
Submitted:
22 January 2024
Posted:
23 January 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Long Covid is a debilitating condition that has been well-documented over the past 4 years and shares many similarities with other post-viral chronic illnesses. Despite this, clinicians are not confident in recognising the signs of Long Covid, or effectively managing the symptoms of their patients. This paper presents a single patient case report from a biomedical researcher who has had Long Covid for 2 years; it is written in relatively plain language to be accessible to both patients and clinicians across multiple specialities. The author has had the ability and expertise to keep up with the Long Covid research literature, and from that has cobbled together a management strategy that has alleviated her own symptoms, and those of other people with whom she has shared her protocol. The author’s experience of developing and managing her Long Covid is presented here, in the hopes that it may be of assistance to clinicians in identifying and managing Long Covid in their own patients.
Keywords:
Long Covid
; patient report
; symptom description
Introduction
Long Covid is a multi-system, systemic condition that follows on from an acute Covid-19 infection and was first described by patient reports in early 2020 [1,2]. Medical recognition of ongoing health issues caused by Covid-19 infections quickly followed, as clinicians began to see patients who simply “never got better” present with an array of symptoms, ranging from crushing fatigue, cognitive, memory and speech issues, joint pain, constant headaches, dizziness, blood pressure and heart rate issues, immune system dysregulation, new allergies, blurred vision, sensory sensitivities, rashes and hives, menstrual abnormalities, and gastrointestinal disturbance [3]. There is a long history of post-viral chronic illness, with the first formal detailed reports of patients who “never recovered” following illness appearing in the 1930s and 1940s, and the term myalgic encephalomyelitis (ME) established in 1955 [4]. The Covid-19 pandemic is the first time that infection acquired chronic conditions have been reported at such a large scale and proportion of the population, with 10% of all infections resulting in Long Covid, and an estimated at least 650 million people worldwide dealing with this new chronic condition [5].
Despite this prevalence and the extremely high-profile media coverage of Long Covid in the past few years, only 7% of clinicians feel confident recognising the signs of this condition, and only 4% of them feel they can manage and treat Long Covid [6]. The separation of medical care into distinct organ/body systems results in a disjointed and distressing experience of medical care for patients with infection-associated chronic conditions, especially because the number of experienced specialists trained in this field is extremely small (eg. https://mecfscliniciancoalition.org/about-us/). The current literature and understanding in the field of Long Covid research is also rapidly evolving and expanding, making it difficult for busy clinicians to maintain up to date knowledge of diagnosis and management options.
Patient-led work has been at the forefront of unravelling Long Covid since the early days of 2020; multiple formal research collectives and individual patients have pushed the science forwards and aided others who have developed this condition. The prevalence of Long Covid and the ongoing rate of infections means there will be a significant health burden well into the future; the author has written this paper in relatively plain language in the hopes that it will assist both clinicians and patients to recognise Long Covid and offer some effective management suggestions for this infection-associated chronic condition.
Patient risk factors for Long Covid
The author is a cis woman and was 35 [7,8] at the time of her one Covid-19 infection in February 2022. She has a history of mild/subclinical hypermobility [9] and bad hayfever/seasonal allergies [10]. She sustained a sacroiliac joint injury in 2019 during her second pregnancy and has since developed sacroiliac joint dysfunction (SIJD), a chronic inflammatory pain condition [11,12].
Vaccination status/experience
The author was vaccinated 9th January and 1st February 2021 with the Pfizer spike protein mRNA vaccine. She experienced multiple unusual side-effects: flaring of her SIJD for a week post both injections, to the extent that walking was extremely painful; severe gastrointestinal cramps and nausea any time she attempted to eat, for 5 days after each injection; pressure/squeezing headache for 5 days following each injection; extremely disturbed menstrual cycle (menstruation onset 48 hours after each injection; very heavy bleeding for 12 days after the first injection and 10 days after the second, with another very heavy 10 day bleed the month after the second injection. The author was taking the combined oral contraceptive pill at the time; the menstruation induced by vaccination overrode active contraceptive pills). This unusual reaction may be indicative of a systemic sensitivity or inappropriate immune response to the presence of the Covid-19 spike protein, potentially indicating increased risk for Long Covid.
Acute infection symptoms
The acute infection period lasted for 3 weeks, and began with diarrhea, aching swollen glands, sore throat, pressure headache, and extreme fatigue. The author then developed a cough, mild fever, runny nose and stuffy sinuses, severe joint and muscle pain, and constantly elevated heart rate between 120-130 bpm regardless of activity level or postural position. At no point did the author’s fever reach above 101oF, and her blood oxygen levels never decreased below 95%. The symptoms were managed with pain and fever medications; there was no ability to access antivirals or other specialised medication.
Long-term symptoms
The author has continued to experience symptoms for the past 2 years consisting of cough, sore throat, unrefreshing sleep, pressure headache, extreme fatigue, hives, severe hayfever reactions, joint pain, joint subluxations, muscle pain, sensory sensitivities, phantom sensations, cognitive, memory and speech issues, covid toes, muscle weakness, tachycardia, heart palpitations, irregular menstruation, vertigo/dizziness, shortness of breath, and post-exertional malaise (PEM) which is the condition in which all symptoms worsen following activity or exertion. See Table 1 for a timeline of when these symptoms appeared, and Figure 1 for examples of hives and covid toes. A plain language description of how the symptoms feel to experience is included, to aid healthcare providers in identifying the occurrence of Long Covid in their patients.

Table 1.
Onset, duration, and plain language description of the long-term symptoms resulting from the author’s Covid-19 infection.
Table 1.
Onset, duration, and plain language description of the long-term symptoms resulting from the author’s Covid-19 infection.
| Symptom | Time of onset | Duration | Plain language description |
|---|---|---|---|
| Cough | Day 2 of infection | 4 months | Month 1: wet and productive cough, month 2-4: unproductive, dry cough |
| Sore throat | Day 2 of infection | Ongoing | Dry, scratchy and painful throat, hurts to swallow |
| Pressure headache | Day 2 of infection | 5 months constant, then 2 days a week ongoing | It feels like a fork is being scraped over the front half of my brain while the back half of my brain is being squeezed in a vice |
| Extreme fatigue | Day 2 of infection | Ongoing | I slept for 16+ hours every day for the first 4 months post infection. If I try to fight or push through feeling tired, I will wind down like I'm running out of batteries and black out from exhaustion, no matter where I am or whether I am lying down. My current sleep baseline is 12 hours a day, with 3-4 days a month needing 16 hours of sleep a day. It feels like I am being drained and weakened, the longer I stay awake past my energy envelope. |
| Unrefreshing sleep | 3 weeks post infection | 22 months constant, then 3 days a week ongoing | No matter how much I sleep, or how well I sleep, I wake up feeling the same or worse as when I went to sleep |
| Joint pain | Day 2 of infection | Ongoing | Deep persistent ache within shoulder, elbow, wrist, and pelvic joints |
| Joint subluxations | 2 weeks post infection | Ongoing | My shoulders now pop out of place and back in if I lift my arm too quickly; it feels like a popping then crunching sensation at the shoulder joint, followed by increased muscle and joint pain in that joint. My ribs will slip out of place and I then have a stabbing sensation in my back every time I try to breathe or bend over, until the joint settles back into place |
| Muscle pain | Day 2 of infection | Ongoing | Burning and aching muscles, similar to the sensation following a hard workout, but present at all times |
| Sensory sensitivities | 3 weeks post infection | Ongoing | I have become extremely jumpy in response to any sudden noise or movement; it’s as if my brain has difficulty filtering out irrelevant stimuli. Listening to music, or fast speaking in television/movies, brings on a pressure headache and makes my brain feel like it’s full of static |
| Phantom sensations | 3 weeks post infection | Ongoing | Pinching and stinging sensations that feel like I am being bitten by a spider; these usually repeat every 10 minutes in the same body location over an hour or two |
| Cognitive deficits | 2 weeks post infection | Ongoing | Difficulty following conversations; video calls are overwhelming and bring on a pressure headache if they last past 15 minutes; constant mistakes while typing; having my brain "shut down" and feel like it's full of static if I try to engage in high level thinking or conversation for longer than 30 minutes at a time |
| Memory dysfunction | 2 weeks post infection | Ongoing | Complete loss of memory from the 2 months post infection; previous recall ability is severely reduced; reliant on lists and online calendars to remember anything where previously I was able to run science experiments, manage a household, and parent without difficulty |
| Speech issues | 2 weeks post infection | Ongoing | Losing words mid-sentence and being unable to recall them; saying the wrong word in a sentence and not realising, then being incapable of producing the right word even when corrected and making an effort to do so |
| Covid toes | 3 weeks post infection | Ongoing | Swollen, painful, red skin that appears on the edge of toenails and spreads down to the nearest knuckle; this skin then dies and forms a large white blister-like patch before peeling off |
| Muscle weakness | Day 2 of infection | Ongoing | Shaky and weak; unable to lift everyday objects, frequently dropping household items, burning myself on the oven or stove multiple times a day because my hands don't respond like they used to |
| Tachycardia | Day 2 of infection | Ongoing | During illness or times of stress, my heart rate increases to 120-130 bpm and stays there regardless of activity level or postural position |
| Palpitations | Day 2 of infection | 22 months constant, now in times of illness | My heart constantly skips beats, lurches and does half-beats, and pauses in the middle of beats so that it feels like it's not going to restart |
| Irregular menstruation | During acute infection | Ongoing | Despite taking the oral contraceptive pill; loss of period during acute illness, followed by extremely heavy 10 day long bleeds every month from March 2022 - September 2022; loss of menstruation starting in December 2022, with 4-6 month gaps between periods for the year of 2023 |
| Vertigo/dizziness | 2 weeks post infection | Ongoing | Brought on by sudden postural changes; at its worst I was unable to sit upright without the entire room tilting and spinning around me; daily occurrences of stumbling sideways due to sudden onset dizziness |
| Shortness of breath | During acute infection | Ongoing | Tightness around my ribs and chest, like an iron band is squeezing me and I can't ever draw in a full breath; worsens with physical exertion |
| Hives | 6 weeks post infection | 18 months | Dry, itchy and painful. I was scratching in my sleep until I bled |
| Severe hayfever reactions | 6 weeks post infection | Ongoing, occur every 2 weeks | Itchy deep within my sinuses and nostrils, uncontrollably sneezing every 90 seconds for 36 hours straight, streaming itchy eyes, sudden pressure headache, severe joint pain, muzzy headed and foggy brained. Feel like I’ve been hit by a truck full of pollen |
| Post-exertional malaise (PEM) | 3 weeks post infection | Ongoing | All of the above symptoms worsen when I over-exert myself mentally, physically or emotionally; PEM also feels like a combination of having a bad hangover, jetlag, coming down with the flu, and extreme exhaustion all at the same time, on top of the other symptoms worsening |
Figure 1.
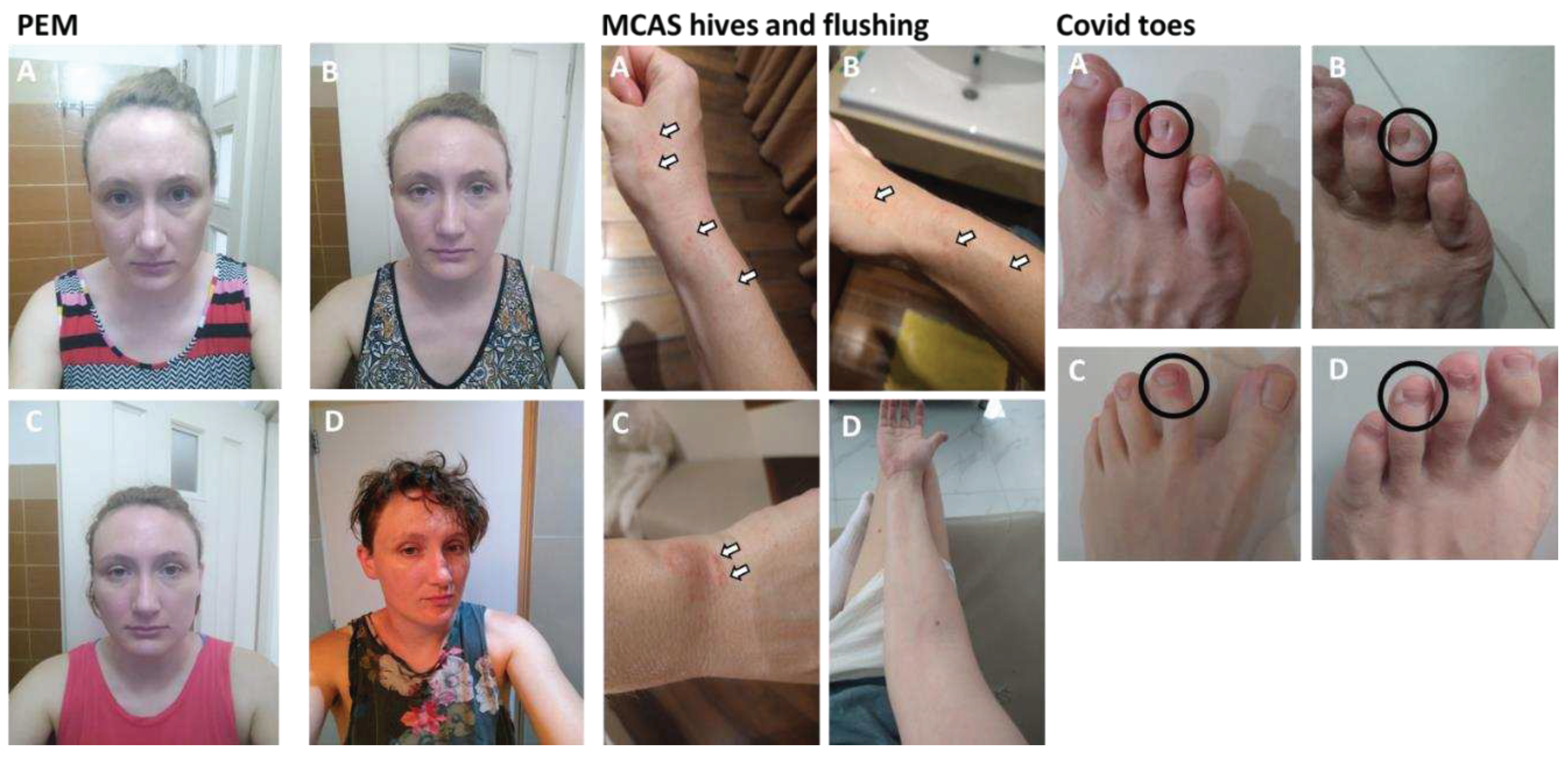
Visual examples of some long-term Long Covid symptoms experienced by the author: PEM (A) day 1 one of a PEM episode after 14 hours sleep (B) day 2 of the same PEM episode after 14 hours sleep (C) day 3 of the same PEM episode after 12 hours sleep (D) the author a few months before her covid infection, under similar photograph conditions. MCAS hives and flushing: (A-C) MCAS hives (white arrows) (D) MCAS flushing in the skin of arms. Covid toes (black circles): (A-B) progression of the red swelling to dead skin blistering observed with Covid toes (C) example of the red swelling (D) example of the dead skin blistering.
Figure 1.
Visual examples of some long-term Long Covid symptoms experienced by the author: PEM (A) day 1 one of a PEM episode after 14 hours sleep (B) day 2 of the same PEM episode after 14 hours sleep (C) day 3 of the same PEM episode after 12 hours sleep (D) the author a few months before her covid infection, under similar photograph conditions. MCAS hives and flushing: (A-C) MCAS hives (white arrows) (D) MCAS flushing in the skin of arms. Covid toes (black circles): (A-B) progression of the red swelling to dead skin blistering observed with Covid toes (C) example of the red swelling (D) example of the dead skin blistering.
At 3 months post infection, the author did not display any organ damage or unusual results other than slightly elevated blood cholesterol in a basic blood panel. She meets diagnostic criteria for postural orthostatic tachycardia syndrome (POTS) [13], mast cell activation syndrome (MCAS) [14], and myalgic encephalomyelitis (ME) [15,16]. The author shows signs of immune system dysfunction; her hepatitis B antibody titres were below detectable levels in May 2022, despite completing the primary vaccine course in 2014, and she has frequent illness at a level beyond her previous experience (in the past 2 years: 4 hand foot and mouth virus infections, 5 sinus infections requiring antibiotics, 3 bouts of RSV, 5 colds, and one influenza infection).
The author has not been able to access specialist Long Covid or post-viral chronic illness care; she is monitored by a general practice clinic and advised on medications by her pharmacist. She is a biomedical researcher who has been able to parse the papers about Long Covid and cobble together some management strategies with the help of her medical team, which are discussed below in the hopes that they will be of assistance to other clinicians.
Management of long-term Long Covid symptoms
The author has been tracking her Long Covid symptoms and management strategies using the Visible app (https://www.makevisible.com/). Lifestyle modifications include resting and pacing according to the ME action net guides (https://www.meaction.net/stoprestpace/), weekly deep-tissue massage therapy, abstaining from alcohol, and using compression garments. Medications, supplements, and other interventions are listed in Table 2, along with dosing, timing, and the side effects experienced by the author. Changes in symptoms are included, and rationale/references provided for each intervention. Over the past 2 years the author has progressed from moderate Long Covid (FUNCAP55 score of 3.42 [15] at 3 months post infection, house-bound and unable to stay awake for longer than 2 hours at a time) to engaging in scientific work part-time and undertaking physiotherapy at least 3 times a week (FUNCAP55 score of 4.22 [15]). These interventions have also alleviated the symptoms of 4 other people with Long Covid whom the author shared her management protocol with, and may be helpful for other patients. Thus, a plain language description of the side-effects and symptom alleviation for each is included in Table 2, to assist healthcare workers in managing Long Covid in their patients.
Discussion
Long Covid is a debilitating and devastating chronic illness; not only does it lead to patients feeling terrible all the time, it also results in loss of employment, inability to parent your children, breakdown of marriages, and destruction of your identity and life as you previously knew it. Long Covid patients are at significantly increased risk for suicide (see review [41]) due both to the unrelenting nature of their illness, and the lack of societal and medical support they receive. The author has been extremely fortunate to have both the education and access to understand and trial various interventions for her Long Covid; other patients do not have these privileges and are thus reliant on medical staff to identify and manage this condition. The author has written up her experience in the hopes that it aids clinicians and other healthcare workers in identifying and supporting their patients with Long Covid. Identifying the signs of Long Covid and appropriately managing symptoms from early in the course of this illness spares patients from increased suffering and may help preserve their health until the time there is a full treatment available.
Acknowledgements
The author would like to thank the Patient-Led Research Collaborative (PLRC) for their support in producing this manuscript, and gratefully acknowledges those who went before her for their advice and guidance regarding Long Covid, particularly Hannah Davis, Renuka Dhinakaran, Kristin Houlihan and LongCovidPharmD.
Conflicts of Interest
The author declares no conflicts of interest; there was no funding provided for this work. There was no use of generative AI in producing any part of this manuscript.
References
- Greenhalgh, T., et al., Management of post-acute covid-19 in primary care. BMJ, 2020. 370: p. m3026. [CrossRef]
- Mohammed F. Islam, J.C.L.A.J., Post-viral fatigue and COVID-19: lessons from past epidemics. Fatigue: Biomedicine, Health & Behavior, 2020. 8(2): p. 61-69. [CrossRef]
- Davis, H.E., et al., Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol, 2023. 21(3): p. 133-146. [CrossRef]
- MEpedia. History of myalgic encephalomyelitis and chronic fatigue syndrome. 2023; Available from: https://me-pedia.org/wiki/History_of_myalgic_encephalomyelitis_and_chronic_fatigue_syndrome#:~:text=It%20was%20named%20myalgic%20encephalomyelitis,redefined%20as%20Chronic%20Fatigue%20Syndrome.
- Ballering, A.V., et al., Persistence of somatic symptoms after COVID-19 in the Netherlands: an observational cohort study. Lancet, 2022. 400(10350): p. 452-461. [CrossRef]
- Foundation, d.B., Poll: Physicians agree Long Covid is a problem but are unprepared to treat it. 2022.
- Bai, F., et al., Female gender is associated with long COVID syndrome: a prospective cohort study. Clin Microbiol Infect, 2022. 28(4): p. 611 e9-611 e16. [CrossRef]
- Torjesen, I., Covid-19: Middle aged women face greater risk of debilitating long term symptoms. BMJ, 2021. 372: p. n829. [CrossRef]
- Gavrilova, N., et al., New Clinical Phenotype of the Post-Covid Syndrome: Fibromyalgia and Joint Hypermobility Condition. Pathophysiology, 2022. 29(1): p. 24-29. [CrossRef]
- Wolff, D., et al., Allergic diseases as risk factors for Long-COVID symptoms: Systematic review of prospective cohort studies. Clin Exp Allergy, 2023. 53(11): p. 1162-1176. [CrossRef]
- Rivera, J., et al., Prevalence of post-COVID-19 in patients with fibromyalgia: a comparative study with other inflammatory and autoimmune rheumatic diseases. BMC Musculoskelet Disord, 2022. 23(1): p. 471. [CrossRef]
- Sapkota, H.R. and A. Nune, Long COVID from rheumatology perspective - a narrative review. Clin Rheumatol, 2022. 41(2): p. 337-348. [CrossRef]
- Raj, S.R., A. Fedorowski, and R.S. Sheldon, Diagnosis and management of postural orthostatic tachycardia syndrome. CMAJ, 2022. 194(10): p. E378-E385. [CrossRef]
- Afrin, L.B., et al., Diagnosis of mast cell activation syndrome: a global "consensus-2". Diagnosis (Berl), 2021. 8(2): p. 137-152. [CrossRef]
- Sommerfelt, K.S., T.; Seton, K.A.; Carding, S.R. Assessing Functional Capacity in ME/CFS: A Patient Informed Questionnaire. Preprints 2023. 2023092091. [CrossRef]
- Grach, S.L., et al., Diagnosis and Management of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Mayo Clin Proc, 2023. 98(10): p. 1544-1551. [CrossRef]
- Butterfield, J.H., Survey of aspirin administration in systemic mastocytosis. Prostaglandins Other Lipid Mediat, 2009. 88(3-4): p. 122-4. [CrossRef]
- Etheresia Pretorius, C.V., Gert Jacobus Laubscher et al. Combined triple treatment of fibrin amyloid microclots and platelet pathology in individuals with Long COVID/ Post-Acute Sequelae of COVID-19 (PASC) can resolve their persistent symptoms. Research Square, 28 December 2021. [CrossRef]
- Snapper, H. and W.P. Cheshire, Oral and intravenous hydration in the treatment of orthostatic hypotension and postural tachycardia syndrome. Auton Neurosci, 2022. 238: p. 102951. [CrossRef]
- Schloss, J.V., Nutritional deficiencies that may predispose to long COVID. Inflammopharmacology, 2023. 31(2): p. 573-583. [CrossRef]
- Ranisavljev, M., et al., Reduced tissue creatine levels in patients with long COVID-19: A cross-sectional study. J Postgrad Med, 2023. 69(3): p. 162-163. [CrossRef]
- Slankamenac, J., et al., Creatine supplementation combined with breathing exercises reduces respiratory discomfort and improves creatine status in patients with long-COVID. J Postgrad Med, 2023. [CrossRef]
- Hsu, R.L., et al., Amyloid-degrading ability of nattokinase from Bacillus subtilis natto. J Agric Food Chem, 2009. 57(2): p. 503-8. [CrossRef]
- Tanikawa, T., et al., Degradative Effect of Nattokinase on Spike Protein of SARS-CoV-2. Molecules, 2022. 27(17). [CrossRef]
- Chansaenroj, J., et al., Long-term persistence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike protein-specific and neutralizing antibodies in recovered COVID-19 patients. PLoS One, 2022. 17(4): p. e0267102. [CrossRef]
- Arman Fesharaki-Zadeh, N.L., Amy F.T. Arnsten, Clinical experience with the α2A-adrenoceptor agonist, guanfacine, and N-acetylcysteine for the treatment of cognitive deficits in “Long-COVID19”. Neuroimmunology Reports, 2023. 3(100154). [CrossRef]
- McPherson, R.A., et al., N -acetylcysteine is associated with reduction of postconcussive symptoms in elderly patients: A pilot study. J Trauma Acute Care Surg, 2022. 93(5): p. 644-649. [CrossRef]
- Zubchenko, S., et al., Herpesvirus infections and post-COVID-19 manifestations: a pilot observational study. Rheumatol Int, 2022. 42(9): p. 1523-1530. [CrossRef]
- German, E.R., M.K. Jairath, and J. Caston, Treatment of Long-Haul COVID Patients With Off-Label Acyclovir. Cureus, 2023. 15(4): p. e37926. [CrossRef]
- Bramante, C.T., et al., Outpatient treatment of COVID-19 and incidence of post-COVID-19 condition over 10 months (COVID-OUT): a multicentre, randomised, quadruple-blind, parallel-group, phase 3 trial. Lancet Infect Dis, 2023. 23(10): p. 1119-1129. [CrossRef]
- Andrzejewski, S., et al., Metformin directly acts on mitochondria to alter cellular bioenergetics. Cancer Metab, 2014. 2: p. 12. [CrossRef]
- Appelman, B., et al., Muscle abnormalities worsen after post-exertional malaise in long COVID. Nat Commun, 2024. 15(1): p. 17. [CrossRef]
- Chen, T.H., C.J. Chang, and P.H. Hung, Possible Pathogenesis and Prevention of Long COVID: SARS-CoV-2-Induced Mitochondrial Disorder. Int J Mol Sci, 2023. 24(9). [CrossRef]
- Cookson, H. and C. Grattan, An update on mast cell disorders. Clin Med (Lond), 2016. 16(6): p. 580-583. [CrossRef]
- Salvucci, F., et al., Antihistamines improve cardiovascular manifestations and other symptoms of long-COVID attributed to mast cell activation. Front Cardiovasc Med, 2023. 10: p. 1202696. [CrossRef]
- Heald, A., et al., Reducing fatigue-related symptoms in Long COVID-19: a preliminary report of a lymphatic drainage intervention. Cardiovasc Endocrinol Metab, 2022. 11(2): p. e0261. [CrossRef]
- Espejo, J.A., M. Garcia-Escudero, and E. Oltra, Unraveling the Molecular Determinants of Manual Therapy: An Approach to Integrative Therapeutics for the Treatment of Fibromyalgia and Chronic Fatigue Syndrome/Myalgic Encephalomyelitis. Int J Mol Sci, 2018. 19(9). [CrossRef]
- Li, H., et al., Chronic fatigue syndrome treated by the traditional Chinese procedure abdominal tuina: a randomized controlled clinical trial. J Tradit Chin Med, 2017. 37(6): p. 819-826. [CrossRef]
- Bourne, K.M., et al., Compression Garment Reduces Orthostatic Tachycardia and Symptoms in Patients With Postural Orthostatic Tachycardia Syndrome. J Am Coll Cardiol, 2021. 77(3): p. 285-296. [CrossRef]
- Eastin E F, T.A., Quach T C, et al. New Alcohol Sensitivity in Patients With Post-acute Sequelae of SARS-CoV-2 (PASC): A Case Series. Cureus, 2023. 15. [CrossRef]
- Sher, L., Long COVID and the risk of suicide. Gen Hosp Psychiatry, 2023. 80: p. 66-67. [CrossRef]
Table 2.
Interventions, medications and supplements used by the author to manage her Long Covid symptoms. A plain language description of side effects and symptom changes are included to help clinicians with treating their own patients. Rationale and references are provided for further information.
Table 2.
Interventions, medications and supplements used by the author to manage her Long Covid symptoms. A plain language description of side effects and symptom changes are included to help clinicians with treating their own patients. Rationale and references are provided for further information.
| Intervention | Time of day | Dosage | Side effects | Symptoms alleviated | Rationale & references |
|---|---|---|---|---|---|
| Aspirin | 7am | 160mg | Nil | Cognitive and speech issues, joint pain, joint subluxations, extreme fatigue | Aspirin brings down MCAS symptoms [17], reduces incidence of blood clots, and breaks down Long Covid microclots [18] |
| Rehydration salts, berocca and creatine | 7am | 1 litre water with 1 pouch rehydration salts, 1 berocca tablet, 1 scoop creatine | Nil | Vertigo/dizziness, pressure headache, muscle weakness | Bolus fluids alleviate POTS symptoms [19], B vitamins are deficient in Long Covid [20], creatine relieves Long Covid symptoms [21,22] |
| Nattokinase | 9pm | 6000 units | Occasional nausea and heart burn sensation; taking 2 hours after dinner helps prevent this | Long and heavy menstruation, extreme fatigue, cognitive and speech issues, covid toes | Nattokinase breaks down amyloid clots [23] and also breaks down Covid-19 spike protein [24], which is known to persist in the body after Covid-19 infection [25] |
| N-acetylcysteine (NAC) | 9pm | 1 tablet | Nil | Cognitive and speech issues | NAC is known to reduce cognitive issues in Long Covid [26] and following concussion [27] |
| Acyclovir | 9pm every 2 days | 400mg | Upper left abdominal pain; lightheadedness; nausea; adjusting dosage helped stop these | Cognitive and speech issues, extreme fatigue | Herpes virus activation in Long Covid is known to contribute to health issues [28] and acyclovyr has been trialled as a treatment in a small group of Long Covid patients [29] |
| Metformin | 9pm | 500mg | Nausea and upset stomach alternating between diarrhea and constipation for the first 10 days | Cognitive, speech and memory issues, extreme fatigue, muscle weakness, muscle pain, covid toes, unrefreshing sleep, sensory sensitivities, palpitations, and tachycardia | Metformin reduces incidence of Long Covid if given during acute infection [30], and aids in mitochondrial repair and function [31] which are deficient in Long Covid [32,33] |
| Ibuprofen | 9pm | 400mg | Nil | Muscle pain and joint pain | Ibuprofen is an anti-inflammatory pain medication |
| Antihistamine (fexofenadine hydrochloride) | 9pm | 180mg | Nil | Hives, severe hayfever reactions, joint subluxations, extreme fatigue, cognitive issues, palpitations | Antihistamines are used for the management of MCAS [34] and alleviate Long Covid symptoms [35] |
| Multivitamin | 9pm | 1 tablet | Nil | Long Covid patients display vitamin deficiencies [20] | |
| Massage therapy | 9am | 90 minutes weekly | Increased fatigue immediately after, I usually sleep after a massage | Muscle pain, joint pain, muscle weakness, extreme fatigue, cognitive issues | Lymphatic drainage massage alleviates Long Covid symptoms [36], and full body massage alleviates ME symptoms [37,38] |
| Thuan Moc ointment | 9am and 9pm | Apply directly to hives | Nil | Hives (completely eliminated after a few weeks of use) | Most likely due to the willow bark extract in the cream |
| Compression socks | All day | Feeling spacey and light-headed | Extreme fatigue, PEM | Compression socks help to regulate blood pressure issues caused by POTS [39] | |
| Abstinence from alcohol | Constant | Extreme fatigue, joint pain, muscle pain, headache, vertigo/dizziness | Alcohol exacerbates Long Covid symptoms [40] | ||
| Resting and pacing | All the time | Scheduling rest before and after activity; making sure to sleep whenever I felt tired | Nil | Extreme fatigue, cognitive and speech issues, muscle pain, PEM | Resting and pacing is a well-established management technique for infection-associated chronic conditions (https://www.meaction.net/stoprestpace/) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



