
Submitted:
31 January 2024
Posted:
02 February 2024
You are already at the latest version
Abstract
Introduction:
Advanced glycation end-products (AGEs) may play a relevant role as inducers in the chronic inflammatory pathway present in immune-mediated diseases, such as systemic lupus erythematosus (SLE). AGEs concentrations have been associated, with discrepant results to date, with some parameters such as disease activity or accrual damage, suggesting their potential usefulness as biomarkers of the disease.
Objectives:
To confirm differences in AGEs levels measured by cutaneous autofluorescence between SLE patients and healthy controls (HC) and study their correlation with various disease parameters.
Methods:
Cross-sectional study, where AGEs levels were measured by skin autofluorescence, and SLE patients’ data were compared with those of sex- and age-matched HC in a 1:3 proportion through a multiple linear regression model. Correlations of AGEs levels with demographic and clinical data were analyzed through ANOVA tests. Both analyses were adjusted for confounders.
Results:
AGEs levels in SLE patients were significantly higher than in HC (p<0.001). We found statistically significant positive correlation with SLE disease activity index (SLEDAI) and damage index (SDI), physician and patient global assessment, C-reactive protein, leukocyturia, complement C4, IL6 and oral ulcers. We also found a negative statistically significant correlation with current positivity of anti-nuclear and anti-Ro60 antibodies.
Conclusions:
AGEs seem to have a role in LES pathophysiology, becoming a new management and prognosis biomarker in this disease. The association with specific antibodies and disease manifestations may indicate a specific clinical phenotype related to higher AGEs levels.
Keywords:
Systemic lupus erythematosus
; Advanced glycation end products
; Cardiovascular disease
; Biomarkers
1. Introduction
Systemic lupus erythematosus (SLE) is a chronic systemic autoimmune disease characterized by inflammation and tissue organ damage. Its etiology is complex and not fully understood, as contributing mechanisms include genetic, hormonal and environmental factors, the production of pathogenic antibodies, and the deposition of immune complexes [1].
Advanced Glycation End-products (AGEs) are one type of the endogenous inducers (signals produced by stressed, damaged or otherwise malfunctioning tissues) postulated to have an important role in chronic inflammation [2]. AGEs are a set of compounds whose formation is a complicated molecular process resulting from the non-enzymatic interaction of reducing sugars and associated metabolites with peptides, proteins, and amino acids, through the Maillard reaction [3]. A nucleophilic addition reaction between a free amino group from a protein and a carbonyl group from a reducing sugar results in the formation of an unstable, freely reversible Schiff base, which is rearranged to a more stable intermediate, an Amadori product [4]. Schiff bases and Amadori products are reversible reaction products that can react irreversibly with amino acid residues of peptides or proteins to form protein adducts or protein crosslinks [5]. Or, alternatively, they can undergo further oxidation, dehydration, polymerization and oxidative breakdown reactions to give rise to numerous other AGEs [6]. AGEs can also accumulate under hyperglycaemic and pro-oxidative conditions, including diabetes mellitus (DM) [7], ageing [8], cardiovascular disease [9], chronic renal failure [10], and neurological disorders [11]. Although this reaction can occur in all proteins, its action is more common in those that present a slow metabolic turnover, such as collagen This is why these compounds have also been physiologically linked to aging processes, having been reported that AGEs levels correlate with age in the general population [12].
The mechanisms of toxicity of AGEs are mainly related to two facts. On the one hand, glycation favors cross-links between the modified proteins, causing structural alterations and a resulting gradual deterioration in cell and tissue function [13]. In addition, these unions decrease the solubility of proteins, making them more resistant to proteolysis and generating new immunological epitopes [14]. On the other hand, AGEs are recognized by their own receptor (RAGE), a member of the immunoglobulin superfamily, which is expressed in multiple cells like neutrophils, macrophages, T lymphocytes and synovial fibroblasts [15]. RAGE is divided into extracellular, transmembrane, and intracellular segments [16]. The interaction of AGEs with RAGE can activate the downstream nuclear factor kappa-B (NF-ϰB) signaling pathway and promote the secretion of TNF-α, IL-1, IL-6, and other cytokines, contributing to inflammation [17]. Furthermore, oxidative modification of proteins has been shown to elicit antibodies in a variety of diseases including SLE [14].
sRAGE is a positively charged 48-kDa cleavage product from RAGE that keeps the ligand binding site but loses the other two domains [18]. sRAGE binding to ligands terminates intracellular signal transduction due to the loss of the transmembrane and intracellular fragments and inhibits the proinflammatory processes mediated by RAGE and its ligands by acting as a decoy which competitively binds to RAGE ligands [19]. However, sRAGE has also been linked to inflammation in SLE [20].
So far, more than 20 AGEs have been described in tissues. Among them, the most studied are protein adducts, such as Nξ-(carboxymethyl)lysine (CML), Nεξ-(carboxyethyl)lysine (CEL) or pyrraline; and intra- and intermolecular linkages, including pentosidine, glucosepane, and imidazolium compounds [21]. Due to their stability, the most measured AGEs are CML and pentosidine. The concentration of these, although present in tissues with up to 2 degrees of difference, has shown a high correlation with each other. Classical AGEs measurement methods include chromatographic techniques associated to mass spectrometry and immunochemical methods, such as immunosorbent assay enzyme linked (ELISA) [22]. However, a part of the AGEs has the characteristic of being fluorescent (for example pentosidine) so it is possible to quantify them in a single measurement using an autofluorescence reader. This technique, developed by Meerwaldt et al. in 2004, allows, through a non-invasive method, the measurement of fluorescent AGEs stored in the skin. Measuring accumulated AGEs makes this assessment more appropriate to quantify the concentration of AGEs in an individual throughout their life than that of a single specific moment in relation to an acute process. It has been described that this autofluorescent measurement correlates with the concentration of AGEs, both fluorescent and not fluorescent, measured in skin biopsies [23].
In systemic autoimmune diseases, such as SLE, increased AGEs formation can be expected, as inflammation is one of the hallmarks of the disease. Chronic inflammation in SLE appears to be associated with an intensified glycation process and the formation of AGEs, having higher values of the latter compared to healthy controls (HC) been demonstrated in some studies [24,25,26,27,28]. At the same time, through their pathogenic mechanisms, AGEs are also involved in the generation of inflammation and reactive oxygen species, creating a positive feedback that enhances inflammation and AGEs levels.
Regarding atherosclerosis, it has been observed that AGE-AGE covalent intermolecular unions in collagen I fibers induce an increase in molecular packing, causing an increase in vascular rigidity. In addition, the accumulation of AGEs in the vascular wall induces the adherence of blood cells to the endothelium, capturing immunoglobulins and apoproteins that favor the inflammatory process [29]. Moreover, an AGE-modified form of LDL (low-density lipoproteins) has been found to circulate in human plasma, and AGE modifications have been identified as being present on both the apoprotein and the phospholipid components of LDL, converting them to glycated LDLs. It has been proposed that those AGE-modified peptides contribute to tissue injury by reattaching to susceptible target proteins both within and outside the vasculature, making them even more atherogenic [30,31]. In SLE, the presence of accelerated atherosclerosis that cannot be fully explained by traditional risk factors for cardiovascular disease is a well-recorded phenomenon [32]. Some studies have suggested that increased levels of AGEs might contribute to the development of this accelerated atherosclerosis in SLE and, therefore, could be used as early markers for cardiovascular disease in this pathology [27,28].
Apart from age and atherosclerosis, some exogenous factors have also been reported to be positively correlated with AGEs levels like smoking status [24,33] or some foods [34]. Treatment with drugs such as aminoguanidine, vitamins, angiotensin-converting enzyme (ACE) inhibitors, angiotensin-II receptor blockers, statins, and metformin inhibit AGEs formation while Alagebrium breaks their crosslinks [35]. Moreover, it seems that the level of circulating AGEs are genetically determined, as shown in a cohort study of healthy monozygotic and heterozygotic twins [36].
Lately, there has been increased attention on the potential of RAGE and AGEs to target diseases, especially chronic inflammatory diseases such as SLE. Some studies have expounded on their usefulness as biomarkers of SLE diagnosis and prognosis, their relation with accelerated atherosclerosis, as well as their potential place as targets for new treatments. However, we find some controversial results in the literature, showing that more and better studies are needed to fully elucidate their role in SLE.
Having into account that the relation between skin AGEs and SLE have only been reported in one previous paper, the purpose of this work, that studies the levels of AGEs in a Spanish cohort suffering from SLE, tries to answer that unmet need encompassing several specific goals. First, to describe AGEs concentrations in SLE and compare them to age- and sex-matched HC. Secondly, to search for correlations between AGEs concentrations and SLE characteristics such as specific manifestations, indexes of activity or accrual damage, or patient reported outcomes (PROs). And finally, to explore AGEs relationship with cardiovascular disease and cardiovascular risk factors (CVRF). All of it with the ultimate aim of investigating AGEs role as potential SLE biomarkers in SLE, as well as their application in routine clinical practice as a tool for improving diagnosis, monitoring, and prognosis of the disease, or as surrogate markers for the assessment of cardiovascular risk in this population.
2. Methodology
2.1. Subjects
Cross-sectional study conducted at the Hospital del Mar where patients of all ages who were visited at the SLE outpatient clinic, met the 1997 American College of Rheumatology (ACR) [37] or the 2012 Systemic Lupus International Collaborating Clinics (SLICC) classificatory criteria [38] for SLE, accepted to participate and signed the informed consent were randomly included. The exclusion criteria were pregnancy, DM, treatment with corticosteroids at a dose equivalent to prednisone > 20 mg/day, active malignancy, and fibromyalgia. Patients and the public were not involved in the design, conduct, reporting, or dissemination of this work.
2.2. Healthy controls
The control population was selected from the ILERVAS cohorts (Vascular and Renal Translational Research Group, IRBLleida), which includes HC selected from primary care health centers, with at least one traditional CVRF and aged between 50 and 70 years if women or between 45 and 65 years if men. The traditional CVRF included were: arterial hypertension (AHT) and/or dyslipidemia (DLP) and/or obesity (defined as a body mass index (BMI)>30 Kg/m2), and/or history in first-degree relatives of premature cardiovascular disease (men before 65-year-old and women before 60 years-old) and/or smokers and former smokers (< 10 years since quitting). Exclusion criteria were: history of cardiovascular disease (angina, myocardial infarction, cerebrovascular accident, peripheral arterial disease, intestinal ischemia or ischemia of some other territory), history of carotid surgery or surgery of arteries from other territories, DM and/or chronic renal disease (CRD), institutionalized population, population on long-term home-care, active neoplastic processes, life expectancy < 18 months [39]. AGEs levels were measured by autofluorescence in all the HC.
2.3. Variables
A blood test was performed at the moment of the AGEs skin measurement. Variables were categorized according to categories already established in the literature (f.i: remission, low activity…), to tertiles or to individualized categories according to their distributions on our sample. Multiple variables were recorded: demographics, disease characteristics, different indexes for measuring SLE activity and accrual damage, PROs, cardiovascular variables and AGEs. With respect to the analysis of autoantibodies, antinuclear antibodies were determined by indirect immunoflurescence and considered positive if >1:80, anti-Ro60 was determined by either multiplex immunoassay, being positive if titers>1 IA or by blot, and anti-dsDNA by multiplex immunoassay with titers > 10 UI/mL considered positive. AGEs measurement is specified in section D while the other variables and their classifications are detailed in Supplementary Figure S1.
2.4. Assessment of AGES accumulation
In all patients, accumulated AGEs were measured non-invasively in the skin by an autofluorescence reader (Age Reader Mu Connect®) as described previously in the literature [23]. A light source emitting light at a wavelength of 320 to 400 nm excites fluorescent moieties in compounds in the skin to produce fluorescence at a wavelength of 420 to 600 nm (peak 440 nm). The output represents the ratio between autofluorescence in the range 420 to 600 nm and excitation light in the range 320 to 400 nm and is reported in arbitrary units (AU). Three consecutive AGEs measurements were taken from the ventral (anterior) surface of the forearm of each participant 10 cm below the elbow fold, avoiding any tattoos or heavily pigmented areas of skin. Measurements were performed at room temperature, while patients were in a seated position [40] (See Supplementary Figure S2). The mean value of the three measures was calculated and compared with AGEs values from age-matched HC obtained from previous works [23].
2.5. Ethics approval and consent to participate
All patients signed the informed consent form to participate in the study. The protocol for our study was consistent with the provisions of the Declaration of Helsinki and was approved by the ethics committee of the Hospital del Mar (CEIm-PSMAR 2018/7907/I).
2.6. Statistical methods
2.6.1. Comparison of accumulated AGEs between patients and controls
A random sample of 97 individuals with systemic lupus erythematosus was calculated to be sufficient to estimate, with 95% confidence and an accuracy of +/- 0.1 units, the population mean of values (with an expected standard deviation of about 0.5 units [28]). HC were sex- and age-matched with a factor of approximately 3:1 to each of the SLE patients, and selected according to the common variables between both groups. Due to the limited age range of our control group, some of the SLE patients had to be excluded as it was not possible to age-match them with HC. In addition, SLE patients with cardiovascular disease could not be included in the analysis due to it being an exclusion criterion in the HC sample. Difference of AGEs between SLE cases and HC was assessed through a fixed-effects analysis of covariance (ANCOVA) model adjusted for the confounding factors.
In order to identify potentially confounding variables, in addition to a bibliographic review about previously reported factors related to AGEs, a bivariate analysis was performed separating by cases and HC, and by tertiles of AGEs. Categorical data was described with absolute and relative frequencies, whereas continuous variables were displayed as mean (standard deviation), or as median (interquartile range) if non-normally distributed. For normal variables, the Student’s t-test was used in the former analysis, and the ANOVA test in the later. The Kruskall-Wallis' test was employed for non-normal continuous variables, and the χ² or Fisher test for categorical variables. We also computed a p-value to assess the trend within the tertiles of AGEs. We applied the Pearson test for continuous variables, the Spearman test for non-normal continuous variables, and the χ² distribution for categorical variables. The significance level for these explorative analyses of confounding variables was taken to be < 0.1.
Variables with statistically significant differences both between groups and with the AGEs response variable were considered potential confounders and were examined through interaction graphs before including them in the final model.
2.6.2. Relation between characteristics of SLE and accumulated AGEs
An exploratory analysis was conducted using ANOVA tests adjusted for both age and current smoking status to investigate the association between SLE patient characteristics and the level of accumulated AGEs, including all patients from the cross-sectional study. For a better analysis, skewed variables of interest were categorized into tertiles or according to non-linear patterns, evaluated with general additive models. Associations with a p value < 0.1 were considered significant and, if consistent, were examined individually. First of all, the identification of potentially confounding variables was performed as described in the previous analysis (F.1). Then multiple lineal regression models studying association between AGEs levels and each variable of interest were fitted considering the corresponding confounding factors, to avoid spurious associations. In this case, the significance level was taken to be < 0.05.
If there were any missing data in the study blood test variables or in the retrieved SLE characteristics, the patient was excluded. If there were missing data in other variables, the patient was included assuming the reduction of statistical power due to missing data.
In both analysis, continuous variables included in the final models were mean-centered to facilitate interpretation. The assumptions of linearity, homoscedasticity and normality of the residuals were verified and the presence of influential points in each model was evaluated. All statistical work was carried out using R version 4.1.2.
3. Results
3.1. Characteristics of patients and controls
The differences between the 189 HC and 62 cases are shown in Table 1: HC had a higher BMI and a higher incidence of dyslipidemia (both in total cholesterol and LDL values), obesity, hypertension and active smoking. Patients with SLE had higher AGEs values and creatinine concentrations. As all the HC were Caucasian, we performed a sensitivity analysis to assess the influence of ethnicity, testing only Caucasian patients against HC. We did not find any differences, so we kept all the ethnicities in the final analysis.
3.2. Comparison of AGEs in SLE patients vs healthy controls
First of all, in order to evaluate possible confounding factors, we explored the associations between AGEs levels (stratified in tertiles) and data of all the participants of the study (both SLE patients and HC). The bivariate analysis showed a significant positive relationship between smoking and AGEs levels, while creatinine showed a trend in that same direction. On the contrary, the presence of dyslipidemia was associated with lower values of AGEs (Supplementary Table S2). Analyzing both groups separately, a significant positive association was found between tertiles of AGEs and both age and smoking, in the two groups. In HC, a significant negative association with dyslipidemia was also found (data not shown).
According to these results and the differences found between SLE patients and HC, interaction graphs were created to visually assess smoking, age, dyslipidemia, and creatinine as cofounding variables. We found differences in the slopes of age and dyslipidemia (Supplementary Figure S3) which were then evaluated in the fixed-effects analysis of covariance model Supplementary Table S3. Smoking was also added to the model due to extensive literature linking it to AGEs values. Furthermore, in the smoking interaction graph we observed that the slopes of non-smokers and former smokers behaved similarly, with only a slight increase in mean cumulative AGEs in non-smokers with SLE, but apparently insignificant, so we unified non-smokers and former smokers in the same group vs active smokers to increase statistical power (Supplementary Figure S3a).
Finally, according to all the data explored, the multivariate model was adjusted with age, smoking, dyslipidemia, creatinine, and the interaction terms. None of the interaction terms were statistically significant so they were finally removed from the model except for the interaction between dyslipidemia and group (LES or HC). This one, was not omitted because it allowed us to observe the effect (p=0.062) of dyslipidemia, granting a better estimation of the AGEs value (Table 2). This was verified by adjusting it without the interaction, where the main effect of dyslipidemia was lost. Dyslipidemia was also adjusted for age and smoking (since HC with dyslipidemia were younger and smoked less), and its effect remained unchanged, ruling out that it was confused by other variables (See Supplementary Table S3). The model reported a statistically significant difference between SLE and HC in AGEs values, showing that AGEs values in SLE patients were 0.721 (95% CI [0.566; 0.876]) units higher (p<0.001) than HC. See Table 2 for the analysis of covariance of fixed effects and Supplementary Figure S4 for the effects graphic.
3.3. Characteristics of SLE patients according to AGEs levels: bivariate analysis.
A total of 122 SLE patients were included. All the variables that showed statistically significant differences according to AGEs tertiles in the bivariate analysis are depicted in Table 3, adjusted by age (p-value M1) and by both age and smoking (p-value M2). The demographic characteristics and other SLE variables of interested are detailed in Supplementary Table S1.
3.4. Correlations between AGEs and SLE characteristics: multivariate analysis.
SLE characteristics that were significant in the exploratory analysis and that might be related to AGEs levels were tested in a model adjusted for previously selected confounding variables (see Methodology), avoiding spurious associations. After adjustment, several SLE characteristics showed associations with AGEs levels.
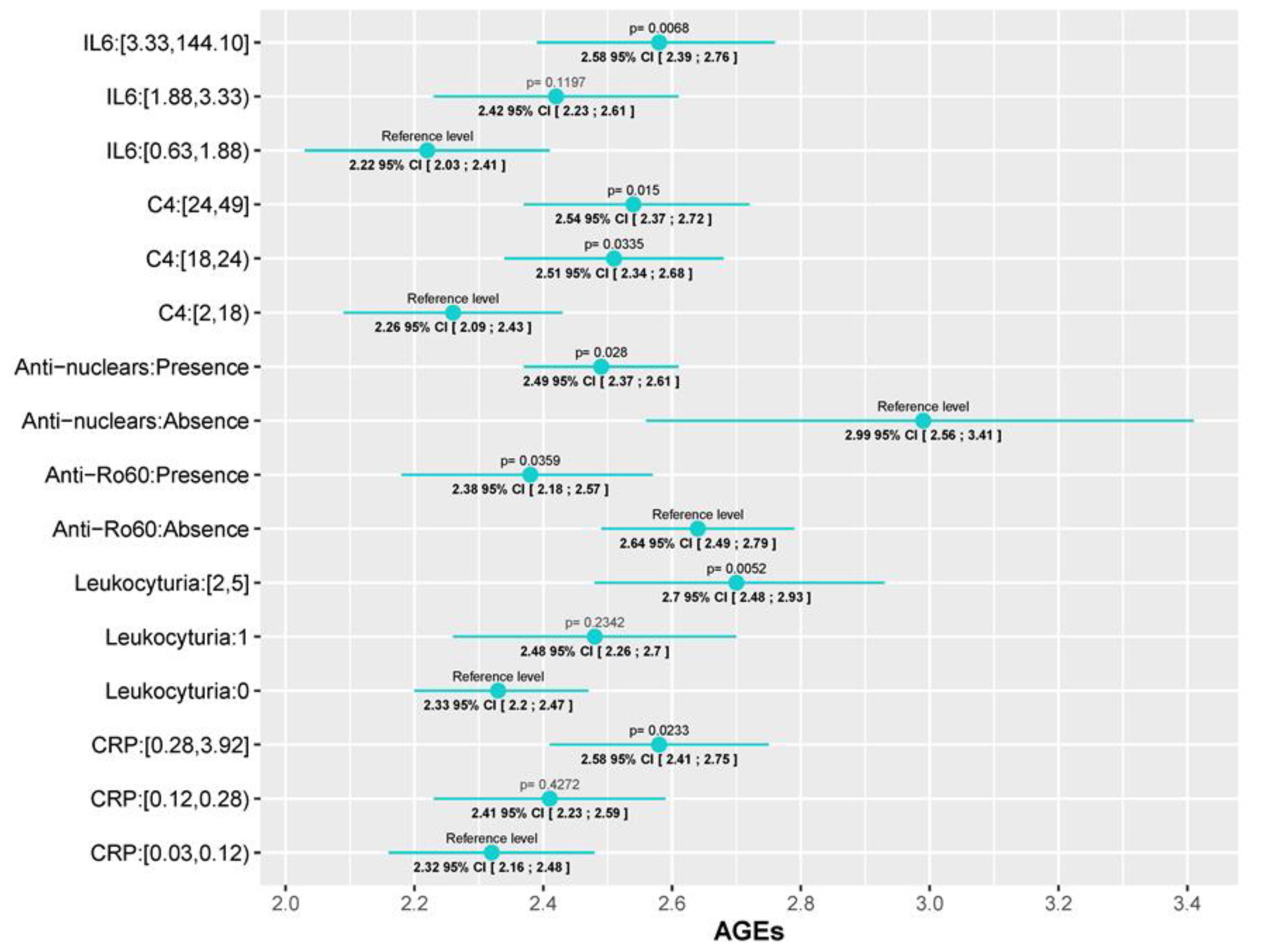
First of all, two of the most important SLE disease indexes, SLEDAI and SDI, were significantly associated with AGEs levels. While for the SLEDAI we found a progressive increase in AGEs values as the SLEDAI activity escalated (AGEs values in patients with moderate and severe activity were 0.2 (95% CI [0.0006; 0.4], p=0.0493) and 0.52 (95% CI [0.177; 0.86], p= 0.003) units higher than patients in remission/mild, respectively), we only found differences in SDI between those with low (0-2) and high scores (5, 6) (AGEs values 0.717 (95% CI [0.139;1.295], p=0.0156) units higher). This association with disease activity is also reflected in both the physician global assessment (PGA) and the patient global assessment (PtGA). In those cases, values higher than 1 (PGA) or 3 (PtGA) were associated with an AGEs level increase (PGA score of 1-2 and a PGA score higher than 2 had AGEs levels 0.033 (95% CI [0.058;0.61], p=0.018) and 0.39 (95% CI [0.094;0.694], p=0.01) units higher than patients with a PGA of 0, respectively; and patients with a PtGA score >3 had AGEs lelvels 0.26 (95% CI [0.063;0.46], p=0.01) units higher than patients with PtGA score ≤ 3. Regarding serum biomarkers, we observed an increment in AGEs levels as CRP and IL-6 increase, but significant differences were only detected between the 3rd and 1st tertile: 0.259 (95%CI [0.035;0.48], p=0,02) for CRP and 0.352 (95% CI [0.1;0.6], p=0.006) for IL-6. The same tendency was observed in the level of leukocyturia (0.369, 95%CI [0.112;0.626], p=0.005) and C4 complement, although in this last one, significant differences with the 2nd tertile were also observed (0.25 (95%CI [0.02;0.48], p=0.0335) for the 2nd tertile; and 0.28 (95%CI [0.056;0.514], p=0.015) for the 3rd one). With reference to autoantibodies, a negative association was found between AGEs levels and both the presence of antinuclear antibodies (ANA) or anti-Ro60 antibodies in the blood test performed for the study, where AGEs values were 0.496 (95%CI [0.937;0.054], p=0.028) and 0.26 (95%CI [0.5;0.017], p=0.035) units lower, respectively. Finally, patients which had ever presented oral ulcers, a prevalent SLE manifestation, had AGEs values 0.216 (95% CI [0.02;0.41], p=0.03) units higher than patients who had never. All these data are depicted, according to the prediction of each model, in Figure 1 and Figure 2 which graphically represent the mean and its corresponding 95% CI of AGEs for each category of variables. P-values <0.05 indicate significant differences between the categories and the reference level of each variable. Also, the fixed-effects ANCOVA model between AGEs and each of the variables are provided in Supplementary Table S4.
4. Discussion
We observed statistically significant differences between AGEs values measured by skin autofluorescence in SLE patients vs HC. This difference has only been studied in two previous works [27,28] with small sample sizes (55 and 30 cases respectively, matched 1:1 with HC), having our study several stronger points. First, we have increased the sample size, especially the HC sample, by matching cases with HC in a 1:3 proportion instead of a 1:1 proportion, making the study more robust. Secondly, we selected HC that had at least one CVRF, so they would be more comparable to our patients who at least have one CVRF, being that the disease itself. This is based on the well-reported knowledge that AGEs are related to inflammation and cardiovascular risk on the one hand and, on the other, that patients with autoimmune diseases like rheumatoid arthritis, have an increased risk of cardiovascular disease that makes necessary to add a fixed multiplier of 1.5 to 2 to the established cardiovascular disease prediction general algorithms in order to adjust for the increased risk due to the disease [27,41], they selected a second control population with essential hypertension (EH), apart from the one conformed by HC. They found statistically significant differences in AGEs levels between SLE patients and HC but not between the SLE and the essential hypertension cohort, suggesting that finding differences when selecting HC with at least one CVRF could traduce a higher statistical power and a reduced probability of committing a type I error. Furthermore, they selected an SLE population with inactive disease, which might not reflect the reality of SLE patients in terms of disease characteristics in the way our patients might, which were included independently of their disease activity.
Additionally, we carefully examined all possible confounding factors to void drawing premature conclusions. Two controversial points were raised during the analyses. First, we observed only a positive trend shown by creatinine in the bivariate analysis of AGEs levels in the whole sample. We discussed if that trend could have a fictitious origin since patients with SLE had higher creatinine levels (although in normal range) and were mostly located in the third AGEs tertile, and also because the trend was not observed when we analyzed the two groups separately. However, we finally decided to include creatinine in the model because there is ample evidence of a higher accumulation of AGEs in patients with renal failure [42] and lupus nephritis [25], and a difference could exist between groups because renal disease was an exclusion criterion in the HC group. Secondly, we found a negative association between dyslipidemia and AGEs, which was observed both in the combined analysis of the whole sample and in the HC separately (suggesting that such association comes from the HC group). The only data in the literature that could explain this negative association comes from the reported effect of lipid-lowering drugs in reducing AGEs levels [43]. Among HC, only 27 of the 85 with dyslipidemia (32%) were being treated with lipid-lowering agents, so we hypothesized that the rest could be controlling it with a lower-fat diet, which has also been associated with reduced AGEs levels [34]. Hence, we ended up including dyslipidemia in the model.
As for the interaction term between the main effect and dyslipidemia, although it was not found to be significant in the model, graphically the interaction seemed clear, especially in the group of SLE patients (Supplementary Figure S3). This could be due to a lack of statistical power, since in the group of SLE patients there were only 8 dyslipidemic cases, unlike the 85 dyslipidemic HC. Therefore, the statistical power to detect this difference was much lower in the patient group, generating a less precise CI to reject the alternative hypothesis and leading to a lack of significance.
Regarding the study of AGEs relationship with SLE characteristics, we have found associations between AGEs levels and some disease activity indexes: SLEDAI, PGA, PtGA, CRP, and IL6. As reflected in the Results section, the rise of AGEs levels with the increase of SLEDAI, which is the activity index most frequently used for SLE in clinical practice nowadays, showed a robust correlation. This association was also observed with other markers of activity commonly used to assess the disease state: PGA, PtGA and IL6. PGA is a part of the main indexes used currently to define remission or low disease activity in SLE. PtGA may be a more subjective parameter which can be influenced by external factors but that is clearly related to quality of life in SLE patients. IL6 is not used routinely in the follow-up of SLE patients but it is widely known its role in inflammation in general and in rheumatic diseases in particular.
In the case of PCR, a significant association was only found between the upper tertile (0.28-3.92 mg/dL) and the first (<0.12), suggesting that the highest levels of AGEs were found among the patients with higher CRP values, both normal and abnormal values (reference values in our laboratory <0.5 mg/dL). However, this correlation is only supported up to CRP values < 0.7 (R2=0.42, p<0.0001), as graphically reflected in Supplementary Figure S5. No correlation was found with higher PCR levels, which could be justified by a small number of patients with abnormal PCR levels. There was also a positive association with higher C4 levels, which draws attention because low C4 levels are the ones traditionally associated with high disease activity. However, although a decrease in complement levels is included in SLE classificatory criteria, there is wide controversy in the literature about the limited usefulness of the current techniques and types of complement measured in SLE and their ability to reflect disease activity [44]. Other uncertainties about complement are whether low levels should be persistent or combined (both C3 and C4) to be significant [45,46]. In our study, C3 levels showed a statistically significant direct correlation with C4 values (p= <0.001) but not with AGEs levels. There was not an association between having normal C4 levels at the moment of the study and not having had hypocomplementemia ever: 43% of the patients with current normal C4 levels had history of hypocomplementemia and 57% did not, while 77% of the patients with history of low C4 had now normal levels). This could traduce either fluctuant titers or normalized levels of C4 in response to treatment/lower disease activity and a need for further studies to elucidate the relation between complement and AGEs.
We also found a relationship between AGEs and indexes of accrual damage, the SDI. There is only a previous work in the literature that analyzed this association [28]. They found a correlation between AGEs and SDI in the univariate analysis that was lost after adjusting for age as well as in the multivariate analysis. In our case, the association persisted after adjusting for age and smoking status and any other possible confounding factor in the multivariate analysis. Taking into account this association, measuring AGEs levels could have a high impact in the prognosis of the disease helping to identify a subtype of patients with a more serious disease marked by higher accrual damage, which would be susceptible of a stricter follow-up and intensive treatment regimen, and subsequently allowing to improve these patients’ outcomes.
Specific manifestations (oral ulcers) or autoantibodies profile (less frequent anti-Ro60+ antibodies), could indicate a different clinical phenotype in SLE patients with less inflammation and thus, with lower AGEs levels. In clinical practice, it is very common to find overlaps of autoimmune diseases in the same patient, being especially frequent in SLE its overlap with Sjögren syndrome (SjS). It is known that both diseases have different inflammatory profiles [47], which could explain why there could be differences in AGEs levels between patients anti-Ro60 positive and negative. AGEs concentrations have been scarcely studied in SjS and efforts have not been directed to skin AGEs but RAGE and sRAGE with conflicting results [48,49,50], so more studies are needed to investigate AGEs levels in SjS and their differences both with SLE patients and with patients with a SLE-SjS overlap. Unfortunately, we could not validate this hypothesis in our study as the presence of SjS was recorded together with other autoimmune diseases as presence of overlapping syndrome in general, making not possible to study the association only in SjS. Furthermore, some patients had ongoing diagnostic SjS tests at the moment of our work. Similarly, oral ulcers are much more frequent in SLE than other autoimmune disease, potentially traducing a more typical SLE disease than in those without, which might justify differences in AGEs levels.
Regarding the negative relation found between AGEs and ANA antibodies, all patients were ANA+ at SLE diagnosis but 10 of them (8.2%) converted during disease follow-up and were ANA- at the moment of the study. It has been reported that the reduction of ANA responses might reflect the natural history of the disease as well as the effects of therapy [51]. Accordingly, these patients could have increased AGEs levels due to longer disease duration or more intense need for therapy due to more severe disease, and consequent more accrual damage and potentially higher AGEs levels. In our cohort, currently ANA- patients showed higher disease duration (15 vs 10 years) and higher SDI (same levels of p25 and p50 but differences in p75: 1.56 vs 0.68) although the differences were not statistically significant, probably due to lack of statistical power on account of the small sample size, also shown by the wide CI of this variable Supplementary Table S4. We didn’t observe differences in terms of taking immunosuppressants in the moment of the study between ANA+ and ANA- patients, but we didn’t retrieve data of the therapy history of patients, so we cannot rule out differences in the number of immunosuppressants or time taking therapy between both groups.
Despite the known relationship between AGEs and atherosclerosis, we did not find any correlation between AGEs levels and either CVRF or CVE. However, the p-value in the bivariate analysis was <0.1 and, considering that we have a small number of patients with CVE (N=9), it is likely that our results are limited by a lack of statistical power which prevents us from drawing conclusions about the role of AGEs in cardiovascular risk. Furthermore, we assessed cardiovascular disease only through traditional CVRF or CVE and did not perform additional tests like the intima-media thickness of the common carotid artery measured by ultrasound [28] or the small artery elasticity measured by pulse-wave analysis using tonometric recordings of the radial artery [27], both of which have been associated with AGEs levels in previous works. We also reassessed the correlation between AGEs and SDI excluding all variables related to cardiovascular disease (expressed as CVE in our study) as De Leeuw et al. do in their work [28]. They found a correlation in the bivariate analysis between skin AGEs and SDI, also after correction for the damage caused by CV disease. This association was not seen after adjusting for age or in the multivariate analysis. In our cohort, this new analysis did not alter the statistical correlation between SDI and AGEs, indicating that the association is not attributable to AGEs being associated to CV damage.
Only one of the two previous works studying skin AGEs in SLE have analyzed their association with disease characteristics, finding an association with age, creatinine, disease duration, the intima-media thickness of the common carotid artery, and the SDI in the univariate analysis, and only with age and disease duration in the multivariate one [28]. Our work has carried out a much more extensive analysis taking into account a great amount of demographic and clinical variables and performing a more complex statistical analysis considering all possible confounding factors, which provides a much deeper knowledge into these relationships and opens the door to the feasibility of using AGEs as a clinical tool for SLE management and prognosis.
Our study presents several limitations. Firstly, due to the retrospective nature of the study some data could not be retrieved like the cumulative GC dose that the patients had taken throughout the disease and we could only assess the impact of GC through the current dose at the moment of the study. Likewise, the design makes impossible to assess causality, which warrants future prospective studies. Secondly, and in order to clarify the effect on longstanding disease and therapy in AGEs levels, studies in newly diagnosed patients should be performed.
To our knowledge this is the second work to study and the first to find an association between SLE activity parameters and skin AGEs. We have found a correlation with, not one, but several SLE activity biomarkers and, also, with damage indexes. Furthermore, we have described, for the first time, skin AGEs associations with specific serological and clinical parameters that could define more precisely a specific type of patients in whom AGEs could have a particularly meaningful contribution. Therefore, our results are innovative and indicative of the promising role of AGEs and the AGEs skin reader as a tool to be implemented in daily clinical practice as a noninvasive, fast, real-time surrogate biomarker of SLE disease activity, damage and specific manifestations.
5. Conclusion
SLE patients present higher skin AGEs levels than HC, supporting the hypothesis of the association between AGEs and SLE. Furthermore, the correlation observed between skin AGEs levels and SLE activity and damage markers indicate that AGEs seem to have a role as a new biomarker in this disease related to management and prognosis, which would have enormous implications in a field currently uncovered in SLE. The association with specific antibodies and disease manifestations may indicate a particular clinical phenotype related to higher AGEs levels, unveiling another potential clinical use of these products.
Funding
This work was supported by the Instituto de Salud Carlos III (ISCIII) and the European Union (Grants number "PI18/00059", RETIC RD16/0009/0011), as well as by the Fundación Española de Reumatología through the Ayuda a la Intensificación de la Actividad Investigadora awarded in 2021, the Diputació de Lleida and Ministerio de Ciencia, Innovación y Universidades (IJC2018-037792-I).
Acknowledgments
We gratefully acknowledge all investigators who form part of the ILERVAS project. We would also like to thank the PhD program of the Universitat Autònoma de Barcelona, Dr. Isaac Alarcón Valero and Dr. María Grau Magaña for their support throughout the research process. The authors would like to thank to Virtudes María, Marta Elias, Teresa Molí, Cristina Domínguez, Noemí Nova, Alba Prunera, Núria Sans, Meritxell soria, Francesc Pons, Rebeca Senar, Pau Guix, Fundació Renal Jaume Arnó, and the Primary Care teams of the province of Lleida for recruiting participants and their efforts in the accurate development of the ILERVAS project. Samples were obtained with support from IRBLleida Biobank (B.0000682) and Plataforma Biobancos PT17/0015/0027.
Conflicts of Interest
All authors have read the journal's authorship agreement and policy on disclosure of potential conflicts of interest. The authors declare that they have no conflict of interest.
List of abbreviations
| AGEs: | Advanced glycation end-products |
| SLE: | systemic lupus erythematosus |
| HC: | healthy controls |
| SLEDAI: | SLE disease activity index |
| SDI: | damage index |
| PROs: | patient reported outcomes |
| RAGE: | AGEs receptor |
| LDL: | low-density lipoproteins |
| CVRF: | cardiovascular risk factors |
| SLICC: | Systemic Lupus International Collaborating Clinics |
| BMI: | body mass index |
| ANCOVA: | analysis of covariance |
| PGA: | physician global assessment |
| PtGA: | patient global assessment |
| ANA: | antinuclear antibodies |
| SjS: | Sjögren syndrome |
References
- Pan, L.; Lu, M.P.; Wang, J.H.; et al. Immunological pathogenesis and treatment of systemic lupus erythematosus. World J Pediatr 2020, 16, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Medzhitov, R. Origin and physiological roles of inflammation. Nature 2008, 454, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Rabbani, N.; Thornalley, P.J. Advanced glycation end products in the pathogenesis of chronic kidney disease. Kidney Int 2018, 93, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Delrue, C.; Speeckaert, R.; Joris, R. Delanghe and Marijn M. Speeckaert *. The Potential Influence of Advanced Glycation End Products and (s)RAGE in Rheumatic Diseases. Int J Mol Sci 2023, 24, 2894. [Google Scholar] [CrossRef] [PubMed]
- Gkogkolou, P.; Böhm, M. Advanced glycation end products: Keyplayers in skin aging? Dermatoendocrinol 2012, 4, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N. Advanced glycation endproducts - Role in pathology of diabetic complications. Diabetes Res Clin Pract 2005, 67, 3–21. [Google Scholar] [CrossRef]
- Baynes, J.W. Chemical modification of proteins by lipids in diabetes. Clin Chem Lab Med 2003, 41, 1159–1165. [Google Scholar] [CrossRef]
- Turner, D.P. Advanced glycation end-products: A biological consequence of lifestyle contributing to cancer disparity. Cancer Res 2015, 75, 1925–1929. [Google Scholar] [CrossRef]
- Del Turco, S.; Basta, G. An update on advanced glycation endproducts and atherosclerosis. BioFactors 2012, 38, 266–274. [Google Scholar] [CrossRef]
- Sugiyama, S.; Miyata, T.; Inagi, R.; et al. Implication of the glycoxidation and lipoxidation reactions in the pathogenesis of dialysis-related amyloidosis (Review). Int J Mol Med 1998, 2, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Liu, D.; Sun, L.; et al. Advanced glycation end products and neurodegenerative diseases: Mechanisms and perspective. J Neurol Sci 2012, 317, 1–5. [Google Scholar] [CrossRef]
- Flier, J.S.; Underhill, L.H.; Brownlee, M.; et al. Advanced Glycosylation End Products in Tissue and the Biochemical Basis of Diabetic Complications. N Engl J Med 1988, 318, 1315–1321. [Google Scholar] [CrossRef] [PubMed]
- Vistoli, G.; De Maddis, D.; Cipak, A.; et al. Advanced glycoxidation and lipoxidation end products (AGEs and ALEs): An overview of their mechanisms of formation. Free Radic Res 2013, 47, 3–27. [Google Scholar] [CrossRef] [PubMed]
- Kurien, B.T.; Hensley, K.; Bachmann, M.; et al. Oxidatively modified autoantigens in autoimmune diseases. Free Radic Biol Med 2006, 41, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Pullerits, R.; Bokarewa, M.; Dahlberg, L.; et al. Decreased levels of soluble receptor for advanced glycation end products in patients with rheumatoid arthritis indicating deficient inflammatory control. Arthritis Res Ther 2005, 7, R817–24. [Google Scholar] [CrossRef]
- Hudson, B.I.; Lippman, M.E. Targeting RAGE Signaling in Inflammatory Disease. Annu Rev Med 2018, 69, 349–364. [Google Scholar] [CrossRef]
- Chiappalupi, S.; Sorci, G.; Vukasinovic, A.; et al. Targeting RAGE prevents muscle wasting and prolongs survival in cancer cachexia. J Cachexia Sarcopenia Muscle 2020, 11, 929–946. [Google Scholar] [CrossRef]
- Sárkány, Z.; Ikonen, T.P.; Ferreira-da-Silva, F.; et al. Solution structure of the soluble receptor for advanced glycation end products (sRAGE). J Biol Chem 2011, 286, 37525–37534. [Google Scholar] [CrossRef]
- Geroldi, D.; Falcone, C.; Emanuele, E. Soluble Receptor for Advanced Glycation End Products: From Disease Marker to Potential Therapeutic Target. Curr Med Chem 2006, 13, 1971–1978. [Google Scholar] [CrossRef]
- Nienhuis, H.L.; De leeuw, K.; Bijzet, J.; et al. Skin autofluorescence is increased in systemic lupus erythematosus but is not reflected by elevated plasma levels of advanced glycation endproducts. Rheumatology 2008, 47, 1554–1558. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, S.R.; Baynes, J.W. Maillard reaction products in tissue proteins: New products and new perspectives. Amino Acids 2003, 25, 275–281. [Google Scholar] [CrossRef]
- Perrone, A.; Giovino, A.; Benny, J.; et al. Advanced Glycation End Products (AGEs): Biochemistry, Signaling, Analytical Methods, and Epigenetic Effects. Oxid Med Cell Longev 2020, 3818196. [Google Scholar] [CrossRef]
- Meerwaldt, R.; Graaf, R.; Oomen, P.H.N.; et al. Simple non-invasive assessment of advanced glycation endproduct accumulation. Diabetologia 2004, 47, 1324–1330. [Google Scholar] [CrossRef] [PubMed]
- Nowak, A.; Przywara-Chowaniec, B.; Damasiewicz-Bodzek, A.; et al. Advanced glycation end-products (Ages) and their soluble receptor (srage) in women suffering from systemic lupus erythematosus (sle). Cells 2021, 10, 3523. [Google Scholar] [CrossRef]
- Ene, C.D.; Georgescu, S.R.; Tampa, M.; et al. Cellular response against oxidative stress, a novel insight into lupus nephritis pathogenesis. J Pers Med 2021, 11, 693. [Google Scholar] [CrossRef]
- Chen, D.Y.; Chen, Y.M.; Lin, C.C.; et al. The potential role of advanced glycation end products (AGEs) and soluble receptors for AGEs (sRAGE) in the pathogenesis of adult-onset still’s disease. BMC Musculoskelet Disord 2015, 16, 111. [Google Scholar] [CrossRef]
- Nienhuis, H.L.A.; de Leeuw, K.; Bijzet, J.; et al. Small artery elasticity is decreased in patients with systemic lupus erythematosus without increased intima media thickness. Arthritis Res Ther 2010, 12, R181. [Google Scholar] [CrossRef] [PubMed]
- de leeuw, K.; Graaff, R.; de Vries, R.; et al. Accumulation of advanced glycation endproducts in patients with systemic lupus erythematosus. Rheumatology 2007, 46, 1551–1556. [Google Scholar] [CrossRef] [PubMed]
- Quyyumi, A.A. Inflamed Joints and Stiff Arteries. Circulation 2006, 114, 1137–1139. [Google Scholar] [CrossRef]
- Makita, Z.; Yanagisawa, K.; Kuwajima, S.; et al. The role of advanced glycosylation end-products in the pathogenesis of atherosclerosis. Nephrol Dial Transplant 1996, 11, 31–33. [Google Scholar] [CrossRef]
- Vekic, J.; Zeljkovic, A.; Cicero, A. F.; Janez, A.; Stoian, A. P.; Sonmez, A.; Rizzo, M. The Role of Advanced Glycation End Products on Dyslipidemia. Metabolites 2023, 13, 77. [Google Scholar]
- De Leeuw, K.; Freire, B.; Smit, A.J.; et al. Traditional and non-traditional risk factors contribute to the development of accelerated atherosclerosis in patients with systemic lupus erythematosus. Lupus 2006, 15, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Chavakis, T.; Bierhaus, A.; Nawroth, P.P. RAGE (receptor for advanced glycation end products): A central player in the inflammatory response. Microbes Infect 2004, 6, 1219–1225. [Google Scholar] [CrossRef]
- Goldberg, T.; Cai, W.; Peppa, M.; et al. Advanced glycoxidation end products in commonly consumed foods. J Am Diet Assoc 2004, 104, 1287–1291. [Google Scholar] [CrossRef] [PubMed]
- Prasad, K.; Mishra, M. Do Advanced Glycation End Products and Its Receptor Play a Role in Pathophysiology of Hypertension? Int J Angiol 2017, 26, 1–11. [Google Scholar] [CrossRef]
- Leslie, R.D.G.; Beyan, H.; Sawtell, P.; et al. Level of an advanced glycated end product is genetically determined: A study of normal twins. Diabetes 2003, 52, 2441–2444. [Google Scholar] [CrossRef]
- Hochberg, M.C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 1997, 40, 1725–1725. [Google Scholar] [CrossRef]
- Petri, M.; Orbai, A.M.; Alarcõn, G.S.; et al. Derivation and validation of the systemic lupus international collaborating clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum 2012, 64, 2677–2686. [Google Scholar] [CrossRef]
- Available online: https://elbusdelasalut.cat/professionals/protocol-estudi/.
- Shardlow, A.; McIntyre, N.J.; Kolhe, N.V.; et al. The association of skin autofluorescence with cardiovascular events and all-cause mortality in persons with chronic kidney disease stage 3: A prospective cohort study. PLoS Med 2020, 17, e1003163. [Google Scholar] [CrossRef]
- Peters, M.J.L.; Symmons, D.P.M.; McCarey, D.; et al. EULAR evidence-based recommendations for cardiovascular risk management in patients with rheumatoid arthritis and other forms of inflammatory arthritis. Ann Rheum Dis 2010, 69, 325–331. [Google Scholar] [CrossRef]
- Raj, D.S.; Choudhury, D.; Welbourne, T.C. Advanced glycation end products: A nephrologist’s perspective. Am J Kidney Dis 2000, 35, 365–380. [Google Scholar] [CrossRef]
- Sourris, K.C.; Watson, A.; Jandeleit-Dahm, K. Inhibitors of Advanced Glycation End Product (AGE) Formation and Accumulation. Handb Exp Pharmacol 2021, 264, 395–423. [Google Scholar] [CrossRef]
- Weinstein, A.; Alexander, R.V.; Zack, D.J. A Review of Complement Activation in SLE. Curr Rheumatol Rep 2021, 23, 1–8. [Google Scholar] [CrossRef]
- Gandino, I.J.; Scolnik, M.; Bertiller, E.; et al. Complement levels and risk of organ involvement in patients with systemic lupus erythematosus. Lupus Sci Med 2017, 4, e000209. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Lin, S.; Yang, S.; et al. Diagnostic value of serum complement C3 and C4 levels in Chinese patients with systemic lupus erythematosus. Clin Rheumatol 2015, 34, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.E.; Mun, S.; Kim, S.M.; Shin, W.; Jung, W.; Paek, J.; Cha, S. The inflammatory signature in monocytes of Sjögren’s syndrome and systemic lupus erythematosus, revealed by the integrated Reactome and drug target analysis. Genes Genomics 2022, 44, 1215–1229. [Google Scholar] [CrossRef]
- Stewart, C.; Cha, S.; Caudle, R.M.; et al. Decreased levels of soluble receptor for advanced glycation end products in patients with primary Sjögren’s syndrome. Rheumatol Int 2008, 28, 771–776. [Google Scholar] [CrossRef]
- Katz, J.; Stavropoulos, F.; Bhattacharyya, I.; et al. Receptor of advanced glycation end product (RAGE) expression in the minor salivary glands of patients with Sjögren’s syndrome: A preliminary study. Scand J Rheumatol 2004, 33, 174–178. [Google Scholar] [CrossRef] [PubMed]
- Kanne, A.M.; Jülich, M.; Mahmutovic, A.; et al. Association of High Mobility Group Box Chromosomal Protein 1 and Receptor for Advanced Glycation End Products Serum Concentrations With Extraglandular Involvement and Disease Activity in Sjögren’s Syndrome. Arthritis Care Res 2018, 70, 944–948. [Google Scholar] [CrossRef]
- Pisetsky, D.S.; Lipsky, P.E. New insights into the role of antinuclear antibodies in systemic lupus erythematosus. Nat Rev Rheumatol 2020, 16, 565–579. [Google Scholar] [CrossRef]
Figure 1.
Statistically significant associations between AGEs levels and SLE characteristics and indexes. P-values <0.05 (bold) indicate significant differences between the categories and the reference level of each variable; p-values not in bold indicate associations not statistically signifi-cant. PtGA: patient global assessment; PGA: physician global assessment; SDI: SLE damage index; SLEDAI: SLE disease activity index.
Figure 1.
Statistically significant associations between AGEs levels and SLE characteristics and indexes. P-values <0.05 (bold) indicate significant differences between the categories and the reference level of each variable; p-values not in bold indicate associations not statistically signifi-cant. PtGA: patient global assessment; PGA: physician global assessment; SDI: SLE damage index; SLEDAI: SLE disease activity index.
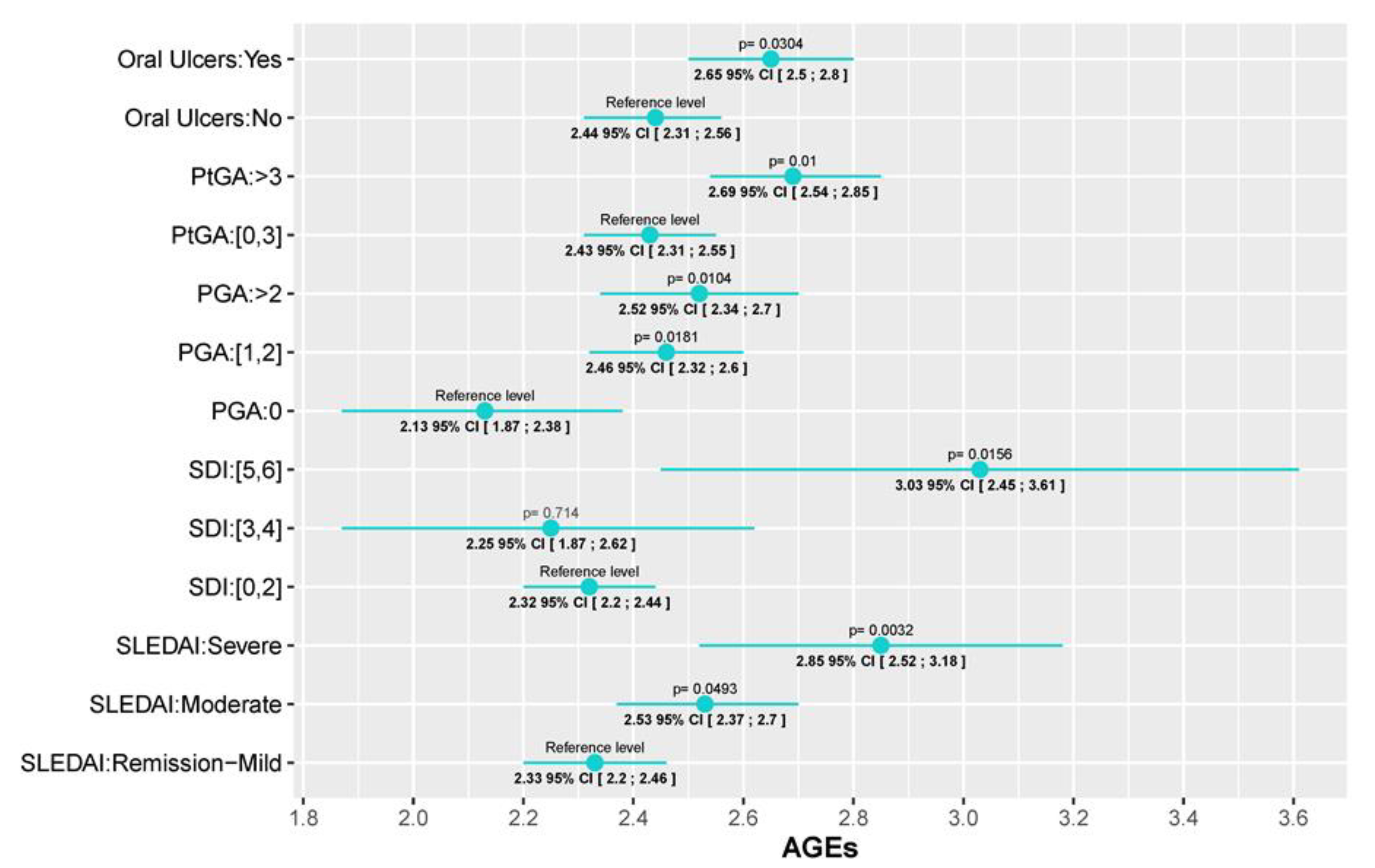
Figure 2.
Statistically significant correlations between AGEs levels and SLE serological parame-ters. The change in AGEs values is depicted according to the reference category of each variable. p-value is considered significant if <0.05. IL-6: interleukin 6 (pg/mL); C4: complement 4 (mg/dL); CRP: C-reactive protein (mg/dL).
Figure 2.
Statistically significant correlations between AGEs levels and SLE serological parame-ters. The change in AGEs values is depicted according to the reference category of each variable. p-value is considered significant if <0.05. IL-6: interleukin 6 (pg/mL); C4: complement 4 (mg/dL); CRP: C-reactive protein (mg/dL).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



