
Submitted:
19 January 2024
Posted:
19 January 2024
You are already at the latest version
Abstract
Keywords: renal replacement therapy. Point-of-Care Ultrasound; intensive care; acute kidney injury; nephrologist.Point of care ultrasonography (POCUS) is gaining heightened significance in critical care settings as it allows for quick decision making at the bedside. While computerized to-mography is still considered the standard imaging modality for many diseases, the risks and delays associated with transferring a critically ill patient out of the Intensive Care Unit (ICU) have prompted physicians to explore alternative tools. Ultrasound guidance has increased safety of invasive procedures in the ICU, such as the placement of vascular catheters and drainage of collections. Ultrasonography is now seen as an extension of the clinical examination, providing quick answers for rapidly deteriorating patients in the ICU. The field of nephrology is increasingly acknowledging the value of diagnostic Point-of-Care Ultrasound (POCUS). By employing multi-organ POCUS, nephrologists can address specific queries arising during the diagnosis and treatment of patients with acute kidney injury. This approach aids in ruling out hydronephrosis and offering immediate information on hemodynamics, thereby consolidating patient data and facilitating the development of personalized treatment strategies.
Keywords:
renal replacement therapy
; Point-of-Care Ultrasound
; intensive care
; acute kidney injury
1. Introduction
The incidence of acute kidney injury (AKI) requiring renal replacement therapy (RRT) has significantly increased over the years, affecting up to 15% of critically ill patients.(1–3) Intradialytic hypotension (IDH) has been found to complicate 10-70% of intermittent hemodialysis sessions, around 40-60% of sustained low-efficiency dialysis sessions, and 19-43% of continuous renal replacement therapy treatments. While the association between intradialytic hypotension and adverse outcomes is unclear, studies on critically ill patients have shown a higher mortality rate and impaired renal recovery in those who experience IDH.(4–6) Additionally, critically ill patients treated with vasopressors for shock often experience significant and prolonged relative hypotension, which is associated with poor kidney-related outcomes. (7)There is no definitive evidence supporting the routine use of any specific intervention to prevent IDH, as its causes are multifactorial and include both the dialysis process itself and factors related to critically ill patients(8).The combination of decreased blood volume and impaired vascular resistance, along with reduced cardiovascular reserve, can lead to hemodynamic instability. Furthermore, the dialysis process has the potential to disrupt compensatory mechanisms, increasing the risk of hypotension. Point-of-Care Ultrasonography (POCUS) is now used in many clinical settings to enhance patients’ management. Assessment of predialytic cardiopulmonary profiles, defined on sonographic findings, could facilitate IDH prediction and is emerging as part of critically ill patients’ bedside evaluation. Additionally, several other patient-related factors, such as baseline cardiac dysfunction, vascular tone, and impaired compensatory responses, can contribute to IDH. Therefore, bedside ultrasound for cardiovascular performance assessment serves as a valuable tool for conducting a comprehensive evaluation of patients requiring renal replacement therapy. In this review, we discuss the rationale behind nephrologists performing POCUS, explain the fundamental principles of focused ultrasonography, and provide our expert perspective on its effectiveness for delineating and comprehending the mechanisms of hypotension in patients undergoing renal replacement therapy (RRT). We also discuss how POCUS can contribute to personalize resuscitation and improve patient outcomes.
- The Use of Point-of-Care Ultrasound in the Field of Acute Care Nephrology
Caring for acutely ill patients with AKI who are undergoing RRT can be extremely difficult. The nephrologist is tasked not only with managing the kidney disease and dialysis procedure itself, but also addressing all the consequences that arise from the disrupted balance within the body. The use of POCUS has expanded significantly(Figure 1) and has become an effective tool in diagnosing the cause of renal dysfunction, identifying pulmonary infiltrates, and assessing volume and acute circulatory failure in these patients.(9,10) Despite its clear benefits and acceptance in other medical fields, POCUS is still not widely used by nephrologists.(11) The reasons for this are not clear, but it may be due to a lack of exposure and expertise during training, time constraints for busy nephrologists, and a lack of standardized protocols for using POCUS. However, there has been a recent increase in interest among nephrologists, and POCUS training is now being incorporated into fellowship programs.(12) This adoption of POCUS by nephrologists will provide them with a valuable tool that can greatly impact the management of AKI patients.
- Lung Ultrasonography for Nephrologists
Nephrologists and AKI patients struggle to control volume overload and its complications. However, traditional physical examination signs of volume overload, such as rales and edema, are not reliable indicators of pulmonary congestion.(14) The reliable detection of pulmonary congestion holds potential for predicting the need for additional ultrafiltration. (13) From a technical perspective, the appearance of normal lung structure is hindered by reverberation artifacts caused by the density difference between skin and soft tissue (water density) and the alveolar sac (air density) in ultrasound images.(15) In healthy individuals, the lung exhibits a pattern of horizontal reflections called the A-line pattern. As pulmonary congestion increases, this pattern shifts to a vertically oriented B-line pattern. B-lines manifest as hyperechoic lines extending to the ultrasound field's edge, moving synchronously with respiration. Quantifying pulmonary congestion involves counting B-lines across multiple intercostal spaces, with the 8-zone anterior lung ultrasound being the most validated method for research.(16) The more B-lines counted, the greater the pulmonary congestion, which correlates with extravascular lung water.(17) Quantitative lung ultrasound has shown good reliability and agreement among different ultrasound transducers. The optimal images are obtained by setting the focal depth at the pleural line, increasing gain in the far field, and turning off harmonics. Lung ultrasound surpasses physical examination and chest x-ray in predicting acute cardiogenic pulmonary edema.(18) It is also sensitive in detecting pleural effusions, which appear as anechoic structures between the lung and diaphragm. Lung ultrasound can be easily taught using a remote, web-based application and can be incorporated into outpatient care. The Lung Ultrasound Score (LUS) is a tool that has gained traction among nephrologists for its utility in assessing and managing patients with kidney diseases. This scoring system is based on the quantification of B-lines with a quick eight-zone protocol (Figure 2) that can be complete under two minutes.(19) . The LUS is particularly relevant in nephrology for evaluating fluid status in patients with conditions like chronic kidney disease (CKD) and end-stage renal disease (ESRD), where fluid overload is a common and serious complication. In practice, the lung is divided in eight zones and each zone is scored based on the number and intensity of B-lines observed. The cumulative score provides a semi-quantitative assessment of lung water, which correlates with the degree of pulmonary congestion. This method offers a more nuanced and precise approach to fluid management compared to traditional methods like physical examination or chest X-ray, particularly in dialysis patients where accurate assessment of dry weight is crucial. It is non-invasive, radiation-free, and can be performed at the bedside with portable ultrasound machines. This makes it an ideal tool for real-time monitoring and decision-making in both acute and chronic care settings. However, the accuracy of LUS depends on the operator's skill and experience, highlighting the need for adequate training and standardization in its application.
- Cardiac Ultrasonography for Nephrologists
The main goal of basic cardiac ultrasonography is to provide succinct and targeted qualitative assessments that aid in guiding management decisions. This non-invasive imaging technique is particularly valuable in assessing left ventricular hypertrophy, cardiac chamber sizes, valvular heart disease, and systolic and diastolic function – all of which are common in CKD patients. It also plays a crucial role in evaluating fluid status and cardiac output, essential in managing fluid overload, a frequent challenge in dialysis patients. Moreover, regular cardiac ultrasonography can help in the early detection of cardiovascular diseases, allowing for timely intervention. This is vital since traditional cardiovascular risk factors often do not fully explain the high incidence of heart disease in CKD patients. The cognitive skills needed include assessing the overall size and function of the left ventricle, distinguishing between segmental and global wall motion abnormalities, evaluating the size and function of the right ventricle, and identifying severe valvular dysfunction using color Doppler.(20) Basic cardiac ultrasonography helps in accurately categorizing shock and identifying potentially life-threatening causes of shock, which is not uncommon in critically ill patients evaluated by nephrologists.(21) It can quickly determine if there is evidence of hypovolemia, a pericardial effusion, or cardiac tamponade. The presence of an enlarged right ventricle may indicate acute cor pulmonale and impending right ventricular failure(22).
- Abdominal Ultrasonography for Nephrologists
One of the primary applications of abdominal ultrasound in nephrology is the assessment of chronic kidney disease (CKD). It helps in determining the size and echogenicity of the kidneys, which can provide insights into the chronicity and etiology of renal impairment. Smaller, echogenic kidneys are often indicative of chronic irreversible damage. Additionally, Doppler ultrasound can assess renal blood flow, aiding in the diagnosis of renal artery stenosis, a potentially treatable cause of hypertension and kidney failure.In acute kidney injury (AKI), abdominal ultrasound helps in differentiating pre-renal, renal, and post-renal causes. It can identify obstructions in the urinary tract, such as stones or clots, and can also detect conditions like hydronephrosis. It can also guide percutaneous procedures, like kidney biopsies or the placement of dialysis catheters, reducing the risk of complications. Furthermore, abdominal ultrasonography is beneficial in screening for renal malignancies and in the follow-up of renal transplant patients. It can monitor graft size, detect complications like collections or obstruction, and assess vascular anastomoses.
The contribution of venous congestion to kidney disfunction is increasingly being acknowledged hence unresoled congestion is linked to unfavorable kidney outcomes in patients with heart failure.(23). Similarly, any condition that results in elevated central venous pressure, such as pulmonary hypertension, can lead to impaired kidney perfusion by increasing cardiac afterload. POCUS allows clinicians to objectively evaluate hemodynamics at the bedside, thereby guiding patient management. Although inferior vena cava (IVC) POCUS is employed to estimate right atrial pressure, it cannot demonstrate organ congestion and bears several limitations, including influence of ventilation settings, patient’s inspiratory efforts, coexisting cardiac conditions and intra-abdominal hypertension.(23,24) Recently, venous excess Doppler ultrasound has emerged as a real-time tool to assess venous congestion at the organ level. (24,25) Severe flow abnormalities in hepatic, portal, and kidney parenchymal veins have been shown to predict the risk of congestive kidney injury and aid in monitoring the efficacy of decongestive therapy.(26) Herein, we provide a brief overview of the various components of venous excess Doppler ultrasound and share our perspective on incorporating this innovative tool in nephrology practice.
- POCUS in Hemodynamic Instability during Acute Kidney Injury and Acute Renal Replacement Therapy
Hemodynamic instability is a prevalent condition in critical illness and can have a significant impact on patient outcomes in the ICU. This instability can interfere with tissue perfusion and oxygen delivery, leading to multiorgan dysfunction. AKI is also frequently observed in critically ill patients and can further aggravate patient outcomes. Hypotension and AKI] are often associated through direct and indirect mechanisms, with both conditions potentially stemming from a single underlying cause of organ damage. Approximately 10-20% of ICU patients with AKI require acute RRT, and their expected mortality rate is nearly 50%.(27)The epidemiological and pathophysiological correlation between hypotension and RRT is acknowledged albeit a clear definition of hemodynamic instability during RRT remains elusive. Reports on critically ill patients indicate that IDH is linked to increased mortality and compromised renal recovery. POCUS assessment can provide nephrologists with hemodynamic parameters that can be targeted and integrated to organ perfusion surrogates to potentially yield best results.(28–31) The utilization of POCUS in revealing these mechanisms holds significant implications for the management of patients, as reducing ultrafiltration may not always be the optimal course of action, particularly in instances of substantial fluid overload.(32)
- 1)
- Pre-Load Dependence and POCUS
Ultrasound has emerged as a crucial tool for assessing volume status and response to volume resuscitation in critically ill patients. Its non-invasive nature and low cost makes it an attractive option, and clinicians can perform repeat ultrasounds at the patient’s bedside as needed. Extensive research has focused on the elasticity of large veins, including the IVC and internal jugular vein, to determine standardized parameters for fluid responsiveness, such as the collapsibility index.(33) These parameters are linked to traditional predictors of fluid responsiveness, such as central venous pressure.(34). Recent studies have shown that large arteries, such as the common carotid artery, are also dynamically compliant and can predict fluid responsiveness.(35) However, it is important to note that ultrasound interpretation is operator-dependent. To address this issue, standardized parameters like angulation probe and corrected flow time can be calculated using ultrasound, potentially minimizing discrepancies in image interpretation among providers.(36)
- 2)
- Ventricule arterial Couplling and POCUS
The concept that optimal cardiovascular performance is achieved when the heart and arterial system are coupled has been well established through various studies.(37) When the heart pumps blood into the vascular tree at a rate and volume that matches the capability of the arterial system to receive it, both cardiovascular performance and its associated cardiac energetics are optimized. Deviations from this optimal state, such as high or, low contractility, or arterial tone, can lead to cardiac failure, independent of other disease processes. Ventriculo-arterial coupling (VAC) analysis quantifies the optimal matching of left ventricular workload and arterial system, with minimal changes in left ventricular (LV) pressure and complete transfer of mechanical energy from the ventricle to the arterial system.(38) The role of VAC in managing critically ill patients with severe hemodynamic instability and shock is increasingly recognized. VAC is calculated as the ratio of arterial elastance (Ea) to ventricular elastance (Ees), proposed by Suga(39)as a measure of cardiovascular mechanical efficiency and interaction between cardiac performance and vascular function. The Ea/Ees ratio(39) is a reliable and effective measure of cardiovascular performance, with optimal efficiency achieved when the ratio is near 1. VAC is an effective index of LV mechanical performance and dynamic modulation of the cardiovascular system(40), reflecting cardiac energetics as well. The balance between myocardial oxygen consumption and mechanical energy required for cardiac work is optimal when the heart and peripheral vascular system are coupled. The area of the LV pressure-volume (P-V) loop during a single cardiac cycle represents the total mechanical energy of the heart during that beat and correlates linearly with myocardial oxygen consumption. Understanding VAC requires knowledge of the determinants Ea and Ees, and their bedside measurement in critically ill patients. LV contractile function can be evaluated by the relationship between end-systolic pressure (ESP) and end-systolic volume(Figure 3). Non-invasive measurement approaches for measuring VACg have been developed(41), with the modified single beat method validated against invasive measurement of Ees. This method utilizes echocardiographic measures of LV end-diastolic and end-systolic areas, LVEF, stroke volume, pre-ejection time, and systolic time interval, coupled with systolic and diastolic arterial pressure measurements. Ea is calculated as ESP/stroke volume or 0.9 × systolic arterial pressure/stroke volume. These measures can be readily obtained at the bedside for assessing VAC in critically ill patients. Overall, the resuscitation algorithm for critically ill patients on RRT is a dynamic process, requiring continuous reassessment and adjustment based on the patient's evolving clinical status. It underscores the importance of a balanced approach to fluid management and hemodynamic support to optimize patient outcomes.
- 3)
- Myocardial function and POCUS
Several studies have been conducted to evaluate the accuracy of left ventricular assessment by non-cardiologists in detecting left ventricular systolic dysfunction after varying training programs.(42–44)These studies have demonstrated good sensitivity in determining left ventricular function at the extreme ends, such as assessing a left ventricular ejection fraction (LVEF) above or below 50% (sensitivity 74-95%) and an LVEF above or below 30% (sensitivity 100%).(45) This indicates that even with limited training, physicians, residents, and medical students can accurately differentiate between normal and abnormal and severe and non-severely impaired left ventricular systolic function. With more extensive training, the sensitivity and specificity of determining the specific degree of left ventricular dysfunction improve(Figure 4).
It has been demonstrated that focused cardiac ultrasound(46), even in the hands of novice users, is superior to clinical examination by experts in identifying cardiac abnormalities. For example, Kobal et al.(47) found that after 18 hours of training, two first-year medical students correctly detected 75% of the 239 abnormal findings on formal echocardiography with a specificity of 87% compared to 49% (specificity 76%) identified by five experienced cardiologists. Such results were obtained even with the inclusion of patients who are frequently challenging to image, as 33% were in ICU environment, 28% had atrial fibrillation, and 11% had chronic lung disease. Similarly, when comparing only severe pathology (LVEF ≤35% or severe valve pathology), the cardiologists identified only 68% compared with the 96% identified by the students using hand-carried ultrasound. Comparable sensitivity has been demonstrated when comparing cardiologists using hand-held ultrasound (HHU) only with cardiologists performing physical examination alone in patients referred for routine outpatient transthoracic echocardiography. In this study, the HHU group identified 82% of the abnormalities whereas the physical exam group identified only 47%.
In another study(48) the use of POCUS by non-cardiologist physicians was examined for its potential to enhance the assessment of cardiac abnormalities compared to physical examination alone. Ten hospitalists examined 354 general medical inpatients and then performed POCUS as part of a focused training program in hand-held echocardiography compared formal echocardiography exam. Overall, POCUS improved the diagnostic accuracy for determining LV dysfunction, cardiomegaly, and pericardial effusions, which was most significant in patients where an abnormality was present. However, interestingly, HHU did not perform similarly with valvular disease as the hospitalists were more likely to overcall the presence and degree of aortic and mitral regurgitation. This highlights the importance of proper training and supervision in the use of POCUS and HHU for accurate diagnosis and management of cardiac abnormalities. However, it's important to note that while POCUS is a powerful tool, it requires specific skills and training. Interpretation of findings must be done within the clinical context, and when necessary, collaboration with cardiologists for comprehensive evaluation and management is recommended.
- 4)
- Systemic venous congestion and POCUS
Traditional methods of assessing fluid status and cardiac function often fall short in accurately identifying venous congestion, a condition that can lead to organ dysfunction and worsened prognosis in critically ill patients.(49) The Venous Excess Ultrasound (VExUS) score emerges as a promising tool in this context. VExUS is an ultrasound-based scoring system that assesses venous congestion by examining the IVC, hepatic vein (HV), portal vein (PV), and intra-renal venous (IRV) Doppler waveforms(Figure 5). This approach provides a more comprehensive understanding of the patient's resuscitation strategy, incorporating the concept of fluid tolerance (FT).(50) VExUS can guide clinicians in making more informed decisions regarding fluid administration, deresuscitation, and potentially preventing the progression of kidney dysfunction. Recent studies incorporating VExUS into critical care protocols have shown that patients with reduced scores over 48 hours and higher doses of diuretics had significantly more RRT-free days in 28 days. (51)The ability of VExUS to non-invasively and dynamically assess venous congestion offers a significant advantage over traditional hemodynamic monitoring techniques, which often fail to detect subtle changes in venous return and congestion. The application of VExUS has been associated with the prognostication of AKI in patients with cardiorenal syndrome, aiding in the clinical decision to perform fluid removal.(52)Furthermore, VExUS-guided fluid management has the potential to personalize and optimize fluid therapy, moving beyond the 'one-size-fits-all' approach.(53) This personalized management is particularly beneficial in the heterogeneous population of critically ill patients, where the physiological response to illness and therapy can vary markedly.
Conclusions
Hemodynamic instability is a frequent condition in critically ill patients undergoing RRT and is associated with increased mortality rates and potential impairment of renal recovery. While excessive ultrafiltration is a known cause of hypotension, it may not always constitute the primary underlying mechanism. Multiple other RRT-related factors can contribute to decreased cardiac output, decreased peripheral resistance, or both. In the management of patients requiring RRT, POCUS plays a crucial role in the initial diagnostic assessment of hemodynamically unstable patients, as well as in monitoring the outcomes of therapeutic interventions. We strongly advocate for the incorporation of POCUS into the standard of care for all nephrologists and urge hospitals to provide the necessary resources to support a successful program.
Author Contributions
R.P and U.A.P.F : literature search, figures U.A.P.F, data collection P.S and C.P , writing R.P and R.C, drafting and critically revising the manuscript for important intellectual content B.B and B.C; and acquisition, analysis, and interpretation of the data T.D.C and D.S.B and F.G drafting and critically revising the manuscript for important intellectual content F.O.C. All authors have read and agreed to the published version of the manuscript.
Funding
All co-authors agree that the research did not receive any specific funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
This paper and the research behind it would not have been possible without the exceptional support of Hospital Israelita Albert Einstein and Critical Care Department HIAE.
Conflicts of Interest
All authors declare no conflicts of interest.
References
- Vanholder, R.; Annemans, L.; Braks, M.; Brown, E.A.; Pais, P.; Purnell, T.S.; Sawhney, S.; Scholes-Robertson, N.; Stengel, B.; Tannor, E.K.; et al. Inequities in kidney health and kidney care. Nat. Rev. Nephrol. 2023, 19, 694–708. [Google Scholar] [CrossRef] [PubMed]
- Griffin, B.R.; Liu, K.D.; Teixeira, J.P. Critical Care Nephrology: Core Curriculum 2020. Am. J. Kidney Dis. 2020, 75, 435–452. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, P.J.; Crippa, I.A.; Sannier, A.; Koopmansch, C.; Bienfait, L.; Allard, J.; Sexton, D.J.; Fontana, V.; Rorive, S.; Vincent, J.-L.; et al. Critically ill patients with acute kidney injury: clinical determinants and post-mortem histology. Clin. Kidney J. 2023, 16, 1664–1673. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, A.B.; Vehbi, S.; Covic, A.; Burlacu, A.; Covic, A.; Kanbay, M. An update review on hemodynamic instability in renal replacement therapy patients. Int. Urol. Nephrol. 2022, 55, 929–942. [Google Scholar] [CrossRef] [PubMed]
- Kanbay, M.; A Ertuglu, L.; Afsar, B.; Ozdogan, E.; Siriopol, D.; Covic, A.; Basile, C.; Ortiz, A. An update review of intradialytic hypotension: concept, risk factors, clinical implications and management. Clin. Kidney J. 2020, 13, 981–993. [Google Scholar] [CrossRef]
- Macedo, E.; Karl, B.; Lee, E.; Mehta, R.L. A randomized trial of albumin infusion to prevent intradialytic hypotension in hospitalized hypoalbuminemic patients. Crit. Care 2021, 25, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.I. Impact of drugs on intradialytic hypotension: Antihypertensives and vasoconstrictors. Semin. Dial. 2017, 30, 532–536. [Google Scholar] [CrossRef] [PubMed]
- Wyckoff, M.H.; Greif, R.; Morley, P.T.; Ng, K.-C.; Olasveengen, T.M.; Singletary, E.M.; Soar, J.; Cheng, A.; Drennan, I.R.; Liley, H.G.; et al. 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation 2022, 146, E483–E557. [Google Scholar] [CrossRef]
- Batool, A.; Chaudhry, S.; Koratala, A. Transcending boundaries: Unleashing the potential of multi-organ point-of-care ultrasound in acute kidney injury. World J. Nephrol. 2023, 12, 93–103. [Google Scholar] [CrossRef]
- Al-Saray, M.Z.; Ali, A. Lung Ultrasound and Caval Indices to Assess Volume Status in Maintenance Hemodialysis Patients. POCUS J. 2023, 8, 52–59. [Google Scholar] [CrossRef]
- Romero-González, G.; Manrique, J.; Slon-Roblero, M.F.; Husain-Syed, F.; De la Espriella, R.; Ferrari, F.; Bover, J.; Ortiz, A.; Ronco, C. PoCUS in nephrology: a new tool to improve our diagnostic skills. Clin. Kidney J. 2022, 16, 218–229. [Google Scholar] [CrossRef] [PubMed]
- Moore CA, Ross DW, Pivert KA, Lang VJ, Sozio SM, Charles O’Neill W. Point-of-Care Ultrasound Training during Nephrology Fellowship A National Survey of Fellows and Program Directors. Clinical Journal of the American Society of Nephrology 2022, 17.
- Reisinger, N.K.A. Current opinion in quantitative lung ultrasound for the nephrologist. Curr Opin Nephrol Hypertens. 2023; 32, 509–514. [Google Scholar]
- Menon, S.; Krallman, K.A.; Fuhrman, D.Y.; Gorga, S.M.; Ricci, Z.; Stanski, N.L.; Selewski, D.T.; Soranno, D.E.; Zappitelli, M.; Zang, H.; et al. Worldwide Exploration of Renal Replacement Outcomes Collaborative in Kidney Disease (WE-ROCK). Kidney Int. Rep. 2023, 8, 1542–1552. [Google Scholar] [CrossRef] [PubMed]
- Gayen, S.; Kim, J.S.; Desai, P. Pulmonary Point-of-Care Ultrasonography in the Intensive Care Unit. AACN Adv. Crit. Care 2023, 34, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Volpicelli, G.; Gargani, L. A simple, reproducible and accurate lung ultrasound technique for COVID-19: when less is more. Intensiv. Care Med. 2021, 47, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Picano, E.; Frassi, F.; Agricola, E.; Gligorova, S.; Gargani, L.; Mottola, G. Ultrasound Lung Comets: A Clinically Useful Sign of Extravascular Lung Water. J. Am. Soc. Echocardiogr. 2006, 19, 356–363. [Google Scholar] [CrossRef]
- Mayr, U.; Lukas, M.; Habenicht, L.; Wiessner, J.; Heilmaier, M.; Ulrich, J.; Rasch, S.; Schmid, R.M.; Lahmer, T.; Huber, W.; et al. B-Lines Scores Derived From Lung Ultrasound Provide Accurate Prediction of Extravascular Lung Water Index: An Observational Study in Critically Ill Patients. J. Intensiv. Care Med. 2020, 37, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Grubic, N.; Belliveau, D.J.; Herr, J.E.; Nihal, S.; Wong, S.W.S.; Lam, J.; Gauthier, S.; Montague, S.J.; Durbin, J.; Mulvagh, S.L.; et al. Training of Non-expert Users Using Remotely Delivered, Point-of-Care Tele-Ultrasound: A Proof-of-Concept Study in 2 Canadian Communities. Ultrasound Q. 2023, 39, 118–123. [Google Scholar] [CrossRef]
- Rajamani, A.; Galarza, L.; Sanfilippo, F.; Wong, A.; Goffi, A.; Tuinman, P.; Mayo, P.; Arntfield, R.; Fisher, R.; Chew, M.; et al. Criteria, Processes, and Determination of Competence in Basic Critical Care Echocardiography Training: A Delphi Process Consensus Statement by the Learning Ultrasound in Critical Care (LUCC) Initiative. Chest 2022, 161, 492–503. [Google Scholar] [CrossRef]
- Yoshida, T.; Yoshida, T.; Noma, H.; Nomura, T.; Suzuki, A.; Mihara, T. Diagnostic accuracy of point-of-care ultrasound for shock: a systematic review and meta-analysis. Crit. Care 2023, 27, 1–11. [Google Scholar] [CrossRef]
- Qaseem, A.; Etxeandia-Ikobaltzeta, I.; Mustafa, R.A.; Kansagara, D.; Fitterman, N.; Wilt, T.J.; Clinical Guidelines Committee of the American College of Physicians; Batur, P.; Cooney, T.G.; Crandall, C.J.; et al. Appropriate Use of Point-of-Care Ultrasonography in Patients with Acute Dyspnea in Emergency Department or Inpatient Settings: A Clinical Guideline From the American College of Physicians. Ann. Intern. Med. 2021, 174, 985–993. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, S.; Koratala, A. Assessment of venous congestion by Doppler ultrasound: a valuable bedside diagnostic tool for the new-age nephrologist. CEN Case Rep. 2020, 10, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Via, G.; Tavazzi, G.; Price, S. Ten situations where inferior vena cava ultrasound may fail to accurately predict fluid responsiveness: a physiologically based point of view. Intensiv. Care Med. 2016, 42, 1164–1167. [Google Scholar] [CrossRef]
- Koratala, A.; Reisinger, N. Venous Excess Doppler Ultrasound for the Nephrologist: Pearls and Pitfalls. Kidney Med. 2022, 4, 100482. [Google Scholar] [CrossRef] [PubMed]
- Ross, D.W.; A Moses, A.; Niyyar, V.D. Point-of-care ultrasonography in nephrology comes of age. Clin. Kidney J. 2022, 15, 2220–2227. [Google Scholar] [CrossRef] [PubMed]
- Makhija N, Magoon R, Das D, Saxena A. Haemodynamic predisposition to acute kidney injury: Shadow and light! Journal of Anaesthesiology Clinical Pharmacology 2022, 38, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Ledoux-Hutchinson, L.; Wald, R.; Malbrain, M.L.N.G.; Carrier, F.M.; Bagshaw, S.M.; Bellomo, R.; Adhikari, N.K.J.; Gallagher, M.; Silver, S.A.; Bouchard, J.; et al. Fluid Management for Critically Ill Patients with Acute Kidney Injury Receiving Kidney Replacement Therapy: An International Survey. Clin J Am Soc Nephrol. 2023, 18, 705–715. [Google Scholar] [CrossRef]
- Ramadan, A.; Abdallah, T.; Abdelsalam, H.; Mokhtar, A.; Razek, A.A. Evaluation of parameters used in echocardiography and ultrasound protocol for the diagnosis of shock etiology in emergency setting. BMC Emerg. Med. 2023, 23, 132. [Google Scholar] [CrossRef] [PubMed]
- De Backer D, Aissaoui N, Cecconi M, Chew MS, Denault A, Hajjar L, et al. How can assessing hemodynamics help to assess volume status? Intensive Care Med. 2022, 48, 1482–1494. [CrossRef]
- Winning, J.; A Claus, R.; Huse, K.; Bauer, M. Molecular biology on the ICU. From understanding to treating sepsis. Minerva Anestesiologica 2006, 72, 255–67. [Google Scholar]
- Spano, S.; Maeda, A.; Lam, J.; Chaba, A.; See, E.; Mount, P.; Nichols-Boyd, M.; Bellomo, R. Cardiac Output Changes during Renal Replacement Therapy: A Scoping Review. Blood Purif. 2023, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Schotola, H.; Sossalla, S.T.; Renner, A.; Gummert, J.; Danner, B.C.; Schott, P.; Toischer, K. The contractile adaption to preload depends on the amount of afterload. ESC Hear. Fail. 2017, 4, 468–478. [Google Scholar] [CrossRef] [PubMed]
- Koh, S.; Kim, S.-J.; Lee, S. Associations between central pulse pressure, microvascular endothelial function, and fluid overload in peritoneal dialysis patients. Clin. Exp. Hypertens. 2023, 45, 2267192. [Google Scholar] [CrossRef] [PubMed]
- Cheong, I.; Castro, V.O.; Sosa, F.A.; Oribe, B.T.; Früchtenicht, M.F.; Tamagnone, F.M.; Merlo, P.M. Passive leg raising test using the carotid flow velocity–time integral to predict fluid responsiveness. J. Ultrasound 2023, 27, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Di Nicolò, P.; Tavazzi, G.; Nannoni, L.; Corradi, F. Inferior Vena Cava Ultrasonography for Volume Status Evaluation: An Intriguing Promise Never Fulfilled. J. Clin. Med. 2023, 12, 2217. [Google Scholar] [CrossRef] [PubMed]
- Zuo, M.-L.; Chen, Q.-Y.; Pu, L.; Shi, L.; Wu, D.; Li, H.; Luo, X.; Yin, L.-X.; Siu, C.-W.; Hong, D.-Q.; et al. Impact of Hemodialysis on Left Ventricular-Arterial Coupling in End-Stage Renal Disease Patients. Blood Purif. 2023, 52, 702–711. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Taberner, A.J.; Loiselle, D.S.; Tran, K. Cardiac efficiency and Starling's Law of the Heart. J. Physiol. 2022, 600, 4265–4285. [Google Scholar] [CrossRef] [PubMed]
- Suga, H. Time Course of Left Ventricular Pressure-Volume Relationship under Various Enddiastolic Volume. Jpn. Hear. J. 1969, 10, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Zhang, M. Echocardiography assessment of right ventricular-pulmonary artery coupling: Validation of surrogates and clinical utilities. Int. J. Cardiol. 2024, 394, 131358. [Google Scholar] [CrossRef]
- Ikonomidis I, Aboyans V, Blacher J, Brodmann M, Brutsaert DL, Chirinos JA, et al. The role of ventricular–arterial coupling in cardiac disease and heart failure: assessment, clinical implications and therapeutic interventions. A consensus document of the European Society of Cardiology Working Group on Aorta & Peripheral Vascular Diseases, European Association of Cardiovascular Imaging, and Heart Failure Association. Eur J Heart Fail. 2019, 21, 402–424.
- Lebeau, R.; Robert-Halabi, M.; Pichette, M.; Vinet, A.; Sauvé, C.; Dilorenzo, M.; Le, V.; Piette, E.; Brunet, M.; Bédard, W.; et al. Left ventricular ejection fraction using a simplified wall motion score based on mid-parasternal short axis and apical four-chamber views for non-cardiologists. BMC Cardiovasc. Disord. 2023, 23, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Schick, A.L.; Kaine, J.C.; Al-Sadhan, N.A.; Lin, T.; Baird, J.; Bahit, K.; Dwyer, K.H. Focused cardiac ultrasound with mitral annular plane systolic excursion (MAPSE) detection of left ventricular dysfunction. Am. J. Emerg. Med. 2023, 68, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Upadhrasta, S.; Raafat, M.H.; Conti, R.A. Reliability of focused cardiac ultrasound performed by first-year internal medicine residents at a community hospital after a short training. J. Community Hosp. Intern. Med. Perspect. 2019, 9, 373–376. [Google Scholar] [CrossRef] [PubMed]
- McLeod P, Beck S. Update on echocardiography: do we still need a stethoscope? Intern Med J. 2022, 52, 30–36. [CrossRef]
- Kirkpatrick, J.N.; Swaminathan, M.; Adedipe, A.; Garcia-Sayan, E.; Hung, J.; Kelly, N.; Kort, S.; Nagueh, S.; Poh, K.K.; Sarwal, A.; et al. American Society of Echocardiography COVID-19 Statement Update: Lessons Learned and Preparation for Future Pandemics. J. Am. Soc. Echocardiogr. 2023, 36, 1127–1139. [Google Scholar] [CrossRef] [PubMed]
- Kobal, S.L.; Trento, L.; Baharami, S.; Tolstrup, K.; Naqvi, T.Z.; Cercek, B.; Neuman, Y.; Mirocha, J.; Kar, S.; Forrester, J.S.; et al. Comparison of Effectiveness of Hand-Carried Ultrasound to Bedside Cardiovascular Physical Examination. Am. J. Cardiol. 2005, 96, 1002–1006. [Google Scholar] [CrossRef] [PubMed]
- Martin LD, Howell EE, Ziegelstein RC, Martire C, Whiting-O’Keefe QE, Shapiro EP, et al. Hand-carried Ultrasound Performed by Hospitalists: Does It Improve the Cardiac Physical Examination? Am J Med. 2009, 122, 35–41. [CrossRef]
- Banjade, P.; Subedi, A.; Ghamande, S.; Surani, S.; Sharma, M. Systemic Venous Congestion Reviewed. Cureus 2023, 15, e43716. [Google Scholar] [CrossRef] [PubMed]
- Kattan E, Castro R, Miralles-Aguiar F, Hernández G, Rola P. The emerging concept of fluid tolerance: A position paper. J Crit Care. 2022, 71, 154070.
- Rihl MF, Pellegrini JAS, Boniatti MM. VExUS Score in the Management of Patients With Acute Kidney Injury in the Intensive Care Unit: AKIVEX Study. Journal of Ultrasound in Medicine, 2023; 42, 2547–2556.
- Bhardwaj, V.; Vikneswaran, G.; Rola, P.; Raju, S.; Bhat, R.S.; Jayakumar, A.; Alva, A. Combination of Inferior Vena Cava Diameter, Hepatic Venous Flow, and Portal Vein Pulsatility Index: Venous Excess Ultrasound Score (VEXUS Score) in Predicting Acute Kidney Injury in Patients with Cardiorenal Syndrome: A Prospective Cohort Study. Indian J. Crit. Care Med. 2020, 24, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Viana-Rojas, J.A.; Argaiz, E.; Robles-Ledesma, M.; Arias-Mendoza, A.; Nájera-Rojas, N.A.; Alonso-Bringas, A.P.; Ríos-Arce, L.F.D.L.; Armenta-Rodriguez, J.; Gopar-Nieto, R.; la Cruz, J.L.B.-D.; et al. Venous excess ultrasound score and acute kidney injury in patients with acute coronary syndrome. Eur. Hear. Journal. Acute Cardiovasc. Care 2023, 12, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.-T.; Liu, D.-W.; Zhang, H.-M.; Chai, W.-Z.; Du, W.; He, H.-W.; Liu, Y. [Impact of extended focus assessed transthoracic echocardiography protocol in septic shock patients]. Zhonghua Yi Xue Za Zhi 2011, 91, 1879–1883. [Google Scholar] [PubMed]
- Guarracino, F.; Bertini, P.; Pinsky, M.R. Management of cardiovascular insufficiency in ICU: the BEAT approach. Minerva Anestesiol. 2021, 87, 476–480. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, D.A.; Mezière, G.A. Relevance of Lung Ultrasound in the Diagnosis of Acute Respiratory Failure*: The BLUE Protocol. Chest 2008, 134, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Beaubien-Souligny, W.; Rola, P.; Haycock, K.; Bouchard, J.; Lamarche, Y.; Spiegel, R.; Denault, A.Y. Quantifying systemic congestion with Point-Of-Care ultrasound: development of the venous excess ultrasound grading system. Ultrasound J. 2020, 12, 1–12. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Volpicelli, G.; Mussa, A.; Garofalo, G.; Cardinale, L.; Casoli, G.; Perotto, F.; Fava, C.; Frascisco, M. Bedside lung ultrasound in the assessment of alveolar-interstitial syndrome. Am. J. Emerg. Med. 2006, 24, 689–696. [Google Scholar] [CrossRef]
Figure 1.
Point of care Ultrasounds protocols for Acute Care Nephrology.RV: right ventricle; LV left ventricle; VTI:velocity time integral; IVC: inferior vena cava; LL: lower limbs ;FATE extended(54):The focus-assessed transthoracic echocardiography ;BEAT(55): Browse the heart ,Elastances, Assess volume status and Treat; BLUE(56) : The bedside lung ultrasound in emergency ; RUSH[4]: The rapid ultrasound in shock examination ; VExUS(57) : venous excess ultrasound .
Figure 1.
Point of care Ultrasounds protocols for Acute Care Nephrology.RV: right ventricle; LV left ventricle; VTI:velocity time integral; IVC: inferior vena cava; LL: lower limbs ;FATE extended(54):The focus-assessed transthoracic echocardiography ;BEAT(55): Browse the heart ,Elastances, Assess volume status and Treat; BLUE(56) : The bedside lung ultrasound in emergency ; RUSH[4]: The rapid ultrasound in shock examination ; VExUS(57) : venous excess ultrasound .
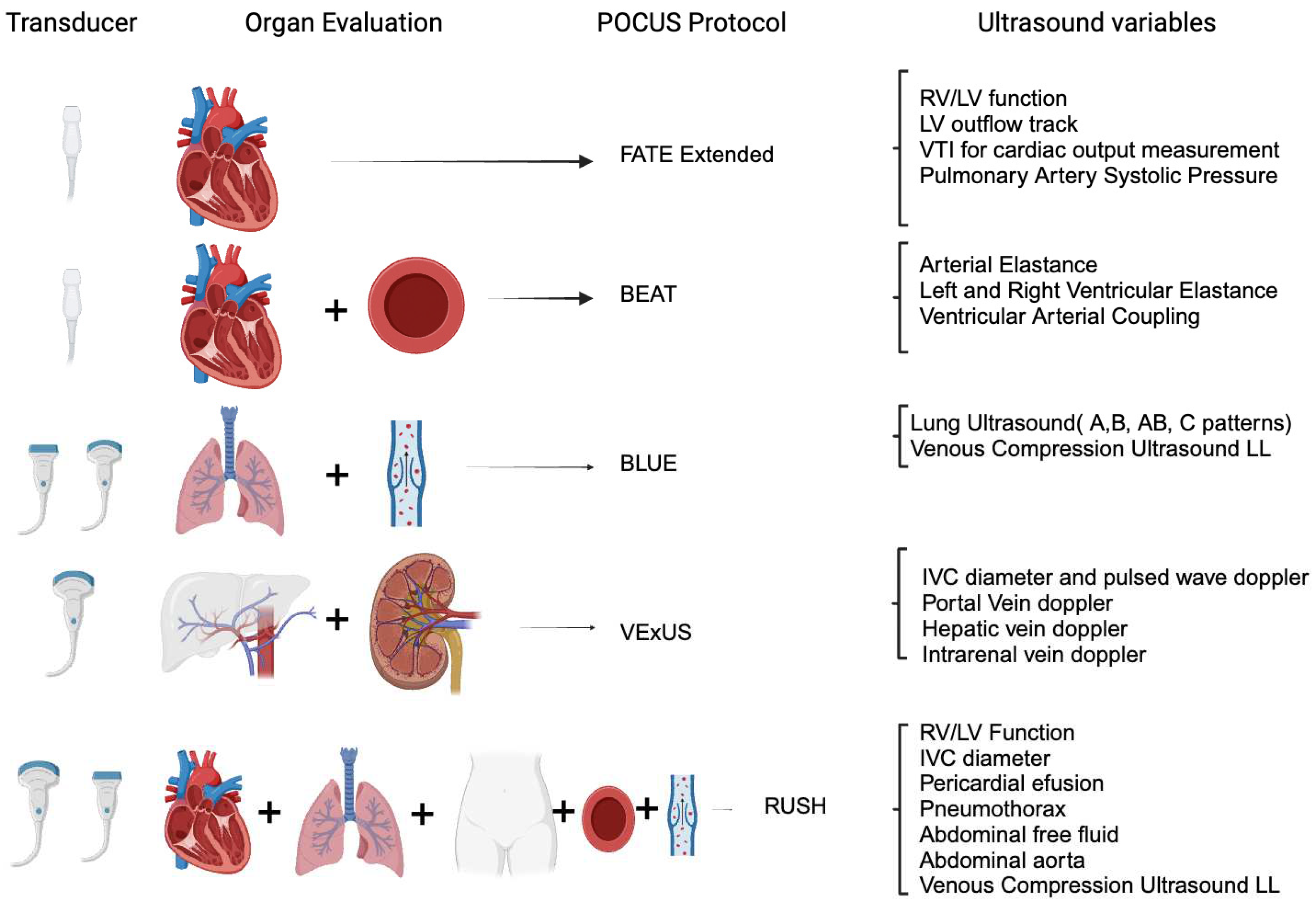
Figure 2.
Diagram of Lung Ultrasound Score(LUS) adapted from Volpiceli et al.(58) Score grade from 0 to 24, higher the score more lung disease. A useful toot to diagnostic, monitoring treatment and prognostic factor. Z: zone.
Figure 2.
Diagram of Lung Ultrasound Score(LUS) adapted from Volpiceli et al.(58) Score grade from 0 to 24, higher the score more lung disease. A useful toot to diagnostic, monitoring treatment and prognostic factor. Z: zone.
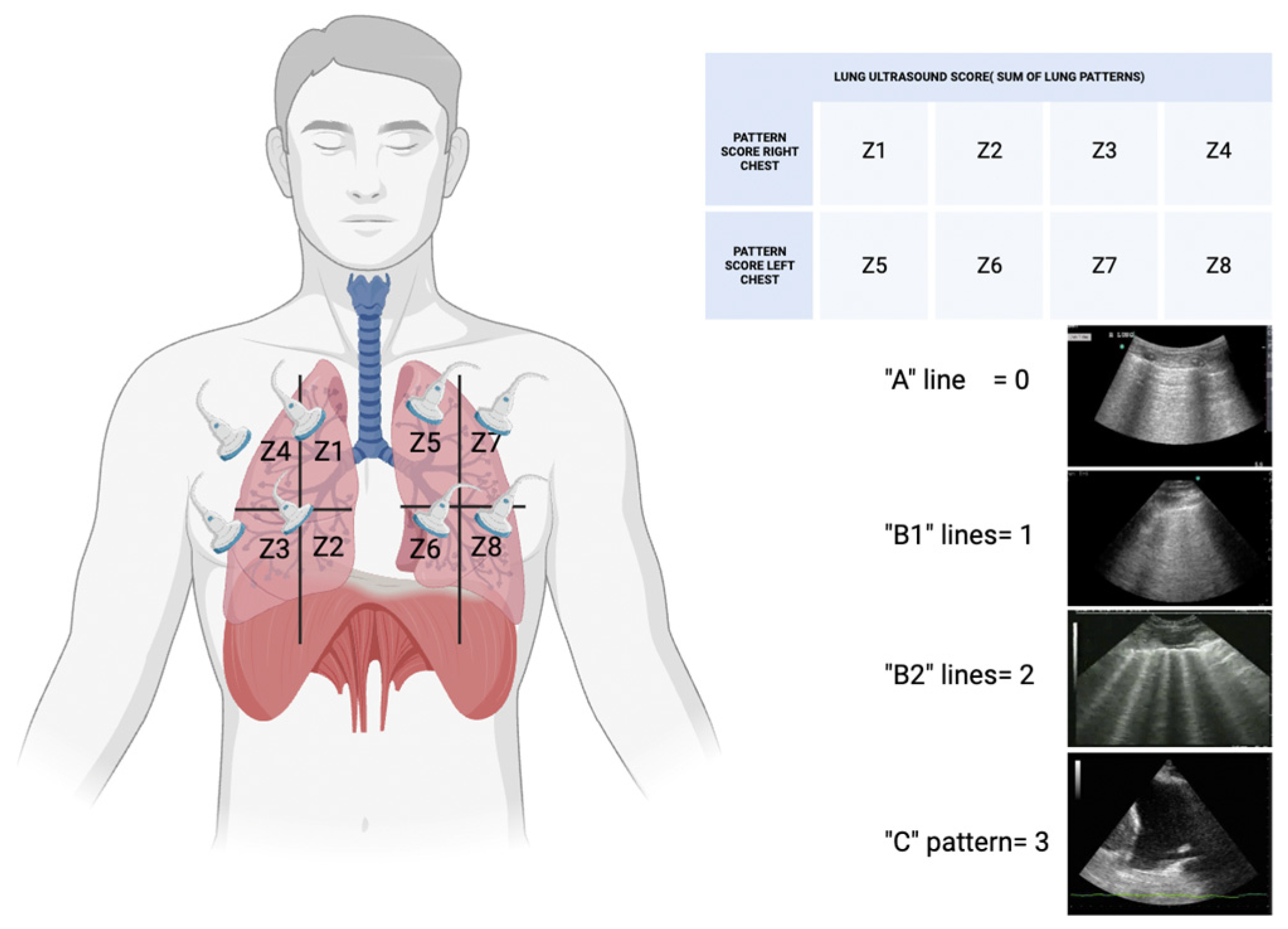
Figure 3.
Resuscitation algorithm based on optimizing intra-dialitic hypotension and fluid overload in Critically Ill Patients Undergoing Renal Replacement Therapy. PLR: passive leg raising. VAC: left ventricular-arterial coupling; Ea: efective arterial elastance; Ees: left ventricular efective end-systolic elastance; FATE: The focus-assessed transthoracic echocardiography, LV: left ventricle; RV: right ventricle; US: ultrasound.
Figure 3.
Resuscitation algorithm based on optimizing intra-dialitic hypotension and fluid overload in Critically Ill Patients Undergoing Renal Replacement Therapy. PLR: passive leg raising. VAC: left ventricular-arterial coupling; Ea: efective arterial elastance; Ees: left ventricular efective end-systolic elastance; FATE: The focus-assessed transthoracic echocardiography, LV: left ventricle; RV: right ventricle; US: ultrasound.
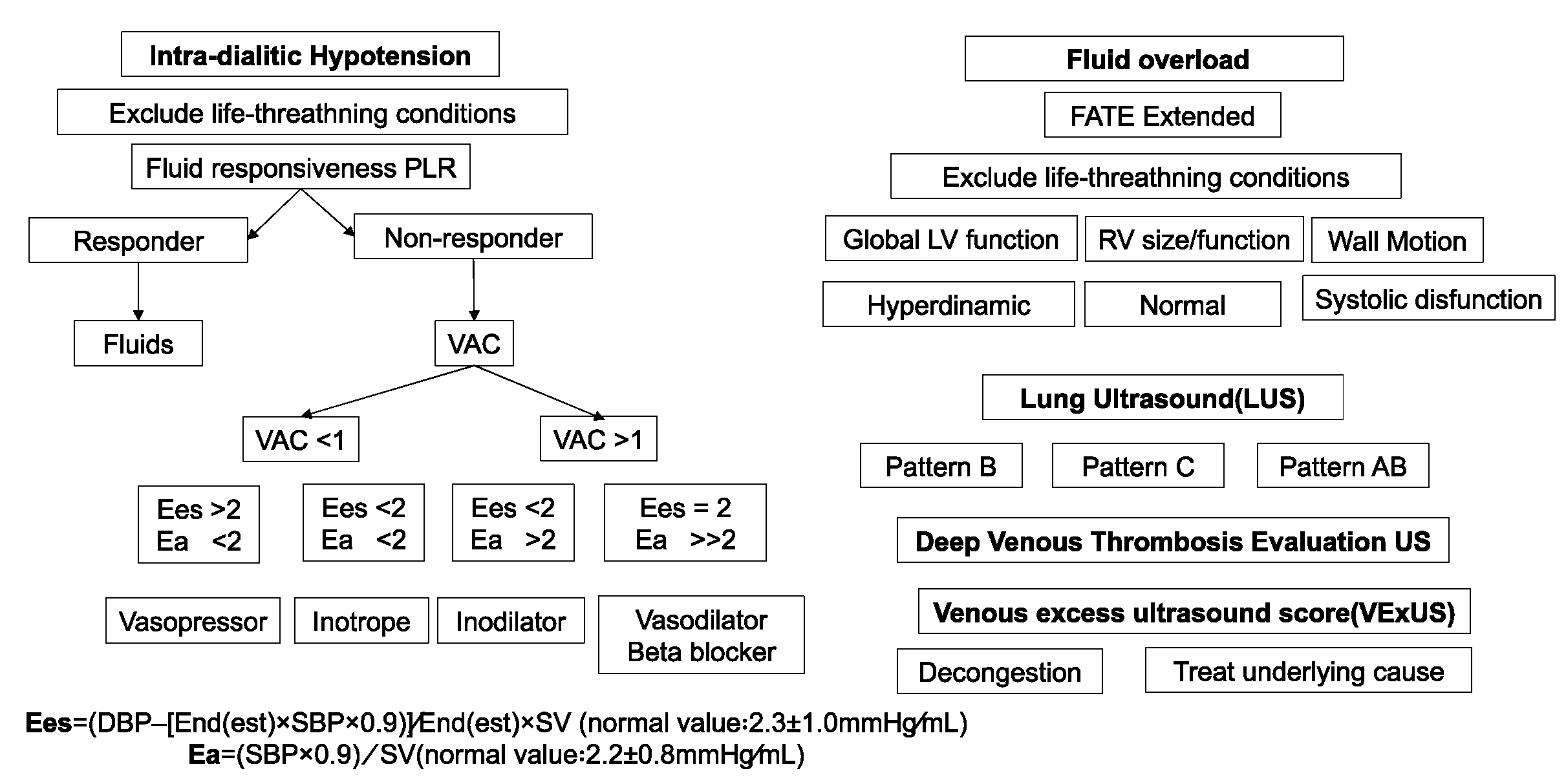
Figure 4.
A: Apical four chamber (A4C) view with dilated right ventricle (RV); B: colour doppler tricuspid regurgitation A4C; C: paraesternal short axis view (PSA) showing enlarged RV with flattened interventricular septum; D: dilated inferior vena cava; E: continuous wave doppler of tricuspid regurgitation showing estimated pulmonary systolic pressure of 96 mmHg in a patient with acute pulmonary embolism; F: Subcostal view with dilated left chambers; G PSA showing enlarges left ventricle with severe systolic disfunction related to myocarditis.
Figure 4.
A: Apical four chamber (A4C) view with dilated right ventricle (RV); B: colour doppler tricuspid regurgitation A4C; C: paraesternal short axis view (PSA) showing enlarged RV with flattened interventricular septum; D: dilated inferior vena cava; E: continuous wave doppler of tricuspid regurgitation showing estimated pulmonary systolic pressure of 96 mmHg in a patient with acute pulmonary embolism; F: Subcostal view with dilated left chambers; G PSA showing enlarges left ventricle with severe systolic disfunction related to myocarditis.
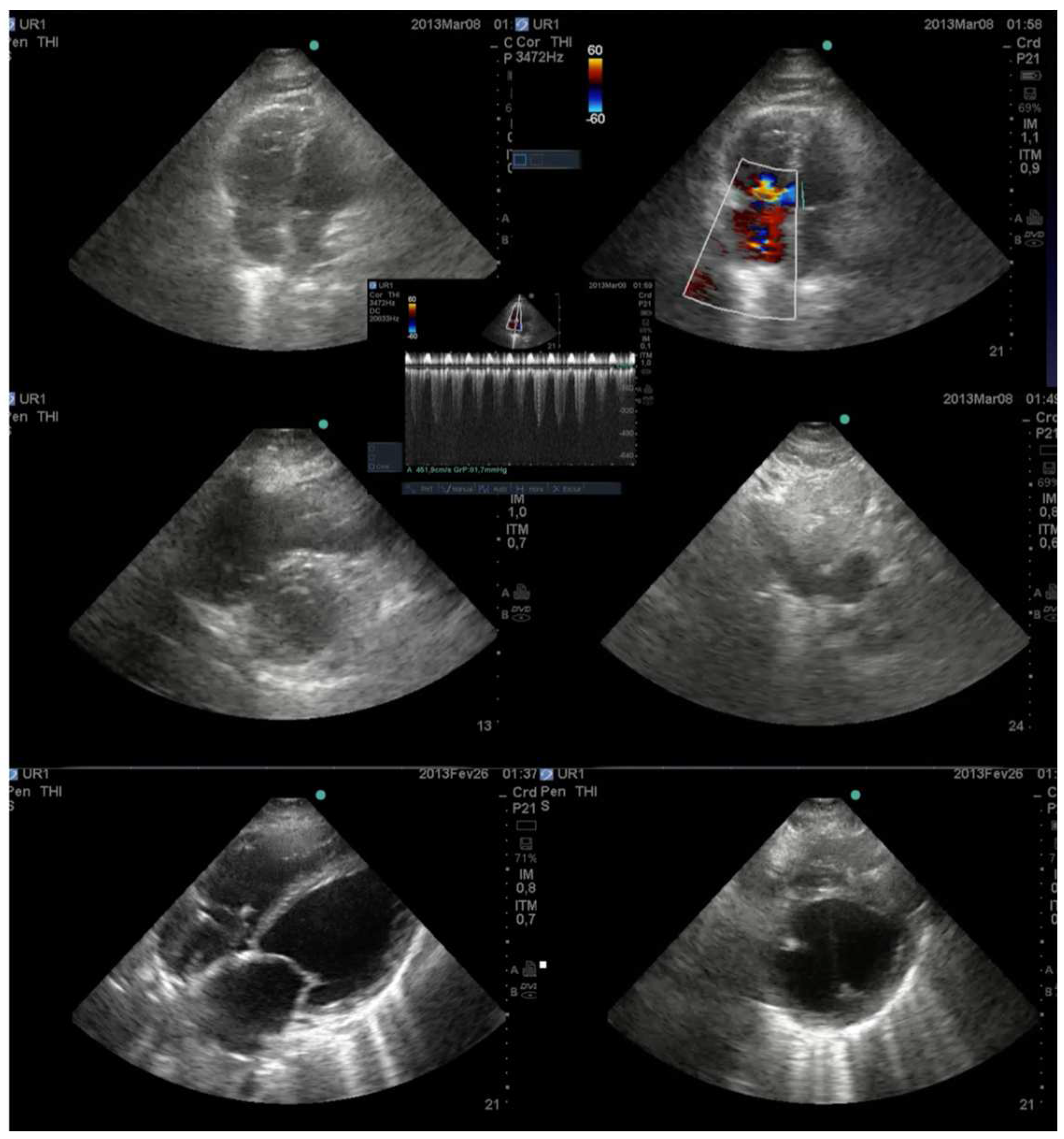
Figure 5.
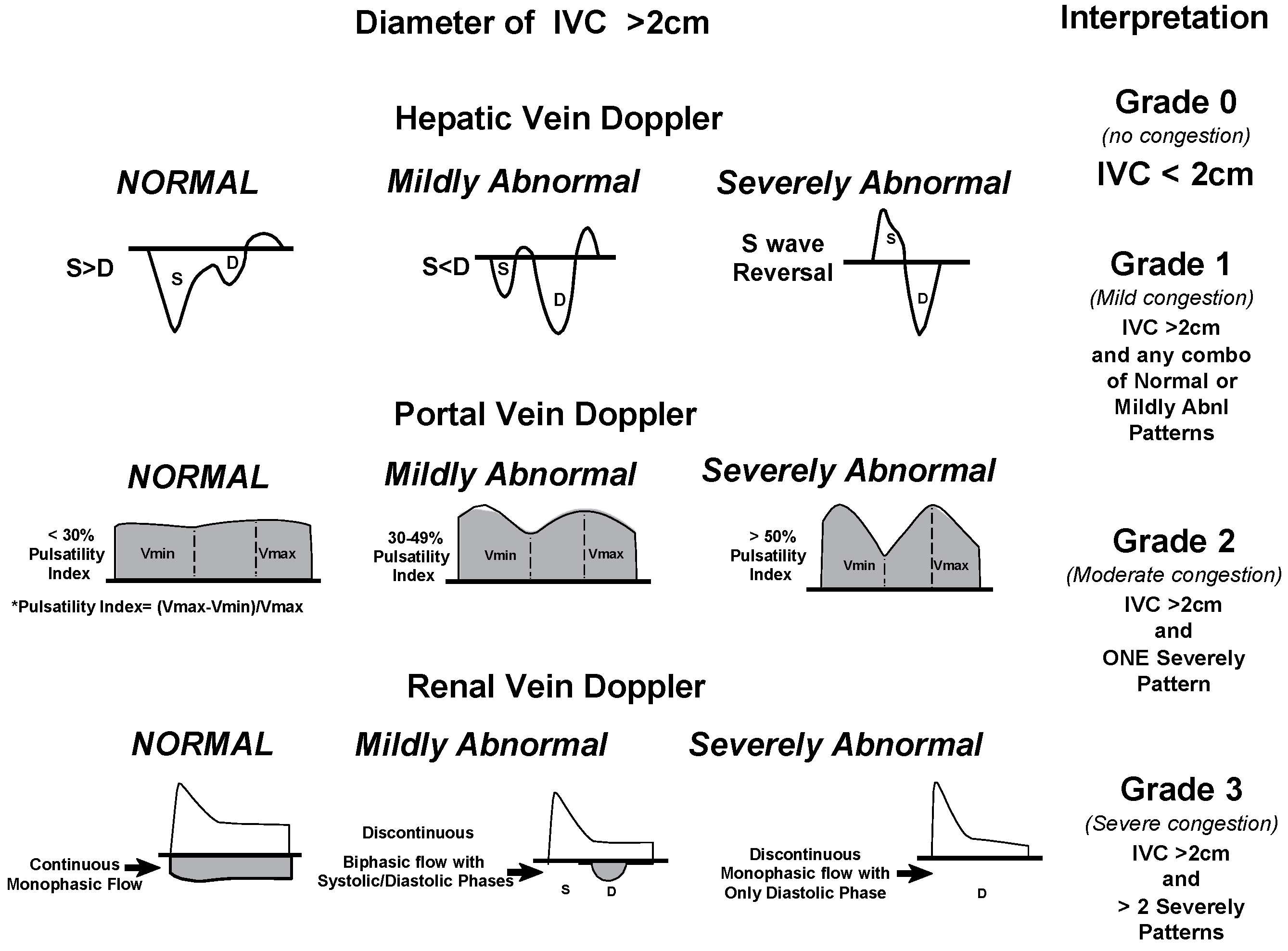
Venous excess Doppler ultrasound grading. Based on the degree of anomalies on the hepatic, portal, and intrarenal venous Doppler, three degrees of congestion are identified when the diameter of the IVC is greater than 2 cm. When the S wave on a hepatic vein Doppler is smaller than the D wave but remains below the baseline, it is classified as mildly abnormal; when the S wave is inverted, it is classified as seriously abnormal. When the pulsatility is between 30% and 50%, the portal vein Doppler is deemed slightly abnormal; when it is ≥50%, it is deemed seriously abnormal. * Pulsatility measurement points. When an intrarenal vein Doppler has a distinct D and S component and is pulsatile, it is considered mildly aberrant; when it shows a monophasic D-only pattern, it is considered highly abnormal. With permission, this figure was modified from NephroPOCUS.com. Abbreviations: VExUS, or venous excess Doppler ultrasonography; IVC, or inferior vena cava.
Figure 5.
Venous excess Doppler ultrasound grading. Based on the degree of anomalies on the hepatic, portal, and intrarenal venous Doppler, three degrees of congestion are identified when the diameter of the IVC is greater than 2 cm. When the S wave on a hepatic vein Doppler is smaller than the D wave but remains below the baseline, it is classified as mildly abnormal; when the S wave is inverted, it is classified as seriously abnormal. When the pulsatility is between 30% and 50%, the portal vein Doppler is deemed slightly abnormal; when it is ≥50%, it is deemed seriously abnormal. * Pulsatility measurement points. When an intrarenal vein Doppler has a distinct D and S component and is pulsatile, it is considered mildly aberrant; when it shows a monophasic D-only pattern, it is considered highly abnormal. With permission, this figure was modified from NephroPOCUS.com. Abbreviations: VExUS, or venous excess Doppler ultrasonography; IVC, or inferior vena cava.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



