
Submitted:
25 January 2024
Posted:
25 January 2024
You are already at the latest version
Abstract
In the face of 21st-century environmental challenges, including climate change, migration pressures, and waste disposal issues, certain healthcare sectors, notably dentistry, pose a significant global environmental footprint with concerns about carbon emissions and waste production. This scoping review delves into the paradox that healthcare, while dedicated to safeguarding health, inadvertently contributes to environmental degradation through waste accumulation and disposal. The analysis of relevant pertinent literature emphasizes the imperative for an environmentally sustainable approach to dental waste measurement, disposal methods, and comprehensive education for stakeholders. Aligned with the World Conference on Sustainable Development and the United Nations' 2030 Agenda, the study adhered to PRISMA-ScR scoping review guidelines and Institute of Medicine's recommendations. The study utilized Medline/PubMed and international organization websites for data retrieval, employing Boolean operator queries in Medline. A systematic literature analysis identified six cross-sectional studies (2004-2018) highlighting variations in dental waste composition due to the lack of standardized identification methods. This heterogeneity underscores the need for a proposed research model, emphasizing comprehensive methodologies and healthcare staff training in waste management. The study advocates for environmentally conscious dental practices, contributing to broader sustainable healthcare goals through sharing of a research protocol for dental solid waste management.
Keywords:
environmental impact
; waste production
; dental waste
; carbon footprint
; dental services
; dental practicel
; research model
1. Introduction
Humanity confronts profound environmental challenges in the 21st century [1]. Climate change manifests in rising ocean temperatures, land degradation, altered precipitation, sea level rise, ocean acidification, extreme weather events, and biodiversity loss. Climate change, coupled with migration pressures, waste accumulation and threats to food and health security, poses the most urgent challenges to sustaining the planet [2]. Epidemiological studies estimate that climate change currently may have an impact on more than 150,000 deaths worldwide per year and between 2030 and 2050 this number will rise to 250,000 additional deaths per year [3]. Examining the global healthcare system reveals that its environmental, social, and economic sustainability is questionable due to significant carbon dioxide and waste production and disposal issues [4,5].
Sustainability on the other edge, entails human activities meeting present needs without compromising the needs of future generations, achieving a balance between economic growth, environmental care, and social well-being [6]. In dental clinical practice, sustainability involves providing ethical, high-quality care using efficient materials, emitting low carbon dioxide and producing less waste [7]. The three pillars of sustainability, social equity, economic sustainability, and environmental preservation emerged from the 2005 World Conference on Sustainable Development [8,9,10]. The 2030 Agenda for Sustainable Development, adopted in 2015, outlines 17 goals across social, economic, and environmental categories specifically identifying the problem of waste accumulation and disposal [8,9,10].
Dental waste poses significant environmental challenges, with dental mercury, primarily from dental amalgam waste, being a major contributor [8]. Regulations enforcing proper collection of mercury-contaminated waste, especially from extracted teeth with amalgam fillings, are crucial to prevent the release of harmful mercury vapor during combustion [8,9]. However, adherence to hazardous waste collection rules varies worldwide [10,11]. Additionally, the systematic classification of solid waste in dental practices reveals alarming figures, with infectious waste constituting more than 90% [8]. The absence of waste management plans in surveyed clinics, coupled with dentists' lapses in handling mercury-containing waste, and recycling in the dental office raises concerns about effective healthcare waste disposal [11]. Public safety concerns heighten as dentists must navigate the critical issue of dental waste, recognizing it as a pressing environmental concern especially with the protocols arisen during and after covid-19 pandemic [10,11]. Urgent measures and comprehensive waste management strategies are imperative to address these challenges effectively [12]. In this sense, the World Dental Federation published a statement entitled "Sustainability in Dentistry" in 2017. This document is based on the Sustainable Development Goals of the United Nations 2030 Agenda for Sustainable Development that was developed in 2017 [13]. The goal is to lay the groundwork for defining a greener and more sustainable dental clinical practice, emphasizing the use of new equipment technology to reduce waste production and disposal among other issues.
A systematic review on dental solid waste is missing from the relevant literature. Thus, this review aims to comprehensively address the multifaceted challenges surrounding dental solid waste (DSW) production and management of the last twenty-four years. Objectives include quantitatively assessing DSW scale, investigating disposal challenges, and examining the environmental impact. The review evaluates global adherence to hazardous waste collection rules in dental facilities, analyzes the systematic classification of solid waste in dental practices, and explores any lapses in handling mercury-containing waste. Additionally, it examines the post-pandemic impact on dental waste management and critically evaluates research methodologies in existing studies. The overarching goal is to provide nuanced insights and recommendations for advancing sustainable practices through waste management within dental clinical settings by systematically evaluating existing data and proposing a future research model on the issue.
2. Materials and Methods
For this study we addressed the design and implementation of a scoping review. All publications from 2000 to November 2023 reporting on waste management in dental practices and dental laboratories, as well as the ecological footprint of dentistry, were included in the study. To be considered for inclusion in the study sample, publications could not be narrative reviews, systematic reviews, letters to the editor, or editorials. Any study that did not explain the process for collecting, separating, and analyzing dental waste, lacked an abstract or use other than the English language, was further excluded. In Table S1, and S2, the papers that were excluded and their reasons for exclusion are summarized.
The Preferred Reporting Items for PRISMA-ScR scoping review statement [14] and the Institute of Medicine's guidelines [15] were followed in this study. The electronic database of Medline/PubMed was consulted for this study. It was consulted the websites of international organizations such as the Health and Social Care Information Centre, the United Nations Framework Convention on Climate Change, the American Society for Testing and Materials, the World Dental Federation, the World Economic Forum, and Public Health England accessed by 18 November 2023.
Using queries with Boolean operators as keywords for titles and abstracts, an electronic search was performed in Medline (via PubMed). Specifically, we used the following search query: ("dental laboratoires") OR ("dental practice") OR ("dentistry") AND ("sustainab*") OR ("green dentistry")) AND (("waste management") OR ("carbon footprint") OR ("green dentistry") OR ("dental solid waste") OR ("carbon emissions"). The references of each paper were reviewed, and conference abstracts were searched as well. 1 November 2023 was the last search date. Papers that had already been published at the time of the search were only included in the analysis.
Overall, 13 cross-sectional studies published through November 2023 were assessed for eligibility but only 6 full text articles were included in the final analysis. In 7 of the excluded studies, dental waste was measured and separated by weight/day or grams/day, rather than by the W/W% ratio. Due to the variability of sampling days, dental structures involved, and lack of raw data in each study, it was not feasible to group and compare the data on W/W% ratios. Considering the heterogeneous nature of the w/w % ratio in these studies, exclusion was decided due to the number of samples, the different units of measurement and the classification of waste. Based on the search strategy, PRISMA-ScR Flow Chart [14] demonstrates the results (Figure 1).
3. Results
3.1. Data Charting Process
Data collection protocols were designed based on forms with 12 variables for each study. Data were obtained from the studies for the following variables: sampling year, study location, number of overall samples, the sector of the health care facility (public, private), number of general dental practice, number of dental clinics with specialties, number of laboratories, amount of infectious and potentially infectious waste, amount of toxic/chemicals/ pharmaceuticals waste, amount of domestic type waste, total dental hazardous waste, total dental solid waste. The selected studies were examined independently.
3.2. Data Items and Synthesis of the Results
Data were collected for each trial as follows: 1) Main author, year of publication and study location, 2) Period of study, 3) Objective/Aim, 4) Details of methodology, 5) Details of primary and secondary outcome, 6) Funding sources, 7) Critical appraisal of individual sources of evidence, 8) Included cross sectional studies using Critical Appraisal Tool were assessed for current scoping review [55]. Data from the included cross-sectional studies are presented in a narrative format in Table 1.
An analysis of qualitative data was conducted on 6 cross-sectional studies out of 13 potentially eligible studies. Of the 6 included studies, 4 were conducted in Iran and 2 in Greece. The descriptive tables of the results of cross-sectional studies were created using StataCorp software. Stata: Release 13 (Table 2).
All studies used longitudinal designs as continuous or repeated measures to follow the rate of generation of dental waste over prolonged periods of time. Sampling days range from 3 to 26. In 3 studies, samples were collected between 31 May and 5 July 2002, 22 April and 5 July 2013 and June to September 2016 respectively. Another 2 studies collected samples for 1 year (April 2011-2012) twice monthly and 4 samples in each season of 2010, respectively. According to one study, samples were taken at a time interval that was not specified. It was calculated that 63, 84, 104, 120, 400, 3816 samples were taken in total respectively in each study. The number of dental care-related structures participating in each survey was 38, 4, 21, 30, 20, 159, respectively too. Nabizadeh et al (2012) collected their data from 28 dental practices in the public sector and 10 dental laboratories [58]. It is important to note that 10 of the 28 dental clinics were involved in general dentistry and 8 were involved in dental specialties. A study was conducted by Komilis, et al. (2009) utilized samples from 4 dental laboratories to compile their study [56]. Koolivand et al. (2012) analyzed waste generation in 30 general and private dental practices [57]. Mandalidis et al. (2019) conducted their investigation into 19 private and 1 public general dentistry practices, while Bazrafshan et al. (2014) included 123 private and 36 public dental practices in their study [59,61]. Finally, Majlesi et al. collected data from 21 general dentistry practices in the public sector [60]. The included research studies aimed to analyze the production rate and composition of dental solid waste. To accomplish this, they collected the waste of the dental care centers under study within the time frame determined by each survey. Following, qualified personnel followed safety and avoidance measures to divide the collected waste into fractions. For each fraction, its composition was categorized into infectious and toxic, toxic/chemicals/pharmaceuticals, and domestic.
3.3. Critical Appraisal within Sources of Evidence
Table 3 presents data on the critical appraisal of the sources of evidence included.
More information on the data derived from each study is presented in detail in Table 4.
Iran was the country with the largest number of included studies (n=4, 66%), followed by Greece (n = 2, 33%). Studies (n=3, 50%) collected their samples daily for a continuous period, whereas other studies (n=2, 33%) collected their samples twice a month during the study year or one sample during each season. There was no information about the specific period of sampling in one study (n=1, 16%). A longitudinal cross-sectional design was chosen by all researchers (n=6, 100%).
Most research groups included in their studies (n=3, 50%) dental facilities in both the private and public sectors, whereas studies (n=2, 33%) collected data only from private dental facilities. A study (n=1, 16%) focused on dental practices in the public sector. In four studies (n=4, 66%), data were collected from dental practices providing general dentistry, two studies (n=2, 33%) collected from dental laboratories, and one study (n=1, 16%) collected from dental practices providing specialty dentistry. In terms of study funding, one (n=1, 16%) study reported no funding, while two (n=2, 33%) studies did not provide information. It has been reported that three (n=3, 50%) studies received funding, with three cases involving university resources. The mean number of days of sampling is 13. The sample size of one study (n=1, 16%) included general dentistry, dental laboratories, and specialty dentistry. Each study's sample size varied. The calculated mean is 764.5 for the number of overall samples. The variation of the values of the overall samples of dental solid waste is included in the range of 764.5± 3000 and is substantial as the min value 63 and max value 3816 are outliers.
The composition of dental solid waste was measured in weight/weight percent in all included studies (n=6). Two studies (n=2, 33%) calculated 21,4% and 26% in the infectious and potentially infectious waste category based on their sample, while 2 studies (n=2, 33%) calculated 80% and 88,5% in the same category. In addition, 2 studies (n=2, 33%) figured intermediate values 48.5% and 64%. A mean of 60,2 w/w% is found in the infectious and toxic categories of dental waste, though there are several outliers. However, the results from studies in the category toxic/chemicals/pharmaceuticals were not as widely varied. toxic/chemicals/pharmaceutical category has a mean of 5,4%, while the variable distribution is 5,4±3,8 %. As a result of the outliers, the distribution of the domestic type of dental waste is wide. According to the data, domestic dental waste has a mean of 39,8 w/w%. Domestic waste and waste with a high potential for infection had the highest percentages in all included studies, while toxic and chemical, pharmaceutical waste had the lowest (Table 5).
4. Limitations of the Studies Included
Due to the lack of a representative sample in the design of the descriptive studies included in this review, the results cannot be generalized and there is no external validity of their findings. Aside from Nabizadeh et al. (2012) and Bazrafshan et al. (2014), none of the other studies mentions the criteria for selecting dental structures or the method for calculating samples [58,59]. Nabizadeh et al. (2012), however, do not indicate when the survey was conducted [58]. Also, it is unclear from Bazrafshan et al. (2014) and Mandalidis et al. (2018) whether the dental clinics selected deal with general dentistry or specializations [59,61]. In addition, all the included studies do not provide any information on the general characteristics of the participating dentists, such as their gender, age, and educational background. Further, the number of dental patients visiting the dental units included in the studies daily as well as the types and/or frequency of dental work performed are not provided in the studies. Moreover, no study provides information on the number of dental units in each dental facility. Additionally, it has not been investigated whether the characteristics of the study population have a confounding effect on the composition of dental solid waste collected from the sample in any of the studies. The samples in studies of Komilis (2009), Majlesi et al. (2016) and Mandalidis et al. (2018) were collected consecutively over a specific period of time [56,60,61]. It may, however, affect patients' natural flow of dental work, the frequency of their dental visits, and the workflow of dental unit employees during certain times of the year. But neither of the above-mentioned studies discussed the criteria for selecting the sampling interval.
Overall, the most significant limitation of the current studies lies in the lack of a representative sample, limiting the generalizability of the findings to the broader population. Furthermore, the criteria for selecting dental structures, the method for calculating samples, and essential information about participating dentists' characteristics were often undisclosed or inadequately addressed [56,57,58,59,60,61]. This limitation necessitates the inclusion of a more diverse and representative sample in future studies to enhance external validity.
5. Proposed Research Model
Considering the difficulties of conducting a dental solid waste collection study, as our data suggest, this scoping review proposes a cross-sectional study design, as described in all included studies. For the purpose of selecting dental practices, it is necessary that they reflect the characteristics of each dental community in the city in which the study will take place. The relevant dental association should be consulted before selecting dental practices that will participate in the study to determine the percentage of general and specialized dentists, the number of working dentists, the level of university education, and general characteristics, such as gender and age. Based on these findings, a determination should be made as to how many dentists with specialties and generalists are required for the study to have external validity. Then, it would be preferable if the sampling intervals were established throughout the dental clinic's opening hours and days with normal patient flow. Subscequently, the classification of the waste samples should then be well defined and waste samples should be seperated into categories. It is imperative that trained staff should segregate waste and that there should be a discrepancy check among the staff members. Overall, there should also be detailed descriptions of the separation method as well as a standardized approach for all participants. Further, precision should be maintained in the use of equipment, such as scales. Finally, to analyze and evaluate the results, it is necessary to consider confounding factors, such as the dentist's age or university education level. We suggest stratifying the findings based on race, age, dental specialty, and level of university education. The model is presented in Table 6.
6. Discussion
The exploration of dental solid waste (DSW) has gathered considerable attention in recent years, reflecting the growing significance of sustainability in healthcare practices. In our scoping review, we delved into six pertinent studies to comprehensively understand the methodology and findings associated with DSW [57,58,59,60,61].
Notably, data on DSW composition exhibited considerable variability among the studies, particularly in categories such as toxics/chemicals/pharmaceuticals, infectious waste, and domestic waste. The observed heterogeneity in data could be attributed to the absence of a standardized method for identifying and categorizing DSW among researchers and participating dentists thus although we used a systematic review approach the present review is considered as a scoping one. This lack of consistency is also described in the relevant literature in other healthcare domains. Considering the methodological deficiencies of published studies as well as the heterogeneity of literature regarding other healthcare domains, such as medical waste and pharmaceutical waste, it is imperative that particular guidelines and regulations be developed for the management of medical waste, as well as technologies, knowledge, and financing to upgrade medical waste management in the world today [62,63].
Despite differences in the methodology, a similar w/w% composition below 10% was found across the 6 included studies in the category of toxics/chemicals/pharmaceuticals. The results of the studies in the categories of infectious waste and potentially infectious waste as well as domestic type waste appeared to be unevenly distributed at the extremes of the range, i.e., 20% and 80%. According to the study conducted by Kizlary et al. (2005) which was excluded due to non-measurement of waste composition in w/w percentage scale, a total of 11.168 kilograms of infectious and potentially infectious waste were produced each day, whereas only 387 kilograms were produced by domestic waste [19]. Conversely, Vieira et al., (2009) which was excluded from our analysis too due to using different classification of medical waste, reported that 24.3%, 48.1%, and 27.6% of waste were non-infectious, infectious, and domestic waste, respectively [25]. Mandalidis' data et al. (2019) indicate that in terms of hazardous waste, unit production rate was 48.7x1.3g/patient/day (mean and standard error) [61]. Thus according to their evaluation, the DSW production rates were 53.3 x 1.4 g/patient/d and 381 x 15 g/practice/d [61] which is a considerable amount of waste to discuss upon.
This heterogeneity of the extracted data from relevant studies discussing the issue, is due to the absence of a repeatable method of identifying dental solid waste among researchers or dentists participating in each study. The difficulty of properly managing wastes is primarily related to separate infectious and potentially infectious waste types. The study by Koolivand et al (2012) concluded that healthcare centers lack effective practices on waste minimization, separation, reuse, and recycling as well as inadequate practices on disposing of sharps, potentially infectious waste, and other hazardous waste [57]. Thus it seems necessary to evolve educational strategies concerning waste seperation issues. As health care workers, dentists and dental auxilliary staff should learn to assess the hazardous and infectious status of dental solid waste, by understanding its possible role in cross-infection and follow specific protocols for waste acumulation and disposal.
According to WHO standards, waste types cover a wide range of materials, including infectious wastes, pathological wastes, sharps wastes, chemical wastes, pharmaceutical wastes, cytotoxic wastes, radioactive wastes, and non-hazardous/general wastes. In accordance with WHO and CE regulations, all healthcare facilities are required to dispose of waste appropriately [2,29,64,65] to diminish the carbon footprint. Studying the carbon footprint in NHS, seventeen dental procedures were identified, emitting 1798.9 tonnes of CO2 equivalent annually. Travel was the largest contributor (45.1%), followed by procurement (35.9%) and building energy (18.3%). Waste disposal accounted for 0.22% of NHS dental services' overall carbon footprint, with 90.3% of emissions derived from domestic waste [5,66]. To achieve the goal of reduced carbon footprint, dental care facilities should curently develop a formal waste management plan. As part of this plan, everyone involved in the generation, handling, and treatment of waste should have access to combined knowledge and decision making. Aside from training and familiarizing dentists and dental staff with the proper disposal of dental waste, raising patient awareness is also an essential step in this direction. By educating patients about the green dental economy and reducing the environmental footprint, dentistry will be able to achieve the fulfillment of sustainability criteria in health care [11,42]. This holistic approach ensures that all stakeholders contribute to minimizing the environmental impact of dental services through less waste and appropriate disposal of it.
Conclusions
Dental solid waste composition and generation rate cannot be determined from the available extracted data due to a lack of evidence and heterogeneity, thus a new research protocol should be followed in future studies. For valid conclusions to be drawn, descriptive studies involving a sufficient number of general, or specialist dental care dentists should be conducted. This scoping review revealed, however, that health care staff and dentistry practitioners could benefit from training on the effective handling of dental waste. By following this approach, it becomes achievable to guarantee that care is delivered while prioritizing environmental considerations.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Studies excluded from the review and reasons for their exclusion. Table S2: Checklist for analytical cross-sectional studies included.
Author Contributions
Conceptualization, I.M. and M.A.; methodology, I.M. and M.A.; software, I.M.; validation, I.M., M.C. and M.A.; formal analysis, I.M.; investigation, I.M., M.C. and M.A.; resources, I.M., M.C. and M.A.; data curation, I.M. and M.A.; writing—original draft preparation, I.M., M.C. and M.A.; writing—review and editing, I.M., M.C. and M.A.; visualization, I.M. and M.A.; supervision, M.A.; project administration, M.A.; funding acquisition, M.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Upon request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Forzieri, G.; Cescatti, A.; Silva, F.B.; Feyen, L. Increasing risk over time of weather-related hazards to the European population: a data-driven prognostic study. The Lancet Planetary Health 2017, 1, 200-208. [CrossRef]
- World Economic Forum. The Global Risks Report 2020, Geneva, 2020. Available online: http://www3.weforum.org/docs/WEF_Global_Risk_Report_2020.pdf. (accessed on 18 November 2023).
- Martin, N.; Sheppard, M.; Gorasia, G.; Arora, P.; Cooper, M.; Mulligan, S. Awareness and barriers to sustainability in dentistry: A scoping review. J Dent, 2021, 112. [CrossRef]
- Duane, B.; Stancliffe, R.; Miller, F.A.; Sherman, J.; Pasdeki-Clewer, E. Sustainability in Dentistry: A Multifaceted Approach Needed. J. Dent. Res 2020, 99, 998–1003. [CrossRef]
- Public Health England. Carbon modelling within dentistry: Towards a sustainable future; July 2018. Available online: https://www.gov.uk/government/publications/carbon-modelling-within-dentistry-towards-a-sustainable-future (accessed on 18 November 2023).
- Martin, N.; Mulligan, S.; Shellard, I.J.; Hatton, P.V. Consensus on Environmentally Sustainable Oral Healthcare: A Joint Stakeholder Statement. White Rose University Press, 2022, 11–36. [CrossRef]
- FDI World Dental Federation. Sustainability in Dentistry Statement. Madrid: FDI; May 2017. Available online: https://www.fdiworlddental.org/sustainability-dentistry-statement (accessed on 18 November 2023).
- ASTM. Standard Practice for Managing Sustainability in Dentistry. ASTM International, ASTM E3014–15; 1 May 2015; ICS 11.060.01. Available online: https://standards.globalspec.com/std/3857932/astm-e3014-15 (accessed on 18 November 2023).
- ASTM. Standard Practice for Managing Sustainability in Dentistry. ASTM International, ASTM E3014–21; 1 September 2021; ICS 11.060.01. Available online: https://standards.globalspec.com/std/14477041/astm-e3014-21 (accessed on 18 November 2023).
- Oviedo-Allison, B.; Shockley, M. The Sustainable Dentist – The New Normal. Dental Medicine Books. York. UK. 2022; ISBN: 978-1-7361051-5-3.
- Antoniadou, M.; Chrysochoou, G.; Tzanetopoulos, R.; Riza, E. Green Dental Environmentalism among Students and Dentists in Greece. Sustainability 2023, 15, 9508. [CrossRef]
- Mazur, M.; Ndokaj, A.; Jedliński, M.; Maruotti, A.; Stamegna, C.; Corridore, D.; Capocci, M.; Ottolenghi, L.; Guerra, F. How Dentistry is impacting the environment. Senses Sci 2019, 6, 922-928. [CrossRef]
- UNFCCC (2015), Paris Agreement. Available online: https://unfccc.int/sites/default/files/english_paris_agreement.pdf. (accessed on 18 November 2023).
- Tricco, AC.; Lillie, E.; Zarin, W.; O'Brien, KK.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, MD.; Horsley, T.; Weeks, L.; Hempel, S. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018, 169, 467-473. [CrossRef]
- Institute of Medicine. Standards for Systematic Reviews. National Academy of Sciences; 2015. Available online: http://www.iom.edu/ Reports/2011/Finding-What-Works-in-Health-Care-Standards-for- Systematic-Reviews/Standards.aspx. (accessed on 18 November 2023).
- Chin, G.; Chong, J.; Kluczewska, A.; Lau, A.; Gorjy, S.; Tennant, M. The environmental effects of dental amalgam. Australian Dental Journal 2000, 45, 246-249. [CrossRef]
- Ozbek, M.; Sanin, FD. A study of the dental solid waste produced in a school of dentistry in Turkey. Waste Manag. 2004, 24, 339-345. [CrossRef]
- Tzoutzas, J.; Panis, V.; Kozirakis, Κ. The disposal of solid dental waste in the Dental School of the University of Athens. Paedodontia 2004, 18, 23–29.
- Kizlary, E.; Iosifidis, N.; Voudrias, E.; Panagiotakopoulos, D. Composition and production rate of dental solid waste in Xanthi, Greece: variability among dentist groups. Waste Manag 2005, 25, 582–591. [CrossRef]
- Nazar, MW.; Pordeus, IA.; Werneck, MA.; Gerenciamento de resíduos sólidos de odontologia em postos de saúde da rede municipal de Belo Horizonte, Brasil [Dental waste management in municipal health clinics in Belo Horizonte, Brazil. Rev Panam Salud Publica 2005, 17, 237-242. [CrossRef]
- Kontogianni, S.; Xirogiannopoulou, A.; Karagiannidis, A. Investigating solid waste production and associated management practices in private dental units. Waste Manag. 2008, 28, 1441–1448. [CrossRef]
- Sudhakar, V.; Chandrashekar, J. Dental health care waste disposal among private dental practices in Bangalore City, India. Int Dent J. 2008, 58, 51-4. [CrossRef]
- Birpinar, ME.; Bilgili, MS.; Erdoğan, T. Medical waste management in Turkey: A case study of Istanbul. Waste Manag. 2009 29, 445-448. [CrossRef]
- Muhamedagic, B.; Muhamedagic, L.; Masic, I. Dental office waste - public health and ecological risk. Mater Sociomed. 2009, 21, 35-38. [CrossRef]
- Vieira, CD.; Carvalho, MA.; Menezes Cussiol, NA.; Alvarez-Leite, ME.; Dos Santos, SG.; da Fonseca Gomes, RM.; Silva, MX.; de Macêdo Farias, L. Composition analysis of dental solid waste in Brazil. Waste Manag 2009, 4, 388-91. [CrossRef]
- Mohamad, I.; Al-Widyan.; Rami, J.; Oweis, Hani Abu-Qdais.; Mutaz, Al-Muhtaseb.; Sa’d, Hamasha. Composition and energy content of dental solid waste. Resources. Conservation and Recycling 2010, 55, 155-160. [CrossRef]
- Sunil Kumar, V.C.; Manjunatha, M.; Badami V.; Pradeep, P.R.; Biomedical waste management: A review J. Oral Health. Comm. Dent. 2012, 6, 141-144.
- Avinash, B.; Avinash, BS..; Shivalinga, BM.; Jyothikiran, S.; Padmini, MN. Going green with eco-friendly dentistry. J Contemp Dent Pract. 2013 1, 766-769. [CrossRef]
- Chartier, Y.; Emmanuel, J.; Pieper, U.; Prüss, A.; Rushbrook, P.; Stringer, R.; Townend, W.; Wilburn, S.; Zghondi, X.; Raki, X. Safe management of waste from healthcare activities. WHO .2nd ed.2014 ISBN 978 92 4 154856 4.
- Rastogi, V.; Sharma, R.; Yadav, L.; Satpute, P.; Sharma, V. Green dentistry, a metamorphosis towards an eco-friendly dentistry: a short communication. J Clin Diagn Res. 2014, 8, 01-2. [CrossRef]
- Al-Qarni, MA.; Shakeela, NV.; Alamri, MA.; Alshaikh, YA. Awareness of Eco-Friendly Dentistry among Dental Faculty and Students of King Khalid University, Saudi Arabia. J Clin Diagn Res. 2016, 10 ,75-78. [CrossRef]
- Richardson, J.; Grose, J.; Manzi, S.; Mills, I.; Moles, DR.; Mukonoweshuro, R.; Nasser, M.; Nichols, A. What's in a bin: A case study of dental clinical waste composition and potential greenhouse gas emission savings. Br Dent J. 2016, 22, 61-66. [CrossRef]
- Mulimani, P. Green dentistry: the art and science of sustainable practice. Br Dent J. 2017,2 3, 954-961. [CrossRef]
- Rathakrishnan, M.; Priyadarhin,i A. Green dentistry: the future. J Int Clin Dent Res Org. 201, 9, 59–61.
- Harford, S.; Duane, B. Sustainable Dentistry: How-to Guide for Dental Practices Sustainable Dentistry How to Guide for Dental Practices Sustainable Dentistry: How-to Guide for Dental Practices, Cent. Sustain. Healthc. (2018). https://sustainablehealthcare.org.uk/dental-guide (accessed on 18 November 2023).
- Phillipson, J. The need for sustainable dentistry. Public Health England. Carbon modelling within dentistry: Towards a sustainable future; BDJ IN PRACTICE, 2018, 31, 17-18.
- Duane, B.; Ramasubbu, D.; Harford, S.; Steinbach, I.; Swan, J.; Croasdale, K.; Stancliffe, R. Environmental sustainability and waste within dental practice. Br Dent J. 2019, 226, 611-618. [CrossRef]
- Hsu, LH.; Hsiao, YH. Facilitating Green Supply Chain in Dental Care through Kansei Healthscape of Positive Emotions. Int J Environ Res Public Health 2019, 16. [CrossRef]
- de Leon, ML. Barriers to environmentally sustainable initiatives in oral health care clinical settings. Can J Dent Hyg. 2020 54, 156-160, PMID: 33240375.
- Duane, B.; Ashley, P.; Saget, S.; Richards, D.; Pasdeki-Clewer, E.; Lyne, A. Incorporating sustainability into assessment of oral health interventions. Br Dent J. 2020 229, 310-314. [CrossRef]
- Subramanian, AK.; Nivethigaa, B.; Srirengalakshmi, M.; Varghese, RM.; Navaneethan, R.; Babu, H. Biomedical waste management practice in dentistry. Bioinformation. 2020, 16, 958-964. [CrossRef]
- Antoniadou, M.; Varzakas, T.; Tzoutzas, I. Circular Economy in Conjunction with Treatment Methodologies in the Biomedical and Dental Waste Sectors. Circ. Econ. Sust 2021, 1, 563–592. [CrossRef]
- Borglin, L.; Pekarski, S.; Saget, S.; Duane, B. The life cycle analysis of a dental examination: Quantifying the environmental burden of an examination in a hypothetical dental practice. Community Dent Oral Epidemiol. 2021, 49, 581-593. [CrossRef]
- Martin, N.; Sheppard, M.; Gorasia, G.; Arora, P.; Cooper, M.; Mulligan, S. Drivers, opportunities and best practice for sustainability in dentistry: A scoping review. J Dent. 2021, 112. [CrossRef]
- Ndokaj, A.; Iacono, R.; Pasqualotto, D.; Stamegna, C.; Capocci, M.; Guerra, F. Trends in Sustainable Dentistry. Clin Ter. 2021, 172, 523-524. [CrossRef]
- Wolf, TG.; Campus, G. Changing Dental Profession-Modern Forms and Challenges in Dental Practice. Int J Environ Res Public Health 2021, 18. [CrossRef]
- Byrne, D.; Saget, S.; Davidson, A.; Haneef, H.; Abdeldaim, T.; Almudahkah, A.; Basquille, N.; Bergin, AM.; Prida, J.; Lyne, A.; Duane, B. Comparing the environmental impact of reusable and disposable dental examination kits: a life cycle assessment approach. Br Dent J. 2022, 233, 317-325. [CrossRef]
- Martin, N.; Mulligan, S.; Fuzesi, P.; Hatton, PV. Quantification of single use plastics waste generated in clinical dental practice and hospital settings. J Dent. 2022, 118. [CrossRef]
- Mazur, M.; Ndokaj, A.; Bietolini, S.; Nisii, V.; Duś-Ilnicka, I.; Ottolenghi, L. Green dentistry: Organic toothpaste formulations. A literature review. Dent Med Probl. 2022, 59, 461-474. [CrossRef]
- Abed, R.; Ashley, P.; Duane, B.; Crotty, J.; Lyne, A. An environmental impact study of inter-dental cleaning aids. J Clin Periodontol. 2023, 50, 2-10. [CrossRef]
- Khanna, R.; Konyukhov, Y.; Maslennikov, N.; Kolesnikov, E.; Burmistrov, I. An Overview of Dental Solid Waste Management and Associated Environmental Impacts: A Materials Perspective. Sustainability 2023, 15. [CrossRef]
- Shinkai, RSA.; Biazevic, MGH.; Michel-Crosato, E.; de Campos, TT. Environmental sustainability related to dental materials and procedures in prosthodontics: A critical review. J Prosthet Dent. 2023, 23. [CrossRef]
- Spaveras, A.; Antoniadou, M. Awareness of Students and Dentists on Sustainability Issues, Safety of Use and Disposal of Dental Amalgam. Dent. J. 2023 ,11,21. [CrossRef]
- Thakar, S.; Kinariwala, N.; Pandya, D.; Parekh, NH.; Patel, NK.; Patel, A. Awareness and Constraints towards the Implementation of Green Dentistry amongst Dental Students and Private Practitioners of West India. J Pharm Bioallied Sci. 2023, 116, 1287-1290. [CrossRef]
- Higgins, JPT.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, MJ.; Welch, VA. Cochrane Handbook for Systematic Reviews of Interventions version 6.4 Cochrane, 2023. Available online: www.training.cochrane.org/handbook. (accessed on 18 November 2023).
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; Mu, P-F.; Chapter 7: Systematic reviews of etiology and risk. In: Aromataris E, Munn Z (Editors). JBI Manual for Evidence Synthesis. JBI, 2020. Available online: https://synthesismanual.jbi.global (accessed on 18 November 2023).
- Komilis, DP.; Voudrias, EA.; Anthoulakis, S..; Iosifidis, N. Composition and production rate of solid waste from dental laboratories in Xanthi, Greece. Waste Manag 2009, 3, 1208-12. [CrossRef]
- Koolivand, A.; Mahvi, AH.; Alipoor, V.; Azizi, K.; Binavapour, M. Investigating composition and production rate of healthcare waste and associated management practices in Bandar Abbass, Iran. Waste Manag Res. 2012, 6, 601-606. [CrossRef]
- Nabizadeh, R.; Koolivand, A.; Jonidi Jafari, A.; Yunesian, M.; Omrani, G. Composition and production rate of dental solid waste and associated management practices in Hamedan, Iran. Waste Manag Res 2012, 30, 619–624. [CrossRef]
- Bazrafshan, E.; Mohammadi, L.; Mostafapour, FK.; Moghaddam, AA. Dental solid waste characterization and management in Iran: a case study of Sistan and Baluchestan Province. Waste Manag Res 2014, 2, 157-164. [CrossRef]
- Majlesi, M.; Alavi, NA.; Mohammadi, AA.; Valipor, S. Data on composition and production rate of dental solid waste and associated management practices in Qaem Shahr, Iran 2016. Data Brief 2018, 19, 1291-1296. [CrossRef]
- Mandalidis, A.; Topalidis, A.; Voudrias, EA.; Iosifidis, N. Composition, production rate and characterization of Greek dental solid waste. Waste Manag 2018, 75, 124-130. [CrossRef]
- Ashtari, A.; Sadegh.; Tabrizi, J.; Rezapour, R.; Rashidian Maleki, M.; Azami-Aghdash, S.; Health Care Waste Management Improvement Interventions Specifications and Results: A Systematic Review and Meta-Analysis. Iran J Public Health 2020, 49, 1611-1621. [CrossRef]
- Benítez-Rico, A.; Pérez-Martínez, A.; Muñóz-López, BI.; Martino-Roaro, L.; Alegría-Baños, JA, Vergara-Castañeda.; A, Islas-García, A. Medical Household Waste as a Potential Environmental Hazard: An Ecological and Epidemiological Approach. Int J Environ Res Public Health 2023, 20. [CrossRef]
- World Health Organization (WHO) (2013) Medical waste. Available online: http://www.who.int/topics/medical_waste/en/ (accessed on 18 November 2023).
- Duane, B.; Hyland, J.; Rowan, JS.; Archibald, B. Taking a bite out of Scotland’s dental carbon emissions in the transition to a low carbon future. Public health 2012, 126, 770–777. [CrossRef]
Figure 1.
Flow chart PRISMA of the study.
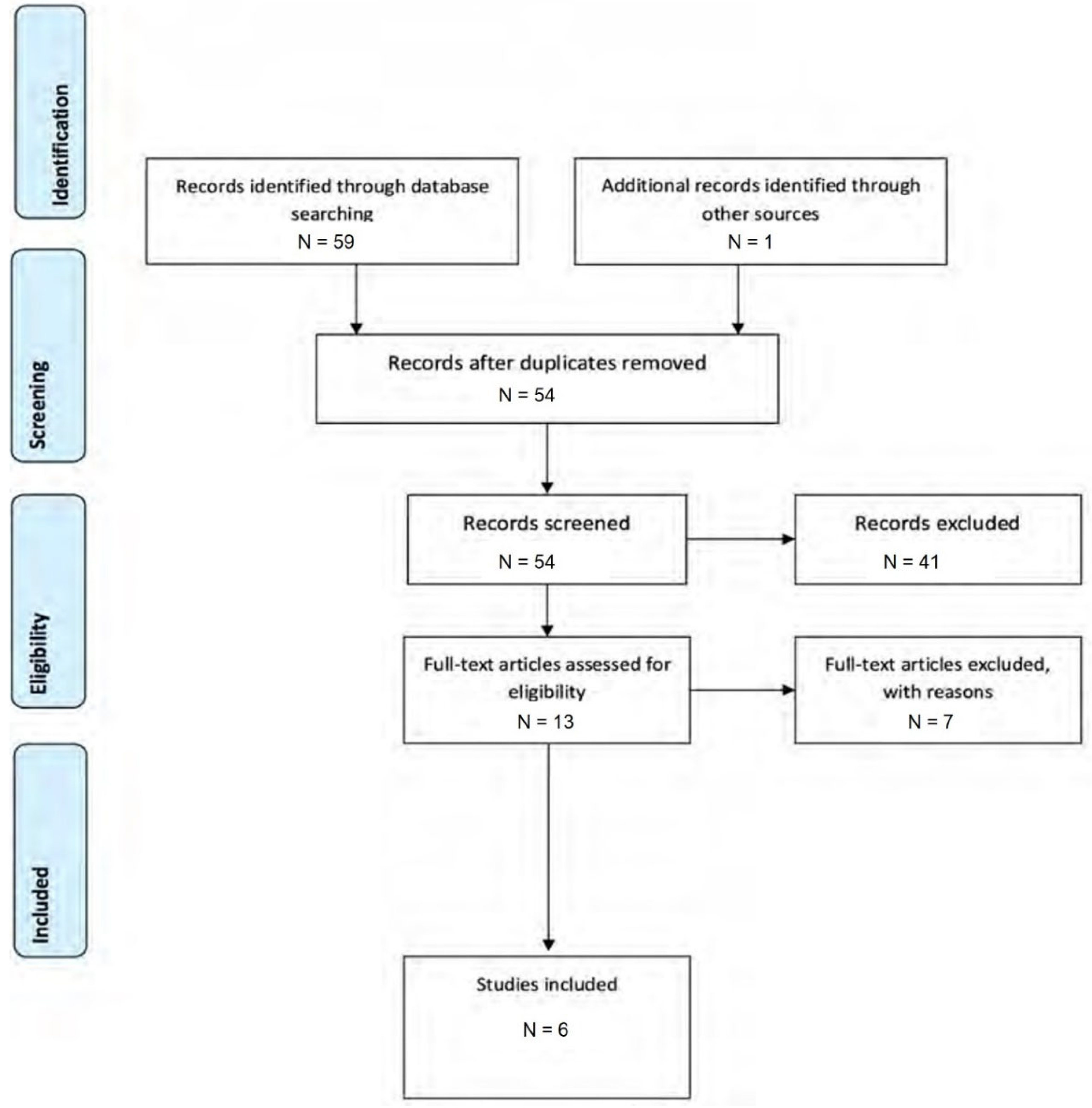

Table 1.
Main characteristics of the studies included in the review.
| Main author (Year) Study location | Period of study | Sector | Objective | Methodology | Results | Funding |
|---|---|---|---|---|---|---|
| Komilis DP. 2009 Greece [56] |
2002 | Private | Analysis of solid waste composition and production rates in dental laboratories. | In Xanthi, Greece, solid waste composition and production rates from four dental laboratories were studied over a two-month period. | During the study, dental laboratories (DLSW) generated 0.059 g of solid waste per capita daily (22 g per capita annually). The waste composition was 74% household-type, 26% infectious, and less than 0.5% toxic. DLSW constituted around 0.007% of Xanthi's municipal solid waste. | No reporting |
| Koolivand A. 2012 Iran [57] |
2010 | Private | Study on healthcare waste composition, production rate, and management practices in Bandar Abbas, southern Iran. | Two random samples were selected from 90 centers, with one sample each in summer and winter. | Average daily waste production rates were 2125.3 grams for clinics, 498.3 grams for dental offices, and 374.9 grams for physician's offices. Domestic and highly infectious waste had the highest percentages, while chemical, pharmaceutical, and sharps waste had the lowest. The survey revealed shortcomings in waste minimization, separation, reuse, and recycling practices in healthcare centers, particularly in managing sharps, potentially infectious, and other hazardous waste. | No funding |
| Nabizadeh R. 2012 Iran [58] |
- | Private & Public | Analysis of dental solid waste composition and production rates in Hamadan, Iran. | Twenty-eight dental clinics were randomly selected, including ten general dentists, eight specialists, five practical dentists, and five denture makers. | Dental offices generate 41,947.43 kg of annual waste, comprising 71.15 tons of domestic waste, 21.40 tons of potentially infectious waste, and 7.26 tons of chemical and pharmaceutical waste, with toxic waste at 0.18%. The majority (80%) includes gypsum, latex gloves, nylon, dental impression material, used medicine ampoules, saliva-contaminated paper towels, and saliva ejectors. | Department of Environmental Health Engineering |
| Bazrafshan E. 2014 Iran [59] |
April 2011–2012 | Private & Public | Evaluation of the hazardous and infectious status of dental solid waste. |
Measured the composition and generation rate of dental solid waste in 123 private and 36 public dental clinics in the Sistan and Baluchestan Province. |
The dental solid waste was categorized into domestic type (11.7%), potentially infectious (80.3%), chemical and pharmaceutical (6.3%), and toxic (1.7%). Daily generation rates per patient for total, domestic-type, potentially infectious, chemical and pharmaceutical, and toxic wastes were 169.9, 8.6, 153.3, 11.2, and 3.3 g/patient, respectively. The daily generation rates for total, domestic-type, potentially infectious, chemical and pharmaceutical, and toxic wastes were 194.5, 22.6, 156.1, 12.3, and 3.4 kilograms. The study recommends implementing source reduction, separation, reuse, and recycling programs for effective dental waste management, emphasizing separate collection and disposal for each type in accordance with relevant criteria. | Health Research Deputy of Zahedan University of Medical Sciences |
| Majlesi M. 2016 Iran [60] | June to September 2016 | Public | Assessment of the composition and production rate of solid waste generated by dental offices. | From June to September 2016, 21 dental offices in Qaem Shar were randomly chosen as sampling sites. These offices were sampled three times each week (on Sunday, Monday, and Tuesday) at the end of the day. | Dental clinics are the main sources of biohazardous and potentially infectious wastes. Critical need for proper management and safe disposal of biohazard wastes to protect public health and the environment. Absence of initiatives in these clinics for waste reduction, segregation, and recycling. Urgency of implementing practices for reducing waste, promoting recycling, and enhancing overall management of dental solid waste. | Shahid Bheshti University of Medical Sciences |
| Mandalidis A. 2018 Greece [61] |
22 April to 5 July 2013 | Private & Public | Evaluation of the composition and production rate of solid waste generated by dental facilities in Greece. | Over a four-week period, dental practices in Xanthi, Greece collected, manually separated, and weighed dental solid waste (DSW). | Dental solid waste (DSW) consisted of 92% hazardous waste and 8% domestic waste. The hazardous waste unit production rate averaged 48.7 ± 1.3 g/patient/day. DSW production rates were 53.3 ± 1.4 g/patient/day and 381 ± 15 g/practice/day. Multiple measurements, including bulk density, calorific value, moisture, ash, and volatile solids, were recorded. | No reporting |
Table 2.
Descriptive tables of the results of cross-sectional studies.
| Location | Freq. | Percent | Cum. |
|---|---|---|---|
| Iran | 4 | 66.67 | 66.67 |
| Greece | 2 | 33.33 | 100.00 |
| Total | 6 | 100.00 | - |
| Sector | Freq. | Percent | Cum. |
| Private sector | 2 | 33.33 | 33.33 |
| Public sector | 1 | 16.67 | 50.00 |
| Both | 3 | 50.00 | 100.00 |
| Total | 6 | 100.00 | - |
| Funding | Freq. | Percent | Cum. |
| NO | 1 | 16.67 | 16.67 |
| YES | 3 | 50.00 | 66.67 |
| NO REPORTING | 2 | 33.33 | 100.00 |
| Total | 6 | 100.00 | - |
Table 3.
Data on the critical appraisal of the source of evidence included.
| Main author(Year) | Sampling year | Study location | N. overall sample | Private sector-0, public-1, both-2 | Private sector | Public sector | N. general dental practice | N. dental clinics special | N. laboratoires | Infectious and potentially infectious waste | Toxic/chemicals/ pharmaceuticals | Domestic type | Total dental hazardous waste | Total dental solid waste |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Komilis 2009 [56] | 31 May to 5 July 2002 | Greece | 104 | 0 | 4 | . | . | . | 4 | 26 | 0.47 | 74 | 26.47 | 100 |
| Koolivand 2012 [57] | 2 samples in summer and 2 samples in winter 2010 | Iran | 120 | 0 | 30 | . | 30 | . | . | 48.5 | 10.7 | 40.9 | 59.2 | 100 |
| Nabizadeh 2012 [58] | . | Iran | 84 | 2 | . | 28 | 10 | 8 | 10 | 21.40 | 7.44 | 71.15 | 28.84 | 100 |
| Bazrafshan 2014 [59] |
For 1 year (April 2011–2012) twice monthly | Iran | 3816 | 2 | 123 | 36 | . | . | . | 80 | 8 | 11.7 | 88 | 100 |
| Majlesi 2016 [60] | June to September 2016 | Iran | 63 | 1 | . | 21 | 21 | . | . | 64.09 | 2.7 | 33.2 | 66.79 | 100 |
| Mandalidis 2018 [61] | From 22 April to 5 July 2013 | Greece | 400 | 2 | 19 | 1 | 20 | . | . | 88.5 | 3.5 | 8.0 | 92 | 100 |
Table 4.
Individual sources of evidence from studies included.
| Main author (Year) |
Inclusion criteria | Study subjects and the setting described in detail | Exposure measured in a valid and reliable way | Objective, standard criteria used for measurement of the condition | Confounding factors identified | Strategies to deal with confounding factors stated | Outcomes measured in a valid and reliable way | Appropriate statistical analysis |
|---|---|---|---|---|---|---|---|---|
| Komilis DP. 2009 [56] | YES | YES | YES | UNCLEAR | NO | NOT APPLICABLE | YES | YES |
| Koolivand 2012 [57] | YES | YES | YES | UNCLEAR | NO | NOT APPLICABLE | YES | YES |
| Nabizadeh 2012 [58] | UNCLEAR | YES | YES | UNCLEAR | NO | NOT APPLICABLE | YES | YES |
| Bazrafshan 2014 [59] |
YES | YES | YES | UNCLEAR | NO | NOT APPLICABLE | YES | YES |
| Majlesi 2016 [60] | YES | YES | YES | UNCLEAR | NO | NOT APPLICABLE | YES | YES |
| Mandalidis 2018 [61] | YES | YES | YES | UNCLEAR | NO | NOT APPLICABLE | YES | YES |
Table 5.
Dental solid waste measurements in the studies included.
| Variable | Obs | Mean | SD | Min | Max |
|---|---|---|---|---|---|
| N. overall samples | 6 | 764.5 | 1500.089 | 63 | 3816 |
| N. of general dental practices | 4 | 20.25 | 8.180261 | 10 | 30 |
| Infectious type of waste | 6 | 54.74833 | 27.71898 | 21.4 | 88.5 |
| Toxic type of waste | 6 | 5.468333 | 3.851973 | .47 | 10.7 |
| Domestic type of waste | 6 | 39.825 | 28.27748 | 8 | 74 |
| Days of sampling | 6 | 13.33333 | 11.12954 | 3 | 26 |
Table 6.
Recommendations for future studies’methodological aspects.
| Aspect | Recommendation |
|---|---|
| Study design and sampling | A cross-sectional study with a sampling strategy reflecting the characteristics of each dental community. Collaboration with dental associations for representative samples. |
| Waste categorization and identification | Establishment of clear definitions and classification criteria for infectious waste, toxic/chemicals/pharmaceuticals, and domestic waste. Implementation of a meticulous waste categorization system. |
| Methodological standardization | Use of a standardized approach to waste separation and measurement. Clear definition of methodological details, including equipment calibration and measurement precision |
| Consideration of confounding factors | Stratification of findings based on potential con-founding factors such as age, gender, and educational background of dentists for a nuanced analysis |
| Training and awareness programs | Inclusion of training and awareness programs for dental practitioners focusing on waste minimization, separation, reuse, and recycling practices. |
| Environmental impact assessment | Integration of a comprehensive environmental impact assessment, including the evaluation of the carbon footprint of dental services in conjunction with waste production and exploration of sustainable practices |
| Patient education initiatives | Exploration of the effectiveness of patient education initiatives to engage patients in understanding the environmental impact of dental practices and waste production and encourage sustainable behaviors. |
| Longitudinal studies for temporal trends | Conduction of longitudinal studies extending over several years to capture temporal trends and variations in waste generation. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



