Submitted:
17 January 2024
Posted:
19 January 2024
You are already at the latest version
Abstract
Hypertension is one of the most common primary cardiometabolic diseases and is a major contributor to cardiac mortality and morbidity. Furthermore, cardiac risk factors such as obesity and sedentary lifestyle are often seen in hypertensive patients. Regular exercise acts against these risk factors and improves the overall health of an individual. High-intensity interval training appears to do so in a more efficient way. We used a systematic literature review (SLR) approach to provide an overview of the present literature highlighting the cardiovascular advantages of HIIT in hypertensive individuals. We reviewed 4004 articles from reputable journals published between 2013 and August 14, 2023, focusing on 7 selected papers for in-depth analysis. This systematic review revealed the protective effects of HIIT against cardiac complications in hypertension. All the reviewed articles showed a decrease in blood pressure and many other risk variables of cardiovascular diseases. However, guidelines for this exercise are needed for maximum benefits. Therefore, further research on HIIT is necessary to fully harness its potential.
Keywords:
hypertension
; cardiac complications
; high-intensity interval training in hypertension
; high blood pressure
; cardiovascular diseases
1. Introduction And Background
Hypertension is a major cause of cardiovascular deaths all around the world. It has been attributed to 13.5% of the world's total premature deaths and has led to 6% of DALYs worldwide. Approximately half of people suffering from stroke and ischemic heart disease are hypertensive [1]. High blood pressure substantially increases the risk of cardiovascular diseases such as stroke, heart failure and ischemic heart disease [2]. Therefore, it is crucial to manage hypertension. Exercise is considered the first-line lifestyle change for hypertensive patients, as it helps in lowering blood pressure up to 5-7 mmHg [3]. High-intensity interval training can be considered a time-efficient alternative to traditional continuous moderate-intensity exercise, and research regarding its benefits in hypertension is significant.
Hypertension can occur due to multiple factors, such as obesity, high alcohol and salt intake, and can even be inherited [5]. It usually coexists with cardiovascular risk factors such as aging, insulin resistance, diabetes, and hyperlipidaemia, which eventually cause organ damage after long periods of time, leading to stroke and heart failure [6]. For these reasons, physical activity is recommended to improve cardiovascular fitness, indicating cardiovascular mortality (7).
All these risk factors cause changes in the structures and functions of blood vessels, which leads to an increase in the hemodynamic load, leading to further damage to the blood vessels [4]. Endothelial dysfunction is known to be the precursor change in hypertension. Exercise, especially high-intensity training, acts on the microvascular level and could improve endothelial function along with angiogenesis stimulation, which helps to reduce blood pressure [3]. It not only protects against hypertension but can also reverse hypertensive changes [9].
Initially, the baseline blood pressure is measured for which a mercury sphygmomanometer is preferred and at least two or three readings with a resting gap of two minutes is recommended at each visit of the patient. Moreover, a complete medical history and physical examination of the patient is recommended to be performed to identify preventable hypertensinogenic risk factors [5]. There are multiple guidelines for hypertension recommended based on systolic and diastolic blood pressure by the National Heart, Lung and Blood Institute (NHLBI), Joint National Committee (JNC), American Heart Association or the American College of Cardiology, which help to increase the awareness of hypertension among people [8].
High-intensity interval training is defined as multiple high-intensity efforts for short periods of time alternating with rest and recovery periods. This type of exercise is a better substitute in terms of time consumption for decreasing cardiovascular morbidity in hypertensive patients. HIIT showed promising benefits in improving blood pressure without even straining the heart [10] and has been more advantageous than continuous training in hypertensive patients [11]. However, it has been identified that the protective effects of HIIT occur when the training program has been performed continuously for 12 weeks or more [9].
2. Review
2.1. Methods
This review focuses on clinical studies concerning the use of HIIT in hypertensive patients to reduce their risk for CVDs. We excluded animal studies and publications that only discussed the cardiovascular benefits of HIIT without presenting clinical data. The review follows the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [25] for 2020 in Figure 1 and only uses data collected from published papers, eliminating the need for ethical approval.
2.2. Systematic Literature Search and Study Selection
We conducted a thorough search for relevant publications by using PubMed, including Medline and Google Scholar. We searched for studies mentioned in review papers, editorials, and commentaries on PubMed. Nevertheless, we continued searching for additional studies that satisfied our inclusion criteria.
We had a list of abstracts that we independently reviewed for inclusion using specific criteria. The criteria included benefits of HIIT, focusing on cardiovascular advantages, especially in hypertensive individuals, and a clearly described clinical cohort in the study. We excluded review papers and animal studies. Six reviewers conducted a dual review, and disagreements were resolved through discussion.
2.3. Inclusion and Exclusion Criteria
We established specific criteria for including and excluding participants to achieve our study goals. Our criteria can be summarized in Table 1.
2.4. Search Strategy
The population, intervention/condition, control/comparison, and outcome (PICO) criteria were utilized to
conduct a thorough literature review. The search was conducted on databases such as PUBMED (including
Medline) and Google Scholar Libraries, using relevant keywords, such as hypertension, HIIT, and cardiovascular advantages. The medical subject heading (MeSH) approach for PubMed (including Medline) and Google Scholar, as detailed in Table 2, was employed to develop a comprehensive search strategy.
2.5. Quality Appraisal
To ensure the reliability of the chosen papers, we utilized various quality assessment tools. We employed the PRISMA checklist and Cochrane bias tool assessment for randomized clinical trials for systematic reviews and meta-analysis. Non-randomized clinical trials were evaluated using the Newcastle‒Ottawa tool scale. We assessed the quality of qualitative studies, as shown in Table 3, using the critical appraisal skills program (CASP) checklist. To avoid any confusion in the classification, we utilized the scale for the assessment of narrative review articles (SANRA) to evaluate the article’s quality.
3. Results
After searching through three selected databases, PubMed, Medline, and Google Scholar, we extracted 1,43,938 articles. We then carefully reviewed each paper and applied specific criteria, which led to the exclusion of 1,31,013 articles. From the remaining 12,925 papers, we chose not to utilize 12,718 of them due to duplicates or unsatisfactory titles and abstracts. We closely examined the remaining 207 papers and excluded 200 more as their content did not meet our inclusion criteria. Finally, we conducted a thorough quality check on the remaining seven papers, which all met our criteria. These seven articles are included in our final systematic review. Table 4 provides a detailed description of each.
4. Discussions
One of the leading causes of mortality among adults remains to be cardiovascular diseases, and an important step in the prevention of these diseases remains risk assessment. There are several guidelines given by researchers for the estimation of CVD risk, such as Cholesterol Clinical Practice 2018, 2017 Hypertension Clinical Practice and ACC/AHA Clinical Practice (16). Risk assessment tools such as Pooled Cohort Equations(17), Framingham General CVD risk profile(17) and Reynolds risk score(19) include many variables and predict the CVD risk of the patients. All these scores include hypertension as one of the variables in predicting the outcome of the disease in patients (16).
The hypertension guidelines have always shown the link between hypertension and cardiovascular risk. A large number of observational studies have also summarized cardiovascular morbidity, such as stroke, sudden death, heart failure, peripheral arterial disease and myocardial infarction with hypertension. Although hypertension remains a major risk factor, the majority of patients have additional risk factors, such as aging, diabetes, and high cholesterol levels, that potentiate each other and increase the overall cardiovascular risk, which would be greater than the sum of the individual risk variables. Therefore, in these high-risk individuals, antihypertensive treatment is strategically given, as it is more difficult to control blood pressure (20). A therapeutic approach with a combination of antihypertensive drugs and nonpharmacological interventions, such as lifestyle modification is recommended to be implemented in all hypertensive patients for effective management of hypertension (21).
Lifestyle modifications such as weight loss and physical activity help in controlling blood pressure as an adjunct to pharmacologic treatment. As a sedentary lifestyle increases the risk of high blood pressure, exercise is strongly recommended for hypertensive patients by the Joint National Committee on Prevention, Detection, Evaluation and Treatment of high blood pressure (22). Recent studies have shown that vigorous exercise for short intervals of time, known as high-intensity interval training (HIIT), has been effective in lowering blood pressure. This type of exercise has also been able to improve the overall health of patients by altering body composition and has an effect on total cholesterol, HDL- cholesterol, LDL-cholesterol, triglycerides, fasting glucose, insulin, and systolic and diastolic blood pressure (13). Although it has been established that HIIT benefits hypertensive patients, the minimum needed duration of the training needs to be established (14).
As the name suggests, HIIT can be described as exercise with high intensity with recovery periods of lower intensity alternatively (13). High-intensity bouts may include running, sprinting, aerobic exercise or swimming (9). Recent studies suggest that HIIT is more beneficial than continuous moderate intensity training (CMIT) in reducing blood pressure, as it improves sympathetic activity in patients (14). Delgado et al.(9) showed that there was improvement in the vascular structure by HIIT in hypertensive patients as there was a decrease in peripheral vascular resistance, sympathetic nervous activity, and the amount of vasoconstrictors and an increase in the levels of nitric oxide in those patients(9).
While reviewing seven different studies, the cardiorespiratory uses of HIIT for hypertensive patients were evaluated. HIIT can improve carotid artery compliance up to 21%, baroreflex sensitivity (12), the rate of oxygen usage by the body while exercising and blood pressure in hypertensive patients (9). Furthermore, HIIT can decrease MSNA levels (14), improve endothelial function and may help in angiogenesis by improving NO and VEGF levels (15). These mechanisms of HIIT improve the metabolic capacity and overall cardiovascular function of patients without cardiac remodelling (10).
Research has demonstrated that HIIT, which consists mainly of walking or running on a treadmill, cycling or swimming, improves blood pressure through multiple mechanisms. All these mechanisms also have a protective effect on the heart and hence reduce cardiovascular risk in patients. It has been able to reverse the altered physiopathology of the disease and improve the overall health of patients. It acts on different systems in the body, such as the autonomic nervous system, vascular system and cardiac system. All these positive effects of HIIT reduce the risk of heart diseases such as stroke, myocardial infarction and heart attack (11).
Although HIIT has a beneficial effect of decreasing cardiovascular risk, more research is suggested for more effective benefits. Most of the research studies consisted of training for less than 3 months (9,10,12,15). Although the studies showed a positive health effect on patients, the long term benefits of HIIT on hypertensive patients are still unknown. Campbell et al.(13) suggested a randomized control trial for a minimum of six months for in-depth knowledge of HIIT and its effect on cardiovascular health. Once the full effects of HIIT are known and validated, it can be incorporated to enhance the cardiovascular health of patients.(13)
The findings based on 65 individual studies by Batacan et al. (23) indicated that the findings from long-term HIIT of more than 12 weeks were more significant in decreasing the heart rate, SBP and fat percentage in obese patients. However, VO2 max was significantly increased with both short-term and long-term exercise (23). The study by Campbell et al. suggested that HIIT may not have a dose response relationship (13).
No recent study has exclusively elaborated the cardiovascular benefits of HIIT in hypertensive patients. Researchers have demonstrated that HIIT could decrease many variables of cardiovascular risk assessment tools, including blood pressure. In today's world, hypertension and CVDs have become common, and it has become crucial to know the best way to manage them (11). Although there have been positive health effects with exercise, implementing it in daily life is still challenging. One significant barrier to exercise is mentioned as lack of time by many individuals (24). Therefore, HIIT can increase exercise compliance in a more time-efficient way and can be considered a more practical exercise method to improve the health of patients (11).
Although some studies have compared the short-term and long-term benefits of this exercise, none of them have tried to determine the optimum dosage (23). The majority of people fail to meet the exercise requirements. Therefore, it is important to establish guidelines for the best method of HIIT in terms of its intensity, duration and recovery intervals based on further research, which will have maximum health advantages (11).
5. Limitations
Our literature review has limitations. Our analysis was limited to English articles published within the past 11 years. We only used free articles, and our study was limited to English papers on the cardiovascular advantages of HIIT. More research is needed for specific conclusions.
6. Conclusions
Our research highlights the advantages of HIIT with regard to cardiovascular diseases in hypertensive individuals. HIIT aims to alleviate the burden of heart problems by acting on various CVD risk factors, of which HTN remains a major one. Some researchers have elaborated the health benefits of HIIT and have suggested the amount of exercise in terms of time. HIIT not only decreases CVD risk but can also improve the exercise compliance of patients. However, large-scale RCTs are required to establish the correct dosage of HIIT for different individuals.
Author Contributions
PY and BKP conceived the original idea which was also discussed with SRL and PY. First proof of concept was done by PY which was extended by BKP. PY carried out the data collection with the assistance of BKP and the data was analysed with the help of PY and SRL. PY wrote the manuscript and all the authors revised the final draft. All the authors have read and approved the final manuscript. All the authors are both to be personally accountable for their own contributions and ensure that the questions related to the accuracy or integrity of any part of the work, even the ones in which they are not personally involved, are appropriately investigated, resolved, and the resolution is documented in the literature.
Funding
This study received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable. If required, the data can be made available in a word or a pdf file.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare that they have no competing interests.
References
- Lawes, C.M.; Hoorn, S.V.; Rodgers, A. Global burden of blood-pressure-related disease. Lancet 2008, 371, 1518. [Google Scholar] [CrossRef] [PubMed]
- Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003, 42, 1206–1252. [CrossRef] [PubMed]
- Pescatello LS, Macdonald HV, Lamberti L, Johnson BT. Exercise for Hypertension: A Prescription Update Integrating Existing Recommendations with Emerging Research. Curr Hypertens Rep. 2015, 17, 87. [CrossRef]
- Yannoutsos A, Levy BI, Safar ME, Slama G, Blacher J. Pathophysiology of hypertension interactions between macro and microvascular alterations through endothelial dysfunction. J Hypertens 2014, 32, 216–224. [CrossRef]
- Carretero, O.A.; Oparil, S. Carretero OA, Oparil S. Essential Hypertension. Circulation 2000, 101, 329–335. [Google Scholar] [CrossRef]
- Messerli, F.H.; Williams, B.; Ritz, E. Essential Hypertension. Lancet 2007, 370, 591–603. [Google Scholar] [CrossRef]
- Lee, D.C.; Artero, E.G.; Sui, X.; Blair, S.N. Mortality trends in the general population: the importance of cardiorespiratory fitness. J Psychopharmacol. 2010, 24 (Suppl. 4), 27–35. [Google Scholar] [CrossRef] [PubMed]
- DePalma SM, Himmelfarb CD, et al. Hypertension guideline update: A new guideline for a new era. J Am Soc Hypertens 2018, 12, 262–265.
- Delgado-Floody P, Izquierdo M, Ramirez-Velez R, et al. Effect of High-Intensity Interval Training on Body Composition, Cardiorespiratory Fitness, Blood Pressure, and Substrate Utilization During Exercise Among Prehypertensive and Hypertensive Patients With Excessive Adiposity. Hypertension 2020, 76, 409–416.
- Grace F, Herbert P, Elliott AD, Richards J, Beaumont A, Sculthorpe NF. High intensity interval training (HIIT) improves resting blood pressure, metabolic (MET) capacity and heart rate reserve without compromising cardiac function in sedentary aging men. Exp Physiol. 2018, 103, 839–847.
- Ciolac, E.G. High-intensity interval training and hypertension: maximizing the benefits of exercise? Am J Cardiovasc Dis. 2012, 2, 102–110. [Google Scholar] [PubMed]
- Mohr M, Nordsborg NB, Lindenskov A, et al. High-Intensity Intermittent Swimming Improves Cardiovascular Health Status for Women with Mild Hypertension. Biomed Res Int. 2014, 2014, 728289.
- Campbell WW, Kraus WE, Powell KE, et al. High-Intensity Interval Training for Cardiometabolic Disease Prevention. Med Sci Sports Exerc. 2019, 51, 1220–1226. [CrossRef] [PubMed]
- Ehlers TS, Sverrisdottir Y, Bangsbo J, Gunnarsson TP. High-Intensity Interval Training Decreases Muscle Sympathetic Nerve Activity in Men With Essential Hypertension and in Normotensive Controls. J Hypertens. 2020, 38, 485–493.
- Taha MM, Mohamed MA, Hasanin ME. EFFECT OF HIGH INTENSITY INTERVAL TRAINING ON ENDOTHELIAL FUNCTION IN POSTMENOPAUSAL HYPERTENSIVE PATIENTS: RANDOMIZED CONTROLLED TRIAL. J Hypertens. 2016, 34, 1234–1241.
- Lloyd-Jones DM, Braun LT, Ndumele CE, Smith SC Jr, et al. Use of Risk Assessment tools to Guide Decision-making in the Primary Prevention of Atherosclerotic Cardiovascular Disease: A Special Report From the American College of Cardiology. J Am Coll Cardiol. 2018, 71, 2817–2817.
- American Heart Association. ASCVD Risk Calculator. https://professional.heart.org/professional/GuidelinesStatements/ASCVDRiskCalculator/UCM_457698_ASCVD-Risk-Calculator.jsp. Accessed [date].
- D'Agostino RB Sr, Vasan RS, Pencina MJ, et al. General Cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation 2008, 117, 743–753. [CrossRef]
- Ridker PM, Paynter NP, Rifai N, Gaziano JM, Cook NR. C-Reactive Protein and Parental History Improve Global Cardiovascular Risk Prediction: The Reynolds Risk Score for Men. Circulation 2008, 118, 2243–2251.
- Kjeldsen, S.E. Hypertension and cardiovascular risk: General aspects. Pharmacol Res. 2018, 129, 95–99. [Google Scholar] [CrossRef]
- Nguyen, Q.; Dominguez, J.; Nguyen, L.; Gullapalli, N. Hypertension Management: An Update. Am J Ther. 2010, 17, e234-46. [Google Scholar]
- Kokkinos, P.F.; Narayan, P.; Papademetriou, V. EXERCISE AS HYPERTENSION THERAPY. Cardiol Clin. 2001, 19, 507–516. [Google Scholar] [CrossRef]
- Batacan RB Jr, Duncan MJ, Dalbo VJ, Tucker PS, Fenning AS. Effects of high-intensity interval training on cardiometabolic health: a systematic review and meta-analysis of intervention studies. Br J Sports Med. 2017, 51, 494–503. [CrossRef] [PubMed]
- Booth, M.L.; Bauman, A.; Owen, N.; Gore, C.J. Physical Activity preferences, Preferred sources of Assistance, and Perceived Barriers to Increased Activity among Physically Inactive Australians. Prev Med. 1997, 26, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009, 6, e1000100. [CrossRef] [PubMed]
Figure 1.
PRISMA flow diagram illustrating the search strategy and study selection process for the systematic review. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Figure 1.
PRISMA flow diagram illustrating the search strategy and study selection process for the systematic review. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
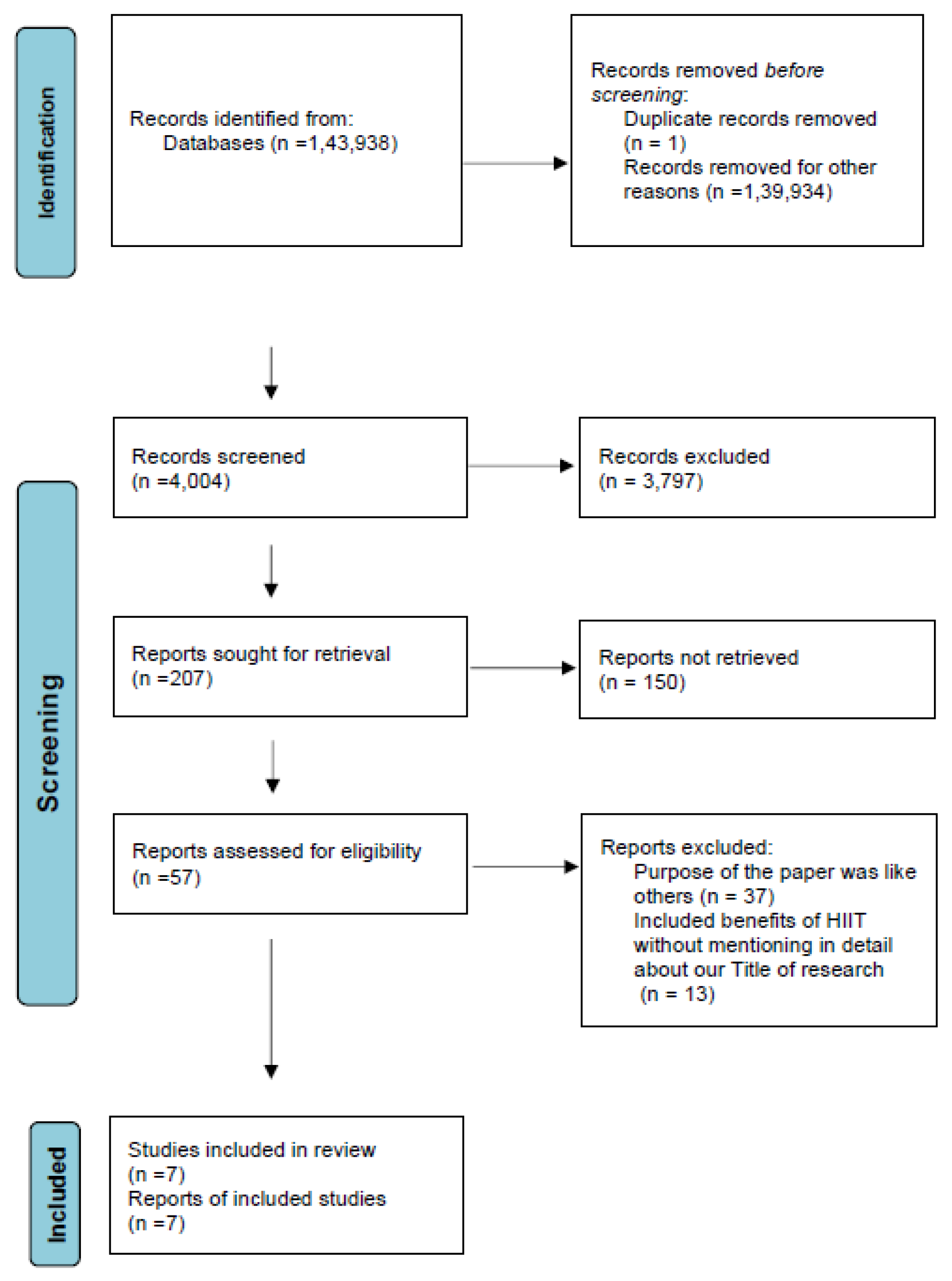

Table 1.
Showing the criteria adopted during the literature search process.
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| a) | Human studies | Animal studies |
| b) | From 2011 to 2023 | Only methodological studies explaining HIIT details |
| c) | English Text | Non-English texts |
| d) | Gender: All | |
| e) | Age: >19 years of age | Age:<19 years |
| f) | Free papers | Papers that needed to be purchased |
| Studies involving clinical data other than cardiovascular diseases |
Table 2.
Showing the search strategy, search engines used, and the number of results displayed. HTN: Hypertension; HIIT: High Intensity Interval training.
Table 2.
Showing the search strategy, search engines used, and the number of results displayed. HTN: Hypertension; HIIT: High Intensity Interval training.
| Database | Search Strategy | Search results | |
|---|---|---|---|
| A) | Pubmed | Hypertension or High Blood Pressure or Cardiovascular benefits or high intensity interval training and advantages | 3,938 |
| B) | Google Scholar | HTN and HIIT or Cardiovascular benefits | 1,40,000 |
Table 3.
Table 3. Showing quality appraisal tools used. PRISMA: Preferred reporting items for systematic reviews and meta-analyses; SANRA: Scale for the assessment of non-systematic review articles.
Table 3.
Table 3. Showing quality appraisal tools used. PRISMA: Preferred reporting items for systematic reviews and meta-analyses; SANRA: Scale for the assessment of non-systematic review articles.
| Quality Appraisal Tools Used | Type of Studies |
|---|---|
| Cochrane Bias Tool Assessment | Randomized Control Trials |
| Newcastle‒Ottawa Tool | Non-RCT and Observational Studies |
| PRISMA Checklist | Systematic Review |
| SANRA Checklist | Any Other Without Clear Method Section |
Table 4.
Summary of the results of the selected papers. CMT: Continuous- moderate intensity training; HFrEF: Heart failure with reduced ejection fraction; HIIT: High Intensity interval Training; HIIT: High intensity interval training.
Table 4.
Summary of the results of the selected papers. CMT: Continuous- moderate intensity training; HFrEF: Heart failure with reduced ejection fraction; HIIT: High Intensity interval Training; HIIT: High intensity interval training.
| Author/Year | Country | Study Design | Database Used | Conclusion |
|---|---|---|---|---|
|
Delgado-Floody et al./2020 (9) |
South America, UK, Spain |
Randomized Control Trial | 42 adults were allocated into 3 groups and were subjected to 16 weeks of HIIT | HIIT can improve the cardiorespiratory fitness of the patients. |
|
Thomas Svare Ehlers et al./2020 (14) |
Brazil | Randomized Control Trial | In this study, exercise training was conducted on outpatients from a hospital for 12 weeks. | HIIT can reduce the cardiovascular risk in patients with HFrEF. |
|
Emmanuel Gomes Ciolac et al./2012 (11) |
Brazil | Systematic Review | Google Scholar | HIT has greater advantages to CMT and more research is required to know the precise quantity of exercise. |
|
Fergal Grace et al./2018 (10) |
Australia UK |
Randomized Control Trial | 44 male patients were subjected to 6 weeks of HIIT. | Cardiovascular health can be improved with HIIT. |
|
Magni Mohr et al./2014 (12) |
Europe | Randomized Control Trail | In this study, 62 hypertensive women were subjected to 15 weeks of swimming. | HIT can improve physical and cardiovascular health. |
|
Mona Taha et al./2016 (15) |
Egypt | Randomized Control Trial | This study included 46 mild hypertensive women who were subjected to weeks of HIT. | HIIT can help in preventing atherosclerosis and decrease cardiovascular risk factors. |
|
Wayne W. Campbell et al./2019 (13) |
USA | Systematic Review | PubMed CINAHL and Cochrane. |
HIT can improve the health f the patients but more research is suggested to know the full effects of HIIT on cardiovascular risk factors. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



