
Submitted:
09 January 2024
Posted:
11 January 2024
You are already at the latest version
Abstract
Abstract:
The Kingdom of Saudi Arabia (KSA) aims to achieve measles elimination by
2015. Since the beginning of elimination efforts in early 2000, there has not been a study tracking the national incidence over time. Thus, we described the distribution and incidence rates (IR) of measles in all 13 provinces of KSA from 2002 – 2012. This should give policymakers a clear picture about how to improve measles surveillance and accelerate elimination efforts. Using the national measles notification data reported to the Ministry of Health from 2002 through 2012 from all 13 provinces of KSA. Trends in annual measles IR stratified by age, gender, nationality, province, month, and immunization status in KSA were determined. There were 9,643 confirmed cases of measles reported in KSA from 2002 – 2012. Most were reported from Makkah (21.9%) and were among the age group 0 – 14 years of age. Madinah province showed a continuous IR increase from 2009. Baha province has been measles free since 2008. KSA could eliminate measles by 2015 by maintaining high vaccination coverage in the population and improving public health surveillance.
Keywords:
Measles
; Elimination
; KSA
; Vaccination
; Immunizable disease
1. Introduction
Measles is a highly viral infectious disease that can cause severe illness, permanent complications, and death [1,2]. It has a basic reproductive rate of 17-20, which means one case of measles in a susceptible community spawns 17-20 new cases [3]. The virus remains contagious and active in the air or on infected surfaces for up to 2 hours [4]. Measles symptoms clinically begin with a prodromal illness characterized by fever, tiredness, coryza, cough, runny nose, and painful red eyes. This is followed a few days later by the appearance of maculopapular rash, which starts on the face and behind the ears, spreads down to the body and lasts for 4-7 days [2,4]. One third of those with measles develop complications due to secondary infections, which can lead to ear infections, diarrhea, dehydration and pneumonia, and may require hospitalization [2].
Complications are common in children under five years of age or adults over the age of 20 [5]. The most dangerous complication is encephalitis (brain infection), which occurs in 1 out of 1000 patients, and death has been reported in 0.3% of the cases [6]. Unvaccinated children and pregnant women are at highest risk of measles and its complications, including death [4]. Before the introduction of the measles vaccine, measles was one of the most overwhelming infectious diseases and caused millions of deaths and disabilities worldwide each year [7].
The key public health strategies to reduce global measles deaths are routine measles immunizations for all children combined with mass immunization campaigns in countries with high case and death rates [4]. The extensive use of the measles vaccine since 1980 has led to a significant decrease in global measles morbidity and mortality. The Measles and Rubella Initiative (MR) was launched in 2001 and led by the Centers for Disease Control and Prevention (CDC), American Red Cross (ARC), United Nations Foundation (UNF), United Nations Children’s Fund (UNICEF), and World Health Organization (WHO) to provide financial and technical support for enhanced measles control activities [1,8]. All six WHO regions are devoted to measles elimination and five regions have set target dates. The WHO Region of the Americas (AMR) achieved the goal in 2002 [9]; the Western Pacific Region (WPR) aimed to eliminate measles by end of 2012; and the Eastern Mediterranean (EMR) and European (EUR) Regions are enhancing their measles control activities in order to eliminate measles by 2015. In 2011, countries in the African Region (AFR) were assigned the goal of eliminating measles by 2020, and in 2010 the South-East Asia Region (SEAR) implemented a resolution urging countries to assemble resources to support their measles elimination goals [1].
KSA is the largest country in the Arabian Peninsula. The birthplace of Islam, the country is home to the two holiest Islamic cities of Makkah and Madinah [10]. The history of measles prevention efforts can be divided into two main parts, the control phase and the elimination phase [11].
The control phase was started in 1974 [12] with the introduction of a single measles vaccine dose (Schwarts) that targeted children from 1-9 years old [13]. Before the introduction of the control phase, children in KSA usually had become immune to measles by the age of 5. At the beginning of control phase, the vaccination was not mandatory. Then, in order to increase the vaccination coverage rate, a royal decree was issued in 1982 that made the measles vaccine a mandatory requirement for all infants in order to obtain the national birth certificate [13]. As a result, the measles vaccine coverage rate increased from 8% in 1980 to 80% in 1984; by 1990, it exceeded 90% [11].
In the early 1990s, the Edmonston-Zagreb Measles Vaccine and the two-dose strategy were implemented in Saudi Arabia to reduce primary measles vaccine failure due to persistent maternal antibodies after the administration of the Schwarts vaccine [11]. The main goal of this phase was to reduce measles mortality and morbidity among KSA’s population. The elimination phase started in 1998 and has continued until the present. In 2001, the introduction of lab confirmation strengthened the measles surveillance system [11].
The goal of this study is to provide information to KSA policymakers about measles trends from 2002 through 2012, and to track the progress towards the goal of elimination and guide policy development.
2. Methods
2.1. Data Source
This study used the national measles notification system’s data reported to the MOH from 2002 through 2012 from all 13 provinces of KSA. The data were first translated from Arabic to English using Google Translate, and the translation process was then evaluated for accuracy by the first author (a native Arabic speaker). The data were de-identified.
2.2. Data Analysis
We calculated only laboratory-confirmed measles cases and cleaned, organized, and removed inaccurate data. Then age groups consistent with the total population were recorded. A dataset was created in SAS and queried to produce frequencies tables, which were exported into Excel. Incidence rate and confidence intervals were calculated in Excel with these tables. The annual incidence rate of measles per 100,000 populations was stratified by nationality, gender, age group, region, month, and immunization status.
Population data was obtained from the Ministry of Economy and Planning and Central Department of Statistics and Information in KSA. It included data for the entire country classified by age, gender, nationality, and province for the years 2002 – 2012. The data include only the first four months of the year of 2012.
3. Results
There were 9,643 confirmed measles cases reported in KSA from 2002 – 2012. The national measles incidence rate (IR) shows a slight decline during the past 11 years with two epidemic spikes in 2004 and 2007 (Figure 1). In 2004, 1,772 (18.4%) cases occurred, and in 2007, 4,649 (48.2%) cases.
Almost all provinces showed a decrease in the measles incidence rate (IR). Madinah reported no cases of measles in 2009 but experienced a continuous increase in the IR from 2010 (Figure 2).
The lowest IR reached was 0.33/100,000 of population in 2009, and the highest was 19.2/100,000 of population in 2007. In general, IR among Saudi nationals were higher than that of non-Saudis except in 2005 (Table 1).
Most measles cases occurred in Makkah (21.9%) followed by Jizan (17.1%), Eastern region (13%), Riyadh (12.4), and Aseer (11.2%) Figure 3).
Most cases occurred among the very young; 73% of cases occurred in the 0-14 age group; 13.4% were in age group 15-24; and 9.7% were within the 25-34 age group (Table 2).
The majority of cases (66%) were reported between February and May.
At the province level, the highest IR rate was observed in Al-Joof in 2007 (171.9 per 100,000), as shown in Figure 4.
The IR was higher among non-Saudis in Madinah and Riyadh provinces only. During the study period, females had a higher IR than males in each year.
In terms of vaccination status, among Saudi nationals, 4742 measles cases (54%) occurred among those not vaccinated; of these, 1018 cases (21.5%) were in Jizan; 854 cases (18%) were in the Eastern province; 851 cases (17.95%) were in Makkah; 669 (14.1%) were in Aseer; and 411 (8.7%) were in Riyadh (Table 3).
Among non-Saudis who had measles, 432 out of 719 (60%) were not vaccinated; 241 (55.8%) were located in Makkah; 93 (21.5%) in Jizan and 40 (9.3%) in the Eastern province (Table 4). Baha province reported no measles cases since 2008, and Joof province reported none since 2011. Hail and Qassim had no reported cases in the first 4 months of 2012.
4. Discussion
The measles rate showed a slight decrease from 2002 – 2012, but epidemics still occurred approximately every 3 years. KSA has maintained a measles vaccination coverage rate of above 95% since 2001 [14]; over half of the cases (54%) occurred among non-vaccinated Saudis and non-Saudis (non-vaccinated people are defined here as those who have not had any previous doses of MCV).
The resurgence of measles could have been due to an accumulation of susceptible cases among those in the vulnerable age group of 0-14 years in highly populated provinces like Makkah, Riyadh, Eastern Province, Aseer and Jizan.
Most of the non-vaccinated cases among both Saudis and non- Saudis were located in Makkah, Jizan, Eastern, and Riyadh provinces. Makkah is a challenging area because of the Hajj, the biggest mass gathering in the world, with an estimated 2-3 million pilgrims traveling there each year [15].. Yemenis accounted for 280 (35%) of the total non-Saudi cases, and 75% of those cases were distributed in the cities of Jizan and Jeddah, which is located in Makkah province.
Measles infections usually occur during late winter and early summer (Figure 5). Saudis may have a higher measles incidence rate than non-Saudis because infections occur and spread mainly among preschool and school-age children, and the majority of the non-Saudis are adults who come to KSA to perform Hajj or Umrah, or to work.
Al-Madinah province should pay close attention to its trends because it is the only province with a continuous increase in the measles incidence among both Saudis and non-Saudis since 2009.
Sustainable elimination has been achieved in Baha province; it is the only province that has been free of measles since 2008. Joof province has also sustained elimination since 2011. This achievement is also possible in the Qassim and Hail provinces, as they showed no measles cases for the first 4 months of 2012.
4.1. Limitations
This study only included confirmed measles cases; suspected cases were out of scope. We did not have complete Saudi census data for all of the different age groups from 2002 – 2012; we calculated the census population data by computing the annual population growth rate from data on the Saudi and non-Saudi population census from 2005 – 2009.
4.2. Recommendations
Because the measles vaccine is safe, effective, and inexpensive (costing less than US$1 [4]), we recommend adding the measles vaccination to the list of required vaccinations for issuance of Hajj or work visas. We recommend data registry training sessions for those who are working on the measles PHS so that the data will be clearer, more readable, and more complete. Also, we recommend paying more attention to the vaccination process in Makkah, Riyadh, Jizan, Eastern Province, and Aseer because these provinces have the greatest number of cases. We recommend targeting preschool and school-age groups and all of those from 0-14 years old every 3 years to reduce the chance of measles resurgence due to the accumulation of non-vaccinated groups. Finally, KSA is moving ahead with continuous steps toward measles elimination by 2015, but we need greater political and public health commitment.
References
- PLAN, S. Global Measles and Rubella 2012.
- Factsheet: measles. N S W Public Health Bull 2012, 23, 209. [CrossRef] [PubMed]
- Cluster, W.H.O.C.D., W.H.O.H. Technology, and Pharmaceuticals, WHO Guidelines for Epidemic Preparedness and Response of Measles Outbreaks. 1999: World Health Organization, Expanded Programme on Immunization, Vaccines and other Biologicals [and] Department of Communicable Disease Surveillance and Response.
- World Health Organization. Measles. 2013 [cited 2013; Available from: http://www.who.int/mediacentre/factsheets/fs286/en/.
- Perry, R.T. and N.A. Halsey, The clinical significance of measles: a review. J Infect Dis 2004. 189 (Suppl 1), S4-16. (Suppl 1).
- Preeta Kutty MD; Jennifer Rota MPH, W.B.P., Susan B. Redd, Measles. 2012, Centers for Disease Control and Prevention.
- Moss, W.J. and D.E. Griffin, Measles. Lancet 2012, 379, 153–64. [Google Scholar] [CrossRef] [PubMed]
- van den Ent, M.M., et al., Measles mortality reduction contributes substantially to reduction of all cause mortality among children less than five years of age, 1990–2008. Journal of Infectious Diseases 2011, 204 (suppl 1), S18-S23. (suppl 1).
- Global control and regional elimination of measles, 2000-2011. MMWR Morb Mortal Wkly Rep 2013, 62, 27–31.
- The World Factbook, C.I.A. 2013; Available online: https://http://www.cia.gov/library/publications/the-world-factbook/geos/sa.html.
- Khalil, M.K. , et al. Measles in Saudi Arabia: from control to elimination. Ann Saudi Med 2005, 25, 324–8. [Google Scholar] [CrossRef] [PubMed]
- Jahan, S. , et al. Measles outbreak in Qassim, Saudi Arabia 2007: epidemiology and evaluation of outbreak response. J Public Health (Oxf) 2008, 30, 384–90. [Google Scholar] [CrossRef] [PubMed]
- Khalil, M.K. , et al. Measles immunization in Saudi Arabia: the need for change. East Mediterr Health J, 2001; 7, 829–34. [Google Scholar]
- Ministry of Health, S.A. Health Statistical Year Book. 2011. p. 44.
- Memish, Z.A. Infection control in Saudi Arabia: meeting the challenge. Am J Infect Control 2002, 30, 57–65. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Incidence Rate of measles per 100,000 population in KSA and its (95% CI), 2002-2012.
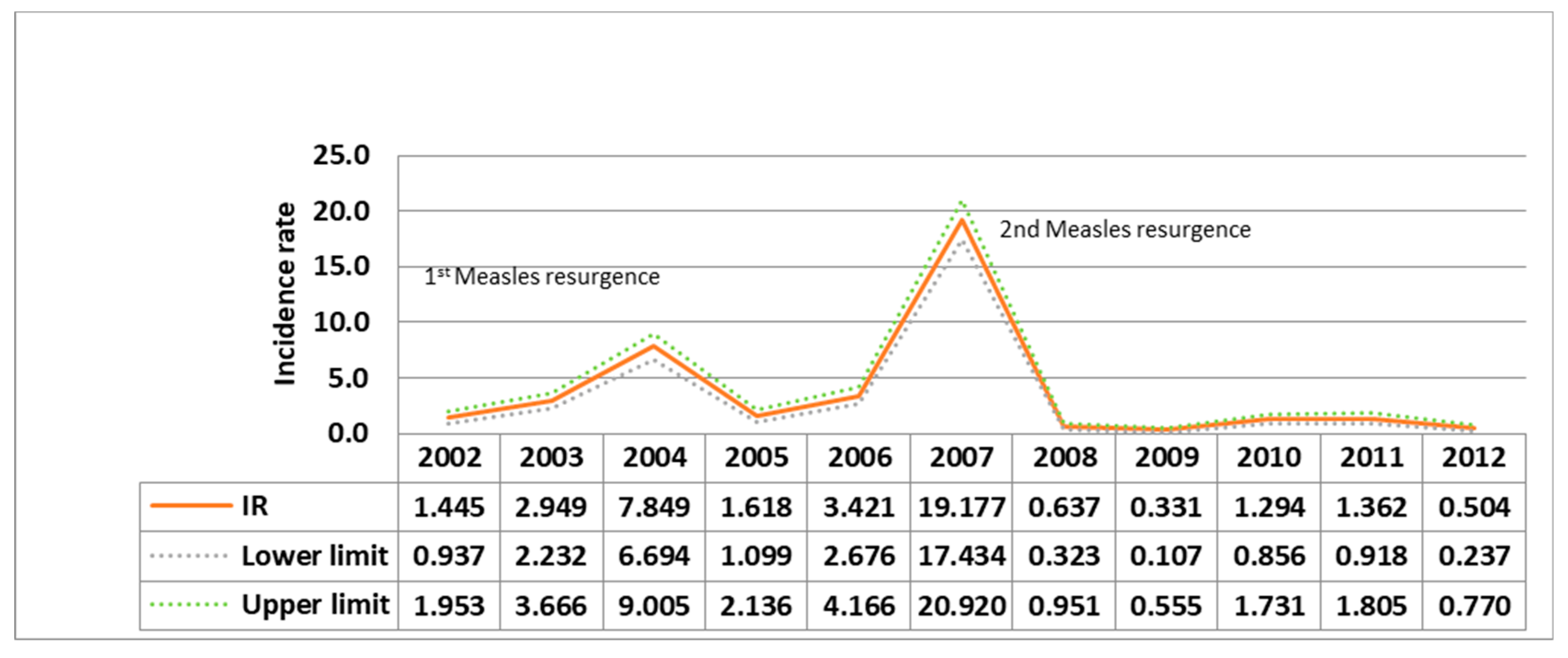
Figure 2.
Measles incidence rate in Medinah province, KSA 2002-2012.
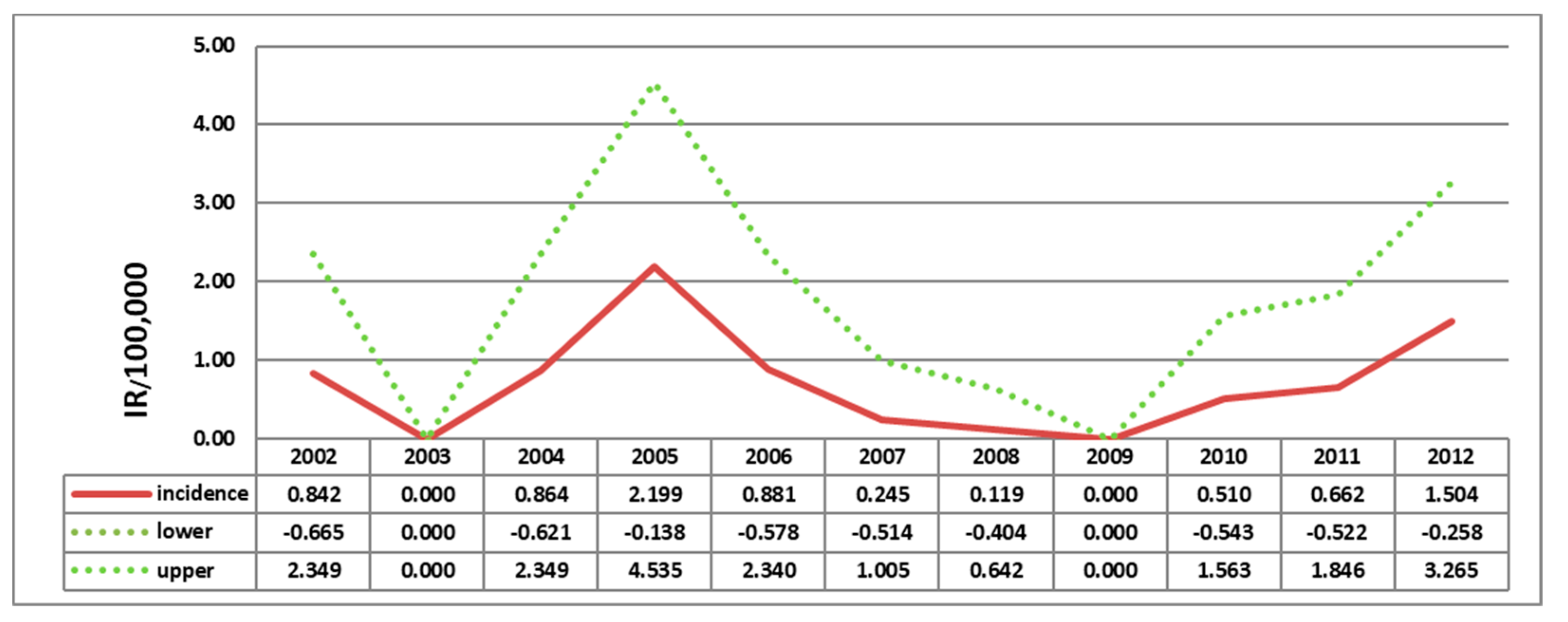
Figure 3.
Total number of confirmed measles cases by province, Saudi Arabia, 2002-2012.
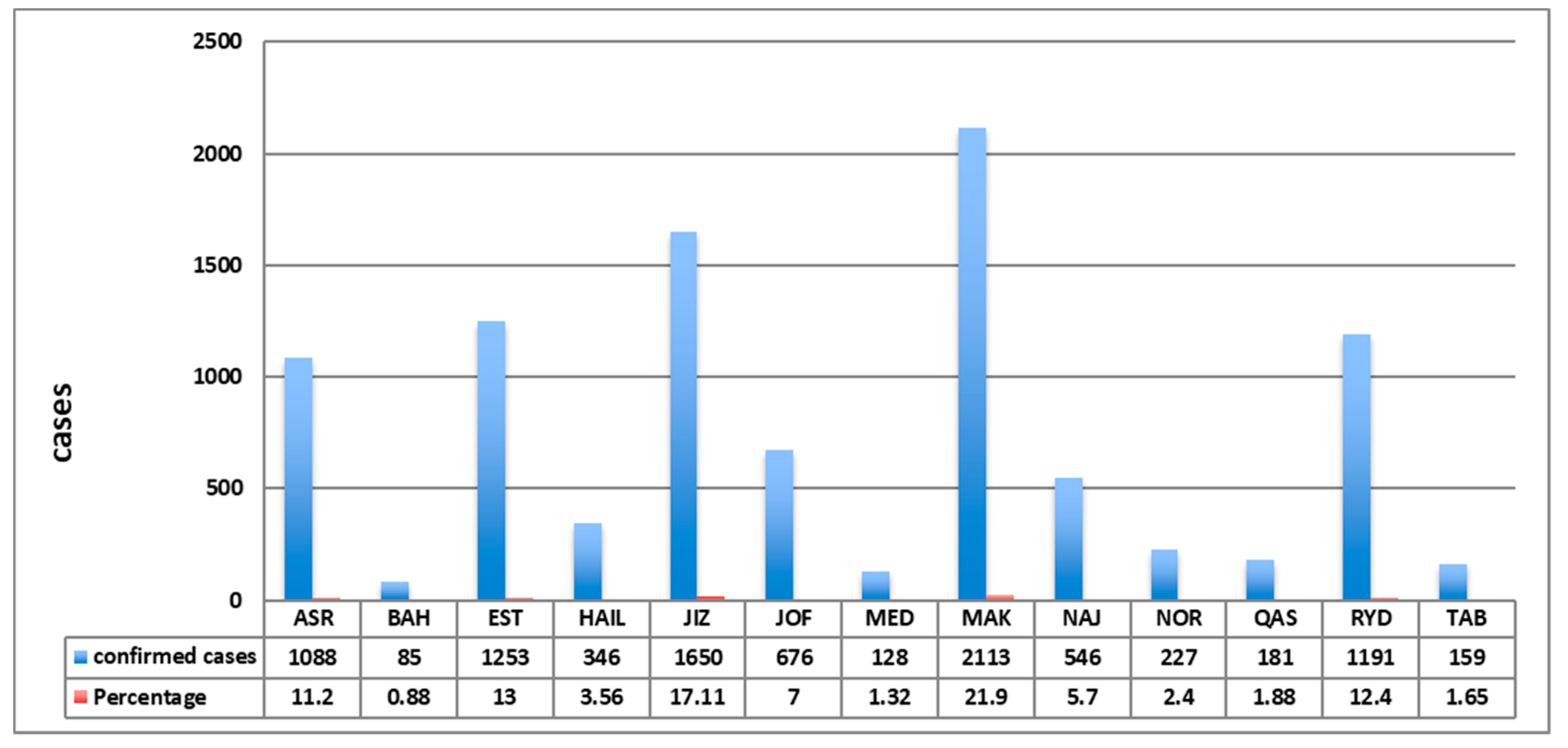
Figure 4.
Measles Incidence Rate per 100,000 population in Al-Joof province, KSA 2002-2012.
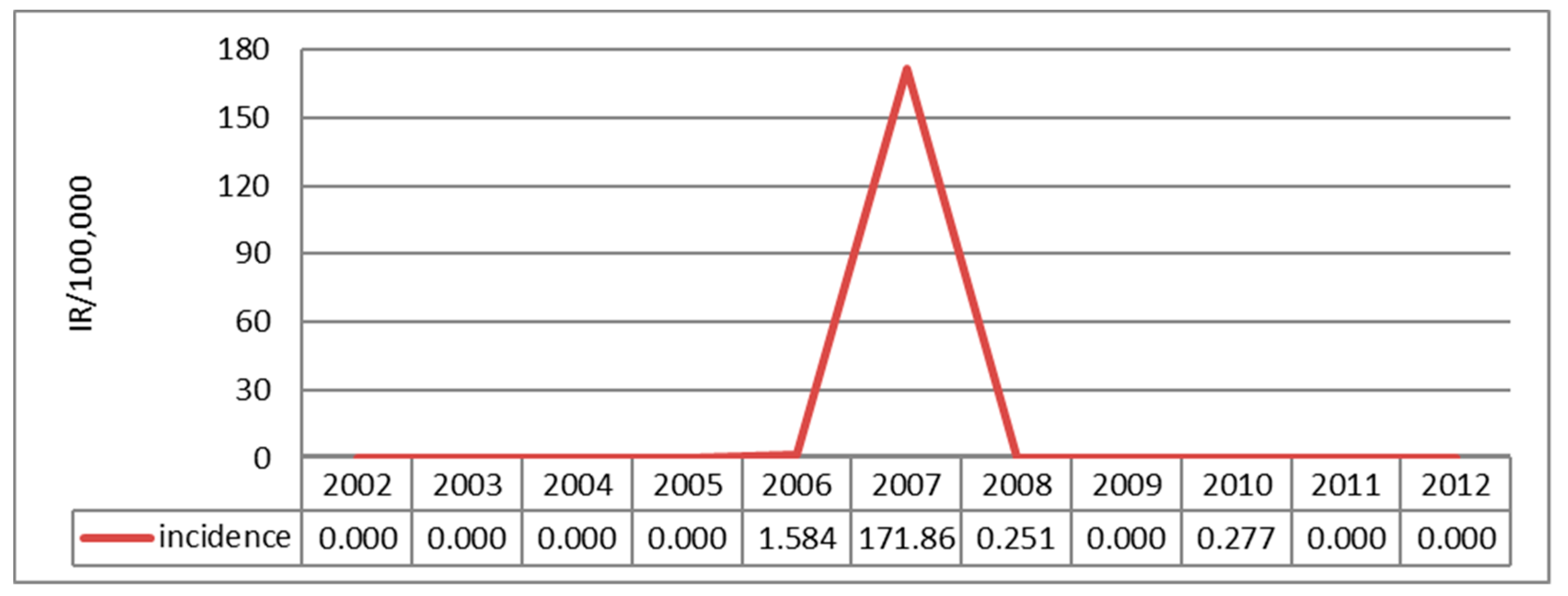

Table 1.
Measles incidence rate per 100,000 population by nationality and year in KSA.
| Year | Saudi | Non-Saudi | ||
|---|---|---|---|---|
| IR | 95% CI | IR | 95% CI | |
| 2002 | 1.97 | (1.27, 2.66) | 0.05 | (-0.13, 0.23) |
| 2003 | 3.73 | (2.79, 4.68) | 0.85 | (0.11, 1.59) |
| 2004 | 9.87 | (8.35, 11.39) | 2.43 | (1.2, 3.67) |
| 2005 | 1.57 | (0.97, 2.17) | 1.74 | (0.71, 2.77) |
| 2006 | 4.23 | (3.26, 5.20) | 1.23 | (0.37, 2.09) |
| 2007 | 25.03 | (22.7, 27.36) | 3.37 | (1.97, 4.78) |
| 2008 | 0.83 | (0.41, 1.25) | 0.11 | (-0.14, 0.35) |
| 2009 | 0.39 | (0.11, 0.68) | 0.16 | (-0.14, 0.46) |
| 2010 | 1.42 | (0.89, 1.96) | 0.95 | (0.22, 1.67) |
| 2011 | 0.53 | (1.16, 2.33) | 0.32 | (-0.09, 0.74) |
| 2012 | 0.53 | (0.21, 0.85) | 0.44 | (-0.04, 0.92) |
Table 2.
Total confirmed measles cases by age group and year in KSA, 2002-2012.
| Age groups in Years | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | Total (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 - 14 |
231 2.40 3.28 74.28 |
529 5.49 7.52 81.51 |
1404 14.58 19.95 79.23 |
303 3.15 4.31 81.02 |
616 6.40 8.75 76.05 |
3251 33.75 46.21 69.93 |
89 0.92 1.26 56.33 |
48 0.50 0.68 57.14 |
228 2.37 3.24 67.86 |
262 2.72 3.72 72.38 |
75 0.78 1.07 59.06 |
7036 73.05 |
| 15 - 24 |
47 0.49 3.63 15.11 |
58 0.60 4.48 8.94 |
189 1.96 14.61 10.67 |
33 0.34 2.55 8.82 |
79 0.82 6.11 9.75 |
749 7.78 57.88 16.11 |
34 0.35 2.63 21.52 |
14 0.15 1.08 16.67 |
41 0.43 3.17 12.20 |
41 0.43 3.17 11.33 |
9 0.09 0.70 7.09 |
1294 13.43 |
| 25 - 34 |
27 0.28 2.89 8.68 |
47 0.49 5.03 7.24 |
134 1.39 14.33 7.56 |
23 0.24 2.46 6.15 |
87 0.90 9.30 10.74 |
467 4.85 49.95 10.05 |
24 0.25 2.57 15.19 |
20 0.21 2.14 23.81 |
40 0.42 4.28 11.90 |
35 0.36 3.74 9.67 |
31 0.32 3.32 24.41 |
935 9.71 |
| 35 - 44 |
6 0.06 1.96 1.93 |
14 0.15 4.58 2.16 |
38 0.39 12.42 2.14 |
13 0.13 4.25 3.48 |
25 0.26 8.17 3.09 |
150 1.56 49.02 3.23 |
8 0.08 2.61 5.06 |
2 0.02 0.65 2.38 |
19 0.20 6.21 5.65 |
20 0.21 6.54 5.52 |
11 0.11 3.59 8.66 |
306 3.18 |
| 45 - 54 |
0 0.00 0.00 0.00 |
1 0.01 2.44 0.15 |
6 0.06 14.63 0.34 |
1 0.01 2.44 0.27 |
2 0.02 4.88 0.25 |
20 0.21 48.78 0.43 |
2 0.02 4.88 1.27 |
0 0.00 0.00 0.00 |
5 0.05 12.20 1.49 |
4 0.04 9.76 1.10 |
0 0.00 0.00 0.00 |
41 0.43 |
| 55 - 64 |
0 0.00 0.00 0.00 |
0 0.00 0.00 0.00 |
0 0.00 0.00 0.00 |
0 0.00 0.00 0.00 |
0 0.00 0.00 0.00 |
7 0.07 63.64 0.15 |
1 0.01 9.09 0.63 |
0 0.00 0.00 0.00 |
3 0.03 27.27 0.89 |
0 0.00 0.00 0.00 |
0 0.00 0.00 0.00 |
11 0.11 |
| ≥ 65 |
0 0.00 0.00 0.00 |
0 0.00 0.00 0.00 |
1 0.01 11.11 0.06 |
1 0.01 11.11 0.27 |
1 0.01 11.11 0.12 |
5 0.05 55.56 0.11 |
0 0.00 0.00 0.00 |
0 0.00 0.00 0.00 |
0 0.00 0.00 0.00 |
0 0.00 0.00 0.00 |
1 0.01 11.11 0.79 |
9 0.09 |
| Total |
311 3.23 |
649 6.74 |
1772 18.40 |
374 3.88 |
810 8.41 |
4649 48.27 |
158 1.64 |
84 0.87 |
336 3.49 |
362 3.76 |
127 1.32 |
9632 100.00 |
|
Frequency Missing = 11 Numbers are arranged longitudinally as below: Frequency Percent Row percent Column percent | ||||||||||||
Table 3.
Measles cases count by Immunization status and province in KSA, 2002-2012.
| Controlling for Nationality = Saudi | ||||||||||||||||||||||||||||
| Immunization Status | Province | |||||||||||||||||||||||||||
| ASR | BAH | EST | HAIL | JIZ | JOF | MED | MAK | NAJ | NOR | QAS | RYD | TAB | Total | |||||||||||||||
| Not Vaccinated |
669 7.61 14.11 62.52 |
31 0.35 0.65 36.90 |
854 9.72 18.01 72.25 |
153 1.74 3.23 44.35 |
1018 11.59 21.47 67.82 |
286 3.25 6.03 42.56 |
56 0.64 1.18 70.00 |
851 9.68 17.95 51.51 |
203 2.31 4.28 39.42 |
92 1.05 1.94 41.63 |
41 0.47 0.86 24.40 |
411 4.68 8.67 35.99 |
77 0.88 1.62 49.68 |
4742 53.97 |
||||||||||||||
| Unknown |
90 1.02 7.26 8.41 |
6 0.07 0.48 7.14 |
119 1.35 9.60 10.07 |
45 0.51 3.63 13.04 |
231 2.63 18.64 15.39 |
214 2.44 17.27 31.85 |
7 0.08 0.56 8.75 |
202 2.30 16.30 12.23 |
117 1.33 9.44 22.72 |
15 0.17 1.21 6.79 |
45 0.51 3.63 26.79 |
131 1.49 10.57 11.47 |
17 0.19 1.37 10.97 |
1239 14.10 |
||||||||||||||
| Vaccinated |
311 3.54 11.08 29.07 |
47 0.53 1.67 55.95 |
209 2.38 7.45 17.68 |
147 1.67 5.24 42.61 |
252 2.87 8.98 16.79 |
172 1.96 6.13 25.60 |
17 0.19 0.61 21.25 |
599 6.82 21.35 36.26 |
195 2.22 6.95 37.86 |
114 1.30 4.06 51.58 |
82 0.93 2.92 48.81 |
600 6.83 21.38 52.54 |
61 0.69 2.17 39.35 |
2806 31.93 |
||||||||||||||
| Total |
1070 12.18 |
84 0.96 |
1182 13.45 |
345 3.93 |
1501 17.08 |
672 7.65 |
80 0.91 |
1652 18.80 |
515 5.86 |
221 2.52 |
168 1.91 |
1142 13.00 |
155 1.76 |
8787 100.00 |
||||||||||||||
|
Frequency Missing = 105 Percent Row percent Column percent | ||||||||||||||||||||||||||||
Table 4.
Total confirmed measles cases by Immunization status and province in KSA, 2002-2012.
| Controlling for Nationality = Non-Saudi | |||||||||||||
| Immunization Status | Province | ||||||||||||
| ASR | BAH | EST | HAIL | JIZ | JOF | MED | MAK | NAJ | QAS | RYD | TAB | Total | |
| Not Vaccinated |
2 0.28 0.46 50.00 |
1 0.14 0.23 100.00 |
40 5.56 9.26 60.61 |
1 0.14 0.23 100.00 |
93 12.93 21.53 65.96 |
1 0.14 0.23 25.00 |
11 1.53 2.55 55.00 |
241 33.52 55.79 61.79 |
17 2.36 3.94 54.84 |
7 0.97 1.62 53.85 |
15 2.09 3.47 38.46 |
2 0.28 0.46 66.67 |
432 60.08 |
| Unknown |
1 0.14 0.99 25.00 |
0 0.00 0.00 0.00 |
13 1.81 12.87 19.70 |
0 0.00 0.00 0.00 |
28 3.89 27.72 19.86 |
3 0.42 2.97 75.00 |
6 0.83 5.94 30.00 |
41 5.70 40.59 10.51 |
4 0.56 3.96 12.90 |
0 0.00 0.00 0.00 |
2 0.28 1.98 5.13 |
0 0.00 0.00 0.00 |
101 14.05 |
| Vaccinated |
1 0.14 0.54 25.00 |
0 0.00 0.00 0.00 |
13 1.81 6.99 19.70 |
0 0.00 0.00 0.00 |
20 2.78 10.75 14.18 |
0 0.00 0.00 0.00 |
3 0.42 1.61 15.00 |
108 15.02 58.06 27.69 |
10 1.39 5.38 32.26 |
6 0.83 3.23 46.15 |
22 3.06 11.83 56.41 |
1 0.14 0.54 33.33 |
186 25.87 |
| Total |
4 0.56 |
1 0.14 |
66 9.18 |
1 0.14 |
141 19.61 |
4 0.56 |
20 2.78 |
390 54.24 |
31 4.31 |
13 1.81 |
39 5.42 |
3 0.42 |
719 100.00 |
|
Frequency Missing = 32 Percent Row percent Column percent | |||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



