
Submitted:
18 January 2024
Posted:
19 January 2024
You are already at the latest version
Abstract
Performance of the overhead squat may affect golf swing mechanics associated with golf-related low back pain. This study investigates the difference in lumbar kinematics and joint loads during the golf downswing between golfers with different overhead squat abilities. Based on the per-formance of the overhead squat test, 21 golfers aged 18 to 30 years were divided into the highest-scoring group (HS, N=10, 1.61 ± 0.05 cm, and 68.06 ± 13.67 kg) and lowest-scoring group (LS, N=11, 1.68 ± 0.10 cm, and 75.00 ± 14.37 kg). Data collection used a motion analysis system, two force plates, and TrackMan. OpenSim software was used to simulate the joint loads for each lum-bar joint. An independent t-test was used for statistical analysis. Compared to golfers demonstrat-ing limitations in the overhead squat test, golfers with better performance in the overhead squat test demonstrated significantly greater angular extension displacement on the sagittal plane, smaller lumbar extension angular velocity, and smaller L4-S1 joint shear force. Consequently, the overhead squat test is found to be a useful index to reflect lumbar kinematics and joint loading patterns during the downswing, and provides a good training guide reference for reducing the risk of a golf-related low back injury
Keywords:
Golf Swing
; Shear force
; Compressive force
; squat
; LBP
1. Introduction
Golf has become an increasingly popular sport worldwide and is viewed as an enjoyable and practical means of staying active throughout an individual’s lifetime. Previous studies have demonstrated that playing golf provides an adequate amount of physical activity to improve overall health and well-being, especially for elderly golfers whose physiological training threshold is lowered by age [1,2]. While golf can provide some benefits for general health and fitness, the sport also appears to have particular risks of injury that may significantly affect players’ enjoyment of the activity [3].
Along with its popularity, the injury rate for golfers has indeed increased steadily over the years, with golf-related low-back pain (LBP) being the most common injury [4,5,6]. There are several factors that may contribute to LBP, including poor swing mechanics and fatigue due to overuse [7]. Rapidly swinging a club is a crucial part of the golf game. In order to create a potential advantage at the beginning of the competition, golfers tend to dedicate considerable practice time for swings each day to generate a fast and powerful swing. Poor swing mechanics combined with the overuse problem may ultimately increase the risk of LBP for golfers. Furthermore, along with improper swing mechanics, sub-optimal physical fitness could produce considerable or abnormal forces localized in the lumbar region [8]. This can cause significant muscle spasms due to back muscle strain or spinal ligament sprain, which usually leads to the development of LBP.
To identify physical deficiencies that are critical to the golf swing and injury prevention, the world’s leading golf education organization, Titleist Performance Institute (TPI), has developed a golf-specific physical screening system similar to the Functional Movement Screen (FMSTM). The TPI has identified some inappropriate swing mechanics that they categorize as “swing faults” to help coaches and golfers better understand swing mechanics and improve their game.
The FMSTM is comprised of seven fundamental movement patterns (tests) that require a balance of mobility and stability [9]. The overhead squat (OHS) is one such test that the FMSTM uses to assess bilateral, symmetrical, and functional mobility of the hips, knees, ankles, shoulders, and thoracic spine, as well as the stability and motor control of core musculature [10]. The TPI also uses the OHS test as one of its movement screens to assess golfers’ strength, flexibility, and balance [11]. An individual with restrictions on spine mobility, hip mobility, or core motor function may fail the OHS test.
Studies on OHS performance have identified some swing faults that are documented by TPI [11]. One of the most common swing faults among amateur golfers is known as “loss of posture” [12], where the golfer has changed the knee flexion angle, trunk flexion angle, or head position between their address posture and impact position [11]. Another common swing fault is “slide,” which is an excessive lateral shift of the hips toward the target on the downswing. Gulgin and his colleagues found that golfers with low overhead squat ability were two to three times more likely to exhibit early hip extension, loss of posture, or slide during the swing in comparison to golfers who could correctly perform an OHS [11]. They further suggested that common swing faults are linked to inconsistent ball striking and reduced performance [11]. Speariett and Armstrong found that the overhead squat is one of the most difficult tests for amateur golfers to perform, so much so that participants who were unable to perform the overhead squat most commonly presented with loss of posture (90%) and slide (80%) [12].
The mechanics of the spine during a golf swing in golfers with or without LBP has been well established. Compared to healthy golfers, those with LBP may generate more lateral bending accompanied by flexion of the spine during the downswing phase [13,14]. Fortunately, professional golfers possess the capability to minimize the recurrence of injuries through technical adjustments [15,16]. Grimshaw and Burden reported the successful elimination of golf-related LBP in professional golfers, partly from reducing the amount of trunk flexion and by adopting a side-bend during the downswing [15]. The side-bend with trunk flexion can limit the amount of trunk rotation available during the golf swing and may apply more shear force to the spine, thus increasing the risk of injury [17]. The physical requirements of the golf swing may be similar to that of the OHS. Likewise, limitations in the mobility of the hip and spine or weaknesses of the core muscles may cause golfers to compensate through the loss of posture and slide.
Golfers with LBP have shown lower hip and spine mobility, and delaying core muscle activation compared to healthy golfers [1,18,19]. Considering that both the golf swing and OHS demand normal function of the core, lower limb, and shoulder mobility in three-dimensional space, the FMS over-head squat which also evaluate core, lower limb, and shoulder mobility maybe a useful test that can assess all of these elements simultaneously. It may therefore be possible to prevent LBP by using the OHS as a test to assess players’ spinal biomechanics during the golf downswing. To the best of our knowledge, no study to date has investigated the impact of overhead squat abilities on lumbar spine flexion and lateral bending biomechanical variables of golf swing.
To understand the mechanisms of LBP, scientists have developed different methodologies that measure the lumbar joint loads during the golf swing. For example, Hosea and his colleagues found that lumbar spine shear force during the golf swing was 80 percent greater in amateurs than in professionals, where the compressive force for both groups was more than eight times body weight (BW) [20]. However, the different methodologies used in these studies may have affected the results obtained. For example, Lim and his colleagues and Hosea found that shear loads were about 1.6 BW to 0.6 BW while the peak compressive loads were greater than 8 BW [20,21]. Although both studies found the lumbar joint loads to increase continuously during the downswing phase there was less agreement in the lumbar shear loads. To address these conflicting results, the current study used a computer modelling and simulation approach to calculate lumbar joint forces during the downswing.
The primary purpose of this study was to determine differences in lumbar spine kinematics and joints loads during the downswing between golfers who execute a proper OHS and those who do not. A secondary aim was to investigate whether the ability of a golfer to perform the OHS test is related to their golf swing performance. We hypothesized that golfers who can perform the overhead squat properly would produce smaller lumbar spine’s joint loads, joint angular displacements, and joint angular velocities on L1-L2, L2-L3, L3-L4, L4-L5, L5-S1 joints during the downswing, and hence better performance compared to golfers who could not complete the OHS test.
2. Materials and Methods
2.1. Participants
Twenty-one right-handed golfers aged 18 to 30 years volunteered to participate in this study. All participants were free of any musculoskeletal injuries or disease that would have prevented them from performing their normal golf swing motion or impeded their ability to participate in the overhead deep squat screen. The study was conducted with ethics approval from the Human Research Ethics Committee of the local institution, and participants provided their written informed consent prior to commencement of testing.
2.2. Experimental Protocol
All experiments were conducted in the Biomechanics Laboratory at National Taiwan Sports University. On arrival, each participant was informed of the study’s purpose and the experimental protocol. Testing was divided into two parts. Each golfer’s overhead squat performance was first measured using the FMSTM kit, after which a biomechanical evaluation of the golf swing was performed using three-dimensional video motion capture techniques.
2.3. Overhead Squat Test
The verbal test instruction of the overhead squat test was based on the description given by Cook [9], where one certified FMSTM instructor executes the test. For the test, every individual wore their personal sneakers and positioned themselves by placing their feet about shoulder-width apart and in alignment with the sagittal plane. After that, they held onto a rod while keeping their elbows flexed at a 90-degree angle with the rod positioned above their heads. Then, the rod was lifted above by raising both shoulders and straightening the arms. Next, the participants were given directions to crouch down as much as they could, ensuring that their heels remained in touch with the ground and the dowel stayed directly above them. Each participant was allowed up to three trials to perform the test successfully. Scoring criteria for the OHS (see Table 1) were used to divide all participants into a high scoring group (HS: 3 points, Figure 1a) and a low scoring group (LS: 2 points or 1 point, Figure 1b&1c) for further analysis.
2.4. Kinematic and Kinetic Data Collection
The kinematic data of each participant’s golf swing using a driver was recorded using an 11 Eagle Digital high-speed camera system (Motion Analysis Corporation, Santa Rosa, USA) that sampled at 250 Hz. On both sides, anatomical landmarks such as the front of the head, rear head, cervical 7, thoracic 10, acromion, upper arm, lateral elbow, radius, ulna, third metacarpophalangeal joint, anterior superior iliac spine, posterior superior iliac spine, thigh, knee, shank, ankle, medial ankle, toe, and heel were marked with forty-nine retro-reflective markers measuring 10-12 mm in diameter (see Figure 2). During the swing, ground reaction force data from the lead and trailing legs were collected using two force plates (AMTI, Advanced Management Technology Inc), with a sampling rate of 1000 Hz. The force information is synchronized with the motion analysis system. A fourth-order low-pass Butterworth filter with a cut-off frequency of 14 Hz was used to filter the kinematic and ground force data. The kinematic and kinetic data were used as input to a musculoskeletal modeling pipeline available in OpenSim to calculate lumbar spine kinematics and joint loading [22].
For the lower lumbar region of the longissimus thoracic, a pair of wireless EMG sensors (Trigno, Delsys Inc., Natick, MA, USA) were placed on the interspace between L1 and L2 on both sides. The EMG and kinematic data were synchronized using a video camera connected to the EMG system, which recorded the golf swing and displayed the images in real time along with the EMG signals in the Delsys EMGworks software (Delsys Inc., Natick, MA, USA). Electromyographic data were filtered (six-pole Butterworth and bandpass filtered 25-500 Hz) and full-wave rectified using signal processing software (EMGworks Analysis software) .
Each participant was given 5 minutes to warm up prior to data collection. The participant was then instructed to stand on the force plates and perform a maximal swing using the driver. Data were collected for 5 trials. The TrackMan (TrackMan IIIe, Vedbaek, Denmark) Doppler radar system was placed behind the ball striking area to measure the speed of the ball after impact.
2.5. Computer Simulation
The full-body lumbar spine model (FBLS, https://simtk.org/home/fullbodylumbar) comprising 21 segments, 30 degrees of freedom, and 324 musculotendon actuators was used to simulate each golf swing [23]. Before the motion capture, the marker setting of FBLS model was modified for scale, so the model and motion capture data could be matched to fit. All data were converted to a useable format, the generic musculoskeletal model was scaled to match each participant’s body anthropometry [22]. The inverse kinematics routine in OpenSim was then used to minimize differences between the positions of skin markers on the participants and virtual markers on the model. This procedure was undertaken in order to achieve a dynamically consistent set of kinematics and kinetics that best matched the experimentally collected data [22].
To investigate the primary aim of this study, results of inverse kinematics were used to derive the lumbar joint angle during impact in the sagittal and frontal plane, peak angular velocity, and angular displacement during the downswing phase in the sagittal and frontal plan.
Next, static optimization (SO) was performed to resolve the net joint moments into individual muscle forces at each instant in time. Finally, the joint reaction analysis tool was used to calculate the internal vertebral joint loads [24]. Lumbar spinal loading was calculated by solving the dynamical equations of motion with the input of muscle forces, gravity, and inertia. Moreover, to attenuate the noise contained within the raw marker data, a filtering process was applied during static optimization, using a low-pass sixth-order Butterworth digital filter at a cut-off frequency of 14 Hz, which was determined based on residual analysis. All loads reported for a given vertebra were those acting upon it from the inferior vertebra. For example, the L5-S1 loads reported are those from S1 acting on L5. The force was calculated using the Newton’s 2nd Law:
where is the force applied by the S1 vertebra to the L5 vertebra, is the matrix of inertial properties of the L5 vertebra, is a vector of angular and linear accelerations of the L5 vertebra, is the force applied by the L4 vertebra to the L5 vertebra, and and are muscle forces and gravitational forces acting on the L5 vertebra. The L5-S1 compressive force was calculated as the component of parallel to the longitudinal axis of the L5 vertebra, which was used for all subsequent analyses. The L5-S1 shear force was calculated the same way, but parallel to the anteroposterior axis of the L5 [24]. Peak shear and compressive forces acting at each lumbar spine joint, specifically, L1-L2, L2-L3, L3-L4, L4-5, and L5-S1, were calculated and used in the statistical analyses described below.
Finally, model simulations were validated by comparing the muscle activations calculated in the model against EMG data measured during the golf swing. The EMG data were normalized by the peak activation measured during the swing phase and was compared to simulated muscle activations, which were defined between 0 and 1. We compared the average activation of the longissimus thoracic muscle of 4 subjects to the corresponding EMG (Figure 3).
2.6. Statistical Analyses
Descriptive statistics were analyzed to assess means and standard deviations between the low scoring group (LS) and high scoring group (HS). A Pearson’s chi-square test was used to compare gender distributions, and an independent t-test was used to determine significant differences in demographic and performance data between different groups. An independent t-test was used to examine differences in all lumbar kinematics and joint loads during the downswing phase of the golf swing between the LS and HS groups. The Pearson correlation is used to tested between the measured EMG and simulated activation level through time series for each muscle to validate the model. Statistical significance was set at p < 0.05, and SPSS 20.0 (SPSS, Chicago, IL) statistical software was used for all data analysis.
3. Results
The Pearson’s chi-squared test showed no significant difference in the gender distribution of the groups, χ2(1, N = 21) = 2.38, p =.123. No significant difference was found between LS and HS in body weight, height, played years, and best scores, except for ball speed of LS (M=142.44, SD=16.95 mph), which was faster than HS (M=126.29, SD=11.52 mph), p=.02, (Table 2).
For simulation validation, both sides of the longissimus thoracic muscle activations were consistent with the measured EMG data (Figure 2). The correlation of normalized measured EMG data and the simulated activations for 4 subjects on the right lumber muscle is 0.72±0.09 and left is 0.74±.21.
3.1. Lumbar Joint Kinematics during the Downswing
There was no significant difference between the two groups in the sagittal-plane lumbar flexion angle at impact and sagittal-plane peak flexion angular velocity during the downswing (Table 3). However, the HS had significantly greater lumbar angular displacement from top to impact (M=24.36, SD=7.11 °, p = .03) and smaller peak extension angular velocity during the downswing (M=40.51, SD=26.79 °/s) compared to LS (M=17.72, SD=5.94 °; M=119.52, SD=59.23 °/s), p = 001 (Table 3). In the frontal plane, there was no significant difference found between the two groups in lumbar right-side bending angle at impact, angular displacement from top to impact, and peak right-side bending angular velocity during the downswing (Table 4).
3.2. Lumbar Joint Loads during the Downswing
Not all lumbar joints were significantly affected by the overhead squat ability in relation to the shear forces applied in the anterior-posterior direction (Table 5). The HS had significantly lower shear forces applied at L4-L5 (M=299.54, SD=37.30 N) (p = .01) and L5-S1 (M=407.90, SD=59.06 N) (p=.002) during the downswing compared to LS (M=387.19, SD=89.16 N; M=525.19, SD=86.69 N). There was no significant difference between the two groups in the compressive forces applied at L1-L2, L2-L3, L3-L4, L4-L5, and L5-S1 during the downswing (Table 6).
4. Discussion
4.1. Influence of OHS on Golf Performance
The primary objective of this study was to investigate whether limitations in performing an overhead squat affects golf swing performance. Participants were placed into one of two groups depending on their ability to perform the overhead squat. There was no significant difference in the best golfing scores between the two groups, however, the ball speed of the LS (M=142.44, SD=16.95 mph) was significantly greater than that of the HS (M=126.29, SD=11.52 mph). Although restricting the hip and shoulder joints has been shown to impair golf swing performance [25], this study failed to identify a significant difference in performance among golfers with different overhead squat abilities with elite golfers. However, it did show the difference of swing kinematics and kinetics on lumber between groups. It demonstrates the elite golfers with the limited squat ability adopt different swing pattern to keep competitive.
Overall golfing performance consists of driving distance, driving accuracy, approach accuracy, and putting, combined with physical attributes [26]. Furthermore, more than one swing is needed during a competition. Our results indicate that golfers with poor OHS ability in the LS group may have a low golf swing efficiency, suggesting that they need to generate greater ball speed to create an advantage when teeing off at the beginning of a hole, and ultimately achieve similar performance in terms of handicap to the HS golfers. The OHS test may therefore be an indicator of the efficiency of the golf game and hence overall performance which including accuracy in any condition.
4.2. Influence of OHS on Lumbar Spine Kinematics in the Sagittal Plane
Contrary to our hypothesis, we found that greater overhead squat ability may result in an advantage for utilizing more lumbar spine angular displacement in the sagittal plane (extension) to perform the golf downswing instead of lumbar spine angular extension velocity, and reduce shear force. In the lumbar spine, rotation is restricted by the annulus anteriorly and the facet joints posteriorly [27]. Although the lumbar spine’s rotation ability is limited, this ability might also be affected by the flexibility of lumbar flexion-extension. Burnett et al. found that the range of lumbar spine axial rotation decreased in end-range flexion and extension postures compared to the neutral spine posture [28]. This suggests that the LS golfers may achieve the end of lumbar flexion or extension earlier than the HS golfers due to the difference in flexibility of the lumbar spine. Once the lumbar spine is at the end-range flexion position, the ability to rotate may be restricted. In addition, axial loading of the spine in end-range flexion sagittal postures may provide a greater risk of injury if the soft tissues are loaded beyond their tolerance level, as this is the position where the passive structures appear to be at their maximal stiffness [28]. Rotating beyond the point of soft-tissue tolerance may contribute to LBP by increasing the shear force acting on the intervertebral disc [29,30].
For accurate contact with the ball, increased trunk flexion is required to return the clubface to the initial set-up position during the downswing at ball impact [31]. However, the lumbar spine will move toward extension before impact. This phenomenon may occur because of the proximal-to-distal sequencing theory [32], which proposes that for best energy transfer and maximum club head speed in the downswing, all segments should accelerate and then decelerate before impact with the ball. This kinematic sequence has been analyzed in golfers with different skill levels. Compared to amateur golfers, professional golfers show a slowing of the pelvis before impact, suggesting that pelvic deceleration before impact is a desirable trait for fast swings [33]. Golfers indeed tend to lock their pelvis before impact to generate a faster club head speed.
Grimshaw and Burden proposed that golfers might maintain a more stationary spine movement during the downswing after 3 months of core stability as well as spinal and hip mobility training [15]. By improving the stability of the core and the mobility of the spine and hip, the activity level of the erector spinae may be less in the HS group as these muscles are no longer required to produce a powerful eccentric contraction to decelerate the rapid motion of the trunk observed in the LS group [15]. This reduction in muscle activation level may reduce lumbar vertebrae joint loads during the golf swing [8,20]. Although Lindsay and Horton found that while there was no significant difference in peak lumbar extension angular velocity between healthy golfers and golfers with LBP, but the magnitude of peak lumbar angular velocity was slightly larger in golfers with LBP [34], which is consistent with results obtained in this study for the HS and LS groups. Compared with the LS, golfers in the HS do not therefore need to generate a relatively high opposite velocity to lock or stop their pelvis to generate a powerful swing, because they have better mobility of the hip and spine joints and better core neuromuscular control. Furthermore, for the same amount of downswing time in both groups, the rapid velocity applied to the lumbar spine may cause a higher joint force in the LS, which in turn may exacerbate symptoms of LBP.
4.3. Impact of OHS on Lumbar Spine Kinematics in the Frontal Plane
After the top of the backswing, the spine should continuously bend towards the right side to hit the ball to the leading (left) side. The increased lateral bending on the lumbar segment’s trailing (right) side at impact may lead to spinal injuries [35]. Our results do not show a difference in lumbar right-side bending angle at impact between the HS and LS groups. By comparison, the left hip internal rotation flexibility is shown to be more suitable. Kim et al. found that the lumbar side bending angle at impact is different between golfers with and without limited hip internal rotation [35]. The golfer without this hip limitation demonstrated a smaller side bending angle at impact, and the left hip internal rotation angle of golfers without the limitation was also greater than that of golfers with limitations at impact [35].
The lumbar side bending angular displacement during the golf downswing is purported to be associated with LBP. However, several studies have found there was no significant difference in the lumbar side bending angular displacement between golfers with and without LBP, or in those with and without limitations in left hip internal rotation [34,35,36]. Cole and Grimshaw also found no significant difference in the lumbar right-side bending angle at impact among golfers with and without LBP [36]. This demonstrates that the right-side bending angle at impact alone may not be sufficient to fully characterize LBP risk.
Although the lumbar side bending angular displacement during the downswing does not appear to be a sensitive measure for distinguishing golfers with LBP from asymptomatic players, Grimshaw and Burden found that after 3 months of coaching focused on improving swing technique, the reduction in the amount of side bending during the downswing helped reduce LBP symptoms that may arise due to chronic overuse [15]. Furthermore, our results indicate that the hip joint and spine joint restrictions have no effect on the lumbar side bending angular displacement during the downswing, which is consistent with the finding by Kim et al. [35]. This suggests that the side bending of the lumbar spine during the downswing is insufficient in revealing the risk of LBP, where use of the physical ability test like OHS shows that lateral bending during the golf downswing may be inappropriate.
Glazier suggested that replacing positional lateral bending data with instantaneous torso lateral bending velocity may better correspond with injury development risk [37]. However, similar to our results, Lindsay and Horton found no difference in the right-side bending velocity in golfers with and without LBP [14]. This may be because of the club difference, where the 7-iron, for example, requires a more vertical swing plane that may produce more lateral motion on the downswing than the driver. Furthermore, Bae et al. found that the lumbar flexion-extension joint power was significantly larger than that of the lumbar lateral bend during the downswing phase [38]. This indicates that the generation of lumbar rotation action during the downswing might be emphasized more in the sagittal plane more than in the frontal plane.
4.4. Impact of OHS on Lumbar Spine Loads
The golf swing is regarded as a three-dimensional movement, with restriction in the spine and hip mobility that may affect the lumbar joint loads and precipitate LBP. Significant differences have been identified in this study between the HS and LS groups in L4-L5 and L5-S1 peak shear forces; in particular, our results indicate that golfers who had better performance in the OHS test also had lower loads applied to the lumbar spine during the downswing. These individuals may therefore have less risk of a golf-related low back injury.
To the best of our knowledge, this is the first study to investigate the relationship between the overhead squat ability and lumbar spine loads during the golf downswing using computer simulation. Peak shear force applied to the L5-S1 joint in the LS group (525.19 ± 86.69, N) was similar to the result reported by Hosea et al. (596 ± 514, N) [20]. Furthermore, shear loads of similar magnitude (i.e., 570 ± 190 N) were seen to produce pars interarticularis fractures with cyclic loading in cadaver specimens [39,40]. Sugaya et al. found that the golf swing’s asymmetrical pattern may cause the degeneration of the right lumbar spine around L4-L5 in right-handed golfers [41]. Moore and Dalley further suggested that most spinal disc herniations occur in the lumbar spine, with 95 percent at L4-L5 or L5-S1 [42]. The current study also found that golfers with limitations in the overhead squat may generate a higher shear force applied to the L5-S1 and L4-L5 joints. Considering that these two joints have the highest risk of injury, applying the OHS as a test tool may provide some useful information for coaches to prevent golf-related low back pain.
Lim et al. proposed that the L4-L5 disc and L5-S1 disc are subjected to large compressive loads due to the weight of the trunk and muscle activity generated during the golf swing [21]. Hosea and his colleagues performed the first two studies that assessed joint loads during the golf swing. They found that compression loads were up to 8 times body weight, or about 6100 ± 2413 N in amateurs and 7584 ± 2422 N in professionals during the golf swing [8,20]. Compressive forces ranging from 3018.92 ± 233.43 N to 3921.69 ± 450.25 N) calculated in the present study are lower than Hosea’s results, but similar to findings reported by Lim et al. [21]. Lim and colleagues proposed that the compressive load consistently increased after the top of the backswing and reached its maximum (4400 N or 6.1 BW) near ball impact [21]. Differences in these results may be due to differences in the methodology used to calculate joint loads in these studies. This is especially the case in studies by Hosea et al. [20], where measured ground reaction forces were not used in the calculation of the lumbar loads [21]. However, none of the above studies reported the compressive loads in each lumbar disc joint. Since the range of motion and stiffness value for each lumbar joint is different, it seems necessary to calculate the joint loads in each lumbar disc joint using computerized simulation methodology. As noted in the current study, the compressive load gradually decreased from S1 to L1 during the downswing phase, which agrees with a simulation study by Bae et al. [38]. This also indicates that the inferior region of the lumbar spine may be at a higher risk of injury than the superior region.
5. Conclusions
We presented the difference in lumbar spine kinematics and joint loads during the golf downswing between golfers with different overhead squat abilities. Golfers with better performance in the overhead squat test demonstrated significantly greater angular extension displacement in the sagittal plane, lower lumbar extension angular velocity, and lower L4-S1 joint shear force compared to golfers with lower performance in the overhead squat test. Due to the requirements of performing the overhead squat, better performance in this test also reflects an advantage in hip and spine flexibility and core stability, which are associated with swing mechanics and risk of LBP. The study’s findings therefore suggest that the overhead squat test can be a useful index in assessing the lumbar kinematics and joint loading patterns during the downswing, and provides a training guide reference to reduce the risk of a golf-related low back injury.
There are several limitations of the current study. First, while different club types could affect lumbar swing kinematics [34,43] and hence the loads applied to the lumbar spine during the downswing phase. Further study is needed to investigate the relationship between the overhead squat ability and lumbar loads during the downswing when an iron club is used. Second, the highest L4-L5 shear loads were found after ball impact [21]. However, the joint loads are also applied to the lumbar spine during the follow-through, and the end of the follow-through is also considered a critical element related to LBP in the golf swing [44]. Future work should examine lumbar kinematic and kinetic variables in the follow-through phase of the golf swing in order to extend the impact of the overhead squat ability on the lumbar joint loading.
Third, the current study only examined lumbar kinematics and joint loads in the sagittal and frontal planes. Axial rotation of the lumbar spine is associated with ball speed, although an over-rotated lumbar spine might result in excess loads that relate to LBP [45,46]. Rapid spinal rotation during the golf swing, combined with physical limitations, may play a role in golf-specific injuries [47]. Hence, additional research may prove beneficial for LBP prevention by investigating the difference in lumbar rotation kinematics between golfers with different overhead squat abilities. Finally, participants in the current study were healthy golfers free from any injuries that may have prevented them from performing the golf swing. To better understand the chronic impact of overhead squat ability on the risk of LBP during the golf swing, the next logical step is to investigate the difference in low back injury rates between HS and LS over time. In this way, the effect of the overhead squat test on LBP prevention could be studied.
Author Contributions
All authors discussed and formulated this study. The manuscript was drafted by Z.-H.C., and W.-T.T. M.P. also contributed to reviewing and editing this manuscript. Conceptualization, Z.-H.C. and W.-T.T.; formal analysis, Z.-H.C. and W.-T.T.; investigation, W.-T.T., T.-Y.H. and Z.-H.C; data curation, Z.-H.C., T.-Y.H. and W.-T.T.; writing—original draft preparation, Z.-H.C., and W.-T.T.; writing— review and editing, M.P. and W.-T.T.; supervision, W.-T.T. and M.P. All authors confirmed the final version before submission. All authors have read and agreed to the published version of the manuscript.
Funding
This study was partially supported by funding from the National Science and Technology Council, Taiwan, grant no. MOST 107-2410-H179-002-MY2.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Fu Jen Catholic University Institutional Review Board Hospital Institutional Review Board (C105069).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data are contained within the manuscript.
Conflicts of Interest
This research, entitled “Relationship Between Overhead Squat Performance and Lum-bar Spine Loads During the Golf Downswing”, has no conflict of interest with regard to personal, financial, professional, political, or legal interests that could have a significant chance of interfering with performance or ethical or legal duties.
References
- Lindsay, D. M., & Vandervoort, A. A. (2014). Golf-related low back pain: a review of causative factors and prevention strategies. Asian journal of sports medicine, 5(4). [CrossRef]
- Versteegh, T. H., Vandervoort, A. A., Lindsay, D. M., & Lynn, S. K. (2008). Fitness, performance and injury prevention strategies for the senior golfer. International Journal of Sports Science & Coaching, 3(1_suppl), 199-214. [CrossRef]
- Cann, A. P., Vandervoort, A. A., & Lindsay, D. M. (2005). Optimizing the benefits versus risks of golf participation by older people. Journal of geriatric physical therapy, 28(3), 85-92. [CrossRef]
- Batt, M. E. (1993). Golfing injuries. An overview. Sports Medicine (Auckland, NZ), 16(1), 64-71. [CrossRef]
- McCarroll, J. R., & Gioe, T. J. (1982). Professional golfers and the price they pay. The Physician and Sportsmedicine, 10(7), 64-70. 7. [CrossRef]
- Gosheger, G., Liem, D., Ludwig, K., Greshake, O., & Winkelmann, W. (2003). Injuries and overuse syndromes in golf. The American journal of sports medicine, 31(3), 438-443. 3. [CrossRef]
- McHardy, A. J., Pollard, H. P., & Luo, K. (2007). Golf-related lower back injuries: an epidemiological survey. Journal of chiropractic medicine, 6(1), 20-26. [CrossRef]
- Hosea, T. M., & Gatt Jr, C. J. (1996). Back pain in golf. Clinics in sports medicine, 15(1), 37-53. 1. [CrossRef]
- Cook, G., Burton, L., & Hoogenboom, B. (2006). Pre-participation screening: the use of fundamental movements as an assessment of function–part 1. North American journal of sports physical therapy: NAJSPT, 1(2), 62.
- Kritz, M., Cronin, J., & Hume, P. (2009). The bodyweight squat: A movement screen for the squat pattern. Strength & Conditioning Journal, 31(1), 76-85. [CrossRef]
- Gulgin, H. R., Schulte, B. C., & Crawley, A. A. (2014). Correlation of Titleist Performance Institute (TPI) level 1 movement screens and golf swing faults. The Journal of Strength & Conditioning Research, 28(2), 534-539. [CrossRef]
- Speariett, S., & Armstrong, R. (2019). The relationship between the Golf-Specific Movement Screen and golf performance. Journal of sport rehabilitation, 29(4), 425-435. [CrossRef]
- Morgan, D., Sugaya, H., Banks, S., & Cook, F. (1997, September). A new ‘twist’on golf kinematics and low back injuries: the crunch factor. In 21st Annual Meeting of the American Society of Biomechanics (pp. 24-27).
- Lindsay, D. M., Horton, J. F., & Paley, R. D. (2002). Trunk motion of male professional golfers using two different golf clubs. Journal of applied biomechanics, 18(4), 366-373. [CrossRef]
- Grimshaw, P. N., & Burden, A. M. (2000). Case report: reduction of low back pain in a professional golfer. Medicine and science in sports and exercise, 32(10), 1667-1673. [CrossRef]
- Lin, Z. J., Peng, Y. C., Yang, C. J., Hsu, C. Y., Hamill, J., & Tang, W. T. (2023). Lower Limb Biomechanics during the Golf Downswing in Individuals with and without a History of Knee Joint Injury. Bioengineering, 10(5), 626. [CrossRef]
- Geisler, P. R. (2001). Golf. In E. Shamus & J. Shamus (Eds.), Sports Injury: Prevention & Rehabilitation. New York: McGraw-Hill Co (pp. 185-225).
- Dolan, P., & Adams, M. A. (1993). Influence of lumbar and hip mobility on the bending stresses acting on the lumbar spine. Clinical Biomechanics, 8(4), 185-192. 4. [CrossRef]
- Horton, J. F. (2000). Abdominal muscle characteristics of elite male golfers with and without chronic low back pain. Kinesiology.
- Hosea, T. M., Gatt, C. J., Galli, K. M., Langrana, N. A., & Zawadsky, J. P. (1990). Biomechanical analysis of the golfer’s back. In A. J. Cochran (Ed.), Science and Golf: Proceedings of the First World Scientific Congress of Golf. New York: E. & F. N. Spon (pp. 43-48).
- Lim, Y. T., Chow, J. W., & Chae, W. S. (2012). Lumbar spinal loads and muscle activity during a golf swing. Sports biomechanics, 11(2), 197-211. 2. [CrossRef]
- Delp, S. L., Anderson, F. C., Arnold, A. S., Loan, P., Habib, A., John, C. T., ... & Thelen, D. G. (2007). OpenSim: open-source software to create and analyze dynamic simulations of movement. IEEE transactions on biomedical engineering, 54(11), 1940-195. [CrossRef]
- Raabe, M. E., & Chaudhari, A. M. (2016). An investigation of jogging biomechanics using the full-body lumbar spine model: Model development and validation. Journal of biomechanics, 49(7), 1238-1243. [CrossRef]
- Steele, K. M., DeMers, M. S., Schwartz, M. H., & Delp, S. L. (2012). Compressive tibiofemoral force during crouch gait. Gait & posture, 35(4), 556-560. [CrossRef]
- Sell, T. C., Tsai, Y. S., Smoliga, J. M., Myers, J. B., & Lephart, S. M. (2007). Strength, flexibility, and balance characteristics of highly proficient golfers. The Journal of Strength & Conditioning Research, 21(4), 1166-1171. [CrossRef]
- Sato, K., & Kenny, I. C. (2013). Current golf performance literature and application to training. Journal of Trainology, 2(2), 23-32. 2. [CrossRef]
- Haher, T. R., O’Brien, M., Kauffman, C., & Liao, K. C. (1993). Biomechanics of the spine in sports. Clinics in sports medicine, 12(3), 449-464. 3. [CrossRef]
- Burnett, A., O’Sullivan, P., Ankarberg, L., Gooding, M., Nelis, R., Offermann, F., & Persson, J. (2008). Lower lumbar spine axial rotation is reduced in end-range sagittal postures when compared to a neutral spine posture. Manual therapy, 13(4), 300-306. [CrossRef]
- Vad, V. B., Bhat, A. L., Basrai, D., Gebeh, A., Aspergren, D. D., & Andrews, J. R. (2004). Low back pain in professional golfers: the role of associated hip and low back range-of-motion deficits. The American journal of sports medicine, 32(2), 494-497. [CrossRef]
- Bogduk, N., & Twomey, L. T. (1997). Clinical anatomy of the lumbar spine and sacrum New York: Churchill Livingstone. Journal of Anatomy, 134, 383-297.
- Joyce, C., Burnett, A., Cochrane, J., & Ball, K. (2013). Three-dimensional trunk kinematics in golf: between-club differences and relationships to clubhead speed. Sports Biomechanics, 12(2), 108-120. [CrossRef]
- Putnam, C. A. (1993). Sequential motions of body segments in striking and throwing skills: descriptions and explanations. Journal of biomechanics, 26, 125-135. [CrossRef]
- Crews, D., & Lutz, R. (2007). Comparison of kinematic sequence parameters between amateur and professional golfers. Science and golf, 5, 30-36.
- Lindsay, D., & Horton, J. (2002). Comparison of spine motion in elite golfers with and without low back pain. Journal of sports sciences, 20(8), 599-605. 8. [CrossRef]
- Kim, S. B., You, J. S. H., Kwon, O. Y., & Yi, C. H. (2015). Lumbopelvic kinematic characteristics of golfers with limited hip rotation. The American journal of sports medicine, 43(1), 113-120. 1. [CrossRef]
- Cole, M. H., & Grimshaw, P. N. (2014). The crunch factor’s role in golf-related low back pain. The Spine Journal, 14(5), 799-807. [CrossRef]
- Glazier, P. S. (2010). Is the ‘crunch factor’an important consideration in the aetiology of lumbar spine pathology in cricket fast bowlers?. Sports medicine, 40(10), 809-815. [CrossRef]
- Bae, T. S., Cho, W., Kim, K. H., & Chae, S. W. (2014). Biomechanical effect of altered lumbar lordosis on intervertebral lumbar joints during the golf swing: A simulation study. Journal of biomechanical engineering, 136(11). [CrossRef]
- Hutton, W. C., Stott, J. R. R., & Cyron, B. M. (1977). Is spondylolysis a fatigue fracture?. Spine, 2(3), 202-209. [CrossRef]
- Cyron, B. M., & Hutton, W. C. (1978). The fatigue strength of the lumbar neural arch in spondylolysis. The Journal of Bone and Joint Surgery. British volume, 60(2), 234-238. 2. [CrossRef]
- Sugaya, H. (1998). Low back injury in elite and professional golfers: an epidemiologic and radiographic study. In Science and GolfIII, Proceedings of the 3rd World Scientific Congress of Golf. Human Kinetics (pp. 83-91).
- Moore, K. L., & Dalley, A. F. (2018). Clinically oriented anatomy. Wolters kluwer india Pvt Ltd.
- Egret, C. I., Vincent, O., Weber, J., Dujardin, F. H., & Chollet, D. (2003). Analysis of 3D kinematics concerning three different clubs in golf swing. International journal of sports medicine, 24(06), 465-470. 06. [CrossRef]
- Edwards, N., Dickin, C., & Wang, H. (2020). Low Back Pain and Golf: A Review of Biomechanical Risk Factors. Sports Medicine and Health Science. [CrossRef]
- Hosea, T. M., Gatt, C. J., & Gertner, E. (1994). Biomechanical analysis of the golfer’s back. In C. N. Stover, J. R. McCarroll & W. J. Mallon (Eds.), Feeling Up to Par: Medicine from Tee to Green. Philadelphia: FA Davis.
- Joyce, C. (2017). An examination of the correlation amongst trunk flexibility, x-factor and clubhead speed in skilled golfers. Journal of Sports Sciences, 35(20), 2035-2041. [CrossRef]
- Tsai, Y. S., Sell, T. C., Smoliga, J. M., Myers, J. B., Learman, K. E., & Lephart, S. M. (2010). A comparison of physical characteristics and swing mechanics between golfers with and without a history of low back pain. journal of orthopaedic & sports physical therapy, 40(7), 430-438. [CrossRef]
Figure 1.
The squat movement examples of high scoring group (1a) and low scoring group (1b).
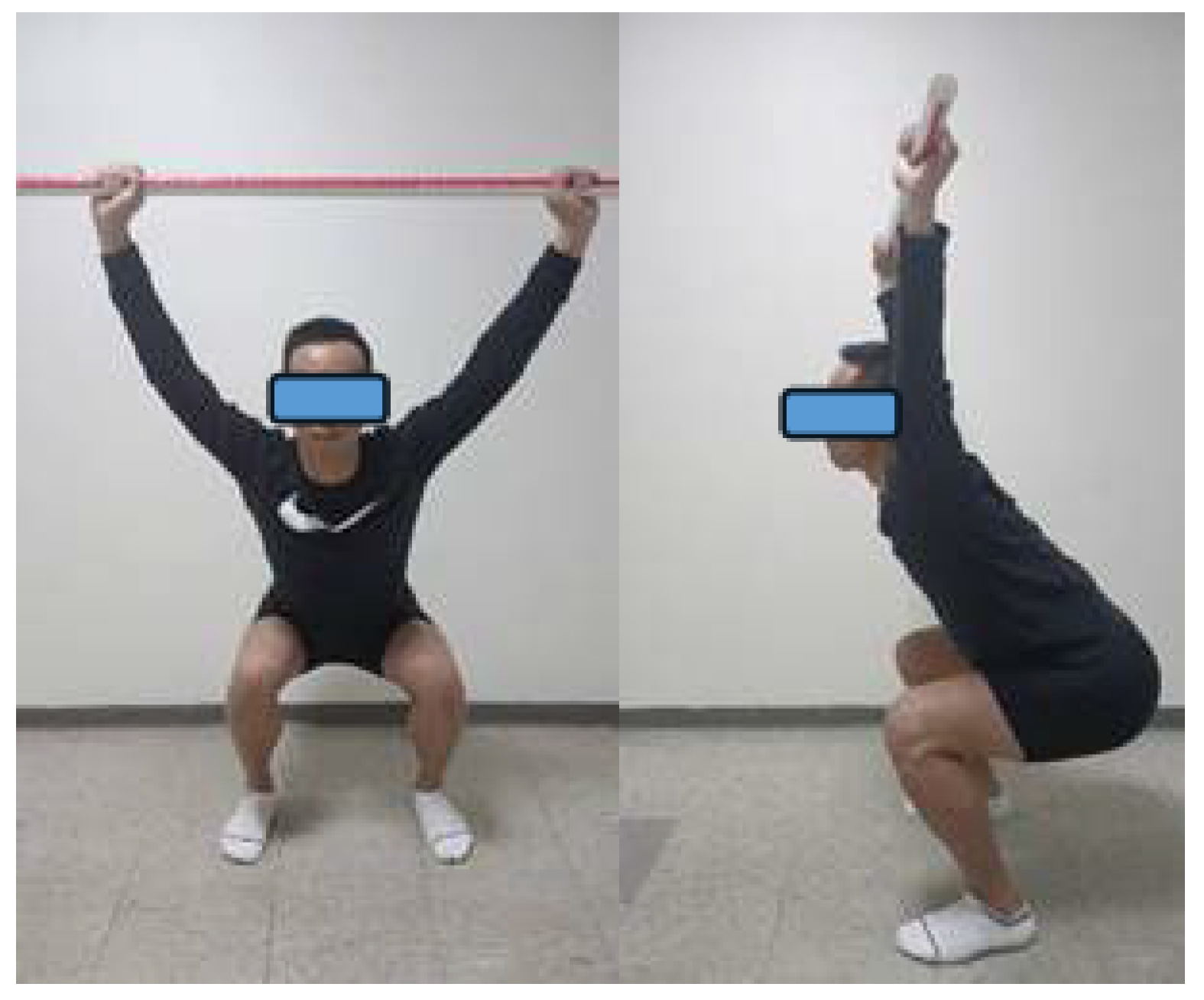
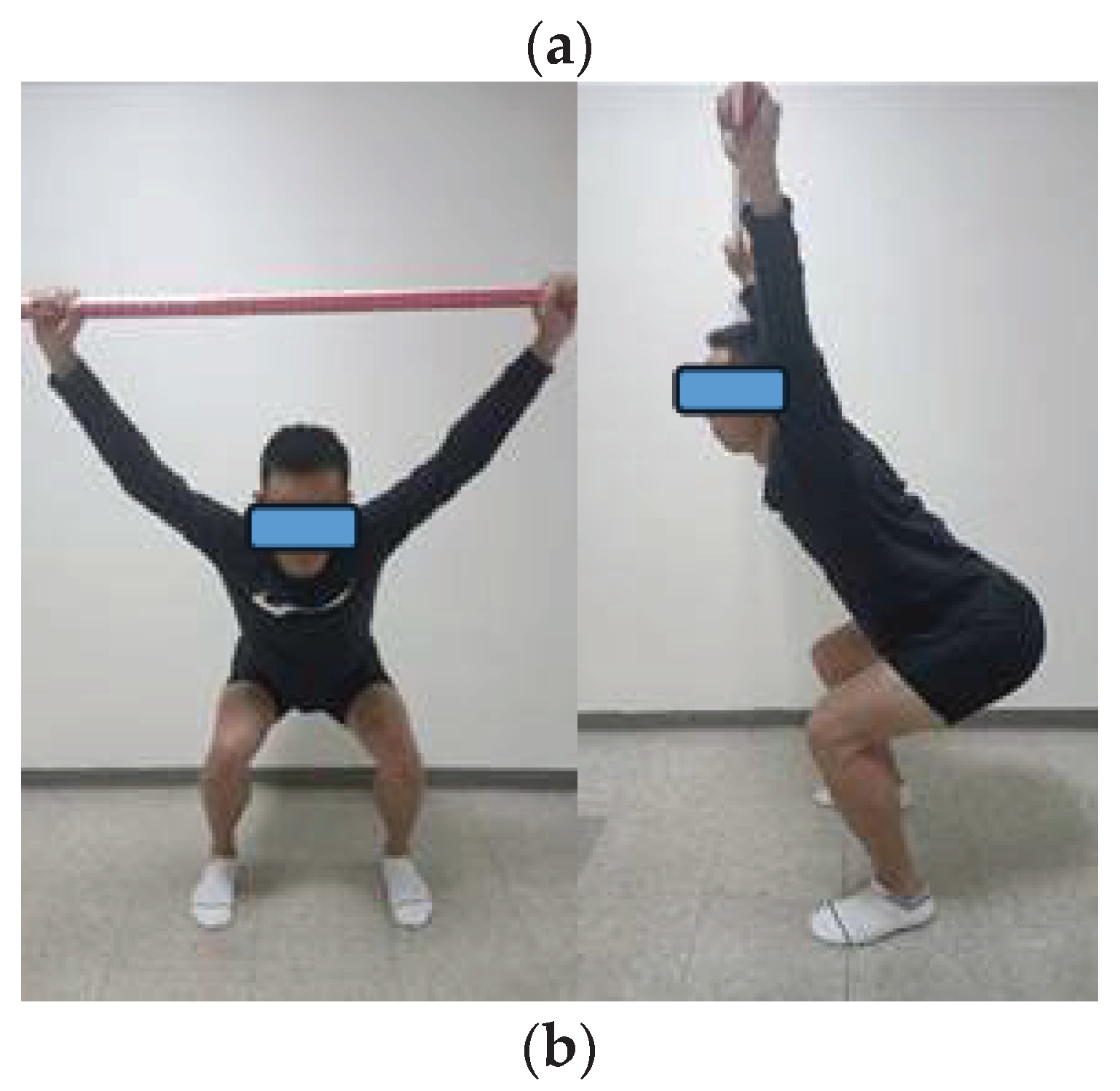
Figure 2.
The full-body lumbar spine (FBLS) model (2a) and the simulation of golf swing (2b).
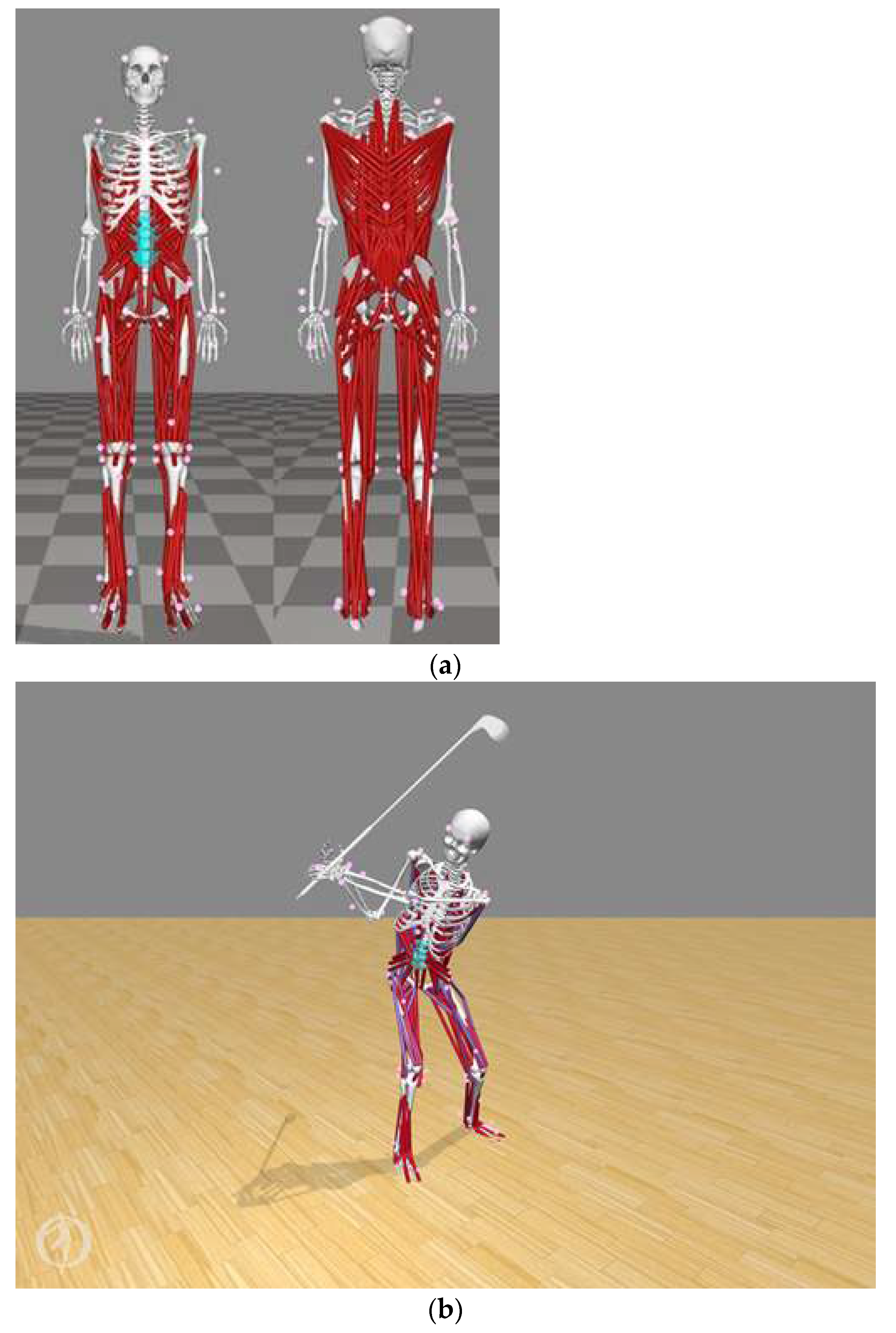
Figure 3.
The model validation on activation level by measured normalized EMG RMS on both sides of lumber area.
Figure 3.
The model validation on activation level by measured normalized EMG RMS on both sides of lumber area.
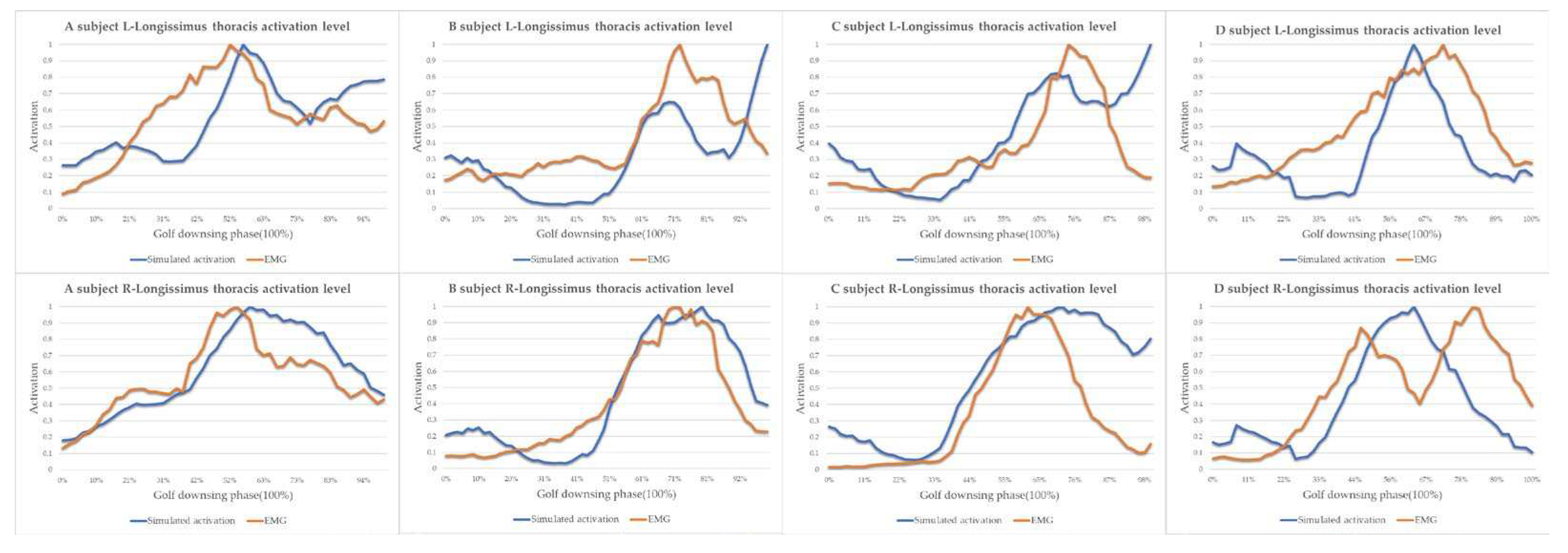

Table 1.
Scoring criteria used for the Overhead Squat (OHS).
| Tests | 3 points | 2 points | 1 point | 0 points |
|---|---|---|---|---|
| Overhead Squat | Upper torso is parallel with tibia or toward vertical. | Meet criteria of 3 points with 2 x 6 board under heels. | Tibia and upper torso are not parallel. | If pain is associated with any portion of this test. |
| Femur is below horizontal. Knees are aligned over feet. Dowel is aligned over feet. |
Knees are not aligned over feet. | Femur is not below horizontal. Knees are not aligned over feet. Lumbar flexion is noted. |
Table 2.
Subject characteristics.
| Mean (SD) | df | t | p | ||
|---|---|---|---|---|---|
| LS-G (N=11) | HS-G (N=10) | ||||
| Downswing time (s) | .29(.06) | .30 (.03) | 19 | -.78 | .452 |
| Height (m) | 1.68 (.10) | 1.61 (.05) | 19 | 2.00 | .061 |
| Weight (kg) | 75.00 (14.37) | 68.06 (13.67) | 19 | 1.13 | .268 |
| Best scores | 68.45 (3.14) | 69.90 (4.07) | 19 | -.92 | .367 |
| Ball speed (mph) | 142.44 (16.95) | 126.29 (11.52) | 19 | 2.53 | .022* |
Note: *p<0.05.
Table 3.
Lumbar kinematics in sagittal plane during golf downswing.
| Mean (SD) | df | t | p | ||
|---|---|---|---|---|---|
| LS-G (N=11) | HS-G (N=10) | ||||
| Lumbar flexion angle at impact (°) | -21.37 (6.39) | -26.20 (5.90) | 19 | 1.792 | .089 |
| Angular Extension/Flexion displacement (°) | 17.72 (5.94) | 24.36 (7.11) | 19 | -2.33 | .031* |
| Peak extension angular velocity (°/s) | 119.52 (59.23) | 40.51 (26.79) | 19 | 3.87 | .000*** |
| Peak flexion angular velocity (°/s) | -269.34 (181.03) | -288.95 (162.68) | 19 | .26 | .798 |
Note: *p<0.05, *** p<0.001; positive values indicate extension and negative values indicate flexion.
Table 4.
Lumbar kinematics in frontal plane during golf downswing.
| Mean (SD) | df | t | p | ||
|---|---|---|---|---|---|
| LS-G (N=11) | HS-G (N=10) | ||||
| Lumbar right side bending angle at impact (°) 1 | 21.07 (.48) | 20.93 (.70) | 19 | .55 | .591 |
| Angular RB/LB displacement (°) 1 | 34.89 (5.95) | 31.21 (7.28) | 19 | -1.27 | .218 |
| Peak right side bending angular velocity (°/s) 1 | 329.35 (43.79) | 287.42 (62.27) | 19 | 1.80 | .088 |
Note:1 Positive values indicate right side bending.
Table 5.
Lumbar joint peak shear force (N) during golf downswing.
| Mean (SD) | df | t | p | ||
|---|---|---|---|---|---|
| LS-G (N=11) | HS-G (N=10) | ||||
| L1-L2 | 712.67 (74.46) | 737.97 (133.89) | 19 | -.54 | .594 |
| L2-L3 | 487.45 (70.43) | 530.31 (104.34) | 19 | -1.11 | .280 |
| L3-L4 | 327.81 (75.54) | 337.94 (56.10) | 19 | -.35 | .733 |
| L4-L5 | 387.19 (89.16) | 299.54 (37.30) | 19 | 2.88 | .010** |
| L5-S1 | 525.19 (86.69) | 407.90 (59.06) | 19 | 3.59 | .002** |
Note: **p<0.01.
Table 6.
Lumbar joint peak compressive force (N) during golf downswing.
| Mean (SD) | df | t | p | ||
|---|---|---|---|---|---|
| LS-G (N=11) | HS-G (N=10) | ||||
| L1-L2 | 3018.92 (233.43) | 3059.77 (356.55) | 19 | -.31 | .757 |
| L2-L3 | 3412.79 (289.78) | 3515.89 (424.28) | 19 | -.66 | .520 |
| L3-L4 | 3668.80 (326.21) | 3797.82 (443.92) | 19 | -.76 | .454 |
| L4-L5 | 3770.94 (338.66) | 3921.69 (450.25) | 19 | -.87 | .394 |
| L5-S1 | 3759.18 (328.70) | 3918.67 (447.88) | 19 | -.94 | .361 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



