
Submitted:
12 January 2024
Posted:
12 January 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
In 2020, following the World Health Organization's declaration of COVID-19 as a pandemic, dental practices faced unprecedented disruptions globally. This retrospective cross-sectional study, conducted at a leading university dental hospital in the Lisbon Metropolitan Area, investigated the impact of these disruptions on dental caries. The study, spanning June 2019 to June 2021, included a full-mouth X-ray examination, along with sociodemographic, behavioral, and medical data. Our sample comprised 3,380 participants (2,007 females and 1,373 males), aged 18 to 99 years, divided into pre-lockdown and post-lockdown groups. We employed the Decayed, Missing, and Filled Teeth (DMFT) index to measure dental caries. Our findings revealed that nearly 90% of participants in both groups experienced dental caries, indicating a statistically significant difference between the pre-lockdown and post-lockdown periods. However, the impact of COVID-19 confinement varied among different demographic sectors, with age, educational background, and professional status emerging as the key determinants. This study highlights the need for a more nuanced understanding of the impact of the pandemic on oral health, emphasizing the role of sociodemographic factors in shaping dental health outcomes during such global health crises.
Keywords:
dental caries
; caries experience
; COVID-19
; prevalence
; pandemic
; epidemiology
; decay missing filled index
; dmf index
1. Introduction
In 2020, the World Health Organization (WHO) declared the COVID-19 outbreak a pandemic [1]. Uncertainty about its spread [2] leads health authorities worldwide to suspend certain clinical practices, including dentistry [3,4]. Owing to these circumstances, the clinical care of patients has undergone remarkable changes, with an unknown impact on oral hygiene and oral health complications [5,6].
Another aspect to consider is how forced lockdowns negatively affected health determinants. Such negative effects of social distancing and decreased support that occurred during lockdowns have been demonstrated in students' mental health [7], stress and poor health in pregnancy [8], weight control [9], and even engaging in positive physical activities that ultimately may trigger undesirable behaviors [10].
One of the expected oral health complications is an increase in dental caries [1]. Dental caries remain one of the most prevalent oral diseases worldwide and are a public health challenge in the 21st century [2,3]. Dental caries contributes to the reduction of quality of life due to significant pain and discomfort [4] and is a marker of social disadvantages and health inequalities [1,5].
However, despite this background, the impact of the COVID-19 pandemic on dental caries prevalence has been very little explored. We retrospectively analyzed a sample of first-incoming patients at a reference Portuguese university dental hospital to understand the effect of the COVID-19 pandemic on dental caries prevalence. Ultimately, we aimed to measure the prevalence of caries before and after the COVID-19 pandemic in the study population.
2. Materials and Methods
The study was conducted following the guidelines for strengthening the reporting of observational studies in epidemiology (STROBE) [11], in accordance with the Declaration of Helsinki of 1975, as revised in 2013, and was approved by the Egas Moniz Ethics Committee (ID number 898). The first appointment included gathering written informed consent from each participant.
2.1. Study Setting and Participants
This study was a retrospective, cross-sectional secondary analysis focusing on new patients at the Egas Moniz Dental Clinic, Almada, Portugal, from June 2019 to June 2021. A detailed database of incoming patients was used for the original data collection. New patients underwent an initial assessment, including a self-reported health questionnaire, comprehensive oral examination, and radiographic evaluation with panoramic radiographs and bitewings. The questionnaire gathered key demographic details, such as age, sex, education, employment, medical history, medication, smoking habits, and dental hygiene. Each patient underwent a customized evaluation and treatment plan. Dental students conducted initial observations with clinical assistants confirming diagnoses and ensuring accurate oral health assessments.
The inclusion criteria required patients to be over 18 years of age and to provide written consent. Exclusion criteria included being edentulous, having incomplete data, or having special needs as they received care in a specialized department.
Data were divided into two groups: Group 1 – pre-lockdown (June 2019 to early March 2020) and Group 2–post-lockdown (May 2020 to June 2021).
2.2. Dependente variables
The principal variable reliant on the DMF index is the cumulative incidence of caries. The most frequently employed dental decay indicator is the same DMF index, which quantifies an individual's total experience with existing and previous instances of dental decay via their accumulated count of Decayed, Missing due to Decay or Filled Teeth (DMFT). This metric reflects a person's holistic history with untreated caries, indicated by the number of decaying teeth, as well as those that have been addressed through fillings or lost owing to extraction consequent to cavities [6,7].
2.3. Independent variables
We gathered data on sociodemographic characteristics and conducted a self-completed questionnaire prior to any clinical assessment. This methodology aims to mitigate the potential response prejudice.
In terms of independent variables, our study incorporated elements that depicted health determinants and socio-demographic characteristics, such as age, gender, educational attainment level, and professional status. Sex was divided into two sections: male and female. Age data were continuously calculated in years before categorization into the following groups: 18-24; 25-44; 45-64; ≥65. The classification of education levels was aligned with the guidelines set by the International Standard Classification of Education (ISCED) in their updated 2011 edition. Lastly, we classified occupational statuses under categories such as studentship or academic pursuits, actively employed personnel or workers currently out-of-job/unemployed persons, along-side pension collectors/retired individuals also included within these research parameters.
We evaluated oral hygiene practices based on the frequency of tooth brushing (2-3 times daily, once per day, 2-6 times weekly, or never), selection of a manual versus electric toothbrush, utilization of dental floss, and mouthwash..
2.4. Statistical Analysis
Data analysis was performed using the IBM SPSS Statistics version 28.0 for Windows (IBM Corp., Armonk, NY, USA). We applied descriptive and inferential statistical methods. The Kolmogorov–Smirnov and Levene tests assessed the homogeneity of variance. The Kruskal–Wallis test, accompanied by Bonferroni correction, was used for normally distributed data with rejected homogeneity of variance, or for non-normally distributed data. The Student’s t-test was used for normally distributed data with accepted homogeneity of variance, whereas the Welch test was applied when homogeneity of variance was rejected. For non-normally distributed data, the Mann–Whitney U test was used.
3. Results
3.1. Participants inclusion and characteristics
From a total of 3,469 incoming patients, 3,380 (97.4%) fulfilled the eligibility criteria, while 89 participants were excluded From the study. Among the excluded individuals, 44 (1.3%) were younger than 18 years and 45 (1.3%) were edentulous (Figure 1).
Table 1 presents a comprehensive sociodemographic, health, and behavioral characterization of 3,380 participants, divided into two periods: pre-lockdown (2,278 participants) and post-lockdown (1,102 participants). The majority of the participants were female, constituting 59.4% overall, with a slight decrease from 60.1% pre-lockdown to 56.8% post-lockdown. Overall, male participants accounted for 40.6%, with an increase from 39.9% pre-lockdown to 43.2% post-lockdown. The average age of the participants was 43.21 years, with a minor decrease from the 43.36 years pre-lockdown to 42.90 years post-lockdown. The age distribution was 21.3% in the 18-24 years category, 32.4% in the 25-44 years category, 32.2% in the 45-64 years category, and 14.2% in the ≥ 65 years category. Regarding education, 22.4% had no studies, 37.4% had completed elementary education, 26.9% had middle-level education, and 3.3% had higher education, with a notable increase in the latter from 0.7% before the lockdown to 8.7% after the lockdown. Regarding occupation, 17.6% were students, 56.1% were employed, 10.4% were unemployed, and 15.9% were retired. In terms of Body Mass Index (BMI), 3.6% fell below 18.5, 46.1% were within the 18.5-24.9 range, 34.1% in the 25.0-29.9 range, and 16.2% were 30.0 or above. Lastly, 79.2% of the participants were non-smokers, although the percentage of active smokers increased from 18.0% pre-lockdown to 26.6% post-lockdown.
Table 2 provides detailed insights into oral healthcare practices and self-reported perceptions of oral health conditions. The use of manual toothbrushes was dominant at 88.6%, and remained steady across both periods. Electric toothbrush usage was minor (10.9%), showing a slight increase from pre-lockdown to post-lockdown.
There was a notable shift in toothbrushing frequency: 75.6% brush 2-3 times daily, declining from 81.2% pre-lockdown to 64.2% post-lockdown. Daily brushing was reported by 15.0%, while those brushing 2-6 times weekly increased significantly from 1.9% to 18.5% post-lockdown. A small fraction (2.1%) never brushed their teeth, increasing marginally from 1.5% pre-lockdown.
Dental floss usage declined from 38.0% pre-lockdown to 26.3% post-lockdown, representing an overall decline of 34.2%. Participants' perceptions of their teeth health were mostly stable across both periods, categorized as excellent (2.5%), very good (9.6%), good (43.3%), weak (29.3%), or very weak (15.2%). Similarly, gum health perceptions showed minor variations, with 4.0% rating it as excellent, 13.0% as very good, 52.2% as good, 24.2% as weak, and 6.5% as very weak. Gum bleeding was reported by 38.5% of participants, with a negligible difference between the two periods.
Table 3 illustrates a comparative review of indicators related to oral health pre- and post-lockdown, focusing on decayed (DT), missing (MT), and filled teeth (FT). In addition, the overall Decayed, Missing and Filled Teeth index measurements were also de-tailed. An interesting observation from the data is the reduction in the DMFT index across different demographics after the lockdown. For instance, females showed a decrease in their DMFT index from 12.38 to 11.01, whereas males saw a reduction from 11.74 to 10.96. This trend may suggest an improvement in oral health or a shift in dental care practices during the lockdown. Age-wise, the youngest group (18-24 years) experienced a slight increase in their DMFT score from 8.25 to 9.76 post-lockdown, hinting at the potentially negative impacts of lockdown on their oral health habits. In contrast, the DMFT scores in the other age groups decreased.
Educational background also plays a significant role. Individuals without formal education showed a noticeable reduction in their DMFT score from 14.34 to 11.48, while those with higher education showed a substantial decrease from 15.00 to 6.82. This finding highlights the influence of education on oral health maintenance. In terms of occupation, students and retired individuals experienced an increase in DMFT scores post-lockdown, whereas employed and unemployed groups saw a decrease.
Tooth brushing frequency correlated with DMFT scores, with brushing 2–6 times weekly, showing a significant decrease in their DMFT score post-lockdown. Furthermore, variations in dental caries experiences were observed across different BMI categories, suggesting a complex relationship between general health and oral hygiene. The data underscore the multifaceted nature of dental health, which is influenced by a blend of demographic characteristics and personal behaviors. The overall trend indicated an improvement in oral hygiene post-lockdown for most groups, although this improvement varied significantly across different demographics and lifestyles.
As shown in Table 4 and Figure 2, there was a significant shift in the prevalence of dental caries following the lockdown period among the 3,380 participants. The percentage of individuals with dental caries (DCP) showed a notable decrease, moving from 91.8% pre-lockdown to 84.5% post-lockdown. This decline signified a marked reduction in the proportion of samples affected by dental caries.
When examining the mean counts for various dental health indicators — Decayed Teeth (DT), Missing Teeth (MT), Filled Teeth (FT), and the overall Decayed, Missing, and Filled Teeth (DMFT) index — several interesting trends emerged. The average count of decayed teeth (DT) decreased from 6.09 pre-lockdown to 5.40 post-lockdown, indicating a reduction in the prevalence of this condition. However, the number of missing teeth (MT) increased slightly increase from 4.47 5.10. Additionally, there was a noticeable decrease in the mean count of filled teeth (FT), from 3.56 pre-lockdown to 3.06 post-lockdown. Correspondingly, the overall DMFT index, which combines these three measures, also showed a decrease, moving from 12.13 pre-lockdown to 10.99 post-lockdown.
4. Discussion
This investigation retrospectively examined the incidence of dental caries in a Portuguese adult group, integrating both clinical evaluations and radiographic investigations during the phases before and after the COVID-19-induced lockdown. The objective of this study was to evaluate how Portugal's oral health was impacted by this lockdown due to COVID-19, contrasting several oral wellness parameters between the two sets - those evaluated pre-lockdown versus post-lockdown–across varied demographic and behavioral factors. These specified parameters range from decayed teeth (DT), missing teeth (MT), filled teeth (FT), and their amalgamated index known as Decayed, Missing, Filled Teeth Index(DMFT).
Notably, 89.4% of participants experienced some degree of exposure to caries. This high percentage of participants with at least one dental carie aligns with findings from previous studies [6,8].
Despite the high prevalence of dental caries in this population, the results indicated a decrease in the average number of dental caries and filled teeth post-lockdown, along with an increase in the average number of missing teeth. These results could be attributed to the reduced access to and utilization of dental-care services during the lockdown. During the pandemic, dental settings encountered significant restrictions owing to their potential role in facilitating COVID-19 transmission, largely because of the nature of dental care procedures. Consequently, many countries have directed dental professionals to limit their services to urgent and emergency care, postponing elective treatments and implementing protocols to minimize transmission risks [9,10]. Routine dental checkups and treatments may have been deferred or canceled, leading to a decrease in the number of filled teeth (FT). However, this could also account for the slight increase in missing teeth (MT), as urgent dental issues might have necessitated extractions rather than restorative treatments [11,12,13]. Moreover, societal apprehension towards contracting COVID-19 has led to a significant decline in the need for dental services, even during emergencies [14,15,16]. The delay or evasion of regular diagnostic procedures and preventative measures is likely to contribute to the global increase in oral diseases [17]. This underlines the significance of sustaining self-care at home concerning oral hygiene when access to professional dentists is limited owing to such circumstances [18].
Another aspect potentially contributing to these results could be changes in oral hygiene practices during the lockdown. Altered daily routines may have affected the oral care habits. It is plausible that people have more time to focus on oral health, potentially leading to improved hygiene practices. This improvement could contribute to the observed reduction in the decayed teeth (DT) count and overall DMFT index. While some studies indicated an increase in the frequency of home oral hygiene maintenance [19], others reported a decrease [20] or no significant change. Our results suggest an increase in the number of individuals who neglect regular tooth brushing and dental floss usage.
Additionally, other studies have noted an increase in dental caries following the lockdown. This increase could be associated with increased consumption of sugary and carbonated drinks during the pandemic, coupled with a decrease in the frequency and quality of oral hygiene [12,21].
Another possible reason for these findings could be related to the social distancing measures implemented during lockdown. Such measures might have reduced the transmission of bacteria, including cariogenic (cavity-causing) bacteria, thereby indirectly affecting the prevalence of dental caries [22].
Considering the demographic and behavioral factors, starting with sex, a reduction in the Decayed Missing Filled Teeth (DMFT) index was noticeable for both sexes following lockdown. Notably, there was an enhanced decline in tooth decay among women compared to men. However, it is important to note that previous research has identified sex-based differences in caries experiences [23]. Various factors, including societal norms, nutritional practices, dietary patterns, and hormonal variations, are known to contribute to sex-specific differences in the occurrence of carious lesions [24,25].
The data demonstrate a consistent increase in DMFT (Decayed, Missing, and Filled Teeth) scores with advancing age across both groups. Notably, the highest DMFT scores were recorded in individuals aged 65 and older in the pre-lockdown period, with scores of 15.39 and in individuals aged 45-64 in the post-lockdown period, with scores of 11.30. This trend highlights the greater prevalence of dental issues in the older population. The age group of 18-24 years showed a significant increase in DMFT scores during the lockdown, jumping from 8.25 to 9.76, indicating that this demographic was particularly affected. Consistent with existing research [6,24,26], our findings reaffirm that age is a key risk factor for dental health issues. Furthermore, this correlation might be influenced by various age-related factors such as dry mouth (xerostomia), use of multiple medications (polypharmacy), functional and cognitive decline, and changes in the oral ecosystem over time [27].
All occupational groups showed a decrease in the DMFT index, with the most significant decrease observed among the students. These variations suggest that the impact of lockdown on dental health may differ according to lifestyle changes associated with occupation. It is well established in the literature [28,29,30] that occupational environments significantly influence oral health.
Regarding the influence of education, people with higher educational levels (higher education) showed a significant decrease in the DMFT index post-lockdown, especially in the filled teeth (FT) category. Individuals with higher educational achievements often exhibit superior oral health. Research indicates that those with higher education generally possess greater awareness of oral health and adhere more effectively to oral hygiene routines. Conversely, those with less educational background are more inclined to neglect regular dental visits and care and frequently resort to emergency and treatment services rather than routine dental check-ups. Consequently, a positive correlation exists between higher educational levels and improved oral health outcomes [31,32,33].
In examining the impact of lockdown on dental health in relation to tooth brushing frequency, our results revealed changes. There was a 17% decrease in the number of individuals who brushed their teeth 1-3 times daily from the prelockdown to the postlockdown period. Simultaneously, there was a 16.6% increase in the frequency of individuals brushing their teeth 1-6 times weekly over the same period. These results are consistent with the conclusion of a study aimed at evaluating the impact on oral health-related behaviors and practices of Portuguese and Spanish children during the COVID-19 lockdown [21].
Our research also identified a significant correlation between elevated Body Mass Index (BMI) and increased Decayed, Missing, and Filled Teeth (DMFT) scores, suggesting a potential interplay between dietary habits, overall health, and oral hygiene. We found that a higher BMI, a metric indicating body fat based on height and weight, was closely linked to the prevalence of dental caries. This trend is particularly noticeable among individuals classified as overweight or obese, who generally show higher levels of tooth decay, a finding that aligns with other studies [34,35,36]. The increased rate of tooth decay in these groups may be related to the consumption of diets high in sugary drinks and food [37]. Although our study points to a correlation between higher BMI and dental cavities, the complex relationship between obesity and oral health, including tooth decay, warrants further investigation. Notably, some studies have reported a contradictory association between lower instances of dental cavities and obesity [38,39], adding to the complexity of these interrelationships. This ambiguity is further supported by previous research conducted in Portugal that observed similar trends [6].
Individuals' perceptions of their teeth health seem to correlate with their DMFT scores. Those with a perception of "weak" or "very weak" tooth health had higher DMFT scores, which increased post-lockdown. This may be related to the limited access to dental care [18].
Strenghts and Limitations
When assessing our research, it is important to consider both its merits and limitations. One significant limitation is the observational design of the study, which hinders our ability to determine causal relationships. However, it is particularly notable that this study involved a large number of participants. Furthermore, the fact that data gathering was predominantly undertaken by students poses a limitation, although this was somewhat counterbalanced by having all diagnoses validated by the credentialed teachers. In addition, changes in dental procedures owing to the COVID-19 pandemic's disruption of dental clinic functions have added another layer of restriction to the study. A noteworthy limitation is the lack of control over potential influencing factors such as fluoride exposure levels, salivary flow rate, or socioeconomic status, especially considering many patients' hesitation about revealing their economic conditions.
There are certain constraints associated with the Decayed, Missing, and Filled Teeth (DMFT) index that we utilized in our investigation. [40]. This measure combines decayed, missing, or filled teeth, but fails to distinguish between different causes of tooth loss other than dental caries, nor does it address the demand for oral healthcare intervention. However, proportions such as those representing decayed teeth out of total DMF count (D/DMF) and filled teeth counted against all accounted within the DMF set (F/DMF) offer a glimpse into unresolved treatment concerns and access to oral health services, respectively. The merit of our study lies in its radiographic verification of dental caries, which bolsters the credibility of our conclusions drawn from the results obtained during this research . Despite these caveats inherent within the analysis framework adopted by us, adherence has been ensured on part of globally acknowledged guiding principles [41,42,43], thereby reinforcing its significance and reliability across an extensive scholarly domain.
5. Conclusions
Our research indicates that COVID-19 confinement has differentially impacted dental health across demographic sectors, with age, education, and professional status being the key determinants. This study emphasizes the need for more detailed approaches to understand and address disparities in oral health.
Author Contributions
Conceptualization, E.G., V.M., and J.B.; Methodology, E.G. and J.B.; Software, E.G.; Validation, E.G., V.M., J.B., A.C.M and J.J.M; Formal analysis, E.G. and L.P.; Investigation, E.G.; Resources, E.G.; Data curation, E.G.; Writing—original draft preparation, E.G., V.M., and J.B.; Writing— Review and Editing, E.G.; Visualization, E.G.; Supervision, E.G, A.C.M and J.J.M.; Project administration, E.G.; Funding acquisition, V.M. and J.B. All authors have read and agreed to the published version of the manuscript.
Funding
This study received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (or Ethics Committee) of Egas Moniz (ID no. 898 on September 24, 2020).
Informed Consent Statement
Informed consent was obtained from all the subjects involved in the study.
Data Availability Statement
The entirety of the data compiled and examined throughout this study can be found within this document. Any additional queries should be directed towards the author in charge of correspondence.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Matsuyama, Y., A. Isumi, S. Doi, and T. Fujiwara, Impacts of the COVID-19 Pandemic Exposure on Child Dental Caries: Difference-in-Differences Analysis. Caries Research, 2023. 56(5-6): p. 546-554.
- Jain, N., U. Dutt, I. Radenkov, and S. Jain, WHO's global oral health status report 2022: Actions, discussion and implementation. Oral Dis, 2023.
- WHO, Global oral health status report: towards universal health coverage for oral health by 2030. 2022, World Health Organization.
- Selwitz, R.H., A.I. Ismail, and N.B. Pitts, Dental caries. Lancet, 2007. 369(9555): p. 51-9.
- Watt, R.G., et al., Ending the neglect of global oral health: time for radical action. Lancet, 2019. 394(10194): p. 261-272.
- Guerreiro, E., et al., Caries Experience and Risk Indicators in a Portuguese Population: A Cross-Sectional Study. Int J Environ Res Public Health, 2023. 20(3).
- Peres, M.A., et al., Oral diseases: a global public health challenge. Lancet, 2019. 394(10194): p. 249-260.
- Guerreiro, E., A.C. Manso, and J.J. Mendes, Employability and Dental Caries Experience. Medical Sciences Forum, 2023. 22(1): p. 44.
- Bekes, K., V. Ritschl, and T. Stamm, COVID-19 Pandemic and Its Impact on Pediatric Dentistry in Austria: Knowledge, Perception and Attitude Among Pediatric Dentists in a Cross-Sectional Survey. J Multidiscip Healthc, 2021. 14: p. 161-169.
- Cagetti, M.G. and E. Angelino, Could SARS-CoV-2 burst the use of Non-Invasive and Minimally Invasive treatments in paediatric dentistry? International Journal of Paediatric Dentistry, 2021. 31(1): p. 27-30.
- Abdelrahman, H., et al., Dental practice closure during the first wave of COVID-19 and associated professional, practice and structural determinants: a multi-country survey. BMC Oral Health, 2021. 21(1): p. 243.
- Gotler, M., et al., The impact of COVID-19 lockdown on maintenance of children's dental health: A questionnaire-based survey. The Journal of the American Dental Association, 2022. 153(5): p. 440-449.
- Iwasaki, M., et al., Interruption of regular dental visits during the COVID-19 pandemic due to concerns regarding dental visits was associated with periodontitis in Japanese office workers. J Periodontal Res, 2021. 56(6): p. 1091-1098.
- Fux-Noy, A., et al., Oral Health Care Delivery for Children During COVID-19 Pandemic—A Retrospective Study. Frontiers in Public Health, 2021. 9.
- Campagnaro, R., et al., COVID-19 pandemic and pediatric dentistry: Fear, eating habits and parent’s oral health perceptions. Children and Youth Services Review, 2020. 118: p. 105469.
- Sen Tunc, E., E. Aksoy, H.N. Arslan, and Z. Kaya, Evaluation of parents' knowledge, attitudes, and practices regarding self-medication for their children’s dental problems during the COVID-19 pandemic: a cross-sectional survey. BMC Oral Health, 2021. 21(1): p. 98.
- Hopcraft, M. and G. Farmer, Impact of COVID-19 on the provision of paediatric dental care: Analysis of the Australian Child Dental Benefits Schedule. Community Dentistry and Oral Epidemiology, 2021. 49(4): p. 369-376.
- Blumer, S., et al., Function of the Family Unit, Oral Hygiene Rules and Attitudes to Dental Health in Children During First-Wave 2020 COVID-19 Lockdown. Journal of Clinical Pediatric Dentistry, 2021. 45(1): p. 1-7.
- Keleş, Z.H. and H. Şar Sancaklı, Evaluation of Knowledge, Attitude and Behaviour on Oral Health Through COVID-19 Pandemic. Meandros Medical and Dental Journal, 2020. 21(3): p. 222-231.
- Brondani, B., et al., Effect of the COVID-19 pandemic on behavioural and psychosocial factors related to oral health in adolescents: A cohort study. Int J Paediatr Dent, 2021. 31(4): p. 539-546.
- Costa, A.L., J.L. Pereira, L. Franco, and F. Guinot, COVID-19 Lockdown: Impact on Oral Health-Related Behaviors and Practices of Portuguese and Spanish Children. International Journal of Environmental Research and Public Health, 2022. 19(23): p. 16004.
- Domingues, C.P.F., et al., The Social Distancing Imposed To Contain COVID-19 Can Affect Our Microbiome: a Double-Edged Sword in Human Health. mSphere, 2020. 5(5): p. 10.1128/msphere.00716-20.
- Bogale, B., et al., Dental caries experience and associated factors in adults: a cross-sectional community survey within Ethiopia. BMC Public Health, 2021. 21(1): p. 180.
- Nicklisch, N., et al., A Healthier Smile in the Past? Dental Caries and Diet in Early Neolithic Farming Communities from Central Germany. Nutrients, 2022. 14(9): p. 1831.
- Qureshi, A., et al., Dietary Factors Influencing the Caries Status of Adults in Karachi, Pakistan: Initial Findings. International Journal of Environmental Research and Public Health, 2022. 19(12): p. 6980.
- Chan, A.K.Y., et al., A Systematic Review on Caries Status of Older Adults. Int J Environ Res Public Health, 2021. 18(20).
- Gavriilidou, N.N. and G.N. Belibasakis, Root caries: the intersection between periodontal disease and dental caries in the course of ageing. British Dental Journal, 2019. 227(12): p. 1063-1067.
- Abdel Fattah, M.A., et al., Epidemiology of dental caries in permanent dentition: evidence from a population-based survey in Egypt. BMC Public Health, 2022. 22(1): p. 2438.
- Costa, S.M., et al., Socioeconomic Factors and Caries in People between 19 and 60 Years of Age: An Update of a Systematic Review and Meta-Analysis of Observational Studies. Int J Environ Res Public Health, 2018. 15(8).
- de Araujo Nobre, M.A., A.M. Sezinando, I.C. Fernandes, and A.C. Araujo, Influence of Smoking Habits on the Prevalence of Dental Caries: A Register-Based Cohort Study. Eur J Dent, 2021. 15(4): p. 714-719.
- Serrano-Sánchez, S., et al., Relationship between Oral Health Knowledge and Maternal Oral Health with Obstetric Risk and Breastfeeding. International Journal of Environmental Research and Public Health, 2022. 19(13): p. 7797.
- Chen, L., et al., Are parents’ education levels associated with either their oral health knowledge or their children’s oral health behaviors? A survey of 8446 families in Wuhan. BMC Oral Health, 2020. 20(1): p. 203.
- Ghanbarzadegan, A., M. Mittinty, D.S. Brennan, and L.M. Jamieson, The effect of education on dental service utilization patterns in different sectors: A multiple mediation analysis. Community Dentistry and Oral Epidemiology, 2023. 51(6): p. 1093-1099.
- Chen, D., et al., Association between Dental Caries and BMI in Children: A Systematic Review and Meta-Analysis. Caries Research, 2018. 52(3): p. 230-245.
- Alshehri, Y.F.A., J.S. Park, E. Kruger, and M. Tennant, Association between body mass index and dental caries in the Kingdom of Saudi Arabia: Systematic review. Saudi Dent J, 2020. 32(4): p. 171-180.
- Paisi, M., et al., Body mass index and dental caries in young people: a systematic review. BMC Pediatr, 2019. 19(1): p. 122.
- Alam, B.F., et al., Relationship of BMI with the diet, physical activity and oral hygiene practices amongst the dental students. BMC Oral Health, 2022. 22(1): p. 311.
- Cheng, Y.H., et al., Prevalence of dental caries and its association with body mass index among school-age children in Shenzhen, China. BMC Oral Health, 2019. 19(1): p. 270.
- Stangvaltaite-Mouhat, L., A.S. Furberg, S.N. Drachev, and T.A. Trovik, Common social determinants for overweight and obesity, and dental caries among adolescents in Northern Norway: a cross-sectional study from the Tromso Study Fit Futures cohort. BMC Oral Health, 2021. 21(1): p. 53.
- Shulman, J.D. and D.P. Cappelli, Chapter 1 - Epidemiology of Dental Caries, in Prevention in Clinical Oral Health Care, D.P. Cappelli and C.C. Mobley, Editors. 2008, Mosby: Saint Louis. p. 2-13.
- Cuschieri, S., The STROBE guidelines. Saudi J Anaesth, 2019. 13(Suppl 1): p. S31-S34.
- Vandenbroucke, J.P., et al., Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Epidemiology, 2007. 18(6): p. 805-35.
- 43. von Elm, E., et al., The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg, 2014. 12(12): p. 1495-9.
Disclaimer/Publisher’s Note: The statements, opinions, and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of the MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions, or products referred to in the content. |
Figure 1.
Participants inclusion flowchart.
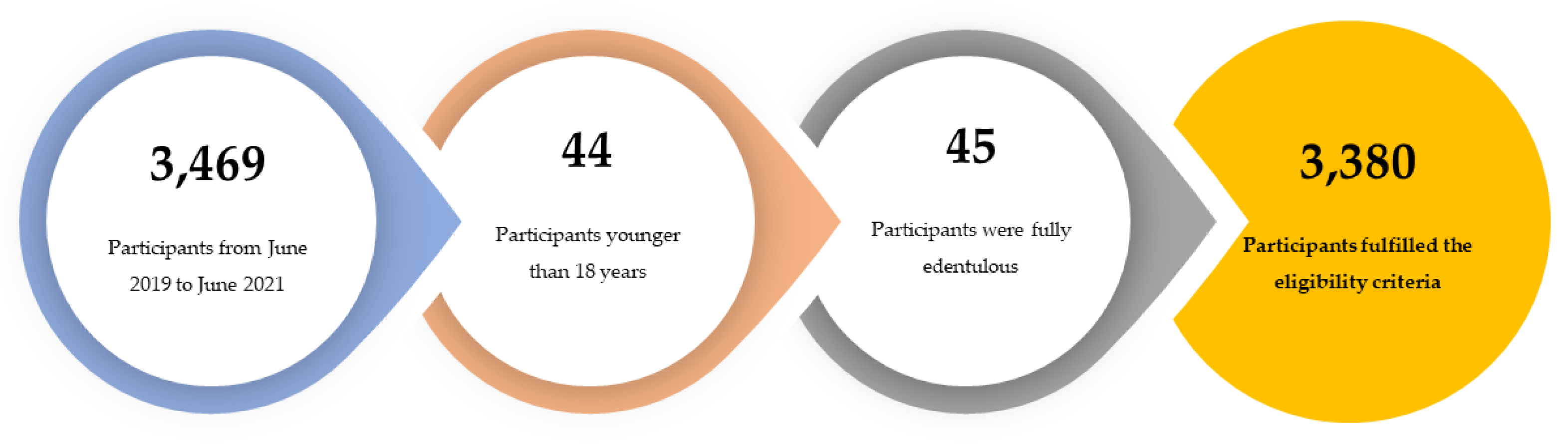
Figure 2.
Comparison of dental caries experience between pre-lockdown and post-lockdown periods.
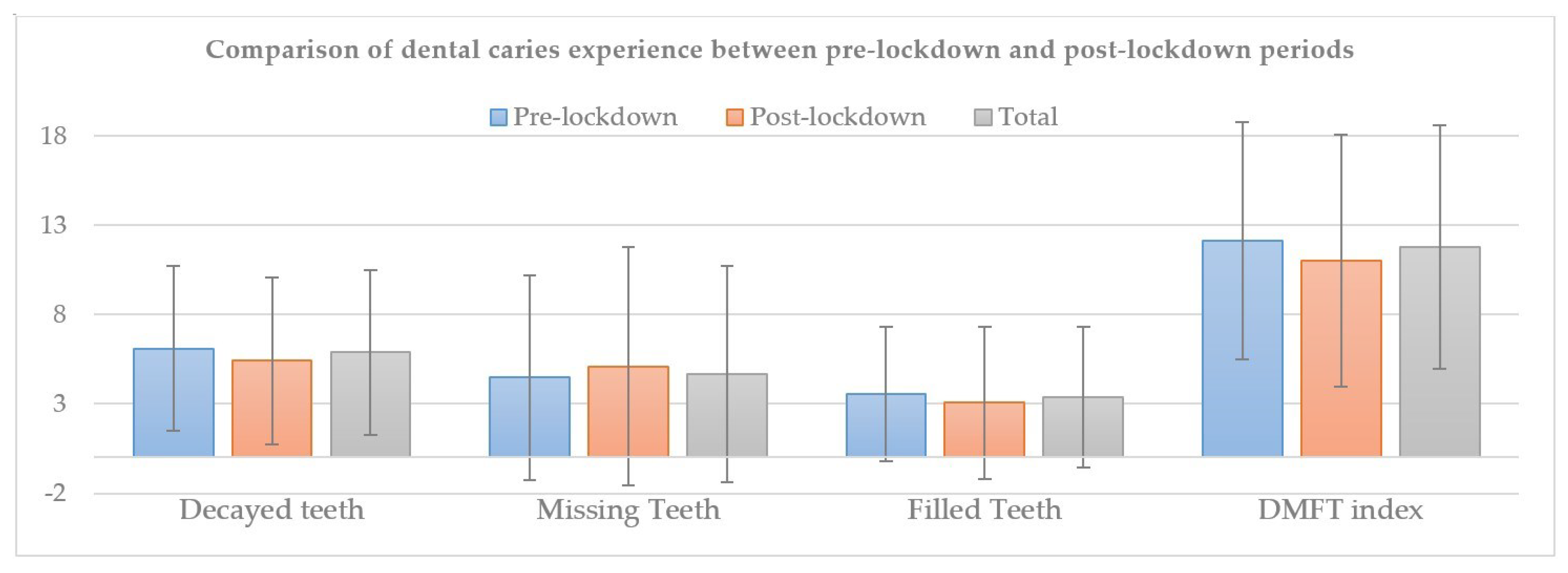

Table 1.
Sociodemographic, health, and behavior characterization of the participants (n = 3,380).
| Variable | Total (n = 3,380) | Pre-lockdown (n =2,278 ) | Post-lockdown (n=1,102) |
|---|---|---|---|
| Sex, % (n) | |||
| Female | 59.4 (2,007) | 60.1 (1,369) | 56.8 (476) |
| Male | 40.6 (1,373) | 39.9 (909) | 43.2 (362) |
| Age, mean | 43.21 | 43.36 | 42.90 |
| Age interval (years), % (n) | |||
| 18-24 | 21.3 (719) | 21.2 (484) | 21.3 (235) |
| 25-44 | 32.4 (1,094) | 32.3 (736) | 32.5 (358) |
| 45-64 | 32.2 (1,088) | 31.9 (727) | 32.8 (361) |
| ≥65 | 14.2 (479) | 14.5 (331) | 13.4 (148) |
| Education, % (n) | |||
| No studies | 22.4 (756) | 24.1 (550) | 18.7 (206) |
| Elementary | 37.4 (1,265) | 37.7 (859) | 36.8 (406) |
| Middle | 26.9 (1,247) | 37.4 (853) | 35.8 (394) |
| Higher | 3.3 (112) | 0.7 (16) | 8.7 (96) |
| Occupation, % (n) | |||
| Student | 17.6 (594) | 18.0 (411) | 16.6 (183) |
| Employed | 56.1 (1,897) | 55.8 (1,271) | 56.8 (626) |
| Unemployed | 10.4 (350) | 9.5 (217) | 12.1 (133) |
| Retired | 15.9 (539) | 16.6 (379) | 14.5 (160) |
| BMI (Kg/m2) % (n) | |||
| < 18,5 | 3.6 (120) | 3.8 (86) | 3.1 (34) |
| 18.5-24.9 | 46.1 (1,558) | 44.5 (1,013) | 49.5 (545) |
| 25.0-29.9 | 34.1 (1,153) | 34.4 (784) | 33.5 (369) |
| ≥ 30.0 | 16.2 (549) | 17.3 (35) | 14.0 (154) |
| Active Smoker % (n) | |||
| No | 79.2 (2,678) | 82.0 (1,869) | 73.4 (809) |
| Yes | 20.8 (702) | 18.0 (409) | 26.6 (293) |
Abbreviations: BMI—Body Mass Index; n—number of participants.
Table 2.
Oral health care and self-reported perception about oral health condition descriptive data (n = 3,380).
Table 2.
Oral health care and self-reported perception about oral health condition descriptive data (n = 3,380).
| Variable | Total (n = 3,380) | Pre-lockdown (n =2,278 ) | Post-lockdown (n=1,102) |
|---|---|---|---|
| Type of toothbrush, % (n) | |||
| Manual | 88.6 (2,993) | 88.5 (2,017) | 88.6 (976) |
| Electric | 10.9 (368) | 10.8 (246) | 11.1 (122) |
| Toothbrush frequency % (n) | |||
| 2–3 times/daily | 75.6 (2,555) | 81.2 (1,847) | 64.2 (708) |
| 1 time/daily | 15.0 (507) | 15.5 (352) | 14.1 (155) |
| 2–6 times/weekly | 7.3 (248) | 1.9 (44) | 18.5 (204) |
| Never | 2.1 (70) | 1.5 (35) | 3.2 (35) |
| Dental Floss usage, % (n) | |||
| No | 65.8 (2,225) | 62.0 (1,413) | 73.7 (812) |
| Yes | 34.2 (1,155) | 38.0 (865) | 26.3 (290) |
| Teeth Heath Perception, % (n) | |||
| Excellent | 2.5 (84) | 2.5 (58) | 2.4 (26) |
| Very good | 9.6 (326) | 9.4 (215) | 10.1 (111) |
| Good | 43.3 (1,465) | 43.7 (995) | 42.6 (470) |
| Weak | 29.3 (990) | 29.4 (670) | 29.0 (320) |
| Very Weak | 15.2 (515) | 14.9 (340) | 15.9 (175) |
| Gums Health perception, % (n) | |||
| Excellent | 4.0 (136) | 4.3 (97) | 3.5 (39) |
| Very good | 13.0 (440) | 12.6 (287) | 13.9 (153) |
| Good | 52.2 (1,766) | 52.4 (1,193) | 52.0 (573) |
| Weak | 24.2 (819) | 24.1 (549) | 24.5 (270) |
| Very Weak | 6.5 (219) | 6.7 (152) | 6.1 (67) |
| Gum bleeding. % (n) | |||
| No | 61.5 (2,078) | 61.3 (1,396) | 61.9 (682) |
| Yes | 38.5 (1,302) | 38.7 (882) | 38.1 (420) |
| Last dental visit, % (n) | |||
| <1 year | 50.7 (1,714) | 51.5 (1,174) | 49.0 (540) |
| 1–2 years | 15.4 (522) | 15.0 (342) | 16.3 (180) |
| 3–4 years | 15.5 (524) | 15.2 (347) | 16.1 (177) |
| ≥5 years | 17.1 (578) | 16.8 (383) | 17.7 (195) |
| Never | 1.2 (42) | 1.4 (32) | 0.9 (10) |
Table 3.
Comparison of dental caries experience between pre-lockdown and post-lockdown periods, considering various variables (n = 3,380).
Table 3.
Comparison of dental caries experience between pre-lockdown and post-lockdown periods, considering various variables (n = 3,380).
| Variable | Pre-lockdown (n =2,278) | Post-lockdown (n=1,102) | ||||||
|---|---|---|---|---|---|---|---|---|
| DT | MT | FT | DMFT | DT | MT | FT | DMFT | |
| Sex | ||||||||
| Female | 5.88 (4.46)a | 4.62 (5.98)a | 3.87 (3.94)a | 12.38 (6.72)a | 5.39 (4.65)a | 5.39 (7.08)a | 3.27 (4.40)a | 11.01 (7.10)a |
| Male | 6.40 (4.8)b | 4.25 (5.34)a | 3.09 (3.39)b | 11.74 (6.50)b | 5.43 (4.63)a | 4.71 (6.03)a | 2.77 (4.00)a | 10.96 (6.98)a |
| Age interval (years) | ||||||||
| 18-24 | 4.91 (4.63)a | 0.32 (0.96)a | 2.10 (2.63)a | 8.25 (6.02)a | 4.50 (4.52)a | 3.08 (5.00)a | 1.39 (2.15)a | 9.76 (7.14)a |
| 25-44 | 6.77 (5.06)b | 2.21 (3.03)b | 3.83 (3.78)b | 11.24 (6.03)b | 5.83 (5.02)b | 3.26 (4.56)a | 2.99 (3.66)b | 11.20 (7.13)b |
| 45-64 | 6.30 (4.19)c | 6.73 (5.63)c | 4.56 (4.22)c | 14.13 (6.12)c | 5.75 (4.52)b | 6.48 (6.91)b | 4.08 (4.98)c | 11.45 (6.80)b |
| ≥65 | 5.82 (4.06)d | 10.63 (7.01)d | 2.89 (3.14)d | 15.39 (6.65)d | 4.97 (3.88)ab | 9.41 (9.32)b | 3.42 (5.21)b | 11.30 (7.15)b |
| Education | ||||||||
| No studies | 7.16 (5.07)a | 8.62 (7.29)a | 2.40 (2.98)a | 14.34 (6.96)a | 6.44 (4.78)a | 8.48 (8.48)a | 2.28 (3.38)a | 11.48 (6.61)a |
| Elementary | 6.22 (4.54)b | 3.72 (4.68)b | 3.49 (3.64)b | 11.49 (6.28)b | 5.44 (4.60)b | 4.29 (5.74)b | 3.67 (4.77)b | 11.59 (6.98)a |
| Middle | 5.22 (4.18)c | 2.43 (3.77)c | 4.40 (4.08)c | 11.29 (6.45)b | 5.09 (4.53)b | 4.59 (5.96)b | 3.29 (4.21)b | 11.14 (7.22)a |
| Higher | 8.56 (4.91)ab | 11.13 (6.32)a | 1.94 (3.24)a | 15.00 (6.61)c | 4.31 (4.60)b | 3.36 (6.30)c | 1.21 (2.63)c | 6.82 (6.17)b |
| Occupation | ||||||||
| Student | 4.27 (4.27)a | 0.41 (1.10)a | 2.35 (2.90)a | 8.28 (6.24)a | 4.33 (4.61)a | 3.83 (5.60)a | 1.38 (2.06)a | 9.55 (7.16)a |
| Employed | 6.44 (4.53)b | 3.87 (4.61)b | 4.22 (4.01)b | 12.16 (6.19)b | 5.80 (4.75)b | 4.48 (5.98)ab | 3.36 (4.32)b | 11.43 (7.01)b |
| Unemployed | 7.90 (5.21)c | 6.02 (6.98)c | 3.10 (3.82)ac | 13.84 (6.23)c | 5.45 (4.74)b | 5.28 (6.65)b | 3.33 (4.10)b | 10.82 (6.94)ab |
| Retired | 5.84 (4.23)d | 10.02 (6.79)d | 2.88 (3.09)c | 15.21 (6.70)d | 5.04 (3.88)b | 8.84 (8.75)c | 3.58 (5.33)b | 11.04 (7.01)b |
| Toothbrush frequency | ||||||||
| 2–3 times/daily | 6.09 (4.63)a | 4.29 (5.65)a | 3.53 (3.76)a | 11.98 (6.64)a | 5.87 (4.52)a | 5.70 (6.79)a | 3.34 (3.88)a | 12.19 (6.74)a |
| 1 time/daily | 6.16 (4.56)a | 5.07 (5.95)b | 3.56 (3.55)a | 12.63 (6.62)a | 5.72 (5.02)a | 5.49 (6.93)a | 3.34 (4.85)a | 10.84 (7.06)b |
| 2–6 times/weekly | 5.18 (4.39)a | 6.07 (7.11)ab | 4.05 (4.20)a | 13.16 (6.06)a | 3.62 (4.21)b | 3.29 (6.01)b | 1.72 (4.04)b | 7.14 (6.68)c |
| Never | 6.40 (4.47)a | 6.03 (5.44)b | 4.49 (4.44)a | 13.31 (6.88)a | 4.97 (5.27)ab | 1.80 (2.86)b | 3.97 (7.27)a | 9.89 (7.12)ab |
| BMI (Kg/m2) | ||||||||
| < 18,5 | 5.56 (4.71)ac | 2.64 (497)a | 2.57 (2.29)a | 10.72 (6.91)a | 3.35 (4.13)a | 4.26 (6.11)a | 1.38 (1.46)a | 9.21 (6.91)a |
| 18.5-24.9 | 5.63 (4.76)a | 3.38 (5.43)a | 3.60 (3.81)a | 11.23 (6.62)a | 5.13 (4.59)b | 4.27 (6.11)a | 2.78 (3.94)a | 10.42 (7.08)a |
| 25.0-29.9 | 6.41 (4.60)bc | 5.25 (5.72)b | 3.71 (3.91)a | 12.76 (6.51)b | 6.09 (4.76)b | 5.57 (6.67)ab | 3.34 (4.44)ba | 11.85 (7.05)b |
| ≥ 30.0 | 6.72 (4.85)b | 6.12 (6.00)c | 3.35 (3.69)a | 13.47 (6.51)b | 5.18 (4.40)b | 7.11 (8.03)b | 3.75 (4.99)a | 11.34 (6.78)ab |
| Teeth Heath Perception | ||||||||
| Excellent | 4.60 (4.13)a | 2.03 (4.38)a | 2.02 (2.59)a | 8.76 (6.82)a | 3.54 (3.58)a | 4.69 (7.86)a | 3.23 (4.18)a | 10.31 (5.87)a |
| Very good | 6.06 (5.08)b | 2.06 (3.69)a | 2.63 (3.34)a | 10.07 (6.29)a | 4.83 (5.08)a | 4.18 (5.89)a | 1.88 (2.99)a | 9.95 (6.71)a |
| Good | 5.87 (4.63)b | 3.79 (5.50)b | 3.47 (3.69)b | 11.55 (6.74)b | 5.20 (4.61)a | 3.82 (5.44)ab | 2.94 (3.79)ab | 10.94 (7.14)a |
| Weak | 6.27 (4.40)b | 5.56 (5.97)c | 3.91 (3.83)c | 13.20 (6.30)c | 5.99 (4.50)b | 6.40 (7.56)ac | 3.31 (4.36)ab | 11.45 (7.09)a |
| Very Weak | 6.64 (4.67)c | 6.26 (6.20)c | 3.97 (3.99)c | 13.56 (6.46)c | 5.52 (4.70)b | 6.82 (7.36)ac | 3.67 (5.55)ab | 11.03 (7.05)a |
Data are presented as mean (standard deviation). Different letters indicate statistically different mean values (Kruskal-Wallis test, P < 0.05). Abbreviations: BMI, Body Mass Index; DT, decayed teeth; MT, missing teeth; FT, filled teeth; DMFT, Decayed, Missing, and Filled Teeth index; n = number of participants. The statistical significance level was set at P < 0.05.
Table 4.
Comparison of dental caries experience between pre-lockdown and post-lockdown periods (n= 3,380).
Table 4.
Comparison of dental caries experience between pre-lockdown and post-lockdown periods (n= 3,380).
| Variable | DCP (%; n) | DT | MT | FT | DMFT |
|---|---|---|---|---|---|
| Pre-lockdown | 91.8 (2,092)a | 6.09 (4.61)a | 4.47 (5.73)a | 3.56 (3.75)a | 12.13 (6.64)a |
| Post-lockdown | 84.5 (931)b | 5.40 (4.64)b | 5.10 (6.66)a | 3.06 (4.24)b | 10.99 (7.05)b |
| Total | 89.4 (3,023) | 5.87 (4.63) | 4.68 (6.06) | 3.39 (3.92) | 11.76 (6.79) |
Data are presented as mean (standard deviation). Different letters indicate statistically different mean values among the variables (Mann-Whitney test, p < 0.05). Abbreviations: DCP, Dental Caries Presence; DT, decayed teeth; MT, missing teeth; FT, filled teeth; DMFT, Decayed, Missing, and Filled Teeth index; n = number of participants. The statistical significance level was set at P < 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



