
Submitted:
25 January 2024
Posted:
26 January 2024
You are already at the latest version
Abstract
A healthy 47-year-old woman consulted the Oral Surgery and Implantology Unit of the University Hospitals of Geneva with a request to treat her painful tooth 11 and replace the missing tooth 21. The dental history revealed that the patient had lost teeth 21 and 22 due to advanced caries. On clinical examination, tooth 11 showed an ill-fitting prosthetic crown with overhanging margins, an increased localized probing depth of 8 mm in the disto-vestibular area and sensitivity to percussion. The edentulous site 21 showed horizontal bone atrophy. Radiological examination revealed a well-defined unilocular radiotransparent lesion surrounded by a thin radiolucent border, located at the apex of tooth 11 and measuring 10 x 8 mm. The treatment consisted of extraction of 11, enucleation of the apical lesion, insertion of implants at sites 11 and 21 with simultaneous bone augmentation in a single surgical procedure with aesthetic and functional results at 3-year follow-up without any complications. Our case highlights that immediate implant placement in case of cystic periapical lesion represents a good valid alternative to standard treatment.
Keywords:
Dental implant
; Immediate implant
; Radicular Cyst
1. Introduction
For many years, the standard procedure for dental implant treatment has been to place dental implant in healed sockets [1]. With the changes observed in implant surgery over time, immediate placement of dental implants in extraction sockets has proven to be a safe and viable treatment option [2,3,4]. This procedure became a strategy favored by clinicians owing to the associated advantages, such as reducing the number of surgical procedures, stress on the patient and morbidities, shortening treatment duration, and better managing of soft tissue and alveolar morphology [5,6].
In the anterior region where the aesthetic result is veryimportance, numerous studies have demonstrated the need for both an intact socket to optimize primary stability and a buccal bone wall thickness of 1mm to guarantee the stability of bone and soft tissues in order to limit the risks of recession [4,5,6].
In recent years, some studies showed high success rates for immediate implant placement in sockets with chronic periapical pathologies or infected sites [7,8]. In these cases, pathogenic bacteria may be present in the extraction sites [8,9] and complete curettage of the granulation tissues and all soft tissue remnants in sockets is required to reduce the inflammatory response and allow osseointegration. However, the risks related to this treatment option continue to be a matter of debate in clinical practice [8,9,10,11].
To the best of our knowledge this study describes for the first time an immediate implant placement in the anterior region of the maxilla following cyst enucleation with good aesthetic and functional results after a follow-up period of 3 years.
2. Case Presentation
A 47-year-old female patient in good general health consulted the Oral Surgery and Implantology Unit of the University Hospitals of Geneva seeking treatment for her painful tooth 11 and for replacing missing teeth 21. The patient had lost teeth 21 and 22 due to advanced carious lesions. Tooth 22 was replaced by a dental implant and tooth 21 had been replaced several months earlier by a removable prosthesis. Clinical examination of the oral cavity was within normal limits. Dental examination revealed fair oral hygiene with dental plaque on the crown of implant at site 22. Particles of bone augmentation materials were visible through the vestibular mucosa. Resin composite filling of tooth 12 was poorly adapted. Tooth 11 presented a poorly adapted prosthetic crown with overhang margins, with an increased localized probing depth of 8 mm in the disto-buccal site and tenderness to percussion. Edentulous site 21 showed horizontal bone atrophy. The intra-oral radiological examination confirmed the different findings observed clinically as tooth 11: a post-crown, inadequate endodontic treatment, a unilocular, well-defined radiolucency surrounded by a thin radiolucent border, centered of the apex of tooth 11, measuring 10 x 8 mm. The residual distance between the roof of the cystic lesion and the nasal cavity measured 2.5 mm (Figure 1a–d).
The presumptive diagnosis of an odontogenic radicular cyst on tooth 11 was made. A root fracture was also suspected. The prognosis for tooth 11 was considered hopeless. The patient asked to restore the 2 anterior teeth while maintaining the diastema that she had previously. Extraction of tooth 11 and enucleation of the apical lesion were proposed and accepted by the patient, who requested immediate implant placement at sites 11 and 21 at the same time. A preoperative prophylactic antibiotic Co-amoxicillin (Co-amoxi mepha, Mepha Pharma, Switzerland) was taken one hour prior to surgery (2g). A mucoperiostal flap was raised on the facial and lingual aspects to obtain a clear view of site 11, the underlying resorbed alveolar ridge and site 21, under local anaesthesia (4% articaine with 1:100.000 adrenaline – Ubistesin™ Forte – 3M ESPE). The cystic lesion was enucleated in toto and root 11 was removed carefully to preserve intact buccal wall and sent for histopathological analysis (Figure 2a–d) which confirmed the diagnosis of radicular cyst (Figure 3a–d).
Implant beds preparation was carried out «freehand» at the future implant positions to its final diameter under constant irrigation with sterile saline according to the manufacturer’s instructions for placing BLT implants (Straumann, Switzerland). The existing removable prosthesis from site 21 was used for the drilling axis at site 11. Gauge were used to control preparation depth and implant axis orientation after each drill (Figure 4).
A Straumann® BLT implant with a diameter of 4.1 mm and a length of 14 mm and a BLT implant with a diameter of 3.3 mm and a length of 12 mm were manually placed at sites 11 and 21, respectively (Figure 5) and good primary stability was achieved for both implants.
The cystic cavity, the gap between the buccal wall and exposed surface of implant at site 11 and the buccal defect of site 21 were filled and augmented using a mixture of autogenous bone chips, retrieved during drilling, and alloplastic bone (bone Ceramic® Straumann, Switzerland) (Figure 6). A collagen membrane (OsteoBiol Evolution, Tecnoss) was used to entirely cover the augmented site and soft tissues were carefully reapproximated and sutured using simple 4-0 Supramid sutures (Figure 6).
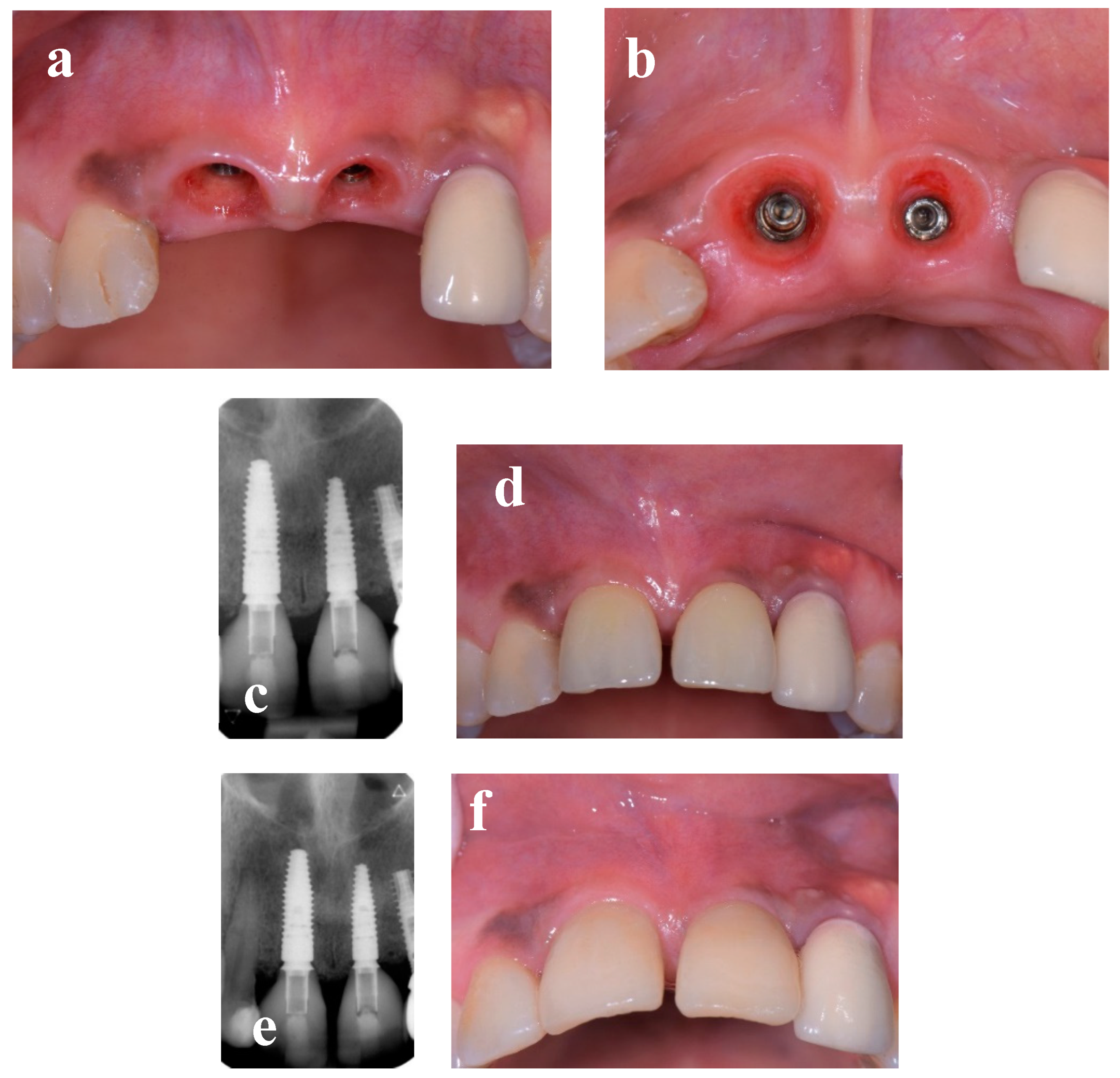
Control intraoral radiographs were taken, and post-operative advice was given to the patient along with a prescription for oral antibiotics (amoxicillin with clavulanic acid 2g/d for 5 days). After a healing period of three months, reopening was performed, and implants were initially restored using temporary crowns to condition the soft tissues followed by two screw-retained single-unit crowns (E-max-press). The implant-supported restorations showed good aesthetic and functional results after a follow-up period of 3 years (Figure 7).
3. Discussion
To the best of our knowledge this case report is the first describing an immediate implantation procedure after tooth extraction and enucleation of a radicular cyst and implantation at the adjacent site with simultaneous bone augmentation. Radicular cyst is the most common inflammatory odontogenic cyst representing 52–68% of all maxillary cysts [12,13] that occur after the development of periapical granuloma. It affects predominantly the upper jaw, in patients between 30 and 40 years and seems to be more common in male [14]. Its origin is inflammatory: in most cases, it is associated with a decayed tooth with necrotic pulp [15] which causes inflammation of the periapical tissues and stimulation of the epithelial rests of Malassez. Radicular cysts are chronic lesion that grow slowly and are most often asymptomatic: their finding can be fortuitous during a radiological examination. Radiologically, it appears as a homogeneous radiolucent lesion, round to oval in shape, well limited, surrounded by a sclerotic border [15], or more rarely multilocular [14], near the apex of a non-vital tooth. Most radicular cysts are small, ranging from 0.5 to 1.5 cm [16]. However, the radiological size of the lesion does not allow a diagnosis to be made. In our case, the cyst was fortuitously discovery as a radiolucent lesion measuring 1 cm in long axis. Large radicular cysts can cause displacement or increased mobility of adjacent teeth [17]. The possibility of root resorption (of the affected tooth or adjacent teeth) by a radicular cyst has been rarely reported [17]. It is probably due to infection or osteoclastic factors produced by the cyst [16]. Histological examination of a radicular cyst shows a central cavity filled with eosinophilic liquid or semi-liquid serosity, with cholesterol crystals derived from the disintegration of erythrocytes, lymphocytes, plasma cells, and macrophages. It is lined by non-keratinized stratified squamous epithelium, containing occasionally rare mucous and exceptionally ciliated cells. The epithelium is often irregular, spongiotic, with polynuclear neutrophils in exocytosis, acanthotic or shows even the presence of atrophic or eroded areas concomitant to the inflammatory process. In some cases, the epithelial proliferation may resemble that of a squamous odontogenic tumor. Rushton bodies, or hyaline bodies, exhibiting a wide variety of shapes, including linear, round, lamellar, or amorphous structures, can be seen in the epithelium as well as the wall of radicular cysts. The epithelium is surrounded by a capsule made up of fibrous connective tissue, containing a chronic inflammatory infiltrate usually dense with numerous silhouettes of cholesterol crystals often associated with foreign-type giant cell granulomas and deposits of hemosiderin [18]. Aspiration of an uninfected radicular cyst reveals serohematic fluid, usually containing an abundance of cholesterol granules that impart a shimmering straw or golden color.
During the early years of dental implantology, the Branemark protocol based on the concept of osseointegration [1] required excellent primary stability [19] and recommended a healing period of 6 months after dental extraction for complete bone recovery [1]. Initially addressed to rehabilitate cases of total edentulism [1,4], implant placement therapy gradually used to restore partially edentulous areas and even missing single teeth [19,20] from the 1990s onwards. In this context, understanding the dimensional changes of the ridge and the biological principles of bone healing after extraction, determining the appropriate time for implant placement after extraction has become paramount and other implant timing such as early implantation and immediate implantation have been investigated [2,3,4,5]. With the advent of Guided Bone Regeneration and the desire to reduce treatment time and due to the increased patients’ demands for aesthetic results, the immediate implantation technique has become widely used [3,4,5] and numerous studies have confirmed the reliability of this technique with success rates similar to implants placed in healed ridges [3,4,5,6]. However, it is essential to point out that this treatment option requires selection of appropriate cases and correct execution of the technique. With regard to clinical and anatomical conditions, many authors recommend a thick gingival biotype and an integral buccal bone wall at the extraction site, [2,3,5,6].Others authors underline the fact that the buccal bone wall should be at least 1 mm thick, since lesser thickness is associated with more extensive vertical cortical bone resorption [4], thus increasing the risk of mucosal recession resulting in a negative impact on the aesthetics of the final result.
In our case, regarding the volumetric stability of the soft and hard tissues following post-extraction remodeling, showed a quantity of keratinized gingiva sufficient. Although the apical bone at site 11 was limited, the bone wall was more than 1mm thick and could therefore allow for the volume stability of the edentulous crest. In terms of proximal bone, the distal site benefited from the support of the periodontal ligament of tooth 12. On the other hand, site 21 was edentulous and showed severe horizontal bone atrophy, which could be corrected. From a mere point of view of the technique’s therapeutic considerations, immediate implantation is indeed classically a flapless surgery, reducing the risks of additional bone resorption in the extraction socket, particularly in the buccal wall, by maintaining vascularization from the periosteum [21] and reducing post-operative morbidity [22]. However, the lack of visibility associated with a flapless technique represents a challenge when preparing the implant bed of a post-extraction socket. This is in fact a complex surgical procedure requiring the intervention of an expert surgeon [23] and presenting risks of perforation of the buccal or palatal bone which can sometimes go undiagnosed or even limit the possibility of placing the implant. The inclination of the axis of future implants should be along the palatal bone, and an implant axis oriented towards the buccal surface of the implant is also a contributing factor to gingival recession [24]. In our case, a flap was necessary to achieve bone augmentation at the adjacent site 21 and to optimize visibility during enucleation of the cystic lesion and drilling at sites 11 and 21. In addition, another aspect to consider with immediate implantation is the achievement of primary stability, since even micro-movements of 50 to 150 μm at the bone-implant interface may favor the development of fibrous tissue, by impairing the formation of new bone at the implant surface, and consequently compromise the osseointegration phenomenon [25]. Several studies have also reported that the high success rates of this technique were associated with the achievement of primary stability [26]. Bone anchorage for primary stability in immediate implantation primarily depends on the bone at the apical and palatal levels of the alveolus [27]. For this reason, particular attention must be paid to the proximity of neighboring anatomical structures such as the maxillary sinuses, nasal cavities, mandibular canal, and mental foramina. In the context of post-extraction sockets requiring the removal of cystic lesions, achieving primary stability can be even more complex due to the presence of the enucleation cavity, which reduces the amount of bone available and requires a more meticulous and precise surgical procedure. In our patient, one of the difficulties was to obtain primary stability because, although the palatal cortex was intact, the post-enucleation apical space was empty of bone for 10mm beyond the dental apex and the residual bone height between the apical level of the cavity and the nasal cavity was 3mm, which greatly limited the possibility of apical anchorage. Nevertheless, primary stability was achieved by optimizing bone anchorage through the palatal bone and residual apical bone to the post-enucleation cavity using a 14mm long BLT implant while maintaining a 2mm safety margin from the nasal cavity. Typically, bone augmentation simultaneous with immediate implantation is required to fill the gaps between the vestibular cortex and the exposed implant surface [28]. In our case, filling was carried out between the vestibular cortex and the implant surface, as well as at the apical level of the post-enucleation cystic cavity using bone ceramics combined with autologous bone taken during drilling. Furthermore, a membrane was used to cover the implant sites, particularly for the Guided Bone Regeneration of the adjacent site 21. Immediate implantation also offers the possibility of an immediate fixed provisional restoration, provided that primary stability is achieved and sufficient insertion torque of around 35 N/cm is applied [29], optimizing peri-implant soft tissue management and the aesthetics of the restoration [30,31,32]. In our case, the insertion torque was sufficient, but the adjacent site requiring implant placement with augmentation did not allow this possibility under optimal conditions. In addition, reopening after the osseointegration phase and soft tissue conditioning using temporary crowns was necessary.
4. Conclusions
Numerous advances in clinical techniques and biomaterials have greatly expanded the indications for dental implant treatment options. According to the literature, this case report for the first time seems to describe an immediate implantation procedure after extraction and enucleation of apical cystic lesion in the anterior region with satisfactory aesthetic results after more than 3 years of follow-up.
Chronic periapical inflammatory lesion does not seem to be an absolute contraindication to immediate implant placement in selected cases but require a careful procedure protocol. Additional studies are necessary to assess the survival rates of immediate implants placed in this clinical setting.
Author Contributions
Conception, draft of the manuscript, preparation of images, patient treatment, A.P.; T. L; draft of the manuscript and radiological interpretation preparation of images, A.P.; M.L.; conception, drafting, and critical review of the manuscript, A.P.; T.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The presented study adhered to the Helsinki Declaration of ethical principles by the World Medical Association. The study did not require approval of the Ethics Commission on Human Research of Geneva (CCER-Geneva) according to the Federal Human Research Act (Art.3al.a), since the study involved less than five patients.
Informed Consent Statement
Written informed consent was obtained from the patient to publish this paper.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Adell, R.; Lekholm, U.; Rockler, B.; Brånemark, P.-I. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int. J. Oral Surg. 1981, 10, 387–416. [Google Scholar] [CrossRef] [PubMed]
- Soegiantho, P.; Suryawinata, P.G.; Tran, W.; Kujan, O.; Koyi, B.; Khzam, N.; Miranda, L.A. Survival of Single Immediate Implants and Reasons for Loss: A Systematic Review. Prosthesis 2023, 5, 378–424. [Google Scholar] [CrossRef]
- Perez, A.; Hamzah, S.; Lombardi, T. Immediate versus Delayed Implant Placement in Patients with Tooth Agenesis: An In-Line Retrospective Pilot Study Comparing Clinical and Patient-Related Outcomes. Appl. Sci. 2023, 13, 9368. [Google Scholar] [CrossRef]
- Buser, D.; Chappuis, V.; Belser, U.C.; Chen, S. Implant placement post extraction in esthetic single tooth sites: when immediate, when early, when late? Periodontol. 2000 2017, 73, 84–102. [Google Scholar] [CrossRef]
- Chen, S.T.; Buser, D. Clinical and esthetic outcomes of implants placed in postextraction sites. Int J Oral Maxillofac Implants 2009, 24, 186–217. [Google Scholar]
- Perez, A.; Caiazzo, A.; Valente, N.A.; Toti, P.; Alfonsi, F.; Barone, A. Standard vs customized healing abutments with simultaneous bone grafting for tissue changes around immediate implants. 1-year outcomes from a randomized clinical trial. Clin. Implant. Dent. Relat. Res. 2020, 22, 42–53. [Google Scholar] [CrossRef]
- Lindeboom, J.A.H.; Tjiook, Y.; Kroon, F.H.M. Immediate placement of implants in periapical infected sites: A prospective randomized study in 50 patients. Oral Surgery, Oral Med. Oral Pathol. Oral Radiol. Endodontology 2006, 101, 705–710. [Google Scholar] [CrossRef]
- Manor, Y.; Alkasem, A.; Mardinger, O.; Chaushu, G.; Greenstein, R.B.N. Levels of bacterial contamination in fresh extraction sites after a saline rinse. Int. J. Oral Maxillofac. Implant. 2015, 30, 1362–1368. [Google Scholar] [CrossRef]
- Fugazzotto, P.A. A retrospective analysis of implants immediately placed in sites with and without periapical pathology in sixty-four patients. J. Periodontol. 2012, 83, 182–186. [Google Scholar] [CrossRef]
- Jung, R.E.; Zaugg, B.; Philipp, A.O.H.; Truninger, T.C.; Siegenthaler, D.W.; Hämmerle, C.H.F. A prospective, controlled clinical trial evaluating the clinical radiological and aesthetic outcome after 5 years of immediately placed implants in sockets exhibiting periapical pathology. Clin. Oral Implant. Res. 2012, 24, 839–846. [Google Scholar] [CrossRef]
- Kakar, A.; Kakar, K.; Leventis, M.D.; Jain, G. Immediate Implant Placement in Infected Sockets: a consecutive cohort study. J Lasers Med Sci 2020, 11, 167–173. [Google Scholar] [CrossRef]
- Johnson, N.R.; Gannon, O.M.; Savage, N.W.; Batstone, M.D. Frequency of odontogenic cysts and tumours: a systematic review. J Investig Clin Dent 2014, 5, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Shivhare, P.; Singh, A.; Haidry, N.; Yadav, M.; Shankarnarayan, L. Multilocular radicular cyst – a common pathology with uncommon radiological appearance. J Clin Diagn Res 2016, 10, 13–15. [Google Scholar] [CrossRef]
- Noda, A.; Abe, M.; Shinozaki-Ushiku, A.; Ohata, Y.; Zong, L.; Abe, T.; Hoshi, K. A bilocular radicular cyst in the mandible with tooth structure components inside. Case Rep. Dent. 2019, 2019, 6245808. [Google Scholar] [CrossRef]
- Quadri, A.; Keerthi, R.; Khan, T.A. Unusual aggressive large radicular cyst invading maxillary sinus: a case report. Int J Sci Stud 2016, 4, 180–183. [Google Scholar]
- Avril, L.; Lombardi, T.; Ailianou, A.; Burkhardt, K.; Varoquaux, A.; Scolozzi, P.; Becker, M. Radiolucent lesions of the mandible: a pattern-based approach to diagnosis. Insights Imaging 2014, 5, 85–101. [Google Scholar] [CrossRef]
- Kolari, V.; Rao, H.T.A.; Thomas, T. Maxillary and mandibular unusually large radicular cyst: A rare case report. Natl. J. Maxillofac. Surg. 2019, 10, 270–273. [Google Scholar] [CrossRef]
- El-Naggar, A.K.; Chan, J.K.C.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO classification of head and neck tumours (4th edition). IARC 2017, 9, 204–207. [Google Scholar]
- Javed, F.; Romanos, G.E. The role of primary stability for successful immediate loading of dental implants. A literature review. J. Dent. 2010, 38, 612–620. [Google Scholar] [CrossRef]
- Trisi, P.; Perfetti, G.; Baldoni, E.; Berardi, D.; Colagiovanni, M.; Scogna, G. Implant micromotion is related to peak insertion torque and bone density. Clin. Oral Implant. Res. 2009, 20, 467–471. [Google Scholar] [CrossRef]
- Ebenezer, V.; Balakrishnan, K.; Asir, R.V.D.; Sragunar, B. Immediate placement of endosseous implants into the extraction sockets. J. Pharm. Bioallied Sci. 2015, 7, 234–237. [Google Scholar] [CrossRef]
- Roe, P.; Kan, J.Y.K.; Rungcharassaeng, K.; Caruso, J.M.; Zimmerman, G.; Mesquida, J. Horizontal and vertical dimensional changes of peri-implant facial bone following immediate placement and provisionalization of maxillary anterior single implants: a 1-year cone beam computed tomography study. Int J Oral Maxillofac Implants 2012, 27, 393–400. [Google Scholar]
- Cosyn, J.; Sabzevar, M.M.; De Bruyn, H. Predictors of inter-proximal and midfacial recession following single implant treatment in the anterior maxilla: a multivariate analysis. J. Clin. Periodontol. 2012, 39, 895–903. [Google Scholar] [CrossRef]
- Buser, D.; Halbritter, S.; Hart, C.; Bornstein, M.M.; Grütter, L.; Chappuis, V.; Belser, U.C. Early Implant Placement With Simultaneous Guided Bone Regeneration Following Single-Tooth Extraction in the Esthetic Zone: 12-Month Results of a Prospective Study With 20 Consecutive Patients. J. Periodontol. 2009, 80, 152–162. [Google Scholar] [CrossRef]
- Hämmerle, C.H.F.; Chen, S.T.; Wilson, T.G. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int. J. Oral Maxillofac. Implant. 2004, 19, 26–28. [Google Scholar]
- Fickl, S.; Zuhr, O.; Wachtel, H.; Bolz, W.; Huerzeler, M. Tissue alterations after tooth extraction with and without surgical trauma: a volumetric study in the beagle dog. J. Clin. Periodontol. 2008, 35, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Rocci, A.; Martignoni, M.; Gottlow, J. Immediate Loading in the Maxilla Using Flapless Surgery, Implants Placed in Predetermined Positions, and Prefabricated Provisional Restorations: A Retrospective 3-Year Clinical Study. Clin Implant Dent Relat Res. 2003, 5, 29–36. [Google Scholar] [CrossRef]
- Merli, M.; Bernardelli, F.; Esposito, M. Immediate versus early nonocclusal loading of dental implants placed with a flapless procedure in partially edentulous patients: preliminary results from a randomized controlled clinical trial. Int J Periodontics Restorative Dent 2008, 28, 453–459. [Google Scholar] [PubMed]
- Degidi, M.; Piattelli, A. A 7-year Follow-up of 93 Immediately Loaded Titanium Dental Implants. J Oral Implantol 2005, 31, 25–31. [Google Scholar] [CrossRef]
- Ottoni, J.M.P.; Oliveira, Z.F.L.; Mansini, R.; Cabral, A.M. Correlation between placement torque and survival of single-tooth implants. Int J Oral Maxillofac Implants 2005, 20, 769–776. [Google Scholar]
- Greenstein, G.; Cavallaro, J. Implant Insertion Torque: Its Role in Achieving Primary Stability of Restorable Dental Implants. Compend. Contin. Educ. Dent. 2017, 38, 88–95. [Google Scholar] [PubMed]
- Balaji, P.; Balaji, S.M.; Ugandhar, P. Immediate implant in single rooted teeth - Study on primary stability and bone formation. Indian J. Dent. Res. 2015, 26, 421–426. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(a-d). Clinical view and intra-oral radiographs showing the initial clinical status of anterior maxillary area.
Figure 1.
(a-d). Clinical view and intra-oral radiographs showing the initial clinical status of anterior maxillary area.
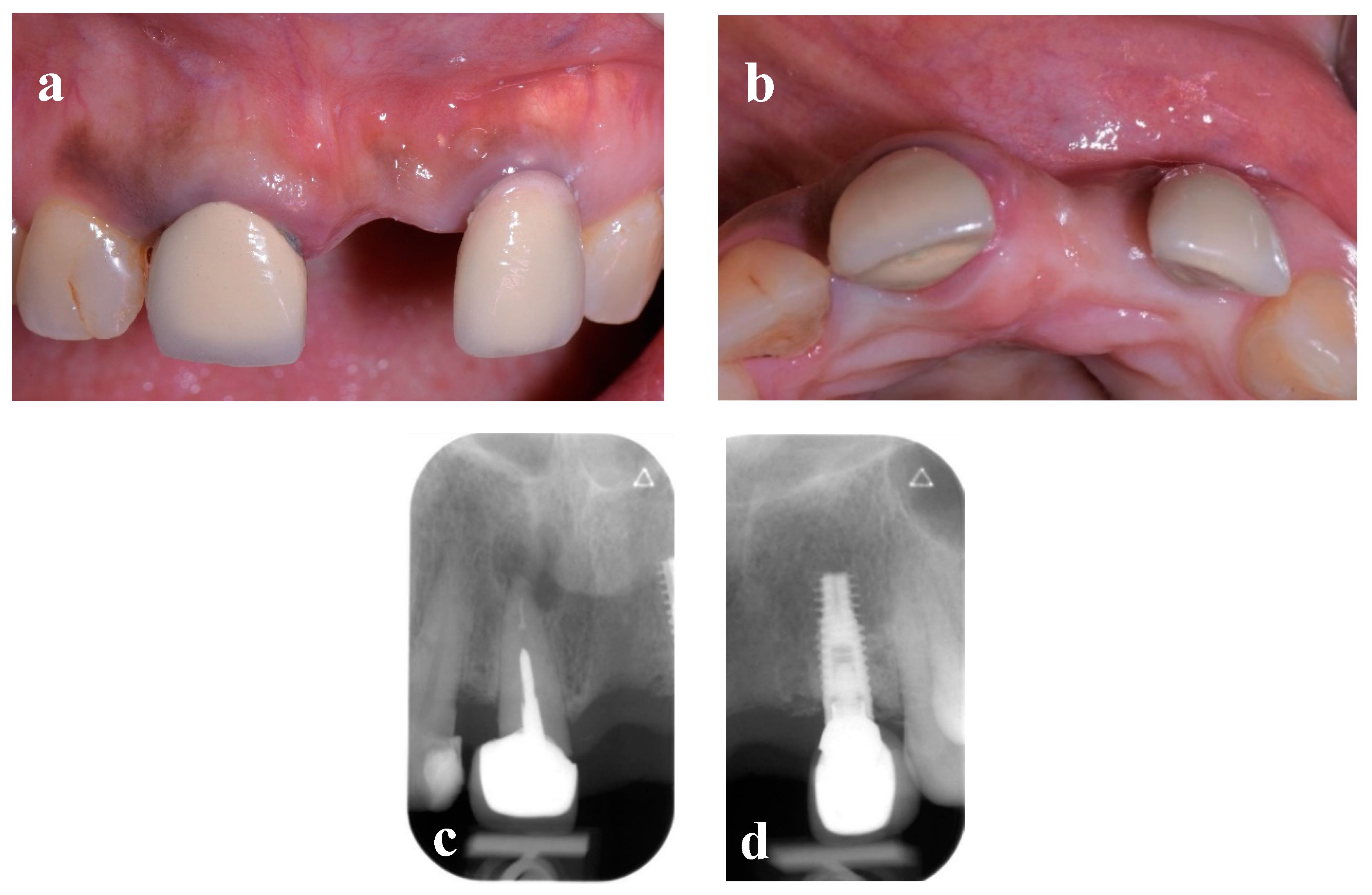
Figure 2.
(a-d). Intraoperative view of buccal mucoperiosteal flap elevation (a), during and (b) after cystectomy (c) and after tooth extraction (d).
Figure 2.
(a-d). Intraoperative view of buccal mucoperiosteal flap elevation (a), during and (b) after cystectomy (c) and after tooth extraction (d).
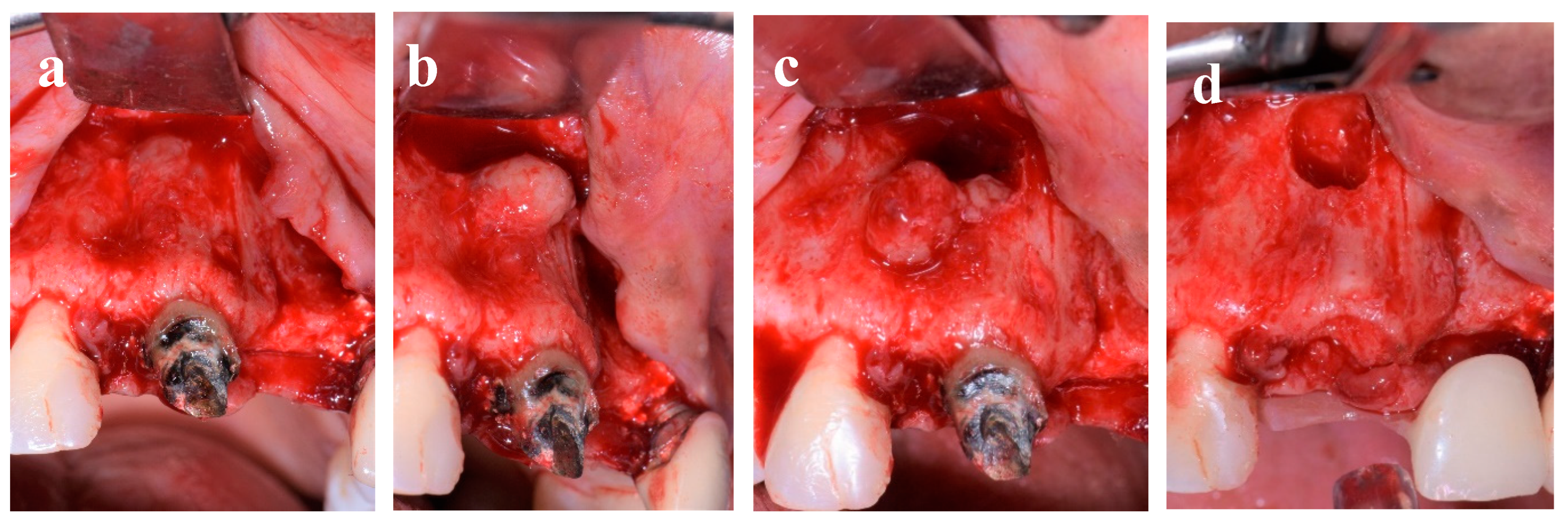
Figure 3.
a-d Histopathological examination of the excised specimen stained by hematoxylin and eosin showing fibrous cyst wall, hemorrhage, and heavy chronic inflammatory infiltrate (a and b, a: 20x, b: 40x magnification). C (hematoxylin and eosin) and d (polarized light) show root canal filling material (60x magnification).
Figure 3.
a-d Histopathological examination of the excised specimen stained by hematoxylin and eosin showing fibrous cyst wall, hemorrhage, and heavy chronic inflammatory infiltrate (a and b, a: 20x, b: 40x magnification). C (hematoxylin and eosin) and d (polarized light) show root canal filling material (60x magnification).
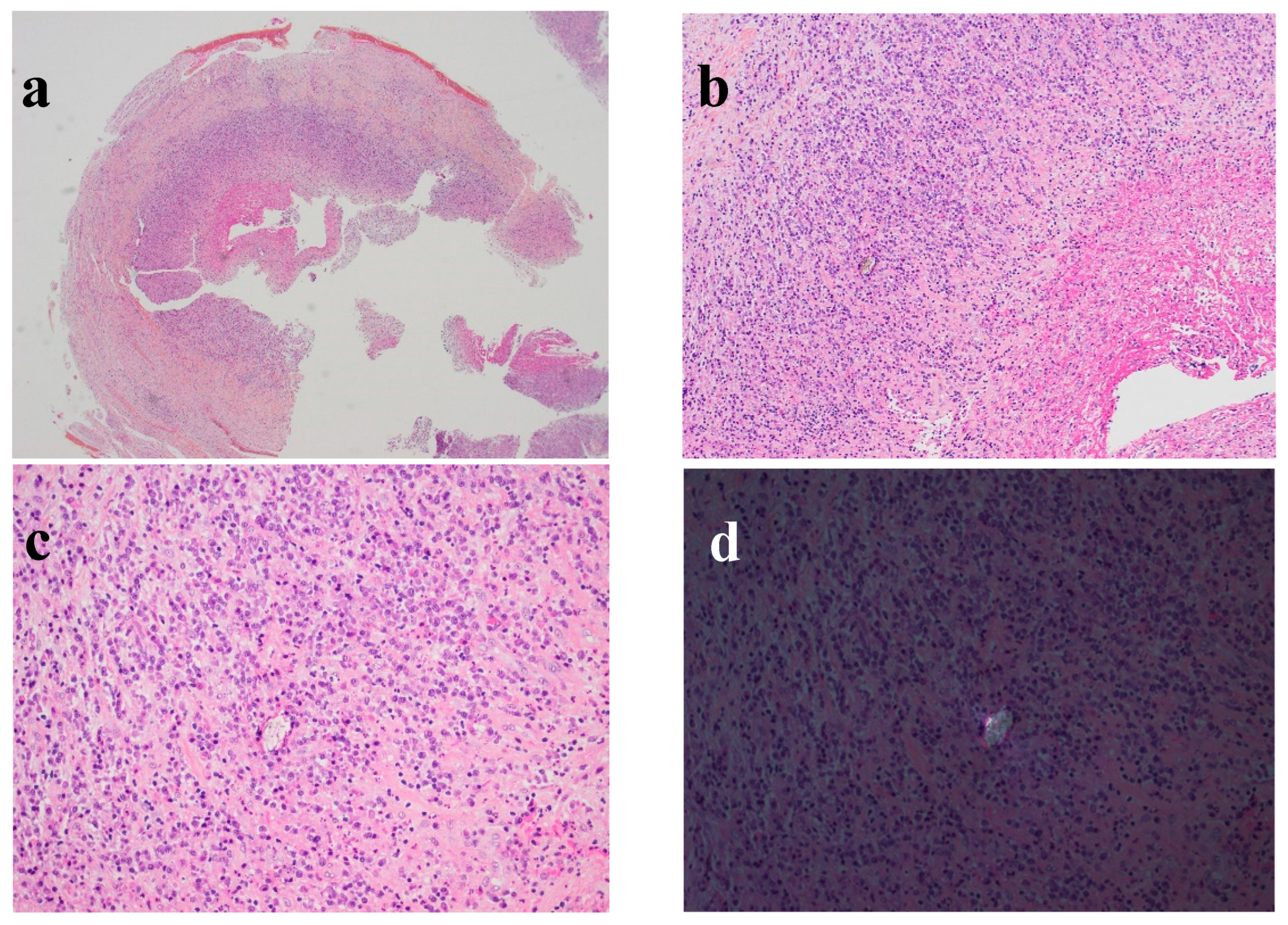
Figure 4.
a-d Buccal view showing control of the drilling axes of site 11 (a), 11 and 21 (b and c) and occlusal view showing implant bed preparation of site 11 (d).
Figure 4.
a-d Buccal view showing control of the drilling axes of site 11 (a), 11 and 21 (b and c) and occlusal view showing implant bed preparation of site 11 (d).
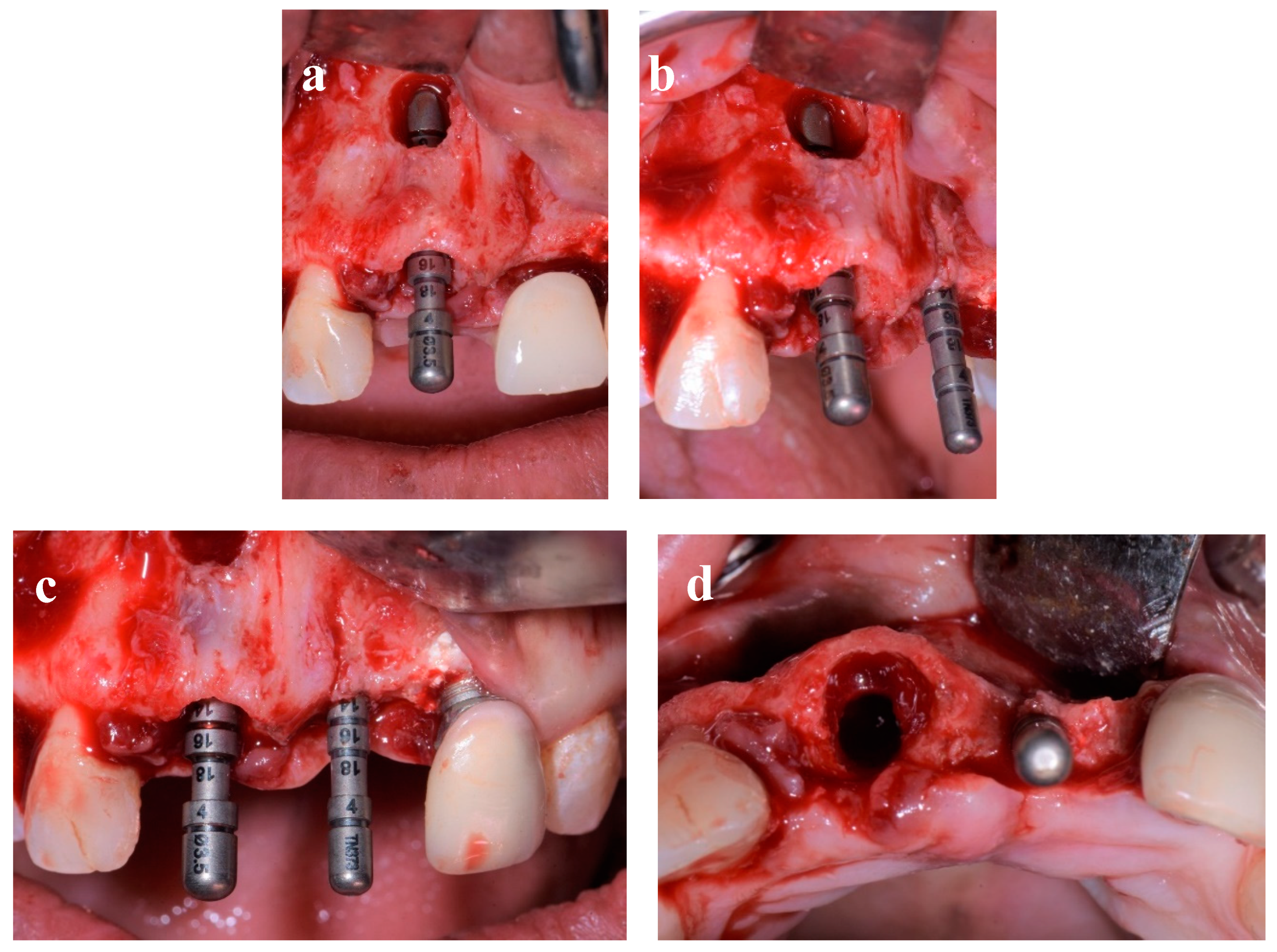
Figure 5.
(a-c). Buccal view after placement of implants at sites 11 and 21 (a) and showing bone defect at the cavity after cystectomy (b) and occlusal view showing the gap between the intact buccal wall and implant site 11 (c).
Figure 5.
(a-c). Buccal view after placement of implants at sites 11 and 21 (a) and showing bone defect at the cavity after cystectomy (b) and occlusal view showing the gap between the intact buccal wall and implant site 11 (c).
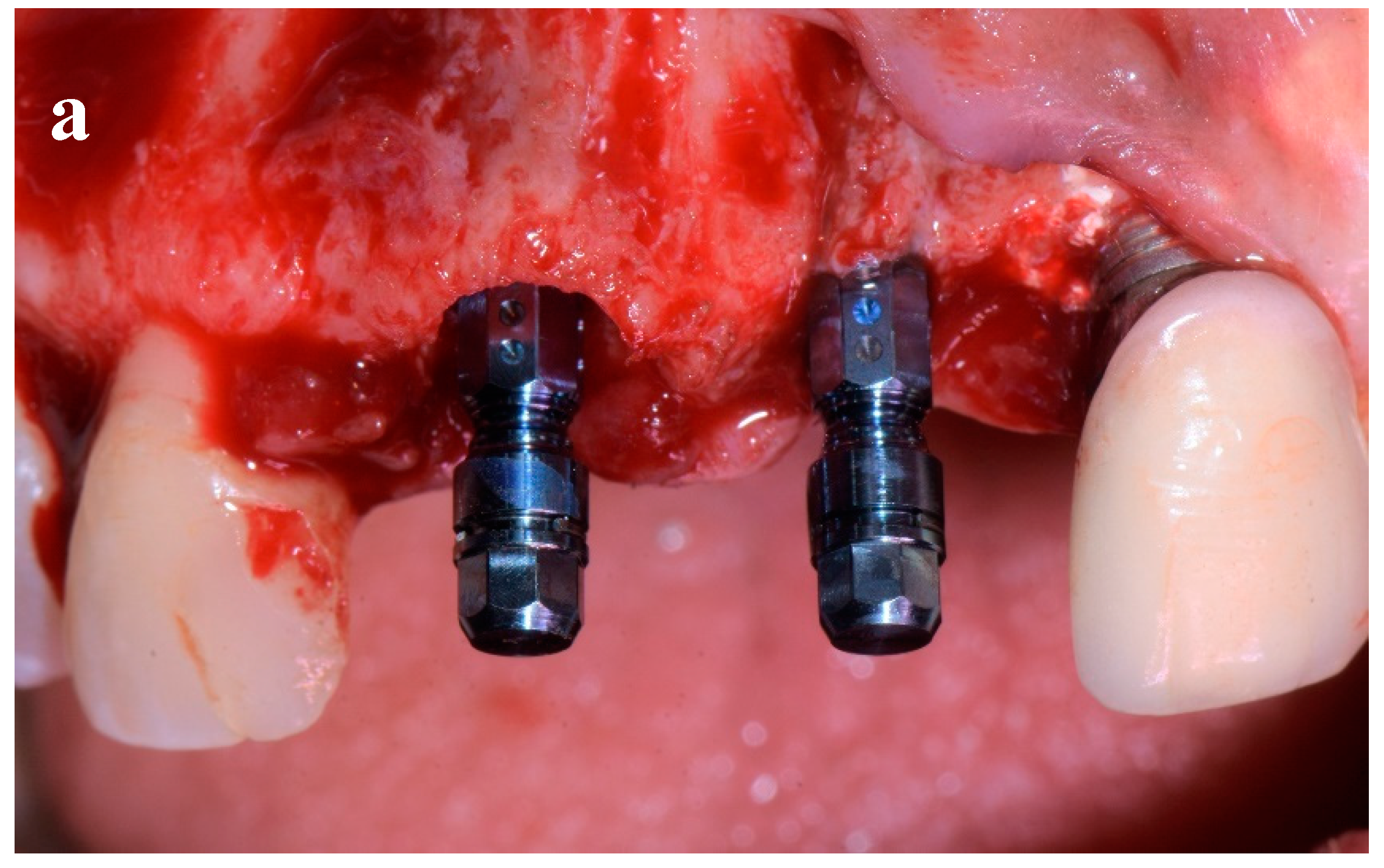
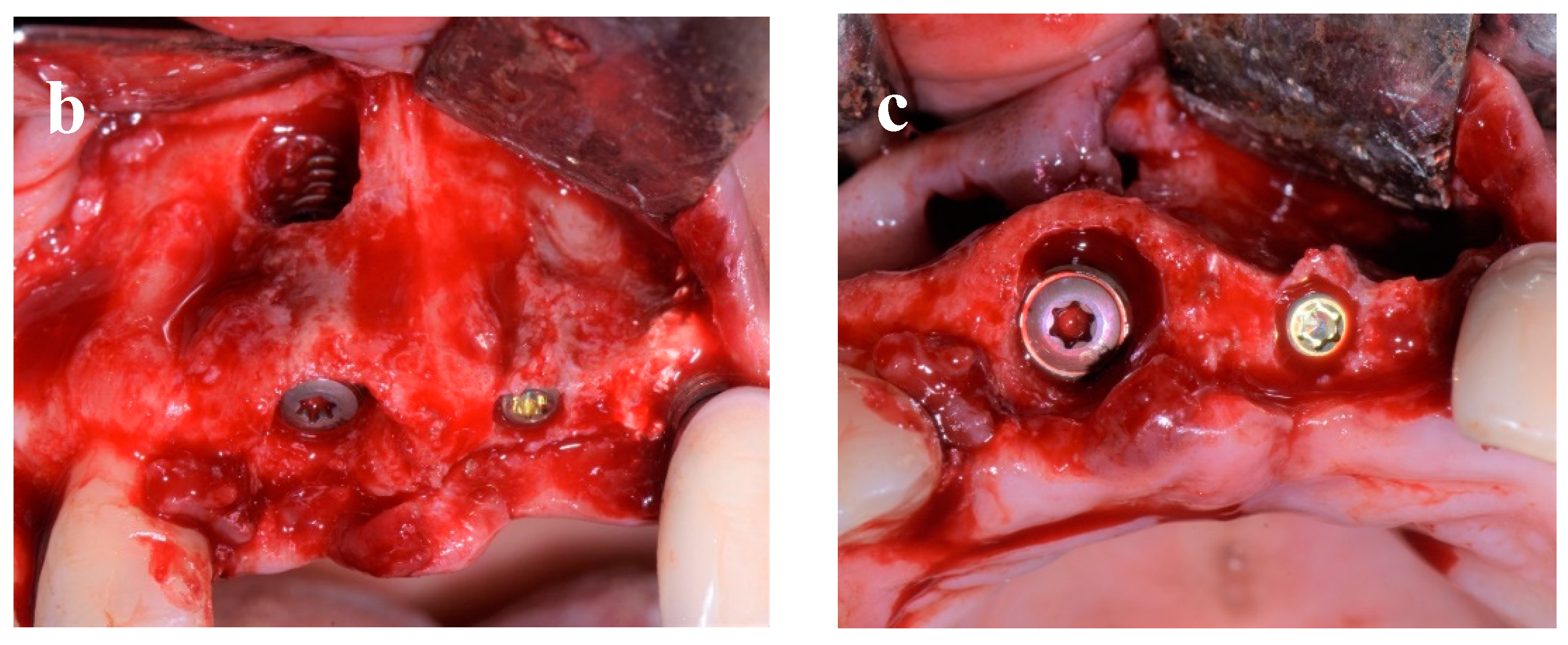
Figure 6.
(a-e). Clinical view showing the augmented sites using autogenous bone chips and alloplastic bone (a) covered by collagen membrane (b), after wound closure (c-d) and periapical 2D radiographs taken immediately after implants placement.
Figure 6.
(a-e). Clinical view showing the augmented sites using autogenous bone chips and alloplastic bone (a) covered by collagen membrane (b), after wound closure (c-d) and periapical 2D radiographs taken immediately after implants placement.
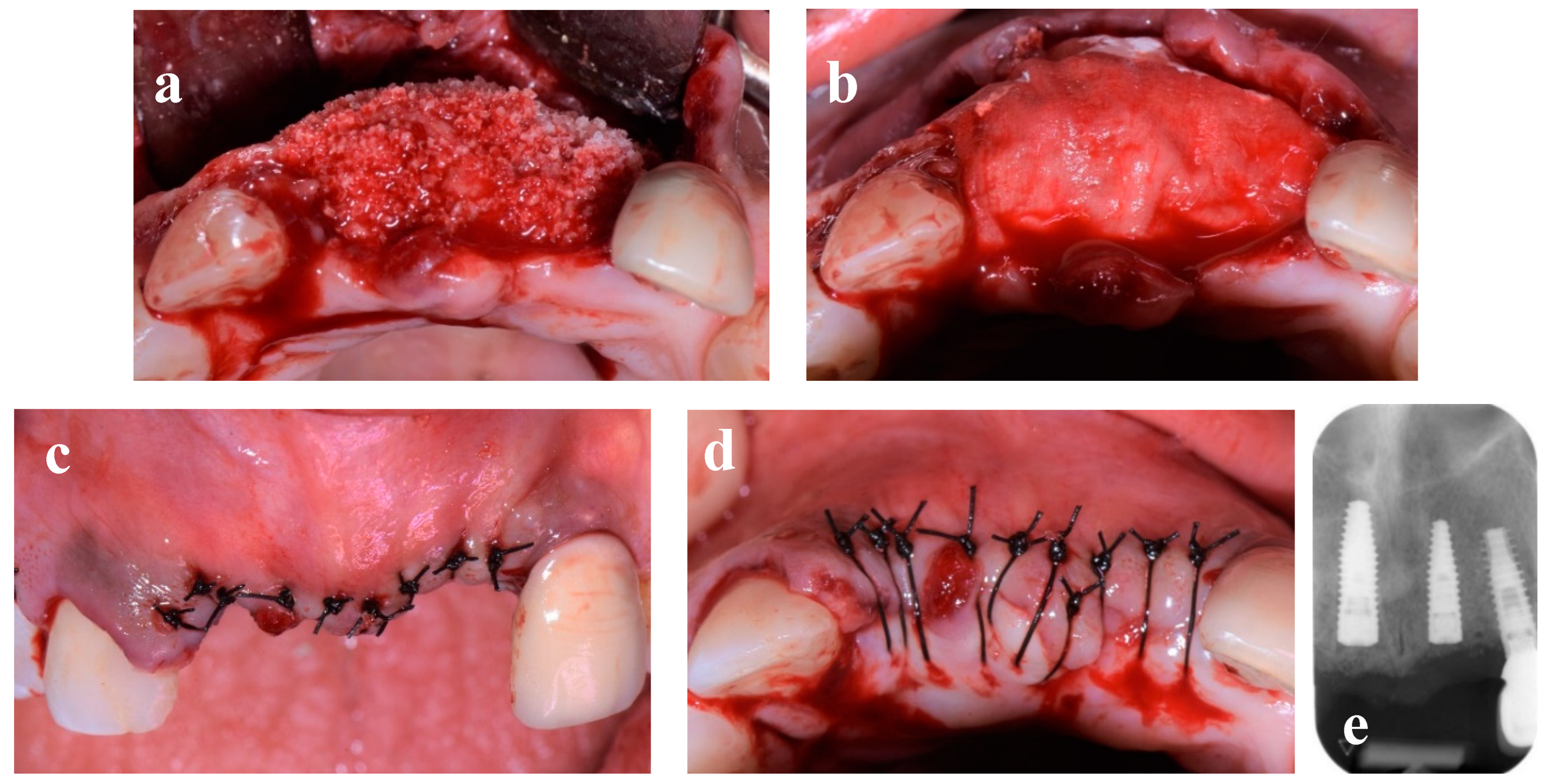
Figure 7.
(a-d). Soft tissues condition when the two screw-retained single-unit crowns (E-max-press) were delivered (a,b), Radiographic and clinical examination after 1 (c,d) and 3 year follow-up period (e,f).
Figure 7.
(a-d). Soft tissues condition when the two screw-retained single-unit crowns (E-max-press) were delivered (a,b), Radiographic and clinical examination after 1 (c,d) and 3 year follow-up period (e,f).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



