
Submitted:
29 January 2024
Posted:
31 January 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Type II pneumocytes are the target of SARS-CoV-2 which alters their redox homeostasis to increase reactive oxygen species (ROS). Melatonin (MT) has antioxidant proprieties and protects mitochondrial function. Here we evaluated whether the treatment with MT compensated for the redox homeostasis alteration in serum from COVID-19 patients. We determined oxidative stress (OS) markers such as carbonyls, glutathione (GSH), total antioxidant capacity (TAC), thiols, nitrites (NO2–), lipid peroxidation (LPO), and thiols groups in serum. We also studied the enzymatic activities of glutathione peroxidase (GPx), -S-transferase (GST), reductase (GR), thioredoxin reductase (TrxR), extracellular superoxide dismutase (ecSOD) and peroxidases. There was a significant increase in LPO and carbonyls (p≤0.03) and a decrease in TAC, NO2–, thiols, GSH, (p<0.001) in COVID-19 patients. The activities of the ecSOD, TrxR, GPx, GST, GR and peroxidases were decreased (p≤ 0.04). The treatment with MT favored the activity of the antioxidant enzymes which contributed to increase TAC and restored the lost redox homeostasis. MT also modulated glucose homeostasis functioning as a glycolytic agent and inhibited the Warburg effect. Thus, MT restores the redox homeostasis which is altered in COVID-19 patients and can be used as adjuvant therapy in the SARS-CoV-2 infection.
Keywords:
Melatonin
; SARS-CoV-2
; oxidative stress
; COVID-19
; redox homeostasis
; antioxidant enzymes
1. Introduction
The type 2 coronavirus that causes severe acute respiratory syndrome (SARS-CoV-2), responsible of the COVID–19 pandemic continues to wreak havoc the population around the world. As of January 2024, a total of 773,449,299 cases had been reported, causing 6,991,842 deaths, despite the administration of 13,59 billons doses of vaccines according to the WHO Coronavirus (COVID-19) Dashboard. Alveolar epithelial type 2 cells are the first target of the SARS-CoV-2 infection through the attachment of the S protein of the virus with the angiotensin-converting enzyme 2 (ACE2) receptor. The serine protease TMPRSS2 [1], facilitates the fusion of the viral membrane with the cellular membrane of the type II pneumocytes, and subsequently the virus hijacks the cellular machinery to complete the replication of new virions [2]. In this process, the host progressively triggers a cytokine storm through the innate immune system to try to counteract the infection, resulting in excessive systemic inflammation which is accompanied by an increase in the radical oxygen species (ROS), lactate creatinine, hyperferretinemia, lymphopenia, and kinase dehydrogenase. The ROS over production induces in turn, the activation of NFkB that promotes an increased production of cytokines which enhance the inflammatory response leading to a positive feedback loop, that promotes acute lung injury (ALI), which rapidly progresses to acute respiratory distress syndrome (ARDS) leading to COVID–19 [3]. The clinical presentations of COVID−19 range from asymptomatic cases to severe pneumonia associated with ARDS and cardiogenic shock. The severe forms are more often present in the elderly population, and in patients with the chronic pathologies that comprise the metabolic syndrome [4].
Despite the availability of various antiviral agents and various vaccines against SARS-CoV-2, the search for adjuvant therapies that can contribute to reduce the severity of the infection through clinical and basic studies continues, with the aim of lowering the viral load that is the source and origin of chronic inflammation, the cytokines storm and the excessive ROS production [5]. In this sense, the use of antioxidants such as melatonin (MT) could decrease the exacerbated inflammatory response, the cytokine storm, the oxidative stress (OS) and correct the alteration in redox homeostasis.
MT, (N-acetyl-5-methoxytryptamine) is an indoleamine, synthesized from the amino acid serotonin. The enzymes that participate in its synthesis are arylalkylamine N-acetyl transferase that converts serotonin to N-acetyl serotonin, which is then converted to MT by acetyl serotonin methyl transferase [6]. MT is also an endocrine molecule secreted by the pineal gland in response to darkness associated to the circadian cycle and secreted into the cerebrospinal fluid and blood having effect in all the cells and tissues [7]. MT has two receptors, MT1 and MT2, which have a high affinity and can be triggered even at low concentrations of MT [8]. MT can also join to nuclear RAR-related orphan receptors and the retinoid Z receptors [9]. However, the molecule of MT is amphiphilic, and therefore it can also cross the cell membrane. MT is also synthesized in the mitochondria [10]. However, MT production can be suppressed by the cytokine storm associate with the severe influenza and SARS-CoV-2 infection in the pineal gland and the mitochondria. This contributes to the deregulation of mitochondrial metabolism, increasing the pro-inflammatory state, and unbalancing the redox homeostasis which is altered by the increase of the ROS [11].
MT incapacitates and prevents the over production of ROS through its pyrrole ring structure that provides it with a high capacity to entrap O2– and hydroxyl (OH–) radicals [12]. ROS sequestration protects cell membrane lipids, cytosol proteins, and nuclear and mitochondrial DNA [13]. MT can also chelate metal ions such as Fe3+ that are involved in the Fenton and Haber-Weiss reactions and decrease the formation of the OH– which participates in the lipid peroxidation (LPO) [14]. MT may also stimulate the antioxidant enzymatic system [15], inhibiting the enzymes that contribute to ROS production such as myeloperoxidase (MPO), lipoxygenase and NADPH oxidases [16]. MT increases the efficiency of the transfer of electrons between the mitochondrial respiratory complexes thereby decreasing electron leakage and super oxide formation [17] and it stabilizes the integrity of the mitochondrial inner membrane [18]. It may also increase the glutathione (GSH) synthesis through the regulation of the γ-glutamyl cysteine synthetase [19].
On the other hand, OS is characterized by an increase in ROS and the depletion of the enzymatic and non-enzymatic antioxidant system that leads to the disturbance of redox homeostasis [20]. Therefore, the objective of this study was to evaluate and demonstrates if the treatment with MT contributes to decrease the OS present in COVID-19 patients, and if it may correct the alteration in redox homeostasis.
2. Results
2.1. Demographic characteristics of the COVID-19 patients
A total of 17 patients were included, 13 (76.47 %) were men and 4 (23.52 %) were women. The demographic characteristics are shown in Table 1. Patients had a median age of 62 with 34–84min-max range. The median body mass index was 30 median with 20–37 min-max range kg/m2. Normal weight was found in 6 (35%), over weight in 3 (18 %) and obesity in 8 (47 %) subjects. Comorbid conditions prior to SARS-CoV-2 infection were diabetes mellitus type 2 in 11 (65 %), hypertension in 7 (41 %), dyslipidemia in 10 (59 %), and chronic obstructive pulmonary disease 1 (6 %). The temperature median was of 36 °C with 36.5, 35.9–37.2 min-max range. Other variables expressed as median and minimum–maximum ranges, respectively, that are included are; arterial blood oxygen pressure (PaO2= 79, 58–152 mmHg), partial pressure of carbon dioxide (PCO2= 31, 27–36 mmHg), Kirby’s index which is PaCO2/inspired fraction of oxygen (FiO2= 145, 49–243 mmHg), oxygen saturation (SpO2/FiO2=160, 50–280 mmHg, heart rate Ipm= 84, 58–106, the arterial pressure= 82, 65–99 mmHg, the body temperature= 36.5, 35.9–37.2 °C, leukocytes= 10.1, 5.3–22.6 103/µL, lymphocytes= 0.66, 0.39–1.29 103/µL, platelets= 275, 180–576 103/µL, ferritin= 665.7, 175–2354 ng/mL), D-dimer= 655.0, 273–5200 ng/dL, CRP= 145.0, 37–308 mg/L, procalcitonin= 0.40, 0.06–34.7 ng/mL, The sepsis score according to SOFA index= 2, 1–3, APACHE= 5.0, 4–7, and SAPS= 26.5, 13–31. The patients with moderate and severe condition were 6 and 11, respectively and the number of days with mechanic ventilation was = 2, 1–2, days in ICU= 14.5, 6–20.
2.2. Demographic characteristics of the healthy subjects y subjects
A total of 20 healthy subjects (HS) were included of which 15 (75 %) were men and 5 (25 %) were women. HS had a median age of 57 with min 27 and max 87 ranges. The values of glucose, uric acid, cholesterol, HDL, LDL, triglycerides, C reactive protein and atherogenic index are shown in Table 2.
Table 3 shows the values of the glucose, insulin and HOMA-index in the COVID-19 patients before and after of the treatment with MT, where it is observed that after of the MT treatment a significant decrease was present in the glucose concentration (p=0.05). The values of IL-6 and HDL are also presented in the same table. The MT treatment decreased the IL-6 levels (p=0.02) and there was a tendency to decrease in the HDL (p=0.09) but without significant difference after of the MT treatment. Other variables, present such median and minimum-maximum range respectively in the same table are; Insulin in ng/mL= 1.30, 0.10–10.10, HOMA-index= 9.71, 16.70–100.15, total cholesterol in mg/dL= 141, 76–196, triglycerides in mg/dL= 140, 67–325, low-density lipoprotein in mg/dL= 83, 40–108 which did not show significant changes after the treatment with MT.
2.3. Oxidative stress markers
The total carbonyl concentration and the LPO index were increased in the serum of the COVID-19 patients in comparison with HS (p=0.03, p<0.001) (Figure 1A and B respectively) but the treatment with MT decreased the concentration of carbonyls and LPO index (p=0.05 and p<0.001). The TAC, NO2–, thiol groups and GSH concentration showed a significant decrease in the COVID-19 patients in comparison with HS (p<0.001), but after the treatment with MT these variables were increased (p=0.01, p<0.001 and p=0.03 respectively, Figure 1C, D, E and F).
2.4. Activities of the enzymes that employ the GSH
Table 3 shows the activities of the enzymes that employ the GSH including; GPx (p=0.001), TxrR (p=0.001), GST (p=0.001) and GR (p=0.04), which show a decrease in the serum of the COVID-19 patients in comparison with HS. However, the treatment with MT favored a significant increase in the activities of these enzymes; GPx (p=0.001), GST (p=0.01) and GR (p=0.003) but the TxrR activity only showed a tendency to increase without reaching statistical significance.
2.5. Activities of the enzymes peroxidases and ecSOD in native gels
Figure 2A shows that the activity of peroxidases in the COVID-19 patients, presented a significant decrease in comparison with HS (p<0.001) but the treatment with MT increase this (p=0.03). The same tendency was present in the ecSOD activity in the COVID-19 patients in comparison with HS (p<0.001) and COVID–19 after of the treatment whit MT (p=0.04).
3. Discussion
In this study we evaluated whether the treatment with MT contributes to decrease the OS present in COVID-19 patients, and if it may correct the alteration in the redox homeostasis. MT reduces the presence of the renin angiotensin receptor in cell membranes lowering the expression of the ACE2 receptor in the lipid rafts of the cell membrane which may reduce the entry of the SARS-CoV-2 [21]. MT also has an inhibitor effect on the Mpro, a cysteine protease necessary for SARS-CoV-2 replication [22]. Despite the afore mentioned, MT is not virucidal, but may indirectly aid in anti-viral actions counteracting the alterations that originate from infection in patients. These benefits of MT can be attributed to its properties as inducer of antioxidant enzyme, stimulator of the immune function, scavenger of free radical and it also may increase the synthesis of GSH [23].
In this sense, our results show that OS markers such as the concentration in the total carbonyls and the LPO index decrease in the serum from COVID-19 patients treated with MT, but that the TAC, NO2–, the thiol groups, the GSH concentration and GST activity were increase after of the treatment with MT. In the infection by SARS-CoV-2, OS is present, and it is characterized by a decrease in the GSH tripeptide, thiols groups, NO2– and GST activity that favor the LPO index, and the oxidative background, that leads to diminish the TAC [24]. In this sense, the ferroptosis present in COVID-19 patients favors LPO when the unsaturated fatty acids are oxidized by the OH–. Ferroptosis is due to the hijacking of the function of mitochondria, the escape of components of the mitochondrial transport chain into the cytosol such as cytochrome c (Cyt c) and COX II, the knockdown of the GPx4 isoform and the destruction of the heme group in some enzymes by hypochlorous acid (HOCl) in the infection by SARS-CoV-2 virus [2]. Our results agree with other previously mentioned reports and suggest that treatment with MT may be utilized as an antioxidant adjuvant therapy in the SARS-CoV-2 infection since it may decrease the OS in the COVID-19 patients. Based on the chemical structure of MT, it may penetrate in the lipid membrane bilayer of the cell and protect cell organelles against the damage by ROS caused by different viral infections [25].
With respect to activities of the enzymes that employ the GSH such as GPx, GST, GR and TrxR which were analyzed in this study, it has been described that the infection by the SARS-CoV-2 leads to a decrease in their activities or expressions [26]. However, the treatment with MT may restore the low activities of these enzymes since it increases the GPx, GR, SOD, and catalase gene expressions and this effect is doses dependent [27]. In this sense, the treatment with MT enhances the mitochondrial SOD expression in elderly rats and prevents the reduction of SOD/GPx and GR/GPx ratios [28]. Another investigation demonstrated that the treatment with MT increases the activity of SOD, the levels of GSH and decreases NOx levels in renal ischemia/reperfusion injury in rats [29]. MT can stimulates ERK1/2 signaling pathway in the presence of excessive ROS through the MT1 and MT2 receptors, and this leads to increases in the expressions of antioxidants enzymes such as GPx, GR, GST, SOD and GSH via stimulation of the Nrf2 [30].
Our results show that the activity of ecSOD which is a SOD isoform that has Cu/Zn in the catalytic center, to carry out the dismutation processes between O2– to H2O2, decreased in the serum of the COVID-19 patients. This was probably due to the excess O2– substrate [26] and suggest that this enzyme is incapable of dismutating the O2– to H2O2, resulting in an increase in OS. The activity/expression of this enzyme is reduced in the SARS-CoV-2 infection [26,31]. However, the treatment with MT increased the ecSOD activity. This result may seem paradoxical because the dismutation process favors the decrease in O2– and an increase the H2O2. However, this radical is the substrate of GPx, GST, TxrR, catalase and peroxidases families and is detoxified to molecular O2 and H2O. Our results showed that the activities of these enzymes were increased by the treatment with MT. In addition, the infiltration of neutrophils and monocytes that is associate with the SARS-CoV-2 infection can activate the myeloperoxidase (MPO), which is a peroxidase that participate as a mechanism of defense to decrease the viral infection, through the synthesis and liberation of HOCl. This molecule is a highly oxidant agent. However, high concentration of HOCl can increase the cytokine storm and O2–, and H2O2 in the infectious processes [32]. In the early stages of the disease, this mechanism plays a crucial role in neutralizing and destroying viral and bacterial proteins [32,33]. However, as already mentioned, it can exert significant cytotoxic effects, when released in large amounts such as in the SARS-CoV-2 infection [34]. For example, HOCl can compete with O2 at the hemoglobin heme binding sites and cause heme degradation and subsequent release of Fe2+ that triggers the Haber-Weiss and Fenton reactions and contribute to the ferroptosis and LPO present in COVID-19 patients [34]. Also, high concentrations of HOCl can decrease the activities of other enzymes such as lactoperoxidase, eosinophil peroxidase, thyroid peroxidase and other peroxidase super family members, even myeloperoxidase itself (inhibition of the product on the enzymatic activity), [34,35]. Our results show that the activities of the peroxidases decreased in the serum of the COVID-19 patients, and that the treatment with MT, favored the activities of these enzymes.
These results suggest that the peroxidase activities are decreased in the COVID-19 patients probably due to the HOCl increase by the severe infection [36]. However, the treatment with MT favors the activities of these enzymes and contributes to decrease the OS [37]. In addition, HOCl overproduction can also mediate the destruction of the heme of the eNOS through a mechanism similar to the destruction of the heme in hemoglobin which results in a decrease in NO [38]. In this sense, the results shown that NO2– decreased but the treatment with MT restored it. The NO2– is a metabolite of the NO and the hypoxic condition in the COVID-19 patients favors a decrease in the O2 concentration. Optimal concentrations of O2 are necessary for NO synthesis by the eNOS pathway [39]. In ARDS and COPD associated to SARS-CoV-2 infection, the hypoxic conditions contribute to inflammation and HOCl overproduction that favor the OS and NO decrease [40]. Also, the increase in the formation of O2– due to the loss of the activity of ecSOD may react with the scarce NO that has been synthesized and thus contribute to decrease its concentration which is associated with the eNOS heme destruction by HOCl. This could contribute to disrupt the redox homeostasis. Furthermore, the scarce NO synthetized might be oxidized by ROS to peroxinitrite which is more aggressive and may contribute to the inflammatory process associated with the interleukin storm that contributes to the damage in the lungs in the COVID-19 patients [41].
Different interleukins participate in the inflammatory processes, including IL-6. Our results show an increase in this interleukin, but treatment with MT decreased it in the serum of the COVID-19 patients. These results suggest the capacity of MT to modulate the inflammatory process. In this sense, a systematic study showed that the treatment with MT a dosage of 5–25 mg/day favored the decrease of the inflammatory markers including IL-6, CRP, and TNF-α in plasma of the COVID-19 patients [42]. In addition, another clinical study in 20 hospitalized Iranian patients with mild to moderate COVID-19 severity, that received MT supplement of 9 mg/day for 14 days there was a significant reduction in TNF-α, IL-1β, IL-2, IL-4, IL-6, IFN-γ via the NLRP3 inflammasome activation, and increased level of SOD and MT contributed to a decrease in the OS status in comparison with the control group [43]. A meta-analysis that included 13 studies in COVID-19 patients where MT was administered there was a significant reduction of TNF-α and IL-6 levels [44]. Therefore, previous studies and our results confirm that the administration with MT in COVID-19 patients decreases the pro-inflammatory state and the interleukin storm. These studies also confirm that the doses of MT utilized in our study are within the pharmacological range and that this molecule is effective in the SARS-CoV-2 infection. In this sense, a cross-sectional clinical trial with adjuvant therapy found that the dose of 3 to 10 mg of MT shows preventative and therapeutic effects against SARS-CoV-2 infection [45]. Different studies in a mast cell line suggest that MT can exert its anti-inflammatory effects through its receptors [46]. Another study showed that MT may exert anti-inflammatory effects through the regulation of sirtuin-1, which inhibits the differentiation of macrophages towards the pro-inflammatory type [47]. Therefore, MT is a significant inhibitor of the activation of the NLRP3 inflammasome by macrophages [48].
On the other hand, MT is capable of modulating glucose homeostasis and energy metabolism contributing to the decrease of the glucose concentration in the serum of patients with COVID-19 after treatment with MT. In this sense, the administration of complementary MT has demonstrated successful outcomes in the management of diabetes and metabolic syndrome [49] through the re-routing of pyruvate metabolism from the cytosol to the mitochondria. In other words, MT may function as a glycolytic agent since it inhibits the Warburg effect [50]. The Warburg effect is present in the SARS-CoV-2 infection, and it is associated to the hijacking of mitochondrial function by the virus to promote its replication [2]. In this condition, it promotes the switching to aerobic glycolysis that leads to the elevation of lactate dehydrogenase and lactic acidosis with Cyt c COX II liberation that promotes hyperferritinemia [51]. The Warburg state favors the up regulation of the inducible factor 1 alpha (HIF-1α) that contributes to conditions of hypoxia in ARDS [52]. In the mitochondria, Cyt C interacts with H2O2 and is converted to oxoferryl Cyt c with pseudoperoxidase activity. The oxoferryl derivative of Cyt c oxidizes MT. These results in the restoration of the normal redox cycle of Cyt c which is essential for the maintenance of mitochondrial bioenergetics which contributes to fight the SARS-CoV-2 infection [53].
Besides the production of MT by the pineal gland, the mitochondria also synthesize MT, and this production is inhibited by SARS-CoV-2 infection [54]. However, the treatment with MT can favor the inhibition the of mitochondrial permeability transition pore and optimize the mitochondrial oxidative phosphorylation that prevents the release of Cyt c, COX II and cardiolipin peroxidation [55]. Furthermore, the circadian gene, Bmal1 that regulates the mitochondrial melatonergic pathway is inhibited during SARS-CoV-2 infection. The treatment with MT is capable of promoting Bmal1 activity and this contributes to inhibit viral replication [56]. In other words, the MT may partly shift glucose metabolism from anaerobic glycolysis to aerobic mitochondrial oxidative phosphorylation, and consequently result in decreased lactate production. Lactate is increased in the COVID-19 patients [57]. In this sense, our results on immune colloidal gold technique show that Cyt c and GPx4 were present in the cytosol, outside and inside the mitochondrial outer matrix of the pneumocyte type II. These results confirm what was previously mentioned about the hijacking of mitochondrial function by the SARS-CoV-2 virus, since both Cyt c and GPx4 are mitochondrial and should be inside and not outside the mitochondria [2].
On the other hand, the administration of MT may reduce the use of pain relievers, sedation, agitation, and anxiety, improving the quality of sleep in COVID-19 patients. Furthermore, MT restores the optimal circadian pattern of the sleep/wakefulness cycle, which improves the clinical condition of the person with SARS-CoV-2 pneumonia [58].
The Figure 4 summarizes the possible benefits of the treatment whit MT in patients with COVID-19.
4. Materials and Methods
4.1. Population that comprised the study
This was a longitudinal (before-after), open, analytical and prospective study run in 17 patients with COVID-19 who received melatonin (MT) treatment. It compared the results in patients with those from 20 healthy subjects (HS). Inclusion criteria: The COVID-19 patients were 34 years old or more, admitted to the intensive care unit (ICU) of the CITIBANAMEX Center and they developed or not septic shock, secondary to moderate or severe pneumonia by SARS-CoV-2 infection. The MT treatment was applied between August and September of 2020. Ethical approval was obtained in 19th August 2020 (Control-9867/2020, register REG. CONBIOETICA-09-CEI-01120160627). The protocol was registered (TRIAL REGISTRATION: ClinicalTrials.gov Identifier: NCT04570254). The Sepsis-3 consent was used for diagnostic criteria of septic shock [59]. An informed consent written for recruitment and the use of patient data was obtained from each patient or their legal representative, in accordance with the Helsinki declaration. COVID-19 patients were considered to have septic shock when there was an acute increase of at least 2 points in the SOFA score [60], with lactate levels ≥ 2 mmol/L, and dependent on a vasopressor for at least 2 hours before recruitment. To evaluate organ dysfunction, the SOFA score (respiratory, hemodynamic, hematologic, hepatic, and neurologic) was calculated at admission and during the days of the treatment [60]. The hospitalized COVID-19 patients were classified as moderate or severe; this classification was decided according to their ventilatory status. COVID-19 patients with the severe condition required invasive mechanical intubation according to the Berlin criteria for ARDS [60,61]. Exclusion criteria were: patients that were under chronic use (last 6 months) or recent use of MT, antioxidants, statins and steroids; patients that were not able to grant an informed consent, or refused to be included, pregnant women or women that were breast feeding. The use of hydroxychloroquine or antivirals was not considered since patients received individualized management according to a proposed algorithm by Soto et al [1]. At the time this study was carried out, the patients were not vaccinated against SARS-CoV-2 because a vaccine had not yet been approved. Some results related to this study were previously reported by Chavarría et al. during the before and after treatment with MT treatment evaluation [62]. Figure 5 describes a flow chart of the recruitment and MT treatment in all COVID-19 patients.
4.2. Detection of SARS-CoV-2 by real-time reverse transcriptase polymerase chain reaction
The Paired Technique nasopharyngeal and saliva swab samples were collected from 16 patients infected by SARS-CoV-2. Samples were classified as positive for SARS-CoV-2 when both the N1 and N2 protein primer-presets were detected. For the presence of the SARS-CoV-2 virus, specific probes for the detection of the virus in conjunction with the real-time reverse transcriptase polymerase chain reaction technique (qRT-PCR) were utilized.
4.3. Healthy subjects
Twenty healthy subjects (HS) 15 men and 5 women were matched by age and gender. HS were negative for the SARS-CoV-2 infection. In the HS there was no inflammatory, degenerative, thyroid, and autoimmune diseases, diabetes mellitus, dyslipidemia or arterial hypertension. The intake of some medications that could interfere with the results of the study such as antioxidant drugs and NSAIDs in HS were considered, and if this happened, the drugs were suspended 48 hours before the obtainment of the sample. Biochemical variables such as glucose, uric acid, cholesterol, triglycerides, HDL, LDL, C reactive protein and atherogenic index were determined.
4.4. Therapeutic Management
The treatment applied during hospitalization was chosen according to standard maneuvers considering the requirements of each individual patient, the hemodynamic, electrolyte demands, and the ventilator demands. Treatment was initiated during the first hour after admission and before the recognition of the presence or absence of septic shock.
Management with crystalloid solutions and/or albumin was considered depending on the hemodynamic status, by means of dynamic indicators. Use of vasopressors to maintain a mean arterial pressure (MAP) ≥65 mmHg was given if necessary. Norepinephrine (NE) was the first option and/or vasopressin was used when there was a need to increase the MAP or reduce the NE dose. Inotropic drugs (dobutamine) were administered in cases of myocardial dysfunction. Transfusion of blood packs were applied in case of a decrease in hemoglobin (<7.0 g/dL) in the absence of severe hypoxemia, myocardial ischemia, or severe bleeding. Mechanical ventilation with initial volumes of 6 mL/kg was used in ARDS patients [60,62,63]. Plateau pressure was maintained at ≤30 cm H2O, and alveolar conduction pressure of ≤13 cm H2O. Positive end expiration pressure titration was managed by the use of the fraction inspired of oxygen/positive end expiration pressure (FiO2/PEEP). The treatment with anticoagulants was based on the Thatched guidelines [64]. The management with the prone position was necessary in patients with PaO2/FiO2 of ≤150 mmHg (65). In all patients, the standard therapeutic management with dexamethasone 8 mg i.v., every 24 hours for 7 days was applied between 1 and 21 days of the onset of symptoms when not counter indicated, and pentoxifylline tablets of 400 mg every 12 hours by oral route or nasal-enteral tube for 5 days (62). It was counter indicated when there was a requirement of O2 >3L, progressive requirement of =2, PAO2/FiO2 ≤250 mmHg, O2 use plus bilateral infiltrates in the radiography, O2 use plus DHL ≤250 U/L or ferritin ≥300 or DD ≥1000 ng/mL, CPK ≥2 times the upper normal value. The following conditions were not considered as counter indications or relative counter indications: glucose >250 mg/dL with hypoglycemic, hypokalemia <3.3 meq, blood pressure >155/95 mmHg with antihypertensive treatment, glaucoma, triglycerides >500 mg/dL (start treatment), history of known peptic ulcer or bleeding from recent gastro intestinal tract, untreated or decompensated dementia or psychiatric illness, use of non-potassium sparing diuretics or use of inhaled B2 agonists. The next conditions were monitored at follow-up: pre-prandial capillary glucometer (7–13–1 hours.) for 10 days, even in fasting patients, MAP per shift and basal potassium every 72 hours.
The dose of the MT therapy was 5 mg (10 prolonged-release capsules) given every 12 hours by oral route or naso-enteral tube for 5 days. The presences of comorbidities or of potential allergies or heart rhythm disorders due to each individual history were considered before the treatment with MT [62]. All data entry was monitored at the coordinating center for patient management, with site visits for source data verification.
4.5. Peripheral blood samples
The collection of peripheral blood samples was carried out by venopuncture. The blood samples of both COVID-19 patients and HS were centrifuged for 20 min at 936 g and 4 °C. The serum was recovered and stored at−30 °C until use. Laboratory tests were carried out for the COVID-19 patients to determine the acute-phase reactants, urea nitrogen, creatinine, glucose, cholesterol, triglycerides, insulin, HDL, LDL, hemoglobin, leukocytes, lymphocytes, platelets, albumin, D-dimer, fibrinogen, ferritin, C-reactive protein, procalcitonin, and interleukin-6 (IL-6). Data from the patient’s medical history including demographic, prior illnesses to SARS-CoV-2 infection, COVID-19 test result, whether mechanical ventilation was used, and treatment type given were used for the analysis of the results. Additionally, OS markers and antioxidant enzymatic system were determined in serum from the COVID-19 patients and HS. The HOMA index for the IR was calculated; HOMA−IR = insulin μU/mL × glucose mM/L/22.5.
4.6. Oxidative stress markers
4.6.1. Carbonyls protein
Carbonyls were detected spectrophotometrically at 370 nm. 100 μL of serum were added to 500 μL of HCl 2.5 N. In parallel, another sample with 500 μL of 2,4-dinitrophenylhydrazine and incubated in the dark at room temperature for one hour. At the end of the incubation period, 500 μL of C2HCl3O2 20% were added, and centrifuged at 15,000 × g for 5 min. The supernatant was discarded. Two washings were performed, adding 1 mL C2H5OH/C4H8O2. It was incubated for 10 min, and centrifuged at 15,000× g for 10 min. Finally, 1 ml of CH6CIN3 at 6 M in KH2PO4 at 20 mM pH 2.3 was added, the mixture was incubated again at 37 °C for 30 min and the absorbance was read [66]. The values are expressed such as carbonyls (nmol/mL of serum)
4.6.2. Evaluation of total antioxidant capacity
Total antioxidant capacity (TAC) was detected spectrophotometrically at 593 nm. 100µLof serum was suspended in 1.5 mL buffer mixture (C2H3O2 at 300 mM pH 3.6, FeCl36H2O at 20 mM and 2,4,6-tris-2pyridyl-s-triazine at 10 mM and HCl at 40 mM). These reactants were added in a ratio of 10:1:1v/v, respectively, after mixing and were incubated at 37 °C for 15 min in the dark [62]. The values are expressed as carbonyls (nM of trolox/mL of serum).
4.6.3. Determination of lipid peroxidation (LPO) levels
LPO was read spectrophotometrically at 532 nm. 100 μL of serum was use for this determination. CH3-OH with BHT at 4% plus KH2PO4 buffer pH 7.4 was added to serum sample and then incubated at 37 °C for 30 min after 1.5 mL of 2-thiobarbituric acid at 0.8 M was then added, and incubated at 90 °C for 1 hour. After 1 mL KCl to 5% plus 4 ml C4H10O, shaken for 30 sec and centrifuged at 4000 rpm for 2 min. The n-butanol phase was extracted, and the absorbance was measured [66]. The values are expressed such as malondialdehyde (MDA/mL of serum).
4.6.4. Nitrites
The Nitrites (NO2−) concentration in serum by the technique of Griess and detected spectrophotometrically at 540 nm. 100 μL of serum previously deproteinized with NaOH at 0.5 N and ZnSO4at 10%, was mixed and centrifuged at 1789 g for10 min, and the supernatant was incubated with 200 μL of sulfanilamide 1% and 200 μL of N-naphthyl-ethyldiamine 0.1% were added, and the total volume was adjusted to 1 mL [62]. The values are expressed such as (nM/mL of serum).
4.6.5. Thiols and glutathione levels
Determination of thiol groups was done spectrophotometrically at 415 nm. 50 µL of serum was used according to Erel and Neselioglu method [67]. The calibration curve was obtained with solution GSSG 1 mg/1 mL. The values are expressed as (μM/mL of serum). Glutathione levels (GSH) was detected spectrophotometrically at 412 nm. 100 µL of serum was used according to Ellman method. The values are expressed such as (μM/mL of serum).
4.6.6. Determinations of antioxidant enzymes that employ GSH
To evaluate the GR, GST and GPx, activities, 100 µL of serum was used, as previously described by different methods [66]. The samples were incubated and monitored at 340 nm for 6 min at 37 °C. The TrxR activity was determined using 100 µL of serum according to the previously described method [66]. The sample was incubated and monitored at 412 nm for 6 min at 37°C. The TrxR activity is expressed as TNB nmol/min/mL the serum with an extinction coefficient of 13600 M−1 cm−1. The GR activity is expressed as μmol of reduced GSSG/min/mL the serum, with an extinction coefficient of 6220 M−1cm−1. The GST activity is expressed as units of GS-TNB mol/min/mL of serum with an extinction coefficient of 14150 M−1cm−1. The GPx activity is expressed as nmol of NADPH oxidized/min/mL the serum, with an extinction coefficient of 6220 M−1cm−1 at 340 nm for NADPH. The extracellular superoxide dismutase (ecSOD) and peroxidases activities were determined by non-denaturing gel electrophoresis [66]. A total of 25 µL of serum was applied directly in non-denaturing 10% polyacrylamide gels. The electrophoresis was carried out at 120 volts for 4 hours. For the ecSOD activity the gel was incubated with nitro blue tetrazolium at 2.45 mM by 20 min, then incubated with buffer of the KH2PO4 at 36 mM, EDTA at 28 mM and riboflavin at 28 μMpH7.8, and exposed 10 min by UV light. Purified SOD from bovine erythrocytes with a specific activity of 112 U/mg of protein (Sigma Aldrich, St. Louis, MO, USA) was used as positive control for calculating the activity of this enzyme. For the peroxidases activity, the gel was washed with distilled water three times, during 5 min, after incubated with3 mg/mL 3,3,5,5-tetramethylbenzidine dissolved in CH3-OH/CH3COOH/H2O (1:1:1 v/v) with H2O2 300 μL for 10 min. 35 μL of horseradish peroxidase was loaded to a final concentration of 178.5 μg as a standard. The activities in the ecSOD and peroxidase gels were analyzed by densitometry with a Kodak Image® 3.5 system.
4.6.7. Interleukin-6 Concentration
IL-6 levels were measured in plasma samples by an enzyme-linked immunosorbent assay (ELISA) using a commercial kit according to the manufacturer’s instructions (BioLegend, San Diego, CA, USA), and 50 μL of serum was used for this determination.
4.6.8. Obtainment of the post-mortem biopsies
Postmortem biopsies were obtained according to Soria-Castro et al; 2021. The lung biopsy, punctures were performed at the apical and sub clavicular regions of the right, and left lung [2].
4.6.10. Immune colloidal gold technique
Small tissues sample of the lung from the postmortem COVID-19 patients and of the control subject were processed according to the immune colloidal gold technique [2]. The samples were cut and mounted on carbon/formvar coated nickel grids. They were then incubated with antiserum for 1 hour, and with the primary antibodies diluted 1:20: Cytochrome C (EPR1327) Rabbit Recombinant monoclonal Ab 133504(Abcam), Glutathione peroxidase 4/GPX4 (E-12) mouse monoclonal sc-166570 (SantaCruz BioTechnology), and COX II (d-5), mouse monoclonal IgM sc-514489 (SantaCruz BioTechnology), were used. Samples were incubated in a moist chamber at 4 °C overnight. The samples were then washed at 24 °C, and incubated with a secondary antibody conjugated with colloidal gold diluted 1:20. The antibodies used were Goat Anti-Rabbit gold 12nm cat. 111-205-144 (Jackson Immuno Research rabbit-anti-mouse gold 25nm cat:25352 (Electron Microscopy Sciences), at 24 °C, and evaluated with a JEM-1011 (JEOL Ltd., Tokyo, Japan) at 80 kV, equipped with AMT 542.391 analysis software [2].
4.7. Statistical Analysis
Continuous variables of the activities of the antioxidant enzymes were expressed as median, first quartiles, second quartile, interquartile range with minimum and maximum range. Categorical variables were expressed as frequencies and percentages. Continuous variables were compared with the Mann–Whitney U rank sum test followed by the normality test (Shapiro–Wilk) between HS vs. before the MT treatment in the COVID-19 patients, and by Kruskall–Wallis test before vs. after the MT treatment in the COVID-19 patients. SigmaPlot® version 15. (Systat Software Inc., SanJose, CA 95131, USA, EE.UU, North First Street, Suite 360, Jandel Corporation, San Jose, CA, USA) was used to generate the analysis and graphs. Differences were considered statistically significant when p ≤0.05.
5. Conclusions
The treatment with MT favors the activity of the antioxidant enzymes such as GPX, GST, GR, ecSOD, peroxidases and increases the marker of OS such as thiols, GSH NO2–. This contributes to decrease the carbonyls and LPO leading to an increase of the TAC. Thus, MT restores the redox homeostasis which is altered in COVID-19 patients. Furthermore, the treatment with MT is capable of modulating glucose homeostasis because it functions as a glycolytic agent since it inhibits the Warburg effect. Therefore, MT can be used as adjuvant therapy in the SARS-CoV-2 infection.
Perspectives
Although there are currently different vaccines against SARS-CoV-2 that allow us to reduce the severity of the infection, the administration of MT as an adjuvant therapy can enhance the innate immune response, which may contribute to a better response in the rate of production of specific antibodies and strengthen the compromised redox homeostasis and mitochondrial function caused by the viral infection [68].
Study limitations
One of the limitations of this study is the small group of COVID-19 patients that were included. Another limitation is the lack of a group of postmortem samples with MT treatment with the immune colloidal gold technique to demonstrate that the treatment is able to prevent mitochondrial sequestration.
Author Contributions
I.P.-T., M.E.S., V.G.-L., and V.C.-T.; revised and structured the manuscript. I.P.-T. L.M.-P., M.E.S., and V.C.-T.; designed the laboratory determinations, the tables, performed and planned the statistical analysis, methodology and statistical analysis. L.M.-P.; designed and created the graphical abstract. A.P.-C. and R.R.V.-V.; treated and recruited the patients in the intensive care unit and collected the biochemical results. E.S.-C. Made the immunogold captured the electron micrographs and the description of the images. E.D.-D. designed and made glucose, insulin and the calculation of HOMA index. All authors have read and agreed to the published version of the manuscript.
Funding
work was supported by Consejo Nacional de Humanidades Ciencias y Tecnologías (CONACHYT) México, Project Number 312167.
Institutional Review Board Statement
The studies involving human participants were reviewed and approved by ethical approval from the local ethics committee on 19 August 2020 (Control-9867/2020, register REG. CONBIOETICA-09 CEI-011–20160627). A written informed consent for enrollment or consent to use patient data was obtained from each patient or their legal surrogate. The protocol was registered (TRIAL REGISTRATION: ClinicalTrials.gov Identifier: NCT 04570254).
Informed Consent Statement
The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article. The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The payment of the open access publishing was covered by the Instituto Nacional de Cardiología Ignacio Chávez. We thank Rocio Torrico-Lavayen for electron microscopy histological technical support. Thanks at Angélica Ruiz-Ramírez and Mohammed El Hafidi for providing us with the antibodies against Cytochrome and COX II.
Conflicts of Interest
The authors declare no conflicts of interest. The authors declare that they have no known competing financial interest or personal relationships that could have appeared to influence the work reported in this paper.
References
- Soto, M.E.; Guarner-Lans, V.; Soria-Castro, E.; Manzano-Pech, L.; Pérez-Torres, I. Is antioxidant therapy a useful complementary measure for Covid-19 treatment? An algorithm for its application. Medicina. (Kaunas). 2020, 56, 386–415. [Google Scholar] [CrossRef] [PubMed]
- Soria-Castro, E.; Soto, M.E.; Guarner-Lans, V.; Rojas, G.; Perezpeña-Diazconti, M.; Críales-Vera, S.A.; Manzano-Pech, L.; Pérez-Torres, I. The kidnapping of mitochondrial function associated with the SARS-CoV-2 infection. Histol. Histopathol. 2021, 36, 947–965. [Google Scholar]
- Zhang, D.; Kukkar, D.; Kim, K.H.; Bhatt, P. A comprehensive review on immunogen and immune-response proteins of SARS-CoV-2 and their applications in prevention, diagnosis, and treatment of COVID-19. Int. J. Biol. Macromol. 2024, 259, 129284. [Google Scholar] [CrossRef]
- Pérez-Torres, I.; Guarner-Lans, V.; Soria-Castro, E.; Manzano-Pech, L.; Palacios-Chavarría, A.; Valdez-Vázquez, R.R.; Domínguez-Cherit, J.G.; Herrera-Bello, H.; Castillejos-Suastegui, H.; Moreno-Castañeda, L.; Alanís-Estrada, G.; Hernández, F.; González-Marcos, O.; Márquez-Velasco, R.; Soto, M.E. Alteration in the lipid profile and the desaturases activity in patients with severe pneumonia by SARS-CoV-2. Front Physiol. 2021, 12, 667024. [Google Scholar] [CrossRef] [PubMed]
- Negru, P.A.; Radu, A.F.; Vesa, C.M.; Behl, T.; Abdel-Daim, M.M.; Nechifor, A.C.; Endres, L.; Stoicescu, M.; Pasca, B.; Tit, D.M.; Bungau, S.G. Therapeutic dilemmas in addressing SARS-CoV-2 infection: Favipiravir versus Remdesivir. Biomed. Pharmacother. 2022, 147, 112700. [Google Scholar] [CrossRef] [PubMed]
- Molina-Carballo, A.; Palacios-López, R.; Jerez-Calero, A.; Augustín-Morales, M.C.; Agil, A.; Muñoz-Hoyos, A.; Muñoz-Gallego, A. Protective effect of melatonin administration against SARS-CoV-2 infection: A systematic review. Curr. Issues. Mol. Biol. 2022, 44, 31–45. [Google Scholar] [CrossRef] [PubMed]
- Boutin, J.A.; Liberelle, M.; Yous, S.; Ferry, G.; Nepveu, F. Melatonin facts: Lack of evidence that melatonin is a radical scavenger in living systems. J. Pineal. Res. 2023, e12926. [Google Scholar] [CrossRef]
- Reppert, S.M. Melatonin receptors: Molecular biology of a new family of G protein-coupled receptors. J. Biol. Rhythm. 1997, 12, 528–531. [Google Scholar] [CrossRef] [PubMed]
- Mehrzadi, S.; Karimi, M.Y.; Fatemi, A.; Reiter, R.J. Hosseinzadeh A. SARS-CoV-2 and other coronaviruses negatively influence mitochondrial quality control: beneficial effects of melatonin. Pharmacol. Ther. 2021, 224, 107825. [Google Scholar] [CrossRef]
- Pontes, G.N.; Cardoso, E.C.; Carneiro-Sampaio, M.M.; Markus, R.P. Pineal melatonin and the innate immune response: the TNF-alpha increase after cesarean section suppresses nocturnal melatonin production. J. Pineal. Res. 2007, 43, 365–371. [Google Scholar] [CrossRef]
- Markus, R.P.; Fernandes, P.A.; Kinker, G.S.; da Silveira, C.M.S.; Marçola, M. Immune-pineal axis—acute inflammatory responses coordinate melatonin synthesis by pinealocytes and phagocytes. Br. J. Pharmacol. 2018, 175, 3239–3250. [Google Scholar] [CrossRef] [PubMed]
- Pablos, M.I.; Guerrero, J.M.; Ortiz, G.G.; Agapito, M.T., Reiter, R.J. Both melatonin and a putative nuclear melatonin receptor agonist CGP 52608 stimulate glutathione peroxidase and glutathione reductase activities in mouse brain in vivo. Neuroendocrinol. Lett. 1997, 18, 49–58.
- Terron, M.P.; Flores, L.J.; Czarnocki, Z. Melatonin and its metabolites: new findings regarding their production and their radical scavenging actions. Acta. Biochim. Pol. 2007, 54, 1–9. [Google Scholar]
- Gulcin, I.; Buyukokuroglu, M.E.; Kufrevioglu, O.I. Metal chelating and hydrogen peroxide scavenging effects of melatonin. J. Pineal. Res. 2003, 34, 278–281. [Google Scholar] [CrossRef] [PubMed]
- Galano, A.; Tan, D.X.; Reiter, R.J. Melatonin and related compounds: Chemical insights into their protective effects against oxidative stress. Curr. Org. Chem. 2017, 21, 2077–2095. [Google Scholar] [CrossRef]
- Yao, Y.; Zhu, W.; Han, D.; Shi, X.; Xu, S. New insights into how melatonin ameliorates bisphenol A-induced colon damage: Inhibition of NADPH oxidase. J. Agric. Food. Chem. 2023, 71, 2566–2578. [Google Scholar] [CrossRef] [PubMed]
- Hardeland, R. Antioxidant protection by melatonin: Multiplicity of mechanisms from radical detoxification to radical avoidance. Endocrine. 2005, 27, 119–130. [Google Scholar] [CrossRef]
- Zhang, H.M.; Zhang, Y. Melatonin: A well-documented antioxidant with conditional pro-oxidant actions. J. Pineal. Res. 2014, 57, 131–146. [Google Scholar] [CrossRef]
- Budkowska, M.; Cecerska-Heryć, E.; Marcinowska, Z.; Siennicka, A.; Dołęgowska, B. The influence of circadian rhythm on the activity of oxidative stress enzymes. Int. J. Mol. Sci. 2022, 23, 14275. [Google Scholar] [CrossRef]
- Soto, M.E.; Guarner-Lans, V.; Díaz-Díaz, E.; Manzano-Pech, L.; Palacios-Chavarría, A.; Valdez-Vázquez, R.R.; Aisa-Álvarez, A.; Saucedo-Orozco, H.; Pérez-Torres, I. Hyperglycemia and loss of redox homeostasis in COVID-19 Patients. Cells. 2022, 11, 932. [Google Scholar] [CrossRef]
- Nakao, T.; Morita, H.; Maemura, K.; Amiya, E.; Inajima, T.; Saito, Y.; Watanabe, M.; Manabe, I.; Kurabayashi, M.; Nagai, R. , Nagai, R.; Komuro, I. Melatonin ameliorates Angiotensin II-induced vascular endothelial damage via its antioxidative properties. J. Pineal. Res. 2013, 55, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Feitosa, E.L.; Júnior, F.T.D.S.S.; NeryNeto, J.A.O.; Matos, L.F.L.; Moura, M.H.S.; Rosales, T.O.; De Freitas, G.B.L. COVID-19: Rational discovery of the therapeutic potential of melatonin as a SARS-CoV-2 main protease inhibitor. Int. J. Med. Sci. 2020, 17, 2133–2146. [Google Scholar] [CrossRef] [PubMed]
- Boga, J.A.; Coto-Montes, A.; Rosales-Corral, S.A.; Tan, D.X.; Reiter, R.J. Beneficial actions of melatonin in the management of viral infections: a new use for this molecular handyman. Rev. Med. Virol. 2012, 22, 323–338. [Google Scholar] [CrossRef] [PubMed]
- Anderson, G.; Reiter, R.J. Melatonin: Roles in influenza, Covid-19, and other viral infections. Rev. Med. Virol. 2020, 30, e2109. [Google Scholar] [CrossRef] [PubMed]
- Bahrampour, J.K.; Pourhanifeh, M.H.; Hosseinzadeh, A.; Hemati, K.; Mehrzadi, S. Melatonin potentials against viral infections including COVID-19: Current evidence and new findings. Virus. Res. 2020, 287, 198108. [Google Scholar] [CrossRef] [PubMed]
- Soto, M.E.; Manzano-Pech, L.; Palacios-Chavarría, A.; Valdez-Vázquez, R.R.; Guarner-Lans, V.; Pérez-Torres, I. N-acetyl cysteine restores the diminished activity of the antioxidant enzymatic system caused by SARS-CoV-2 infection: Preliminary findings. Pharmaceuticals. Basel. 2023, 16, 591. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C.; Mayo, J.C.; Sainz, R.M.; Antolín, I.; Herrera, F. Regulation of antioxidant enzymes: a significant role for melatonin. J. Pineal. Res. 2004, 36, 1–9. [Google Scholar] [CrossRef]
- Öztürk, G.; Akbulut, G.K.; Güney, S.; Acuna-Castroviejo, D. Age-related changes in the rat brain mitochondrial antioxidative enzyme ratios: modulation by melatonin. Exp. Gerontol. 2012, 47, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Sezgin, G.; Özturk, G.; Güney, S.; Sinanoğlu, O.; Tunçdemir, M. Protective effect of melatonin and 1,25-dihydroxyvitamin D3 on renal ischemia-reperfusion injury in rats. Ren. Fail. 2013, 35, 374–379. [Google Scholar] [CrossRef]
- Crespo, I.; Miguel, B.S.; Laliena, A.; Alvarez, M.; Culebras, J.M.; González-Gallego, J.; Tuñón, M.J. Melatonin prevents the decreased activity of antioxidant enzymes and activates nuclear erythroid 2-related factor 2 signaling in an animal model of fulminant hepatic failure of viral origin. J. Pineal. Res. 2010, 49, 193–200. [Google Scholar] [CrossRef]
- Muhammad, Y.; Kani, Y.A.; Iliya, S.; Muhammad, J.B.; Binji, A.; El-Fulaty, A.A.; Kabir, M.B.; Bindawa, K.U.; Ahmed, A. Deficiency of antioxidants and increased oxidative stress in COVID-19 patients: A cross-sectional comparative study in Jigawa, Northwestern Nigeria. SAGE. Open. Med. 2021, 9, 2050312121991246. [Google Scholar] [CrossRef] [PubMed]
- Tang, D.; Comish, P.; Kang, R. The hallmarks of COVID-19 disease. PLoS. Pathog. 2020, 16, e1008536. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, C.H.; Ryu, J.H.; Kim, M.J.; Park, C.Y.; Lee, J.M. Holtzman, M.J.; Joo-Heon Y. Reactive oxygen species induce antiviral innate immune response through IFN-lambda regulation in human nasal epithelial cells. Am. J. Respir. Cell. Mol. Biol. 2013, 49, 855–865. [Google Scholar] [CrossRef] [PubMed]
- Vlasova, I.I. Peroxidase activity of human hemoproteins: Keeping the fire under control. Molecules. 2018, 23, 2561. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Cheng, G. Recombinant myeloperoxidase as a New class of antimicrobial agents. Microbiol. Spectr. 2022, 10, e0052221. [Google Scholar] [CrossRef] [PubMed]
- Camp, O.G.; Bai, D.; Gonullu, D.C.; Nayak, N.; Abu-Soud, H.M. Melatonin interferes with COVID-19 at several distinct ROS-related steps. J. Inorg. Biochem. 2021, 223, 111546. [Google Scholar] [CrossRef] [PubMed]
- Goud, P.T.; Bai, D.; Abu-Soud. H.M. A Multiple-hit hypothesis involving reactive oxygen species and myeloperoxidase explains clinical deterioration and fatality in COVID-19. Int. J. Biol. Sci. 2021, 17, 62–72. [CrossRef] [PubMed]
- Abu-Soud, H.M.; Hazen, S.L. Nitric oxide is a physiological substrate for mammalian peroxidases. J. Biol. Chem. 2000, 275, 37524–37532. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, H. Blood nitrate and nitrite modulating nitric oxide bioavailability: potential therapeutic functions in COVID-19. Nitric. Oxide. 2020, 103, 29–30. [Google Scholar] [CrossRef]
- Kouhpayeh, S.; Shariati, L.; Boshtam, M.; Rahimmanesh, I.; Mirian, M.; Esmaeili, Y.; Najaflu, M.; Khanahmad, N.; Zeinalian, M.; Trovato, M., Tay, F.R.; Khanahmad, H.; Makvandi, P. The molecular basis of COVID-19 pathogenesis, conventional and nanomedicine therapy. Int. J. Mol. Sci. 2021, 22, 5438. [CrossRef]
- Wang, J.; Mei, F.; Bai, L.; Zhou, S.; Liu, D.; Yao, L.; Ahluwalia, A.; Ghiladi, R.A.; Su, L.; Shu, T.; Gong, M.; Wang, X.; Zhu, L.; Cai, K.; Zhang, X. Serum nitrite and nitrate: A potential biomarker for post-COVID-19 complications? Free. Radic. Biol. Med. 2021, 175, 216–225. [Google Scholar] [CrossRef]
- Corrao, S.; Bocchio M.R.; Monaco M.L.; Natoli, G.; Cavezzi, A.; Troiani, E.; Argano, C. Does evidence exist to blunt inflammatory response by nutraceutical supplementation during COVID-19 pandemic? An overview of systematic reviews of vitamin D, vitamin C, melatonin, and Zinc. Nutrients. 2021, 13, 1261. [CrossRef]
- Ghaleh, H.E.G.; Hosseini, A.; Aghamollaei, H.; Fasihi-Ramandi, M.; Alishiri, G.; Saeedi-Boroujeni, A.; Hassanpour, K.; Mahmoudian-Sani, M.R.; Farnoosh, G. NLRP3 inflammasome activation and oxidative stress status in the mild and moderate SARS-CoV-2 infected patients: Impact of melatonin as a medicinal supplement. Z. Naturforsch. C. J. Biosci. 2022, 77, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Zarezadeh, M.; Khorshidi, M.; Emami, M.; Janmohammadi, P.; Kord-Varkaneh, H.; Mousavi, S.M.; Mohammed, S.H.; Saedisomeolia, A.; Alizadeh, S. Melatonin supplementation and pro-inflammatory mediators: A systematic review and meta-analysis of clinical trials. Eur. J. Nutr. 2020, 59, 1803–1813. [Google Scholar] [CrossRef]
- Farnoosh, G.; Akbariqomi, M.; Badri, T.; Bagheri, M.; Izadi, M.; Saeedi-Boroujeni, A.; Rezaie, E.; Ghaleh, H.E.G.; Aghamollaei, H.; Fasihi-Ramandi, M., Hassanpour, K.; Alishiri. G. Efficacy of a low dose of melatonin as an adjunctive therapy in hospitalized patients with COVID-19: A randomized, double-blind clinical Trial. Arch. Med. Res. 2021, 53, 79–85. [CrossRef]
- Alizadeh, N.; Dianatkhah, M.; Alimohamadi, Y.; Moradi, H.; Akbarpour, S.; Akrami, M.; Mansouri, F.; Faraji, N.; Rezaie, Z.; Alizadeh, M.; Hosamirudsari, H. High dose melatonin as an adjuvant therapy in intubated patients with COVID-19: A randomized clinical trial. J. Taibah Univ. Med. Sci. 2022, 17, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Cardinali, D.P.; Brown, G.M.; Pandi-Perumal, S.R. Can Melatonin be a potential "Silver Bullet" in treating COVID-19 patients? Diseases. 2020, 8, 44. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.M.; Zhao, C.C.; Xie, Q.M.; Xu, J.; Fei, G.H. TLR2-melatonin feedback loop regulates the activation of NLRP3 inflammasome in murine allergic airway inflammation. Front. Immunol. 2020, 11, 172. [Google Scholar] [CrossRef]
- Owino, S.; Buonfiglio, D.D.C.; Tchio, C.; Tosini, G. Melatonin signaling a key regulator of glucose homeostasis and energy metabolism. Front. Endocrinol. 2019, 10, 488. [Google Scholar] [CrossRef]
- Reiter, R.J.; Sharma, R.; Rosales-Corral S. Anti-Warburg effect of melatonin: A proposed mechanism to explain its inhibition of multiple diseases Int. J. Mol. Sci. 2021, 22, 764. [CrossRef]
- Gomez-Pastora, J.; Weigand, M.; Kim, J.; Wu, X.; Strayer, J.; Palmer, A.F.; Zborowski, M.; Yazer, M.; Chalmers, J.J. Hyperferritinemia in critically ill COVID-19 patients—Is ferritin the product of inflammation or a pathogenic mediator? Clin. Chim. Acta. 2020, 509, 249–251. [Google Scholar] [CrossRef] [PubMed]
- Sayed, R.K.; Fernández-Ortiz, M.; Diaz-Casado, M.E.; Rusanova, I.; Rahim, I.; Escames, G.; López, L.C.; Mokhtar, D.M.; Acuña-Castroviejo, D. The protective effect of melatonin against age-associated, sarcopenia-dependent tubular aggregate formation, lactate depletion, and mitochondrial changes. J. Gerontol. A. Biol. Sci. Med. Sci. 2018, 73, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Dun.-Xian, T.; Manchester, L.C.; Esteban-Zubero, E.; Zhou, Z.; Reiter, R.J. Melatonin as a potent and inducible endogenous antioxidant: Synthesis and metabolism. Molecules. 2015, 20, 18886–18906. [CrossRef] [PubMed]
- Tarocco, A.; Caroccia, N.; Morciano, G.; Wieckowski, M.R.; Ancora, G.; Garani, G.; Pinton, P. Melatonin as a master regulator of cell death and inflammation: Molecular mechanisms and clinical implications for newborn care. Cell. Death. Dis. 2019, 10, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Juybari, K.B.; Pourhanifeh, M.H.; Hosseinzadeh, A.; Hemati, K.; Mehrzadi, S. Melatonin potentials against viral infections including COVID-19: Current evidence and new findings. Virus. Res. 2020, 287, 198108. [Google Scholar] [CrossRef] [PubMed]
- Anderson, G.; Reiter, R.J. Melatonin: Roles in influenza, COVID-19, and other viral infections. Rev. Med. Virol. 2020, 30, e2109. [Google Scholar] [CrossRef] [PubMed]
- Ramos, E.; López-Muñoz, F.; Gil-Martín, E.; Egea, J.; Álvarez-Merz, I.; Painuli, S.; Semwal, P.; Martins, N.; Hernández-Guijo, J.M.; Romero, A. The coronavirus disease 2019 (COVID-19): Key emphasis on melatonin safety and therapeutic efficacy. Antioxidants. Basel. 2021, 10, 1152. [Google Scholar] [CrossRef] [PubMed]
- Camp, O.G.; Bai, D.; Gonullu, D.C.; Nayak, N.; Abu-Soud, H.M. Melatonin interferes with COVID-19 at several distinct ROS-related steps. J. Inorg. Biochem. 2021, 223, 111546. [Google Scholar] [CrossRef] [PubMed]
- Olson, G.; Andrew, M.D. Diagnosis and treatment of adults with community-acquired pneumonia. JAMA. 2020, 323, 885–886. [Google Scholar] [CrossRef]
- Lambden, S.; Laterre, P.F.; Levy, M.M.; Francois, B. The SOFA score-development, utility, and challenges of accurate assessment in clinical trials. Crit. Care. 2019, 23. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Chavarría, A.P.; Vázquez, R.R.V.; Cherit, J.G.D.; Bello, H.H.; Suastegui, H.C.; Moreno-Castañeda, L.; Estrada, A.G.; Hernández. F.; González-Marcos, O.; Saucedo-Orozco, H.; Manzano-Pech, L.; Márquez-Velasco, R.; Guarner-Lans, V.; Pérez-Torres, I.; Soto, M.E. Antioxidants and pentoxifylline as coadjuvant measures to standard therapy to improve prognosis of patients with pneumonia by COVID-19. Comput. Struct. Biotechnol. J. 2021, 19, 1379–1390.
- Brower, R.G., Lanken P.N., MacIntyre N., Matthay M.A., Morris A., Marek A. National heart, lung, and blood institute ARDS clinical trials network higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N. Engl. J. Med. 2004, 351, 327–336. [CrossRef] [PubMed]
- Thachil, J.; Tang, N.; Gando, S.; Falanga, A.; Cattaneo, M.; Levi, M. ISTH interim guidance on recognition and management of coagulopathy in COVID-19. J. Thromb. Haemost. 2020, 18, 1023–1026. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, H.P.; Timerman, S.; Rodrigues, R.D.R.; Corrêa, T.D.; Schubert, D.U.C.; Freitas, A.P. Position statement: cardiopulmonary resuscitation of patients with confirmed or suspected COVID-19-2020. Arq. Bras. Cardiol. 2020, 114, 1078–1087. [Google Scholar] [CrossRef] [PubMed]
- Soto, M.E.; Pérez-Torres, I.; Manzano-Pech, L.; Soria-Castro, E.; Morales-Marín, A.; Ramírez-Marroquín, E.S.; Martínez-Hernández, H.; Herrera-Alarcón, V.; Guarner-Lans, V. Reduced levels of selenium and thioredoxin reductase in the thoracic aorta could contribute to aneurysm formation in patients with Marfan syndrome. Int. J. Mol. Sci. 2023, 24, 10429. [Google Scholar] [CrossRef] [PubMed]
- Erel, O.; Neşelioğlu, S. Erel, O.; Neşelioğlu, S.; Tunçay,M.E.; Oğuz, E.F.; Eren, F.; Akkuş, M.S.; Güner, H.R.; Ateş, İ.. A sensitive indicator for the severity of COVID-19: thiol. Turk. J. Med. Sci. 2021, 51, 921–928. [Google Scholar] [CrossRef]
- Anderson, G.; Reiter, R.J. Melatonin: Roles in influenza, Covid-19, and other viral infections Rev. Med. Virol. 2020, 30, e2109. [Google Scholar] [CrossRef]
Figure 1.
Activity of the peroxidases (panel A) and ecSOD (panel B) in HS and COVID-19 patients with the treatment before and after treatment with MT. The activities of both enzymes were evaluated on native polyacrylamide gels at 10%. In the first line of both gels, the activity of the commercial enzyme is observed (radish peroxidase and bovine SOD-2 respectively), the graphic shown in blot boxes and whiskers in percentiles 75, 25, median, midline and outliers. Abbreviations ecSOD= Extracellular superoxide dismutase, HS= Healthy subjects, MT= Melatonin.
Figure 1.
Activity of the peroxidases (panel A) and ecSOD (panel B) in HS and COVID-19 patients with the treatment before and after treatment with MT. The activities of both enzymes were evaluated on native polyacrylamide gels at 10%. In the first line of both gels, the activity of the commercial enzyme is observed (radish peroxidase and bovine SOD-2 respectively), the graphic shown in blot boxes and whiskers in percentiles 75, 25, median, midline and outliers. Abbreviations ecSOD= Extracellular superoxide dismutase, HS= Healthy subjects, MT= Melatonin.
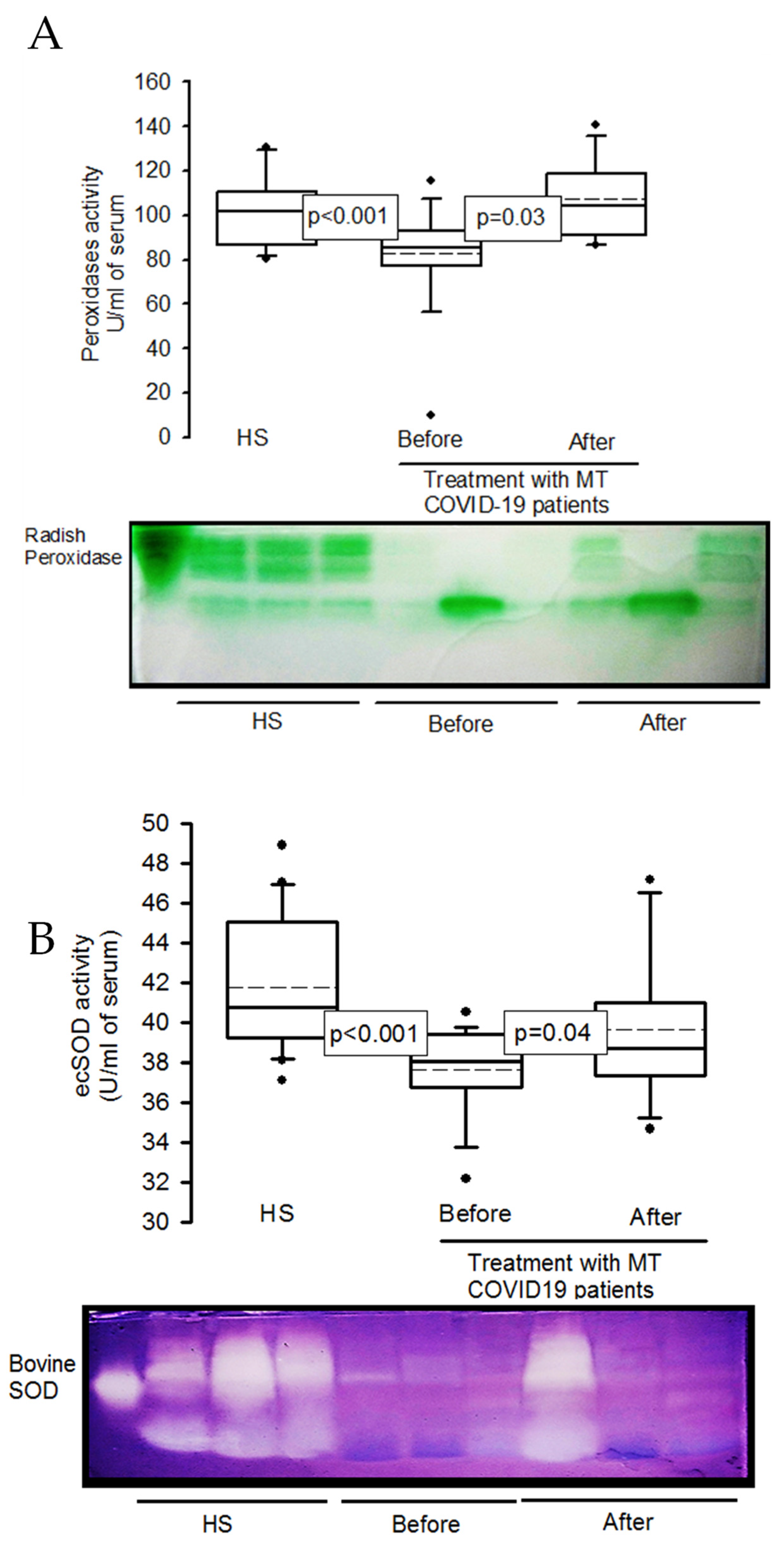
Figure 2.
Oxidative stress markers in HS and patients with COVID-19 before and after treatment with MT. The total carbonyl concentration and LPO index increased in the serum of COVID-19 patients compared to HS, but MT treatment decreased the carbonyl concentration and LPO index in COVID-19 patients. The TAC, NO2–, thiol and GSH concentration groups showed a significant decrease in COVID-19 patients compared to HS, but after treatment with MT these variables increased. Panel (A) carbonyls. Panel (B) lipid peroxidation index. Panel (C) total antioxidant capacity. Panel (D) nitrites. Panel (E) thiol groups and Panel (F) reduced glutathione. Abbreviations: LPO= lipid peroxidation, TAC= total antioxidant capacity, NO2-= nitrites, GSH= reduced glutathione.
Figure 2.
Oxidative stress markers in HS and patients with COVID-19 before and after treatment with MT. The total carbonyl concentration and LPO index increased in the serum of COVID-19 patients compared to HS, but MT treatment decreased the carbonyl concentration and LPO index in COVID-19 patients. The TAC, NO2–, thiol and GSH concentration groups showed a significant decrease in COVID-19 patients compared to HS, but after treatment with MT these variables increased. Panel (A) carbonyls. Panel (B) lipid peroxidation index. Panel (C) total antioxidant capacity. Panel (D) nitrites. Panel (E) thiol groups and Panel (F) reduced glutathione. Abbreviations: LPO= lipid peroxidation, TAC= total antioxidant capacity, NO2-= nitrites, GSH= reduced glutathione.
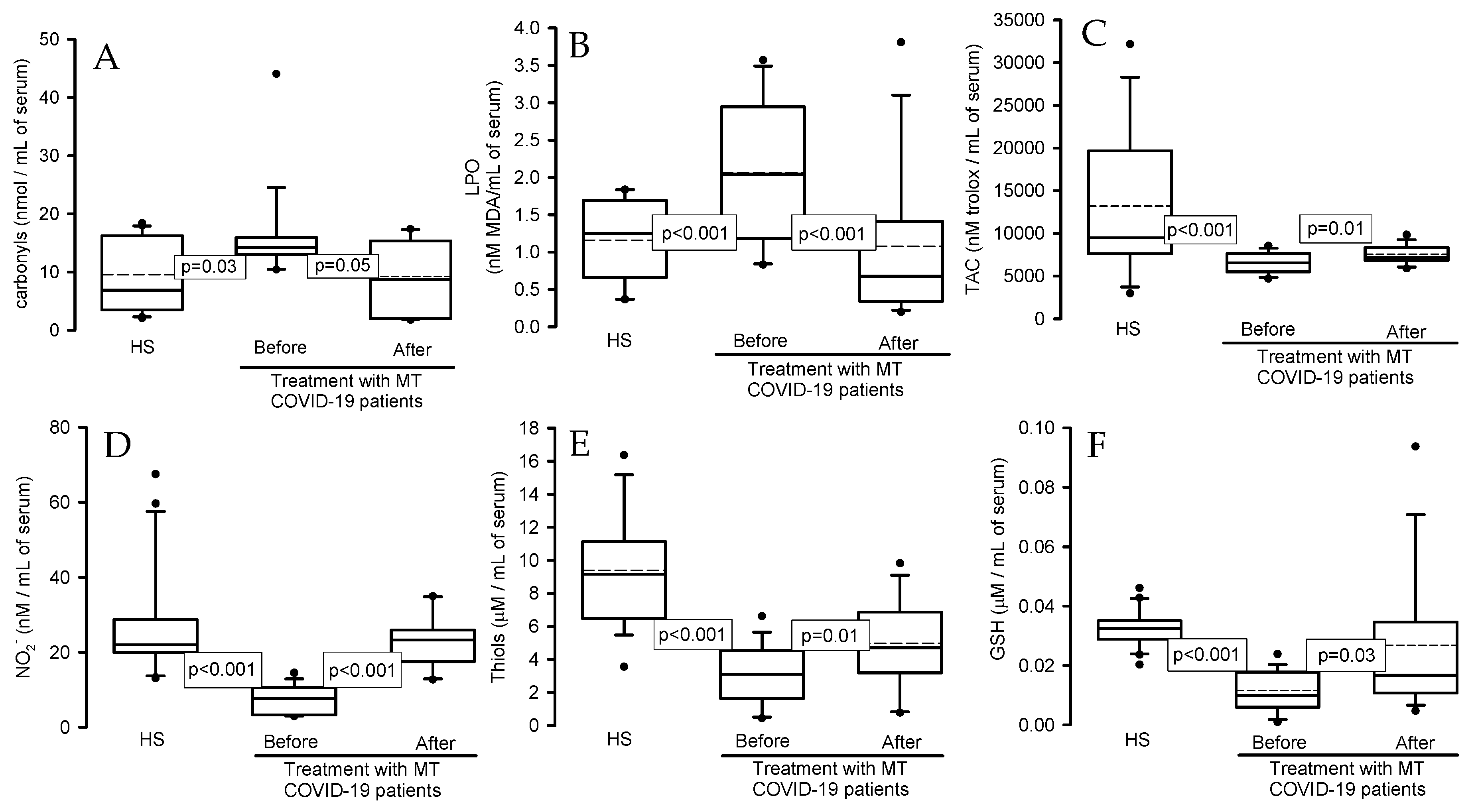
Figure 3.
Representative electron micrograph of lung tissue from: A: Cytochrome C, C: COX II and E: GPX4 = COVID-19 patient, postmortem sample from a 68-year-old female patient with COVID-19 that had associated comorbidities of ischemic heart disease, type II diabetes, morbid obesity, and hypertension, B: Cytochrome C, D: COX II and F: GPX4 = postmortem sample from a biopsy from a 59-year-old female control subject with hypertension, obesity, type 2 diabetes, and pneumonia. The arrows indicate the presence of the immune colloidal for Cytochrome C, COX II and GPX4 respectively. In patients with COVID-19, rupture of the mitochondrial membrane was evident. The images were taken at 50,000× with a Jeol JEM-1011 electron microscope (JEOL Ltd., Tokyo, Japan) to 60 kilovolts equipped with AMT 542.391 analysis software.
Figure 3.
Representative electron micrograph of lung tissue from: A: Cytochrome C, C: COX II and E: GPX4 = COVID-19 patient, postmortem sample from a 68-year-old female patient with COVID-19 that had associated comorbidities of ischemic heart disease, type II diabetes, morbid obesity, and hypertension, B: Cytochrome C, D: COX II and F: GPX4 = postmortem sample from a biopsy from a 59-year-old female control subject with hypertension, obesity, type 2 diabetes, and pneumonia. The arrows indicate the presence of the immune colloidal for Cytochrome C, COX II and GPX4 respectively. In patients with COVID-19, rupture of the mitochondrial membrane was evident. The images were taken at 50,000× with a Jeol JEM-1011 electron microscope (JEOL Ltd., Tokyo, Japan) to 60 kilovolts equipped with AMT 542.391 analysis software.
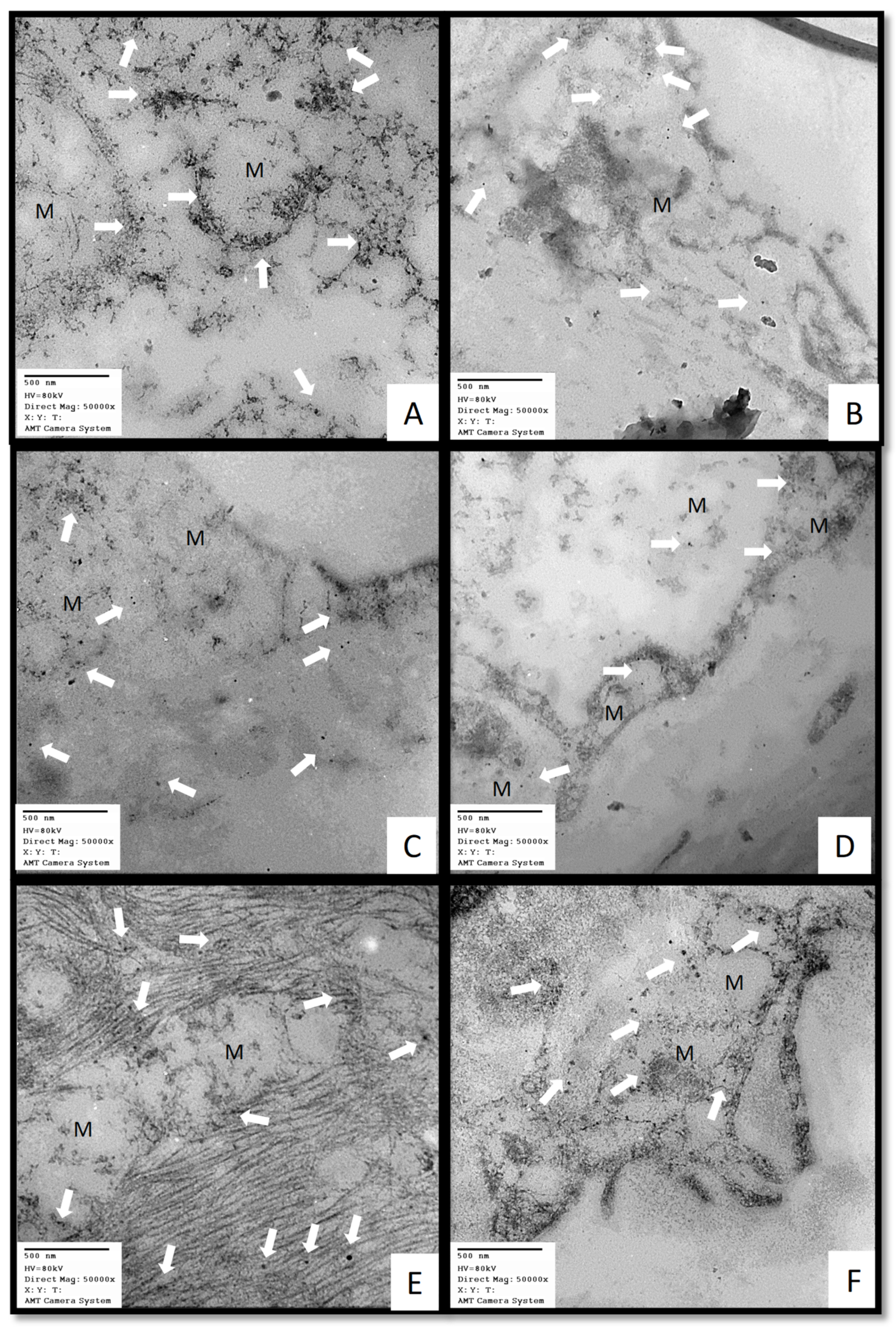
Figure 4.
The adjuvant therapy with the treatment with MT may contribute to restores the redox homeostasis which is altered in COVID-19 patients, favors the activity of the antioxidant enzymes such as GPX, GST, GR, ecSOD, peroxidases and increases the marker of OS such as thiols, GSH NO2–. This contributes to decrease the carbonyls and LPO leading to an increase of the TAC. Furthrmore, MT is capable of modulating glucose homeostasis because it functions as a glycolytic agent since it inhibits the Warburg effect. Abbreviations: GPx =Glutathione peroxidase, GR =Glutathione reductase, GSH =Glutathione, GSSG =Oxidized glutathione, H2 O2 =Hydrogen peroxide, LPO =Lipoperoxidation, O2– =Superoxide anion, OH =Hydroxyl, SOD =Superoxide dismutase, HOCl =Hypochlorous acid, ACE2 =Angiotensin-converting enzyme 2, MT = Melatinin receptor, TMPRSS2= serine protease.
Figure 4.
The adjuvant therapy with the treatment with MT may contribute to restores the redox homeostasis which is altered in COVID-19 patients, favors the activity of the antioxidant enzymes such as GPX, GST, GR, ecSOD, peroxidases and increases the marker of OS such as thiols, GSH NO2–. This contributes to decrease the carbonyls and LPO leading to an increase of the TAC. Furthrmore, MT is capable of modulating glucose homeostasis because it functions as a glycolytic agent since it inhibits the Warburg effect. Abbreviations: GPx =Glutathione peroxidase, GR =Glutathione reductase, GSH =Glutathione, GSSG =Oxidized glutathione, H2 O2 =Hydrogen peroxide, LPO =Lipoperoxidation, O2– =Superoxide anion, OH =Hydroxyl, SOD =Superoxide dismutase, HOCl =Hypochlorous acid, ACE2 =Angiotensin-converting enzyme 2, MT = Melatinin receptor, TMPRSS2= serine protease.
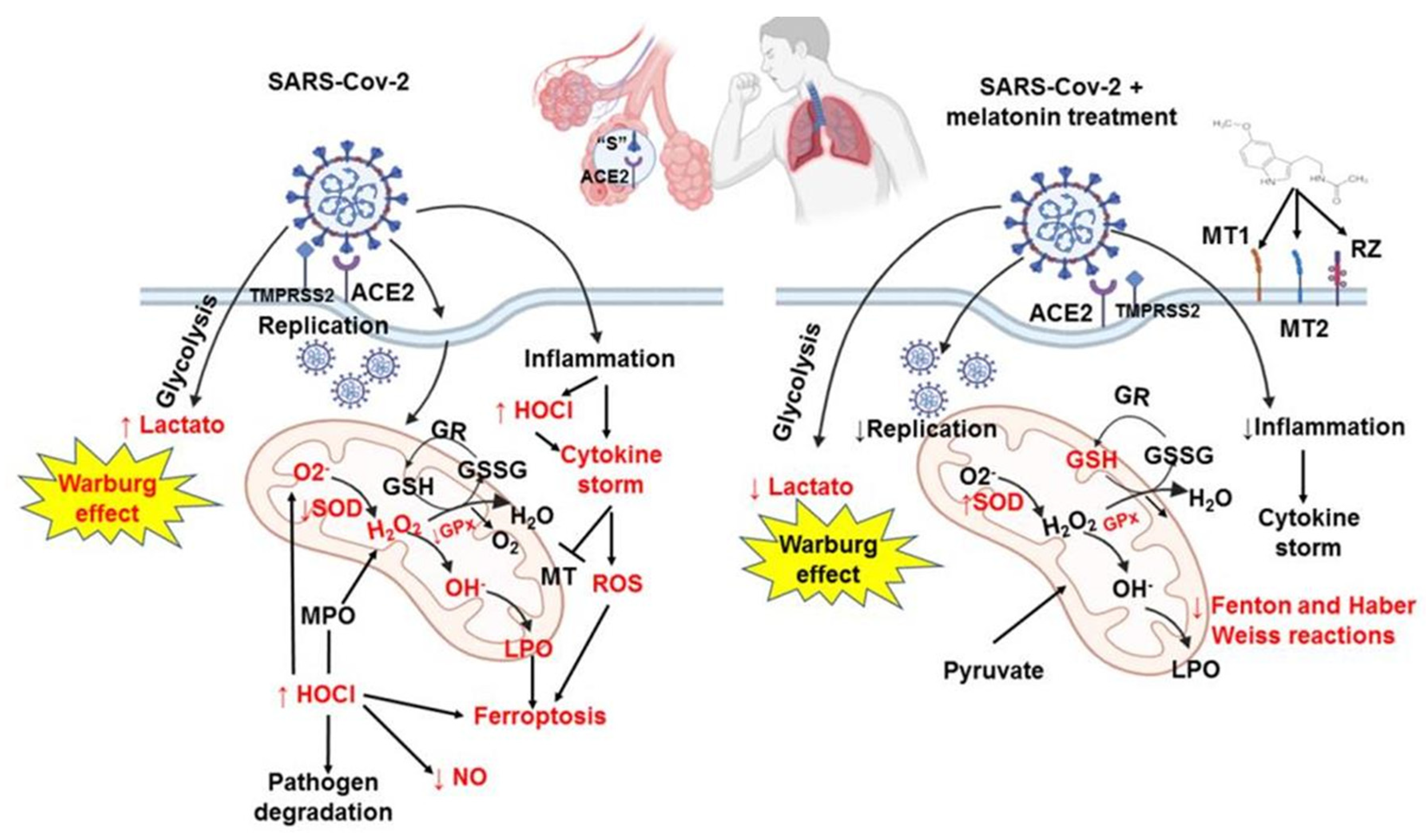
Figure 5.
study flow diagram.
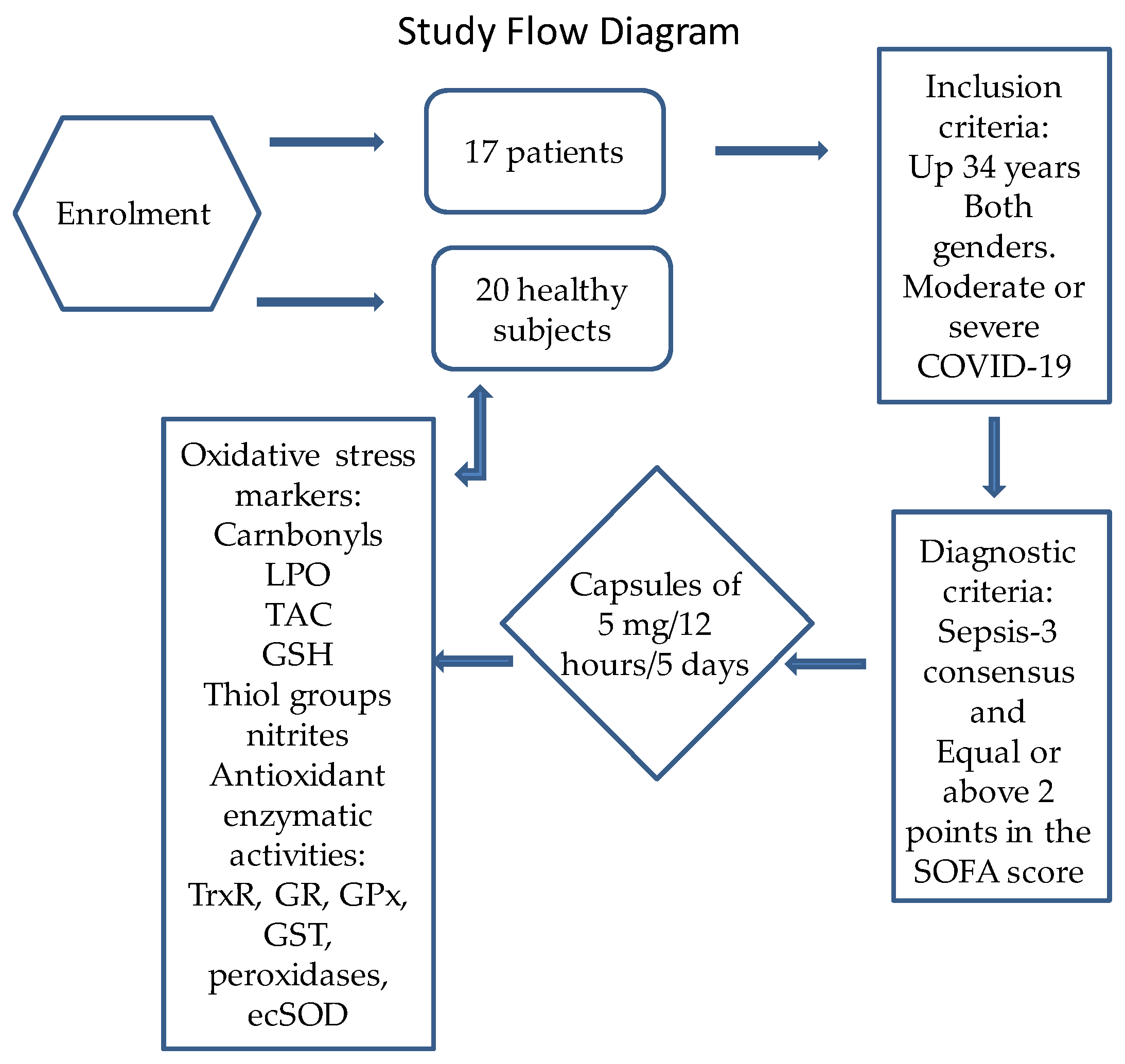

Table 1.
Demographic characteristics in the COVID-19 patients at admission, before and after of the treatment with MT.
Table 1.
Demographic characteristics in the COVID-19 patients at admission, before and after of the treatment with MT.
| Variables | Median and (Min–Max range) |
|---|---|
| Age | 62 (34-84) |
| Body mass index | 30 (20-37) |
| Comorbidities (%) | |
| Diabetes Mellitus | 11 (65) |
| Hypertension | 7 (41) |
| Dyslipidemia | 10 (59) |
| Chronic obstructive pulmonary disease | 1 (6) |
| Normal Weight | 6 (35) |
| Overweight | 3 (18) |
| Obesity | 8 (47) |
| Gasometry and blood biochemistry median and (Min–Max range) | |
| PaO2 | 79 (58-152) |
| PCO2 | 31 (27-36) |
| PaO2/FIO2 (mmHg) | 145 (49-243) |
| SPO2/FIO2 (mmHg) | 160 (50-280) |
| Heart Rate lpm | 84 (58-106) |
| Mean arterial pressure (mmHg) | 82 (65-99) |
| Temperature °C | 36.5 (35.9- 37.2) |
| Creatinine in serum mg/dL | 0.80 (0.60-2.5) |
| Blood urea nitrogen mg/dL | 18.6 (5.8-77.7) |
| Leukocytes 10ˆ3/µL | 10.1 (5.3-22.6) |
| Lymphocytes 10ˆ3/µL | 0.66 (0.39-1.29) |
| Platelets 10ˆ3/µL | 275 (180-576) |
| Ferritin ng/mL | 665.7 (175-2354) |
| D-dimer ng/dL | 655 (27-35,200) |
| C reactive protein mg/dL | 145 (37-308) |
| Procalcitonin ng/dL | 0.40 (0.06-34.7) |
| Score median and (Min-Max range) | |
| SOFA | 2 (1-8) |
| APACHE | 5 (4-7) |
| SAPS | 26.5 (13-31) |
| Days with mechanic ventilation | 2 (1-2) |
| Days in ICU | 14.5 (6-20) |
Abbreviations: IL= interleukin, N/L= neutrophils and/or lymphocytes. FiO2= fraction of inspired oxygen, PAO2= oxygen at arterial pressure, PCO2= carbon dioxide at partial pressure, SpO2= arterial oxygen saturation, TG= triglycerides. SOFA= Organ Failure Sequential Assessment, APACHE= Acute Physiology and Chronic Health Assessment II, SAPS= Simplified Acute Physiology, II Score.
Table 2.
Blood biochemical variables in healthy subjects.
| Variable | Median (Min–Max range) |
|---|---|
| Gender | 15 men and 5 female |
| Age | 57 (27–87) |
| Glucose (mg/dL) | 105.50 (32.00–148.00) |
| Uric acid (mg/dL) | 6.65 (2.95–9.60) |
| Cholesterol (mg/dL) | 166.50 (108.00–276.00) |
| HDL (mg/dL) | 37.00 (24.20–54.60) |
| LDL (mg/dL) | 93.35 (54.20–146.00) |
| TG (mg/dL) | 122.50 (67.50–369.00) |
| C reactive protein (mg/dL) | 1.43 (1.18–9.02) |
| Atherogenic index | 2.60 (0.26–4.48) |
Abbreviations: HDL= high-density, lipoproteins, LDL= low-density lipoproteins, TG= triglycerides.
Table 3.
Blood biochemical variables and HOMA-index in the COVID-19 patients before and after of the treatment with MT.
Table 3.
Blood biochemical variables and HOMA-index in the COVID-19 patients before and after of the treatment with MT.
| Variable | BeforeMedian (min – max range) | AfterMedian (min – max range) |
|---|---|---|
| Glucose (mg/dL) | 204.38 (96.49–460.52)* 1.30 (0.10–10.10) 9.71 (1.67–100.15) | 139.47 (79.82–321.05) 1.30 (0.20–3.70) 8.63 (0.82–64.18) |
| Insulin (ng/mL) | ||
| HOMA-Index | ||
| IL-6 (pg/mL) | 43.28 (7.8–388)** | 7.8 (7.8–128.28) |
| HDL (mg/dL) | 29.9 (14.5–51.30)† | 57.8 (23–90) |
| LDL (mg/dL) | 83.1 (40.7–108.20) | 86.1 (65.5–132) |
| Total cholesterol (mg/dL) | 141 (76–196) | 146 (130–227) |
| TG (mg/dL) | 140 (37–325) | 205 (79–295) |
| Before vs. after of the treatment with MT *p=0.05, **p=0.02, † NS (0.09). Abbreviations: IL= Interleukin, HDL= High-density lipoproteins, LDL= Low-density lipoproteins, TG= Triglycerides | ||
Table 4.
Activities of the four antioxidant enzymes that employ glutathione in COVID-19 patients before and after treatment with melatonin.
Table 4.
Activities of the four antioxidant enzymes that employ glutathione in COVID-19 patients before and after treatment with melatonin.
| Activities enzymes | HS | SARS-CoV-2 infection | |
|---|---|---|---|
| (min/mL of serum) | Before of the treatment with MTMedian (Min-Max range) | After of the treatment with MTMedian (Min-Max range) | |
| GPx (nmol NADPH) | 0.68 (0.08–2.03) | 0.21 (0.05–0.91)*** | 1.15 (0.8–1.44)*** |
| Q1, Q3, IQR | 0.49, 1.64, 1.14 | 0.15, 0.56, 0.41 | 1.05, 1.20, 0.14 |
| TxrR (TNB nmol) | 6.91–3 (–4.4–3–0.02) | 3.14–3 (–1.5–3–8.8–3)*** | 3.30–3 (9.4–3–8.4–3) |
| Q1, Q3, IQR | 3.14–3, 1.42–2, 1.10–2 | 2.20–3, 4.79–3, 2.59–3 | 2.83–3, 5.89–3, 3.06–3 |
| GST (GS-DNB μmol) | 3.37–4 (7.95–5–7.95–4) | 7.95–5 (–1.59–4–1.59–4)*** | 1.59–4 (3.9–5–4.77–4)* |
| Q1, Q3, IQR | 1.39–4, 4.37–4, 2.98–4 | 7.95–5, 1.19–4, 3.97–5 | 9.96–5, 2.9–4, 2.38–4 |
| GR (units) | 1.93 (1.16–10.24) | 1.64 (0.19–2.70)* | 2.32 (0.96–5.60)*** |
| Q1, Q3, IQR | 1.40, 2.61, 1.20 | 0.48, 2.03, 1.54 | 1.45, 3.48, 2.03 |
| HS vs. Before SARS-CoV-2 ***p=0.001, before of the MT vs. after of the MT *p=0.01. Abbreviations: GPx= Glutathione peroxidase, TrxR= Thioredoxin reductase, GST= Glutathione-S-transferase, GR= gluthatione reductase, Q1= first quartile, Q2= second quartile, IQR= interquartile range. The results shown median. First quartile, second quartile, interquartile range and min and max range. | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



