
Submitted:
17 January 2024
Posted:
17 January 2024
You are already at the latest version
Abstract
Light is an electromagnetic radiation that has visible and invisible wavelength spectrum. The visible light can only be detected by the eyes through the optic pathways. With the presence of scalp, cranium and meninges, the brain is seen as being protected from direct exposure to light. For that reason, the brain can be viewed as a black body lying inside a black box. In physics, a black body tends to be in thermal equilibrium with its environment and can tightly regulate its temperature via thermodynamics principles. Therefore, a healthy brain inside a black box should not get exposed to light. On the contrary, photobiomodulation, a form of light therapy to the brain has been shown to have beneficial effects for some neurological conditions. The proposed underlying mechanisms are multiple. Herein we present our intraoperative findings of rapid electrocorticographic brainwave changes when the brain was shone directly with different wavelengths of light during awake brain surgery. Our findings provide literature proof on light’s ability to influence human brain energy and function. Our proposed mechanism for these rapid changes is the presence of plasma-like energy inside the brain which causes fast brain activities that are akin to lightning strikes.
Keywords:
light
; photobiomodulation
; brainwaves
; thermodynamics
; quantum brain
; plasma
; black body
; awake brain surgery
; electrocorticography
1. Introduction
Light is the opposite of darkness, and it is meaningful to followers of many religions across the world such as the festival of light (Diwali) for Hindus, the candle festival for Buddhists, and as a symbol of God and the first creation (metaphorical light or Nur in Arabic) for the Abrahamic religions. In the academic arena, light is viewed as an electromagnetic force or energy or waves after the great Scottish mathematical physicist James Clerk Maxwell proved for the first time in history the unification of electric (with field) and magnetic (with vortex) force. Scientists view electromagnetic light with its highest speed at approximately 300 000 km/sec as fundamental to our health and life [1,2,3,4,5]. Our most important source of natural light is the sun. The sunlight or white light is in fact composed of visible and invisible light frequency spectrum. The visible light (can be processed by our visual system) has wavelengths from about 380 nanometers (violet) to about 780 nanometers (near infrared). In term of frequency, this corresponds to a band in the vicinity of 400 (near infrared) to 790 (violet) terahertz. This visible band has seven main spectral colors: red, orange, yellow, green, cyan, blue, and violet. With reference to the brain, light can only pass through the eyes to enter the brain. Layers of scalp, cranial bone and meninges form a protective barrier from light. Therefore, one may view the brain as lying inside a black box and behaving as a black body (Figure 1). In sum, it seems like the healthy brain should not be exposed directly to external light. Herein we present some interesting brainwave findings during awake cranial surgery when the brain was shone directly with various wavelengths of light. Our findings may provide strong evidence to further study the details of using light as mode of therapy for neurological disorders in human.
2. Case report: findings during awake brain surgery on marked and rapid brainwave changes when the brain was directly exposed to different wavelengths of light
A 32-year-old man was diagnosed with right insular glioma and underwent awake brain surgery. During surgery, the neurosurgeon used an 8x4 electrocorticographic (ECoG) grid electrode which was laid directly onto the ipsilateral frontal lobe to detect early seizure brainwaves and to assess the state of consciousness of the patient. Surgery was initially started at the right temporal lobe with removal of the tumor until the right hippocampus was exposed (Figure 2). No fluorescent agents were used for the surgery.
At one point during the surgery, the neurosurgeon stopped the tumour debulking and changed the Zeiss OPMI Pentero microscope lighting from switching off the light (the whole operative room was also in darkness with obvious parameters readings only noted on anesthetic machines) to switching on the white (xenon at 30% intensity), blue (at 400 nm wavelength), and finally the near infrared laser light (at 780 nm wavelength for autofocus). The final part consisted of superimposing the laser red light hitting the exposed hippocampus with the background of blue light. The purposes were to assess any peculiar features of tumor area when viewed under these different lights and to note any peculiar features of brainwaves when the brain was shone with these lights. Each phase lasted for a few minutes and was marked on the ECoG screen machine (Figures 3, 4A,A1). These were done in a successive manner without brain or grid disturbance. The brainwave morphological features under these four brain conditions were depicted in Figure 4B–E.
In referring to Figure 4B–E, one should notice the presence of gross morphological differences in terms of brainwave log-power when the brain gets exposed to different lights (pay particular attention to the y-axis power lines of 0.01-red line; 1-black-dashed line and 100-black line uV2/Hz when comparing them). Firstly, the brainwave log-power had different morphology under presence of light as compared to in the darkness or in a black box (B versus C) (note: the brain in a cranium is an analogy to the brain in a black box). Secondly, the brainwave log-power morphology for the brain when directly exposed to blue light (400 nm wavelength) (D) and near infrared light (780 nm wavelength i.e. blue superimposed with laser near infrared light) (E) were different when compared to when it was in a black box (B). Finally, brainwaves of the brain which were exposed to blue light had a contradictory feature when compared to near infrared light exposure (D versus E). The brainwave log-power shifted to lower log-power when exposed to blue light (with its mean power around 1 uV/Hz or a black-dashed line). On the other hand, the brainwave log-power shifted towards higher log-power when the brain was exposed to near infrared light (with its mean log-power lies in between 1 and 100 uV/Hz or in between a black-dashed line and a black line). These differences were obviously noted when compared them to the off-light brainwave log-power-morphology (D and E versus B).
Further detailed analyses were made for the obtained brainwaves. The frequency graph analysis is represented in Figure 5A with brainwave frequency (x-axis) versus brainwave power in uV2/Hz. The 11 to 13 electrodes were analyzed for a frequency spectrum when different lights were shone directly to the exposed brain (Figure 5B–E). As noted in morphological analysis, the brainwave frequency spectrum for the light-exposed brain is also different from an inside black box brain (off the light) (C versus B). There were more alpha (green) and beta (blue) waves present when the brain was exposed to light as compared to off the light. An increment in alpha and beta waves were not only present when the brain was directly exposed to xenon-white light, but also to blue and near infrared lights (D and E versus B). Interestingly, theta (yellow) brainwaves were noted to be markedly reduced when the brain was exposed to any light and delta (red) brainwaves were either reduced (C) or increased (D and E) when exposed to light. In other words, brain which was exposed to either blue or near infrared light tends to have more delta, alpha and beta waves. Another interesting difference between blue and near infrared light direct exposure onto the brain was the emergence of gamma waves when near infrared light was shone to the brain (specifically to the hippocampus) as shown in Figure 6.
3. Discussion
The brain is seen as being protected from the light. The scalp, skull and meningeal layers form barriers for the sun or artificial light from shining on or entering the brain. Therefore, the brain is seen as a black body inside the cranium. The only way for light to enter the brain is through the two eyes. Light that enters the eyes will then be processed further at various anatomical levels: optic nerves, chiasm, tracts, radiations, primary visual area Brodmann 17, secondary visual areas Brodmann 18 and 19, and to other association areas of the brain. Another way light can significantly enter the cranium is when the neurosurgeon performs a craniotomy or decompressive craniectomy (DC or removal of large area of cranial bone) for severely injured brain to relieve raised intracranial pressure. Despite the potential benefit of DC, data from studies demonstrated high incidences of neuropsychological impairments in the long-term follow-up of these DC patients [6,7]. The explanations given for these impairments are reduction in cerebral perfusion, alteration in cerebrospinal fluid (CSF) dynamics and atmospheric-gravity force pressing the microgravity-brain environment [8,9]. Another possible reason is that light could penetrate the scalp relatively easier in DC patients. Exposure to bright sun or artificial light is known to trigger migraine headaches as reported in literature [10,11]. On another note, direct light exposure to the brain has also been reported as having beneficial effects. A study done by Naeser et al. (2014) showed significant improvements in cognitive performances in patients with mild head injury [12]. Lately a significant amount of review articles on photobiomodulation (PBM) have similarly pointed out the benefits on neurodegenerative animal models and cellular studies. The hypothetical mechanisms of PBM offered in their articles are related to the extra synthesis of ATP by mitochondria, diffusion of nitric oxide promoting vasodilation, increase in regional cerebral blood flow in cortical areas, increase in antioxidants, augmentation of brain glymphatic drainage system, and decrease in inflammation [13,14,15,16]. With these notes, our clinical findings, which showed significant alteration in brainwave power and frequency when the brain was exposed directly to various lights concur with the aforementioned positive and negative effects of light onto the brain. The right dose of light intensity (luminosity or fluence), type of light, duration, approach or method for light delivery, and area of the brain receiving the light are some possible factors that determine the effectiveness and complication of the therapy. Since there are no concrete explanations that can be offered to explain the mechanisms of action for PBM, in this article we would like to discuss this in accordance with the physics perspective on possible underlying mechanisms for the ‘fast changes’ in brainwaves when four consecutive light conditions were made during awake brain surgery.
Physics perspective on direct light energy onto the brain
From our earlier discussion, a significant amount of light energy enters the brain via only the eyes. The black box analogy of the cranium disfavors the brain from receiving a significant amount of light. Attenuation of light energy occurs when it passes through layers of the cranium. Therefore, the light resistance property of the cranium may offer a protective mechanism in ensuring optimal brain function. Light is a type of electromagnetic energy that can generate heat energy and exists in duality, it can either be regarded as photons (particles of light) or waves [17]. Certainly, heat generation in the brain is related to its metabolism and information processing [18], and with additional exposure to extra cranial heat energy (light), brain temperature can be altered. Hence, intricate brain temperature regulation is seen as vital for processing information. Temperature regulation of the brain is a dynamic process and thought to follow the thermodynamics principles of energy conservation and flow of energy. Energy conservation is in fact the first law of thermodynamics, which states that energy cannot be created or destroyed, it can only change forms or be transferred from one object to another (quantity of energy). Important to note here that, none of the energy transferring processes are efficient, instead, in each process some of the transferred energy turns into heat. Inside the cranium, heat energy or temperature could possibly be regulated by heat conduction (via blood flow and CSF), convection (via air sinuses and CSF), evaporation (CSF and air sinuses), and radiation (cranial black box). Pertaining to flow of energy or the second law of thermodynamics (quality or directionality of energy) which states that the entropy of any system always increases. Entropy is defined as a measure of thermal energy per unit temperature that is unavailable for doing useful work or entropy is a measurement of disorder or energy spread. Low entropy system has a concentrated energy state, whilst high entropy system has spread-out energy state. It seems fitting with research findings that the deep brain nuclei and brainstem have warmer temperatures than the cortices [19,20,21]. It tells us directionality or gradient of energy flow from low entropy area such as the brainstem (concentrated energy) to high entropy area such as the cortex (spread-out energy). In summary, our arguments which cover two salient points: the cranium as a black box which avoids direct light exposure, and brain thermal homeostasis with thermodynamics principles that regulates brain temperature intricately makes physics as an aspect to consider deeply when discussing brain functions.
Pertaining to ‘rapid brainwave changes’ when different light was shone onto the brain, the physics perspective on this matter is likely related to production of brain plasma. The term ‘plasma’ was first proposed by the American Nobel laureate chemist and physicist Irving Langmuir, who viewed it as similar to blood plasma. Here, ‘plasma’ refers to the electrified fluid that carries electrons and charged ions (compared to how blood plasma carries the corpuscles or cells). In physics, plasma by definition must contain assembly of mobile charge carriers of a sufficient density. If the charged density is not sufficiently high, their interaction with the electromagnetic field becomes important and the charged component can also be considered as plasma [22]. In principle, plasma is commonly divided into ultra-hot (a thermonuclear reaction plasma such as in the sun), hot or thermal plasma, cold plasma (non-thermal or non-equilibrium plasma which can be generated at room temperature), and ultra-cold plasma. The term for hot or cold plasma is sometimes referred to as being hot if it is nearly fully ionized or cold if only a small fraction of it is ionized. In this context, presence of light inside the cranial black box may have produced or enhanced brain plasma energy which caused fast alteration in brainwaves. To comprehend this notion, let us have a look at the brain extracellular compartment (ECC). As we are aware, the brain interstitial or ECC does have charged ions (such as Na+, Cl-, H+, Ca2+, K+, Mg2+), charged molecules or polyatomic ions (HCO3-, hyaluronic acid, NAD+, acetate, nitrate, nitrite, sulfate, phosphate, aspartate, glutamate, lysine, arginine, etc.), polar solvents (charged water), gaseous ions (abundant presence of CO2 is easily converted to gaseous ions when electricity or electron movement is applied to them), and electrons (electricity)[23,24,25,26,27]. The interaction of this brain plasma soup with brainwaves (electricity or electron or electromagnetic force) and charged water may result in the formation of magnetohydrodynamics (MHD) or magnetofluid (superfluid) [28,29]. In short, in a slice of alive brain tissue with thousands of neurons, glial cells and interstitial spaces with charged plasma soup, a possible presence of large amount of toroidal electromagnetic waves and poloidal plasma waves may form a more diffuse and widespread rapid energy flow (MHD and perpendicular magnetoacoustics waves) from core to periphery of the brain (Figure 7). Therefore, a first reason to support this perspective (brain also has plasma energy) is a black box feature of the cranium which blocks the light from reaching directly onto the brain and produces additional plasma energy. This idea is further supported by a recent study done by Maccaferri et al. which demonstrated nanoplasmons formation when the light interacts with electrons (electricity) [30]. Our second reason is related to the presence of cortical surface electrons. In 2017, Kiyotaka et al. did a 7-Tesla MRI study of brain cortical surfaces. The unexpected finding was an electron rich layer at glia limitans externa adjacent to CSF cortical cisternal space. Their explanation for the presence of surface electrons adjacent to CSF space was that astrocytes endfeet containing abundant aquaporin-4 (AQP-4) induces glia limitans externa polarization and hence electrons [31]. According to our physics perspective, an interaction between poloidal plasma waves at the cortical surface with water (CSF) may also form abundant electrons as confirmed by physics experiment of which electrons were formed when the plasma interacts with water [28]. Besides, some recent experiments have also shown possible presence of plasma-like energy inside the brain which supports our brain plasma hypothesis and provides explanation for the rapid changes in brainwaves when the light was shone directly to the brain. In 2022, Yidi Zhang et al. have noted two types of wave in the brain, front waves of chemical reactions and travelling waves of neural activity [32]. In 2009 and 2021, Andersen et al. and Drukarch et al. have highlighted the thermodynamics concept for action potential propagation [33,34]. Finally, could the rapid changes in brainwaves when light shone onto the brain be due to the fundamental brain itself? Indeed, the anatomical brain can also be viewed as waves of energy (i.e. duality of a particle: either particle or waves) as highlighted by us on a new perspective to comprehend brain function of which viewing the anatomical brain as package of energy or Quantum brain, rather than particles or an anatomical object (Newtonian brain) [35,36,37].
Photobiomodulation (PBM) and medical application
With our intraoperative findings on the human brain and other clinical-nonclinical findings which showed positive light effect on neurological diseases, further research in this field is highly recommended. It can be a breakthrough in clinical neurosciences whereby light could play a role in the treatment of various neurological diseases. Matters that need to be considered with regards to PBM therapy are the following: 1) area of the brain receiving light therapy – focus onto deep nucleus/small areas or more diffuse onto a large area of the brain such as the prefrontal or orbitofrontal lobe; 2) type of light and its wavelength - such as visible light, ultraviolet light, or infrared light. Concerning infrared light, it was used in depression and was shown to have a promising effect [38]. This clinical finding concurs with our finding in which near infrared light does have higher energy power and gamma waves than others. Thus, (near) infrared light might possibly be used in therapy for depression, blue light for psychosis, and a combination of blue (intensive care stage where electrical seizures may still be present) and infrared (later, in the ward stage when brain energy is low) light for severely head injured patient; 3) light source – coherent or non-coherent light; 4) approaches for light delivery – transcranial, direct onto the brain, or intranasal; 5) fluence or energy density which is calculated by multiplying irradiance (W/cm2) by time (sec), which is defined as the amount of energy per unit of area (J/cm2). Transcranial PBM studies in human have fluences ranging from 10-30 J/cm2 [13,39]; 6) operation mode – continuous wave (CW) or pulsed wave (PW) mode. PW mode has demonstrated significant benefits and better biostimulatory effects than the CW mode [40]; finally; 7) treatment duration and repetition.
4. Conclusions
Light has limited access to the brain. Eyes are the only pathway for extracranial light to enter the brain and thus the intracranial space is regarded as a black box. Therefore, the brain is prevented from receiving the light directly and can be regarded as a black body which is in thermodynamic equilibrium with its environment. Nonetheless, based on our and other scientific findings, shining direct light onto the brain may form a definitive therapy for some neurological and neuropsychiatric disorders in view of its capability to alter brainwaves.
Author Contributions
ZI contributed conception, main content, and design of the manuscript; ZI, ASY, DNF and MHH did the surgery; ZZ, MII, ARIG, JMA and NS read and contributed critical opinions.
Funding
This research received no grant.
Institutional Review Board Statement
Not required because it is a case report of a routine surgical procedure with significant findings related to brainwaves and available light in the standard neurosurgical microscope.
Informed Consent Statement
Informed consent was obtained for the surgery and application of various standard light available in neurosurgical microscope.
Data Availability Statement
The detailed presented data are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Wyse, C. A. , Selman, C., Page, M. M., Coogan, A. N., & Hazlerigg, D. G. (2011). Circadian desynchrony and metabolic dysfunction; did light pollution make us fat?. Medical hypotheses, 77(6), 1139–1144. [CrossRef]
- Yu, B. , & Wang, C. Y. (2022). Osteoporosis and periodontal diseases - An update on their association and mechanistic links. Periodontology 2000, 89(1), 99–113. [CrossRef]
- Schulz, P., & Steimer, T. (2009). Neurobiology of circadian systems. CNS drugs, 23 Suppl 2, 3–13. [CrossRef]
- Walker, W. H. 2nd., Walton, J. C., DeVries, A. C., & Nelson, R. J. (2020). Circadian rhythm disruption and mental health. Translational psychiatry, 10(1), 28. [CrossRef]
- Wirz-Justice, A., Skene, D. J., & Münch, M. (2021). The relevance of daylight for humans. Biochemical pharmacology, 191, 114304. [CrossRef] [PubMed]
- Ballestero, M. F. M. , Furlanetti, L. L., Augusto, L. P., Chaves, P. H. C., Santos, M. V., & de Oliveira, R. S. (2019). Decompressive craniectomy for severe traumatic brain injury in children: analysis of long-term neuropsychological impairment and review of the literature. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery, 35(9), 1507–1515. [CrossRef]
- Yang, X. F. , Wen, L., Shen, F., Li, G., Lou, R., Liu, W. G., et al. (2008). Surgical complications secondary to decompressive craniectomy in patients with a head injury: a series of 108 consecutive cases. Acta neurochirurgica, 150(12), 1241–1248. [CrossRef]
- Woo, P. Y. M. , Mak, C. H. K., Mak, H. K. F., & Tsang, A. C. O. (2020). Neurocognitive recovery and global cerebral perfusion improvement after cranioplasty in chronic sinking skin flap syndrome of 18 years: Case report using arterial spin labelling magnetic resonance perfusion imaging. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia, 77, 213–217. [CrossRef]
- Idris, Z. , Mustapha, M., & Abdullah, J. M. (2014). Microgravity environment and compensatory: Decompensatory phases for intracranial hypertension form new perspectives to explain mechanism underlying communicating hydrocephalus and its related disorders. Asian journal of neurosurgery, 9(1), 7–13. [CrossRef]
- Tekatas, A. , & Mungen, B. (2013). Migraine headache triggered specifically by sunlight: report of 16 cases. European neurology, 70(5-6), 263–266. [CrossRef]
- Lema, A.K. , & Anbesu, E.W. (2022). Computer vision syndrome and its determinants: A systematic review and meta-analysis. SAGE Open Med, 10:20503121221142402. [CrossRef] [PubMed] [PubMed Central]
- Naeser, M. A. , Zafonte, R., Krengel, M. H., Martin, P. I., Frazier, J., Hamblin, M. R., et al. (2014). Significant improvements in cognitive performance post-transcranial, red/near-infrared light-emitting diode treatments in chronic, mild traumatic brain injury: open-protocol study. Journal of neurotrauma, 31(11), 1008–1017. [CrossRef]
- Salehpour, F. , Mahmoudi, J., Kamari, F., Sadigh-Eteghad, S., Rasta, S. H., & Hamblin, M. R. (2018). Brain Photobiomodulation Therapy: a Narrative Review. Mol Neurobiol, 55(8):6601-6636. [CrossRef] [PubMed] [PubMed Central]
- Salehpour, F. , Gholipour-Khalili, S., Farajdokht, F., Kamari, F., Walski, T., Hamblin, M.R., et al. (2020). Therapeutic potential of intranasal photobiomodulation therapy for neurological and neuropsychiatric disorders: a narrative review. Rev Neurosci, 31(3):269-286. [CrossRef] [PubMed] [PubMed Central]
- Abijo, A., Lee, C. Y., Huang, C. Y., Ho, P. C., & Tsai, K. J. (2023). The Beneficial Role of Photobiomodulation in Neurodegenerative Diseases. Biomedicines, 11(7), 1828. [CrossRef]
- Semyachkina-Glushkovskaya, O. , Abdurashitov, A., Klimova, M., Dubrovsky, A., Shirokov, A., Fomin, A., et al. (2020). Photostimulation of cerebral and peripheral lymphatic functions. Translational Biophotonics, 2(1-2), p.e201900036. [CrossRef]
- Rab, A. S. , Polino, E., Man, Z. X., Ba An, N., Xia, Y. J., Spagnolo, N., et al. (2017). Entanglement of photons in their dual wave-particle nature. Nature communications, 8(1), 915. [CrossRef]
- Collell, G. , & Fauquet, J. (2015). Brain activity and cognition: a connection from thermodynamics and information theory. Frontiers in psychology, 6, 818. [CrossRef]
- Hayward, J. N., & Baker, M. A. (1969). A comparative study of the role of the cerebral arterial blood in the regulation of brain temperature in five mammals. Brain research, 16(2), 417–440. [CrossRef]
- Wang, H. , Wang, B., Normoyle, K. P., Jackson, K., Spitler, K., Sharrock, M. F., et al. (2014). Brain temperature, and its fundamental properties: a review for clinical neuroscientists. Front Neurosci, 8:307. [CrossRef] [PubMed] [PubMed Central]
- Idris, Z. , Yee, A. S., Wan Hassan, W. M. N., Hassan, M. H., Ab Mukmin, L., Mohamed Zain, K.A., et al. (2023). Clinical outcomes and thermodynamics aspect of direct brain cooling in severe head injury. Surg Neurol Int,14:158. [CrossRef] [PubMed] [PubMed Central]
- Józef, R. Z. (2005). Physical Plasma Switchability in the Brain, Electromagnetic Biology and Medicine, 24:3, 273-281. [CrossRef]
- Nakada, T. (2009). Neuroscience of water molecules: a salute to Professor Linus Carl Pauling. Cytotechnology 59, 145–152.
- Nicholson, C. , & Hrabětová, S. (2017). Brain Extracellular Space: The Final Frontier of Neuroscience. Biophysical journal, 113(10), 2133–2142. [CrossRef]
- Lei, Y. , Han, H., Yuan, F., Javeed, A., & Zhao, Y. (2017). The brain interstitial system: Anatomy, modeling, in vivo measurement, and applications. Progress in neurobiology, 157, 230–246. [CrossRef]
- Purushotham, S. S. , & Buskila, Y. (2023). Astrocytic modulation of neuronal signalling. Frontiers in network physiology, 3, 1205544. [CrossRef] [PubMed]
- James, E. , Jake, B., Frederik, L., Vindy, T., Ian, H., Emily, H., et al. (2023). Illuminating the brain: Revealing brain biochemistry with synchrotron X-ray spectromicroscopy. Journal of Electron Spectroscopy and Related Phenomena, 266, 147355. [CrossRef]
- Bruggeman, P.J. , Kushner, M. J., Locke, B. R., Gardeniers J. G. E., Graham, W. G., Graves, D. B., et al. (2016). Plasma–liquid interactions: a review and roadmap. Plasma Sources Sci. Technol, 25, 053002. DOI 10.1088/0963-0252/25/5/053002.
- Peng, Y. , Alsagri, A. S., Afrand, M., & Moradi, R. (2019). A numerical simulation for magnetohydrodynamic nanofluid flow and heat transfer in rotating horizontal annulus with thermal radiation. RSC advances, 9(39), 22185–22197. [CrossRef] [PubMed]
- Maccaferri, N. , Zubritskaya, I., Razdolski, I., Chioar, I-A., Belotelov, V., Kapaklis, V., et al. (2020). Nanoscale magnetophotonics. J Appl Phys, 127(8):1– 30. [CrossRef]
- Suzuki, K. , Yamada, K., Nakada, K., Suzuki, Y., Watanabe, M., Kwee, I. L., et al. (2017). MRI characteristics of the glia limitans externa: A 7T study. Magnetic resonance imaging, 44, 140–145. [CrossRef]
- Zhang, Y. , Guo, S., Sun, M., Mariniello, L., Tozzi, A., & Zhao, X. (2022). Front Waves of Chemical Reactions and Travelling Waves of Neural Activity. Journal of NeuroPhilosophy, 1(2). [CrossRef]
- Andersen, S. S. , Jackson, A. D., & Heimburg, T. (2009). Towards a thermodynamic theory of nerve pulse propagation. Progress in neurobiology, 88(2), 104–113. [CrossRef] [PubMed]
- Drukarch, B. , Wilhelmus, M. M. M., & Shrivastava, S. (2021). The thermodynamic theory of action potential propagation: a sound basis for unification of the physics of nerve impulses. Reviews in the neurosciences, 33(3), 285–302. [CrossRef]
- Idris, Z. , Zakaria, Z., Yee, A. S., Fitzrol, D. N., Ghani, A. R. I., Abdullah J. M., et al. (2021). Quantum and Electromagnetic Fields in Our Universe and Brain: A New Perspective to Comprehend Brain Function. Brain Sci,11(5):558. [CrossRef] [PubMed] [PubMed Central]
- Idris, Z. (2020). Quantum Physics Perspective on Electromagnetic and Quantum Fields Inside the Brain. The Malaysian journal of medical sciences:MJMS, 27(1), 1–5. [CrossRef]
- Idris, Z. , Yee, A. S., Wan Hassan, W. M. N., Hassan, M. H., Mohd Zain, K. A., & Abdul Manaf, A. (2022). A Clinical Test for a Newly Developed Direct Brain Cooling System for the Injured Brain and Pattern of Cortical Brainwaves in Cooling, Noncooling, and Dead Brain. Therapeutic hypothermia and temperature management, 12(2), 103–114. [CrossRef]
- Schiffer, F. , Johnston, A. L., Ravichandran, C., Polcari, A., Teicher, M. H., Webb, R. H., et al. (2009). Psychological benefits 2 and 4 weeks after a single treatment with near infrared light to the forehead: a pilot study of 10 patients with major depression and anxiety. Behavioral and brain functions : BBF, 5, 46. [CrossRef]
- Hamblin, M. R. (2016). Shining light on the head: Photobiomodulation for brain disorders. BBA clinical, 6, 113–124. [CrossRef]
- Peoples, C. , Spana, S., Ashkan, K., Benabid, A. L., Stone, J., Baker, G. E., et al. (2012). Photobiomodulation enhances nigral dopaminergic cell survival in a chronic MPTP mouse model of Parkinson's disease. Parkinsonism & related disorders, 18(5), 469–476. [CrossRef]
Figure 1.
Light and brain. (A) Electromagnetic spectrum for the light. (B and C) A healthy brain receives light through the eyes and lies inside a black box, thus behaving like a black body with thermodynamic equilibrium and having properties that are able to tightly regulate its temperature.
Figure 1.
Light and brain. (A) Electromagnetic spectrum for the light. (B and C) A healthy brain receives light through the eyes and lies inside a black box, thus behaving like a black body with thermodynamic equilibrium and having properties that are able to tightly regulate its temperature.
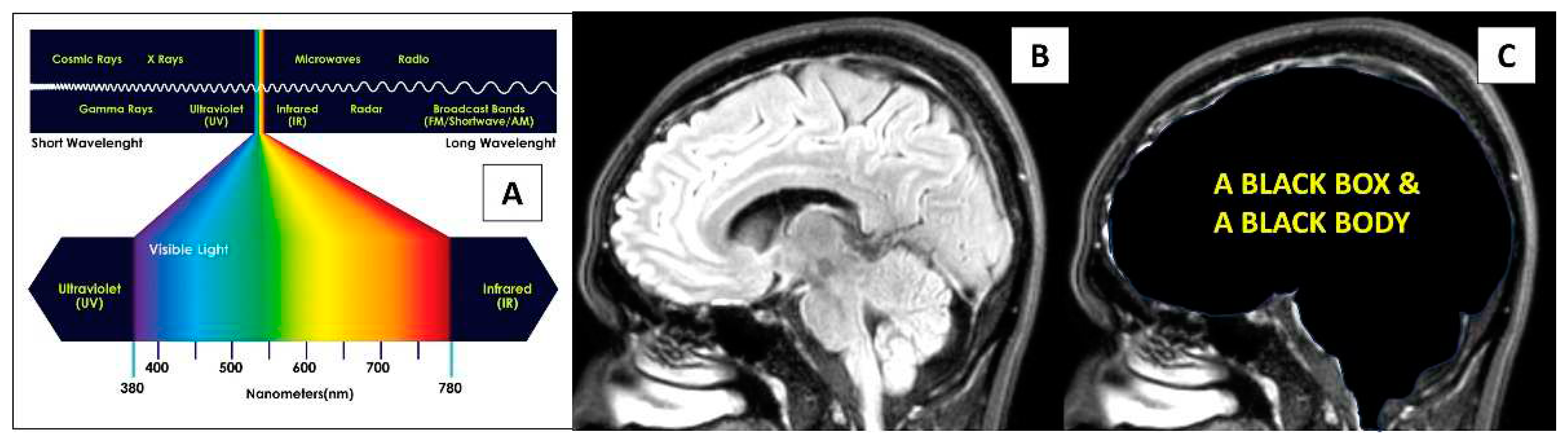
Figure 2.
The awake operative procedure for a right insular glioma surgery. (A) MRI T1-coronal view depicts right insular glioma which spreads to ipsilateral basal ganglia, midline basal forebrain nuclei and temporal lobe. (B) Use of a microscope with xenon white, blue and near infrared coherent laser light for autofocus. (C) A navigation system that helped in removing the tumor. (D, E and F) An 8x4 grid with 32 electrodes was placed over the right frontal lobe and the surgery was first started at the temporal lobe which gradually exposed the hippocampus (black star in E and F). The two MRI images in F are the post-surgery images that show near total removal of the tumor, and the white dashed line in D and E marks a Sylvian area which divides frontal from the temporal lobe.
Figure 2.
The awake operative procedure for a right insular glioma surgery. (A) MRI T1-coronal view depicts right insular glioma which spreads to ipsilateral basal ganglia, midline basal forebrain nuclei and temporal lobe. (B) Use of a microscope with xenon white, blue and near infrared coherent laser light for autofocus. (C) A navigation system that helped in removing the tumor. (D, E and F) An 8x4 grid with 32 electrodes was placed over the right frontal lobe and the surgery was first started at the temporal lobe which gradually exposed the hippocampus (black star in E and F). The two MRI images in F are the post-surgery images that show near total removal of the tumor, and the white dashed line in D and E marks a Sylvian area which divides frontal from the temporal lobe.
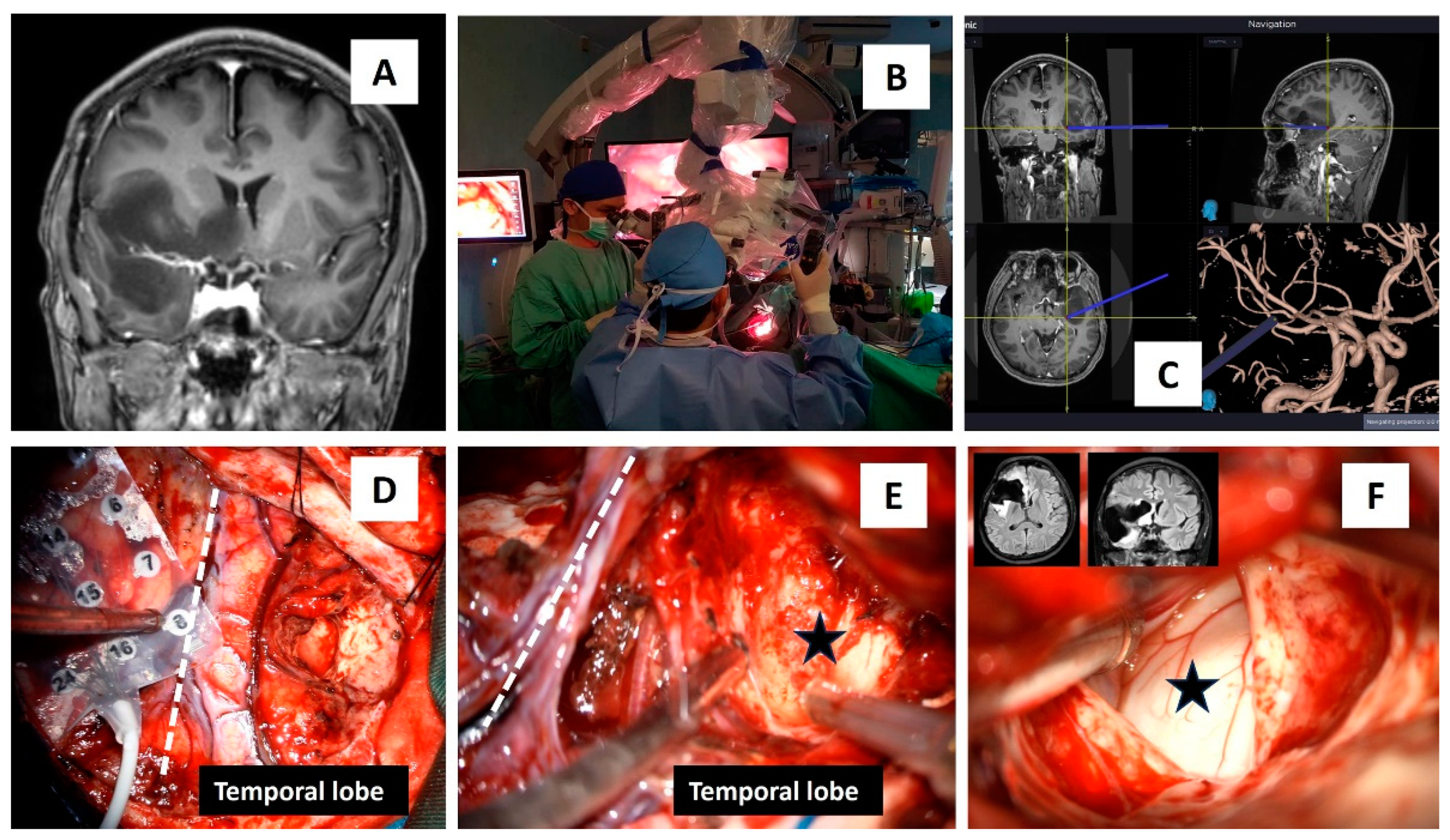
Figure 3.
Shining the brain with four different lights. (A) Off the light. (B) On the white light. (C) On the blue light. (D) The blue light was superimposed with near infrared autofocus laser light. D1 and D2 show additional intraoperative images of which the infrared laser light was shone onto the right hippocampus.
Figure 3.
Shining the brain with four different lights. (A) Off the light. (B) On the white light. (C) On the blue light. (D) The blue light was superimposed with near infrared autofocus laser light. D1 and D2 show additional intraoperative images of which the infrared laser light was shone onto the right hippocampus.
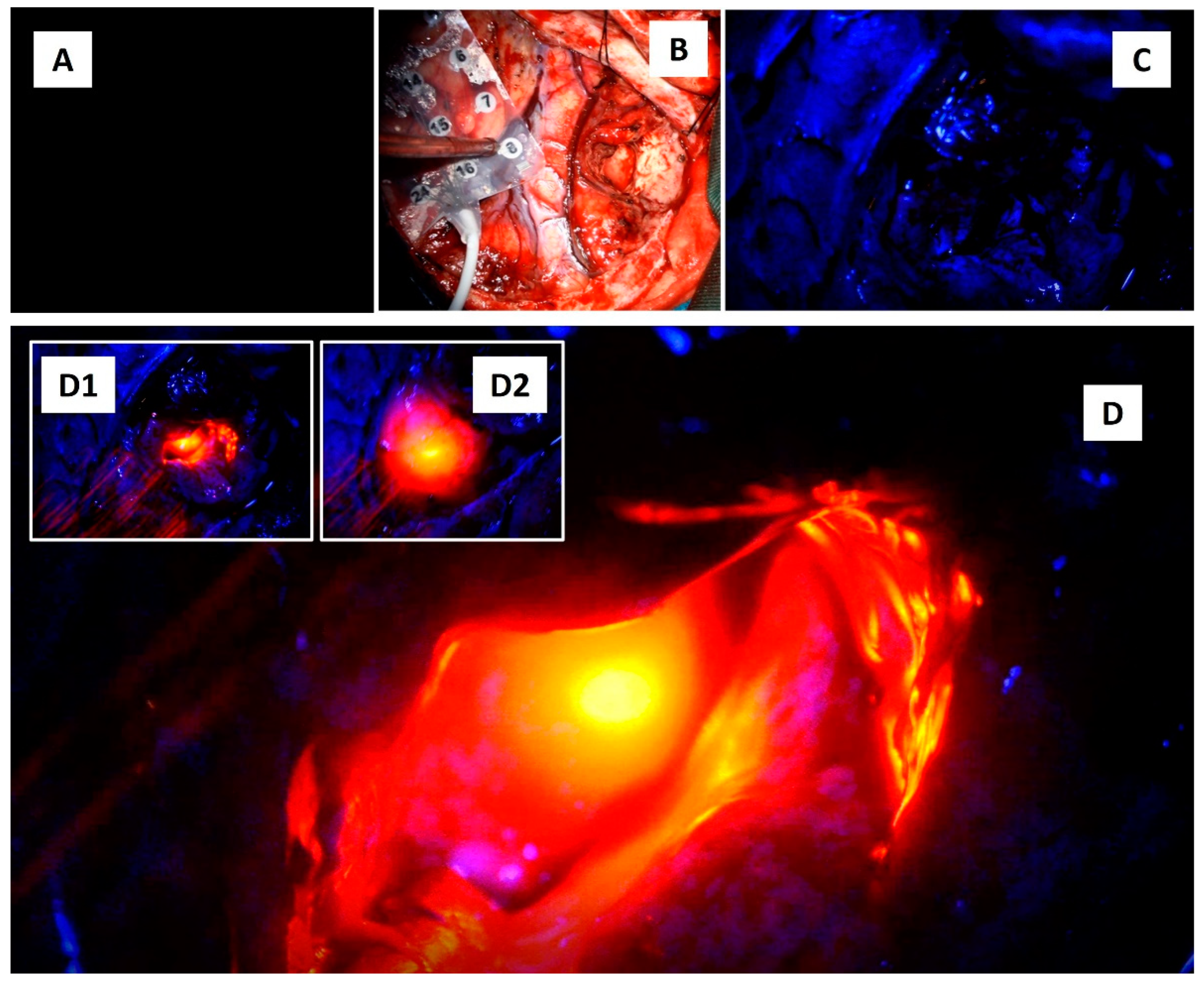
Figure 4.
Light and brainwaves. (A) The brainwaves obtained via an 8x4 grid electrodes during the procedure. Electrodes 10-12, 18,19, and 26-28 were selected for brainwave log-power analysis. The off-light (A1) brainwaves were marked on the screen and were analyzed later for the log-power morphology and frequency pattern (B). Similar analysis was also completed for xenon white light (on-light) (C), blue light (D) and blue light with superimposed near infrared light (E). For B to E graphs: the x-axis represents the brainwave frequency (0 to maximum of 35 Hz) whilst the y-axis represents the log-power of the waves (log values for the amplitude in voltage with power of 2 divided with frequency or uV2/Hz).
Figure 4.
Light and brainwaves. (A) The brainwaves obtained via an 8x4 grid electrodes during the procedure. Electrodes 10-12, 18,19, and 26-28 were selected for brainwave log-power analysis. The off-light (A1) brainwaves were marked on the screen and were analyzed later for the log-power morphology and frequency pattern (B). Similar analysis was also completed for xenon white light (on-light) (C), blue light (D) and blue light with superimposed near infrared light (E). For B to E graphs: the x-axis represents the brainwave frequency (0 to maximum of 35 Hz) whilst the y-axis represents the log-power of the waves (log values for the amplitude in voltage with power of 2 divided with frequency or uV2/Hz).
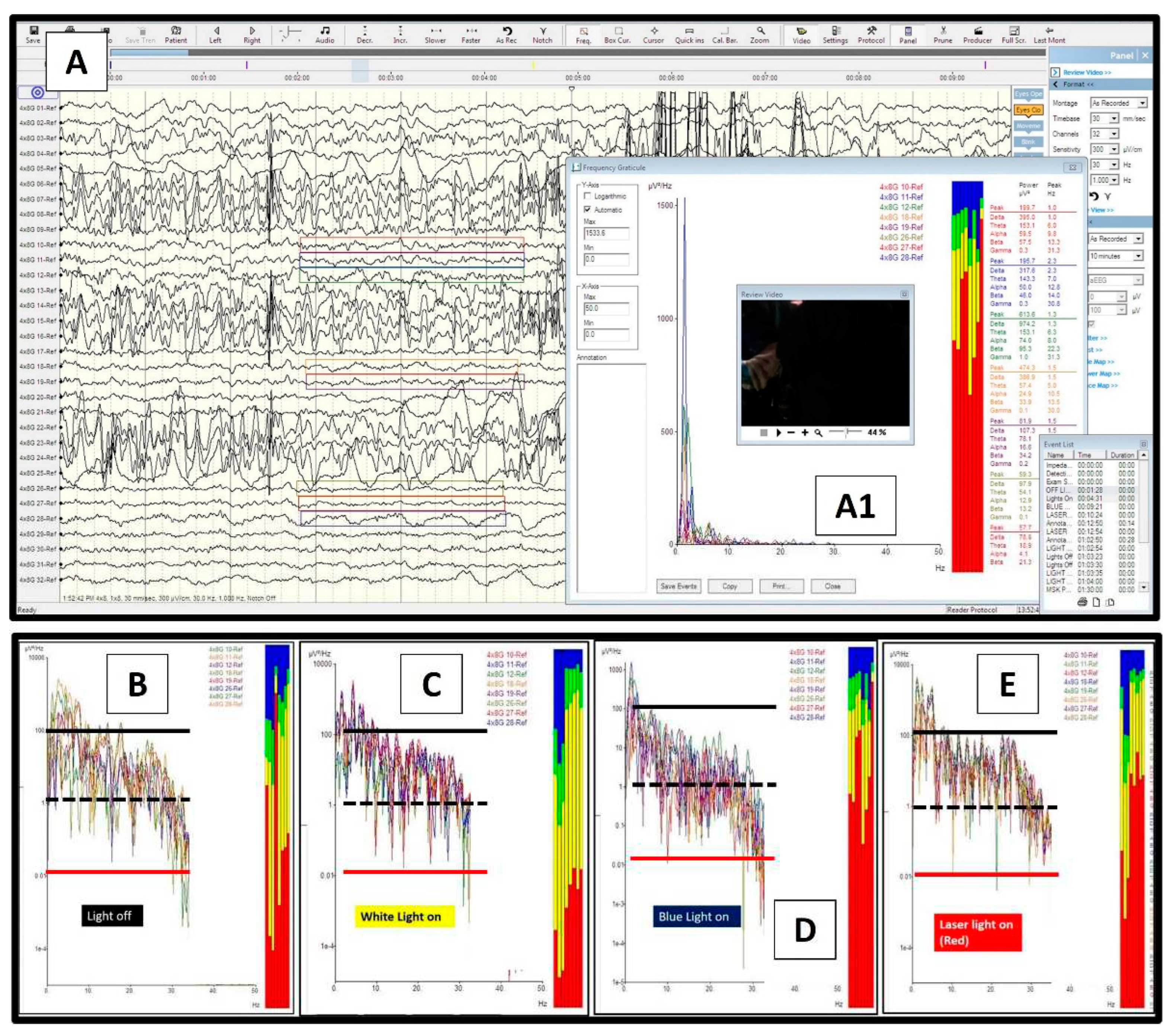
Figure 5.
Brainwave frequency analysis. (A) A consecutive series of different light exposures onto the exposed brain with brainwaves recorded at electrodes 11 to 13. (B, C, D and E) Four different columns represent brainwave spectra and different light exposures directly onto the brain (B for off light, C for white light, D for blue light, and E for near infrared light). Take note that the laser infrared was directed towards the exposed hippocampus, and for the brainwave spectra: red for delta waves [0.5-4 Hz], yellow for theta waves [4-8 Hz], green for alpha waves [8-12 Hz], and blue for beta waves [12-30 Hz].
Figure 5.
Brainwave frequency analysis. (A) A consecutive series of different light exposures onto the exposed brain with brainwaves recorded at electrodes 11 to 13. (B, C, D and E) Four different columns represent brainwave spectra and different light exposures directly onto the brain (B for off light, C for white light, D for blue light, and E for near infrared light). Take note that the laser infrared was directed towards the exposed hippocampus, and for the brainwave spectra: red for delta waves [0.5-4 Hz], yellow for theta waves [4-8 Hz], green for alpha waves [8-12 Hz], and blue for beta waves [12-30 Hz].
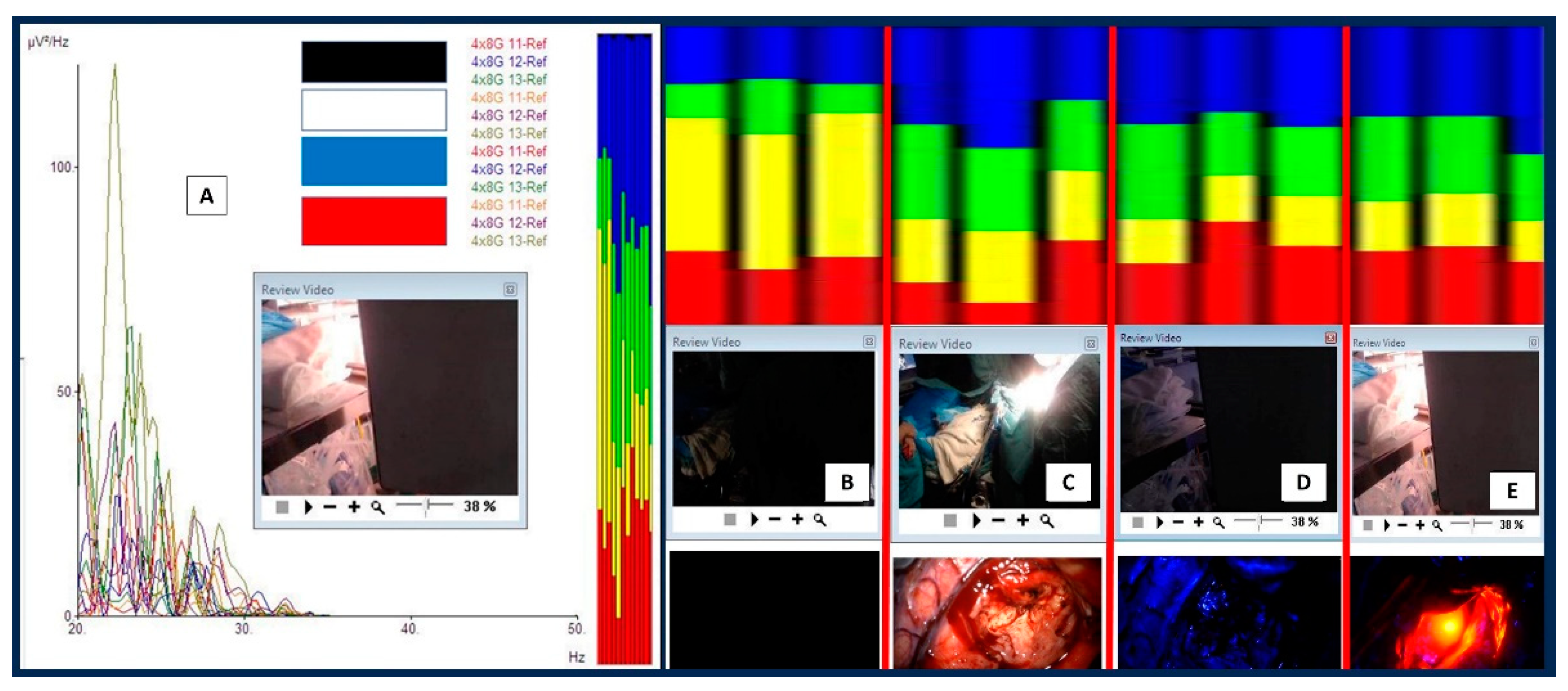
Figure 6.
The difference between near infrared with blue light. When near infrared light was directed towards the hippocampus, gamma waves were noted on frequency analysis. The gamma waves (a black circle on a graph with range just above 30 Hz and black spectrum/white arrows on frequency analysis) disappeared when the near infrared light was off and shifted to the blue light. Note that a black colored brainwave spectrum is for gamma waves (30-50 Hz for our analysis).
Figure 6.
The difference between near infrared with blue light. When near infrared light was directed towards the hippocampus, gamma waves were noted on frequency analysis. The gamma waves (a black circle on a graph with range just above 30 Hz and black spectrum/white arrows on frequency analysis) disappeared when the near infrared light was off and shifted to the blue light. Note that a black colored brainwave spectrum is for gamma waves (30-50 Hz for our analysis).
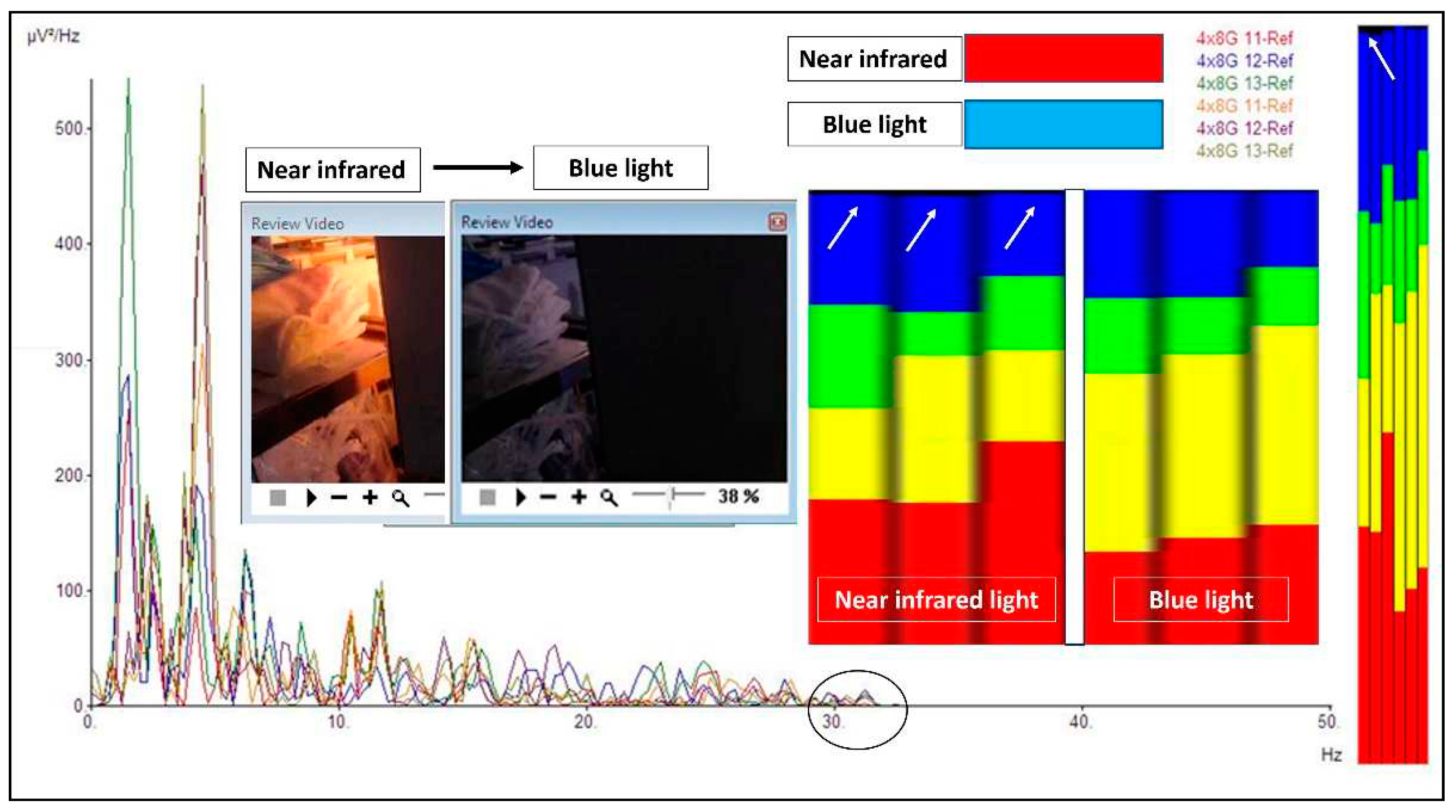
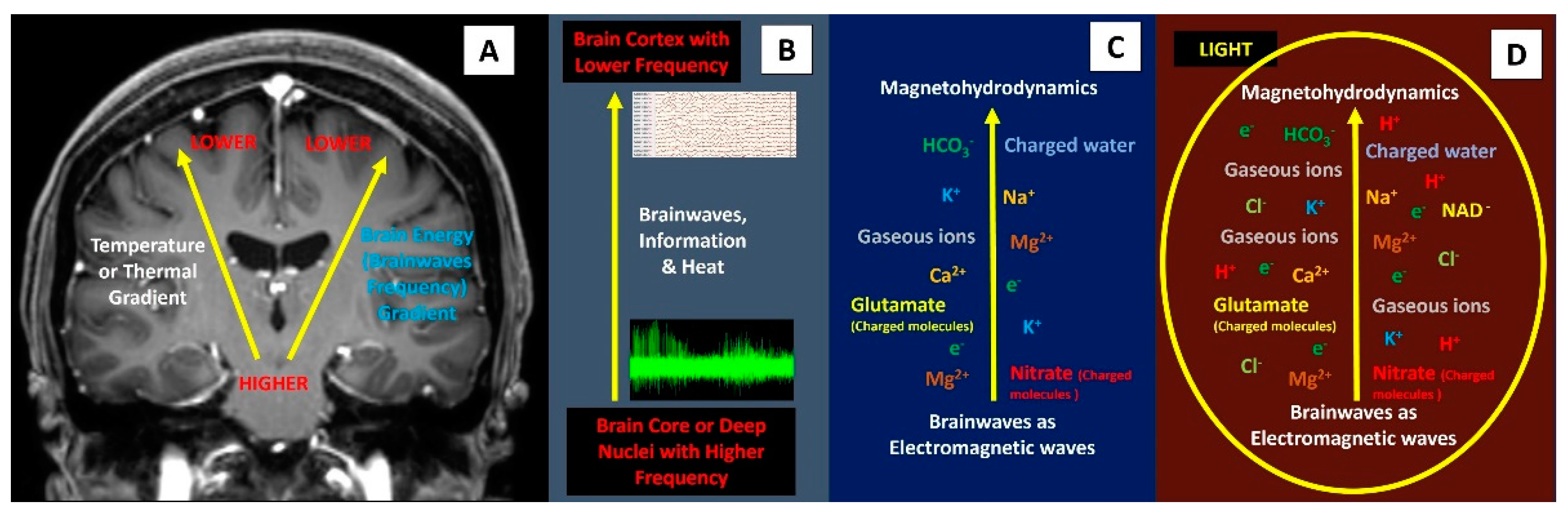
Figure 7.
Brainwaves, thermal gradient, and possible presence of plasma-like brain energy. (A and B) The presence of temperature gradient is related closely to brainwaves and information processing inside the brain. (C) A combination of brainwaves with extracellular plasma soup (charged-ions, charged-molecules, charged-solvent, gaseous ions, and electrons) may form magnetohydrodynamics force which has peculiar features: rapid, has magnetic reconnection and magneto-acoustic waves that help to spread fast and wider brain energy or information. (D) Directly shining the brain with light may form more plasma and hence rapid changes in brainwaves.
Figure 7.
Brainwaves, thermal gradient, and possible presence of plasma-like brain energy. (A and B) The presence of temperature gradient is related closely to brainwaves and information processing inside the brain. (C) A combination of brainwaves with extracellular plasma soup (charged-ions, charged-molecules, charged-solvent, gaseous ions, and electrons) may form magnetohydrodynamics force which has peculiar features: rapid, has magnetic reconnection and magneto-acoustic waves that help to spread fast and wider brain energy or information. (D) Directly shining the brain with light may form more plasma and hence rapid changes in brainwaves.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



