
Submitted:
19 January 2024
Posted:
30 January 2024
You are already at the latest version
Abstract
Nerve-sparing vs. non nerve sparing surgery (NSS vs. non-NSS) is associated with improved functional outcomes in prostatectomy patients. The aim of the present study is to compare the oncological outcomes of patients with high-risk localized prostate cancer undergoing nerve-sparing and non nerve-sparing robot-assisted radical prostatectomy (RARP).
Between November 2002 and December 2018, we prospectively recorded data of patients undergoing RARP for high-risk localized prostate cancer (PCa). NSS (nerve-sparing surgery) was offered based on preoperative clinical characteristics of patients and intraoperative assessment. Patients were stratified into 2 groups according to NSS. The primary outcome was biochemical recurrence (BCR), while positive surgical margin (PSM) and cancer-specific survival (CSS) were secondary outcomes. Logistic regression was used to investigate predictive factors. A total of 779 patients were included in the study, 429 (55.1%) underwent NSS while 350 (44.9%) underwent a non-NSS. After a mean (±SD) follow-up of 192 (±14) months, 328 (42.1%) patients developed BCR, no significant difference was found between NSS and non-NSS group (156 vs. 172; p=0.09). Both univariable and multivariable analysis found that nerve-sparing approach was not a predictor of BCR (p>0.05). NSS vs. non-NSS was not associated with worse oncological outcomes in patients with high-risk PCa
Keywords:
prostate cancer
; robotic prostatectomy
; functional outcomes
1. Introduction
Although radical prostatectomy (RP) is the standard of care in localized prostate cancer (PCa), traditionally, surgery may not be preferred over radiotherapy plus androgen deprivation therapy (ADT) in patients with high-risk prostate cancer [1], due to the expected poor oncological and functional outcomes in this population [2]. Even today, about 20-30% of patients are diagnosed with a high-risk PCa, showing worse histological characteristics, increased risk of positive surgical margins, biochemical recurrence (BCR), disease progression, and mortality [3].
However, several studies have shown that surgery can be offered in selected high-risk patients, often in the context of multimodal treatment [3]. The feasibility of RARP is proven by the associated oncological and functional outcomes. In fact, approximately 25-30% of patients with high-risk prostate cancer undergoing RARP remain free of biochemical recurrence at 10 years [4]. The preservation of neurovascular bundles can result in better postoperative functional outcomes (both erection and urinary continence) [5]. The robotic approach allows a better visualization of anatomical structures and a greater precision of movement, making nerve-sparing (NS) RARP capable to yield an overall potency rate of ≥ 50%, with an early return of continence in 44-72% of cases [6].
Nerve-sparing surgery (NSS) does not compromise oncological outcomes if patients are carefully selected. According to current European Urology Association (EAU) guidelines, NSS should be performed when there is a low-risk of extracapsular extension (based on cT stage, ISUP grade, nomogram, multiparametric MRI). Therefore, the guidelines do not recommend using NSS in high-risk PCa but do not exclude it either.
The aim of this study was to compare oncological outcomes of patients with high-risk localized prostate cancer undergoing RARP with and without NSS..
2. Materials and Methods
We designed a single-center, two-arm, prospective study at our tertiary referral center (Karolinska Institutet, Solna, Sweden), enrolling patients between November 2002 and December 2018. The oncological outcomes were updated to January 2022. The study was conducted in accordance with the Declaration of Helsinki [7] on ethical principles for medical research involving human subjects, and each patient provided a written informed consent to participate. Ethics committee approval was obtained prior to patient enrollment.
2.1. Patient enrollment and stratification
Consecutive patients with localized high-risk PCa undergoing RARP were included in the study. Subjects who received prior pelvic radiation, focal therapy for PCa, androgen deprivation therapy (ADT), surgery for benign prostatic hyperplasia, or salvage RARP were excluded from the study.
According to EAU guidelines, high-risk localized PCa was defined on the basis of the following criteria: Prostate Specific Antigen (PSA) >20 ng/ml or Gleason score (GS) >7 or cT2c. PCa characterized by cT3-4 or cN+ (high-risk locally-advanced) were excluded. RARP was offered after appropriate patient counseling and multidisciplinary case discussion. Type of surgery was chosen by the surgeon after a scrupulous evaluation of the preoperative clinical characteristics of patient and disease (as reported in the “Patient assessment” section), as well as of the intraoperative condition. No nomogram was used to predict the risk of extracapsular extension. Patients were retrospectively stratified into 2 groups based on NSS (yes/no) for the assessment of the oncological outcomes. Some subjects underwent unilateral NSS, they were classified in the NSS group but additional analyzes were performed between unilateral and bilateral NSS.
2.2. Surgical details
Radical prostatectomies were performed by 10 surgeons with robot-assisted technique using a daVinci® Surgical System (Intuitive Surgical, USA). NS dissection was either intra-fascial (dissection in the plane between the prostatic capsule and the periprostatic fascia) or inter-fascial (dissection in the plane between the periprostatic and endopelvic fascia). Non-NS was either partial non-NS (leaving most of the neurovascular bundle on the prostate) or entirely non-NS. Depending on tumor location, apical dissection was either with maximum urethral length, at the level of the apex, or with a margin from the apex. Bladder neck-sparing dissection was avoided in patients with suspicion of bladder-neck invasion.
2.3. Patient assessments and Measured outcomes
All patients underwent a thorough medical history, digital rectal examination (DRE), PSA dosage, transrectal prostate biopsy, and staging imaging before surgery. The histological findings of the biopsies (GS, number, percentage, and location of positive cores) were recorded. Bone scan, abdominal-pelvic computed tomography (CT), and from 2013 multiparametric magnetic resonance imaging (mpMRI) were the imaging techniques used in all patients for staging purposes. Postoperative histological data (pT, pN, postoperative GS, surgical margins status) and need for adjuvant therapy (radiotherapy, ADT) were reported. Erectile function and urinary continence were evaluated preoperatively to decide whether or not NSS was appropriate. More specifically, the International Index of Erectile Function-Erectile Function (IIEF-EF) was self-administrated to all patients, the 24-hour pad weight test was used in in patients who reported any urine leakage. IIEF-EF ≤ 16 points or pad weight test > 100g/24h were considered contraindications to NSS.
Primary oncological outcome evaluated was BCR. Secondary oncological outcomes assessed were positive surgical margins (PSM) and cancer-specific survival (CSS). According to EAU guidelines [8], BCR after radical prostatectomy was defined as PSA > 0.4 ng/mL and rising. Positive surgical margins (PSM) were defined as the presence of tumor tissue on the inked surface of the specimen [9].
2.4. Statistics
The categorical variables were described as frequencies and percentages. The quantitative variables were reported as means and standard deviations (SD) as well as medians and interquartile ranges (IQR). The ANOVA (continuous variables) and the Tukey-Kramer test (discrete variables) were used to conduct multiple group comparisons. Kaplan-Meier curve for BCR and multivariate logistic regression analysis to identify main predictors of BCR and CSS were performed. Supportive analysis was performed in order to confirm that the nerve-sparing technique did not influence the risk of biochemical recurrence. Established risk factors including pre-operatory PSA levels (analyzed as a continuous variable), Gleason score at prostatectomy (analyzed as a dichotomous variable) and pathologic stage (analyzed as a dichotomous variable) were simultaneously assessed using logistic regression as predictors of biochemical recurrence along with the use of nerve-sparing technique. P-value threshold was arbitrarily set at 0.05. IBM SPSS Statistics (IBM Corp Released 2017; IBM SPSS Statistics for Windows, Version 25.0; Armonk, NY: IBM Corp) was used for the statistical analyses.
3. Results
T A total of 779 patients were included in the study. Mean (±SD) age and PSA were 63 (±6.4) years and 14 (±14) ng/mL, respectively. Most common bioptic GS was 3+4 (25.7%) (Table 1). Overall, 429 (55.1%) underwent NSS, while 350 (44.9%) underwent a non-NSS. Adjuvant therapy was administrated to 49 (11.4%) and 90 (25.7%) patients in NSS and non-NSS group, respectively (p=0.07). No difference between NSS and non-NSS group in pT and pN (p>0.05). Noteworthy, most tumors were ≥ pT3a (non-NSS 71.1%, NSS 69.0%), but only a minority of tumors were pN1 (non-NSS 10.3%, NSS 7.0%). PSM was reported after RARP in 254 (32.6%) patients, with no significant difference between NSS and non-NSS group (143 vs. 111; p=0.5) (Table 2). Focality (p=0.3), length(p=0.5), and localization (p=0.5) of the PSM were not statistically related to the type of NS approach (Table 2).
After a mean (±SD) follow-up of 192 (±14) months, 328 (42.1%) patients developed BCR. No significant difference was found between the NSS and the non-NSS group in terms of biochemical recurrence rate (Table 4). Both univariable and multivariable analysis found that NS approach was not generally a predictor of BCR (p>0.05), although Bilateral NS vs NO-NS was associated with increased odds of biochemical recurrence (Table 3). Kaplan Mayer Survival curves for BCR (Figure 1) showed no significant difference among non-NSS, unilateral NSS, and bilateral NSS (long rank test=0.6) (Figure 1).
Mean (±SD) CSS was 70.5 (±26.1) months. No significant difference was described between NSS and non-NSS group (mean CSS, 70,3 vs. 70,7 months). (Table 3).
Both univariable and multivariable analysis showed that NS approach was not a predictor of CSS (p>0.05). Further analysis showed that Nerve sparing surgery was not predictive of biochemical recurrence (OR =0.83; 95% CI =0.60 to 1.14; P = 0.25), after adjusting for pre-operative PSA levels, preoperative Gleason score, age and clinical stage). After adjusting for these same four variables, no association between nerve-sparing surgery and biochemical recurrence was either found when the sub-groups of patients with negative surgical margins (n=488; OR = 0,86; 95% CI=0.58 to 1.28; P = 0.46), postero-lateral only positive surgical margins (n=109; OR = 0.76; 95% CI=0.32 to 1.79; p=0.54) and positive margins other than postero-lateral (n=132; OR = 0.78; 95%CI=0.37 to 1.64;p= 0.52) were separately considered in order to explore the potential interaction of margin status with nerve-sparing surgery as a predictor of biochemical recurrence. Furthermore, nerve-sparing surgery was not predictive of biochemical recurrence even after adjusting for preoperative PSA, pathologic T stage, Gleason score at prostatectomy, age, length of positive surgical margin, lymph-node status. Finally, nerve sparing surgery was not associated with margin status (negative vs. postero-lateral positive vs. non postero-lateral positive, Chi square test, p=0.08)
4. Discussion
Several cohort studies have reported encouraging functional outcomes achieved using a NS approach in patients undergoing RARP[10]. In a retrospective study conducted by Menon [11] et al. and including a total of 1142 prostate cancer patients undergoing NS-RARP followed-up for at least 12 months, 93% of men with no preoperative erectile dysfunction were able to perform intercourse, with an actuarial 5-year BCR rate of 8.4% and a median duration of incontinence of 4 weeks. This cohort included only 8.2% of patients with high-risk prostate cancer. Another smaller, more recently conducted study [12] enrolled 105 prostate cancer patients who underwent intrafascial NS-RARP and were followed-up for 26.5 months (IQR 15.25–48). Importantly, 6- and 12-month postoperative erectile function recovery rates were 88.6% and 94.3%, with an overall positive surgical margins rate of 16.2% and an overall BCR rate of 6.7%. Also in this study, patients with high-risk prostate cancer represented a minority of the study sample (18.1%). Conversely, worse sexual recovery rates were reported in a study by Dell’Oglio [13] et al including a total of 340 men undergoing Retzius-sparing RARP for high-risk prostate cancer, of whom approximately a third showed BCR during follow-up. In the subgroup of 111 men who were assessable for sexual recovery because they were pre-operatively potent, underwent full or partial NSS and were adequately follow-up, only 43.1 and 50% had achieved sexual recovery at 1 and 2 years, respectively. The lower sexual recovery rate reported by Dell’Oglio et al. may be due to the substantial proportion of patients who underwent unilateral NS, which is less effective compared to bilateral NS in preserving potency [14]. Also, NS-RARP seems to yield improved functional outcomes compared to NS laparoscopic radical prostatectomy (LRP). Asimakopoulos et al.[15] assessed pentafecta outcomes associated with RARP vs. LRP after a bilateral NS approach, that is combined oncological and functional outcomes along with assessment of surgical margins and evaluation of early post-surgical complications. Importantly, the authors reported that 45.6% vs. 27.5% of patients achieved pentafecta following RARP vs. LRP. Ou et al. reported a pentafecta rate of 60.4% in a prospective cohort of 230 prostate cancer patients undergoing bilateral NS-RARP [16] while Jazayeri el al. reported a pentafecta rate of 73.9% in a retrospective study of 566 prostate cancer patients treated with NS-RARP [17]. Overall, these summarized findings suggest that NS-RARP has a tremendous potential for improved functional outcomes, while its potentially negative implications in terms of oncologic outcomes require to be further investigated, especially in patients at higher risk of recurrence.
In our prospective cohort of men receiving NS- and non-NS- RARP, who were followed up for a mean time > 10 years, we focused on oncological outcomes only and could prove that the NSS was not associated with any detrimental effect in terms of positive margin rate, BCR rate as well as CSS. Of note, these results were achieved in a population of men affected by high-risk prostate cancer, with approximately 70% of patients showing ≥pT3a disease, which supports the notion that a NS approach can be adopted in selected men with high-risk PCa.
Our study has several strengths, which include large sample size, long follow-up period, and prospective design. On the other side, our research presents multiple limitations. Although comparison between patients receiving with NS- vs. non-NS- RARP was the main study objective, the study design did not include any sample size calculation to assess non-inferiority of the techniques between them. In this regard, it must be noted that BCR rate was numerically (albeit not significantly) superior in NS- vs. non-NS- RARP patients. We are uncertain whether a larger sample size may have allowed to reach statistically significance. Furthermore, patients were not randomized to NS- vs. non-NS- RARP, so we cannot exclude that the two groups were actually unbalanced for some clinically meaningful variable that we could not account for, and patients at lower risk of recurrence may have been more likely to receive NS-RARP.
In conclusion, we conducted a large prospective study to assess the potential differences in oncological outcomes in high-risk PCa patients receiving NS- vs. non-NS- RARP and followed-up for > 10 years. No statistically significant difference in either positive margin rate, BCR, or CSS was reported. Our data therefore add evidence to support the use of a NS approach in high-risk PCa patients undergoing RARP. Further well-designed RCT are needed to confirm our promising results.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Sooriakumaran P, Pavan N, Wiklund PN, Roach 3rd M. Surgery Versus Radiation for High-risk Prostate Cancer: The Fight Continues. But Is It Time To Call a Draw and Reach Consensus? Eur Urol [Internet]. 2019 Apr 1;75(4):556–7. [CrossRef]
- Mossanen M, Nepple KG, Grubb RL 3rd, Androile GL, Kallogjeri D, Klein EA, et al. Heterogeneity in Definitions of High-risk Prostate Cancer and Varying Impact on Mortality Rates after Radical Prostatectomy. Eur Urol Oncol. 2018 Jun;1(2):143–8. [CrossRef]
- Kishan AU, Karnes RJ, Romero T, Wong JK, Motterle G, Tosoian JJ, et al. Comparison of Multimodal Therapies and Outcomes Among Patients With High-Risk Prostate Cancer With Adverse Clinicopathologic Features. JAMA Netw open. 2021 Jul;4(7):e2115312. [CrossRef]
- Abdollah F, Sood A, Sammon JD, Hsu L, Beyer B, Moschini M, et al. Long-term cancer control outcomes in patients with clinically high-risk prostate cancer treated with robot-assisted radical prostatectomy: results from a multi-institutional study of 1100 patients. Eur Urol. 2015 Sep;68(3):497–505. [CrossRef]
- Deng W, Chen R, Zhu K, Cheng X, Xiong Y, Liu W, et al. Functional Preservation and Oncologic Control following Robot-Assisted versus Laparoscopic Radical Prostatectomy for Intermediate- and High-Risk Localized Prostate Cancer: A Propensity Score Matched Analysis. J Oncol. 2021;2021:4375722. [CrossRef]
- Tavukçu HH, Aytac O, Atug F. Nerve-sparing techniques and results in robot-assisted radical prostatectomy. Investig Clin Urol [Internet]. 2016/12/08. 2016 Dec;57(Suppl 2):S172–84. Available from: https://pubmed.ncbi.nlm.nih.gov/27995221. [CrossRef]
- Association, WM. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA [Internet]. 2013 Nov 27;310(20):2191–4. [CrossRef]
- Cornford P, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M, et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II-2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur Urol. 2021 Feb;79(2):263–82. [CrossRef]
- Choo R, Danjoux C, Gardner S, Morton G, Szumacher E, Loblaw DA, et al. Prospective study evaluating postoperative radiotherapy plus 2-year androgen suppression for post-radical prostatectomy patients with pathologic T3 disease and/or positive surgical margins. Int J Radiat Oncol Biol Phys. 2009 Oct;75(2):407–12. [CrossRef]
- Kumar A, Patel VR, Panaiyadiyan S, Seetharam Bhat KR, Moschovas MC, Nayak B. Nerve-sparing robot-assisted radical prostatectomy: Current perspectives. Asian J Urol. 2021 Jan;8(1):2–13. [CrossRef]
- Menon M, Shrivastava A, Kaul S, Badani KK, Fumo M, Bhandari M, et al. Vattikuti Institute prostatectomy: contemporary technique and analysis of results. Eur Urol. 2007 Mar;51(3):648. [CrossRef]
- Shin TY, Lee YS. Robot-assisted radical prostatectomy with clipless intrafascial neurovascular bundle-sparing approach: surgical technique and one-year functional and oncologic outcomes. Sci Rep. 2020 Oct;10(1):17595. [CrossRef]
- Dell’Oglio P, Tappero S, Longoni M, Buratto C, Scilipoti P, Secco S, et al. Retzius-sparing Robot-assisted Radical Prostatectomy in High-risk Prostate Cancer Patients: Results from a Large Single-institution Series. Eur Urol open Sci. 2022 Apr;38:69–78. [CrossRef]
- Greco F, Hoda MR, Wagner S, Reichelt O, Inferrera A, Magno C, et al. Bilateral vs unilateral laparoscopic intrafascial nerve-sparing radical prostatectomy: evaluation of surgical and functional outcomes in 457 patients. BJU Int. 2011 Aug;108(4):583–7. [CrossRef]
- Asimakopoulos AD, Miano R, Di Lorenzo N, Spera E, Vespasiani G, Mugnier C. Laparoscopic versus robot-assisted bilateral nerve-sparing radical prostatectomy: comparison of pentafecta rates for a single surgeon. Surg Endosc. 2013 Nov;27(11):4297–304. [CrossRef]
- Ou Y-C, Yang C-K, Kang H-M, Chang K-S, Wang J, Hung S-W, et al. Pentafecta Outcomes of 230 Cases of Robotic-assisted Radical Prostatectomy with Bilateral Neurovascular Bundle Preservation. Anticancer Res. 2015 Sep;35(9):5007–13.
- Jazayeri SB, Weissman B, Samadi DB. Outcomes following robotic-assisted laparoscopic prostatectomy: Pentafecta and Trifecta achievements. Minerva Urol Nefrol. 2018 Feb;70(1):66–73. [CrossRef]
Figure 1.
Kaplan Meier Survival curves for biochemical recurrence rate stratified by nerve sparing approach.
Figure 1.
Kaplan Meier Survival curves for biochemical recurrence rate stratified by nerve sparing approach.
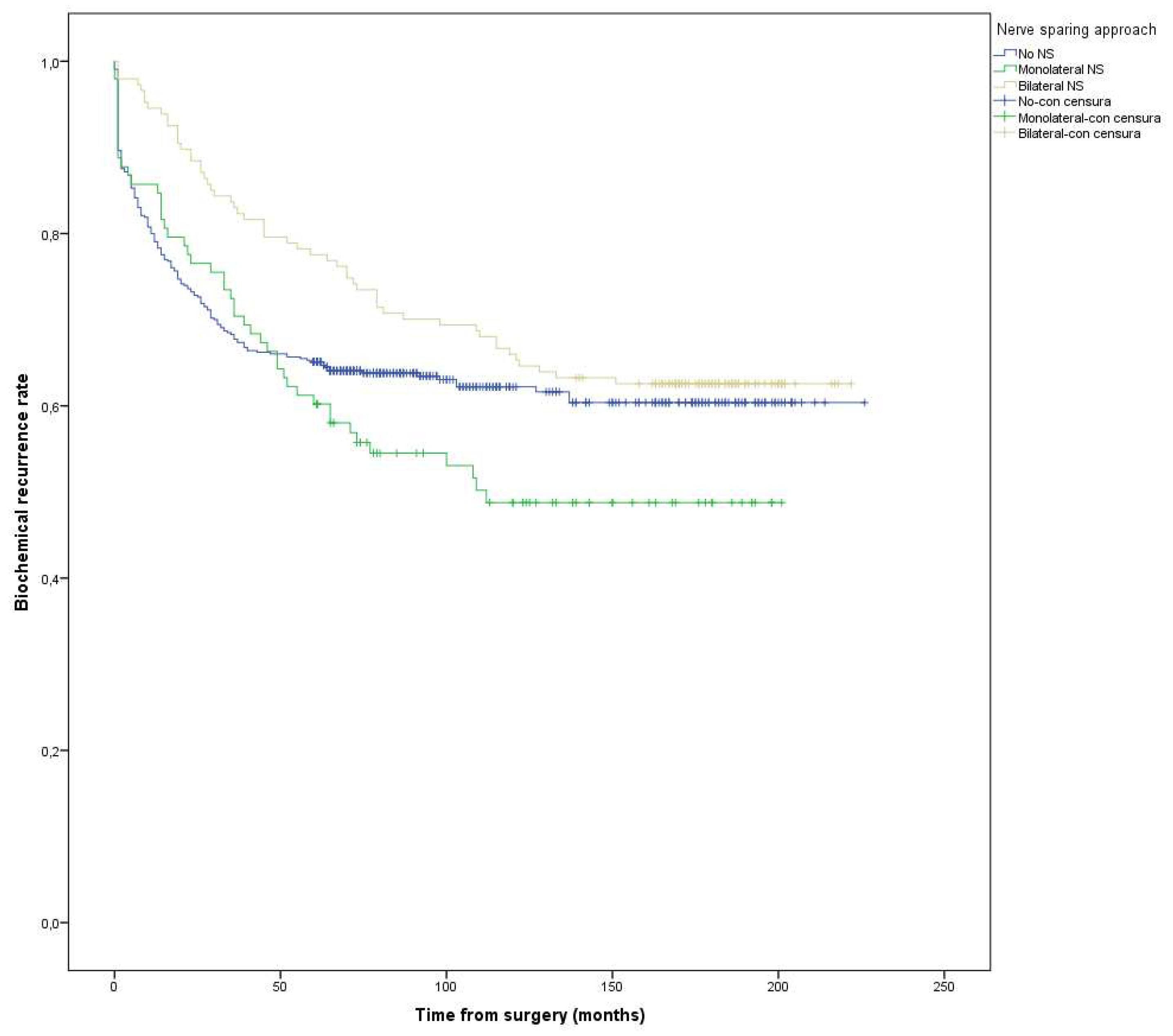
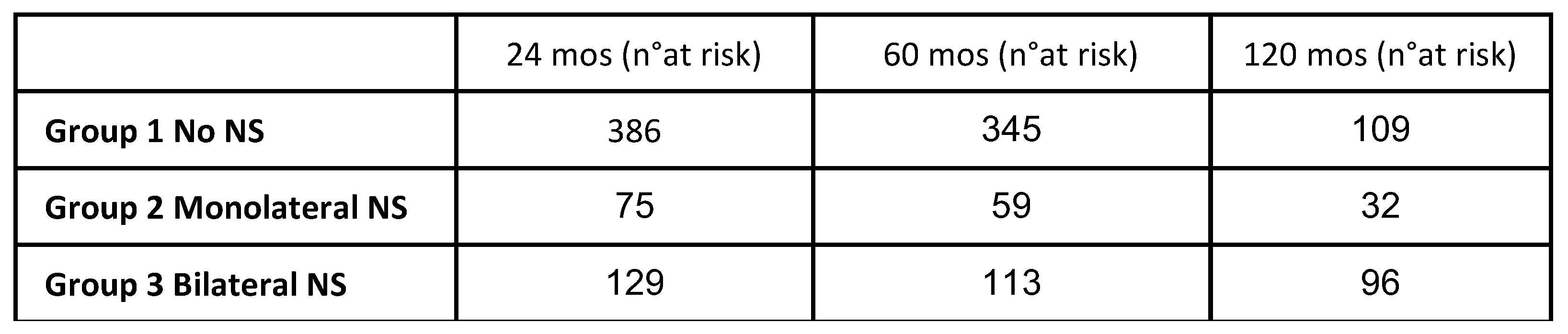

Table 1.
Demographic and clinical characteristics.
| Variable | Overall |
| Age (yrs) Mean (± SD) Median (IQR) |
63 (±6.4) 64 (59-68) |
| PSA (ng/mL) Mean (± SD) Median (IQR) |
14 (± 14) 8.90 (5-19) |
| Nerve Sparing. n (%) Yes No |
429 (54.8%) 350 (45.2%) |
Table 2.
Postoperative pathologic characteristics.
| Variable Pathologic stage, n (%) pT2 pT3a pT3b pT4 Lymph node status, n (%) pNx pN0 pN1 |
Overall | Group 1 (N=350) No NS |
Group 2 (N= 429) NS |
P Value |
|
pT2: 230 (29.56%) pT3a: 393 (50.51%) pT3b: 145 (19.02%) pT4: 7 (0.9%) |
pT2: 101 (28.85%) pT3a: 149 (42.57%) pT3b: 96 (27.42%) pT4: 4 (1.14%) |
pT2: 129 (30.14%) pT3a: 244 (57%)pT3b: 49 (12.15%) pT4: 3 (0.7%) |
0.08 | |
|
pNx: 360 (46.43%) pN0: 349 (44.91%) pN1: 66 (8.65%) |
pNx: 149 (42.69%) pN0: 164 (47%)pN1: 36 (10.31%) |
pNx: 211 (49.42%) pN0: 185 (43.24%) pN1: 30 (7.32%) |
0.09 | |
| Pathologic Gleason Score, n (%) 3+3 3+4 4+3 4+4 >4+4 Positive surgical margins. n (%) |
3+3: 81 (10.51%) 3+4: 218 (27.66%) 4+3:203 (26.36%) 4+4: 137 (17.79%) >4+4: 136 (17.66%) |
3+3: 23 (6.68%)3+4: 75 (21.80%) 4+3:88 (25.58%)4+4: 65 (18.89%) 4+4: 93 (27.03%) |
3+3: 58 (13.61%)3+4: 143 (32.39%) 4+3:115(26.99%) 4+4: 72(16.90%) 4+4: 43(10.09%) |
0.02 |
|
254 (32%) |
111 (31%) |
143 (33%) |
0.5 |
|
| Negative surgical margins, n (%) Monofocal PSM Multifocal PSM Positive surgical margins length, n (%) <= 3 mm >3 mm Localization of the PSM, n (%) Base Posterolateral Anterior Apex Follow up (months) Mean (± SD) Median (IQR) |
524 162 93 |
239 65 46 |
282 96 47 |
0.3 |
|
130 123 |
53 57 |
77 66 |
0.5 |
|
|
63 100 54 91 |
28 (8%) 35 (10%) 27 (8%) 41 (12%) |
30 (7%) 65 (15%) 27 (6%) 50 (12%) |
0.5 |
|
|
192 (±14) 132 (80-180) |
219 (±448) 133 (85-181) |
170 (±296) 125 (78-180) |
0.7 | |
| Biochemical recurrence rate, n (%) Adjuvant therapy. n (%) |
No: 447 (58.33%) Yes: 328 (41.67%) |
No: 178 (54.57%) Yes: 172(45.43%) |
No:273(61.39%)Yes: 156(38.61%) | 0.09 |
| Yes: 135(17.67%) No: 640(82.33%) |
Yes: 90 (25.14%) No: 260(74.86%) |
Yes: 49(15.10%)No:380(84.90%) | 0.07 |
Table 3.
Univariable and multivariable analysis for predictors of Biochemical recurrence and cancer specific survival.
Table 3.
Univariable and multivariable analysis for predictors of Biochemical recurrence and cancer specific survival.
| Univariable analysis for predictors of Biochemical recurrence rate | ||||||||
|---|---|---|---|---|---|---|---|---|
| Variabile | OR | Lower CI | Upper CI | P Value | ||||
| Age > 70 yrs | 1 | 0.7 | 1.5 | 0.7 | ||||
|
Preoperative PSA value <= 10 ng/mL vs > 10 ng/mL |
1.6 |
1.2 |
2.0 |
<0.001 | ||||
| Positive surgical margin (PSM) | 1.5 | 1.2 | 1.9 | <0.001 | ||||
|
Surgical margin status Negative Positive Monofocal Positive Multifocal |
Reference 1.3 1.6 |
1.1 1.2 |
1.9 2.1 |
<0.001 0.005 <0.001 |
||||
|
PSM Length < 3mm vs >= 3mm |
1.4 |
1.1 |
1.9 |
0.007 | ||||
|
Pathologic Gleason Score 3+3 ≤ 3+4 vs 3+3 4+3 vs 3+3 4+4 vs ≤ 3+3 ≥ 4+5 vs ≤ 3+3 |
Reference 1.6 2.3 2.6 3.8 |
1 1.3 1.5 2.3 |
2.8 3.8 4.5 6.4 |
<0.001 0.05 0.01 0.001 0.001 |
||||
|
Pathologic stage Organ confined vs Locally advanced |
2.0 |
1.5 |
2.7 |
<0.001 |
||||
|
Lymph node status Nx N0 vs Nx N1 vs Nx |
Reference 0.9 4.3 |
0.7 3.0 |
1.1 6.0 |
<0.001 0.5 <0.001 |
||||
|
Nerve sparing (NS) approach No NS Monolateral NS vs NO-NS Bilateral NS vs NO-NS |
Reference 1.2 0.7 |
0.9 0.5 |
1.7 1.0 |
0.6 0.1 0.1 |
||||
| Multivariable analysis for predictors of Biochemical recurrence rate | ||||||||
| Variabile | OR | Lower CI | Upper CI | P Value | ||||
| Age >70 yrs | 1.0 | 0.9 | 1.5 | 0.6 | ||||
|
Preoperative PSA value <= 10 ng/mL vs > 10 ng/mL |
1.4 |
1.5 |
2.8 |
<0.001 | ||||
| Positive surgical margin (PSM) | 1.5 | 1.3 | 1.8 | 0.005 | ||||
|
Surgical margin status Negative Positive Monofocal Positive Multifocal |
Reference 1.4 2.3 |
0.9 1.5 |
2.4 3.6 |
<0.001 0.1 <0.001 |
||||
|
PSM Length < 3mm vs >= 3mm |
1.5 |
0.8 |
2.8 |
0.1 |
||||
|
Pathologic Gleason Score 3+3 ≤ 3+4 vs 3+3 4+3 vs 3+3 4+4 vs ≤ 3+3 ≥ 4+5 vs ≤ 3+3 |
Reference 1.6 2.1 2.5 3.4 |
0.9 1.2 1.4 1.9 |
2 3.5 4.4 6 |
<0.001 0.07 <0.001 <0.001 <0.001 |
||||
|
Pathologic stage Organ confined vs Locally advanced |
2.1 |
1.5 |
2.1 |
<0.001 |
||||
|
Lymph node status Nx N0 vs Nx N1 vs Nx |
Reference 0.7 2.5 |
0.7 1.6 |
1 3.8 |
<0.001 0.1 <0.001 |
||||
|
Nerve sparing (NS) approach No NS Monolateral NS vs NO-NS Bilateral NS vs NO-NS |
Reference 0.7 1.3 |
0.5 1.0 |
1.5 1.8 |
0.06 0.7 0.03 |
||||
| Univariable analysis for predictors of Cancer specific survival | ||||||||
| Variabile | HR | 95% CI | Upper CI | P Value | ||||
| Age > 70 anni | 0.3 | 0.04 | 2.8 | 0.3 | ||||
|
Preoperative PSA value <= 10 ng/mL vs > 10 ng/mL |
0.5 |
0.2 |
1.6 |
0.3 |
||||
| Positive surgical margin (PSM) | 1.1 | 0.4 | 3.1 | 0.7 | ||||
|
Surgical margin status Negative Positive Monofocal Positive Multifocal |
Reference 1.4 0.8 |
0.4 0.2 |
4.5 3.2 |
0.7 0.5 0.8 |
||||
|
PSM Length < 3mm vs >= 3mm |
0.7 |
0.2 |
2.3 |
0.6 |
||||
|
Pathologic Gleason Score 3+3 ≤ 3+4 vs 3+3 4+3 vs 3+3 4+4 vs ≤ 3+3 ≥ 4+5 vs ≤ 3+3 |
Reference 0.8 0.7 1.4 16.2 |
0.1 0.1 0.1 1.7 |
5.0 11 4.0 150 |
0.03 0.8 0.7 0.7 0.01 |
||||
|
Pathologic stage Organ confined vs Locally advanced |
3.3 |
0.4 |
26 |
0.2 | ||||
|
Lymph node status Nx N0 vs Nx N1 vs Nx |
Reference 1.4 1.5 |
0.5 1.5 |
4.1 5.9 |
0.04 0.6 <0.001 |
||||
|
Nerve sparing (NS) approach No NS Monolateral NS vs NO-NS Bilateral NS vs NO-NS |
Reference 0.9 1.0 |
0.9 0.9 |
1.5 1.8 |
0.09 0.09 0.09 |
||||
| Multivariable analysis for predictors of Cancer specific survival | ||||||||
| Variabile | HR | Lower CI | Upper CI | P Value | ||||
| Age > 70 anni | 0.6 | 0.2 | 20 | 0.8 | ||||
|
Preoperative PSA value <= 10 ng/mL vs > 10 ng/mL |
0.1 |
0.01 |
1.6 |
0.1 |
||||
| Positive surgical margin (PSM) | 0.4 | 0.3 | 11 | 0.8 | ||||
|
Surgical margin status Negative Positive Monofocal Positive Multifocal |
Reference 0.9 1.0 |
0.7 0.04 |
1.8 90 |
0.9 0.8 0.9 |
||||
|
PSM Length < 3mm vs >= 3mm |
0.9 |
0.05 |
16 |
0.9 |
||||
|
Pathologic Gleason Score 3+3 ≤ 3+4 vs 3+3 4+3 vs 3+3 4+4 vs ≤ 3+3 ≥ 4+5 vs ≤ 3+3 |
Reference 0.6 16 0.7 0.2 |
0.04 0.6 0.03 0.01 |
11 456 20 4 |
0.2 0.8 0.09 0.9 0.3 |
||||
|
Pathologic stage Organ confined vs Locally advanced |
11 |
0.5 |
243 |
0.1 | ||||
|
Lymph node status Nx N0 vs Nx N1 vs Nx |
Reference 1.2 41 |
0.8 1.6 |
1.5 1000 |
0.001 0.06 <0.001 |
||||
|
Nerve sparing (NS) approach No NS Monolateral NS vs NO-NS Bilateral NS vs NO-NS |
Reference 0.9 1.0 |
0.9 0.9 |
1.5 1.8 |
0.09 0.09 0.09 |
||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



