
Submitted:
22 January 2024
Posted:
23 January 2024
You are already at the latest version
Abstract
This paper provides an exhaustive narrative review of third-generation antipsychotics (TGAs), focusing on aripiprazole, cariprazine, brexpiprazole, and lurasidone for managing substance-induced psychosis. It includes a comprehensive literature review to evaluate the efficacy and tolerability of these medications. The paper emphasizes the distinct challenges in treating substance-induced psychosis, which is a psychiatric condition triggered by the misuse or withdrawal of various substances, leading to symptoms like hallucinations and delusions, and is distinct from primary psychotic disorders. It underscores the potential of TGAs in addressing both psychotic symptoms and substance-related issues, while highlighting the need for more research on long-term effects and advocating for an integrated approach combining pharmacological and psychological interventions
Keywords:
substance abuse
; psychostimulants
; schizophrenia
; third generation antipsychotics
; cariprazine
; lurasidone
; aripiprazole
1. Introduction
Based on the existing body of literature, there is robust evidence supporting a correlation between substance abuse and the initiation of psychotic symptoms. Numerous research findings indicate that illicit substances like cannabinoids, cocaine, amphetamines, and hallucinogens exhibit psychotomimetic properties (1-2). This implies that their usage not only triggers temporary psychotic symptoms during acute intoxication but may also result in a syndrome closely resembling a primary psychotic disorder. In recent decades, a diverse range of novel psychoactive substances has emerged, encompassing synthetic cannabinoids, cathinone derivatives, psychedelic phenethylamines, new stimulants, synthetic opioids, tryptamine derivatives, phencyclidine-like dissociatives, piperazines, and GABAA/B receptor agonists. These substances are increasingly prevalent in the landscape of substance abuse (3).
A complex clinical challenge revolves around accurately differentiating substance-induced psychosis from a primary psychotic disorder or a psychotic disorder co-occurring with substance use. This poses a nuanced dilemma and an opportunity for thorough investigation, gaining significance when determining the optimal therapeutic approach for patients. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) T.R. (4), more accurately describes the substance/medication-induced psychotic disorder as a psychiatric condition characterized by delusions and/or hallucinations that arise during or shortly following the intoxication or withdrawal from a substance.
Additionally, the symptoms of a non-substance-induced psychotic disorder are not yet fully understood. Nevertheless, in this context, a particular definition has been formulated utilizing the diagnostic classification of "substance-related exogenous psychosis (SREP)." This concept refers to a range of psychotic symptoms that are temporary or enduring, and are associated with substance use. These include changes in consciousness; feelings of being persecuted; disorders affecting sense perception, like visual and bodily hallucinations; impulsive behavior, self or other directed aggression, and psychomotor restlessness; fluctuations in mood; negative effects such as indifference, lack of motivation, and inability to feel pleasure; an overwhelming feeling of being detached from reality; and maintained self-awareness. (1). Various clinical subtypes of substance-induced psychosis have been delineated, categorized based on prevalent symptoms and implicated neurotransmitters. Examples include synthetic psychosis characterized by predominant dissociative reactions triggered by substances that impact glutamatergic pathways; this form of synthetic psychosis is characterized by dominant paranoia and auditory hallucinations, resulting from substances that primarily target dopaminergic pathways. Additionally, there is a type of synthetic psychosis with prominent hallucinatory symptoms, caused by substances that chiefly affect serotoninergic pathways, among other variations (5)
The occurrence of drug-induced psychosis appears to be associated with various pathogenetic mechanisms: (a) elevated levels of central dopamine, particularly for hallucinogens or psychedelic substances, stimulants, and cathinone derivatives; (b) Activity as an agonist at cannabinoid CB1 receptors, particularly in substances related to cannabis; (c) Agonist activity at 5HT2A receptors in hallucinogenic plants, newer phenethylamines, and tryptamine derivatives; (d) Activity as an antagonist at NMDA receptors (n-methyl-D-aspartate receptors) seen in substances like ketamine and methoxetamine; and (e) Activation of k-opioid receptors in plants such as Salvia divinorum(6).
However, currently, there are no comprehensive guidelines for the management of these patients (7-11). Antipsychotic agents are established as the primary modality for treating schizophrenia and are generally effective in managing substance-induced psychoses as well. These medications are categorized into two groups: typical antipsychotics, also referred to as first-generation antipsychotics (FGA), and atypical antipsychotics, known as second-generation antipsychotics (SGA). The FGA class exhibits a relatively uniform pharmacological profile, whereas the SGA category displays a more diverse range, both pharmacologically and clinically. FGAs are marked by their strong antagonism of the dopamine D2 receptor. This action is beneficial in attenuating the heightened activity of the mesolimbic dopaminergic pathway, thereby mitigating hallucinations and delusions associated with this hyperactivity. However, D2 antagonism in the mesocortical pathway can exacerbate negative and cognitive symptoms. Additionally, pronounced D2 blockade is linked to notable adverse effects, including extrapyramidal symptoms and hyperprolactinemia, arising from receptor inhibition in the nigrostriatal and tuberoinfundibular pathways. SGAs were developed with dual objectives: to reduce the incidence of these adverse effects by moderating the hyperactivity of the mesolimbic dopaminergic circuit in a more physiological manner and to address negative symptoms and cognitive deficits that were either unimproved or worsened by FGAs. Although SGAs lack a unifying pharmacological characteristic, a distinguishing feature of these drugs, in contrast to FGAs, is their concurrent antagonism of both dopamine D2 and serotonin 5-HT2A receptors. The affinity ratio for these receptors has been considered an indicative measure of their "atypicality. nRegarding substance induce psychosis, clear indications have not emerged, as in most cases studies refer to specific psychiatric disorders or the concurrent presence of withdrawal symptoms, without specifically focusing on psychotic symptoms (12-19). According to an Italian study based on a survey of antipsychotic drug prescription practices, in managing patients with psychosis induced by substance, particularly in acute situations, haloperidol has been the most frequently chosen initial treatment drug, followed by aripiprazole and olanzapine, while in the maintenance phase, aripiprazole was the most commonly used first-choice drug, followed by olanzapine. Almost half of the surveyed specialists used long-acting agents, while about a third did not. For clinicians prescribing long-acting medications, factors such as effectiveness, management of impulsivity, and the ability to target specific symptoms were key considerations in their decision-making process. During the maintenance phase, the emphasis was on enhanced patient adherence and drug tolerability (20). The employment of long-acting antipsychotics as the initial treatment for patients experiencing their first episode of psychosis, alongside a substance use disorder, has been instrumental in lowering the chances of relapse and the need for rehospitalization, even in patients presenting with challenging prognostic factors (21).
In recent years, the development of molecules that act as partial agonists, instead of antagonists, at dopaminergic receptors has constituted a major breakthrough in the treatment of psychosis. This innovation has led to the introduction of third-generation antipsychotics, which include medications such as cariprazine, brexpiprazole, and aripiprazole. Additionally, lurasidone, though not classified within this newer generation, demonstrates distinct pharmacodynamic properties. It exhibits antagonistic effects on D2 dopaminergic receptors and serotonin 5-HT2A and 5-HT7 receptors, and it is notable for its robust safety profile. These drugs are increasingly acknowledged for their therapeutic efficacy, safety, and ease of management in clinical settings.
1.1. Research Goals and Objectives:
The purpose of this study is to analyze in a narrative way the currently published literature on the long-term management of substance-induced psychosis, particularly evaluating the use of third-generation antipsychotics (TGAs) (aripiprazole, cariprazine, brexpiprazole) and lurasidone, and to describe any efficacy/tolerability issues recorded. This research aims to fill a critical gap in existing literature by providing a comprehensive overview of the effectiveness and challenges associated with TGAs in the management of substance-induced psychosis.
2. Matherials and Methods
2.1. Data Extraction
Literature search was performed using PubMed (via MEDLINE) and Scopus databases on December 21, 2023, starting from January 1985. We used the following search string: (aripiprazole OR brexpiprazole OR cariprazine OR lurasidone) AND (psychosis OR schizophrenia OR schizoaffective) AND (“substance use disorder” OR cocaine OR alcohol OR cannabis OR heroin OR amphetamine OR metamphetamine OR psychostimulants OR “double diagnosis” OR “dual diagnosis”). During the search the terms were also being converted to: (cannabis/thc/maryuana* OR; amphetamine METH OR * OR psychosis/ non-affective psychosis/schizophrenia*). Only original articles related to the se of third generation antipsychotics (aripiprazole, brexpiprazole, cariprazine) and (lurasidone) in the context of a substance induced psychosis or comorbidid schizophrenia and substance abuse written in English were selected. Experimental and observational studies, post-marketing surveillance reports, case reports, case series, and fatality reports were included. The exclusion criteria included non-original research (e.g., reviews, commentaries, editorials, book chapters, and letters to the editor), non-full-text articles (e.g., meeting abstracts), works in a language other than English. Research incorporating animal or in vitro experiments was considered for inclusion. While letters to the editor, conference proceedings, and book chapters were not directly included in the literature review, they were referenced for obtaining additional secondary sources. Given the vast scope of the topic under study, employing a systematic method for data analysis and conducting statistical comparisons of the collected data was not feasible. The substances discussed exhibit distinct heterogeneity in their characteristics, which necessitated the use of a descriptive methodology to offer a comprehensive and detailed perspective on this subject.
2.2. Data Synthesis Strategy
Narrative reviews are commonly recognized for not incorporating databases and specific inclusion criteria (22-23). Nevertheless, to enhance the clarity and transparency of our research, we have taken into consideration and systematized essential details such as the authors' names, year of publication, study design, demographic variables (gender, age, psychiatric history), specifics of the antipsychotic drugs used (including dosage and administration route), any concurrent substances, and the observed effects of these drugs on both psychotic symptoms and substance-related outcomes. Furthermore, we have considered animal studies and their possible impact on future applications in humans The effectiveness of a narrative review can be enhanced by incorporating methodological aspects from systematic reviews, which are designed to mmminimize bias in choosing articles, and by using a robust bibliographic search technique.The literature search and selection process were conducted by two investigators (V.R and D.D.B), under the guidance of supervisor G.M. This process involved a two-stage independent review by the investigators, followed by a collaborative cross-check to ensure consistency and thoroughness.
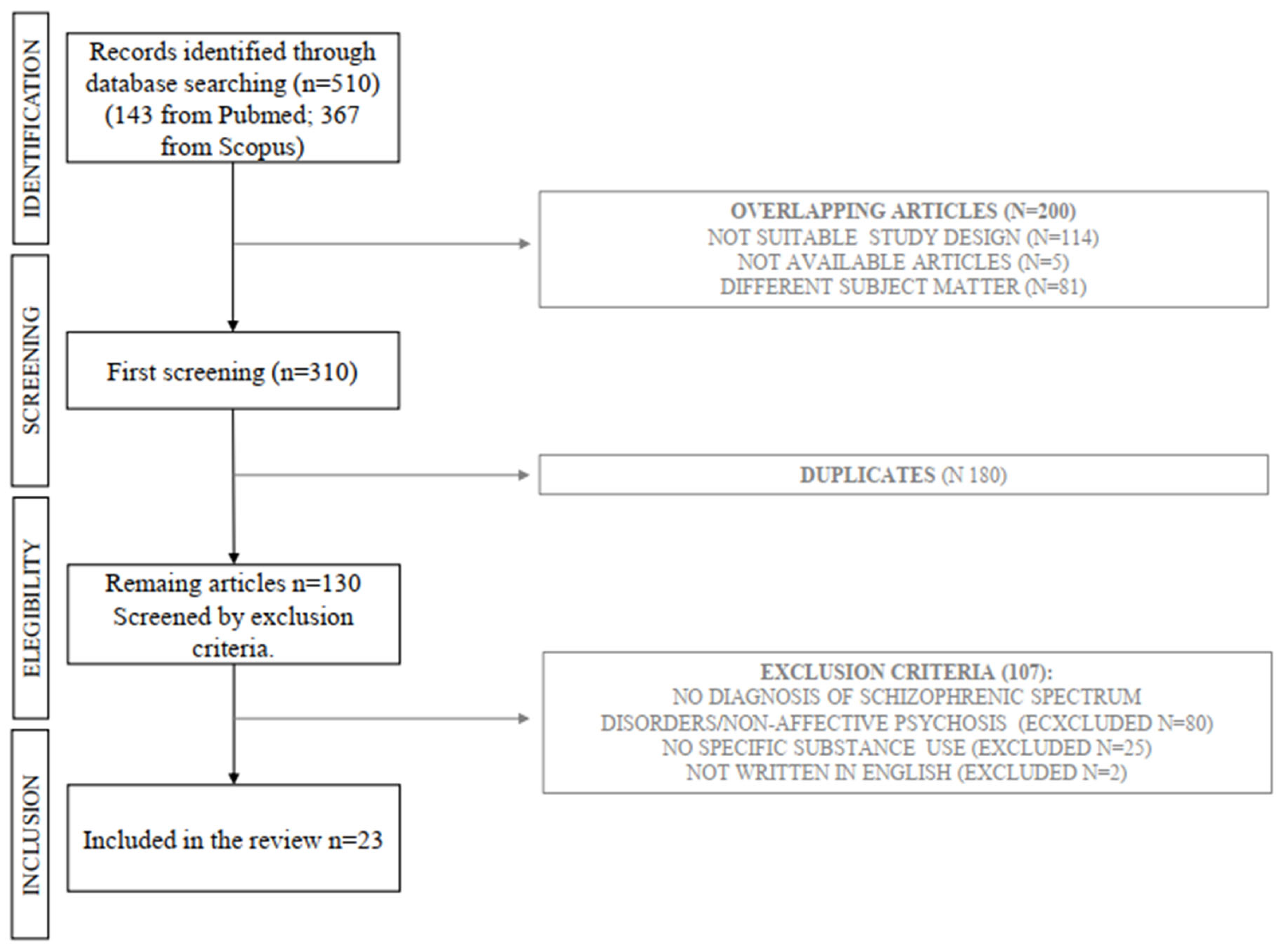
Our initial investigation began with a review of titles and abstracts, progressing to a comprehensive analysis of full texts for articles potentially relevant to our study. Our goal was to encompass a wide range of literature on the subject. We identified 510 articles (143 from PubMed, 367 from Scopus), and selected 23 that corresponded with our predefined topics (12 on aripiprazole, 7 on cariprazine, and 2 each on lurasidone and brexpiprazole). The exclusion of the other 487 articles was due to factors such as irrelevance to the topic (299 articles) or non-compliance with our selection criteria, which included reviews, letters to the editor, commentaries, book chapters, non-English papers, and duplicates (188 articles) as shown in the flow diagram (Figure 1). We have arranged and presented our findings according to study type and substances analyzed in Supplementary Materials (Tables 1 through Table 4). Characteristics of antipsychotic drugs were summarised in Table 5. These format offer a clear, detailed, and comprehensive view of the data, consistent with the descriptive approach of our review.
3. Results
3.1. Aripirazole
Aripiprazole, classified as a partial agonist within the antipsychotic drug category, exhibits lower intrinsic activity at receptors compared to full agonists (24). Its partial agonism at dopamine D2 receptors leads to 1) functional antagonism in the mesolimbic dopamine pathway, reducing positive symptoms caused by excessive dopamine activity, and 2) agonist activity in the mesocortical pathway, addressing negative symptoms and cognitive impairment due to reduced dopamine activity (25-27). This dual effect contributes to significant improvements in both positive and negative psychotic symptoms.
Moreover, aripiprazole avoids complete blockade of the nigrostriatal or tuberoinfundibular pathways, thereby preserving the avoidance of extrapyramidal symptoms and hyperprolactinemia (24). It also demonstrates a favorable cardiac safety profile, preventing QTc prolongation and causing minimal weight gain or sedation. Focusing on substance use, aripiprazole shows promise in animal models, where acute administration prevented increased locomotion induced by stimulants like amphetamine, cocaine, and methylphenidate, and attenuated their reinforcing properties without interfering with spontaneous motor activity (26). It reversed amphetamine-associated anhedonia and prevented the reinstatement of cocaine-seeking behavior (27), suggesting its potential in alleviating withdrawal symptoms linked to dopamine depletion and maintaining balanced dopamine neurotransmission in drug dependence behavior (28).
Clinical observations further support these findings. A 22-year-old male patient meeting ultra-high-risk criteria for psychosis benefited from 10 mg of aripiprazole, though without a decrease in smoking frequency (29). Another case highlighted aripiprazole's role in reducing cannabis intake in a schizophrenic patient (30). Thurston and colleagues observed that adolescents hospitalized for co-occurring psychosis and cannabis use disorder showed rapid reduction in acute psychotic symptoms with aripiprazole compared to risperidone (32). In trials comparing aripiprazole with other antipsychotics, it demonstrated superior efficacy in reducing negative symptoms of amphetamine-induced psychosis compared to risperidone, which was more effective against positive symptoms (34-35). A randomized study found aripiprazole comparable to quetiapine in alleviating psychotic symptoms but more effective in reducing cocaine dependence and usage (36). Beresford's study indicated its potential role in lowering both desire and use of cocaine in schizophrenic patients (37).
However, not all studies yielded positive outcomes. Aripiprazole was no more effective than placebo in maintaining abstinence from methamphetamine use but did facilitate treatment retention and reduce the severity of psychotic symptoms (38).
3.2. Cariprazine
Cariprazine, a third-generation antipsychotic drug approved for schizophrenia (39), is notable for its partial agonism towards D2 receptors. Distinguishing itself from other Second-Generation Antipsychotics (SGAs), it demonstrates a lower intrinsic activity at the D2 receptor compared to aripiprazole and brexpiprazole, approximately 0.15. This positioning suggests a minimized capacity to activate the D2 receptor, offering an intermediary profile between aripiprazole and traditional receptor antagonists with zero intrinsic activity (39-42). The reduced intrinsic activity of cariprazine is associated with a decreased likelihood of side effects such as restlessness and akathisia, commonly observed with aripiprazole (40).
Cariprazine's primary distinction lies in its high affinity for the dopaminergic D3 receptor, exceeding that of endogenous dopamine. This high D3 affinity is significant, considering that most antipsychotics have a lower affinity for this receptor, leading to inadequate D3 receptor occupancy in the brain. This unique affinity of cariprazine is crucial for its clinical efficacy, as indicated by PET studies in schizophrenic patients, demonstrating a stronger effect on the D3 receptor compared to the D2 receptor (41-47, 49) (see Table 6).
Cariprazine also exhibits significant serotonergic activity, with high affinity for the 5-HT2B receptor and moderate affinity for the 5-HT2A and 5-HT1A receptors. This receptor profile is somewhat distinct from many SGAs, which tend to have high affinity for the 5-HT2A receptor. The 5-HT2A/D2 affinity ratio of cariprazine is lower than that of other antipsychotic drugs. Additionally, it has low affinity for the 5-HT7 and 5-HT2C receptors, as well as the noradrenaline α1A and α1C receptors. Its interactions with the 5-HT6, α1a, α2b receptors, and other potential targets are minimal in therapeutic activity (42-43).
When comparing cariprazine with other partial agonists, such as blonanserin (48), an antagonist of dopaminergic D2 and D3 receptors, its D3/D2 affinity ratio is notably higher. This suggests a potential influence on negative symptoms, a theory supported by its unique receptor action. In contrast, brexpiprazole shows higher 5-HT2A/D2 and 5-HT1A/D2 ratios. The combined dopaminergic and serotonergic receptor activities of these drugs modulate specific brain circuits and neurotransmitter release, as observed in increased dopamine release in the prefrontal cortex with olanzapine and lurasidone, enhancing cognitive functions (50). Similarly, cariprazine affects neurotransmitter release in the nucleus accumbens and hippocampus, mainly via D3 receptor interaction, influencing levels of dopamine, norepinephrine, serotonin, and glutamate. This effect is comparable to that of dopaminergic D3 antagonists, contributing to cariprazine's therapeutic impact (50).
In conclusion, the receptor profile of cariprazine provides significant insights into its mechanism of action and its ability to modulate various neurotransmitter systems. Unlike other antipsychotics, cariprazine's efficacy is not only based on its receptor profile but also on its capacity to modulate intracellular mechanisms downstream of these receptors (51-52). Its dual action as a partial agonist at both D2 and D3 receptors, with a stronger effect on the latter, is particularly effective in improving negative symptoms, setting it apart from other SGAs (53).
Another intriguing facet of cariprazine pertains to its activity in the context of substance abuse. Experimental studies have illustrated cariprazine's capacity to mitigate the stimulating effects of cocaine and forestall relapses associated with the abused substance. This observed activity seems to correlate with its partial agonism for dopamine receptors D2 and D3 (54). Notably, a recent study has demonstrated comparable anti-abuse effects using (±)VK4-40, a novel selective partial agonist for the dopaminergic receptor D3. This finding suggests the potential contribution of this specific receptor component to the action of cariprazine (55). Rodriguez et al. (56) presented evidence of the positive impact of cariprazine on positive, negative, and cognitive symptoms in a schizophrenic patient with an extensive history of substance abuse. The patient underwent a transition from haloperidol to cariprazine, leading to a comprehensive amelioration of symptoms associated with schizophrenia. Ricci and colleagues (57) illustrated a favorable effect of cariprazine in mitigating psychotic symptoms induced by methamphetamine in a 25-year-old male who had shown only partial responsiveness to olanzapine and risperidone. Concerning methamphetamine-induced psychosis, Truong et al. (58) showcased both the antipsychotic and anticraving effects of cariprazine through two case reports featuring men aged 33 and 51. These individuals not only presented significant positive symptoms but also demonstrated pronounced substance-seeking behavior. In both cases, cariprazine was initiated at dosages of 1.5 mg and 3 mg, respectively, following prior use of olanzapine and paliperidone, which produced limited efficacy and resulted in significant side effects such as weight gain and metabolic imbalance. In a separate case report (59) the administration of 3 mg of cariprazine effectively alleviated positive symptoms in a 31-year-old male who was HIV positive and had a history of abusing methamphetamine, mephedrone, cocaine, and alcohol.
Another case report (60) has detailed symptomatic improvement in a patient with bipolar disorder and a history of poly-substance abuse, including cannabis, LSD, and methamphetamine. In this instance, cariprazine was introduced as an adjunct to the ongoing therapy (valproate, SSRI, and bupropion) at a maximum dosage of 3 mg. This intervention led to the alleviation of substance cravings and enhancement of affective symptoms.Gentile and colleagues (61) outlined a case involving a 23-year-old patient diagnosed with schizophrenia spectrum disorder and a psychotic onset induced by extensive cannabis use. Following the discontinuation of lurasidone due to ineffectiveness, the administration of cariprazine not only led to an improvement in both negative and positive symptoms but also resulted in a reduction in cannabinoid intake.
3.3. Brexpiprazole
Brexpiprazole, an atypical antipsychotic, received FDA approval in July 2015 for treating schizophrenia and as an adjunct therapy for managing Major Depressive Disorder (MDD). Acting as a partial agonist at 5-HT1A and D2 neuroreceptors, brexpiprazole also engages with noradrenergic receptors, although the clinical significance of this interaction is not fully understood. The safety and efficacy of brexpiprazole were evaluated in four finished placebo-controlled Phase III trials—two targeting Major Depressive Disorder (MDD) as an add-on to antidepressants, and two for schizophrenia. These studies showed that brexpiprazole was more effective than placebo at certain dosages for both disorders (62-64)
For schizophrenia, the recommended initiation is 1 mg once daily, titrating to a target dose of 2 mg to 4 mg daily. As an adjunct therapy for MDD, the initiation dose is advised at 0.5 mg or 1 mg once daily, with a weekly increase to a target dose of 2 mg. Contraindications include prior hypersensitivity reactions to similar medications. Common adverse reactions involve weight gain and akathisia, with additional associations with metabolic changes like dyslipidemia and hyperglycemia. Precautions and warnings for this medication include cerebrovascular adverse reactions in elderly patients with dementia-related psychosis, the risk of neuroleptic malignant syndrome, tardive dyskinesia, leukopenia, orthostatic hypotension, and seizures. A prominent black box warning highlights the increased risk of mortality in elderly patients with dementia-related psychosis, as well as the potential for suicidal thoughts and behaviors in children, adolescents, and young adults. Additionally, its use during pregnancy is cautioned against due to the risk of extrapyramidal and/or withdrawal symptoms in neonates exposed during the third trimester. Brexpiprazole is metabolized by hepatic enzymes, and dose adjustments are necessary if the CYP2D6 or CYP3A4 superfamilies of enzymes are impacted (65). Brexpiprazole functions as a partial agonist at dopamine D2 and serotonin 5-HT1A receptors and a potent antagonist at serotonin 5-HT2A, α1B, α 2C adrenergic receptors. In contrast to aripiprazole, brexpiprazole exhibits significantly greater potency at these three receptors—5HT2A, 5HT1A, and α1B. Despite commonly reported side effects such as EPS and akathisia, the strong affinity of brexpiprazole to these receptors may contribute to a reduction in the occurrence of these symptoms. Brexpiprazole exhibits a higher intrinsic activity at the serotonin 5HT2A receptor and a lower intrinsic activity at the dopamine D2 receptor, along with a stronger affinity for the norepinephrine transporter (66). Hyperprolactinemia, an often undesirable side effect of many antipsychotics, is largely due to the blockade of dopamine D2 receptors, which interrupts the dopaminergic inhibition of prolactin release. In a detailed evaluation, Brexpiprazole shows moderate antagonist activity at dopamine D3 and serotonin 5-HT2B, 5-HT7 receptors, as well as α1A, α1D receptors. It also has a moderate affinity for histamine H1 receptors and a low affinity for muscarinic cholinergic M1 receptors. This pharmacodynamic profile not only enhances brexpiprazole's efficacy but also positions it as a potentially preferred alternative based on patient tolerability and therapy goals (67).
Brexpiprazole undergoes primary metabolism by the enzymes CYP3A4 and CYP2D6. The major metabolite, DM-3411, constitutes between 23% and 48% of brexpiprazole's exposure at steady state, although it has not been demonstrated to contribute to any antipsychotic effects. Various factors influence the rate of brexpiprazole metabolism, subsequently impacting its overall exposure (AUC). Patients who use strong CYP3A4 inhibitors (like erythromycin or itraconazole) or potent CYP2D6 inhibitors (such as bupropion, fluoxetine, or paroxetine) may experience increased exposure to the drug. This heightened exposure is also seen in individuals who are poor metabolizers of CYP2D6. On the other hand, using potent CYP2D6 inducers (for instance, rifampicin or glucocorticoids) is likely to decrease the exposure to brexpiprazole. Additionally, patients with moderate to severe liver impairment (classified as Child-Pugh Class B or C) or those with moderate to severe kidney impairment (with a creatinine clearance rate below 60 mL/min) are subject to increased drug exposure, which may require adjustments in dosage (68-69).
Brexpiprazole demonstrates efficacy in acute schizophrenia based on two studies (70-71). While the 2 mg dose showed inconsistent results, the recommended 4 mg dosage exhibited more consistent benefits. Higher brexpiprazole dosages, especially at 4 mg, significantly improved PANSS-EC score and PANSS scores for negative symptoms, disorganized thought, and uncontrolled hostility/excitement. In a 52-week maintenance study, brexpiprazole outperformed placebo, prolonging time to exacerbation and showing significant benefits in psychosocial, occupational, and cognitive functioning, including attention/vigilance and visual learning (63). Brexpiprazole also demonstrated cognitive improvement in animal models, distinguishing itself from aripiprazole in this regard. Short-term trials showed a good safety profile, with weight gain being the only common adverse event, and long-term studies indicated a decrease in mean body weight change. Akathisia was dose-dependent but generally mild, with no treatment discontinuations (72). Other adverse effects were comparable to placebo, and minimal impacts on glucose, lipids, prolactin, and QTc interval were observed.
As of the current state, only two studies shed light on the role of brexpiprazole in substance-induced psychoses (73-74). Nickols and colleagues conducted research to explore its effects in a mouse model of opioid dependence. Providing preclinical evidences for the efficacy of brexpiprazole as a modulator of dopamine-dependent behaviors during opioid use and withdrawal: this research contributes valuable insights into the potential application of brexpiprazole in forthcoming human studies. The findings suggest a plausible role as a pharmacological adjunct, not only in addressing the emergence of substance-induced psychoses but also in mitigating craving phenomena (73).
One additional study highlight the role of brexpiprazole in substance-induced psychoses. Specifically, Kung and colleagues demonstrate the effectiveness of brexpiprazole in treating psychosis during cannabis withdrawal in a 25-year-old individual at a daily dosage of 3 mg (74).
3.4. Lurasidone
Lurasidone, like other second-generation antipsychotics, functions as a complete antagonist at dopamine D2 and serotonin 5-HT2A receptors, with binding affinities (Ki) of 1 nM and 0.5 nM respectively. A distinctive feature of lurasidone is its high affinity for serotonin 5-HT7 receptors (0.5 nM, on par with its affinity for dopamine D2 and 5-HT2A receptors), and its partial agonist activity at 5-HT1A receptors (Ki, 6.4 nM). The serotonin 5-HT7 receptor is of significant interest, as it is linked to potential procognitive and antidepressant effects. The 5-HT1A receptor is considered important in the treatment of major depressive disorder and schizophrenia. Notably, lurasidone lacks affinity for histamine H1 and muscarinic M1 receptors, contributing to its characteristics of low sedation, minimal weight gain, and limited interference with cognitive and functional assessments (75-76). The pharmacokinetic characteristics of lurasidone support its suitability for once-daily administration, as it has an elimination half-life of 18 hours (77-78). When administered with food, both the mean Cmax and the area under the curve for lurasidone were approximately threefold and twofold greater, respectively, compared to fasting (79). Based on these findings and clinical trial results, it is recommended to take lurasidone once daily in the evening, either with a meal or within 30 minutes after eating. Notably, lurasidone absorption remains unaffected by the fat content of the ingested food (79). Lurasidone is primarily metabolized by the CYP3A4 enzyme system. Consequently, its use is contraindicated when there are strong inducers or inhibitors of CYP3A4 present. Within the category of psychotropic medications, notable examples of strong inhibitors of CYP3A4 include fluvoxamine and fluoxetine. On the other hand, a well-known strong inducer of CYP3A4 is carbamazepine. When moderate inhibitors of CYP3A4 are present, the suggested initial dose of lurasidone is 20 mg/day instead of 40 mg/day, and the highest recommended dose is 80 mg/day rather than 160 mg/day. Lurasidone's pharmacokinetics do not interfere with other drugs, including lithium, valproate, or those metabolized by the CYP3A4 pathway (80)
In patients who have moderate or severe renal or hepatic impairment, the advised initial dosage of this medication is set at 20 mg per day. For those with moderate-to-severe renal impairment or moderate hepatic impairment, the maximum dosage should not surpass 80 mg per day. In cases of severe hepatic impairment, the dosage should be restricted to a maximum of 40 mg per day. Lurasidone demonstrated good tolerability, with consistent side effects observed in both short-term and long-term use. In trials spanning six weeks, the most frequently reported adverse reactions to lurasidone included drowsiness, restlessness, nausea, Parkinson-like symptoms, and sleeplessness (81). Lurasidone demonstrated good tolerability, with consistent side effects observed in both short-term and long-term use. In trials spanning six weeks, the most frequently reported adverse reactions to lurasidone included drowsiness, restlessness, nausea, Parkinson-like symptoms, and sleeplessness (83). Finally, Lurasidone was as- sociated with lower weight gain and metabolic disturbances than brexpiprazole (82-83).
An analysis that combined data from eight short-term (6-week) placebo-controlled studies conducted across the United States, Europe, Asia, and South America revealed the effectiveness of lurasidone (40–160 mg/day) in treating schizophrenia (84). The findings indicated that lurasidone demonstrated efficacy compared to a placebo, leading to improvements in positive symptoms, negative symptoms, and general psychopathology. Additionally, the meta-analysis highlighted that lurasidone was well-tolerated, showing minimal impact on body weight, glucose, and lipid parameters. Continuation studies spanning 6 to 22 months affirmed the sustained efficacy of lurasidone in the treatment of schizophrenia, maintaining minimal effects on body weight and metabolic parameters (85-88). A recent 26-week open-label study, focusing on lurasidone doses of 40–80 mg/day, extended these positive results to patients with schizophrenia in Asia, including Japan, Taiwan, Korea, and Malaysia (89).
Concerning the use of lurasidone in psychopathological conditions induced by substances, there is limited literature available. Despite being an approved medication for psychotic disorders in individuals aged 15 and older, there are currently no trials or extensive clinical observations of lurasidone in the context of substance-induced psychoses. Only two studies have addressed the role of lurasidone in these circumstances.
The initial study (90) comprises four clinical observations of young patients experiencing cannabis-induced psychosis. These individuals exhibited improvements in both positive and negative symptomatology, as well as mood, following the administration of lurasidone. The dosage of lurasidone ranged from 74 mg to 111 mg and was prescribed as both an initial treatment in drug-naive patients and after the failure of therapy with aripiprazole and paliperidone. In contrast, the second study (91) appears to be more comprehensive, focusing on the utilization of lurasidone in young individuals with complex psychopathological conditions. Notably, the study reports the beneficial use of lurasidone in a 14-year-old with a history of alcohol, cannabis, and LSD abuse, coupled with behavioral issues (self-injurious behaviors) and psychotic symptoms such as auditory hallucinations.
4. Discussion
From the above-mentioned data, third-generation antipsychotics and lurasidone emerge as a promising therapeutic strategy in the treatment of substance-induced psychoses. Aripiprazole has been effective in improving a wide range of psychotic symptoms, including both positive and negative aspects, as well as impacting substance use disorders positively. Its mode of action is unique; it's a partial agonist, meaning it doesn't stimulate receptors as strongly as full agonists. Its effectiveness lies in its dual role: it diminishes positive symptoms by antagonizing the mesolimbic dopamine pathway and improves negative symptoms and cognitive deficits by activating the mesocortical pathway. This selective mechanism helps aripiprazole to avoid severe side effects like motor disorders and elevated prolactin levels, common in other antipsychotics. Additionally, it's known for its cardiac safety, causing negligible QTc prolongation and having a low risk of weight gain or sedation. In research with animals, aripiprazole has been observed to curb the heightened activity caused by stimulants such as amphetamine, cocaine, and methylphenidate, and reduce their addictive qualities without hampering normal motor functions. It also reverses the lack of pleasure associated with amphetamine use and hinders the recurrence of cocaine-seeking behaviors. These findings indicate that aripiprazole might be effective in easing withdrawal symptoms associated with dopamine deficiency and, due to its broad receptor activity, could represent a new strategy for achieving balanced dopamine levels in the treatment of drug addiction.
Cariprazine’s receptor profile, particularly its high affinity for the D3 receptor and reduced intrinsic activity at D2 receptors, makes it an effective treatment for schizophrenia, improving both positive and negative symptoms. Its ability to modulate different neurotransmitter systems further highlights its potential as a distinct and effective antipsychotic medication. Cariprazine's role in substance abuse treatment is noteworthy. From the studies reviewed, emerge its effectiveness in reducing the stimulating effects of substances like cocaine and mitigating cravings and relapses. This effect is possibly due to its partial agonism at D2 and D3 receptors. Case studies show cariprazine’s beneficial impact on schizophrenic patients with a history of substance abuse and its effectiveness in treating psychosis induced by substances like methamphetamine.
Brexpiprazole exhibits potential efficacy in the domain of substance abuse therapy. Primarily indicated for the management of schizophrenia and as an adjunctive treatment in Major Depressive Disorder (MDD), its unique pharmacodynamic properties extend to the mitigation of substance-induced psychotic disorders. Operating as a partial agonist at the 5-HT1A and D2 neuroreceptors, brexpiprazole also engages with noradrenergic receptors. Consequently, albeit preliminary and limited in scope, research indicates its utility in addressing psychotic sequelae associated with cannabis consumption and in modulating dopaminergic activity in heroin-exposed rodents.
Lurasidone has shown potential in treating psychopathological conditions related to substance abuse, although research in this area is limited. Known for its antagonistic action at dopamine D2 and serotonin 5-HT2A receptors, and strong affinity for serotonin 5-HT7 receptors, lurasidone is unique in its partial agonism at 5-HT1A receptors. This receptor profile contributes to its low sedative effects and minimal impact on weight and cognitive functions, making it an appealing option in treating substance-induced psychoses. In the context of substance abuse, recent studies has shown lurasidone to be effective in treating young individuals with substance-induced psychosis, particularly from cannabis, improving various symptoms including mood. It has also been beneficial for a complex case involving a young person with alcohol, cannabis, and LSD abuse, along with behavioral and psychotic symptoms. It's important to consider that lurasidone is an approved medication for treating schizophrenia in individuals as young as 13, an age group particularly susceptible to substance use. Consequently, this could make it a viable option for treatment in this younger demographic in the future.
Finally, despite aripiprazole showing more scientific evidence, there are currently limited specific clinical studies demonstrating its long-term efficacy. Several critical issues emerged from our observation, including:
Firstly, these drugs may exhibit variable efficacy in managing psychotic symptoms associated with substance use, as the nature and complexity of substance-induced psychoses can differ significantly from those purely psychiatric in origin. Additionally, third-generation antipsychotics may not optimally address specific aspects of substance-induced psychoses, such as the management of cognitive disorders and compulsive impulses, which often characterize these conditions.
Another significant limitation concerns side effects. Third-generation antipsychotics, although to a lesser extent, can induce metabolic disorders and increase the risk of tardive dyskinesia, posing additional challenges in the treatment of substance-induced psychoses. Furthermore, patient compliance may become an issue due to these side effects, compromising treatment adherence.
5. Conclusions
In summary, the core feature of third-generation antipsychotics like aripiprazole, brexpiprazole, and cariprazine is their partial agonism at D2 dopaminergic receptors. This characteristic offers at least three potential benefits compared to the traditional antagonism approach:
- In cases of mesolimbic dopaminergic overactivity linked to positive symptoms, the partial agonist competes with dopamine for receptors. This competition displaces dopamine, decreasing the system's excessive activity and returning it to a 'physiological range'.
-The effects of the partial agonist don't typically include significant adverse reactions, suchcs extrapyramidal symptoms or hyperprolactinemia. This is because the molecule's intrinsic activity prevents a substantial reduction in dopaminergic functionality at the striatal and pituitary levels.
-Owing to its intrinsic activity, the partial agonist may bolster weakened dopaminergic transmission in the prefrontal cortex. This enhancement could improve cognitive dysfunctions and symptoms linked to diminished dopaminergic functionality. These pharmacodynamic properties make them especially useful in cases of substance-induced psychosis.
Concerning lurasidone, its efficacy lies in its binding to D2 receptors, which helps in reducing positive symptoms. Additionally, its agonist activity at the 5HT2A and 5HT7 receptors results in the release of dopamine, contributing to the improvement of affective and cognitive symptoms. This mechanism of action could provide a foundation for additional research and the initiation of studies in patients with substance-induced psychosis.
Finally, it is essential to consider that third-generation antipsychotics may not fully address the underlying cause of substance-induced psychoses, linked to the intake of specific psychoactive substances. Therefore, a comprehensive therapeutic approach should include not only symptomatic treatment with antipsychotics but also targeted intervention for substance dependence and relapse prevention through psychological interventions and rehabilitation programs. In summary, while third-generation antipsychotics are valuable in treating psychoses, their effectiveness and appropriateness in substance-induced psychoses require particular attention and an integrated approach.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Main findings of retrieved studies in aripiprazole; Table S2: Main findings of retrieved studies in cariprazine: Table S3: Main findings of retrieved studies in brexpiprazole; Table 4: Main findings of retrieved studies in lurasidone.
Author Contributions
Conceptualization, VALERIO RICCI (V.R) and GIUSEPPE MAINA (G.M); methodology, V.R.; validation, V.R, G.M and DOMENICO DE BERARDIS (D.D.M.); formal analysis, V.R.; investigation, V.R.; resources, D.D.B and V.R .; data curation, D.D.B and V.R writing—original draft preparation, V.R.; writing—review and editing, V.R and D.D.B.; visualization, D.D.B; supervision, G.M.;All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data avalaibility statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy reason.
Conflict Interest
G.M (Giuseppe Maina) ): has been a consultant and/or a speaker and/or has received research grants from Angelini, Doc Generici, Janssen-Cilag, Lundbeck, Otsuka, Pfizer, Servier, Recordati. V.R., D.D.B nothing to declare.
References
- Martinotti, G.; De Risio, L.; Vannini, C.; Schifano, F.; Pettorruso, M.; Di Giannantonio, M. Substance-related exogenous psychosis: a postmodern syndrome. CNS Spectrums 2021, 26 (1), 84–91. [CrossRef]
- Orsolini, L.; Chiappini, S.; Papanti, D.; De Berardis, D.; Corkery, J. M.; Schifano, F. The Bridge Between Classical and "Synthetic"/Chemical Psychoses: Towards a Clinical, Psychopathological, and Therapeutic Perspective. Frontiers in Psychiatry 2019, 10, 851. [CrossRef]
- Schifano, F.; Napoletano, F.; Chiappini, S.; Guirguis, A.; Corkery, J. M.; Bonaccorso, S.; Ricciardi, A.; Scherbaum, N.; Vento, A. New/emerging psychoactive substances and associated psychopathological consequences. Psychological Medicine 2021, 51 (1), 30–42. [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed., Text Rev.; American Psychiatric Publishing: Washington, DC, 2022.
- Ricci, V.; Ceci, F.; Di Carlo, F.; Lalli, A.; Ciavoni, L.; Mosca, A.; Sepede, G.; Salone, A.; Quattrone, D.; Fraticelli, S.; Maina, G.; Martinotti, G. Cannabis use disorder and dissociation: A report from a prospective first-episode psychosis study. Drug and Alcohol Dependence 2021, 229 (Pt A), 109118. [CrossRef]
- Schifano, F. Recent Changes in Drug Abuse Scenarios: The New/Novel Psychoactive Substances (NPS) Phenomenon. Brain Sciences 2018, 8 (12), 221. [CrossRef]
- European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). Co-morbid substance use and mental disorders in Europe: A review of the data. 2013; pp. 1-12.
- Chetty, A.; Guse, T.; Malema, M. Integrated vs non-integrated treatment outcomes in dual diagnosis disorders: A systematic review. Health SA = SA Gesondheid 2023, 28, 2094. [CrossRef]
- Han, B.; Compton, W. M.; Blanco, C.; Colpe, L. J. Prevalence, Treatment, And Unmet Treatment Needs Of US Adults With Mental Health And Substance Use Disorders. Health Affairs (Project Hope) 2017, 36 (10), 1739–1747. [CrossRef]
- Hakobyan, S.; Vazirian, S.; Lee-Cheong, S.; Krausz, M.; Honer, W. G.; Schutz, C. G. Concurrent Disorder Management Guidelines. Systematic Review. Journal of Clinical Medicine 2020, 9 (8), 2406. [CrossRef]
- Arnau, F.; Benito, A.; Villar, M.; Ortega, M. E.; López-Peláez, L.; Haro, G. Addressing Dual Disorders in a Medium-Term Admission Unit. Brain Sciences 2021, 12 (1), 24. [CrossRef]
- Murthy, P.; Chand, P. Treatment of dual diagnosis disorders. Current Opinion in Psychiatry 2012, 25 (3), 194–200. [CrossRef]
- Murthy, P.; Mahadevan, J.; Chand, P. K. Treatment of substance use disorders with co-occurring severe mental health disorders. Current Opinion in Psychiatry 2019, 32 (4), 293–299. [CrossRef]
- Janiri, L.; Martinotti, G.; Di Nicola, M. Aripiprazole for relapse prevention and craving in alcohol-dependent subjects: results from a pilot study. Journal of Clinical Psychopharmacology 2007, 27 (5), 519–520. [CrossRef]
- Price, Jobe, L. B.; Mårtensson, S.; Düring, S. W. Polypharmacy in antipsychotic pharmacological treatment among patients with dual diagnosis in Denmark. Nordic Journal of Psychiatry 2023, 1-8. Advance online publication. [CrossRef]
- Temmingh, H. S.; Williams, T.; Siegfried, N.; Stein, D. J. Risperidone versus other antipsychotics for people with severe mental illness and co-occurring substance misuse. The Cochrane Database of Systematic Reviews 2018, 1 (1), CD011057. [CrossRef]
- Grau-López, L.; Roncero, C.; Daigre, C.; Miquel, L.; Barral, C.; Gonzalvo, B.; Collazos, F.; Casas, M. Observational study on medications prescribed to dual-diagnosis outpatients. Journal of Addiction Medicine 2014, 8 (2), 84–89. [CrossRef]
- Grau-López, L.; Szerman, N.; Torrens, M.; Basurte, I.; Vega, P.; Martínez-Raga, J.; Casas, M.; Roncero, C. Professional perception of clozapine use in patients with dual psychosis. Actas Espanolas de Psiquiatria 2020, 48 (3), 99–105.
- Martinotti, G.; Chiappini, S.; Mosca, A.; Miuli, A.; Santovito, M. C.; Pettorruso, M.; Skryabin, V.; Sensi, S. L.; Giannantonio, M. D. Atypical Antipsychotic Drugs in Dual Disorders: Current Evidence for Clinical Practice. Current Pharmaceutical Design 2022, 28 (27), 2241–2259. [CrossRef]
- Clerici, M.; de Bartolomeis, A.; De Filippis, S.; Ducci, G.; Maremmani, I.; Martinotti, G.; Schifano, F. Patterns of Management of Patients With Dual Disorder (Psychosis) in Italy: A Survey of Psychiatrists and Other Physicians Focusing on Clinical Practice. Frontiers in Psychiatry 2018, 9, 575. [CrossRef]
- Abdel-Baki, A.; Thibault, D.; Medrano, S.; Stip, E.; Ladouceur, M.; Tahir, R.; Potvin, S. Long-acting antipsychotic medication as first-line treatment of first-episode psychosis with comorbid substance use disorder. Early Intervention in Psychiatry 2020, 14 (1), 69–79. [CrossRef]
- Cipriani, A.; Geddes, J. Comparison of systematic and narrative reviews: the example of the atypical antipsychotics. Epidemiologia e Psichiatria Sociale 2003, 12 (3), 146-153. [CrossRef]
- Collins, J. A.; Fauser, B. C. Balancing the strengths of systematic and narrative reviews. Human Reproduction Update 2005, 11 (2), 103–104. [CrossRef]
- Lieberman J. A. Dopamine partial agonists: a new class of antipsychotic. CNS Drugs 2004, 18 (4), 251–267. [CrossRef]
- Orsolini, L.; Tomasetti, C.; Valchera, A.; Vecchiotti, R.; Matarazzo, I.; Vellante, F.; Iasevoli, F.; Buonaguro, E. F.; Fornaro, M.; Fiengo, A. L.; Martinotti, G.; Mazza, M.; Perna, G.; Carano, A.; De Bartolomeis, A.; Di Giannantonio, M.; De Berardis, D. An update of safety of clinically used atypical antipsychotics. Expert Opinion on Drug Safety 2016, 15 (10), 1329–1347. [CrossRef]
- Leite, J. V.; Guimarães, F. S.; Moreira, F. A. Aripiprazole, an atypical antipsychotic, prevents the motor hyperactivity induced by psychotomimetics and psychostimulants in mice. European Journal of Pharmacology 2008, 578 (2-3), 222–227. [CrossRef]
- Sørensen, G.; Sager, T. N.; Petersen, J. H.; Brennum, L. T.; Thøgersen, P.; Hee Bengtsen, C.; Thomsen, M.; Wörtwein, G.; Fink-Jensen, A.; Woldbye, D. P. Aripiprazole blocks acute self-administration of cocaine and is not self-administered in mice. Psychopharmacology 2008, 199 (1), 37–46. [CrossRef]
- Natesan, S.; Reckless, G. E.; Nobrega, J. N.; Fletcher, P. J.; Kapur, S. Dissociation between in vivo occupancy and functional antagonism of dopamine D2 receptors: comparing aripiprazole to other antipsychotics in animal models. Neuropsychopharmacology 2006, 31 (9), 1854–1863. [CrossRef]
- Rolland, B.; Geoffroy, P. A.; Jardri, R.; Cottencin, O. Aripiprazole for treating cannabis-induced psychotic symptoms in ultrahigh-risk individuals. Clinical Neuropharmacology 2013, 36 (3), 98–99. [CrossRef]
- Desseilles, M.; Mathot, F.; Desseilles, M. Aripiprazole diminishes cannabis use in schizophrenia. The Journal of Neuropsychiatry and Clinical Neurosciences 2008, 20 (1), 117–118. [CrossRef]
- Feltenstein, M. W.; Altar, C. A.; See, R. E. Aripiprazole blocks reinstatement of cocaine seeking in an animal model of relapse. Biological Psychiatry 2007, 61 (5), 582–590. [CrossRef]
- Thurstone, C.; Loh, R.; Foreman, K.; Thurstone, C. A.; Wolf, C. Program Evaluation to Aid Choice of Aripiprazole or Risperidone for Hospitalized Adolescents with Cannabis Use Disorder and Psychosis. Journal of Child and Adolescent Psychopharmacology 2023, 33 (8), 332–336. [CrossRef]
- Futamura, T.; Akiyama, S.; Sugino, H.; Forbes, A.; McQuade, R. D.; Kikuchi, T. Aripiprazole attenuates established behavioral sensitization induced by methamphetamine. Progress in Neuro-Psychopharmacology & Biological Psychiatry 2010, 34 (6), 1115–1119. [CrossRef]
- Farnia, V.; Shakeri, J.; Tatari, F.; Juibari, T. A.; Yazdchi, K.; Bajoghli, H.; Brand, S.; Abdoli, N.; Aghaei, A. Randomized controlled trial of aripiprazole versus risperidone for the treatment of amphetamine-induced psychosis. The American Journal of Drug and Alcohol Abuse 2014, 40 (1), 10–15. [CrossRef]
- Wang, G.; Zhang, Y.; Zhang, S.; Chen, H.; Xu, Z.; Schottenfeld, R. S.; Hao, W.; Chawarski, M. C. Aripiprazole and Risperidone for Treatment of Methamphetamine-Associated Psychosis in Chinese Patients. Journal of Substance Abuse Treatment 2016, 62, 84–88. [CrossRef]
- Skryabin, V. Y.; Vinnikova, M. A.; Ezhkova, E. V.; Titkov, M. S.; Bulatova, R. A. Atypical Antipsychotics in the Treatment of Patients with a Dual Diagnosis of Schizophrenia Spectrum Disorders and Substance Use Disorders: The Results of a Randomized Comparative Study. Journal of Addictive Diseases 2021, 39 (4), 513–525. [CrossRef]
- Beresford, T. P.; Clapp, L.; Martin, B.; Wiberg, J. L.; Alfers, J.; Beresford, H. F. Aripiprazole in schizophrenia with cocaine dependence: a pilot study. Journal of Clinical Psychopharmacology 2005, 25 (4), 363–366. [CrossRef]
- Sulaiman, A. H.; Gill, J. S.; Said, M. A.; Zainal, N. Z.; Hussein, H. M.; Guan, N. C. A randomized, placebo-controlled trial of aripiprazole for the treatment of methamphetamine dependence and associated psychosis. International Journal of Psychiatry in Clinical Practice 2013, 17 (2), 131–138. [CrossRef]
- Edinoff, A.; Ruoff, M. T.; Ghaffar, Y. T.; Rezayev, A.; Jani, D.; Kaye, A. M.; Cornett, E. M.; Kaye, A. D.; Viswanath, O.; Urits, I. Cariprazine to Treat Schizophrenia and Bipolar Disorder in Adults. Psychopharmacology Bulletin 2020, 50 (4), 83–117. [CrossRef]
- Stahl, S. M. Drugs for psychosis and mood: unique actions at D3, D2, and D1 dopamine receptor subtypes. CNS Spectrums 2017, 22 (5), 375–384. [CrossRef]
- Calabrese, F.; Tarazi, F. I.; Racagni, G.; Riva, M. A. The role of dopamine D3 receptors in the mechanism of action of cariprazine. CNS Spectrums 2020, 25 (3), 343–351. [CrossRef]
- Kiss, B.; Horváth, A.; Némethy, Z.; Schmidt, E.; Laszlovszky, I.; Bugovics, G.; Fazekas, K.; Hornok, K.; Orosz, S.; Gyertyán, I.; Agai-Csongor, E.; Domány, G.; Tihanyi, K.; Adham, N.; Szombathelyi, Z. Cariprazine (RGH-188), a dopamine D(3) receptor-preferring, D(3)/D(2) dopamine receptor antagonist-partial agonist antipsychotic candidate: in vitro and neurochemical profile. The Journal of Pharmacology and Experimental Therapeutics 2010, 333 (1), 328–340. [CrossRef]
- Kiss, B.; Krámos, B.; Laszlovszky, I. Potential Mechanisms for Why Not All Antipsychotics Are Able to Occupy Dopamine D3 Receptors in the Brain in vivo. Frontiers in Psychiatry 2022, 13, 785592. [CrossRef]
- Wesołowska, A.; Partyka, A.; Jastrzębska-Więsek, M.; Kołaczkowski, M. The preclinical discovery and development of cariprazine for the treatment of schizophrenia. Expert Opinion on Drug Discovery 2018, 13 (8), 779–790. [CrossRef]
- Legros, C.; Rojas, A.; Dupré, C.; Brasseur, C.; Riest-Fery, I.; Muller, O.; Ortuno, J. C.; Nosjean, O.; Guenin, S. P.; Ferry, G.; Boutin, J. A. Approach to the specificity and selectivity between D2 and D3 receptors by mutagenesis and binding experiments part I: Expression and characterization of D2 and D3 receptor mutants. Protein Science: A Publication of the Protein Society 2022, 31 (12), e4459. [CrossRef]
- Legg, D. R. K.; Dubroff, J. G.; Labban, K. J.; Mach, R. H. Selectivity of probes for PET imaging of dopamine D3 receptors. Neuroscience Letters 2019, 691, 18–25. [CrossRef]
- Lacroix, Weerasinghe, D. K.; Hodge, J. M.; Pasco, J. A.; Samarasinghe, R. M.; Azimi Manavi, B.; Williams, L. J. Antipsychotic-induced bone loss: the role of dopamine, serotonin and adrenergic receptor signalling. Frontiers in Cell and Developmental Biology 2023, 11, 1184550. [CrossRef]
- Huang, M.; Panos, J. J.; Kwon, S.; Oyamada, Y.; Rajagopal, L.; Meltzer, H. Y. Comparative effect of lurasidone and blonanserin on cortical glutamate, dopamine, and acetylcholine efflux: role of relative serotonin (5-HT)2A and DA D2 antagonism and 5-HT1A partial agonism. Journal of Neurochemistry 2014, 128 (6), 938–949. [CrossRef]
- Girgis, R. R.; Slifstein, M.; D'Souza, D.; Lee, Y.; Periclou, A.; Ghahramani, P.; Laszlovszky, I.; Durgam, S.; Adham, N.; Nabulsi, N.; Huang, Y.; Carson, R. E.; Kiss, B.; Kapás, M.; Abi-Dargham, A.; Rakhit, A. Preferential binding to dopamine D3 over D2 receptors by cariprazine in patients with schizophrenia using PET with the D3/D2 receptor ligand [(11)C]-(+)-PHNO. Psychopharmacology 2016, 233 (19-20), 3503–3512. [CrossRef]
- Huang, M.; He, W.; Kiss, B.; Farkas, B.; Adham, N.; Meltzer, H. Y. The Role of Dopamine D3 Receptor Partial Agonism in Cariprazine-Induced Neurotransmitter Efflux in Rat Hippocampus and Nucleus Accumbens. The Journal of Pharmacology and Experimental Therapeutics 2019, 371 (2), 517–525. [CrossRef]
- Yun, S.; Yang, B.; Anair, J. D.; Martin, M. M.; Fleps, S. W.; Pamukcu, A.; Yeh, N. H.; Contractor, A.; Kennedy, A.; Parker, J. G. Antipsychotic drug efficacy correlates with the modulation of D1 rather than D2 receptor-expressing striatal projection neurons. Nature Neuroscience 2023, 26 (8), 1417–1428. [CrossRef]
- Sanson, A.; Riva, M. A. Anti-Stress Properties of Atypical Antipsychotics. Pharmaceuticals (Basel, Switzerland) 2020, 13 (10), 322. [CrossRef]
- Németh, G.; Laszlovszky, I.; Czobor, P.; Szalai, E.; Szatmári, B.; Harsányi, J.; Barabássy, Á.; Debelle, M.; Durgam, S.; Bitter, I.; Marder, S.; Fleischhacker, W. W. Cariprazine versus risperidone monotherapy for treatment of predominant negative symptoms in patients with schizophrenia: a randomised, double-blind, controlled trial. Lancet (London, England) 2017, 389 (10074), 1103–1113. [CrossRef]
- Román, V.; Gyertyán, I.; Sághy, K.; Kiss, B.; Szombathelyi, Z. Cariprazine (RGH-188), a D₃-preferring dopamine D₃/D₂ receptor partial agonist antipsychotic candidate demonstrates anti-abuse potential in rats. Psychopharmacology 2013, 226 (2), 285–293. [CrossRef]
- Jordan, C. J.; He, Y.; Bi, G. H.; You, Z. B.; Cao, J.; Xi, Z. X.; Newman, A. H. (±)VK4-40, a novel dopamine D3 receptor partial agonist, attenuates cocaine reward and relapse in rodents. British Journal of Pharmacology 2020, 177 (20), 4796–4807. [CrossRef]
- Rodriguez Cruz, J.; Sahlsten Schölin, J.; Hjorth, S. Case Report: Cariprazine in a Patient With Schizophrenia, Substance Abuse, and Cognitive Dysfunction. Frontiers in Psychiatry 2021, 12, 727666. [CrossRef]
- Ricci V, Di Salvo G, Maina G. Remission of persistent methamphetamine-induced psychosis after cariprazine therapy: presentation of a case report. J Addict Dis 2022, 40(1), 145-148. [CrossRef]
- Truong, T. T.; Li, B. Case Series: Cariprazine for treatment of methamphetamine use disorder. The American Journal on Addictions 2022, 31(1), 85–88. [CrossRef]
- Montes, J. M.; Montes, P.; Hernández-Huerta, D. Cariprazine in Three Acute Patients with Schizophrenia: A Real-World Experience. Neuropsychiatric Disease and Treatment 2021, 17, 291–296. [CrossRef]
- Vannucchi, T.; Taddeucci, C.; Tatini, L. Case Report: Functional and Symptomatic Improvement With Cariprazine in Various Psychiatric Patients: A Case Series. Frontiers in Psychiatry 2022, 13, 878889. [CrossRef]
- Gentile, A.; Marini, S.; Matarazzo, I.; De Berardis, D.; Ventriglio, A. Cariprazine in the treatment of psychosis with comorbid cannabis use: A case report (2022). Psychiatry Research Communications 2022, 2 (2), art. no. 100048. [CrossRef]
- Maeda, K.; Sugino, H.; Akazawa, H.; Amada, N.; Shimada, J.; Futamura, T.; Yamashita, H.; Ito, N.; McQuade, R. D.; Mørk, A.; Pehrson, A. L.; Hentzer, M.; Nielsen, V.; Bundgaard, C.; Arnt, J.; Stensbøl, T. B.; Kikuchi, T. Brexpiprazole I: in vitro and in vivo characterization of a novel serotonin-dopamine activity modulator. The Journal of Pharmacology and Experimental Therapeutics 2014, 350 (3), 589–604. [CrossRef]
- Maeda, K.; Lerdrup, L.; Sugino, H.; Akazawa, H.; Amada, N.; McQuade, R. D.; Stensbøl, T. B.; Bundgaard, C.; Arnt, J.; Kikuchi, T. Brexpiprazole II: antipsychotic-like and procognitive effects of a novel serotonin-dopamine activity modulator. The Journal of Pharmacology and Experimental Therapeutics 2014, 350 (3), 605–614. [CrossRef]
- Stahl, S. M. Mechanism of action of brexpiprazole: comparison with aripiprazole. CNS Spectrums 2016, 21 (1), 1–6. [CrossRef]
- Edinoff, A. N.; Wu, N. W.; Maxey, B. S.; Ren, A. L.; Leethy, K. N.; Girma, B.; Odisho, A.; Kaye, J. S.; Kaye, A. J.; Kaye, A. M.; Kaye, A. D.; Mychaskiw, G.; Viswanath, O.; Urits, I. Brexpiprazole for the Treatment of Schizophrenia and Major Depressive Disorder: A Comprehensive Review of Pharmacological Considerations in Clinical Practice. Psychopharmacology Bulletin 2021, 51 (2), 69–95.
- Montejo, Brand, B. A.; Willemse, E. J. M.; Hamers, I. M. H.; Sommer, I. E. Evidence-Based Recommendations for the Pharmacological Treatment of Women with Schizophrenia Spectrum Disorders. Current Psychiatry Reports 2023, 25 (11), 723–733. [CrossRef]
- Mauri, M. C.; Paletta, S.; Di Pace, C.; Reggiori, A.; Cirnigliaro, G.; Valli, I.; et al. Clinical Pharmacokinetics of Atypical Antipsychotics: An Update. Clinical Pharmacokinetics 2018, 57. Springer International Publishing. [Internet].
- Das, S.; Barnwal, P.; Winston, A. B.; Mondal, S.; Saha, I. Brexpiprazole: so far so good. Therapeutic Advances in Psychopharmacology 2016, 6(1), 39–54. [CrossRef]
- Correll, C. U.; Skuban, A.; Ouyang, J.; Hobart, M.; Pfister, S.; McQuade, R. D.; Nyilas, M.; Carson, W. H.; Sanchez, R.; Eriksson, H. Efficacy and safety of brexpiprazole for the treatment of acute schizophrenia: a 6-week randomized, double-blind, placebo-controlled trial. Am J Psychiatry 2015, 172, 870–880. [CrossRef]
- Kane, J. M.; Skuban, A.; Ouyang, J.; Hobart, M.; Pfister, S.; McQuade, R. D.; Nyilas, M.; Carson, W. H.; Sanchez, R.; Eriksson, H. A multicenter, randomized, double-blind, controlled phase 3 trial of fixed-dose brexpiprazole for the treatment of adults with acute schizophrenia. Schizophr Res 2015, 164, 127–135. [CrossRef]
- Fleischhacker, W. W.; Hobart, M.; Ouyang, J.; Forbes, A.; Pfister, S.; McQuade, R. D.; Carson, W. H.; Sanchez, R.; Nyilas, M.; Weiller, E. Efficacy and safety of brexpiprazole (OPC-34712) as maintenance treatment in adults with schizophrenia: a randomized, double-blind, placebo-controlled study. Int J Neuropsychopharmacol 2017, 20, 11–21. [CrossRef]
- Siwek, M.; Wojtasik-Bakalarz, K.; Krupa, A. J.; Chrobak, A. A. Brexpiprazole-Pharmacologic Properties and Use in Schizophrenia and Mood Disorders. Brain Sciences 2023, 13 (3), 397. [CrossRef]
- Nickols, J. E. R.; Dursun, S. M.; Taylor, A. M. W. Preclinical evidence for the use of the atypical antipsychotic, brexpiprazole, for opioid use disorder. Neuropharmacology 2023, 233, 109546. [CrossRef]
- Kung, F. H.; Lin, H. Y.; Tai, Y. M.; et al. Brexpiprazole in the Treatment of Cannabis Withdrawal Psychotic Disorder. Am J Ther 2022, 29(4), 492-493. [CrossRef]
- Ishibashi, T.; Horisawa, T.; Tokuda, K.; Ishiyama, T.; Ogasa, M.; Tagashira, R.; Matsumoto, K.; Nishikawa, H.; Ueda, Y.; Toma, S.; Oki, H.; Tanno, N.; Saji, I.; Ito, A.; Ohno, Y.; Nakamura, M. Pharmacological profile of lurasidone, a novel antipsychotic agent with potent 5-hydroxytryptamine 7 (5-HT7) and 5-HT1A receptor activity. J Pharmacol Exp Ther 2010, 334(1), 171–181. [CrossRef]
- Miura, I.; Horikoshi, S.; Ichinose, M.; Suzuki, Y.; Watanabe, K. Lurasidone for the Treatment of Schizophrenia: Design, Development, and Place in Therapy. Drug Design, Development and Therapy 2023, 17, 3023–3031. [CrossRef]
- Sunovion. Latuda (Lurasidone HCl) Tablets: Highlights of Prescribing Information. Sunovion, 2013. http://www.latuda.com/LatudaPrescribingInformation.pdf.
- European Medicines Agency. Latuda: EPAR - Product Information. Annex I: Summary of Product Characteristics. EMA, 2014. http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002713/WC500164683.pdf.
- Preskorn, S.; Ereshefsky, L.; Chiu, Y. Y.; Poola, N.; Loebel, A. Effect of food on the pharmacokinetics of lurasidone: results of two randomized, open-label, crossover studies. Human psychopharmacology 2013, 28 (5), 495–505. [CrossRef]
- Chiu, Y. Y.; Ereshefsky, L.; Preskorn, S. H.; Poola, N.; Loebel, A. Lurasidone drug-drug interaction studies: a comprehensive review. Drug metabolism and drug interactions 2014, 29 (3), 191–202. [CrossRef]
- Sanford, M. Lurasidone: In the Treatment of Schizophrenia. CNS Drugs 2013, 27, 67–80.
- Ng-Mak, D.; Tongbram, V.; Ndirangu, K.; Rajagopalan, K.; Loebel, A. Efficacy and Metabolic Effects of Lurasidone Versus Brexpiprazole in Schizophrenia: A Network Meta-Analysis. J. Comp. Eff. Res. 2018. [CrossRef]
- Corponi, F.; Fabbri, C.; Bitter, I.; Montgomery, S.; Vieta, E.; Kasper, S.; Pallanti, S.; Serretti, A. Novel Antipsychotics Specificity Profile: A Clinically Oriented Review of Lurasidone, Brexpiprazole, Cariprazine, and Lumateperone. Eur. Neuropsychopharmacol. 2019, 29 (9), 971–985. [CrossRef]
- Zheng W, Cai DB, Yang XH, et al. Short-term efficacy and tolerability of lurasidone in the treatment of acute schizophrenia: a meta-analysis of randomized controlled trials. J Psychiatr Res 2018, 103, 244–251. [CrossRef]
- Citrome L, Cucchiaro J, Sarma K, et al. Long-term safety and tolerability of lurasidone in schizophrenia: a 12-month, double-blind, active-controlled study. Int Clin Psychopharmacol 2012, 27(3), 165–176. [CrossRef]
- Stahl SM, Cucchiaro J, Simonelli D, Hsu J, Pikalov A, Loebel A. Effectiveness of lurasidone for patients with schizophrenia following 6 weeks of acute treatment with lurasidone, olanzapine, or placebo: a 6-month, open-label, extension study. J Clin Psychiatry 2013, 74 (05), 507–515. [CrossRef]
- Wei, Y. M.; Wang, X. J.; Yang, X. D.; Wang, C. S.; Wang, L. L.; Xu, X. Y.; Zhao, G. J.; Li, B.; Zhu, D. M.; Wu, Q.; Shen, Y. F. Safety and effectiveness of lurasidone in the treatment of Chinese schizophrenia patients: An interim analysis of post-marketing surveillance. World journal of psychiatry 2023, 13(11), 937–948. [CrossRef]
- Correll CU, Cucchiaro J, Silva R, Hsu J. Long-term safety and effectiveness of lurasidone in schizophrenia: a 22-month, open-label extension study. CNS Spectr 2016, 21(5), 393–402. [CrossRef]
- Higuchi T, Ishigooka J, Iyo M, Hagi K. Safety and effectiveness of lurasidone for the treatment of schizophrenia in Asian patients: results of a 26-week open-label extension study. Asia Pac Psychiatry 2020, 12(1), e12377. [CrossRef]
- Ricci, V.; Martinotti, G.; De Berardis, D.; Maina, G. Lurasidone use in Cannabis-Induced Psychosis: A Novel Therapeutic Strategy and Clinical Considerations in Four Cases Report. International journal of environmental research and public health 2022, 19(23), 16057. [CrossRef]
- Mole, T. B.; Furlong, Y.; Clarke, R. J.; Rao, P.; Moore, J. K.; Pace, G.; Van Odyck, H.; Chen, W. Lurasidone for Adolescents With Complex Mental Disorders: A Case Series. Journal of pharmacy practice 2022, 35(5), 800–804. [CrossRef]
Figure 1.
Flow-chart of study search and selection process.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



