
Submitted:
17 January 2024
Posted:
18 January 2024
You are already at the latest version
Abstract
Out of a worldwide annual incidence of ~150 million cases for urinary tract infection (UTI), >25% of outpatient prescriptions of oral antimicrobial treatment (OAT) are for cystitis not complicated by sepsis. OAT aids the immune cells infiltrating urothelium to eliminate uropathogens attaching and invading urothelium amidst hyperosmotic urine. This adaptability of uropathogens and the short interval between Penicillin sale and the first antimicrobial resistance (AMR) report suggests that AMR is a 3.8 billion years old evolutionary conserved heritable trait of surviving environmental threats through exponential proliferation of mutant strains selected by Darwinian principle. Therefore, OAT success with minimal AMR can be ensured by antimicrobial stewardship (AMS) following the principle of 5Ds -drug, dose, duration, drug-route, and de-escalation. While convenient to administer, the onset of minimum inhibitory concentration (MIC) for OAT in urine is a window of opportunity for uropathogens to survive the first contact with OAT and the descendant colonies armed with AMR are likely to survive subsequent higher urine OAT levels. Meanwhile, intravesical antimicrobial treatment (IAT) delivers the first strike well above MIC. The root cause analysis of AMR dovetails with the strengths, weaknesses, opportunity, and threat (SWOT) analysis of OAT in this interdisciplinary review.
Keywords:
UTI
; AMR
; oral treatment and intravesical treatment
1. Introduction
The earliest imprint of life left by microbes on Earth goes back 3.8 billion years. As the estimated age of our planet is only 4.54 billion years, the earliest imprints of life preserved on rocks are a testament to the adaptability of microbes [1] to survive catastrophes [2] that made many larger life forms extinct. While their size is microscopic, an unparalleled proliferation pace with genetic drift [3,4,5] equips microbes to be the most prevalent life forms on the planet, capable of thriving amidst all other forms of life, including in the highly acidic pH of stomach [1] and hyperosmotic urine [6] of mammals. The variable pH and osmolality of urine (Figure 1) [7] nearly mimics the threats to survival faced 3.8 billion years ago by the ancestors of uropathogens, [8] capable of invading the lower urinary tract while competing for nutrients with the commensal microbiome [9]. Microbes employ mechanisms of commensalism [10], mutualism, and parasitism to survive [11,12] hostile environments. This broad-based review is focused on the intrinsic deficiencies of oral antimicrobial treatments (OAT) in their perpetual battle with microbes infecting the bladder lining- urothelium, called uncomplicated cystitis, hereafter in this discussion [13]. The strengths, weaknesses, opportunity, and threat (SWOT) analysis of OAT for uncomplicated cystitis is complemented by a root cause analysis (RCA) of antimicrobial resistance (AMR) in cystitis [11,14,15] to shed light on the modest success of antimicrobial stewardship (AMS).
2. Antimicrobial resistance (AMR)
The WHO now recognizes AMR as one of the greatest threats to global healthcare. The action triggered by alarm raised by the WHO [15,16,17] is captured in over 249,067 results generated by a recent PubMed search on “Antimicrobial resistance”. Although efforts to contain AMR are capturing the attention of healthcare providers now[2], we postulate that AMR is just an expression of the 3.8 billion years old evolutionary conserved hereditary trait [3,4,5,6,12] of microbes to adapt and survive environmental stresses such as natural or synthetic antimicrobial substances. Our postulate is supported by the first published report on AMR arriving just few years after the commercial sale of Penicillin in 1941 [18].
2.1. Contribution of Urinary tract infection (UTI) To AMR
With ~150 million cases/year globally [13], UTI refers to infection anywhere along the upper or lower urinary tract, but cystitis is a term reserved for the infected urothelium of the bladder (Figure 1). An estimated 25-40% primary care prescriptions of OAT are triggered by uncomplicated cystitis [19]. As per Infectious Diseases Society of America guidelines, first-line OAT for acute uncomplicated cystitis includes sulfamethoxazole-trimethoprim followed by nitrofurantoin, oral β-lactams, and fluoroquinolones should be reserved as the last line of defense against cystitis in outpatient settings [20]. Non-compliance with these guidelines and antimicrobial stewardship (AMS) for cystitis are believed to be major contributors to AMR [11,21,22].
A multi-centre observational cohort US study of 3779 patients recruited from a network of 15 geographically diverse emergency departments found that the incidences of uncomplicated and complicated cystitis were comparable [14] and the most common uropathogens were Gram negative strains of Escherichia coli (63.2%) followed by Klebsiella pneumoniae (13.2%), Proteus mirabilis and Gram positive strains of Enterococcus faecalis and other species (5.8%) and Staphylococcus saprophyticus. Since uropathogens endowed with specific virulence factors also survive in hyperosmotic urine, it is likely that the gain of virulence and resistance [17,23] is driven by shared biochemical mechanisms.
A prior exposure to OAT or injectable antimicrobials in the previous 90 days more than doubled the odds ratio for multi-drug resistance (MDR) in uropathogens isolated from urine samples of acute cystitis patients [14]. The study also reported that the incidence of uropathogenic E. coli (UPEC) fluoroquinolone-resistance ranged from 10.5% to 29.7% by site and uropathogens producing extended spectrum β-lactamase ranged from 3.6% to 11.6% by site. Intriguingly, a third of patients with a resistant isolate did not have any documented risk factors for resistance [14].
2.2. AMR and Pregnancy
Compared to men, incidence of cystitis is much higher in women with 50% lifetime incidence and a third experience recurrences within months [24]. While OAT is recommended for treating recurrent UTI in non-pregnant women [25], their use is contra-indicated in pregnant women owing to the potential teratogenicity of antimicrobials [26]. Therefore, after adjusting for age and socio-economic status, a significantly higher incidence of AMR noted in non-pregnant women relative to pregnant women can be reasonably attributed to OAT used by non-pregnant women [27]. Thus, a prospective study on 1758 women of childbearing age [27] bolsters the link between the widespread use of OAT and AMR.
3. The Urinary Bladder
The primary function of the bladder is to not just store urine excreted by the kidney but also to participate in the maintenance of homeostasis of plasma osmolality by altering the pH and osmolality of urine [7,28,29,30,31]. The homeostasis of plasma is hallmarked by stability of plasma pH, nutrients, and electrolyte levels. The bladder participates in homeostasis via endocrine and stretch mediated urine reabsorption [7,28,29,31,32] , thereby the bladder acts as a backstop to the constant but slow rate of urine production by the kidneys during sleep to prevent nocturnal voiding episodes (nocturia), a symptom of cystitis [33]. The bladder is lined by a multicellular layer of urothelium [34], a highly metabolically active [35] multifunctional tissue that monitors bladder distension [36], signals constitutional changes to the detrusor, micturition centers and the immune system [37]. Umbrella cells rely on restricted transcellular permeability [38] of the asymmetric membrane on the apical side to survive the low pH and threefold higher osmotic pressure of urine [7,39] than the serum (Figure 1). Intermediate cells replacing the infected, superficial urothelial cells are smaller in size than the mature umbrella cells [40], which allows for greater passive, paracellular diffusion of urine constituents [41,42,43], leading to dysuria, which also is a symptom of cystitis [35].
Figure 1.
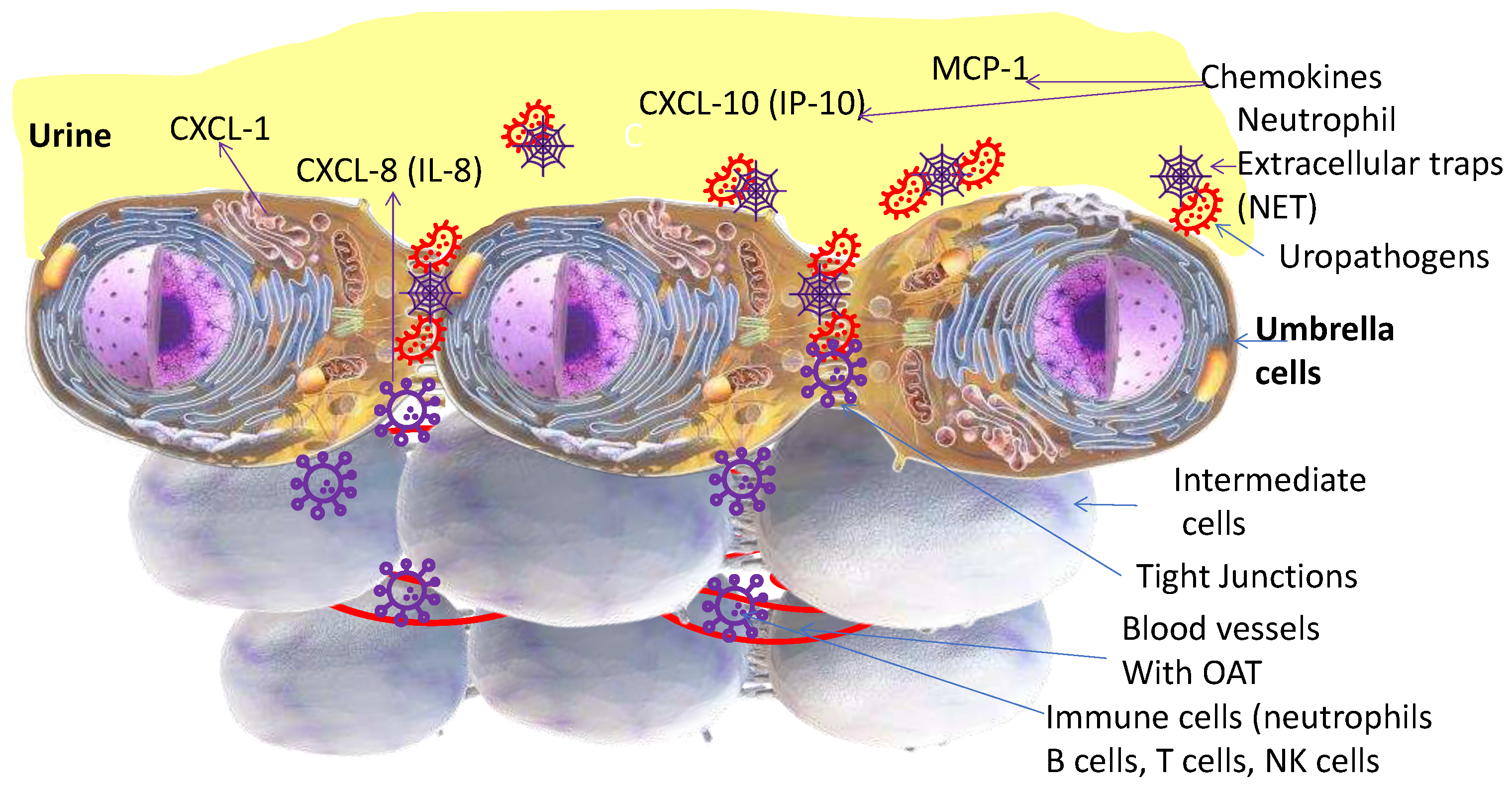
The bladder luminal surface is lined with long-lived, highly differentiated, hexagonal shaped umbrella cells ranging in 20-150µm diameter with an apical layer formed by an asymmetric membrane, hallmarked by restricted permeability to urine constituents. Umbrella cells with an asymmetric membrane cover most of the luminal surface of the bladder but the apico-lateral surface between adjacent umbrella cell borders is lined by finger-like projections-tight junctions-amenable to passive paracellular diffusion of urine constituents. Infiltrating neutrophils near the infected foci release neutrophil extracellular traps (NET) into the lumen to ensnare the invading uropathogens and release substances that are detected in urine dipstick tests for UTI.
Figure 1.
The bladder luminal surface is lined with long-lived, highly differentiated, hexagonal shaped umbrella cells ranging in 20-150µm diameter with an apical layer formed by an asymmetric membrane, hallmarked by restricted permeability to urine constituents. Umbrella cells with an asymmetric membrane cover most of the luminal surface of the bladder but the apico-lateral surface between adjacent umbrella cell borders is lined by finger-like projections-tight junctions-amenable to passive paracellular diffusion of urine constituents. Infiltrating neutrophils near the infected foci release neutrophil extracellular traps (NET) into the lumen to ensnare the invading uropathogens and release substances that are detected in urine dipstick tests for UTI.
3.1. Neutrophils
As illustrated in Figure 1, neutrophils localized near umbrella cells post-infection by uropathogens in rodent models are foot soldiers of the innate immune response [44,45]. Neutrophils activated by chemokines [37] release a mesh-like structure called neutrophil extracellular traps (NET) to entrap the invading uropathogens in the urine-filled lumen [46] and those attaching to umbrella cells. The breakdown products of glycosaminoglycans products can mimic the function of NET [47]. NET includes a DNA backbone embedded with antimicrobial proteins including myeloperoxidase, neutrophil elastase, and histones [48], which are detectable in urine dipsticks. The combative role of neutrophils and NET can be inferred from the lower incidence of cystitis symptoms in 2nd and 3rd trimester of pregnancy, despite an abundance of bacteriuria with uropathogens [15]. Pregnancy-related hormonal changes [49] modulate the innate immune cell activity and cause neutrophilia- marked by an abrupt rise in the number of neutrophils in the 2nd and 3rd trimester of pregnancy [50]. Neutrophils are considered to modulate innate and adaptive immune response [51] through interaction with macrophages, dendritic cells, natural killer cells and T and B lymphocytes [52], generate reactive nitrogen species, reactive oxygen species, and secrete a variety of cytokines and chemokines (CXCL-1, 8,) to combat cystitis [37]. The elevated urine levels of chemokines released by infected urothelium [37] decline with OAT and the breakdown products of glycosaminoglycans [47] from kidney to bladder are also detectable in urine.
4. Cystitis Etiology and Treatment
Bacterial cystitis symptomatology is described by the symptoms of frequency, urgency and/or dysuria that also overlap with symptoms of interstitial cystitis and other urological diseases to complicate the diagnosis [35]. A history of two or more episodes of bacterial cystitis is an independent risk factor [11,25] for recurrent cystitis, defined as ≥2 episodes in 6 months or ≥3 in a year. Compared to men, higher incidence of cystitis in women is generally linked to their shorter urethra and easier entry of microbes from adjacent cavities of vagina and anus [53]. It is also likely that periodic shedding of urothelium, exclusively in female mammalian bladder [54,55,56] may shed light on the higher incidence of cystitis in women [35] accompanying lower incidence of urothelial carcinoma [57].
Cystitis is responsible for more non-elective hospital admissions in multiple sclerosis than any of its plethora of impairments [58]. Imaging based differentiation of upper and lower UTI (cystitis) is critical before initiating aggressive treatment reserved for complicated cystitis. The need for translational research to understand the pathogenesis of human cystitis cannot be overstated [59] considering the fact that critical elements of cystitis pathogenesis identified in mouse models, which are the intracellular bacterial colonies in the superficial umbrella cells of infected mice [12,60] could not be reproduced in the pig model of acute cystitis [61]. Given that pigs can weigh as much as humans and human bladder wall is as thick as that of pig bladder [62], human pathogenesis of cystitis is more likely to track the pathogenesis in the pig model [61].
As the microbiome of the bladder is influenced by the microbiome of adjacent organs [63,64], it is plausible that symbionts of other organs may become opportunist uropathogens, hallmarked by their attachment to umbrella cells (Figure 1) and possession of specific virulence factors and the secretion of proteolytic enzymes [65], biofilm production [66] to survive in urine, quorum-sensing community support networks, short life spans and rapid proliferation of mutant colonies with vertical and horizontal transmission [1] of new genetic features through plasmid transfer, which helped identify DNA as the genetic material[67]. The highest prevalence of uropathogenic E. coli (UPEC) informed its selection for inoculation of pig bladder to model human cystitis, where the ingress of UPEC into umbrella cells was noted near tight junctions (Figure 1) [61].
4.1. SWOT of Oral Antimicrobial Therapy (OAT) for UTI
The primary strengths of OAT are simplicity and convenience, as self-medication does not burden doctors or nurses with having to administer the treatments. The primary weaknesses of OAT are inter-individual variability in clinical outcomes and AMR owing to inter-individual variability in pharmacokinetics [17] of OAT delaying the arrival of minimum inhibitory concentration (MIC) in urine. MIC is the lowest antimicrobial concentration required to prevent the visible growth of the test strain of a microbe after a definite incubation period under strictly controlled in vitro conditions [68].
The antimicrobial effect of OAT takes effect only after the absorbed dose fraction gets filtered from plasma by the kidneys into urine (Figure 2). The variability in the pharmacokinetics of OAT stem from the variable absorption from the gut [69,70], first pass metabolism in liver, and systemic distribution followed by renal excretion (Figure 2) for an intermittent ureteric delivery of OAT into urine. Since the bladder [71] receives only 10% of the cardiac output delivered by the renal arteries to kidneys [72,73], the exposure of bladder mucosa to circulating drug levels[74] is minimal compared to the exposure of the luminal side to the urine drug levels(Figure 2). For all intents and purposes, bladder exposure to circulating OAT (Figure 3) leaves a time window of opportunity for invading microbes to activate AMR for the following reasons:
- A.
- The variability in initial drug concentration due to variable absorption from gut and variability in urine in-flow rate of 0.3-15mL/min (~50x difference) [33]
- B.
- C.
A simple multiplication of the noted ranges; >50x >100x >300,000x incriminates potential differences in the physical and physicochemical characteristics of urine in stark contrast to the homeostasis of plasma volume and pH for optimal functioning of cells. The plot depicted below is projected from published human urine and plasma levels of nitrofurantoin in healthy human volunteers after oral dosing [69], which must be read with the following caveats: while there can be fixed sampling time points for plasma, there was no fixed sampling of urine after oral dosing. Based on frequent voiding of cystitis patients, one can infer that concentration build-up noted in healthy volunteers voiding less frequently (Figure 2) may not materialize in cystitis patients. Moreover, malaise and dehydration secondary to cystitis will alter the urine flow rate, pharmacokinetic parameters, and renal toxicity of OAT.
Figure 2.
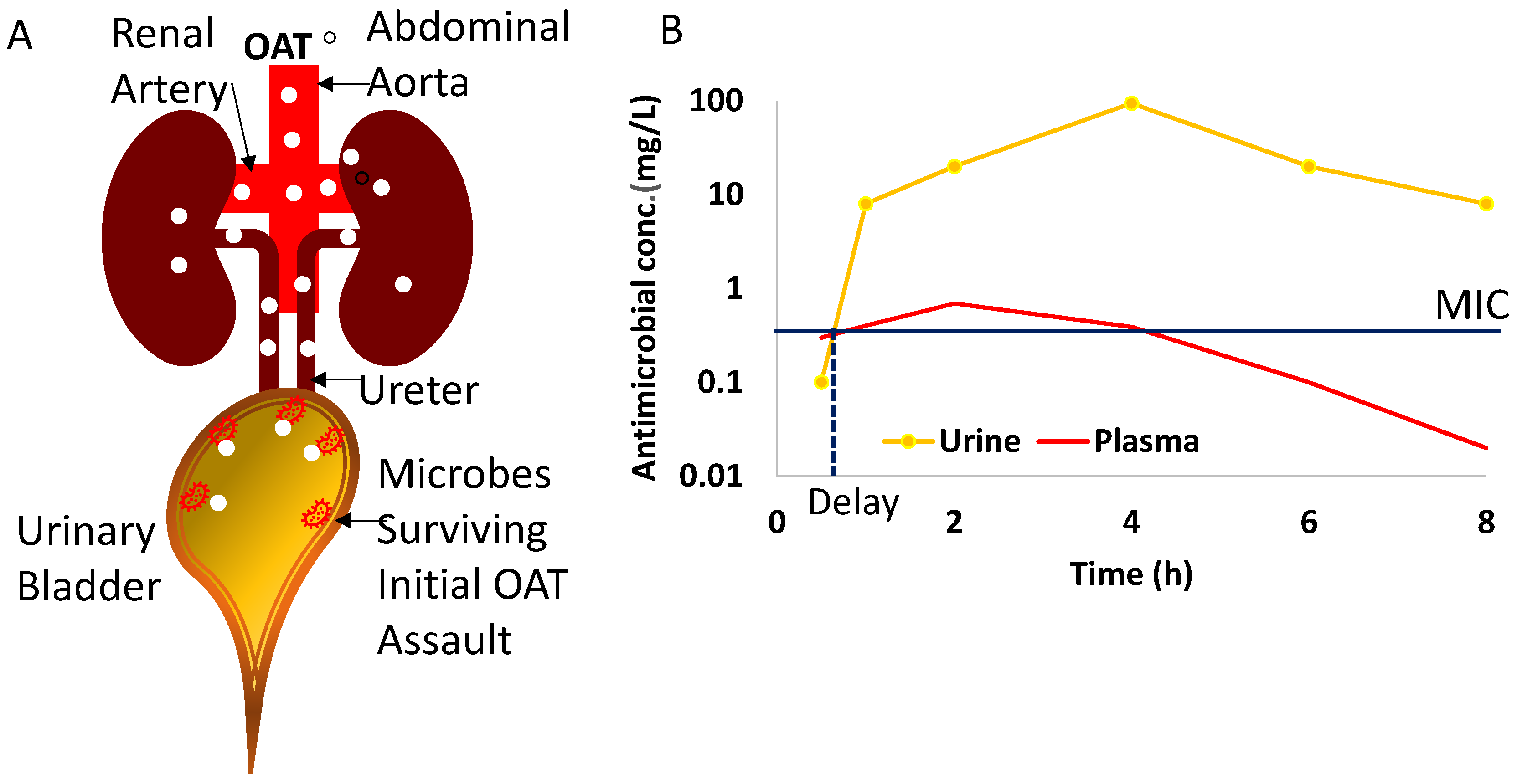
Panel A - Oral antimicrobial treatment (OAT) reaches uropathogens infecting the bladder urothelium after the absorbed dose fraction is delivered to the kidneys via renal arteries and OAT gets excreted into urine. As a result, there is an initial mismatch between the initial urine concentration of OAT and the number of microbes infecting the urothelium. Panel B- Projected plots for serum and urine levels after a single dose of OAT (nitrofurantoin). Time 0 is the time of drug administration and the delay in reaching urinary MIC leaves a window of opportunity for the activation of AMR genes. Then the resistant descendants selected by the Darwinian principle proliferate exponentially. Please note the log-scale of the y-axis.
Figure 2.
Panel A - Oral antimicrobial treatment (OAT) reaches uropathogens infecting the bladder urothelium after the absorbed dose fraction is delivered to the kidneys via renal arteries and OAT gets excreted into urine. As a result, there is an initial mismatch between the initial urine concentration of OAT and the number of microbes infecting the urothelium. Panel B- Projected plots for serum and urine levels after a single dose of OAT (nitrofurantoin). Time 0 is the time of drug administration and the delay in reaching urinary MIC leaves a window of opportunity for the activation of AMR genes. Then the resistant descendants selected by the Darwinian principle proliferate exponentially. Please note the log-scale of the y-axis.
Furthermore, the pharmacokinetic/pharmacodynamic modelling of OAT [78] found that drug exposure that suppresses the emergence of AMR in Gram-negative bacteria varies for each drug molecule. Modeling projects that the target plasma concentration should be 4-1000-fold higher than MIC to prevent AMR, which is however unfeasible owing to the toxicity and lower therapeutic index of OAT. If one were to analyze combat of OAT with uropathogens through a military lens, then the use of overwhelming force on first contact with the adversary (microbes) is more likely to extinguish any hope of resurgence (gain of AMR) [79]. Accordingly, urine concentration of OAT at first contact with the microbial colonies [4,5] infecting the urothelium is a crucial determinant in the emergence of a drug-resistant strain that proliferates exponentially to survive even subsequently higher drug concentration in urine (Figure 2). Therefore, the duration (Figure 3) between the arrival of the first drug molecule in urine and urinary MIC is a proverbial “window of opportunity” for microbes to activate latent AMR genes [3,80] or shelter from OAT by entering into leaky tight junctions of inflamed urothelium[41,61] or exfoliated vesicles. Uropathogens can adapt to OAT through a panoply of pathways [6] including negative tropism, acceleration of mutations [81], sheltering under biofilm, expulsion of OAT by membrane pumps. Biodiversity suggests there may be other mechanisms as well [81]. Thus, delay in urinary MIC of OAT in the wake of initial conditions is a threat for the emergence and prevalence of AMR.
4.1.1. Delay and variability in urinary MIC
As depicted in the plots (Figure 2 B), even though the peak urine concentration Cmax of oral nitrofurantoin is twenty-five-fold higher than in plasma Cmax, the initial delay in reaching urine MIC leaves a window of opportunity (Figure 3) for the activation of AMR genes to survive subsequent higher concentration of nitrofurantoin. Nitrofurantoin reaches its peak serum concentration (Cmax) in the time range of 2-24 hours (Tmax ) after oral dosing [69] and only 20-25% of an absorbed dose of nitrofurantoin is ultimately excreted in urine [69] as opposed to 40-60% for sulfamethoxazole and trimethoprim [63,70].
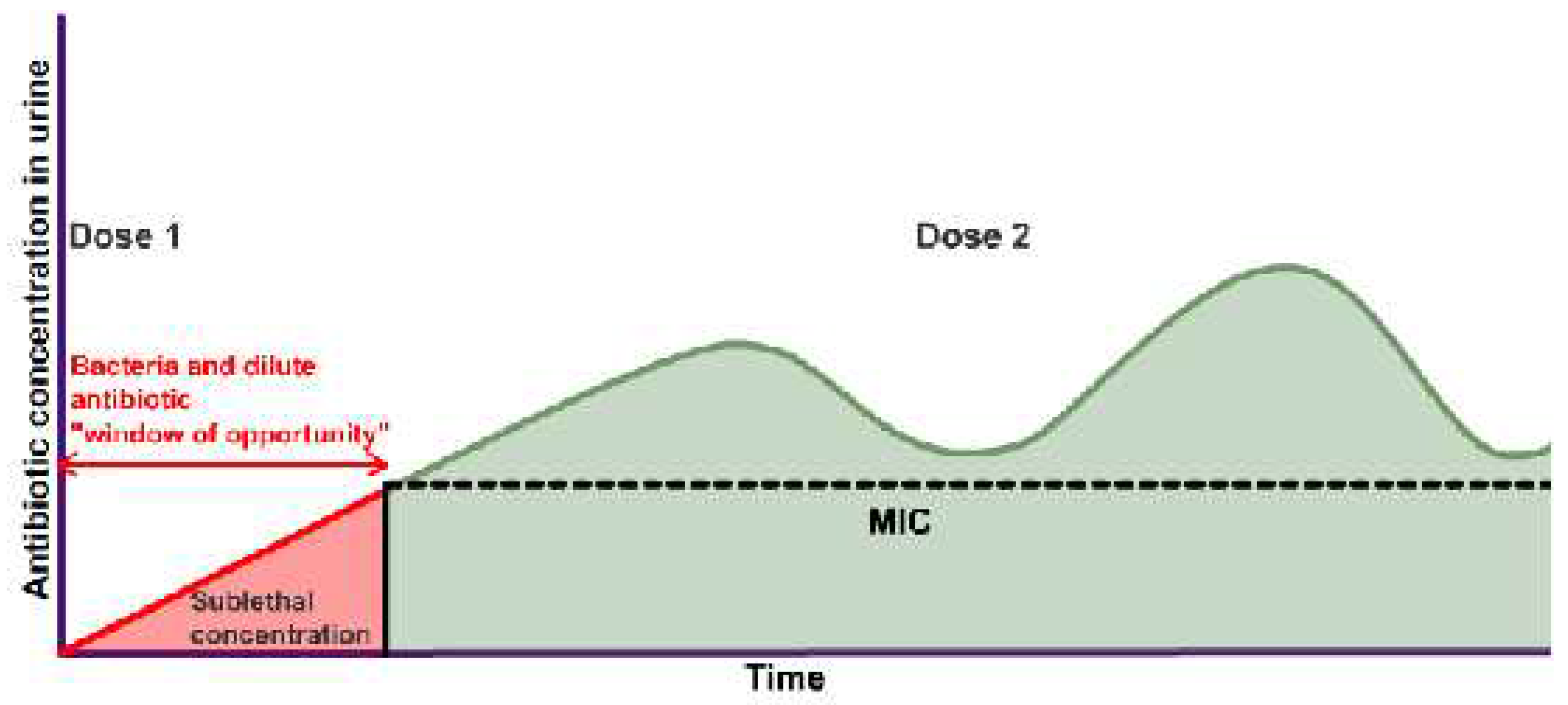
The figure above vividly illustrates with a mirage graph that OAT being dripped into urine of variable volumes at variable pH from kidneys to bladder may sufficiently facilitate the evasive actions of microbes to gain AMR. The graph is referred to as “mirage” because data points are unknowable and indeterminable for real-world treatment. Furthermore, MIC of OAT is sensitive to pH and the wide range of potential intravesical acidity/alkalinity makes it untenable to extrapolate in vitro MIC to the bladder. It is noteworthy that laboratory-based efficacy testing of MIC for cystitis [82] does not account for the variability in urine flow.
Figure 3.
Repeat dosing of OAT is projected to engender time dependent variability in antibiotic concentration in urine with respect to MIC and leave a window of opportunity for activation of AMR.
Figure 3.
Repeat dosing of OAT is projected to engender time dependent variability in antibiotic concentration in urine with respect to MIC and leave a window of opportunity for activation of AMR.
4.1.2. Why urine levels are higher than plasma levels of OAT?
Given that only 20-25% of the absorbed dose of nitrofurantoin is ultimately excreted in urine [69], the remainder of the absorbed dose (100-20= 80%) should have generated relatively higher plasma levels. Understanding of this anomaly requires a deep dive into pharmacokinetics to understand the counter-intuitive concept of volume of distribution (Vd), which is a theoretical volume for the distribution for any drug [77]. Accordingly, 75-80% of absorbed dose of nitrofurantoin (fraction not excreted in urine) is diluted on 0.46Liters/kg [83] of body weight or 32.2Liters for a 70kg adult to generate <1mg/L plasma concentration whereas 20-25% of absorbed dose is diluted in just 1.5L of 24h urine to generate >10mg/L (Figure 2). Simply stated, the bigger denominator for 75-80% dose leads to 25-fold lower plasma levels than the urine levels of nitrofurantoin.
The variability in the time taken to reach peak urinary concentration (Tmax ) of OAT results from highly variable physiological and pharmacokinetic activities preceding the entry of OAT into urine, which are:
The study on healthy humans [69] implicated the role of factors listed above in the inter-individual variability in the mean value of urine Tmax, which is delayed by 2.5 hours relative to the plasma Tmax. The variability in the urine Tmax contributes to the variability in the emergence of AMR [6]. Compared to humans, it can be difficult to get urine samples “on demand” from dogs [85] and that sampling flaw may have generated the distorted inference that urinary Tmax occurs an hour earlier than plasma Tmax and former ranges from 0 to 8h in healthy beagles upon repeat oral dosing of nitrofurantoin every 8h [85].
5. Root cause analysis of OAT contribution to AMR
Last October, the National health service (NHS) England reported that AMR was associated with 1.8 million hospital admissions in the last 5 years and UTI was causative in over 800,000 with people over 65 years old providing most cases. A quarter of urine samples analyzed in the first half of 2023 had drug resistant bacteria and there was only a 1.6% reduction in the total number of antibiotic-resistant infections from 2018-2023, far below the ambitious goal of 10% by 2025. AMR is believed to be the proximate cause of over 300,000 deaths annually in India, the most populated country[16]. A tidal wave of momentum recognizes antimicrobial stewardship (AMS) as a critical tool to assail AMR [86]. According to NHS England, AMS refers to an organizational or healthcare system-wide approach to retard evolution of AMR by promoting and monitoring judicious use of antimicrobials to preserve their future effectiveness by optimal selection, dosing, and duration resulting in the best clinical outcome with minimal side effects to the patients [87]. However, widespread preference for oral fluoroquinolones to treat uncomplicated cystitis is not in accordance with AMS or treatment guidelines [22]. Importantly, a multimodal AMS initiative decreased outpatient usage of fluoroquinolone for cystitis by 39% [21] in a large Texas health system from 2016-2018. A modest success of AMS with OAT in cystitis merits a root cause analysis of AMR in light of the factors discussed in detail in preceding paragraphs and stated succinctly here:
Cystitis treatment failures and AMR results from a bladder milieu that allows adaptable microbes to evade, escape or expel antimicrobials [14].
Interchangeable use of UTI and cystitis. While absorbed OAT can reach pathogens of upper urinary tract via perfused blood, uropathogens causing cystitis can only be eliminated by the urinary fraction of absorbed OAT(Figure 2) because circulating levels [74] of OAT are less likely to reach the planktonic microbes and those attaching to the apical side of umbrella cells (Figure 1).
The combat between OAT and the uropathogens provoking cystitis is heavily influenced by the physiology of urine flow [17] and physicochemistry.
The principle of 5Ds -drug, dose, duration, drug-route, and de-escalation for AMS [87] advocates getting the right drug concentration in urine above MIC (Figure 2, Figure 3 and Figure 4) [80,88].
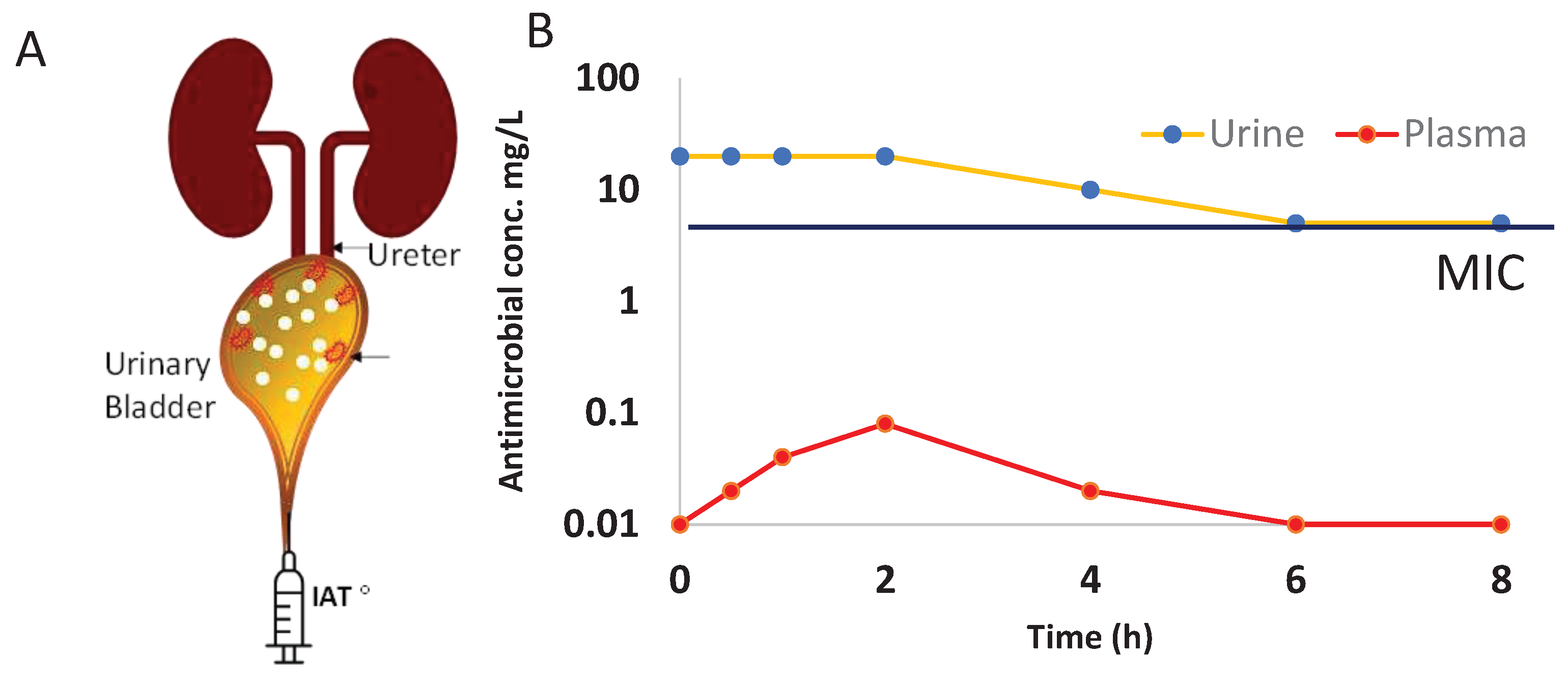
The principle of 5”D”s can be best illustrated by intravesical Gentamicin 80mg(Figure 4B), delivering a bactericidal concentration with 90% elimination of live bacteria within 3h with a comparative lower incidence of AMR [89] and recurrence [90] than reported with OAT [14,79]. As opposed to urine and plasma plots of OAT shown in Figure 2B, the plot of Figure 4B is projected from a recent study on post-operative prophylaxis by intravesical Gentamicin [91]. As depicted by the low plasma levels (red curve of Figure 4B), the limited bioavailability from bladder can allow local administration of drug concentration (yellow curve of Figure 4B) that would be in a toxic range with systemic delivery [88]. Accordingly, one can safely deliver doses that generate concentration 4-1000-fold higher than MIC [78] via the intravesical route at first contact with microbes to lower the likelihood of AMR development [79] whereas OAT exposes bladder urothelium to a higher concentration [69,70] in a gradual fashion allowing uropathogens to adapt and survive with AMR [15,86]. Although, intravesical antimicrobial therapy (IAT) (Figure 4) complies with the prescription of 5”D”s, IAT with aminoglycosides or any other broad-spectrum antibiotics is yet to receive a regulatory approval for therapy or prophylaxis [80].
6. Discussion
Preceding paragraphs elucidate that current clinical practices of OAT prescriptions for cystitis and the physiology of urine flow into bladder [7,28,29] are critical determinants of AMR prevalence [14,16]. To avoid confusion among health practitioners, we suggest that cystitis should be treated as a distinct entity within the broad category of UTI in light of the SWOT and root cause analysis of AMR stemming from OAT for cystitis. While IAT for cystitis is both intracavity and topical (Figure 4), OAT reaches the same site after urinary excretion and therefore the dynamic entry of the excreted fraction of absorbed OAT in the milieu of urine are critical factors in the efficacy of OAT and ensuing AMR [17].
We performed SWOT of OAT here but SWOT of uropathogens is necessary to ensure treatment success. The major strengths of uropathogens are adaptability to survive the hyperosmotic urine while the weakness is outlined by the susceptibility reports and threat of AMR can be gleaned from both unknown and indeterminable Tmax in urine, which is a moving target for reasons discussed here. As illustrated by Figure 2, the variability in the initial intravesical conditions [4,5] can be consequential to the OAT sensitivity of bacterial descendants [5] but standard OAT offers no basis for knowing the duration of the window of opportunity.
Recent studies suggest that evolutionary changes may mitigate AMR [1], but since hope is never a winning strategy in any war, we should be ready for AMR aggravated by climate change [2]. To slow the pace of evolution of AMR, the US Food and Drug Administration- and European Medicines Agency recently approved, Dequalinium chloride to inhibit the activation of the Escherichia coli general stress response, which promotes fluoroquinolone-induced mutagenic DNA break repair [8]. The entrapment of uropathogens by NET is mimicked by glycosaminoglycans [47] and a recent retrospective analysis of 151 patients found intravesical chondroitin sulphate to be superior to OAT in the treatment of recurrent cystitis [92]. This recent study confirmed reports from other groups using hyaluronic acid and chondroitin sulphate for prophylaxis of cystitis in spinal cord injured and spinal cord intact individuals [93,94]. Other groups have explored antimicrobial peptides [17] and bacteriophage treatment [23] as non-antibiotic prophylactic approaches for UTI.
Analogous to the fecal microbiota transplantation for managing recurrent Clostridioides difficile infection [95], intravesical instillation of innocuous microbes into the bladder [9,10] is a non-antibiotic approach for cystitis. The intravesical inoculation of E. coli 83972 ASB strain in atonic bladders of 21 spinal cord injured patients with chronic bacteriuria [10] achieved successful long-term bladder colonization in 13 participants that lasted for more than a year without causing bacteremia or sepsis. Another group diversified the urinary microbiome and disrupted the colonization by virulent strains of uropathogens in 26 patients with neurogenic bladder, who regularly self-catheterized with instillation of Lactobacillus rhamnosus GG [9].
As the science of OAT for cystitis is poorly understood and with limited available options for resistant uropathogens, many experts advise us to be judicious in picking battles with uropathogens and avoid pre-emptive strikes on ASB [22] with broad spectrum OAT before dysuria appears [96]. Only initiate OAT for uncomplicated cystitis if symptoms are refractory to non-steroidal analgesics. OAT prescriptions [96] for ASB with pyuria [53] have the potential to alter the diversity of the microbiome in favor of resistant pathogens [14] and adversely impact the memory of innate immune cells to combat uropathogens.
Despite fortuitous successful OAT treatment of a high proportion of cases, the approach may produce failures and accentuate the evolution of AMR and complications we observe in clinical services. Extrapolation of treating bacterial infections in other parts of body to cystitis should be re-evaluated in light of the pharmacokinetic considerations described here as an essential feature of AMS. Based on current understanding of the adaptability of uropathogens, we deign to hypothesize that any antibacterial treatment protocol [80] that fails to account for the evolutionary predisposition of microbes that have been adapting to climate change for billions of year [2] may be destined to fail the test of time. As the future of antibiotics evidently rests so firmly upon AMS [21,22,86], we leave that thought for all the stakeholders of health to consider.
Author Contributions
Conceptualization, PT and SG.; writing—original draft preparation, PT and SG.; writing—review and editing, ST and LS. All authors have read and agreed to the published version of the manuscript.”.
Funding
This work was partly supported by funding from the National Cancer Institute, CA252590 and National institute of Aging RO1 AG076575. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
Institutional Review Board Statement
“Not applicable”.
Informed Consent Statement
“Not applicable.”.
Data Availability Statement
not applicable
Conflicts of Interest
Pradeep Tyagi PhD holds patent in intravesical drug delivery system licensed to Lipella Pharmaceuticals and Scott Glickman FRCS is medical director of Uropharma Ltd.
References
- Nguyen, A.N.T.; Gorrell, R.; Kwok, T.; Connallon, T.; McDonald, M.J. Horizontal gene transfer facilitates the molecular reverse-evolution of antibiotic sensitivity in experimental populations of H. pylori. Nat Ecol Evol 2024. [Google Scholar] [CrossRef]
- Wong, C. Antibiotic resistance is a growing threat - is climate change making it worse? Nature 2024. [Google Scholar] [CrossRef]
- Gonze, D.; Coyte, K.Z.; Lahti, L.; Faust, K. Microbial communities as dynamical systems. Curr Opin Microbiol 2018, 44, 41–49. [Google Scholar] [CrossRef]
- Wright, E.S.; Gupta, R.; Vetsigian, K.H. Multi-stable bacterial communities exhibit extreme sensitivity to initial conditions. FEMS Microbiol Ecol 2021, 97. [Google Scholar] [CrossRef] [PubMed]
- Wright, E.S.; Vetsigian, K.H. Stochastic exits from dormancy give rise to heavy-tailed distributions of descendants in bacterial populations. Mol Ecol 2019, 28, 3915–3928. [Google Scholar] [CrossRef]
- Zhang, K.; Potter, R.F.; Marino, J.; Muenks, C.E.; Lammers, M.G.; Dien Bard, J.; Dingle, T.C.; Humphries, R.; Westblade, L.F.; Burnham, C.A.; et al. Comparative genomics reveals the correlations of stress response genes and bacteriophages in developing antibiotic resistance of Staphylococcus saprophyticus. mSystems 2023, 8, e0069723. [Google Scholar] [CrossRef]
- Cahill, D.J.; Fry, C.H.; Foxall, P.J. Variation in urine composition in the human urinary tract: evidence of urothelial function in situ? J Urol 2003, 169, 871–874. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Y.; Pribis, J.P.; Dooling, S.W.; Garcia-Villada, L.; Minnick, P.J.; Xia, J.; Liu, J.; Mei, Q.; Fitzgerald, D.M.; Herman, C.; et al. Drugging evolution of antibiotic resistance at a regulatory network hub. Sci Adv 2023, 9, eadg0188. [Google Scholar] [CrossRef] [PubMed]
- Groah, S.L.; Rounds, A.K.; Perez-Losada, M. Intravesical Lactobacillus rhamnosus GG Alters Urobiome Composition and Diversity Among People With Neurogenic Lower Urinary Tract Dysfunction. Top Spinal Cord Inj Rehabil 2023, 29, 44–57. [Google Scholar] [CrossRef]
- Hull, R.; Rudy, D.; Donovan, W.; Svanborg, C.; Wieser, I.; Stewart, C.; Darouiche, R. Urinary tract infection prophylaxis using Escherichia coli 83972 in spinal cord injured patients. J Urol 2000, 163, 872–877. [Google Scholar] [CrossRef]
- Zhang, H.L.; Perez, R.; Krishnan, J.; Lautenbach, E.; Anderson, D.J. Risk Factors for Recurrence of Community-Onset Urinary Tract Infections Caused by Extended-Spectrum Cephalosporin-Resistant Enterobacterales. Open Forum Infect Dis 2023, 10, ofad561. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhou, Z.; Zheng, L.; Gong, Z.; Li, Y.; Jin, Y.; Huang, Y.; Chi, M. Urinary Tract Infections Caused by Uropathogenic Escherichia coli: Mechanisms of Infection and Treatment Options. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Mengistu, D.A.; Alemu, A.; Abdukadir, A.A.; Mohammed Husen, A.; Ahmed, F.; Mohammed, B. Incidence of Urinary Tract Infection Among Patients: Systematic Review and Meta-Analysis. Inquiry 2023, 60, 469580231168746. [Google Scholar] [CrossRef] [PubMed]
- Faine, B.A.; Rech, M.A.; Vakkalanka, P.; Gross, A.; Brown, C.; Harding, S.J.; Slocum, G.; Zimmerman, D.; Zepeski, A.; Rewitzer, S.; et al. High prevalence of fluoroquinolone-resistant UTI among US emergency department patients diagnosed with urinary tract infection, 2018-2020. Acad Emerg Med 2022, 29, 1096–1105. [Google Scholar] [CrossRef] [PubMed]
- Rafat, D.; Agrawal, A.; Khalid, S.; Khan, A.U.; Nawab, T.; Sultan, A. Bacterial abundance and antimicrobial resistance patterns of uropathogens among pregnant women with asymptomatic bacteriuria: Association with glycemic status. Eur J Obstet Gynecol Reprod Biol X 2024, 21, 100263. [Google Scholar] [CrossRef] [PubMed]
- Nair, M.; Zeegers, M.P.; Varghese, G.M.; Burza, S. India's National Action Plan on Antimicrobial Resistance: a critical perspective. J Glob Antimicrob Resist 2021, 27, 236–238. [Google Scholar] [CrossRef] [PubMed]
- Von Vietinghoff, S.; Shevchuk, O.; Dobrindt, U.; Engel, D.R.; Jorch, S.K.; Kurts, C.; Miethke, T.; Wagenlehner, F. The global burden of antimicrobial resistance - urinary tract infections. Nephrol Dial Transplant 2023. [Google Scholar] [CrossRef]
- Plough, H.H. Penicillin resistance of Staphylococcus aureus and its clinical implications. Am J Clin Pathol 1945, 15, 446–451. [Google Scholar] [CrossRef]
- Milano, A.; Sulejmani, A.; Intra, J.; Sala, M.R.; Leoni, V.; Carcione, D. Antimicrobial Resistance Trends of Escherichia coli Isolates from Outpatient and Inpatient Urinary Infections over a 20-Year Period. Microb Drug Resist 2022, 28, 63–72. [Google Scholar] [CrossRef]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis 2011, 52, e103–120. [Google Scholar] [CrossRef]
- Lin, K.; Zahlanie, Y.; Ortwine, J.K.; Mang, N.S.; Wei, W.; Brown, L.S.; Prokesch, B.C. Decreased Outpatient Fluoroquinolone Prescribing Using a Multimodal Antimicrobial Stewardship Initiative. Open Forum Infect Dis 2020, 7, ofaa182. [Google Scholar] [CrossRef]
- Yu, J.Y.; McKenna, V.A.; Dumyati, G.K.; Lubowski, T.J.; Carreno, J.J. Antibiotic Prescribing in New York State Medicare Part B Beneficiaries Diagnosed With Cystitis Between 2016 and 2017. Open Forum Infect Dis 2020, 7, ofz544. [Google Scholar] [CrossRef]
- Green, S.I.; Clark, J.R.; Santos, H.H.; Weesner, K.E.; Salazar, K.C.; Aslam, S.; Campbell, J.W.; Doernberg, S.B.; Blodget, E.; Morris, M.I.; et al. A Retrospective, Observational Study of 12 Cases of Expanded-Access Customized Phage Therapy: Production, Characteristics, and Clinical Outcomes. Clin Infect Dis 2023, 77, 1079–1091. [Google Scholar] [CrossRef]
- Vazquez-Montes, M.; Fanshawe, T.R.; Stoesser, N.; Walker, A.S.; Butler, C.; Hayward, G. Epidemiology and microbiology of recurrent UTI in women in the community in Oxfordshire, UK. JAC Antimicrob Resist 2024, 6, dlad156. [Google Scholar] [CrossRef]
- Albert, X.; Huertas, I.; Pereiro, II; Sanfelix, J. ; Gosalbes, V.; Perrota, C. Antibiotics for preventing recurrent urinary tract infection in non-pregnant women. Cochrane Database Syst Rev 2004, 2004, CD001209. [Google Scholar] [CrossRef]
- Gould, A.P.; Winders, H.R.; Stover, K.R.; Bookstaver, P.B.; Griffin, B.; Bland, C.M.; Eiland, L.S.; Murray, M. Less common bacterial, fungal and viral infections: review of management in the pregnant patient. Drugs Context 2021, 10. [Google Scholar] [CrossRef]
- Mohapatra, S.; Venugopal, S.J.; Kalaivani, M.; Kant, S.; Tak, V.; Panigrahy, R.; Chunchanur, S.K.; Kocher, D.; Behera, B.; Pundir, S.; et al. Antibiotic resistance of uropathogens among the community-dwelling pregnant and nonpregnant female: a step towards antibiotic stewardship. BMC Infect Dis 2022, 22, 939. [Google Scholar] [CrossRef] [PubMed]
- Shafik, A.; Ahmed, I.; El Sibai, O.; Shafik, A.A. Does the composition of voided urine reflect that of the renal pelvis? Urol Res 2006, 34, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Baumgarten, R.; van de Pol, M.H.; Deen, P.M.; van Os, C.H.; Wetzels, J.F. Dissociation between urine osmolality and urinary excretion of aquaporin-2 in healthy volunteers. Nephrol Dial Transplant 2000, 15, 1155–1161. [Google Scholar] [CrossRef]
- Ashdown, H.H. Absorption from the Mucous Membrane of the Urinary Bladder. J Anat Physiol 1887, 21, 299–324 291. [Google Scholar] [PubMed]
- Torimoto, K.; Matsushita, C.; Itami, Y.; Iwamoto, T.; Owari, T.; Gotoh, D.; Miyake, M.; Hori, S.; Nakai, Y.; Aoki, K.; et al. Assessment of bladder function for stabilizing urinary volume overnight with recording of brain waves (ABSORB study). Low Urin Tract Symptoms 2022, 14, 72–77. [Google Scholar] [CrossRef]
- Hilson, A.J.; Lewis, C.A.; Harland, S.J. The permeability of the human bladder to water assessed using tritiated water. Contrib Nephrol 1990, 79, 41–44. [Google Scholar] [CrossRef]
- Watanabe, H.; Azuma, Y. Periodical measurement of urine volume in the bladder during sleep: Temporary volume reduction suggestive of absorption. Int J Urol 2016, 23, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.M.; Vodovotz, Y.; Yoshimura, N.; Chermansky, C.J.; Fitzgerald, J.; Tyagi, P. Temporally complex inflammatory networks in an animal model reveal signatures for interstitial cystitis and bladder pain syndrome phenotype. Neurourol Urodyn 2023, 42, 1839–1848. [Google Scholar] [CrossRef]
- Tyagi, P.; Maranchie, J.; Dhir, R.; Moon, C.H.; Biatta, S.; Balasubramani, G.K.; Yoshimura, N.; Fitzgerald, J.; Chermansky, C.; Kaufman, J.; et al. Unraveling the Complexity of bladder-centric chronic pain by intravesical contrast enhanced MRI. Continence (Amst) 2023. [Google Scholar] [CrossRef]
- Singh, N.; Zabbarova, I.; Ikeda, Y.; Kanai, A.; Chermansky, C.; Yoshimura, N.; Tyagi, P. Role of hyperpolarization-activated cyclic nucleotide-gated channels in aging bladder phenotype. Life Sci 2022, 289, 120203. [Google Scholar] [CrossRef] [PubMed]
- Tyagi, P.; Tyagi, V.; Qu, X.; Chuang, Y.C.; Kuo, H.C.; Chancellor, M. Elevated CXC chemokines in urine noninvasively discriminate OAB from UTI. Am J Physiol Renal Physiol 2016, 311, F548–554. [Google Scholar] [CrossRef] [PubMed]
- Sonn, G.A.; Jones, S.N.; Tarin, T.V.; Du, C.B.; Mach, K.E.; Jensen, K.C.; Liao, J.C. Optical biopsy of human bladder neoplasia with in vivo confocal laser endomicroscopy. J Urol 2009, 182, 1299–1305. [Google Scholar] [CrossRef]
- Gupta, D.K.; Lewis, C.E.; Varady, K.A.; Su, Y.R.; Madhur, M.S.; Lackland, D.T.; Reis, J.P.; Wang, T.J.; Lloyd-Jones, D.M.; Allen, N.B. Effect of Dietary Sodium on Blood Pressure: A Crossover Trial. JAMA 2023, 330, 2258–2266. [Google Scholar] [CrossRef]
- Russell, S.K.; Harrison, J.K.; Olson, B.S.; Lee, H.J.; O'Brien, V.P.; Xing, X.; Livny, J.; Yu, L.; Roberson, E.D.O.; Bomjan, R.; et al. Uropathogenic Escherichia coli infection-induced epithelial trained immunity impacts urinary tract disease outcome. Nat Microbiol 2023, 8, 875–888. [Google Scholar] [CrossRef]
- Eldrup, J.; Thorup, J.; Nielsen, S.L.; Hald, T.; Hainau, B. Permeability and ultrastructure of human bladder epithelium. Br J Urol 1983, 55, 488–492. [Google Scholar] [CrossRef]
- Staehelin, L.A.; Chlapowski, F.J.; Bonneville, M.A. Lumenal plasma membrane of the urinary bladder. I. Three-dimensional reconstruction from freeze-etch images. J Cell Biol 1972, 53, 73–91. [Google Scholar] [CrossRef]
- Volter, D.; Schmidt, B. The reabsorption of creatinine from the rabbit bladder. Urol Res 1975, 3, 183–186. [Google Scholar] [CrossRef]
- Islam, M.M.; Takeyama, N. Role of Neutrophil Extracellular Traps in Health and Disease Pathophysiology: Recent Insights and Advances. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol 2015, 13, 269–284. [Google Scholar] [CrossRef]
- Krivosikova, K.; Supcikova, N.; Gaal Kovalcikova, A.; Janko, J.; Pastorek, M.; Celec, P.; Podracka, L.; Tothova, L. Neutrophil extracellular traps in urinary tract infection. Front Pediatr 2023, 11, 1154139. [Google Scholar] [CrossRef]
- Schmidt, E.P.; Overdier, K.H.; Sun, X.; Lin, L.; Liu, X.; Yang, Y.; Ammons, L.A.; Hiller, T.D.; Suflita, M.A.; Yu, Y.; et al. Urinary Glycosaminoglycans Predict Outcomes in Septic Shock and Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med 2016, 194, 439–449. [Google Scholar] [CrossRef]
- Mambatta, A.K.; Jayarajan, J.; Rashme, V.L.; Harini, S.; Menon, S.; Kuppusamy, J. Reliability of dipstick assay in predicting urinary tract infection. J Family Med Prim Care 2015, 4, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Bogovic Crncic, T.; Girotto, N.; Ilic Tomas, M.; Kristofic, I.; Klobucar, S.; Baticic, L.; Curko-Cofek, B.; Sotosek, V. Innate Immunity in Autoimmune Thyroid Disease during Pregnancy. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Lurie, S.; Rahamim, E.; Piper, I.; Golan, A.; Sadan, O. Total and differential leukocyte counts percentiles in normal pregnancy. Eur J Obstet Gynecol Reprod Biol 2008, 136, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Feng, C.; Zhang, X.; Lu, J.; Zhao, Y. The Diverse Biological Functions of Neutrophils, Beyond the Defense Against Infections. Inflammation 2017, 40, 311–323. [Google Scholar] [CrossRef]
- Tyagi, P.; Motley, S.S.; Koyama, T.; Kashyap, M.; Gingrich, J.; Yoshimura, N.; Fowke, J.H. Molecular correlates in urine for the obesity and prostatic inflammation of BPH/LUTS patients. Prostate 2018, 78, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Durkin, M.J.; Schmitz, V.; Hsueh, K.; Troubh, Z.; Politi, M.C. Older adults' and caregivers' perceptions about urinary tract infection and asymptomatic bacteriuria guidelines: a qualitative exploration. Antimicrob Steward Healthc Epidemiol 2023, 3, e224. [Google Scholar] [CrossRef] [PubMed]
- Saito, T.; Hitchens, T.K.; Foley, L.M.; Singh, N.; Mizoguchi, S.; Kurobe, M.; Gotoh, D.; Ogawa, T.; Minagawa, T.; Ishizuka, O.; et al. Functional and histologic imaging of urinary bladder wall after exposure to psychological stress and protamine sulfate. Sci Rep 2021, 11, 19440. [Google Scholar] [CrossRef] [PubMed]
- Veranic, P.; Jezernik, K. Succession of events in desquamation of superficial urothelial cells as a response to stress induced by prolonged constant illumination. Tissue Cell 2001, 33, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Tyagi, P.; Tyagi, V.; Yoshimura, N.; Witteemer, E.; Barclay, D.; Loughran, P.A.; Zamora, R.; Vodovotz, Y. Gender-based reciprocal expression of transforming growth factor-beta1 and the inducible nitric oxide synthase in a rat model of cyclophosphamide-induced cystitis. J Inflamm (Lond) 2009, 6, 23. [Google Scholar] [CrossRef]
- Tyagi, P.; Moon, C.H.; Connell, M.; Ganguly, A.; Cho, K.J.; Tarin, T.; Dhir, R.; Sholosh, B.; Maranchie, J. Intravesical Contrast-Enhanced MRI: A Potential Tool for Bladder Cancer Surveillance and Staging. Curr Oncol 2023, 30, 4632–4647. [Google Scholar] [CrossRef]
- Asemota, A.O.; Schneider, E.B.; Mowry, E.M.; Venkatesan, A. Common comorbid and secondary conditions leading to hospitalization in multiple sclerosis patients in the United States. Clin Neurol Neurosurg 2023, 232, 107851. [Google Scholar] [CrossRef]
- Seok, J.; Warren, H.S.; Cuenca, A.G.; Mindrinos, M.N.; Baker, H.V.; Xu, W.; Richards, D.R.; McDonald-Smith, G.P.; Gao, H.; Hennessy, L.; et al. Genomic responses in mouse models poorly mimic human inflammatory diseases. Proc Natl Acad Sci U S A 2013, 110, 3507–3512. [Google Scholar] [CrossRef]
- Wang, C.; Bauckman, K.A.; Ross, A.S.B.; Symington, J.W.; Ligon, M.M.; Scholtes, G.; Kumar, A.; Chang, H.W.; Twentyman, J.; Fashemi, B.E.; et al. A non-canonical autophagy-dependent role of the ATG16L1(T300A) variant in urothelial vesicular trafficking and uropathogenic Escherichia coli persistence. Autophagy 2019, 15, 527–542. [Google Scholar] [CrossRef]
- Staerk, K.; Gronnemose, R.B.; Palarasah, Y.; Lund, L.; Andersen, T.E. Intracellular uropathogenic Escherichia coli are undetectable in urinary bladders after oral mecillinam treatment: An experimental study in a pig model of cystitis. Microb Pathog 2022, 173, 105817. [Google Scholar] [CrossRef] [PubMed]
- Tyagi, P.; Moon, C.; Singh, N.; Connell, M.; Maranchie, J.; Chermansky, C.; Yoshimura, N.; Kaufman, J. High Resolution 3D T1-Mapping of Pig Bladder Wall by Intravesical Contrast Enhanced MRI At 3T. J Urol 2021, 206, e390. [Google Scholar] [CrossRef]
- Tartaglione, T.A.; Johnson, C.R.; Brust, P.; Opheim, K.; Hooton, T.M.; Stamm, W.E. Pharmacodynamic evaluation of ofloxacin and trimethoprim-sulfamethoxazole in vaginal fluid of women treated for acute cystitis. Antimicrob Agents Chemother 1988, 32, 1640–1643. [Google Scholar] [CrossRef] [PubMed]
- Mores, C.R.; Price, T.K.; Wolff, B.; Halverson, T.; Limeira, R.; Brubaker, L.; Mueller, E.R.; Putonti, C.; Wolfe, A.J. Genomic relatedness and clinical significance of Streptococcus mitis strains isolated from the urogenital tract of sexual partners. Microb Genom 2021, 7. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.T.; Han, D.E.; Lee, D.H.; Kim, J.W.; Park, H.S.; Moon, D.G.; Oh, M.M. Single-dose amikacin plus 7 days of amoxicillin/clavulanate to treat acute cystitis caused by extended-spectrum beta-lactamase-producing Escherichia coli: A retrospective cohort study. Investig Clin Urol 2021, 62, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Periasamy, S.; Joo, H.S.; Duong, A.C.; Bach, T.H.; Tan, V.Y.; Chatterjee, S.S.; Cheung, G.Y.; Otto, M. How Staphylococcus aureus biofilms develop their characteristic structure. Proc Natl Acad Sci U S A 2012, 109, 1281–1286. [Google Scholar] [CrossRef]
- Avery, O.T.; Macleod, C.M.; McCarty, M. Studies on the Chemical Nature of the Substance Inducing Transformation of Pneumococcal Types : Induction of Transformation by a Desoxyribonucleic Acid Fraction Isolated from Pneumococcus Type Iii. J Exp Med 1944, 79, 137–158. [Google Scholar] [CrossRef] [PubMed]
- Duployez, C.; Loiez, C.; Cattoen, C.; Descamps, D.; Wallet, F.; Vachee, A.; Microbiologist Network from, N.-P.-d.-C. In vitro susceptibility to mecillinam of Escherichia coli strains isolated from the urine of pregnant women. Med Mal Infect 2016, 46, 436–441. [Google Scholar] [CrossRef]
- Huttner, A.; Wijma, R.A.; Stewardson, A.J.; Olearo, F.; Von Dach, E.; Harbarth, S.; Bruggemann, R.J.M.; Mouton, J.W.; Muller, A.E. The pharmacokinetics of nitrofurantoin in healthy female volunteers: a randomized crossover study. J Antimicrob Chemother 2019, 74, 1656–1661. [Google Scholar] [CrossRef]
- Hirai, T.; Shiraishi, C.; Nakai, S.; Ushiro, M.; Hanada, K.; Iwamoto, T. Population kinetic-pharmacodynamic analysis of serum potassium in patients receiving sulfamethoxazole/trimethoprim. Basic Clin Pharmacol Toxicol 2022, 131, 380–391. [Google Scholar] [CrossRef]
- Sadahiro, S.; Ishida, H.; Suzuki, T.; Ishikawa, K.; Tajima, T.; Makuuchi, H. Vesicular blood flow after ligation of the internal iliac arteries in low anterior resection or abdominoperineal resection. Dis Colon Rectum 1999, 42, 1475–1479. [Google Scholar] [CrossRef]
- Parmelee, D.J.; Walovitch, R.C.; Ouellet, H.S.; Lauffer, R.B. Preclinical evaluation of the pharmacokinetics, biodistribution, and elimination of MS-325, a blood pool agent for magnetic resonance imaging. Invest Radiol 1997, 32, 741–747. [Google Scholar] [CrossRef]
- Zhang, H. Trisodium-[(2-(R)-[(4,4-diphenylcyclohexyl)phosphono-oxymethyl]-diethylenetriaminepentaacetato)(aquo)gadolinium(III): Gadofosveset. In Molecular Imaging and Contrast Agent Database (MICAD); Bethesda (MD), 2004.
- Miodonski, A.J.; Litwin, J.A. Microvascular architecture of the human urinary bladder wall: a corrosion casting study. Anat Rec 1999, 254, 375–381. [Google Scholar] [CrossRef]
- Smith, S.G.; Griffith, B.E.; Zaharoff, D.A. Analyzing the effects of instillation volume on intravesical delivery using biphasic solute transport in a deformable geometry. Math Med Biol 2019, 36, 139–156. [Google Scholar] [CrossRef]
- Lee, P.J.; Kuo, H.C. High incidence of lower urinary tract dysfunction in women with recurrent urinary tract infections. Low Urin Tract Symptoms 2020, 12, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Tyagi, P.; Ganguly, A.; Chermansky, C.; Tarin, T.V.; Yoshimura, N.; Maranchie, J. Does large volume of distribution of lidocaine masks its systemic uptake from bladder? Am J Clin Exp Urol 2023, 11, 121–135. [Google Scholar]
- Sumi, C.D.; Heffernan, A.J.; Lipman, J.; Roberts, J.A.; Sime, F.B. What Antibiotic Exposures Are Required to Suppress the Emergence of Resistance for Gram-Negative Bacteria? A Systematic Review. Clin Pharmacokinet 2019, 58, 1407–1443. [Google Scholar] [CrossRef]
- Mouhssine, M.; Al Ani, D.; Al Shibli, A.; Ghatasheh, G.; Al Amri, A.; Matta, H.; Chedid, R.; Narchi, H. Intravesical gentamicin instillation in the prevention of recurrent urinary tract infections in children with neurogenic bladder- a single-center retrospective observational study. J Pediatr Urol 2023, 19, 64 e61-64 e67. [Google Scholar] [CrossRef] [PubMed]
- Zoqlam, R.; Lazauskaite, S.; Glickman, S.; Zaitseva, L.; Ilie, P.C.; Qi, S. Emerging molecular mechanisms and genetic targets for developing novel therapeutic strategies for treating bladder diseases. Eur J Pharm Sci 2022, 173, 106167. [Google Scholar] [CrossRef]
- Alpers, D.H.; Tomkins, G.M. The Order of Induction and Deinduction of the Enzymes of the Lactose Operon in E. Coli. Proc Natl Acad Sci U S A 1965, 53, 797–802. [Google Scholar] [CrossRef]
- Alou, L.; Aguilar, L.; Sevillano, D.; Gimenez, M.J.; Cafini, F.; Valero, E.; Relano, M.T.; Prieto, J. Urine bactericidal activity against resistant Escherichia coli in an in vitro pharmacodynamic model simulating urine concentrations obtained after 2000/125 mg sustained-release co-amoxiclav and 400 mg norfloxacin administration. J Antimicrob Chemother 2006, 57, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhou, L.; Unadkat, J.D.; Mao, Q. Effect of pregnancy on nitrofurantoin disposition in mice. J Pharm Sci 2009, 98, 4306–4315. [Google Scholar] [CrossRef]
- Ma, Q.; Gao, Y.; Lu, J.; Liu, X.; Wang, R.; Shi, Y.; Liu, J.; Su, H. The effect of regular aerobic exercise on renal function in patients with CKD: A systematic review and meta-analysis. Front Physiol 2022, 13, 901164. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, C.; Michanek, P.; Salomonsson, M.; Tegner, C.; Pelander, L. Nitrofurantoin plasma- and urine exposure in eight healthy beagle dogs following standard nitrofurantoin dosing regimen. Res Vet Sci 2022, 152, 150–155. [Google Scholar] [CrossRef]
- Parekh, S.; Hayes, C.V.; Loader, J.; Ashiru-Oredope, D.; Hand, K.; Hicks, G.; Lecky, D. The Use of the TARGET Antibiotic Checklist to Support Antimicrobial Stewardship in England's Community Pharmacies. Antibiotics (Basel) 2023, 12. [Google Scholar] [CrossRef]
- NICE antimicrobial stewardship: right drug, dose, and time? Lancet 2015, 386, 717. [CrossRef] [PubMed]
- Morris, C.J.; Rohn, J.L.; Glickman, S.; Mansfield, K.J. Effective Treatments of UTI-Is Intravesical Therapy the Future? Pathogens 2023, 12. [Google Scholar] [CrossRef]
- Andretta, E.; Longo, R.; Balladelli, M.; Sgarabotto, C.; Sgarabotto, D. Intravesical Gentamicin: An Option for Therapy and Prophylaxis against Recurrent UTIs and Resistant Bacteria in Neurogenic Bladder Patients on Intermittent Catheterization. Antibiotics (Basel) 2022, 11. [Google Scholar] [CrossRef]
- Bilsen, M.P.; van Uhm, J.I.M.; Stalenhoef, J.E.; van Nieuwkoop, C.; Groenwold, R.H.H.; Visser, L.G.; Lambregts, M.M.C. Intravesical aminoglycoside instillations as prophylaxis for recurrent urinary tract infection: patient satisfaction, long-term safety and efficacy. JAC Antimicrob Resist 2023, 5, dlad040. [Google Scholar] [CrossRef]
- Rieger, M.M.; Shah, N.M.; Ferrante, K.L.; Tan-Kim, J.; Jacobs, M.B.; Brubaker, L.; Alperin, M. Intraoperative Gentamicin Intravesical Instillation for Prevention of Urinary Tract Infection After Urogynecologic Surgery: A Randomized Controlled Trial. Urogynecology (Phila) 2022, 28, 825–833. [Google Scholar] [CrossRef]
- Rahnama'i, M.S.; Javan Balegh Marand, A.; Roschmann-Doose, K.; Steffens, L.; Arendsen, H.J. The efficacy and safety of intravesical chondroitin sulphate solution in recurrent urinary tract infections. BMC Urol 2022, 22, 188. [Google Scholar] [CrossRef] [PubMed]
- Gugliotta, G.; Calagna, G.; Adile, G.; Polito, S.; Saitta, S.; Speciale, P.; Palomba, S.; Perino, A.; Granese, R.; Adile, B. Is intravesical instillation of hyaluronic acid and chondroitin sulfate useful in preventing recurrent bacterial cystitis? A multicenter case control analysis. Taiwan J Obstet Gynecol 2015, 54, 537–540. [Google Scholar] [CrossRef] [PubMed]
- King, G.K.; Goodes, L.M.; Hartshorn, C.; Thavaseelan, J.; Jonescu, S.; Watts, A.; Rawlins, M.; Woodland, P.; Synnott, E.L.; Barrett, T.; et al. Intravesical hyaluronic acid with chondroitin sulphate to prevent urinary tract infection after spinal cord injury. J Spinal Cord Med 2023, 46, 830–836. [Google Scholar] [CrossRef] [PubMed]
- Bosch, B.; Hartikainen, A.; Ronkainen, A.; Scheperjans, F.; Arkkila, P.; Satokari, R. Development of a Protocol for Anaerobic Preparation and Banking of Fecal Microbiota Transplantation Material: Evaluation of Bacterial Richness in the Cultivated Fraction. Microorganisms 2023, 11. [Google Scholar] [CrossRef]
- Frimodt-Moller, N.; Bjerrum, L. Treating urinary tract infections in the era of antibiotic resistance. Expert Rev Anti Infect Ther 2023, 21, 1301–1308. [Google Scholar] [CrossRef]
Figure 4.
Panel A - Intravesical antimicrobial therapy (IAT) delivers a bactericidal dose to microbial colonies invading the bladder without the delay associated with OAT. Exposure to the high dose does not give as much time for the activation of AMR and proliferation of resistant colonies. Panel B - Projected plots for serum and urine levels after a single intravesical dose of aminoglycoside (Gentamicin) for cystitis reveals an absence of delay in reaching MIC and delivering a lethal blow to microbes with concomitant low plasma levels- owing to the poor systemic absorption-avoids the renal and ototoxicity. Notice the log-scale of the y-axis.
Figure 4.
Panel A - Intravesical antimicrobial therapy (IAT) delivers a bactericidal dose to microbial colonies invading the bladder without the delay associated with OAT. Exposure to the high dose does not give as much time for the activation of AMR and proliferation of resistant colonies. Panel B - Projected plots for serum and urine levels after a single intravesical dose of aminoglycoside (Gentamicin) for cystitis reveals an absence of delay in reaching MIC and delivering a lethal blow to microbes with concomitant low plasma levels- owing to the poor systemic absorption-avoids the renal and ototoxicity. Notice the log-scale of the y-axis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



