
Submitted:
01 February 2024
Posted:
02 February 2024
Read the latest preprint version here
Abstract
Background: Granular cell tumor is a benign neurogenic tumor of the subcutaneous and submucosal area. The tongue is the most affected site of the oral cavity. The clinical presentation is non-specific and manifests as a submucosal nodule or mass. Because of its non-specific presentation, a definitive diagnosis an only be established after a histopathological examination and an immunohistochemical study to search for a neurogenic origin. Methods: We report the case of a 48-year-old man who was referred for the management of a nodular lesion on the tip of his tongue that had increased in size over the previous three months. Results: A complete surgical excision was performed for the histopathological exam, and an immunohistochemical study confirmed a strong expression of S100 and CD68. A diagnosis of granular cell tumor was confirmed. There was no recurrence et three years follow-up. Conclusion: the GCT is a rare tumor of nervous origin of the oral mucosa, it is non-specific in expression, with a good prognosis after complete excision. the histological and immunohistochemical diagnosis of the lesion is essential for the diagnosis.
Keywords:
Benign nerve sheath tumors
; Abrikossoff’s tumor
; granular cell
; oral pathologist
; peripheral nerve disorders
; tongue
; s100 protein.
1. Introduction
Granular cell tumor, formerly called Abrikossoff’s tumor, is considered as a benign tumor of the subcutaneous and submucosa area. The preferential localization is the head and neck mucosa, and especially the dorsal tongue mucosa [1]. This tropism related to its tissue origin because granular cell tumors are considered nerve sheath tumors. Their clinical expression is similar to other solitary, small and benign tumors of the oral mucosa. These tumors are painless and grow slowly, except rare syndromic forms [1,2]. The diagnosis is based on pathological examination and immunohistochemical confirmation of neural origin with S100 and CD68 expression [2]. The classical treatment for a granular cell tumor is surgical excision with safety margins. Recurrence most often result from an incomplete resection or malignant forms. The benign form has an excellent prognosis, although its pathogenesis remains unknown. Professionals in oral medicine should be familiar with granular cell tumors. Furthermore, granular cell tumors should be considered a differential diagnosis for any isolated nodule of the oral mucosa, particularly on the tongue.
2. Case Presentation
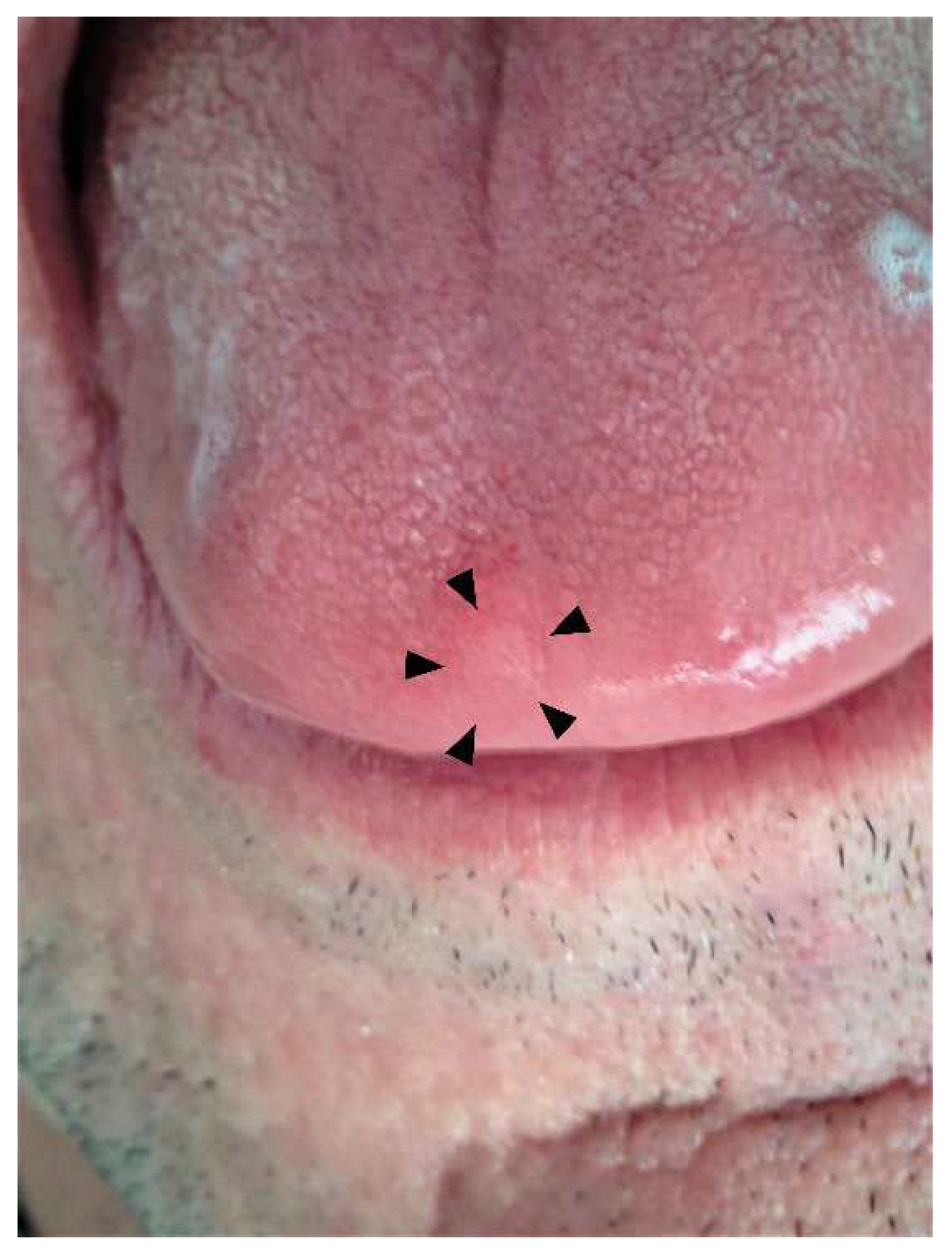
A 48-year-old man with no medical or surgical history was referred by his dentist for an asymptomatic lingual nodule. According to the patient, the lesion had been progressing for three months. He also had trouble speaking. The intraoral examination revealed a submucosal nodule covered with healthy mucosa. The nodule was located on the dorsum of the tip of the tongue, [Figure 1] measured about 3 mm in diameter, and was firm to palpation.
Palpation of the cervicofacial lymph nodes was normal. Diagnostic hypotheses included fibroepithelial nodule, neurogenic benign tumor, fibroma, and myogenic benign tumor among others. An excisional biopsy was performed based on the benign clinical features.
Microscopical analysis revealed a massive, non-encapsulated, well limited tumor and under an acanthosic epithelium [Figure 2A].
The proliferation was composed of large, granular cells with centrally located, small, dark, nucleolated nuclei, with an abundant eosinophilic cytoplasm dissociating muscular bundles [Figure 2B,C].
Figure 3.
Representative histological and immunohistochemical findings. (A, B) Hematein-Eosin-Saffron Stain revealed acanthosic epithelium and massive tumor well limited and no encapsulated with pseudo infiltrative and fibrosis aspect dissociating muscular bundles in the under mucosa part and pushing effect in the deep part. The resection was complete.(A: x2.5; B x10 magnification). (C) large granular cells with central small dark nuclei with an abundant eosinophilic cytoplasm. (D) periodic acid-Schiff (PAS) stain revealed PAS-positive cytoplasmic granulation. (E) strongly positive immunostaining for S100 (yellow head of arrow shown nervous thread as internal positive control) (x20 magnification). (F) strongly positive immunostaining for CD68.G: Ki-67 immunolabelling shown absence of proliferation of tumor cell (insert: positive control in oral epithelium).
Figure 3.
Representative histological and immunohistochemical findings. (A, B) Hematein-Eosin-Saffron Stain revealed acanthosic epithelium and massive tumor well limited and no encapsulated with pseudo infiltrative and fibrosis aspect dissociating muscular bundles in the under mucosa part and pushing effect in the deep part. The resection was complete.(A: x2.5; B x10 magnification). (C) large granular cells with central small dark nuclei with an abundant eosinophilic cytoplasm. (D) periodic acid-Schiff (PAS) stain revealed PAS-positive cytoplasmic granulation. (E) strongly positive immunostaining for S100 (yellow head of arrow shown nervous thread as internal positive control) (x20 magnification). (F) strongly positive immunostaining for CD68.G: Ki-67 immunolabelling shown absence of proliferation of tumor cell (insert: positive control in oral epithelium).
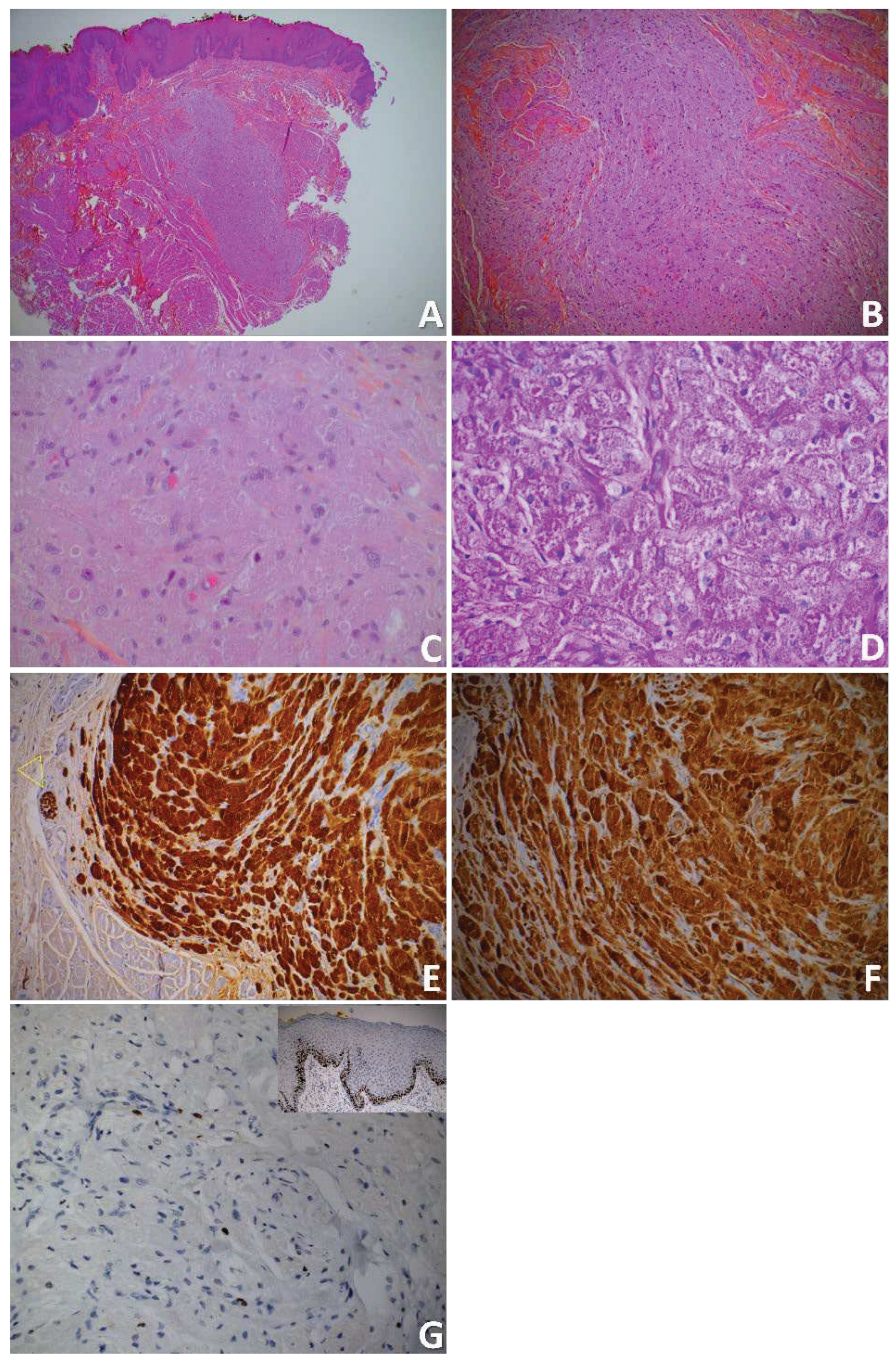
No mitosis, necrosis, or marked cellular atypia were identified. The PAS staining revealed PAS-positive cytoplasmic granulation [Figure 2D]. Immunohistochemical staining showed that tumor cells were strongly positive for S100 protein [Figure 2E] and CD68 [Figure 2F] but negative for AE1/AE3 immunostaining. Ki-67 immunostaining did not shown immunoreactivity for tumor cells. [Figure 2G].
All investigations agree with the diagnosis of a granular cell tumor.
The surgical resection was completed. At Three years follow-up, the patient had no recurrence.
3. Discussion
Granular cell tumor (GCT) is an rare, benign soft tissue tumor, it is classified by WHO [2] among soft tissue and neural tumors in the section tumors of the oral cavity and mobile tongue. It was described for the first time by Abrikossoff in 1926 as a tumor of stratified muscle origin. It was initially called myoblastoma [3] because of the unencapsulated tumor and intermingling of the skeletal muscle bundles. Since then, it has acquired other names, including granular cell neurofibroma, granular cell schwannoma and Abrikossoff’s tumor. Today, the immunohistochemical studies are consistent with Schwannian origin, which suggests a peripheral nerve sheath differentiation and neural origin [2,4]. This hypothesis is in agreement with the ultrastructural observations in electron microscopy studies [5,6] and the absence of the myoglobin in the granular cytoplasm of the cells. The etiopathogenesis of GCT remains uncertain, and some authors suggest a reactive origin [1]. GCT can affect any subcutaneous and submucosal sites in the body. The intraoral GCT are generally diagnosed between the 40 and 60 years old. With a peak in patients who are in their 50s [1,2]. Our 48-year-old patient was is in the peak age range of prevalence when he was diagnosed. However, rare pediatric cases have been reported [7]. There have been no reported cases in elderly subjects. The oldest reported patient was 68 years old [8]. Black populations are more affected than white population, and women are more affected than men, with female-to-male ratio of 2:1 [2]. However, women represent more than 75% of GCT cases in this intraoral location [1]. The oral cavity is the most common location reported in the literature, with a prevalence of about 70%. The tongue is the most common intraoral site with more than 85% [1,2]. GCT usually occurs on the dorsum of the tongue along the lateral edge and less frequently on the tip of the tongue. The average size is 1 cm, but GCTs can range form a few millimeters to 3 cm.
Clinically, GCT of the oral mucosa appears as a single isolated lesion,. However, it can also occur as multiple lesions [9], especially in the context of syndromes such Leopard syndrome, neurofibromatosis, Noonan syndrome, and Watson syndrome [10].
Within the oral cavity, it usually presents as a slow-growing, well-limited, round or oval submucosal, asymptomatic mass, usually discovered incidentally. It is generally asymptomatic, but patients often complain of a growing mass that can sometimes cause discomfort or pain. On palpation, the GCT is usually painless, firm, rubbery, well-limited, and nonencapsulated. The surface mucosa is usually healthy with a slightly modified, grainy appearance and a lack of taste buds. Our patient reported discomfort in speaking caused by the GCT at the tip of the tongue. The GCT had increased in size for about 3 months. The size of the lesion remained small, about 3 mm on the day of the consultation. The surface appearance was healthy.
For the superficial lesions, the appearance can be yellowish or creamy-white. Local trauma at the site of the lesion has been reported sporadically, in addition to ulceration from the consumption of alcohol, tobacco, or nicorandil [11,12].
The clinical expression of GCT remains nonspecific and requires a differential diagnosis with other nodular lesions of slow and painless growth in the oral mucosa. It is difficult to distinguish a GCT in front of a submucosal nodule of the tongue from a neurofibroma, schwannoma, lipoma, or even a benign fibroepithelial hyperplasia [12]. Radiological examination is of little used, particularly in small lesions with a clearly benign appearance. However, if the tumor reveals signs of aggressiveness, such as infiltration of neighboring structures, location on deep plane, high speed of growth, and rapid recurrence, a computer tomography or magnetic resonance imaging should be used to detect tumor infiltration and metastases [13].
Histopathological examination is essential to establish definitive diagnosis. GCT is an unencapsulated tumor whose cells intermingle with adjacent normal tissue by bands of connective tissue. GCT is characterized by the presence of sheets and cords of large, polygonal, round, or elongated cells with indistinct membranes containing abundant eosinophilic granular cytoplasm. The granules are PAS positive. The nuclei are small and central located with dense chromatin.
Two architectural growth patterns can be distinguished in the GCTs [14]. The first pattern is, with a nodule surrounded by the residual structure, often pushing on muscle and collagen fibers. A large nerve trunk is often found in the center. The second pattern features cords and small nests infiltrating the surrounding mesenchymal structures, where only small nerve bundles are present. Both patterns are present in GCT. In our case, the tumor was nodular, pushing into the deepest part. A pseudo infiltrative pattern was present in the deepest part of the submucosa. We did not observe a large nervous trunk in the tumor. Only small nerve bundles were present [Figure 2E]. Necrosis and mitosis were absent. All these microscopical criteria are characteristic of the majority of typical GCTs, which are benign tumors with no metastatic potential, as reported by Fanburg-Smith et al. [15]. However, features such as mitotic figures, spindle cell formation, slight nuclear polymorphism, or increased nuclear cytoplasmic ratio can present focally with atypical forms of GCTs. These slight modifications remain far outside the spectrum of cytonuclear modifications of malignant forms, which present numerous unfavorable histological criteria, such as strong cellularity, cellular atypia, spiny cells, cellular polymorphism, an increased nuclear-cytoplasmic ratio with prominent nucleoli, and the presence of focal or extensive tumor necrosis [16]. Nasser et Al proposed using the Ki-67 and p53 immunolabelling index to differentiate between benign and aggressive/malignant behavior. A rate of Ki-67 of 10% was suggested for a cutoff [17]. In our observation, the Ki-67 index was less than 5%. However, metastases is the only definitive criterion for malignancy in GCT, regardless of the histopathologic characteristics. Malignant GCTs are rare, representing approximately 2% of cases [17]. To our knowledge, no case of malignant GCT of oral localization has been reported in the literature to date. GCTs can induce pseudoepiheliomatous hyperplasia with acanthosis on the overlying epithelium, appearing it about 30% to 50% of the cases in the oral cavity. This can be pronounced and appear as a well-differentiated cell carcinoma, leading to an incorrect diagnosis, particularly with shallow surgical biopsies of large lesions. Some authors have reported that histopathological examination exhibits pathognomonic features, making an immunohistochemical examination unnecessary [18]. However, Immunohistochemical examination have shown that granular cell have high reactivity for S100 protein, CD68, vimentin, and neuron-specific enolase (NSE). An immunohistochemical examination is essential to establish a definitive diagnosis because it is difficult to clinically diagnose GCT [19]. Notably, cases of GCT with negative S100 staining have been reported [20]. Management of oral GCT is primarily surgical with a an excellent prognostic without recurrence when the excision is complete. Our patient had no recurrence at his three years follow-up, and the mucosa on the tip of the tongue was healthy.
4. Conclusions
GCT are benign tumors of neural origin with nonspecific clinical expression. They present in the majority of cases in the form of a nodular mucosal swelling in the oral mucosa. The clinical characteristics are those of a slow-growing, painless, benign lesion with a typical surface appearance of healthy mucosa. Oral symptomatology is linked to its size and the degree of modification of the mucosal surface. GCTs sometimes cause speech disturbances. Surgical treatment by complete excision is the treatment of choice, and recurrences are exceptional. A posteriori diagnosis using histological and immunostaining examination for nerve sheaths is required to confirm a neural origin for this rare tumor of the oral mucosa.
Author Contributions
HH Conceived the idea, reviewed and approved the manuscript, and involved in patient management. HH and CB drafted the manuscript, and involved in patient management. AD reviewed and approved the manuscript, especially for histopathological sections.
Funding
This research received no external funding
Institutional Review Board Statement
Ethical review and approval were waived for this study since IRB is not required for single patient case studies.
Informed Consent Statement
Finally, regarding CARE guidelines, we obtain the signed informed consent of the patient to publish online his case in an open access format paper. We believe that authors have an ethical duty to obtain informed consent from the patient to publish patient information in a case report. Consent becomes informed when the patient or a relative reads the case report and approves its contents, as happened in this case.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Mendoza ILI de Ortega, K.L.; Trierveiler, M.; et al. Oral granular cell tumour: A multicentric study of 56 cases and a systematic review. Oral Dis 2020, 26, 573–589. [Google Scholar] [CrossRef] [PubMed]
- El-Naggar, A.K.; Chan, J.K.C.; Grandis, J.R.; Takata, T.; Slootweg, P.J. (Eds.). (2017). WHO Classification of Head and Neck Tumours. (4th edition). (Vol. 9). https://publications.iarc.fr/Book-And-Report-Series/Who-Classification-Of-Tumours/WHO-Classification-Of-Head-And-Neck-Tumours-2017 (accessed 10 May 2023). 10 May.
- Abrikossoff, A. Uber myome, ausgehend von der quergestreiften willkurlichen Muskulatur. Virchows Arch Pathol Anat Physiol Klin Med 1926, 260, 215–233. [Google Scholar] [CrossRef]
- Franco, T.; De Freitas Filho, S.A.J.; Muniz, L.-B.; De Faria, P.R.; Loyola, A.M.; Cardoso, S.V. Oral peripheral nerve sheath tumors: A clinicopathological and immunohistochemical study of 32 cases in a Brazilian population. J Clin Exp Dent 2017, 9, e1459–65. [Google Scholar] [CrossRef] [PubMed]
- Manara, G.C.; De Panfilis, G.; Bacchi, A.B.; et al. Fine structure of granular cell tumor of Abrikosov. J Cutan Pathol 1981, 8, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Okada, H.; Yamamoto, H.; Kawana, T.; Katoh, T.; Kozawa, Y.; Hayashi, I. Granular cell tumor of the tongue: an electron microscopical and immunohistochemical study. J Nihon Univ Sch Dent 1990, 32, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Nagaraj, P.B.; Ongole, R.; Bhujanga-Rao, B.R. Granular cell tumor of the tongue in a 6-year-old girl--a case report. Med Oral Patol Oral Cirugia Bucal 2006, 11, E162–E164. [Google Scholar]
- Karakostas, P.; Matiakis, A.; Anagnostou, E.; Kolokotronis, A. Oral granular cell tumor: Report of case series and a brief review of the literature. Balk J Dent Med 2017, 21, 116–118. [Google Scholar] [CrossRef]
- Bomfin, L.E.; De Abreu Alves, F.; De Almeida, O.P.; Kowalski, L.P.; Da Cruz Perez, D.E. Multiple granular cell tumors of the tongue and parotid gland. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009, 107, e10–e13. [Google Scholar] [CrossRef] [PubMed]
- Bamps, S.; Oyen, T.; Legius, E.; Vandenoord, J.; Stas, M. Multiple granular cell tumors in a child with Noonan syndrome. Eur J Pediatr Surg Off J Austrian Assoc Pediatr Surg Al Z Kinderchir 2013, 23, 257–259. [Google Scholar] [CrossRef]
- Dive, A.; Dhobley, A.; Fande, P.Z.; Dixit, S. Granular cell tumor of the tongue: Report of a case. J Oral Maxillofac Pathol 2013, 17, 148. [Google Scholar] [CrossRef] [PubMed]
- Cole, E.; Rahman, N.; Webb, R. Case series: Two cases of an atypical presentation of oral granular cell tumour. Case Rep Med 2012, 2012, 159803. [Google Scholar] [CrossRef] [PubMed]
- Budiño-Carbonero, S.; Navarro-Vergara, P.; Rodriguez-Ruiz, J.; Modelo-Sánchez, A.; Torres-Garzón, L.; Rendón-Infante, J.I.; Fortis-Sánchez, E. Granular cell tumors: Review of the parameters determining possible malignancy. Med Oral Organo Of Soc Espanola Med Oral Acad Iberoam Patol Med Bucal 2003, 8, 294–298. [Google Scholar]
- Maiorano, E.; Favia, G.; Napoli, A.; Resta, L.; Ricco, R.; Viale, G.; Altini, M. Cellular heterogeneity of granular cell tumours: A clue to their nature? J Oral Pathol Med Off Publ Int Assoc Oral Pathol Am Acad Oral Pathol 2000, 29, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Fanburg-Smith, J.C.; Meis-Kindblom, J.M.; Fante, R.; Kindblom, L.G. Malignant granular cell tumor of soft tissue: Diagnostic criteria and clinicopathologic correlation. Am J Surg Pathol 1998, 22, 779–794. [Google Scholar] [CrossRef]
- Machado, I.; Cruz, J.; Lavernia, J.; Llombart-Bosch, A. Solitary, multiple, benign, atypical, or malignant: The “Granular Cell Tumor” puzzle. Virchows Arch Int J Pathol 2016, 468, 527–538. [Google Scholar] [CrossRef] [PubMed]
- Nasser, H.; Ahmed, Y.; Szpunar, S.; Kowalski, P. Malignant granular cell tumor: A look into the diagnostic criteria. Pathol Res Pract 2011, 207, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Tamiolakis, P.; Chrysomali, E.; Sklavounou-Andrikopoulou, A.; Nikitakis, N.G. Oral neural tumors: Clinicopathologic analysis of 157 cases and review of the literature. J Clin Exp Dent 2019, 11, e721–31. [Google Scholar] [CrossRef] [PubMed]
- Atarbashi-Moghadam, S.; Saebnoori, H.; Shamloo, N.; Barouj, M.D.; Saedi, S. Granular cell odontogenic tumor, an extremely rare case report. J Dent 2019, 20, 220–223. [Google Scholar] [CrossRef]
- Rawal, Y.B.; Dodson, T.B. S-100 negative granular cell tumor (So-called primitive polypoid non-neural granular cell tumor) of the oral cavity. Head Neck Pathol 2017, 11, 404–412. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
Clinical preoperative view of the nodule of the tip of the tongue.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



