
Submitted:
31 January 2024
Posted:
01 February 2024
You are already at the latest version
Abstract
During the postpartum period, psychological disorders may emerge. Aims and objectives: 1 With the current study, we aim to raise awareness among healthcare professionals about postpartum depression (PPD) in women. To reach the aim we will perform the following tasks: (i) identify biological peripartum risk factors and calculate pooled prevalence of PPD for each of them; (ii) explore the strength of relationship between peripartum risk factors and PPD; (iii) rank the predictors by their prevalence and magnitude of association with PPD. The knowledge obtained will support the development and implementation of early diagnostic and preventive strategies. Methods and analysis: we will systematically go through peer-reviewed publications available in the PubMed search engine and online databases: Scopus, Web of Science, EMBASE. The scope of the review will include articles published any time in English, Arabic, or Polish. We will deduplicate literature sources with the Covidence software, evaluate heterogeneity between the study results, and critically assess credibility of selected articles with the Joanna Briggs Institute’s bias evaluation tool. The information to extract is incidence rate, prevalence, and odds ratio between each risk factor and PPD. A comprehensive analysis of the extracted data will allow us to achive the objectives. The study findings will contribute to risk stratification and more effective management of PPD in women.
Keywords:
postpartum
; depression postpartum
; blues postpartum
; psychosis review article
; risk factors
1. Introduction
Postpartum depression (PPD) is a debilitating mental disorder that occurs in 14% of women after childbirth [1]. Determinants of PPD can be grouped into socioeconomic, demographic and biological ones. The first group includes income, educational level, cultural background; the second group covers age, sex, race/ethnicity, marital status; the last group can be categorized into obstetric, maternal and neonatal risks. With an exception to the mode of delivery, biological peripartum determinants of PPD are sparsely represented in the literature [2].
The prevalence of PPD varies significantly across the countries with the highest numbers in South Africa and Southern Asia: 39.96 and 22.32%, respectively [1,3,4,5,6,7]. The lowest rates for PPD are documented in Oceania – 11.11% [3]. In the Middle East, PPD affects 27% of mothers, and the United Arab Emirates is a country with an enormously high percentage of women suffering from this disorder – 35% [6]. The high incidence of PPD in economically developed countries suggests the necessity of studying biological risk factors of the disease.
PPD significantly decreases quality of life. Mothers with PPD struggle to perform daily chores, care for children, and establish a bond with them, which may negatively affect infant development [8,9,10]. Severe episodes of PPD can lead to infanticide [11]. The disorder may trigger dissatisfaction with marriage, paternal postpartum depression, violence, and divorce [12,13,14]. Untreated cases can develop into major depressive disorder and increase the risk of suicide [15,16,17,18,19,20]. Early detection and treatment of PPD help to maintain positive family dynamics after childbirth. However, risk stratification remains a challenge.
Recent studies on the prevalence of postpartum depression and associated factors focused mainly on demographic and socioeconomic factors [21,22,23,24]. According to the studies, mothers from all socioeconomic strata are at risk for postpartum depression [25]. A little is known about biological predictors of PPD, although some of the risk factors can be modified or used for screening purposes. This serves as a motivation for the current study. To find biological risk factors, we will analyse pathogenic mechanisms of PPD such as the adaptive changes in neuropsychoendocrinology [26] and disruption in neurotransmission and brain connectivity [27]. Certain transformations in these systems occur due to psychological stressors and adaptation to a new environment [28]. Negative birth experience (difficult labor, obstetric complications and neonate pathologies) may account for persistent negative thoughts and anxiety resulting in development of PPD.
Since PPD is significantly undertreated, authors argue for the necessity of the preventative strategies that form more effective parenting skills and increased attachment to infant [29,30]. The occupational therapist maintains women’s readiness to childbirth. The specialist helps the patients to look at their limitations as a problem to be solved rather than as total inability [31,32]. Although efficient, the preventive measures are recourse-consuming, therefore they can be prescribed only to carefully selected cohorts of women who are at risk of this disease. To detect indications for PPD prevention, physicians need a reliable screening program with accurate risk assessment.
The existing screening for PPD does not meet the demand of time. First, some women may be reluctant to share their symptoms as a means of protecting their social standing and worry about others’ perceptions of inefficiency in their parental responsibilities [33]. Second, a routine assessment of the mothers’ mood is not consistently performed in some healthcare institutions. Third, biological, psychological, and socio-economic determinants act simultaneously [34,35,36,37,38]. In this meta-analysis, we will explore the relationship between PPD and multiple biological risk factors in the prepartum period. These factors can be detected directly from electronic patients’ data. The systematic synthesis of these data will promote evidence-based practices of PPD screening, prevention and treatment [39].
2. Objectives
The meta-analysis aims to explore biological risk factors of PPD, such as neonatal pathology (e.g., low Apgar Score, NICU admission, shoulder dystocia), mode of delivery, and obstetric complications (e.g., episiotomy, uterine curettage, and postpartum haemorrhage). The objectives of this project will be as follows:
- Identify biological peripartum risk factors and calculate pooled prevalence of PPD for each of them.
- Explore associations between biological peripartum risk factors and PPD.
- Rank the predictors by their prevalence and strength.
3. Materials and Methods
For preparing the protocol, we followed the checklist of the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocol (PRISMA-P) [40]. The PRISMA-P checklist is available in online supplemental material file 1. The protocol is registered with the international database for systematic reviews PROSPERO database (registration number CRD42022372067).
3.1. Study Design and Data Source
To perform a comprehensive systematic literature review, we will submit queries to three biomedical databases (Web of Science, EMBASE, and Scopus) and PubMed search engine. The search keywords and medical subject headings are listed in Table 1. We will extract English, Arabic, or Polish papers without time restrictions and screen the retrieved papers manually.
3.2. Eligibility Criteria
The review will cover generally healthy females without known risks for PPD before the last childbirth. Fetal abnormalities, maternal diseases, violence, and other traumatic life experiences will serve as exclusion criteria. To avoid bias connected with history of a risk factor we will focus on the last childbirth, its complications and birth modality. We will consider for the review only the original publication reporting findings on the women who live healthy lifestyles.
This study will analyse peer-reviewed papers about changes in postpartum mood, PPD, depressive disorder, or suicidal ideation in females after the delivery without restrictions on their age. The review scope will also include publications about pregnant women who had psychiatric consultation/referral or suicidal attempts following childbirth. Table 2 summarises the inclusion and exclusion criteria for the literature.
We will exclude grey literature, protocol papers, editorial letters, reviews, and case studies from the current review. Articles describing mental problems, neurocognitive diseases, and mood disorders prior to the delivery will not be considered. Also, the project will not cover COVID-19-related factors of postpartum mental health in women.
3.3. Study Records
Selection process. Papers extracted from the biomedical databases will be uploaded to the Covidence software for automatic deduplication and further screening. An initial title and abstract screening will be done against the eligibility criteria by two reviewers. Then, the whole text will be examined. If the reviewers disagree on eligibility of an article, the third reviewer will resolve the conflict. The PRISMA flowchart will show the selection process and results.
Data extraction. Two reviewers will independently extract information to an online spreadsheet for future analysis. The reference will include authors, country, publication year, sample size, and study design. The reviewers will collect data related to the PPD assessment and its biological risk factors. These will include their frequency measures, time since giving birth, assessment tools (e.g., Edinburgh Postnatal Depression Scale, Beck Depression Inventory, etc.), applied cut-off values, and scores in the questionnaires. Data on socioeconomic and demographic determinants will also be extracted to serve as possible covariates for comprehensive analysis: one can use this information for calculating adjusted odds ratio (OR). To derive conclusions about the strength of the association between PPD and its predictors, we will copy OR, pair coefficients of correlation and p-values to the spreadsheet.
Quality assessment of individual studies. We will use Joanna Briggs Institute checklists for a critical appraisal of cross-sectional, case-control, and cohort studies [41]. Two reviewers will independently assess each study against the corresponding checklist. In case of their disagreement, the third reviewer will decide on the final quality score of the study. The research team will apply funnel-plot-based methods to deal with potential publication bias [42]. In particular, we will construct funnel plots with Begg’s and Egger’s test [43,44].
Data analysis and synthesis. Once the data extraction is completed, we will check articles for inter-study homogeneity with the I2 test [45]. The possible sources of heterogeneity are the age of study participants and the time passed from childbirth. Study cohorts may also differ in the formal diagnosis of PPD and its severity. To control for this difference, we will divide the total population into two categories: the women at risk of the disorder and the women diagnosed with PPD. We will use weighted prevalence functions to continue meta-analysis even if the I2 index exceeds 75%, which indicates a strong between-study variability [46].
The subgroup analysis will be performed to evaluate the consistency of findings across multiple observational groups. In this way we will deal with the anticipated high inter-study variability. Specifically, we plan to apply a random effects model which helps to generalize findings beyond the included papers [47]. All articles will be grouped according to the peripartum risk factors which they describe: obstetric factors (mode of birth, epidural anesthesia), maternal complications (hemorrhage, vaginal lacerations, etc.), neonate complications (APGAR score, shoulder dystocia, diseases, etc.).
3.4. Study Methodology
To address the first specific objective, the research team will look for the biologial peripartum determinants of PPD. In this study we will consider the factors that have a biological nature, act at the time of delivery or shortly after it and pose a risk to the women’s mood postpartum. Then we will calculate the pooled incidence and prevalence of PPD in women for a specific group of peripartum complications.
Working on the second specific objective, we will explore the relationship between PPD and peripartum complications. An additional subgroup analysis will be conducted to identify the relationship between peripartum risk factors and the severity of PPD according to Edinburgh Postnatal Depression Scale, Beck Depression Inventory, and other questionnaires. The link between variables will be expressed in OR, r-coefficient, and p-values.
For the third specific objective, we will create ranking charts representing the contribution of different etiological factors to the total PPD incidence (see Figure 1). The statistical analysis will be performed in R package “meta” [46]. After constructing forest plots and ranking charts, we will do sensitivity analysis with the leave-one-out method to check the robustness of the final results and to assess the effect of a single study on the overall outcome.
4. Discussion
The proposed meta-analysis will summarize existing knowledge on the role of biological peripartum determinants of mental health in women after childbirth. Types of birth were the only biological peripartum risk factors extensively covered in recent studies. Previous studies revealed a greater chance of developing PPD in women who delivered via cesarean section (CS). The emergency cesarean section (CS) predisposes women to PPD by inducing fear, preoperative anxiety [48], and posttraumatic stress [49]. The general anesthesia in CS may also trigger depression at the molecular level [50]. The vaginal delivery is also associated with multiple complications such as postpartum hemorrhage [51,52], genital tract lacerations [53,54], bleeding, etc. The preferences of modes of delivery may impact females’ perceptions about childbirth experience and postpartum health [55]. Hence, the mode of birth should be included as a cofounder in the current study, although we mainly target other biological peripartum risk factors that have not been studied well.
In the following paragraphs, we give a short description of obstetric, maternal and neonatal risks. Literature findings on their association with PPD is scarce. Observational studies produced conflicting findings about the role of labor complications in development of PPD. Neonatal pathology also results in adverse psychological effects that have not been studied well [56].
Neonatal Status refers to such characteristics as birth weight, gestational age, APGAR score, health complications, admission to the neonatal intensive care unit [57,58,59,60,61,62]. The severe conditions, such as asphyxia, can significantly impair mother’s mental health. Besides, the neonate’s temperament [58], sleep patterns [63], and breastfeeding behavior can also be stressful [64] thus leading to anxiety and PPD.
Obstetric Complications account for around 800 maternal deaths daily [65], they are more common in developing countries [65]. In women with peripartum complications, the prevalence of PPD ranges from 12.5% to 44.2% [66]. The incomplete list of the complications include protracted cervical dilation, endometriosis, preeclampsia, gestational diabetes, miscarriage and preterm childbirth in the future pregnancies [67,68,69,70,71,72,73,74]. Postpartum hemorrhage is one of the most frequent pregnancy consequence, and it remains among the top leading causes of maternal mortality worldwide [75,76]. Some studies failed to find a direct association between the hemorrhage and PPD [77,78]. Still, post-hemorrhagic anemia, negative birth experience, and fear of death are independently linked with the elevated risk of depression [57,79,80,81].
Obstetric Procedures. In this research, we will review systematically the PPD due to the peripartum obstetric complications that were not properly studied as risk factors of PPD. Episiotomy incision may cause bleeding, swelling, infection, and perineal pain [82,83], which affects mother’s quality of life, sexual and mental health [84]. The question of how episiotomy affects the mother’s mood is still debated [79,84]. Postpartum uterine curettage is associated with bleeding, anemia and psychological discomfort [57,79,80,81]. After the curettage, women could experience cervix damage, Asherman’s syndrome, and infections. In the long term, they may also suffer from painful or irregular menstruation cycles [85]. Adverse effects of obstetric procedures include restrictions on sexual life and physical activity imposed by physicians [86].
5. Conclusion
A comprehensive understanding of biopsychosocial precursors to PPD is required to improve prevention, early detection, and treatment of PPD in women. With the current study, we want to raise awareness among healthcare professionals about the pathology and to unravel the role of biological peripartum risk factors in its development. The results of the proposed systematic review and meta-analysis will serve as a guideline for its accurate screening thus preventing unnecessary suffering for women, their children and families.
6. Strength and Limitations
- The protocol is prepared in accordance with the PRISMA-P checklist for systematic reviews; the protocol is registered with the international database for the systematic reviews PROSPERO.
- The study will focus on the biological peripartum risk factors for PPD, which are not studied well/
- The socioeconomic and demographic risks will also be included into analysis as co-founders.
- We will perform subgroup analysis to evaluate the consistency of findings across multiple observational groups.
- A notable limitation of this systematic review is the scarcity of findings on biological peripartum risk factors for PPD.
Review Status
The review was started in June 2023.
Potential Amendments
To avoid potential changes, we predetermined the inclusion and exclusion criteria and performed a preliminary search. Any changes that are required during the review preparation process will be reported by updating the online registered PROSPERO protocol.
Patients and Public Involvement
Patients or the general public are not participants in the study.
Ethics and Dissemination
An ethics approval is not required for the systematic review. The results of the study will be presented at scientific conferences as a poster or presentation in addition to being published in a peer-reviewed journal.
Patient Consent for Publication
Not applicable.
Author Contributions
Conceptualization: K.Z., Y.S. and D.S.; writing (original draft preparation): M.A.A., and Y.S.; study methodology:D.S., K.Z. and Y.S.; visualization: M.A.A; writing (review and editing)—by K.Z., Y.S.; problem investigation—by M.A.A., G.S.S., M.A.; supervision—by S.A.A and K.Z.; project administration– K.Z.; funding acquisition— Y.S. All authors contributed to the article and approved the submitted version.
Funding
This project was supported by the College of Medicine and Health Sciences, UAEU, SURE+ grant G00004391 (PI: YS)
Conflicts of Interest
The research will be carried out without any financial or commercial ties that might be viewed as having a possible conflict of interest, according to the authors.
References
- Liu, X.; Wang, S.; Wang, G. Prevalence and risk factors of postpartum depression in women: a systematic review and meta-analysis. Journal of Clinical Nursing 2022, 31, 2665–2677. [Google Scholar] [CrossRef] [PubMed]
- Yim, I.S.; Tanner Stapleton, L.R.; Guardino, C.M.; Hahn-Holbrook, J.; Dunkel Schetter, C. Biological and psychosocial predictors of postpartum depression: systematic review and call for integration. Annual review of clinical psychology 2015, 11, 99–137. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Liu, J.; Shuai, H.; Cai, Z.; Fu, X.; Liu, Y.; Xiao, X.; Zhang, W.; Krabbendam, E.; Liu, S.; et al. Mapping global prevalence of depression among postpartum women. Translational psychiatry 2021, 11, 543. [Google Scholar] [CrossRef] [PubMed]
- Shorey, S.; Chee, C.Y.I.; Ng, E.D.; Chan, Y.H.; San Tam, W.W.; Chong, Y.S. Prevalence and incidence of postpartum depression among healthy mothers: A systematic review and meta-analysis. Journal of psychiatric research 2018, 104, 235–248. [Google Scholar] [CrossRef] [PubMed]
- Affonso, D.D.; De, A.K.; Horowitz, J.A.; Mayberry, L.J. An international study exploring levels of postpartum depressive symptomatology. Journal of psychosomatic research 2000, 49, 207–216. [Google Scholar] [CrossRef]
- Alshikh Ahmad, H.; Alkhatib, A.; Luo, J. Prevalence and risk factors of postpartum depression in the Middle East: a systematic review and meta–analysis. BMC pregnancy and childbirth 2021, 21, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Haque, A.; Namavar, A.; Breene, K.A. Prevalence and risk factors of postpartum depression in Middle Eastern/Arab women. Journal of Muslim mental health 2015, 9. [Google Scholar] [CrossRef]
- Faisal-Cury, A.; Bertazzi Levy, R.; Kontos, A.; Tabb, K.; Matijasevich, A. Postpartum bonding at the beginning of the second year of child’s life: the role of postpartum depression and early bonding impairment. Journal of Psychosomatic Obstetrics & Gynecology 2020, 41, 224–230. [Google Scholar]
- Netsi, E.; Pearson, R.M.; Murray, L.; Cooper, P.; Craske, M.G.; Stein, A. Association of persistent and severe postnatal depression with child outcomes. JAMA psychiatry 2018, 75, 247–253. [Google Scholar] [CrossRef]
- Mughal, S.; Azhar, Y.; Siddiqui, W.; May, K. Postpartum depression (nursing). In StatPearls [Internet]; StatPearls Publishing, 2022. [Google Scholar]
- Naviaux, A.F.; Janne, P.; Gourdin, M. Psychiatric considerations on infanticide: throwing the baby out with the bathwater. Psychiatria Danubina 2020, 32, 24–28. [Google Scholar]
- Barooj-Kiakalaee, O.; Hosseini, S.H.; Mohammadpour-Tahmtan, R.A.; Hosseini-Tabaghdehi, M.; Jahanfar, S.; Esmaeili-Douki, Z.; Shahhosseini, Z. Paternal postpartum depression’s relationship to maternal pre and postpartum depression, and father-mother dyads marital satisfaction: A structural equation model analysis of a longitudinal study. Journal of Affective Disorders 2022, 297, 375–380. [Google Scholar] [CrossRef]
- Salm Ward, T.; Kanu, F.A.; Robb, S.W. Prevalence of stressful life events during pregnancy and its association with postpartum depressive symptoms. Archives of women’s mental health 2017, 20, 161–171. [Google Scholar] [CrossRef]
- Johannsen, B.M.; Mægbæk, M.L.; Bech, B.H.; Laursen, T.M.; Munk-Olsen, T. Divorce or Separation Following Postpartum Psychiatric Episodes: A Population-Based Cohort Study. The Journal of Clinical Psychiatry 2021, 82, 29461. [Google Scholar] [CrossRef]
- Lindahl, V.; Pearson, J.L.; Colpe, L. Prevalence of suicidality during pregnancy and the postpartum. Archives of women’s Mental Health 2005, 8, 77–87. [Google Scholar] [CrossRef]
- Bagheri, P.; Rostami, M. Postpartum depression and suicide in Iran. Women’s Health 2021, 17, 17455065211043994. [Google Scholar] [CrossRef]
- Hanach, N.; Radwan, H.; Fakhry, R.; Dennis, C.L.; Issa, W.B.; Faris, M.E.; Obaid, R.S.; Al Marzooqi, S.; Tabet, C.; De Vries, N. Prevalence and risk factors of postpartum depression among women living in the United Arab Emirates. Social psychiatry and psychiatric epidemiology 2023, 58, 395–407. [Google Scholar] [CrossRef]
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS medicine 2006, 3, e442. [Google Scholar] [CrossRef]
- de Avila Quevedo, L.; Scholl, C.C.; de Matos, M.B.; da Silva, R.A.; da Cunha Coelho, F.M.; Pinheiro, K.A.T.; Pinheiro, R.T. Suicide risk and mood disorders in women in the postpartum period: a longitudinal study. Psychiatric quarterly 2021, 92, 513–522. [Google Scholar] [CrossRef]
- Lee, Y.L.; Tien, Y.; Bai, Y.S.; Lin, C.K.; Yin, C.S.; Chung, C.H.; Sun, C.A.; Huang, S.H.; Huang, Y.C.; Chien, W.C.; et al. Association of postpartum depression with maternal suicide: a nationwide population-based study. International journal of environmental research and public health 2022, 19, 5118. [Google Scholar] [CrossRef]
- Moraes, I.G.d.S.; Pinheiro, R.T.; Silva, R.A.d.; Horta, B.L.; Sousa, P.L.R.; Faria, A.D. Prevalence of postpartum depression and associated factors. Revista de Saúde Pública 2006, 40, 65–70. [Google Scholar] [CrossRef]
- Park, J.h.; Karmaus, W.; Zhang, H. Prevalence of and risk factors for depressive symptoms in Korean women throughout pregnancy and in postpartum period. Asian nursing research 2015, 9, 219–225. [Google Scholar] [CrossRef]
- Drozd, F.; Haga, S.M.; Valla, L.; Slinning, K. Latent trajectory classes of postpartum depressive symptoms: A regional population-based longitudinal study. Journal of Affective Disorders 2018, 241, 29–36. [Google Scholar] [CrossRef]
- Selcuki, N.F.T.; Bahat, P.Y.; Turan, G.; Aksoy, U.; Bagci, K.; Ozdemir, I. Postpartum evaluation of the role of maternal characteristics and mode of delivery on maternal attachment, anxiety and depression; a study conducted in Turkey. Acta Bio Medica: Atenei Parmensis 2022, 93. [Google Scholar]
- Goyal, D.; Gay, C.; Lee, K.A. How much does low socioeconomic status increase the risk of prenatal and postpartum depressive symptoms in first-time mothers? Women’s Health Issues 2010, 20, 96–104. [Google Scholar] [CrossRef]
- Skalkidou, A.; Hellgren, C.; Comasco, E.; Sylvén, S.; Poromaa, I.S. Biological aspects of postpartum depression. Women’s health 2012, 8, 659–672. [Google Scholar] [CrossRef]
- Payne, J.L.; Maguire, J. Pathophysiological mechanisms implicated in postpartum depression. Frontiers in neuroendocrinology 2019, 52, 165–180. [Google Scholar] [CrossRef] [PubMed]
- Abdollahi, F.; Lye, M.S.; Zarghami, M. Perspective of postpartum depression theories: A narrative literature review. North American journal of medical sciences 2016, 8, 232. [Google Scholar]
- Werner, E.; Miller, M.; Osborne, L.M.; Kuzava, S.; Monk, C. Preventing postpartum depression: review and recommendations. Archives of women’s mental health 2015, 18, 41–60. [Google Scholar] [CrossRef]
- Sangsawang, B.; Wacharasin, C.; Sangsawang, N. Interventions for the prevention of postpartum depression in adolescent mothers: a systematic review. Archives of women’s mental health 2019, 22, 215–228. [Google Scholar] [CrossRef]
- Acharya, V. Preparing for motherhood: a role for occupational therapy. World Federation of Occupational Therapists Bulletin 2014, 70, 16–17. [Google Scholar] [CrossRef]
- Osorio-Castaño, J.H.; Carvajal-Carrascal, G.; Rodríguez-Gázquez, M. Preparation for motherhood during Pregnancy: a Concept Analysis. Investigacion y educacion en enfermeria 2017, 35, 295–305. [Google Scholar] [CrossRef]
- Cox, E.Q.; Sowa, N.A.; Meltzer-Brody, S.E.; Gaynes, B.N. The perinatal depression treatment cascade: baby steps toward improving outcomes. The Journal of clinical psychiatry 2016, 77, 20901. [Google Scholar] [CrossRef]
- Li, Q.; Yang, S.; Xie, M.; Wu, X.; Huang, L.; Ruan, W.; Liu, Y. Impact of some social and clinical factors on the development of postpartum depression in Chinese women. BMC pregnancy and childbirth 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Guintivano, J.; Sullivan, P.; Stuebe, A.; Penders, T.; Thorp, J.; Rubinow, D.; Meltzer-Brody, S. Adverse life events, psychiatric history, and biological predictors of postpartum depression in an ethnically diverse sample of postpartum women. Psychological medicine 2018, 48, 1190–1200. [Google Scholar] [CrossRef]
- Marín-Morales, D.; Toro-Molina, S.; Peñacoba-Puente, C.; Losa-Iglesias, M.; Carmona-Monge, F.J. Relationship between postpartum depression and psychological and biological variables in the initial postpartum period. Maternal and Child Health Journal 2018, 22, 866–873. [Google Scholar] [CrossRef]
- Ostacoli, L.; Cosma, S.; Bevilacqua, F.; Berchialla, P.; Bovetti, M.; Carosso, A.R.; Malandrone, F.; Carletto, S.; Benedetto, C. Psychosocial factors associated with postpartum psychological distress during the Covid-19 pandemic: a cross-sectional study. BMC pregnancy and childbirth 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Qi, W.; Zhao, F.; Liu, Y.; Li, Q.; Hu, J. Psychosocial risk factors for postpartum depression in Chinese women: a meta-analysis. BMC Pregnancy and Childbirth 2021, 21, 1–15. [Google Scholar] [CrossRef]
- Loudon, H.; Nentin, F.; Silverman, M.E. Using clinical decision support as a means of implementing a universal postpartum depression screening program. Archives of women’s mental health 2016, 19, 501–505. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P.; et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. International journal of surgery 2010, 8, 336–341. [Google Scholar] [CrossRef]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: an introduction to the JBI critical appraisal tool. JBI evidence synthesis 2020, 18, 2127–2133. [Google Scholar] [CrossRef]
- Lin, L.; Chu, H. Quantifying publication bias in meta-analysis. Biometrics 2018, 74, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. bmj 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 1088–1101. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Statistics in medicine 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Ahn, E.; Kang, H. Introduction to systematic review and meta-analysis. Korean journal of anesthesiology 2018, 71, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Tufanaru, C.; Munn, Z.; Stephenson, M.; Aromataris, E. Fixed or random effects meta-analysis? Common methodological issues in systematic reviews of effectiveness. JBI Evidence Implementation 2015, 13, 196–207. [Google Scholar] [CrossRef] [PubMed]
- Bansal, T.; Joon, A. A comparative study to assess preoperative anxiety in obstetric patients undergoing elective or emergency cesarean section. Anaesthesia, Pain & Intensive Care 2019, 25–30. [Google Scholar]
- Orovou, E.; Dagla, M.; Iatrakis, G.; Lykeridou, A.; Tzavara, C.; Antoniou, E. Correlation between kind of cesarean section and posttraumatic stress disorder in Greek women. International journal of environmental research and public health 2020, 17, 1592. [Google Scholar] [CrossRef] [PubMed]
- Meky, H.K.; Shaaban, M.M.; Ahmed, M.R.; Mohammed, T.Y. Prevalence of postpartum depression regarding mode of delivery: a cross-sectional study. The Journal of Maternal-Fetal & Neonatal Medicine 2020, 33, 3300–3307. [Google Scholar]
- Wang, K.; Qiu, J.; Meng, L.; Lai, X.; Yao, Z.; Peng, S. Postpartum hemorrhage and postpartum depressive symptoms: A retrospective cohort study. Depression and anxiety 2022, 39, 246–253. [Google Scholar] [CrossRef]
- Parry-Smith, W.; Okoth, K.; Subramanian, A.; Gokhale, K.M.; Chandan, J.S.; Humpston, C.; Coomarasamy, A.; Nirantharakumar, K.; Šumilo, D. Postpartum haemorrhage and risk of mental ill health: A population-based longitudinal study using linked primary and secondary care databases. Journal of Psychiatric Research 2021, 137, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Asif, S.; Mulic-Lutvica, A.; Axfors, C.; Eckerdal, P.; Iliadis, S.I.; Fransson, E.; Skalkidou, A. Severe obstetric lacerations associated with postpartum depression among women with low resilience–a Swedish birth cohort study. BJOG: An International Journal of Obstetrics & Gynaecology 2020, 127, 1382–1390. [Google Scholar]
- Hall, W.A.; Hauck, Y.L.; Carty, E.M.; Hutton, E.K.; Fenwick, J.; Stoll, K. Childbirth fear, anxiety, fatigue, and sleep deprivation in pregnant women. Journal of Obstetric, Gynecologic & Neonatal Nursing 2009, 38, 567–576. [Google Scholar]
- Nilvér, H.; Begley, C.; Berg, M. Measuring women’s childbirth experiences: a systematic review for identification and analysis of validated instruments. BMC pregnancy and childbirth 2017, 17, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Field, T. Postpartum depression effects on early interactions, parenting, and safety practices: a review. Infant Behavior and Development 2010, 33, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kukulskienė, M.; Žemaitienė, N. Postnatal depression and post-traumatic stress risk following miscarriage. International journal of environmental research and public health 2022, 19, 6515. [Google Scholar] [CrossRef]
- JayaSalengia, B.; Rajeswari, S.; Nalini, S. The relationship between maternal confidence, infant temperament, and postpartum depression. Iranian journal of nursing and midwifery research 2019, 24, 437. [Google Scholar] [PubMed]
- Grippi, C. Factors That Influence Women’s Symptoms of Postpartum Depression After Discharge of Their Preterm Infants From the NICU. Journal of Obstetric, Gynecologic & Neonatal Nursing 2021, 50, 610–620. [Google Scholar]
- Wyatt, T.; Shreffler, K.M.; Ciciolla, L. Neonatal intensive care unit admission and maternal postpartum depression. Journal of reproductive and infant psychology 2019, 37, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Garfield, C.F.; Lee, Y.S.; Warner-Shifflett, L.; Christie, R.; Jackson, K.L.; Miller, E. Maternal and paternal depression symptoms during NICU stay and transition home. Pediatrics 2021, 148. [Google Scholar] [CrossRef]
- Tsai, J.M.; Tsai, L.Y.; Tsay, S.L.; Chen, Y.H. The prevalence and risk factors of postpartum depression among women during the early postpartum period: a retrospective secondary data analysis. Taiwanese Journal of Obstetrics and Gynecology 2023, 62, 406–411. [Google Scholar] [CrossRef]
- Ölmestig, T.K.; Siersma, V.; Birkmose, A.R.; Kragstrup, J.; Ertmann, R.K. Infant crying problems related to maternal depressive and anxiety symptoms during pregnancy: a prospective cohort study. BMC pregnancy and childbirth 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Islam, M.J.; Broidy, L.; Baird, K.; Rahman, M.; Zobair, K.M. Early exclusive breastfeeding cessation and postpartum depression: Assessing the mediating and moderating role of maternal stress and social support. PloS one 2021, 16, e0251419. [Google Scholar] [CrossRef] [PubMed]
- Pregnancy-related complications. Available online: https://www.who.int/teams/integrated-health-services/clinical-services-and-systems/surgical-care/pregnancy- related-complications (accessed on 27 December 2022).
- Tsakiridis, I.; Bousi, V.; Dagklis, T.; Sardeli, C.; Nikolopoulou, V.; Papazisis, G. Epidemiology of antenatal depression among women with high-risk pregnancies due to obstetric complications: a scoping review. Archives of gynecology and obstetrics 2019, 300, 849–859. [Google Scholar] [CrossRef]
- Gao, L.; Qu, J.; Wang, A.Y. Anxiety, depression and social support in pregnant women with a history of recurrent miscarriage: a cross-sectional study. Journal of reproductive and infant psychology 2020, 38, 497–508. [Google Scholar] [CrossRef] [PubMed]
- Laganà, A.S.; La Rosa, V.L.; Rapisarda, A.M.C.; Valenti, G.; Sapia, F.; Chiofalo, B.; Rossetti, D.; Ban Frangež, H.; Vrtačnik Bokal, E.; Vitale, S.G. Anxiety and depression in patients with endometriosis: impact and management challenges. International journal of women’s health 2017, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Auger, N.; Low, N.; Paradis, G.; Ayoub, A.; Fraser, W.D. Preeclampsia and the longitudinal risk of hospitalization for depression at 28 years. Social psychiatry and psychiatric epidemiology 2021, 56, 429–436. [Google Scholar] [CrossRef]
- Bergink, V.; Laursen, T.; Johannsen, B.; Kushner, S.; Meltzer-Brody, S.; Munk-Olsen, T. Pre-eclampsia and first-onset postpartum psychiatric episodes: a Danish population-based cohort study. Psychological Medicine 2015, 45, 3481–3489. [Google Scholar] [CrossRef]
- Byrn, M.; Penckofer, S. The relationship between gestational diabetes and antenatal depression. Journal of Obstetric, Gynecologic & Neonatal Nursing 2015, 44, 246–255. [Google Scholar]
- Zhu, Y.; Zhang, C. Prevalence of gestational diabetes and risk of progression to type 2 diabetes: a global perspective. Current diabetes reports 2016, 16, 1–11. [Google Scholar] [CrossRef]
- Hompoth, E.A.; Pető, Z.; Fűrészné Balogh, V.; Töreki, A. Associations between depression symptoms, psychological intervention and perinatal complications. Journal of Clinical Psychology in Medical Settings 2020, 27, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Koutra, K.; Vassilaki, M.; Georgiou, V.; Koutis, A.; Bitsios, P.; Kogevinas, M.; Chatzi, L. Pregnancy, perinatal and postpartum complications as determinants of postpartum depression: the Rhea mother–child cohort in Crete, Greece. Epidemiology and psychiatric sciences 2018, 27, 244–255. [Google Scholar] [CrossRef] [PubMed]
- Likis, F.; Sathe, N.; Morgans, A.; et al. Management of postpartum hemorrhage; agency for healthcare research and quality, 2015; p. 613. [Google Scholar]
- Kassebaum, N.J.; Bertozzi-Villa, A.; Coggeshall, M.S.; Shackelford, K.A.; Steiner, C.; Heuton, K.R.; Gonzalez-Medina, D.; Barber, R.; Huynh, C.; Dicker, D.; et al. Global, regional, and national levels and causes of maternal mortality during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet 2014, 384, 980–1004. [Google Scholar] [CrossRef] [PubMed]
- Meltzer-Brody, S.; Maegbaek, M.; Medland, S.; Miller, W.; Sullivan, P.; Munk-Olsen, T. Obstetrical, pregnancy and socio-economic predictors for new-onset severe postpartum psychiatric disorders in primiparous women. Psychological medicine 2017, 47, 1427–1441. [Google Scholar] [CrossRef]
- Eckerdal, P.; Kollia, N.; Löfblad, J.; Hellgren, C.; Karlsson, L.; Högberg, U.; Wikström, A.K.; Skalkidou, A. Delineating the association between heavy postpartum haemorrhage and postpartum depression. PloS one 2016, 11, e0144274. [Google Scholar] [CrossRef]
- Zaręba, K.; Banasiewicz, J.; Rozenek, H.; Wójtowicz, S.; Jakiel, G. Peripartum predictors of the risk of postpartum depressive disorder: Results of a case-control study. International journal of environmental research and public health 2020, 17, 8726. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, L.; Guo, N.; Jiang, H. Postpartum depression and postpartum post-traumatic stress disorder: prevalence and associated factors. BMC psychiatry 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Wassef, A.; Nguyen, Q.D.; St-André, M. Anaemia and depletion of iron stores as risk factors for postpartum depression: a literature review. Journal of Psychosomatic Obstetrics & Gynecology 2019, 40, 19–28. [Google Scholar]
- Karbanova, J.; Rusavy, Z.; Betincova, L.; Jansova, M.; Necesalova, P.; Kalis, V. Clinical evaluation of early postpartum pain and healing outcomes after mediolateral versus lateral episiotomy. International Journal of Gynecology & Obstetrics 2014, 127, 152–156. [Google Scholar]
- Macarthur, A.J.; Macarthur, C. Incidence, severity, and determinants of perineal pain after vaginal delivery: a prospective cohort study. American journal of obstetrics and gynecology 2004, 191, 1199–1204. [Google Scholar] [CrossRef]
- Faisal-Cury, A.; Menezes, P.R. Type of delivery is not associated with maternal depression. Archives of Women’s Mental Health 2019, 22, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Santamaria, X.; Isaacson, K.; Simón, C. Asherman’s syndrome: it may not be all our fault. Human Reproduction 2018, 33, 1374–1380. [Google Scholar] [CrossRef] [PubMed]
- Bahat, P.Y.; Turan, G.; Selçuki, N.F.T.; Çakmak, K.; Kaya, C. Comparison of Depression and Anxiety Scores in Multi/Nulliparous Women who have Undergone Dilatation and Curettage. Acta Bio Medica: Atenei Parmensis 2022, 93. [Google Scholar]
Figure 1.
Study pipeline.
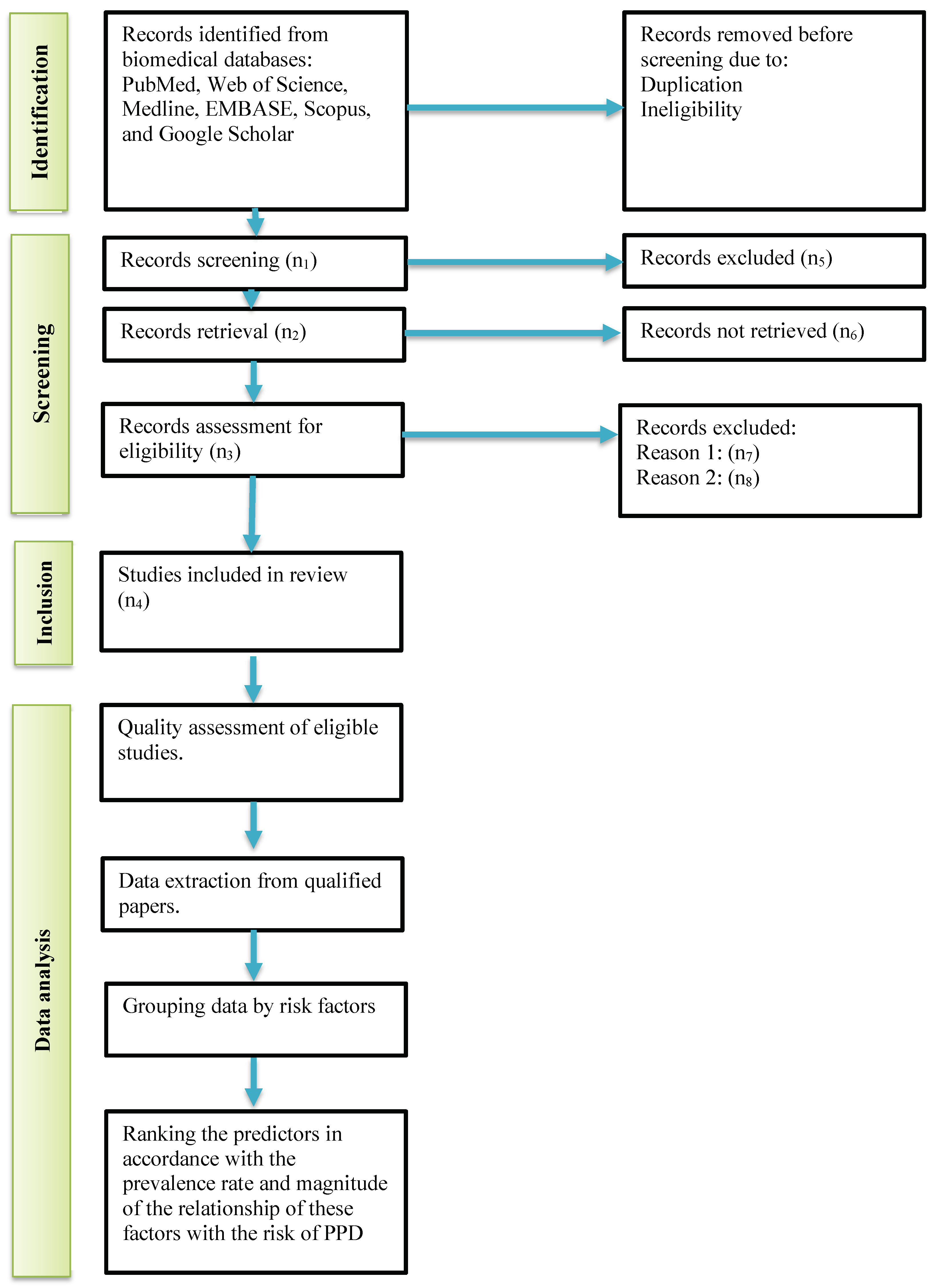

Table 1.
Keywords and medical subject headings for PubMed/Medline
| No | Search string |
Number of articles |
|---|---|---|
| 1 |
"postpartum period"[MeSH Terms]
OR "postpartum"[Title/Abstract] OR "puerperium"[Title/Abstract] OR "pregnancy"[MeSH Terms] OR "pregnancy"[Title/Abstract] |
1,136,113 |
| 2 |
"depression, postpartum"[MeSH Terms]
OR "depressive disorder"[MeSH Terms] OR "depression"[MeSH Terms] OR "depressive disorder"[MeSH Terms] OR "mood disorders" [MeSH Terms] OR "suicide"[MeSH Terms] OR "postpartum depression"[Title/Abstract] OR "mood disorder" [Title/Abstract] OR "baby blues"[Title/Abstract] |
361,517 |
| 3 |
((((((((((((((((((((((risk factors[MeSH Terms])
(Obstetric Labor Complications[MeSH Terms])) OR (fetal disease[MeSH Terms])) OR (pregnancy complications[MeSH Terms])) OR (complication*[Title/Abstract])) OR (intrapartum complication[Title/Abstract])) OR (birt complication*[Title/Abstract])) OR (maternal complication*[Title/Abstract])) OR (shoulder dystocia[Title/Abstract])) OR (hemorrhage[Title/Abstract])) OR (hemorrhage[Title/Abstract])) OR (asphyxia[Title/Abstract])) OR (baby complication[Title/Abstract])) OR (vaginal birth[Title/Abstract])) OR (vaginal delivery[Title/Abstract])) OR (caesarean section[Title/Abstract])) OR (vacuum extractor[Title/Abstract])) OR (forceps delivery[Title/Abstract])) OR (vaginal tears[Title/Abstract])) OR (vaginal laceration[Title/Abstract])) OR (episiotomy[Title/Abstract])) OR (uterine curettage[Title/Abstract]) |
2,579,080 |
| 4 |
"Forecasting"[MeSH Terms:noexp]
OR "predict*"[Title/Abstract] OR "determinants"[Title/Abstract] |
2,264,321 |
| 5 | #1 AND #2 AND #3 AND #4 | 2156 |
Table 2.
Inclusion and exclusion criteria
| Inclusion criteria | Exclusion criteria | |
| for literature | for participants | |
|
1. Cross-sectional or longitudinal design original studies. 2. English, Arabic, or Polish peer-reviewed articles. 3. Articles reporting risk factors for PPD. 4. Studies focused on changes in postpartum mood, suicidal ideation, and suicides following birth with diagnosed PPD after the last birth. 5. Study subjects who had psychiatric consultation or referral due to symptoms of PPD with following diagnosis of PPD after the last birth. |
1. grey literature 2. Case studies, reviews, metaanalyses, and letters to the editor case studies. 3. Research describing mental problems, neurocognitive diseases, and mood disorders that were present before birth. 4. studies that did not report sensitivity and specificity 5. Studies reporting the relationship between the PPD and factors occurring due to COVID-19. . |
Pregnant women with the following diseases and conditions diagnosed before the last birth: 1. mental and psychological disorders (F00-F99 in ICD-10) 2. cerebrovascular diseases (I60-I69) 3. organic pathologies of the central nervous system (e.g., brain and meninges tumors – C71, D32-33) 4. Serious abnormalities or diseases known before the last birth that are known risk factors for PPD (O35.9 in ICD10) 5. Partner or other type of violence. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



