
Submitted:
30 January 2024
Posted:
31 January 2024
You are already at the latest version
Abstract
Congenital malformations are functional and structural alterations in embryonic or foetal development resulting from a variety of factors including maternal health status. This study aimed to investigate the association between maternal birth weight (MBW) and the prevalence of congenital malformations in the offspring using data from a nationwide birth cohort study in Japan including 103,060 pregnancies. A binary logistic regression model with adjustment for various covariates revealed that MBW of <2,500 g (low MBW) was associated with increased risk of congenital heart disease (adjusted odds ratio: 1.388, [95% confidence interval: 1.075–1.792]), angioma (1.491 [1.079–2.059]), and inguinal hernia (1.746, [1.189–2.565]), while MBW of ≥4,000 g (high MBW) with congenital anomalies of the urinary tract (2.194, [1.261–3.819]), and arrhythmia (1.775, [1.157–2.725]), compared with those with MBW of 3,000-3,499 g. Low MBW was associated with cleft lip and/or palate (1.473, [1.052–2.064]), congenital heart disease (1.615, [1.119–2.332]), genital organs(1.648, [1.130–2.405]), hypospadias (1.804, [1.130–2.881]), and inguinal hernia (1.484, [1.189–1.851]) in male infants and CAKUT (1.619, [1.154–2.273]) in female infants, whereas high MBW was associated with congenital heart disease(1.745, [1.058–2.877]) and CAKUT (2.470, [1.350–4.517]) in male infants. The present study is the first to demonstrate a link between MBW and congenital malformations in Japanese children. While these results must be interpreted with caution, MBW should be considered a major predictor of congenital malformation risk.
Keywords:
Birth cohort
; Congenital malformations
; Maternal birth weight
1. Introduction
Congenital anomalies (CAs) include functional and structural alterations in embryonic or foetal development resulting from genetic, environmental, or unknown causes that originate during pregnancy, are present at birth, and cause physical or mental impairment (1). While complex genetic and environmental interactions are proposed, most CAs are of unknown aetiology. To date, approximately 50% CAs have been linked to specific causes including genetic, socioeconomic, demographic, environmental, infectious, and maternal nutritional risk factors [1]. One of the consequences of these defects is the high death rate within the first year of life and can contribute to long-term chronic illness and disabilities.
Epidemiological studies have linked maternal health status, such as obesity, diabetes, and nutrition which influence the intrauterine environment, to increased risk of CAs. Mother’s own birth weight has been reported to be associated with risk of certain noncommunicable diseases (NCD) in her later life, such as cardiovascular disease (CVD), diabetes mellitus (DM), and hypertensive disorders [2,3]. Recent studies have also reported that maternal birth weight (MBW) is associated with major pregnancy complications, including hypertensive disorders of pregnancy (HDP), delivery of small-for-gestational-age infants, and gestational diabetes mellitus (GDM) [4,5,6,7,8,9].
The Japan Environment and Children’s Study (JECS) is a nationwide prospective birth cohort study funded by the Ministry of the Environment of Japan. The JECS aims to investigate the long-term effects of exposure to chemical substances in the environment on the growth, development, incidence of disease, and change in health conditions of children, and the present study aimed to assess the association between MBW and the risk of common congenital anomalies and malformations after adjusting for potential confounding risk factors in a large nationwide birth cohort study.
2. Materials and Methods
2.1. Study Design
This prospective study used data from the JECS, a nationwide birth cohort study being conducted in Japan. The main objective of the JECS is to investigate the environmental factors associated with offspring health and development. A total of 103,060 pregnancies (and their paired partner and infant, if accessible) were recruited from 15 Regional Centres in Japan between January 2011 and March 2014. The JECS protocol was reviewed and approved by the Ministry of Environment's Institutional Review Board on Epidemiological Studies and the Ethics Committees of all participating institutions and written informed consent was obtained from all the participants in the JECS. Details of the study design and baseline characteristics of the JECS participants have been described previously [10,11]. Maternal information was obtained from two self-administered questionnaires, MT1 and MT2, which were collected during the first, and the second or third trimester, respectively. Information on drug use during pregnancy was obtained from two interviews, ‘In-T1’ and ‘In-T2’ [12]. The study participants also answered two more questionnaires, C6m and C2y, six months and two years after delivery, respectively. The present study was based on the data set “jecs-ta-20190930” which was released in October 2019 by the Programme Office.
2.2. Maternal Birth Weight (MBW)
2.3. Infant Congenital Malformations Selection
The primary outcome of interest in this study was congenital malformations in the infants. After physicians, midwives/nurses, and/or Research Co-ordinators transcribed information on infant congenital malformations, the datasets on infant congenital malformations at birth ( Dr0m) and one month after birth ( Dr1m) were provided. The details of infant congenital malformations in the JECS have been described previously [16]. Additionally, if the caregivers answered that their infant was diagnosed as having congenital malformations at the C2y questionnaire, information on infant congenital malformations was also transcribed by physicians from medical records (namely, “Disease Data Registry”). Information on “Disease Data Registry”, including infant congenital malformations, was provided in the dataset “jecs-qa-20210401”. If infant congenital malformations were diagnosed in either the Dr0m, the Dr1m, or the “Disease Data Registry”, the malformations were defined as positive in this study, except for umbilical hernia. Umbilical hernia was defined as positive if it was diagnosed in either the Dr0m, or the “Disease Data Registry” in this study. In a previous study, congenital anomalies of the kidney and urinary tract (CAKUT) were defined as hydronephrosis, cystic renal malformations, renal agenesis, and bladder exstrophy/cloacal exstrophy [17].
Considering the sample size, we selected several eligible infant congenital malformations as outcomes to be analysed as follows: “nervous system”, “eye, ear, and face”, “cleft lip and/or cleft palate”, “congenital heart disease”, “arrhythmia”, “urinary system (CAKUT)”, “genital organs in male infants”, “limbs” of musculoskeletal system, “angioma” of skin, and “inguinal hernia”. Among “genital organs in male infants”, hypospadias and cryptorchidism/nonpalpable testis were also selected as separate outcomes.
2.4. Data Collection and Classification of Other Variables
The maternal age in the MT1 questionnaire was provided in the dataset. Maternal height and prepregnancy body weight (BW) were transcribed from medical records. If either maternal height or pre-pregnancy BW was missing, self-reported values were obtained. The pre-pregnancy body mass index (BMI) was calculated as follows: pre-pregnancy BW in kilograms divided by the height in centimetres squared. Physicians, midwives, nurses, and/or Research Co-ordinators transcribed information on parity, conception method, HDP, GDM, delivery week, infant birth weight and sex, from the medical records. Two parity groups were formed: primiparous and multiparous. Conception methods were classified as spontaneous pregnancy, non-assisted reproductive technology (ART), and ART. Non-ART was defined as ovulatory induction, and artificial insemination by the husband was defined as in vitro fertilisation and embryo transfer (IVF-ET), and intracytoplasmic sperm injection (ICSI). Medical history of maternal diseases (hypertension, type 1 diabetes, type 2 diabetes, kidney disorders, mental diseases, congenital heart diseases, uterine malformations, malformations of the urinary tract, or genital organs) was collected from the MT1 questionnaire. Medical history of kidney disease was defined as immunoglobulin A nephropathy, glomerular nephritis, and/or nephrotic syndrome. Medical history of mental diseases was also obtained, being defined as depression, anxiety disorder, schizophrenia, or dysautonomia. Data on smoking history, alcohol consumption, and marital status were obtained using the MT1 questionnaire. Choices of smoking history of the MT1 questionnaire were “Never”, “Previously did, but quit before realizing current pregnancy”, “Previously did, but quit after realizing current pregnancy”, and “Currently smoking”. In this study, the smoking status was reclassified according to the presence or absence of current smoking. Choices of alcohol consumption in the MT1 questionnaire were “Never”, “Quit drinking”, and “Continue drinking”. Alcohol consumption was classified according to the presence or absence of continued alcohol consumption. Marital status was classified as unmarried, divorced, widowed, unmarried, divorced, or widowed. Glycosylated haemoglobin (HbA1c) levels, defined by the National Glycohemoglobin Standardization Program (NGSP), were assayed at <24 weeks of gestation, using high-performance liquid chromatography (ADAMS-A1c HA-8160, Arkray, Inc., Kyoto, Japan) [18]. Information regarding use of any drug (methimazole, selective serotonin reuptake inhibitor [SSRI], antidepressant drug except for SSRI, antianxiety, sleeping pill, antipsychotic, valproic acid, antiepileptic except for valproic acid, lithium carbonate, and other psychoactive drugs) at <12 weeks of gestation and use of folic acid supplement at <12 weeks of gestation were obtained from the In-T1 and In-T2 interviews. Both the maternal highest level of education and annual household income were obtained from the MT2 questionnaire. Maternal highest level of education was categorized as follows: <13 years (junior high school or high school) and ≥13 years(high school or technical junior college or technical/vocational college or associate degree or bachelor's degree or Graduate degree [Master's/Doctorate]). Annual household income was categorized into <4.4-5.99 and ≥6 million Japanese Yen. Information on chromosomal abnormalities or other syndromes of infants was obtained from Dr0m, Dr1m, and C2y.
2.5. Statistical Analysis
Continuous and categorical variables of characteristics of study participants, including infant congenital malformations, were expressed as mean (standard deviation [SD]) and number (percentage), respectively.
The association between MBW and the prevalence of infant congenital malformations was investigated using a binary logistic regression model, and the odds ratios (OR) were calculated. If a complete or quasi-complete separation existed, the Firth method was applied to the binary logistic regression model [19]. Participants with a MBW of 3,000–3,499 g were assigned to the reference category. Model 1 was defined as the crude model. Model 2 was adjusted for covariates as follows: maternal age in the MT1 questionnaire, pre-pregnancy BMI, conception method, parity (primipara or not), history of mental illness, history of maternal congenital heart disease, history of maternal uterine malformation and/or urogenital malformation, history of kidney diseases, smoking status, alcohol consumption, marital status, education level, annual income, use of any drug at <12 weeks of gestation (methimazole, SSRI, antidepressant drug except for SSRI, antianxiety, sleeping pill, antipsychotic, valproic acid, antiepileptic except for valproic acid, lithium carbonate, and other psychoactive drug), use of folic acid supplement at <12 weeks of gestation, HbA1c level at <24 weeks of gestation, and infant sex. No strong multicollinearity among covariates was confirmed using the variance inflation factor of a general linear model with infant congenital malformations as the dependent variable. As several covariates had missing data, multiple imputations using a Markov chain Monte Carlo simulation were applied. After generation of ten datasets and their analysis, the adjusted ORs of the combined ten results are reported in the manuscript.
Stratified analysis according to infant sex was also performed to investigate differences in the association of MBW with congenital malformations between male and female infants. In the stratified analysis, infant sex was not included in Model 2.
Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, North Carolina, USA) and R (version 4. 1. 2) [20].
3. Results
3.1. Characteristics of Study Participants
A flowchart of the study is shown in Figure 1. Of the 103,060 pregnancies who participated in the JECS, 5,653 pregnancies with multiple participation were excluded. Participants with multiple pregnancies (N=8,023), abortion or stillbirth (N=1,432), consent withdrawal or censoring (N=6,489), non-Japanese nationals (n=400), missing data on the nationality of participants (N=5,814), missing data on MBW (N=3,579), and improbable data on MBW (i.e. <500 g or >6,000 g) (N=28) were excluded. Furthermore, all questionnaires for Dr0m, Dr1m, and C2y were missing (N=24); chromosomal abnormalities or other infant syndromes (N=199), skeletal dysplasia of infants (N=128), and improbable data because of mismatch of infant sex and genital anomalies (N=6) were also excluded. Finally, 78,366 mothers and their infants were eligible for analysis in this study. The numbers and percentages of mothers according to the category of MBW were as follows: <2,500 g (N=3,850; 4.9%), 2,500–2,999 g (N=23,161; 29.5 %), 3,000–3,499 g (N=38,146; 48.7 %), 3,500–3,999 g (N=11,435; 14.6 %), and ≥4,000 g (N=1,774; 2.3 %), respectively.
The maternal and neonatal characteristics of the study participants are shown in Table 1. The mean (SD) maternal age at MT1 and pre-pregnancy BMI were 30.9 (5.0) years and 21.2 (3.2) kg/m2, respectively. The percentages of preterm deliveries and low birth weight (LBW) infants were 4.4 and 7.9%, respectively. The proportions of underweight, new-onset HDP, GDM, preterm delivery, maternal highest level of education <13 years, unmarried, divorced, or widowed, annual household income of <4 million Japanese Yen, small for gestational age (SGA) infants, and LBW in those with MBW <2,500 g were higher than those with other categories of MBW. The proportions of participants with obese, large for gestational age (LGA) infants, and macrosomia in participants with MBW of ≥4,000 g was higher than those with other categories of MBW.
3.2. Prevalence of Infant Congenital Malformations
The prevalence of infant congenital malformations among all participants were as follows: cleft lip and/or cleft palate (0.21%), congenital heart disease (1.36 %), CAKUT (0.35 %), genital organs in male infants (1.12%), limbs (0.28 %), angioma (0.77 %), and inguinal Hernia (0.49 %). As shown in Table 2, relatively higher prevalence of infant congenital malformations were observed in infants born from mothers with MBW <2,500 g than those with other MBW categories: cleft lip and/or cleft palate (0.31 %), genital organs in male infants (1.63 %), angioma (1.12 %), and inguinal hernia (0.81 %). By contrast, each prevalence of arrhythmia (0.28 %) and CAKUT (0.79 %) in infants born from participants with MBW of ≥4,000 g was higher than those with other MBW categories. The prevalence of infant congenital heart diseases born from mothers with MBW of <2,500 g (1.79 %) and ≥4,000 g (1.75 %) was higher than those with other MBW categories.
3.3. Association between MBW and Prevalence of Infant Congenital Malformations
As shown in Table 3, MBW was significantly associated with the prevalence of several infant congenital malformations, including congenital heart disease, arrhythmia, CAKUT, angioma, and inguinal hernia. Compared with participants with MBW of 3,000–3,499 g, those with MBW of <2,500 g had significantly higher odds of congenital heart disease, genital organs in male infants, angioma, and inguinal hernia, In model 2, the adjusted ORs were 1.388 (95% confidence interval [CI]: 1.075–1.792) for congenital heart disease, 1.648 (95% CI: 1.130–2.405) for genital organs in male infants, 1.804 (95% CI: 1.130–2.881) for hypospadias in male infants, 1.491 (95% CI: 1.079–2.059) for angioma, and 1.746 (95% CI: 1.189–2.565) for inguinal hernia, respectively. Participants with MBW of ≥4,000 g had significantly higher odds of arrhythmia and CAKUT, compared with those with MBW of 3,000––3,499 g. In model 2, the adjusted ORs were 1.775 (95% CI: 1.157–2.725) for arrhythmia and 2.194 (95% CI: 1.261–3.819) for CAKUT, respectively.
3.4. Association between MBW and Prevalence of Infant Congenital Malformations Stratified by Infant Sex
Congenital malformations are known to have biased sex distributions. In order to investigate this, we further performed a stratified analysis by infant sex, shown in Table 4. Participants with MBW of <2,500 g was associated with increasing odds of cleft lip and/or cleft palate in male infants. The adjusted OR was 1.473 (95% CI: 1.052–2.064) in model 2. In female infants, the association of MBW with cleft lip and/or cleft palate was not statistically significant. The U-shaped association of MBW with congenital heart disease in male infants existed. In model 2, the adjusted ORs in MBW of <2,500 g and ≥4,000 g were 1.615 (95% CI: 1.119–2.332) and 1.745 (95% CI: 1.058–2.877), respectively. By contrast, the association of MBW with congenital heart disease in female infants was not statistically significant. In both male and female infants, participants with MBW of ≥4,000 g were associated with increasing odds of arrhythmia, although the adjusted OR did not reach statistical significance in male infants. In model 2, the adjusted ORs were 1.840 (95% CI: 0.999–3.387) in male infants and 1.788 (95% CI: 1.047–3.052) in female infants, respectively. Participants with MBW of ≥4,000 g were associated with increasing odds of CAKUT in male infants (the adjusted OR was 2.470 [95% CI: 1.350–4.517] in model 2), whereas those with MBW of <2,500 g were associated with increasing odds of CAKUT in female infants (The adjusted OR was 1.619 [95% CI: 1.154–2.273] in model 2). In the analysis for association of MBW with inguinal hernia, participants with MBW of <2,500 g had significantly higher odds of inguinal hernia in male infants, compared to those with MBW of 3,000–3,499 g (the adjusted OR was 1.484 [95% CI: 1.189–1.851] in model 2). However, the association between MBW and inguinal hernia in female infants was not statistically significant.
4. Discussion
Numerous studies have identified parental, genetic, epigenetic, and environmental risk factors for congenital anomalies in neonates and infants [1]. Meanwhile, MBW has been reported to be associated with various perinatal complications, such as GDM [5] and PTD [21]. To the best of our knowledge, this study is the first to demonstrate an association between MBW and the prevalence of congenital malformations in offspring of Japanese population. Low MBW was associated with congenital heart disease, angioma, and inguinal hernia, while high MBW was associated with congenital anomalies of the kidney, urinary tract, and arrhythmia. Low MBW was associated with cleft lip and/or palate, congenital heart disease, genital organs, hypospadias, and inguinal hernia in male infants and CAKUT in female infants, whereas high MBW was associated with congenital heart disease and CAKUT in male infants.
Low MBW and high birth weight were associated with congenital heart defects (CHD) in male infants. Generally, congenital malformations have a sex-biased distribution. Consistent with our findings, male infants were found to have higher prevalence of CHD than female infants [22]. CHDs are among the most common and serious birth defects. Though several established causes of CHDs have been identified, including maternal exposure, maternal phenotypes, chromosomal abnormalities, and single-gene disorders; the causative genetic mechanisms behind CHD remain poorly understood and more than half of CHD patients lack a genetic diagnosis [23]. Low and high MBW have been reported as risk factors for an abnormal metabolic status, including obesity, gestational diabetes, and diabetes mellitus. Hyperglycaemia and micronutrient deficiency in mothers are known to relate to CHD in their offspring [24,25]. Hyperglycaemia has been well studied in both human and animal models. Hyperglycaemia during embryogenesis induces hypoxia, leading to reduced PAX3 expression, which can cause CDH [26,27]. Together with these observations, oxidative stress or epigenetic changes induced by inappropriate nutrition during pregnancy, the preconception period, or even much before pregnancy, which are related to low and high MBW, might be one of the presumed mechanisms by which MBW can cause CDH.
In the current study, the association between low MBW in both sexes and high MBW in male infants, was found to be quite distinct. CAKUT constitutes 20–30% of all congenital malformations, and its prevalence has been estimated to range between three and six per 1,000 births, most commonly in males. Several genes such as PAX2 and HNF1B have been identified to be related to CAKUT, and epigenetic changes in these genes are responsible for the pathogenesis of the disease [28]. Maternal factors were associated with the CAKUT scores. Maternal obesity, gestational diabetes, and diabetes mellitus are known to be risk factors of CAKUT in the offspring [29,30,31,32,33]. MBW are reported to be risk factors of obesity, gestational diabetes, and diabetes mellitus. Maternal hyperglycaemia leads to increased oxidative stress via the production of reactive oxygen species (ROS), partly by mitochondria. The produced ROS cause membrane damage, which in turn activates programmed cell death via proapoptotic proteins. The upregulation of pro-apoptotic proteins leads to endoplasmic reticulum stress and cell death. Abnormal apoptosis causes malformations in the major organs of during development of foetus [34]. Together with these observations, oxidative stress or epigenetic changes induced by inappropriate nutrition during pregnancy, the preconception period, or even before pregnancy, which are related to maternal LBW and HBW, might be one of the presumed mechanisms by which MBW causes CAKUT.
Preterm infants are at risk of inguinal hernia and angioma [35,36]. Both Inguinal hernias and angiomas occur in up to 4 percent of children and are among the most common indications for paediatric surgery [36,37]. Low MBW, sometimes caused by a preterm birth, is also associated with inguinal hernias in male offspring and angiomas in all infants. Interestingly, the renin-angiotensin system (RAS) may play a role in endothelial cell proliferation in haemangiomas. Pregnant women born with LBWs have an increased risk of hypertensive disorders during pregnancy, which contributes to the risk of developing chronic hypertension in infants, in which the RAS is highly involved [38]. In line with these insights, maternal LBW may increase the risk of inguinal hernia or angioma in offspring via impaired RAS.
In summary, there is indirect evidence supporting the association between MBW and congenital anomalies in offspring; however, further analysis is required to unravel the molecular mechanism.
This study has several strengths. First, the study participants were recruited from a wide geographical area of Japan. Therefore, the external validity of the results of this study was high. Second, this study considered many variables, including maternal physiological and socioeconomic factors, in its statistical analysis. However, this study also has several limitations. Information on MBW was obtained from a self-reported questionnaire; therefore, it may have been misclassified. Notably, birth weights collected from medical records and self-reports were comparable [39]. Hence, we believe that this limitation did not strongly affect our findings. Second, this was a single-ethnicity study. The genetic background is homogeneous, which enables a reduction in genetic variation; however, it may not be adaptable to other ethnicities. Further studies involving different ethnicities are required to confirm our findings.
5. Conclusions
MBW should be considered as one of the major parameters to be collected at the first visit to obstetrics clinics along with past medical history, familial history, and maternal parameters especially birth weight for recognising the risk of congenital malformations in the offspring. However, the results of the current study must be interpreted with caution, as MBW and infants’ congenital malformations remain an association, but not a direct cause. Future studies are required to unravel the mechanism of the relationship between MBW and the risk of congenital malformations of the offspring; so that ap-propriate intervention can be provided to patients to reduce the risk of giving birth to offspring with congenital malformations.
Author Contributions
Hirotaka Hamada: HH, Noriyuki Iwama: NI, Hasumi Tomita: HT, Kazuma Tagami: KT, Natsumi Kumagai: NK, Rie Kudo: RK, Hongxin Wang: HW, Seiya Izumi: SI, Zen Watanabe: ZW, Mami Ishikuro: MI, Taku Obara: TO, Nozomi Tatsuta: NT, Hirohito Metoki: HM, Chiharu Ota: CO, Masatoshi Saito: MS, Shinichi Kuriyama: SK, Takahiro Arima: TA, Nobuo Yaegashi: NY. HH: Conceptualization, Methodology, Writing-Original draft.. NI: Conceptualization, Methodology, Formal analysis, and Co-writing Original draft. HT: Conceptualization, Writing - Review & Editing. KT: Writing - Review & Editing. NK: Writing - Review & Editing. RK: Writing - Review & Editing. HW: Writing - Review & Editing. SI: Writing - Review & Editing. ZW: Writing - Review & Editing. MI: Writing - Review & Editing, Investigation. TO: Writing - Review & Editing, Investigation. NT: Writing - Review & Editing, Investigation. HM: Writing - Review & Editing, Investigation. CO: Writing - Review & Editing, Investigation, Project administration. MS: Writing - Review & Editing. SK: Writing - Review & Editing, Investigation. TA: Writing - Review & Editing, Investigation, Project administration. NY: Writing - Review & Editing, Investigation, Supervision, Project administration.
Funding
This study was funded by the Ministry of the Environment, Japan. The findings and conclusions of this article are solely the responsibility of the authors and do not represent the official views of the government.
Institutional Review Board Statement
The JECS protocol was reviewed and approved by the Ministry of Environment's Institutional Review Board on Epidemiological Studies and the Ethics Committees of all participating institutions.
Informed Consent Statement
Written informed consent was obtained from all the participants in the JECS.
Data Availability Statement
Data are unsuitable for public deposition because of ethical restrictions and the legal framework of Japan. It is prohibited by the Act on the Protection of Personal Information (Act No. 57 of 30 May 2003 amended on 9 September 2015) to publicly deposit data containing personal information. Ethical guidelines for medical and health research involving human participanta enforced by the Japan Ministry of Education, Culture, Sports, Science and Technology and the Ministry of Health, Labour and Welfare also restrict the open sharing of epidemiological data. All enquiries about access to data should be sent to jecs-en@nies.go.jp. The person responsible for handling enquiries sent to this e-mail address is Dr. Shoji F. Nakayama, JECS Programme Office, National Institute for Environmental Studies. [Regarding data for the paper publication, http://www.env.go.jp/chemi/ceh/en/index.html (accessed 9 August 2021)].
Acknowledgments
We thank all participants and staff of the JECS. We also acknowledge Editage (https://www.editage.com/) for their help with English proofreading of the manuscript.
Conflicts of Interest
No authors have competing interests to declare.
Appendix A
Members of the JECS Group as of 2023: Michihiro Kamijima (principal investigator, Nagoya City University, Nagoya, Japan), Shin Yamazaki (National Institute for Environmental Studies, Tsukuba, Japan), Yukihiro Ohya (National Center for Child Health and Development, Tokyo, Japan), Reiko Kishi (Hokkaido University, Sapporo, Japan), Nobuo Yaegashi (Tohoku University, Sendai, Japan), Koichi Hashimoto (Fukushima Medical University, Fukushima, Japan), Chisato Mori (Chiba University, Chiba, Japan), Shuichi Ito (Yokohama City University, Yokohama, Japan), Zentaro Yamagata (University of Yamanashi, Chuo, Japan), Hidekuni Inadera (University of Toyama, Toyama, Japan), Takeo Nakayama (Kyoto University, Kyoto, Japan), Tomotaka Sobue (Osaka University, Suita, Japan), Masayuki Shima (Hyogo Medical University, Nishinomiya, Japan), Seiji Kageyama (Tottori University, Yonago, Japan), Narufumi Suganuma (Kochi University, Nankoku, Japan), Shoichi Ohga (Kyushu University, Fukuoka, Japan), and Takahiko Katoh (Kumamoto University, Kumamoto, Japan).
References
- Oliveira, C.; Fett-Conte, A. Birth Defects: Risk Factors and Consequences. J Pediatr Genet 2015, 02, 085–090. [Google Scholar] [CrossRef] [PubMed]
- Arima, Y.; Fukuoka, H. Developmental Origins of Health and Disease Theory in Cardiology. Journal of Cardiology 2020, 76, 14–17. [Google Scholar] [CrossRef]
- Hanson, M. The Birth and Future Health of DOHaD. J Dev Orig Health Dis 2015, 6, 434–437. [Google Scholar] [CrossRef] [PubMed]
- Egeland, G.M.; Skjærven, R.; Irgens, L.M. Birth Characteristics of Women Who Develop Gestational Diabetes: Population Based Study. BMJ 2000, 321, 546–547. [Google Scholar] [CrossRef] [PubMed]
- Innes, K.E. Association of a Woman’s Own Birth Weight With Subsequent Risk for Gestational Diabetes. JAMA 2002, 287, 2534. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, J.C.; Williams, M.A.; Luthy, D.A.; Emanuel, I.; Shy, K. Weight at Birth and Subsequent Risk of Preeclampsia as an Adult. Am J Obstet Gynecol 2003, 189, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Andraweera, P.H.; Dekker, G.; Leemaqz, S.; McCowan, L.; Myers, J.; Kenny, L.; Walker, J.; Poston, L.; Roberts, C.T. ; the SCOPE Consortium Effect of Birth Weight and Early Pregnancy BMI on Risk for Pregnancy Complications. Obesity 2019, 27, 237–244. [Google Scholar] [CrossRef]
- Bay, B.; Ingerslev, H.J.; Lemmen, J.G.; Degn, B.; Rasmussen, I.A.; Kesmodel, U.S. Preimplantation Genetic Diagnosis: A National Multicenter Obstetric and Neonatal Follow-up Study. Fertility and Sterility 2016, 106, 1363–1369. [Google Scholar] [CrossRef]
- Á Rogvi, R.; Forman, J.L.; Damm, P.; Greisen, G. Women Born Preterm or with Inappropriate Weight for Gestational Age Are at Risk of Subsequent Gestational Diabetes and Pre-Eclampsia. PLoS ONE 2012, 7, e34001. [Google Scholar] [CrossRef]
- Kawamoto, T.; Nitta, H.; Murata, K.; Toda, E.; Tsukamoto, N.; Hasegawa, M.; Yamagata, Z.; Kayama, F.; Kishi, R.; Ohya, Y.; et al. Rationale and Study Design of the Japan Environment and Children’s Study (JECS). BMC Public Health 2014, 14, 25. [Google Scholar] [CrossRef]
- Michikawa, T.; Nitta, H.; Nakayama, S.F.; Yamazaki, S.; Isobe, T.; Tamura, K.; Suda, E.; Ono, M.; Yonemoto, J.; Iwai-Shimada, M.; et al. Baseline Profile of Participants in the Japan Environment and Children’s Study (JECS). Journal of Epidemiology 2018, 28, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Nishigori, H.; Obara, T.; Nishigori, T.; Metoki, H.; Ishikuro, M.; Mizuno, S.; Sakurai, K.; Tatsuta, N.; Nishijima, I.; Fujiwara, I.; et al. Drug Use before and during Pregnancy in Japan: The Japan Environment and Children’s Study. Pharmacy 2017, 5, 21. [Google Scholar] [CrossRef] [PubMed]
- Shibata, M.; Ogawa, K.; Kanazawa, S.; Kawasaki, M.; Morisaki, N.; Mito, A.; Sago, H.; Horikawa, R.; Arata, N. Association of Maternal Birth Weight with the Risk of Low Birth Weight and Small-for-Gestational-Age in Offspring: A Prospective Single-Center Cohort Study. PLoS ONE 2021, 16, e0251734. [Google Scholar] [CrossRef]
- Low Birthweight: Country, Regional and Global Estimates; Wardlaw, T., Wardlaw, T.M., Weltgesundheitsorganisation, *!!! REPLACE !!!*, Eds.; World Health Organization: Geneva, 2004; ISBN 978-92-806-3832-5. [Google Scholar]
- Wagata, M.; Ishikuro, M.; Obara, T.; Nagai, M.; Mizuno, S.; Nakaya, N.; Nakamura, T.; Hirata, T.; Tsuchiya, N.; Metoki, H.; et al. Low Birth Weight and Abnormal Pre-Pregnancy Body Mass Index Were at Higher Risk for Hypertensive Disorders of Pregnancy. Pregnancy Hypertension 2020, 22, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Mezawa, H.; Tomotaki, A.; Yamamoto-Hanada, K.; Ishitsuka, K.; Ayabe, T.; Konishi, M.; Saito, M.; Yang, L.; Suganuma, N.; Hirahara, F.; et al. Prevalence of Congenital Anomalies in the Japan Environment and Children’s Study. Journal of Epidemiology 2019, 29, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Nishihama, Y.; Tatsuta, N.; Iwai-Shimada, M.; Nakai, K.; Arima, T.; Fujiwara, I.; Yaegashi, N.; Takeuchi, A.; Nakayama, S.F. The Association between Gestational Use of Personal Care Products and Neonatal Urological Abnormality at Birth: The Japan Environment and Children’s Study. Reproductive Toxicology 2020, 93, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Iwama, N.; Sugiyama, T.; Metoki, H.; Saito, M.; Hoshiai, T.; Watanabe, Z.; Tanaka, K.; Sasaki, S.; Sakurai, K.; Ishikuro, M.; et al. Associations between Glycosylated Hemoglobin Level at Less than 24 Weeks of Gestation and Adverse Pregnancy Outcomes in Japan: The Japan Environment and Children’s Study (JECS). Diabetes Research and Clinical Practice 2020, 169, 108377. [Google Scholar] [CrossRef] [PubMed]
- Heinze, G.; Schemper, M. A Solution to the Problem of Separation in Logistic Regression. Statistics in Medicine 2002, 21, 2409–2419. [Google Scholar] [CrossRef] [PubMed]
- R Core Team R: A Language and Environment for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 29 January 2024).
- Su, R.; Zhu, W.; Wei, Y.; Wang, C.; Feng, H.; Lin, L.; Hod, M.; Hadar, E.; Yang, H. Relationship of Maternal Birth Weight on Maternal and Neonatal Outcomes: A Multicenter Study in Beijing. J Perinatol 2016, 36, 1061–1066. [Google Scholar] [CrossRef]
- Lisi, A.; Botto, L.D.; Rittler, M.; Castilla, E.; Bianchi, F.; Botting, B.; De Walle, H.; Erickson, J.D.; Gatt, M.; De Vigan, C.; et al. Sex and Congenital Malformations: An International Perspective. Am. J. Med. Genet. 2005, 134A, 49–57. [Google Scholar] [CrossRef]
- Diab, N.S.; Barish, S.; Dong, W.; Zhao, S.; Allington, G.; Yu, X.; Kahle, K.T.; Brueckner, M.; Jin, S.C. Molecular Genetics and Complex Inheritance of Congenital Heart Disease. Genes 2021, 12, 1020. [Google Scholar] [CrossRef]
- Lee, K.-S.; Choi, Y.-J.; Cho, J.; Lee, H.; Lee, H.; Park, S.J.; Park, J.S.; Hong, Y.-C. Environmental and Genetic Risk Factors of Congenital Anomalies: An Umbrella Review of Systematic Reviews and Meta-Analyses. J Korean Med Sci 2021, 36, e183. [Google Scholar] [CrossRef] [PubMed]
- Mires, S.; Caputo, M.; Overton, T.; Skerritt, C. Maternal Micronutrient Deficiency and Congenital Heart Disease Risk: A Systematic Review of Observational Studies. Birth Defects Research 2022, 114, 1079–1091. [Google Scholar] [CrossRef]
- Choudhury, T.Z.; Majumdar, U.; Basu, M.; Garg, V. Impact of Maternal Hyperglycemia on Cardiac Development: Insights from Animal Models. Genesis 2021, 59, e23449. [Google Scholar] [CrossRef] [PubMed]
- Negrato, C.A.; Marques, P.R.; Leite, H.B.; Torigoe, C.N.; Silva, B.F.; Costa, K.; Kamei, J.M.; Zampa, C.L.; Toni, A.C.R.G.; Pereira, I.C.G.S.; et al. Glycemic and Nonglycemic Mechanisms of Congenital Malformations in Hyperglycemic Pregnancies: A Narrative Review. Archives of Endocrinology and Metabolism 2022. [Google Scholar] [CrossRef]
- Nicolaou, N.; Renkema, K.Y.; Bongers, E.M.H.F.; Giles, R.H.; Knoers, N.V.A.M. Genetic, Environmental, and Epigenetic Factors Involved in CAKUT. Nat Rev Nephrol 2015, 11, 720–731. [Google Scholar] [CrossRef] [PubMed]
- Postoev, V.A.; Grjibovski, A.M.; Kovalenko, A.A.; Anda, E.E.; Nieboer, E.; Odland, J.Ø. Congenital Anomalies of the Kidney and the Urinary Tract: A Murmansk County Birth Registry Study. Birth Defects Research 2016, 106, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Tain, Y.-L.; Luh, H.; Lin, C.-Y.; Hsu, C.-N. Incidence and Risks of Congenital Anomalies of Kidney and Urinary Tract in Newborns: A Population-Based Case–Control Study in Taiwan. Medicine 2016, 95, e2659. [Google Scholar] [CrossRef]
- Macumber, I.; Schwartz, S.; Leca, N. Maternal Obesity Is Associated with Congenital Anomalies of the Kidney and Urinary Tract in Offspring. Pediatr Nephrol 2017, 32, 635–642. [Google Scholar] [CrossRef]
- Groen In ’T Woud, S.; Renkema, K.Y.; Schreuder, M.F.; Wijers, C.H.W.; Van Der Zanden, L.F.M.; Knoers, N.V.A.M.; Feitz, W.F.J.; Bongers, E.M.H.F.; Roeleveld, N.; Van Rooij, I.A.L.M. Maternal Risk Factors Involved in Specific Congenital Anomalies of the Kidney and Urinary Tract: A Case–Control Study. Birth Defects Research 2016, 106, 596–603. [Google Scholar] [CrossRef]
- Boato, R.T.; Aguiar, M.B.; Mak, R.H.; Colosimo, E.A.; Simões E Silva, A.C.; Oliveira, E.A. Maternal Risk Factors for Congenital Anomalies of the Kidney and Urinary Tract: A Case-Control Study. Journal of Pediatric Urology 2023, 19, 199–e1. [Google Scholar] [CrossRef] [PubMed]
- Ornoy, A.; Reece, E.A.; Pavlinkova, G.; Kappen, C.; Miller, R.K. Effect of Maternal Diabetes on the Embryo, Fetus, and Children: Congenital Anomalies, Genetic and Epigenetic Changes and Developmental Outcomes. Birth Defects Research Pt C 2015, 105, 53–72. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, V.; Edwards, C.F.; Bichianu, D.C. Inguinal Hernia in Premature Infants.
- Smith, C.J.F.; Friedlander, S.F.; Guma, M.; Kavanaugh, A.; Chambers, C.D. Infantile Hemangiomas: An Updated Review on Risk Factors, Pathogenesis, and Treatment. Birth Defects Research 2017, 109, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Auger, N.; Del Giorgio, F.; Le-Nguyen, A.; Bilodeau-Bertrand, M.; Piché, N. Maternal Risk Factors for Paediatric Inguinal Hernia. British Journal of Surgery 2021, 109, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Kanda, T.; Murai-Takeda, A.; Kawabe, H.; Itoh, H. Low Birth Weight Trends: Possible Impacts on the Prevalences of Hypertension and Chronic Kidney Disease. Hypertens Res 2020, 43, 859–868. [Google Scholar] [CrossRef]
- Little, R.E. Birthweight and Gestational Age: Mothers’ Estimates Compared with State and Hospital Records. Am J Public Health 1986, 76, 1350–1351. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of this study.
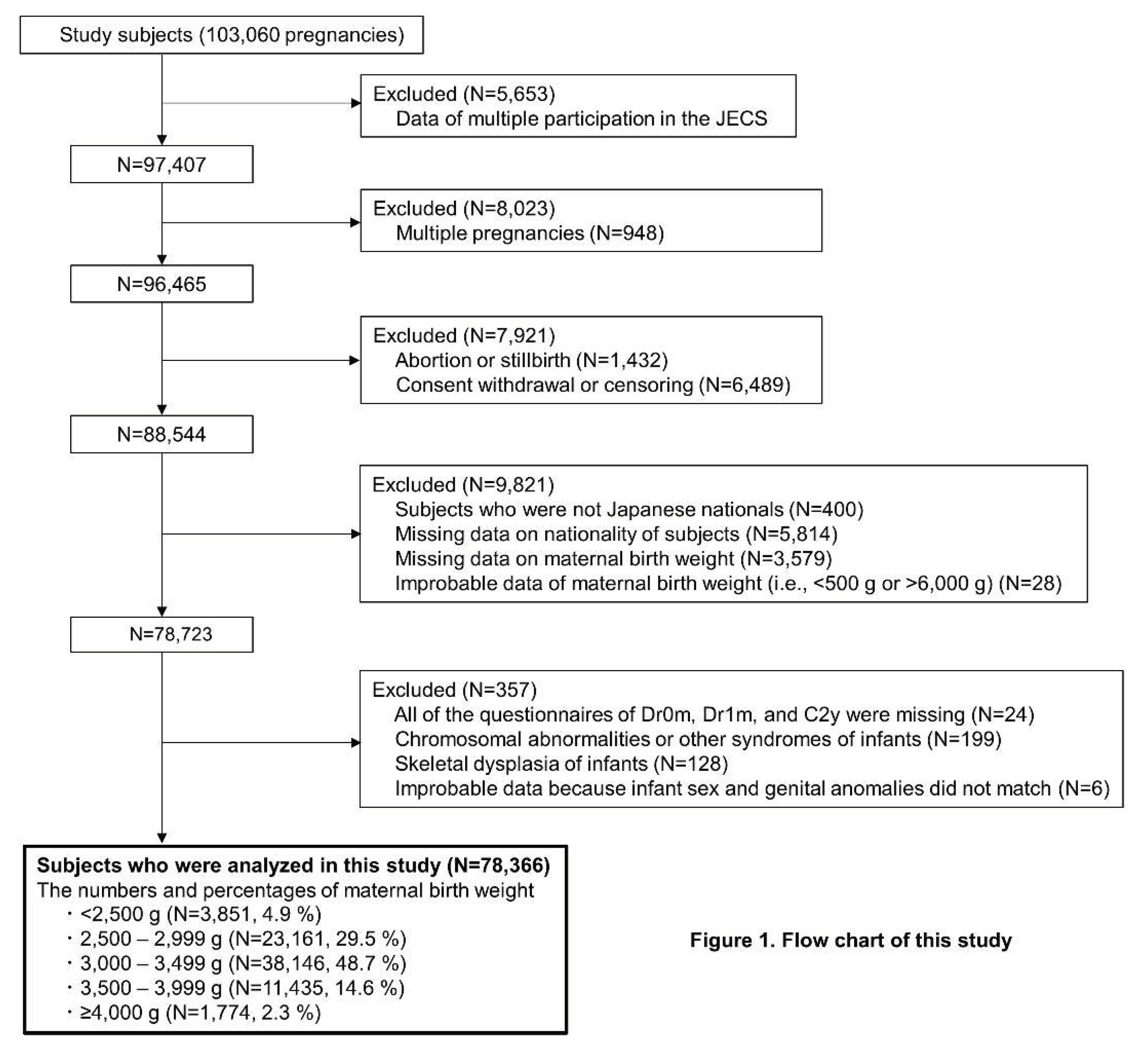

Table 1.
Characteristics of study participants.
| Variables | All participants (N=78,366) | Participants according to maternal birth weight | ||||
|---|---|---|---|---|---|---|
| <2,500 g (N=3,850) | 2,500–2,999 g (N=23,161) | 3,000–3,499 g (N=38,146) | 3,500–3,999 g (N=11,435) | ≥4,000 g (N=1,774) | ||
| Maternal age at the MT1 questionnaire, years | 30.9 (5.0) | 30.6 (5.2) | 30.7 (5.0) | 31.0 (4.9) | 31.2 (4.9) | 31.5 (4.8) |
| Category of maternal age at the MT1 questionnaire, N (%) | ||||||
| <25 years | 7,897 (10.1) | 498 (12.9) | 2,631 (11.4) | 3,653 (9.6) | 976 (8.5) | 139 (7.8) |
| 25–29.9 years | 22,832 (29.1) | 1,118 (29.0) | 6,971 (30.1) | 11,005 (28.8) | 3,270 (28.6) | 468 (26.4) |
| 30–34.9 years | 27,679 (35.3) | 1,298 (33.7) | 7,949 (34.3) | 13,727 (36.0) | 4,054 (35.5) | 651 (36.7) |
| ≥35 years | 19,480 (24.9) | 905 (23.5) | 5,478 (23.7) | 9,530 (25.0) | 3,061 (26.8) | 506 (28.5) |
| Missing | 478 (0.6) | 31 (0.8) | 132 (0.6) | 231 (0.6) | 74 (0.6) | 10 (0.6) |
| Pre-pregnancy BMI, kg/m2 | 21.2 (3.2) | 20.9 (3.3) | 20.9 (3.2) | 21.2 (3.2) | 21.5 (3.3) | 22.0 (3.6) |
| Category of pre-pregnancy BMI, N (%) | ||||||
| Underweight (<18.5 kg/m2) | 12,733 (16.2) | 790 (20.5) | 4,370 (18.9) | 5,973 (15.7) | 1,443 (12.6) | 157 (8.9) |
| Normal range (18.5–24.9 kg/m2) | 57,638 (73.5) | 2,682 (69.7) | 16,664 (71.9) | 28,251 (74.1) | 8,686 (76.0) | 1,355 (76.4) |
| Obese (≥25.0 kg/m2) | 7,936 (10.1) | 373 (9.7) | 2,105 (9.1) | 3,901 (10.2) | 1,297 (11.3) | 260 (14.7) |
| Missing | 59 (0.1) | 5 (0.1) | 22 (0.1) | 21 (0.1) | 9 (0.1) | 2 (0.1) |
| Parity, N (%) | ||||||
| Primipara | 33,188 (42.3) | 1,742 (45.2) | 9,997 (43.2) | 15,854 (41.6) | 4,888 (42.7) | 707 (39.9) |
| Multipara | 43,210 (55.1) | 2,015 (52.3) | 12,539 (54.1) | 21,364 (56.0) | 6,263 (54.8) | 1,029 (58.0) |
| Missing | 1,968 (2.5) | 93 (2.4) | 625 (2.7) | 928 (2.4) | 284 (2.5) | 38 (2.1) |
| Conception method, N (%) | ||||||
| Spontaneous pregnancy | 72,566 (92.6) | 3,567 (92.6) | 21,492 (92.8) | 35,385 (92.8) | 10,487 (91.7) | 1,635 (92.2) |
| Non-ART | 2,984 (3.8) | 147 (3.8) | 860 (3.7) | 1,423 (3.7) | 490 (4.3) | 64 (3.6) |
| ART | 2,446 (3.1) | 111 (2.9) | 701 (3.0) | 1,159 (3.0) | 408 (3.6) | 67 (3.8) |
| Missing | 370 (0.5) | 25 (0.6) | 108 (0.5) | 179 (0.5) | 50 (0.4) | 8 (0.5) |
| History of hypertension, N (%) | ||||||
| Yes | 355 (0.5) | 29 (0.8) | 119 (0.5) | 153 (0.4) | 46 (0.4) | 8 (0.5) |
| No | 77,536 (98.9) | 3,790 (98.4) | 22,910 (98.9) | 37,763 (99.0) | 11,317 (99.0) | 1,756 (99.0) |
| Missing | 475 (0.6) | 31 (0.8) | 132 (0.6) | 230 (0.6) | 72 (0.6) | 10 (0.6) |
| History of type 1 diabetes, N (%) | ||||||
| Yes | 61 (0.1) | 3 (0.1) | 19 (0.1) | 30 (0.1) | 7 (0.1) | 2 (0.1) |
| No | 77,830 (99.3) | 3,816 (99.1) | 23,010 (99.3) | 37,886 (99.3) | 11,356 (99.3) | 1,762 (99.3) |
| Missing | 475 (0.6) | 31 (0.8) | 132 (0.6) | 230 (0.6) | 72 (0.6) | 10 (0.6) |
| History of type 2 diabetes, N (%) | ||||||
| Yes | 96 (0.1) | 8 (0.2) | 31 (0.1) | 40 (0.1) | 12 (0.1) | 5 (0.3) |
| No | 77,795 (99.3) | 3,811 (99.0) | 22,998 (99.3) | 37,876 (99.3) | 11,351 (99.3) | 1,759 (99.2) |
| Missing | 475 (0.6) | 31 (0.8) | 132 (0.6) | 230 (0.6) | 72 (0.6) | 10 (0.6) |
| HbA1c (NGSP) level at <24 weeks of gestation, % | 5.2 (0.3) | 5.2 (0.3) | 5.2 (0.3) | 5.2 (0.3) | 5.2 (0.3) | 5.2 (0.3) |
| History of kidney disorder, N (%) | ||||||
| Yes | 341 (0.4) | 23 (0.6) | 102 (0.4) | 150 (0.4) | 55 (0.5) | 11 (0.6) |
| No | 77,550 (99.0) | 3,796 (98.6) | 22,927 (99.0) | 37,766 (99.0) | 11,308 (98.9) | 1,753 (98.8) |
| Missing | 475 (0.6) | 31 (0.8) | 132 (0.6) | 230 (0.6) | 72 (0.6) | 10 (0.6) |
| History of mental diseases, N (%) | ||||||
| Yes | 5,961 (7.6) | 323 (8.4) | 1,762 (7.6) | 2,849 (7.5) | 887 (7.8) | 140 (7.9) |
| No | 71,930 (91.8) | 3,496 (90.8) | 21,267 (91.8) | 35,067 (91.9) | 10,476 (91.6) | 1,624 (91.5) |
| Missing | 475 (0.6) | 31 (0.8) | 132 (0.6) | 230 (0.6) | 72 (0.6) | 10 (0.6) |
| History of congenital heart diseases, N (%) | ||||||
| Yes | 259 (0.3) | 22 (0.6) | 79 (0.3) | 109 (0.3) | 44 (0.4) | 5 (0.3) |
| No | 77,632 (99.1) | 3,797 (98.6) | 22,950 (99.1) | 37,807 (99.1) | 11,319 (99.0) | 1,759 (99.2) |
| Missing | 475 (0.6) | 31 (0.8) | 132 (0.6) | 230 (0.6) | 72 (0.6) | 10 (0.6) |
| Uterine malformation, N (%) | ||||||
| Yes | 223 (0.3) | 8 (0.2) | 74 (0.3) | 110 (0.3) | 27 (0.2) | 4 (0.2) |
| No | 77,668 (99.1) | 3,811 (99.0) | 22,955 (99.1) | 37,806 (99.1) | 11,336 (99.1) | 1,760 (99.2) |
| Missing | 475 (0.6) | 31 (0.8) | 132 (0.6) | 230 (0.6) | 72 (0.6) | 10 (0.6) |
| Malformation of urinary tract or genital organs, N (%) | ||||||
| Yes | 30 (0.0) | 0 (0.0) | 11 (0.0) | 15 (0.0) | 4 (0.0) | 0 (0.0) |
| No | 77,861 (99.4) | 3,819 (99.2) | 23,018 (99.4) | 37,901 (99.4) | 11,359 (99.3) | 1,764 (99.4) |
| Missing | 475 (0.6) | 31 (0.8) | 132 (0.6) | 230 (0.6) | 72 (0.6) | 10 (0.6) |
| Currently smoking, N (%) | ||||||
| Yes | 3,104 (4.0) | 209 (5.4) | 999 (4.3) | 1,456 (3.8) | 362 (3.2) | 78 (4.4) |
| No | 74,288 (94.8) | 3,584 (93.1) | 21,877 (94.5) | 36,217 (94.9) | 10,934 (95.6) | 1,676 (94.5) |
| Missing | 974 (1.2) | 57 (1.5) | 285 (1.2) | 473 (1.2) | 139 (1.2) | 20 (1.1) |
| Continue drinking, N (%) | ||||||
| Yes | 7,943 (10.1) | 359 (9.3) | 2,304 (9.9) | 3,906 (10.2) | 1,175 (10.3) | 199 (11.2) |
| No | 69,624 (88.8) | 3,440 (89.4) | 20,623 (89.0) | 33,854 (88.7) | 10,150 (88.8) | 1,557 (87.8) |
| Missing | 799 (1.0) | 51 (1.3) | 234 (1.0) | 386 (1.0) | 110 (1.0) | 18 (1.0) |
| Use of any drug before 12 weeks of gestation (methimazole, SSRI, antidepressant drug except for SSRI, antianxiety, sleeping pill, antipsychotic, valproic acid, antiepileptic except for valproic acid, lithium carbonate, and other psychoactive drug), N (%) | 2,154 (2.7) | 133 (3.5) | 672 (2.9) | 1,011 (2.7) | 298 (2.6) | 40 (2.3) |
| Use of folic acid supplement before 12 weeks of gestation, N (%) | 25,604 (32.7) | 1,267 (32.9) | 7,493 (32.4) | 12,543 (32.9) | 3,749 (32.8) | 552 (31.1) |
| New-onset HDP, N (%) | ||||||
| Yes | 779 (1.0) | 48 (1.2) | 238 (1.0) | 386 (1.0) | 90 (0.8) | 17 (1.0) |
| No | 77,587 (99.0) | 3,802 (98.8) | 22,923 (99.0) | 37,760 (99.0) | 11,345 (99.2) | 1,757 (99.0) |
| GDM, N (%) | ||||||
| Yes | 2,132 (2.7) | 153 (4.0) | 682 (2.9) | 976 (2.6) | 272 (2.4) | 49 (2.8) |
| No | 76,092 (97.1) | 3,689 (95.8) | 22,435 (96.9) | 37,105 (97.3) | 11,143 (97.4) | 1,720 (97.0) |
| Missing | 142 (0.2) | 8 (0.2) | 44 (0.2) | 65 (0.2) | 20 (0.2) | 5 (0.3) |
| Maternal highest level of education, N (%) | ||||||
| <13 years | 26,252 (33.5) | 1,518 (39.4) | 7,994 (34.5) | 12,581 (33.0) | 3,536 (30.9) | 623 (35.1) |
| ≥13 years | 51,185 (65.3) | 2,280 (59.2) | 14,894 (64.3) | 25,107 (65.8) | 7,779 (68.0) | 1,125 (63.4) |
| Missing | 929 (1.2) | 52 (1.4) | 273 (1.2) | 458 (1.2) | 120 (1.0) | 26 (1.5) |
| Marital status, N (%) | ||||||
| Unmarried or divorced or widowed | 3,185 (4.1) | 211 (5.5) | 1,020 (4.4) | 1,466 (3.8) | 429 (3.8) | 59 (3.3) |
| Married | 74,426 (95.0) | 3,588 (93.2) | 21,923 (94.7) | 36,320 (95.2) | 10,896 (95.3) | 1,699 (95.8) |
| Missing | 755 (1.0) | 51 (1.3) | 218 (0.9) | 360 (0.9) | 110 (1.0) | 16 (0.9) |
| Annual household income (million, Japanese Yen), N (%) | ||||||
| <4 | 28,310 (36.1) | 1,551 (40.3) | 8,592 (37.1) | 13,631 (35.7) | 3,899 (34.1) | 637 (35.9) |
| 4–5.99 | 36,476 (46.5) | 1,656 (43.0) | 10,544 (45.5) | 17,902 (46.9) | 5,552 (48.6) | 822 (46.3) |
| ≥6 | 8,204 (10.5) | 353 (9.2) | 2,371 (10.2) | 4,088 (10.7) | 1,211 (10.6) | 181 (10.2) |
| Missing | 5,376 (6.9) | 290 (7.5) | 1,654 (7.1) | 2,525 (6.6) | 773 (6.8) | 134 (7.6) |
| Delivery week, weeks | 39.3 (1.5) | 39.0 (1.7) | 39.2 (1.6) | 39.3 (1.5) | 39.4 (1.5) | 39.4 (1.5) |
| Preterm delivery at <37 weeks of gestation, N (%) | ||||||
| Yes | 3,476 (4.4) | 242 (6.3) | 1,174 (5.1) | 1,571 (4.1) | 420 (3.7) | 69 (3.9) |
| No | 74,748 (95.4) | 3,600 (93.5) | 21,943 (94.7) | 36,510 (95.7) | 10,995 (96.2) | 1,700 (95.8) |
| Missing | 142 (0.2) | 8 (0.2) | 44 (0.2) | 65 (0.2) | 20 (0.2) | 5 (0.3) |
| Infant sex, N (%) | ||||||
| Male | 40,117 (51.2) | 1,963 (51.0) | 11,820 (51.0) | 19,535 (51.2) | 5,884 (51.5) | 915 (51.6) |
| Female | 38,249 (48.8) | 1,887 (49.0) | 11,341 (49.0) | 18,611 (48.8) | 5,551 (48.5) | 859 (48.4) |
| Infant birth weight, g | 3,026 (411) | 2,877 (425) | 2,933 (400) | 3,044 (395) | 3,171 (415) | 3,258 (425) |
| Category of infant birth weight in percentiles, N (%) | ||||||
| SGA (<10th percentile) | 5,751 (7.3) | 542 (14.1) | 2,418 (10.4) | 2,348 (6.2) | 401 (3.5) | 42 (2.4) |
| AGA (≥10th percentile and <90th percentile) | 62,580 (79.9) | 2,975 (77.3) | 18,625 (80.4) | 31,036 (81.4) | 8,716 (76.2) | 1,228 (69.2) |
| LGA (≥90th percentile) | 7,708 (9.8) | 221 (5.7) | 1,403 (6.1) | 3,652 (9.6) | 1,974 (17.3) | 458 (25.8) |
| Missing | 2,327 (3.0) | 112 (2.9) | 715 (3.1) | 1,110 (2.9) | 344 (3.0) | 46 (2.6) |
| Category of infant birth weight in grams, N (%) | ||||||
| Low birth weight (<2,500 g) | 6,176 (7.9) | 570 (14.8) | 2,520 (10.9) | 2,526 (6.6) | 497 (4.3) | 63 (3.6) |
| Normal birth weight (≥2,500 g and <4,000 g) | 71,333 (91.0) | 3,247 (84.3) | 20,497 (88.5) | 35,252 (92.4) | 10,684 (93.4) | 1,653 (93.2) |
| Macrosomia (≥4,000 g) | 673 (0.9) | 20 (0.5) | 91 (0.4) | 283 (0.7) | 226 (2.0) | 53 (3.0) |
| Missing | 184 (0.2) | 13 (0.3) | 53 (0.2) | 85 (0.2) | 28 (0.2) | 5 (0.3) |
| Data are expressed as mean (SD) or the number (percentage). ART, assisted reproductive technology; AGA, appropriate gestational age; BMI, body mass index; GDM, gestational diabetes mellitus; HDP, hypertensive disorders of pregnancy; LGA, large for gestational age; NGSP, National Glycohemoglobin Standardization Program; SD, standard deviation; SGA, small gestational age; SSRI, selective serotonin reuptake inhibitor. | ||||||
Table 2.
Prevalence of infant congenital malformations.
| Infant congenital malformations | All participants (N=78,366) | Participants according to maternal birth weight | ||||
|---|---|---|---|---|---|---|
| <2,500 g (N=3,850) | 2,500–2,999 g (N=23,161) | 3,000–3,499 g (N=38,146) | 3,500–3,999 g (N=11,435) | ≥4,000 g (N=1,774) | ||
| Nervous system, Cases (%) | 205 (0.26) | 14 (0.36) | 60 (0.26) | 93 (0.24) | 33 (0.29) | 5 (0.28) |
| Anencephaly, Cases (%) | 11 (0.01) | 0 (0.00) | 4 (0.02) | 5 (0.01) | 2 (0.02) | 0 (0.00) |
| Encephalocele, Cases (%) | 14 (0.02) | 0 (0.00) | 3 (0.01) | 7 (0.02) | 4 (0.03) | 0 (0.00) |
| Microcephaly, Cases (%) | 25 (0.03) | 1 (0.03) | 9 (0.04) | 12 (0.03) | 2 (0.02) | 1 (0.06) |
| Hydrocephalus, Cases (%) | 59 (0.08) | 7 (0.18) | 12 (0.05) | 32 (0.08) | 7 (0.06) | 1 (0.06) |
| Holoprosencephaly, Cases (%) | 20 (0.03) | 2 (0.05) | 6 (0.03) | 7 (0.02) | 5 (0.04) | 0 (0.00) |
| Craniotabes, Cases (%) | 58 (0.07) | 4 (0.10) | 19 (0.08) | 22 (0.06) | 12 (0.10) | 1 (0.06) |
| Agenesis of corpus callosum, Cases (%) | 17 (0.02) | 1 (0.03) | 4 (0.02) | 8 (0.02) | 4 (0.03) | 0 (0.00) |
| Spina bifida, Cases (%) | 24 (0.03) | 2 (0.05) | 7 (0.03) | 12 (0.03) | 1 (0.01) | 2 (0.11) |
| Eye, ear, and face, Cases (%) | 228 (0.29) | 7 (0.18) | 71 (0.31) | 118 (0.31) | 27 (0.24) | 5 (0.28) |
| Eyelid coloboma, Cases (%) | 12 (0.02) | 1 (0.03) | 3 (0.01) | 8 (0.02) | 0 (0.00) | 0 (0.00) |
| Microphthalmia (anophthalmia), Cases (%) | 13 (0.02) | 0 (0.00) | 2 (0.01) | 9 (0.02) | 1 (0.01) | 1 (0.06) |
| Cataract, Cases (%) | 28 (0.04) | 1 (0.03) | 8 (0.03) | 15 (0.04) | 4 (0.03) | 0 (0.00) |
| Microtia, Cases (%) | 39 (0.05) | 0 (0.00) | 13 (0.06) | 24 (0.06) | 2 (0.02) | 0 (0.00) |
| Atresia of external auditory canal, Cases (%) | 35 (0.04) | 0 (0.00) | 13 (0.06) | 14 (0.04) | 7 (0.06) | 1 (0.06) |
| Cryptotia, Cases (%) | 30 (0.04) | 0 (0.00) | 14 (0.06) | 12 (0.03) | 3 (0.03) | 1 (0.06) |
| Low-set ear, Cases (%) | 29 (0.04) | 1 (0.03) | 11 (0.05) | 14 (0.04) | 3 (0.03) | 0 (0.00) |
| Hearing loss, Cases (%) | 61 (0.08) | 5 (0.13) | 15 (0.06) | 31 (0.08) | 8 (0.07) | 2 (0.11) |
| Facial cleft, Cases (%) | 7 (0.01) | 0 (0.00) | 2 (0.01) | 4 (0.01) | 1 (0.01) | 0 (0.00) |
| Cleft lip and/or cleft palate, Cases (%) | 165 (0.21) | 12 (0.31) | 56 (0.24) | 70 (0.18) | 26 (0.23) | 1 (0.06) |
| Circulatory system, Cases (%) | 1,141 (1.46) | 72 (1.87) | 331 (1.43) | 516 (1.35) | 187 (1.64) | 35 (1.97) |
| Congenital heart disease, Cases (%) | 1,068 (1.36) | 69 (1.79) | 311 (1.34) | 485 (1.27) | 172 (1.50) | 31 (1.75) |
| Arrhythmia, Cases (%) | 84 (0.11) | 3 (0.08) | 25 (0.11) | 34 (0.09) | 17 (0.15) | 5 (0.28) |
| Respiratory system, Cases (%) | 32 (0.04) | 1 (0.03) | 7 (0.03) | 17 (0.04) | 6 (0.05) | 1 (0.06) |
| Pulmonary sequestration, Cases (%) | 8 (0.01) | 0 (0.00) | 2 (0.01) | 3 (0.01) | 3 (0.03) | 0 (0.00) |
| CCAM, Cases (%) | 14 (0.02) | 1 (0.03) | 3 (0.01) | 7 (0.02) | 3 (0.03) | 0 (0.00) |
| Pulmonary hypoplasia, Cases (%) | 14 (0.02) | 0 (0.00) | 3 (0.01) | 9 (0.02) | 1 (0.01) | 1 (0.06) |
| Digestive system, Cases (%) | 62 (0.08) | 1 (0.03) | 26 (0.11) | 25 (0.07) | 9 (0.08) | 1 (0.06) |
| Oesophageal atresia, Cases (%) | 6 (0.01) | 0 (0.00) | 4 (0.02) | 1 (0.00) | 1 (0.01) | 0 (0.00) |
| Duodenal atresia, Cases (%) | 11 (0.01) | 0 (0.00) | 3 (0.01) | 6 (0.02) | 1 (0.01) | 1 (0.06) |
| Small intestinal atresia, Cases (%) | 17 (0.02) | 0 (0.00) | 5 (0.02) | 10 (0.03) | 2 (0.02) | 0 (0.00) |
| Imperforate anus (anorectal anomaly), Cases (%) | 35 (0.04) | 1 (0.03) | 16 (0.07) | 12 (0.03) | 5 (0.04) | 1 (0.06) |
| Urinary system (CAKUT), Cases (%) | 271 (0.35) | 17 (0.44) | 66 (0.28) | 135 (0.35) | 39 (0.34) | 14 (0.79) |
| Hydronephrosis, Cases (%) | 229 (0.29) | 13 (0.34) | 61 (0.26) | 109 (0.29) | 33 (0.29) | 13 (0.73) |
| Cystic renal anomalies, Cases (%) | 31 (0.04) | 2 (0.05) | 4 (0.02) | 19 (0.05) | 5 (0.04) | 1 (0.06) |
| Renal agenesis, Cases (%) | 17 (0.02) | 2 (0.05) | 2 (0.01) | 11 (0.03) | 2 (0.02) | 0 (0.00) |
| Bladder exstrophy/cloacal exstrophy, Cases (%) | 2 (0.00) | 0 (0.00) | 0 (0.00) | 2 (0.01) | 0 (0.00) | 0 (0.00) |
| Genital organs in male infants, Cases/N (%) | 448/40,117(1.12) | 32/1,963(1.63) | 139/11,820(1.18) | 194/19,535(0.99) | 74/5,884(1.26) | 9/915(0.98) |
| Hypospadias, Cases/N (%) | 271/40,117(0.68) | 21/1,963(1.07) | 85/11,820(0.72) | 118/19,535(0.60) | 40/5,884(0.68) | 7/915(0.77) |
| Cryptorchidism/nonpalpable testis, Cases/N (%) | 266/40,117(0.66) | 18/1,963(0.92) | 82/11,820(0.69) | 115/19,535(0.59) | 46/5,884(0.78) | 5/915(0.55) |
| Micropenis, Cases/N (%) | 4/40,117(0.01) | 0/1,963(0.00) | 1/11,820(0.01) | 2/19,535(0.01) | 1/5,884(0.02) | 0/915(0.00) |
| Bifid scrotum, Cases/N (%) | 8/40,117(0.02) | 0/1,963(0.00) | 3/11,820(0.03) | 3/19,535(0.02) | 2/5,884(0.03) | 0/915(0.00) |
| Genital organs in female infants, Cases/N (%) | 11/38,249(0.03) | 0/1,887(0.00) | 4/11,341(0.04) | 6/18,611(0.03) | 1/5,551(0.02) | 0/859(0.00) |
| Clitoral hypertrophy, Cases/N (%) | 7/38,249(0.02) | 0/1,887(0.00) | 4/11,341(0.04) | 3/18,611(0.02) | 0/5,551(0.00) | 0/859(0.00) |
| Abnormal vagina opening, Cases/N (%) | 4/38,249(0.01) | 0/1,887(0.00) | 0/11,341(0.00) | 3/18,611(0.02) | 1/5,551(0.02) | 0/859(0.00) |
| Musculoskeletal system, Cases (%) | 289 (0.37) | 8 (0.21) | 94 (0.41) | 135 (0.35) | 40 (0.35) | 12 (0.68) |
| Congenital diaphragmatic hernia, Cases (%) | 29 (0.04) | 1 (0.03) | 9 (0.04) | 13 (0.03) | 6 (0.05) | 0 (0.00) |
| Umbilical hernia, Cases (%) | 32 (0.04) | 3 (0.08) | 8 (0.03) | 14 (0.04) | 4 (0.03) | 3 (0.17) |
| Gastroschisis, Cases (%) | 5 (0.01) | 0 (0.00) | 2 (0.01) | 1 (0.00) | 1 (0.01) | 1 (0.06) |
| Scoliosis, Cases (%) | 2 (0.00) | 0 (0.00) | 0 (0.00) | 2 (0.01) | 0 (0.00) | 0 (0.00) |
| Limbs, N (%) | 221 (0.28) | 4 (0.10) | 75 (0.32) | 105 (0.28) | 29 (0.25) | 8 (0.45) |
| Polydactyly of upper limb, Cases (%) | 79 (0.10) | 2 (0.05) | 31 (0.13) | 38 (0.10) | 6 (0.05) | 2 (0.11) |
| Syndactyly of upper limb, Cases (%) | 37 (0.05) | 1 (0.03) | 14 (0.06) | 13 (0.03) | 8 (0.07) | 1 (0.06) |
| Brachydactyly of upper limb, Cases (%) | 10 (0.01) | 1 (0.03) | 5 (0.02) | 3 (0.01) | 1 (0.01) | 0 (0.00) |
| Cleft hand of upper limb, Cases (%) | 6 (0.01) | 0 (0.00) | 3 (0.01) | 3 (0.01) | 0 (0.00) | 0 (0.00) |
| Defect of upper limb, Cases (%) | 2 (0.00) | 0 (0.00) | 1 (0.00) | 1 (0.00) | 0 (0.00) | 0 (0.00) |
| Polydactyly of lower limb, Cases (%) | 82 (0.10) | 0 (0.00) | 22 (0.09) | 43 (0.11) | 13 (0.11) | 4 (0.23) |
| Syndactyly of lower limb, Cases (%) | 88 (0.11) | 2 (0.05) | 21 (0.09) | 45 (0.12) | 16 (0.14) | 4 (0.23) |
| Short toe, Cases (%) | 2 (0.00) | 0 (0.00) | 1 (0.00) | 1 (0.00) | 0 (0.00) | 0 (0.00) |
| Cleft foot, Cases (%) | 6 (0.01) | 0 (0.00) | 3 (0.01) | 3 (0.01) | 0 (0.00) | 0 (0.00) |
| Defect of lower limb, Cases (%) | 3 (0.00) | 0 (0.00) | 1 (0.00) | 2 (0.01) | 0 (0.00) | 0 (0.00) |
| Skin, Cases (%) | 610 (0.78) | 43 (1.12) | 174 (0.75) | 292 (0.77) | 89 (0.78) | 12 (0.68) |
| Angioma, Cases (%) | 600 (0.77) | 43 (1.12) | 172 (0.74) | 286 (0.75) | 87 (0.76) | 12 (0.68) |
| Epidermolysis bullosa hereditaria/ incontinence of pigment, Cases (%) | 10 (0.01) | 0 (0.00) | 2 (0.01) | 6 (0.02) | 2 (0.02) | 0 (0.00) |
| Inguinal Hernia, Cases (%) | 382 (0.49) | 31 (0.81) | 106 (0.46) | 175 (0.46) | 59 (0.52) | 11 (0.62) |
| Data are expressed as the number (percentage). Abbreviations: CAKUT, congenital anomalies of the kidney and urinary tract; CCAM, congenital cystic adenomatoid malformation | ||||||
Table 3.
Association between MBW and prevalence of infant congenital malformations.
| Infant congenital malformations | Maternal birth weight | ||||
|---|---|---|---|---|---|
| <2,500 g (N=3,850) | 2,500–2,999 g (N=23,161) | 3,000–3,499 g (N=38,146) | 3,500–3,999 g (N=11,435) | ≥4,000 g (N=1,774) | |
| Nervous system | |||||
| Cases (%) | 14 (0.36) | 60 (0.26) | 93 (0.24) | 33 (0.29) | 5 (0.28) |
| Model 1, Crude OR (95% CI)a | 1.538 (0.848–2.590) | 1.066 (0.768–1.469) | Reference | 1.196 (0.794–1.756) | 1.256 (0.470–2.724) |
| Model 2, Adjusted OR (95% CI)a, b | 1.242 (0.947–1.628) | 1.029 (0.878–1.206) | Reference | 1.098 (0.905–1.332) | 1.144 (0.751–1.744) |
| Eye, ear, and face | |||||
| Cases (%) | 7 (0.18) | 71 (0.31) | 118 (0.31) | 27 (0.24) | 5 (0.28) |
| Model 1, Crude OR (95% CI)a | 0.626 (0.273–1.222) | 0.994 (0.738–1.329) | Reference | 0.774 (0.501–1.153) | 0.997 (0.372–2.134) |
| Model 2, Adjusted OR (95% CI)a, b | 0.792 (0.552–1.136) | 0.998 (0.864–1.153) | Reference | 0.875 (0.714–1.073) | 0.987 (0.649–1.502) |
| Cleft lip and/or cleft palate | |||||
| Cases (%) | 12 (0.31) | 56 (0.24) | 70 (0.18) | 26 (0.23) | 1 (0.06) |
| Model 1, Crude OR (95% CI)a | 1.759 (0.918–3.096) | 1.321 (0.927–1.872) | Reference | 1.254 (0.789–1.936) | 0.457 (0.052–1.666) |
| Model 2, Adjusted OR (95% CI)a, b | 1.331 (0.994–1.784) | 1.154 (0.973–1.368) | Reference | 1.114 (0.896–1.385) | 0.668 (0.304–1.466) |
| Circulatory system | |||||
| Congenital heart diseases | |||||
| Cases (%) | 69 (1.79) | 311 (1.34) | 485 (1.27) | 172 (1.50) | 31 (1.75) |
| Model 1, Crude OR (95% CI) | 1.417 (1.099–1.828) | 1.057 (0.916–1.220) | Reference | 1.186 (0.995–1.413) | 1.381 (0.958–1.992) |
| Model 2, Adjusted OR (95% CI)b | 1.388 (1.075–1.792) | 1.050 (0.909–1.212) | Reference | 1.179 (0.989–1.405) | 1.370 (0.949–1.977) |
| Arrhythmia | |||||
| Cases (%) | 3 (0.08) | 25 (0.11) | 34 (0.09) | 17 (0.15) | 5 (0.28) |
| Model 1, Crude OR (95% CI)a | 1.005 (0.273–2.639) | 1.218 (0.723–2.024) | Reference | 1.693 (0.931–2.969) | 3.435 (1.240–7.793) |
| Model 2, Adjusted OR (95% CI)a, b | 1.029 (0.613–1.729) | 1.123 (0.881–1.432) | Reference | 1.284 (0.977–1.688) | 1.775 (1.157–2.725) |
| Urinary system (CAKUT) | |||||
| Cases (%) | 17 (0.44) | 66 (0.28) | 135 (0.35) | 39 (0.34) | 14 (0.79) |
| Model 1, Crude OR (95% CI) | 1.249 (0.753–2.070) | 0.805 (0.599–1.081) | Reference | 0.964 (0.674–1.377) | 2.240 (1.289–3.891) |
| Model 2, Adjusted OR (95% CI)b | 1.254 (0.756–2.083) | 0.809 (0.602–1.087) | Reference | 0.957 (0.669–1.368) | 2.194 (1.261–3.819) |
| Genital organs in male infants, N | N=1,963 | N=11,820 | N=19,535 | N=5,884 | N=915 |
| Cases (%) | 32 (1.63) | 139 (1.18) | 194 (0.99) | 74 (1.26) | 9 (0.98) |
| Model 1, Crude OR (95% CI) | 1.652 (1.133–2.408) | 1.186 (0.953–1.477) | Reference | 1.270 (0.970–1.662) | 0.990 (0.506–1.939) |
| Model 2, Adjusted OR (95% CI)b | 1.648 (1.130–2.405) | 1.189 (0.954–1.481) | Reference | 1.264 (0.965–1.655) | 0.974 (0.497–1.907) |
| Hypospadias in male infants | |||||
| Cases (%) | 21 (1.07) | 85 (0.72) | 118 (0.60) | 40 (0.68) | 7 (0.77) |
| Model 1, Crude OR (95% CI) | 1.779 (1.116–2.837) | 1.192 (0.901–1.577) | Reference | 1.126 (0.786–1.614) | 1.269 (0.590–2.727) |
| Model 2, Adjusted OR (95% CI)b | 1.804 (1.130–2.881) | 1.199 (0.906–1.587) | Reference | 1.115 (0.778–1.599) | 1.250 (0.581–2.691) |
| Cryptorchidism/nonpalpable testis in male infants | |||||
| Cases (%) | 18 (0.92) | 82 (0.69) | 115 (0.59) | 46 (0.78) | 5 (0.55) |
| Model 1, Crude OR (95% CI) | 1.563 (0.949–2.574) | 1.180 (0.888–1.567) | Reference | 1.331 (0.944–1.875) | 0.928 (0.378–2.277) |
| Model 2, Adjusted OR (95% CI)b | 1.515 (0.919–2.498) | 1.170 (0.880–1.556) | Reference | 1.332 (0.945–1.879) | 0.912 (0.371–2.240) |
| Musculoskeletal system | |||||
| Limbs | |||||
| Cases (%) | 4 (0.10) | 75 (0.32) | 105 (0.28) | 29 (0.25) | 8 (0.45) |
| Model 1, Crude OR (95% CI) | 0.377 (0.139–1.023) | 1.177 (0.875–1.584) | Reference | 0.921 (0.610–1.390) | 1.641 (0.799–3.373) |
| Model 2, Adjusted OR (95% CI)b | 0.370 (0.136–1.007) | 1.168 (0.868–1.573) | Reference | 0.912 (0.604–1.378) | 1.634 (0.794–3.363) |
| Skin | |||||
| Angioma | |||||
| Cases (%) | 43 (1.12) | 174 (0.75) | 292 (0.77) | 89 (0.78) | 12 (0.68) |
| Model 1, Crude OR (95% CI) | 1.495 (1.083–2.064) | 0.990 (0.819–1.197) | Reference | 1.015 (0.798–1.291) | 0.902 (0.505–1.609) |
| Model 2, Adjusted OR (95% CI)b | 1.491 (1.079–2.059) | 0.993 (0.821–1.201) | Reference | 1.004 (0.789–1.278) | 0.882 (0.494–1.576) |
| Inguinal hernia | |||||
| Cases (%) | 31 (0.81) | 106 (0.46) | 175 (0.46) | 59 (0.52) | 11 (0.62) |
| Model 1, Crude OR (95% CI) | 1.761 (1.200–2.584) | 0.998 (0.783–1.270) | Reference | 1.125 (0.837–1.513) | 1.354 (0.735–2.494) |
| Model 2, Adjusted OR (95% CI)b | 1.746 (1.189–2.565) | 0.997 (0.783–1.271) | Reference | 1.119 (0.832–1.504) | 1.344 (0.729–2.479) |
| a Firth logistic regression model was applied. b Adjusted for maternal age in the MT1 questionnaire, pre-pregnancy BMI, conception method, parity (primipara or not), history of mental illness, history of kidney disease, history of congenital heart disease, history of uterine malformation and/or urogenital malformation, smoking status, alcohol consumption, marital status, education level, annual income, use of any drug before 12 weeks of gestation (methimazole, SSRI, antidepressant drug except for SSRI, antianxiety, sleeping pill, antipsychotic, valproic acid, antiepileptic except for valproic acid, lithium carbonate, and other psychoactive drug), use of folic acid supplement at <12 weeks of gestation, HbA1c level at <24 weeks of gestation, and infant sex. In the analysis of the association between maternal birth weight and genital organs in male infants, the infant sex was not included in the model. Abbreviations: BMI, body mass index; CAKUT, congenital anomalies of the kidney and urinary tract; CI, confidence interval; HbA1c, glycosylated haemoglobin; OR, odds ratio; SSRI, selective serotonin reuptake inhibitor. | |||||
Table 4.
Association between MBW and prevalence of infant congenital malformations stratified infant sex.
Table 4.
Association between MBW and prevalence of infant congenital malformations stratified infant sex.
| Infant congenital malformations | Maternal birth weight | ||||
|---|---|---|---|---|---|
| <2,500 g | 2,500–2,999 g | 3,000–3,499 g | 3,500–3,999 g | ≥4,000 g | |
| The number of male and female infants | |||||
| Male infants, N | 1,963 | 11,820 | 19,535 | 5,884 | 915 |
| Female infants, N | 1,887 | 11,341 | 18,611 | 5,551 | 859 |
| Nervous system | |||||
| Male infants | |||||
| Cases (%) | 9 (0.46) | 30 (0.25) | 55 (0.28) | 17 (0.29) | 2 (0.22) |
| Model 1, Crude OR (95% CI)a | 1.706 (0.803–3.240) | 0.908 (0.577–1.402) | Reference | 1.047 (0.594–1.755) | 0.961 (0.199–2.804) |
| Model 2, Adjusted OR (95% CI)a, b | 1.306 (0.936–1.821) | 0.952 (0.769–1.178) | Reference | 1.024 (0.790–1.328) | 0.988 (0.536–1.822) |
| Female infants | |||||
| Cases (%) | 5 (0.26) | 30 (0.26) | 38 (0.20) | 16 (0.29) | 3 (0.35) |
| Model 1, Crude OR (95% CI)a | 1.409 (0.511–3.172) | 1.301 (0.803–2.089) | Reference | 1.438 (0.786–2.516) | 1.971 (0.537–5.149) |
| Model 2, Adjusted OR (95% CI)a, b | 1.192 (0.780–1.823) | 1.138 (0.906–1.428) | Reference | 1.208 (0.916–1.592) | 1.437 (0.850–2.428) |
| Eye, ear, and face | |||||
| Male infants | |||||
| Cases (%) | 2 (0.10) | 45 (0.38) | 68 (0.35) | 12 (0.20) | 3 (0.33) |
| Model 1, Crude OR (95% CI)a | 0.363 (0.075–1.048) | 1.098 (0.750–1.593) | Reference | 0.605 (0.315–1.066) | 1.090 (0.301–2.768) |
| Model 2, Adjusted OR (95% CI)a, b | 0.599 (0.326–1.101) | 1.048 (0.874–1.257) | Reference | 0.777 (0.580–1.040) | 1.041 (0.618–1.753) |
| Female infants | |||||
| Cases (%) | 5 (0.26) | 26 (0.23) | 50 (0.27) | 15 (0.27) | 2 (0.23) |
| Model 1, Crude OR (95% CI)a | 1.074 (0.393–2.374) | 0.861 (0.530–1.365) | Reference | 1.029 (0.563–1.775) | 1.072 (0.221–3.141) |
| Model 2, Adjusted OR (95% CI)a, b | 1.047 (0.687–1.591) | 0.932 (0.744–1.168) | Reference | 1.015 (0.773–1.334) | 1.014 (0.552–1.865) |
| Cleft lip and/or cleft palate | |||||
| Male infants | |||||
| Cases (%) | 9 (0.46) | 33 (0.28) | 43 (0.22) | 14 (0.24) | 1 (0.11) |
| Model 1, Crude OR (95% CI)a | 2.179 (1.014–4.208) | 1.274 (0.806–1.995) | Reference | 1.107 (0.590–1.957) | 0.735 (0.083–2.729) |
| Model 2, Adjusted OR (95% CI)a, b | 1.473 (1.052–2.064) | 1.132 (0.912–1.406) | Reference | 1.050 (0.789–1.396) | 0.845 (0.386–1.846) |
| Female infants | |||||
| Cases (%) | 3 (0.16) | 23 (0.20) | 27 (0.15) | 12 (0.22) | 0 (0.00) |
| Model 1, Crude OR (95% CI)a | 1.255 (0.338–3.358) | 1.403 (0.803–2.433) | Reference | 1.525 (0.754–2.914) | 0.393 (0.003–2.802) |
| Model 2, Adjusted OR (95% CI)a, b | 1.137 (0.678–1.906) | 1.183 (0.913–1.533) | Reference | 1.219 (0.890–1.671) | 0.626 (0.169–2.314) |
| Circulatory system | |||||
| Congenital heart diseases | |||||
| Male infants | |||||
| Cases (%) | 34 (1.73) | 144 (1.22) | 206 (1.05) | 82 (1.39) | 17 (1.86) |
| Model 1, Crude OR (95% CI) | 1.654 (1.147–2.384) | 1.157 (0.934–1.434) | Reference | 1.326 (1.025–1.716) | 1.776 (1.078–2.926) |
| Model 2, Adjusted OR (95% CI)b | 1.615 (1.119–2.332) | 1.154 (0.931–1.430) | Reference | 1.317 (1.017–1.704) | 1.745 (1.058–2.877) |
| Female infants | |||||
| Cases (%) | 35 (1.85) | 167 (1.47) | 279 (1.50) | 90 (1.62) | 14 (1.63) |
| Model 1, Crude OR (95% CI)a | 1.257 (0.869–1.762) | 0.983 (0.809–1.191) | Reference | 1.087 (0.852–1.374) | 1.125 (0.631–1.845) |
| Model 2, Adjusted OR (95% CI)a, b | 1.113 (0.934–1.327) | 0.988 (0.897–1.087) | Reference | 1.041 (0.925–1.173) | 1.062 (0.815–1.383) |
| Arrhythmia | |||||
| Male infants | |||||
| Cases (%) | 0 (0.00) | 13 (0.11) | 15 (0.08) | 9 (0.15) | 2 (0.22) |
| Model 1, Crude OR (95% CI)a | 0.321 (0.003–2.379) | 1.440 (0.684–2.994) | Reference | 2.036 (0.874–4.500) | 3.447 (0.682–11.141) |
| Model 2, Adjusted OR (95% CI)a, b | 0.558 (0.169–1.947) | 1.190 (0.855–1.656) | Reference | 1.427 (0.988–2.059) | 1.840 (0.999–3.387) |
| Female infants | |||||
| Cases (%) | 3 (0.16) | 12 (0.11) | 19 (0.10) | 8 (0.14) | 3 (0.35) |
| Model 1, Crude OR (95% CI)a | 1.771 (0.469–4.912) | 1.052 (0.504–2.117) | Reference | 1.462 (0.618–3.172) | 3.897 (1.031–10.823) |
| Model 2, Adjusted OR (95% CI)a, b | 1.394 (0.833–2.333) | 1.056 (0.763–1.462) | Reference | 1.171 (0.808–1.698) | 1.788 (1.047–3.052) |
| Urinary system (CAKUT) | |||||
| Male infants | |||||
| Cases (%) | 8 (0.41) | 51 (0.43) | 102 (0.52) | 31 (0.53) | 12 (1.31) |
| Model 1, Crude OR (95% CI) | 0.780 (0.379–1.603) | 0.826 (0.589–1.156) | Reference | 1.009 (0.674–1.510) | 2.532 (1.387–4.622) |
| Model 2, Adjusted OR (95% CI)b | 0.808 (0.392–1.664) | 0.837 (0.597–1.173) | Reference | 0.996 (0.665–1.491) | 2.470 (1.350–4.517) |
| Female infants | |||||
| Cases (%) | 9 (0.48) | 15 (0.13) | 33 (0.18) | 8 (0.14) | 2 (0.23) |
| Model 1, Crude OR (95% CI)a | 2.805 (1.287–5.547) | 0.759 (0.404–1.362) | Reference | 0.850 (0.374–1.723) | 1.617 (0.330–4.845) |
| Model 2, Adjusted OR (95% CI)a, b | 1.619 (1.154–2.273) | 0.860 (0.647–1.141) | Reference | 0.926 (0.649–1.321) | 1.267 (0.691–2.322) |
| Musculoskeletal system | |||||
| Limbs | |||||
| Male infants | |||||
| Cases (%) | 1 (0.05) | 46 (0.39) | 56 (0.29) | 16 (0.27) | 4 (0.44) |
| Model 1, Crude OR (95% CI) | 0.178 (0.025–1.281) | 1.359 (0.919–2.009) | Reference | 0.948 (0.544–1.654) | 1.527 (0.553–4.221) |
| Model 2, Adjusted OR (95% CI)b | 0.176 (0.024–1.270) | 1.354 (0.915–2.003) | Reference | 0.922 (0.528–1.609) | 1.514 (0.547–4.194) |
| Female infants | |||||
| Cases (%) | 3 (0.16) | 29 (0.26) | 49 (0.26) | 13 (0.23) | 4 (0.47) |
| Model 1, Crude OR (95% CI)a | 0.696 (0.191–1.791) | 0.978 (0.613–1.533) | Reference | 0.914 (0.481–1.621) | 1.974 (0.642–4.658) |
| Model 2, Adjusted OR (95% CI)a, b | 0.822 (0.491–1.375) | 0.981 (0.788–1.221) | Reference | 0.960 (0.719–1.281) | 1.404 (0.882–2.233) |
| Skin | |||||
| Angioma | |||||
| Male infants | |||||
| Cases (%) | 16 (0.82) | 72 (0.61) | 99 (0.51) | 35 (0.59) | 5 (0.55) |
| Model 1, Crude OR (95% CI)a | 1.655 (0.946–2.713) | 1.205 (0.887–1.630) | Reference | 1.186 (0.797–1.723) | 1.180 (0.439–2.540) |
| Model 2, Adjusted OR (95% CI)b | 1.292 (0.999–1.670) | 1.101 (0.948–1.278) | Reference | 1.082 (0.896–1.307) | 1.082 (0.709–1.651) |
| Female infants | |||||
| Cases (%) | 27 (1.43) | 100 (0.88) | 187 (1.00) | 52 (0.94) | 7 (0.81) |
| Model 1, Crude OR (95% CI)a | 1.452 (0.979–2.134) | 0.878 (0.686–1.118) | Reference | 0.938 (0.683–1.266) | 0.864 (0.379–1.675) |
| Model 2, Adjusted OR (95% CI)a, b | 1.196 (0.980–1.461) | 0.939 (0.832–1.059) | Reference | 0.963 (0.827–1.122) | 0.914 (0.636–1.314) |
| Inguinal hernia | |||||
| Male infants | |||||
| Cases (%) | 23 (1.17) | 56 (0.47) | 106 (0.54) | 30 (0.51) | 9 (0.98) |
| Model 1, Crude OR (95% CI)a | 2.209 (1.378–3.397) | 0.876 (0.630–1.205) | Reference | 0.950 (0.624–1.404) | 1.912 (0.916–3.530) |
| Model 2, Adjusted OR (95% CI)a, b | 1.484 (1.189–1.851) | 0.938 (0.800–1.099) | Reference | 0.972 (0.798–1.186) | 1.373 (0.989–1.907) |
| Female infants | |||||
| Cases (%) | 8 (0.42) | 50 (0.44) | 69 (0.37) | 29 (0.52) | 2 (0.23) |
| Model 1, Crude OR (95% CI)a | 1.207 (0.548–2.326) | 1.193 (0.826–1.711) | Reference | 1.425 (0.912–2.171) | 0.778 (0.161–2.252) |
| Model 2, Adjusted OR (95% CI)a, b | 1.092 (0.772–1.543) | 1.091 (0.914–1.302) | Reference | 1.195 (0.968–1.475) | 0.877 (0.474–1.622) |
| a Firth logistic regression model was applied. b Adjusted for maternal age at the MT1 questionnaire, pre-pregnancy BMI, conception method, parity (primipara or not), history of mental illness, history of kidney disease, history of congenital heart disease, history of uterine malformation and/or urogenital malformation, smoking status, alcohol consumption, marital status, education level, annual income, use of any drug before 12 weeks of gestation (methimazole, SSRI, antidepressant drug except for SSRI, antianxiety, sleeping pill, antipsychotic, valproic acid, antiepileptic except for valproic acid, lithium carbonate, and other psychoactive drug), use of folic acid supplement at <12 weeks of gestation, and HbA1c level at <24 weeks of gestation. Abbreviations: BMI, body mass index; CAKUT, congenital anomalies of the kidney and urinary tract; CI, confidence interval; HbA1c, glycosylated haemoglobin; OR, odds ratio; SSRI, selective serotonin reuptake inhibitor. | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



