
Submitted:
29 January 2024
Posted:
02 February 2024
You are already at the latest version
Abstract
Although there is a vast body of neuroscientific research on cognitive behavioral therapy (CBT), many therapists are confused about how to incorporate the evidence into their clinical practice. This narrative review translates neuroscientific research on CBT for depression into a therapist-friendly formulation model. Four brain networks that are particularly relevant to depression, including the Central Executive Network, Default mode Network, Salience Network, and Affective Network, were identified based on their interactions and described in relation to depressive symptoms. Additionally, it clarified how each CBT technique works on a brain map. Assessment, intervention selection, and patient psychoeducation based on this model will facilitate the clinical application of neuroscience in CBT.
Keywords:
Depression
; Cognitive Behavioral Therapy
; Brain Network Model
; Formulation
1. Introduction
Cognitive behavioral therapy (CBT) has long been the cornerstone of psychotherapy for a wide range of psychological disorders, such as depression [1,2], anxiety disorders [3,4], insomnia [5,6], and pain [7]. The CBT focuses on identifying and modifying the maladaptive thought patterns and behaviors believed to underlie and perpetuate these conditions. However, the objectivity and reproducibility of these action processes based on psychological hypotheses are still in doubt [8]. How to resolve this issue is an ongoing discussion among experts in the fields of neuropsychiatry and clinical psychology [9,10,11].
Recently, a vast body of evidence has shown that the CBT functions in the brain. Meta-analysis has been employed to examine the cross-sectional neural effects of CBT in patients with various psychiatric disorders, including major depressive, anxiety, and eating disorders [10]. No significant changes have been found in the emotional task; however, cognitive-task functional magnetic resonance imaging shows that the activation of the left anterior cingulate gyrus, left middle frontal gyrus, and left cuneus decreases from pre-CBT to post-CBT. Additionally, the reviewed literature has found that the CBT-affected regions overlap in the central executive network (CEN), default mode network (DMN), and salience network (SN). Other meta-analyses and systematic reviews have shown that these regions are involved in neural effects and are predictors of CBT [12,13,14,15,16,17]. However, many CBT therapists fail to incorporate neuroscientific evidence into their practices. Although all aspects of the mind are generated by the brain, CBT therapists underestimate the relationship between the brain and the treatments they use. An overview of these neuroscientific studies is insufficient; we intend to translate this evidence into clinical practice.
1.1. What is available neuroscience integration for therapists?
An emerging trend in the integration of neuroscience into CBT practice is the incorporation of therapeutic techniques based on neuroscience principles [11]. Current studies indicate that the combination of the stimulation or modulation of specific brain regions, such as transcranial direct current stimulation (tDCS), transcranial magnetic stimulation (TMS), and neurofeedback, can enhance the efficacy of CBT [11]. The scope of this application varies, and a recent review has discussed the evidence for the effectiveness of CBT in combination with brain stimulation methods, such as tDCS and TMS, for addiction [18]. However, the practical application of such interventions has been hindered by cost considerations, which have limited widespread interest in clinical practice. Psychological therapists, particularly those delivering CBT outside medical settings and lacking training in advanced measurement techniques, may face substantial resistance to implementing these approaches.
Neurocounseling and neuroeducation can aid clinical activities with neuroevidence. Neurocounseling is defined as “the integration of neuroscience into the practice of counseling by teaching and illustrating the physiological underpinnings of many of our mental health concerns” [19]. This assistance extends beyond therapists to patients and others and is expected to reduce stigma and shame about their illnesses [20]. Additionally, neurological mechanisms can be associated with psychosocial issues, as shown in existing neuroscientific evidence, allowing the utilization of talk therapy to work with specific brain regions. Furthermore, neuroeducation is partially consistent with the definition of neurocounseling, which is strictly defined as “a didactic or experiential-based intervention that aims to reduce client distress and improve client outcome by helping clients understand the neurological processes underlying mental functioning” [21]. These two approaches have the greatest advantage of not requiring special equipment or training while incorporating neuroscience into the traditional counseling process. Therefore, even therapists without such resources can immediately apply neuroscience in their clinical practice. Educating individuals about the neurological basis of psychosocial issues can empower them to understand their conditions and treatment options. This may reduce hesitance to seek help and contribute to effective evidence-based interventions.
1.2. Our goals
Currently, the neurological evidence on cognitive-behavioral therapy is understood in terms of individual techniques. To significantly utilize the evidence in real-world practice, a comprehensive model is required to aid in case formulation, including assessment and treatment selection. Knowing how individual techniques integrate and relate to each other on the platform of the brain allows for flexibility in selecting and combining techniques for therapists. The primary aim of this narrative review is to provide an extensive overview of the neurological evidence, with a particular emphasis on brain imaging, for the application of CBT in the treatment of depression. Furthermore, this review proposes a comprehensive model for integrating neurological findings into the CBT practice. By elucidating the neurological mechanisms and their relationship with CBT techniques, this model aims to enhance the psychotherapeutic process, ultimately contributing to improved outcomes in individuals with depression.
2. Three-Core-Network Model for Depression
Specific brain lesions that engage in depression or depression-related behaviors have been found in various regions [22,23,24]. The current mainstream recognizes depression as a result of dysfunctional brain networks based on the interactions between anatomically distant brain regions [25,26]. Many reviews and studies have focused on three core networks, called the triple network model [27,28,29,30,31,32]. These consist of the CEN, DMN, and SN. It is well known in the field of depression, as well as in general cognitive science, that the interaction of these three networks contributes to various cognitive aspects of a human being [33,34]. The involvement of these networks in depression has already been described in the literature, as described above; therefore, this paper summarizes them to the extent that CBT therapists can easily share them with their patients.
The CEN, also called the frontoparietal network or cognitive control network, is responsible for cognitive/executive functions, such as goal-oriented action planning, active control of attention, cognitive flexibility, logical judgment, and decision-making. These are closely related to problem-solving and self-control skills in the context of CBT, i.e., skills related to adaptive cognitive-emotional control and active cognitive-behavioral control. As is known from the classical brain model of depression [35], reduced CEN activity has been consistently reported in patients with depression. The lateral prefrontal and lateral posterior parietal cortices are the central regions, and abnormal functional connectivity between these regions is strongly associated with severity, executive function, and diagnostic markers [36,37,38].
The DMN is a medial midline network that is activated in the resting state, with the medial prefrontal cortex and posterior cingulate cortex/precuneus as the central regions. These brain regions are involved in the processing of the self and contribute to introspection and autobiographical memory. DMN activity is stronger at rest in individuals with depression than in healthy individuals [39], suggesting that the DMN induces depression-specific states of introspection, such as rumination [40]. As self-recognition and rumination are frequent targets of CBT for depression, it is important to understand the involvement of the DMN in these symptoms. DMN activity often contrasts with that of the CEN. It is necessary to switch the CEN/DMN appropriately during on/off tasks [41]. Patients with difficulty performing tasks with the CEN are thought to have strong DMN activity and self-referential processes that interfere with task performance [42,43].
The SN detects salient stimuli and events to guide behavior. Within this central region, the insular cortex is responsible for switching between the CEN and DMN, whereas the dorsal anterior cingulate cortex is associated with monitoring and selecting behaviors [44]. In depression, the SN works with the affective network (AN) to enhance negative information processing and enforces adherence to self-referential processes through strong functional coupling with the DMN [45]. In particular, the transmission system from the DMN to the SN may underlie the negative bias observed in depression [46]. Therefore, the SN is the center of interactions between other networks, facilitating self-control [47]. Therapists can suspect SN lesions in patients with negative biases in emotion, attention, and memory as well as attention rigidity [48].
The CEN, DMN, and SN reflect self-control, self-related thoughts/memory, and passive attention/processing bias, respectively, in depression. It is important to understand these symptomatic concepts comprehensively and not independently. If your patients report that they are always caught up in negative thoughts and always focus on them but are not aware of other sources of information in the environment, you may be aware of the possibility that these three networks are interdependent and dysfunctional. This is because the brain of the patient keeps the SN overly attentive to DMN activity, and the persistent DMN activity interferes with the utilization of the CEN. The papers cited above and related reviews [27,49,50] provide readers with further insight into the relationship between the three networks and depression.
3. Extensions to the Four-Network Model
Depressed mood is a core symptom, and depression is referred to as a mood/affective disorder. Therefore, it is essential to incorporate the AN into the three-network model of depression. The first depression model that focuses on the interactions between brain networks comprises an AN [25]. A recent study comparing the neural effects of CBT and pharmacotherapy has evaluated the AN, as well as the CEN, DMN, and SN [51]. These four networks are recognized as fundamental components in modeling neuropathology and CBT mechanisms related to depression [52]. The AN is a complex network of brain regions responsible for processing and regulating emotions [53]. The key components include the amygdala, ventromedial prefrontal cortex, and orbitofrontal cortex. The AN is vital in shaping emotional responses, affective learning, and emotional regulation. Many researchers have reported that the AN in patients with depression often exhibits abnormalities in activity and connectivity, leading to a heightened experience of negative emotions and impaired emotional regulation [54,55]. The importance of the AN in relation to CBT for depression has been reported primarily in discussions on treatment responsiveness [56]. For example, both selective serotonin reuptake inhibitors and CBT reduce hyperarousal in the AN and SN in response to emotional stimuli, and the level of activity in these brain regions before treatment predicts the degree of improvement in symptoms [57]. Interestingly, the degree of enhancement in these brain regions did not necessarily match the extent of symptom improvement. Additionally, extreme AN overactivity is not successfully improved by CBT. Among patients with depression, non-responders to treatment exhibit high hyperactivity in the right amygdala before treatment [58]. Thus, many depression treatment guidelines recommend CBT for mild to moderate depression. Although the AN is a critical component in the success or failure of a treatment, direct improvement with CBT may be difficult to achieve. Therefore, CBT therapists should develop strategies based on an integrated model that includes the other three networks to effectively calm the AN or improve it indirectly through interactions with networks other than the AN.
Here, before incorporating the specific techniques of CBT into the model, I first consider how AN can be integrated into the three networks. The cross-inhibitory relationship between AN and CEN is well known; for emotional responses via bottom-up processing in AN, top-down processing occurs in the CEN (particularly on the left side) for cognitive reappraisal via processing works, and emotion is appropriately regulated [59,60]. Patients with depression exhibit both CEN hypoactivity and AN hyperactivity, making emotion regulation difficult [35,61,62]. The cooperative activation of the AN and SN during exposure to negative situations enhances the detection of negative stimuli and emotions and evokes a strong negative effect [63]. It has even been reported that functional connectivity between the AN and SN predicts a relapse of depression that has been in remission [64]. The relationship between the AN and DMN has been modeled as having low associations with the initial depression network models [25]. In the area of social cognitive science, there is an “extended social-affective default mode network” that adds AN regions, such as the amygdala and hippocampus, to the DMN [65]. It is primarily implicated in empathy based on self-reference in the DMN and emotional responses in the AN [66]. However, the association between DMN–AN interaction and depression remains unclear.
Based on these findings, a four-network model is proposed (Figure 1A). This chart can be used by therapists to obtain visual information regarding the interactions between networks. When neighboring networks oppose each other (or are independent), the health of an individual is good. Even if the AN responds temporarily to a negative situation, the CEN inhibits it, and the SN discourages it from looking for similar negative stimuli. As mentioned in Section 2, switching between the CEN and DMN according to the on/off task assists in appropriate cognitive activity. The SN is responsible for the switching; therefore, the excessive binding of the SN and DMN is not recommended [45,67]. Contrasting results have been observed in patients with depression (Figure 1B). The AN responsible for the core symptoms is overly aroused and invades other network areas to create an emotionally dominant state. This is also known as “amygdala hijacking” as an alert response to anxiety and fear. The collaboration between the AN and SN produces a cascade of negative moods and attention [63]. The CEN, which is supposed to stop that flare-up, is underpowered, and proper emotional regulation is lost [61]. Thereafter, the SN works with the DMN to increase attention to negative introspective thoughts and further interfere with CEN activity in task performance situations [42,43,68]. Therapists can use this model as a basis for assessing the brain state of a patient in correspondence with the characteristic symptoms of the patient.
4. Integration of Cognitive Behavioral Therapy Techniques into the Four-Network Model
A comprehensive model that elucidates how individual CBT techniques integrate and relate to each other within the brain framework can provide therapists with high flexibility in choosing and combining techniques for individual patients.
Many studies have summarized that CBT for depression improves the emotional regulation system of the CEN–AN. In particular, it improves the activity level of the CEN and its ability to regulate top-down processes [69,70]. These studies have implemented Beck’s cognitive therapy packages consisting of cognitive-behavioral techniques centered on cognitive reconstruction. In this technique, the anterior cingulate cortex (ACC) region leading from the CEN to the AN is considerably altered [12]. Surprisingly, the recovery of the ACC with respect to emotional regulation is a common neural mechanism in other psychotherapies, such as dynamics psychotherapy [13]. Given the functions of the CEN, it is expected that improved problem-solving skills will further bolster this network. Although few studies have been done, there is a recent report that problem-solving training improves the function of the DMN and the attention span of the CEN [71]. Furthermore, rumination-focused CBT, which targets repetitive negative thoughts, such as rumination, works specifically on the dorsolateral prefrontal cortex of the CEN [72,73]. Additionally, it appears to normalize connectivity between the CEN and DMN [73]. Behavioral activation, which supports increased reward-taking behavior, promotes improved regulation skills in the CEN when anticipating unpleasant outcomes [74] and metacognitive skills in the DMN region [75]. Additionally, this approach reduces the functional connectivity between the DMN and SN [45] and within the DMN [76,77]. Mindfulness-based CBT controls attention and promotes the appropriate disruption of self-referential processing. This reduces functional connectivity within the DMN more than behavioral activation [77], and the DMN is associated with long-term effects [78]. Rumination leads to a decrease in SN connectivity and improves sustained attention function [79]. In internetwork interactions, functional connectivity of the SN–DMN and SN–CEN has been shown to increase [80]. In other words, mindfulness interventions may enhance the switching between these networks through the SN function.
To address these findings, each CBT technique was placed in a four-network model (Figure 2). This model can serve as a roadmap for therapists, helping them make informed decisions regarding the most effective approaches for specific cases. When developing a treatment plan with a patient to gain control of rumination, we could discuss whether to (a) inhibit the DMN to decrease the occurrence of rumination, (b) engage the SN to facilitate a break from rumination, or (c) activate the CEN to successfully perform cognitive tasks as an alternative to rumination.
5. Utilizing the Four-Network Model beyond Cognitive Behavioral Therapy
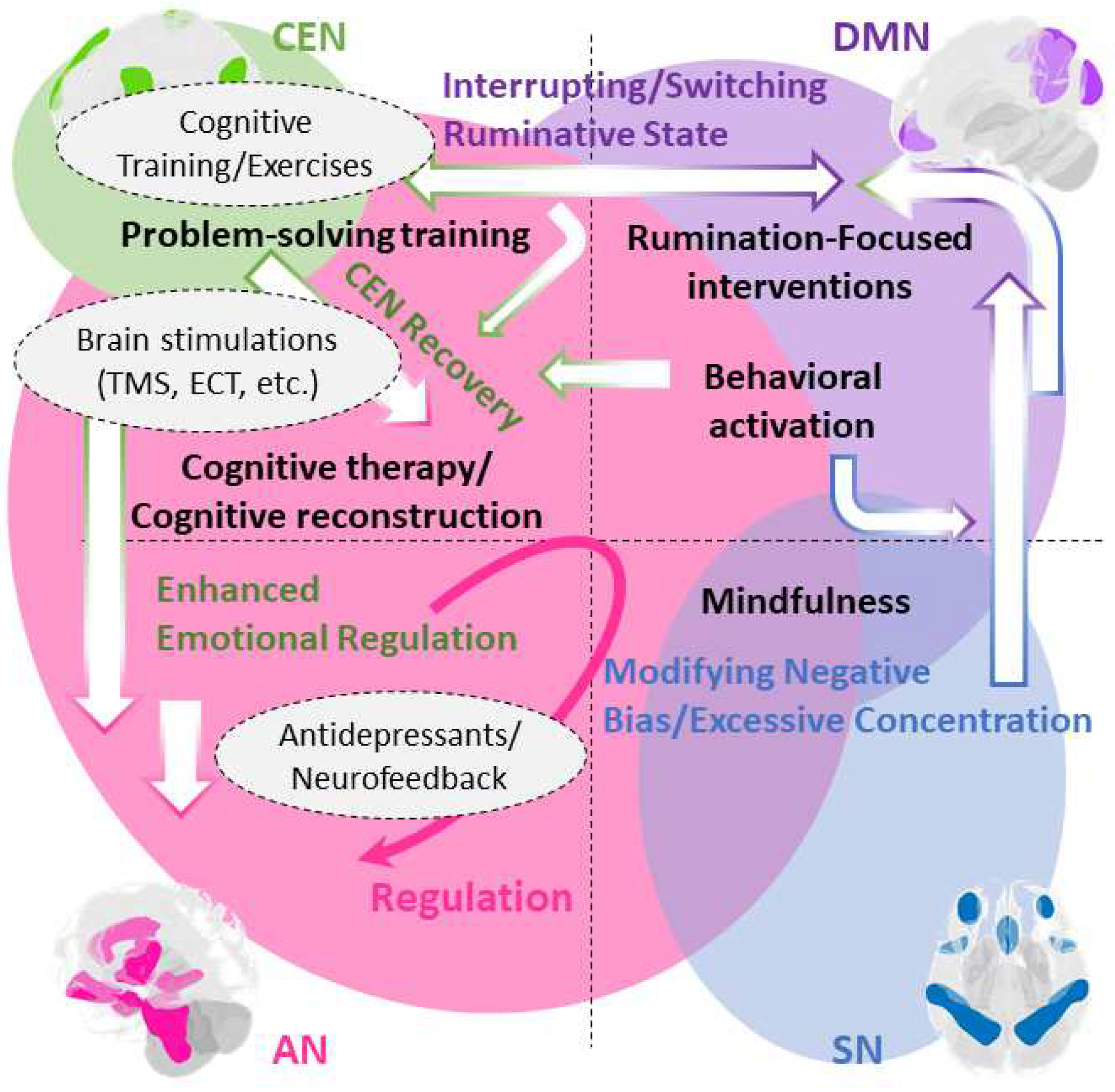
CBT therapists are typically unable to strategize how other specialty treatments, including pharmacotherapy and neurological modulation, can be linked to their treatment strategies. The four-network model can help facilitate their understanding and collaboration (Figure 3). Pharmacotherapy is considered for both acute and extreme AN activity. While this is a conventional guideline-based treatment, the CBT therapist can provide rich information to the patient about why the strategy is necessary using the brain model [81]. Antidepressants affect AN bottom-up responses and relatively broad networks, whereas CBT enhances top-down control, starting with the CEN [70,82]. Additionally, neurofeedback may be used to work on brain regions or networks where CBT has difficulty reaching to augment the neural effects of CBT. Many neurofeedback studies on depression have aimed to promote AN self-regulation [83]. This may be used in combination with the bottom-up therapeutic effects of the AN. Amygdala neurofeedback before CBT increases the concentration on positive thoughts and behaviors and results in high rates of long-term remission [56]. Additionally, patients and their therapists can consider incorporating exercises to stimulate the CEN before starting CBT. Brief cognitive tasks that use working memory [84] and verbal productive functions [85] can specifically stimulate these areas. A rich counseling technique for targeting specific brain regions has been consolidated [20]. Many brain stimulation therapies (neuromodulation), such as TMS, have the potential for antidepressant effects via the CEN [86]. For patients receiving multiple treatments, the integration of each treatment action into a four-network model is educational.
6. Conclusions
This narrative review attempts to bridge the gap between the psychological foundations of CBT and emerging neuroscientific evidence. By providing a deep understanding of the neurological underpinnings of CBT, we aspire to pave the way for an effective and evidence-based approach to the treatment of depression and other related conditions within the domains of neuropsychiatry and clinical psychology. Thus, this paper highlights the connections between neurocounseling and neuroeducation, which are more practical than the neuromodulation treatments that have already been discussed. Many CBT therapists are aware of the growing body of neuroscientific evidence; however, they are unsure of how to utilize it in real clinical situations. This study presents a visual compass to guide therapists as they navigate an uncharted brain ocean.
Funding
This research was funded by the JSPS (grant number 21K13727).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this study.
Acknowledgments
I would like to thank Editage (www.editage.jp) for English language editing.
Conflicts of Interest
The author declares no conflict of interest.
Abbreviations
CBT: Cognitive Behavioral Therapy
CEN: Central Executive Network
DMN: Default Mode Network
SN: Salience Network
tDCS: transcranial Direct Current Stimulation
TMS: Transcranial Magnetic Stimulation
AN: Affective Network
ACC: Anterior Cingulate Cortex
References
- Cuijpers, P.; Karyotaki, E.; Weitz, E.; Andersson, G.; Hollon, S.D.; Van Straten, A. The Effects of Psychotherapies for Major Depression in Adults on Remission, Recovery and Improvement: A Meta-Analysis. J. Affect. Disord. 2014, 159, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Berking, M.; Andersson, G.; Quigley, L.; Kleiboer, A.; Dobson, K.S. A Meta-Analysis of Cognitive-Behavioural Therapy for Adult Depression, Alone and in Comparison with Other Treatments. Can. J. Psychiatry 2013, 58, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Papola, D.; Ostuzzi, G.; Tedeschi, F.; Gastaldon, C.; Purgato, M.; Del Giovane, C.; Pompoli, A.; Pauley, D.; Karyotaki, E.; Sijbrandij, M.; et al. Comparative Efficacy and Acceptability of Psychotherapies for Panic Disorder with or without Agoraphobia: Systematic Review and Network Meta-Analysis of Randomised Controlled Trials. Br. J. Psychiatry 2022, 221, 507–519. [Google Scholar] [CrossRef]
- Cuijpers, P.; Cristea, I.A.; Karyotaki, E.; Reijnders, M.; Huibers, M.J.H.H. How Effective Are Cognitive Behavior Therapies for Major Depression and Anxiety Disorders? A Meta-Analytic Update of the Evidence. World Psychiatry 2016, 15, 245–258. [Google Scholar] [CrossRef]
- Trauer, J.M.; Qian, M.Y.; Doyle, J.S.; Rajaratnam, S.M.W.; Cunnington, D. Cognitive Behavioral Therapy for Chronic Insomnia. Ann. Intern. Med. 2015, 163, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Hertenstein, E.; Trinca, E.; Wunderlin, M.; Schneider, C.L.; Züst, M.A.; Fehér, K.D.; Su, T.; Straten, A. v.; Berger, T.; Baglioni, C.; et al. Cognitive Behavioral Therapy for Insomnia in Patients with Mental Disorders and Comorbid Insomnia: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2022, 62, 101597. [Google Scholar] [CrossRef]
- Williams, A.C. de C.; Fisher, E.; Hearn, L.; Eccleston, C. Psychological Therapies for the Management of Chronic Pain (Excluding Headache) in Adults. Cochrane database Syst. Rev. 2020, 8, CD007407. [Google Scholar] [CrossRef]
- Leichsenring, F.; Steinert, C. Is Cognitive Behavioral Therapy the Gold Standard for Psychotherapy? The Need for Plurality in Treatment and Research. JAMA - J. Am. Med. Assoc. 2017, 318, 1323–1324. [Google Scholar] [CrossRef]
- Salzano, S.; Zappullo, I.; Baiano, C.; Conson, M. The Integrated Neuropsychological Therapy: A Psychotherapy Model Tying Neuropsychology and Cognitive Behavioral Therapy. J. Cogn. Psychother. 2023, JCP-2021-0020.R1. [CrossRef]
- Yuan, S.; Wu, H.; Wu, Y.; Xu, H.; Yu, J.; Zhong, Y.; Zhang, N.; Li, J.; Xu, Q.; Wang, C. Neural Effects of Cognitive Behavioral Therapy in Psychiatric Disorders: A Systematic Review and Activation Likelihood Estimation Meta-Analysis. Front. Psychol. 2022, 13. [Google Scholar] [CrossRef]
- Månsson, K.N.T.; Lueken, U.; Frick, A. Enriching CBT by Neuroscience: Novel Avenues to Achieve Personalized Treatments. Int. J. Cogn. Ther. 2021, 14, 182–195. [Google Scholar] [CrossRef]
- Franklin, G.; Carson, A.J.; Welch, K. a. Cognitive Behavioural Therapy for Depression: Systematic Review of Imaging Studies. Acta Neuropsychiatr. 2015, 1–14. [Google Scholar] [CrossRef]
- Sankar, A.; Melin, A.; Lorenzetti, V.; Horton, P.; Costafreda, S.G.; Fu, C.H.Y. A Systematic Review and Meta-Analysis of the Neural Correlates of Psychological Therapies in Major Depression. Psychiatry Res. Neuroimaging 2018, 279, 31–39. [Google Scholar] [CrossRef]
- Picó-Pérez, M.; Fullana, M.A.; Albajes-Eizagirre, A.; Vega, D.; Marco-Pallarés, J.; Vilar, A.; Chamorro, J.; Felmingham, K.L.; Harrison, B.J.; Radua, J.; et al. Neural Predictors of Cognitive-Behavior Therapy Outcome in Anxiety-Related Disorders: A Meta-Analysis of Task-Based FMRI Studies. Psychol. Med. 2023, 53, 3387–3395. [Google Scholar] [CrossRef]
- Cohen, S.E.; Zantvoord, J.B.; Wezenberg, B.N.; Bockting, C.L.H.; van Wingen, G.A. Magnetic Resonance Imaging for Individual Prediction of Treatment Response in Major Depressive Disorder: A Systematic Review and Meta-Analysis. Transl. Psychiatry 2021, 11, 168. [Google Scholar] [CrossRef] [PubMed]
- Strege, M. V; Siegle, G.J.; Richey, J.A.; Krawczak, R.A.; Young, K. Cingulate Prediction of Response to Antidepressant and Cognitive Behavioral Therapies for Depression: Meta-Analysis and Empirical Application. Brain Imaging Behav. 2023, 17, 450–460. [Google Scholar] [CrossRef] [PubMed]
- Kalin, N.H. Insights and Advances Into Treatments for Major Depression. Am. J. Psychiatry 2023, 180, 173–176. [Google Scholar] [CrossRef]
- Perrotta, D.; Perri, R.L. Mini-Review: When Neurostimulation Joins Cognitive-Behavioral Therapy. On the Need of Combining Evidence-Based Treatments for Addiction Disorders. Neurosci. Lett. 2022, 777, 136588. [Google Scholar] [CrossRef] [PubMed]
- Russell-Chapin, L.A. Integrating Neurocounseling into the Counseling Profession: An Introduction. J. Ment. Heal. Couns. 2016, 38, 93–102. [Google Scholar] [CrossRef]
- Russell-Chapin, L.A.; Pacheco, N.C.; DeFord, J.A. Practical Neurocounseling; Russell-Chapin, L., Pacheco, N., DeFord, J., Eds.; Routledge: New York, 2020; ISBN 9780367824402. [Google Scholar]
- Miller, R. Neuroeducation: Integrating Brain-Based Psychoeducation into Clinical Practice. J. Ment. Heal. Couns. 2016, 38, 103–115. [Google Scholar] [CrossRef]
- Nawaz, H.; Shah, I.; Ali, S. The Amygdala Connectivity with Depression and Suicide Ideation with Suicide Behavior: A Meta-Analysis of Structural MRI, Resting-State FMRI and Task FMRI. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2023, 124, 110736. [Google Scholar] [CrossRef]
- Bondi, E.; Maggioni, E.; Brambilla, P.; Delvecchio, G. A Systematic Review on the Potential Use of Machine Learning to Classify Major Depressive Disorder from Healthy Controls Using Resting State FMRI Measures. Neurosci. Biobehav. Rev. 2023, 144, 104972. [Google Scholar] [CrossRef]
- Kotoula, V.; Evans, J.W.; Punturieri, C.; Johnson, S.C.; Zarate, C.A. Functional MRI Markers for Treatment-Resistant Depression: Insights and Challenges. In Progress in brain research; Netherlands, 2023; 278, 117–148. [CrossRef]
- Kaiser, R.H.; Andrews-Hanna, J.R.; Wager, T.D.; Pizzagalli, D.A. Large-Scale Network Dysfunction in Major Depressive Disorder: A Meta-Analysis of Resting-State Functional Connectivity. JAMA psychiatry 2015, 72, 603–611. [Google Scholar] [CrossRef]
- Korgaonkar, M.S.; Goldstein-Piekarski, A.N.; Fornito, A.; Williams, L.M. Intrinsic Connectomes Are a Predictive Biomarker of Remission in Major Depressive Disorder. Mol. Psychiatry 2020, 25, 1537–1549. [Google Scholar] [CrossRef]
- Balogh, L.; Tanaka, M.; Török, N.; Vécsei, L.; Taguchi, S. Crosstalk between Existential Phenomenological Psychotherapy and Neurological Sciences in Mood and Anxiety Disorders. Biomedicines 2021, 9, 340. [Google Scholar] [CrossRef]
- Young, I.M.; Dadario, N.B.; Tanglay, O.; Chen, E.; Cook, B.; Taylor, H.M.; Crawford, L.; Yeung, J.T.; Nicholas, P.J.; Doyen, S.; et al. Connectivity Model of the Anatomic Substrates and Network Abnormalities in Major Depressive Disorder: A Coordinate Meta-Analysis of Resting-State Functional Connectivity. J. Affect. Disord. Reports 2023, 11, 100478. [Google Scholar] [CrossRef]
- Bertocci, M.A.; Afriyie-Agyemang, Y.; Rozovsky, R.; Iyengar, S.; Stiffler, R.; Aslam, H.A.; Bebko, G.; Phillips, M.L. Altered Patterns of Central Executive, Default Mode and Salience Network Activity and Connectivity Are Associated with Current and Future Depression Risk in Two Independent Young Adult Samples. Mol. Psychiatry 2023, 28, 1046–1056. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, Y.; Wu, X.; Huang, H.; Jia, Y.; Zhong, S.; Wu, X.; Zhao, L.; He, Y.; Huang, L.; et al. Shared and Specific Functional Connectivity Alterations in Unmedicated Bipolar and Major Depressive Disorders Based on the Triple-Network Model. Brain Imaging Behav. 2020, 14, 186–199. [Google Scholar] [CrossRef]
- Li, J.; Liu, J.; Zhong, Y.; Wang, H.; Yan, B.; Zheng, K.; Wei, L.; Lu, H.; Li, B. Causal Interactions Between the Default Mode Network and Central Executive Network in Patients with Major Depression. Neuroscience 2021, 475, 93–102. [Google Scholar] [CrossRef]
- Wang, Q.; Tian, S.; Zhao, P.; Cao, Q.; Lu, Q.; Yao, Z. Association Between Antidepressant Efficacy and Interactions of Three Core Depression-Related Brain Networks in Major Depressive Disorder. Front. Psychiatry 2022, 13. [Google Scholar] [CrossRef]
- Menon, V. Large-Scale Brain Networks and Psychopathology: A Unifying Triple Network Model. Trends Cogn. Sci. 2011, 15, 483–506. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Zhang, S.; Yin, S.; Ren, W.; He, R.; Li, J. The Fronto-Insular Cortex Causally Mediates the Default-Mode and Central-Executive Networks to Contribute to Individual Cognitive Performance in Healthy Elderly. Hum. Brain Mapp. 2018, 39, 4302–4311. [Google Scholar] [CrossRef]
- Mayberg, S. Limbic-Cortical Dysregulation: Depression. J. Neuropsychiatr. 1997, 9, 471–481. [Google Scholar] [CrossRef]
- Baker, J.T.; Dillon, D.G.; Patrick, L.M.; Roffman, J.L.; Brady, R.O.; Pizzagalli, D.A.; Öngür, D.; Holmes, A.J. Functional Connectomics of Affective and Psychotic Pathology. Proc. Natl. Acad. Sci. 2019, 116, 9050–9059. [Google Scholar] [CrossRef] [PubMed]
- Dahl, C.J.; Wilson-Mendenhall, C.D.; Davidson, R.J. The Plasticity of Well-Being: A Training-Based Framework for the Cultivation of Human Flourishing. Proc. Natl. Acad. Sci. 2020, 117, 32197–32206. [Google Scholar] [CrossRef] [PubMed]
- Pan, F.; Xu, Y.; Zhou, W.; Chen, J.; Wei, N.; Lu, S.; Shang, D.; Wang, J.; Huang, M. Disrupted Intrinsic Functional Connectivity of the Cognitive Control Network Underlies Disease Severity and Executive Dysfunction in First-Episode, Treatment-Naive Adolescent Depression. J. Affect. Disord. 2020, 264, 455–463. [Google Scholar] [CrossRef]
- Sundermann, B.; Beverborg, M.O. lütke; Pfleiderer, B. Meta-Analysis of Resting-State FMRI in Depression: Generating Spatial Hypotheses for Potential Clinical Applications. PeerJ Prepr. 2014, 1–25. [CrossRef]
- Zhou, H.-X.; Chen, X.; Shen, Y.-Q.; Li, L.; Chen, N.-X.; Zhu, Z.-C.; Castellanos, F.X.; Yan, C.-G. Rumination and the Default Mode Network: Meta-Analysis of Brain Imaging Studies and Implications for Depression. Neuroimage 2020, 206, 116287. [Google Scholar] [CrossRef]
- Sridharan, D.; Levitin, D.J.; Menon, V. A Critical Role for the Right Fronto-Insular Cortex in Switching between Central-Executive and Default-Mode Networks. Proc. Natl. Acad. Sci. 2008, 105, 12569–12574. [Google Scholar] [CrossRef]
- Manoliu, A.; Meng, C.; Brandl, F.; Doll, A.; Tahmasian, M.; Scherr, M.; Schwerthöffer, D.; Zimmer, C.; Förstl, H.; Bäuml, J.; et al. Insular Dysfunction within the Salience Network Is Associated with Severity of Symptoms and Aberrant Inter-Network Connectivity in Major Depressive Disorder. Front. Hum. Neurosci. 2013, 7, 930. [Google Scholar] [CrossRef]
- Hugdahl, K.; Kazimierczak, K.; Beresniewicz, J.; Kompus, K.; Westerhausen, R.; Ersland, L.; Grüner, R.; Specht, K. Dynamic Up- and down-Regulation of the Default (DMN) and Extrinsic (EMN) Mode Networks during Alternating Task-on and Task-off Periods. PLoS One 2019, 14, e0218358. [Google Scholar] [CrossRef]
- Menon, V.; Uddin, L.Q. Saliency, Switching, Attention and Control: A Network Model of Insula Function. Brain Struct. Funct. 2010, 1–13. [Google Scholar] [CrossRef]
- Yokoyama, S.; Okamoto, Y.; Takagaki, K.; Okada, G.; Takamura, M.; Mori, A.; Shiota, S.; Ichikawa, N.; Jinnin, R.; Yamawaki, S. Effects of Behavioral Activation on Default Mode Network Connectivity in Subthreshold Depression: A Preliminary Resting-State FMRI Study. J. Affect. Disord. 2018, 227, 156–163. [Google Scholar] [CrossRef]
- Guha, A.; Yee, C.M.; Heller, W.; Miller, G.A. Alterations in the Default Mode-Salience Network Circuit Provide a Potential Mechanism Supporting Negativity Bias in Depression. Psychophysiology 2021, 58. [Google Scholar] [CrossRef] [PubMed]
- Krönke, K.-M.; Wolff, M.; Shi, Y.; Kräplin, A.; Smolka, M.N.; Bühringer, G.; Goschke, T. Functional Connectivity in a Triple-Network Saliency Model Is Associated with Real-Life Self-Control. Neuropsychologia 2020, 149, 107667. [Google Scholar] [CrossRef] [PubMed]
- Malejko, K.; Brown, R.C.; Plener, P.L.; Bonenberger, M.; Graf, H.; Abler, B. Differential Neural Processing of Unpleasant Sensory Stimulation in Patients with Major Depression. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Macêdo, M.A.; Sato, J.R.; Bressan, R.A.; Pan, P.M. Adolescent Depression and Resting-State FMRI Brain Networks: A Scoping Review of Longitudinal Studies. Brazilian J. Psychiatry 2022. [Google Scholar] [CrossRef] [PubMed]
- Schimmelpfennig, J.; Topczewski, J.; Zajkowski, W.; Jankowiak-Siuda, K. The Role of the Salience Network in Cognitive and Affective Deficits. Front. Hum. Neurosci. 2023, 17. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, B.; Cha, J.; Choi, K.; Nemeroff, C.; Craighead, W.E.; Mayberg, H. Changes in Functional Connectivity in Remitters to CBT Versus Pharmacotherapy for Depression. Biol. Psychiatry 2022, 91, S51–S52. [Google Scholar] [CrossRef]
- Sun, J.; Ma, Y.; Guo, C.; Du, Z.; Chen, L.; Wang, Z.; Li, X.; Xu, K.; Luo, Y.; Hong, Y.; et al. Distinct Patterns of Functional Brain Network Integration between Treatment-Resistant Depression and Non Treatment-Resistant Depression: A Resting-State Functional Magnetic Resonance Imaging Study. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2023, 120, 110621. [Google Scholar] [CrossRef]
- Bush, G.; Luu, P.; Posner, M.I. Cognitive and Emotional Influences in Anterior Cingulate Cortex. Trends Cogn. Sci. 2000, 4, 215–222. [Google Scholar] [CrossRef]
- Johnstone, T.; van Reekum, C.M.; Urry, H.L.; Kalin, N.H.; Davidson, R.J. Failure to Regulate: Counterproductive Recruitment of Top-Down Prefrontal-Subcortical Circuitry in Major Depression. J. Neurosci. 2007, 27, 8877–8884. [Google Scholar] [CrossRef]
- Zhang, X.; Zhu, X.; Wang, X.; Zhu, X.; Zhong, M.; Yi, J.; Rao, H.; Yao, S. First-Episode Medication-Naive Major Depressive Disorder Is Associated with Altered Resting Brain Function in the Affective Network. PLoS One 2014, 9, e85241. [Google Scholar] [CrossRef]
- Compère, L.; Siegle, G.J.; Riley, E.; Lazzaro, S.; Strege, M.; Pacoe, E.; Canovali, G.; Barb, S.; Huppert, T.; Young, K. Enhanced Efficacy of CBT Following Augmentation with Amygdala RtfMRI Neurofeedback in Depression. J. Affect. Disord. 2023, 339, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Gorka, S.M.; Young, C.B.; Klumpp, H.; Kennedy, A.E.; Francis, J.; Ajilore, O.; Langenecker, S.A.; Shankman, S.A.; Craske, M.G.; Stein, M.B.; et al. Emotion-Based Brain Mechanisms and Predictors for SSRI and CBT Treatment of Anxiety and Depression: A Randomized Trial. Neuropsychopharmacology 2019, 44, 1639–1648. [Google Scholar] [CrossRef] [PubMed]
- Doerig, N.; Krieger, T.; Altenstein, D.; Schlumpf, Y.; Spinelli, S.; Späti, J.; Brakowski, J.; Quednow, B.B.; Seifritz, E.; Holtforth, M. grosse Amygdala Response to Self-Critical Stimuli and Symptom Improvement in Psychotherapy for Depression. Br. J. Psychiatry 2016, 208, 175–181. [Google Scholar] [CrossRef]
- Rive, M.M.; van Rooijen, G.; Veltman, D.J.; .Phillips, M.L.; Schene, A.H.; Ruhé, H.G. Neural Correlates of Dysfunctional Emotion Regulation in Major Depressive Disorder. A Systematic Review of Neuroimaging Studies. Neurosci. Biobehav. Rev. 2013, 37, 2529–2553. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Ferguson, M.A.; Grafman, J.; Cohen, A.L.; Fox, M.D. A Lesion-Derived Brain Network for Emotion Regulation. Biol. Psychiatry 2023, 94, 640–649. [Google Scholar] [CrossRef] [PubMed]
- Zilverstand, A.; Parvaz, M.A.; Goldstein, R.Z. Neuroimaging Cognitive Reappraisal in Clinical Populations to Define Neural Targets for Enhancing Emotion Regulation. A Systematic Review. Neuroimage 2017, 151, 105–116. [Google Scholar] [CrossRef]
- Siegle, G.J.; Steinhauer, S.R.; Thase, M.E.; Stenger, V.A.; Carter, C.S. Can’t Shake That Feeling: Event-Related FMRI Assessment of Sustained Amygdala Activity in Response to Emotional Information in Depressed Individuals. Biol. Psychiatry 2002, 51, 693–707. [Google Scholar] [CrossRef]
- Hamilton, J.P.; Etkin, A.; Furman, D.J.; Lemus, M.G.; Johnson, R.F.; Gotlib, I.H. Functional Neuroimaging of Major Depressive Disorder: A Meta-Analysis and New Integration of Baseline Activation and Neural Response Data. Am. J. Psychiatry 2012, 169, 693–703. [Google Scholar] [CrossRef]
- Dunlop, B.W.; Cha, J.; Choi, K.S.; Nemeroff, C.B.; Craighead, W.E.; Mayberg, H.S. Functional Connectivity of Salience and Affective Networks among Remitted Depressed Patients Predicts Episode Recurrence. Neuropsychopharmacology 2023, 48, 1901–1909. [Google Scholar] [CrossRef]
- Amft, M.; Bzdok, D.; Laird, A.R.; Fox, P.T.; Schilbach, L.; Eickhoff, S.B. Definition and Characterization of an Extended Social-Affective Default Network. Brain Struct. Funct. 2015, 220, 1031–1049. [Google Scholar] [CrossRef]
- Göttlich, M.; Ye, Z.; Rodriguez-Fornells, A.; Münte, T.F.; Krämer, U.M. Viewing Socio-Affective Stimuli Increases Connectivity within an Extended Default Mode Network. Neuroimage 2017, 148, 8–19. [Google Scholar] [CrossRef]
- Manoliu, A.; Riedl, V.; Zherdin, A.; Mühlau, M.; Schwerthöffer, D.; Scherr, M.; Peters, H.; Zimmer, C.; Förstl, H.; Bäuml, J.; et al. Aberrant Dependence of Default Mode/Central Executive Network Interactions on Anterior Insular Salience Network Activity in Schizophrenia. Schizophr. Bull. 2014, 40, 428–437. [Google Scholar] [CrossRef]
- Delaveau, P.; Arruda Sanchez, T.; Steffen, R.; Deschet, K.; Jabourian, M.; Perlbarg, V.; Gasparetto, E.L.; Dubal, S.; Costa e Silva, J.; Fossati, P. Default Mode and Task-positive Networks Connectivity during the N-Back Task in Remitted Depressed Patients with or without Emotional Residual Symptoms. Hum. Brain Mapp. 2017, 38, 3491–3501. [Google Scholar] [CrossRef]
- Marwood, L.; Wise, T.; Perkins, A.M.; Cleare, A.J. Meta-Analyses of the Neural Mechanisms and Predictors of Response to Psychotherapy in Depression and Anxiety. Neurosci. Biobehav. Rev. 2018, 95, 61–72. [Google Scholar] [CrossRef]
- DeRubeis, R.J.; Siegle, G.J.; Hollon, S.D. Cognitive Therapy vs. Medication for Depression: Treatment Outcomes and Neural Mechanisms. Nat. Rev. Neurosci. 2008, 9, 788–796. [Google Scholar] [CrossRef]
- Alescio-Lautier, B.; Chambon, C.; Deshayes, C.; Anton, J.-L.; Escoffier, G.; Ferrer, M.-H.; Paban, V. Problem-Solving Training Modifies Cognitive Functioning and Related Functional Connectivity in Healthy Adults. Neuropsychol. Rehabil. 2023, 33, 103–138. [Google Scholar] [CrossRef] [PubMed]
- Baeken, C.; Wu, G.-R.; Rogiers, R.; Remue, J.; Lemmens, G.M.; Raedt, R. De Cognitive Behavioral Based Group Psychotherapy Focusing on Repetitive Negative Thinking: Decreased Uncontrollability of Rumination Is Related to Brain Perfusion Increases in the Left Dorsolateral Prefrontal Cortex. J. Psychiatr. Res. 2021, 136, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, R.H.; Watkins, E.R.; Peters, A.T.; Feldhaus, C.G.; Barba, A.; Carbray, J.; Langenecker, S.A. Targeting Ruminative Thinking in Adolescents at Risk for Depressive Relapse: Rumination-Focused Cognitive Behavior Therapy in a Pilot Randomized Controlled Trial with Resting State FMRI. PLoS One 2016, 11, e0163952. [Google Scholar] [CrossRef] [PubMed]
- Mori, A.; Okamoto, Y.; Okada, G.; Takagaki, K.; Jinnin, R.; Takamura, M.; Kobayakawa, M.; Yamawaki, S. Behavioral Activation Can Normalize Neural Hypoactivation in Subthreshold Depression during a Monetary Incentive Delay Task. J. Affect. Disord. 2016, 189, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Shiota, S.; Okamoto, Y.; Okada, G.; Takagaki, K.; Takamura, M.; Mori, A.; Yokoyama, S.; Nishiyama, Y.; Jinnin, R.; Hashimoto, R.; et al. The Neural Correlates of the Metacognitive Function of Other Perspective: A Multiple Regression Analysis Study. Neuroreport 2017, 28. [Google Scholar] [CrossRef]
- Cernasov, P.; Walsh, E.C.; Kinard, J.L.; Kelley, L.; Phillips, R.; Pisoni, A.; Eisenlohr-Moul, T.A.; Arnold, M.; Lowery, S.C.; Ammirato, M.; et al. Multilevel Growth Curve Analyses of Behavioral Activation for Anhedonia (BATA) and Mindfulness-Based Cognitive Therapy Effects on Anhedonia and Resting-State Functional Connectivity: Interim Results of a Randomized Trial. J. Affect. Disord. 2021. [Google Scholar] [CrossRef]
- Cernasov, P.; Kinard, J.; Phillips, R.; Halverson, T.; Greene, R.; Arnold, M.; Lowery, S.; Luke, S.; Kelley, L.; McLamb, M.; et al. Mindfulness-Based Cognitive Therapy Attenuates Default-Mode Network Connectivity in Patients With Clinically Significant Anhedonia. Biol. Psychiatry 2020, 87, S197. [Google Scholar] [CrossRef]
- Bessette, K.L.; Jacobs, R.H.; Heleniak, C.; Peters, A.T.; Welsh, R.C.; Watkins, E.R.; Langenecker, S.A. Malleability of Rumination: An Exploratory Model of CBT-Based Plasticity and Long-Term Reduced Risk for Depressive Relapse among Youth from a Pilot Randomized Clinical Trial. PLoS One 2020, 15, e0233539. [Google Scholar] [CrossRef] [PubMed]
- van der Velden, A.M.; Scholl, J.; Elmholdt, E.-M.; Fjorback, L.O.; Harmer, C.J.; Lazar, S.W.; O’Toole, M.S.; Smallwood, J.; Roepstorff, A.; Kuyken, W. Mindfulness Training Changes Brain Dynamics During Depressive Rumination: A Randomized Controlled Trial. Biol. Psychiatry 2023, 93, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Bremer, B.; Wu, Q.; Mora Álvarez, M.G.; Hölzel, B.K.; Wilhelm, M.; Hell, E.; Tavacioglu, E.E.; Torske, A.; Koch, K. Mindfulness Meditation Increases Default Mode, Salience, and Central Executive Network Connectivity. Sci. Rep. 2022, 12, 13219. [Google Scholar] [CrossRef]
- Roiser, J.P.; Sahakian, B.J. Hot and Cold Cognition in Depression. CNS Spectr. 2013, 18, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, B.W.; Cha, J.; Choi, K.S.; Rajendra, J.K.; Nemeroff, C.B.; Craighead, W.E.; Mayberg, H.S. Shared and Unique Changes in Brain Connectivity Among Depressed Patients After Remission With Pharmacotherapy Versus Psychotherapy. Am. J. Psychiatry 2023, 180, 218–229. [Google Scholar] [CrossRef]
- Trambaiolli, L.R.; Kohl, S.H.; Linden, D.E.J.; Mehler, D.M.A. Neurofeedback Training in Major Depressive Disorder: A Systematic Review of Clinical Efficacy, Study Quality and Reporting Practices. Neurosci. Biobehav. Rev. 2021, 125, 33–56. [Google Scholar] [CrossRef]
- Barbey, A.K.; Koenigs, M.; Grafman, J. Dorsolateral Prefrontal Contributions to Human Working Memory. Cortex 2013, 49, 1195–1205. [Google Scholar] [CrossRef]
- Backes, H.; Dietsche, B.; Nagels, A.; Stratmann, M.; Konrad, C.; Kircher, T.; Krug, A. Increased Neural Activity during Overt and Continuous Semantic Verbal Fluency in Major Depression: Mainly a Failure to Deactivate. Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264, 631–645. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.J.; Hoy, K.E.; Daskalakis, Z.J.; Fitzgerald, P.B. Repetitive Transcranial Magnetic Stimulation for Treatment Resistant Depression: Re-Establishing Connections. Clin. Neurophysiol. 2016, 127, 3394–3405. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Four-network model and formulation of depression based on it. Solid double arrows represent bidirectional controlling/opposing relationships. Solid single arrows represent instructive effects. Dashed arrows connect independently or only when necessary. Double lines with circles represent excessive linkages/collaborative relationships. (A): All brain networks are well controlled. The boxed descriptions are functions for each network and each other. (B): Typical brain network for depression. CEN: Central executive network; DMN: Default mode network; AN: Affective Network; SN: Salience Network.
Figure 1.
Four-network model and formulation of depression based on it. Solid double arrows represent bidirectional controlling/opposing relationships. Solid single arrows represent instructive effects. Dashed arrows connect independently or only when necessary. Double lines with circles represent excessive linkages/collaborative relationships. (A): All brain networks are well controlled. The boxed descriptions are functions for each network and each other. (B): Typical brain network for depression. CEN: Central executive network; DMN: Default mode network; AN: Affective Network; SN: Salience Network.
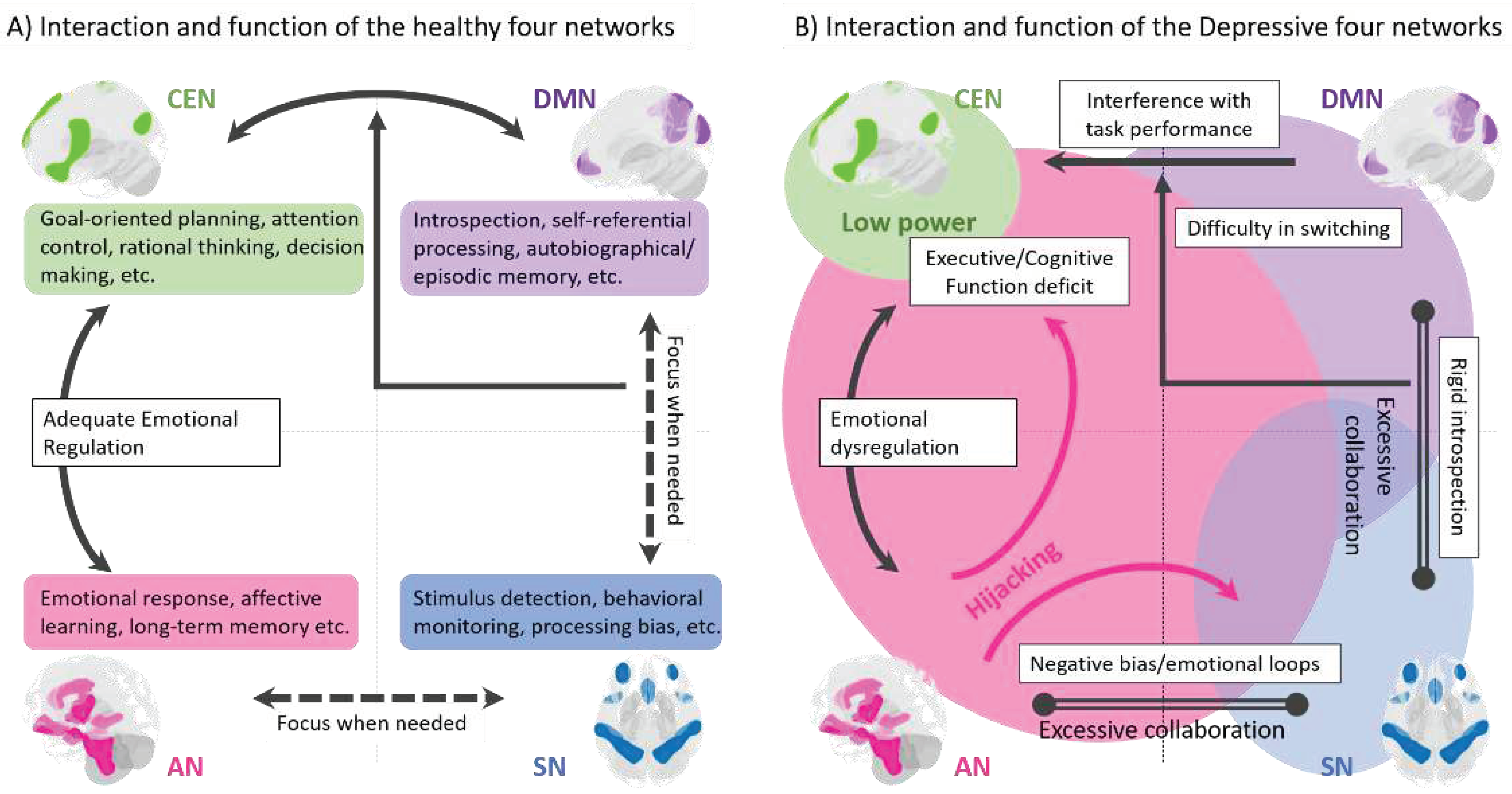
Figure 2.
Therapeutic action formulation of cognitive behavioral therapy (CBT) on a four-network model of depression. Each CBT technique, shown in bold, is arranged with respect to the brain network on which it acts. The arrows beside the techniques indicate the pathway of action of each treatment. CEN: Central executive network; DMN: Default mode network; AN: Affective Network; SN: Salience Network.
Figure 2.
Therapeutic action formulation of cognitive behavioral therapy (CBT) on a four-network model of depression. Each CBT technique, shown in bold, is arranged with respect to the brain network on which it acts. The arrows beside the techniques indicate the pathway of action of each treatment. CEN: Central executive network; DMN: Default mode network; AN: Affective Network; SN: Salience Network.
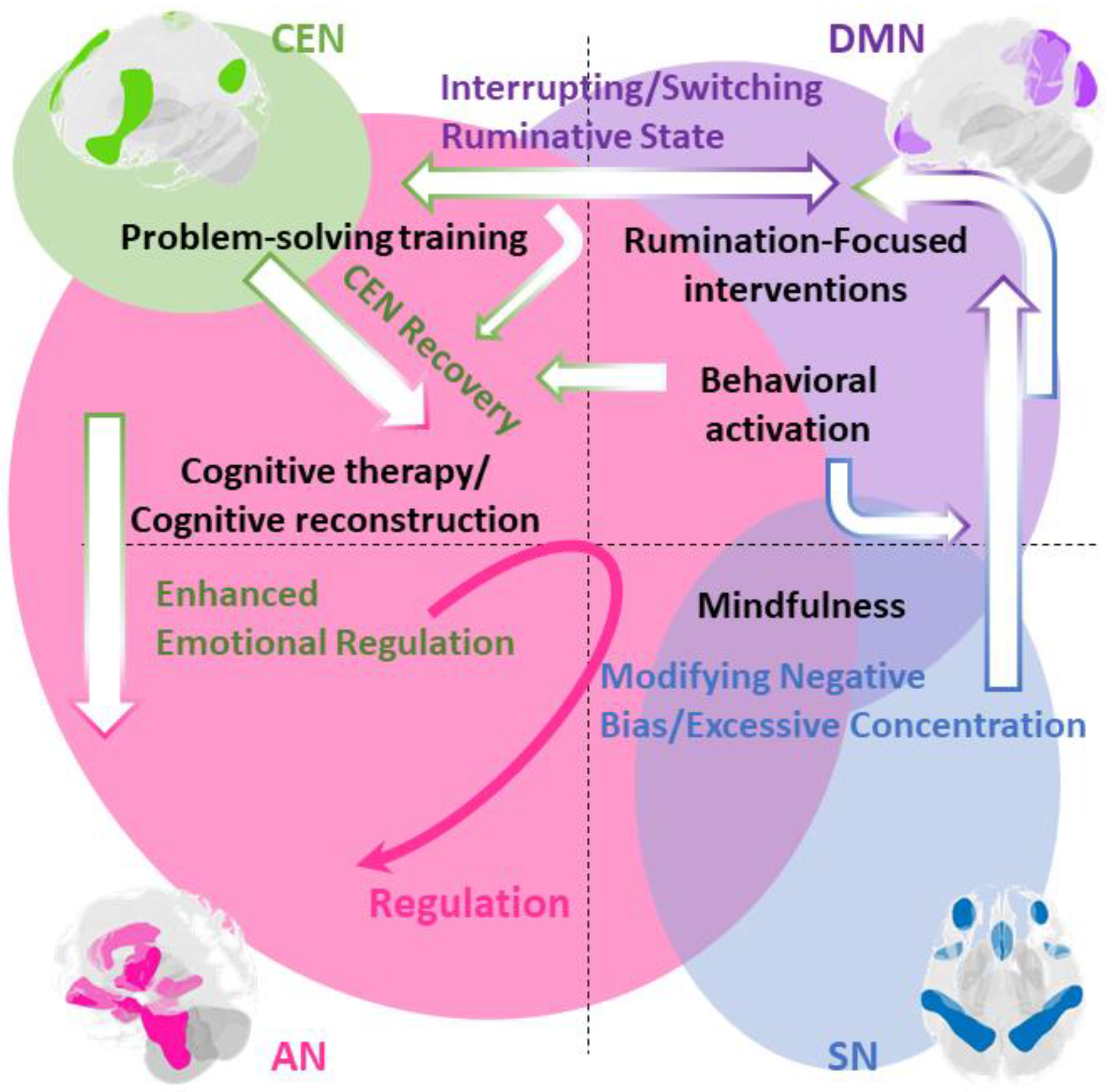
Figure 3.
Planning in conjunction with other treatments. Cognitive training and exercise promote the activation of the CEN. Brain stimulation therapies produce antidepressant effects on other networks via the CEN. Antidepressants and neurofeedback can selectively work on brain networks that CBT cannot reach. These can be deployed flexibly, according to the type of training and the brain region targeted. CEN: Central executive network; DMN: Default mode network; AN: Affective Network; SN: Salience Network.
Figure 3.
Planning in conjunction with other treatments. Cognitive training and exercise promote the activation of the CEN. Brain stimulation therapies produce antidepressant effects on other networks via the CEN. Antidepressants and neurofeedback can selectively work on brain networks that CBT cannot reach. These can be deployed flexibly, according to the type of training and the brain region targeted. CEN: Central executive network; DMN: Default mode network; AN: Affective Network; SN: Salience Network.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



