía, M. L., Acar-Denizli, N., Salmerón, J. M., & Estalella, G. M. Impact of the COVID-19 pandemic on stress, resilience and depression in health professionals: A cross-sectional study. International Nursing Review 2021, 68(4), 461-470. [CrossRef]
- Yun, Z., Zhou, P., & Zhang, B. High-Performance Work Systems, Thriving at Work, and Job Burnout among Nurses in Chinese Public Hospitals: The Role of Resilience at Work. Healthcare (Basel, Switzerland) 2022, 10(10), 1935. [CrossRef]
- Miyazaki, A., Sankai, T., & Omiya, T. Experience and Resilience of Japanese Public Health Nurses during the COVID-19 Pandemic and Their Impact on Burnout. Healthcare (Basel, Switzerland) 2023, 11(8), 1114. [CrossRef]
- Rodríguez-Rey, R., Palacios, A., Alonso-Tapia, J., Pérez, E., Álvarez, E., Coca, A., Mencía, S., Marcos, A., Mayordomo-Colunga, J., Fernández, F., Gómez, F., Cruz, J., Ordóñez, O., & Llorente, A. Burnout and posttraumatic stress in paediatric critical care personnel: Prediction from resilience and coping styles. Australian Critical Care 2019, 32(1), 46–53. [CrossRef]
- Jiménez-Fernández, R., Corral-Liria, I., Trevissón-Redondo, B., Lopez-Lopez, D., & Losa-Iglesias, M. Burnout, resilience and psychological flexibility in frontline nurses during the acute phase of the COVID-19 pandemic (2020) in Madrid, Spain. Journal of Nursing Management 2022, 30(7), 2549-2556. [CrossRef]
- Luceño-Moreno, L., Talavera-Velasco, B., García-Albuerne, Y., & Martín-García, J. Symptoms of Posttraumatic Stress, Anxiety, Depression, Levels of Resilience and Burnout in Spanish Health Personnel during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health 2020, 17(15), 5514. [CrossRef]
- Luceño-Moreno, L., Talavera-Velasco, B., Vázquez-Estévez, D., & Martín-García, J. Mental Health, Burnout, and Resilience in Healthcare Professionals After the First Wave of COVID-19 Pandemic in Spain: A Longitudinal Study. Journal of Occupational and Environmental Medicine 2022, 64(3), e114–e123. [CrossRef]
- Castillo-González, A., Velando-Soriano, A., De La Fuente-Solana, E. I., Martos-Cabrera, B. M., Membrive-Jiménez, M. J., Lucía, B., & Cañadas-De La Fuente, G. A. Relation and effect of resilience on burnout in nurses: A literature review and meta-analysis. International Nursing Review 2023. [CrossRef]
- León-Pérez, J.M.; Antino, M. & León-Rubio, J.M. Adaptation of the short version of the Psychological Capital Questionnaire (PCQ-12) into Spanish / Adaptación al español de la versión reducida del Cuestionario de Capital Psicológico (PCQ-12), International Journal of Social Psychology 2017, 32:1, 196-213. [CrossRef]
- León-Pérez, J.M., Antino, M., & León-Rubio, J.M.. The Role of Psychological Capital and Intragroup Conflict on Employees' Burnout and Quality of Service: A Multilevel Approach. Frontiers in Psychology 2016, 7, 212663. [CrossRef]
- Wang, Q., Luan, Y., Liu, D., Dai, J., Wang, H., Zhang, Y., Wang, S., Dong, X., & Bi, H. Guided self-help mindfulness-based intervention for increasing psychological resilience and reducing job burnout in psychiatric nurses: A randomized controlled trial. International Journal of Nursing Practice 2023, e13204. [CrossRef]
- Moffatt-Bruce, S. D., Nguyen, M. C., Steinberg, B., Holliday, S., & Klatt, M.. Interventions to Reduce Burnout and Improve Resilience: Impact on a Health System's Outcomes. Clinical Obstetrics and Gynecology 2019, 62(3), 432–443. [CrossRef]
- Safaeian, A., Tavakolifard, N., & Roohi, A. Investigating the effectiveness of innovative intervention based on compassion, awareness, resilience, and empowerment on burnout in nurses of two educational hospitals in Isfahan. Journal of Education and Health Promotion 2022, 11, 65. [CrossRef]
- Strout, K., Schwartz-Mette, R., McNamara, J., Parsons, K., Walsh, D., Bonnet, J., O'Brien, L. M., Robinson, K., Sibley, S., Smith, A., Sapp, M., Sprague, L., Sabegh, N. S., Robinson, K., & Henderson, A. Wellness in Nursing Education to Promote Resilience and Reduce Burnout: Protocol for a Holistic Multidimensional Wellness Intervention and Longitudinal Research Study Design in Nursing Education. JMIR Research Protocols 2023, 12, e49020. [CrossRef]
- Ho, A. H., Ngo, T. A., Ong, G., Chong, P. H., Dignadice, D., & Potash, J. A Novel Mindful-Compassion Art-Based Therapy for Reducing Burnout and Promoting Resilience Among Healthcare Workers: Findings From a Waitlist Randomized Control Trial. Frontiers in Psychology 2021, 12, 744443. [CrossRef]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review 1977, 84(2), 191–215. [CrossRef]
- Molero Jurado, M. D., Oropesa Ruiz, N. F., Simón Márquez, M. D., & Gázquez Linares, J. J. Self-Efficacy and Emotional Intelligence as Predictors of Perceived Stress in Nursing Professionals. Medicina 2019, 55(6), 237. [CrossRef]
- Wu, Chao MMa; Ge, Yiling MBa; Xu, Chao MMa; Zhang, Xinyan MBb; Lang, Hongjuan MMa. A correlation study of emergency department nurses’ fatigue, perceived stress, social support, and self-efficacy in grade III A hospitals of Xi’an. Medicine 2020 99(32): p e21052, August 07, 2020. 07 August. [CrossRef]
- Janko, M. R., & Smeds, M. R.. Burnout, depression, perceived stress, and self-efficacy in vascular surgery trainees. Journal of Vascular Surgery 2018, 69(4), 1233-1242. [CrossRef]
- Smeds, M. R., Janko, M. R., Allen, S., Amankwah, K., Arnell, T., Ansari, P., Balters, M., Hess, D., Ferguson, E., Jackson, P., Kimbrough, M. K., Knight, D., Johnson, M., Porter, M., Shames, B. D., Schroll, R., Shelton, J., Sussman, J., & Yoo, P. Burnout and its relationship with perceived stress, self-efficacy, depression, social support, and programmatic factors in general surgery residents. The American Journal of Surgery 2020, 219(6), 907-912. [CrossRef]
- Firdausi, A. N., Fitryasary, R. I., Tristiana, D., Fauziningtyas, R., & Thomas, D. C. Self-efficacy and social support have relationship with academic burnout in college nursing students. Journal of the Pakistan Medical Association 2023, 73(02), S63-S66. [CrossRef]
- Bernales-Turpo, D., Quispe-Velasquez, R., Flores-Ticona, D., Saintila, J., Ruiz Mamani, P. G., Huancahuire-Vega, S., Morales-García, M., & Morales-García, W. C. Burnout, Professional Self-Efficacy, and Life Satisfaction as Predictors of Job Performance in Health Care Workers: The Mediating Role of Work Engagement. Journal of Primary Care & Community Health 2022. [CrossRef]
- Messerotti, A., Banchelli, F., Ferrari, S. et al. Investigating the association between physicians self-efficacy regarding communication skills and risk of “burnout”. Health Qual Life Outcomes 2020, 18, 271. [CrossRef]
- Chen, J., Li, J., Cao, B., Wang, F., Luo, L., & Xu, J. Mediating effects of self-efficacy, coping, burnout, and social support between job stress and mental health among young Chinese nurses. Journal of Advanced Nursing 2020, 76(1), 163-173. [CrossRef]
- Liu, M., Liu, L., Lv, Z., Ma, F., Mao, Y., & Liu, Y. Effects of burnout and work engagement in the relationship between self-efficacy and safety behaviours—A chained mediation modelling analysis. Journal of Advanced Nursing 2023. [CrossRef]
- He, W., Li, M., Ye, J., Shen, Y., Cao, Y., Zhou, S. & Han, X. Regulatory emotional self-efficacy as a mediator between high-performance work system perceived by nurses on their job burnout: a cross-sectional study, Psychology, Health & Medicine 2023, 28:3, 743-754. [CrossRef]
- Eurofound, Working conditions and sustainable work: An analysis using the job quality framework, Challenges and prospects in the EU series, Publications Office of the European Union, Luxembourg, 2021.
- Van Laar D, Edwards JA, Easton S. The Work-Related Quality of Life scale for healthcare workers. Journal of Advanced Nursing. 2007;60(3):325-333. [CrossRef]
- González-Rico, P.; Guerrero-Barona, E.; Chambel, M.J.; Guerrero-Molina, M. Well-Being at Work: Burnout and Engagement Profiles of University Workers. International Journal of Environmental Research and Public Health 2022, 19, 15436. [CrossRef]
- Falatah, R., & Alhalal, E. A structural equation model analysis of the association between work-related stress, burnout and job-related affective well-being among nurses in Saudi Arabia during the COVID-19 pandemic. Journal of Nursing Management 2022, 30(4), 892–900. [CrossRef]
- Bakker, A. B., Demerouti, E., & Sanz-Vergel, A. (2023). Job Demands–Resources Theory: Ten Years Later. Annual Review of Organizational Psychology and Organizational Behavior. 2023, 10, 25-53. [CrossRef]
- Chen, Y. C., Guo, Y. L., Chin, W. S., Cheng, N. Y., Ho, J. J., & Shiao, J. S. Patient-Nurse Ratio is Related to Nurses' Intention to Leave Their Job through Mediating Factors of Burnout and Job Dissatisfaction. International Journal of Environmental Research and Public Health 2019, 16(23), 4801. [CrossRef]
- Al Sabei, S. D., Labrague, L. J., Al-Rawajfah, O., AbuAlRub, R., Burney, I. A., & Jayapal, S. K. Relationship between interprofessional teamwork and nurses' intent to leave work: The mediating role of job satisfaction and burnout. Nursing Forum 2022, 57(4), 568–576. [CrossRef]
- Gong, S., Li, J., Tang, X., & Cao, X. Associations among professional quality of life dimensions, burnout, nursing practice environment, and turnover intention in newly graduated nurses. Worldviews on Evidence-Based Nursing 2022, 19(2), 138–148. [CrossRef]
- Foroughi Koldaer, Z., Akbari, B., & Asadi majreh, S. Structural model of the relationship between psychological capital and perceived social support with anxiety through mediation of burnout in female nurses. Medical Journal of Mashhad University of Medical Sciences 2021, 64(3), 3143-3153. [CrossRef]
- Chami-Malaeb, R. Relationship of perceived supervisor support, self-efficacy and turnover intention, the mediating role of burnout, Personnel Review 2022, Vol. 51 No. 3, pp. 1003-1019. [CrossRef]
- Kim, S. R., Park, O. L., Kim, H. Y., & Kim, J. Y. Factors influencing well-being in clinical nurses: A path analysis using a multi-mediation model. Journal of Clinical Nursing 2019, 28(23-24), 4549–4559. [CrossRef]
- Jarrar, M., Al-Bsheish, M., Albaker, W., Alsaad, I., Alkhalifa, E., Alnufaili, S., Almajed, N., Alhawaj, R., Al-Hariri, M. T., Alsunni, A. A., Aldhmadi, B. K., & Alumran, A. Hospital Work Conditions and the Mediation Role of Burnout: Residents and Practicing Physicians Reporting Adverse Events. Risk Management and Healthcare Policy 2023, 16, 1–13. [CrossRef]
- Yıldırım, N., Coşkun, H., & Polat, Ş. The Relationship Between Psychological Capital and the Occupational Psychologic Risks of Nurses: The Mediation Role of Compassion Satisfaction. Journal of Nursing Scholarship 2021, 53(1), 115–125. [CrossRef]
- 58. Lee LJ Lee LJ, Wehrlen L, Ding Y, Ross A. Professional quality of life, sleep disturbance and health among nurses: A mediation analysis. Nurs Open. 2022;9(6):2771-2780. [CrossRef]
- Shdaifat E, Al-Shdayfat N, Al-Ansari N. Professional Quality of Life, Work-Related Stress, and Job Satisfaction among Nurses in Saudi Arabia: A Structural Equation Modelling Approach. J Environ Public Health. 2023; 2023:2063212. Published 2023 Jan 31. [CrossRef]
- Marques-Pinto, A., Jesus, É. H., Mendes, A. M. O. C., Fronteira, I., & Roberto, M. S. Nurses' Intention to Leave the Organization: A Mediation Study of Professional Burnout and Engagement. The Spanish Journal of Psychology 2018, 21, E32. [CrossRef]
- Polat, Ş., Hamit, C., & Yıldırım, N. Multiple Mediation Role of Emotion Management and Burnout on the Relationship between Cognitive Flexibility and Turnover Intention among Clinical Nurses. International Journal of Caring Sciences September-December 2022 15(3), 1990-2000.
- Sun, J., Sarfraz, M., Ivascu, L., Iqbal, K., & Mansoor, A. How Did Work-Related Depression, Anxiety, and Stress Hamper Healthcare Employee Performance during COVID-19? The Mediating Role of Job Burnout and Mental Health. International Journal of Environmental Research and Public Health 2022, 19(16), 10359. [CrossRef]
- Jiang, M., Li, Z., Zheng, X., Liu, M., & Feng, Y. The influence of perceived stress of Chinese healthcare workers after the opening of COVID-19: the bidirectional mediation between mental health and job burnout. Frontiers in Public Health 2023, 11, 1252103. [CrossRef]
- Hernández, R., Fernández, C., & Baptista, P. [Research Methodology] Metodología de la investigación. México: Compañía, 2006.
- León Rubio, J.M. & Avargues Navarro, M.L. [Appendix E: Psychosocial risks] Anexo E: Riesgos Psicosociales. J.J. Moreno Hurtado (Coord.). Manual de Evaluación de Riesgos Laborales, Junta de Andalucía, Consejería de Empleo, Dirección General de Seguridad y Salud Laboral. 2005: 226-234.
- Warr P. The measurement of well-being and other aspects of mental health. Journal of Occupational Psychology 1990, 63, 193–210. [CrossRef]
- Warr P., Cook J. & Wall T. Scales for the measurement of some work attitudes and aspects of psychological well-being. Journal of Occupational Psychology 1979, 52, 129–148. [CrossRef]
- Schaufeli, W. B., Salanova, M., Gonzàlez-Romà, V., & Bakker, A. B. The measurement of burnout and engagement: A confirmative analytic approach. Journal of Happiness Studies. 2002, 3:71-92.
- Schaufeli, W. B., Martinez, I. M., Pinto, A. M., Salanova, M., & Bakker, A. B. Burnout and engagement in university students: A cross-national study. Journal of Cross-Cultural Psychology 2002, 33(5), 464-481. [CrossRef]
- Melamed S, Kushnir T, Shirom, A Burnout and risk factors for cardiovascular diseases. Behav Med 1992, 18:53-60. [CrossRef]
- SShirom, A., & Melamed, S. A comparison of the construct validity of two burnout measures in two groups of professionals. International Journal of Stress Management 2006, 13(2), 176. [CrossRef]
- Lundgren-Nilsson, Å., Jonsdottir, I. H., Pallant, J., & Ahlborg, G. Internal construct validity of the Shirom-Melamed Burnout questionnaire (SMBQ). BMC Public Health 2012, 12(1), 1. [CrossRef]
- Hobfoll, S. E. Conservation of resources: A new attempt at conceptualizing stress. American Psychologist 1989, 44, 513–524. [Google Scholar] [CrossRef] [PubMed]
- Hobfoll, S. E., & Shirom, A. Stress and burnout in work organizations. In R. T. Golembiewski (Ed.), Handbook of organization behavior (pp. 41–61). New York: Dekker, 1993.
- Hobfoll, S. E., & Shirom, A. Conservation of resources theory: Applications to stress and management in the workplace. In R. T. Golembiewski (Ed.), Handbook of organization behavior (2nd Rev. ed., pp. 57–81). New York: Dekker, 2000.
- Connor, K. M., & Davidson, J. R. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depress Anxiety 2003, 18(2), 76-82. [CrossRef]
- Bandura, A. Guide for constructing self-efficacy scales. F. Pajares & T. Urdan (eds.), Self-Efficacy Beliefs of Adolescents. IAP, 2006: 307-337.
- Hayes, A. F. Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. Guilford Publications, 2017.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



