
Submitted:
29 January 2024
Posted:
30 January 2024
You are already at the latest version
Abstract
In May of 2022, millions of U.S. parents faced uncertainty in safely feeding their infants due to the infant formula shortage. Methods: An anonymous, electronic, cross-sectional, retrospective survey was used. Results: U.S. parents (n =187) whose infants were 10.2 weeks old during the short-age completed the survey. Eighty-one percent of parents switched formulas during the shortage, 87% switched because they could not find the formula they typically used, 34% switched 3-5 times, 29% of parents visited ≥ 4 stores/24 hours and 26% of parents traveled >20 miles/24 hours to purchase formula. Use of infant formula increased (p< 0.01); in infants requiring specialty for-mula, use of intact cow’s milk formula increased (p < 0.05) and use of premature infant formulas decreased (p < 0.05). Infants relying on specialty formulas experienced at least one undesirable outcome compared with non-specialty users. Parents used social media, relatives/friends, and healthcare providers for support during the shortage, but their helpfulness scores were suboptimal. Parents reported needs for greater infant formula availability, free prenatal lactation education and postpartum lactation support. Conclusions: Government, regulatory and healthcare policy oversight are needed to protect the infant feeding system, including more commercially available products, access to banked donor milk and lactation support.
Keywords:
Keywords: Breastfeeding
; consumer behavior
; equity
; feeding practices
; food security
; health
; government and regulatory policies
; infant formula shortage
; lactation
; pediatrics
1. Introduction
In 2022, the United States (U.S.) faced an acute infant formula shortage that was initiated by a recall by Abbott Nutrition, the largest U.S. infant formula manufacturer that provides 40% of the nation’s infant formula. [1] Abbott voluntarily recalled several brands of its powdered formula products due to bacterial contamination from Cronobacter sakazakii [2]. Additionally, Abbott also voluntarily closed one of the country’s largest manufacturing plant in Michigan that was found to be connected to the contamination [3]. These events were exacerbated by supply chain issues related to the COVID-19 pandemic and restrictive U.S. trade and tariff policies that led to a reduction of available infant formula [4]. By the end of May 2022 the shortage reached its height, with a national out-of-stock rate for infant formula as high as 90% in several states [5] which left millions of parents to face uncertainty in safely feeding their infants [6,7]. In response, the U.S government introduced “Operation Fly” to assist families in accessing safe imported infant formulas.
The 2022 infant formula shortage was especially distressful for vulnerable populations such as families from low-income communities that participate in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and heavily rely on infant formula (consume >50% of U.S. produced formula) [8,9] and infants requiring specialty formulas due to medical or other conditions [10]. Infants that require specialty formulas due to metabolic or medical conditions such as inborn error of metabolism, low birth weight or other medical or dietary conditions represent approximately 6% of infants that use infant formula in the U.S.[11].
Due to the inaccessibility of infant formula, health officials were concerned parents would rely on unsafe infant feeding practices that the American Academy of Pediatrics (AAP), Centers for Disease Control and Prevention (CDC) and Food and Drug Administration (FDA) recommend against. Such unsafe infant feeding practices include: 1) modifying formula by diluting it with water [12]; 2) making homemade infant formula [13]; 3) feeding cow’s milk before one year of age [14]; and 4) informal human milk sharing [15]. In a recent prospective cross-sectional study, predominately of families from low-income communities, the number of individuals that used at least one unsafe infant feeding practice increased from 8% before to 48.5% during the 2022 infant formula shortage. Specifically, the percentage of parents that reported infant feeding practices before and during the infant formula shortage significantly increased from 2% to 28% for banked donor milk use; 5% to 26% for use of human milk from informal sharing; and 2% to 29% for use of watered-down infant formula [16]. These unsafe infant feeding practices increase the health and safety risks of infants who rely on infant formula exclusively or as a supplement to human milk.
To date, no studies have reported the impact of the 2022 infant formula shortage on parental consumer behaviors, infant health or quality of life outcomes or breastfeeding outcomes. The purpose of this study was to identify infant feeding practices, health, and quality of life outcomes during the 2022 infant formula shortage. We conducted a retrospective cross-sectional analysis and needs assessment in families from middle-high income communities and reported a high percentage of infants who required specialty formulas. The goal of this study was to identify areas within regulatory and healthcare policies and programs that could improve the resiliency of the infant food system and prevent a future infant feeding crisis.
2. Materials and Methods
2.1. Subjects and Design
Parents who were signed up with Bobbie Labs listserv who agreed to be contacted for future research purposes were emailed an invitation email to participate in an anonymous, cross-sectional, electronic survey. Individuals who met all study criteria completed the survey between December 18, 2022, and January 31, 2023. The first one hundred individuals who completed the survey received a $50 electronic gift card. Parents were eligible to participate if they fulfilled the following criteria: 1) were 18 years old or older; 2) lived with their infants in the U.S. in May 2022; 3) were the parent of an infant who was 6 months old or younger in May 2022; 4) their infant consumed some amount of infant formula before the May 2022 shortage; 5) they experienced challenges with feeding their infant because of the infant formula shortage in May 2022; and 6) they agreed that only one parent of one baby from the same household would complete the survey. Parents reported their demographics and answered questions about their infant feeding practices, experiences, and sentiments in response to the infant formula shortage. The study was approved by the UC Davis Institutional Review Board (IRB ID: 1920147).
The online survey was created in Qualtrics 2022 (Provo, Utah, USA) and included ninety-four unique questions. Participants answered yes/no, multiple choice, rating on a sliding scale (0 to 10), and open-ended questions. The survey contained questions about demographics including, infant and parental age, socioeconomic status, and ethnicity. Participants were asked what their infants typically ate over a 7-day period right before and a 7-day period during the infant formula shortage. Additionally, use of human milk from informal sharing, homemade infant formula, watered-down formula and expired infant formula were aggregated into one variable as “unsafe infant feeding practices” for a 7-day period right before and a 7-day period during the most challenging time of the shortage.
Participants were asked to select all the resources that provided guidance or support in feeding their infants during the shortage. Participants were also asked to rate on a sliding scale from 0 to 10 how helpful a list of resources have been with providing guidance or support to feed their infants or to select “non-applicable” if they did not experience any help from the listed resource. Infant feeding sources and resources used in this survey were adapted from the Infant Feeding Practices Study II (IFPS II) [17] which differentiated lactation consultants from other healthcare providers and included up-to-date online resources such as social media, and blogs.
Participants were asked to rate on a sliding scale from 0 to 10 how helpful a list of activities would be in helping families feed their infants in the “near future” or to select “non-applicable” if they were unsure. These activities were compiled from comments posted on several multiple social media outlets (Reddit, Facebook, Twitter) by parents during the height of the 2022 infant formula shortage. The survey used in this study is available as Supplementary File S1.
2.2. Data Validation
To ensure the data collected from the study survey was reliable and not completed in duplicate by the same individuals, individuals completed two surveys. The first survey was used for screening and prompted individuals from the Bobbie Labs listserv to answer questions about their eligibility. Individuals who met all eligibility criteria were emailed the cross-sectional survey and were required to use the same email addresses entered in the screening survey. The cross-sectional survey excluded individuals with the same email addresses. Data for completed surveys were included in the statistical analyses.
2.3. Statistics
All statistical analyses were conducted using IBM SPSS Statistics version 29 and figures were generated in Graphpad PRISM v.10.1.2 Statistical significance was considered as p < 0.05. Bonferroni-adjusted p-values for multiple comparisons are reported herein. Descriptive statistics (means, standard deviations, ranges, frequencies, and percentages) are reported for demographics, breastfeeding experience, infant feeding practices, consumer behavior, infant outcomes, use and sentiments about resources, and sentiments about future activities that could help families feed their infants in the future.
To understand how infant feeding changed in response to the infant formula crisis, parents were asked what their infants typically ate over a 7-day period right before and a 7-day period during the most challenging time of the infant formula shortage. Parents were also asked how they obtained formula before and during the shortage. Data were treated as binary (yes/no) responses and the McNemar test was used to determine if there were differences for each item before and during the infant formula shortage.
Parents were asked if their infants experienced any problems in response to changing infant formulas during the shortage. Parents selected problems from a list which were treated as binary (yes/no) responses and Pearson Chi-Square, 2-sided test and Phi correlation were used to determine differences and their effect sizes, respectively, in the number of individuals whose infants experienced problems based on their requirement for specialty formulas (vs. no requirement for specialty formulas).
The survey prompted parents to select all that apply from a list of nineteen resources that provided guidance or support in feeding their infants during the infant formula shortage. Parents who selected “yes” to using any of the nineteen resources, were asked to rate on a scale 0-10 how helpful those resources have been in providing guidance or support in feeding their infants during the infant formula shortage. Parents were also asked to rate on a scale 0-10 how helpful they think seventeen activities would be in helping families feed their babies in the “near future”.
This study also collected qualitative data and prompted parents to offer open responses about how they dealt with the infant formula shortage and the actions they feel should be taken by health authorities, food companies, and the government that could help them feed their infants during this crisis and prevent future crises. Open-ended responses were searched for repetition in 5% or more of respondents and reduced to thirty-eight words, themes, or key phrases shown in Table S1. Canva® 2023 was used to manually generate a word cloud of terms for which font size and color are proportional to the frequency of repeated words, themes, or key phrases.
3. Results
3.1. Demographics and Participant Characteristics
A total of 213 individuals initiated and 178 completed the survey. Respondents resided in thirty-seven unique U.S. states (Figure S1). All respondents identified themselves as the parent (biological or not biological) of an infant who was six months old or younger in May 2022. Ninety-three percent of parents who completed the survey were female and 77% were white, 12.4% were Asian, 0.6% were black, 0.6% were American Indian or Alaska Native, 0.6% were unsure of their race, and 3.4% reported to belong to two or more races. Approximately 88% of parents had earned a bachelor’s degree or higher and 55% of parents reported annual household incomes at or above $150,000/year. Six percent of parents had reported they or their infants’ co-parent had received benefits from Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) within the past 12 months of completing the survey (Table 1).
Ninety-three percent of infants in this study joined their family through pregnancy. Eighty-nine percent of infants were born at term (≥ 37 weeks gestation) with an average age of 10.2 weeks at the time of the survey. Sixty-eight percent of female parents were primiparous when they completed the survey and 96% of female parents reported they had ever breastfed or fed expressed milk to their infants (Table 2). Twenty-one percent (n = 38) of parents reported their infants required a specialty formula during the infant formula shortage due a metabolic or medical condition (data not shown) for the following reasons: allergy (3.4%), colic (4.5%), constipation (5.6%), gas (8%), intolerance (1%), malabsorption (0.6%), prematurity (5.6%), rash (0.6%), reflux (6.2%), and other (3.4%) (Figure S2).
3.2. Infant Feeding Practices before and during the Infant Formula Shortage
Prior to the shortage, 81% of infants in this study consumed their mothers’ own breast milk (MOM) but this value decreased to 76% during the infant formula shortage (trend, unadjusted p = 0.022). On the other hand, the use of infant formula significantly increased from 84% before the shortage to 93% during the shortage (adjusted p< 0.01) (Figure 1A). The use of any unsafe infant feeding practice such as: human milk from informal sharing, or homemade infant formula, or diluted formula, or expired infant formula was low (2%) did not change (data not shown). The use of animal milks, plant-based milks, toddler formula, baby cereal or other foods or beverages were not significantly different, however, there was a trend for an increase in “other dairy foods yogurt, cheese, ice cream, pudding, etc.” (trend, unadjusted p = 0.039) from 2% before to 6% during the infant formula shortage (Figure 1B). When asked how sure respondents were of their answers, 91% and 89% were “extremely sure” to questions about infant diet before and during the shortage, respectively (data not shown).
Eighty-nine percent of parents used U.S. infant formula brands before the shortage, however, this value decreased to 79% during the shortage. Additionally, 2% of parents used imported infant formula before the shortage and this value increased to 7% during the shortage (Figure S3). Of the types of infant formulas used before and during the shortage, intact cow’s milk formula increased from 18% to 39% (trend, unadjusted p = 0.039) and premature formula significantly decreased from 33% to 9% (p adjusted p < 0.05) (Figure 2).
3.3. Consumer Behavior and Experience in Response to the Infant Formula Shortage
When asked how parents obtained infant formula, 3% purchased formula via social media before the shortage but this increased to 10% during the shortage (adjusted p<0.05). The percent of parents that acquired free infant formula from healthcare providers significantly decreased from 40% before to 20% during the shortage (adjusted p < 0.01) but reliance on shipments of formula from friends or family within the U.S. significantly increased from 11% before to 25% (adjusted p<0.01) (Figure 3).
Eighty-one percent of parents switched infant formulas during the shortage, and of these individuals, 87% switched because they could not find the formula they typically used. Thirty-four percent of parents who switched infant formula brands or types during the shortage, switched infant formulas 3 to 5 times. Twenty percent of parents reported having 4 weeks-worth or more of infant formula at home during the infant formula shortage. Over a 24-hour period, 29% of parents visited four or more stores and 26% of parents traveled more than twenty miles to one store to purchase infant formula. In this study, 13.9% of parents reported using Operation Fly during the shortage (Table S2).
3.4. Infant Outcomes to the Infant Formula Shortage
Sixty-one percent of parents who switched formulas, reported that their infants had one or more problems in response to switching. A sub-analysis revealed that infants requiring specialty formulas experienced more problems than infants who did not require specialty formulas. Compared with non-specialty formula users, more parents whose infants required specialty formulas reported their infants experienced any problems (unadjusted p = 0.045) and specifically vomiting (unadjusted p = 0.026) in response to switching formulas (Figure 4).
3.5. Parental Use of Resources and Sentiments
The most used resources used by parents for support and guidance in feeding their infants during the shortage were the following: social media (51%), healthcare providers (48%), relatives or friends (43%), lactation consultant or lactation counselor (30%), infant formula companies’ websites (21%), blogs (18%), health authorities’ websites (18%), media (news or magazines including TV broadcast, online articles) (16%) and breastfeeding support groups (14%) (Figure 5A). Parents’ mean ratings for the helpfulness of each resource were: social media (7.8), healthcare providers (6.8), relatives or friends (7.6), lactation consultant or lactation counselor (6.2), infant formula companies’ websites (6.0), blogs (6.5), health authorities’ websites (6.0), media (4.5) and breastfeeding support groups (6.2) (Figure 5B). Of the parents that used healthcare providers for support, 27% received recommendations to switch formulas, 25% received formula samples and 16% received information about lactation and breastfeeding from their infant’s healthcare provider (Figure S4).
To assess parents’ unmet needs, they were asked to rate the potential helpfulness of activities that would help families feed their infants in the “near future”. The highest mean scores for these future activities include: more infant formula brands are available through WIC (9.6); parents can choose any infant formula brand without restrictions (9.1); health insurance and Medicare pay for all U.S. brands (8.9) and imported brands (8.4) of infant formula; information is available online that describes formula brands that meet infants’ unique health needs (8.8) and infant formula availability in stores (8.5); women receive free postpartum lactation support (8.8) and free prenatal lactation education (8.1) (Figure 6).
Regarding parents’ perceptions about the safety and quality of infant formula, the following percent of parents agreed or strongly agreed to these statements: ready-to-feed infant formula is safe for infants (80%), concentrated liquid infant formula is safe for infants (64%) and infant formula powder is safe for infants (89%). When asked how they related to some situations associated with the infant formula shortage, the following percent of parents agreed or strongly agreed to these statements: they did not have enough food to feed their infants (22%), concerned about what they would feed their infants if they stopped breastfeeding (83%), concerned about how their infants would tolerate a new infant formula that was available (91%), introduced solid food to their infants earlier than initially planned (16%) (Figure 7).
3.6. Breastfeeding Goals, Experience and Support
Because exclusive human milk feeding is recommended for infants during the first six months of life, female parents were asked questions about their breastfeeding goals, experience, and support. Nearly 81% of female parents had plans to exclusively breastfeed and 87% of female parents reported that they did not exclusively breastfeed as long as they had planned (Table S3).
With respect to breastfeeding support, 86.3% of female parents received breastfeeding support from a lactation professional within 72-hours postpartum and 18% of these parents paid out-of-pocket for lactation support services. With respect to receiving prenatal and early postpartum lactation support, 49% of female parents reported that they participated in a prenatal breastfeeding support group or class and 35% of female parents reported that they participated in a postpartum breastfeeding support group or class (Table S3). Parents’ mean ratings for helpfulness of prenatal and postpartum breastfeeding support group or class were 5.5 and 6.7, respectively (Figure S5). To assess the unmet breastfeeding support needs of parents who did not participate in a prenatal or postpartum breastfeeding support groups/classes, free prenatal and postpartum breastfeeding support groups or classes were scored 7.5 and 7.9, respectively, for their potential helpfulness (Figure S6).
3.7. Non-Structured Qualitative Assessment
This study collected qualitative data in an opened-ended question that asked respondents how they dealt with the infant formula shortage and the actions they feel should be taken by health authorities, food companies, and the government that could help them feed their infants during this crisis and prevent future crises (Table S4). Open-ended responses were shared by 124 parents and converted into a word cloud. The following were the most frequently used word cloud terms in descending order: formula, breastfeeding, pumping, prevent, stressful, access, imported, impaired choice, breastfeeding challenges, and low milk supply (Figure S7).
4. Discussion
The 2022 infant formula shortage was an unprecedented infant feeding crisis that led to nationwide food and nutrition insecurity in our most vulnerable population [7]. This study used a semi-structural questionnaire to investigate infant feeding practices, parents’ consumer behaviors and infant outcomes in response to the shortage to identify areas within government, regulatory and healthcare systems and policies that could result in a resilient infant food system.
The use of human milk from informal sharing, homemade infant formula, diluted formula, or expired infant formula was low in this population and did not change in response to the infant formula shortage. These findings are in contrast to Cernioglo et al. that reported a significant increase in the use of any unsafe infant feeding practice from 8% before the infant formula shortage to nearly half during the infant formula shortage [16]. The differences in use of unsafe infant feeding practices between Cernioglo et al., and our study may reflect the differences between the two populations’ socioeconomic statuses and supported by Marino et al., that reported higher use of unsafe infant feeding practices by families from lower compared with higher income communities[18].
While the use of cow milk, goat milk, and alternative milk beverages were low (<1%) and did not change, other complementary foods such as baby cereal was used by 7% of parents before and during the shortage, and the use of other dairy such as yogurt increased from 2% before to 6% during the shortage. These data are consistent with a cross-sectional analysis by Marino and co-workers for which 10% of infant formula users added cereal to formula and 7% fed their infants with solid foods instead of feeding infant formula [18].
The use of pasteurized donor human milk was low (2-4%) and did not significantly change in response to the shortage. Use of pasteurized donor human milk in our study was lower than a recent cross-sectional study of 2,315 individuals by DiMaggio and colleagues that reported 8% of survey respondents reported using donor milk [23]. Similar reports were made by the Human Milk Bank Association of North America (HMBANA) which experienced a high demand for donor milk during the 2022 infant formula shortage [19]. However, our data are consistent with a generally low use of pasteurized donor human milk in mostly term and healthy infants which is largely reserved for premature and very low birthweight infants.
Approximately 80% of infants were combination feeders (mother’s own breast milk and formula) and unexpectedly, use of infant formula significantly increased during the shortage when out-of-stock rates climbed as high as 90% in some states. This study found 14% of parents acquired imported formulas through Operation Fly, however the survey did not prompt families to report how many units of formula they acquired so we are unable to estimate the impact of the federal program. Additionally, in response to the shortage, the number of parents who acquired free infant formula samples from healthcare providers decreased, yet more parents purchased infant formula via social media and acquired formula from shipments sent from family and friends in the United States. These data are consistent with a recent qualitative study that reported white female parents expressed positive feelings for having supportive family members and friends who helped them find formula which was not described by any Black, or SNAP or WIC eligible participants [20]. This study also revealed that about 20% of parents stockpiled infant formula during the shortage with 4 weeks-worth or more of infant formula at home. The American Academy of Pediatrics’ recommends purchasing no more than a 10-day to 2-week supply of formula to prevent hoarding [21].
Consumer behavior questions were asked to investigate the burden parents experienced in navigating the May 2022 infant formula shortage. Approximately 90% of parents used U.S. brands of infant formula which is consistent with the dominance of the infant formula market by U.S. companies [33]. Approximately 80% of parents switched infant formula types or brands during the shortage, and of these individuals, 87% switched because they could not find the formula they typically used. One third or more of parents switched infant formula brands or types 3 to 5 times, and over a 24-hour period visited four or more stores and traveled more than twenty miles to one store to purchase infant formula. These data are similar to a recent report from an online survey in 1,070 U.S consumers, of which one-third had to tried to purchase formula during the May 2022 infant formula shortage and of those consumers, 30% reported purchasing formula at multiple stores [22]. A recent qualitative study by Sylvetsky and colleagues reported that parents spent hours searching for formula by driving from store to store and searching online during the May 2022 infant formula shortage [20]. These data identify a high burden to parents and potentially those from low-income communities for which transportation and time are barriers in accessing food [23].
Switching infant formula brands and types reduced infant quality of life and especially in infants that relied on specialty formulas. Approximately 60% parents who switched formulas reported that their infants had one or more problems in response to switching infant formulas. In a sub-group analysis, the number of infants that experienced problems in response to switching formulas was higher in infants requiring specialty formulas compared with infants that did not require specialty formulas. These data may be explained in part to the increased use of intact cow’s milk formula during the shortage. These observations are supported by Marino et al., that found two-thirds of parents whose infants relied on specialty formulas reported difficulties accessing these formulas during the COVID-19 pandemic [18].
Parents relied on several resources to navigate the infant formula shortage with social media and healthcare providers (50%) as the most used resources followed by relatives or friends (43%) about one-third of parents used a lactation consultant or lactation counselor. These data are much lower compared with the CDC and FDA’s 2006 Infant Feeding Practices Study II (IFPSII) in which about 80% of parents acquired information about infant feeding practices from healthcare professionals, followed by relatives or friends, and books or videos [17]. Discrepancies in the data may result in the size and composition of each study. IFPSII enrolled a larger and more representative sample size of 2,000 women across the nation relative to this study’s smaller sample size of 178. The mean helpfulness scores of these resources were moderate with social media scoring the highest suggesting social media as a powerful tool for diet and health education and support and confirmed by other studies [16,20]. Parents’ mean helpfulness scores of future activities that would facilitate feeding infants in the “near future” include freedom to choose infant formula brands, health insurance coverage for infant formula, online resources describing formula types or brands that meet infants’ unique health needs and free universal prenatal lactation education and postpartum lactation support. These activities highlight facilitator that would address the barriers in infant feeding that are summarized in the word cloud.
Because exclusive human milk feeding is recommended for infants during the first six months of life, female parents were asked questions about their breastfeeding goals, experience, and support. Most (80.5%) female parents planned to exclusively breastfeed their infants, however 87% did not meet their exclusive breastfeeding goals. These data are fairly consistent with the CDC Breastfeeding Report Card for which most U.S. infants (84.1%) have ever consumed any breast milk but only 25% of infants meet the national recommendations of exclusive breastfeeding through 6 months of life [24]. These data suggest that while most parents aim to meet national health recommendations to exclusively breastfeed their infants until 6 months of age, they are unable or choose not to. There are a several factors that explain why women are unable to meet their breastfeeding goals from lack of federal paid family and medical leave that prevent women from having the time and support to initiate and sustain breastfeeding; a lack of flexibility and privacy for mothers to breastfeed or pump while at work; and barriers in affording or accessing prenatal lactation education and postpartum lactation support which are not part of standard care [25,26,27].
Female participants were asked about their experience with prenatal lactation education and postpartum lactation support. Approximately 50% of female parents participated in a prenatal breastfeeding support group or class and 35% of female parents participated in a postpartum breastfeeding support group or class. The helpfulness scores for these two activities were low (5.5 and 6.7, respectively), however, their mean helpfulness scores were higher (7.5 and 7.9, respectively) by female parents who did not participate in these activities. These data suggest there is a high unmet need for universal and free breastfeeding education and support that are critical for increasing breastfeeding intention, initiation, duration and exclusivity [28,29].
This is the first report of infant feeding outcomes and consumer behavior in response to the May 2022 infant formula shortage with different limitations and strengths. The limitations include the study design which was retrospective which is at risk for high recall errors. Specifically, parents completed the survey 7-8 months following the height of the May 2022 infant formula shortage. This may explain in part the fewer number of parents reporting use of unsafe infant feeding practices compared to a more recent prospective cross-sectional study in a similar population [30]. Second, our target population included parents who subscribed to the Bobbie Labs listserv and limits the generalizability of the results. Nearly 80% of respondents were derived of largely white communities with annual household incomes equal to or greater than $100,000, and not representative of U.S. families that were severely impacted by the infant formula shortage. Notably, our survey failed to capture many responses from individuals who represent families from low-income, black, and Hispanic communities that were hit the hardest by the shortage [10]. There are also several strengths of this study. First, data from this cross-sectional study was collected from a large sample of parents who resided across the United States which improves the study’s generalizability. Second, nearly 90% of respondents reported being “extremely sure” about their answers choices regarding their infant’s feeding practices before and during the shortage demonstrating potential low recall biases. Additionally, 70% of parents answered the open-response question which suggests high engagement with the survey and a proxy for high-quality data. Finally, the survey collected a combination of categorical and continuous data on infant feeding, parental experiences and sentiments and infant outcomes that could identify areas in policy and educational strategies to assist families in averting future infant feeding crises. We propose a call to action to government, regulatory, health and workplace policies that prioritize infant feeding practices that deliver optimal nutrition, safety, and food security. First, the U.S. infant formula supply is controlled by U.S. trade and regulatory policies that result in a U.S. infant formula monopoly [31]. High tariffs on formula thwart the import of infant formula to the U.S. and federal policies that govern the manufacture and labeling of infant formula exclude them from enter the U.S. legally [4]. Systemic failures that reduce infant formula diversification and support a monopoly inequitably impacted low-income communities such as WIC recipients and nutritionally vulnerable infants [4]. There is recent temporary solution with recent modifications to the Access to Baby Formula Act that becomes law in February 2024. This amendment to the Child Nutrition Act of 1966 will develop a waiver authority to address emergencies, disasters, and supply chain disruptions by ensuring WIC state offices can secure supplies from additional manufacturers outside of their contracts. Yet, this law is a stopgap and prevention of another feeding crisis will depend on systemic changes to healthcare policies that also protect the infant feeding system with access to banked donor milk and lactation education and support. The accessibility and growth of donor milk banking services are thwarted in part to a lack of federal public health policies that integrate donor milk banking or regulate its operations. Finally, the U.S. government and healthcare system should commit to implementing policies that prioritize lactation education and support. The suboptimal breastfeeding rates in the U.S. and within low-income communities are a result of a lack of federal paid family and medical leave; a lack of flexibility and privacy for mothers to breastfeed or pump while at work; and difficultly affording lactation services, which are not part of standard care. The future of individual, community and societal health rely on optimal early life nutrition that is resilient and equitable for all.
5. Conclusions
This study is the first to report infant outcomes, parental consumer behavior and needs in infant feeding in response to the 2022 infant formula shortage. Most parents in this study switched infant formula brands or types because they could not find the formula they typically used. One third of parents who switched formulas had changed formula brands or types of multiple times; frequently visited stores and traveled long distances to purchase formulas. Infant formula use increased in response to the infant formula shortage which suggests this population had the resources and support unlike families from low-income communities that used unsafe infant feeding practices. The most vulnerable infants who required specialty formulas had experienced more problems to switching formulas. While parents used social media, healthcare providers and relatives/friends for support during the shortage, these resources’ helpfulness scores were suboptimal. Parents reported that wide availability of infant formula options, infant formula covered by insurance without restrictions, free, universal prenatal lactation education, and postpartum lactation support as solutions to the crisis. Our report highlights barriers in safely feeding infants and presents potential health disparities in families from low-income communities and with nutritionally vulnerable infants. Our results demonstrate the need for systemic changes to policies that diversify and fortify the infant food supply, ensure equitable and reliable access to banked donor milk, and integrate universal prenatal and postnatal breastfeeding support in healthcare are critical to protect the most vulnerable population from another feeding crisis.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: Map of parental residence across thirty-seven states; Figure S2: Percent of parents that reported reasons their infants required specialty formulas; Figure S3: Manufacturing locations of typical formulas consumed by infants before and during the infant formula shortage; Figure S4: Guidance or support provided by healthcare providers to parents during the infant formula shortage; Figure S5: Scores in helping female parents achieve their breastfeeding goals with prenatal and postpartum breastfeeding classes or support groups that they had completed; Figure S6: Scores in helping women achieve their breastfeeding goals with future free prenatal and postpartum breastfeeding classes or support groups; Figure S7: Word cloud that summarizes parents’ open-ended responses; Table S1: Words, themes and key phrases used to generate a word cloud; Table S2: Practices experienced by parents in response to the infant formula shortage; Table S3: Breastfeeding experience and goals; Table S4: Open-ended responses by participants.
Author Contributions
Conceptualization, J.T.S.; methodology, J.T.S., K.C., D.M.D. and A.F.P.; investigation, J.T.S. and K.C.; formal analysis and visualization, J.T.S., K.C. and K.D-M.; interpretation of data, J.T.S., K.C., K.D-M., and M.W.; writing—original draft preparation, J.T.S., K.C., K.D-M., M.W.; writing—review and editing J.T.S., K.C., K.D-M., M.W., D.M.D. and A.F.P.; supervision and funding acquisition, J.T.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the 2020 UC Davis Chancellor’s Innovation Award and a gift from Bobbie.
Institutional Review Board Statement
The University of California Davis Institutional Review Board approved all aspects of the study (IRB #: 1920147). All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We thank the parents in this study for taking their time to complete the survey and to share their very thoughtful and heartfelt responses.
Conflicts of Interest
J.T.S. received a gift from Bobbie to support this project. Bobbie was not involved in analyzing the data generated from this or drafting this manuscript. D.M.D. and A.F.P. are medical consultants to Bobbie Labs.
References
- Jaffe, S. US infant formula crisis increases scrutiny of the FDA. The Lancet 2022, 399, 2177–2178. [Google Scholar] [CrossRef] [PubMed]
- Food, U.; Administration, D. FDA Investigation of Cronobacter Infections: Powdered Infant Formula (February 2022). FDA. Available online at: https://www.fda.gov/food/outbreaks-foodborne-illness/fda-investigation-cronobacter-infections-powdered-infant-formula-february-2022 (accessed October 15, 2022) 2022.
- Abrams, S.A.; Duggan, C.P. Infant and child formula shortages: now is the time to prevent recurrences. The American Journal of Clinical Nutrition 2022, 116, 289–292. [Google Scholar] [CrossRef]
- Naylor, L. The monstrosity of the corporate control of food shortages: The geopolitics of the 2022 infant feeding crisis in the United States. Geoforum 2022, 137, 146–150. [Google Scholar] [CrossRef]
- Paris, M. One in Five US States Is 90% Out of Baby Formula. Bloomberg 2022.
- Rupnicki, S. Breastfeeding Report Card United States, 2020. CDC: Atlanta, GA, USA 2020.
- Sandoval Edgar, M., Amanda, Ngo, Amanda. A Baby Formula Shortage Leaves Desperate Parents Searching for Food. The New York Times 2022.
- Doherty, T.; Coutsoudis, A.; McCoy, D.; Lake, L.; Pereira-Kotze, C.; Goldhagen, J.; Kroon, M. Is the US infant formula shortage an avoidable crisis? The Lancet 2022, 400, 83–84. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture, E.R.S. U.S. Department of Agriculture, E.R.S. Infants in USDA’s WIC Program consumed an estimated 56 percent of U.S. infant formula in 2018. 2022.
- Jung, J.; Widmar, N.O.; Ellison, B. The Curious Case of Baby Formula in the United States in 2022: Cries for Urgent Action Months after Silence in the Midst of Alarm Bells. Food Ethics 2023, 8, 4. [Google Scholar] [CrossRef] [PubMed]
- Rossen, L.M.; Simon, A.E.; Herrick, K.A. Types of Infant Formulas Consumed in the United States. Clin Pediatr (Phila) 2016, 55, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Abrams, S.A. With the baby formula shortage, what should I do if I can't find any? American Academy of Pediatrics 2022.
- Parents, F.F.A. Caregivers to Not Make or Feed Homemade Infant Formula to Infants| FDA.
- Leung, A.K.; Sauve, R.S. Whole cow's milk in infancy. Paediatrics & child health 2003, 8, 419–421. [Google Scholar]
- Meek, J.Y.; Noble, L. Breastfeeding and the use of human milk. Pediatrics 2022.
- Cernioglo, K.; Smilowitz, J.T. Infant feeding practices and parental perceptions during the 2022 United States infant formula shortage crisis. BMC Pediatrics 2023, 23, 320. [Google Scholar] [CrossRef] [PubMed]
- Fein, S.B.; Grummer-Strawn, L.M.; Raju, T.N. Infant feeding and care practices in the United States: results from the Infant Feeding Practices Study II. Pediatrics 2008, 122, S25–S27. [Google Scholar] [CrossRef] [PubMed]
- Marino, J.A.; Meraz, K.; Dhaliwal, M.; Payán, D.D.; Wright, T.; Hahn-Holbrook, J. Impact of the COVID-19 pandemic on infant feeding practices in the United States: Food insecurity, supply shortages and deleterious formula-feeding practices. Maternal & Child Nutrition 2023, e13498.
- Ceron, E. Demand Is Up at Human Milk Banks Amid Baby Formula Crisis. Bloomberg 2022.
- Sylvetsky, A.C.; Hughes, S.A.; Kuttamperoor, J.T.; Moore, H.R.; Murphy, J.; Sacheck, J.; Smith, E.R. Mothers’ Experiences During the 2022 Infant Formula Shortage in Washington D.C. Maternal and Child Health Journal 2023, 10.1007/s10995-023-03860-9. [CrossRef]
- Pediatrics, A.A.o. Baby Formula Shortages: What Parents Need to Know. Availabe online: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://publications.aap.org/DocumentLibrary/Solutions/PPE/BabyFormulaShortages_ppe_document263_en.pdf (accessed on.
- Kalaitzandonakes, M.; Ellison, B.; Coppess, J. Coping with the 2022 infant formula shortage. Preventive Medicine Reports 2023, 32, 102123. [Google Scholar] [CrossRef] [PubMed]
- Vilar-Compte, M.; Burrola-Méndez, S.; Lozano-Marrufo, A.; Ferré-Eguiluz, I.; Flores, D.; Gaitán-Rossi, P.; Teruel, G.; Pérez-Escamilla, R. Urban poverty and nutrition challenges associated with accessibility to a healthy diet: a global systematic literature review. International Journal for Equity in Health 2021, 20, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Control, C.f.D.; Prevention. Breastfeeding Report Card United States, 2020. Atlanta, GA: Centers for Disease Control and Prevention, 2020. 2020.
- Bookhart, L.H.; Joyner, A.B.; Lee, K.; Worrell, N.; Jamieson, D.J.; Young, M.F. Moving beyond breastfeeding initiation: A qualitative study unpacking factors that influence infant feeding at hospital discharge among urban, socioeconomically disadvantaged women. Journal of the Academy of Nutrition and Dietetics 2021, 121, 1704–1720. [Google Scholar] [CrossRef] [PubMed]
- Chopel, A.; Soto, D.; Joiner, B.J.; Benitez, T.; Konoff, R.; Rios, L.; Castellanos, E. Multilevel factors influencing young mothers’ breastfeeding: a qualitative CBPR study. Journal of Human Lactation 2019, 35, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Lowe, N.K. The Surgeon General's call to action to support breastfeeding. Journal of Obstetric, Gynecologic & Neonatal Nursing 2011, 40, 387–389. [Google Scholar]
- McFadden, A.; Gavine, A.; Renfrew, M.J.; Wade, A.; Buchanan, P.; Taylor, J.L.; Veitch, E.; Rennie, A.M.; Crowther, S.A.; Neiman, S. Support for healthy breastfeeding mothers with healthy term babies. Cochrane database of systematic reviews 2017. [CrossRef]
- Balogun, O.O.; O'Sullivan, E.J.; McFadden, A.; Ota, E.; Gavine, A.; Garner, C.D.; Renfrew, M.J.; MacGillivray, S. Interventions for promoting the initiation of breastfeeding. Cochrane Database of Systematic Reviews 2016. [CrossRef]
- DiMaggio, D.M.; Du, N.; Porto, A.F. Nutritional and safety concerns of infant feeding trends. Journal of Pediatric Gastroenterology and Nutrition 2022, 74, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Evich, H.B. Duckworth Asks FTC to Examine Formula Market. POLITICO 2022.
Figure 1.
Infant feeding practices before and during the infant formula shortage. (A) Human milk and infant formulas. MOM = mother’s own milk; BM = breast milk; DHM: donor human milk; IF = infant formula. **p < 0.01 (n =178). (B) Complementary foods and beverages (n =178).
Figure 1.
Infant feeding practices before and during the infant formula shortage. (A) Human milk and infant formulas. MOM = mother’s own milk; BM = breast milk; DHM: donor human milk; IF = infant formula. **p < 0.01 (n =178). (B) Complementary foods and beverages (n =178).
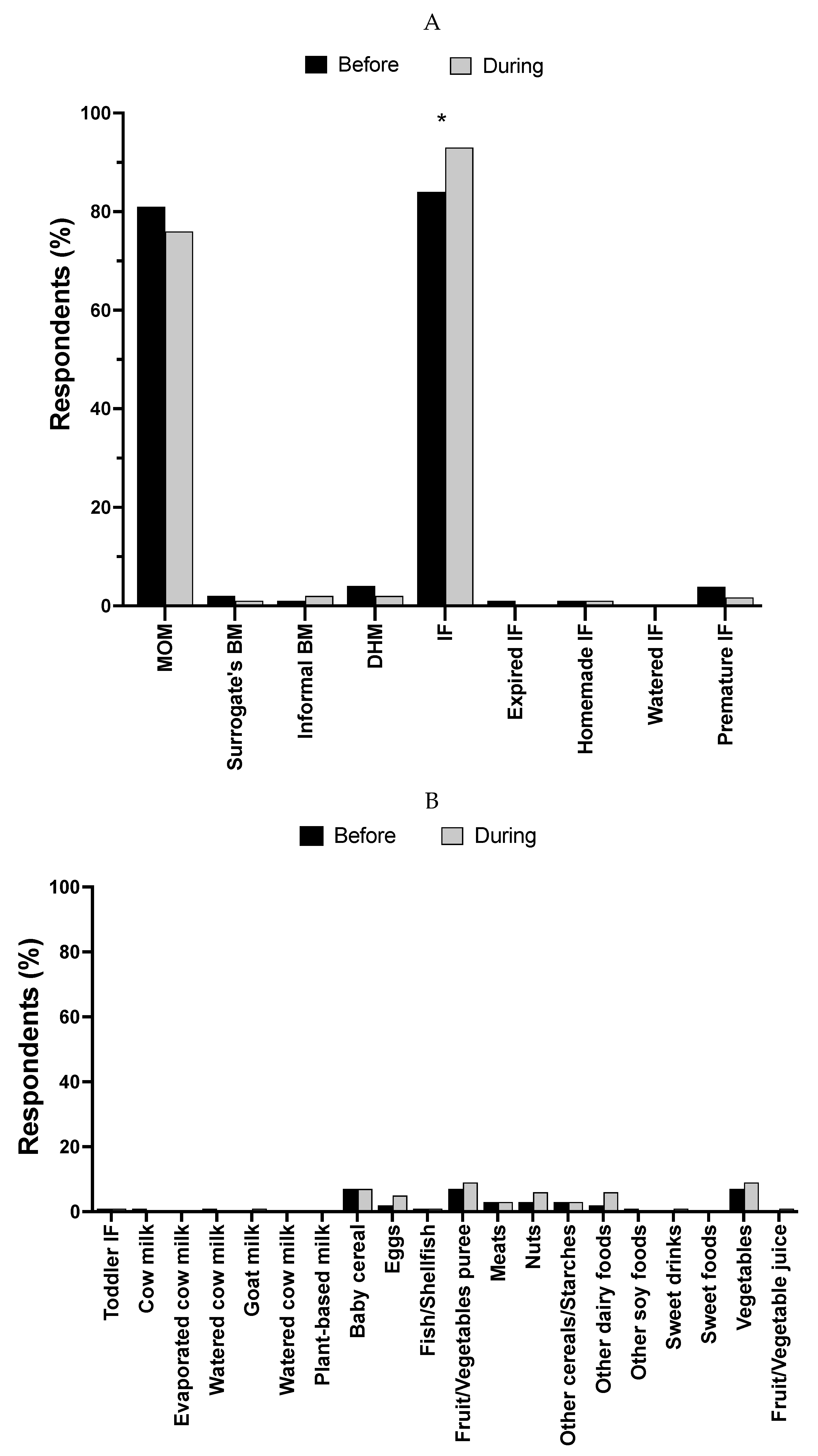
Figure 2.
Type of specialty infant formula used before and during the infant formula shortage. AA = amino acids; IF = infant formula. *p < 0.05 (n = 33).
Figure 2.
Type of specialty infant formula used before and during the infant formula shortage. AA = amino acids; IF = infant formula. *p < 0.05 (n = 33).
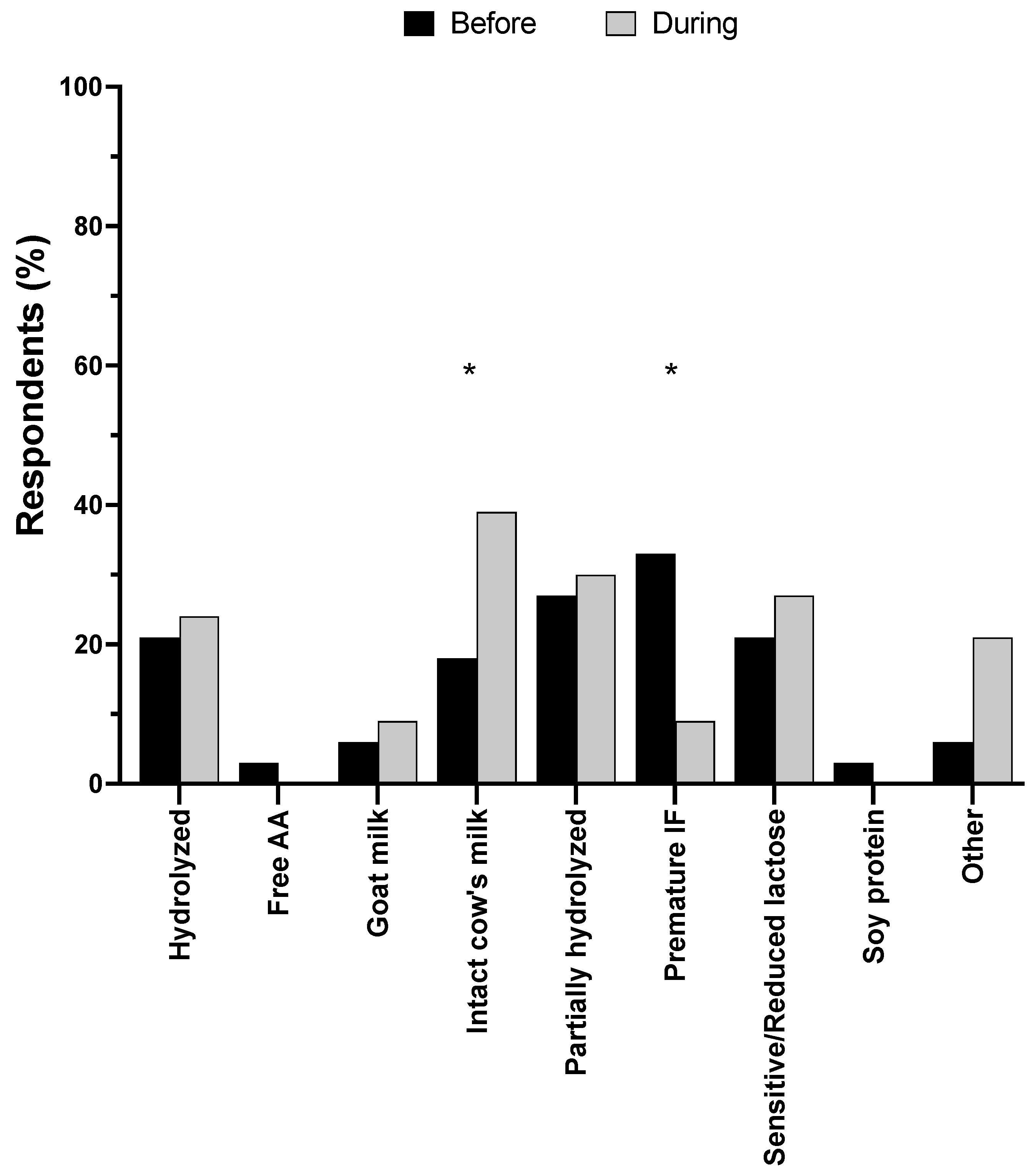
Figure 3.
Methods used by parents to obtain infant formula before and during the infant formula shortage. HCP = healthcare provider; FF = friends or family. *p <0.05; **p <0.01 (n = 178).
Figure 3.
Methods used by parents to obtain infant formula before and during the infant formula shortage. HCP = healthcare provider; FF = friends or family. *p <0.05; **p <0.01 (n = 178).
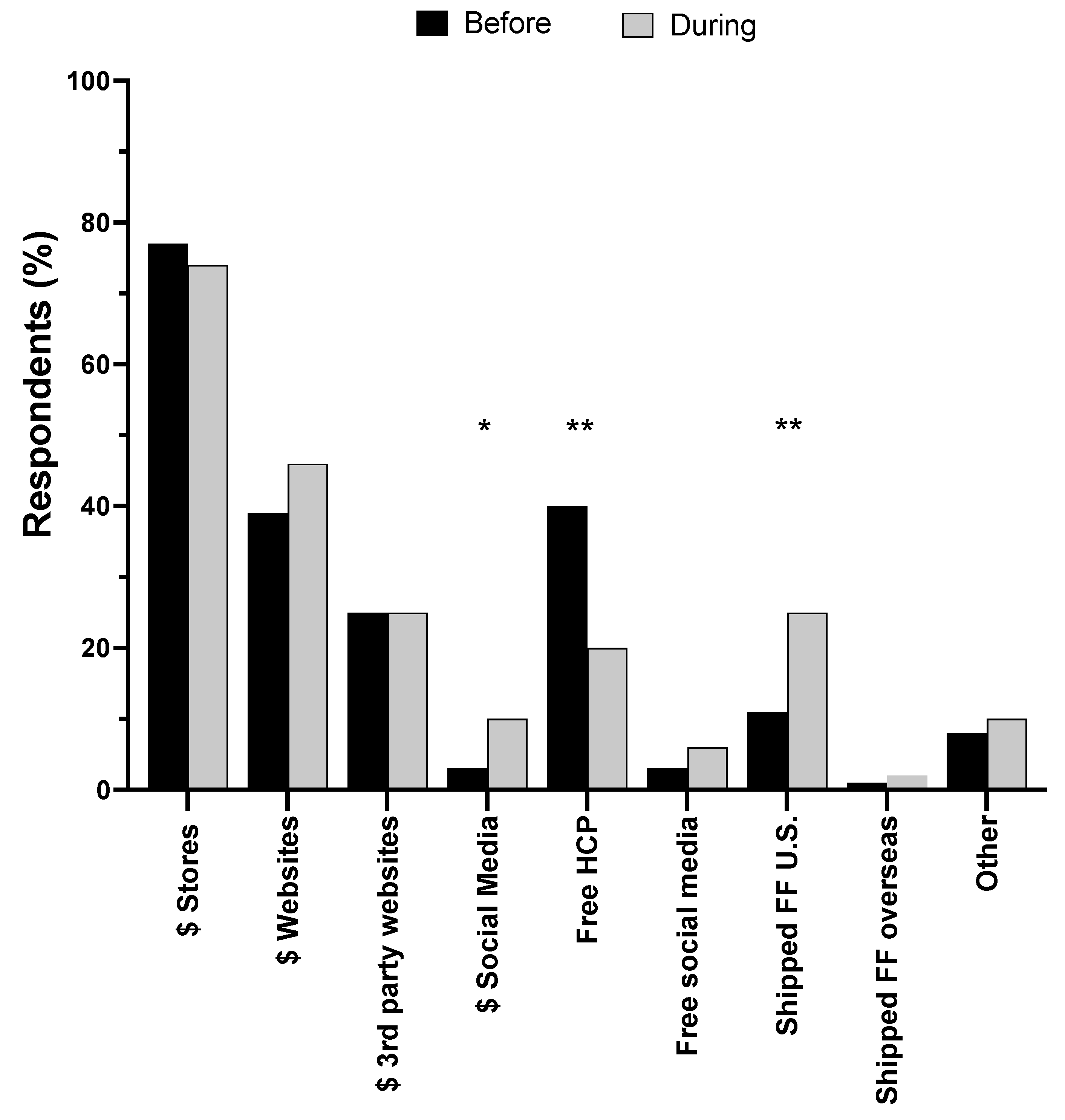
Figure 4.
Health outcomes experienced by infants during the shortage. Infants that required specialty formulas (n = 32) vs. infants that did not require specialty formulas (n =109).
Figure 4.
Health outcomes experienced by infants during the shortage. Infants that required specialty formulas (n = 32) vs. infants that did not require specialty formulas (n =109).
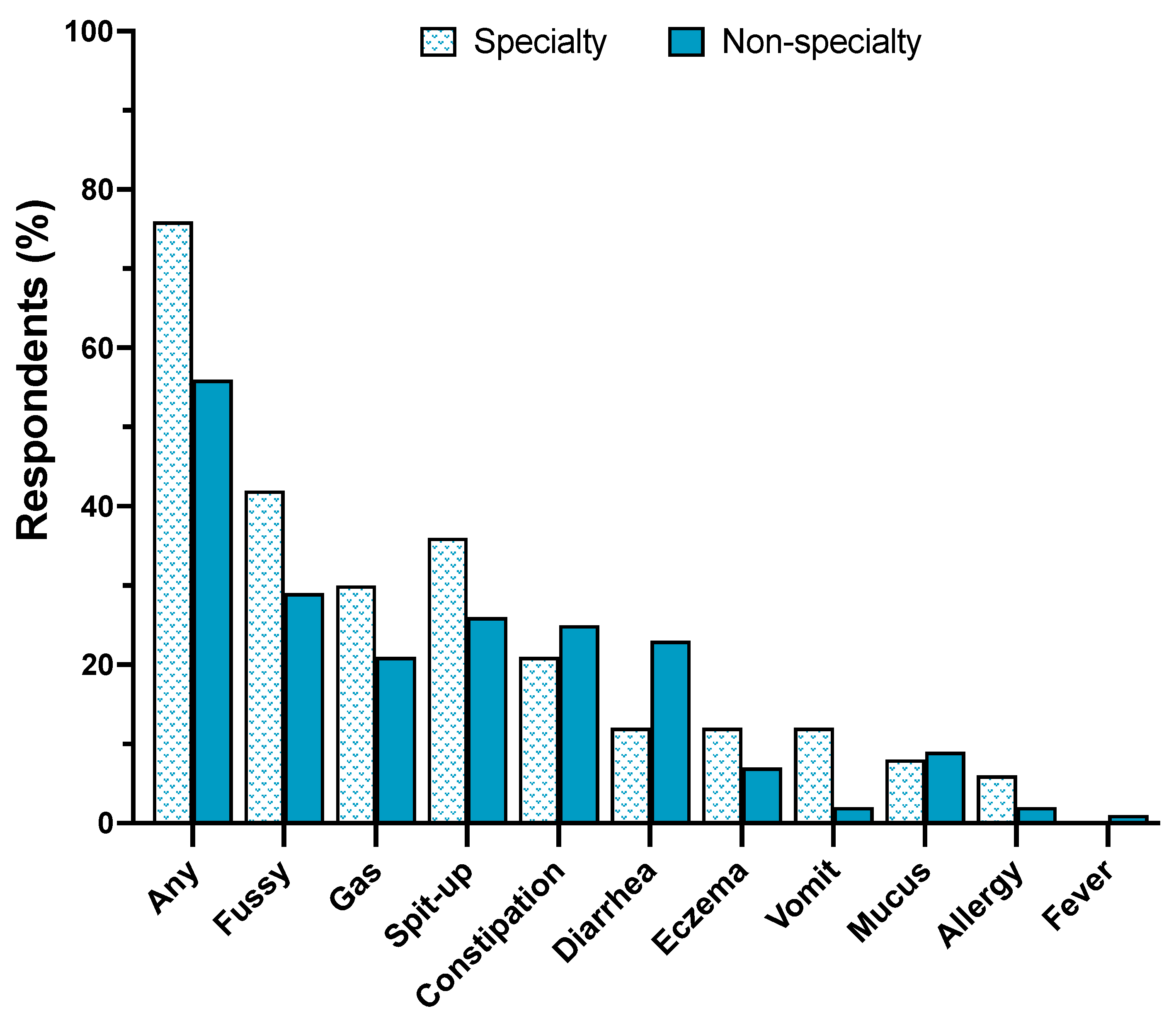
Figure 5.
Resources parents used to obtain guidance or support to help them feed their infants during the infant formula shortage. (A). Percent of parents that used each resource. (B). Parents’ ratings on the helpfulness of each resource. Dietitian ( n = 7); social media (n = 89); relatives or friends (n = 76); WIC (n = 3); nurse midwife (n = 9); HCP (n = 84); blogs (n = 33); doula (n = 10); birthing class (n = 12); BF support group (n = 24); LC (n = 53); websites IF companies (n = 37); websites health authorities (n = 32); websites other (n = 9); videos (n = 9); other (n = 4); news (n = 28); radio (n = 4); telephone (n = 1). HCP = healthcare provider; BF = breastfeeding; LC = lactation consultant or lactation counselor; IF = infant formula.
Figure 5.
Resources parents used to obtain guidance or support to help them feed their infants during the infant formula shortage. (A). Percent of parents that used each resource. (B). Parents’ ratings on the helpfulness of each resource. Dietitian ( n = 7); social media (n = 89); relatives or friends (n = 76); WIC (n = 3); nurse midwife (n = 9); HCP (n = 84); blogs (n = 33); doula (n = 10); birthing class (n = 12); BF support group (n = 24); LC (n = 53); websites IF companies (n = 37); websites health authorities (n = 32); websites other (n = 9); videos (n = 9); other (n = 4); news (n = 28); radio (n = 4); telephone (n = 1). HCP = healthcare provider; BF = breastfeeding; LC = lactation consultant or lactation counselor; IF = infant formula.
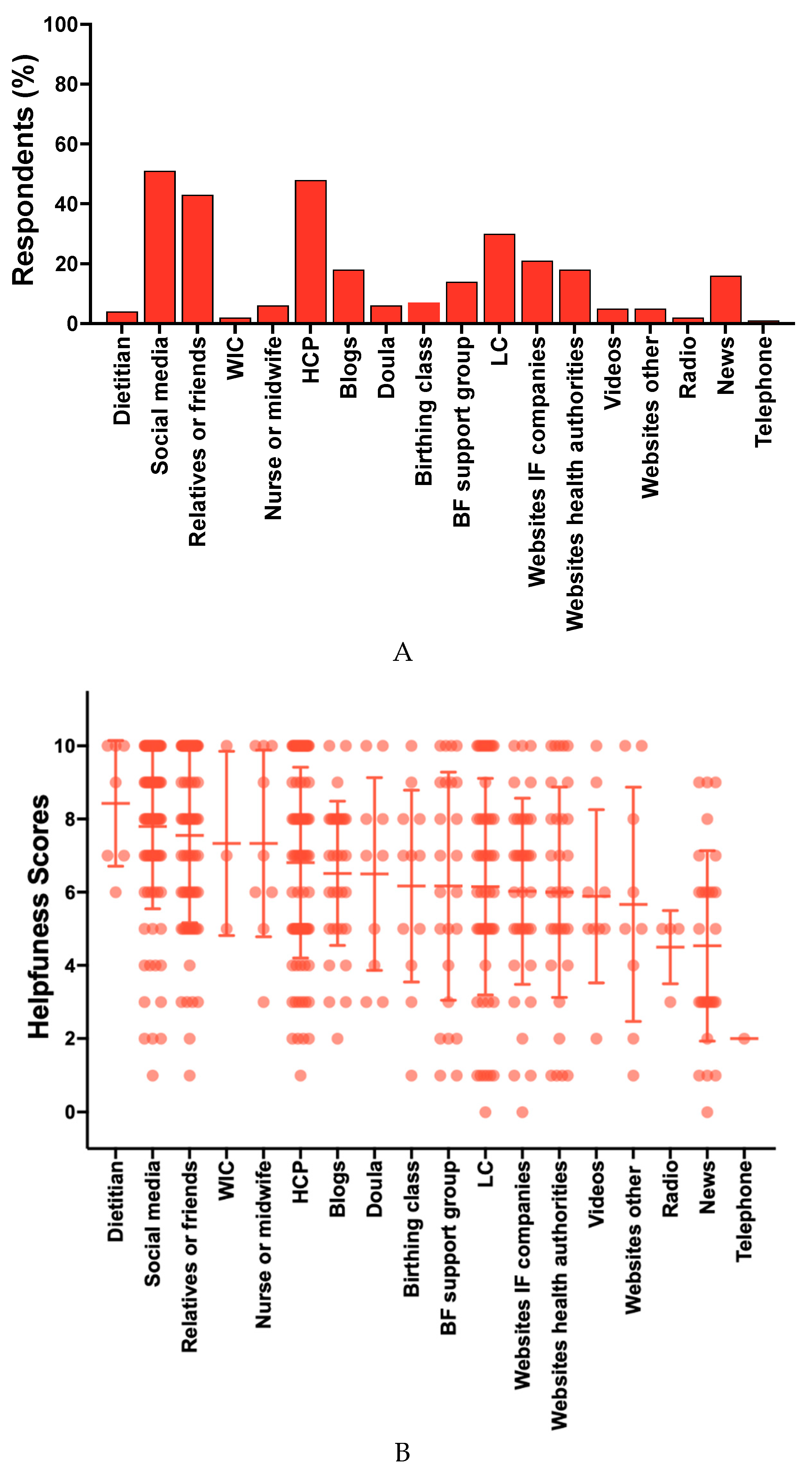
Figure 6.
Parents’ ratings on the helpfulness of activities that would help families feed their infants in the near future. More IF brands WIC (n = 9); no restrictions IF (n = 166); insurance pays for U.S. IF (n = 169); LC support postpartum (n = 169); info online lists similar IF (n = 171); more IF brands sold in U.S. (n =166); info online lists where to buy IF (n = 171); insurance pays for imported IF (n =167); LC education prenatal (n = 168); insurance pays for DHM (n = 152); bottle-feeding education (n = 169); free DHM (n = 148); stockpile prevention (n = 163); discounted DHM (n = 140); LC support relactation (n = 157); online videos relactation (n = 158); online homemade IF recipes (n = 154). IF = infant formula; LC = lactation consultant or lactation counselor; DHM = donor human milk.
Figure 6.
Parents’ ratings on the helpfulness of activities that would help families feed their infants in the near future. More IF brands WIC (n = 9); no restrictions IF (n = 166); insurance pays for U.S. IF (n = 169); LC support postpartum (n = 169); info online lists similar IF (n = 171); more IF brands sold in U.S. (n =166); info online lists where to buy IF (n = 171); insurance pays for imported IF (n =167); LC education prenatal (n = 168); insurance pays for DHM (n = 152); bottle-feeding education (n = 169); free DHM (n = 148); stockpile prevention (n = 163); discounted DHM (n = 140); LC support relactation (n = 157); online videos relactation (n = 158); online homemade IF recipes (n = 154). IF = infant formula; LC = lactation consultant or lactation counselor; DHM = donor human milk.
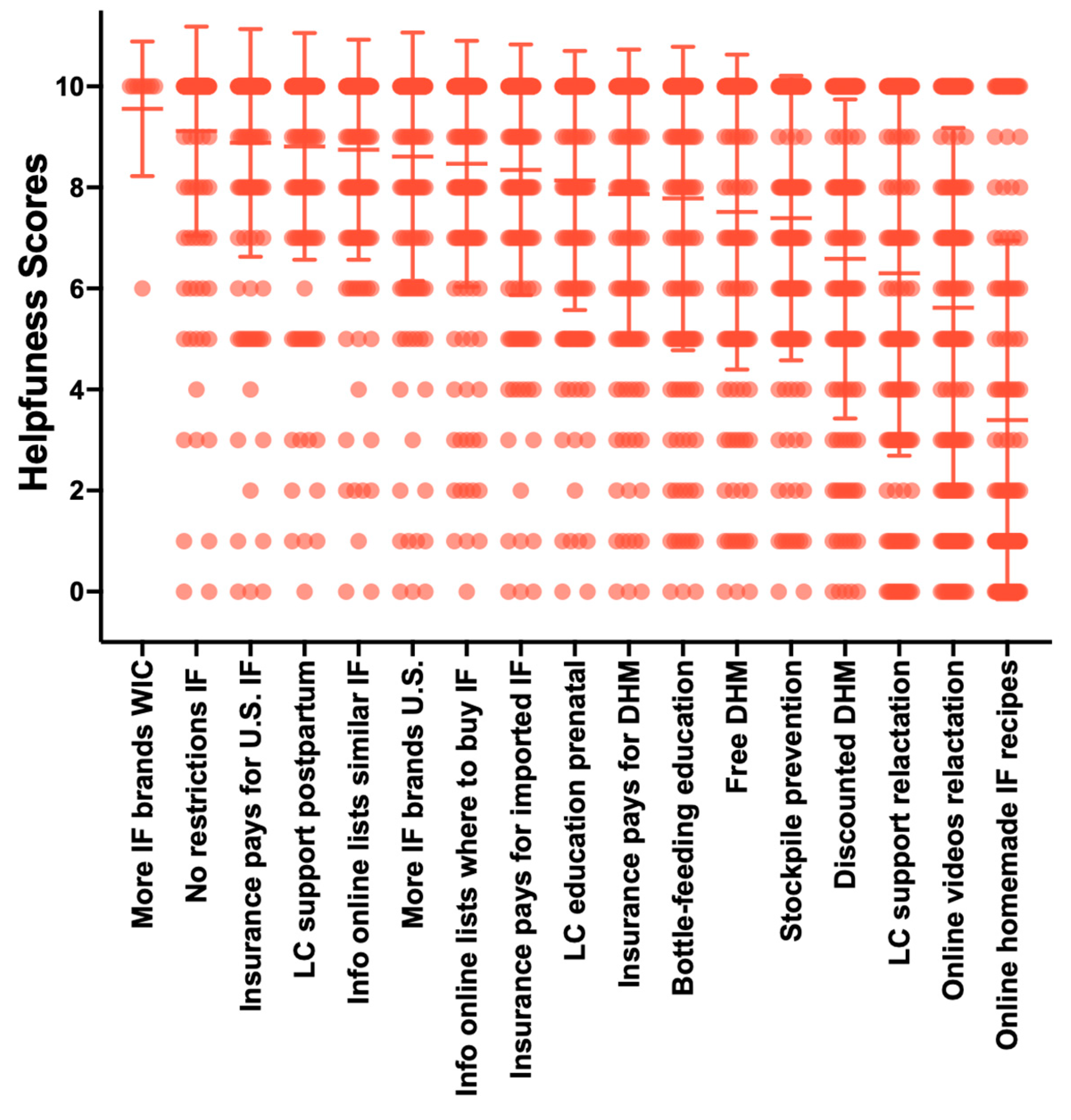
Figure 7.
Parents’ perceptions and relatedness to statements about infant formula. IF = infant formula; BF = breastfeeding. (n = 178).
Figure 7.
Parents’ perceptions and relatedness to statements about infant formula. IF = infant formula; BF = breastfeeding. (n = 178).
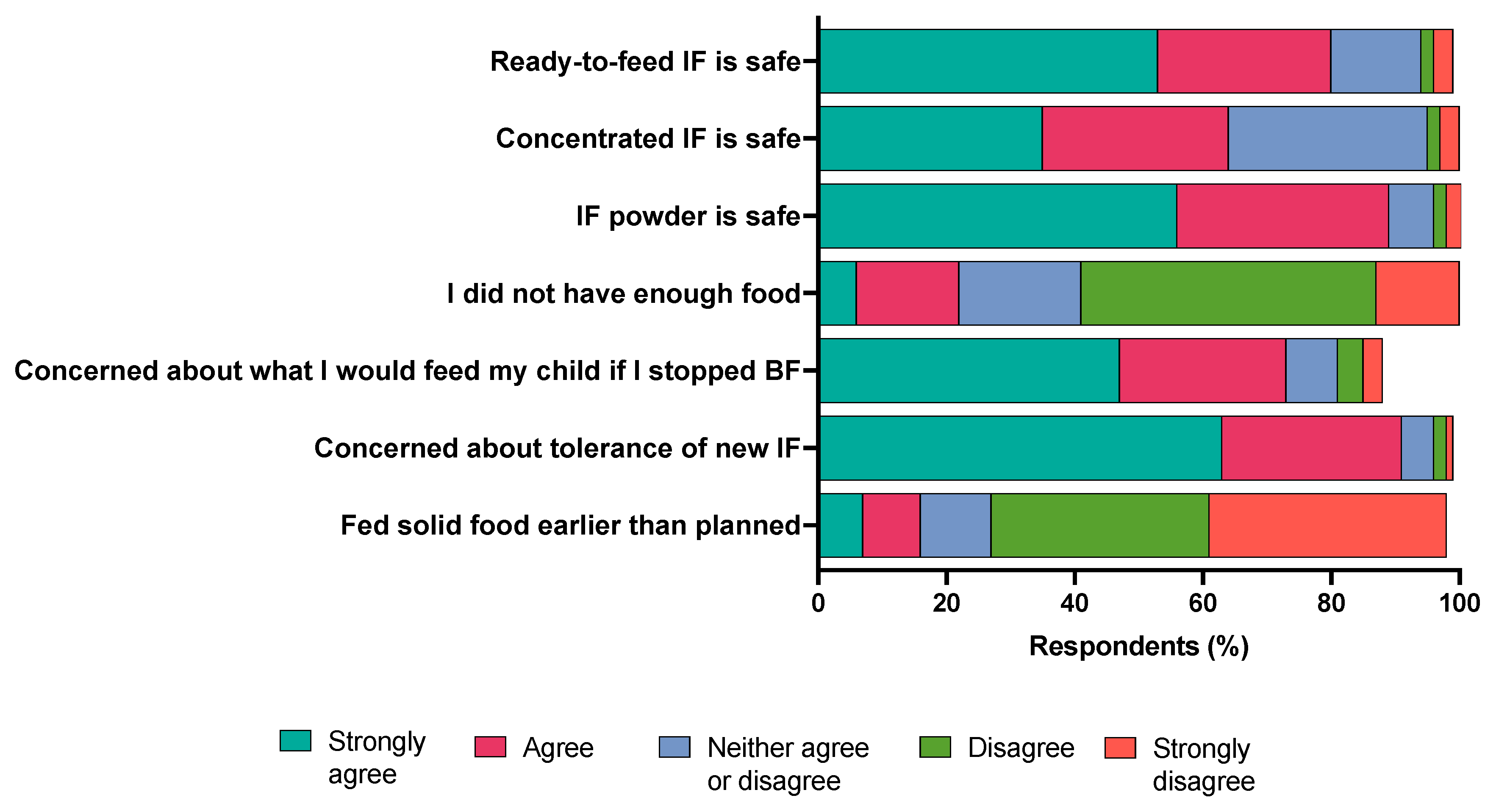

Table 1.
Parental characteristics.
| Parental Sex, % (n) | |
| Female | 93.3% (166) |
| Male | 5.1% (9) |
| Decline | 1.7% (3) |
| Ethnicity, % (n) | |
| Hispanic | 10.7% (19) |
| Non-Hispanic | 87.1 % (155) |
| Decline | 2.2% (4) |
| Race, % (n) | |
| White | 77% (137) |
| Asian | 12.4% (22) |
| Black/African American | 0.6% (1) |
| American Indian/Alaska Native | 0.6% (1) |
| Unsure | 0.6% (1) |
| 2 or more | 3.4% (6) |
| Decline | 3.9% (7) |
| Other | 1.7% (3) |
| Education, % (n) | |
| High School | 1.7% (3) |
| Some college | 2.2% (4) |
| Associate's degree | 8.4% (15) |
| Bachelor's degree | 44.4% (79) |
| Master's degree | 30.9% (55) |
| Professional or doctorate | 12.4% (22) |
| Marital Status, % (n) | |
| Married/unmarried couple | 92.7% (165) |
| Divorced/separated | 1.1% (2) |
| Never married | 6.2% (11) |
| Household size (people), % (n) | |
| 1 | 0.6% (1) |
| 2 | 0.6% (1) |
| 3 | 57.9% (103) |
| 4 | 29.2% (52) |
| 5 | 10.1% (18) |
| 6 | 0.6% (1) |
| 7 | 1.1% (2) |
| Household Income, % (n) | |
| Less than $25,000 | 1.1% (2) |
| $25,000 - $34,999 | 1.1% (2) |
| $35,000 - $49,999 | 1.7% (3) |
| $50,000 - $74,999 | 5.6% (10) |
| $75,000 - $99,999 | 7.3% (13) |
| $100,000 - $149,999 | 23% (41) |
| $150,000 - $199,999 | 20.2% (36) |
| More than $200,000 | 34.3% (61) |
| Unsure | 1.1% (2) |
| Decline | 4.5% (8) |
| Receiving WIC Benefits, % (n) | |
| Yes | 6.2% (11) |
| No | 93.3% (166) |
| Decline | 0.6% (1) |
Table 2.
Infant characteristics and female parental reproductive history.
| Mean ± SD | Range (weeks) | |
| Infant age | 10.2 ± 6.8 | 0.29 – 24.7 |
| Number of pregnancies, % (n)1 | ||
| 0 | 1.2% (2) | |
| 1 | 52.4% (87) | |
| 2 | 24.7% (41) | |
| 3 | 12.0% (20) | |
| 4 | 4.2% (7) | |
| 5 | 3.0% (5) | |
| 6 | 1.2% (2) | |
| 7 | 1.2% (2) | |
| Parity, % (n)1 | ||
| Primiparous | 68% (111) | |
| Multiparous | 32% (53) | |
| Infant relationship, % (n) | ||
| Pregnancy | 92.7% (165) | |
| Partner pregnancy | 5.1% (9) | |
| Surrogacy | 0.6% (1) | |
| Adoption | 1.1% (2) | |
| Decline | 0.6% (1) | |
| Multiple births, % (n) | ||
| Single | 96.1% (171) | |
| Twins | 3.9% (7) | |
| Infant gestational age at birth, % (n) | ||
| Term | 89.3% (159) | |
| Preterm | 10.7% (19) | |
| Ever breastfed, % (n)2 | ||
| Yes | 96.4% (159) | |
| No | 3.6% (6) | |
| Delivery location, % (n)3 | ||
| Birth center | 3.1% (5) | |
| Hospital | 96.3% (154) | |
| Other | 0.6% (1) | |
| Delivery mode, % (n)3 | ||
| C-section emergent | 14.4% (23) | |
| C-section scheduled | 21.3% (32) | |
| Vaginal | 64.4% (103) | |
| Infants transferred to NICU, % (n)3 | ||
| Yes | 13.1% (21) | |
| No | 86.9% (139) | |
| Skin to skin contact, % (n)3 | ||
| Yes | 89.4% (143) | |
| No | 8.8% (14) | |
| Unsure | 1.3% (2) | |
| Decline | 0.6% (1) | |
| Infant fed 72h postnatal, % (n) | ||
| Mom´s breast milk3 | ||
| Yes | 89.4% (143) | |
| No | 10.6% (17) | |
| Donor human milk3 | ||
| Yes | 9.4% (15) | |
| No | 90.6% (145) | |
| Infant formula3 | ||
| Yes | 52.5% (84) | |
| No | 47.5% (76) | |
| Other3 | ||
| Yes | 1.9% (3) | |
| No | 98.1% (157) |
1 Twelve respondents did not complete this question. 2 Thirteen respondents did not complete this question. 3 Eighteen respondents did not complete this question.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



