
Submitted:
25 January 2024
Posted:
25 January 2024
You are already at the latest version
Abstract
This study aimed to assess the enhancement of physical fitness and quality of life through an 8 weeks strength program training in male adolescents soccer players. A lower body muscle groups intervention was performed, with 17 players in the experimental group (EG) and 15 in the control group (CG). The EG carried out soccer training complemented by specific strength work. Pre and post- intervention assessments included body composition, jump height, speed with change of direction, maximum speed in 20 m, movement velocity in back-squat, perceived fatigue effort, academic performance and quality of life. A general linear repeated measures model analysis was used considering for each variable, the interaction between groups (CG, EG) and time (basal, final), to analyze the differences between and within groups. The results showed reduction of fat in the upper limbs and trunk EG, improvements in jump height, maximum speed of 20 m, changes of direction and quality of life increased (p<0.05) in the EG too. It was concluded that a strength program could improve some components of physical performance in male adolescents soccer players.
Keywords:
adolescentes varones
; fútbol
; ejercicio
; educación Física.
; movement velocity
1. Introduction
Strength training is understood as the physical conditioning method that seeks to improve a person’s ability to overcome a muscle resistance [1].
For a long period of time, it was recommended that children and teenagers should not perform strength work as it was believed to increase the danger of injury or affect their growth negatively [2]. In addition, uncertainty about the effectiveness of strength training at early ages was propagated, arguing that it was not effective [3,4].
However, nowadays there is now a broad international consensus advocating youth intervention in properly screened strength training, endorsed by the American Pediatric Association, among others, related to health and training [5]. Additionally, several studies demonstrate the safety and efficacy of these trainings in promoting the health and performance of participants [6] and highlight the importance of strength development for its positive effects in numerous aspects [2].
In this way, children and adolescents participating in mass collective sports such as soccer may employ strength training as it offers improvements in their physical performance [7]. Therefore, muscle power can be improved by strength training [8,9]; being a key physical capacity, to perfect performance in soccer [10].
In recent years, there has been an increase in the number of young people participating in strength training programs while doing sport [11]; and more and more studies are showing that a correct design and implementation of training containing specific strength exercises can offer benefits in health and in the development of conditional and coordinative abilities that improve physical performance [12]. In addition, the earlier the practice is started, the greater the improvements in the motor system and the more adherence will be created in the future, making possible a better preparation for future physical activities. In terms of general benefits, three groups stand out: benefits at the musculoskeletal level, benefits in overweight or obese patients and psychosocial benefits [1].
Despite the concerns about strength training in adolescence mentioned above, there is evidence that this type of work provides benefits that go beyond sports performance; favoring the growth, maturation and health of the participant. Also, favorable aspects are analyzed in body composition, bone system, cardiovascular functioning [2]; and in academic performance, observing better functioning of the cognitive and sensory aspects of the brain [13] and a better quality of life (QoL) [14].
According to global recommendations, children and adolescents aged 5-17 years should incorporate vigorous-intensity aerobic activities, as well as those that strengthen muscle and bone, at least 3 days a week [15]. For this purpose, a structured work system is elaborated with specific activities to develop this capacity; taking into account the psychological, physiological and sociological factors of the participant [16]. When an ability is trainable, it means that it has the possibility of improvement by responding to training stimuli. In relation to strength, improvement not only depends on the conditions of the load used, but the characteristics of the participants are also involved [2].
On other hand, soccer sports practice is intermittent [17], and is characterized by the repetition of high intensity acyclic actions [18], such as accelerations, jumps, changes of direction and sprints; therefore, there is a complementarity between strength training and soccer-specific training, which can lead to better results compared to the soccer-only approach. Strength training can enhance a player’s ability to perform explosive movements and prolong his or her performance on the field [19].
There are few studies that focus on the development of these training modalities in adolescents soccer players. As the scientific literature in this area is limited [20], widespread application in soccer is difficult [8]. The lack of clear and concise information on proper dosing of load volume and intensity may be a contributing factor. In this sense this study aimed to assess the enhancement of physical fitness and quality of life through an 8 weeks strength targeted specific program training in male adolescents soccer players aged 12 and 13 years.
2. Materials and Methods
2.1. Intervention Design
An 8-week strength targeted specific pre-post study was conducted in physically active male participants aged 12 to 13 years. These participants contributed 3 times a week to soccer training sessions and, in addition, were familiarized with basic strength training exercises. There were two groups: an experimental group (EG), which was the players of the Peloteros de la Sierra Sur Sports Club (Seville, Spain), and a control group (CG), which was the soccers´ category of the Gilena Football Club (Seville, Spain). The intervention of the EG took place at the training center of the club. Data on the anamnesis and physical examination (injuries) of participants were reported by the participating clubs to the researchers.
At the beginning and at the end of the study, participants were assessed for body composition, countermovement jumping, back squats at 75% of their RM, speed in the 4 x 10 meter test, speed in the 20 meter sprint test and perceived effort according to the Borg scale. In addition, academic performance and quality of life with health were measured by two questionnaires. These variables were taken from EG and CG (Figure 1).
The CONSORT Statement was taken into account for the design of this study.
2.2. Participants.
The participation in this was voluntary and it was possible for them to resign at any time. In addition, an informed consent form was signed by both their legal guardians and the sports management of both clubs. The participants recruited were briefed on the protocol and purpose of the study and all signed a written consent prior to the start of the research. The study was conducted in accordance with the Declaration of Helsinki (52nd General Assembly Edinburgh, Scotland, October 2000).
2.2.1. Sample Collection Criteria
For the selection of the sample, inclusion and exclusion criteria were used to ensure that all participants had equal conditions. In the case of the inclusion criteria, the following were required: I. Be between 12 and 13 years of age at the initial measurement; II. Have been training in soccer for more than one year; III. Possess some familiarity with basic strength training exercises; IV. Lack musculoskeletal injuries that could interfere with the exercise program to be carried out during the research. As for the exclusion criteria, the following were highlighted: I. Failure to attend more than two strength training sessions. II. Having any medical conditions that would contraindicate the practice of physical exercise. Finally, it should be noted that all players have their respective medical examinations, which are performed annually by their clubs.
2.3. Intervention
The intervention was carried out in the EG, who performed soccer training complemented with strength training; while a CG who did not perform the intervention program, but did perform the soccer training, participated in the intervention. This strength intervention lasted 8 weeks. The strength training program consisted of 16 training sessions, carried out with a frequency of 2 sessions per week. This training consisted of 5 exercises, targeting 5 different specific muscle groups of the lower body: calf muscles, quadriceps, hamstrings, abductors and adductors. Three sets of 12 repetitions each were performed, with a recovery between sets of 2 minutes and a medium movement velocity.
The strength program was of a continuous nature, it was supervised through a direct observation by a specialist technician and was performed before each soccer training session. It is important to highlight that in the exercises mentioned below, a light load was included whenever necessary, this increasing the stimulus. The exercises performed were: squats with jumping; frontal lunges; lateral lunges; unilateral dead weight; ballerinas. The specific soccer training was carried out 3 days a week, with a duration of 120 minutes per day. All training sessions were held in the afternoon, always complying with the established schedule. The soccer training was based on technical-tactical aspects and was the same in both teams; in addition, both the EG and the CG had the same training frequency. The volume of soccer-specific work was similar in both groups, with exercises focused on pressure after loss, progression, ball circulation, field occupation, among others.
The external load used by some participants was calculated and added according to their RM [21]. This load was established according to the familiarity with strength training and high sports performance shown to their coaches in soccer; in addition, we had the help of the club, who have previous records of those participants who require greater stimulation thanks to interventions carried out previously. Finally, questionnaires were completed thanks to the participants’ family members who provided information on academic results [22]; while the participants reflected on the frequency with which they performed certain actions related to QoL and health [23].
2.4. Variables
Body composition with bioimpedance.
Anthropometric measurements and body composition of all participants were recorded during their first and last visits. Bioelectrical impedance (Tanita MC-780MA; Tanita Corporation, Tokyo, Japan) was measured to report body composition, with special emphasis on body fat percentage and body mass index (BMI). The measurement was performed according to the protocol of The International Society for the Advancement of Kinanthropometry (ISAK). Height was measured using a stadiometer (Seca 214 portable stadiometer; Seca, Hamburg Germany). The participant stood barefoot, upright, and facing the horizon.
Muscular power in countermovement jumping (CMJ).
A warm-up consisting of three CMJs at a moderate intensity (60-70% of perceived maximum performance) was performed. Subsequently, with two minutes rest between them, the participants were instructed to start with an initial upright position, descend by bending their knees at a 90° angle, keeping their hands on their hips with the trunk upright, taking care not to interrupt the movement from the beginning of the jump to the end. Three CMJ were performed, with a recovery period of 45 s between jumps, observed by an evaluator who stood at a distance of 1.5 m in the frontal plane to control the correct execution of the jump and record the maximum height (cm) reached in the three attempts [24]. The height reached was recorded using an infrared measurement sensor (ADR Jumping, Ciudad Real, Spain).
Movement velocity and power in back-squats at 75%.
In order to guarantee the participant’s maximum performance while eliminating possible muscle fatigue, it is important to note that all back-squats were performed the day after the rest of the tests. For the warm-up, back-squats were performed with a free barbell weighing 15 kg. Subsequently, the load was increased based on their RM. To achieve this, the maximum explosive speed was used for a total of 3 repetitions. Their technique was assessed, and corrections were made when necessary. To ensure that the technique was considered satisfactory, participants stood with their feet shoulder-width apart and the bar resting on their shoulder blades, while their hands gripped the bar. Afterward, they flexed their knees to 90 degrees, and subsequently, they performed the extension back to the original standing position [25]. The primary load for all participants was 15 kg and was gradually increased by 2.5 kg until an average velocity of 0.86 m/s was reached. Subsequently, the load was adjusted in smaller increments (1.25 kg) for each participant, so as to calculate 75% 1 RM accurately, when the velocity reached 0.76 m/s. To ensure safe weight lifting, there were well-trained volunteers on both sides of the bar. The rest between sets was 3 minutes. Only the fastest average speed repetition was considered for the analysis. The velocity was controlled by a linear position transducer (encoder) (Speed4Lift v.4.1, Speed4Lift, Madrid, Spain) [26].
Back-squats to failure at 75%.
After 20 minutes of active rest, 3 repetitions with free bar (15 kg) were performed for a new warm-up. Subsequently, the weight set the previous day for each participant was set at 75%; with this weight the participants performed the maximum number of back-squats possible. It is important to note that there were qualified technicians intervening and assisting in the performance of this test, to ensure the safety of the adolescents at all times. This test was performed twice, with a 5-minute rest per participant. The highest number of repetitions that each participant was able to perform was recorded.
4 x 10 meters test.
They performed a brief dynamic warm-up for 5 minutes, in order to favor their flexibility and avoid injuries. The warm-up consisted of continuous running, stretching, joint mobility exercises and multiple displacements, varying the intensity. Next, the test extracted from the ALPHA-Fitness battery [27] and used in a study [28]. Two parallel lines were established at a distance of 10 meters. In this line 5 marks were highlighted: a) start mark; b) first sponge mark; c) second sponge mark; d) third sponge mark and e) finish mark. The objective of this test focuses on moving through the 5 marks at maximum speed and in the correctly established order. The sponge at mark b should end at mark c; the sponge at mark c should end at mark d and the sponge at mark d should end at the finish mark. The measurement was made with a stopwatch (seconds), two measurements were made and the best result was recorded. The maximum speed when running and turning in a delimited area was recorded, it could be done twice. The best repetition was selected for further analysis.
20 meters sprint test.
After 15 minutes of active rest, the test was performed to measure the reaction speed and acceleration they possess over 20 meters [2]. The participant waited for the start sample, after that, he/she ran at maximum speed up to the established mark at a total distance of 20 meters. To perform this test, it is required to delimit the starting line and the final line of 20 meters. The measurement was made with a stopwatch (seconds), two measurements were taken and the best result was recorded. The maximum reaction and acceleration speed over a distance of 20 meters was recorded. Participant’s perceived fatigue effort during the assessment.
Perceived effort.
At the end of each evaluation the participants’ perception of effort was measured by the Borg scale, offering a score from 1 to 10. In addition, the perceived effort after each workout performed was also evaluated [29].
Academic results.
We analyzed whether the practice of collective sports complemented with strength training improved academic results, by means of an ad hoc questionnaire completed by the parents of the participants when they were minors. In addition, the grades of the first trimester and those of the second trimester were assessed to analyze whether after sports practice the academic results were modified, based on the instrument used in a scientific article [30]. The mentioned questionnaire is similar to the one used in a scientific article where each subject is valued with insufficient, sufficient, good, notable and outstanding [31].
Health-related quality of life.
The health-related QoL of the participants was assessed by means of a questionnaire: Kiddo-Kindl [32], before and after the intervention. The reliability index was .87 with a factorial structure of six dimensions: emotional well-being, self-esteem, school welfare and interest, fun with peers, family well-being and physical well-being; as conducted in a study, where the validity and reliability of the instrument was guaranteed worldwide and cross-culturally as it was suitable for measuring QoL [14]. This questionnaire was completed by the participants, at home, under the supervision of their legal guardian, with the aim of analyzing whether sports practice with a strength intervention favors the participants’ QoL.
2.5. Sample Size
As the RM on strength exercise was one of the main outcomes for this study, the sample size was determined by calculating the statistical power based on a previous study [2] with a power of 0.80 and a two-tailed α level set to 0.05; the minimum number of participants required to detect a 10% difference in RM was estimated as 32.
2.6. Statistical Analysis
SPSS 29 software was used to examine the data, obtaining descriptive statistics such as the mean and standard deviation of each variable investigated. Reliability was assessed by intraclass correlation coefficients and coefficients of variation. The homogeneity of variance of the EG and CG groups was examined using Levene’s test, and the normality of the data was assessed using the Shapiro-Wilk test. A general linear repeated measures model analysis was used considering for each variable [33]; the interaction between groups (CG, EG) and time (Basal, Final), to analyze the differences between groups and within groups. Repeated measures test effect size was calculated using partial eta squared (η2p), with small considered below 0.25, medium as 0.26-0.63 and large above 0.63). Statistical significance was set at p 0.05 for all inference tests [34].
3. Results
A total of 32 physically active children were recruited. All participants completed the trial (Figure 2).
The characteristics and body composition of the participants at baseline and the 8-week visit (both EG and CG) are shown in Table 1.
Although there was an increase in height due to growth, there were not improvements in weight, percentage, of fat and BMI in the time*group interaction, neither in the EG nor in the CG. However, a reduction in the percentage of fat in the upper extremities and trunk was observed in the EG. As for the lower extremities, no improvements were observed in any group, neither during the time elapsed between baseline and final measurements (Table 1).
The EG obtained improvements in the CMJ after the period of time between the baseline and the final measurement. The intervention seemed to have had an effect since improvements were observed in the time*group interaction (Table 2).
The RM in back-squats, the MV and MP in back-squats at 75% of RM and back-squats to failure, improvements were examined between baseline and end of the intervention program in both groups (Table 2).
The 4 x 10-meter test and the 20-meter sprint test showed improvements after the strength intervention as shown in Table 2.
The 4 x 10-meter test showed improvements in both teams after the time period between the baseline and the final measurement; thus, the intervention caused a significant effect as improvements were shown in the time*group interaction (Table 2).
The 20-meter sprint test showed improvements between baseline and final time only in the EG; however, the CG did not obtain relevant improvements. However, the intervention had a significant effect since improvements were observed in the time*group interaction (Table 2).
In perceived fatigue effort, measured by the Borg scale, was reported effect for time (p = 0.002; η2p = 0.521), but neither was reported any effect for group (p = 0.847; η2p = 0.003) nor time*group (p = 0.922; η2p = 0.001).
In the academic results, improvements were observed for time (p = 0.006; η2p = 0.428) and for group (p = 0.020; η2p = 0.328); however, no improvements were found in the interaction time*group (p = 0.540; η2p = 0.027).
Health-related QoL, in general, showed improvements in both groups between baseline and final measurements; in addition, the intervention had a significant effect as improvements were observed in the time*group interaction (Table 3).
It was observed that self-esteem obtained improvements between the baseline and the final measurement in the EG; even, improvements were observed in the time*group interaction, so the strength intervention caused a significant effect (Table 3).
While emotional and school well-being only obtained improvements in relation to baseline and final time in both groups (Table 3).
4. Discussion
The aim of this study was to assess the enhancement of physical fitness and quality of life through an 8 weeks strength program training comparing two groups of Spanish male adolescents soccer players aged 12 and 13 years. The main findings shows that the EG experimented fat reduction in their upper extremities and trunk, improvements in the fitness variables CMJ, the 4x10-meter test, the 20-meter sprint test as well as, in health-related QoL.
A well-designed strength-training program can be considered as a safe strategy to improve this physical quality of participants [35]. The main findings of the study suggest that the practice of soccer supplemented with a strength training program for 8 weeks with a frequency of 2 days per week and a volume of 5 exercises with 3 sets, each of 12 repetitions and a rest of 2 minutes; produces improvements in the sports performance and physical fitness of adolescents soccer players.
Several studies [36,37,38,39], affirm that strength training in soccer players is likely to be adequate to achieve interesting results on strength in their sports performance [40].
In our study it could be observed that a frequency of 2 days per week of strength training could be sufficient to introduce adolescents’ players to strength development. In this sense, these results could be translational because the study was done in compulsory schooling individuals who have along the academic year physical education classes with a frequency of two sessions per week.
Similarly, other studies use the same frequency with a similar prototype population, achieving improvements on this physical capacity [2,41,42]. On the contrary, reducing the work to one week would minimize the effect of the program on strength gain [37].
In our study, although no influences on BMI were found, there were improvements about fat reduction in upper extremities and trunk of the EG. Following this line, a review [43] reported positive changes in body composition without improvements in BMI. Puberty is a stage of continuous physiological changes and growing up, that have an impact on the development of physical abilities [44]. In relation to the EG improvement of physical condition in the trunk and upper extremities, we believe that they were due to the duration of the program, since it complies with 8 weeks, a period stipulated to obtain improvements according to several studies [36,37,39]. Therefore, the improvements obtained in our participants could be due to the effect of the strength training program and not only to physiological reasons related to their growth; with the exception of age. In this sense the longer and quicker growth of legs compared to legs could explain why we found differences in fat reduction only in the upper adolescents’ extremities. Furthermore, during the strength program, the EG participants included external loads that favored the upper body, since they involved an external stimulus to which their bodies were not accustomed. However, the lower train of the participants did not obtain improvements in fat reduction, and this could also be due to the continuous development of these extremities in sports such as soccer, which implies much more delayed effects in the lower train than in the upper train [45].
One interesting aspect is the improvement in the CMJ variable, because of the desirable jumping ability in some actions of soccer players like “head a ball” or to the goalkeeper functions. In our study it was possible to verify the improvement obtained in the CMJ variable, through the strength-training program in adolescents soccer players, who increased their jump height and, therefore, their flight time. This same conclusion was obtained in a similar study with a similar sample, where a strength and plyometric training program was proposed [46].
About other physical fitness qualities, the progress of several skills in collective sports such as soccer can be influenced by a properly developed physical quality [47]. Running speed, reaction speed, agility and changes of direction are characteristics of the sport in question and some studies with similar samples claim a transfer from strength training to speed over 30 meters [19,48]. Similarly, the results of our study showed a beneficial correspondence between strength development and running time in tests such as the 20-meter sprint test and the 4 x 10-meter test [49].
The competitive period in which the participants found themselves, is characterized by a high technical-tactical training load, issue that could affect sports performance in variables such as back-squats. In addition, knee flexion angle and execution technique could have influenced the results, as no significant interaction was observed after the intervention [50].
No improvements were observed in the perception of effort after the intervention, which could be related to external factors not considered in this study (like the puberty hormonal release) that could affect this variable. In addition, it would be possible that there was a relationship between emotional state, cognitive perceptions, and physical state, which influenced the subjective perception of the individual effort [51].
Regarding academic performance, it is important to note that the EG already had a high academic average, so further increasing their performance is a complicated aspect. Although the practice of physical activity is related to obtaining good academic results [52], we do not have evidence to affirm that strength training did not seem to increase academic performance in our study.
Finally, QoL (overall and self-esteem) is one of the variables that presented improvements after the practice of soccer and strength training in our study. We want to highlight the intervention by the World Health Organization who affirm our results, since they defend that physical activity improves mood and decreases the risk of suffering from stress, anxiety and depression; increasing self-esteem and providing greater well-being psychological well-being. Nowadays emotional in sports aspects are getting more and more relevancy. The improvement in the EG Overall and self-steem QoL punctuation, shows that this strength-program would be good to enhance it.
The main limitation is that it is a not random sample. On the contrary we think that the study has the strength of constitute a practical and feasible intervention that could be translocate to the academic and competitive sectors.
5. Conclusions
We conclude that a strength program could improve some components of physical performance in male adolescents soccer players, like jump height, maximum speed of 20 m, and changes of direction; reducing the fat in uppers limbs and trunk, as well as an increment in the overall and self-steem QoL.
These findings may have practical applicability in sports performance and the physical conditions involved in competitive soccer practice. The improvement of the variables studied, especially those related to the power of the lower body, has a direct transfer in the aerial game of both the field players and the goalkeeper in the practice of soccer.
Author Contributions
Conceptualization, S.D.H. and J.M.J.C.; methodology, S.D.H. and J.M.J.C.; software, S.D.H., A.R.S. and J.M.J.C.; validation, A.R.S. and J.M.J.C; formal analysis, S.D.H. and J.M.J.C.; investigation, S.D.H. and J.M.J.C.; resources, S.D.H., A.R.S. and J.M.J.C.; data curation, S.D.H., A.R.S. and J.M.J.C.; writing—original draft preparation, S.D.H. and J.M.J.C.; writing—review and editing, S.D.H., A.R.S. and J.M.J.C.; visualization, S.D.H., A.R.S. and J.M.J.C.; supervision, A.R.S. and J.M.J.C.; project administration, J.M.J.C.; funding acquisition, A.R.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
The project protocol was approved by the ethics committee of the University of Sevilla (reference 0291-N-23).
Data Availability Statement
Not applicable.
Acknowledgments
In particular, thanks to my family for always supporting me, for helping me in the recording of results and for offering me the necessary resources to fulfill my objectives. Next, thanks to my tutor for guiding me through this new experience and helping me in all the necessary tasks. On the other hand, I would like to thank all the children and parents who have collaborated in this study for their interest, without them it would not have been possible. Last but not least, I would like to thank both clubs: Peloteros de la Sierra Sur Sports Club and Gilena Football Club; without forgetting their respective coaches, José Manuel Pozo and Jesús Carmona.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Comité Nacional de Medicina del Deporte Infantojuvenil. Entrenamiento de la fuerza en niños y adolescentes: beneficios, riesgos y recomendaciones. Arch Argent Pediatr. 2018, 116, S82–S91. [Google Scholar] [CrossRef]
- Sánchez-Sánchez, J.; Pérez, S.; Yagüe, J. M.; Royo, J. M.; Martín, J. L. Implementation of a resistence training on young football players. Revista Internacional de Medicina y Ciencias de la Actividad Fisica y del Deporte 2015, 15, 45–59. [Google Scholar] [CrossRef]
- Durán-Jácome, J. F.; Torres-Palchisaca, Z. Práctica de la halterofilia a edades tempranas. Consecuencias en el crecimiento. Revista Arbitrada Interdisciplinaria Koinonía 2021, 6, 187–205. [Google Scholar] [CrossRef]
- Falk, B.; Tenenbaum, G. The effectiveness of resistance training in children. A meta-analysis. Sports Medicine 1996, 22, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Yépez-Ormaza, P.; García-Herrera, D.; Cárdenas-Cordero, N.; Erazo Álvarez, J. Plataformas digitales: Mundo primario como estrategia para el desarrollo del lenguaje en niños. Revista Arbitrada Interdisciplinaria Koinonía 2020, 5, 358–376. [Google Scholar] [CrossRef]
- Peña, G.; Heredia, J. R.; Lloret, C.; Martín, M.; Da Silva-Grigoletto, M. E. Iniciación al entrenamiento de fuerza en edades tempranas: revisión. Revista Andaluza de Medicina del Deporte 2016, 9, 41–49. [Google Scholar] [CrossRef]
- Lesinski, M.; Prieske, O.; Granacher, U. Effects and dose-response relationships of resistance training on physical performance in youth athletes: A systematic review and meta-analysis. British Journal of Sports Medicine 2016, 50, 781–795. [Google Scholar] [CrossRef]
- Granacher, U.; Lesinski, M.; Büsch, D.; Muehlbauer, T.; Prieske, O.; Puta, C.; Gollhofer, A.; Behm, D. G. Effects of resistance training in youth athletes on muscular fitness and athletic performance: A conceptual model for long-term athlete development. Front Physiol. 2016, 7. [Google Scholar] [CrossRef]
- Slimani, M.; Paravlic, A.; Granacher, U. A meta-analysis to determine strength training related dose-response relationships for lower-limb muscle power development in young athletes. Front Physiol. 2018, 9. [Google Scholar] [CrossRef]
- Negra, Y.; Chaabene, H.; Sammoud, S.; Bouguezzi, R.; Mkaouer, B.; Hachana, Y.; Granacher, U. Effects of plyometric training on components of physical fitness in prepuberal male soccer athletes: The role of surface instability. Journal of Strength and Conditioning Research 2017, 31, 3295–3304. [Google Scholar] [CrossRef]
- Faigenbaum, A. D.; Myer, G. D. Pediatric resistance training: benefits, concerns and program design considerations. Curr Sports Med Rep 2010, 9, 161–8. [Google Scholar] [CrossRef]
- Lloyd, R. S.; Faigenbaum, A. D.; Stone, M. H.; Oliver, J. L.; Jeffreys, I.; Moody, J. A.; Brewer, C.; Pierce, K. C.; McCambridge, T. M.; Howard, R.; Herrington, L.; Hainline, B.; Micheli, L. J.; Jaques, R.; Kraemer, W. J.; McBride, M. G.; Best, T. M.; Chu, D. A.; Alvar, B. A.; Myer, G. D. Position statement on youth resistance training: the 2014 International Consensus. Br J Sports Med. 2014, 48, 498–505. Available online: https://soi.org/10.1136/bjsports-2013-092952. [CrossRef]
- Merino, W. C.; Jiménez Plaza, A. D. Actividad deportiva, su incidencia en el rendimiento académico. Revista Publicando 2017, 10, 542–549. [Google Scholar]
- Guadarrama, R.; César, J.; Veytia, M.; Márquez, O. Confiabilidad y estructura factorial de Kiddo-Kindl, una herramienta de medición para la calidad de vida de los adolescentes mexicanos. Revistas de la Universidad de Oviedo 2015, 20, 1–10. Available online: https://www.unioviedo.es/reunido/index.php/Rema/article/view/10827/10294.
- Bull, F. C.; Al-Ansari, S. S.; Biddle, S.; Borodulin, K.; Buman, M. P.; Cardon, G.; Carty, C.; Chaput, J. P.; Chastin, S.; Chou, R.; Dempsey, P. C.; DiPietro, L.; Ekelund, U.; Firth, J.; Friedenreich, C. M.; Garcia, L.; Gichu, M.; Jago, R.; Katzmarzyk, P. T.; Lambert, E.; Leitzmann, M.; Milton, K.; Ortega, F. B.; Ranasinghe, C.; Stamatakis, E.; Tiedemann, A.; Troiano, R. P.; Van der Ploeg, H. P.; Wari, V.; Willumsen, J. F. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Bompa, T.; Buzzichelli, C. Periodization: Theory and Methodology of Training, 5th ed.; Human Kinetics: England, 2018; pp. 344–349. [Google Scholar]
- Di Salvo, V.; Baron, R.; Tschan, H.; Calderon Montero, F. J.; Bachl, N.; Pigozzi, F. Performance characteristics according to playing position in elite soccer. International Journal of Sports Medicine 2007, 28, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Bradley, P. S.; Sheldon, W.; Wooster, B.; Olsen, P.; Boanas, P.; Krustrup, P. High-intensity running in English FA Premier League soccer matches. Journal of Sports Sciences 2009, 27, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Christou, M.; Smilios, I.; Sotiropoulos, K.; Volaklis, K.; Pilianidis, T.; Tokmakidis, S. P. Effects of resistance training on the physical capacities of adolescent soccer players. Journal of Strength and Conditioning Research 2006, 20, 783–791. [Google Scholar] [CrossRef]
- McQuilliam, S. J.; Clark, D. R.; Erskine, R. M.; Brownlee, T. E. Free-Weight Resistance Training in Youth Athletes: A Narrative Review. Sports medicine (Auckland, N.Z.) 2020, 50, 1567–1580. [Google Scholar] [CrossRef]
- Torres Luque, G.; Carrasco Páez, L. El entrenamiento de fuerza en niños. Apunts. Educación Física y Deportes 2000, 3, 64–71. Available online: https://raco.cat/index.php/ApuntsEFD/article/view/306891.
- López-Bonilla, J. M.; López-Bonilla, L. M.; Serra, F.; Ribeiro, C. Relacion entre actitudes hacia la actividad física y el deporte y rendimiento académico de los estudiantes universitarios españoles y Portugueses. Revista Iberoamericana de Psicologia del Ejercicio y el Deporte 2015, 10, 275–284. [Google Scholar]
- Manuel, J.; Andreu, P. La Práctica de Actividad Física y su Relación con el Rendimiento Académico La Práctica de Actividad Física y su Relación con el Rendimiento Académico. Revista de Educación física 2016, 34, 1–10. Available online: https://www.researchgate.net/publication/313443769.
- Markovic, G.; Dizdar, D.; Jukic, I.; Cardinale, M. Reliability and factorial validity of squat and countermovement jump tests. J. Strenght Cond. Res. 2004, 18, 551–555. [Google Scholar]
- Caulfield, S.; Berninger, D. Exercise technique for free weight and machine training. In Essentials of Strength Training and Conditioning, 4th ed.; Gregory, G., Travis, N., Eds.; Human Kinetics: United States, 2016; Volume 4, pp. 735–736. [Google Scholar]
- Jurado-Castro, J.M.; Campos-Pérez, J.; Vilches-Redondo, M.Á.; Mata, F.; Navarrete-Pérez, A.; Ranchal-Sanchez, A. Morning versus Evening Intake of Creatine in Elite Female Handball Players. Int. J. Environ. Res. Public Health 2022, 19, 393. [Google Scholar] [CrossRef]
- Ruíz, J. R.; España, V.; Castro, J.; Artero, E. G.; Ortega, F. B.; Cuenca, M.; Jiménez, D.; Chillón, P.; Girela M., J.; Mora, J.; Gutiérrez, A.; Suni, J.; Sjöstrom, M.; Castillo, M. J. Batería ALPHA-Fitness: test de campo para la evaluación de la condición física relacionada con la salud en niños y adolescentes. Nutrición Hospitalaria 2011, 26, 1210–1214. [Google Scholar] [CrossRef]
- Gámez, M.; Fernández, A.; Muller, S.; Losada M., C. Diferencias de las capacidades físico-coordinativas en niños de 6 a 12 años. Journal of Physical Education and Human Movement 2022, 4, 1–10. [Google Scholar] [CrossRef]
- Rada, D. A.; Fandiño, G. A.; Vergara, A. C.; Sáenz, J. S.; Cardozo, L. A.; Fernández, J. A. Intensity in Competition of Youth Soccer Players. Revista Edu-fisica.com Ciencias Aplicadas al Deporte 2019, 11, 36–55. Available online: http://revistas.ut.edu.co/index.php/edufisica.
- López-Bonilla, J. M.; López-Bonilla, L. M.; Serra, F.; Ribeiro, C. Relacion entre actitudes hacia la actividad física y el deporte y rendimiento académico de los estudiantes universitarios españoles y Portugueses. Revista Iberoamericana de Psicologia del Ejercicio y el Deporte 2015, 10, 275–284. [Google Scholar]
- Manuel, J.; Andreu, P. La Práctica de Actividad Física y su Relación con el Rendimiento Académico La Práctica de Actividad Física y su Relación con el Rendimiento Académico. Revista de Educación física 2016, 34, 1–10. Available online: https://www.researchgate.net/publication/313443769.
- Rajmil, L.; Serra-Sutton, V.; Fernández-López, J.A.; Berraa, S.; Aymerich, M.; Cieza, A.; Ferrer, M.; Bullinger, M.; Ravens-Sieberer, U. Versión española del cuestionario alemán de calidad de vida relacionado con la salud en población infantil y de adolescentes: el Kindl. Anales de Pediatría 2004, 60, 514–521. [Google Scholar] [CrossRef]
- Atkinson, G.; Neville, A. M. Métodos estadísticos para evaluar el error de medición (fiabilidad. en variables relevantes para la medicina deportiva. Medicina deportiva 1998, 26, 217–238. [Google Scholar]
- Ferguson, C. J. An Effect Size Primer: A Guide for Clinicians and Researchers. Professional Psychology: Research and Practice 2009, 40, 532–538. [Google Scholar] [CrossRef]
- Faigenbaum, A. D. Strength training for children and adolescents. Clinics in Sports Medicine 2000, 19, 593–619. [Google Scholar] [CrossRef] [PubMed]
- Faigenbaum, A. D.; Westcott, W. L.; Loud, R. L.; Long, C. The effects of different resistance training protocols on muscular strength and endurance development in children. Pediatrics 1999, 104. [Google Scholar] [CrossRef]
- Faigenbaum, A. D.; Milliken, L. A.; Loud, R. L. R.; Burak, B. T.; Doherty, C. L.; Westcott, W. L. Comparison of 1 and 2 days per week of strength training in children. Research quarterly for exercise and sport 2002, 73, 416–424. [Google Scholar] [CrossRef]
- Ingle, L.; Sleap, M.; Tolfrey, K. The effect of a complex training and detraining programme on selected strength and power variables in early pubertal boys. Journal of Sports Sciences 2006, 24, 987–997. [Google Scholar] [CrossRef]
- Ozmun, J. C.; Mikesky, A. E.; Surburg, P. R. Neuromuscular adaptations following prepubescent strength training. Medicine & Science in Sports & Exercise 1994, 26, 510–514. [Google Scholar]
- Raya González, J.; Sánchez Sánchez, J. Strenght Training Methods for Improving Actions in Football. Apunts. Educación Física y Deportes 2018, 132, 72–93. [Google Scholar] [CrossRef]
- Faigenbaum, A. D.; Milliken, L.; Moulton, L.; Westcott, W. L. Early muscular fitness adaptations in children in response to two different resistance training regimens. Pediatric Exercise Science 2005, 17, 237–248. [Google Scholar] [CrossRef]
- Sadres, E.; Eliakim, A.; Constantini, N.; Lidor, R.; Falk, B. The Effect of Long-Term Resistance Training on Anthropometric Measures, Muscle Strength, and Self Concept in Pre-Pubertal Boys. Pediatric Exercise Science 2001, 13, 357–372. [Google Scholar] [CrossRef]
- Valle, V. M.; Vanaclocha, P.; Villa-González, E. Efectos del Entrenamiento de Fuerza Pediátrico sobre parámetros de salud en niños: una revisión sistemática. Sportis. Scientific Journal of School Sport, Physical Education and Psychomotricity 2022, 8, 283–308. [Google Scholar] [CrossRef]
- Faigenbaum, A. D.; Kraemer, W. J.; Blimkie, C. J. R.; Jeffreys, I.; Micheli, L. J.; Nitka, M.; Rowland, T. W. Youth resistance training: updated position statement paper from the national strength and conditioning association. Journal of strength and conditioning research 2009, 23 (Suppl. S5). [Google Scholar] [CrossRef]
- Parrado, F. E. Relación del Entrenamiento de la Fuerza en Futbolistas: una Revisión Documental. Coporación Universitaria Minuto de Dios, Colombia, 2021.
- Arroyo, O. D.; Jascue, D. A. Efectos de un programa de entrenamiento pliométrico en la fuerza explosiva de miembros inferiores en niños indígenas jugadores de futbol de 10 a 12 años de edad del club JIISA. Universidad del Valle, Colombia. 2019. Available online: https://bibliotecadigital.univalle.edu.co/handle/10893/21022.
- Pradet, M. La preparación física, 1st ed.INDE: España, 1999. [Google Scholar]
- Lillegard, W. A.; Brown, E. W.; Wilson, D. J.; Henderson, R.; Lewis, E. Efficacy of strength training in prepubescent to early postpubescent males and females: effects of gender and maturity. Pediatric rehabilitation 1997, 1, 147–157. [Google Scholar] [CrossRef]
- Pantoja-García, D.; Larumbe-Zabala, E. Comparison of motor performance between child soccer players and sedentary children during the prepubescent phase: A pilot study. Kronos 2012, 11, 5–13. [Google Scholar]
- Ramírez, R.; Ramiro, J.; Olmedo, I. E. Correlación entre fuerza máxima y saltabilidad en futbolistas competitivos. Universidad de los Lagos, Chile, Efdeportes: Revista digital, 2009.
- Vallejos, P. H. Desempeño físico en futbolistas con discapacidad motora en distintas modalidades de fútbol reducido. Universidad Gabriela Mistral, Santiago de Chile, 2018.
- López de los Mozos Huertas, J. Condición física y rendimiento académico. Physical condition and academic performance. Journal of Sport and Health Research 2018, 10, 349–360. [Google Scholar]
Figure 1.
Experimental design.
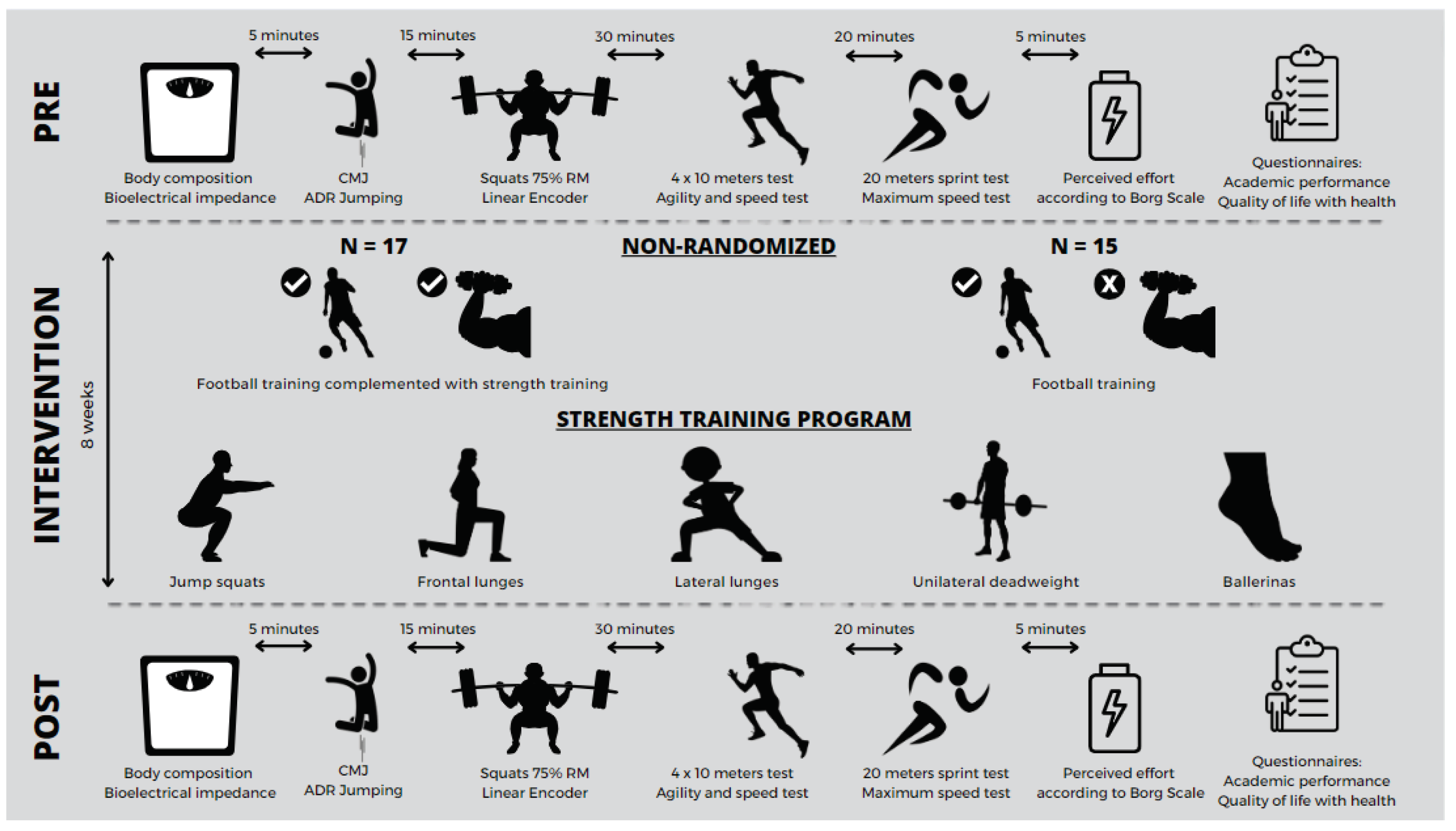
Figure 2.
Flowchart using the guidelines CONSORT (Consolidated Standards of Reporting Trials).
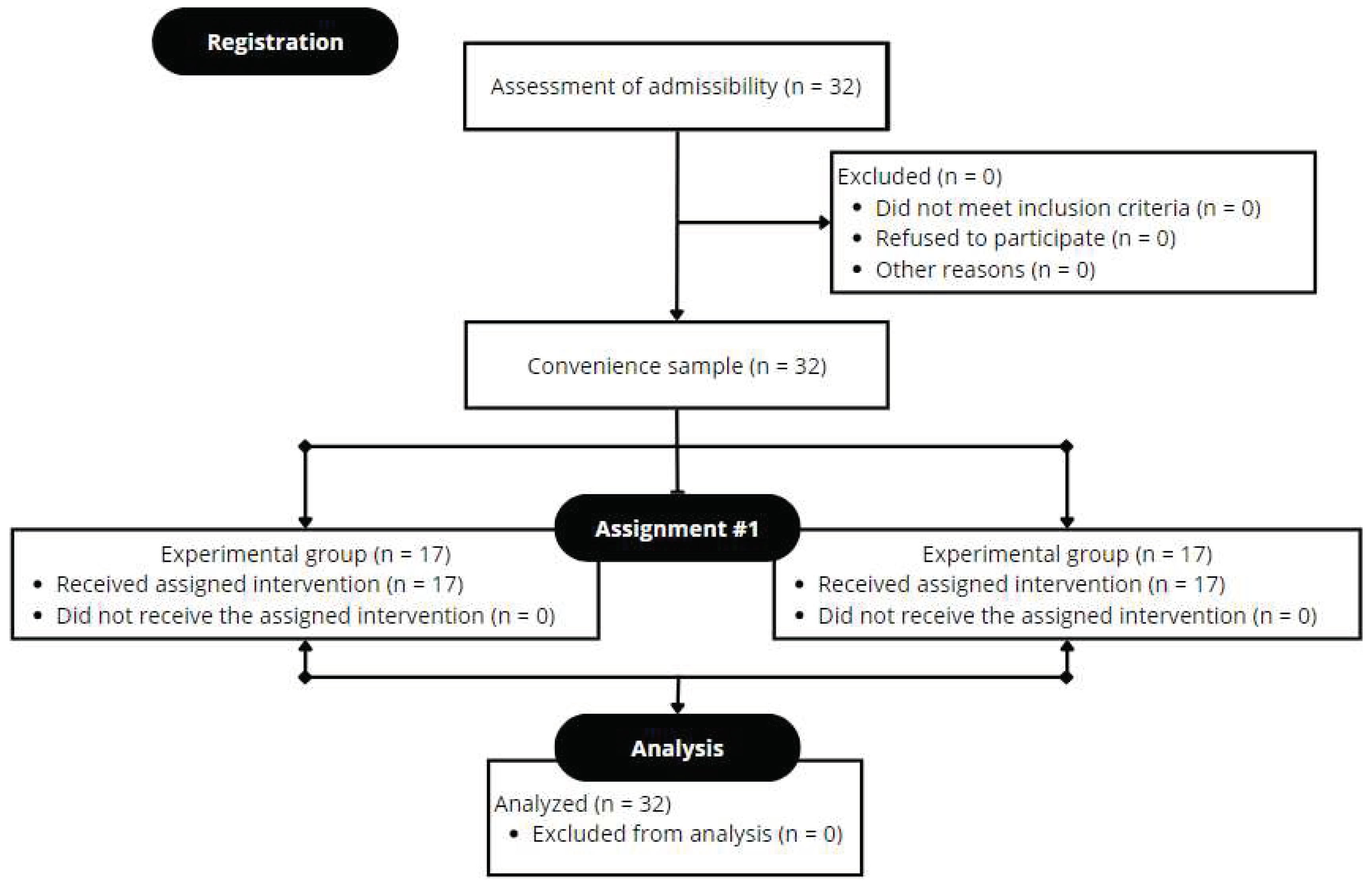

Table 1.
Descriptive characteristics and comparative analysis of averages for measurements in body composition of both groups at the beginning and at the end of the strength training program.
Table 1.
Descriptive characteristics and comparative analysis of averages for measurements in body composition of both groups at the beginning and at the end of the strength training program.
| VARIABLE | GROUP | BASALINE (WEEK 0) | FINAL (WEEK 8) |
P VALUE TIME | η2p | P VALUE GROUP | η2p | P VALUE TIME* GROUP | η2p |
|---|---|---|---|---|---|---|---|---|---|
|
AGE (years) |
EG | 12.5 ± 0.5 | 12.7 ± 0.6 | 0.004* | 0.467 | 0.265 | 0.088 | 0.719 | 0.010 |
| CG | 12.7 ± 0.5 | 12.9 ± 0.7 | |||||||
|
HEIGHT (cm) |
EG | 154.9 ± 7.9 | 155.1 ± 8 | 0.024* | 0.313 | 0.012* | 0.373 | 0.181 | 0.124 |
| CG | 161.4 ± 6.3 | 162.5 ± 6.7 | |||||||
|
WEIGHT (kg) |
EG | 43.5 ± 7.6 | 44 ± 7.8 | 0.003* | 0.475 | 0.063 | 0.226 | 0.356 | 0.061 |
| CG | 50.9 ± 12 | 51.8 ± 12.1 | |||||||
|
BMI (kg/m2) |
EG | 18 ± 2.1 | 18.2 ± 2.1 | 0.261 | 0.089 | 0.327 | 0.069 | 0.597 | 0.021 |
| CG | 19.4 ± 4.1 | 19.5 ± 4.1 | |||||||
|
FAT (%) |
EG | 18.5 ± 2.7 | 17.3 ± 2.7 | 0.027* | 0.304 | 0.672 | 0.013 | 0.139 | 0.149 |
| CG | 18.6 ± 4 | 18.3 ± 4.3 | |||||||
|
RA-FAT (%) |
EG | 30.2 ± 4.1 | 28.5 ± 3.4 | 0.023* | 0.319 | 0.050* | 0.248 | 0.025* | 0.310 |
| CG | 27.4 ± 4.5 | 26.8 ± 3.8 | |||||||
|
LA-FAT (%) |
EG | 30 ± 3.3 | 28 ± 3.4 | 0.002* | 0.518 | 0.382 | 0.055 | 0.043* | 0.261 |
| CG | 28.1 ± 4 | 27.7 ± 4.2 | |||||||
|
TR-FAT (%) |
EG | 15.2 ± 3.1 | 14 ± 3.1 | 0.105 | 0.177 | 0.824 | 0.004 | 0.034* | 0.284 |
| CG | 14.8 ± 4.6 | 15.1 ± 4.9 | |||||||
|
RL-FAT (%) |
EG | 19.7 ± 2.8 | 19 ± 2.7 | 0.104 | 0.177 | 0.373 | 0.057 | 0.257 | 0.091 |
| CG | 20.5 ± 4.1 | 20.4 ± 4.4 | |||||||
|
LL-FAT (%) |
EG | 20.4 ± 2.8 | 19.6 ± 2.7 | 0.205 | 0.112 | 0.351 | 0.062 | 0.149 | 0.143 |
| CG | 21.2 ± 4.3 | 21.3 ± 4.7 |
Note. *Statistically significant difference, p<0,05. RA: right arm; LA: left arm; CG: control group; EG: experimental group; BMI: body mass index; RL: right leg; LL: left leg; TR: trunk.
Table 2.
Descriptive characteristics and comparative analysis of averages for measurements in RM, CMJ, 4 x 10 meters test and 20 meters sprint test in both groups, at the beginning and at the end of the strength training program.
Table 2.
Descriptive characteristics and comparative analysis of averages for measurements in RM, CMJ, 4 x 10 meters test and 20 meters sprint test in both groups, at the beginning and at the end of the strength training program.
| VARIABLE | GROUP | BASALINE (WEEK 0) | FINAL (WEEK 8) | P VALUE TIME | η2p |
P VALUE GROUP | η2p |
P VALUE TIME* GROUP | η2p |
|---|---|---|---|---|---|---|---|---|---|
|
CMJ (cm) |
EG | 34.7 ± 4.3 | 36.1 ± 3.7 | 0.006* | 0.430 | 0.385 | 0.054 | 0.007* | 0.415 |
| CG | 34 ± 3.9 | 34 ± 3.6 | |||||||
|
BACK-SQUAT RM (kg) |
EG | 33.3 ± 6.4 | 38.2 ± 6.8 | 0.006* | 0.424 | 0.002* | 0.496 | 0.086 | 0.196 |
| CG | 42.7 ± 5.7 | 44.3 ± 7.7 | |||||||
|
75 % BACK-SQUAT MV (m/s) |
EG | 0.73 ± 0.06 | 0.68 ± 0.04 | <0.001* | 0.611 | 0.044* | 0.260 | 0.588 | 0.021 |
| CG | 0.7 ± 0.04 | 0.66 ± 0.03 | |||||||
|
75 % BACK-SQUAT PV (m/s) |
EG | 1.06 ± 0.06 | 2.32 ± 3.3 | 0.164 | 0.134 | 0.135 | 0.153 | 0.155 | 0.139 |
| CG | 1.05 ± 0.09 | 1.03 ± 0.09 | |||||||
|
75 % BACK-SQUAT MP (w) |
EG | 311.9 ± 60.2 | 294.7 ± 55 | 0.001* | 0.540 | 0.186 | 0.122 | 0.662 | 0.014 |
| CG | 349 ± 85.6 | 335 ± 79.3 | |||||||
|
75 % BACK-SQUAT PP (w) |
EG | 452.4 ± 78 | 921 ± 1203 | 0.159 | 0.136 | 0.303 | 0.076 | 0.158 | 0.137 |
| CG | 523.4 ± 129.5 | 525.2 ± 127 | |||||||
| BACK-SQUATS TO FAILURE (Number of repetitions) | EG | 7.6 ± 1 | 8.1 ± 0.9 | 0.010* | 0.388 | 0.436 | 0.044 | 0.582 | 0.022 |
| CG | 7.2 ± 1 | 7.8 ± 1.1 | |||||||
|
4 X 10 METERS TEST (seg) |
EG | 10.67 ± 0.3 | 10.42 ± 0.3 | <0.001* | 0.808 | <0.001* | 0.617 | <0.001* | 0.743 |
| CG | 10.06 ± 0.2 | 10.06 ± 0.2 | |||||||
|
20 METERS SPRINT TEST (seg) |
EG | 3.84 ± 0.15 | 3.72 ± 0.14 | <0.001* | 0.691 | 0.939 | 0.000 | 0.003* | 0.471 |
| CG | 3.79 ± 0.12 | 3.77 ± 0.15 |
Note. *Statistically significant difference, p<0,05. CMJ: countermovement jump; MP: mean power; PP: peak power; RM: repetition maximum; MV: mean velocity; PV: peak velocity.
Table 3.
Descriptive characteristics and comparative analysis of averages for measurements of health-related quality of life in both groups at the beginning and at the end of the strength training program.
Table 3.
Descriptive characteristics and comparative analysis of averages for measurements of health-related quality of life in both groups at the beginning and at the end of the strength training program.
| VARIABLE | GROUP | BASAL TIME | FINAL TIME | P VALUE TIME | η2p |
P VALUE GROUP | η2p |
P VALUE TIME* GROUP | η2p |
|---|---|---|---|---|---|---|---|---|---|
|
QoL EMOTIONAL WELL-BEING |
EG | 4.3 ± 0.6 | 4.5 ± 0.5 | 0.002* | 0.520 | 0.020* | 0.328 | 0.841 | 0.003 |
| CG | 3.8 ± 0.6 | 3.9 ± 0.4 | |||||||
|
QoL SELF-ESTEEM |
EG | 4.2 ± 0.7 | 4.6 ± 0.4 | 0.003* | 0.472 | 0.237 | 0.098 | 0.014* | 0.360 |
| CG | 4.1 ± 0.7 | 4.1 ± 0.5 | |||||||
| QoL SCHOOL | EG | 4.1 ± 0.8 | 4.6 ± 0.4 | 0.049* | 0.250 | 0.030* | 0.293 | 0.063 | 0.225 |
| CG | 3.5 ± 1.3 | 3.6 ± 1.2 | |||||||
| QoL FRIENDS | EG | 4.7 ± 0.2 | 4.8 ± 0.3 | 0.282 | 0.082 | 0.048* | 0.252 | 0.774 | 0.006 |
| CG | 4.4 ± 0.5 | 4.5 ± 0.4 | |||||||
| QoL FAMILY WEEL-BEING | EG | 4.6 ± 0.3 | 4.7 ± 0.3 | 0.132 | 0.154 | 0.081 | 0.201 | 0.845 | 0.003 |
| CG | 4.3 ± 0.5 | 4.4 ± 0.4 | |||||||
| QoL PHYSICAL WEEL-BEING | EG | 3.7 ± 0.6 | 4.4 ± 0.4 | <0.001* | 0.711 | 0.493 | 0.034 | 0.105 | 0.176 |
| CG | 3.7 ± 0.4 | 4.1 ± 0.5 | |||||||
| OVERALL QUALITY OF LIFE | EG | 4.3 ± 0.4 | 4.6 ± 0.2 | <0.001* | 0.783 | 0.004* | 0.464 | 0.018* | 0.340 |
| CG | 4 ± 0.3 | 4.1 ± 0.3 |
Note. *Statistically significant difference, p<0,05. QoL: quality of life
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



