
Submitted:
10 January 2024
Posted:
10 January 2024
You are already at the latest version
Abstract
Background: Inflammation is an important mechanism in atherosclerosis and plaque formation. C-reactive protein (CRP) is a common inflammatory biomarker associated with the risk of coro-nary heart disease. We investigated the relationship of CRP with findings from myocardial per-fusion imaging (MPI). Methods: In this retrospective study, 102 consecutive patients (mean age 71 years, 68% males) that underwent MPI (for diagnostic reasons or quantification of myocardial ischemia) and CRP determination (upper limit: 6mg/L) within 1 month from MPI, were included. Patients had no infection or recent acute coronary syndrome. Results: the median CRP level was 4mg/L (2,10) among the study population. Patients with raised CRP had higher summed stress score (SSS) (P = 0.006) and summed rest score (SRS) (P = 0.001) and higher risk for SSS > 3 (OR 9.25, 95% CI 2.03-42.13, P = 0.001) compared to those with low CRP. The association of SSS and SRS with CRP levels was more evident in patients over 70 years (P = 0.027 and P = 0.005 respectively). No significant difference in summed difference score was shown. The two groups had no difference in other risk factors (p > 0.05 for all comparisons). Conclusion: A high level of CRP was associated with the presence and extent of stress-induced myocardial ischemia in MPI.
Keywords:
C-reactive protein
; ischemia
; SPECT
; myocardial perfusion imaging
; cardiac imaging
1. Introduction
Coronary artery disease consists of the leading etiology of death suggesting that its effective management is pivotal to reduce morbidity and mortality [1]. In general, atherosclerosis is mainly responsible for cardiovascular disease, with atherosclerotic lesions affecting mainly the large and medium-sized elastic and muscular arteries [2,3]. Inflammation is an important part of the vascular atherosclerotic process, consisted of a slowly progressive inflammatory activity manifested by increasing serum inflammatory cytokines. Inflammatory cytokines, such as interleukin 6 (IL-6), stimulate the production of acute-phase reactants, including C-reactive protein (CRP) [4], an easily measured and most widely used biomarker for detecting an acute inflammatory process or for monitoring several chronic inflammatory conditions [5,6]. CRP is synthesized in the liver and may identify external pathogens and injured cells leading to activation of phagocytosis with subsequent removal of the pathogens and damaged cells. However, these processes could become pathologic due to abnormal stimulation of the immune system leading to activation of autoantibodies and complement system with inflammatory cytokines and further tissue damage [7,8,9].
In any event, cumulative evidence indicates that inflammation, at both focal and systemic levels, plays a role in disruption of atherosclerotic plaques and acute cardiovascular consequences [10]. CRP examination should be performed when there is an indication of either infection or an inflammatory process. Its evaluation in cardiovascular disease appears to be associated with altered CRP and increased cardiovascular risk [11,12,13]. Thus, recent studies are trying to elucidate if inflammatory biomarkers such as CRP may identify patients at risk for acute cardiovascular events for early treatment [14].
Apart from its rapid rise and involvement during an acute inflammatory process, indolent or modest but persistent increase of CRP or high sensitivity CRP (hs-CRP) has been correlated with the presence of coronary artery disease (CAD) and higher risk of future cardiovascular events in apparently healthy individual [5,15,16,17,18,19]. For example, an increased CRP even in stable coronary artery disease, was a significant predictor of harmful cardiovascular conditions independently on the specific therapeutic management [20]. In addition, high serum CRP level was associated with the presence, but not the degree of CAD in patients with stable angina [21]. Even though an elevated serum CRP level did not correlate with the degree of angiographic abnormalities in coronary arteries, it could possibly help discover new cases of coronary lesions in follow up examinations [22].
Myocardial perfusion imaging (MPI) with single photon emission tomography (SPECT), represents a non-invasive examination that plays a pivotal role in diagnosis of cardiac disease. This test obtains important information on myocardial perfusion and assesses viable or ischemic myocardial tissue in various conditions, such as angina, non-specific chest pain, outcome of therapeutic coronary interventions and overall prognosis. Current MPI reconstructs three-dimensional perfusion images of myocardial slices with discrete view of normal and abnormal areas for accurate detection of coronary artery disease [23].
MPI provides important information about the existence and severity of myocardial ischemia and macrovascular or microvascular CAD [23,24,25,26]. Two decades ago, Lombardi et al, in a small, interesting study, showed that high CRP levels might predict exercise induced MPI ischemia and patient’s outcome [27]. Stress tests were performed for evaluation of chest pain or after a myocardial infarction. In another small study, patients with angiographically coronary slow flow (possibly due to endothelial inflammation) had higher hs-CRP levels compared to controls (no slow flow). Moreover, in a proportion of patients with an MPI study, hs-CRP predicted positive MPI results [28]. However, data about the association of CRP with MPI findings are limited [27,28,29,30].
In the present study, we investigated the association of serum CRP levels with the presence and extent of ischemia detected after stress induced MPI SPECT, performed for diagnostic or prognostic reasons.
2. Methods
2.1. Study Population
In this retrospective single-center study, a thorough search of all patients that had MPIs performed in the Nuclear Medicine Department of our University Hospital from 1 January 2022 to 31 December 2022, and in addition had CRP measurements within one month before or after MPI. Patients were subjected to MPI SPECT study for diagnostic clinical reasons (suspected CAD) or prognostic (quantification of myocardial ischemia) reasons.
Exclusion criteria included presence of clinical signs or findings of infection, or recent (during the last 3 months before the MPI study) acute coronary syndrome (ST elevation acute myocardial infarction, non-ST elevation acute myocardial infarction, or unstable angina). Additionally, patients with a medical history of an immunologic disease were excluded from the study, unless they had stable disease (clinical remission) at the time of the CRP measurement.
2.2. Ethics
The protocol of this study was approved by the Hospital’s Clinical Research Committee. As this was a retrospective analysis of MPI SPECT data, no written patients’ consent was required by our Hospital’s Clinical Research Committee.
2.3. Study Protocol
The application of myocardial perfusion SPECT was performed according to the guidelines of the European Association of Nuclear Medicine (EANM) [31]. MPI SPECT procedure was explained in detail to the patients. The same data acquisition parameters were used in all patients. A single-day protocol was used, with stress and rest images acquired in that order, approximately two hours apart [32,33]. Medical history information involved symptoms, classic risk factors for CAD like smoking behavior, hypertension, diabetes mellitus, dyslipidemia, obesity (considered if body mass index was greater than or equal to 30 kg/m2), and family history of CAD, previous history of diagnosed cardiovascular disease and other health problems such as neurological diseases, rheumatological diseases, mental diseases, etc. Furthermore, detailed information was provided for their health status at the time of the examination.
Blood pressure and oxygen saturation was measured in all patients and a 12-lead electrocardiogram was acquired. Maximal or symptom-limited treadmill exercise (Bruce protocol) was selected for patients capable to perform physical exercise; otherwise, an intravenous dipyridamole (0.56 mg/kg body weight) stress was applied, either alone, or in combination with a single-stage 3-min Bruce treadmill exercise. All studies were performed with Technetium-99m tetrofosmin, an MPI radiopharmaceutical that was labeled in-house according to the manufacturer’s instructions.
2.4. Visual Analysis of Myocardial Perfusion SPECT
The recorded raw tomographic data under stress and rest were processed and reconstructed in the three planes (short axis, horizontal long axis, and vertical long axis) according to established algorithms and assessed by two experienced board-certified nuclear medicine physicians, using a 17-segment polar map as previously reported [34,35] in both stress and rest images. Each segment was scored with a scale of 0 to 4, depending on the degree of the perfusion deficit. Between the two readers, no serious inter-reader variability was seen. The differences were approximately +/- 2. A summed stress score (SSS) of over 3 was considered as myocardial ischemia [SSS corresponds to either stress-induced or resting perfusion defects (i.e., ischemia + infarct)]. Myocardial ischemia was mild for SSS 4 to 8, moderate for SSS 9 to 13, and high if SSS was above thirteen [36,37]. Summed rest score (SRS) corresponds to perfusion defects at rest indicating probable myocardial scar. Furthermore, the summed difference score (SDS = SSS – SRS), is an important measurement since it denotes the presence of reversibility after exercise or pharmacologic stress.
2.5. CRP Measurements
All enrolled subjects had a serum CRP value available within one month of the MPI SPECT. For CRP measurements the quantitative IMAGER 800 Immunochemistry System (Beckman Coulter, USA) was used, which applies rate nephelometry and performs a patented dynamic blanking algorithm for selected analytes; the upper limit for CRP in our Institution is 6mg/L.
2.6. Statistical Analysis
Continuous data are presented as mean+/-standard deviation or median values (interquartile range) while dichotomous data are presented as number (percentage). Comparisons between the two groups of patients (high vs low CRP) were made using the Fischer χ2 test for dichotomous variables and student’s t-test and Mann-Whitney U test for continuous variables. General Linear model analysis was used to detect potential interactions of CRP levels with other parameters and associations with SPECT findings. A two-tailed P - value < 0.05 was used to determine significant associations. All analyses were performed with the software IBM SPSS Statistics version 21 (IBM, Armonk, NY, USA).
3. Results
Within a year of search from the medical records of the Nuclear Medicine Department of our University Hospital, we retrieved MPIs of 102 patients (69 male). Our population characteristics are presented in Table 1.
Among them, 69 patients were subjected to an MPI scan due to non-specific cardiac symptoms (workup to rule out CAD). The mean age of all participants was 71 years, of whom 68% were males and 32% had a history of “obstructive” macrovascular CAD (confirmed with a previous coronary angiography). The prevalence of classical risk factors was 77% for hypertension, 39% for diabetes mellitus, 64% for dyslipidemia and 26% for smoking. Moreover, 26% of the population was obese and 38% had increased CRP values (> 6mg/L). The median value of CRP levels was 4mg/L (2mg/L, 10 mg/L) in the total population [2 (2,3) mg/L in the low CRP group versus 12 (9,23) mg/L in the high CRP group, p<0.001)].
SPECT study results revealed that 78% of the participants had a high summed stress score (SSS > 3) and 60% a high summed difference score (SDS > 1). Patients with increased CRP compared to patients with low CRP, had higher SSS (p = 0.006) and SRS (P = 0.001). In addition, a higher risk for increased SSS > 3 was noted in patients with increased CRP (OR 9.25, 95% CI 2.03, 42.13, P = 0.001). However, no differences were observed in the other studied clinical risk factors (P> 0.05 for all comparisons) between the two groups (Table 1).
Figure 1 shows stress-rest bull’s eye images of three patients. (A), shows a normal MPI (SSS=0), of a patient with normal CRP at 2 mg/L. (B) and (C), shows abnormal MPIs. The SSS in the second patient (B) was 19, SRS 17, and SDS 2, indicating severe myocardial ischemia with irreversible lesions. This patient had a high CRP of 24 mg/L. Finally, SSS of the third patient (C) was 15, SRS 5 and SDS 10 (severe myocardial ischemia, with good reversibility - green arrows), and CRP 11 mg/L.
The association of SSS and SRS with CRP levels was more evident in older patients, i.e.> 70 years old, P = 0.027 and P = 0.005 respectively for interaction with age (Figure 2). No significant difference in SDS was shown between patients with increased versus low CRP levels.
3. Discussion
Nuclear medicine is a medical specialty using radioactive isotopes for imaging and treatment, providing important disease information in several medical specialties including cardiology [37,38,39,40,41]. One of the most widely used methods in nuclear cardiology is MPI SPECT, that may be used either for diagnosis or prognosis of various heart conditions [23].
MPI SPECT represents a precision medicine tool able to accurately differentiate between normal and abnormal processes inside the heart [42,43]. Various radiotracers may be used for the MPI SPECT, such as technetium-99m tetrofosmin or technetium-99m sestamibi which are dispersed passively within the myocardium depending on its viability, and thallium-201, which is distributed actively within the myocardial cells. These radiotracers were injected, and pictures were taken both at rest and during stress provoked either by exercise or pharmacologically. In cases where the radiotracer uptake was normal during both at rest and exercise the examination was normal, denoting healthy myocardial tissue. When there was poor uptake post exercise and improving during rest the examination indicated a reversible perfusion defect. If the uptake was poor during both exercise and not improving at rest the examination indicated that the myocardial tissue was constantly injured such as after a myocardial infarction [23]. MPI, in addition to its detection of coronary artery disease, it can assess the myocardial status of patients with coronary microvascular dysfunction, which represents an abnormal vasoconstrictor/vasodilatory coronary capability [44,45].
CRP represents a greatly conserved plasma protein involved in the general reaction to an inflammatory process [46]. It is a highly conserved protein of five subunits that bind to phosphocholine in a Ca2+-dependent manner. It represents an acute phase plasma protein and a constituent of the acute phase response [47]. Recent evidence indicates that atherosclerosis is linked to vascular inflammation involving both innate and adaptive immune responses and mobilization of monocytes, macrophages, neutrophils, and lymphocytes [48]. A prospective study in 316 patients with STEMI managed with primary PCI, reported that the estimated CRP velocity, which is defined as the value of the first CRP measurement divided by the time from the patient’s first reported symptom, was associated with microvascular infarct pathology [49]. A strong relation was found between CRP and the future risk of a fatal or non-fatal coronary event. A 1-SD increase in the log-transformed value of CRP was associated with a remarkable 50% increase in coronary risk, and subjects in the highest quintile of the CRP distribution thus showed a 2.6-fold increase in their risk of a future coronary event [50].
In the current study, we studied the association of high levels of CRP and abnormal MPI. A significant association of impaired myocardial perfusion in SPECT imaging with prevalent inflammation (as assessed by increased CRP levels i.e.> 6 mg/L) was shown; this effect was more prominent in older patients (> 70 years old). Subclinical inflammation is an integral part of the atherosclerotic process and its progression and has been previously associated with increased risk for cardiovascular events [51,52]. Whether levels of inflammation may be related to the presence of myocardial ischemia in patients with symptoms suggestive of CAD is a matter of ongoing research. A limited number of studies have reported a significant positive association of inflammation with MPI SPECT ischemia findings, although not consistently [27,29,30].
In patients with symptomatic angina or history of myocardial infarction, stress-induced myocardial ischemia extent in SPECT was higher in case of increased CRP levels (approximately 5-fold increased risk); high CRP levels predicted both exercise-induce ischemia and outcome [27], while in stable CAD patients that underwent SPECT imaging and/or new regional wall motion abnormality on transthoracic echocardiography during mental stress each 1 mg/L increase in CRP was associated (in univariate logistic regression analysis) with a 20% higher risk of reversible perfusion defect/ischemia [53] and this relationship remained in multivariate analysis. The increasing risk for positive ischemic test across tertiles of CRP demonstrated a non-significant trend. However, we must take into account that non-cardiac stress related disorders may be associated with both higher inflammation markers (including CRP) and greater risk of cardiovascular diseases [54,55]. In high-risk asymptomatic outpatients (based on the European SCORE model) without known CAD, hs-CRP has been found to be an independent predictor of myocardial perfusion defects and has been suggested to be used as a criterion to guide myocardial SPECT imaging in asymptomatic patients [30], which also seems to apply for chronic kidney disease patients [56,57,58]. Majstorov et al showed that in patients with confirmed or suspected CAD, those patients with mild or moderate perfusion defects in SPECT had significantly higher CRP values (2.7 mg/L vs. 4.2 mg/L, p = 0.01) compared to patients with normal or near normal myocardial perfusion [59]. In contrast to these results, Rathcke et al. showed that in a population of patients with an intermediate risk of having CAD or with known history of CAD, those subjects with abnormal MPI had similar CRP levels with those with normal MPI [60]. Interleukin-6, YKL-40 and N-terminal fragment of the prohormone brain natriuretic peptide levels were significantly elevated in the group with abnormal MPI [6059]. Recently another index, the ratio of two inflammatory markers (CRP to albumin, CAR) was investigated for the prediction of ischemia. In multivariate analysis CAR showed the best capability to discriminate myocardial ischemia detected by MPI [61]. Finally, whether changes in inflammatory indices may result in changes in SPECT imaging is not known. However, results from the PLATO Trial have shown that one month after myocardial infarction, the degree of change (decrease) of hs-CRP is more pronounced in patients without obstructive compared to patients with obstructive CAD [62].
We found that the association of SSS and SRS with CRP levels was more evident in older (>70 years) patients. This may be explained by the higher risk of CAD in elderly population since age is the strongest risk factor related to CAD [63]. We could hypothesize that the possibility of this association to be significant is greater when the areas of ischemia in MPI are longer and more frequent. Regarding the validity of the method in the elderly, Rai et al. evaluated the optimal non-invasive stress tests in elderly patients [64]. In their meta-analysis, the test with the greater risk (abnormal compared to normal stress) of future cardiac events was found to be MPI. These results indicated that MPI accurately stratified risk in the elderly [65]. Moreover, a second hypothesis could be that our result is the effect of confounding bias. Baseline CRP or hs-CRP levels increase with ageing [65,66,67,68] and therefore, both higher levels of CRP and the presence of ischemia in MPI could be the consequences of ageing. In that case, it would be expected that MPI cannot have any prognostic value that is not truthful [64].
The predictive role of CRP has been also investigated in relation to other myocardial perfusion imaging modalities. In patients with microvascular dysfunction and cardiac syndrome X that underwent positron emission tomography, those who had CRP > 3mg/L had more severe impairment of coronary flow reserve (2.14 ± 0.33 vs. 3.16 ± 0.76; P = 0.001); furthermore, a negative correlation between CRP levels and coronary flow reserve (R = -0.49, P = 0.02) was shown [69]. In patients with typical angina pectoris without CAD, increased CRP levels were associated with an impaired myocardial perfusion reserve index following stimulation with intravenous adenosine and intracoronary acetylcholine in cardiac magnetic resonance [70].
According to the last published survey, the total number of myocardial perfusion scintigraphy studies in European countries was lower than ICAs during the same time-period [71,72]. Despite patients with positive result on MPI are significantly more likely to have obstructive CAD (as assessed by ICA) than those who did not undergo non-invasive testing, MPI is performed in only one out of four patients before elective ICA [73]. If we take into consideration that most (but not all) asymptomatic or stable CAD patients have a benign prognosis and they would be treated conservative [73], it is essential not only to increase MPI diagnostic yield, but also to find additional markers in combination with MPI results that they optimize the impact on prognosis of MPI. Can CRP or other inflammatory indices be used in combination with MPI for these purposes? Does combined testing (MPI and CRP) improve the probability of obstructive CAD? Would the addition of an inflammatory marker beyond MPI results help us to make a decision about performing or not angioplasty and stenting in an angiographically non-significant (or even significant) lesion? The hypothesis is that in patients with ischemia in MPI, inflammatory indices are higher if coronary artery plaque burden is higher in angiography or (even better) intravascular imaging. There are no data about this hypothesis and studies to address this area are needed. Nowadays, the invasive evaluation of ischemia by means of physiological assessment remain the gold standard for percutaneous coronary intervention decision-making [74], although it is still (as the MPI testing) underused in real life clinical practice [75,76].
3.1. Limitations
Our study was retrospective and included a limited number of variables in association with SPECT findings. CRP values were not acquired at the same day of the SPECT in most cases, but rather assessed in a close date to the exam. Furthermore, we did not use a hs-CRP assay which is the case in most of the previous epidemiological studies; hence results may be different in studies using different assays. Another important limitation is the fact that we did not have an invasive coronary angiography to associate CRP values with the existence and extension of CAD. Finally, we used the cut-off value of 6mg/L to distinguish patients with high or low CRP values. Although other values have been used (and patients with CRP levels between 3 and 6 mg/L are not considered as they have normal values from many investigators), other studies showed that this value may have the best prognostic value [77].
4. Conclusions
We investigated the association of serum CRP levels with MPI SPECT findings in a population of patients with suspected or stable CAD. A high level of CRP has been found to be associated with the presence and extent of stress induced myocardial ischemia in MPI SPECT. Larger prospective studies are needed to examine whether indices of subclinical inflammation add diagnostic value to an MPI SPECT study so that they would be part of a diagnostic work up for CAD.
Author Contributions
Conceptualization, C.S.K. and C.S.; methodology, A.K., P.K. and A.B.; Formal analysis, A.B.; Investigation, A.K.; Recourses, A.K. and P.K.; Writing—original draft preparation, A.R.; writing—review and editing, C.S. and C.S.K.; supervision, C.S., and C.S.K.; project administration, C.S.K. and C.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of the University Hospital of Ioannina (protocol code: 34; date of approval: 11 February 2021).
Informed Consent Statement
Patient consent was waived because, in retrospective studies, our Hospital’s Clinical Research Committee does not require written patient consent. Additionally, all the collected data were coded with no patient personal information provided, and thus no patient could be identified.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy issues.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; Isasi, C.R.; Jiménez, M.C.; Jordan, L.C.; Judd, S.E.; Lackland, D.; Lichtman, J.H.; Lisabeth, L.; Liu, S.; Longenecker, C.T.; Mackey, R.H.; Matsushita, K.; Mozaffarian, D.; Mussolino, M.E.; Nasir, K.; Neumar, R.W.; Palaniappan, L.; Pandey, D.K.; Thiagarajan, R.R.; Reeves, M.J.; Ritchey, M.; Rodriguez, C.J.; Roth, G.A.; Rosamond, W.D.; Sasson, C.; Towfighi, A.; Tsao, C.W.; Turner, M.B.; Virani, S.S.; Voeks, J.H.; Willey, J.Z.; Wilkins, J.T.; Wu, J.H.; Alger, H.M.; Wong, S.S.; Muntner, P. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2017 update: A Report From the American Heart Association. Circulation 2017, 135, e146-e603. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis — An Inflammatory Disease. N. Eng. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Stary, H.C.; Chandler, A.B.; Glagov, S.; Guyton, J.R.; Insull, W.; Rosenfeld, M.E.; Schaffer, S.A.; Schwartz, C.J.; Wagner, W.D.; Wissler, R.W. A definition of initial, fatty streak, and intermediate lesions of atherosclerosis. A report from the Committee on Vascular Lesions of the Council on Arteriosclerosis, American Heart Association. Circulation 1994, 89, 2462–2478. [Google Scholar] [CrossRef] [PubMed]
- Hansson, G.K. Inflammation, atherosclerosis, and coronary artery disease. N. Eng. J. Med. 2005, 352, 1685–1695. [Google Scholar] [CrossRef] [PubMed]
- Lapic, I.; Padoan, A.; Bozzato, D.; Plebani, M. Erythrocyte Sedimentation Rate and C-Reactive Protein in Acute Inflammation. Am J Clin Pathol. 2020, 153, 14–29. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; Kastelein, J.J.P.; Cornel, J.H.; Pais, P.; Pella, D.; Genest, J., Cifkova; Lorenzatti, A.; Forster, T.; Kobalava, Z.; Vida-Simiti, L.; Flather, M.; Shimokawa, H.; Ogawa, H.; Dellborg, M.; Rossi, P.R.F.; Troquay, R.P.T.; Libby, P.; Glynn, R.J.; CANTOS Trial Group. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Cleland, D.A.; Eranki, A.P. StatPearls [Internet]; Stat Pearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Jungen, M.J.; Ter Meulen, B.C.; van Osch, T.; Weinstein, H.C.; Ostelo, R.W.J.G. Inflammatory biomarkers in patients with sciatica: a systematic review. BMC Musculoskelet Disord. 2019, 20, 156. [Google Scholar] [CrossRef] [PubMed]
- Kramer, N.E.; Cosgrove, V.E.; Dunlap, K.; Subramaniapillai, M.; McIntyre, R.S.; Suppes, T. A clinical model for identifying an inflammatory phenotype in mood disorders. J. Psychiatr. Res. 2019, 113, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Madjid, M.; Willerson, J.T. Inflammatory markers in coronary heart disease. Br. Med. Bull. 2011, 100, 23–38. [Google Scholar] [CrossRef]
- Eschborn, S.; Weitkamp, J.H. Procalcitonin versus C-reactive protein: review of kinetics and performance for diagnosis of neonatal sepsis. J. Perinatol. 2019, 39, 893–903. [Google Scholar] [CrossRef]
- Darooghegi Mofrad, M.; Milajerdi, A.; Koohdani, F.; Surkan, P.J.; Azadbakht, L. Garlic Supplementation Reduces Circulating C-reactive Protein, Tumor Necrosis Factor, and Interleukin-6 in Adults: A Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Nutr. 2019, 149, 605–618. [Google Scholar] [CrossRef] [PubMed]
- Dick, A.G.; Magill, N.; White, T.C.H.; Kokkinakis, M.; Norman-Taylor, F. C-reactive protein: what to expect after bony hip surgery for nonambulatory children and adolescents with cerebral palsy. J. Pediatr. Orthop. B. 2019, 28, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Calabro, P.; Golia, E.; Yeh, E.T. Role of C-reactive protein in acute myocardial infarction and stroke: possible therapeutic approaches. Curr. Pharm. Biotechnol. 2012, 13, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Black, S.; Kushner, I.; Samols, D. C-reactive Protein. J. Biol. Chem. 2004, 279, 48487–48490. [Google Scholar] [CrossRef] [PubMed]
- Emerging Risk Factors Collaboration; Kaptoge, S.; Di Angelantonio, E.; Lowe, G.; Pepys, M.B.; Thompson, S.G.; Collins, R.; Danesh, J. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis. Lancet 2010, 375, 375–140. [Google Scholar]
- Jan, M.I.; Khan, R.A.; Fozia, Ahmad, I.; Khan, N.; Urooj, K.; Shah, A.U.H.A.; Khan, A.U.; Ali, T.; Ishtiaq, A.; Shah, M.; Ullah, A.; Murtaza, I.; Ullah, R.; Alotaibi, A.; Murthy, H.C.A. C-Reactive Protein and High-Sensitive Cardiac Troponins Correlate with Oxidative Stress in Valvular Heart Disease Patients. Oxid. Med. Cell Longev. 2022, 2022, 5029853. [Google Scholar] [CrossRef] [PubMed]
- Casas, J.P.; Shah, T.; Hingorani, A.D.; Danesh, J.; Pepys, M.B. C-reactive protein and coronary heart disease: a critical review. J. Intern. Med. 2008. [Google Scholar] [CrossRef]
- Yousuf, O.; Mohanty, B.D.; Martin, S.S.; Joshi, P.H.; Blaha, M.J.; Nasir, K.; Blumenthal, R.S.; Budoff, M.J. High-sensitivity C-reactive protein and cardiovascular disease: a resolute belief or an elusive link? J. Am. Coll Cardiol. 2013, 62, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Sabatine, M.S.; Morrow, D.A.; Jablonski, K.A.; Rice, M.M.; Warnica, J.W.; Domanski, M.J.; Hsia, J.; Gersh, B.J.; Rifai, N.; Ridker, P.M.; Pfeffer, M.A.; Braunwald, E.; PEACE Investigators. Prognostic significance of the Centers for Disease Control/American Heart Association high-sensitivity C-reactive protein cut points for cardiovascular and other outcomes in patients with stable coronary artery disease. Circulation 2007, 115, 1528–1536. [Google Scholar] [CrossRef] [PubMed]
- Younan, H.; Al-Khashab, K. Correlation of high sensitivity C-reactive protein to presence, extent and severity of angiographic coronary artery disease in patients with chronic stable angina. Egypt Heart J. 2008, 60, 53–60. [Google Scholar]
- Razban, M.M.; Eslami, M.; Bagherzadeh, A. The relationship between serum levels of hs-CRP and coronary lesion severity. Clujul Med. 2016, 89, 322–6. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.J.; Alzahrani, T. Myocardial Perfusion Scan. In: StatPearls [Internet] Treasure Island (FL), 2023, StatPearls Publishing 2023.
- Sioka, C.; Nikas, D.; Tsoumani, A.; Kiortsis, D.N.; Fotopoulos, A.; Kostadima, V. Transient myocardial ischemia due to corticosteroid use in a patient with multiple sclerosis diagnosed with myocardial perfusion imaging. J. Nucl. Cardiol. 2021, 28, 1805–1808. [Google Scholar] [CrossRef] [PubMed]
- Kotsalou, I.; Georgoulias, P.; Karydas, I.; Fourlis, S.; Sioka, C.; Zoumboulidis, A.; Demakopoulos, N. A rare case of myocardial infarction and ischemia in a cannabis-addicted patient. Clin. Nucl. Med. 2007, 32, 130–131. [Google Scholar] [CrossRef]
- Sioka, C.; Papadimitropoulos, K.; Michalis, L.; Pappas, K.; Lakkas, L.; Fotopoulos, A.; Dounousi, E. Myocardial ischemia with normal coronary angiography in a chronic kidney disease patient. Cardiol. J. 2019, 26, 620–621. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, F.; Tundo, F.; Terranova, P.; Battezzati, P.M.; Ramella, M.; Bestetti, A.; Tagliabue, L. Prognostic value of C-reactive protein in patients with stress induced myocardial ischemia. Int. J. Cardiol. 2005, 98, 313–317. [Google Scholar] [CrossRef]
- Yurtdas, M.; Yaylali, Y.T.; Kaya, Y.; Ozdemir, M. Increased plasma high-sensitivity C-reactive protein and myeloperoxidase levels may predict ischemia during myocardial perfusion imaging in slow coronary flow. Arch. Med. Res. 2014, 45, 63–69. [Google Scholar] [CrossRef]
- Fleming, R.M.; Harrington, G.M. What is the relationship between myocardial perfusion imaging and coronary artery disease risk factors and markers of inflammation? Angiology 2008, 59, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Mitevska, I.; Srbinovska, E.; Stojanovska, L.; Antova, E.; Apostolopoulos, V.; Bosevski, M. Single-Photon Emission Computed Tomography Myocardial Ischemia Detection in High-Risk Asymptomatic Patients: Correlation with Coronary Calcium Score and High-Sensitivity C-Reactive Protein. Indian J. Nuc. Med. 2019, 34, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Verberne, H.J.; Acampa, W.; Anagnostopoulos, C.; Ballinger, J.; Bengel, F.; De Bondt, P.; Buechel, R.R.; Cuocolo, A.; van Eck-Smit, B.L.; Flotats, A.; Hacker, M.; Hindorf, C.; Kaufmann, P.A.; Lindner, O.; Ljungberg, M.; Lonsdale, M.; Manrique, A.; Minarik, D.; Scholte, A.J.; Slart, R.H.; Trägårdh, E.; de Wit, T.C.; Hesse, B.; European Association of Nuclear Medicine (EANM). EANM procedural guidelines for radionuclide myocardial perfusion imaging with SPECT and SPECT/CT: 2015 revision. Eur. J. Nucl. Med. Mol. Imaging, 2015; 42, 1929–1940. [Google Scholar]
- Sioka, C.; Moulias, C.; Voulgari, P.V.; Fotopoulos, A.; Bassukas, I.D. Single photon emission computed tomography myocardial perfusion imaging in patients with moderate to severe psoriasis. Nucl. Med. Rev. Cent. East Eur. 2021, 24, 46–50. [Google Scholar] [CrossRef]
- Fotopoulos, A.; Papadimitropoulos, K.; Papadopoulos, A.; Lakkas, L.; Spiliotopoulou, M.; Kotrotsios, T.D., Pappas; Notopoulos, A.; Sioka, C. Myocardial ischemia in female patients with rheumatoid arthritis assessed with single photon emission tomography-myocardial perfusion imaging. Nucl. Med. Rev. Cent. East Eur. 2019, 22, 8–13. [Google Scholar]
- Fotopoulos, A.; Petrikis, P.; Iakovou, I.; Papadopoulos, A.; Sakelariou, K.; Gkika, E.; Lakkas, L.; Touzios, C. The impact of depression and anxiety in prognosis of patients undergoing myocardial perfusion imaging with 99mTc tetrofosmin SPECT for evaluation of possible myocardial ischemia. Nucl. Med. Rev. Cent. East Eur. 2020, 23, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Batsi, C.; Gkika, E.; Astrakas, L.; Papadopoulos, A.; Iakovou, I.; Dogoritis, A.; Fotopoulos, A.; Sioka, C. Vitamin D Deficiency as a Risk Factor for Myocardial Ischemia. Medicina 2021, 57, 774. [Google Scholar] [CrossRef] [PubMed]
- Sioka, C.; Zotou, P.; Papafaklis, M.I.; Bechlioulis, A.; Sakellariou, K.; Rammos, A.; Gkika, E.; Lakkas, L.; Alexiou, S.; Kekiopoulos, P.; Naka, K.K.; Katsouras, C. Body Mass Index Is Independently Associated with the Presence of Ischemia in Myocardial Perfusion Imaging. Medicina 2022, 58, 987. [Google Scholar] [CrossRef] [PubMed]
- Bairactaris, C.; Demakopoulos, N.; Tripsianis, G.; Sioka, C.; Farmakiotis, D.; Vadikolias, K.; Heliopoulos, I.; Georgoulias, P.; Tsougos, I.; Papanastasiou, I.; Piperidou, C. Impact of dopamine transporter single photon emission computed tomography imaging using I-123 ioflupane on diagnoses of patients with parkinsonian syndromes. J. Clin. Neurosci. 2009, 16, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Sioka, C.; Assimakopoulos, A.; Fotopoulos, A. The diagnostic role of (18)F fluorodeoxyglucose positron emission tomography in patients with fever of unknown origin. Eur. J. Clin. Invest. 2015, 45, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Sioka, C.; Fotopoulos, A.; Kyritsis, A.P. Paraneoplastic neurological syndromes and the role of PET imaging. Oncology 2010, 78, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Tsiambas, E.; Fotiades, P.P.; Sioka, C.; Kotrotsios, D.; Gkika, E.; Fotopoulos, A.; Mastronikolis, S.N.; Armata, I.E.; Giotakis, E.; Ragos, V. Novel molecular and metabolic aspects in osteosarcoma. J. BUON. 2017, 22, 1595–1598. [Google Scholar] [PubMed]
- Lakkas, L.; Serim, B.D.; Fotopoulos, A.; Iakovou, I.; Doumas, A.; Korkmaz, U.; Michalis, L.K.; Sioka, C. Infection of cardiac prosthetic valves and implantable electronic devices: early diagnosis and treatment. Acta. Cardiol. 2021, 76, 569–575. [Google Scholar] [CrossRef]
- Giardino, A.; Gupta, S.; Olson, E.; Sepulveda, K.; Lenchik, L.; Ivanidze, J.; Rakow-Penner, R.; Patel, M.J.; Subramaniam, R.M.; Ganeshan, D. Role of imaging in the era of precision medicine. Acad. Radiol. 2017, 24, 639–649. [Google Scholar] [CrossRef]
- Sheikh, A. Evolution of Quantification in clinical nuclear medicine: A brief overview of salient uses and upcoming trends. J. Nucl. Med. Radiat. Ther. 2018, 9, 05. [Google Scholar] [CrossRef]
- Markoula, S.; Tsoumani, A.; Votti, C.A.; Beltsiou, M.; Lakkas, L.; Pappas, K.; Iakovou, I.; Fotopoulos, A.; Kyritsis, A.P.; Sioka, C. Myocardial perfusion imaging single photon emission computed tomography may detect silent myocardial ischemia in patient with epilepsy. Nucl. Med. Rev. Cent. East Eur. 2022, 25, 105–111. [Google Scholar] [CrossRef]
- Sioka, C.; Georgiou, G.; Katsouras, C.; Pappas, K.; Kiortsis, D.N.; Fotopoulos, A.; Petrikis, P. Silent severe myocardial ischemia in a past illicit drug user imaged with myocardial perfusion scintigraphy. Perfusion 2022, 37, 863–865. [Google Scholar] [CrossRef] [PubMed]
- Black, S.; Kushner, I.; Samols, D. C-reactive Protein. J. Biol. Chem. 2004, 279, 48487–48490. [Google Scholar] [CrossRef] [PubMed]
- Pathak, A.; Agrawal, A. Evolution of C-Reactive Protein. Front. Immunol. 2019, 30, 943. [Google Scholar] [CrossRef] [PubMed]
- Moriya, J. Critical roles of inflammation in atherosclerosis. J. Cardiol. 2019, 73, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Holzknecht, M.; Tiller, C.; Reindl, M.; Lechner, I.; Troger, F.; Hosp, M.; Mayr, A.; Brenner, C.; Klug, G.; Bauer, A.; Metzler, B.; Reinstadler, S.J. C-reactive protein velocity predicts microvascular pathology after acute ST-elevation myocardial infarction. Int. J. Cardiol 2021, 1, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Koenig, W.; Sund, M.; Frohlich, M.; Fischer, H.G.; Lowel, H.; Döring, A.; Hutchinson, W.L.; Pepys, M.B. C-Reactive protein, a sensitive marker of inflammation, predicts future risk of coronary heart disease in initially healthy middle-aged men: results from the MONICA (Monitoring Trends and Determinants in Cardiovascular Disease) Augsburg Cohort Study, 1984 to 1992. Circulation 1999, 99, 237–242. [Google Scholar] [PubMed]
- Shah, P.K.; Lecis, D. Inflammation in atherosclerotic cardiovascular disease. F1000Res. 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Toth, P.P. Subclinical atherosclerosis: what it is, what it means and what we can do about it. Int. J. Clin. Pract. 2008, 62, 1246–1254. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Burg, M.M.; Vashist, A.; Collins, D.; Liu, J.; Jadbabaie, F.; Graeber, B.; Earley, C.; Lampert, R.; Soufer, R. C-reactive protein and vulnerability to mental stress-induced myocardial ischemia. Mol. Med. 2006, 12, 269–274. [Google Scholar] [CrossRef]
- Kennedy, E.; Niedzwiedz, C.L. The association of anxiety and stress-related disorders with C-reactive protein (CRP) within UK Biobank. Brain Behav. Immun. Health. 2012, 19, 100410. [Google Scholar] [CrossRef]
- Song, H.; Fang, F.; Arnberg, F.K.; Mataix-Cols, D.; Fernández de la Cruz, L.; Almqvist, C.; Fall, K.; Lichtenstein, P.; Thorgeirsson, G.; Valdimarsdóttir, U.A. Stress related disorders and risk of cardiovascular disease: population based, sibling controlled cohort study. BMJ 2019, 365, l1255. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.B.; Lee, S.K.; Park, J.S.; Moon, D.H. Prevalence of coronary artery disease using thallium-201 single photon emission computed tomography among patients newly undergoing chronic peritoneal dialysis and its association with mortality. Ame J. Nephrol. 2004, 24, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, S.; Kawano, Y.; Nakajima, K.; Hase, H.; Joki, N.; Hatta, T.; Nishimura, S.; Moroi, M.; Nakagawa, S.; Kasai, T.; Kusuoka, H.; Takeishi, Y.; Momose, M.; Takehana, K.; Nanasato, M.; Yoda, S.; Nishina, H.; Matsumoto, N.; Nishimura, T. Prognostic study of cardiac events in Japanese patients with chronic kidney disease using ECG-gated myocardial Perfusion imaging: Final 3-year report of the J-ACCESS 3 study. J. Nuc. Cardiol. 2019, 26, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.B.; Min, W.K.; Lee, S.K.; Park, J.S.; Hong, C.D.; Yang, W.S. Persistent elevation of C-reactive protein and ischemic heart disease in patients with continuous ambulatory peritoneal dialysis. Am. J. Kidney Dis. 2002, 39, 342–346. [Google Scholar] [CrossRef] [PubMed]
- Majstorov, V.; Pop Gjorceva, D.; Vaskova, O.; Vavlukis, M.; Peovska, I.; Maksimovic, J.; Kuzmanovska, S.; Zdraveska-Kocovska, M. C-reactive protein in patients with normal perfusion and mild to moderate perfusion defects who have undergone myocardial perfusion imaging with 99m-Tc sestamibi gated spect. Prilozi 2008, 29, 67–76. [Google Scholar] [PubMed]
- Rathcke, C.N.; Kjøller, E.; Fogh-Andersen, N.; Zerahn, B.; Vestergaard, H. NT-proBNP and circulating inflammation markers in prediction of a normal myocardial scintigraphy in patients with symptoms of coronary artery disease. PLoS One. 2010, 5, e14196. [Google Scholar] [CrossRef]
- Efe, S.Ç.; Özdemir Candan, Ö.; Gündoğan, C.; Öz, A.; Yüksel, Y.; Ayca, B.; Çermik, T.F. Value of C-reactive Protein/Albumin Ratio for Predicting Ischemia in Myocardial Perfusion Scintigraphy. Mol. Imaging Radionucl. Ther. 2020, 29, 112–117. [Google Scholar] [CrossRef]
- Hjort, M.; Eggers, K.M.; Lakic, T.G.; Lindbäck, J.; Budaj, A.; Cornel, J.H.; Giannitsis, E.; Katus, H.A.; Siegbahn, A.; Storey, R.F.; Becker, R.C.; Wallentin, L.; Lindahl, B. Biomarker Concentrations and Their Temporal Changes in Patients with Myocardial Infarction and Nonobstructive Compared With Obstructive Coronary Arteries: Results From the PLATO Trial. J. Am. Heart Assoc, 2023; 12, e027466. [Google Scholar]
- Rodgers, J.L.; Jones, J.; Bolleddu, S.I.; Vanthenapalli, S.; Rodgers, L.E.; Shah, K.; Karia, K.; Panguluri, S.K. Cardiovascular Risks Associated with Gender and Aging. J. Cardiovasc. Dev. Dis. 2019, 6, 19. [Google Scholar] [CrossRef]
- Rai, M.; Baker, W.L.; Parker, M.W.; Heller, G.V. Meta-analysis of optimal risk stratification in patients >65 years of age. Am. J. Cardiol. 2012, 110, 1092–1099. [Google Scholar] [CrossRef]
- Singh, T.; Newman, A.B. Inflammatory markers in population studies of aging. Ageing Res. Rev. 2011, 10, 319–329. [Google Scholar] [CrossRef]
- Tang, Y.; Fung, E.; Xu, A.; Lan, H.Y. C-reactive protein and ageing. Clin. Exp. Pharmacol. Physiol. 2017, 44 (Suppl. 1), 9–14. [Google Scholar] [CrossRef]
- Tang, Y.; Liang, P.; Chen, J.; Fu, S.; Liu, B.; Feng, M.; Lin, B.; Lee, B.; Xu, A.; Lan, H.Y. The baseline levels and risk factors for high-sensitive C-reactive protein in Chinese healthy population. Immun. Ageing 2018, 15, 21. [Google Scholar] [CrossRef] [PubMed]
- de Almeida Roediger, M.; de Fátima Nunes Marucci, M.; Duim, E.L.; Santos, J.L.F.; de Oliveira Duarte, Y.A.; de Oliveira, C. Inflammation and quality of life in later life: findings from the health, well-being and aging study (SABE). Health Qual. Life Outcomes 2019, 17, 26. [Google Scholar] [CrossRef]
- Recio-Mayoral, A.; Rimoldi, O.E.; Camici, P.G.; Kaski, J.C. Inflammation and microvascular dysfunction in cardiac syndrome X patients without conventional risk factors for coronary artery disease. JACC Cardiovasc. Iimaging 2013, 6, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Wöhrle, J.; Nusser, T.; Merkle, N.; Kestler, H.A.; Grebe, O.C.; Marx, N.; Höher, M.; Kochs, M.; Hombach, V. Myocardial perfusion reserve in cardiovascular magnetic resonance: Correlation to coronary microvascular dysfunction. J. Cardiovasc. Magn Reson. 2006, 8, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Reyes, E.; Wiener, S.; Underwood, S.R.; European Council of Nuclear Cardiology. Myocardial perfusion scintigraphy in Europe 2007: a survey of the European Council of Nuclear Cardiology. Eur. J. Nucl. Med. Mol. Imaging, 2012; 39, 160–164. [Google Scholar]
- Cook, S.; Walker, A.; Hügli, O.; Togni, M.; Meier, B. Percutaneous coronary interventions in Europe: prevalence, numerical estimates, and projections based on data up to 2004. Clin. Res. Cardiol. 2007, 96, 375–382. [Google Scholar] [CrossRef]
- Buechel, R.R.; Kaufmann, B.A.; Tobler, D.; Wild, D.; Zellweger, M.J. Non-invasive nuclear myocardial perfusion imaging improves the diagnostic yield of invasive coronary angiography. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 842–847. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; Agewall, S.; Dickstein, K.; Edvardsen, T.; Escaned, J.; Gersh, B.J.; Svitil, P.; Gilard, M.; Hasdai, D.; Hatala, R.; Mahfoud, F.; Masip, J.; Muneretto, C.; Valgimigli, M.; Achenbach, S.; Bax, J.J.; ESC Scientific Document Group. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Toth, G.; Johnson, G.; Wijns, N.P.; Toth, B.; Achim, A.; Fournier, S.; Barbato, E. Revascularization decisions in patients with chronic coronary syndromes: Results of the second International Survey on Interventional Strategy (ISIS-2). Int. J. Cardiol. 2021, 336, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Achim, A.; Leibundgut, G. FAME 3 fails to defame coronary artery bypass grafting: what went wrong in the percutaneous coronary intervention arm? Eur. J. Cardiothorac. Surg. 2022, 62, ezac036. [Google Scholar] [CrossRef] [PubMed]
- Bian, J.; Guo, S.; Huang, T.; Li, X.; Zhao, S.; Chu, Z.; Li, Z. CRP as a potential predictor of outcome in acute ischemic stroke. Biomed. Rep. 2023, 18, 17. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Three patients with different stress-rest Bull’s eyes MPIs are depicted. (A), normal MPI and normal CRP; (B), abnormal MPI and high CRP; (C), abnormal MPI and high CRP; Black arrows shows defects; Green arrowheads shows reversible defects. MPI: Myocardial Perfusion Imaging; SSS: Summed Stress Score; SRS: Summed Rest Score; SDS: Summed Difference Score; CRP: C-Reactive Protein.
Figure 1.
Three patients with different stress-rest Bull’s eyes MPIs are depicted. (A), normal MPI and normal CRP; (B), abnormal MPI and high CRP; (C), abnormal MPI and high CRP; Black arrows shows defects; Green arrowheads shows reversible defects. MPI: Myocardial Perfusion Imaging; SSS: Summed Stress Score; SRS: Summed Rest Score; SDS: Summed Difference Score; CRP: C-Reactive Protein.
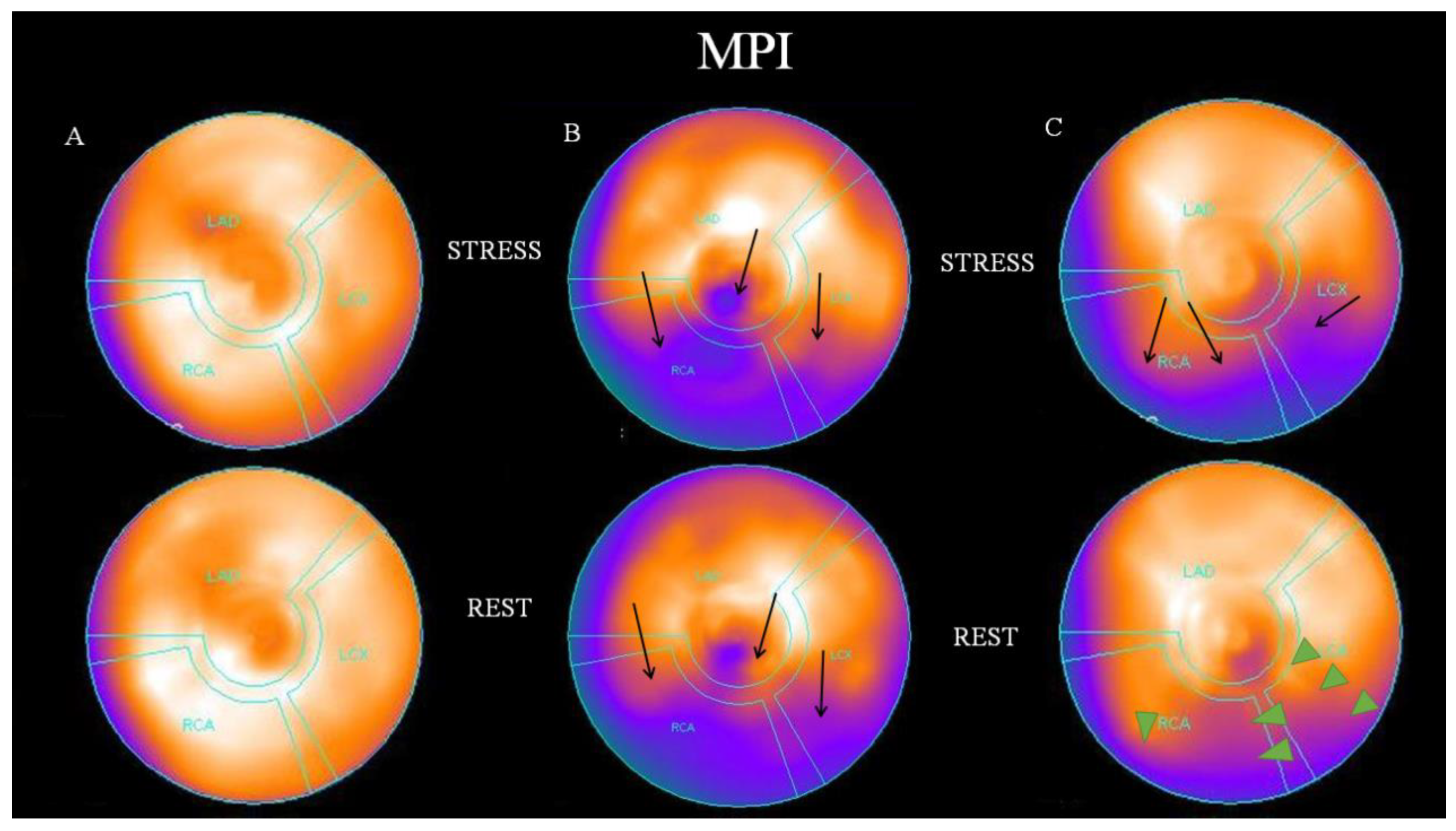
Figure 2.
Upper left: High CRP is associated with a higher SSS (p=0.006) in overall population. Upper right: High CRP is associated with a higher SRS (p=0.001) in overall population. Lower left: The correlation of increased CRP with a higher SSS (p=0.027) is more evident in patients older than 70 years old. Lower right: The correlation of increased CRP with a higher SRS (p=0.005) is more evident in patients older than 70 years old. SSS=Summed Stress Score SRS=Summed Rest Score.
Figure 2.
Upper left: High CRP is associated with a higher SSS (p=0.006) in overall population. Upper right: High CRP is associated with a higher SRS (p=0.001) in overall population. Lower left: The correlation of increased CRP with a higher SSS (p=0.027) is more evident in patients older than 70 years old. Lower right: The correlation of increased CRP with a higher SRS (p=0.005) is more evident in patients older than 70 years old. SSS=Summed Stress Score SRS=Summed Rest Score.
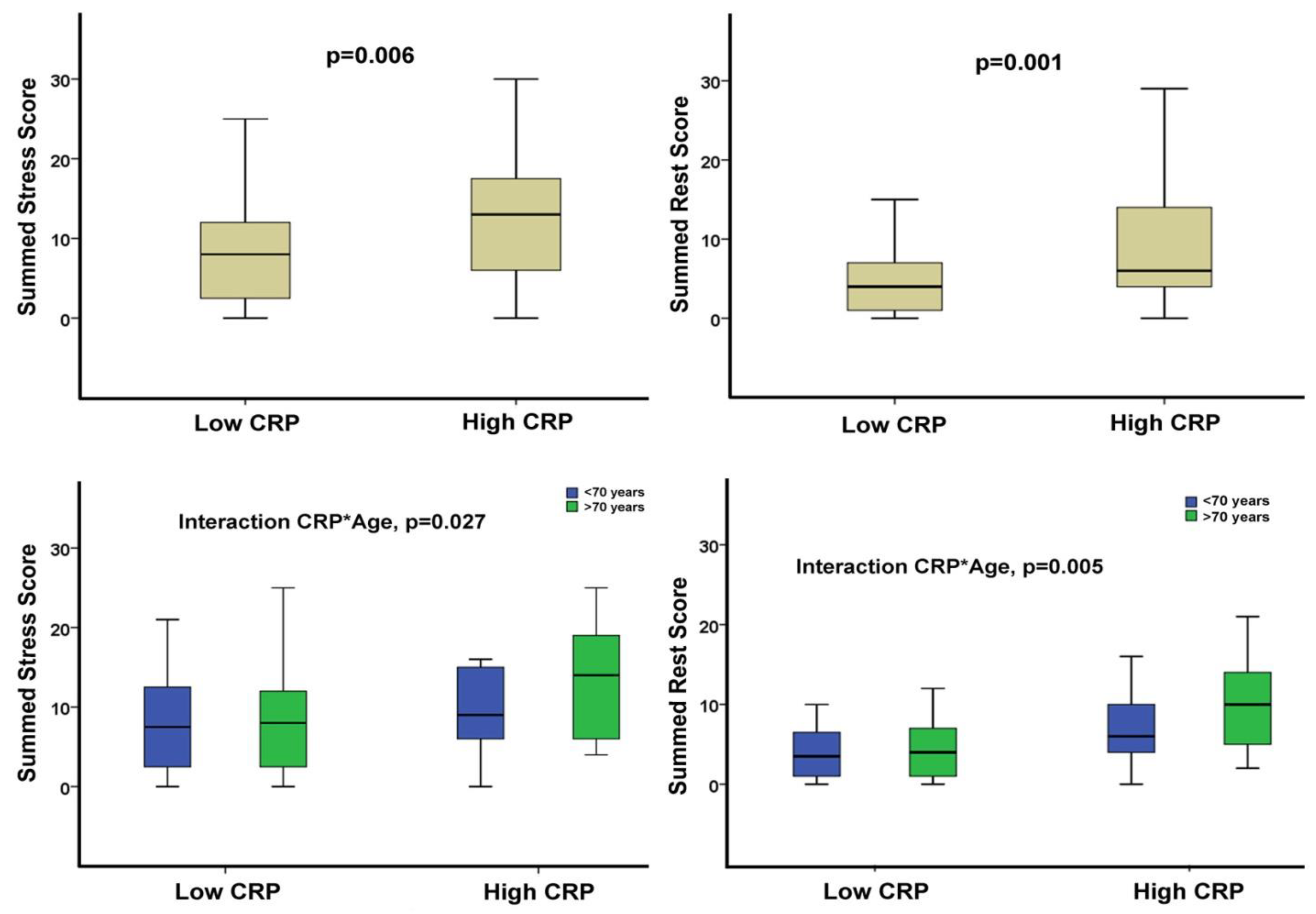

Table 1.
Population characteristics and association of CRP levels with various variables.
| Total populationN=102 | CRP ≤ 6 mg/LN=63 | CRP > 6 mg/LN=39 | P value | |
|---|---|---|---|---|
| Age, yrs | 71±11 | 69±11 | 72±11 | 0.189 |
| Male gender, n (%) | 69 (68) | 40 (64) | 29 (74) | 0.254 |
| CAD Hx, n (%) | 33 (32) | 21 (33) | 12 (31) | 0.788 |
| Hypertension, n (%) | 78 (77) | 50 (79) | 28 (72) | 0.381 |
| DM, (%) | 40 (39) | 24 (38) | 16 (41) | 0.768 |
| Dyslipidemia, n (%) | 65 (64) | 42 (67) | 23 (59) | 0.432 |
| Obesity, (%) | 26 (26) | 16 (25) | 10 (26) | 0.978 |
| Smoking (%) | 26 (26) | 16 (25) | 10 (26) | 0.978 |
| SSS | 8 (4, 15) | 8 (2, 12) | 13 (6, 18) | 0.006 |
| SRS | 5 (2, 9) | 4 (1, 7) | 6 (4, 14) | 0.001 |
| SDS | 2 (1, 6) | 2 (0, 5) | 3 (1, 6) | 0.703 |
| SSS>3 | 79 (78) | 42 (67) | 37 (95) | 0.001 |
| SDS>1 | 61 (60) | 37 (59) | 24 (62) | 0.779 |
| CRP, mg/L | 4 (2, 10) | 2 (2, 3) | 12 (9, 23) | <0.001 |
CAD: Coronary artery disease, DM: Diabetes mellitus, SDS: Summed difference score, SRS: Summed rest score, SSS: Summed stress score.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



