
Submitted:
14 January 2024
Posted:
15 January 2024
You are already at the latest version
Abstract
Food allergy (FA) affects approximately 6–8% of children worldwide causing a significant impact on the quality of life of children and their families. In the years, the possible role of weaning in the development of FA has been studied. According to recent studies, the role of weaning in its development is still controversial and influenced by several factors, such as the type of food, the age at food introduction and family history. In this narrative review, we aimed to collected the most recent evidence about weaning and its role in FA development, organizing the gathered data based on both the type of study and the food.
Keywords:
food allergy
; weaning
; FA in weaning
; early introduction
; egg allergy
1. Introduction
Food allergy (FA) can be defined as an adverse reaction to a specific food antigen, normally harmless to the healthy population, which is mediated by immunological mechanisms in subjects susceptible to that specific allergen [1]. Any food can cause FA, however only a small group of food accounts for most of these reactions. Chicken eggs, cow’s milk, peanuts, tree nuts, fish, crustacean shellfish, wheat and soy are mostly implicated [2]. Food allergies can be categorized into IgE-mediated and non-IgE-mediated ones. The former are characterized by the presence of IgE antibodies specific for an allergen, which are formed by B-cells after their stimulation consequent to antigen presentation by the Antigen-Presenting Cells (APCs) to T-cells. Upon re-exposure to the same allergen histamine and other mediators are released and this results in immediate hypersensitivity allergy symptoms [3,4]. The non- IgE mediated forms of FA are a minority of the total and worse characterized and are usually due to acute or chronic inflammation in the gastrointestinal (GI) tract [5,6]. The clinical manifestations of food allergies are highly variable including skin, GI, respiratory and systemic manifestations with varying severity [7,8,9]. The diagnostic approach begins with a careful medical history collection and a physical examination. A food diary can be often helpful to track contact with the culprit food [10]. Blood tests can be performed, although oral food challenge (OFC) currently represents the diagnostic gold standard [11]. Once the diagnosis has been established, the treatment is the elimination of the offending allergen. Patients at risk of anaphylaxis should be trained to recognize early symptoms and should be instructed in the proper use of self-injectable epinephrine [12].
Development of FA can be influenced by different elements, such as the timing of introduction of the suspected food. The aim of this narrative review is to collect all the studies that concern the effects of early introduction of potential allergens during weaning in infants at risk of developing FA.
2. Digestion and Mucosal Barrier
2.1. Digestion
Through the GI tract the ingested food undergoes a series of degradation processes that allow the absorption of nutrients [13]. The first step in proteins degradation occurs in the mouth [14]. Once the denaturized proteins reach the small intestine they are subjected to both endopeptidase and exopeptidase activity: the former are represented by trypsin, chymotrypsin and elastase; the latter are carboxypeptidase A and B [15]. An important role in this phase is performed by the epithelial brush border, thanks to the anchorage of endopeptidase on their apical side, and to the activity of the exopeptidase which are presented on it [16].
The digestive process can be influenced by different factors, such as enzymatic activity, gastric pH, subject health status, diet and GI microbiota [17, 18].
2.2. Mucosal Barrier: Composition and Role
The intestinal barrier represents one of the first and most important defense mechanisms and it plays a role in the pathophysiology of food allergies. One of its main purposes is to maintain intestinal homeostasis, limiting allergens access and permitting the passage of nutrients to the subepithelial space. This protective function can be ensured thanks to the two-layer composition of the intestinal barrier: an external physical layer and an internal immunological layer [19].
One of the elements that are part of the former is the epithelial monolayer, in which different types of cells can be found, such as the enterocytes, goblet cells, enteroendocrine cells, Paneth cells and the stem cells located at the crypt’s base [20]. In a healthy subjects the paracellular transition of elements is well regulated by the presence of junctional complexes between enterocytes [21].
Above the epithelial layer there is a strong element, which is the mucus layer, composed of high O-glycosylated glycoproteins which are secreted by the prior mentioned goblet cells [22]. This layer plays both a protective role against GI microbes and permits the passage of nutrients and essential molecules [23, 24].
The internal immunological layer is composed primarly of immune cells that reside whithin the intestinal epithelium. The innate immune system represents the first line of the immunological layer; the prime mechanism is the activation of the pattern-recognition receptors (PRRs), like the Toll-Like Receptors (TLRs). These receptors lead to a cytokine release which is responsible for the activation of the innate immune cells and the release of antimicrobial elements and inflammatory cytokines [25]. When the innate immune system is not sufficient, the adaptive system is activated. The main actors of the adaptive immune system are the lymphocytes, also thanks to the secretion of sIgA, while the other mechanism is mediated by the oral tolerance [26].
The above mentioned barrier works differently in allergic people when compared to healthy subjects [27]. It is unclear whether if FA is responsible for increased permeability of the mucosal barrier or wheter subjects with a high intestinal permeability are at a greater risk of developing food allergies. Several studies have been conducted on this topic, concluding that both theories could be valid [19]. The other mechanism possibly responsible for the onset of food allergies is the different uptake that characterizes the atopic subjects [28]. An allergic reaction is triggered when intact proteins or their fragments that are not well degraded pass through the epithelial layer. Studies conducted on rats and mice show that in the allergic models, the passage of bigger fragments or entire proteins through the epithelial layer happens exclusively via the transcellular pathway, facilitating the formation of the IgE/CD3 complex [29, 30] .
Atopic subjects present an enhanced transport, that is composed of two phases: phase I occurs thanks to a higher concentration of IgE CD3 receptors (FcεRII) on the enterocytes of allergic subjects and happens when dietary allergens bind to the IgE/CD3, guaranteeing their transport to the lamina propria; phase II starts once dietary allergens are released by the IgE/CD3 complex into the lamina propria and bind to the IgE already attached to the tissue resident mast cells, inducing a degranulation response. The mediators released by these mast cells (histamine, prostaglandins and proteases) affects the junctional complexes (Figure 1) [27].
3. Microbiota and Food Allergies
Our organism is colonized by an enormous number of micro-organisms. Most of them live in our gut, constituting the so-called gut microbiota. The human gut microbiota represents a complex ecosystem contributing to essential functions for the host, such as promoting metabolic benefits, ensuring immune homeostasis and immune responses, and protecting against pathogen colonization [31-34].
Gut microbiota composition can be influenced by different factors, such as dietary habits, the use of formulas instead of breastfeeding, antibiotic therapies, and others. It’s composition changes substantially at two stages: from birth to weaning, and from weaning to adulthood driven by further diversification of the diet [35].
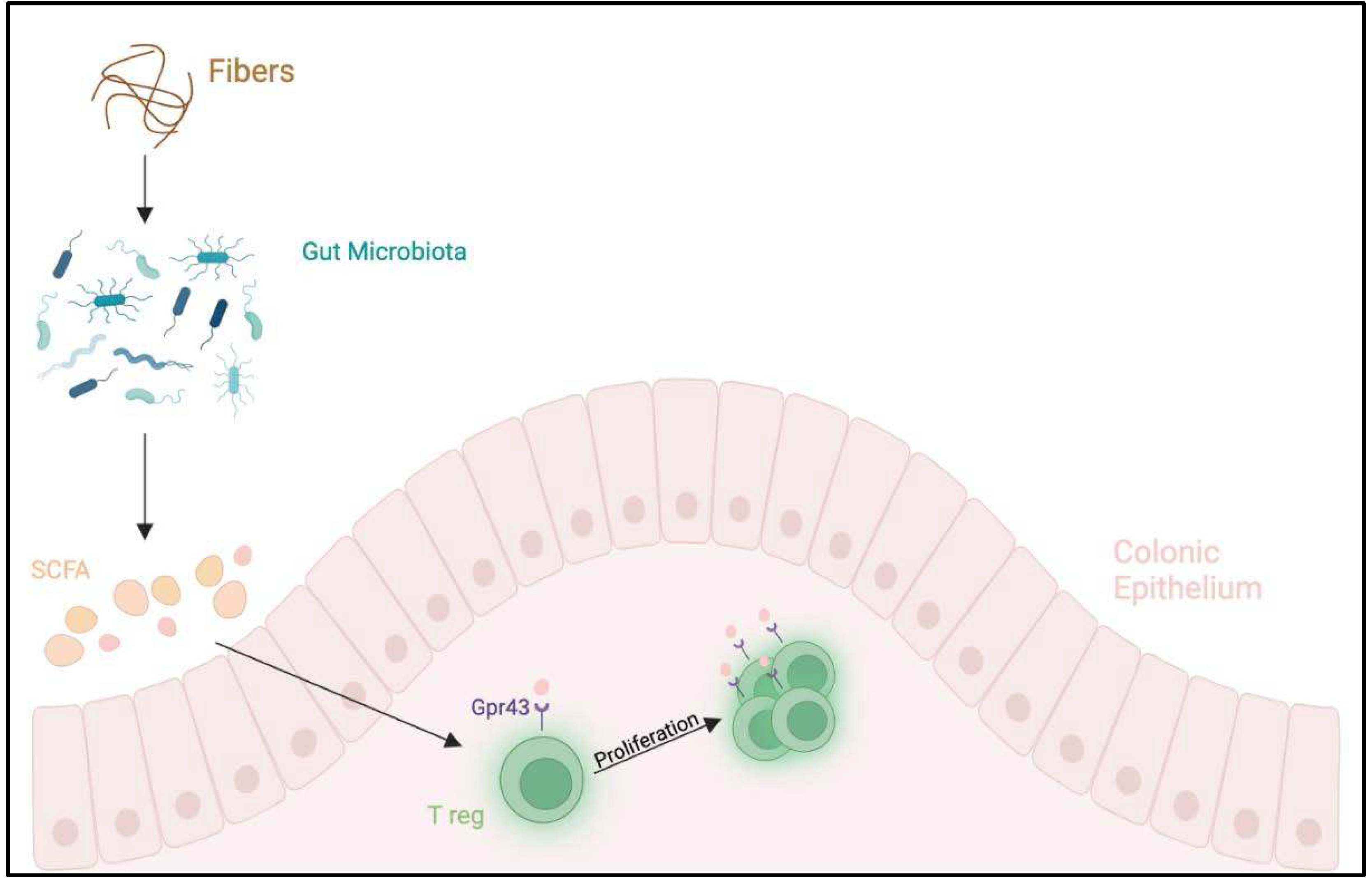
The relationship between the host and the microbiota is symbiotic and can maintain a stable environment where microorganisms are fed with nutrients supplied in the intestinal tract, while the host gains products from microbial fermentation conversion of dietary indigestible components, fibers, into short-chain fatty acids (SCFA); mainly acetate, propionate and butyrate, contributing to an estimated 10% of our energy requirement, vitamin K and B12 production, and protection against potential pathogens. An alterations of gut microbiota can influence the development of several diseases, such as functional GI diseases, infections, IBD, liver diseases, GI malignancies, obesity and metabolic syndrome, diabetes mellitus, autism, allergic diseases, and others (Figure 2) [34,35].
Environmental factors such as antibiotic use during infancy and maternal antibiotic use during pregnancy, change the intestinal bacterial populations increasing the risk of FA development.
Studies conducted on gnotobiotic (germ-free) mice, demonstrated that a Clostridia-containing microbiota can play a protective role in terms of FA development, and its presence can be altered by the use of antibiotics. Clostridia colonization induces IL-22 production by both RAR-related orphan receptor gamma (RORγt)+ ILCs (innate lymphoid cells) and T cells in the intestinal lamina propria (LP) and this cytokine acts to reduce uptake of orally administered dietary antigen into the systemic circulation, contributing, in part, to protection against sensitization [19,36,37,38].
In germ-free mouse models gut-associated lymphoid tissues (GALT) fails to develop when microbial colonization is delayed, leading to a Th2 skewed immune response. Microbial colonization has been shown to be important in the development of Th1 response and regulatory T cells (Tregs), which are necessary to maintain immunologic balance and promote tolerance. Moreover, gut microbiota plays a significant role in the development and maintenance of barrier function and its alteration may promote allergic sensitization [19,39].
Gut microbiota is responsible for the activation of TLR in intestinal epithelial cells (IECs). TLR4 deficient mice have been shown to have a Th-2 skewed immune response and an increased susceptibility to FA. Finally, a specific microbiota signature was recently linked to mice carrying a gain-of-function mutation in the IL-4 receptor α chain that results in an increased susceptibility to oral allergic sensitization and anaphylaxis [22,40,41].
4. Weaning and Its Role in Allergies
FA is a substantial and evolving public health issue, recently emerging over the last 10-15 years, and its prevalence has increased over the recent decades [44]. The clinical approach to FA has always been controversial. In the past, the prevention for FA was based on food avoidance. In high-risk infants (i.e with atopy in first-degree family members) certain food avoidance was recommended in pregnancy and during breastfeeding to prevent the onset of allergic diseases [45]. Additionally, the major scientific societies used to recommend a late introduction of allergenic foods on weaning for children who are at risk of allergies’ development: cow’s milk until the age of 12 months, eggs until 2 years and peanuts, tree nuts and fish until 3 years was recommended to be avoided [46]. These recommendations came from the assumption that a certain degree of “immaturity” of the mucosal immunity during infancy would allow an easier sensitization towards food antigens [47]. Despite these recommendations, several studies through the years have shown that a delayed exposure to allergenic foods not only did not reduce the risk of FA [48-50] but could lead to serious consequences on patients’ and families’ quality of life, rising costs for society [51].
Therefore, current guidelines issued by the several scientific societies, such as the World Health Organization (WHO), the America Academy of Pediatrics (AAP) [52], the European Academy of Allergy and Clinical Immunology (EAACI) [53], the European Society for Pediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) [54], and the European Food Safety Authority (EFSA) no longer recommend this approach, based on the fact that no scientific evidence justifies a delayed introduction of solid foods after 6 months of age to prevent allergy both in high and low-risk infants.
On the contrary, clinical practice guidelines now recommend earlier introduction of allergenic foods, and infant feeding practices have changed substantially in some regions [44]. It is still unclear whether earlier introduction of allergenic foods will reduce overall FA prevalence in population. Several studies have reported reduced FA following earlier introduction of multiple allergenic foods, particularly in peanut and egg allergy [45,46,47]. However, there is low-certainty evidence that early fish introduction was associated with reduced allergic rhinitis and allergic sensitization [49]. The aim of this narrative review is to collect and summarize all the studies that concern the effects of an early introduction of potential allergens during weaning in infants, drawing conclusions about the possible role of weaning in preventing FA development in both high risk and low risk infants.
5. Methods
Several studies tried to demonstrate the role of weaning in the management of FA. In this review we selected the most relevant articles on this topic from Pubmed and Scopus dashboard. The following keywords were used for the research: “food allergy”, “weaning”, “FA in weaning”, “early introduction”, “egg allergy”. Studies from 2008 to 2023 were selected, excluding reviews and meta-analyses.
6. Discussion
To assess the role of weaning in the development of FA, we analysed several studies, evaluating the possible consequences of an early food introduction (eggs, cow’s milk, peanuts, and others). Most of these studies were performed in high-risk population. Patients are considered at high risk of developing FA whether they have history of eczema or if they have first-degree relative with history of eczema, asthma, allergic rhinitis, or food allergy.
7. Studies
7.1. Studies Performed in High-Risk Populations
7.1.1. Egg Proteins
Regarding hen’s egg, five intervention studies showed no clear reduction of allergic manifestations [56-60]. However, one study from Japan showed a significant reduction of hen’s egg allergy without adverse events: a two-step egg introduction for prevention of egg allergy in high-risk infants with eczema was performed in the Prevention of Egg Allergy with Tiny Amount Intake Trial (PETIT), a randomized, double-blind, placebo-controlled trial (RDBPCT), conducted by Natsume, et al in 2017 in which infants aged 4-5 months were enrolled to investigated whether or not early stepwise introduction of eggs in infants with eczema combined with optimal eczema treatment would prevent egg allergy at 1 year of age. 147 infants were randomly assigned to early introduction of egg or placebo. The primary outcome was the proportion of participants with hen's egg allergy confirmed by OFC at 12 months of age, assessed blindly by standardized methods, in all randomly allocated participants who received the intervention. The final results showed that five (8%) of 60 participants had an egg allergy in the egg group compared with 23 (38%) of 61 in the placebo group (RR (95% CI):0.22 (0.09-=.54); P= 0.0001). The authors concluded that the introduction of heated egg in a stepwise manner along with aggressive eczema treatment is a safe and efficacious way to prevent hen's egg allergy in high-risk infants [55].
A RDBPCT was performed by Palmer, et al in 2013 to determine whether early regular oral egg exposure woukd reduce subsequent IgE-mediated egg allergy in infants with moderate-to-severe eczema. 86 infants were allocated to the group that received 1 teaspoon of pasteurized raw whole egg powder (n 49) or rice powder (n 37) daily from 4 to 8 months of age. The primary outcome was to investigate the onset IgE-mediated egg allergy at 12 months. A high proportion, 31% (15/49), of infants randomized to receive egg had an allergic reaction to the egg powder and did not continue powder ingestion. At 4 months of age, before any known egg ingestion, 36% (24/67) of infants already had egg specific IgE levels. At 12 months, a lower (but not significant) proportion of infants in the egg group (33%) were given a diagnosis of IgE-mediated egg allergy compared to the control group (51%; relative risk, 0.65; 95% CI, 0.38-1.11; P=0.11). The Authors concluded that an early, regular oral exposure to egg in infants with moderate-severe eczema may induce immune tolerance [56].
Again, Palmer et al in 2017 conducted a RCT in which infants at hereditary risk of developing hen’s egg allergy aged 4 to 6 months were randomly allocated to receive daily pasteurized raw whole egg powder (n = 407) or a color-matched rice powder (n = 413) to age 10 months. All infants followed an egg-free diet and cooked egg was introduced to both groups at age 10 months. The primary outcome was IgE-mediated egg allergy defined by a positive pasteurized raw egg challenge and egg sensitization at age 12 months. This study concluded that there is no significant difference between the two studied groups: egg group 7.0% vs control 10.3%; adjusted relative risk, 0.75; 95% CI, 0.48-1.17; P = 0.20 [57].
In 2017 the Australian group of Tan, conducted a RCT to assess whether dietary introduction of egg between 4 and 6 months in infants at risk of allergy would reduce sensitization to egg (Beating Egg Allergy Trial, BEAT). Infants with a skin prick test (SPT) response to egg white (EW) of less than 2 mm were randomized at age 4 months to receive whole-egg powder or placebo (rice powder) until 8 months of age. The primary outcome was an EW SPT response of 3 mm or greater at age 12 months. 319 infants were randomized: 165 to egg and 154 to placebo. Sensitization to EW at 12 months was 20% and 11% in infants randomized to placebo and egg, respectively. Introduction of whole-egg powder into the diets of high-risk infants reduced sensitization to EW and induced egg-specific IgG4 levels. However, 8.5% of infants randomized to egg were not amenable to this primary prevention [58].
7.1.2. Cow’s Milk, Peanut, Hard-Boiled Hen’s Egg, Sesame, Whitefish (cod), and Wheat
A recent RCT conducted in Japan in 2022 evaluated multiple food allergies could be safely prevented by simultaneously administering very small amounts of multiple foods. Infants aged 3 to 4 months, diagnosed with atopic dermatitis, from 14 primary care pediatric clinics in Japan were enrolled. The infants were administered either mixed allergenic food powder (MP) containing egg, cow’s milk, wheat, soybean, buckwheat, and peanuts, or placebo powder (PP). The amount of powder was increased in a stepwise manner on weeks 2 and 4 and continued until week 12. The occurrence of FA episodes after powder intervention was assessed at 18 months of age. A total of 163 participants were randomly allocated to either the MP group (n 83) or the PP group (n 80). The incidence of FA episodes by 18 months was significantly different between the MP and PP groups (7/83 vs. 19/80, respectively; risk ratio 0.301 [95% CI 0.116e0.784]; P= 0.0066). The occurrence of egg allergy was lower in the MP group. In addition, FA episodes from any of the other five foods were significantly reduced [59].
7.1.3. Rusk-like Biscuit Powder
A protocol for a RDBPCT, single-center clinical trial is ongoing in Berlin: 150 infants with atopic eczema at 4–8 months of age will be randomized in a 2:1 manner into an active group that will receive rusk-like biscuit powder with hen’s egg (HE), cow’s milk (CM), peanuts (PN), and hazelnuts (HN) (initially approximately 2 mg of each food protein) for 6–8 months . In the placebo group, a sugar free rusk-like biscuit powder, without HE, CM, PN, and HN, will be provided, analogously to the intervention group, on a daily basis. The amount of allergens in the powder will be increased by three times every 6 weeks. All study participants who are sensitized to HE, CM, PN, or HN at the end of the interventional period will undergo an OFC to the respective food in a further visit. The primary endpoint is to determine the occurrence of IgE-mediated FA to at least one of the four foods after 6–8 months of intervention (i.e., at around 1 year of age). The secondary endpoints include the occurrence of multiple food allergies, severity of eczema, wheezing, and sensitization levels against food allergens [60].
7.1.4. Peanut
Du Toit started the Learning Early About Peanut Allergy (LEAP) study in 2015 in England, which included 640 babies aged between 4 and 11 months who had severe eczema or an allergy to egg, or both. Patients were grouped into two different study cohorts based on the results of a skin-prick test for peanut; participants in each study cohort were then randomly assigned to a group in which dietary peanut would be consumed or a group in which its consumption would be avoided. Among the 530 infants in the intention-to-treat population, who initially had negative results on the SPT, the prevalence of peanut allergy at 60 months of age was 13.7% in the avoidance group and 1.9% in the consumption group (P<0.001). Among 98 participants in the intention-to-treat population, who initially had positive test results, the prevalence of peanut allergy was 35.3% in the avoidance group and 10.6% in the consumption group (P=0.004) [61].
7.2. Studies Performed in Low-Risk Populations
7.2.1. Egg Proteins
In 2017 Bellach, et al conducted a RDBPCT to assess the possible role of early hen’s egg introduction in preventing sensitization (Hen’s Egg Allergy Prevention, HEAP). 383 infants not sensitized to hen’s egg at 4 to 6 months of age were randomized to the placebo and the intervention group. First, 524 infants were enrolled in the study, but, in the end, 298 patients were evaluated for the primary outcome, showing that 5.6% (6/124) in the study group and 2.6% (4/152) in the placebo group were sensitized to hen’s egg at age 12 months (P 0.35); in addition, 2.1% were confirmed to have hen’s egg allergy versus 0.6 in the placebo group. In this study there was no evidence that early consumption of hen’s egg prevents hen’s egg allergy [62].
7.2.2. Cow’s Milk, Peanut, Hard-Boiled Hen’s Egg, Sesame, Whitefish (Cod), and Wheat
In 2016 Perkin, et al conduced the Enquiring About Tolerance (EAT) study which is a population-based randomized controlled trial that enrolled exclusively breastfed infants from England and Wales regardless of atopic status or family history of allergy to assess whether the introduction of six common foods could prevent FA in a general population. The early introduction group (EIG) continued breastfeeding with sequential introduction of 6 allergenic foods between 4 and 6 months of age: cow’s milk, peanut, hard-boiled hen’s egg, sesame, whitefish (cod), and wheat; the standard introduction group continued exclusive breastfeeding for around 6 months. 1303 infants were enrolled. The control about tolerance were based on the execution of SPT’S, blood exams, eczema (SCORAD score), microbiota, growth and a food diary, at one and three years of age. The analysis showed allergy to one or more of the six intervention foods developed in 7.1% of the participants in the standard-introduction group (42 of 595 participants) and in 5.6% of those in the early-introduction group (32 of 567) [63].
7.3. Studies Performed in Both High-Risk and Low-Risk Populations
7.3.1. Cow’s Milk Proteins
In 2008 Sneijder conducted a study evaluating the association between the introduction of cow’s milk products or other solid food products and atopic manifestations in the second year of life. 2558 infants were enrolled and data on the introduction of cow’s milk products and other food products, and on the outcomes (eczema, atopic dermatitis, recurrent wheeze, any sensitization, sensitization against cow’s milk, hen’s egg, peanut, and at least one inhalant allergen), were collected through questionnaires at 34 weeks of gestation and 3, 7, 12, and 24 months postpartum. They showed that a delayed introduction of both cow’s milk products and other food products was associated with a higher risk for eczema (P =.01 and .02 for trend, respectively), while a delay in other food products introduction was associated with a higher risk for AD according to UK-WP criteria (P =.00 trend) [64].

Table 1.
Main clinical studies evaluating the possible role of weaning in preventing food allergies development in infants.
Table 1.
Main clinical studies evaluating the possible role of weaning in preventing food allergies development in infants.
| Author, Year, Country, Trial | Study Design | Sample Size | Population | Inclusion criteria | Allergen | Follow-up | Outcome |
|---|---|---|---|---|---|---|---|
| Snijders et al., 2008 Netherlands KOALA [64] |
Prospective birth cohort study | 2558 infants | General Population | Pregnant women with diverse lifestyles | Cow’s milk products and other solid products. | Questionnaires at 7,12, 24 months; Specific IgE > 0.3 UI/ml against eggs, cow’s milk at age 2 |
Delayed introduction of CMP and other food products associated with higher risk for eczema (P =.01 and .02 for trend, respectively); No association between delay introduction of CMP and AD; delay introduction of other food associated with higher risk for AD (P=.00 trend) and increased risk of atopy development at the age of 2 years |
| Palmer et al., 2013 Australia STAR [56] |
RDBPCT | 86 infants: 49 SG 37 CG |
High risk | 4 month of age singleton term infants with moderate-to-severe eczema no prior egg or solid food ingestion | Hen’s egg (0,9 g/day) |
OFC and SPT at 12 months | At 12 months 33% SG, 51% CG were diagnosed IgE-mediated egg allergy (relative risk, 0.65; 95% CI, 0.38-1.11; P=0.11) |
| Du Toit et al., 2015 England LEAP [61] |
RCT | 640 infants: 319 SG 321 CG |
Infants 4 to 11 months of age with severe eczema, egg allergy, or both | High risk | Peanut (6 g/week) |
Open OFC or DBPCFC at 12, 30, and 60 months |
In the intention to treat population: 13.7% in the CG and 1.9% in the SG who had negative SPT developed peanut allergy (P<0.001) |
| Perkin et al, 2016 England EAT [63] |
RCT | 1303 infants: 652 SG 651 CG |
Exclusively breastfed infants for ≥ months, regardless of atopic status or family history of allergy | General population |
Cow’s milk, peanut, hard-boiled hen’s egg, sesame, whitefish (cod), and wheat at 3 and 6 months of age (4 g/week) |
OFC at 1 and 3 years of age after allergenics food introduction | Among Infants with sensitization to 1 or more foods at enrollment, EIG infants developed significantly less FA than SIG infants SIG, 3+34.2%; EIG, 19.2%; P= 5 .03 |
| Bellach et al., 2017 Germany HEAP [62] |
RDBPCT | 383 infants: 184 SG 199 CG |
GA >/= 34 weeks and birth weight >/= 2.5 kg Specific IgE to egg <0.35 kU/L |
General Population 4-6 months |
Hen’s egg 2,5 g 3 times/week from 4-6 to 12 months |
OFC and specific IgE ≥0.35 KU/l at 12 months after hen’s egg introduction |
sensitized to hen’s egg at age 12 months : 5.6% (6/124) in SG 2.6% (4/152) in CG (P= 0.35) Allergy to hen’s egg 2.1% in SG 0.6% in CG (relative risk,3.30;95%CI, 0.35-31.32; P=0.35) No prevention in hen’s egg sensitization nor egg allergy |
| Tan et al, 2017 Australia BEAT [58]. |
RDBCT | 319 infants: SG 165 CG 154 |
Infants with at least 1 first-degree relative with allergic disease and SPT<2 mm | High risk | Hen’s egg 350 mg from4-8 months |
EW SPT response of 3 mm or greater OFC to whole egg at age 12 months. |
Sensitization to EW at 12 months: 20% in CG 11% in SG Allergy to EW at 12 months: 10,5% in CG 6,2% in SG (odds ratio, 0.46;95% CI, 0.22-0.95; P=0.03) |
| Natsume et al, 2017 Japan PETIT [55] |
RDBPCT | 147 infants | 4-5 months of age of age with eczema | High risk | Eggs 50 mg/die (3-9 months) 250 mg/die (9-12 months) |
Open OFC at 12 months of age |
Five (8%) of 60 participants had an egg allergy in the SG compared to 23 (38%) of 61 in the CG (risk ratio 0.221;95% CI,0.090-0.543; P=0.0001) |
| Palmer et al, 2017 Australia STEP [57] |
RCT | 820 infants: SG 165 CG 154 |
Singleton infants with atopic mothers, recruited before age 6.5 months No prior egg ingestion and allergic disease |
High risk | Hen’s egg pasteurized raw whole egg powder (SG = 407) or a rice powder (CG = 413) from 6 to 10 months; introduction egg at 10 months |
OFC to egg at 12 months and SPT positive | At 12 months: IgE mediated food allergy : SG 7.0% vs CG 10.3% (RR(95%CI) 0.75 (0.48-1,17) P=0.20) |
| Nishimura et al., 2022 Japan SEED [59] |
RCT | 163 children 83 SG 80 CG |
3-4 months old with atopic dermatitis | Egg, milk, wheat, soybean, buckwheat, and peanuts | Amount of powder increased at weeks 2, and 12 week. The occurrence of FA at 18 months old |
Incidence of FA episodes by 18 months: SG 7/83 vs CG 19/80; (risk ratio 0.301 [95% CI 0.116e0.784]; P = 0.0066). Egg allergies were reduced in the SG group |
|
| Kalb et al, 2022 German TEFFA [60]. |
RCT | 150 infants with atopic eczema at 4–8 months randomized in a 2:1 manner into an SG and CG | 4-8 months old infants with eczema | High risk | Rusk-like biscuit powder with HE, CM, PN, HN 2 mg for 6-8 months |
After 6 months of intervention, they will check sensitization against hen’s egg, cow’s milk, hazelnut, and peanut | At 12 months Egg allergy: SG 2.1% CG 06% (3.30;95% CI,0.31-3132 P=0.35) |
Table 1: KOALA (in Dutch): Child, Parent and Health: Lifestyle and Genetic Constitution; CMP: Cow Milk Proteins; AD: Atopic Dermatitis; STAR=Solid Timing for Allergy Research; RDBPCT= Randomized Double Blind Placebo Controlled Trial; SG: Study group; CG: Control group; LEAP= Learning Early About Peanut; RCT= Randomized Controlled Trial; EAT= Enquiring About Tolerance; OFC= Oral Food Challenge EIG: Early Introduction Group; SIG: Sequential Introduction Group; HEAP= Hen’s Egg Allergy Prevention; GA: Gestational Age; BEAT= Beating Egg Allergy Trial; EW: Egg White; SPT= Skin Prick Test; PETIT= Prevention of Egg Allergy with Tiny Amount Intake Trial; STEP = Starting Time of Egg Protein; ; SEED= FA= Food Allergy; TEFFA= early Feeding to Prevent Food allergy in Infant with Eczema; HE: Hen’s Egg; PN: Peanuts: HN: Hazelnuts;.
8. Limitations
The present study is not free from some limitation. The main one is represented by the fact that the analyzed studies have been conducted in high-income countries. Therefore, the results cannot be applied to countries and regions all over the world. This could represent a potential “selection bias”.
9. Conclusions
FA represent a significant burden, affecting financial, social and health aspects. Therefore, their prevention would have a significant impact. The possible role of an early introduction of food in subjects both at high and low risk of developing FA have been investigated in the literature. Most of the studies of this review did not show any relationship between an early introduction of the suspected food and a reduced incidence of allergy. On the other hand, several RCT support the importance of an early introduction of allergenic food to prevent the development of FA, especially in high-risk populations, compared to low-risk ones. In particular, trials conducted so far show that early introduction of allergenic foods such as peanut and chicken egg can have a preventive effect on allergy to these foods in high-risk populations. This effect seems to be less obvious in the general population. Further studies are needed, especially on the general population to be able to provide indications in this regard. It is also likely that other elements, such as the form in which the allergen is introduced and/or the continuity of its intake, play an important role in the prevention of food allergy. However, at the moment, the data obtained make it difficult to develop universal guidelines.
In conclusion, further studies are needed to clarify the timing of food introduction and to understand whether weaning can play a main role in FA prevention, in both high and low-risk populations.
Author Contributions
Conceptualization, C.A. and G.B. methodology, C.A., M.G.P. and A.M.Z.; software, NO.; validation C.A., A.M.Z. and M.G.P.; formal analysis, NO; investigation, C.A., G.B., M.G.P., D.D.C.; V.M.; resources, A.G.; F.O.; V.M.; data curation, A.G., E.F., C.R., L.T., A.F.C., C.F. ; D.D.C., and E.S., writing—original draft preparation, A.G., E.F., C.R., L.T., A.F.C., C.F.; F.O. and E.S.; writing—review and editing, C.A., G.B., A.G., F.O.; V.M.; visualization, C.A., G.B., M.G.P. and A.M.Z.; supervision, C.A., A.M.Z. and M.G.P.; project administration, C.A. and G.B.; funding acquisition NO. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- De Martinis M, Sirufo MM, Suppa M, Ginaldi L. New Perspectives in Food Allergy. Int J Mol Sci. 2020 Feb 21;21(4):1474. [CrossRef]
- Sicherer SH, Warren CM, Dant C, Gupta RS, Nadeau KC. Food Allergy from Infancy Through Adulthood. J Allergy Clin Immunol Pract. 2020 Jun;8(6):1854–64. [CrossRef]
- Reyes-Pavón D, Jiménez M, Salinas E. Physiopathology of food allergies. Rev Alerg Mex. 2020;67(1):34–53. [CrossRef]
- Michelet M, Balbino B, Guilleminault L, Reber LL. IgE in the pathophysiology and therapy of food allergy. Eur J Immunol. 2021 Mar;51(3):531–43. [CrossRef]
- Cianferoni, A. Non-IgE Mediated Food Allergy. Curr Pediatr Rev. 2020;16(2):95–105.
- Zhang S, Sicherer S, Berin MC, Agyemang A. Pathophysiology of Non-IgE-Mediated Food Allergy. Immunotargets Ther. 2021;10:431–46. [CrossRef]
- Chong KW, Ruiz-Garcia M, Patel N, Boyle RJ, Turner PJ. Reaction phenotypes in IgE-mediated food allergy and anaphylaxis. Ann Allergy Asthma Immunol. 2020 May;124(5):473–8. [CrossRef]
- Domínguez O, Plaza AM, Alvaro M. Relationship Between Atopic Dermatitis and Food Allergy. Curr Pediatr Rev. 2020;16(2):115–22. [CrossRef]
- Zubeldia-Varela E, Barker-Tejeda TC, Blanco-Pérez F, Infante S, Zubeldia JM, Pérez-Gordo M. Non-IgE-Mediated Gastrointestinal Food Protein-Induced Allergic Disorders. Clinical Perspectives and Analytical Approaches. Foods. 2021 Nov 2;10(11):2662. [CrossRef]
- Cafarotti A, Giovannini M, Begìn P, Brough HA, Arasi S. Management of IgE-mediated food allergy in the 21st century. Clin Exp Allergy. 2023 Jan;53(1):25–38. [CrossRef]
- Barni S, Liccioli G, Sarti L, Giovannini M, Novembre E, Mori F. Immunoglobulin E (IgE)-Mediated Food Allergy in Children: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Management. Medicina (Kaunas). 2020 Mar 4;56(3):111. [CrossRef]
- Peters RL, Krawiec M, Koplin JJ, Santos AF. Update on food allergy. Pediatr Allergy Immunol. 2021 May;32(4):647–57. [CrossRef]
- Bøgh KL, Madsen CB. Food Allergens: Is There a Correlation between Stability to Digestion and Allergenicity? Crit Rev Food Sci Nutr. 2016 Jul 3;56(9):1545–67. [CrossRef]
- van Lieshout GAA, Lambers TT, Bragt MCE, Hettinga KA. How processing may affect milk protein digestion and overall physiological outcomes: A systematic review. Crit Rev Food Sci Nutr. 2020;60(14):2422–45. [CrossRef]
- Bhagavan NV, Ha CE. Chapter 11 - Gastrointestinal Digestion and Absorption. In: Bhagavan NV, Ha CE, editors. Essentials of Medical Biochemistry (Second Edition) [Internet]. San Diego: Academic Press; 2015 [cited 2023 Aug 14]. p. 137–64. Available from: https://www.sciencedirect.com/science/article/pii/B9780124166875000117. 9780.
- Nilius B, Gudermann T, Jahn R, Lill R, Petersen OH, De Tombe PP, editors. Reviews of Physiology, Biochemistry and Pharmacology [Internet]. Cham: Springer International Publishing; 2015 [cited 2023 Aug 14]. (Reviews of Physiology, Biochemistry and Pharmacology; vol. 168). Available from: https://link.springer.com/10.1007/978-3-319-22503-6.
- Verhoeckx K, Bøgh KL, Dupont D, Egger L, Gadermaier G, Larré C, Mackie A, Menard O, Adel-Patient K, Picariello G, Portmann R, Smit J, Turner P, Untersmayr E, Epstein MM. The relevance of a digestibility evaluation in the allergenicity risk assessment of novel proteins. Opinion of a joint initiative of COST action ImpARAS and COST action INFOGEST. Food Chem Toxicol. 2019 Jul;129:405–23. [CrossRef]
- Dallas DC, Sanctuary MR, Qu Y, Khajavi SH, Van Zandt AE, Dyandra M, Frese SA, Barile D, German JB. Personalizing protein nourishment. Crit Rev Food Sci Nutr. 2017 Oct 13;57(15):3313–31. [CrossRef]
- Ballegaard ASR, Bøgh KL. Intestinal protein uptake and IgE-mediated food allergy. Food Res Int. 2023 Jan;163:112150. [CrossRef]
- Umar, S. Intestinal stem cells. Curr Gastroenterol Rep. 2010 Oct;12(5):340–8.
- Steed E, Balda MS, Matter K. Dynamics and functions of tight junctions. Trends in Cell Biology. 2010 Mar 1;20(3):142–9. [CrossRef]
- Parrish A, Boudaud M, Kuehn A, Ollert M, Desai MS. Intestinal mucus barrier: a missing piece of the puzzle in food allergy. Trends Mol Med. 2022 Jan;28(1):36–50. [CrossRef]
- Ermund A, Schütte A, Johansson MEV, Gustafsson JK, Hansson GC. Studies of mucus in mouse stomach, small intestine, and colon. I. Gastrointestinal mucus layers have different properties depending on location as well as over the Peyer’s patches. American Journal of Physiology-Gastrointestinal and Liver Physiology. 2013 Sep;305(5):G341–7. [CrossRef]
- Atuma C, Strugala V, Allen A, Holm L. The adherent gastrointestinal mucus gel layer: thickness and physical state in vivo. Am J Physiol Gastrointest Liver Physiol. 2001 May;280(5):G922-929. [CrossRef]
- Santaolalla R, Abreu MT. Innate immunity in the small intestine. Current Opinion in Gastroenterology. 2012 Mar;28(2):124. [CrossRef]
- Brandtzaeg, P. The gut as communicator between environment and host: Immunological consequences. European Journal of Pharmacology. 2011 Sep 1;668:S16–32. [CrossRef]
- Perrier C, Corthésy B. Gut permeability and food allergies. Clin Exp Allergy. 2011 Jan;41(1):20–8. [CrossRef]
- Graversen KB, Ballegaard ASR, Kræmer LH, Hornslet SE, Sørensen LV, Christoffersen HF, Jacobsen LN, Untersmayr E, Smit JJ, Bøgh KL. Cow’s milk allergy prevention and treatment by heat-treated whey—A study in Brown Norway rats. Clinical & Experimental Allergy. 2020;50(6):708–21. [CrossRef]
- So AL, Pelton-Henrion K, Small G, Becker K, Oei E, Tyorkin M, Sperber K, Mayer L. Antigen Uptake and Trafficking in Human Intestinal Epithelial Cells. Dig Dis Sci. 2000 Jul 1;45(7):1451–61. [CrossRef]
- Yu LCH, Yang PC, Berin MC, Leo VD, Conrad DH, Mckay DM, Satoskar AR, Perdue MH. Enhanced transepithelial antigen transport in intestine of allergic mice is mediated by IgE/CD23 and regulated by interleukin-4. Gastroenterology. 2001 Aug 1;121(2):370–81. [CrossRef]
- Pickard JM, Zeng MY, Caruso R, Núñez G. Gut microbiota: Role in pathogen colonization, immune responses, and inflammatory disease. Immunol Rev. 2017 Sep;279(1):70–89. [CrossRef]
- Heintz-Buschart A, Wilmes P. Human Gut Microbiome: Function Matters. Trends Microbiol. 2018 Jul;26(7):563–74. [CrossRef]
- Kamada N, Seo SU, Chen GY, Núñez G. Role of the gut microbiota in immunity and inflammatory disease. Nat Rev Immunol. 2013 May;13(5):321–35. [CrossRef]
- Bibbò S, Ianiro G, Giorgio V, Scaldaferri F, Masucci L, Gasbarrini A, Cammarota G. The role of diet on gut microbiota composition. Eur Rev Med Pharmacol Sci. 2016 Nov;20(22):4742–9.
- Wopereis H, Oozeer R, Knipping K, Belzer C, Knol J. The first thousand days - intestinal microbiology of early life: establishing a symbiosis. Pediatr Allergy Immunol. 2014 Aug;25(5):428–38. [CrossRef]
- Wiertsema SP, van Bergenhenegouwen J, Garssen J, Knippels LMJ. The Interplay between the Gut Microbiome and the Immune System in the Context of Infectious Diseases throughout Life and the Role of Nutrition in Optimizing Treatment Strategies. Nutrients. 2021 Mar 9;13(3):886. [CrossRef]
- West CE, Jenmalm MC, Prescott SL. The gut microbiota and its role in the development of allergic disease: a wider perspective. Clin Exp Allergy. 2015 Jan;45(1):43–53. [CrossRef]
- Stefka AT, Feehley T, Tripathi P, Qiu J, McCoy K, Mazmanian SK, Tjota MY, Seo GY, Cao S, Theriault BR, Antonopoulos DA, Zhou L, Chang EB, Fu YX, Nagler CR. Commensal bacteria protect against food allergen sensitization. Proc Natl Acad Sci U S A. 2014 Sep 9;111(36):13145–50. [CrossRef]
- Prince BT, Mandel MJ, Nadeau K, Singh AM. Gut Microbiome and the Development of Food Allergy and Allergic Disease. Pediatr Clin North Am. 2015 Dec;62(6):1479–92. [CrossRef]
- Lee KH, Song Y, Wu W, Yu K, Zhang G. The gut microbiota, environmental factors, and links to the development of food allergy. Clin Mol Allergy. 2020;18:5. [CrossRef]
- Rachid R, Stephen-Victor E, Chatila TA. The microbial origins of food allergy. J Allergy Clin Immunol. 2021 Mar;147(3):808–13. [CrossRef]
- Shu SA, Yuen AWT, Woo E, Chu KH, Kwan HS, Yang GX, Yang Y, Leung PSC. Microbiota and Food Allergy. Clin Rev Allergy Immunol. 2019 Aug;57(1):83–97. [CrossRef]
- Maslowski KM, Vieira AT, Ng A, Kranich J, Sierro F, Yu D, Schilter HC, Rolph MS, Mackay F, Artis D, Xavier RJ, Teixeira MM, Mackay CR. Regulation of inflammatory responses by gut microbiota and chemoattractant receptor GPR43. Nature. 2009 Oct 29;461(7268):1282–6. [CrossRef]
- Prescott S, Allen KJ. Food allergy: riding the second wave of the allergy epidemic. Pediatr Allergy Immunol. 2011 Mar;22(2):155–60. [CrossRef]
- Høst A, Koletzko B, Dreborg S, Muraro A, Wahn U, Aggett P, Bresson JL, Hernell O, Lafeber H, Michaelsen KF, Micheli JL, Rigo J, Weaver L, Heymans H, Strobel S, Vandenplas Y. Dietary products used in infants for treatment and prevention of food allergy. Joint Statement of the European Society for Paediatric Allergology and Clinical Immunology (ESPACI) Committee on Hypoallergenic Formulas and the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) Committee on Nutrition. Arch Dis Child. 1999 Jul;81(1):80–4. [CrossRef]
- American Academy of Pediatrics Committee on Nutrition: Hypoallergenic infant formulas. Pediatrics. 1989 Jun;83(6):1068–9.
- Bailey M, Haverson K, Inman C, Harris C, Jones P, Corfield G, Miller B, Stokes C. The development of the mucosal immune system pre- and post-weaning: balancing regulatory and effector function. Proc Nutr Soc. 2005 Nov;64(4):451–7. [CrossRef]
- Arshad SH, Bateman B, Sadeghnejad A, Gant C, Matthews SM. Prevention of allergic disease during childhood by allergen avoidance: the Isle of Wight prevention study. J Allergy Clin Immunol. 2007 Feb;119(2):307–13. [CrossRef]
- Zutavern A, Brockow I, Schaaf B, von Berg A, Diez U, Borte M, Kraemer U, Herbarth O, Behrendt H, Wichmann HE, Heinrich J, LISA Study Group. Timing of solid food introduction in relation to eczema, asthma, allergic rhinitis, and food and inhalant sensitization at the age of 6 years: results from the prospective birth cohort study LISA. Pediatrics. 2008 Jan;121(1):e44-52. [CrossRef]
- Lack G, Fox D, Northstone K, Golding J, Avon Longitudinal Study of Parents and Children Study Team. Factors associated with the development of peanut allergy in childhood. N Engl J Med. 2003 Mar 13;348(11):977–85.
- Anvari S, Chokshi NY, Kamili QUA, Davis CM. Evolution of Guidelines on Peanut Allergy and Peanut Introduction in Infants: A Review. JAMA Pediatr. 2017 Jan 1;171(1):77–82.
- Greer FR, Sicherer SH, Burks AW, American Academy of Pediatrics Committee on Nutrition, American Academy of Pediatrics Section on Allergy and Immunology. Effects of early nutritional interventions on the development of atopic disease in infants and children: the role of maternal dietary restriction, breastfeeding, timing of introduction of complementary foods, and hydrolyzed formulas. Pediatrics. 2008 Jan;121(1):183–91.
- Muraro A, Halken S, Arshad SH, Beyer K, Dubois AEJ, Du Toit G, Eigenmann PA, Grimshaw KEC, Hoest A, Lack G, O’Mahony L, Papadopoulos NG, Panesar S, Prescott S, Roberts G, de Silva D, Venter C, Verhasselt V, Akdis AC, Sheikh A, EAACI Food Allergy and Anaphylaxis Guidelines Group. EAACI food allergy and anaphylaxis guidelines. Primary prevention of food allergy. Allergy. 2014 May;69(5):590–601.
- Fewtrell M, Bronsky J, Campoy C, Domellöf M, Embleton N, Fidler Mis N, Hojsak I, Hulst JM, Indrio F, Lapillonne A, Molgaard C. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J Pediatr Gastroenterol Nutr. 2017 Jan;64(1):119–32.
- Natsume O, Kabashima S, Nakazato J, Yamamoto-Hanada K, Narita M, Kondo M, Saito M, Kishino A, Takimoto T, Inoue E, Tang J, Kido H, Wong GWK, Matsumoto K, Saito H, Ohya Y, PETIT Study Team. Two-step egg introduction for prevention of egg allergy in high-risk infants with eczema (PETIT): a randomised, double-blind, placebo-controlled trial. Lancet. 2017 Jan 21;389(10066):276–86. [CrossRef]
- Palmer DJ, Metcalfe J, Makrides M, Gold MS, Quinn P, West CE, Loh R, Prescott SL. Early regular egg exposure in infants with eczema: A randomized controlled trial. J Allergy Clin Immunol. 2013 Aug;132(2):387-392.e1. [CrossRef]
- Palmer DJ, Sullivan TR, Gold MS, Prescott SL, Makrides M. Randomized controlled trial of early regular egg intake to prevent egg allergy. J Allergy Clin Immunol. 2017 May;139(5):1600-1607.e2. [CrossRef]
- Wei-Liang Tan J, Valerio C, Barnes EH, Turner PJ, Van Asperen PA, Kakakios AM, Campbell DE, Beating Egg Allergy Trial (BEAT) Study Group. A randomized trial of egg introduction from 4 months of age in infants at risk for egg allergy. J Allergy Clin Immunol. 2017 May;139(5):1621-1628.e8. [CrossRef]
- Nishimura T, Fukazawa M, Fukuoka K, Okasora T, Yamada S, Kyo S, Homan M, Miura T, Nomura Y, Tsuchida S, Yajima S, Aoki S, Nakamura Y, Hosaka T, Hidaka H, Yamamori H, Inoue A, Morimoto J. Early introduction of very small amounts of multiple foods to infants: A randomized trial. Allergol Int. 2022 Jul;71(3):345–53. [CrossRef]
- Kalb B, Meixner L, Trendelenburg V, Unterleider N, Dobbertin-Welsch J, Heller S, Dölle-Bierke S, Roll S, Lau S, Lee YA, Fauchère F, Braun J, Babina M, Altrichter S, Birkner T, Worm M, Beyer K. Tolerance induction through early feeding to prevent food allergy in infants with eczema (TEFFA): rationale, study design, and methods of a randomized controlled trial. Trials. 2022 Mar 12;23(1):210. [CrossRef]
- Du Toit G, Roberts G, Sayre PH, Bahnson HT, Radulovic S, Santos AF, Brough HA, Phippard D, Basting M, Feeney M, Turcanu V, Sever ML, Gomez Lorenzo M, Plaut M, Lack G, LEAP Study Team. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med. 2015 Feb 26;372(9):803–13. [CrossRef]
- Bellach J, Schwarz V, Ahrens B, Trendelenburg V, Aksünger Ö, Kalb B, Niggemann B, Keil T, Beyer K. Randomized placebo-controlled trial of hen’s egg consumption for primary prevention in infants. J Allergy Clin Immunol. 2017 May;139(5):1591-1599.e2. [CrossRef]
- Perkin MR, Logan K, Marrs T, Radulovic S, Craven J, Flohr C, Lack G, EAT Study Team. Enquiring About Tolerance (EAT) study: Feasibility of an early allergenic food introduction regimen. J Allergy Clin Immunol. 2016 May;137(5):1477-1486.e8. [CrossRef]
- Snijders BEP, Thijs C, van Ree R, van den Brandt PA. Age at first introduction of cow milk products and other food products in relation to infant atopic manifestations in the first 2 years of life: the KOALA Birth Cohort Study. Pediatrics. 2008 Jul;122(1):e115-122. [CrossRef]
Figure 1.
Increased protein uptake in allergic individuals. The IgE receptor CD23 is upregulated on the enterocytes surface of atopic subjects and the formation of the complex IgE/CD23 after allergens exposure allows for passage through the epithelial layer (phase 1). Once the allergens gets in contact with the subepithelial mast cells, the degranulation response is induced. The mediators released by the mast cells modify the cells junctional complex, increasing the paracellular space and increasing protein uptake (phase 2). Created with biorender.com/.
Figure 1.
Increased protein uptake in allergic individuals. The IgE receptor CD23 is upregulated on the enterocytes surface of atopic subjects and the formation of the complex IgE/CD23 after allergens exposure allows for passage through the epithelial layer (phase 1). Once the allergens gets in contact with the subepithelial mast cells, the degranulation response is induced. The mediators released by the mast cells modify the cells junctional complex, increasing the paracellular space and increasing protein uptake (phase 2). Created with biorender.com/.
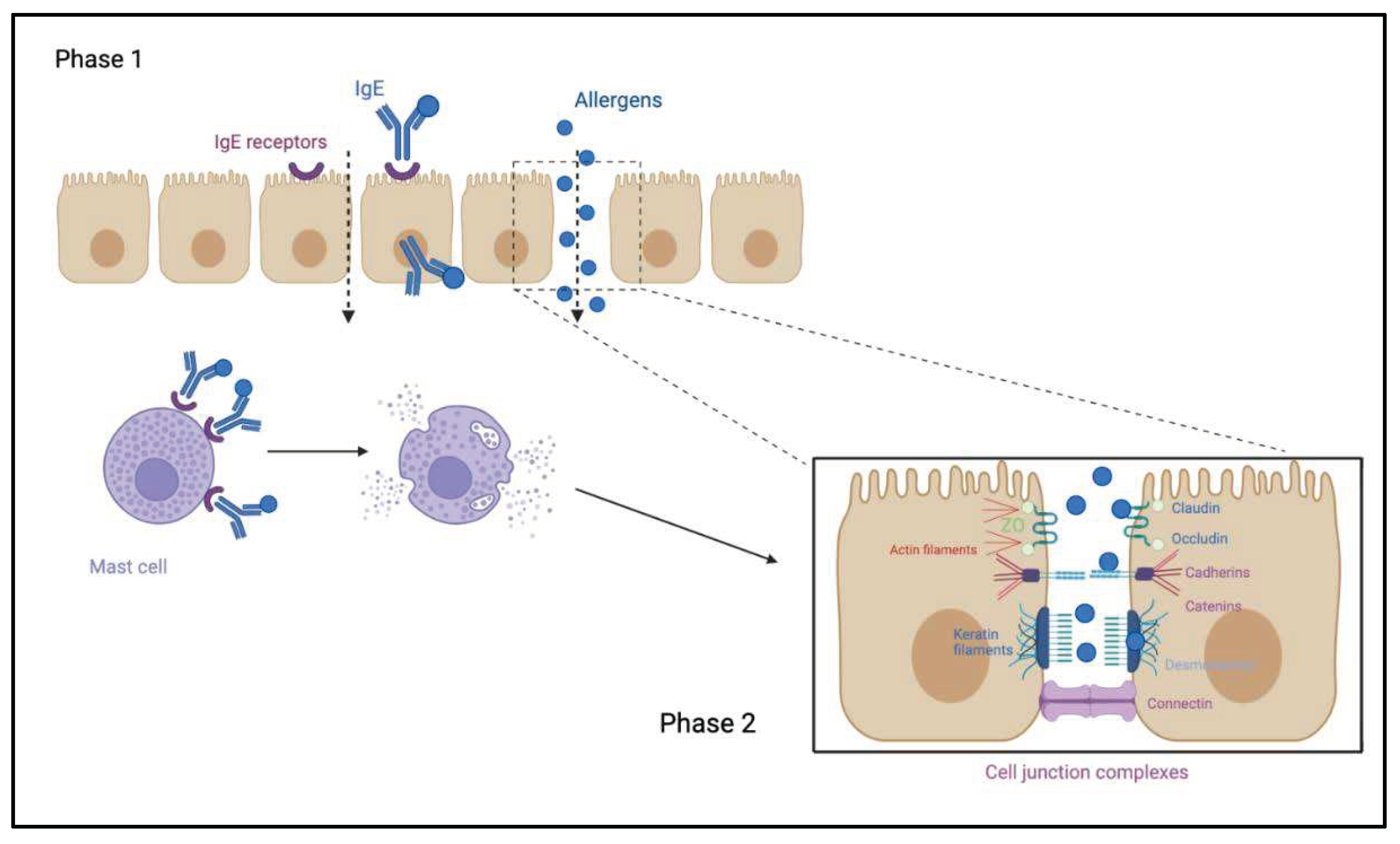
Figure 2.
Human intestinal lumen is colonized by different types of microorganisms, better known as gut microbiota. Dietary fibers fermentation by these microorganisms produces SCFA (acetate, butyrate, propionate), which bind specific G protein-coupled receptors (GPRs) on the IECs surfaces such as GPR43. Recent studies demonstrated the role of these receptors in regulating inflammation, GI functions, allergies development and other manifestations [43]. Created with biorender.com/.
Figure 2.
Human intestinal lumen is colonized by different types of microorganisms, better known as gut microbiota. Dietary fibers fermentation by these microorganisms produces SCFA (acetate, butyrate, propionate), which bind specific G protein-coupled receptors (GPRs) on the IECs surfaces such as GPR43. Recent studies demonstrated the role of these receptors in regulating inflammation, GI functions, allergies development and other manifestations [43]. Created with biorender.com/.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



