
Submitted:
29 January 2024
Posted:
01 February 2024
You are already at the latest version
Abstract
: Suicide is a serious public health problem, with a global mortality rate of 1.4% of all deaths worldwide, and the leading cause of unnatural death in Spain. The use of clinical simulation has proven to be a beneficial tool in the training of nursing students. Such experiences allow them to develop cognitive and affective skills that are fundamental for the detection of warning signs and use of interventions in cases of people who want to take their own lives. Working in a mental health environment can be difficult for nursing students; therefore, the purpose of this study was to explore the perceptions of nursing students on the approach, management and intervention of suicidal crisis through clinical mental health simulation. Methods: qualitative descriptive phenomenological study through focus groups and reflective narratives in a sample of 45 students. A thematic analysis was performed using ATLAS-ti. Results: After the analysis, three themes were obtained: (a) management and handling of emotions (b) identification of suicide motives (c) intervention in suicidal crisis. Discussion: Clinical simulation in mental health allows students to exercise clinical judgment reasoning, detect warning signs for a better treatment approach, and provide tools for effective intervention and management of patient care. The results of this study indicate that nursing students face challenges in approaching mental health clinical simulation due to lack of prior exposure.
Keywords:
suicide
; mental health
; simulation training
; nursing student
; qualitative research
1. Introduction
In 1986, the World Health Organization (WHO) defined suicide as “an act with a lethal outcome, deliberately initiated and carried out by the subject, knowing or expecting its lethal outcome and through which he/she intends to obtain the desired changes”. [1,2] Although there is no universal consensus on the nomenclature of suicidal behavior, related concepts are based on two criteria: “self-inflicted” and “purpose of death.” [3,4]
Suicide is one of the leading causes of death in the general population and the third leading cause of adolescent death in the world [5]. It is recognized as a serious public health problem that causes more than 700,000 deaths per year, with figures of eleven suicides per day, a figure that is multiplied by 20 when referring to attempts, being the first cause of external death in Spain, [6,7] while in the USA, suicide is the tenth leading cause of death in the United States, with more than 47 000 deaths in 2019. [8] Given its prevalence and global burden, the reduction of suicide deaths has been a global goal of the WHO and has been included as an indicator (indicator 3.4.2 Reduce Suicide Death Rates) within the United Nations Sustainable Development Goals for 2030. [9] Furthermore, it should be taken into account that, in addition to lethality, suicidal behavior (suicidal ideation, suicide attempt, suicide plan, and death by suicide) produces a negative psychological impact on the personal and close circles of the person who takes his or her own life, including health professionals. [10]
Suicide is a complex phenomenon, influenced by diverse causes at both individual and contextual levels. [5,11] Addressing this problem requires a comprehensive perspective of prevention, [5] based on multiple interventions that act both at the collective and individual level that has been changing according to culture, religion and intellectual principles of history [11,12] These interventions are aimed at people at risk and imply the need for training of nursing professionals in the management of these behaviors. [12,13] To address suicide risk and prevention, it is crucial to detect risk factors such as the presence of mental disorders, [5,11,12,14,15] history of previous suicide attempts, [5,12,14,15] advanced age, [15] substance abuse, [5,16] family problems [14] and conflicting relationships, sociocultural and economic problems, [14] use of psychotropic drugs, [15] social isolation, [11,12] access to lethal means, [15] and hopelessness [12] are the most relevant risk factors, since they represent a danger for the development of this behavior, as well as the elements that provide security for life maintenance. In addition, the causes that may precipitate suicidal behavior should be identified.
This comprehensive approach allows for the development of effective strategies such as developing awareness campaigns to reduce the stigma associated with mental health by promoting early detection of signs of risk, implementing follow-up and support programs for those who have previously attempted to take their own lives, ensuring access to mental health services, developing prevention and treatment programs for substance use, [13] as well as offering counseling and family support services, [12,13,17] fostering social connectedness, [11,12] through community programs [12] and stigma reduction, [12,18] support groups, [10,11,17] implement strategies to reduce access to lethal means such as gun access restrictions and safety education [8] and medication management, [13] education of frontline professionals, with special attention to nurses [10,17,18] addressing the different dimensions of this issue, in addition to brief active contact [17] and digitally driven outreach and interventions. [8,13,17] All of the above contribute to suicide prevention in a more effective way. [11,12,17] The following are some of the most effective ways to prevent suicide [11,12,17].
Most people who died by suicide had contact with the health care system in the year prior to their death [8,19], so the nursing professional has a role in suicide prevention by identifying and addressing risk factors and detecting warning signs. [20] However, this can be hindered by lack of training, lack of support and lack of protocols, [21] indicating in studies such as Silva’s that 53% of nurses in the United States indicated that they had not received prior training in suicide prevention or assessment. [10,17,18,22] Suicide attempts represent a significant clinical challenge in the field of mental health, demanding accurate and effective interventions to prevent future episodes and promote the recovery of affected individuals. [13] The inherent complexity of these cases underscores the need for clinical training strategies that train nursing professionals in the acquisition of practical assessment and management skills in different situations. [19,23]
This training should be included in undergraduate education, and it is essential to provide nursing students with specialized knowledge on early detection of warning signs, suicide risk assessment, communication skills, empathy and active listening, as well as intervention strategies. [10,14] This training not only enables them to recognize risk and protective factors, but also enables them to provide a supportive, understanding and caring environment that is essential in the process of recovery and suicide prevention, which can contribute to comprehensive care that is sensitive to the emotional and psychological needs of patients at risk of suicide. [16] Performing a mental status examination and suicide risk assessment is an important skill required of nurses when in the clinical setting. Because nursing students often express anxiety and lack of confidence in doing so, the use of standardized patients provides an excellent opportunity to practice and master this skill in a simulated setting. [24]
Overall, simulation has become an important tool in the field of mental health, as it simulates clinical settings and reveals the potential for advancing this practice. It is considered an innovative and essential tool for improving clinical competence and decision making in critical situations. [25] Although simulation offers important benefits to clinical training in mental health, its educational development is limited with respect to other specialties and faces controversies that hinder its full integration. [26] Extensive research has demonstrated the benefits of incorporating clinical simulation into psychiatric/mental health nursing curricula, emphasizing increased confidence and critical thinking to address the aforementioned difficulties. [18] Significant changes have occurred over the past decade, with a growing number of recent experiments and meta-analyses strongly supporting the use of simulation-based mental health education for health care professionals [27].
Improving identification and intervention with patients at risk of suicide requires innovative training techniques that safely and effectively teach or enhance the skills of professionals Advanced clinical simulation, including virtual simulation allows the transmission of suicide prevention strategies using a realistic and risk-free environment. [29] The construction of simulation scenarios allows not only training in critical situations, but the opportunity to discuss and reflect on the topic, increasing awareness and understanding of the issue, and may increase prevention rates. [30].
Therefore, the aim of the study is to explore the perceptions of nursing students on the approach, management and intervention in suicidal crisis through experiences based on clinical mental health simulation.
2. Materials and Methods
2.1. Study design
A qualitative descriptive phenomenological study was conducted with the aim of exploring the perceptions and experiences of students during the clinical simulation in mental health of patients at risk of suicide, taking into account their circumstances and their own points of view. [31]
2.2. Participants and sampling
Non-probability and purposive sampling was performed by selecting participants based on their ability to provide relevant information in response to the research questions. [32].
Inclusion criteria consisted of: (a) third-year undergraduate students in Nursing (b) enrolled in Mental Health Nursing at a Spanish university. Students were selected because of their knowledge and exposure to clinical simulation in mental health. Participation was offered on a voluntary basis to all students. The total possible sample was 48 participants (n=48). Recruitment was carried out until data saturation was obtained. [33]
2.3. Data collection
To assess various perspectives, focus groups (FGs) were conducted during the simulation experiences, supplemented by researchers’ field notes and participants’ written reflective narratives. This qualitative approach to data collection allowed for a deeper and more contextualized understanding of the lived experiences during the simulations. The GFs provided a space for interaction among participants, facilitating the emergence of different opinions and perceptions. Researchers’ field notes, along with individual reflective narratives, added layers of understanding by capturing direct observations and personal perspectives. Data were collected between October and December 2023.
Each GF consisted of 10-11 participants, led by a moderator and an observer. Themoderator posed questions to which each participant responded by speaking in turn. The observer supported the moderator, identifying key points and taking notes. A topic guide was used, which was focused enough to collect information about the study area, yet open enough to stimulate discussion and interaction among participants (Table 1). However, data collection in qualitative studies is flexible; consequently, during the focus groups, the moderator asked about those areas of interest that participants raised in relation to the research question. [31,33] All FGs were audio- and video-recorded with the prior permission of the participants. The average duration of each FG was 49 minutes, with 4 focus groups being conducted, at which time no new information emerged from the data analysis.
In addition, the students who had participated in the simulation-based experience voluntarily made a written reflective narrative through the Moodle virtual campus answering the following open questions: How did you feel during the simulation? What difficulties did you encounter in dealing with the case? What aspects do you think are points for improvement and what did you learn from it? How do you think clinical simulation can help you in the management of the patient with suicidal crisis? Thirty-two reflective narratives were collected with a total of 11279 written words.
2.3.1. High Fidelity Simulation Procedure
The central objective of the simulation scenario was to train students in the approach, management and intervention in suicidal crisis. This training was carried out through experiences based on clinical mental health simulation, where students developed specific 199 nursing competencies to respond effectively to suicidal crisis situations. To this end, two high-fidelity clinical simulation scenarios were developed, taking into account the NANDA, NOC, NIC taxonomy related to each (Table 2). [34] Both the NIC taxonomy interventions and the nursing activities served as a guide to discuss the students’ performance during the debriefing phase. [17,35]
The actors who assumed the role of standardized patients were teachers specialized in mental health. They developed scripts and expertly impersonated various scenarios, providing participants with realistic and enriching experiences to enhance their clinical skills.
All clinical simulation sessions adhered to the Best Practices proposed by the International Association for Nursing Clinical Learning and Simulation (INACSL) throughout its four phases: [36] pre-briefing, briefing, development of the simulated scenario and debriefing. These phases were carried out and supervised by two university professors with experience in clinical simulation methodology. It is relevant to highlight that in the pre-briefing phase a psychologically safe context was fostered, according to the guidelines of Rudolph et al. [37] Likewise, in the debriefing phase it was carried out following the good judgment model, which allows participants to make mistakes and discuss them feeling valued and capable, and instructors, to show their experience and make constructive criticism, so that meaningful and reflective learning is promoted in which participants and instructors relate new experience and knowledge with the one they already possess. [37,38]
Through simulated scenarios, they learn to recognize warning signs, assess the level of risk and make the right decisions about necessary interventions. Regarding the encouragement of reflection and feedback done in debriefing, reflection is promoted and constructive feedback is provided. [39] At the same time, by using a safe environment, it allows for reflection and practice of mental health first aid. [40] This allows students to analyze their actions, identify areas for improvement, and understand how their interventions could impact real situations
2.4. Data analysis
Data collection was based on a full verbatim transcription of the researchers’ GFs and field notes, as well as students’ reflective narratives to open-ended questions posed on the virtual campus. The data were stored, managed, classified and organized with the help of the qualitative data analysis software ATLAS-ti 8.0. A thematic analysis was performed by identifying text fragments with relevant information to answer the research question. [41] From these narratives, the most descriptive contents (codes) were identified. Subsequently, these units were grouped by their common meaning (categories), and in turn into groups of thematic codes. Finally, the themes describing the participants’ experiences were identified. In this way, an explicit description of the students perceptions of the experience was obtained.
Three researchers, experts in qualitative research, developed the entire process of obtaining categories and subcategories independently, ending the process with the exchange of both and a consensus on the final decisions of the analysis. In case of divergence of opinions, the identification of the theme was based on consensus among the members of the research team.
2.5. Ethical considerations
Ethical authorization to conduct the research was obtained from the Research Ethics Committee of the Instituto de Investigación Sanitaria Fundación Jiménez Díaz (EOH040- 257 21_FJD). All participants gave written consent before participating in this study. To ensure anonymity and confidentiality, a code was assigned to each participant in the GFs and 259 reflective narratives E
2.6. Strictness criteria
The study was conducted in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ). [42] Data triangulation was applied among researchers involved in the analysis, and the analysis process was subject to review by independent researchers to ensure credibility. Transferability was ensured by detailed description of the research setting, as well as participants, context, and method. Confirmability was achieved by introducing variability in participants’ experiences; each researcher conducted the reading and analysis independently, contrasting and then reaching agreement on emerging themes and subthemes. [43]
3. Results
3.1. Demographic data
Of the total number of nursing students who met the criteria, 45 (93.8%) participated. Those participants who did not attend the simulation were due to different reasons such as lack of time, work shifts or other reasons. The majority of participants were female 41 (91.1%), compared to 8.9% who were male (8.9%). They ranged in age from 20-27 years (mean age = 21.3; SD = 2.29%). The discrepancy between students and genders is mainly due to the fact that the majority of students enrolled in the profession in Spanish universities are women. The participants belonged to the third year of nursing.
3.2. Themes
Three thematic blocks with their categories were identified: (a) management and handling of emotions (b) identification of the reasons for suicide (c) intervention.

Table 3.
Themes and categories.
| Themes (T) | Categories | |
|---|---|---|
| T 1 | Management and handling of emotions | Fear, uncertainty, empathy, trust, learning, specialty. |
| T 2 | Indicators of suicidal behavior | Risk factors and protective factors, precipitating factors of suicidal behavior, suicidal history, ambivalence. |
| T 3 | Suicidal crisis intervention | Establishment of the relationship, intervention strategies and alternatives. |
- Theme 1: Management and handling of emotions.
Participation generated palpable expectation and nervousness, indicating a significant emotional immersion: “I was expectant and nervous” E1.
The presence of uncertainty was highlighted as a challenging element, as participants recognized the lack of control over the situation:
“The uncertainty, isn’t it? Because in the end the situation doesn’t depend on you...”GF3
Some participants expressed a strong sense of empathy for the simulated patient:
“I don’t know... as if he was always telling bad things, you empathized a lot with him... and you said fuck... and you wanted to find something good for him to get out of that... out of that loop from which he wants to commit suicide... I don’t know...” GF2 “I have felt the desperation that they suffer, the inability to cope with situations”GF1
The presence of fear was highlighted, especially in relation to sensitive topics such as suicide “I felt fear because suicide seems to me a very important topic” E2. But just the simulation was revealed as an effective tool to overcome such fear, evidenced by statements indicating greater confidence and preparedness:
“My fear of these situations has been removed and I find myself much more prepared” E15 “I gained confidence by remembering the points explained earlier”E4
Even for some students it motivated them to consider specialization in mental health, demonstrating a positive impact on career aspirations. In some cases, there was a perceptual shift, with participants initially disinterested in mental health expressing renewed interest and enthusiasm.
“I have been very motivated thinking about the possibility of doing the mental health specialty” E27 “I thought I didn’t like mental health, but since the simulation it has caught my attention and I am really looking forward to it”E31
The simulation was perceived as a challenge that facilitated deep reflection, creating a meaningful bridge between academic theory and practical application:
“It has been challenging, helping us to reflect and having a link between theory and practice.”E20
“I have been able to learn the keys to interventions for these patients.”E22
The inclusion of real actors as patients was identified as a key factor in increasing the realism of the simulation in this type of patient. the student 19 added:
“It has been fundamental to have a real actor as a patient, it has made the simulation much more realistic” .(E19).
- Theme 2: Indicators of suicidal behavior.
In the reflective narratives provided by the participating students, the importance assigned to the identification of motives and factors related to patients who present suicidal intentions stands out. “It is important to identify the reasons why the person is in that situation” (E1). This statement is supported and enriched by the comments collected during the FGs. In one of the groups, various aspects that could contribute to the patient’s situation were explored:
“The economic issue, the family issue, the divorce issue, the relationship with the daughters, all these are risk factors”GF1.
This observation underscores the diversity of factors that students consider crucial to understanding the complexity of situations related to suicidal intent. Additionally, protective factors also emerged as key elements in the participants’ reflections:
“...it is an indicator, it is a protective factor the issue of beliefs”GF4.
This recognition suggests that students are not only focused on the risk aspects, but also value the identification of elements that can mitigate the risk of suicide in patients. Suicidal career experiences, according to participants’ narratives, are revealed as a complex cumulative process. One participant expressed:
“The suicidal career can be very varied, but such events accumulate that I accumulate and there comes a time when I can’t take it anymore and that drop is predisposed”GF3.
This story illustrates the multiplicity of events that, over time, can contribte to the development of suicidal ideation, emphasizing the importance of considering the cumulative process in assessment and intervention. In relation to family relationships, they provided additional insights into the ambivalence experienced by some participants. The complexity of family relationships was described, especially in the context of the maternal figure: 351
“The wife... the daughters... have been a bit ambivalent, right? At the beginning it seemed like... then it seemed like... with you it seemed like”(GF1). 354
The creation of ambivalence in decision making related to suicidal career was a recurring theme:
“Creating ambivalence yes it can be all and I at the end for them to decide and make that decision to take another path”GF2,
“Once the life hitch was identified, it has been easier to establish ambivalence”E9. 360
This finding highlights the complexity of psychological and emotional factors that may influence the final decision to take suicidal action, underscoring the need for specialized interventions focused on internal conflict resolution.
- Theme 3: Suicide crisis intervention.
As previously evidenced, students, through the simulation, have gained a deeper understanding of the necessary approach, as reflected in the statement:
“We have learned how the approach to the simulation should be, following the steps”(E12).
They recognize the importance of establishing a solid initial connection, as expressed by a GF participant:
“The connection, what’s the first thing to do? Hook up with the person, otherwise you’re not going to have anything”GF4.
This statement suggests an awareness of the proper sequence of steps to establish effective relationships. Creating an appropriate rapport is seen as essential to ensure the safety of both self and simulated patient.
“I introduced myself, tried to get him to talk to me and got down to his level”GF2.
Students believe that they have followed protocols to safeguard safety:
“I position myself as a safety measure to ensure that the person does not catch me at a given moment and throw me away, but I put myself at his or her level.
The intervention reveals the implementation of specific strategies
“My partners and I did a pretty thorough approach...using relaxation techniques...looking for alternatives”E4.
This approach suggests the practical application of therapeutic techniques and an active search for solutions. However, uncertainty and concern about the effectiveness of the strategies employed arises, as evidenced by the statement:
“Sometimes I’ve felt like it was like what the two partners said a little bit, you’re left kind of thinking I don’t know if what I’m going to say now is going to be impactful enough for me to pay attention”GF2.
The importance of offering viable alternatives is highlighted in both the individual narratives and the FGs. One participant noted:
“I think the main thing is to accompany them, listen to them and make them feel supported...give alternatives that we can give him because he himself is not seeing them”E5.
The need to provide concrete options and emotional support to the patient is emphasized. In addition, communication of the availability of other alternatives is evident.
“I told him that there were other alternatives to quitting that, even though he tried it once, it doesn’t mean it’s the only one, that he can try again”(GF3). 410
These results illustrate the complexity of the intervention, highlighting the importance of effective strategies and the consideration of various alternatives to address simulated mental health situations. Figure 1 allows establishing the following themes, 1. Management and handling of emotions which has five subthemes (Empathy, Uncertainty, Specialty, Fear, Learning). The second theme deals with indicators of suicidal behavior which has 5 subthemes (Learning, Ambivalences, Precipitating factors of suicidal behavior, Suicidal history and risk factors). The third theme deals with suicidal crisis interventions with five sub-themes (Alternatives, Intervention strategies, Uncertainty, Empathy and Learning). All of them are interrelated with each other and with the simulation using the ATLAS-Ti program, which according to the analysis may be influencing the suicidal risk presented.
4. Discussion
The aim of this study was to explore the perceptions of nursing students in relation to the approach, management and intervention in suicidal crisis through experiences based on mental health clinical simulation. The use of clinical simulation in the field of mental health nursing, especially in suicide crisis intervention and management, stands out as an innovative and essential pedagogical approach in student education, supported by previous studies. [44,45] The results of the study are aligned with previous research, evidencing that simulation experiences provide students with the unique opportunity to confront, manage, and make decisions in a controlled and safe environment, contributing significantly to improving their confidence and competence in suicidal crisis intervention. [30] The development of fundamental skills, such as meaningful connection with patients through the practice of active listening, empathy, and effective use of verbal and nonverbal language, was highlighted as a crucial aspect of establishing therapeutic relationships and providing support to people in suicidal crisis. [18,46] Likewise, the identification and assessment of risks and warning signs during the simulation allowed students to effectively assess risk factors associated with suicide, consolidating their preparedness for real situations. [24]
In relation to the identification of motives for suicide, the importance that participants assigned to understanding the underlying reasons for suicidal intentions is highlighted. The identification of protective factors was also recognized as crucial, evidencing the students’ balanced perspective by not focusing exclusively on risk aspects. In addition, the notion of the suicidal career as a complex cumulative process was explored, highlighting the importance of considering development over time in assessment and intervention. The results reveal a mindful, multidimensional approach toward identifying motives and factors in patients with suicidal intent, as well as a deep understanding of the importance of establishing a strong initial connection. These results comprehensively inform the importance of a thorough assessment and consideration of various elements in clinical practice and health professional training. They highlight the importance of simulations in the training of mental health professionals, [47] not only for their ability to develop practical skills, but also for their influence on participants’ personal perceptions and career aspirations. The inclusion of emotional elements and contextual realism emerge as key elements in maximizing the positive impact of simulations on professional development. This is in line with studies indicating that simulated patient training using actors allows realism to be achieved in different pathological situations and represents a resource for improving educational interventions in new situations. [48,49]
With respect to suicide crisis intervention, participants gained a deeper understanding of the approach needed through simulation. The importance of establishing a strong initial connection was recognized as critical, indicating an awareness of the proper sequence of steps to establish effective relationships. The implementation of specific strategies, such as the use of relaxation techniques and active solution finding, illustrates the practical application of therapeutic approaches. However, uncertainty about the effectiveness of these strategies was also apparent, highlighting the need to continue to develop intervention skills on an ongoing basis in students. [16] The management and regulation of emotions during the simulations emerges as a deeply immersive experience for the participants, marked by the presence of expectation, nervousness and even fear, underlining the intensity of the simulated situations. Despite the acknowledged uncertainty and sense of lack of control, the simulation reveals itself as an effective tool for overcoming fear, evidenced by an increase in confidence and a sense of preparedness. [10] It is noteworthy to observe that, although students verbalize having experienced the simulated situations as real, facing challenges in a controlled environment strengthens their ability to handle crises more safely and effectively in professional life. [50]
Therefore, the results of this study highlight the satisfaction of nursing students with the simulation experience in suicidal crisis management. Beyond their improved competencies and confidence, the simulation has had a transformative impact on the participants’ career aspirations, motivating them to consider specialization in mental health. This perceptual shift involves not only a deeper appreciation of the complexity of suicide crisis intervention, but also overcoming previous stigmas associated with mental health. [51] Thus, simulation emerges not only as an effective tool for practical training, but also as a positive catalyst in the perception and approach of future nursing professionals to the vital area of mental health.
5. Strengths and limitations of the study
The fundamental strengths of this study lie in the fact that our research provides an innovative perspective on the need to transform the traditional university teaching model, advocating the creation of new realistic scenarios for the acquisition of knowledge. Another strength of the study is the training offered to nursing students prior to their entry into the workplace, which provides a solid knowledge base for their future practice, while strengthening their confidence in managing patients at risk of suicide.
Regarding the limitations of the study, it was carried out with nursing students from a Spanish university. Therefore, the results cannot be generalized to other nursing students from other universities. The present study reflects the perceptions of nursing students in different high-fidelity clinical simulation scenarios based on a patient at risk of suicide. It is of interest to extend the qualitative study on a larger scale with new scenarios of clinical mental health cases in simulation and associated studies with quantitative methodology to evaluate the degree of effectiveness of the educational intervention.
6. Conclusions
The results of this study indicate that nursing students face challenges in approaching clinical mental health simulation due to lack of prior exposure. Simulation in suicide intervention is presented as an effective tool to overcome these difficulties by providing a controlled environment. The results show that, despite initial insecurity, students experience a positive change in their attitudes, expressing greater interest in the mental health specialty and reducing the associated stigma. In conclusion, clinical simulation not only improves skills, but also contributes significantly to changing perceptions towards mental health.
Author Contributions
Conceptualization, Pablo Del Pozo-Herce, Alberto Tovar-Reinoso, Antonio Martínez-Sabater, Elena Chover-Sierra, Raúl Juárez-Vela and Eva García-Carpintero-Blas; Data curation, Teresa Pacheco-Tabuenca, Silvia González-Fernán and Iván Santolalla-Arnedo; Formal analysis, Pablo Del Pozo-Herce, Alberto Tovar-Reinoso, Teresa Pacheco-Tabuenca and Jorge Carrasco-Yubero; Funding acquisition, Elena Chover-Sierra; Investigation, Pablo Del Pozo-Herce, Elena Chover-Sierra and Teresa Pacheco-Tabuenca; Methodology, Pablo Del Pozo-Herce, Jorge Carrasco-Yubero and Raúl Juárez-Vela; Project administration, Pablo Del Pozo-Herce, Elena Chover-Sierra and Raúl Juárez-Vela; Resources, Alberto Tovar-Reinoso, Antonio Martínez-Sabater and Juan Luis Sánchez-González; Software, Antonio Martínez-Sabater, Elena Chover-Sierra, Teresa Pacheco-Tabuenca and Juan Luis Sánchez-González; Supervision, Antonio Martínez-Sabater, Teresa Pacheco-Tabuenca, Teresa Sufrate-Sorzano, Raúl Juárez-Vela and Eva García-Carpintero-Blas; Validation, Antonio Martínez-Sabater, Teresa Pacheco-Tabuenca and Jorge Carrasco-Yubero; Visualization, Juan Luis Sánchez-González and Raúl Juárez-Vela; Writing – original draft, Pablo Del Pozo-Herce and Antonio Martínez-Sabater; Writing – review & editing, Alberto Tovar-Reinoso, Elena Chover-Sierra, Juan Luis Sánchez-González, Silvia González-Fernán, Iván Santolalla-Arnedo, Teresa Sufrate-Sorzano, Raúl Juárez-Vela and Eva García-Carpintero-Blas.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Instituto de Investigación Sanitaria Fundación Jiménez Díaz (protocol code EOH040-21_FJD).
Informed Consent Statement
Informed consent was obtained from all student nurses involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
The authors acknowledge all the students who took part in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Suicide mortality data. 2021. Available online: https://www.who.int/es/news-room/fact-sheets/detail/suicide.
- Sufrate-Sorzano, T. Suicide prevention from the classroom. Nursing interventions and tools for suicide prevention: Activity book. Siníndice. 2021. Spain.
- Harmer, B.; Lee, S.; Duong, T.V.H.; Saadabadi, A. Suicidal Ideation. Stat Pearls [Internet]. Treasure Island (FL): StatPearls Publishing. 2024.
- Echávarri-Gorricho, A. Concept and classification of suicidal behavior. 2010. Available online: ftp.formainap.navarra.es/2014/2014-3E604-9971-SUICIDIO/TEMA%201.pdf.
- Hernández-Bello, L.; Hueso-Montoro, C.; Gómez-Urquiza, J.L.; Cogollo-Milanés, Z. Prevalence and associated factor for ideation and suicide attempt in adolescents: A systematic review. Rev Esp Public Health. 2020, 10, 94. [Google Scholar]
- National Institute of Statistics. Deaths from causes, gender and age groups. 2020. Available online: https://www.ine.es/jaxiT3/Datos.htm?t=7947 (accessed on 15 November 2023).
- Spanish Foundation for Suicide Prevention. Suicide Observatory in Spain. 2022 [online]. Available online: https://www.fsme.es/observatorio-del-suicidio-2022-definitivo/ (accessed on 18 December 2023).
- Darnell, D.; Areán, P.A.; Dorsey, S.; Atkins, D.C.; Tanana, M.J.; Hirsch, T.; Mooney, S.D.; Boudreaux, E.D.; Comtois, K.A. Harnessing Innovative Technologies to Train Nurses in Suicide Safety Planning With Hospitalized Patients: Protocol for Formative and Pilot Feasibility Research. JMIR Res Protoc. 2021, 15, 10. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. 72nd World Health Assembly. 2019. Available online: https://apps.who.int/gb/ebwha/pdf_files/WHA72/A72_11Rev1-sp.pdf.
- Heyman, I.; Webster, B.J.; Tee, S. Curriculum development through understanding the student nurse experience of suicide intervention education--A phenomenographic study. Nurse Educ Pract. 2015, 15, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Motillon-Toudic, C.; Walter, M.; Séguin, M.; Carrier, J.D.; Berrouiguet, S.; Lemey, C. Social isolation and suicide risk: Literature review and perspectives. Eur. Psychiatry. 2022, 65, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Oexle, N.; Rüsch, N. Stigma—Risk factor and consequence of suicidal behavior: Implications for suicide prevention. Nervenarzt. 2018, 89, 779–783. [Google Scholar] [CrossRef] [PubMed]
- Menon, V.; Vijayakumar, L. Interventions for attempted suicide. Curr Opin Psychiatry. 2022, 1, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Farmani, A.; Rahimianbougar, M.; Mohammadi, Y.; Faramarzi, H.; Khodarahimi, S.; Nahaboo, S. Psychological, Structural, Social and Economic Determinants of Suicide Attempt: Risk Assessment and Decision Making Strategies. Omega. 2023, 86, 1144–1166. [Google Scholar] [CrossRef]
- Beghi, M.; Butera, E.; Cerri, C.G.; Cornaggia, C.M.; Febbo, F.; Mollica, A.; Berardino, G.; Piscitelli, D.; Resta, E.; Logroscino, G.; Daniele, A.; et al. Suicidal behaviour in older age: A systematic review of risk factors associated to suicide attempts and completed suicides. Neurosci Biobehav Rev. 2021, 127, 193–211. [Google Scholar] [CrossRef]
- Ferrara, P.; Terzoni, S.; Ruta, F.; Poggi, A.D.; Destrebecq, A.; Gambini, O.; D’agostino, A. Nursing students’ attitudes towards suicide and suicidal patients: A multicentre cross-sectional survey. Nurse Educ Today. 2022, 109, 105258. [Google Scholar] [CrossRef]
- Sufrate-Sorzano, T.; Juárez-Vela, R.; Ramírez-Torres, C.A.; Rivera-Sanz, F.; Garrote-Camara, M.E.; Roland, P.P.; Gea-Sánchez, M.; Del Pozo-Herce, P.; Gea-Caballero, V.; Angulo-Nalda, B.; et al. Nursing interventions of choice for the prevention and treatment of suicidal behaviour: The umbrella review protocol. Nurs Open. 2022, 9, 845–850. [Google Scholar] [CrossRef]
- Richard, O.; Jollant, F.; Billon, G.; Attoe, C.; Vodovar, D.; Piot, M.A. Simulation training in suicide risk assessment and intervention: A systematic review and meta-analysis. Medical Educ. online. 2023, 28, 2199469. [Google Scholar] [CrossRef] [PubMed]
- Vannoy, S.D.; Fancher, T.; Meltvedt, C.; Unützer, J.; Duberstein, P.; Kravitz, R.L. Suicide inquiry in primary care: Creating context, inquiring, and following up. Ann Fam Med. 2010, 8, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Hawgood, J.; Woodward, A.; Quinnett, P.; De Leo, D. Gatekeeper Training and Minimum Standards of Competency. Crisis. 2022, 43, 516–522. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.H.M.; Fuxman, S.; Humm, L.; Tirone, N.; Pires, W.J.; Cole, A.; Goldstein, G.J. Suicide risk assessment training using an online virtual patient simulation. mHealth. 2019, 5, 31. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.; Smith, A.R.; Dodd, D.R.; Covington, D.W.; Joiner, T.E. Suicide-Related Knowledge and Confidence Among Behavioral Health Care Staff in Seven States. Psychiatr Serv. 2016, 67, 1240–1245. [Google Scholar] [CrossRef] [PubMed]
- Silverman, M.M.; Berman, A.L. Suicide risk assessment and risk formulation part I: A focus on suicide ideation in assessing suicide risk. Suicide Life Threat Behav. 2014, 44, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Goh, Y.S.; Selvarajan, S.; Chng, M.L.; Tan, C.S.; Yobas, P. Using standardized patients in enhancing undergraduate students’ learning experience in mental health nursing. Nurse Educ. today. 2016, 45, 167–172. [Google Scholar] [CrossRef]
- Lilly, M.L.; Hermans, M.; Crawley, B. Psychiatric nursing emergency: A simulated experience of a wrist-cutting suicide attempt. J psychosoc nurs ment health serv. 2012, 50, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Keltner, N.L.; Grant, J.S.; McLernon, D. Use of actors as standardized psychiatric patients. J psychosoc nurs ment health serv. 2011, 49, 34–40. [Google Scholar] [CrossRef]
- Piot, M.A.; Attoe, C.; Billon, G.; Cross, S.; Rethans, J.J.; Falissard, B. Simulation Training in Psychiatry for Medical Education: A Review. Front. Psychiatry. 2021, 12, 658967. [Google Scholar] [CrossRef]
- Vallance, A.K.; Hemani, A.; Fernandez, V.; Livingstone, D.; McCusker, K.; Toro-Troconis, M. Using virtual worlds for role 613 play simulation in child and adolescent psychiatry: An evaluation study. Psychiatr Bull. 2014, 38, 204–210. [Google Scholar] [CrossRef]
- O’Brien, K.H.M.; Quinlan, K.; Humm, L.; Cole, A.; Pires, W.J.; Jacobs, A.; Goldstein-Grumet, J. A qualitative study of 616 provider feedback on the feasibility and acceptability of virtual patient simulations for suicide prevention training. Mhealth. 617 2022, 30, 31. [Google Scholar] [CrossRef]
- Phillips, E.C.; Neagle, G.; Cameron, B.; Moneypenny, M. It’s okay to talk: Suicide awareness simulation. Clin Teach. 2019, 16, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Korstjens, I.; Moser, A. Series: Practical guidance to qualitative research. Part 2: Context, research questions and designs. Eur J Gen Pract. 2017, 23, 274–279. [Google Scholar] [CrossRef]
- Creswell, J.W.; Poth, C.N. Qualitative inquiry and research design. Choosing among five approaches. 4th ed. Thousand Oaks, CA: Sage. 2018.
- Moser, A.; Korstjens, I. Series: Practical guidance to qualitative research. Part 3: Sampling, data collection and analysis. Eur J gen Pract. 2018, 24, 9–18. [Google Scholar] [CrossRef]
- 34. Nanda International, NANDA. Nursing diagnoses: Definitions and classification 2018–2020. Elsevier, 2019.
- Butcher, H.K.; Bulechek, G.M.; Dochterman, J.M.; Wagner, C.M. Nursing Interventions Classification (NIC); Elsevier. 2018. St. Louis, MO, USA.
- Sittner, B.J.; Aebersold, M.L.; Paige, J.B.; Graham, L.L.; Schram, A.P.; Decker, S.I.; Lioce, L. INACSL Standards of Best Practice for Simulation: Past, Present, and Future. Nur educ perspect. 2015, 36, 294–298. [Google Scholar] [CrossRef]
- Rudolph, J.W.; Raemer, D.B.; Simon, R. Establishing a safe container for learning in simulation: The role of the presimulation briefing. Simul Healthc. 2014, 9, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Maestre, J.M.; Rudolph, J.W. Theories and styles of debriefing: The good judgment method as a tool for formative assessment in healthcare. Rev Esp Cardiol. 2015, 68, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Kirkbakk-Fjær, K.; Hedelin, B.; Moen, Ø.L. Undergraduate Nursing Students’ Evaluation of the Debriefing Phase in Mental Health Nursing Simulation. Issues Ment Health Nurs. 2016, 37, 360–366. [Google Scholar] [CrossRef]
- Ng, R.; O’Reilly, C.L.; Collins, J.C.; Roennfeldt, H.; McMillan, S.S.; Wheeler, A.J.; El-Den, S. Mental Health First Aid crisis 649 role-plays between pharmacists and simulated patients with lived experience: A thematic analysis of debriefing. Soc 650 Psychiatry Psychiatr Epidemiol. 2023, 58, 1365–1373. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. What can “thematic analysis” offer health and wellbeing researchers? Int J Qualitative Stud Health Well-being. 2014, 9, 26153. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Morse, J.M. Critical Analysis of Strategies for Determining Rigor in Qualitative Inquiry. Qual Health Res. 2015, 25, 1212–1222. [Google Scholar] [CrossRef] [PubMed]
- Soccio, D.A. Effectiveness of Mental Health Simulation in Replacing Traditional Clinical Hours in Baccalaureate Nursing Education. J. Psychosoc. Nurs. Ment Health Serv. 2017, 55, 36–43. [Google Scholar] [CrossRef] [PubMed]
- McGough, S.; Heslop, K. Developing Mental Health-Related Simulation Activities for an Australian Undergraduate Nursing Curriculum. J. Nurs. Educ. 2021, 60, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Simonelli-Muñoz, A.J.; Jiménez-Rodríguez, D.; Arrogante, O.; Plaza Del Pino, F.J.; Gallego-Gómez, J.I. Breaking the Stigma 668 in Mental Health Nursing through High-Fidelity Simulation Training. Nurs. Rep. 2023, 13, 1593–1606.669. [Google Scholar] [CrossRef]
- Lilly, M.L.; Hermanns, M.; Crawley, B. Clinical Simulation in Psychiatric-Mental Health Nursing: Post-Graduation Follow Up. J. Psychosoc. Nurs. Ment Health Serv. 2016, 54, 40–46. [Google Scholar] [CrossRef]
- Koch, C.; Meier, S.; Fischer, C.; Brich, J. Simulated patients to demonstrate common stroke syndromes: Accurate and convincing. Cerebrovasc Dis. 2023, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lawton, A.J.; Greco, L.; Airaldi, R.; Tulsky, J.A. Development of an Actor Rehearsal Guide for Communication Skills Courses. BMJ Palliat Care. 2024. [Google Scholar] [CrossRef]
- Godzik, C.M.; Solomon, J.; Yacinthus, B. Using standardized mental health patient simulations to increase critical thinking and confidence in undergraduate nursing students. Arch. Psychiatr. 2023, 43, 76–80. [Google Scholar] [CrossRef]
- Öz, F.; Turgut, A.N.; Meriç, M. Nursing student’s attitudes toward death and stigma toward individuals who attempt suicide. Perspect Psychiatr Care. 2022, 58, 1728–1735. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Qualitative Data Analysis.
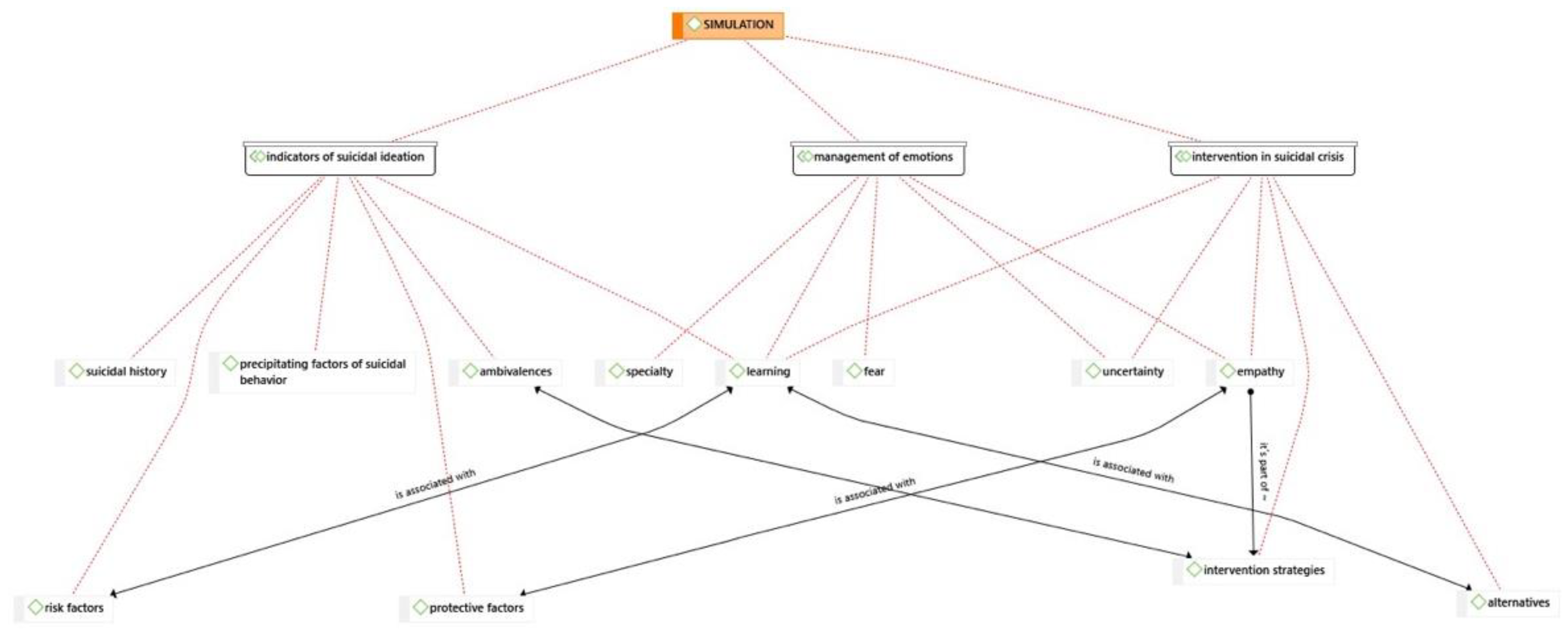
Table 1.
Interview Guide.
| Post-Clinical simulation phase |
|
Table 2.
Scheme imulated scenario, NANDA-I (NANDA-I Taxonomy) Nursing Interventions Classification (NIC) and outcomes (NOC) and related nursing activities for resolution.
Table 2.
Scheme imulated scenario, NANDA-I (NANDA-I Taxonomy) Nursing Interventions Classification (NIC) and outcomes (NOC) and related nursing activities for resolution.
| Simulated Scenario 1 | NANDA | NIC Intervention |
NOC Outcomes |
Nursing Activities |
|---|---|---|---|---|
| 34-year-old male, who on our arrival was on the M-40 bridge. He presented suicidal ideation and intention to jump. As background, he refers to an argument with his wife, he has two daughters that he has not seen for some time, cocaine consumption and his van broke down just today when he was going to deliver an order. There is no one else on the bridge, only you (nursing students). You are the first to intervene and establish the first contact with the person. |
(00150) Suicide risk |
(6486) Environmental management: Safety (4500) Prevention of substance abuse (6340) Suicide prevention |
(1408) Self-control of suicidal impulses (1904) Risk management: drug use |
|
| Simulated Scenario 2 |
NIC Intervention |
NOC Outcomes |
Nursing Activities | |
| Middle-aged man threatening to take his own life on the viaduct in Segovia (Madrid). No further information is available at the Emergency Service Center. You arrive as the first unit to intervene. When you arrive, the person is at high risk of suicide, as he is attached to a railing on the outside of the bridge. It is you (nursing students) who make the first contact. | (00124) Despair (00150) Suicide risk |
(5230) Increasing coping (5270) Emotional support (4920) Active Listening (6654) Surveillance: security |
(1302) Coping with problems (1305) Psychosocial modification: life change |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



