
Submitted:
04 February 2024
Posted:
05 February 2024
You are already at the latest version
Abstract
Background: Despite scientific advances, the management of procedural pain in neonates remains suboptimal. Applying adequate therapy to control pain during the neonatal period is a moral and ethical act. In recent decades, ample evidence has accumulated regarding the risks, associated with both untreated pain and the use of more aggressive analgesic therapy. Thus, the emphasis in neonatal clinical practice is on non-aggressive pain management techniques, including homeopathic agents. The efficacy and safety of homeopathic agents for reducing procedural pain in neonates is the subject of the present study. Materials and Methods: Healthy full-term newborn babies with an average age of 72-84 hours were included. They were divided into three study groups: group (A) – not anesthetised, /n= 67/, group (B) – anesthetised with Arnica D30 /n=40/ and group (C)- anesthetised with Sol.Glucose 25% /n=40/. The severity of the pain was assessed using the multimodal - Neonatal Infant Pain Scale (NIPS) and the unimodal - Neonatal Facial Coding System (NFCS) scale. Assessments were done 30s before, 30 seconds after, and 5 minutes after the painful stimulus caused by the heel prick. Heart rate, transcutaneous oxygen saturation, respiratory rate and blood pressure were examined at the same intervals. The results obtained were processed statistically by descriptive analysis and ANOVA at a significance level of p< 0.05. Results: 5 minutes after heel prick both scales showed a statistically significant lower score in those given Arnica D30, compared to those who received Sol.Glucose 25%. When monitoring the physiological indicators, we found a significant increase in the heart rate 30 seconds after the procedure.5 minutes after the heel prick we recorded significantly respiratory rate and systolic blood pressure in all three groups compared to pre-procedural values. Conclusions: Arnica D30 has better analgesic effects compared to Sol.Glucose 25% for newborn babies after heel prick tests.
Keywords:
newborn
; procedural pain
; non-pharmacological methods
; homeopathy
1. Introduction
In recent years, much has been discussed around the diagnosis and methods to control pain in newborn babies. The daily care of newborns, as well as diagnostic and treatment activities, are the cause of discomfort, stress and pain to varying degrees. Heel pricking is considered to be the third most intensive pain procedure in intensive care units and represents 79.2% of all painful manipulations performed without analgesia.[1]. The use of Arnica D30 for managing procedural pain in newborns is a new alternative in clinical practice, which is the basis for our study. The aim of this is to determine and compare the analgesic effect of Arnica D30 and Sol.Glucose 25% on procedural pain induced by heel prick.
2. Materials and Methods
A prospective study on healthy, full-term newborns /n= 164/ in the Obstetrics and Gynecology Clinic, Neonatology Department of the "St. Georgi"- the city of Plovdiv for the period from 07.10.2016 to 15.04.2017, at an average age of 72-84 hours. Our study was based on CONSORT guideline. The full-term newborns were divided into three groups: control group - without anesthesia A( n=67), anesthetised with Arnica D30 B( n=57), and with Sol.Glucose 25% C( n=40). The study group had birth weight 3261.60 ± 205.35, and no evidence of perinatal asphyxia. 68 (41.47%) of the study group had a normal birth, 91 (55.49%) by caesarean section, 4 (2.44%) by vacuum extractor and 1 (0.60%) using forceps. Procedural pain was induced in each newborn during the national neonatal screening for phenylketonuria, congenital hypothyroidism and congenital adrenal hyperplasia between the 72nd and 84th hour after birth by a single puncture of the heel on the latero- or postero-medial surface with a medical needle №20. The procedure is carried out when the baby is calm and about 40 minutes after feeding. The severity of the procedural pain was assessed by video surveillance before, during and after the procedure using the Neonatal Infant Pain Scale (NIPS) and the Neonatal Facial Coding System (NFCS). Analysis of the videos was performed by two independent neonatologist surveyors, trained to use the relevant pain assessment scales. In cases of discrepancy in the values of the evaluation score up to 2, arbitration was carried out by a third neonatologist - an expert on the indicated scales, and his assessment was accepted as final. Patients with a difference of more than 2 points were excluded from the study. Heart rate, respiratory rate, arterial blood pressure and transcutaneous saturation (tSpO2) were also monitored with a Biocare iM/2014 monitor. Results were taken 30 seconds before the heal prick test, 30 seconds and 5 min after, as well as in the interval 12–24 h. In Group B neonates, Arnica D30 is administered orally as an individual solution of three pills in sterile water for analgesia. Each intake was 1 ml. The first reception is 2 hours before, the second immediately after the prick test, and the third in the interval 12 - 24 hours after the procedure, i.e. - a total of 3x1ml per os. For newborns of group C, the anesthesia was performed by Sol.Glucose 25% 2 ml. per os 2 min before the heel prick.
2.1. Inclusion and Exclusion Criteria
2.1.1. Inclusion Criteria
Full-term newborns - definition of full-term according to the criteria of ICD 10 /birth at a gestational age of 37 full weeks to less than 42 full weeks (259-293) days/i.e. 37-41 GA with + 6 days (chronological gestational age).
No primary resuscitation - Apgar at the 1st and 5th minutes of birth - optimal 8-10.
Normal postpartum adaptation - physiological jaundice (indirect bilirubin below 240μmol/L between the 72nd - 84th hour (Brϋster - Wirtz table), normal weight loss after birth (<10% of birth weight).
No abnormalities in muscle tone, reflexes, and motor activity assessed by clinical examina-tion prior to initiation of screening.
No drug therapy – no antimicrobial preparations, symptomatic drugs, biological products, oxygen therapy or intensive treatment.
Written informed consent from the mother for participation in the study.
2.1.2. Exclusion Criteria
Abnormal body temperature measured axillary for 5 min /normal for the newborn: 36.1-37.5 Cº/ [2].
Respiratory failure- rhythmic breathing disorders, apnea > 20 sec.; with cardiocirculatory disorders – bradycardia, tachycardia, rhythm changes, episodes of oxygen desaturation, heart failure; early jaundice until the 24th hour; hepatosplenomegaly – liver size >1.5-2 cm. and spleen > 0.5 cm, palpated below the edge of the costal arch, omphalitis, impaired enteral tolerance – refusal of food, vomiting, residual stomach contents (over 5 ml), unstable defecation; haemorrhagic syndrome – hematemesis, rectal bleeding, melena, bleeding from the navel and puncture sites; skin changes – pustular rash, petechiae; fever; capillary refill time > 3s.
Deviations from the reference ranges of paraclinical parameters [2].
Seizures or seizure equivalents.
Skin changes - allergic rash, intertrigo.
Microbiological isolates from ear discharge and stomach aspirate, examined up to the 6th hour after birth.
Crying and increased motor activity of the newborn before starting the procedure.
Technical problems while shooting a video clip.
Difference (over 2 points) in the pain score between surveyors assessing the pain.
2.2. Statistical Methods
Results are presented as the mean value, standard deviation, and standard error for continuous variables while for categorical variables as the whole numbers (N). An Analysis of Variance (ANOVA) test was used to determine whether there was a statistically significant difference between the means of three independent groups. To find out exactly which groups differed from each other, a post hoc test (also known as a multiple comparison test) was also conducted, which allowed us to examine the difference between means. Data were statistically analyzed using IBM SPSS software, version 27. Statistical significance was set at p < 0.05.
This work was carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving human subjects.The study was approved by the Scientific Ethics Committee of Medical University-Plovdiv – No Р-7326/ 5.10.2016 year.
3. Results
Before and the 30th seconds after the procedure pain, there were no statistically significant differences between the groups, assessed with both scales (Table 1).
In NIPS at the 5th minute, we found significant differences in the following components of the scale: facial expression (p=0.001); cry-(p=0.013); breathing patterns -(p=0.001); arms -(p=0.000); legs - (p=0.006) and overall assessment (p=0,000) (Table 2).
When applying Post Hoc Tests a significant difference was registered between groups B and C in breathing patterns (p=0.0001); arms(p=0.016); and overall assesment (p=0.037)(Table 3).

Table 3.
Post Hoc Tests.
| NIPS -5th min | Groups | Groups | Mean Difference | Sig. |
| Breathing patterns | Arnica D30 Sol. Glucose 25% |
Sol.Glucose 25% Arnica D30 |
-,334* ,334* |
0,0001 0,0001 |
| Arms | Arnica D30 Sol. Glucose 25% |
Sol.Glucose 25% Arnica D30 |
-,239* ,239* |
0,016 0,016 |
| Overall Assesment |
Arnica D30 Sol. Glucose 25% |
Sol.Glucose 25% Arnica D30 |
-1,181* 1,181* |
0,037 0,037 |
* The mean difference is significant at the 0.05 level.
Table 4.
Evaluation of observed NFCS scale at 5 minutes depending on analgesia method.
| NFCS-5th min. | Groups | N | Mean | Std.Deviation | F | Sig. level |
| Brow bulge | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
,41 ,32 ,34 |
,492 ,469 ,490 |
0,571 | 0,566 |
| Eye squeeze | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
,54 ,30 ,52 |
,502 ,481 ,490 |
4,306 | 0,015* |
| Nasolabial furrow | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
,48 ,30 ,36 |
,503 ,462 ,496 |
2,367 | 0,097 |
| Open mouth | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
,87 ,70 ,75 |
,336 ,453 ,304 |
4,095 | 0,018* |
| Taut tongue | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
,29 ,16 ,23 |
,456 ,368 ,452 |
1,608 | 0,204 |
| Chin quiver | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
,29 ,11 ,22 |
,456 ,310 ,439 |
3,704 | 0,027* |
| Tongue sticking out | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
,20 ,15 ,17 |
,404 ,368 ,423 |
,360 | 0,698 |
| Stretch mouth | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
,54 ,32 ,37 |
,503 ,471 ,506 |
3,183 | 0,045 |
| Overall Assesment |
without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
3,85 2,35 2,95 |
2,502 2,443 2,469 |
5,273 | 0,006* |
In NFCS at the 5th minutes after heel prick, we reported significant differences in the following indicators of the scale: eye squeeze (p=0,015); open mouth (p=0,018); chin quiver (p=0,027) and overall assessment (p=0,006) (Table 4).
When applying Post Hoc Tests, a significant difference was registered between groups B and C at eye squeeze(p=0,021), open mouth(p=0,049) and overall assessment (p=0,041) (Table 5).
We tracked the dynamics of physiological indicators - markers of pain. We found significantly transcutaneous oxygen saturation (p= 0,001), respiratory rate(p= 0,000) and systolic blood pressure(p= 0,009) values before the procedure (Table 6). Tracking at 30th sec and the 5th min. reported statistical significance in heart rate (p= 0,012), respiratory rate (p= 0,007) and systolic blood pressure (p= 0,000) (Table 7).
Using analysis Post Hoc Tests confirmed significant differences between groups В and С (Тable 8). We found significantly slowed respiratory rate before the procedure and higher heartbeat- at the 30th sec.in those anesthetised with glucose solution. We also reported higher systolic blood pressure (regardless of the reference limits for this age) in neonates had received Sol.Glucose 25% before the procedure and at the 5th min after the procedural pain (Table 8).
4. Discussion
Procedural pain occurs when the integrity of the skin or tissue is damaged by diagnostic or therapeutic manipulations [3]. Most common in the neonatal period are venipuncture, muscle injections, endotracheal intubation, eye examination, lumbar puncture, blood collection from the heel and others. Prevention and treatment of pain in neonates is important because exposure to repeated painful stimuli early in life has immediate short-term and long-term adverse effects, including irritability, disturbed sleep-wake state, ventilation-perfusion mismatch, increased oxygen consumption and impaired nutritional intake [4,5].
Numerous studies have documented neonatal responses to pain, which include autonomic (eg, increases in heart rate, blood pressure), hormonal (eg, cortisol and catecholamine responses), and behavioral changes (eg, facial grimace). These responses form the basis of the many pain assessment tools used to evaluate acute pain in the neonate. Physiologic parameters include changes in heart rate, respiratory rate, blood pressure, vagal tone, heart rate variability, breathing pattern, oxygen saturation, intracranial pressure, palmar sweating, skin color, or pupillary size. Behavioral responses include crying patterns, acoustic features of infant crying, facial expressions, hand and body movements, muscle tone, sleep patterns, behavioral state changes, and consolability [6].
According to the international consensus for the assessment of neonatal pain, two of the most frequently applied scales in term and preterm newborns are: Neonatal Infant Pain Scale (NIPS) and Neonatal Facial Coding System (NFCS). The multimodal NIPS is used to assess pain in preterm and term neonates [7]. It includes one physiological /breathing patterns / and five behavioural reactions: facial expression; cry; arms; legs; and state of arousal [7,8]. Items are rated 0 or 1. Only the crying factor is rated 0,1 or 2. The sum of the items is referred to as an evaluation score and gives a quantitative assessment of the presence and severity of pain. The inventors of the scale and other authors accept the presence of pain at a score ≥ 4 [9,10]. Independently, the minimum score is 0 points, and the maximum is 7 points.
The unimodal NFCS was created in 1987 by Grunau et al. and has later undergone various modifications [11]. Mimic changes for pain assessment in full-term and premature newborns in the original scale are as follows: 1. Brow bulge; 2. Eyes squeeze; 3. Nasolabial furrow; 4. Open lips; 5.Taut tongue; 6.Tongue sticking out; 7.Chin quiver; 8. Stretched mouth: 8.1 Horizontal mouth, 8.2 Vertical mouth, 8.3 Oo-shaped mouth.11 The evaluation is rated 0 or 1 according to the presence or absence of the corresponding indicator. When using the NFCS an optimal score of 8 is accepted, and pain is reported at ≥ 3 [12,13].
Based on literature data, we accepted the following: absent pain when score is less than 4 ac-cording to NIPS or less than 3 according to NFCS; pain when NIPS score was ≥ 4; NFCS score was ≥3, and very severe pain - when score is above 6 in NIPS and above 7 in NFCS , with a maximum score 7 in the NIPS, and 8 in the NFCS [8,13,14,15].
Over the past two decades, analgesia with sweet solution has been extensively studied in neonates undergoing painful procedures. Sweet taste is thought to trigger the release of endogenous opioids. The analgesic effectiveness of the solution may depend on its degree of sweetness, arranged in the following order according to the degree of manifestation: sucrose, fructose, glucose and lactose [16]. Many studies have shown that oral sucrose is safe and effective in reducing nociception in single and short-term procedures, and as a result it has been proposed as the standard of treatment on procedural pain [17]. Analgesic effect of sweet solution is controversial when applied to several consecutive painful procedures [18]. It has been suggested that the greatest analgesic effect is achieved when the sweet solution is given approximately two minutes before the start of the painful procedure. According to one hypothesis, this interval coincides with the endogenous release of opioids, but the mechanism of its analgesic action is still incompletely understood and partly controversial [19].
Recent systematic reviews have shown that sweet taste is effective in reducing behavioral indicators of pain in infants up to 1 year of age during common minor procedures such as venipuncture, bladder catheterization, circumcision, subcutaneous, intramuscular injections, ophthalmoscopy, placement of nasogastric tube, and heel prick tests [20,21]. As the most common painful procedure, heel prick tests were investigated in 38 studies [21]. In some of them, with glucose intake, different scales were used to evaluate the behavioral markers-NIPS [22,23], PIPP[23,24], DAN[25], NFCS [26,27] and was also reported the dynamics on the physiological indicators of pain [27,28,29]. Most of the studies prove the analgesic effect of sweet solutions, but some of them do not register it for procedural pain [21,23,30]. Akcam M.[31] reported no difference in control of procedural pain between glucose and fructose, and data comparing the analgesic effects of sucrose and glucose were variable [21]. Guala A et al.[29] and Isik U et al. [32] found during heel prick tests no significant difference between the two carbohydrates in changes to heart rate, but the second cohort recorded a shorter crying time with sucrose compared to glucose. Suhrabi et al. [33] register no difference in NIPS score at 1st and 2nd min after immunization, which was also confirmed by Kumari S.[34] in a double-blind randomized controlled trial, where 25% glucose and 24% sucrose were comparable as analgesia for pain relief during heel prick. Therefore 25% glucose solution can be used as an alternative to sucrose to reduce procedural pain in healthy term and preterm neonates. There is evidence that sucrose and glucose (20% to 50%) significantly reduce NIPS values in the heel prick [21,22,34,35].
Comparing the glucose group with the NIPS control group in the present study found that the anesthetised patients had a significantly lower score compared to the 5th min control group (p=0.000). That is a reduction in pain intensity and duration after administration of 25% glucose solution, which confirms the analgesic effect of glucose in procedural pain caused by a heel prick test. A lower NIPS score was recorded with the administration of 25% glucose solution, both after venipuncture [36] and with intramuscular injections [33].
According to the literature data, facial manifestations of procedural pain were detected in 99% of newborns within 6 seconds after a heel prick test, and are thought to be very sensitive indicators of infant pain [37]. Using the NFCS pain rating scale, Ogawa et al. [26] and Okan F et al.[27] found a significantly lower pain severity when applying sweet solutions after procedural pain, such as a heel prick test. Gaspardo et al. [38] assessed newborns' facial activity by NFCS, using the behavioral marker of cry, and the physiological marker of heart rate, after administration of sweet solutions in venipuncture, and also proved their analgesic effect. According to our results, the overall NFCS score there are a tendency towards a lower score at the 5th minute, below 3 (2.95), which is minimal for pain (p=0,006).
In their study, Asmerom et al. [39] reported that a single dose of sucrose reduced behavioral indicators of pain by heel prick tests in preterm infants, but increased the physiological markers of oxidative stress and heart rate. These results coincide with ours: the application of Sol. Glucose 25% recorded the highest values of heart rate at the 30th second, as well as lower oxygen saturation and slower breathing even before the procedural pain. These statistically significant pre-screening differences in respiratory rate, oxygen saturation, and systolic and diastolic blood pressure, are assumed to be the result of the action of the applied oral intake of Sol.Glucose 25% associated with intracellular oxidative stress as well as sympathetic activation [16]. Published studies also found increases in heart rate, decreases in oxygen saturation, and lower respiratory rates, but without statistically significant results [40,41].
In the present study, at the 30th second the higher heart rate in the anesthetised newborns is striking (p=0.012), which is probably related to the described supposed influence of the sweet solution [21]. At the 5th minute after the procedure, we report significant differences in the values of the indicators: respiratory rate lower (p=0.007) and systolic pressure higher (p=0.000), which we associate with the continued effect of the glucose solution. Our results match with those of Liaw JJ et al. [42], where after application of Hbvax under anesthesia with glucose solution were reported a higher value of heart rate and a decrease in respiratory rate, as well as their significant stabilization. Jatana SK et al. [28] also reported a significant increase in heart rate, and a decrease in crying time and oxygen saturation under glucose analgesia following blood collection from the heel.
In the interval 12-24 hours we found no deviations from the norm for the age of the monitored physiological indicators - heart rate, respiratory rate, transcutaneous saturation and arterial pressure after analgesia with Sol.Glucosae 25% .
Homeopathic agents can be used for certain conditions in the neonatologist's clinical practice [43,44,45]. The use of homeopathic agents with Arnica in newborns after traumatic births or other injuries (venipuncture) is appropriate because it improves the physical and mental recovery of the body. In connection with these effects, the intake of Arnica as well as Staphysagria and Calendula is recommended to boys post circumcision [46].The use of Arnica before and after surgery to reduce hematoma, swelling, tenderness, and pain has been documented. The effect is associated with variations in efficacy (potency) and frequency of dosing. A potency of 30C is recommended [44]. The use of Arnica Montana as a homeopathic product is based on its composition and effects - content of lactones (analgesic, anti-inflammatory, antiecchymotic effect), phenols (antibacterial action), flavanoids (venous tropism). The anti-inflammatory, anti-microbial, antioxidant, and immunomodulatory activities of the chemical compounds in Arnica have been investigated in different models [47]. It is preferred as a non-pharmacological alternative, due to the proven effect in clinical neonatological and pediatric practice in the treatment of trauma with hematomas, fractures, cephalhematomas and other conditions accompanied by varying degrees of pain [44,45]. It is especially preferred in the healing of wounds of different origins [46]. Additionally, Arnica administered orally in homeopathic dilutions has shown positive clinical effects in reducing postoperative pain, edema, and ecchymosis. Topical application of Arnica combined with oral homeopathic dilutions has been found to have a synergistic effect in reducing postoperative pain[ 48]. In vitro studies show that the most active components of Arnica, as well as other preparations from the Asteraceae family, are helenalin and the secuterpene lactones - 11a,13-dihydrohelenalin and hamisonolide [48]. First Lyss et al. found that helenalin inhibits the transcription nuclear factor,factor kappa B (NF-kB) by altering and stabilizing the NF-kB/inhibitor of kappa B (I kappa B) complex in T cells, B cells and epithelial cells and abolishes kappa gene expression. This is one of the earliest pieces of evidence of Arnica's anti-inflammatory properties. A later study showed that helenalin could inhibit human neutrophil migration, chemotaxis, 5-lipoxygenase activity, and leukotriene C4 synthetase. It leads to reduced expression of the cell surface receptors CD25, CD28, CD27 and CD120b, which play a key role in the activation of NF-kB in T cells. This supports the mechanism proposed by Lyss in 1997[48-49]. NF-kB activation is associated with the induction of pain and inflammation, characterized by the release of proinflammatory cytokines (tumor necrosis factor-alpha [TNF-a] and interleukin-1beta [IL-1b] and local leukocyte recruitment [50].
Comparing the non-anesthetised newborns with those who received Arnica D30 showed a lower rating on both pain scales for the anesthetised before and at 5 minutes after the procedure. The effect was most pronounced in those who received Arnica at the 5th minute - a score was achieved showing the absence of pain in this group, which means that the pain sensation is the shortest. When monitoring changes in heart rate during the observed intervals, no significant difference was found. The present study found that transcutaneous oxygen saturation after administration of Arnica D30 was higher and systolic pressure was lower at the 5th minute compared to non-anesthetised and those, who received Sol.Glucosae 25% . It is noteworthy that when taking Arnica D30, the smallest dynamics are recorded in the respiratory and heart rate values before and at the 5th minute after the heel prick. This once again confirms the anesthetic effect (reducing the duration and severity of pain) of the preparation Arnica D30.
In the interval 12-24h. we did not find deviations from the norm for the age of the monitored physiological indicators - heart rate, respiratory rate, oxygen saturation and arterial pressure after anesthesia with Arnica D30.
In our available literature, no data were found on the use of Arnica D30 in the neonatal period and childhood for the treatment of procedural pain, which did not allow us to compare our results with similar studies. To confirm the effect of Arnica Montana, future studies are needed in three areas: inflammatory processes, pain management, and postoperative conditions, necessitating new meta-analyses in a large number of patients [48]. This will help to validate complementary medicine as part of the therapeutic approach in a wide range of areas.
5. Conclusions
1.Arnica D30 has better analgesic effect compared to Sol.Glucose 25% in procedural pain induced by heel prick tests in term neonates.
2. Unlike Sol.Glucose 25%, Arnica D30 does not affect changes in physiological parameters: respiratе rate, oxygen saturation and sistolic blood pressure before procedural pain and more quickly leads to their normalization after it.
Author Contributions
Conceptualization: P.P, M.K and I.P.; methodology: P.P, M.K., M.R. and I.P. .; software, P.P, M.R., S.D.; validation: P.P, M.R, I.P.; formal analysis, P.P, M.R. I.P.; investigation, P.P, M.K.; resources: P.P, M.K, S.D.; data curation: P.P, M.K..; writing—original draft preparation, P.P, I.P; writing—review and editing: P.P, M.K, I.P., M.R.,S.D.; visualization, P.P, M.R., S.D.; supervision, M.K., I.P.; project administration: P.P., M.K..; All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Scientific Ethics Committee of Medical University-Plovdiv (protocol code No Р-7326/ 05.10.2016) for studies involving humans. .
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Shen, M.; El Chaar, G. Reducing pain from heel lances in neonates following education on oral sucrose. Int Clin Pharm 2015, 37,529-536. [CrossRef]
- Rennie, J.M.; & Kendall, G.A. Manual of Neonatal Intensive Care (5th ed.). CRC Press 2013; London; pp382-383.
- Anand, K.J.S. Assessment of neonatal pain.UpToDate 2018.
- American Academy of Pediatrics Committee on Fetus and Newborn; American Academy of Pediatrics Section on Аnesthesiology and Pain medicine. Prevention and Management of Procedural Pain in the Neonate: An Update; Pediatrics. January 2016.
- Hall, R.W.; Anand, K.J.S. Pain Management in Newborns. Clin Perinatol. 2014; 41(4); 895–924. [CrossRef]
- Roué, Jean-Michel. Assessment of neonatal pain. UpToDate 2023.
- Lawrence, J.; Alcock, D.; Mc Grath, P.; Kay, J.; Mac Murray,S.B.; Dulberg, C. The Development of a Tool to Assess Neonatal Pain. Neonatal Network 1993; 12;59-66.
- da Paixão Freitas, Z.M.; Pereira C.U.; da Paixão Oliveira D.M. Pain Scale: When the Training Influences Its Use. Open Journal of Nursing 2018; 8:130-138. [CrossRef]
- Bernardo, G.; Riccitelli, M.; Sordino, D.; Giordano, M.; Piccolo, S.; Buonocore, G.; Perrone, S. Oral 24% sucrose associated with non-nutritive sucking for pain control in healthy term newborns receiving venepuncture beyond the first week of life. Journal of Pain Research. 2019;12: 299-305.
- de Cassia Pinheiro da Motta, G., Machado Schardosim, J.; Chollopetz da Cunha M.L. Neonatal Infant Pain Scale: Cross-Cultural Adaptation and Validation in Brazil. Journal of Pain and Symptom Management 2015;50(3): 394-401. [CrossRef]
- Grunau, R.V.E.; Craig, K.D. Pain expression in neonates: facial action and cry. Pain. 1987; 28:395–410. [CrossRef]
- Grunau R.V.E.; Craig K.D. Facial activity as a measure of neonatal pain expression. Advances in Pain Research and Therapy. Raven Press. 1990; 15:147-155.
- Hardeep, K.; Gaurav M. A Comprehensive analysis of Neonatal pain and measures to reduce pain. Journal of Pediatric Critical Care.2019; 6;1: 43-48.
- Roué, J.M.; Rioualen, S.; Gendras, J.; Misery, L.; Gouillou, M.; Sizun, J. Multi-modal painassessment: are near-infrared spectroscopy, skin conductance, salivary cortisol, physiologic parameters, and neonatal Facial coding system interrelated during venepuncture in healthy, term neonates? Journal of Pain Research 2018;11:2257-2267. [CrossRef]
- Sposito, N.P.B.; Rossato, L.M.; Bueno, M.; Kimura, A.F.; Costa, T.; Guedes, D.M.B. Assessment and management of pain in newborns hospitalized in a Neonatal Intensive Care Unit: a cross-sectional study. Rev Lat Am Enfermagem. 2017; 12;25: e2931. [CrossRef]
- Bueno, M.; Yamada, J.; Harrison, D.; Khan, S.; Ohlsson, A.; Adams-Webber, T. et al. Systematic review and meta-analysis of non-sweetened solutions to relieve pain in neonates. Pain Res Manag.2013;18 (3): 153-161.
- Liu, Y.; Huang, X.; Luo, B.; Peng W. Effects of combined oral sucrose and nonnutritive sucking (NNS) on procedural pain of NICU newborns, 2001 to 2016: A PRISMA-compliant systematic review and meta-analysis. Medicine (Baltimore). 2017;96(6):e6108. [CrossRef]
- Bhalla, T.; Shepherd, E.; Tobias, J. Neonatal pain management. Saudi J Anaesth. 2014; 8(Suppl 1): S89–S97.
- Messerer, B.; Krauss-Stoisser, B.; Urlesberger, B. Nichtmedikamentöse Maßnahmen sowie topische Analgetika und orale Zuckerstoffe im Schmerzmanagement. Der Schmerz 2014; 28: 31–42. [CrossRef]
- Yamada, J.; Bueno, M.; Santos, L.; Haliburton, S.; Campbell-Yeo, M,; Stevens, B. Sucrose analgesia for heel-lance procedures in neonates. Cochrane Database Syst Rev. 2023; 30;8(8):CD014806. [CrossRef]
- Stevens, B.; Yamada, J.; Ohlsson, A.; Haliburton, S.; Shorkey, A. Sucrose for analgesia in newborn infants undergoing painful procedures. Cochrane Database Syst Rev. 2016;16;7:CD001069.
- Ahn, H.Y.; Jang, M.Y.; Hur, M.H. The effect of oral glucose on pain relief in newborns. Taehan Kanho Hakhoe Chi. 2006;36:992–1001. [CrossRef]
- Bonetto, G.; Salvatico, E.; Varela, N.; Cometto, C.; Gomez, P.F.; Calvo, B. Pain prevention in term neonates: Randomized trial for three methods. Arch Argent Pediatr.2008; 106:392–6. [CrossRef]
- Brovedani, P.; Montico, M.; Shardlow, A.; et al. Suckling and sugar for pain reduction in babies. Lancet 2007; 369:1429. [CrossRef]
- Bellieni, C.V.; Bagnoli, F.; Perrone, S.; Nenci, A.; Cordelli, D.M.; Fusi, M.; Ceccarelli, S.; Buonocore, G. Effect of multisensory stimulation on analgesia in term neonates: a randomized controlled trial.Pediatr Res. 2002;51(4):460-3. [CrossRef]
- Ogawa, S.; Ogihara, T.; Fujiwara, E.; Ito, K.; Nakano, M.; Nakayama, S.; Hachiya, T.; Fujimoto, N.; Abe, H.; Ban, S.; Ikeda, E.; Tamai, H. Venepuncture is preferable to heel lance for blood sampling in term neonates. Arch Dis Child Fetal Neonatal Ed. 2005; 90(5): F432-6. [CrossRef]
- Okan, F.; Coban, A.; Ince, Z.; Yapici, Z.; Can, G. Analgesia in preterm newborns: The comparative effects of sucrose and glucose. Eur J Pediatr. 2007; 166:1017–24. [CrossRef]
- Jatana, S.K.; Dalal, S.S.; Wilson, C.G. Analgesic Effect of Oral Glucose in Neonates Med J Armed Forces India. 2003; 59(2); 100–104.
- Guala, A.; Pastore, G.; Liverani, M.E. et al. Glucose or sucrose as an analgesic for newborns: A randomised controlled blind trial. Minerva Pediatr. 2001;53:271–4.
- Slater, R. et al. Oral sucrose as an analgesic drug for procedural pain in newborn infants: a randomised controlled trial. 2010; Lancet 376(9748):1225–1232. [CrossRef]
- Akcam, M. Oral fructose solution as an analgesic in the newborn: A randomized, placebo-controlled and masked study. Pediatr Int 2004;46:459–462. [CrossRef]
- Isik, U.; Ozek, E.; Bilgen, H.; Cebeci, D. Comparison of oral glucose and sucrose solutions on pain response in neonates. Journal of Pain 2000;1:275-8. [CrossRef]
- Suhrabi, Z.; Taghinejad, H.; Valian, K.; Sayehmiri, K.; Taheri. S. A comparative study on the efficacy of glucose and sucrose on the vaccination pain: a randomized controlled clinical trial. Journal of Clinical and Diagnostic Research 2014; 8(10): PC01-03.
- Kumari, S.; Datta, V.; Rehan, H. Comparison of the efficacy of oral 25% glucose with oral 24% sucrose for pain relief during heel lance in preterm neonates: a double blind rando-mized controlled trial. J Trop Pediatr 2016. 63(1):30–35.
- Tutag Lehr, V.; Cortez, J.; Grever, W.; Cepeda, E.; Thomas, R.; Aranda, J.V. Randomized placebo controlled trial of sucrose analgesia on neonatal skin blood flow and pain response during heel lance. The Clinical Journal of Pain 2015;31(5):451-8. [CrossRef]
- Liu, M.F.; Lin, K.C.; Chou, Y.H.; Lee, T.Y. Using non-nutritive sucking and oral glucose solution with neonates to relieve pain: a randomised controlled trial. J Clin Nurs. 2010;19(11-12):1604-11. [CrossRef]
- Gray, L.; Garza, E.; Zageris, D. et al. Sucrose and warmth for analgesia in healthy newborns: an RCT. Pediatrics 2015;135: e607. [CrossRef]
- Gaspardo, C.M.; Miyase, C.I.; Chimello, J.T.; Martinez, F.E.; Martins Linhares, M.B. Is pain relief equally efficacious and free of side effects with repeated doses of oral sucrose in preterm neonates? Pain 2008; 137:16-25. [CrossRef]
- Asmerom, Y.; Slater, L.; Boskovic, D.S.; Bahjri, K.; Holden, M.S.; Phillips, R. et al. Oral sucrose for heel lance increases adenosine triphosphate use and oxidative stress in preterm neonates. The Journal of Pediatrics 2013;163(1):29-35.e1. [CrossRef]
- Milazzo, W.; Fielder, J.; Bittel, A.; Coil, J.; McClure, M.; Tobin, P. et al. Oral sucrose to decrease pain associated with arterial puncture in infants 30 to 36 weeks’ gestation. A randomized clinical trial. Advances in Neonatal Care 2011;11(6):406-11. [CrossRef]
- Montoya, I.G.; Gázquez, M.A.R.; Cadavid, L.A.M.; Jaramillo, A.Q. The use of sucrose for the prevention of pain during venipuncture in neonates. Enfermería Clínica 2009;19:267-74.
- Liaw, J.J.; Zeng, W.P.; Yang, L.; Yuh, Y.S.; Yin, T.; Yang, M.H. Nonnutritive sucking and oral sucrose relieve neonatal pain during intramuscular injection of hepatitis vaccine. J Pain Symptom Manage 2011;42(6):918-30. [CrossRef]
- Burke, L. Homeopathy for Pain Management. Alternative and complementary therapies. 2017; 23:176-183.
- Martin, P. Аrnica and Aconite - homeopathic newborn care -Midwifery Today- Summer 2009:30-66.
- Burgari, R. Homeopathic treatment of newborn and infant children. (1st ed.). Similia;Russia; 2002:17-40.
- Castro, F.C.; Magre, A.; Cherpinski, R.; Zelante, P.M.; Neves; L.M.; Esquisatto, M.A. et al. Effects of microcurrent application alone or in combination with topical Hypericum perforatum L. and Arnica montana L. on surgically induced wound healing in Wistar rats. Homeopathy 2012;101(3):147-53. [CrossRef]
- Smith, A.G.; Miles, V.N.; Holmes, D.T.; Chen, X.; Lei, W. Clinical Trials, Potential Mechanisms, and Adverse Effects of Arnica as an Adjunct Medication for Pain Management. Medicines (Basel). 2021; 9;8(10):58. [CrossRef]
- Iannitti, T.; Morales-Medina, J.C.; Bellavite, P.; Rottigni, V.; Palmieri, B. Effectiveness and Safety of Arnica montana in Post-Surgical Setting, Pain and Inflammation. Am J Ther. 2016;23(1):e184-97. [CrossRef]
- Olioso, D.; Marzotto, M.; Bonafini, C.; Brizzi, M.; Bellavite, P. Arnica montana effects on gene expression in a human macrophage cell line. Evaluation by quantitative Real-Time PCR. Homeopathy 2016;105 (2): 131-47. [CrossRef]
- Kawakami, A.P.; Sato, C.; Cardoso, T.N.; Bonamin, L.V. Inflammatory Process Modulation by Homeopathic Arnica montana 6CH: The Role of Individual Variation. Evid Based Complement Alternat Med. 2011; 2011:917541. [CrossRef]
Figure 1.
Study design.
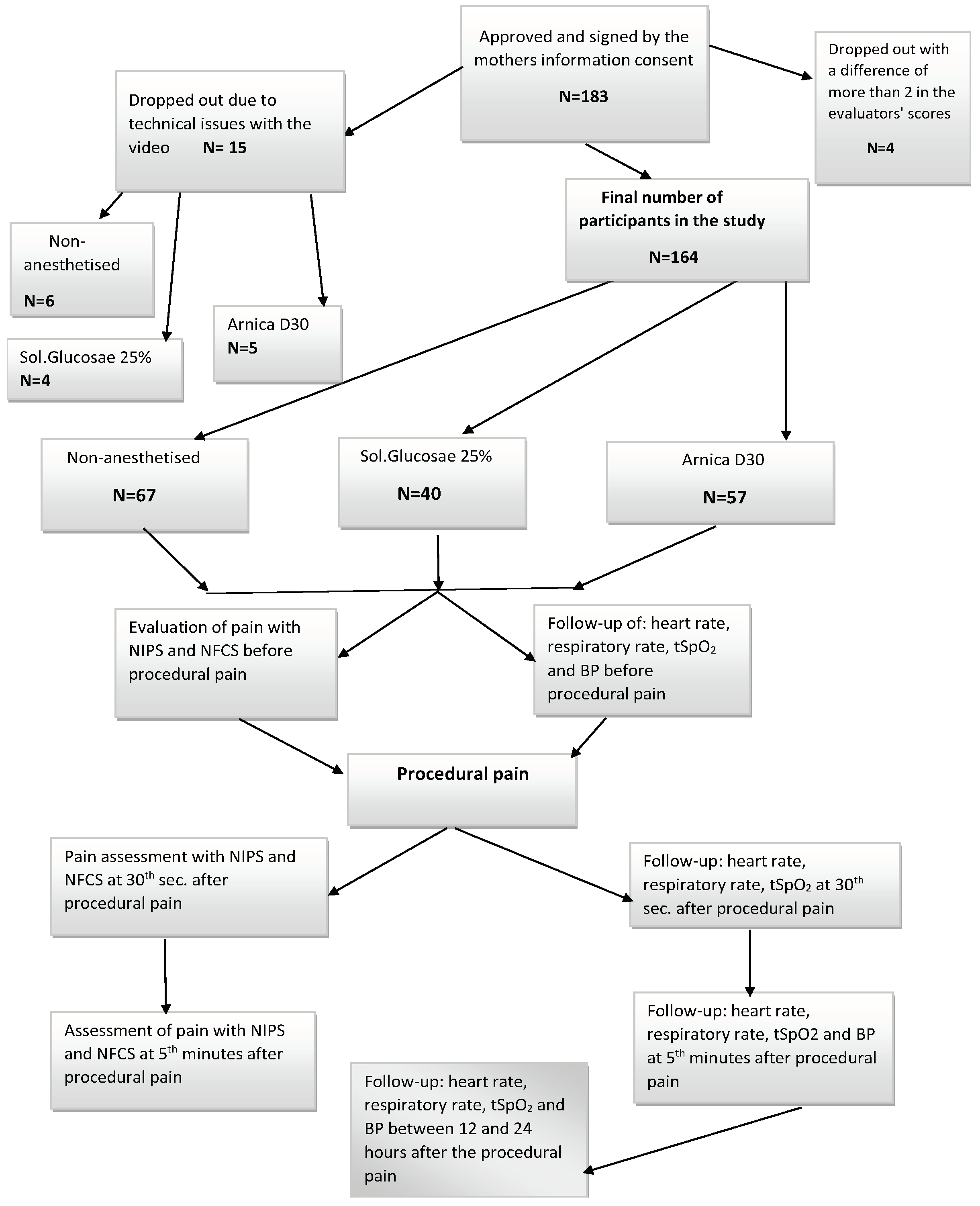
Table 1.
General assessment on the pain scales before and and the 30th sec. after the procedure. At the 5th minute, on both scales, a lower score was reported in the newborns with Arnica D30 compared to those who received Sol.Glucose 25%. In both groups, the overall score corresponds to no pain. Statistically significant differences in total evaluations of NIPS and NFCS were registered (Table 2 and Table 4). .
Table 1.
General assessment on the pain scales before and and the 30th sec. after the procedure. At the 5th minute, on both scales, a lower score was reported in the newborns with Arnica D30 compared to those who received Sol.Glucose 25%. In both groups, the overall score corresponds to no pain. Statistically significant differences in total evaluations of NIPS and NFCS were registered (Table 2 and Table 4). .
| Рain rating scales | Groups | before the procedure | SD | F | Sig. level | at the 30th sec. | SD | F | Sig. level |
|---|---|---|---|---|---|---|---|---|---|
| NIPS – Overall Assesment |
Without anesthesia -/А/ | 1,79±0,18 | 1,46 | 1,227 | 0,296 | 6,73±0,11 | 0,898 | 1,702 | 0,186 |
| Arnica D30-/В/ | 1,35±0,22 | 1,65 | 6,89±0,09 | 0,673 | |||||
| Sol.Glucosae 25%- /С/ | 1,50±0,28 | 1,70 | 6,98±0,03 | 0,158 | |||||
| NFCS – Overall Assesment |
Without anesthesia -/А/ | 1,24±0,15 | 1,24 | 0,408 | 0,666 | 6,85±0,09 | 0,751 | 2,499 | 0,085 |
| Arnica D30–/В/ | 1,04±0,18 | 1,04 | 6,28±0,10 | 0,959 | |||||
| Sol.Glucosae 25%-/С/ | 1,24±0,20 | 1,24 | 6,88±0,05 | 0,335 |
Table 2.
Evaluation of observed NIPS scale at 5 minutes after depending on analgesia method.
| NIPS -5th min | Groups | N | Mean | Std.Deviation | F | Sig. level |
|---|---|---|---|---|---|---|
| Face expression | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
,74 ,40 ,60 |
,441 ,495 ,496 |
7,834 | 0,001** |
| Cry | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
,91 ,47 ,68 |
,830 ,758 ,859 |
4,471 | 0,013* |
| Breathing patterns | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
,75 ,49 ,83 |
,438 ,504 ,385 |
7,789 | 0,001** |
| Arms | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
,88 ,56 ,80 |
,327 ,501 ,405 |
9,580 | 0,000*** |
| Legs | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
,85 ,60 ,70 |
,359 ,495 ,464 |
5,324 | 0,006** |
| State of arousal | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
,35 ,21 ,28 |
,480 ,411 ,452 |
1,443 | 0,239 |
| OverallAssesment | without analgesia Arnica D30 Sol. Glucose 25% |
67 57 40 |
4,46 3,00 3,28 |
2,127 2,699 2,552 |
8,989 | 0,000*** |
*p<0.05; **p<0.01; ***p<0.001 (ANOVA).
Table 5.
Post Hoc Test.
| Groups | Groups | Mean Difference | Sig. |
| Arnica D30 | Sol.Glucose 25% | -,274* | 0,021 |
| Sol. Glucose 25% | Arnica D30 | ,274* | 0,021 |
| Arnica D30 | Sol.Glucose 25% | -,181* | 0,049 |
| Sol. Glucose 25% | Arnica D30 | ,181* | 0,049 |
| Arnica D30 | Sol.Glucose 25% | -1,234* | 0,041 |
| Sol. Glucose 25% | Arnica D30 | 1,234* | 0,041 |
* The mean difference is significant at the 0.05 level. .
Table 6.
Dynamics of physiological indicators in the groups before the procedure.
| Indicators | Groups | before the procedure | Std. | Sig. level | |
| Deviation | F | ||||
| Heartbeat | not anesthetised/А/ | 136,85±2,74 | 22,456 | 0,377 | 0,687 |
| ArnicaD30/В/ | 141.00±2,77 | 18,664 | |||
| Sol.Glucose 25%/С/ | 139,50±3,36 | 21,281 | |||
| Oxygen saturation | not anesthetised | 97,04±0,57 | 4,637 | 7,275 | ,001** |
| Arnica D30 | 97,33±0,56 | 2,754 | |||
| Sol.Glucose 25% | 94,58±0,81 | 5,103 | |||
| Breathing frequency | not anesthetized | 43,29±1,16 | 9,444 | 18,285 | ,000*** |
| Arnica D30 | 42,45±1,38 | 10,21 | |||
| Sol.Glucose 25% | 30,15±2,51 | 15,858 | |||
| Systolic blood pressure | not anesthetised | 79,46±2,12 | 15,853 | 4,91 | ,009** |
| Arnica D30 | 81,44±1,95 | 13,802 | |||
| Sol.Glucose 25% | 90,03±3,17 | 18,218 | |||
| Diastolic blood pressure | not anesthetised | 46,20±1,48 | 11,082 | 2,483 | 0,087 |
| Arnica D30 | 47,80±1,70 | 12,151 | |||
| Sol.Glucose25% | 52,27±2,65 | 15,195 |
Table 7.
Dynamics of physiological indicators in the groups at the 30thsec. and on the 5th min after the procedure.
Table 7.
Dynamics of physiological indicators in the groups at the 30thsec. and on the 5th min after the procedure.
| Indicators | Groups | Std. | F | Sig. Level | Std. | Sig. level | |||
| at the 30th sec. | Deviation | on the 5th min. | Deviation | F | |||||
| Heartbeat | not anesthetised/А/ | 158,07±3,49 | 28,557 | 4,569 | ,012* | 143,99±3,67 | 30,017 | 1,358 | 0,26 |
| ArnicaD30 /В/ | 162,37±3,21 | 27,369 | 141,35±3,57 | 23,579 | |||||
| Sol.Glucose 25%/С/ | 170,70±4,01 | 25,341 | 137,18±4,89 | 30,937 | |||||
| Oxygen saturation | not anesthetised | 88,13±1,09 | 8,881 | 1,777 | 0,173 | 94,12±1,08 | 8,845 | 2,675 | 0,072 |
| Arnica D30 | 89,93±0,81 | 5,812 | 97,00±0,50 | 4,767 | |||||
| Sol.Glucose 25% | 86,08±1,75 | 10,781 | 93,08±1,09 | 6,776 | |||||
| Breathing frequency | not anesthetized | 30,47±1,19 | 9,67 | 0,256 | 0,774 | 45,34±1,68 | 13,749 | 5,143 | ,007** |
| Arnica D30 | 29,61±2,09 | 15,391 | 40,13±1,81 | 13,433 | |||||
| Sol.Glucose 25% | 31,54±2,17 | 13,553 | 35,03±3,58 | 22,668 | |||||
| Systolic blood pressure | not anesthetised | - | - | 93,16±1,98 | 14,68 | 8,503 | ,000*** | ||
| Arnica D30 | - | - | 86,35±2,38 | 17,013 | |||||
| Sol.Glucose 25% | 101,10±2,64 | 14,211 | |||||||
| Diastolic blood pressure | not anesthetised | - | - | 53,45±1,89 | 14,004 | 0,941 | 0,393 | ||
| ArnicaD30 | - | - | 53,75±1,88 | 13,409 | |||||
| Sol.Glucose 25% | 57,62±2,82 | 15,197 |
Table 8.
Post Hoc Tests.
| Physiological markers | Groups | Groups | Mean Difference | Sig. |
| Respiratory rate - before the procedure | Arnica D30/В/ | Sol.Glucose 25% | 12,305* | 0,00 |
| Sol. Glucose 25%/С/ | Arnica D30 | -12,305* | 0,00 | |
| Systolic blood pressure- before the procedure | Arnica D30 | Sol.Glucose 25% | -8,590* | 0,043 |
| Sol. Glucose 25% | Arnica D30 | 8,590* | 0,043 | |
| Heartbeat- at the 30th sec. | Arnica D30 | Sol.Glucose 25% | -16,682* | 0,010 |
| Sol. Glucose 25% | Arnica D30 | 16,682* | 0,010 | |
| Systolic blood pressure-at the 5th min. | Arnica D30 | Sol.Glucose 25% | -14,751* | 0,00 |
| Sol. Glucose 25% | Arnica D30 | 14,751* | 0,00 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



