
Submitted:
19 January 2024
Posted:
22 January 2024
You are already at the latest version
Abstract
Cenobamate is approved by the European Medicine Agency for the treatment of adult patients with epilepsy (PWEs) who suffer from ongoing focal-onset seizures despite appropriate treatment with at least two established antiseizure medications. Pivotal trials and post-marketing real-world observational studies have suggested a high efficacy with unusually high seizure-free rates.
We sought to investigate the serum trough levels of cenobamate under steady-state conditions in seizure-free versus non-responding PWEs, and in PWEs who experienced adverse events versus those who did not.
We analyzed samples from 101 PWEs treated with adjunct cenobamate under steady-state conditions. In all, 36 PWEs were seizure-free and 65 were non-responders. In 31 PWEs, adverse events were apparent, whereas in the remaining 70, no tolerability issues were reported.
We found a linear correlation between the daily doses (range: 100 mg – 400 mg) and the plasma levels (3.8 mg/l – 54.6 mg/l).
Neither the daily doses nor the plasma levels differed significantly between seizure-free and non-responding PWEs or between PWEs with a satisfactory tolerability and those who experienced adverse events.
The main reason for this result was that the individual therapeutic ranges varied widely: seizure freedom and adverse effects were observed alongside low doses and plasma levels in some PWEs. Conversely, there were examples of PWEs who did not respond or who reported no tolerability issues at high doses or plasma levels. Still, to evaluate the individual therapeutic range and to better understand the influence of other drugs in cases where concomitant medications are used, the therapeutic drug monitoring of cenobamate may be useful.
Keywords:
epilepsy
; cenobamate
; plasma levels
; therapeutic drug monitoring
; effectiveness
; correlation
1. Introduction
Cenobamate (YKP 3089) (C10H10CIN5O2) ((IR)-1-(2-Chlorophenyl)-2-(2H-tetrazol-2-yl) ethyl carbamate) is a new antiseizure medication (ASM) that was synthesized, developed, and investigated in preclinical and clinical trials by SK Life Science Inc. It is a tetrazole alkyl carbamate derivative with one chiral center. Cenobamate is structurally related to, but different from, carisbamate, which was previously investigated as a potential ASM. However, the carisbamate program was not pursued because one pivotal randomized controlled trial did not show statistically significant superiority for its efficacy over a placebo [1,2,3,4].
In 2021, cenobamate was approved by the European Medicines Agency (EMA) for the adjunct treatment of adult patients with epilepsy (PWEs) with focal-onset seizures who did not respond in a satisfying way after an appropriate treatment with at least two established ASMs [5]. The approval was based on the results of one proof-of-concept study with the well-established photosensitivity model [6], two randomized placebo-controlled trials [7,8], and one open-label safety study [9].
The pharmacological profile of cenobamate has been extensively investigated [5,10,11,12,13,14,15,16,17]. In brief, the key points are as follows:
The oral CNB absorption rate is 88% or higher and almost independent of food intake. The time to the maximum serum concentration after oral intake (Tmax) varies between 0.8 and 4 hours. The plasma protein binding rate is 60% and the distribution volume accounts for approximately 40 – 50 l. After single and multiple applications, the maximum serum concentration Cmax increases in a dose-proportional manner. Although the area under the curve (AUC) increases after single doses in a more-than-linear way, an almost dose-proportional increment was observed in the clinically relevant daily dose range between 50 mg and 500 mg. The oral clearance is low; it decreases from approximately 1,4 l/h to 0.50 l/h with increasing doses and ranges between 0.45 and 0.63 l/h at oral daily doses between 100 mg and 400 mg, which are recommended according to the summary of the product characteristics (SmPC). The elimination half-life time T1/2 varies between 30 and 76 hours with increasing doses. For daily doses between 100 mg and 400 mg, T1/2 is about 50 – 60 hours. Considering this pharmacokinetic profile, a once-daily dosing in the evening is possible and, therefore, recommended. Under these conditions, plasma steady-state concentrations are reached after approximately 14 days.
Cenobamate is extensively metabolized in the liver. It undergoes glucuronidation via UGT2B7 and, to a lesser extent, via UGT2B4, and oxidation via CYP2E1, CYP2A6, CYP2B6, and, to a lesser extent, via CYP2C19 and CYP3A4/5. It is mainly excreted renally (87.8%; 5.2% is excreted in the feces).
Certain populations require special attention if the use of cenobamate is intended. The cenobamate plasma concentrations were shown to be increased in patients with a liver (plasma AUC = 2.1-2.3-fold higher) or renal (plasma AUC = 1.4-1.5-fold higher) impairment in pharmacokinetic studies [15,16]. Dose adjustments should be made according to the prescribing information. The pharmacokinetics did not differ significantly based on gender or race, or among elderly people (age > 65 years) compared with younger people (18 – 45 years) [16].
The precise mode of action has not yet been fully uncovered [4,5,11,15,16]. Two potentially complementary mechanisms have been described so far. One mechanism involves cenobamate reducing repetitive neuronal discharges through the inhibition of voltage-dependent sodium channels [5,7,10,16,18]. In particular, cenobamate enhances the rapid and complete inactivation of sodium channels and inhibits the non-activating component of the sodium current (INaP) in hippocampal rat neurons in a concentration-dependent manner, similarly to lacosamide [3,5,6,10,11,16,18].
A second mechanism of action is related to γ-amino butyric acid (GABA) [5,8,12,16,18]. Cenobamate potentiates GABA-induced currents in acutely isolated CA3 pyramidal cells in a concentration-dependent manner. It enhances tonic GABAA currents and shows a positive allosteric modulation of GABA-induced currents mediated by GABAA receptors. This effect was similar for all the tested GABAA receptors containing six different alpha subunits (α1β2γ2 or α2-6β3γ2). The results showed that CNB acted as a positive allosteric modulator of high-affinity GABAA receptors, activated by GABA at a site independent of the benzodiazepine binding site, and efficiently enhanced tonic inhibition in hippocampal neurons [10,18]. There is additional evidence that cenobamate interacts with both synaptic and extra-synaptic GABAA receptors by exerting effects on both phasic (Iphasic) and tonic (Itonic) GABAA currents [18].
Despite the limitations of fixed-dose placebo-controlled trials, such as relatively short maintenance periods, the phase-2 trials have already suggested that cenobamate might be a particularly effective ASM, even when compared to the results of similar successful studies with other recently investigated and approved ASMs [2]. The results of these trials indicate that cenobamate could be nothing less than a game-changer [3,19].
Indeed, and in line with pivotal trials, the open-label extension data and some real-world studies support this view [20,21,22,23,24,25].
The Kork Epilepsy Center is one of the leading tertiary-referral epilepsy centers in Germany [26]. We had the opportunity to join two of the pivotal trials with cenobamate [8,9] so that we were familiar with the practical handling of cenobamate and the perspective it offers. Since many of our clients suffer from long-lasting and difficult-to-treat epilepsies, we can usually collect a high number of PWEs who are waiting for a new treatment option within a relatively short period of time. In addition, we run a therapeutic drug-monitoring laboratory that offers plasma-level measurements of almost all the ASMs currently available. To define the clinical importance of the plasma levels of recently introduced ASMs, we regularly perform appropriate studies, such as our publications about the therapeutic drug monitoring of lacosamide and perampanel [27,28]. With cenobamate, we were able to establish our own therapeutic drug monitoring essay in 2021 prior to its introduction on the market, the details of which are described in the Methods section.
Here, we present our data on adult patients with focal-onset seizures who were treated with add-on cenobamate, and in whom we were able to assess cenobamate doses and the resulting plasma levels and to correlate them with efficacy and tolerability under plasma steady-state conditions.
2. Methods
This study is part of the ongoing CENKORK study, which is a prospective, monocenter, open-label, non-interventional study in adult PWEs who were initiated with adjunct cenobamate after the introduction of cenobamate to the German market in June of 2021 and during the following year.
We measured the plasma levels of the participants whenever possible to determine the clinical usefulness of therapeutic drug monitoring of cenobamate.
The following inclusion criteria were applied:
- Initiation of add-on cenobamate between June 2021 and June 2022;
- Stable antiseizure medication during the three months prior to the initiation of cenobamate;
- Once-daily cenobamate dosing in the evening;
- Serum collection in the morning;
- Complete documentation of seizures and tolerability during the three months prior to the initiation of cenobamate;
- Seizure frequency of at least one per month and no seizure-free intervals of at least four weeks during the preceding three months according to their self-reports and seizure calendars;
- Recruitment for the CENKORK observational trial;
- Adult age;
- Informed consent;
- Therapeutic drug monitoring at the laboratory of the Kork Epilepsy Center;
- Out-patient appointment and examination on the same day of the therapeutic drug monitoring by the first author (BJS).
The exclusion criteria were as follows:
- Alteration in the daily dose of cenobamate within the preceding four weeks;
- Alteration in antiseizure or other chronically applied co-medication within the preceding four weeks;
- Incomplete documentation of seizure situation or tolerability;
- History of non-epileptic seizures;
- Status epilepticus during the preceding three months;
We assessed various demographic data, including age, gender, age at onset of epilepsy, seizure and epilepsy classification, etiology, previous ASMs and their number, the current ASM treatment, and the seizure frequency during the three months prior to the initiation of cenobamate.
The data were pseudonymized prior to the data analysis.
The PWEs were followed concerning the cenobamate titration and dosing, their seizure frequency and intensity, and adverse events. No fixed appointment schedules were used. The PWEs were followed on an individual basis. In every case, direct communication was possible so that dose adjustments could be performed.
Due to the unusually high efficacy of cenobamate according to the literature [2,5,7,8,9,15,16,21,22,23,24,25,29,30], we decided to analyze the data only in the PWEs who became completely seizure-free during the three-month period versus the PWEs who experienced no effects on their seizure frequency or a seizure reduction of <50%. Thus, we excluded the so-called ≥50% responders to more accurately differentiate between unequivocal responders (seizure-free PWEs) and non-responding PWEs.
Although the long elimination half-life of cenobamate might allow plasma levels to be considered almost independently of the daytime and mode of intake [13,17], the plasma levels were only accepted when the blood samples were obtained in the morning, independently of food intake, which has no relevant impact on the absorption [5,15,16].
Cenobamate was titrated according to the schedule used in the phase-III trial by Sperling et al. (2020) [9], which is also recommended in the SmPC for the European Union. Thus, once-daily dosing was intended with 12,5 mg of cenobamate during titration weeks one and two, followed by dose increases to 25 mg during weeks three and four, 50 mg during weeks five and six, and 100 mg thereafter. At this timepoint, we regularly contacted the participants to communicate the subsequent strategy according to the efficacy and tolerability at week seven. In every case, we tried to dose as efficiently as possible on an individual basis, with 400 mg as the maximum dose according to the results of the pivotal trial by Krauss et al. (2020) [8] and the European SmPC. Depending on the efficacy and an acceptable tolerability, we would not necessarily exclude higher dosing in single cases in our clinical practice. However, this was not the case in this study (see results).
The cenobamate serum levels were measured in our own certified therapeutic drug monitoring laboratory by means of liquid chromatography mass spectrometry (LCMS).
A quantitative analysis of cenobamate (C10H10ClN5O2 → 267.67 g/mol) was performed using a mass spectrometric method. The ammonium adduct [M+NH4]+ was analyzed as an intense target ion. An isotope-labeled internal standard [13C6] cenobamate was used.
Sample preparation:
An amount of 100 µl of serum with 100 µl of an internal standard solution and 500 µl of methanol were mixed (for 10 sec) and cooled (for 15 min). After centrifugation (10000 rpm for 7 min), the supernatant was diluted with water (1:1).
The chromatographic conditions were as follows:
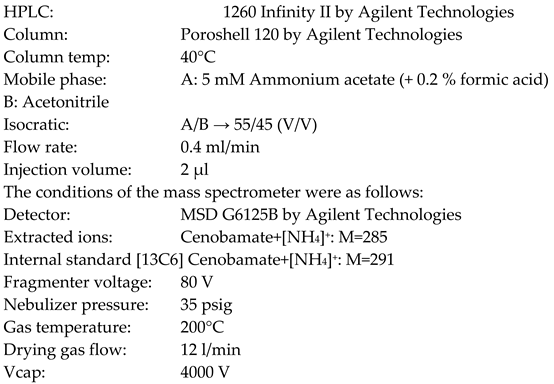
The quantification of cenobamate in serum allowed for the selective and sensitive determination of the compound. The linearity was investigated in a range from 0.1 µg/ml to 100 µg/ml. The measuring range was approved from 0.5 µg/ml to 50 µg/ml. The quantification limit was 0.5 µg/ml. The precision was <5%. The dilutions were unremarkable. Interference (by other ASMs) was not observed. Abnormalities in the stability of cenobamate in serum (< 5 days) were not detected.
As there were no commercially available interlaboratory tests for cenobamate, the samples were compared at another laboratory at regular intervals. Spiked control material achieved the necessary accuracy at all times.
At the time of measuring the cenobamate plasma concentration, the additional medication, tolerability, and seizure situation were assessed. For the classification of efficacy, the preceding three months were compared with the three-month period prior to the initiation of cenobamate. An assessment of tolerability was performed on the day of the plasma level measurement by means of a direct interview and a clinical examination by one of us (BJS).
The outcome variables of this investigation were as follows:
- Is there a direct proportionality between the daily doses and the plasma levels as predicted by the literature, at least in lower to medium doses?
- Are there differing levels of daily doses and plasma levels concerning efficacy?
- Are there differing levels of daily doses and plasma levels concerning tolerability?
- Is it possible from these real-world data to define the therapeutic range that is required to achieve an appropriate efficacy without a risk of adverse events?
All the statistical analyses performed were descriptive in nature. Continuous endpoints are reported using means +/- SD, and categorical data are reported using frequencies and percentages. The baseline characteristics and post-baseline measures are reported from the analyses, including the cenobamate dose and the serum levels, separated by the status of the response (non-response vs. seizure freedom). Similarly, the status of adverse events (present vs. absent) is reported. A linear regression and Pearson's correlation analysis were also performed between the cenobamate daily dose and the serum levels. The frequency and percentage of subjects with no response or seizure freedom are reported using the serum concentration.
This study was conducted according to the Declaration of Helsinki code of ethics.
It was approved by the local ethical committee of the Medical Faculty at the University of Freiburg, Germany (No. 22-1139) and registered at the German registry of clinical studies, DRKS (DRKS-ID DRKS00030916). Participants gave their informed consent.
3. Results
The plasma levels were obtained from 101 PWEs; 36 of them were seizure-free and 65 were non-responding according to the definitions mentioned above. Adverse events were reported by 31 PWEs.
The demographic data are shown in Table 1.
The PWE group suffered from difficult-to-treat epilepsies with a long duration of the disease, with a mean duration above 20 years; a mean of around 10 previously used antiseizure medications, usually one or two concomitant ASMs; and a seizure frequency of more than 10 per month, despite this baseline medication. No significant differences were apparent between the groups. Among the seizure-free PWEs, more subjects were male (57% male versus 43% female). The duration of epilepsy was slightly longer in non-responding patients and in PWEs who did not experience adverse events. The seizure frequency prior to cenobamate was higher in PWEs who experienced adverse events. However, these differences were well within the confidence intervals.
Independently of the efficacy and the tolerability, we found a strong and linear correlation between the daily cenobamate dose and the plasma levels (see Figure 1 and Figure 2). In the whole group, the correlation coefficient was 0.701; in seizure-free PWEs, it was 0.844, and in non-responders, it was 0.644.
4. Efficacy
The mean daily doses were 240.3 ± 102.0 mg and 260.8 ± 73.2 mg, respectively, with a dose range between 100 mg and 400 mg in both groups.
In seizure-free PWEs, the corresponding cenobamate plasma levels varied between 3.8 mg/l and 33.7 mg/l (mean of 17,8 ± 7.1 mg/l), compared to a range between 3.9 mg/l and 54.6 mg/l and a mean of 20.9 ± 8.8 mg/l in non-responders.
5. Adverse events
Adverse events were reported in 30.7% of PWEs (n = 31). They consisted of somnolence (n = 19, 61.3% of all PWEs who experienced adverse events), followed by dizziness (n = 5, 16.1%) and ataxia (n = 3, 9.7%), along with single cases of a dazed state, diplopia, gynecomastia, increased liver enzymes, a depressive mood, a mood alteration, and tremors. The rate of adverse events was 25% among seizure-free patients (n = 9) and 33.8% among the non-responding PWEs (n = 22). The daily cenobamate doses and plasma levels of PWEs who experienced adverse events and those who did not experience them did not differ significantly. In PWEs who did not experience adverse events, the mean daily dose was 257.1 ± 90,6 mg (100 – 400 mg); in PWEs who did experience adverse events, it was 245.2 mg ± 70.0 mg (100 mg – 400 mg). The corresponding mean cenobamate plasma levels were 19.5 ± 7.7 mg/l (3.8 – 37.8 mg(l) and 20.4 ± 9.8 mg/l (3.9 – 54.6 mg/l), respectively. These results were not significantly different. When we addressed typical neurotoxic symptoms such as dizziness, ataxia, and blurred or double vision, the daily doses of cenobamate in the seven affected PWEs varied between 200 mg and 400 mg, with the plasma levels ranging between 13.6 and 54.6 mg/l. The concomitant medications were levetiracetam (n = 2), lamotrigine (n = 3), levetiracetam and oxcarbazepine (n = 1), and oxcarbazepine and phenobarbital (n = 1).
The complete results concerning the efficacy and tolerability are shown in Table 2.
6. Discussion
To the best of our knowledge, our study reports the first major data collection of cenobamate plasma levels in real life. In line with the literature [5,10,11,12,13,14,15,16,17], we found a linear correlation between the daily doses and the plasma levels, even at higher doses according to a dose-proportional increment. Thus, even under a varying concomitant ASM treatment, as in our study, the plasma levels corresponding with dose increments are well predictable.
Therapeutic drug monitoring is an established tool to improve the quality of ASM therapy. Especially with first- and second-generation ASMs such phenobarbital, phenytoin, and carbamazepine, so-called therapeutic ranges have been defined and are still widely used [28]. The definition of a therapeutic or reference range is a drug-specific span between upper and lower limits that defines the range of doses resulting in probable antiseizure efficacy without dose-related adverse events [31]. The concept of such a general definition has been questioned. Instead, the use of a more individualized therapeutic range has been proposed [32].
We established our LCMS essay early in 2021, around the time of the introduction of cenobamate to the market in Germany. Due to its long half-life, the once-daily dosing regimen in the evening, and a maximum time of four hours to achieve maximum plasma concentration (Tmax), relevant and interfering plasma level fluctuations after the blood sampling in the morning are very unlikely, similarly to the situation with perampanel [28]. At a steady state, plasma level fluctuations are very limited [17]. Our experience supports this statement: we measured the daytime cenobamate levels under steady-state conditions in two of our in-patients at various timepoints (8 and 12 a.m., 4 p.m., and immediately prior to the intake of cenobamate in the evening). The fluctuations in the plasma levels were very slight and within a deviation of 10%. Therefore, we feel confident that our method was appropriate for addressing the study variables. Furthermore, we excluded any interfering modifications by concomitant medications or hepatic or renal impairments, and we used the cenobamate steady-state levels exclusively.
The definition of a so-called therapeutic range was not possible.
When comparing the data of seizure-free versus non-responding PWEs, no significant differences were found concerning both the doses and plasma levels. The main reason for this is that the individual therapeutic ranges varied widely: seizure freedom as well as adverse effects were observed alongside low doses and plasma levels in some PWEs. Conversely, there were examples of PWEs who did not respond or reported no tolerability issues at high doses or plasma levels.
Our findings emphasize the recently proposed concept of an individualized therapeutic range [32] in favor of a general one: in seizure-free PWEs, it might be helpful to document not only the dose, but also the corresponding plasma level. The group comparison between dramatic responders and non-responders did not provide any effect-specific general recommendations. Likewise, adverse events and a good tolerability did not correlate with the plasma levels in general. Considering typical neurotoxic adverse events such as dizziness, blurred vision, and ataxia, we also found a wide range of doses and plasma levels: the daily doses varied between 200 mg and 400 mg, and the plasma levels varied between 13.6 mg/l and 54.6 mg/l.
From the pivotal trials and the published real-world evidence, it has been claimed that combinations of cenobamate with sodium-channel-blocking agents (for pharmacodynamic reasons) or with clobazam (for pharmacokinetic reasons) are associated with a higher risk of adverse events [33,34]. We could not confirm this assumption from our data because these adverse events were more common under combinations with levetiracetam and lamotrigine, although the plasma level of the latter usually drops under the influence of cenobamate [5,11,15,16]. However, these findings were observations in small subgroups, and certainly require support from larger studies and cohorts.
It is tempting to speculate that responders at low doses and plasma levels may have been sensitive to the unique GABAergic mechanism of cenobamate, especially if these PWEs were previously treated with an ASM with a comparable effect on sodium channels to cenobamate. If such a specific effect occurs, the correlation with the dose and plasma levels might be less important.
Data on the clinical experience with cenobamate plasma levels are scarce. The levels of ≥50% responders in two of the pivotal studies [7, 8) recorded plasma levels between 5 and 35 µg/ml in more than 95% of patients [35]. This is almost identical with the levels we found in seizure-free PWEs. However, we compared these findings with those in non-responding PWEs and did not find an inter-group difference.
In clinical practice, it might be more important to collect and understand the plasma levels of concomitant ASMs that are influenced by cenobamate. This will be the objective of another study. The methodology will be more challenging because plausible conclusions will only be possible if PWEs are included with a stable concomitant medication over a longer period of time so that true cenobamate-induced alterations can be found and judged appropriately. This will require following the courses of individual PWEs over months, which was not performed in the study reported here.
7. Strengths and limitations
Our study has the strength that the data were collected under identical circumstances. Data heterogeneity was reduced by the exclusive use of personal patients according to a monocenter design, and the plasma levels were obtained only at our center and investigated in our therapeutic drug monitoring laboratory.
The limitations result from the relatively low amount of data. However, the results were consistent, so we doubt that more data would have changed the key messages of our investigation.
8. Conclusions
Despite the close and linear correlation between the daily doses and plasma levels of cenobamate, a global therapeutic range could not be defined due to the highly individual reactions concerning the efficacy and tolerability at widely differing doses and levels. Still, Therapeutic drug monitoring might be useful in well-defined clinical situations, such as investigations into the adherence or impact of potentially interacting concomitant medications or factors such as hepatic or renal impairment. The routine therapeutic drug monitoring of cenobamate is not recommended.
Author Contributions
Bernhard J. Steinhoff: idea, design, conceptualization, methodology, submission to ethical committee, writing, editing, project administration, and funding acquisition. Dimitra Georgiou: conceptualization and data acquisition. Daniel Dietmann: development of the therapeutic drug monitoring method and measurement of the plasma levels. Tassanai Intravooth: submission to ethical committee, registration at German registry of clinical studies (DRKS), and writing—review and editing.
Funding
Angelini Pharma supported this study with the help of statistics. Language editing was performed by MDPI. This study was partly funded by the Dr. Anneliese Brinkmann Stiftung.
Institutional Review Board Statement
This study was conducted according to the Declaration of Helsinki code of ethics. It was approved by the local ethical committee of the Medical Faculty at the University of Freiburg, Germany (No. 22-1139), and registered at the German registry of clinical studies, DRKS (DRKS-ID DRKS00030916).
Informed Consent Statement
Informed consent was obtained from all the subjects involved in this study.
Data Availability Statement
Data were pseudonymized for the statistical analysis. Raw data are stored at the archive of the Kork Epilepsy Center.
Acknowledgments
The authors want to thank Dr. Karthinathan Thangavelu for the professional and helpful statistical advice and support. This was greatly appreciated. .
Conflicts of Interest
B.J.S.: advisory and consulting honoraria: Angelini, Jazz/GW Pharmaceuticals, Precisis, Roche Diagnostics, UCB. Speaker’s honoraria: Al Jazeera, Angelini, Bial, Desitin, Eisai, Jazz/GW Pharmaceuticals, Medscape, Tabuk, Teva, UCB, Zogenix. Research support: Eisai, European Union, Jannsen-Cilag, Jazz/GW Pharmaceuticals, SK Life Sciences, UCB, Zogenix. D.G., D.D., and T.I.: Nothing to disclose.
References
- Sperling MR, Greenspan A, Cramer JA, Kwan P, Kälviäinen R, Halford JJ, Schmitt J, Yuen E, Cook T, Haas M, Novak G. Carisbamate as adjunctive treatment of partial onset seizures in adults in two randomized, placebo-controlled trials. Epilepsia. 2010;51(3):333-43. [CrossRef]
- Lattanzi, S, Trinka, E, Zaccara, G, Striano, P, Russo, E, Del Giovane, C, Silvestrini, M, Brigo, F. Adjunctive treatment of focal-onset seizures in adults: A systematic review and network meta-analysis. Drugs 2022 Feb;82(2):199-218. [CrossRef]
- Vossler, DG Remarkably high efficacy of cenobamate in adults with focal-onset seizures: A double-blind, randomized, placebo-controlled trial. Epilepsy Curr. 24;20(2):85-87. [CrossRef]
- Wheless, JW Adjunctive cenobamate for the treatment of focal onset seizures in adults with epilepsy: a critical review. Expert Rev Neurother 2020 Nov;20(11):1085-1098. [CrossRef]
- Steinhoff, BJ. Anti-convulsant Agents: Cenobamate. In: Riederer, P., Laux, G., Nagatsu, T., Le, W., Riederer, C. (eds) NeuroPsychopharmacotherapy. Springer, Cham, 2022. [CrossRef]
- Kasteleijn-Nolst Trenite DGA, DiVentura BD, Pollard JR, Krauss, GL, Mizne, S, French, JA. Suppression of the photoparoxysmal response in photosensitive epilepsy with cenobamate (YKP3089). Neurology. 2019;93(6):e559–e567.
- Chung SS, French JA, Kowalski J, Krauss, GL, Lee, SK, Maciejowski, M, Rosenfeld, WE, Sperling, MR, Mizne, S, Kamin, M. Randomized phase 2 study of adjunctive cenobamate in patients with uncontrolled focal seizures. Neurology. 2020 Jun 2;94(22):e2311–e2322.
- Krauss GL, Klein P, Brandt C, Lee, SK, Milanov, I, Milovanovic, M, Steinhoff, BJ, Kamin, M. Safety and Efficacy of Adjunctive Cenobamate (YKP3089) in patients with uncontrolled focal seizures: a multicentre, double-blind, randomised, placebo-controlled, dose-response trial. Lancet Neurol. 2020;19(1):38–48.
- Sperling MR, Klein P, Aboumatar S, Gelfand, M, Halford, JJ, Krauss, GL, Rosenfeld, WE, Vossler, DG, Wechsler, R, Borchert, L, Kamin, M. Cenobamate (YKP3089) as adjunctive treatment for uncontrolled focal seizures in a large, phase 3, multicenter, open-label safety study. Epilepsia 2020;Jun;61(6):1099–1108.
- Nakamura, M, Cho, JH, Shin, HS, Jang, IS. Effects of cenobamate (YKP3089), a newly developed anti-epileptic drug, on voltage-gated sodium channels in rat hippocampal CA3 neurons. Eur J Pharmacol 2019 Jul 15:855:175-182. [CrossRef]
- Keam, SJ Cenobamate: First approval. Drugs 2020;80(1):73-78. [CrossRef]
- Sharma, R, Song, ES, Nakamura, M, Neupane, C, Jeon, BH, Shin, H, Melnick, SM, Klenn, KJ, Jang, I, Park, JB. Positive allosteric modulation of GABAA receptors by a novel antiepileptic drug cenobamate. Eur J Pharmacol 2020 Jul 15:879:173117. [CrossRef]
- Vernillet, L, Greene, SA, Kamin, M. Pharmacokinetics of cenobamate: results from single and multiple oral ascending dose studies in healthy subjects. Clin Pharmacol Drug Dev 2020 May;9(4):428-443. [CrossRef]
- Vernillet, L, Greene, SA, Kim, HW, Melnick, SM, Glenn, K. Mass balance, metabolism, and excretion of cenobamate, a new antiepileptic drug, after a single oral administration in healthy male subjects. Eur J Drug Metab Pharmacokinet. 2020 Aug;45(4):513-522. [CrossRef]
- Roberti, R, De Caro, C, Iannone, LF, Zaccara, G, Lattanzi, S, Russo, E. Pharmacology of cenobamate: mechanism of action, pharmacokinetics, drug-drug interactions and tolerability. CNS Drugs 2021 Jun;35(6):609-618. [CrossRef]
- Steinhoff, BJ. Cenobamate tablets as a treatment for focal-onset seizures in adults. Expert Rev Clin Pharmacol 2021 Feb;14(2):161-172. [CrossRef]
- Darpo, B, Sager, PT, Xue, H, Kamin, M. A phase I clinical study evaluating the effects of cenobamate on the QT interval. Clin Pharmacol Drug Dev 2022 Apr;11(4):523-534. [CrossRef]
- Guignet, M, Campbell, A, White, HS. Cenobamate (XCOPRI): Can preclinical and clinical evidence provide insight in its mechanism of action? Epilepsia 2020;61:2329-2339. [CrossRef]
- French, J. Cenobamate for focal seizures – a game changer? Nat Rev Neurol 2020 Mar;16(3):133-134. [CrossRef]
- Beltrán-Corbellini Á, Romeral-Jiménez M, Mayo P, Sánchez-Miranda Román I, Iruzubieta P, Chico-García JL, Parra-Díaz P, García-Morales I, Toledano R, Aledo-Serrano Á, Gil-Nagel A. Cenobamate in patients with highly refractory focal epilepsy: A retrospective real-world study. Seizure 2023; Oct:111:71-77. [CrossRef]
- Klein, P, Aboumatar, S, Brandt, C, Dong, F, Krauss, GL, Mizne, S, Sanchez-Alvarez, JC, Steinhoff, BJ, Villanueva, V. Long-Term Efficacy and Safety From an Open-Label Extension of Adjunctive Cenobamate in Patients With Uncontrolled Focal Seizures. Neurology 2022 Jun 15;99(10):e989-e998. [CrossRef]
- Makridis, KL, Kaindl, AM. Real-world experience with cenobamate: A systematic review and meta-analysis. Seizure 2023; Sep 9:112:1-10. [CrossRef]
- Stern S, Weingarten M, Mandapati S, Ferrari L, Wade CT. Real-world analysis of retention on cenobamate in patients with epilepsy in the United States. Epilepsy Res 2023; Aug 15:197:107207. [CrossRef]
- Villanueva V, Santos-Carrasco D, Cabezudo-García P, Gómez-Ibáñez A, Garcés M, Serrano-Castro P, Castro-Vilanova MD, Sayas D, Lopez-Gonzalez FJ, Rodríguez-Osorio X, Torres-Gaona G, Saiz-Diaz RA, Hampel KG, Martinez-Ferri M, Aguilar-Amat MJ, Mercedes-Alvarez B, García-Morales V, Del Villar-Igea A, Massot-Tarrús A, Rodríguez-Uranga JJ. Real-world safety and effectiveness of cenobamate in patients with focal onset seizures: Outcomes from an Expanded Access Program. Epilepsia Open 2023; Sep;8(3):918-929. [CrossRef]
- Peña-Ceballos J, Moloney PB, Munteanu T, Doyle M, Colleran N, Liggan B, Breen A, Murphy S, El-Naggar H, Widdess-Walsh P, Delanty N. Adjunctive cenobamate in highly active and ultra-refractory focal epilepsy: A "real-world" retrospective study. Epilepsia 2023; 2023 May;64(5):1225-1235. [CrossRef]
- Steinhoff, BJ, Büchel, R, Stefan F. The Kork Epilepsy Center., Kehl-Kork, Germany. Epilepsy Behav 2017 Nov:76S:S26-S29. [CrossRef]
- Hillenbrand, B, Wisniewski, I, Jürges, U, Steinhoff, BJ. Add-on lacosamide: a retrospective study on the relationship between serum concentration, dosage, and adverse events. Epilepsy Behav 2011 Nov;22(3):548-51. [CrossRef]
- Steinhoff, BJ, Hübers, E, Kurth, C, Jürges, U. Plasma concentration and clinical effects of perampanel-The Kork experience. Seizure 2019 Apr:67:18-22. [CrossRef]
- Klein, P, Krauss, GL, Steinhoff, BJ, Devinsky, O, Sperling, MR. Failure to use new breakthrough treatments for epilepsy. Epilepsia 2023 Jun;64(6):1458-1465. [CrossRef]
- Villanueva V, Serratosa JM, Toledo M, Ángel Calleja M, Navarro A, Sabaniego J, Pérez-Domper P, Álvarez-Barón E, Subías S, Gil A. Number needed to treat and associated cost analysis of cenobamate versus third-generation anti-seizure medications for the treatment of focal-onset seizures in patients with drug-resistant epilepsy in Spain. Epilepsy Behav 2023; Feb:139:109054. [CrossRef]
- Steinhoff BJ, Fröscher W. Importance of therapeutic drug monitoring of anticonvulsants. An overview. Z Epileptol 2011;24:6–11. [CrossRef]
- Patsalos PN, Spencer EP, Berry DJ. Therapeutic drug monitoring of antiepileptic drugs in epilepsy: a 2018 update. Ther Drug Monit 2018 Oct;40(5):526-548. [CrossRef]
- Steinhoff, BJ, Rosenfeld, WE, Serratosa, JM, Brandt, C, Klein, P, Toledo, M, Krauss, GL. Practical guidance for the management of adults receiving adjunctive cenobamate for the treatment of focal epilepsy – expert opinion. Epilepsy Behav 2021 Oct:123:108270. [CrossRef]
- Schmitz, B, Lattanzi, S, Vonck, K, Kälviäinen, R, Nashef, L, Ben-Menachem, E. Cenobamate in refractory epilepsy: Overview of treatment options and practical considerations. Epilepsia Open 2023 Dec;8(4):1241-1255. [CrossRef]
- Green, SA, Kamin, M. Cenobamate trough plasma concentrations in patients with uncontrolled focal seizures achieving ≥50% and 100% seizure reduction in two randomized clinical studies. Poster presentation, S1.003, AAN 2021 Virtual Congress, 17-22 April.
Figure 1.
Correlation between daily doses of cenobamate (mg) and corresponding plasma levels (mg/l).
Figure 1.
Correlation between daily doses of cenobamate (mg) and corresponding plasma levels (mg/l).

Figure 2.
Correlation between daily doses of cenobamate (mg) and corresponding plasma levels (mg/l) in seizure-free and non-responding patients with epilepsy.
Figure 2.
Correlation between daily doses of cenobamate (mg) and corresponding plasma levels (mg/l) in seizure-free and non-responding patients with epilepsy.
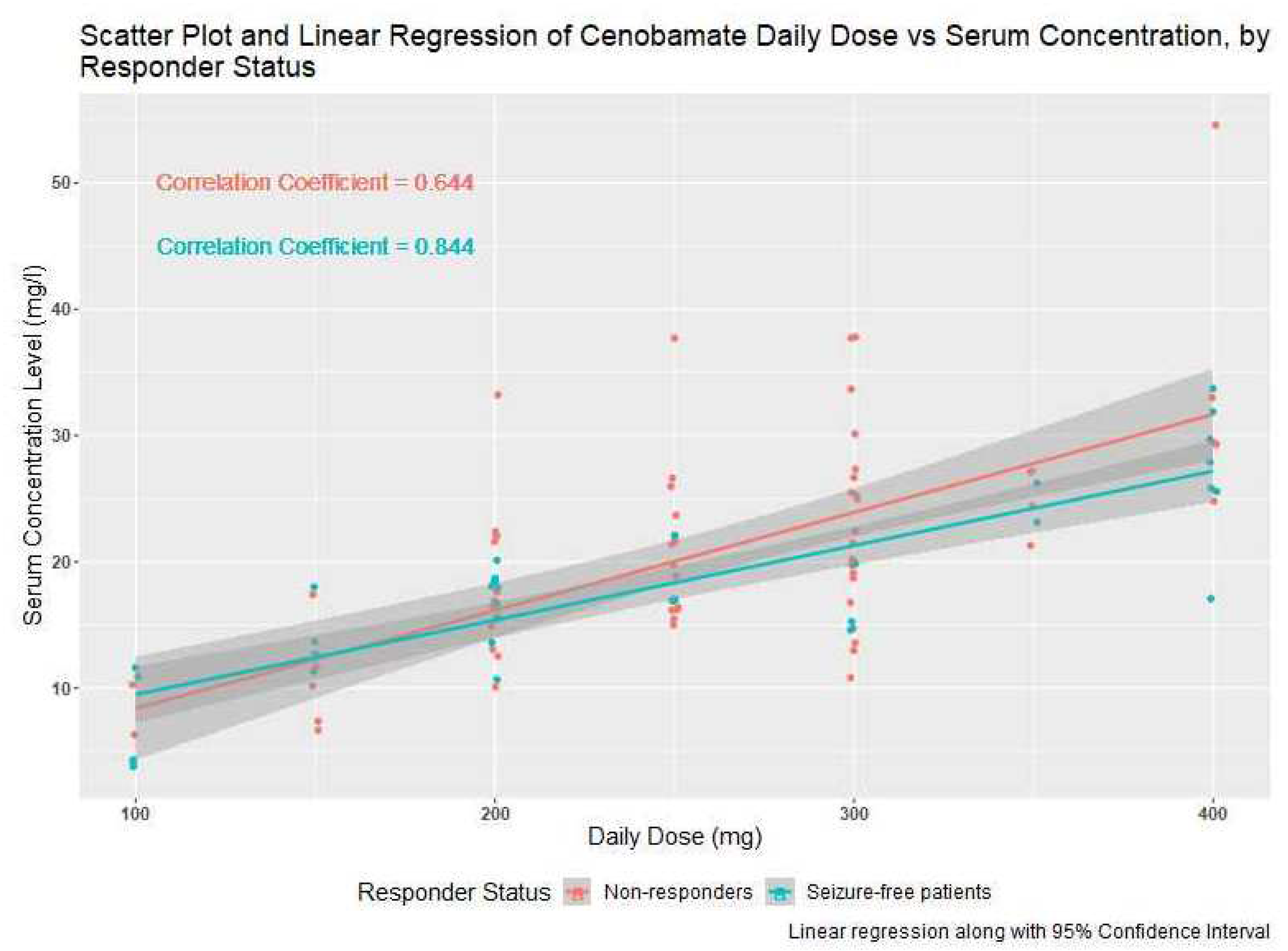

Table 1.
Demographic data.
| Seizure-free patients | Non-responding patients | No adverse events | Adverse events | |
|---|---|---|---|---|
| n | 36 | 65 | 70 | 31 |
| age (years) (mean) | 37.5 ± 15.9 | 37.9 ± 12.5 | 38.0 ± 14.0 | 37.3 ± 13.4 |
| Age (years) (median) | 32.5 | 35 | 33.5 | 39 |
| Age (years) range | 19 - 76 | 21 - 72 | 19 - 76 | 20 – 72 |
| Female (n, %) | 15 (43) | 36 (55) | 35 (50) | 16 (52) |
| Male (n, %) | 21 (57) | 29 (45) | 35 (50) | 15 (48 |
| Duration of epilepsy (years) (mean) | 22.5 ± 11.9 | 26.7 ± 14.5 | 26.7 ± 13.7 | 21.6 ± 13.3 |
| Duration of epilepsy (years) (median) | 20 | 25 | 23 | 15 |
| Duration of epilepsy (years) (range) | 7 – 55 | 1 – 56 | 6 – 56 | 1 - 48 |
| Seizure frequency per month prior to cenobamate (in case of daily seizures limited to 30) (mean) | 13.8 ± 12.8 | 13 ± 11.3 | 12.4 ± 11.5 | 15.2 ± 12.3 |
| Seizure frequency per month prior to cenobamate (in case of daily seizures limited to 30) (median) | 8 | 10 | 8 | 10 |
| Seizure frequency per month prior to cenobamate (in case of daily seizures limited to 30) (range) | 1 - 30 | 1 - 30 | 1 – 30 | 1 - 30 |
| Number of previous antiseizure medications (mean) | 9.6 ± 2.7 | 10.5 ± 4.5 | 10.0 ± 4.0 | 10.7 ± 3.8 |
| Number of previous antiseizure medications (median) | 10 | 10 | 10 | 10 |
| Number of previous antiseizure medications (range) | 4 - 15 | 4 - 27 | 4 – 27 | 5 - 19 |
| Number of comcomitant antiseizure medications (mean) | 1.5 ± 0.6 | 1.6 ± 0.7 | 1.6 ± 0.7 | 1.5 ± 0.6 |
| Number of concomitant antiseizure medications (median) | 1 | 2 | 2 | 1 |
| Number of concomitant antiseizure medications (range) | 1 – 3 | 0 - 3 | 0 – 3 | 1 – 3 |
Table 2.
Results.
| Seizure-free patients | Non-responding patients | No adverse events | Adverse events | |
|---|---|---|---|---|
| n | 36 | 65 | 70 | 31 |
| Seizure-free n (%) | 36 (100) | 0 (0) | 27 (39) | 9 (29) |
| Adverse events n (%) | 9 (25) | 22 (34) | 0 (0) | 31 (100) |
| Daily cenobamate dose (mean) | 240.3 ± 102.0 mg | 260.8 ± 73.2 mg | 257.1 ± 90.6 mg | 245.2 ± 70.0 mg |
| Daily cenobamate dose (median) | 200 mg | 250 mg | 250 mg | 250 mg |
| Daily cenobamate dose (range) | 100 – 400 mg | 100 mg – 400 mg | 100 – 400 mg | 100 – 400 mg |
| Cenobamate plasma level (mean) | 17.8 ± 7.1 mg/l | 20.9 ± 8.8 mg/l | 19.5 ± 7.7 mg/l | 20.4 ± 9.8 mg/l |
| Cenobamate plasma level (median) | 17.6 mg/l | 19.9 mg/l | 18.6 mg/l | 18.4 mg/l |
| Cenobamate plasma level (range) | 3.8 – 33.7 mg/l | 3.9 – 54.6 mg/l | 3.8 – 37.8 mg/l | 3.9 – 54.6 mg/l |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



