
Preprint
Review
Lung Microbiota and Ventilator‐Associated Pneumonia in the Neonatal Period
Altmetrics
Downloads
139
Views
52
Comments
0
A peer-reviewed article of this preprint also exists.


This version is not peer-reviewed
Submitted:
31 January 2024
Posted:
01 February 2024
You are already at the latest version
Alerts
Abstract
The lung microbiota is a complex community of microorganisms that colonize the respiratory tract of individuals from or even before birth. Although the lungs were traditionally believed to be sterile, recent research has shown that there is a diversity of bacterial species in the respiratory system. Knowledge about the lung microbiota in the newborn and its relationship with bacterial infections is of vital importance to understand the pathogenesis of respiratory diseases in neona-tal patients undergoing mechanical ventilation. In this article, the current evidence on the compo-sition of the lung microbiota in the newborn will be reviewed, as well as its role in the develop-ment of bacterial infections in mechanically ventilated neonates. Although advances in many as-pects of the neonatal intensive care unit care have significantly improved the survival of preterm infants, the diagnosis and treatment of ventilator-associated pneumonia has not progressed in recent decades. Avoiding dysbiosis caused by inappropriate use of antibiotics around birth, as well as avoiding intubation of patients or promoting early removal of endotracheal tubes are among the most important preventive measures for ventilator-associated pneumonia. The use of probiotics and prebiotics to prevent infectious, allergic or metabolic complications in the short or long term constitutes a very important field of research in perinatal medicine.
Keywords:
Subject: Medicine and Pharmacology - Pediatrics, Perinatology and Child Health
1. Introduction
In adults, it is estimated that the most common healthcare-related infection is pneumonia, with approximately a third of cases being related to mechanical ventilation [1]. Although mortality attributable to ventilator-associated pneumonia (VAP) is difficult to establish, it seems clear that this complication is accompanied by an increase in the duration of mechanical ventilation and the length of stay of patients in the Intensive Care Units (ICU) [2]. However, the concept of VAP is complex and difficult to establish in clinical practice, which makes it difficult to standardize criteria and generalize them so that they are useful in clinical decision making, as well as for benchmarking purposes and in research, especially epidemiological research. Traditionally, clinical, radiological and microbiological criteria have been used in adults, such as those of the North American Centers for Disease Control and Prevention (CDC) [3]. However, its application in the neonatal period is not simple and there are not many quality studies that have validated its usefulness [4].
In the last decades, recent advances in laboratory technology, made us witness a shift of paradigm. The lung, long considered a sterile organ, has turned out to have its own microbiota that is established from the moment of birth, or even before. Under normal and balanced conditions it seems to protect the health of the individual. On the contrary, alterations in the normal colonization process could be the origin of different pathologies, both in the short and long term, in later stages of life. The development of metagenomics, that is the study of the structure and function of entire nucleotide sequences isolated and analyzed from all the organisms, typically microbes such as those residing on human skin, gut, lungs, etc., has provided us with information about the functional characteristics of a given microbial community. It allows to obtain genomic sequences of microorganisms without the need to cultivate them, extracting and analyzing their DNA without previous amplification. Techniques have been developed to exclude dead bacteria and avoid biased results, amplifying the DNA of the viable ones. However, it should be noted that bacterial viability is not required to induce or propagate inflammatory responses, so the identification of non-viable bacteria could also be clinically relevant [5]. All this has led to a change of direction in microbiology due to its high performance and relatively low cost. Knowledge of the bacterial influence on cellular functioning in their corresponding niches may allow the development of new and promising therapies. A comprehensive overview of the evolution of culture-based microbiological techniques toward culture-independent DNA sequencing techniques is beyond the scope of this review. For a detailed study of it, as well as to become familiar with all the related terminology (transcriptome, proteome, metabolome, etc.), see Sherman MP, et al. [6].
2. The Lung Microbiota and Microbiome
The microbiota is the set of live microorganisms that develop in a specific environment and can be commensal, symbiotic or pathogenic. It is estimated that the human body has a similar number of eukaryotic cells and microorganisms, most of which are found in the intestine, skin and oral cavity [7]. In turn, we use the term microbiome to refer to the complete set of microorganisms, their genes, and their biomolecules in a certain environment [8]. This could be highly variable depending on the geographical location, age, health status, etc. [9]. Alterations in the microbiome are called “dysbiosis” and this situation can be associated with significant alterations in the individual’s health status [10]. As a general rule, it is accepted that greater diversity in the microbiota is related to greater chances of health, while its reduction could favor the development of diseases through various mechanisms. Diversity describes the number of different taxa within a community. In turn, the microbial variation in a sample is called “α diversity”, while the variation in microbial communities between samples is called “β diversity” [11,12].
The process of lung colonization in the newborn is not fully understood. Technical and even ethical difficulties have prevented its study in detail [4]. Saprophytic or commensal bacteria that usually colonize different human organs are not usually isolated in conventional cultures and, therefore, their study has been elusive until the arrival of new DNA sequencing and transcriptomics methods, such as the sequencing of the variable regions of the 16S ribosomal RNA gene (16S-rRNA), the gene most frequently used for bacterial identification. On the other hand, access to proximal anatomical areas, such as the nasopharyngeal or oropharyngeal cavity, the anorectal tract or the vagina, is relatively simple. However, access to the distal airway without contamination by agents located in more proximal locations has always been a great challenge, mostly in the smaller patients, such as the neonate. For this reason, the lungs were not initially included in the human microbiome project [13].
It is generally accepted that colonization patterns in the newborn differ depending on the route of delivery [14], with the lung microbiota being more diverse in those born vaginally than in those born by cesarean section. Furthermore, the predominant microbiota in babies born vaginally, both in the intestine and in the lungs, is usually related to the mother’s vaginal microbiota, while in babies born by cesarean section follows the mother’s skin microbiota pattern. Other studies show, however, that pulmonary colonization of the newborn could begin already in the womb [15,16,17], although there is also some controversy [18]. Of note, Lal et al. showed similar microbiomes in the respiratory tract of newborns delivered vaginally or by cesarean section, suggesting an acquisition of microbial DNA likely through the placenta [11]. Interestingly, this study also showed an established and similar respiratory microbiome at birth in preterm and full-term infants. Differences in methodology or target populations are probably the basis for these discrepancies. In any case the debate continues. Now there is growing belief that there is an intrauterine microbiota that influences fetal programming and development [19] and it may be related to preterm birth and neonatal respiratory diseases [20]. Furthermore, it is widely accepted that the composition of the newborn’s lung microbiota is dynamic and changes under local selective pressures, but also with age, the environment, the type of diet, presence of stress, etc. A large proportion of neonates are exposed to antibiotics administered to their mothers as prophylaxis against group B streptococcal disease, chorioamnionitis, premature rupture of membranes, etc. [21]. Many of them also continue to receive empiric antibiotics, such as ampicillin and gentamicin [22], after birth. Although these interventions may be instrumental in reducing infant mortality, they may also have adverse effects on the microbiota in the short and long term [23].
Currently, the concept of the intestinal-pulmonary axis is gaining more and more interest and relevance [24,25,26]. Some studies suggest initial oropharyngeal and digestive colonization, with the respiratory system secondarily colonized by descending route or microaspirations [27]. In addition to a direct role in terms of the characteristics and variety of the microbiota of both organs or systems, there is evidence of a remote immunomodulatory effect through certain micrometabolites produced by intestinal bacteria [28]. Bacterial fermentation of dietary fibers generates metabolic products that act as local and systemic signaling molecules helping to maintain immune and tissue homeostasis. Among the most studied, short chain fatty acids (SCFA) exert immunomodulatory functions in the bone marrow, influencing immune cells generation and development [29]. Furthermore, the gut microbiota possesses a metabolic capacity that the human gastrointestinal tract has not, providing the host with additional nutrients and energy [30]. Colonic anaerobiosis is essential for the growth of a balanced community of SCFA-producing microbiota mainly from the phyla Firmicutes and Bacteroidetes, and prevents the growth of dysbiotic bacterial communities, such as Proteobacteria [31].
On the other hand, some studies have related the use of H2 blockers with changes in the microbiota, both intestinal and respiratory, and this was clinically associated with an increased risk of late onset sepsis, necrotizing enterocolitis and pneumonia [32]. In fact, the use of probiotics and prebiotics has been proposed to prevent these complications, but so far the low to moderate evidence on their effects together with the potential associated morbidity and mortality in very or extremely preterm neonates makes it necessary more large, high-quality clinical trials to provide evidence of the validity and applicability of such interventions [33]. In addition to modifying the susceptibility to certain infections, it is likely that the airway microbiota also influences the structural development of the lung at critical moments [34]. Finally, the interaction between the intestine and the lungs could be in both directions. Respiratory viral infections, such as respiratory syncytial virus or influenza, could alter the intestinal microbiota [35], increasing the risk of subsequent enteric infection [36], while influenza-induced intestinal microbial changes increase the susceptibility to secondary pneumococcal infection [37].
Regarding the type of organisms colonizing the respiratory tract, once again, the studies are methodologically diverse and there is no absolute certainty regarding what the “normal” microbiota is in a healthy newborn. Nevertheless, it is generally accepted that the most favorable microbiome would be the one produced after a vaginal birth and the baby is breastfed by his own mother [38]. However, it is also recognized that there may be great interindividual variability [39]. The bacterial phyla and genera most frequently present in the human microbiota, both in health and disease, are summarized in Table 1. In healthy adults, the most frequently found bacteria correspond to the phylum Bacteroidetes, especially the genus Prevotella, and the phylum Firmicutes, mainly the genera Streptococcus and Veillonella [40].
In the upper airways of healthy full-term newborns, large numbers of Staphylococcus spp., and later Corynebacterium spp., and Dolosigranulum spp., can be found during the first week of life, which is associated with greater stability of the bacterial community and good respiratory health. These saprophytic bacteria can inhibit the growth of Staphylococcus aureus and Streptococcus pneumoniae, probably through the production of certain antimicrobial peptides [41]. In contrast, in babies born by cesarean section, Staphylococcus aureus persists, and anaerobes appear, including Prevotella, Veillonella, and Porphyromonas spp. [42]. On the other hand, as mentioned above, breastfeeding protects against infections, either through the transmission of antibodies [43], or protective microorganisms, such as Bifidobacterium spp. or Lactobacillus spp. [44], along with certain oligosaccharides that favor their development [45]. On the contrary, the use of antibiotics can lead to a decrease in beneficial bacteria, such as Dolosigranulum spp. and Corynebacterium spp., and a higher proportion of potential pathogens such as Haemophilus, Streptococcus and Moraxella [46], increasing the risk of respiratory tract infections [47], and even bacterial resistance in the long term [48]. For a more in-depth discussion of the mechanisms that contribute to the establishment of a healthy respiratory microbiota, and the specific host-microbiota interactions that support it, as well as the interrelationship between bacteria, or between bacteria and viruses (virome) or fungi (mycobiome) also present in the human body, see the interesting and comprehensive review by Man WH et al. [49].

Table 1.
Main phyla and genera of bacteria in the human microbiome, some of them present in human milk (Adapted from Jeurink PV, et al. [44]).
Table 1.
Main phyla and genera of bacteria in the human microbiome, some of them present in human milk (Adapted from Jeurink PV, et al. [44]).
| Phyla | Actinobacteria | Bacteroidetes | Firmicutes | Proteobacteria | Tenericutes | Verrucomicrobia |
|---|---|---|---|---|---|---|
| Genus |
Bifidobacterium Corynebacterium Dermatobacter Kocuria Mycobacterium Parascovia Propionibacterium Rothia |
Bacteroides Prevotella Porphyromonas Rikenella |
Bacillus Clostridium Dolosigranulum Enterococcus Lactobacillus Leuconostoc Pediococcus Staphylococcus Streptococcus Veillonella Weisella |
Acinetobacter Bradyrhizobiaceae Burkholderia Escherichia Haemophilus Helicobacter Moraxella Neisseria Novosphingobium Pateurella Pseudomonas Ralstonia Salmonella Serratia Sphingobium Sphingomonas Sphingopyxis |
Mycoplasma Ureaplasma |
Akkermansia |
In premature babies at risk of bronchopulmonary dysplasia, bronchial aspirates showed an increase in pathogens such as Staphylococcus aureus, Pseudomonas aeruginosa and Streptococcus spp. [50], or Ureaplasma spp. [51]. It has also been suggested that bacterial diversity in intubated patients decreases during antibiotic treatment [52]. This could increase the development of pneumonia due to resistant pathogens that may be present in biofilms that develop in endotracheal tubes [53]. On the other hand, the communication mechanisms between cells and tissues in an organism, at various levels (hormones, neurotransmitters, citokines, etc.) can produce cross-talk with the world of microbes [54]. This knowledge has led to the development of the “microbial endocrinology” [55]. An example of these interactions could be the significant growth demonstrated in vitro of Pseudomonas aeruginosa in the presence of catecholamines (norepinephrine and dopamine) [56]. However, to date, no study has evaluated whether exogenous catecholamines independently influence the lung microbiome.
In any case, accurately specifying the source of the microbiota in the newborn, as well as its evolution as the individual develops and is exposed to other environmental factors, would require detailed sequencing of the genome of organisms from multiple locations, not only from the newborn itself, but also from the birth canal, the mother skin and breast milk, the skin of the health personnel who assist the birth, the ecology of the units where patients are admitted, etc. [57].
3. Ventilator-Associate Pneumonia (VAP)
3.1. Definition and Epidemiology
VAP is an inflammation of the lung produced by infectious agents that were not present or in incubation when the patient was started on mechanical ventilation (MV). Clinically it is defined as a nosocomial lung infection diagnosed in patients undergoing MV for at least 48 hours. It is considered the second most common cause of nosocomial infection in neonatal and pediatric intensive care patients. It is estimated that its incidence ranges between 1 and 63 episodes per 1,000 days of ventilation depending on the degree of development of the countries [58]. Apart from differences in patients and units characteristics, this variability could also be explained by the use of different diagnostic criteria to define VAP. Among the factors that favor abnormal bacterial colonization and lung infections in the newborn are, apart from the immaturity of the patient’s immune system, pre and postnatal malnutrition, naso- or orotracheal intubation and reintubations and, above all, the duration of mechanical ventilation, the use of previous antibiotics, and the environmental ecology of the units [59,60]. Of all of them, prolonged intubation is the one that has been most independently associated with the appearance of VAP [61]. Intubation alters the natural lung defense mechanisms, such as ciliary movements to clear mucus or coughing. Furthermore, tubes surpass the glottis and the larynx, connecting the oropharynx with the pulmonary ecosystem, altering the abundance and composition of the microbiota. Bacterial biofilms formed on the walls of the tubes protect them from antibiotics and the immune system [62].
According to the CDC, VAP is identified through a combination of imaging, clinical, and laboratory criteria, and it is considered ventilator-associated when the patient is on mechanical ventilation for > 2 consecutive days at the time of the event, and the ventilator was in place on the day of the event or the day before [3]. Table 2 is an adaptation of the CDC clinical and radiological criteria for patients ≤ 12 months of age. This criteria allow the diagnosis of “clinically defined pneumonia” even without pathogen isolation, given the difficulty in obtaining uncontaminated samples from the respiratory tract of infants. However, some authors have emphasized the importance of microbiological diagnosis to avoid overdiagnosis of VAP and excessive use of antibiotics [63]. On the contrary, the isolation of pathogens without clinical and radiological signs could simply represent a colonization of the respiratory tract. In short, the current CDC definitions are not specific for the neonatal population and even less so for the group of very-low-birth-weight (VLBW) infants. Isolated positive tracheal culture alone does not distinguish between bacterial colonization and respiratory infection. Clinical and laboratory signs are generally nonspecific and may correspond to other conditions such as bronchopulmonary dysplasia and nosocomial sepsis. Radiological reports in infants with airway colonization without definitive clinical and laboratory evidence of infection could be misleading [64]. All of this reflects the difficulty in establishing homogeneous and universal diagnostic criteria for neonatal VAP. The inter-observer variability, as well as the absence of a “gold or reference standard” with which to compare the diagnostic criteria, make the precision of the diagnoses, their sensitivity, specificity and predictive values relatively weak and studies difficult to compare with each other. For certain clinical conditions, in addition to the clinical and radiological criteria, the CDC offers microbiological criteria for the diagnosis of VAP that are summarize in Table 3.
Given the lack of consensus regarding the definition of VAP in neonates and the low reliability of chest X-ray, lung ultrasound is now being considered a potential alternative diagnostic tool. A recent study by Tusor et al. [65] showed that a multiparameter VAP score combining clinical, microbiology and lung ultrasound, improved the sensitivity, specificity, and the area under curve for VAP detection in preterm infants with chronic lung disease in comparison with clinical information only or with the combination of clinical information plus chest-X-ray. In 2013 for adults [66] and later in 2019 for pediatric and neonatal patients [67], the National Healthcare Safety Network (NHSN) of the CDC replaced the criteria of VAP surveillance by surveillance of ventilator-associated events (VAEs), defined primarily as an increase in respiratory support (oxygen or pressure) in a previously stable or improving mechanically ventilated patient. The aim was to obtain a more general and objective criterion of complications associated with the ventilator, to detect both infectious and non-infectious complications. These VAE definitions have the necessary validity and reliability to be used in external quality assessments and benchmarking [68]. However, VAP definitions, despite the difficulties described, have shown to be useful as a measure of improving the internal quality of centers at an individual level [69].
3.2. Sample Collection and Pathogens Implicated in VAP
Regarding the methodology for obtaining lung samples, once again the neonatal patient represents a significant challenge. In this group of patients less invasive techniques are usually used, such as direct tracheal aspiration (TA) in intubated patients, which does not allow differentiation between colonization and infection, with almost universal bacterial growth being found when the endotracheal tube has been in place for more than 10 days [70]. In adults, bronchoscopic bronchoalveolar lavage (BAL) and protected brush are very reliable techniques since they avoid contamination of the samples; however, they are not applicable in the newborn due to the small diameter of the endotracheal tube. On the contrary, the use of blind invasive sampling techniques is feasible and seems to minimize the sample contamination [61]. In this study carried out with blind-protected BAL, the most frequently isolated pathogens were Pseudomonas aeruginosa and Staphylococcus aureus, with the isolate being polymicrobial in 16.7% of the cases. [61]. Other studies have shown predominance of Gram-negative rods, especially Klebsiella pneumoniae, Escherichia Coli, Enterobacter spp., Acinetobacter spp., Citrobacter spp., Acinetobacter baumanii, and Stenotrophomonas maltophilia [71,72,73,74,75], and Gram-positive cocci, such as Coagulase negative Staphilococcus, Staphilococcus aureus, Enterococcus, and Group B Streptococcus [73,76]. It is important to highlight that when TA are direct through an endotracheal tube, polymicrobial isolation can reach up to 58% [71].
Given the difficulty of differentiating pneumonia from bacterial colonization, specific biomarkers of VAP have been sought in the adult population, such as the presence of intracellular microorganisms, the detection of elastin fibers, the test for antibody-coated bacteria, the level of endotoxins in the BAL fluid, the local production of interleukin-8, the levels of lactate dehydrogenase and the decrease of surfactant protein A, with poor results. Perhaps the most validated technique with greater specificity, as long as the patient does not receive prior antibiotic therapy, is the search for intracellular bacteria in polymorphonuclear leukocytes or macrophages. However, this technique requires a considerable time effort on the part of the microbiologist, and also requires the performance of BAL, which is not always available or free of risks for the patient [77].
As mentioned before, in the neonatal patient, Cernada et al. [60] proposed the use of BAL with catheters with blind protection, although it is still necessary to carry out comparative trials versus traditional TA for culture, as well as to identify reliable biomarkers of lung infection to diagnose VAP. In their excellent review they discuss the potential usefulness of various markers still under investigation, such as Procalcitonin, Cytokines such as IL-1, IL-6, IL-8, IL-10, and TNF-α, the Soluble Form of the Triggering Receptor Expressed on Myeloid Cells (s-TREM), and plasminogen activation inhibitor-1 (PLA-1). Of them, in a study from Srinivasan et al. [78], elevated levels of PLA-1 had the strongest association with a clinical diagnosis of VAP and was the best biomarker to differentiate VAP from colonization in a pediatric population. More recently, Pinilla-González et al. in an interesting study concluded that TNF-α in BAL fluid and glutathione sulfonamide in both, BAL fluid and TA were associated with VAP in preterm newborns making them useful as early biomarkers of VAP, although further studies with more patients are needed to confirm these results [79]. Finally, as in adults, perhaps Gram stain studies in TA samples are the most promising. In the study by Katayama et al. [80] in VLBW infants, a sensitivity of 82 and 100%, and a specificity of 100 and 82%, was found for Gram-positive and Gram-negative VAP, respectively. Furthermore, initial antibiotic therapy based on TA with Gram stain was effective in 96% of cases. More recently, Ergenekon E, et al. elegantly showed in a TA fluid cytospin sample from a patient with severe BPD and VAP abundant intraepithelial bacteria, which are no longer detectable after a course of intravenous antibiotics, whereas TA fluid cultures grew the same microorganisms before and after treatment [81].
3.3. Management
The proper management of VAP is based on two fundamental issues: prevention and careful treatment, avoiding overtreatment as well as not treating established cases. Most clinicians choose to treat most suspected cases because of the potentially high risk of undertreatment. A basic aspect of the prevention of healthcare-associated infections is the protection and promotion of the establishment of an appropriate microbiota that competes with pathogens for the colonization of the corresponding ecological niches. In this regard, it is known that early, inappropriate or excessive use of broad-spectrum antibiotics is significantly associated with the emergence of multidrug-resistant pathogens [82]. In addition to this, different sets of measures have been developed that, despite the limitation of not having clearly established and universal diagnostic criteria, have shown effectiveness in reducing VAP in local settings. A summary of the potential measures suggested by different authors and adapted from bundles developed for the prevention of VAP in adults is shown in Table 4 [83].
Otherwise, specific treatment is aimed at broad-spectrum antibiotic coverage based on the predominant pathogens in the units, with subsequent de-escalation based on bacterial isolation and the antibiogram. However, it is necessary to take into account that neonatal VAP does not usually progress to systemic bacteremia or rapid clinical deterioration, and it is accompanied by a lower mortality rate compared to neonatal bacteremia or VAP in adults [84]. Therefore, it is worth reconsidering the need to use broad-spectrum antibiotics to treat neonates with VAP without concurrent bacteremia.
Another important aspect of the treatment has to do with the replacement of the theoretically most favorable microbiota that must occupy a certain niche to compete with pathogens. The intestinal microflora has anti-inflammatory, antioxidant and analgesic properties, and produces vitamins, which protects the intestine against the action of pathogenic bacteria that can cause chronic diseases [85]. Given the increasing antibiotic resistance in recent times, the investigation of the therapeutic potential of the intestinal microbiota is of paramount importance. At present there are no conclusive studies that allow us to establish a specific guideline with a sufficient level of evidence, but the use of probiotics and prebiotics has been proposed for years in an attempt to restore the intestinal microbiome. Initial studies administering Lactobacillus and/or Bifidobacterium in premature neonates seemed promising for preventing severe necrotizing enterocolitis and mortality [86], although as discussed above, these results were not subsequently confirmed, especially in extremely premature infants [33]. In a model of newborn rhesus macaques, Stevens et al. [23] observed that exposure to antibiotics early in life promoted inflammatory changes and made them more susceptible to bacterial pneumonia. The transfer of fecal microbiota allowed partial correction of general immune maladaptation and protection against severe pneumonia. The authors conclude that their findings show the importance of the gut microbiota in programming lung immunity and support the idea that the gut microbiota promotes balance between pathways that drive tissue repair and inflammatory responses associated with clinical recovery of infection in babies. The possibility of using immunomodulatory drugs or oral or nebulized probiotics has also been suggested. Some experimental studies in mice have already shown that nasal administration of probiotic bacteria can protect against respiratory infections [87].
In humans, a study carried out almost a decade ago in adult volunteers showed that nasal inoculation of Neisseria lactamica displaced Neisseria meningitidis and that this inhibition of meningococcal carriage could be even more potent than after glycoconjugate meningococcal vaccination. The authors conclude that Neisseria lactamica or its components could be a novel bacterial medicine to suppress meningococcal outbreaks [88]. Similarly, a study that evaluated the prophylactic use of probiotics for the prevention of VAP in children admitted to a high-risk paediatric ICU where baseline VAP rates were high showed a 77% decrease in the incidence of VAP. The intervention was found to be safe and the results seems promising in this setting [89]. However, the recent PROSPECT trial on the prevention of severe pneumonia and endotracheal colonization by intratracheal administration of the probiotic L rhamnosus GG compared with placebo in adults, resulted in no significant difference in the development of ventilator-associated pneumonia [90]. Therefore, more studies are still necessary in this field.
4. Conclusions
The knowledge of the microbiome of the respiratory system, especially at the distal or pulmonary level, in the newborn has only just begun. Now it is well recognized the importance of the maternal microbiota and its influence even before birth. The type of birth and feeding of the baby, as well as the environment in which them occur, are essential for establishing the individual’s microbiota pattern. The inappropriate use of antibiotics administered to both, the mother and the newborn, are among the factors that most affect the establishment and development of a healthy and protective microbiota. The dysbiosis that follows its administration has been associated with several health problems in the short and long term. In the present review we focused on the development of VAP, especially in intubated preterm newborns. Although precise diagnostic criteria are far from being achieved, the appropriate use of antibiotics in the perinatal period, as well as avoiding endotracheal intubations or shortening invasive mechanical ventilation times, are among the most relevant preventive measures. The potential use of oral or aerosol probiotics to prevent or treat complications derived from dysbiosis constitutes a field of greatest interest in modern perinatology.
Author Contributions
All authors participated in the Conceptualization of the manuscript and contributed to the literature review and selection of the most relevant papers. FGMR prepared and wrote the original draft. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This review did not require ethical approval.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data have been generated in this review.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Magill SS, O’Leary E, Janelle SJ, Thompson DL, Dumyati G, Nadle J, Wilson LE, Kainer MA, Lynfield R, Greissman S, Ray SM, Beldavs Z, Gross C, Bamberg W, Sievers M, Concannon C, Buhr N, Warnke L, Maloney M, Ocampo V, Brooks J, Oyewumi T, Sharmin S, Richards K, Rainbow J, Samper M, Hancock EB, Leaptrot D, Scalise E, Badrun F, Phelps R, Edwards JR; Emerging Infections Program Hospital Prevalence Survey Team. Changes in Prevalence of Health Care-Associated Infections in U.S. Hospitals. N Engl J Med. 2018, 379, 1732–1744. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, Napolitano LM, O’Grady NP, Bartlett JG, Carratalà J, El Solh AA, Ewig S, Fey PD, File TM Jr, Restrepo MI, Roberts JA, Waterer GW, Cruse P, Knight SL, Brozek JL. Management of Adults with Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis 2016, 63, e61-e111, Epub 2016 Jul 14. Erratum in: Clin Infect Dis. 2017;64(9):1298. Erratum in: Clin Infect Dis. 2017 Oct 15;65(8):1435. Erratum in: Clin Infect Dis. 2017;65(12):2161. PMID: 27418577; PMCID: PMC4981759. [CrossRef] [PubMed]
- CDC. Pneumonia (Ventilator-associated [VAP] and Non-ventilator-associated Pneumonia [PNEU]) Event. (2024).
- Baltimore, RS. The difficulty of diagnosing ventilator-associated pneumonia. Pediatrics 2003, 112(6 Pt 1), 1420-1. [Google Scholar] [CrossRef] [PubMed]
- Rogers GB, Stressmann FA, Koller G, Daniels T, Carroll MP, Bruce KD. Assessing the diagnostic importance of nonviable bacterial cells in respiratory infections. Diagn Microbiol Infect Dis. 2008, 62, 133–41. [Google Scholar] [CrossRef] [PubMed]
- Sherman MP, Minnerly J, Curtiss W, Rangwala S, Kelley ST. Research on neonatal microbiomes: what neonatologists need to know. Neonatology. 2014, 105, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Sender R, Fuchs S, Milo R. Are we really vastly outnumbered? revisiting the ratio of bacterial to host cells in humans. Cell. 2016, 164, 337–40. [Google Scholar] [CrossRef] [PubMed]
- Marchesi JR, Ravel J. The vocabulary of microbiome research: a proposal. Microbiome. 2015, 3, 31. [Google Scholar] [CrossRef] [PubMed]
- Yatsunenko T, Rey FE, Manary MJ, Trehan I, Dominguez-Bello MG, Contreras M, Magris M, Hidalgo G, Baldassano RN, Anokhin AP, Heath AC, Warner B, Reeder J, Kuczynski J, Caporaso JG, Lozupone CA, Lauber C, Clemente JC, Knights D, Knight R, Gordon JI. Human gut microbiome viewed across age and geography. Nature. 2012, 486, 222–7. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Petersen C, Round JL. Defining dysbiosis and its influence on host immunity and disease. Cell Microbiol. 2014, 16, 1024–33. [Google Scholar] [CrossRef] [PubMed]
- Lal CV, Travers C, Aghai ZH, Eipers P, Jilling T, Halloran B, Carlo WA, Keeley J, Rezonzew G, Kumar R, Morrow C, Bhandari V, Ambalavanan N. The Airway Microbiome at Birth. Sci Rep. 2016, 6, 31023. [CrossRef] [PubMed]
- Kim BR, Shin J, Guevarra R, Lee JH, Kim DW, Seol KH, Lee JH, Kim HB, Isaacson R. Deciphering Diversity Indices for a Better Understanding of Microbial Communities. J Microbiol Biotechnol. 2017, 27, 2089–2093. [Google Scholar] [CrossRef] [PubMed]
- Huttenhower C, Gevers D, Knight R, Abubucker S, Badger JH, Chinwalla AT, et al. Structure, function and diversity of the healthy human microbiome. Nature. 2012, 486, 207–14. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Bello MG, Costello EK, Contreras M, Magris M, Hidalgo G, Fierer N, Knight R. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns. Proc Natl Acad Sci USA. 2010, 107, 11971–5. [Google Scholar] [CrossRef] [PubMed]
- DiGiulio DB, Romero R, Amogan HP, Kusanovic JP, Bik EM, Gotsch F, et al. Microbial prevalence, diversity and abundance in amniotic fluid during preterm labor: a molecular and culture-based investigation. PLoS One. 2008, 3, e3056. [Google Scholar] [CrossRef] [PubMed]
- Jones HE, Harris KA, Azizia M, Bank L, Carpenter B, Hartley JC, et al. Differing prevalence and diversity of bacterial species in fetal membranes from very preterm and term labor. PLoS One. 2009, 4, e8205. [Google Scholar] [CrossRef] [PubMed]
- Aagaard K, Ma J, Antony KM, Ganu R, Petrosino J, Versalovic J. The placenta harbors a unique microbiome. Sci Transl Med. 2014, 6, 237ra65. [Google Scholar] [CrossRef] [PubMed]
- Lauder AP, Roche AM, Sherrill-Mix S, Bailey A, Laughlin AL, Bittinger K, Leite R, Elovitz MA, Parry S, Bushman FD. Comparison of placenta samples with contamination controls does not provide evidence for a distinct placenta microbiota. Microbiome. 2016, 4, 29. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen HJ, Gur TL. Intrauterine Microbiota: Missing, or the Missing Link? Trends Neurosci. 2019, 42, 402–413. [Google Scholar] [CrossRef] [PubMed]
- 20. Pammi M, Lal CV, Wagner BD, Mourani PM, Lohmann P, Luna RA, Sisson A, Shivanna B, Hollister EB, Abman SH, Versalovic J, Connett GJ, Bhandari V, Ambalavanan N. Airway Microbiome and Development of Bronchopulmonary Dysplasia in Preterm Infants: A Systematic Review. J Pediatr. 2019, 204, 126-133.e2. [CrossRef] [PubMed]
- Spaetgens R, DeBella K, Ma D, Robertson S, Mucenski M, Davies HD, Perinatal antibiotic usage and changes in colonization and resistance rates of group B streptococcus and other pathogens. Obstet. Gynecol. 2002, 100, 525–533. [CrossRef]
- Stoll BJ, Hansen NI, Sanchez PJ, Faix RG, Poindexter BB, Van Meurs KP, Bizzarro MJ, Goldberg RN, Frantz III ID, Hale EC, Shankaran S, Kennedy K, Carlo WA, Watterberg KL, Bell EF, Walsh MC, Schibler K, Laptook AR, Shane AL, Schrag SJ, Das A, Higgins RD; Eunice Kennedy Shriver National Institute of Child and Human Development Neonatal Research Network, Early onset neonatal sepsis: The burden of group B Streptococcal and E. coli disease continues. Pediatrics. 2011, 127, 817–826. [Google Scholar] [CrossRef]
- Stevens J, Steinmeyer S, Bonfield M, Peterson L, Wang T, Gray J, Lewkowich I, Xu Y, Du Y, Guo M, Wynn JL, Zacharias W, Salomonis N, Miller L, Chougnet C, O’Connor DH, Deshmukh H. The balance between protective and pathogenic immune responses to pneumonia in the neonatal lung is enforced by gut microbiota. Sci Transl Med. 2022, 14, eabl3981. [Google Scholar] [CrossRef] [PubMed]
- Dang AT, Marsland BJ. Microbes, metabolites, and the gut-lung axis. Mucosal Immunol. 2019, 12, 843–850. [Google Scholar] [CrossRef] [PubMed]
- 25. Tirone C, Pezza L, Paladini A, Tana M, Aurilia C, Lio A, D’Ippolito S, Tersigni C, Posteraro B, Sanguinetti M, Di Simone N, Vento G. Gut and Lung Microbiota in Preterm Infants: Immunological Modulation and Implication in Neonatal Outcomes. Front Immunol. 2019, 10, 2910. [CrossRef] [PubMed]
- Alcazar CG, Paes VM, Shao Y, Oesser C, Miltz A, Lawley TD, Brocklehurst P, Rodger A, Field N. The association between early-life gut microbiota and childhood respiratory diseases: a systematic review. Lancet Microbe. 2022, 3, e867–e880. [Google Scholar] [CrossRef] [PubMed]
- Gleeson K, Eggli DF, Maxwell SL. Quantitative aspiration during sleep in normal subjects. Chest. 1997, 111, 1266–72. [Google Scholar] [CrossRef] [PubMed]
- Samuelson DR, Welsh DA, Shellito JE. Regulation of lung immunity and host defense by the intestinal microbiota. Front Microbiol. 2015, 6, 1085. [CrossRef] [PubMed]
- Koh A, De Vadder F, Kovatcheva-Datchary P, Bäckhed F. From Dietary Fiber to Host Physiology: Short-Chain Fatty Acids as Key Bacterial Metabolites. Cell 2016, 165, 1332–1345. [CrossRef] [PubMed]
- Krajmalnik-Brown R, Ilhan ZE, Kang DW, DiBaise JK. Effects of gut microbes on nutrient absorption and energy regulation. Nutr Clin Pract. 2012, 27, 201–14. [Google Scholar] [CrossRef] [PubMed]
- Litvak Y, Byndloss MX, Bäumler AJ. Colonocyte metabolism shapes the gut microbiota. Science. 2018, 362, eaat9076. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Terrin G, Passariello A, De Curtis M, Manguso F, Salvia G, Lega L, Messina F, Paludetto R, Canani RB. Ranitidine is associated with infections, necrotizing enterocolitis, and fatal outcome in newborns. Pediatrics. 2012, 129, e40–e45. [Google Scholar] [CrossRef] [PubMed]
- Sharif S, Meader N, Oddie SJ, Rojas-Reyes MX, McGuire W. Probiotics to prevent necrotising enterocolitis in very preterm or very low birth weight infants. Cochrane Database Syst Rev. 2023, 7, CD005496. [Google Scholar] [CrossRef] [PubMed]
- Yun Y, Srinivas G, Kuenzel S, Linnenbrink M, Alnahas S, Bruce KD, Steinhoff U, Baines JF, Schaible UE. Environmentally determined differences in the murine lung microbiota and their relation to alveolar architecture. PLoS One. 2014, 9, e113466. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- 35. Groves HT, Cuthbertson L, James P, Moffatt MF, Cox MJ, Tregoning JS. Respiratory Disease following Viral Lung Infection Alters the Murine Gut Microbiota. Front Immunol 2018, 9, 182. [CrossRef] [PubMed]
- Yildiz S, Mazel-Sanchez B, Kandasamy M, Manicassamy B, Schmolke M. Influenza A virus infection impacts systemic microbiota dynamics and causes quantitative enteric dysbiosis. Microbiome. 2018, 6, 9. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- 37. Sencio V, Barthelemy A, Tavares LP, Machado MG, Soulard D, Cuinat C, Queiroz-Junior CM, Noordine ML, Salomé-Desnoulez S, Deryuter L, Foligné B, Wahl C, Frisch B, Vieira AT, Paget C, Milligan G, Ulven T, Wolowczuk I, Faveeuw C, Le Goffic R, Thomas M, Ferreira S, Teixeira MM, Trottein F. Gut Dysbiosis during Influenza Contributes to Pulmonary Pneumococcal Superinfection through Altered Short-Chain Fatty Acid Production. Cell Rep 2020, 30, 2934–2947.e6. [CrossRef] [PubMed]
- Penders J, Thijs C, Vink C, Stelma FF, Snijders B, Kummeling I, et al. Factors influencing the composition of the intestinal microbiota in early infancy. Pediatrics. 2006, 118, 511–21. [Google Scholar] [CrossRef] [PubMed]
- Bogaert D, Keijser B, Huse S, Rossen J, Veenhoven R, van Gils E, et al. Variability and diversity of nasopharyngeal microbiota in children: a metagenomic analysis. PLoS One. 2011, 6, e17035. [Google Scholar] [CrossRef] [PubMed]
- Charlson ES, Bittinger K, Haas AR, Fitzgerald AS, Frank I, Yadav A, Bushman FD, Collman RG. Topographical continuity of bacterial populations in the healthy human respiratory tract. Am J Respir Crit Care Med. 2011, 184, 957–63. [Google Scholar] [CrossRef] [PubMed]
- Brugger SD, Eslami SM, Pettigrew MM, Escapa IF, Henke MT, Kong Y, Lemon KP. Dolosigranulum pigrum Cooperation and Competition in Human Nasal Microbiota. mSphere. 2020, 5, e00852–20. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bosch AATM, Levin E, van Houten MA, Hasrat R, Kalkman G, Biesbroek G, de Steenhuijsen Piters WAA, de Groot PCM, Pernet P, Keijser BJF, Sanders EAM, Bogaert D. Development of Upper Respiratory Tract Microbiota in Infancy is Affected by Mode of Delivery. EBioMedicine. 2016, 9, 336-345. [CrossRef] [PubMed]
- Koch MA, Reiner GL, Lugo KA, Kreuk LS, Stanbery AG, Ansaldo E, Seher TD, Ludington WB, Barton GM. Maternal IgG and IgA Antibodies Dampen Mucosal T Helper Cell Responses in Early Life. Cell. 2016, 165, 827–41. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jeurink PV, van Bergenhenegouwen J, Jiménez E, Knippels LM, Fernández L, Garssen J, Knol J, Rodríguez JM, Martín R. Human milk: a source of more life than we imagine. Benef Microbes. 2013, 4, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Madan JC, Koestler DC, Stanton BA, Davidson L, Moulton LA, Housman ML, Moore JH, Guill MF, Morrison HG, Sogin ML, Hampton TH, Karagas MR, Palumbo PE, Foster JA, Hibberd PL, O’Toole GA. Serial analysis of the gut and respiratory microbiome in cystic fibrosis in infancy: interaction between intestinal and respiratory tracts and impact of nutritional exposures. mBio. 2012, 3, e00251–12. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Teo SM, Mok D, Pham K, Kusel M, Serralha M, Troy N, Holt BJ, Hales BJ, Walker ML, Hollams E, Bochkov YA, Grindle K, Johnston SL, Gern JE, Sly PD, Holt PG, Holt KE, Inouye M. The infant nasopharyngeal microbiome impacts severity of lower respiratory infection and risk of asthma development. Cell Host Microbe. 2015, 17, 704–15. [Google Scholar] [CrossRef] [PubMed]
- Vissing NH, Chawes BL, Bisgaard H. Increased risk of pneumonia and bronchiolitis after bacterial colonization of the airways as neonates. Am J Respir Crit Care Med. 2013, 188, 1246–52. [Google Scholar] [CrossRef] [PubMed]
- Jakobsson HE, Jernberg C, Andersson AF, Sjölund-Karlsson M, Jansson JK, Engstrand L. Short-term antibiotic treatment has differing long-term impacts on the human throat and gut microbiome. PLoS One. 2010, 5, e9836. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Man WH, de Steenhuijsen Piters WA, Bogaert D. The microbiota of the respiratory tract: gatekeeper to respiratory health. Nat Rev Microbiol. 2017, 15, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Stressmann FA, Connett GJ, Goss K, Kollamparambil TG, Patel N, Payne MS, Puddy V, Legg J, Bruce KD, Rogers GB. The use of culture-independent tools to characterize bacteria in endo-tracheal aspirates from pre-term infants at risk of bronchopulmonary dysplasia. J Perinat Med. 2010, 38, 333–7. [Google Scholar] [CrossRef] [PubMed]
- Beeton ML, Maxwell NC, Davies PL, Nuttall D, McGreal E, Chakraborty M, Spiller OB, Kotecha S. Role of pulmonary infection in the development of chronic lung disease of prematurity. Eur Respir J. 2011, 37, 1424–30. [Google Scholar] [CrossRef] [PubMed]
- Flanagan JL, Brodie EL, Weng L, Lynch SV, Garcia O, Brown R, Hugenholtz P, DeSantis TZ, Andersen GL, Wiener-Kronish JP, Bristow J. Loss of bacterial diversity during antibiotic treatment of intubated patients colonized with Pseudomonas aeruginosa. J Clin Microbiol. 2007, 45, 1954–62. [Google Scholar] [CrossRef] [PubMed]
- Cairns S, Thomas JG, Hooper SJ, Wise MP, Frost PJ, Wilson MJ, Lewis MA, Williams DW. Molecular analysis of microbial communities in endotracheal tube biofilms. PLoS One. 2011, 6, e14759. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dickson RP, Erb-Downward JR, Huffnagle GB. Homeostasis and its disruption in the lung microbiome. Am J Physiol Lung Cell Mol Physiol. 2015, 309, L1047–L1055. [Google Scholar] [CrossRef] [PubMed]
- Sandrini S, Aldriwesh M, Alruways M, Freestone P. Microbial endocrinology: host-bacteria communication within the gut microbiome. J Endocrinol. 2015, 225, R21–R34. [Google Scholar] [CrossRef] [PubMed]
- Freestone PP, Hirst RA, Sandrini SM, Sharaff F, Fry H, Hyman S, O’Callaghan C. Pseudomonas aeruginosa-catecholamine inotrope interactions: a contributory factor in the development of ventilator-associated pneumonia? Chest. 2012, 142, 1200–1210. [Google Scholar] [CrossRef] [PubMed]
- Gallacher DJ, Kotecha S. Respiratory Microbiome of New-Born Infants. Front Pediatr 2016, 4, 10. [CrossRef] [PubMed]
- Iosifidis E, Pitsava G, Roilides E. Ventilator-associated pneumonia in neonates and children: a systematic analysis of diagnostic methods and prevention. Future Microbiol 2018, 13, 1431-1446. [CrossRef] [PubMed]
- Tan B, Zhang F, Zhang X, Huang YL, Gao YS, Liu X, Li YL, Qiu JF. Risk factors for ventilator-associated pneumonia in the neonatal intensive care unit: a meta-analysis of observational studies. Eur J Pediatr. 2014, 173, 427–34. [Google Scholar] [CrossRef] [PubMed]
- Cernada M, Brugada M, Golombek S, Vento M. Ventilator-associated pneumonia in neonatal patients: an update. Neonatology. 2014, 105, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Cernada M, Aguar M, Brugada M, Gutiérrez A, López JL, Castell M, Vento M. Ventilator-associated pneumonia in newborn infants diagnosed with an invasive bronchoalveolar lavage technique: a prospective observational study. Pediatr Crit Care Med. 2013, 14, 55–61. [Google Scholar] [CrossRef] [PubMed]
- 62. Fernández-Barat L, López-Aladid R, Torres A. Reconsidering ventilator-associated pneumonia from a new dimension of the lung microbiome. EBioMedicine 2020, 60, 102995. [CrossRef] [PubMed]
- Morris AC, Kefala K, Simpson AJ, Wilkinson TS, Everingham K, Kerslake D, Raby S, Laurenson IF, Swann DG, Walsh TS. Evaluation of the effect of diagnostic methodology on the reported incidence of ventilator-associated pneumonia. Thorax. 2009, 64, 516–22. [Google Scholar] [CrossRef] [PubMed]
- Cordero L, Ayers LW, Miller RR, Seguin JH, Coley BD. Surveillance of ventilator-associated pneumonia in very-low-birth-weight infants. Am J Infect Control. 2002, 30, 32–9. [Google Scholar] [CrossRef] [PubMed]
- Tusor N, De Cunto A, Basma Y, Klein JL, Meau-Petit V. Ventilator-associated pneumonia in neonates: the role of point of care lung ultrasound. Eur J Pediatr. 2021, 180, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Magill SS, Klompas M, Balk R, Burns SM, Deutschman CS, Diekema D, Fridkin S, Greene L, Guh A, Gutterman D, Hammer B, Henderson D, Hess DR, Hill NS, Horan T, Kollef M, Levy M, Septimus E, Vanantwerpen C, Wright D, Lipsett P. Developing a new, national approach to surveillance for ventilator-associated events: executive summary. Infect Control Hosp Epidemiol. 2013, 34, 1239–43. [Google Scholar] [CrossRef] [PubMed]
- Cocoros NM, Kleinman K, Priebe GP, Gray JE, Logan LK, Larsen G, Sammons J, Toltzis P, Miroshnik I, Horan K, Burton M, Sims S, Harper M, Coffin S, Sandora TJ, Hocevar SN, Checchia PA, Klompas M, Lee GM; Pediatric Ventilator-Associated Conditions Study Team. Ventilator-Associated Events in Neonates and Children--A New Paradigm. Crit Care Med. 2016, 44, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Whitesel ED, Gupta M. A glass half-full: defining ventilator-associated pneumonia in the neonatal intensive care unit. Pediatr Res. 2020, 87, 1155–1156. [Google Scholar] [CrossRef] [PubMed]
- Niedzwiecka T, Patton D, Walsh S, Moore Z, O’Connor T, Nugent L. What are the effects of care bundles on the incidence of ventilator-associated pneumonia in paediatric and neonatal intensive care units? A systematic review. J Spec Pediatr Nurs. 2019, 24, e12264. [Google Scholar] [CrossRef] [PubMed]
- Willson DF, Conaway M, Kelly R, Hendley JO. The lack of specificity of tracheal aspirates in the diagnosis of pulmonary infection in intubated children. Pediatr Crit Care Med. 2014, 15, 299–305. [Google Scholar] [CrossRef] [PubMed]
- 71. Apisarnthanarak A, Holzmann-Pazgal G, Hamvas A, Olsen MA, Fraser VJ. Ventilator-associated pneumonia in extremely preterm neonates in a neonatal intensive care unit: characteristics, risk factors, and outcomes. Pediatrics. 2003, 112(6 Pt 1), 1283-9. [CrossRef] [PubMed]
- Yuan TM, Chen LH, Yu HM. Risk factors and outcomes for ventilator-associated pneumonia in neonatal intensive care unit patients. J Perinat Med. 2007, 35, 334–8. [Google Scholar] [CrossRef] [PubMed]
- Garland, JS. Strategies to prevent ventilator-associated pneumonia in neonates. Clin Perinatol. 2010, 37, 629–43. [Google Scholar] [CrossRef] [PubMed]
- Deng C, Li X, Zou Y, Wang J, Wang J, Namba F, Hiroyuki Y, Yu J, Yamauchi Y, Guo C. Risk factors and pathogen profile of ventilator-associated pneumonia in a neonatal intensive care unit in China. Pediatr Int. 2011, 53, 332–7. [Google Scholar] [CrossRef] [PubMed]
- Afjeh SA, Sabzehei MK, Karimi A, Shiva F, Shamshiri AR. Surveillance of ventilator-associated pneumonia in a neonatal intensive care unit: characteristics, risk factors, and outcome. Arch Iran Med. 2012, 15, 567–71. [Google Scholar] [PubMed]
- Geffers C, Baerwolff S, Schwab F, Gastmeier P. Incidence of healthcare-associated infections in high-risk neonates: results from the German surveillance system for very-low-birthweight infants. J Hosp Infect. 2008, 68, 214–21. [Google Scholar] [CrossRef] [PubMed]
- el-Ebiary M, Soler N, Monton C, Torres A: Markers of ventilator-associated pneumonia. Clin Intensive Care 1995, 121–126.
- Srinivasan R, Song Y, Wiener-Kronish J, Flori HR. Plasminogen activation inhibitor concentrations in bronchoalveolar lavage fluid distinguishes ventilator-associated pneumonia from colonization in mechanically ventilated pediatric patients. Pediatr Crit Care Med. 2011, 12, 21–7. [Google Scholar] [CrossRef] [PubMed]
- Pinilla-Gonzalez A, Lara-Cantón I, Torrejón-Rodríguez L, Parra-Llorca A, Aguar M, Kuligowski J, Piñeiro-Ramos JD, Sánchez-Illana Á, Navarro AG, Vento M, Cernada M. Early molecular markers of ventilator-associated pneumonia in bronchoalveolar lavage in preterm infants. Pediatr Res. 2023, 93, 1559–1565. [Google Scholar] [CrossRef] [PubMed]
- Katayama Y, Minami H, Enomoto M, Takano T, Hayashi S, Lee YK. Usefulness of Gram staining of tracheal aspirates in initial therapy for ventilator-associated pneumonia in extremely preterm neonates. J Perinatol. 2010, 30, 270–4. [Google Scholar] [CrossRef] [PubMed]
- Ergenekon E, Çataltepe S. Ventilator-associated pneumonia in the NICU: time to boost diagnostics? Pediatr Res. 2020, 87, 1143–1144. [Google Scholar] [CrossRef] [PubMed]
- Wang HC, Tsai MH, Chu SM, Liao CC, Lai MY, Huang HR, Chiang MC, Fu RH, Hsu JF. Clinical characteristics and outcomes of neonates with polymicrobial ventilator-associated pneumonia in the intensive care unit. BMC Infect Dis. 2021, 21, 965. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Weber, CD. Applying Adult Ventilator-associated Pneumonia Bundle Evidence to the Ventilated Neonate. Adv Neonatal Care. 2016, 16, 178–90. [Google Scholar] [CrossRef] [PubMed]
- Papazian L, Klompas M, Luyt CE. Ventilator-associated pneumonia in adults: a narrative review. Intensive Care Med. 2020, 46, 888–906. [Google Scholar] [CrossRef] [PubMed]
- Linares DM, Ross P, Stanton C. Beneficial Microbes: The pharmacy in the gut. Bioengineered. 2016, 7, 11–20. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- AlFaleh K, Anabrees J. Probiotics for prevention of necrotizing enterocolitis in preterm infants. Cochrane Database Syst Rev. 2014, 10, CD005496, Update in: Cochrane Database Syst Rev. 2020 Oct 15;10:CD005496. [CrossRef] [PubMed]
- Forsythe, P. Probiotics and lung diseases. Chest. 2011, 139, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Deasy AM, Guccione E, Dale AP, Andrews N, Evans CM, Bennett JS, Bratcher HB, Maiden MC, Gorringe AR, Read RC. Nasal Inoculation of the Commensal Neisseria lactamica Inhibits Carriage of Neisseria meningitidis by Young Adults: A Controlled Human Infection Study. Clin Infect Dis. 2015, 60, 1512–20. [Google Scholar] [CrossRef] [PubMed]
- Banupriya B, Biswal N, Srinivasaraghavan R, Narayanan P, Mandal J. Probiotic prophylaxis to prevent ventilator associated pneumonia (VAP) in children on mechanical ventilation: an open-label randomized controlled trial. Intensive Care Med. 2015, 41, 677–85. [Google Scholar] [CrossRef] [PubMed]
- Johnstone J, Meade M, Lauzier F, Marshall J, Duan E, Dionne J, Arabi YM, Heels-Ansdell D, Thabane L, Lamarche D, Surette M, Zytaruk N, Mehta S, Dodek P, McIntyre L, English S, Rochwerg B, Karachi T, Henderson W, Wood G, Ovakim D, Herridge M, Granton J, Wilcox ME, Goffi A, Stelfox HT, Niven D, Muscedere J, Lamontagne F, D’Aragon F, St-Arnaud C, Ball I, Nagpal D, Girard M, Aslanian P, Charbonney E, Williamson D, Sligl W, Friedrich J, Adhikari NK, Marquis F, Archambault P, Khwaja K, Kristof A, Kutsogiannis J, Zarychanski R, Paunovic B, Reeve B, Lellouche F, Hosek P, Tsang J, Binnie A, Trop S, Loubani O, Hall R, Cirone R, Reynolds S, Lysecki P, Golan E, Cartin-Ceba R, Taylor R, Cook D; Prevention of Severe Pneumonia and Endotracheal Colonization Trial (PROSPECT) Investigators and the Canadian Critical Care Trials Group. Effect of Probiotics on Incident Ventilator-Associated Pneumonia in Critically Ill Patients: A Randomized Clinical Trial. JAMA. 2021, 326, 1024–1033. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Table 2.
Diagnostic criteria for ventilator-associated pneumonia (VAP) in infants aged 1 year or younger (Adapted from CDC, 2024 [3]).
Table 2.
Diagnostic criteria for ventilator-associated pneumonia (VAP) in infants aged 1 year or younger (Adapted from CDC, 2024 [3]).
| Imaging | Patient without underlying diseases 1 or more (or with underlying diseases 2 or more) imaging test results with one of the following:New and persistent or Progressive and persistent
|
| Signs and Symptoms |
|
Table 3.
Microbiological criteria for ventilator-associated pneumonia (Adapted from CDC,2024 [3]).
| Laboratory |
At least one of the following:
|
| Threshold values for cultured specimens according to the collection technique | |
| Specimen collection / technique | Values |
| Lung tissue Bronchoscopically (B) obtained specimens Bronchoalveolar lavage (B-BAL) Protected BAL (B-PBAL) Protected specimen brushing (B-PSB) Nonbronchoscopically (NB) obtained (blind) specimens NB-BAL NB-PSB Endotracheal aspirate (TA) |
≥ 104 CFU/g tissue ≥ 104 CFU/ml ≥ 104 CFU/ml ≥ 103 CFU/ml ≥ 104 CFU/ml ≥ 103 CFU/ml ≥ 105 CFU/ml |
CFU = colony forming units, g = gram, ml = milliliter.
Table 4.
Interventions to prevent neonatal VAP, adapted from adults bundles [83].
Table 4.
Interventions to prevent neonatal VAP, adapted from adults bundles [83].
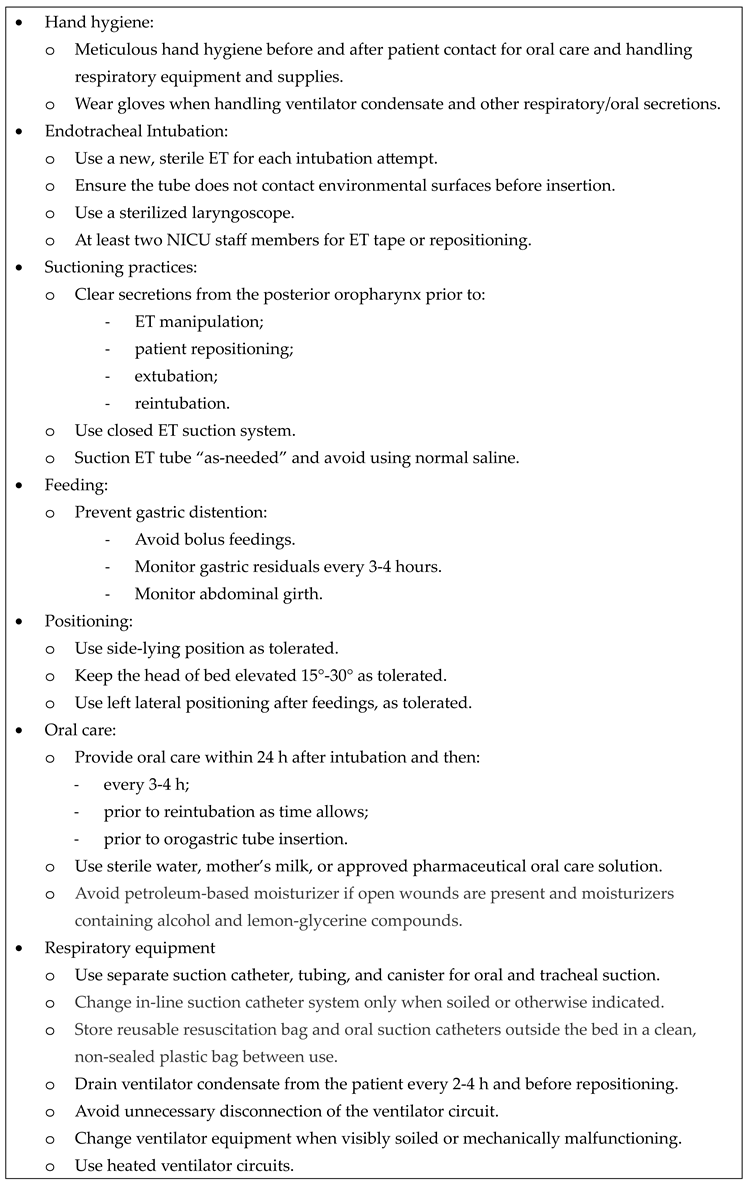 |
ET, endotracheal tube; NICU, neonatal intensive care unit.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



MDPI Initiatives
Important Links
© 2024 MDPI (Basel, Switzerland) unless otherwise stated