
Submitted:
25 January 2024
Posted:
25 January 2024
You are already at the latest version
Abstract
Pituitary adenomas are benign brain tumors that pose a heavy burden on patients worldwide. However, the local burden of disease is yet to be established due to scarcity of data. In line with this, this study aims to present the challenges and gaps in the treatment of pituitary adenomas in the Philippines. A scoping review of available relevant literature on epidemiology, clinical experience with treatment, health financing, and healthcare delivery system based on the Preferred Reporting Items for Systematic reviews and Meta-analysis guidelines extension for Scoping Reviews was conducted. The scarcity of updated local clinical data, inequity of distribution of resources, inadequate government support, and lack of affordable diagnostic testing, medications and neurosurgical procedures are the factors that hinder provision of adequate care of pituitary adenomas in the Philippines. There are notable treatment gaps in the management of pituitary adenomas in the Philippines, which may be addressed by strengthening universal healthcare. Strategies to address these gaps were proposed, including improving public-private insurance coverage, increasing manpower, enhancing accessibility to resources, and spreading more awareness.
Keywords:
Pituitary adenoma
; treatment gaps
; healthcare
1. Introduction
Pituitary adenomas are primary brain tumors that are usually benign. With its increasing incidence and prevalence, and its potential to cause significant morbidity, these tumors may impose a heavy burden on both patients and their families as well as our health care systems [1]. Symptoms usually arise from compression of adjacent structures (blurring of vision, visual field defects, diplopia, increased intracranial pressure) as well as signs and symptoms of deficient or excess hormone production [2,3,4]. In recent studies, pituitary adenomas have been found to comprise approximately 10-15% of brain tumors, being the third most common intracranial neoplasm after meningiomas and gliomas [2,5]. With the widespread use of better diagnostic modalities and imaging techniques, prevalence has also increased [2]. Locally, there is still paucity of epidemiological data for pituitary adenomas.
Treatment options for pituitary adenomas include surgical excision, medical therapies, and radiotherapy. In general, surgery is recommended primarily in symptomatic patients with nonfunctioning pituitary adenomas and Cushing’s disease [3,6]. It is, however, offered for prolactinomas only when they have either resistance or drug intolerance to medical treatment with dopamine agonists (DA) [2,3].
The burden of disease is still considered severe and chronic as these patients usually need life-long care and treatment hence, it is important to determine and bridge the gaps in the management of pituitary adenoma [7]. To date, there is no report available on the treatment gaps in the management of pituitary adenomas in our country. Therefore, this study aimed to review the present health care service delivery for patients with pituitary adenomas in the Philippines, and to identify any existing gaps and challenges in the management of these tumors.
2. Materials and Methods
Protocol
The authors used the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines in performing this review [8]. The authors confirm that this scoping review was prepared in accordance with the Committee on Publication Ethics rules and regulations. Given the nature of this study, institutional and ethics review board approval was not required.
Eligibility Criteria
We included systematic reviews, meta-analyses, guidelines, randomized controlled trials, retrospective cohort studies, case series and reports, and textbooks done in the Philippines and with authors affiliated with institutions in the country. Studies involving adult and pediatric subjects were included. Studies using animal subjects were also included. There was no limitation in the publication year of the studies. We excluded abstracts and articles that were not written in English.
Information/Data sources
International medical databases including Pubmed, SCOPUS, EBSCO, ClinicalTrial.gov, Western Pacific Region Index Medicus, and EMBASE were used in searching for relevant studies. The local medical database, Health Research and Development Information Network was also used in finding studies. Available and relevant literature via official websites including the Philippine Department of Health (DOH), Philippine Health Insurance Corporation (Philhealth), Philippine Statistics Authority (PSA), and medical associations (Philippine Neurological Association, Academy of Filipino Neurosurgeons, and Philippine College of Endocrinology, Diabetes, and Metabolism) were obtained.
Search and selection of sources
A scoping review of literature from the earliest indexed record of the databases until August 31, 2023 was conducted. The search terms (‘pituitary adenoma’ OR ‘pituitary macroadenoma’ OR ‘pituitary microadenoma’) AND ‘Philippines’ were used. Database searches were combined. Titles and abstracts were evaluated and were screened based on the eligibility criteria. After duplicates were excluded, full-text articles were reviewed.
Charting of data and synthesis of results
Pertinent information regarding legislation, epidemiology, healthcare financing, information systems, workforce, pharmacotherapy, surgical management, and healthcare services in the local treatment of pituitary adenoma were obtained. Authors, titles, and institutional affiliation were extracted from the published studies. Data on the availability and cost of diagnostics, medications, and surgeries were also acquired from private and government medical institutions. The core topics were analyzed using a qualitative content approach. Data obtained were narratively described and summarized into figures and tables. A conceptual framework was done to show the determined treatment gaps and challenges.
3. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
3.1. Search of studies
A total of 63 articles were obtained from the search (Figure 1), with 49 articles remaining after duplicates were removed. Thirty articles not related to pituitary adenomas in the Philippines were excluded. Nineteen articles were assessed for eligibility, with two articles excluded because they had no Filipino authors and four articles had only abstracts available. A total of 13 articles were included for synthesis.
3.2. Epidemiology of Pituitary Adenoma in the Philippines
Currently, there is no available epidemiological study of pituitary adenoma in the Philippines, and only hospital-based reports and data are accessible. A 2003 study looked at 120 patients diagnosed with pituitary adenomas at the Philippine General Hospital (PGH). Sixty two percent of the patients were female while 38% were male, with ages ranging from 15 to 75 years old (2). The most common presenting symptoms were headache (n = 120, 54%) and visual disturbances (n = 120, 42%). Of the 120 patients, 15% presented with acromegaly with elevated growth hormones and only two had cushingoid features. Cranial imaging findings showed that 90% were macroadenomas, with 94% suprasellar at the time of diagnosis. Eighty four patients underwent surgery, with 82% (n = 84) being done via a transsphenoidal approach [2]. Another retrospective study done in a private tertiary institution with 45 patients showed that males and females were almost equally affected, with ages ranging from 31 to 60. The most common symptoms were visual disturbances (n = 45, 35%) and headache (n = 45, 28%). Cranial imaging findings were consistent with a pituitary adenoma in 73% (n = 45) of patients, with the majority having microadenomas (n = 45, 73%) [9]. Seventy six percent of the patients (n = 45) underwent surgery, mostly through the transsphenoidal approach (n = 45, 49%). Eleven percent (n = 45) had subsequent gamma knife stereotactic radiation [9].
In a 2013 case series done in PGH on patients presenting with Cushing’s syndrome, adrenocorticotropic hormone (ACTH)-producing pituitary adenomas were found to be the most common cause of Cushing’s syndrome, comprising 42% (n = 103) of cases [10]. This is consistent with the usual etiologies of endogenous Cushing’s syndrome worldwide. Table 1 (Appendix A) shows the summary of the clinical profile and the outcomes of patients with pituitary adenoma in the Philippines from published case reports.
3.3. Local Research in Pituitary Adenoma
As of August 2023, there were only 13 indexed research studies from the Philippines (Table 2-Appendix B): five case reports, six retrospective studies, one systematic review, and one cross-sectional study.
3.4. The Healthcare System of the Philippines
Healthcare in the Philippines is delivered through a dual system composed of the public sector and the private sector [11]. The DOH supervises the government corporate hospitals, specialty and regional hospitals, while local government units (LGUs) manage the district and provincial hospitals, and other rural health units [11]. This system is dependent on the premise that the LGUs are the most informed of their constituents’ health needs, thus being able to immediately respond and provide for their needs [11,12]. In addition, the topography of the Philippines, being an archipelago with 7641 islands, also contributes to the maldistribution of health facilities, health personnel and specialists, especially in isolated rural areas [11].
3.4. Healthcare Financing and Coverage in the Philippines
In 2021, the Current Health Expenditure (CHE) of the Philippines reached USD 19.2 billion (USD 1.00 = PHP 56.60 as of August 26, 2023), which was 18.5% higher than in 2020. On average, every Filipino spent USD 173.80 for healthcare [13]. In the past decade, the government’s contribution to healthcare financing has increased from 21% to 38.7%, while out-of-pocket spending has decreased from 58.9% to 45.0% [14]. Although government health expenditure has increased significantly, it remains outstripped by private sector funding sources [11]. PhilHealth introduced social health insurance in 1995 to serve as coverage for Filipinos not able to financially cover their healthcare needs. This government health insurance system reportedly provides coverage for 92% of the population, of which 40% belong to the poor sector of the population, fully subsidized by the government [11]. However, services that are covered are mostly inpatient care, with outpatient care costs provided only for the lower income members [11]. Even with the expansion of Philhealth coverage, out-of-pocket payments remain high (44%), serving as the major source of funding for healthcare [11,12].
PhilHealth coverage for central nervous system neoplasms are divided into benign or malignant cases. Pituitary tumors fall under the category of benign neoplasms of endocrine glands with a case rate of USD 211.90. Complications arising from pituitary adenoma treatment that are covered by PhilHealth are under disorders of the pituitary gland, with a case rate of USD 208.40 or Cushing’s syndrome with a case rate of USD 167.80 [15].
In 2019, the “Malasakit” (Concern) Centers were established in all DOH hospitals in the country as well as in PGH as mandated by Republic Act No. 11463. They serve as a one-stop shop for medical and financial assistance from the DOH, Department of Social Welfare and Development, Philippine Charity Sweepstakes Office, and PhilHealth. They will also facilitate access to financial assistance programs provided by other government agencies, LGUs, nongovernmental organizations, and private institutions and individuals [16].
There are also available non-government agencies that provide funding for healthcare of patients with neurologic diseases such as the Philippine Brain Tumor Alliance, Sagip Buhay Medical Foundation Inc., and Let's Save the Brain Foundation, that help in funding diagnostic workups, treatment regimens, and surgical needs of patients [12,17,18,19].
3.5. Specialist Training and Medical Education
The diagnosis of pituitary adenomas requires a multidisciplinary approach with a group of specialists including endocrinologists, neurologists, and neurosurgeons, working together to develop an “individualized patient-centric” approach [20,21]. Currently, the ratio of medical doctors per 10,000 patients is 7.86 [22]. As of October 2023, there are 702 PNA board-certified adult neurologists and 100 board-certified pediatric neurologists, but the distribution is skewed towards the urban areas, with approximately 45% working in the National Capital Region (NCR) [23,24,25]. One adult neurologist is available for every 140,000 adult Filipinos, while one pediatric neurologist for every 315, 000 Filipino children.
As of October 2023, there are 174 board-certified neurosurgeons practicing in the Philippines, or approximately one neurosurgeon for every 600,000 Filipinos [26]. There are 11 accredited training institutions for adult neurology, each with four to five graduates per year: 11 institutions for neurosurgery, each with one to three graduates per year, and three institutions for pediatric neurology in the Philippines, each with one to three graduates per year as well [25,26]. Currently, there are only 525 endocrinologists in the Philippines, with 422 who are board-certified mostly practicing in the NCR [27]. In the country, there are now 12 training institutions under the Philippine College of Endocrinology, Diabetes and Metabolism, each with an average of 2 to 6 graduates per institution per year, a total of 25-30 graduates per year [27]. On the other hand, there are 112 practicing radiation oncologists distributed in 51 facilities throughout the country at present [28,29]. There are nine residency training programs that produce an average of 1 to 2 graduates per year [29].
3.6. Challenges on Diagnostics
ACTH-producing pituitary adenoma is the most frequent cause of Cushing’s Syndrome [10,30]. Following the algorithm for assessment of patients suspected with Cushing’s Syndrome, 24-hr urinary free cortisol, overnight dexamethasone suppression test, and serum ACTH are necessary diagnostic tests [10,31]. Midnight salivary cortisol may also be used; however, it is available only in selected laboratories [31]. Cranial magnetic resonance imaging with contrast is needed to document the presence of a pituitary lesion, and the presence of any hemorrhage. [18,32]. Evaluation of levels of different hormones such as prolactin, thyroid-stimulating hormone (TSH), free T4, follicle-stimulating hormone (FSH), estradiol or testosterone, ACTH, growth hormone (GH), insulin growth factor-1 (IGF-1) and fasting early morning cortisol are also necessary [21].
Endocrine tests are offered in laboratories and large tertiary centers which are usually privately-owned with prices ranging from USD 6-57 [33]. In 2016, DOH reported that there were 429 CT machines (4.2 machines per 1 million population) and 78 magnetic resonance imaging (MRI) units (0.8 MRI units per 1 million population) across government hospitals as well as private imaging facilities [33]. Price ranges from USD 150-200, depending on the institution [22]. Table 3 (Appendix C) shows the summary of estimated prices of some diagnostic tests needed for the evaluation of pituitary adenomas. Based on current medical case rates, neurosurgical procedures, specifically craniotomy and biopsy with or without excision of tumor have rates ranging from USD 2060-4120 [15,23].
3.6. Challenges on Treatment
A multidisciplinary approach is necessary for the ideal treatment of pituitary adenomas. For non-functioning macroadenomas, prompt surgical resection via a transsphenoidal approach or craniotomy is recommended in patients with visual abnormalities such as visual field defect and ophthalmoplegia [34,35], and more emergently in patients who present with pituitary apoplexy, loss of endocrine function, and significant tumor growth [20,36,37,38,39]. The PhilHealth coverage for excision of pituitary tumor via a transsphenoidal approach only amounts to USD 900, which at most covers less than half of the minimum cost of surgery [15].
For patients with functioning tumors, management depends on the hormone involved. For prolactin-secreting adenomas, DAs are the first-line treatment [20]. Currently available DAs are cabergoline and bromocriptine. Cabergoline is more than 90% effective in normalizing prolactin levels and decreasing tumor size with the advantage of being given only twice weekly; unfortunately, it is expensive, not readily available in the country, and has to be imported from other countries like India [20,39]. Bromocriptine is available in some local drugstores costing around USD 2 per tablet [40]. For patients with persistently elevated IGF-1 and GH, somatostatin analogs are given, such as octreotide, lanreotide, and pasireotide. Only octreotide long-acting release (LAR) is available in the Philippines, given subcutaneously at doses 20-40 mg monthly, with prices ranging from USD 10-17 per 0.1/mL 1mL ampule [40]. It can be subsidized occasionally through medical social services but not sustainable on a long-term basis as the cost remains prohibitive. Lanreotide autogel 90 mg pre-filled formulation was previously available in the country. However, its FDA approval had expired in 2021 [41]. For patients with recurrent and refractory Cushing’s disease, drug therapy that targets steroidogenesis such as ketoconazole and metyrapone may be used. However, there is a low utilization rate in our setting on top of the difficulty in access and high costs. For patients with non-functioning tumors presenting with hormonal deficiencies, lifelong monitoring of hormone levels is necessary to ensure appropriate and correct dosing of hormone replacement therapy. Regular monitoring of hormones entails additional costs on top of large out-of-pocket expenses for hormone replacement. The most common hormone deficiencies associated with large non-functioning adenomas include cortisol, thyroid hormones and sex steroids. Glucocorticoid replacement using hydrocortisone, prednisone and prednisolone are often the agents of choice. Both prednisone and prednisolone are available in most pharmacies but hydrocortisone has to be purchased from special compounding pharmacies. All these agents are relatively affordable. Thyroid hormone replacement in the form of levothyroxine is accessible and affordable for most patients. Sex hormone replacement utilizes testosterone injections (testosterone enanthate, cypionate, or undecanoate) for men and oral (estradiol valerate) or injected estradiol (estradiol benzoate or equivalent ester) for premenopausal women. Unfortunately, most of these sex hormone replacement therapies are not readily available in the local setting. Patients in need of these replacement regimens often purchase from online sellers and bodybuilding or supplement shops.
Radiotherapy (RT) is considered in patients with recurrent tumors and progressive residual tumors [20]. As of 2019, there are 50 RT-capable centers in the Philippines. However, most are located in the Metro Manila area, with 1-2 major hospitals in the other two major islands in the country having this capability (Cebu in the Visayas and Davao in Mindanao) [23]. The cost for RT depends on the number of sessions, usually costing USD 2000-4000 for the entire treatment duration [23,38]. In addition, patients undergoing radiotherapy should subsequently be monitored for the development of panhypopituitarism which occurs approximately 5-10 years post-RT. Replacement of deficient hormones with appropriate monitoring is needed for this subset of patients.
4. Discussion
Pituitary adenomas require collaborative efforts of specialists with a combined surgical and medical approach. The necessary diagnostics and treatment modalities are available in the Philippines, but access remains limited to urbanized centers as in other low to middle income countries, thus adding to the difficulty in decreasing the burden of the disease. Updated research on pituitary adenomas and their management is also sparse. There are no high-volume specialized pituitary centers where such data can be generated. Despite policies in place, timely diagnosis and universal access to treatment for patients with pituitary adenomas remain difficult.
Tumor excision and medical control of clinical symptoms are the mainstays in the treatment of pituitary adenomas. These treatment modalities are expensive in the Philippines due to limited insurance coverage from government or private sources, and expenses are shouldered mostly by the patients themselves. Currently, there are no studies on the comparative cost of treatment in Southeast Asia. Access and cost of medications also pose a challenge, with most first-line drugs unavailable locally. Logistically, most of the brain surgery and radiotherapy capable secondary and tertiary medical centers are concentrated in urban centers, thus rendering treatment options even less accessible to the greater majority of patients belonging to the lower socioeconomic strata. The scarcity of specialists also has a significant impact since a collaborative approach is necessary for adequate management of the disease. There is no data yet for the ideal ratio of specialists to patients; however, according to the World Health Organization, the ideal doctor-patient ratio is 10:10,000 [22]. In 2021, the Philippines had 7.86 medical doctors per 10,000 population [22].
In general, treatment of diseases in the Philippines faces economic, administrative, and social challenges. Figure 2 (Appendix D) shows the summary of proposed challenges in the current state of healthcare for patients with pituitary adenomas in the Philippines. Some recommendations on how to address these gaps in treatment are also included. Our review and qualitative analysis revealed that health financing and manpower are the major areas for improvement in the effective management of patients with pituitary adenoma. Access to hospitals where treatments are available, including surgery and radiotherapy is a resolvable issue. This can be addressed by increasing government healthcare insurance coverage and urging private insurance companies to cover non-emergency cases for brain surgery [23]. In addition, establishment of larger centers across the country to decongest the already crowded and long queues in Metro Manila. The unavailability of some medications in the local market can be solved by increasing availability and volume of these drugs, especially in public pharmacies. Government academic centers together with the DOH can spearhead the procurement process based on need and utilization measures. Also, establishing more training programs to produce more endocrinology, neurology, and neurosurgery graduates may help address the lack of specialists. Producing an updated database on epidemiology and local experience in managing pituitary adenomas will help formulate administrative programs that can further bridge gaps in treatment. Lastly, setting up a streamlined referral system or network based on the working database or registry across different centers that cater to the care of patients with pituitary adenoma will definitely help improve our process flow.
One limitation of this review is the unavailability of access to unpublished studies. Despite our efforts to be as comprehensive as possible, this review may not have retrieved all pertinent studies in the published, unpublished, and unreported literature. The search algorithm and the keywords that were used may have failed to include other pertinent terms. Only articles published in English were included, thus some studies written in other languages may have been missed. Moreover, the reviewer used her judgment to determine whether the studies have met the criteria and may be subject to reviewer bias.
To our best knowledge, this is the first scoping review that described gaps and challenges in the treatment of pituitary adenomas in the Philippines. Findings of this study advocate better recognition for patients, clinicians, researchers, and legislators alike.
5. Conclusions
There are gaps in the management of pituitary adenomas in the Philippines. These include availability and affordability of medications, lack of manpower, as well as inequity in access to facilities, inadequate coverage of government and private healthcare insurance, and scarcity of local studies and epidemiologic data.
Author Contributions
Data curation, interpretation of data, formal analysis, writing-original draft, writing-review, and editing, MMBT and MALUH; Data curation, formal analysis, interpretation of data, writing-review, editing, and study supervision, AEC, PDM, and HHCC; Conceptualization, methodology, interpretation of data, writing-review, editing, and study supervision, RDGJ. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix

Table A1.
Summary of clinical outcomes of pituitary adenoma cases.
| Author | Age/ Sex |
Type of adenoma | Clinical Presentation | Imaging findings | Hormonal Profile | Surgical Treatment | Medical Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|
| Bunoy et al., 2012 (4) | 38/M | Macro- adenoma |
Seizures, frontal headache, blurring of vision (bitemporal hemianopsia) | 4.0 x 5.0 x 4.5 cm sellar-suprasellar mass | Low cortisol, high TSH, normal ACTH | Cranioto- my with excision of the tumor |
Methima- zole, prednisone |
Improved |
| Mendo-za et al., 2015 (32) | 46/F | Macro- adenoma |
Amenorrhea, acromegaly | 2.1 x 3.3 x 2.4 cm sellar-suprasellar mass with foci of intratumoral hemorrhages suggestive of subclinical pituitary apoplexy | High GH, high prolactin | None | Cabergo- line 0.5 mg tablet once a week |
Improved |
| Tating et al., 2016 (30) | 13/M | Micro- adenoma |
Bilateral lower extremity weakness, hypertension | 0.8 x 0.9 x 0.8 cm anterior pituitary gland mass | High ACTH, high cortisol | Transphenoid-al adenomectom-y was indicated but deferred because dexamethasone suppression test revealed high serum cortisol and 24-hr free urine cortisol | None | Expired |
| Sandoval et al., 2020 (31) | 37/F | Macro- adenoma |
Amenorrhea, progressive weight gain, facial roundness, leg weakness, easy bruisability, blurring of vison (bitemporal hemianopsia), hyperpigmented fingernails | 4.6 x 4.1 x 7 cm lobulated, heterogeneously enhancing sellar-suprasellar mass with cystic and necrotic components | High ACTH | Transphenoid-al excision | None | Improved |
| Jordan et al., 2022 (39) | 40/F | Giant adenoma | Acromegaly, headache, blurring of vision (bitemporal hemianopsia) | 6.4 x 7.0 x 5.5 cm lobulated pituitary mass with cystic degeneration and necrosis | High GH, high IGF-1 | Surgical resection via transcranial approach | Bromocrip-tine, radiotherapy | Improved |
B Table A2.
Summary of indexed articles.
| Author | Title | Journal | Institution | Publication Year | Study Design |
|---|---|---|---|---|---|
| Villegas et al. (9) | A review of patients with pituitary tumors at St. Luke’s Medical Center from January 1997 to September 2000 | Philippine Journal of Internal Medicine | St. Luke’s Medical Center | 2002 | Retrospective study |
| Alinsonorin et al. (2) | Pituitary adenoma: clinical profile of 120 patients at the Philippine General Hospital | Philippine Journal of Internal Medicine | Philippine General Hospital | 2003 | Retrospective, descriptive |
| Fonte et al. (41) | Treatment outcomes of pituitary tumors at the University of Santo Tomas Hospital: 2004-2008 | Philippine Journal of Internal Medicine | University of Santo Tomas Hospital |
2009 | Retrospective cohort |
| Bunoy et al. (4) | Inappropriate secretion of thyroid stimulating hormone in a Filipino patient with a pituitary macroadenoma | Journal of ASEAN Federation of Endocrine Societies | St. Luke’s Medical Center | 2012 | Case report |
| Lo et al. (10) | Endogenous Cushing’s syndrome: the Philippine General Hospital experience | Journal of ASEAN Federation of Endocrine Societies | Philippine General Hospital | 2014 | Cross-sectional |
| Jordan et al. (39) | The sleeping giant: an atypical case of a giant pituitary adenoma presenting as acromegaly with minimal symptoms of mass effect | Journal of ASEAN Federation of Endocrine Societies | St. Luke’s Medical Center | 2014 | Case report |
| Mendoza et al. (32) | Acromegaly with cardiomegaly, cardiac thrombus and hemorrhagic cerebral infarct: a case report of therapeutic dilemma with review of literature | International Journal of Endocrinology and Metabolism | University of Santo Tomas Hospital |
2015 | Case report |
| Tating et al. (30) | Cushing’s syndrome from pituitary microadenoma and pulmonary nodules | Oncology Nursing Forum | Philippine General Hospital | 2016 | Case report |
| Faltado et al. (6) | Factors associated with postoperative diabetes insipidus after pituitary surgery | International Journal of Endocrinology and Metabolism | Philippine General Hospital | 2017 | Retrospective cohort |
| Carampatana-Jandug et al. (38) | In-hospital postoperative complications in patients with pituitary adenoma who underwent pituitary surgery from January 2010 to December 2015: a multicenter study | International Journal of Endocrinology and Metabolism | Chong Hua Hospital | 2017 | Retrospective cohort |
| Cudal et al. (37) | Postoperative complications of trans-sphenoidal surgery in a local tertiary hospital during hospital stay | Philippine Journal of Internal Medicine | Makati Medical Center | 2018 | Retrospective cross- sectional |
| Sandoval et al. (31) | Nail hyperpigmentation in ACTH-secreting pituitary adenoma (Cushing’s disease) and its resolution after successful trans-sphenoidal excision | BMJ Case Reports | Philippine General Hospital | 2020 | Case report |
| Seng et al. (3) | Extracapsular resection of pituitary adenomas: a systemic review | Asian Journal of Neurosurgery | Philippine General Hospital | 2023 | Systematic review |
C. Table 3.
Price range of diagnostic tests.
| Laboratory Test/ Imaging | Cost Government- subsidized (USD) |
Cost No government no subsidy (USD) |
Cost Private (USD) |
|---|---|---|---|
| IGF-1 | NA | NA | 175.00 |
| ACTH | NA | NA | 136.90 |
| Cortisol | NA | NA | 52.80 |
| Prolactin | 5.80 | 8.50 | 9.10-31.20 |
| FSH | 6.10 | 9.70 | 11.50-24.20 |
| LH | 9.20 | 12.40 | 13.00-24.20 |
| Estradiol | 6.90 | 10.60 | 11.10-46.80 |
| Testosterone | 15.30 | 32.20 | 33.80-46.80 |
| TSH | 6.10 | 10.50 | 12.10-14.40 |
| FT3 | 8.30 | 12.90 | 13.60-49.90 |
| FT4 | 6.40 | 10.00 | 10.50-49.90 |
| Cranial MRI with contrast | 153.70 | 179.30 | 190.00-210.90 |
| Cranial MRI - plain | 75.60 | 91.30 | 96.60-107.30 |
| Cranial CT scan with contrast | 86.30 | 98.10 | 103.00-112.80 |
| Cranial CT scan - plain | 26.30 | 54.40 | 65.30-73.50 |
CT - computerized tomography, MRI - magnetic resonance imaging, NA - not available, IGF-1 - Insulin-like growth hormone-1, ACTH - Adrenocorticotropic hormone, FSH - follicle stimulating hormone, LH - luteinizing hormone, TSH - thyroid stimulating hormone, FT3 - free triiodothyronine, FT4 - free thyroxine hormone.
D. Figure 2.
Conceptual framework exhibiting gaps in the treatment of pituitary adenoma in the Philippines.
D. Figure 2.
Conceptual framework exhibiting gaps in the treatment of pituitary adenoma in the Philippines.

References
- Daly, A.F.; Beckers, A. The epidemiology of pituitary adenomas. Endocrinol Metab Clin North Am. 2020, 49, 347–55. [Google Scholar] [CrossRef]
- Alinsonorin, D.; Santos-Batongbacal, M.; Paz-Pacheco, E.; Trajano-Acampado, L. Pituitary adenoma: clinical profile of 120 patients at the Philippine General Hospital. Philipp J Int Med. 2003, 41, 323–29. [Google Scholar]
- Seng, K.S.; Malilay, O.R.M. Extracapsular resection of pituitary adenomas: a systematic review. Asian J Neurosurg. 2023, 18, 5–11. [Google Scholar] [CrossRef]
- Bunoy, L.S.; Co, J.M.I.O. Inappropriate secretion of thyroid stimulating hormone in a Filipino patient with a pituitary macroadenoma. J ASEAN Fed Endocr Soc. 2012, 27(1), 114–8. [Google Scholar] [CrossRef]
- Chavez, S.; Tan, C. Pituitary macroadenoma presenting as a synchronous occurrence of acromegaly and cushing’s disease. Rev Argent Endocrinol Metab. 2021, 58, 226. [Google Scholar]
- Faltado, A.L.; Macalalad-Josue, A.A.; Li, R.J.S.; Quisumbing, J.P.M.; Yu, M.G.Y.; Jimeno, C.A. Factors associated with postoperative diabetes insipidus after pituitary surgery. Endocrinol Metab. 2017, 32, 426. [Google Scholar] [CrossRef]
- Biermasz, N.R. The burden of disease for pituitary patients. Best Pract Res Clin Endocrinol Metab. 2019, 33, 101309. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and xxplanation. Ann Intern Med. 2018, 169, 467–73. [Google Scholar] [CrossRef] [PubMed]
- Villegas, M.; Quinto, G.; Quimpo, J. A Review of patients with pituitary tumors at St. Luke’s Medical Center from January 1997 to September 2000. Philipp J Intern Med. 2002, 40, 40–3. [Google Scholar]
- Lo, T.E.; Cabradilla, J.M.; Lim, S.A.; Jimeno, C.A. Endogenous Cushing’s syndrome: the Philippine General Hospital experience. J Solid Tumors. 2013, 4, 1–10. [Google Scholar]
- Dayrit, M.M.; Lagrada, L.P.; Picazo, O.F.; Pons, M.C.; Villaverde, M.C. The Philippines Health System Review; World Health Organization: New Delhi, India, 2018; Vol 8, No. 2; pp. 1–12. [Google Scholar]
- Pagaling, G.T.; Turalde, C.W.R.; Jamora, R.D.G. Autoimmune encephalitis in the Philippines: a scoping review on the treatment gaps, challenges, and current state of care. Front Neurol. 2022, 13, 788309. [Google Scholar] [CrossRef]
- Health expenses remain a big burden for Pinoys despite UHC. Philippines: Philippine Institute for Developmental Studies. Available online: https://www.pids.gov.ph/details/news/in-the-news/health-expenses-remain-a-big-burden-for-pinoys-despite-uhc# (accessed on 12 August 2023).
- World Health Organization Global health expenditure database. Available online: https://apps.who.int/nha/database/country_profile/Index/en (accessed on 18 August 2023).
- Philippine Health Insurance Corporation List of Medical Case Rates. Available online: https://www.philhealth.gov.ph/circulars/2017/annexes/0019/AnnexA-MedicalCaseRates (accessed on 12 August 2023).
- Official Gazette of the Republic of the Philippines Republic Act No. 11463. Available online: https://www.officialgazette.gov.ph/2019/12/03/republic-act-no-11463/ (accessed on 12 August 2023).
- Let’s Save The Brain. Available online: https://letssavethebrain.org/about-us/ (accessed on 16 August 2023).
- Philippine Cancer Resources Cancer Index. Available online: http://www.cancerindex.org/Philippines (accessed on 15 December 2023).
- Sagip Buhay Medical Foundation, Inc. UP-PGH Department of Medicine. Available online: https://uppghmedicine.com.ph/services/sagip/ (accessed on 15 December 2023).
- Russ, S.; Shafiq, I. Pituitary adenoma; StatPearls Publishing [Internet]: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK554451/ (accessed on 22 August 2023).
- Tan, G.H. Diabetes care in the Philippines. Ann Glob Health. 2016, 81, 863. [Google Scholar] [CrossRef]
- World Health Organization The Global Health Observatory. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/medical-doctors-(per-10-000-population) (accessed on 15 December 2023).
- Mondia, M.W.L.; Espiritu, A.I.; Batara, J.M.F.; Jamora, R.D.G. Neuro-oncology in the Philippines: a scoping review on the state of medical practice, deterrents to care and therapeutic gaps. Ecancermedicalscience. 2021, 15, 1238. [Google Scholar] [CrossRef]
- Ignacio, K.H.D.; Espiritu, A.I.; Jamora, R.D.G. The current status and challenges in multiple sclerosis management in the Philippines. Mult Scler Relat Dis. 2020, 46, 102510. [Google Scholar] [CrossRef]
- PNA Fellows Philippine Neurological Association. Available online: https://www.philippineneurologicalassociation.com/pna-fellows (accessed on 15 December 2023).
- Academy of Filipino Neurosurgeons, Inc. Members. Available online: https://www.afninc.org/members-2/ (accessed on 26 October 2023).
- Training Institutions Philippine College of Endocrinology Diabetes and Metabolism. Available online: https://endo-society.org.ph/training-institutions/ (accessed on 5 December 2023).
- Division for Human Health: DIRAC (Directory of Radiotherapy Centres). Available online: https://dirac.iaea.org/Query/Countries (accessed on 5 December 2023).
- Facilities of Philippine Radiation Oncology Society. Available online: https://pros.org.ph/facilities/ (accessed on 5 December 2023).
- Tating, D.L.R.P.; Montevirgen, N.D.S.; Cajucom, L. Cushing’s syndrome from pituitary microadenoma and pulmonary nodules. Oncol Nurs Forum. 2016, 43, 136–40. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, M.A.S.; Bruno, R.G. Nail hyperpigmentation in ACTH-secreting pituitary adenoma (Cushing’s disease) and its resolution after successful trans-sphenoidal excision. BMJ Case Rep. 2020, 13, e234905. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, E.; Malong, C.L.; Tanchee-Ngo, M.J.; Mercado-Asis, L. Acromegaly with cardiomyopathy, cardiac thrombus and hemorrhagic cerebral infarct: a case report of therapeutic dilemma with review of literature. Int J Endocrinol Metab. 2015, 13, e18841. [Google Scholar] [CrossRef] [PubMed]
- Laboratory test prices. Available online: https://www.nwdi.com.ph/prices (accessed on 5 August 2023).
- Cudal, B.; Montano, C.; Pontillas, A.; Baraoidan, R. Post-operative complications of trans-sphenoidal surgery in a local tertiary hospital during hospital stay. Philipp J Int Med. 2018, 56(1), 15–8. [Google Scholar]
- Carampatana-Jandug, C.; Esguerra, J.M.; Panilagao, G.; Mejia, A.; Rama, J.; Bilocura, F.E. In-hospital postoperative complications in patients with pituitary adenoma who underwent pituitary surgery from January 2010 to December 2015: a multicenter study. J Endocr Metab. 2017, 7(4), 122–30. [Google Scholar] [CrossRef]
- Jordan, C.; Carmen, C.C.; Esposo, E.; Rosales, R.; Maravilla, R.D. The sleeping giant: an atypical case of a giant pituitary adenoma presenting as acromegaly with minimal symptoms of mass effect. J ASEAN Fed Endoc Soc. 2019, 34, 76. [Google Scholar]
- Te, J.; Pacia, E. Neuronavigation vs traditional C-arm fluoroscopy in transsphenoidal surgery for the excision of pituitary macroadenomas: a comparative study from the University of Santo Tomas Hospital, Philippines. J Am Coll Surg. 2018, 227, 1–2. [Google Scholar] [CrossRef]
- Fonte, J.; Matawaran, B.; Cunanan, E.; Mercado-Asis, L. Treatment outcomes of pituitary tumors at the University of Santo Tomas Hospital: 2004-2008. Philipp J Int Med. 2009, 47, 121–8. [Google Scholar] [CrossRef]
- De Roxas, R.C.; Pedro, K.M.; Rivera, J.P.; Batara, J.M.F. Current treatment status of adult brain tumors in the Philippine General Hospital. J Neurol Neurorehab Res. 2017, 2, 3–4. [Google Scholar] [CrossRef]
- Drug Price Reference Index Department of Health Philippines. Available online: https://dpri.doh.gov.ph/home/drug_2020_index/659 (accessed on 5 September 2023).
- Philippine Food and Drug Administration. Available online: https://verification.fda.gov.ph/drug_productsview.php?showdetail=®istration_number=DR-XY45172 (accessed on 18 December 2023).
Figure 1.
Flow chart of methodology adapted from the PRISMA guidelines for scoping reviews.
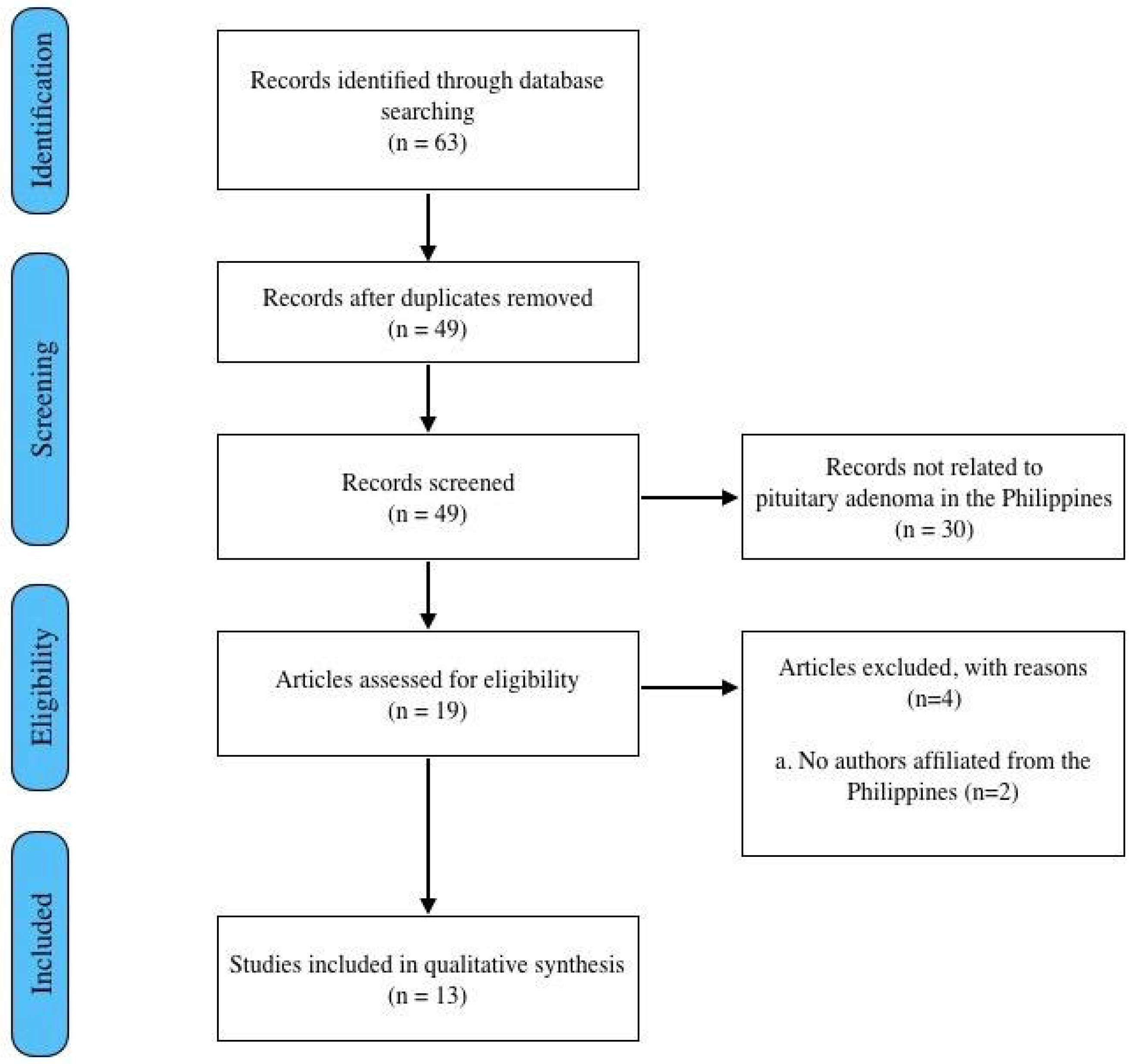
Figure 2.
Conceptual framework exhibiting gaps in the treatment of pituitary adenoma in the Philippines.
Figure 2.
Conceptual framework exhibiting gaps in the treatment of pituitary adenoma in the Philippines.
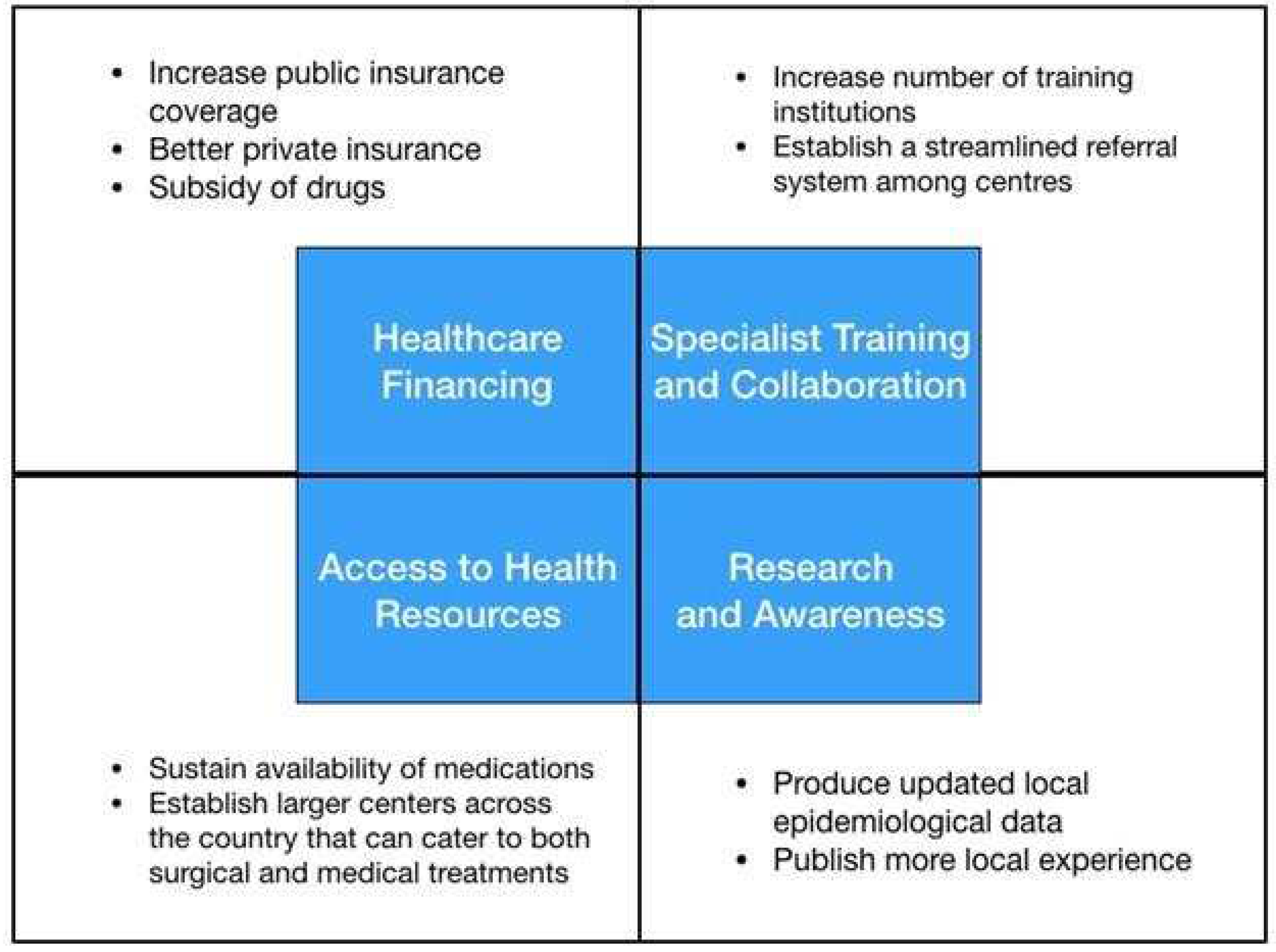
Table 1.
Summary of clinical outcomes of pituitary adenoma cases.
| Author | Age/ Sex |
Type of adenoma | Clinical Presentation | Imaging findings | Hormonal Profile | Surgical Treatment | Medical Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|
| Bunoy et al., 2012 (4) | 38/M | Macro- adenoma |
Seizures, frontal headache, blurring of vision (bitemporal hemianopsia) | 4.0 x 5.0 x 4.5 cm sellar-suprasellar mass | Low cortisol, high TSH, normal ACTH | Cranioto- my with excision of the tumor |
Methima- zole, prednisone |
Improved |
| Mendo-za et al., 2015 (32) | 46/F | Macro- adenoma |
Amenorrhea, acromegaly | 2.1 x 3.3 x 2.4 cm sellar-suprasellar mass with foci of intratumoral hemorrhages suggestive of subclinical pituitary apoplexy | High GH, high prolactin | None | Cabergo- line 0.5 mg tablet once a week |
Improved |
| Tating et al., 2016 (30) | 13/M | Micro- adenoma |
Bilateral lower extremity weakness, hypertension | 0.8 x 0.9 x 0.8 cm anterior pituitary gland mass | High ACTH, high cortisol | Transphenoid-al adenomectom-y was indicated but deferred because dexamethasone suppression test revealed high serum cortisol and 24-hr free urine cortisol | None | Expired |
| Sandoval et al., 2020 (31) | 37/F | Macro- adenoma |
Amenorrhea, progressive weight gain, facial roundness, leg weakness, easy bruisability, blurring of vison (bitemporal hemianopsia), hyperpigmented fingernails | 4.6 x 4.1 x 7 cm lobulated, heterogeneously enhancing sellar-suprasellar mass with cystic and necrotic components | High ACTH | Transphenoid-al excision | None | Improved |
| Jordan et al., 2022 (39) | 40/F | Giant adenoma | Acromegaly, headache, blurring of vision (bitemporal hemianopsia) | 6.4 x 7.0 x 5.5 cm lobulated pituitary mass with cystic degeneration and necrosis | High GH, high IGF-1 | Surgical resection via transcranial approach | Bromocrip-tine, radiotherapy | Improved |
Table 2.
Summary of indexed articles.
| Author | Title | Journal | Institution | Publication Year | Study Design |
|---|---|---|---|---|---|
| Villegas et al. (9) | A review of patients with pituitary tumors at St. Luke’s Medical Center from January 1997 to September 2000 | Philippine Journal of Internal Medicine | St. Luke’s Medical Center | 2002 | Retrospective study |
| Alinsonorin et al. (2) | Pituitary adenoma: clinical profile of 120 patients at the Philippine General Hospital | Philippine Journal of Internal Medicine | Philippine General Hospital | 2003 | Retrospective, descriptive |
| Fonte et al. (41) | Treatment outcomes of pituitary tumors at the University of Santo Tomas Hospital: 2004-2008 | Philippine Journal of Internal Medicine | University of Santo Tomas Hospital |
2009 | Retrospective cohort |
| Bunoy et al. (4) | Inappropriate secretion of thyroid stimulating hormone in a Filipino patient with a pituitary macroadenoma | Journal of ASEAN Federation of Endocrine Societies | St. Luke’s Medical Center | 2012 | Case report |
| Lo et al. (10) | Endogenous Cushing’s syndrome: the Philippine General Hospital experience | Journal of ASEAN Federation of Endocrine Societies | Philippine General Hospital | 2014 | Cross-sectional |
| Jordan et al. (39) | The sleeping giant: an atypical case of a giant pituitary adenoma presenting as acromegaly with minimal symptoms of mass effect | Journal of ASEAN Federation of Endocrine Societies | St. Luke’s Medical Center | 2014 | Case report |
| Mendoza et al. (32) | Acromegaly with cardiomegaly, cardiac thrombus and hemorrhagic cerebral infarct: a case report of therapeutic dilemma with review of literature | International Journal of Endocrinology and Metabolism | University of Santo Tomas Hospital |
2015 | Case report |
| Tating et al. (30) | Cushing’s syndrome from pituitary microadenoma and pulmonary nodules | Oncology Nursing Forum | Philippine General Hospital | 2016 | Case report |
| Faltado et al. (6) | Factors associated with postoperative diabetes insipidus after pituitary surgery | International Journal of Endocrinology and Metabolism | Philippine General Hospital | 2017 | Retrospective cohort |
| Carampatana-Jandug et al. (38) | In-hospital postoperative complications in patients with pituitary adenoma who underwent pituitary surgery from January 2010 to December 2015: a multicenter study | International Journal of Endocrinology and Metabolism | Chong Hua Hospital | 2017 | Retrospective cohort |
| Cudal et al. (37) | Postoperative complications of trans-sphenoidal surgery in a local tertiary hospital during hospital stay | Philippine Journal of Internal Medicine | Makati Medical Center | 2018 | Retrospective cross- sectional |
| Sandoval et al. (31) | Nail hyperpigmentation in ACTH-secreting pituitary adenoma (Cushing’s disease) and its resolution after successful trans-sphenoidal excision | BMJ Case Reports | Philippine General Hospital | 2020 | Case report |
| Seng et al. (3) | Extracapsular resection of pituitary adenomas: a systemic review | Asian Journal of Neurosurgery | Philippine General Hospital | 2023 | Systematic review |
Table 3.
Price range of diagnostic tests.
| Laboratory Test/Imaging | Cost Government- subsidized (USD) |
Cost No government no subsidy (USD) |
Cost Private (USD) |
|---|---|---|---|
| IGF-1 | NA | NA | 175.00 |
| ACTH | NA | NA | 136.90 |
| Cortisol | NA | NA | 52.80 |
| Prolactin | 5.80 | 8.50 | 9.10-31.20 |
| FSH | 6.10 | 9.70 | 11.50-24.20 |
| LH | 9.20 | 12.40 | 13.00-24.20 |
| Estradiol | 6.90 | 10.60 | 11.10-46.80 |
| Testosterone | 15.30 | 32.20 | 33.80-46.80 |
| TSH | 6.10 | 10.50 | 12.10-14.40 |
| FT3 | 8.30 | 12.90 | 13.60-49.90 |
| FT4 | 6.40 | 10.00 | 10.50-49.90 |
| Cranial MRI with contrast | 153.70 | 179.30 | 190.00-210.90 |
| Cranial MRI - plain | 75.60 | 91.30 | 96.60-107.30 |
| Cranial CT scan with contrast | 86.30 | 98.10 | 103.00-112.80 |
| Cranial CT scan - plain | 26.30 | 54.40 | 65.30-73.50 |
CT - computerized tomography, MRI - magnetic resonance imaging, NA - not available, IGF-1 - Insulin-like growth hormone-1, ACTH - Adrenocorticotropic hormone, FSH - follicle stimulating hormone, LH - luteinizing hormone, TSH - thyroid stimulating hormone, FT3 - free triiodothyronine, FT4 - free thyroxine hormone.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



