
Submitted:
09 January 2024
Posted:
11 January 2024
You are already at the latest version
Abstract
Radiomics represents the science of extraction and analysis of a multitude of quantitative features from medical imaging, unrevealing quantitative potentiality of Radiologic images.
This scientific review aims to provide radiologists a comprehensive understanding of radiomics, emphasizing its principles, applications, challenges, limits, and future prospects. Limits of standardization of actual scientific production are analyzed with the possible solutions proposed by some papers reported and commented.
As the continuous evolution of medical images is ongoing, radiologists must be aware of new perspective to perform a central role in patients management.
Keywords:
Radiomics
; Radiology new techonologies
; Abdominal imaging
; Artificial Intelligence.
1. Introduction
Radiomics represents the science of extraction and analysis of a multitude of quantitative features (intensity, shape, texture, and spatial relationships), from medical images generated through various imaging modalities, including computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET).
The data extraction process upgrades the traditional radiology methods interpretation which relies priorly on qualitative visual assessments. This is a complex process influenced by technical and biological variability [1,2,3,4].
Many papers demonstrate correlation between radiomics data, biological and anatomo-pathological features of neoplasms; in some cases that data strictly correlate with their prognosis and success of therapy. Even though there is still a difficulty to obtain standardized results from different studies.
The main application in oncology are classification and clinical outcome prediction. Both applications will be a very interesting development of the future radiology role in the oncologic patients’ managements with the future possibility of virtual biopsy. Quantitative analysis of radiomic features allows for the identification subtle patterns and changes in medical images that may not be apparent through visual inspection alone. This capability enhances the early detection and diagnosis of diseases, potentially leading to improved outcomes and survival rates. [5,6,7,8].
Radiomics contributes to a paradigm shift in healthcare by promoting data-driven decision-making. The large-scale analysis of imaging data can uncover patterns, trends, and associations that may be challenging to discern through traditional methods, empowering clinicians with additional tools for informed decision-making.
As the field continues to evolve, radiologists and healthcare practitioners must adapt to and embrace the opportunities presented by radiomics for improved patient care and outcomes.
2. Relevant Sections
2.1. Radiomics Workflow
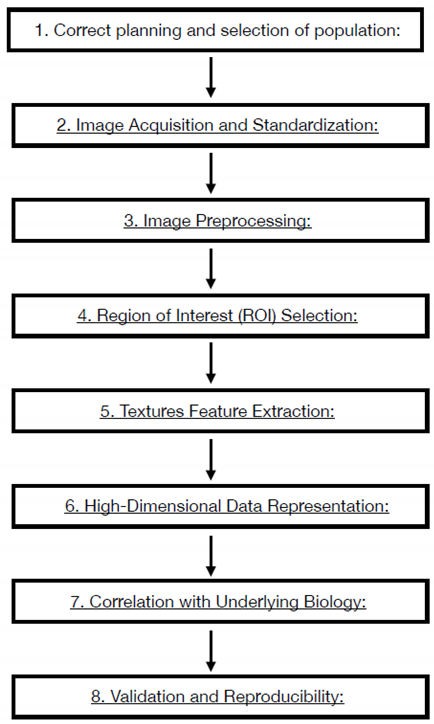
Radiomics needs precise workflow to correctly obtain reproducible data and results (Table 1). All steps need to be strictly followed up and evaluated to be sure that results will be reproducible and conclusions will be proportioned to the hypothesis and to the results data. Every passage has some critical points that could affect the result. Critically evaluate of every passage is necessary to correctly complete the path to the results:
- Correct planning and selection of population: The Radiomics study must answer to a precise clinical question still open and debated, the study must be built with enough data to demonstrate the clinical hypothesis. Attrite data errors are common, needing a precise model validation, measuring the predict performance of the model. The training sample is necessary to measure the capability of the software to work properly and , should be around one-third of the sample size.
- Image Acquisition and Standardization: Radiomics workflow begins with the acquisition of medical images through various modalities such as CT, MRI, or PET. Standardization of imaging protocols is crucial to ensure consistency across studies and institutions. This involves establishing uniform parameters for image acquisition, resolution, contrast type and parameters of administration. Anonymization process is a delicate point and necessary to undergo law prescription and patient privacy respect. The necessity of homogenous data is critical. Artificial intelligence algorithms that work on the modality acquisition software help to produce and homogenize data obtained from different device using optimization process derived from database and tailoring the acquisition parameters to patient to obtain homogeneous quality images.
- Image Preprocessing: Raw medical images often undergo preprocessing steps to enhance the quality of data for analysis. Preprocessing may involve noise reduction, normalization, and correction for artifacts to ensure the reliability of extracted features. MRI filters for homogenization are proposed in many papers and should be used to obtain the possibility to extract texture parameters homogenously.
- Region of Interest (ROI) Selection: The process involves defining the Region of Interest (ROI), which represents the area of the image containing the lesion or tissue of interest. Accurate ROI delineation is critical, and it can be performed manually or through automated/semi-automated (region growing or thresholding) segmentation techniques. In the field of automated methods deep learning Artificial Intelligence software are developing very promising results. All the methods described have weak points: manual segmentation Is time consuming, manual and semi-automated segmentation present an observer-bias; automated softwares are not still robust enough to be objective. The use of automated software could introduce variability in obtaining Radiomics features as many of them are good enough to isolate entire organs but not enough for single tumor lesions segmentation. 3D segmentation will perform a more precise measure but introduce time spanding procedur if manual or semiautomated and great technical difficulty to automated software. Manual and semiautomatic segmentation with readers correlation seems to be the best way to obtain correct data.
- Textures Feature Extraction: Radiomics features are quantitative measurements extracted from ROIs, encompassing a range of parameters such as intensity, morphology, texture. Intensity features include statistical measures like mean, median, and standard deviation, while texture features capture patterns and variations within the image. The process to extrapolate these parameters are different, using the Image Biomarker Standardization Initiative (IBSI) guidelines is mandatory to obtain reproducible measurements. An example of texture parameters different orders is:
- First order statistics compose by 19 features.
- Shaped based (3d) compose by 16 features.
- Shaped based (2d) compose by 10 features.
- Gray Level Co-occurrence Matrix compose by 24 features.
- Gray Level Run Length Matrix compose by 16 features.
- Gray Level Size Zone Matrix compose by 16 features.
- Neighbouring Gray Tone Difference Matrix compose by 5 features.
- Gray Level Dependence Matrix compose by 14 features.

Table 1.
This is only an example of possible texture parameters extracted from images (https://pyradiomics.readthedocs.io/en/latest/index.html); many other parameters could add different information. As it could be easily understood the great number of parameters produced are hardly to correlate and managed, requiring sophisticated software analysis.
- 6.
- High-Dimensional Data Representation: The extracted features result in a high-dimensional dataset, where each data point represents a specific quantitative aspect of the image. This high-dimensional data is the basis for subsequent analyses and need to be accurate selected to obtain correct results. The number of feature correlate with the possibility of overfitting of the model. The selection and reduction of features dimension is an important step to produce generalizable and reproducible results. In literature, there is not generalized definitive rules to assess the correct reduction and selection of parameters. In this step the role of artificial software analysis seems to obtain the principal role to manage the correct pathway. First step is the exclusion of non-reproducible value, in particular, data coming from manual or semiautomated selection of ROI. Test-retest robustness of data extracted from features should be assessed. In this step the use of phantom could help defining correct evaluation.
- 7.
- Correlation with Underlying Biology: Radiomic features are not arbitrary; they correlate with underlying biological and pathological characteristics. The challenge is to identify and understanding these correlations, linking the quantitative features to the physiological, genetic, and molecular attributes of the imaged tissue. Artificial intelligence software elaboration allows an automated integration of data from images and biological features. These algorithms aid in predicting outcomes, classifying diseases, and uncovering relationships that might be challenging for human observers to discern.
- 8.
- Validation and Reproducibility: Rigorous validation is crucial to ensure the reliability and reproducibility of radiomic features. Validation consists in assessing the performance of radiomic models using independent datasets and considering factors such as intra- and inter-observer variability. Understanding and applying these principles allow radiologists to navigate the essence of radiomics, harnessing the quantitative power of medical imaging for enhanced diagnostic and prognostic capabilities. As radiomics continues to evolve, adherence to these principles ensures the credibility and utility of findings in this new technology. Some standardization processes are suggesting with the Image biomarker standardization initiative (IBSI). The IBSI provide standardized image biomarker nomenclature and definitions, a standardized general image processing workflow, tools for verifying radiomics software implementations and reporting guidelines for radiomic studies [9,10].
2.2. Radiomics Standardization and Verification Process
Many papers are written about Radiomics, but reproduction and verification of results are often very difficult; results are sometimes impossible to repeat, using the same patient cohort and calculation method. The processes are subjected to a wide range of errors and difficult standardized passages. Lack of standardized imaging protocols and analysis methodologies hampers the comparability of results across different studies and institutions. Variability in image acquisition parameters, preprocessing steps, and feature extraction methods can lead to inconsistent findings, limiting the reproducibility of radiomic studies. Manual delineation of regions of interest (ROIs) introduces subjectivity and variability in the selection of image features. Inter-observer variability among radiologists in defining ROIs can impact the reliability of radiomic features, emphasizing the need for automated segmentation tools. As mentioned before the automated segmentation tools, even the recent one based on artificial intelligent neural engines are still not affordable enough in segmenting intraparenchymal lesions.
Radiomic features may be influenced by biological factors such as patient physiology, variations in organ function, and changes in tissue composition. Technical confounders, including differences in imaging equipment and techniques, can introduce variability that may not be related to the underlying pathology. Radiomic analyses often require large and different datasets to draw meaningful conclusions, but obtaining such datasets can be challenging. Insufficient data quality, especially in rare diseases or specific patient subgroups, may limit the generalizability of radiomic models. The high-dimensional nature of radiomic datasets increases the risk of overfitting, where a model may perform well on training data but struggle to generalize to new, unseen data. Complex models with many features may capture noise in the data rather than genuine patterns, reducing the model’s predictive power. Addressing these challenges requires collaborative efforts from researchers, clinicians, and technology developers. Continued research and advancements in methodology, standardization, and interdisciplinary collaboration will play a pivotal role in overcoming these limitations and unlocking the full potential of radiomics in clinical practice. Lack of standardized imaging protocols and analysis methodologies hampers the comparability of results across different studies and institutions. Variability in image acquisition parameters, preprocessing steps, and feature extraction methods can lead to inconsistent findings, limiting the reproducibility of radiomic studies.
Training big database are mandatory to train the software before running on the selected data; international institutions are building free database to train artificial intelligence algorithms.
2.3. Ethical issue and Data Privacy
When medical data are analyzed ethical, and privacy are a critical point to concern. Data security, privacy, informed consent and anonymization are the main goal to achieve to operate in security with digital technologies. Informed consent should take in consideration the complexity of information to be received. Potential uses, risk and benefits especially if fully automated software analysis is used. Storage and Transmission of data should be securely performed and systems of prevention of unauthorized access should be apply. Encryption of data is mandatory when data are transmitted between different institutions. Patients should have data control of personal data and be completely informed about their uses, benefits, or risks of using software analysis. Adherence to local and international data protection regulations, such as GDPR in Europe or HIPAA in the United States, is critical. Researchers and healthcare providers must comply with these regulations to protect patient privacy. Research involving radiogenomics should undergo ethical review by institutional review boards or ethics committees to ensure that the study meets ethical standards and respects patient rights. Addressing these ethical and data privacy issues is crucial for building trust among patients, healthcare providers, and researchers involved in radiogenomic studies. Establishing robust ethical guidelines and adhering to data protection regulations are essential steps in advancing the field responsibly. There is also a big issue when automatized software will be introduced in Radiology especially when software will produce data about the possibility to use or not use some customized drugs or therapy. Medical decision like this invest ethical issue and decisions will be the sum of many other sensible information. Explicability is a main bioethical rule that must be introduced when using artificial intelligence automated softwares.
2.4. Explicability of Radiomics Software
Explicability is the capability to correct evaluating and interpreting the results and decision made by an algorithm. The understanding of processes and regulation of the algorithm used is crucial when data form these softwares have a direct impact on patient care and management.
Trustability is another crucial concept that is strictly linked with explicability; healthcare professionals need to know these two concepts to understand a model’s prediction.
There are some crucial point during Radiomics workflow that need to be processed by explicability software.
Extracting many features assess the differences in building interpreting models, understanding which feature contributes most to a prediction’s model.
The machine learning models used in radiomics should be interpretable. Interpretability can be achieved using explainable AI (XAI) techniques. These technique are post-hoc which aim is transform the black box in a glass box [11] to understand how a model arrives to a particular decision.
Methods like feature importance, SHAP (SHapley Additive exPlanations), and LIME (Local Interpretable Model-agnostic Explanations) can be applied to make the decision-making process more transparent.
Explicability is an essential point for building a correct alliance between software and human to ensure the best and mindful decision for patient’s care. The deep knowing of the mechanism that correlate images to clinical and genomic results are necessary for modern Radiologists.
At least every software is completely unuseful if not correlated to a user friendly interface providing doctors easy utilization and understanding the radiological workflow. Visualization tools and dashboards must help convey complex information in a comprehensible format.
2.5. Biological Correlation and Radiogenomics
Biological correlation of radiomics results remain the most important target of new applications. Radiogenomic development that correlates radiological radiomics features with genetic specific patterns allows to unlock potential future use. This step is still ongoing and complex to demonstrate on large scale.
The goal of radiogenomics is to identify genetic markers or signatures that can predict the response to radiotherapy or chemotherapy. The future is to correlate precisely with genomics and anatomopathologic patterns to arrive to virtual biopsy.
Radiogenomics explores the relationship between an individual’s genetic map and the characteristics of radiological images.
The integration of radiogenomics into radiology has the potential to personalize medical imaging and treatment strategies based on a patient’s genetic profile. By understanding the genetic factors that may affect imaging characteristics, clinicians can tailor diagnostic and therapeutic approaches to individual patients, leading to more precise and effective medical interventions.
Radiogenomics could help better understanding the biological variability that effects radiological imaging variability; the correlation between genetic profile with a specific texture features could be the key to identify early modifications of tissue in neoplastic disease as predictive biomarkers. Predictive biomarkers could help to correlate patient’s response to treatment, assessing disease progression or patients’ risk tailored evaluation. That is the way to unlock finally the precision medicine that could change the approach to patients and diseases.
2.6. Radiomics Mean Application, Towards Patient Custom Care
Quantitative analysis of radiomic features allows to distinguish between benign and malignant lesions, facilitating earlier and more accurate diagnoses. Radiomics offers valuable prognostic insights by identifying imaging biomarkers associated with disease progression. The ability to stratify patients based on their radiomic profile enables clinicians to tailor treatment plans according to individual risk profiles. Monitoring changes in radiomic features over the course of treatment allows for real-time assessment of treatment response. Radiomics aids in identifying early signs of treatment efficacy or failure, guiding timely adjustments to therapeutic strategies [12,13,14]. Radiomics supports the concept of personalized medicine by providing a quantitative basis for tailoring treatments to individual patients. The unique radiomic signature of a patient’s lesion can inform decisions about the most effective and targeted therapeutic interventions. In screening programs, radiomics enhances risk stratification by identifying subtle imaging patterns associated with increased disease risk. This allows for more targeted and efficient screening efforts, focusing resources on individuals with higher likelihoods of developing specific conditions.
2.7. Organs Software Applications
Many applications are developing to obtain quantitative information in different organs and diseases. A review of actual scientific papers is reported:
- -
- Neuroimaging Applications: Radiomics is widely used in stroke imaging disease. One of the main application is ischemic stroke. Ischemic stroke is defined as a neurological deficit lasting more than 24h with a correspondent radiological imaging. Radiomics softwares help finding differences between ischemic stroke images and transient ischemic attack. Knowing that ischemic stroke is 85% of the stroke subtype with a high morbility of disability, it is highly important to have a rapid confirmation of pathology and Brain angioCT is the exam of choice with an important role of time in therapy success. Rapid Systemic thrombolytic treatment (no more than 4.5 h from symptoms) with plasminogen activator and local interventional radiology treatment with thrombectomy is the way to reduce morbidity and mortality. In the very acute phase of ischemic stroke attack CT imaging interpretation could be challenging. Some texture feature are reported to better correlate to ischemic suffering tissue. The identification of a penumbra cerebral tissue that could be reperfused without damage improve the decision making process widening the window treatment. The penumbra core area could be evaluated from an artificial intelligence algorithm calculating the apparent diffusion coefficient and cerebral blood flow maps obtained with a contrast enhanced CT perfusion exam in patient with symptoms from no more than 9 h. The radiomics nomogram obtained strongly predicts clinical outcomes at 7 days and at 3 months. These evaluation selected patient that could be treated with thombolysis even if symptoms were recognized inside a 9 hours windows, reducing potential complication of hemorrhage damage of reperfused tissue. Same interesting evaluation is demonstrated by some papers using radiomics on MR imaging. Some other papers investigate the ability of MR imaging radiomics evaluation to predict the hemorrhagic complication at distance, for example 72h after trombolytic treatment, in these papers the results were compared with only radiological visual evaluation determining a high advantage given by Radiomics evaluation. Selecting correct patients for endovascular recanalization expecially when thrombus is in the distal portion lower the number of procedure fail and reduce risks in frail patients. Radiomics evaluation have an high impact in stroke patient management and have completed replaced the morphological evaluation of thrombus with CT characteristics such as length, volume, or permeability. Other application of Brain Radiomics is to characterize brain metastasis and to differentiate them from primitive tumor; Radiomics well correlate in differentiating tumor subtypes, assessing treatment response, and predicting patient outcomes in brain oncology. Promising results are in evaluating neurodegenerative diseases, often diffuse pathology with difficult possibility of characterization [15,16,17,19,20,21,22,28].
- -
- Cardiovascular Imaging: Radiomics has many promised applications in cardiovascular imaging. From image quality and dose optimization to cardiac function evaluation, segmentation and automatic reconstruction. That point will soon improve radiological workflow reducing time consuming operation and allowing radiologist time to concentrate on interpreting images and not in reconstruction operations.
Risk stratification with the implementation of patient history and anamnesis data are promised future applications [23,24,25,26].
- -
- Pulmonary Imaging: In pulmonary imaging, radiomics is valuable for characterizing lung nodules, distinguishing between benign and malignant lesions, and assessing the progression of respiratory diseases. Radiomic analysis of lung images contributes to early detection and personalized management strategies [27,28,29,30,31].
- -
- Gastrointestinal and Oncologic Imaging: Radiomics is widely applied in oncologic imaging for the characterization of tumors, lymph nodes, and metastases. In gastrointestinal imaging, it aids in the identification of biomarkers associated with disease progression and treatment response. Some softwares have a promised impact on evaluation of prostate cancer multiparametric MRI values, which need a preliminary long, spending time, images elaboration before Radiologist report with p-rads criteria [32,33,34,35,36,37,38,39,40,41].
3. Discussion and Future Perspectives
Radiomics application continue to evolve and expand clinical applications. Data driven decision is crucial in the future personal-precision medicine era. The possibility of early evaluation of different therapies could have a big impact in oncologic patients’ management. Many papers are published with local evidence or specific application. To avoid fragmentation of results and a general lack of reproducibility there is the need of standardized scientific workflow and object evaluation of experiments. Some attempts are performed in recent literature to standardize and objectively evaluates the value of an experimental sets.
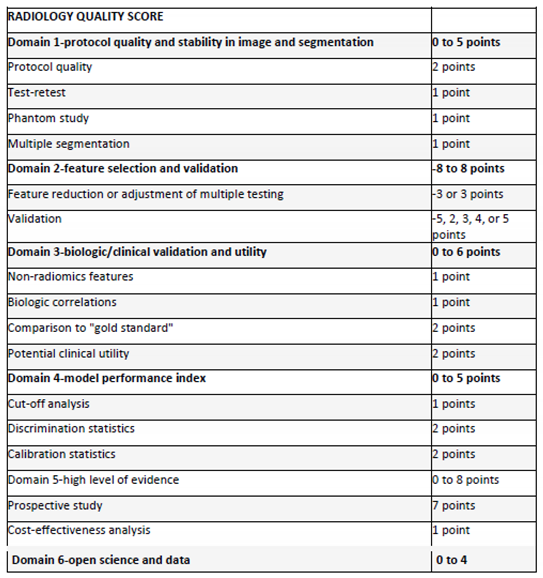
The radiomics quality score proposed based on sixteen points with potential 36 points maximum value proposed by Lambin et al. try to objectively evaluate the quality of an original research [4].
There is a need of standardized database to objective train algorithms and software. The papers need a specific and objective clinical question to answer. The integration with multiple texture parameters needs a clear preliminary evaluation of database size strictly linked to scientific clinical questions. The integration with artificial intelligence software is a necessity when such a big data needs to be analyzed; that synergy must bring automatized software evaluation model to be effective in clinical practice.
Radiological community and patients, need to be clearly instructed about the advantages and disadvantage of using these new technologies. Radiological community is clearly demanding for automated software with a particular attention to explicability unraveling the black box of actual software and algorithm [42]. That’s a crucial point to leave the cloche to medical doctors and the supervision to humans as in the aviation service is clearly settled from years. Quantitive images are a revolution we need to unravel real advantages in patients management; that revolution could not be divided from the use of artificial intelligence software to correlate very big data from multimodality texture analysis and genomic information. That procedure called Radiogenomic set a wider point of view on these new technologies.
Scientific society must work hard to obtain standardized procedure, to create big common database for software training. These databases are not only built from single modality images but needs to be built as a digital twin for patient disease to train and check these technologies during all the disease patient’s history [43].
Radiologists are the main actor in the success of implementation of radiomic technologies in the clinical practice. Radiologists’ communities are aware and trained in rapid technological revolution. The introduction of Radiomics and Radiogenomics technologies will bring some significant evolution in the information given to clinicians putting Radiologists role even further in the center of patient’s workflow.
The future scenarios of Radiological rooms are the interaction of Radiologists with data coming from different softwares on PACS, suggesting an augmented radiological workflow, starting from automated report of number and location of lesions, automatic co-registration and comparison between previous exams, analysis and characterization of malignant or benign lesions characteristics, automated classification of rads and recist criteria, production of semiautomated structured reports. That workflow improves the role of radiologists and the number of information that radiologists’ reports bring inside. There will be a major improvement in Radiologists communication with clinicians reducing the time facing computer mirror to improve time to communicate to patients and colleagues.
References
- Lambin P, Rios-Velazquez E, Leijenaar R et al (2012) Radiomics: extracting more information from medical images using advanced feature analysis. Eur J Cancer 48(4):441–446. [CrossRef]
- Tomaszewski MR, Gillies RJ (2021) The biological meaning of radiomic features. Radiology 298(3):505–516. [CrossRef]
- Gillies RJ, Kinahan PE (2016) Hricak H (2016) Radiomics: images are more than pictures, they are data. Radiology 278(2):563–577. [CrossRef]
- Lambin P, Leijenaar RTH, Deist TM et al (2017) Radiomics: the bridge between medical imaging and personalized medicine. Nat Rev Clin Oncol 14(12):749–762. [CrossRef]
- O’Connor JP, Aboagye EO, Adams JE et al (2017) Imaging biomarker roadmap for cancer studies. Nat Rev Clin Oncol 14:169–186. [CrossRef]
- Van Timmeren JE, Cester D, Tanadini-Lang S, Alkadhi H, Baessler B (2020) Radiomics in medical imaging-"how-to" guide and critical reflection. Insights Imaging 11(1):91. [CrossRef]
- Song J, Yin Y, Wang H, Chang Z, Liu Z, Cui L (2020) A review of origi- nal articles published in the emerging field of radiomics. Eur J Radiol 127:108991. [CrossRef]
- Fusco R, Granata V, Grazzini G, Pradella S, Borgheresi A, Bruno A, Palumbo P, Bruno F, Grassi R, Giovagnoni A, Grassi R, Miele V, Barile A. Radiomics in medical imaging: pitfalls and challenges in clinical management. Jpn J Radiol. 2022 Sep;40(9):919-929. Epub 2022 Mar 28. PMID: 35344132. [CrossRef]
- Zwanenburg A, Leger S, Vallieres M, Lock S. Image biomarker standardisation initiative. arXiv preprint arXiv:1612.07003.
- Lambin P. Radiomics Digital Phantom, CancerData(2016). [CrossRef]
- Neri, E., Aghakhanyan, G., Zerunian, M. et al. Explainable AI in radiology: a white paper of the Italian Society of Medical and Interventional Radiology. Radiol med 128, 755–764 (2023). [CrossRef]
- Radiomics of Brain MRI: Utility in Prediction of Metastatic Tumor Type. Helge C. Kniep, Frederic Madesta, Tanja Schneider, Uta Hanning, Michael H. Schönfeld, Gerhard Schön, Jens Fiehler, Tobias Gauer, René Werner, and Susanne Gellissen. Radiology 2019 290:2, 479-487. [CrossRef]
- Granata V, Fusco R, De Muzio F, Brunese MC, Setola SV, Ottaiano A, Cardone C, Avallone A, Patrone R, Pradella S, Miele V, Tatangelo F, Cutolo C, Maggialetti N, Caruso D, Izzo F, Petrillo A. Radiomics and machine learning analysis by computed tomography and magnetic resonance imaging in colorectal liver metastases prognostic assessment. Radiol Med. 2023 Sep 11. Epub ahead of print. PMID: 37697033. [CrossRef]
- Granata V, Fusco R, De Muzio F, Cutolo C, Mattace Raso M, Gabelloni M, Avallone A, Ottaiano A, Tatangelo F, Brunese MC, Miele V, Izzo F, Petrillo A. Radiomics and Machine Learning Analysis Based on Magnetic Resonance Imaging in the Assessment of Colorectal Liver Metastases Growth Pattern. Diagnostics (Basel). 2022 Apr 29;12(5):1115. PMID: 35626271; PMCID: PMC9140199. [CrossRef]
- Vivek Verma, Charles B. Simone, Sunil Krishnan, Steven H. Lin, Jinzhong Yang, Stephen M. Hahn, The Rise of Radiomics and Implications for Oncologic Management, JNCI: Journal of the National Cancer Institute, Volume 109, Issue 7, July 2017, djx055. [CrossRef]
- Fritz, Benjamin, et al. "Radiomics and deep learning for disease detection in musculoskeletal radiology: an overview of novel MRI-and CT-based approaches." Investigative radiology 58.1 (2023): 3-13.
- Crivelli, Paola, et al. "A new challenge for radiologists: radiomics in breast cancer." BioMed research international 2018 (2018). [CrossRef]
- Rogers, William, et al. "Radiomics: from qualitative to quantitative imaging." The British journal of radiology 93.1108 (2020): 20190948. [CrossRef]
- Wagner, Matthias W., et al. "Radiomics, machine learning, and artificial intelligence—what the neuroradiologist needs to know." Neuroradiology (2021): 1-11.
- Pontillo, G., et al. "A combined radiomics and machine learning approach to overcome the clinicoradiologic paradox in multiple sclerosis." American Journal of Neuroradiology 42.11 (2021): 1927-1933. [CrossRef]
- Chen, Qian, et al. "Radiomics in stroke neuroimaging: techniques, applications, and challenges." Aging and disease 12.1 (2021): 143.Kniep, Helge C., et al. "Radiomics of brain MRI: utility in prediction of metastatic tumor type." Radiology 290.2 (2019): 479-487.
- Ponsiglione, Andrea, et al. "Cardiac CT and MRI radiomics: systematic review of the literature and radiomics quality score assessment." European Radiology (2022): 1-10. [CrossRef]
- Spadarella, Gaia, et al. "Radiomics in cardiovascular disease imaging: from pixels to the heart of the problem." Current Cardiovascular Imaging Reports 15.2 (2022): 11-21. [CrossRef]
- Raisi-Estabragh, Zahra, et al. "Cardiac magnetic resonance radiomics: basic principles and clinical perspectives." European Heart Journal-Cardiovascular Imaging 21.4 (2020): 349-356. [CrossRef]
- Cetin, Irem, et al. "Radiomics signatures of cardiovascular risk factors in cardiac MRI: results from the UK Biobank." Frontiers in Cardiovascular Medicine 7 (2020): 591368. [CrossRef]
- Hassani, Cameron, et al. "Radiomics in pulmonary lesion imaging." American Journal of Roentgenology 212.3 (2019): 497-504.
- Wilson, Ryan, and Anand Devaraj. "Radiomics of pulmonary nodules and lung cancer." Translational lung cancer research 6.1 (2017): 86. [CrossRef]
- Lafata, Kyle J., et al. "An exploratory radiomics approach to quantifying pulmonary function in CT images." Scientific reports 9.1 (2019): 11509. [CrossRef]
- Ather, S., T. Kadir, and F. Gleeson. "Artificial intelligence and radiomics in pulmonary nodule management: current status and future applications." Clinical radiology 75.1 (2020): 13-19. [CrossRef]
- Ferrari, R., Mancini-Terracciano, C., Voena, C., Rengo, M., Zerunian, M., Ciardiello, A., Grasso, S., Mare, V., Paramatti, R., Russomando, A., Santacesaria, R., Satta, A., Solfaroli Camillocci, E., Faccini, R., & Laghi, A. (2019). MR-based artificial intelligence model to assess response to therapy in locally advanced rectal cancer. European Journal of Radiology, 118. [CrossRef]
- Cozzi D, Bicci E, Cavigli E, Danti G, Bettarini S, Tortoli P, Mazzoni LN, Busoni S, Pradella S, Miele V. Radiomics in pulmonary neuroendocrine tumours (NETs). Radiol Med. 2022 Jun;127(6):609-615. Epub 2022 May 10. PMID: 35538389. [CrossRef]
- Caruso D et al. "Radiomics in oncology, part 1: Technical principles and gastrointestinal application in CT and MRI." Cancers 13.11 (2021): 2522. [CrossRef]
- De Santis D et al. "Radiomics analysis in gastrointestinal imaging: a narrative review." Digestive Medicine Research (2023): 1-13.
- Wesdorp, Nina J., et al. "Advanced analytics and artificial intelligence in gastrointestinal cancer: a systematic review of radiomics predicting response to treatment." European journal of nuclear medicine and molecular imaging 48 (2021): 1785-1794. [CrossRef]
- Wang, Yue, et al. "Potential value of CT radiomics in the distinction of intestinal-type gastric adenocarcinomas." European Radiology 30 (2020): 2934-2944. [CrossRef]
- Granata V, Fusco R, De Muzio F, Cutolo C, Setola SV, Dell’Aversana F, Grassi F, Belli A, Silvestro L, Ottaiano A, Nasti G, Avallone A, Flammia F, Miele V, Tatangelo F, Izzo F, Petrillo A. Radiomics and machine learning analysis based on magnetic resonance imaging in the assessment of liver mucinous colorectal metastases. Radiol Med. 2022 Jul;127(7):763-772. Epub 2022 Jun 2. PMID: 35653011. [CrossRef]
- Chiti G, Grazzini G, Flammia F, Matteuzzi B, Tortoli P, Bettarini S, Pasqualini E, Granata V, Busoni S, Messserini L, Pradella S, Massi D, Miele V. Gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs): a radiomic model to predict tumor grade. Radiol Med. 2022 Sep;127(9):928-938. Epub 2022 Aug 2. PMID: 35917099. [CrossRef]
- Palatresi D, Fedeli F, Danti G, Pasqualini E, Castiglione F, Messerini L, Massi D, Bettarini S, Tortoli P, Busoni S, Pradella S, Miele V. Correlation of CT radiomic features for GISTs with pathological classification and molecular subtypes: preliminary and monocentric experience. Radiol Med. 2022 Feb;127(2):117-128. Epub 2022 Jan 12. PMID: 35022956. [CrossRef]
- Galluzzo A, Boccioli S, Danti G, De Muzio F, Gabelloni M, Fusco R, Borgheresi A, Granata V, Giovagnoni A, Gandolfo N, Miele V. Radiomics in gastrointestinal stromal tumours: an up-to-date review. Jpn J Radiol. 2023 May 12. Epub ahead of print. PMID: 37171755. [CrossRef]
- Santini D, Danti G, Bicci E, Galluzzo A, Bettarini S, Busoni S, Innocenti T, Galli A, Miele V. Radiomic Features Are Predictive of Response in Rectal Cancer Undergoing Therapy. Diagnostics (Basel). 2023 Aug 2;13(15):2573. PMID: 37568936; PMCID: PMC10417449. [CrossRef]
- Brunese MC, Fantozzi MR, Fusco R, De Muzio F, Gabelloni M, Danti G, Borgheresi A, Palumbo P, Bruno F, Gandolfo N, Giovagnoni A, Miele V, Barile A, Granata V. Update on the Applications of Radiomics in Diagnosis, Staging, and Recurrence of Intrahepatic Cholangiocarcinoma. Diagnostics (Basel). 2023 Apr 20;13(8):1488. PMID: 37189589; PMCID: PMC10137417. [CrossRef]
- Pesapane, F., Rotili, A., Penco, S., Nicosia, L., & Cassano, E. (2022). Digital twins in radiology. Journal of Clinical Medicine, 11(21), 6553.
Table 2.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



