
Submitted:
05 February 2024
Posted:
05 February 2024
You are already at the latest version
Abstract
Cardiotoxicity is an unwanted side-effect arising from different medications. The term describes a diminution of heart function, affecting especially left ventricular ejection fraction, which can progress to heart failure. Pediatric oncology patients treated with drugs of the anthracycline group, e.g., doxorubicin, can evolve to heart failure patients in adult age. Nuclear Medicine imaging of fatty acid oxidation and glycolysis accurately describes normal and altered heart metabolism. The most common finding is a state of cardiac glycolysis, which is reflected by increased uptake of 18F-desoxyglucose (18F-FDG) at a time when fatty acid oxidation is decreased. Glycolysis has recently been recognized as being the result of coenzyme Q10 deficiency as part of adaptation to hypoxia. Low LEVF correlates with impaired fatty acid oxidation. This deficiency can arise from chemotherapy and radiation and can be corrected by supplementation. Drugs like enalapril can improve fatty acid utilization. We will review relevant Nuclear Medicine imaging studies as well as fundamental biochemical data that demonstrate this pathogenetic path.
Keywords:
Coenzyme Q10
; glycolysis
; hypoxia
; 18fluoro-desoxyglucose
; 18F-FDG
; positron emission tomography
; BMIPP
; fatty acid oxidation
; baseline diagnosis
; pediatric oncology
; post-partum cardiomyopathy.
1. Introduction to Pediatric Oncology and Cardiotoxicity
The historical aspects of clinical pediatric oncology as a medical specialty were described by Pearson in 2002 who traced its begin to medical care of hematological diseases [1]. In 1996 Daniela Cardinale working at the Cardiology Unit of the European Oncology Institute in Milano, proposed cardiooncology as a new field in medicine [2]. These contributions have led to clinical work from the standpoint of oncologists and cardiologists in relation to changes of heart function in the sense of cardiotoxicity.
Cardiotoxicity is understood as a clinical entity related to diminished heart function, which Beutner first described in 1946 in relation with the use of injectable anesthetics [3]. Many pharmaceutical substances were recognized as cardiotoxic in the following decades [4]. These drugs belong to different pharmacological groups and have been enumerated in a publication by the American Heart Association (Tables 1 and 2 in [5]). Drugs that are effective in anti-cancer treatments can affect heart function in different ways [6,7,8], leading to cardiac damage and heart failure [9]. Cardiotoxic anti-cancer drugs include anthracyclines, alkylating agents, topoisomerase inhibitors, taxanes, and others [10].
In 2022 Cardinale and coworkers described cardiotoxicity as a series of changes in the heart including cell injury, deformation, and left ventricular dysfunction (Figure 1 in [11]). In a joint publication with Tsiouris et al., they stressed the relevance of left ventricular function evaluation [12]. López-Sendón and coworkers described an incidence of cardiotoxicity of 37.5% among 865 patients included in a prospective study[13]. Cardiotoxicity has been recently evaluated in the form of a Delphi study by Gavila et al. [14]. The authors pointed out the need to identify affected patients using cardiological diagnostic criteria such as the periodic evaluation of the left ventricular ejection fraction. The authors praised their work as the first one to produce statements related to prevention, assessment, and monitoring of cardiac toxicity after chemotherapy. The publication, unfortunately, did not suggest a therapeutic procedure to achieve these goals. Belger and coworkers analyzed risk factors in relation to cardiotoxicity and concluded inconclusively that “a better understanding” would be desirable [15]. The same applies to surveillance programs based on epidemiological data [16,17]. Epidemiology alone, cannot deliver treatment options.
Figure 1.
taken from Umezawa R et al. J Radiat Res 2013;54:880-9. https://doi.org/10.1093/jrr/rrt011.
Figure 1.
taken from Umezawa R et al. J Radiat Res 2013;54:880-9. https://doi.org/10.1093/jrr/rrt011.
An important aspect of heart physiology to be kept in mind is the balance between energy requirement and energy supply. In 2017 Brown and coworkers described this issue and discussed a potential role of mitochondrial dysfunction in heart disease expecting that further research would fulfill therapeutic goals (Figure 1 in [18]).
In this review we will deal with cardiac side effects of anthracyclines and those due to external radiation therapy. We will focus on research and development work of daunomycin (adriamycin, doxorubicin) since this group of substances is relevant for treating breast cancer and other solid tumors.
Our emphasis will be on metabolic aspects such as fatty acid oxidation and glycolysis, two basic metabolic processes related to heart function. We will construct this description based on Nuclear Medicine diagnostic imaging together with biochemical parameters. Searching the early literature for biochemical elements related to heart failure, we identified a series of publications that related coenzyme Q10 (CoQ10) deficiency to heart disease. For this reason we have chosen the 1970 publication by Folkers, Littarru, Ho, Runge, Havanonda, and Cooley as a central reference for our review [19].
1.1. Pharmaceutical Development of Natural Anti-Tumor Substances
A historical account of the early research of new anti-tumor substances in Italy was published by Cassinelli in 2016 [20]. He described how in May 1960, a fruitful connection had been established by Dr. Bertini, CEO of Farmitalia, and Prof. Bucalossi, director of the Istituto Nazionale dei Tumori, to start research on new natural anti-tumor substances. Adriamycin was isolated as an antibiotic substance in the Farmitalia Research Laboratories working with a mutant strain Streptomyces peucetius bacterium (Streptomyces peucetius caesius). Dott. Aurelio Di Marco reported the discovery of daunomycin in 1964 [21]. In the same year, Dubost et al., reported the discovery of rubidomycin, a substance related to daunomycin [22]. A description of the therapeutical use of daunomycin followed in 1967 [23]. In 1969 Arcamone et al. reported the production of the new anti-tumor substance 14-hydroxydaunomycicn (Adriamycin) [24]. Phase I and preliminary Phase II studies with adriamycin were published in 1970 [25]. The patent, describing the anti-tumoral activity of the compound, was granted in 1971 to Farmitalia Carlo Erba Spa [26]. At that time, no cardiac side effects were mentioned.
In 1969 Bonadonna et al., described indeed ECG changes after treatment with adriamycin, i.e., doxorubicin [27]. Previously, in 1967, Tan et al. had also reported cardiotoxicity after the administration of daunomycin [28].
In 1981, Di Marco published a historical review on the discovery of daunorubicin [29]. Readers interested in further historical aspects of these developments can also consult the publication by Waksman and Woodruf on the discovery of Actinomyces antibioticus [30]. An important notion to be kept in mind is that actinomycin has a quinone structure as described by Dalgliesh and Todd in 1949 [31]. Additional studies from the early past century had evaluated quinones concerning their structure and biochemistry and their role as disinfectants and antibiotics [32,33,34,35,36].
In the 1970s, scientific data relating adriamycin to mitochondrial function appeared. In 1974 Iwamoto, Hansen, Porter, and Folkers, working with beef heart mitochondria, described that adriamycin had an inhibitory action on cell respiration by affecting CoQ10 enzymes related to the electron transfer processes [37]. The rationale for their study was based on the quinoid and hydroquinoid structures of adriamycin and daunorubicin. In their conclusions, they described this potential inhibition of CoQ10 by adriamycin. In 1976 Kishi et al. demonstrated a beneficial effect of CoQ10 supplementation for preventing adriamycin-induced inhibition of myocardial mitochondria affecting the NADH-oxidase and the succinoxidase systems. A molar ratio of 3:1 of CoQ10 to adriamycin prevented this inhibition [38]. An additional mechanism of cardiotoxicity by doxorubicin is the alteration of fatty acid oxidation and interference of carnitine palmitoyltransferase [39,40].
In 1986 Davies and Doroshow identified Complex I of mitochondrial OXPHOS as an essential metabolic site for doxorubicin [41]. An accompanying study showed that cardiac damage through doxorubicin was due to the production of a hydroxyl radical [42]. Following this line of research, Schimmel et al., illustrated oxidative stress mechanisms arising from anthracyclines based on their quinone structure (Figure 1 in [43]). A recent 2020 study on cardiotoxicity and doxorubicin involving respiratory Complex I and mitochondria was published by Wallace, Sardão, and Oliveira [44].
In an experimental setting with male Sprague-Dawley rats weighing 180-200g, Folkers et al. showed in 1978 that the administration of CoQ10 at a dose of 1mg/ml/kg resulted in "rescue" of electrocardiographic abnormalities caused by adriamycin cardiotoxicity [45]. These experiments showed clearly a relation of the drug to CoQ10 and placed CoQ10 in the category of a therapeutical option. Saltiel and McGuire presented a similar line of thought in 1983, mentioning the use of CoQ10, selenium sulfide, or α-tocopherol, among others, to prevent cardiotoxicity [46].
In 1981 Ohhara, Kanaide, and Nakamura presented data on the protection against cardiotoxicity due to adriamycin achieved by administering CoQ10. This effect was associated with a higher cardiac contractile tension and higher ATP stores [47].
The beneficial effects of CoQ10 or α-tocopherol had been previously shown by Lubawy, Whaley, and Hurley in an experimental setting in 1979 [48].
In 1982 Takimoto et al., described a protective effect of CoQ10 on the heart after the combined use of 500 rad irradiation with 60Co plus a mixture of adriamycin, cyclophosphamide and 5-FU can lead to cardiac toxicity [49]. In 1984 Tsubaki et al. described a preventive effect of CoQ10 administration on alterations of the ECG in patients treated either with adriamycin or daunorubicin [50].
An elegant experiment by Sarvazyan in 1996 delivered imaging data that demonstrated oxidation-sensitive fluorescence in isolated cardiac myofibers after administration of 160µM of doxorubicin. They showed that an oxidative mechanism was seen already 20 minutes after exposure [51]. Newer data from Doroshow complement these observations by demonstrating that quinones and anthracycline antibiotics can stimulate oxygen radical production in cardiac cells [52]. In 2005 Conklin reported an alteration of mitochondrial function as the side effect of anthracyclines and proposed using CoQ10 to prevent these changes [53]. Recently, Botehlho et al., showed protective effects of CoQ10 in an experimental model of doxorubicin-induced cardiotoxicity in 2020 [54].
While these valuable studies show beneficial cardiac effects of CoQ10 administration, they do not supply a full explanation of the underlying biochemical situation (Figure 3 in [55]). This can also be seen in a proposed protocol for early detection of subclinical left ventricular dysfunction by Caspi and Aronson (Figure 1 in [56]).
After tumors have been treated successfully, childhood cancer survivors face the risk of developing chronic heart diseases in adult age. Oeffinger et al., have called this a chronic health condition where the most common diseases are second cancers, cardiovascular disease, renal disease, musculoskeletal problems, and endocrine diseases [57]. Robison and Hudson described a complex health situation for childhood cancer survivors arising from the use of radiation, chemotherapy, or surgery (Figure 2 in [55]). The appearance of disease seems to have a variable latency time. Tumor types at the primary diagnosis can be leukemia, lymphoma, central nervous system tumors, Wilms tumor, neuroblastoma, rhabdomyosarcoma, and bone cancer [58]. Another medical situation associated with cardiotoxicity in adult life is hematopoietic stem cell transplantation [59].
Figure 2.
taken from Yan R et al. Korean J Radiol. 2015 Jul-Aug;16(4):919-928. https://doi.org/10.3348/kjr.2015.16.4.919.
Figure 2.
taken from Yan R et al. Korean J Radiol. 2015 Jul-Aug;16(4):919-928. https://doi.org/10.3348/kjr.2015.16.4.919.
A clinical description of Hodgkin’s lymphoma, published by Brice, de Kerviler, and Friedberg, pointed out that many patients died because of late toxic effects of the treatment [60]. Maraldo et al. approached the topic of cardiovascular disease after therapy for Hodgkin’s lymphoma in 2015 using a questionnaire approach. The authors found 19% of cases reporting ischemic heart disease, 12% with congestive heart failure, as well as arrhythmia and valvular disease [61]. Bergom et al., analyzed radiation-induced cardiac changes in 2021. They proposed that the goal of screening should be the detection of cardiac injury before it becomes clinically evident, expecting that dosimetry and advanced imaging would answer this problem [62].
1.2. Investigating Cardiotoxicity in Pediatric Oncology
Cardiotoxicity related to the administration of adriamycin is known as a syndrome that affects cardiac function leading to functional changes of the left ventricle. In 1973 Lefrak, Pitha, Rosenheim, and Gottlieb published an analysis of clinical and pathological characteristics found in patients who presented cardiotoxicity due to adriamycin [63]. Their study included 399 patients who presented advanced carcinomas. They observed cardiotoxic effects such as transient changes in the ECG in 45 cases and severe congestive heart failure in 11. Eight patients with heart failure died because of cardiac decompensation. Cardiac involvement was suggested by diminution of QRS voltage, ventricular failure and cardiac dilatation, and lack of response to inotropic drugs. Postmortem studies showed a decrease in cardiomyocytes, loss of contractile elements, mitochondrial swelling, and intramitochondrial dense inclusion bodies. Electron microscopy studies showed alterations in mitochondria, including swelling and absence or degeneration of cristae (Fig. 12 in [63]). Since a therapeutic approach to this problem was not available at that time, they simply suggested to limit the total dose to less than 550mg/m2.
An early diagnostic approach to adriamycin cardiotoxicity and irradiation was the endomyocardial biopsy, as reported by Billingham in 1977 [64]. In 1979 Ulmer, Ludwig, and Geiger presented the assessment of systolic time intervals to detect cardiotoxicity [65]. Potential benefits and limitations in the use of M-mode echocardiography for the diagnosis of doxorubicin cardiotoxicity were presented by Markiewicz et al. in 1980 [66]. Ritchie et al. advocated radionuclide angiography as a basis and follow-up examination when anthracyclines were administered [67]. Lahtinen et al., introduced radionuclide ventriculography in 1982 and found the method better than echocardiography and systolic time intervals [68]. In 1981, Lewis et al. described the application of echocardiography [69]. In 2000, Agarwala et al., described multiple gated acquisition scans (MUGA) [70]. A recent publication by Leerink et al. described changes of ejection fraction values in cases of cardiotoxicity. Surveillance intensity was adapted to the EF values [71].
In 1995, Shulkin et al., described the use of Nuclear Medicine diagnostic imaging using 18F-fluorodeoxyglucose positron emission tomography (18F-FDG) [72]. In 2007 an updated version of this topic appeared [73]. Two Figures in this publication showed cardiac uptake: Figure 2 shows the initial staging for a patient with an embryonal sarcoma; Figure 7 showed a similar pattern in follow-up examinations in a young patient with recurrent neuroblastoma. The authors did not explain the meaning of these cardiac images.
2. General Aspects of Anthracyclines and Cardiotoxicity
2.1. Cardiotoxicity due to Irradiation
Reports on the toxic effects or irraditaion on the heart have appeared since the late 1940s. In 1964 Vince described the radiation dose administered to children with congenital heart disease during X-ray examinations. Over time, between 1931 and 1948, the recommended amount had been reduced as a measure to prevent side effects of radiation such as shortening of life span, increased incidence of malignant tumors, and premature aging [74].
The mechanistic background of radiation-induced cardiac damage has been characterized by newer studies [75]. Marks et al. described the development of cardiac perfusion defects following radiotherapy for left-sided breast cancer. The incidence of these changes showed an increase over time [76]. Boerma and Hauer-Jensen described the evidence on radiation-induced heart disease stressing the appearance of capillary changes, coronary artery disease, and fibrosis [77]. Insight into clinical aspects of radiation-induced cardiotoxicity has been summarized by Yang et al. [78].
Tapio has summarized experimental and clinical data on radiation-induced changes, mentioning biochemical mechanisms such as alterations in fatty acid oxidation and of PPARα signaling (Figure 1 in [79]). In 2021 Azimzadeh et al. showed that activation of PPARα by fenofibrate administration improved lipid metabolism and mitochondrial respiration [80]. Turunen et al. showed in 2000 that PPARα exerted a positive influence on the biosynthesis of ubiquinone [81], thus indicating once more the central role of CoQ10. An additional biochemical alteration following irradiation is the decrease of selenium content in the heart, liver, and muscle [82].
2.2. The Use of Nuclear Medicine Diagnostic Imaging to Visualize Cardiac Metabolism and Cardiotoxicity
The following paragraphs will discuss the use of radionuclide imaging to demonstrate fatty acid uptake based on 123I-beta-methyl-iodophenylpentadecanoic acid (BMIPP). Fatty acid uptake and oxidation is the primary source of energy for the heart.
Knapp introduced the BMIPP tracer into clinical practice in 1986 [83]. In 1989 Ogata reported experimental data suggesting that adriamycin induced mitochondrial function impairment by decreasing myocardial uptake of BMIPP in rats, while heart perfusion evaluated with 201Tl, was uneventful compared to the control group [84]. The author had administered 4mg/kg of adriamycin intraperitoneally for six days. The main changes observed in light and electron microscopy were related to changes in the mitochondria. Myofibrils and the nucleus were only minimally changed.
In 1993 Wakasugi evaluated myocardial metabolism using two radionuclide imaging techniques BMIPP and 18F-FDG. They were applied in an experimental model with male Wistar rats where the animals had been treated with 2mg/kg of adriamycin once weekly for 6 to 10 weeks. A radionuclide imaging evaluation was done two weeks after completing the treatment. A series of changes were seen in those rats treated for more than eight weeks. The changes included a mortality rate of 60%, decreased myocardial weight, low albumin levels, diminished ventricular motion, and left ventricular ejection fraction. Levels of triglycerides and cholesterol were elevated. The imaging studies showed a decrease in accumulation of both 18F-FDG and BMIPP [85]. Both experimental and clinical data have described low uptake of BMIPP following administration of adriamycin [84,86]. Loss of cardiac function due to doxorubicin has been described in cell culture using 99mTc-Sestamibi [87], a tracer that shows mitochondrial membrane potential. Takemura and Fujiwara published an experimental characterization of cardiotoxicity due to doxorubicin showing interstitial fibrosis, cardiomyocyte vacuolation, and fibrosis [88].
In 1999 Inubushi evaluated this relation between fatty acid oxidation by BMIPP imaging and LEVF and showed a positive correlation between both methods [89]. It follows, that low LEVF values, which are often taken a cardiotoxicity marker, represent impaired cardiac free fatty acid utilization.
A functional relation between BMIPP and doxorubicin toxicity was described by Saito et al. in 2000 using a quantitative method for the determination of the k-value of tracer uptake [90]. The study group included 36 subjects treated with a mean dose of 257.8 mg/m2 doxorubicin due to various malignancies. The imaging procedures were done 7 to 28 days after treatment. Using this quantitative method, they described a harmful effect such that low k-values were evident (Figure 3 in [90]). This parameter was found to be associated with a poor prognosis. Using this methodology, Saito et al., assessed fatty acid oxidation in connection with taxan chemotherapy and showed that cardiac fatty acid metabolism was diminished after chemotherapy while perfusion remained normal (Figure 5 in [91]). BMIPP uptake was lower after chemotherapy and correlated with lower LVEF values (Figure 3 and 4 in [91]).
Figure 3.
Taken from Borde et al. PMID: 22761982, DOI: 10.4329/wjr.v4.i5.220. This publication is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license.
Figure 3.
Taken from Borde et al. PMID: 22761982, DOI: 10.4329/wjr.v4.i5.220. This publication is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license.
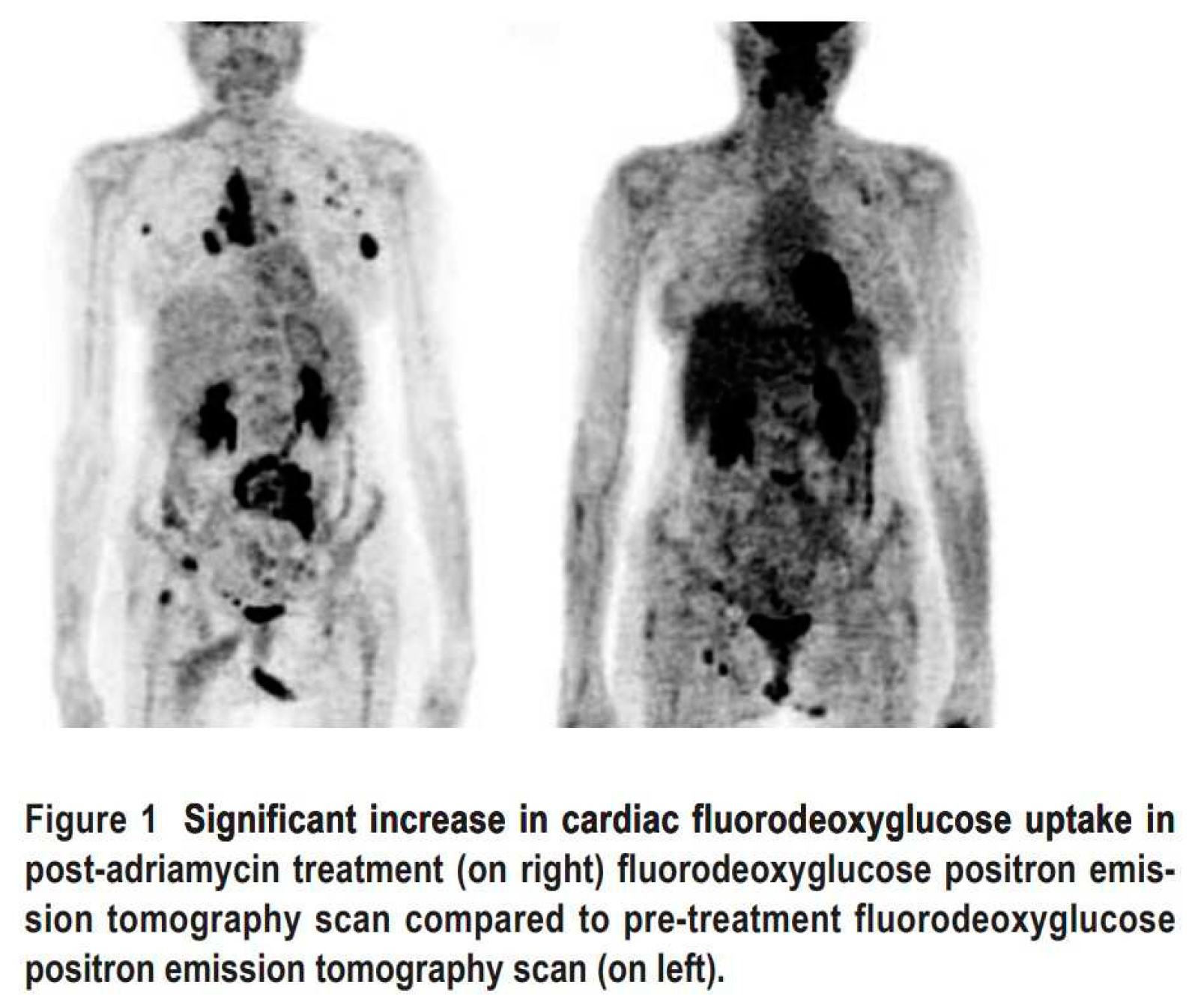
Figure 4.
taken from Dourado et al. Arq Bras Cardiol 2022, 118(6):1049-1058. PMID: 35703659. https://doi.org/10.36660/abc.20210463.
Figure 4.
taken from Dourado et al. Arq Bras Cardiol 2022, 118(6):1049-1058. PMID: 35703659. https://doi.org/10.36660/abc.20210463.
A clinical retrospective study published by Sarocchi evaluated 43 patients with Hodgkin's lymphoma who had received doxorubicin. The final 18F-FDG PET imaging procedure was done almost two years after treatment. They found an increase of cardiac 18F-FDG uptake in doxorubicin-treated patients together with a decline in left ventricular ejection fraction [92]. In 2019 this research group proposed that an increased myocardial 18F-FDG uptake could be taken as a doxorubicin-induced oxidative stress marker [93].
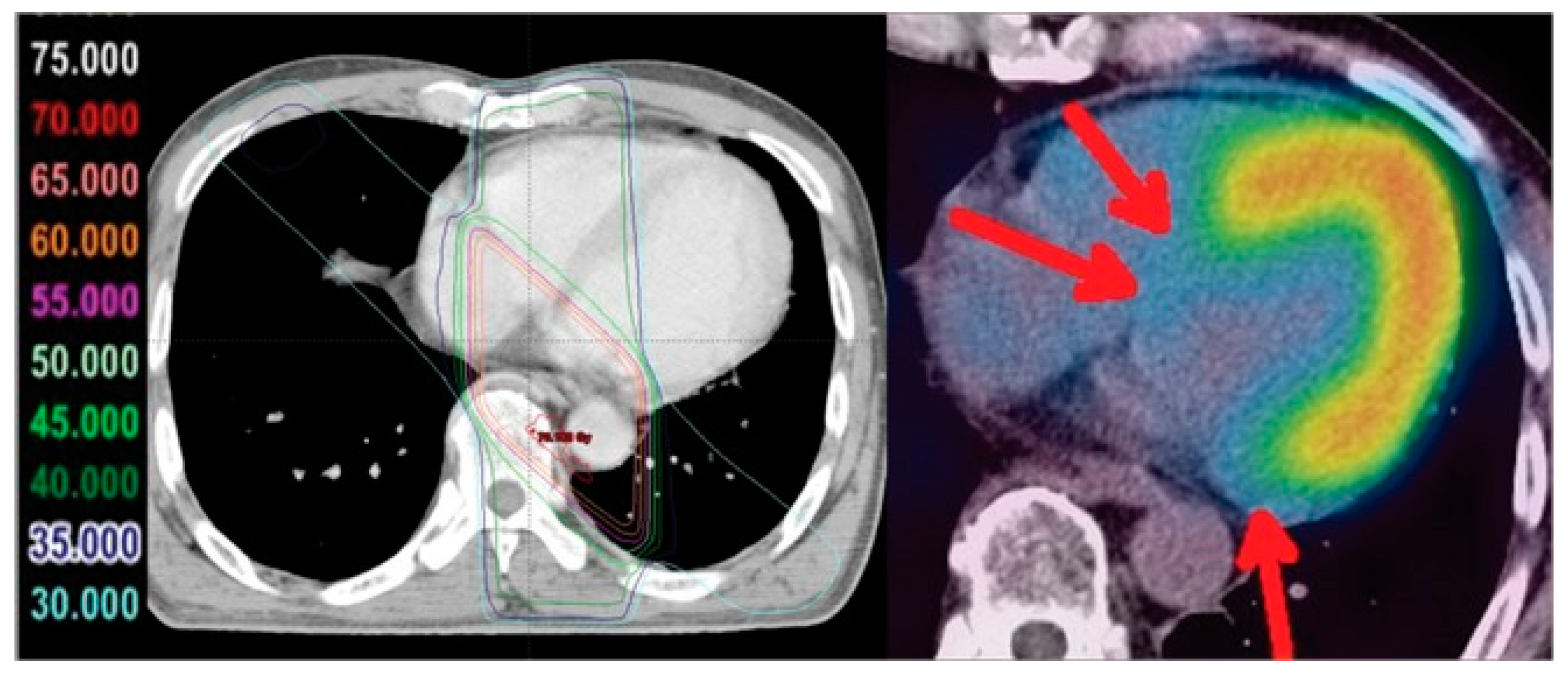
In clinical settings, some treatment approaches combine chemotherapy with external radiation therapy. In 1977 Billingham et al. described an enhancement effect of adriamycin cardiotoxicity when irradiation had been added [64]. An interesting fact concerning this effect was that irradiation showed this negative effect even when the treatment had been administered months to years before. The severity of these findings was confirmed by histopathology. In 2013 Umezawa et al. [94] evaluated radiation-induced cardiotoxicity using BMIPP radionuclide imaging in patients who had received different irradiation doses for esophageal cancer. The original Figure 3 from page 885 demonstrates the deleterious effect of external irradiation on the heart, i.e., disrupted fatty acid metabolism seen as a BMIPP uptake defect. The authors concluded that these images suggest myocardial damage. The loss of tracer uptake (red arrows) was described as being directly related to the administered radiation dose.
Besides these imaging results, previous studies from this research group had shown high myocardial 18F-FDG uptake following irradiation for esophageal cancer [95] together with significant elevation of BNP levels [96]. These results supported the diagnosis of cardiac damage with loss of fatty acid uptake, increased glycolysis, and an elevated level of cardiac damage marker.
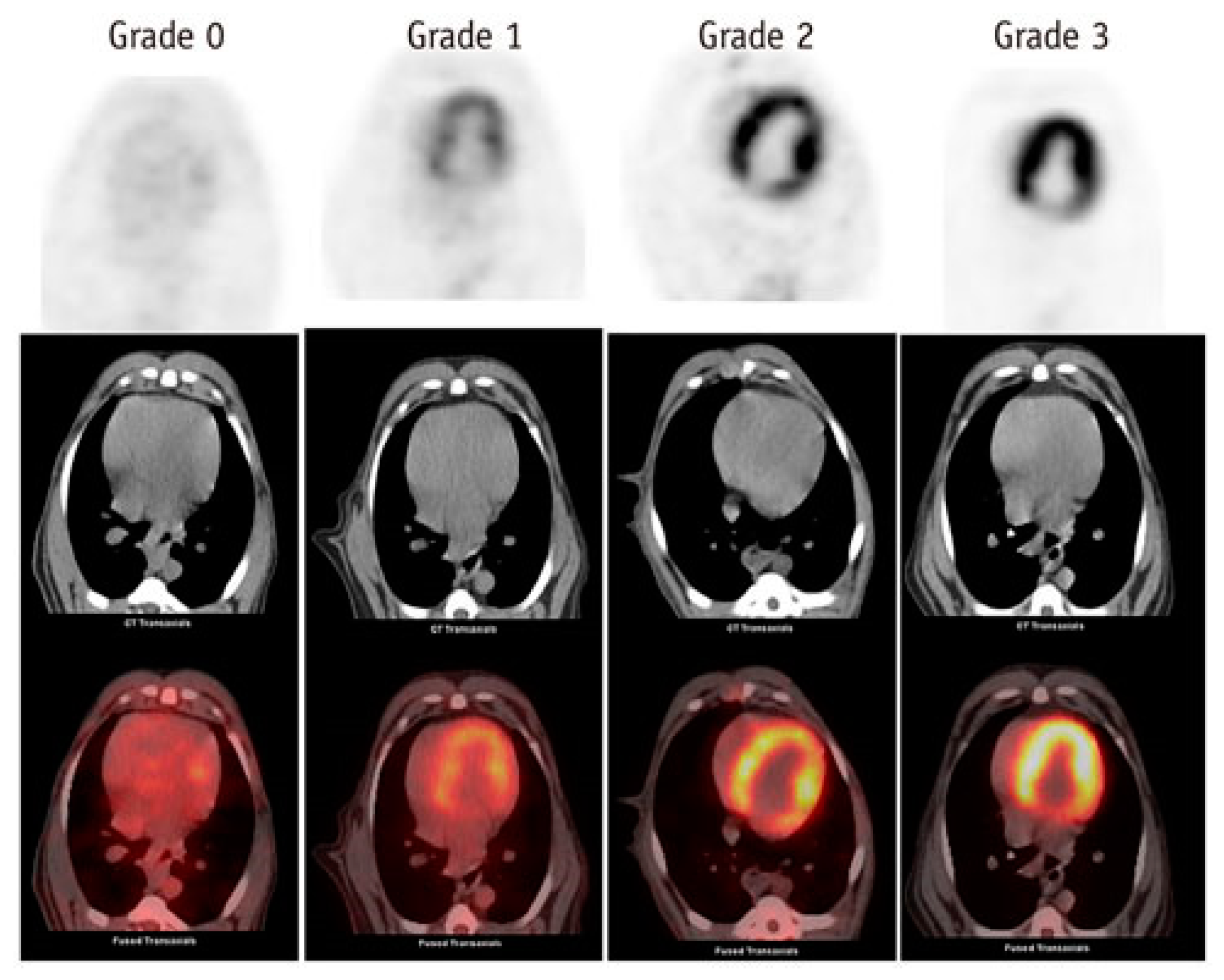
The experimental effect of external X-ray radiation with 20 Gy dose on heart metabolism of beagle dogs was investigated by Yan et al. [97]. 18F-FDG PET was done initially as well as three months later. They found high tracer uptake in the irradiated field and hypothesized that this was due to microvascular damage and mitochondrial injury. The results varied in intensity and were shown in a grading fashion (Figure 2 in [97]).
Anthracycline administration has been found to induce elevations of BNP. A poor prognosis of the disease was observed in patients with persistent elevations of BNP [98]. A persistent elevation of NT-proBNP following high dose chemotherapy for aggressive malignancies was associated with cardiac dysfunction [99]. Concerns about cardiotoxicity in the same setting have been reported by Zaucha-Prażmo et al. [100]. High-dose cyclophosphamide as part of BEAC treatment (BCNU, Etoposide, Cytarabine, Cyclophosphamide) can lead to acute subclinical systolic dysfunction, which was accompanied by an elevation of NT-proBNP levels. It is important to note that the patients in this study had elevated NT-proBNP levels, 445±65 pmol/L, before therapy [101]. This fact suggests that cardiac impairment was already present in these patients.
2.3. Nuclear Medicine Diagnostic Imaging of Cardiotoxicity Using 18F-FDG
In 2012 Borde, Kand, and Basu described the patterns of change of 18F-FDG uptake in lymphoma patients treated with adriamycin. Subgroup A of this study (n=8) showed an increased cardiac uptake (Figure 1 in [105]). Their original image is reproduced here.
Several studies have documented cardiac uptake of 18F-FDG as seen in staging examinations [106,107,108]. Jingu et al., described increased 18F-FDG uptake after radiotherapy for oesophageal cancer (Figure 1 in [109]). Specific description of cardiac uptake, however, was not discussed in these studies. Gorla et al., described a substantial increment of cardiac 18F-FDG uptake (Figure 1C and 1D in [110]) in a patient with Hodgkin’s lymphoma who had been treated according to an ABVD regimen. The authors suggested that this uptake represented cardiotoxicity after administration of adriamycin.
Matteo Bauckneht and coworkers have published a series of papers investigating the effects of doxorubicin on cardiac 18F-FDG metabolism since 2017 [92,93,111,112,113]. In the 2019 publication they concluded that this procedure was a biomarker for oxidative damage due to doxorubicin [93]. In his PhD thesis published 2020 [111] he added the following comment:
“These results substantiate emerging literature putting attention on the effects of anthracyclines on myocardial retention of FDG, and raise research and realistic prospects. First, our and other authors’ work prompts the question of which mechanism underlies the higher accumulation of FDG in the myocardium exposed to DXR as compared with control conditions. Finding the answer would imply gaining insights into the pathogenesis of DXR cardiotoxicity, which is complicated and still to be fully resolved, and possibly laying the foundations for novel strategies to avoid or mitigate cardiac injury”.
In 2020 Haider et al., discussed the importance of cardiac 18F-FDG uptake pattern in relation to risk stratification of cardiovascular disease [114]. They found a relation between focal tracer uptake and a higher risk for cardiac changes and lower LVEF values (Figure 3 in [114]).
Gherghe et al., conducted a prospective study on cardiotoxicity following HER2 inhibitor therapy evaluating radionuclide ventriculography and NT-proBNP as a biomarker revealing a negative correlation between both parameters (Figure 4 in [115]). This association was found both in the baseline and in the follow-up examination. We interpret this finding as a sign for pre-existing cardiac disease.
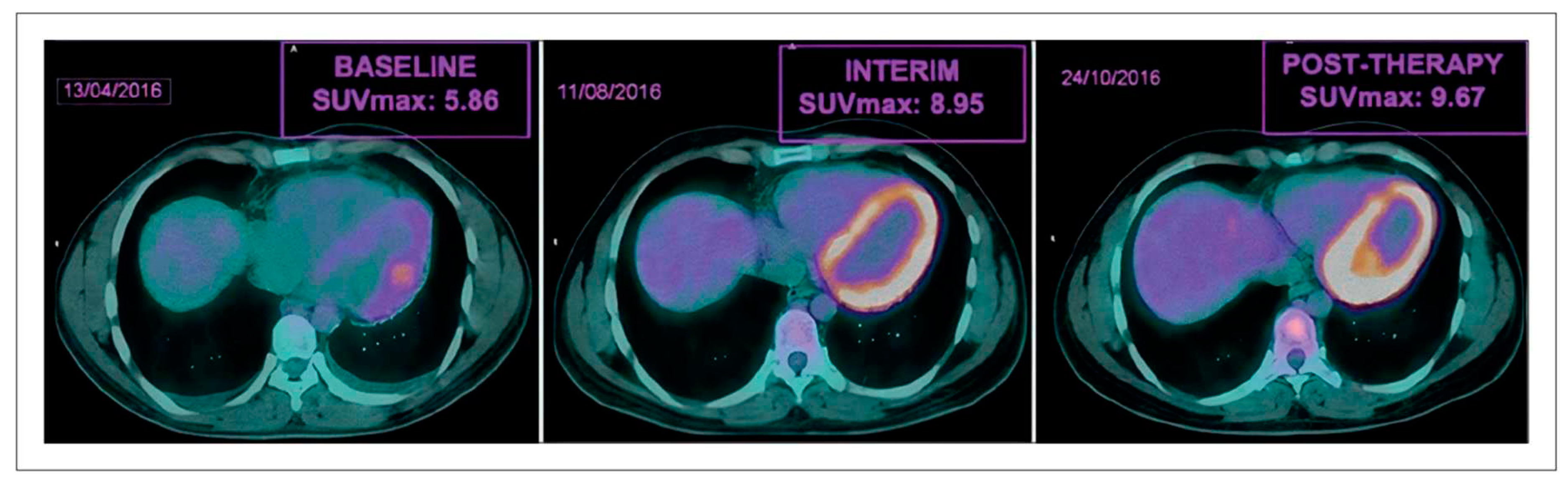
In 2022 Dourado et al., demonstrated increased 18F-FDG cardiac uptake after chemotherapy and interpreted the findings as a sign of cardiotoxicity (Figure in [116]).
In an accompanying editorial, Mesquita and Rezente stressed the importance of the findings in view of the association between diagnostic imaging and potential identification and definition of heart disease preventive interventions [117].
The spectrum of Nuclear Medicine methods for cardiac diagnostic imaging have been summarized by Cadour, Thuny, and Sourdon in 2022. Figure 1 includes methods for perfusion, mitochondrial, and metabolic imaging [118]. A recent review by Cannizzaro and coworkers, described current cardiac imaging methods for cardiotoxicity. The authors recognized that cardiac metabolic dysfunction, e.g., myocardial perfusion and mitochondrial function, might be found in these patients [119]. Citing Cadour, Thuny, and Sourdon [118] they dismissed the clinical utility of these imaging methods.
In 2023 an evaluation of cardiotoxicity due to anthracycline administration was published by Becker, Arruda, Berenguer, Buril, Cardinale, and Brandão [120]. Their analysis summarizes mechanisms of cardiotoxicity in Figure 2 including damage of mitochondria, accumulation of iron, inhibition of topoisomerase, induction of a proinflammatory state, and damage to sarcomeres. Although they recognized the importance of metabolic imaging, there was no treatment recommendation for these patients [120].
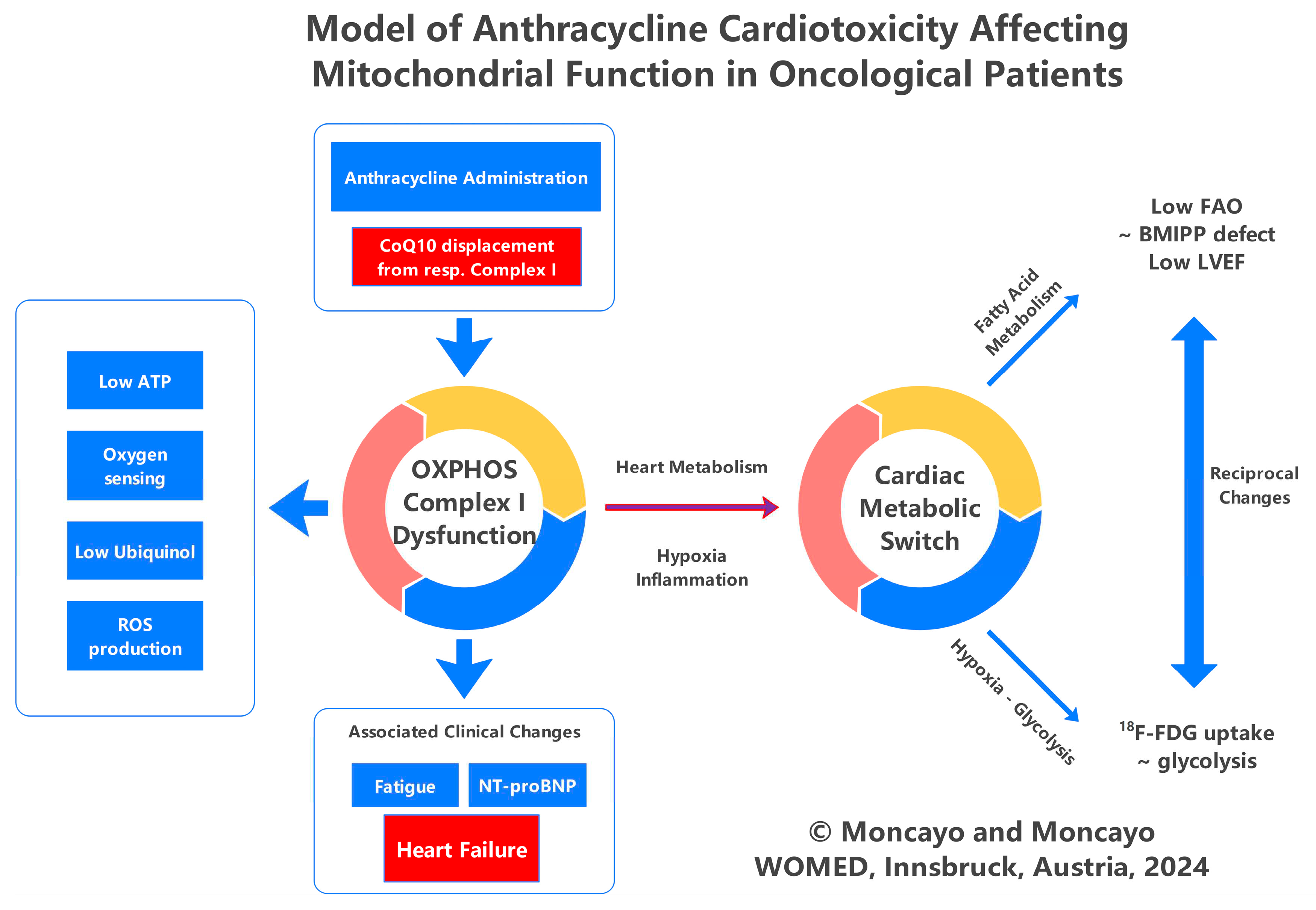
Our understanding of cardiotoxicity and heart failure is shown in Figure 5. The central issue is loss of mitochondrial function due to CoQ10 deficiency. In a series of publications, we have demonstrated both this pathogenetic principle as well as the treatment strategy for thyroid disease [121,122,123,124,125]. One key event related to CoQ10 deficiency is the development of hypoxia [126]. We have recently analyzed further biochemical changes of hypoxia stressing the role of CoQ10 deficiency [127].
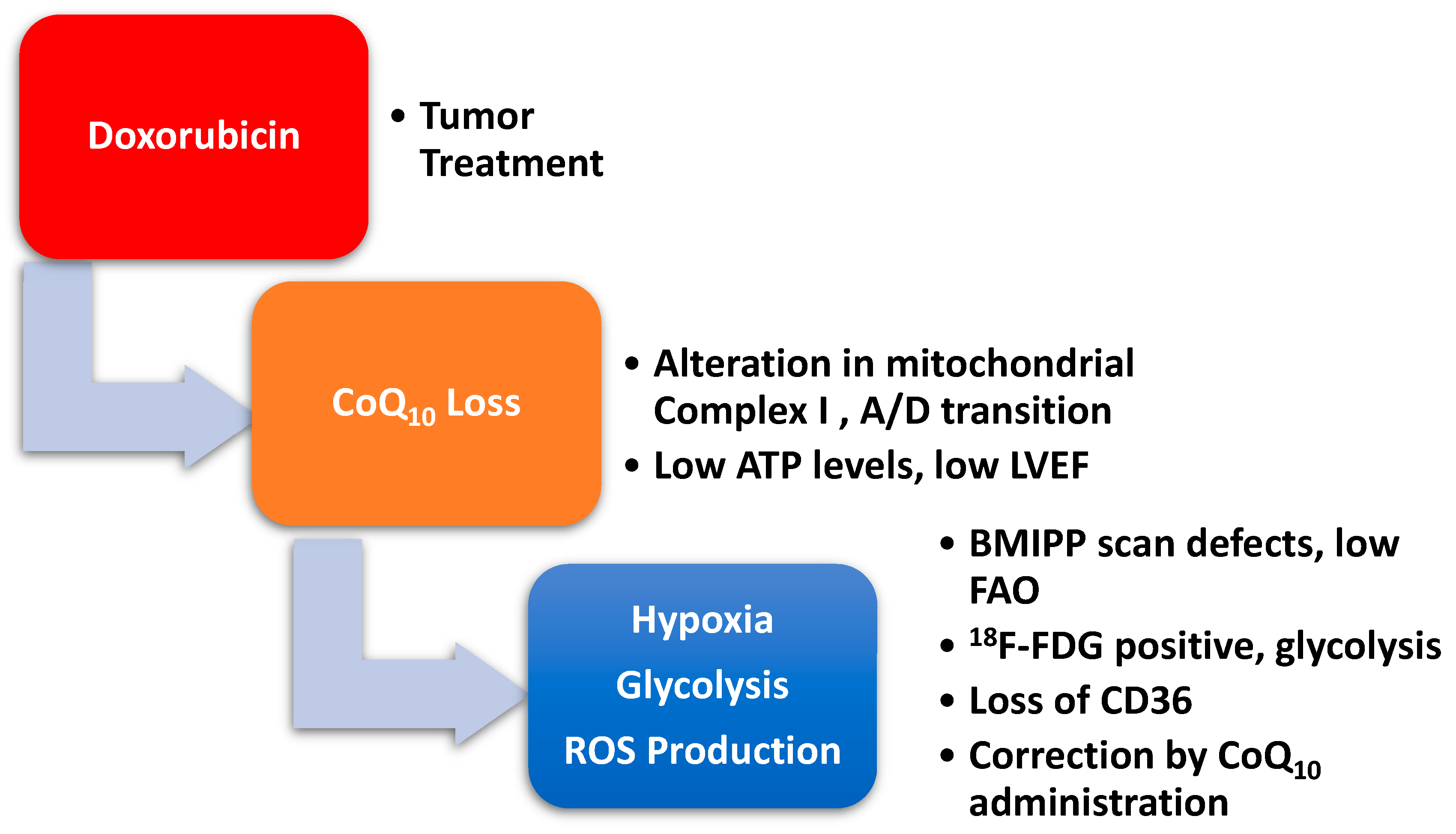
Figure 5.
Administration of doxorubicin will cause a displacement of CoQ10 from mitochondrial respiratory Complex I leading to an acquired dysfunction. Low level of ATP production will affect cardiac function which is reflected by diminished left ventricular ejection fraction. Nuclear Medicine diagnostic imaging will show decreased fatty acid utilization in the BMIPP scan, and increased glycolysis in the 18F-FDG positron emission tomography. Clinical research data have shown a relation between deficient CD36 expression and low fatty acid utilization. CoQ10 supplementation can treat these defects.
Figure 5.
Administration of doxorubicin will cause a displacement of CoQ10 from mitochondrial respiratory Complex I leading to an acquired dysfunction. Low level of ATP production will affect cardiac function which is reflected by diminished left ventricular ejection fraction. Nuclear Medicine diagnostic imaging will show decreased fatty acid utilization in the BMIPP scan, and increased glycolysis in the 18F-FDG positron emission tomography. Clinical research data have shown a relation between deficient CD36 expression and low fatty acid utilization. CoQ10 supplementation can treat these defects.
2.4. Doxorubicin-Induced Mitochondrial Damage and Reduced Cardiac Function
2.5. Looking beyond Oncology: Postpartum Cardiomyopathy and Cardiotoxicity. The Role of Selenium and BMIPP
In recent years a new clinical entity was associated with cardiotoxicity, i.e., postpartum cardiomyopathy has been described. In 1988 Davis and Brown described a woman who developed congestive heart failure postpartum. Seven years before this event, she had received doxorubicin because of osteosarcoma [128]. Newer case reports and risk evaluations have appeared since 2013 [129,130,131,132].
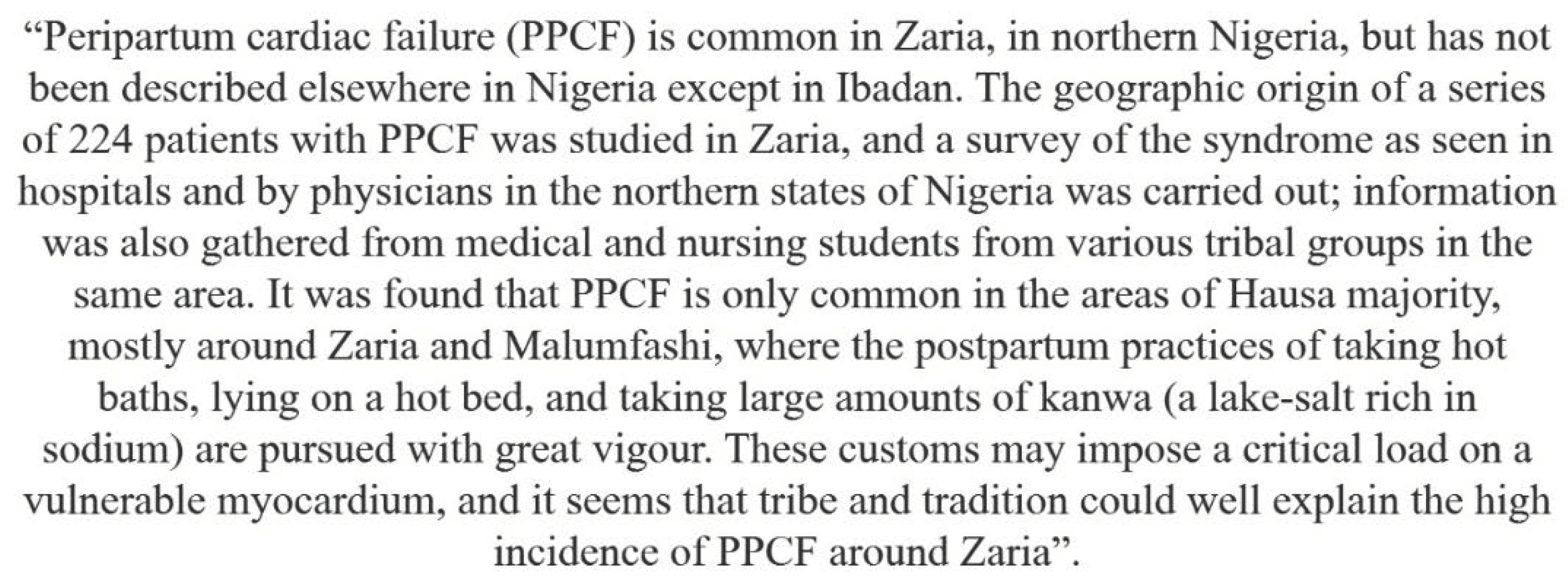
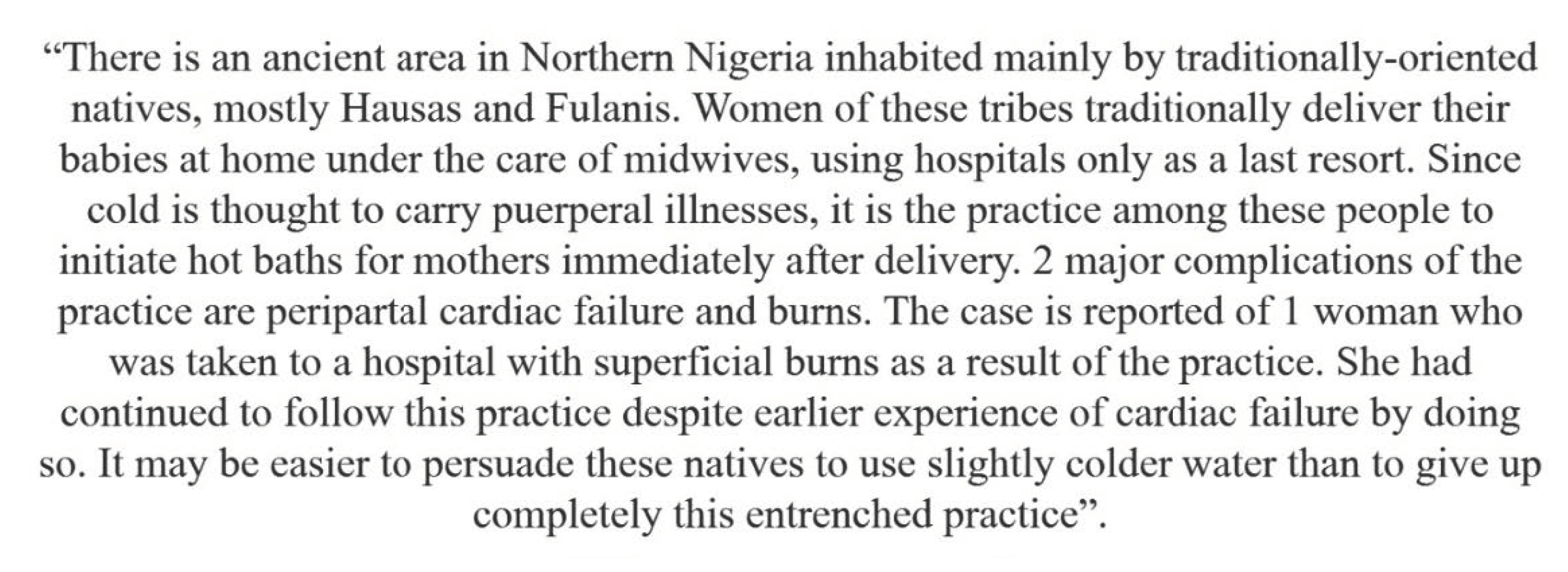
Descriptions of peripartum heart failure (PPCM) have been published for 170 years. Early reports were published by Ritchie in 1849 [133]) and by Porak in 1880 [134]. A review on PPCM published by Gouley in 1937 considered the disease to be idiopathic [135]. In the 1930s, Hull in 1937 and 1938 [136,137]. The term PPCM was used by Demakis and Rahimtoola in 1971 [138]. In 1974 Davidson et al. made a detailed description of cardiac failure in the perpartum as seen in Nigeria, mentioning the potential connection to heat stress (Table 1, page 206 in [139]). A citation of Davidson is shown in Box 1 and a similar source from Ezem et al. from 1980 [140] in Box 2.
Box 1. Description of PPCM by Davidson [139].
Box 2. Description of PPCM by Ezem [140].
As of 2024, the pathogenesis of PPCM has not been explained. Jha and Jha reviewed current data on the disease and produced a tentative model of pathogenesis built around the production of reactive oxidative substances (ROS). The weak point of the model is that ROS production has not been explained (Figure 2 in [141]).
In 1992 Cénac had described low selenium levels in PPCM patients [142,143,144,145,146]. Karaye reproduced these findings in 2015 [147]. However, further biochemical dimensions of the results were not recognized. Situations where selenium levels are deficient correlate also with CoQ10 deficiency [148,149]. This indirect evidence would validate are model of cardiotoxicity in PPCM. CoQ10 has not been evaluated in PPCM.
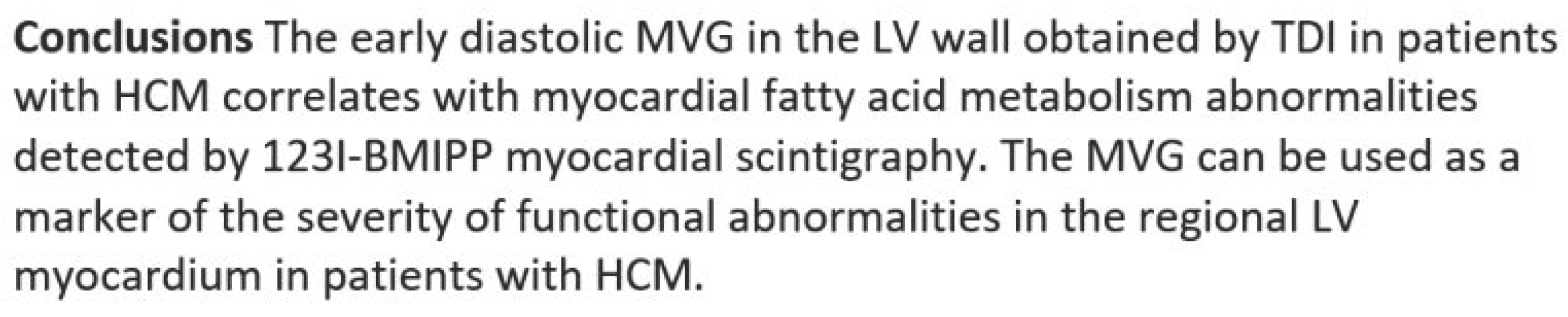
Thet Thet et al. reported the results of 123I-BMIPP scintigraphy carried out in a woman who was referred because of hypertrophic cardiomyopathy while breastfeeding her child. While the authors described the uptake of the tracer in the breast of the lactating woman, other findings were not described. Figure 2c clearly shows that the septum and the apex had uptake defects [150]. The fact that BMIPP uptake defects can be found in hypertrophic cardiomyopathy [151] supports our interpretation. As described in the preceding sections, low BMIPP uptake correlates with low LVEF, thus explaining heart failure. This has also been shown in a comparative study using BMIPP and tissue Doppler imaging such that BMIPP defects correlated with decreased ventricular function [152]. Box 3 shows the original conclusions of the study.
Box 3. Correlation between altered fatty acid metabolism and Doppler imaging [152].
A disease found to be associated with PPCM is preeclampsia. Cardiac changes seen in these patients bear some similarity to those seen in cardiotoxicity [153,154,155,156,157]. Bello et al. proposed that both diseases have similar pathogenesis [153].
Altered genes related to thioredoxin reductase have been described in preeclampsia associated with PPCM [158]. Apart from genetic alterations, low selenium levels, i.e. availability, could affect the function of thioredoxin reductase since it is the main constituent [159]. Lack of anti-oxidative protection could influence ROS release [160]. Clinical observations have associated selenium deficiency with exercise intolerance, higher mortality, and mitochondrial alterations [161]. Diminished uptake of BMIPP in asymptomatic subjects has also been described as being associated with lower exercise tolerance [162].
Additional biochemical information on preeclampsia relates to CoQ10. Enrique Teran and associates have described low levels of CoQ10 in eclampsia patients compared to normal pregnancies [163,164]. In 2018 they proposed that mitochondrial dysfunction due to CoQ10 deficiency was the disease mechanism in eclampsia [165].
2.6. Connecting Heat Stress to Cardiovascular Disease and PPCM
The original setting of PPCM is related to heat exposure. The most salient evidence on the influence of heat stress on mitochondrial function comes from the known thermo-lability of Complex I and especially of CoQ10 [166]. Pobezhimova et al. have shown that under experimental conditions, heat stress affects the function of Complex I, the main change being its inactivation [167]. A similar result of altered function of Complex, I through heat exposure, has been reported by Ludwig et al., in a system that used beef heart mitochondria [168]. The isolated CoQ10 substance also shows lability to heat stress at 45° to 55°C [169]. A decrease in the levels of CoQ10 will alter and diminish the function of Complex I of OXPHOS. Mitochondria lacking CoQ10 will then produce more ROS. If this occurs in the heart, then heart function will be compromised. In 1999 Ide et al. proposed that Complex I could be the source of ROS in the failing heart [170]. The heart is indeed the organ with the highest CoQ10 content in the body, and low levels can consequently affect cardiac function [171]. A similar situation can be expected in conditions such as cardiomyopathy [172].
Recently two publications have looked at the relationship between cardiac disease and heat stress. Ranek et al. described changes of heat shock proteins in heart failure, pointing towards the increased expression of hsp70, hsp90 and BAG-3 [173]. In 2012 Iguchi et al. looked at cardiovascular and hormonal changes following heat stress produced by sitting in a heat stress chamber for 30 minutes at 73°C [174]. They demonstrated that this stimulus had an elevation of hsp72 and prolactin. The increase in prolactin levels seemed related to the endurance capacity in response to exercise under heat conditions [175]. Heat exposure and muscular activity can also affect blood magnesium levels inducing a severe decrease to suboptimal levels [176].
In a recent epidemiological analysis, Wang et al. described an association between previous heat stress situations and heart disease [177]. Nzvere et al. have reached similar conclusions in evaluating long-term consequences of heatstroke in reference to cardiac disease [178]. We propose that these authors were dealing with exposure to heatstroke which had led to a condition of CoQ10 deficiency. Unfortunately, this biochemical situation was neither investigated nor treated.
In short, the take-home message from the data cited in this section can be stated as follows. Heat stress can lead to lower magnesium levels and elevation of prolactin. Heat stress can affect CoQ10, which will consequently alter and diminish the function of Complex I of OXPHOS. Loss of magnesium will affect the function of Complex V. Mitochondria lacking CoQ10 will then produce more ROS and less ATP. One can expect that inefficient ATP production in the mitochondria will be associated with fatigue as a key symptom. Combining magnesium, selenium, and CoQ10 will restore mitochondrial function and prevent ROS production.
2.7. Gonadotoxicity
The radiosensitivity of ovary to radiation has been known for decades. Medical history contains an account of methods to destroy ovarian function more than 100 years ago. The use of Roentgen rays for achieving castration was described as an auxiliary therapy for breast cancer [185]. The technique had been promoted and developed since 1889, when presented at a surgical congress. Following this same therapy concept, Willis et al. presented data on female castration utilizing irradiation in 1940 [186]. In 1963 Brinkley et al. described the effects of deep X-rays for treating breast cancer in relation to menopause. The study included 267 women treated between 1942 and 1952 at Addenbrooke’s Hospital in Cambridge [187]. A follow-up evaluation done some 16 years later revealed increased mortality related to heart disease, cerebrovascular disease, and cancer at the heavily irradiated sites. The course of breast cancer was not influenced by this therapy[188]. Ovarian ablation through radiotherapy was still used in 1994 for breast cancer [189]. Effects of gonadal irradiation were described by Lushbaugh and Casarett in 1976 [190].
In 1989 Wallace et al. described ovarian function changes in patients treated with whole abdominal external radiation. Treatments had been done between 1942 and 1985. The authors identified fifty-three patients for the evaluation and concluded a poor outlook for normal ovarian function after therapy [191].
Ovarian biopsies in ten patients treated for childhood leukemia were analyzed by Marcello et al. in 1990. In the small series of cases, they found a reduction in the number of follicles, ovarian fibrosis, and changes in the structure of blood capillaries [192].
Larsen et al. evaluated ovarian function in 100 cancer survivors in Denmark. The patients had received both chemotherapy as well as radiation as treatment modalities. The study found that one out of six patients developed premature ovarian failure. [193].
Chemaitilly et al. conducted a retrospective analysis of cancer survivors looking for the development of acute ovarian failure. A detailed analysis of the treatment modality and dose was carried out. Starting from 14372 patients included in the Childhood Cancer Survivor Study, the authors selected 3390 cases for the study. Inclusion criteria included age > 18yr and having valid data on menstrual history. Acute ovarian failure was defined as cessation or absence of menstruation within five years after therapy. The affected patients were younger than 20 years at the time of diagnosis and 32.9 years of age at the study. The initial diagnoses included leukemia, lymphomas, Wilms’ tumor, neuroblastoma, soft-tissue sarcoma, and other entities. Treatment modalities are shown in Table 1 in [194]. Acute ovarian failure was found in 6.3% of cases.
Schilsky et al. described gonadal dysfunction after chemotherapy given to cancer patients. The same group described gonadal changes after cancer treatment in children [195]. Similar observations were published by Whitehead et al. in 1983 [196]. The authors commented that the mechanisms of ovarian changes were poorly understood.
The question of fertility and reproduction in young patients after therapy for cancer was addressed by Meirow in 2000 [197]. Levine et al. have described the development of premature menopause in cancer survivors treated with either procarbazine or radiotherapy or who had had stem cell transplantation [198]. Recommendations for surveillance for cancer survivors due to potential risks for cardiomyopathy and premature ovarian failure have been published without including suggestions for treatment [199,200].
3. Discussion and Conclusions
Based on the evidence presented we propose that the pathogenic mechanism of anthracycline cardiotoxicity is caused by CoQ10 deficiency following chemotherapy or radiation resulting in acquired mitochondrial dysfunction. A central metabolic event is the switch from fatty acid oxidation to glycolysis. Low level of fatty acids utilization correlates with diminished LVEF values which characterize heart failure (Figure 6). We believe that this same principle can explain other heart affections characterized by low values of left ventricular ejection fraction.
The visualization of glycolysis using 18F-FDG allows the interpretation that glycolysis is an expression of hypoxia [127].
We propose that clinical evaluation of oncological patients must include determinations of CoQ10 and NT-proBNP [201] prior to therapy as well as during follow-up. Administration of CoQ10 has been shown to increase mitochondrial levels [202], by which treatment of cardiotoxicity is feasible. We have published further details on CoQ10 physiology and supplementation elsewhere in 2023 [127].
Figure 6.
Anthracycline administration will cause a displacement of COQ10 from Complex I of the OXPHOS chain. Heart metabolism will switch from FAO to a hypoxic condition associated with glycolysis. Low utilization of FA correlates with low LVEF. Altered function of Complex I will lead to low ATP production, oxygen sensing can be compromised, ubiquinol levels can be low, ROS production increases. The main symptom is fatigue. Elevated NT-proBNP is a biomarker of the process. Failure to correct CoQ10 levels can end in heart failure.
Figure 6.
Anthracycline administration will cause a displacement of COQ10 from Complex I of the OXPHOS chain. Heart metabolism will switch from FAO to a hypoxic condition associated with glycolysis. Low utilization of FA correlates with low LVEF. Altered function of Complex I will lead to low ATP production, oxygen sensing can be compromised, ubiquinol levels can be low, ROS production increases. The main symptom is fatigue. Elevated NT-proBNP is a biomarker of the process. Failure to correct CoQ10 levels can end in heart failure.
Author Contributions
Conceptualization, writing, editing RM and HM. Graphic work was done by RM.
Funding
This work received self-funding by WOMED.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Pearson, H.A. History of pediatric hematology oncology. Pediatr Res 2002, 52, 979–992. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D. Una nuova frontiera: la cardioncologia. Cardiologia 1996, 41, 887–891. [Google Scholar] [PubMed]
- Beutner, R. The cardiac toxicity of injectable local anesthetics. Fed Proc 1946, 5, 166. [Google Scholar] [PubMed]
- Butany, J.; Ahn, E.; Luk, A. Drug-related cardiac pathology. J Clin Pathol 2009, 62, 1074–1084. [Google Scholar] [CrossRef] [PubMed]
- Page, R.L., 2nd; O'Bryant, C.L.; Cheng, D.; Dow, T.J.; Ky, B.; Stein, C.M.; Spencer, A.P.; Trupp, R.J.; Lindenfeld, J. Drugs That May Cause or Exacerbate Heart Failure: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e32–69. [Google Scholar] [CrossRef] [PubMed]
- Meinardi, M.T.; van der Graaf, W.T.; van Veldhuisen, D.J.; Gietema, J.A.; de Vries, E.G.; Sleijfer, D.T. Detection of anthracycline-induced cardiotoxicity. Cancer treatment reviews 1999, 25, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Altena, R.; Perik, P.J.; van Veldhuisen, D.J.; de Vries, E.G.; Gietema, J.A. Cardiovascular toxicity caused by cancer treatment: strategies for early detection. Lancet Oncol 2009, 10, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Altena, R.; Hubbert, L.; Kiani, N.A.; Wengström, Y.; Bergh, J.; Hedayati, E. Evidence-based prediction and prevention of cardiovascular morbidity in adults treated for cancer. Cardiooncology 2021, 7, 20. [Google Scholar] [CrossRef] [PubMed]
- Cuomo, A.; Rodolico, A.; Galdieri, A.; Russo, M.; Campi, G.; Franco, R.; Bruno, D.; Aran, L.; Carannante, A.; Attanasio, U.; et al. Heart Failure and Cancer: Mechanisms of Old and New Cardiotoxic Drugs in Cancer Patients. Card Fail Rev 2019, 5, 112–118. [Google Scholar] [CrossRef]
- Thomas, S.A. Chemotherapy Agents That Cause Cardiotoxicity. US Pharm 2017, 42, HS24–HS33. [Google Scholar]
- Cardinale, D.; Mills, N.L.; Mueller, C. Cardiac biomarkers in the field of cardio-oncology. Eur Heart J Acute Cardiovasc Care 2022, 11, e1–e2. [Google Scholar] [CrossRef] [PubMed]
- Tsiouris, K.M.; Mitsis, A.; Grigoriadis, G.; Karanasiou, G.; Lakkas, L.; Mauri, D.; Toli, M.A.; Alexandraki, A.; Keramida, K.; Cardinale, D.; Fotiadis, D.I. Risk Stratification for Cardiotoxicity in Breast Cancer Patients: Predicting Early Decline of LVEF After Treatment(). Annu Int Conf IEEE Eng Med Biol Soc 2023, 2023, 1–4. [Google Scholar] [CrossRef] [PubMed]
- López-Sendón, J.; Álvarez-Ortega, C.; Zamora Auñon, P.; Buño Soto, A.; Lyon, A.R.; Farmakis, D.; Cardinale, D.; Canales Albendea, M.; Feliu Batlle, J.; Rodríguez Rodríguez, I.; et al. Classification, prevalence, and outcomes of anticancer therapy-induced cardiotoxicity: the CARDIOTOX registry. Eur Heart J 2020, 41, 1720–1729. [Google Scholar] [CrossRef] [PubMed]
- Gavila, J.; Seguí, M.; Calvo, L.; López, T.; Alonso, J.J.; Farto, M.; Sánchez-de la Rosa, R. Evaluation and management of chemotherapy-induced cardiotoxicity in breast cancer: a Delphi study. Clin Transl Oncol 2017, 19, 91–104. [Google Scholar] [CrossRef] [PubMed]
- Belger, C.; Abrahams, C.; Imamdin, A.; Lecour, S. Doxorubicin-induced cardiotoxicity and risk factors. Int J Cardiol Heart Vasc 2024, 50, 101332. [Google Scholar] [CrossRef] [PubMed]
- Martinez, H.R.; Beasley, G.S.; Goldberg, J.F.; Absi, M.; Ryan, K.A.; Guerrier, K.; Joshi, V.M.; Johnson, J.N.; Morin, C.E.; Hurley, C.; et al. Pediatric Cardio-Oncology Medicine: A New Approach in Cardiovascular Care. Children (Basel) 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, C.L. Cancer Survivorship. N Engl J Med 2018, 379, 2438–2450. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.A.; Perry, J.B.; Allen, M.E.; Sabbah, H.N.; Stauffer, B.L.; Shaikh, S.R.; Cleland, J.G.; Colucci, W.S.; Butler, J.; Voors, A.A.; et al. Mitochondrial function as a therapeutic target in heart failure. Nature reviews. Cardiology 2017, 14, 238–250. [Google Scholar] [CrossRef] [PubMed]
- Folkers, K.; Littarru, G.P.; Ho, L.; Runge, T.M.; Havanonda, S.; Cooley, D. Evidence for a deficiency of coenzyme Q10 in human heart disease. Int Z Vitaminforsch 1970, 40, 380–390. [Google Scholar] [PubMed]
- Cassinelli, G. The roots of modern oncology: from discovery of new antitumor anthracyclines to their clinical use. Tumori 2016, 2016, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Dimarco, A.; Gaetani, M.; Orezzi, P.; Scarpinato, B.M.; Silvestrini, R.; Soldati, M.; Dasdia, T.; Valentini, L. 'Daunomycin', A new antibiotic of the rhodomycin group. Nature 1964, 201, 706–707. [Google Scholar] [CrossRef] [PubMed]
- Dubost, M.; Ganter, P.; Maral, R.; Ninet, L.; Pinnert, S.; Preudhomme, J.; Werner, G.H. Rubidomycin: A New Antibiotic with Cytostatic Properties. Cancer Chemother Rep 1964, 41, 35–36. [Google Scholar]
- Di Marco, A. Attività biologica ed utilizzazione terapeutica dell'antibiotico daunomicina. Tumori 1967, 53, 269–291. [Google Scholar] [CrossRef] [PubMed]
- Arcamone, F.; Cassinelli, G.; Fantini, G.; Grein, A.; Orezzi, P.; Pol, C.; Spalla, C. Adriamycin, 14-hydroxydaunomycin, a new antitumor antibiotic from S. peucetius var. caesius. Biotechnol Bioeng 1969, 11, 1101–1110. [Google Scholar] [CrossRef] [PubMed]
- Bonadonna, G.; Monfardini, S.; De Lena, M.; Fossati-Bellani, F.; Beretta, G. Phase I and preliminary phase II evaluation of adriamycin (NSC 123127). Cancer Res 1970, 30, 2572–2582. [Google Scholar] [PubMed]
- Arcamone, F.; Cassinelli, G.; di Marco, A.; Gaetani, M. Patent application Farmitalia Research Laboratories 251 NSA. 1967.
- Bonadonna, G.; Monfardini, S.; De Lena, M.; Fossati-Bellani, F. Clinical evaluation of adriamycin, a new antitumour antibiotic. British medical journal 1969, 3, 503–506. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.; Tasaka, H.; Yu, K.P.; Murphy, M.L.; Karnofsky, D.A. Daunomycin, an antitumor antibiotic, in the treatment of neoplastic disease. Clinical evaluation with special reference to childhood leukemia. Cancer 1967, 20, 333–353. [Google Scholar] [CrossRef] [PubMed]
- Di Marco, A.; Cassinelli, G.; Arcamone, F. The discovery of daunorubicin. Cancer Treat Rep 1981, 65 Suppl 4, 3–8. [Google Scholar]
- Waksman, S.A.; Woodruff, H.B. Actinomyces antibioticus, a New Soil Organism Antagonistic to Pathogenic and Non-pathogenic Bacteria. J Bacteriol 1941, 42, 231–249. [Google Scholar] [CrossRef] [PubMed]
- Dalgliesh, C.E.; Todd, A.R. Actinomycin. Nature 1949, 164, 820. [Google Scholar] [CrossRef] [PubMed]
- Thalhimer, W.; Palmer, B. The Bactericidal Action of Quinone and Other Phenol Oxidation Products as Determined by the Rideal-Walker Method. J Infect Dis 1911, 9, 172–180. [Google Scholar] [CrossRef]
- Cooper, E.A. On the Relations of the Phenols and their Derivatives to Proteins. A contribution to our knowledge of the Mechanism of Disinfection: Part III. The Chemical Action of Quinone upon Proteins. The Biochemical journal 1913, 7, 186–196. [Google Scholar] [CrossRef] [PubMed]
- Morgan, G.T.; Cooper, E.A. The Bactericidal Action of the Quinones and Allied Compounds. The Biochemical journal 1921, 15, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann-Ostenhof, O. Die Biochemie der Chinone. Experientia 1947, 3, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Arcamone, F.; Cassinelli, G.; Franceschi, G.; Penco, S.; Pol, C.; Redaelli, S.; Selva, A. Structure and Physicochemical Properties of Adriamycin (Doxorubicin). Berlin, Heidelberg, 1972; pp. 9-22.
- Iwamoto, Y.; Hansen, I.L.; Porter, T.H.; Folkers, K. Inhibition of coenzyme Q10-enzymes, succinoxidase and NADH-oxidase, by adriamycin and other quinones having antitumor activity. Biochem Biophys Res Commun 1974, 58, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Kishi, T.; Watanabe, T.; Folkers, K. Bioenergetics in clinical medicine: prevention by forms of coenzyme Q of the inhibition by adriamycin of coenzyme Q10-enzymes in mitochondria of the myocardium. Proc Natl Acad Sci U S A 1976, 73, 4653–4656. [Google Scholar] [CrossRef] [PubMed]
- Abdel-aleem, S.; el-Merzabani, M.M.; Sayed-Ahmed, M.; Taylor, D.A.; Lowe, J.E. Acute and chronic effects of adriamycin on fatty acid oxidation in isolated cardiac myocytes. J Mol Cell Cardiol 1997, 29, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.R.; Hong, Y.M.; Boriack, R.L.; Bennett, M.J. Effect of L-carnitine supplementation on cardiac carnitine palmitoyltransferase activities and plasma carnitine concentrations in adriamycin-treated rats. Pediatr Res 2003, 53, 788–792. [Google Scholar] [CrossRef] [PubMed]
- Davies, K.J.; Doroshow, J.H. Redox cycling of anthracyclines by cardiac mitochondria. I. Anthracycline radical formation by NADH dehydrogenase. J Biol Chem 1986, 261, 3060–3067. [Google Scholar] [CrossRef] [PubMed]
- Doroshow, J.H.; Davies, K.J. Redox cycling of anthracyclines by cardiac mitochondria. II. Formation of superoxide anion, hydrogen peroxide, and hydroxyl radical. J Biol Chem 1986, 261, 3068–3074. [Google Scholar] [CrossRef] [PubMed]
- Schimmel, K.J.; Richel, D.J.; van den Brink, R.B.; Guchelaar, H.J. Cardiotoxicity of cytotoxic drugs. Cancer treatment reviews 2004, 30, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Wallace, K.B.; Sardão, V.A.; Oliveira, P.J. Mitochondrial Determinants of Doxorubicin-Induced Cardiomyopathy. Circulation research 2020, 126, 926–941. [Google Scholar] [CrossRef] [PubMed]
- Folkers, K.; Choe, J.Y.; Combs, A.B. Rescue by coenzyme Q10 from electrocardiographic abnormalities caused by the toxicity of adriamycin in the rat. Proc Natl Acad Sci U S A 1978, 75, 5178–5180. [Google Scholar] [CrossRef] [PubMed]
- Saltiel, E.; McGuire, W. Doxorubicin (adriamycin) cardiomyopathy. West J Med 1983, 139, 332–341. [Google Scholar] [PubMed]
- Ohhara, H.; Kanaide, H.; Nakamura, M. A protective effect of coenzyme Q10 on the adriamycin-induced cardiotoxicity in the isolated perfused rat heart. J Mol Cell Cardiol 1981, 13, 741–752. [Google Scholar] [CrossRef] [PubMed]
- Lubawy, W.C.; Whaley, J.; Hurley, L.H. Coenzyme Q10 or alpha-tocopherol reduce the acute toxicity of anthramycin in mice. Res Commun Chem Pathol Pharmacol 1979, 24, 401–404. [Google Scholar] [PubMed]
- Takimoto, M.; Sakurai, T.; Kodama, K.; Yokoi, H.; Suzuki, Y.; Enomoto, K.; Okada, N. [Protective effect of CoQ 10 administration on cardial toxicity in FAC therapy]. Gan To Kagaku Ryoho 1982, 9, 116–121. [Google Scholar] [PubMed]
- Tsubaki, K.; Horiuchi, A.; Kitani, T.; Taniguchi, N.; Masaoka, T.; Shibata, H.; Yonezawa, T.; Tsubakio, T.; Kawagoe, H.; Shinohara, Y.; et al. [Investigation of the preventive effect of CoQ10 against the side-effects of anthracycline antineoplastic agents]. Gan To Kagaku Ryoho 1984, 11, 1420–1427. [Google Scholar] [PubMed]
- Sarvazyan, N. Visualization of doxorubicin-induced oxidative stress in isolated cardiac myocytes. Am J Physiol 1996, 271, H2079–2085. [Google Scholar] [CrossRef] [PubMed]
- Doroshow, J.H. Effect of Anticancer Quinones on Reactive Oxygen Production by Adult Rat Heart Myocytes. Oxid Med Cell Longev 2020, 2020, 8877100. [Google Scholar] [CrossRef] [PubMed]
- Conklin, K.A. Coenzyme Q10 for prevention of anthracycline-induced cardiotoxicity. Integr Cancer Ther 2005, 4, 110–130. [Google Scholar] [CrossRef] [PubMed]
- Botelho, A.F.M.; Lempek, M.R.; Branco, S.; Nogueira, M.M.; de Almeida, M.E.; Costa, A.G.; Freitas, T.G.; Rocha, M.; Moreira, M.V.L.; Barreto, T.O.; et al. Coenzyme Q10 Cardioprotective Effects Against Doxorubicin-Induced Cardiotoxicity in Wistar Rat. Cardiovasc Toxicol 2020, 20, 222–234. [Google Scholar] [CrossRef] [PubMed]
- Robison, L.L.; Hudson, M.M. Survivors of childhood and adolescent cancer: life-long risks and responsibilities. Nat Rev Cancer 2014, 14, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Caspi, O.; Aronson, D. Surviving Cancer without a Broken Heart. Rambam Maimonides Med J 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Oeffinger, K.C.; Mertens, A.C.; Sklar, C.A.; Kawashima, T.; Hudson, M.M.; Meadows, A.T.; Friedman, D.L.; Marina, N.; Hobbie, W.; Kadan-Lottick, N.S.; et al. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med 2006, 355, 1572–1582. [Google Scholar] [CrossRef] [PubMed]
- Turcotte, L.M.; Liu, Q.; Yasui, Y.; Arnold, M.A.; Hammond, S.; Howell, R.M.; Smith, S.A.; Weathers, R.E.; Henderson, T.O.; Gibson, T.M.; et al. Temporal Trends in Treatment and Subsequent Neoplasm Risk Among 5-Year Survivors of Childhood Cancer, 1970-2015. JAMA 2017, 317, 814–824. [Google Scholar] [CrossRef] [PubMed]
- Tichelli, A.; Bhatia, S.; Socié, G. Cardiac and cardiovascular consequences after haematopoietic stem cell transplantation. British journal of haematology 2008, 142, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Brice, P.; de Kerviler, E.; Friedberg, J.W. Classical Hodgkin lymphoma. Lancet 2021, 398, 1518–1527. [Google Scholar] [CrossRef] [PubMed]
- Maraldo, M.V.; Giusti, F.; Vogelius, I.R.; Lundemann, M.; van der Kaaij, M.A.; Ramadan, S.; Meulemans, B.; Henry-Amar, M.; Aleman, B.M.; Raemaekers, J.; et al. Cardiovascular disease after treatment for Hodgkin's lymphoma: an analysis of nine collaborative EORTC-LYSA trials. Lancet Haematol 2015, 2, e492–502. [Google Scholar] [CrossRef] [PubMed]
- Bergom, C.; Bradley, J.A.; Ng, A.K.; Samson, P.; Robinson, C.; Lopez-Mattei, J.; Mitchell, J.D. Past, Present, and Future of Radiation-Induced Cardiotoxicity: Refinements in Targeting, Surveillance, and Risk Stratification. JACC CardioOncol 2021, 3, 343–359. [Google Scholar] [CrossRef]
- Lefrak, E.A.; Pitha, J.; Rosenheim, S.; Gottlieb, J.A. A clinicopathologic analysis of adriamycin cardiotoxicity. Cancer 1973, 32, 302–314. [Google Scholar] [CrossRef] [PubMed]
- Billingham, M.E.; Bristow, M.R.; Glatstein, E.; Mason, J.W.; Masek, M.A.; Daniels, J.R. Adriamycin cardiotoxicity: endomyocardial biopsy evidence of enhancement by irradiation. Am J Surg Pathol 1977, 1, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Ulmer, H.E.; Ludwig, R.; Geiger, H. Assessment of adriamycin cardiotoxicity in children by systolic time intervals. Eur J Pediatr 1979, 131, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Markiewicz, W.; Robinson, E.; Peled, B.; Kaufman, S.; Carter, A. Early detection of doxorubicin cardiotoxicity by M-mode echocardiography. Cancer Chemother Pharmacol 1980, 5, 119–125. [Google Scholar] [CrossRef]
- Ritchie, J.L.; Singer, J.W.; Thorning, D.; Sorensen, S.G.; Hamilton, G.W. Anthracycline cardiotoxicity: clinical and pathologic outcomes assessed by radionuclide ejection fraction. Cancer 1980, 46, 1109–1116. [Google Scholar] [CrossRef] [PubMed]
- Lahtinen, R.; Uusitupa, M.; Kuikka, J.; Länsimies, E. Non-invasive evaluation of anthracycline-induced cardiotoxicity in man. Acta Med Scand 1982, 212, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Lewis, A.B.; Crouse, V.L.; Evans, W.; Takahashi, M.; Siegel, S.E. Recovery of left ventricular function following discontinuation of anthracycline chemotherapy in children. Pediatrics 1981, 68, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Agarwala, S.; Kumar, R.; Bhatnagar, V.; Bajpai, M.; Gupta, D.K.; Mitra, D.K. High incidence of adriamycin cardiotoxicity in children even at low cumulative doses: role of radionuclide cardiac angiography. J Pediatr Surg 2000, 35, 1786–1789. [Google Scholar] [CrossRef] [PubMed]
- Leerink, J.M.; van der Pal, H.J.H.; Kremer, L.C.M.; Feijen, E.A.M.; Meregalli, P.G.; Pourier, M.S.; Merkx, R.; Bellersen, L.; van Dalen, E.C.; Loonen, J.; et al. Refining the 10-Year Prediction of Left Ventricular Systolic Dysfunction in Long-Term Survivors of Childhood Cancer. JACC CardioOncol 2021, 3, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Shulkin, B.L.; Mitchell, D.S.; Ungar, D.R.; Prakash, D.; Dole, M.G.; Castle, V.P.; Hernandez, R.J.; Koeppe, R.A.; Hutchinson, R.J. Neoplasms in a pediatric population: 2-[F-18]-fluoro-2-deoxy-D-glucose PET studies. Radiology 1995, 194, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Jadvar, H.; Connolly, L.P.; Fahey, F.H.; Shulkin, B.L. PET and PET/CT in pediatric oncology. Semin Nucl Med 2007, 37, 316–331. [Google Scholar] [CrossRef] [PubMed]
- Vince, D.J. Medical radiation to children with congenital heart disease. Can Med Assoc J 1964, 91, 1345–1349. [Google Scholar] [PubMed]
- Darby, S.C.; Cutter, D.J.; Boerma, M.; Constine, L.S.; Fajardo, L.F.; Kodama, K.; Mabuchi, K.; Marks, L.B.; Mettler, F.A.; Pierce, L.J.; et al. Radiation-related heart disease: current knowledge and future prospects. Int J Radiat Oncol Biol Phys 2010, 76, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Marks, L.B.; Yu, X.; Prosnitz, R.G.; Zhou, S.M.; Hardenbergh, P.H.; Blazing, M.; Hollis, D.; Lind, P.; Tisch, A.; Wong, T.Z.; Borges-Neto, S. The incidence and functional consequences of RT-associated cardiac perfusion defects. Int J Radiat Oncol Biol Phys 2005, 63, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Boerma, M.; Hauer-Jensen, M. Preclinical research into basic mechanisms of radiation-induced heart disease. Cardiol Res Pract 2010, 2011. [Google Scholar] [CrossRef] [PubMed]
- Yang, E.H.; Marmagkiolis, K.; Balanescu, D.V.; Hakeem, A.; Donisan, T.; Finch, W.; Virmani, R.; Herrman, J.; Cilingiroglu, M.; Grines, C.L.; et al. Radiation-Induced Vascular Disease-A State-of-the-Art Review. Front Cardiovasc Med 2021, 8, 652761. [Google Scholar] [CrossRef] [PubMed]
- Tapio, S. Pathology and biology of radiation-induced cardiac disease. J Radiat Res 2016, 57, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Azimzadeh, O.; Subramanian, V.; Sievert, W.; Merl-Pham, J.; Oleksenko, K.; Rosemann, M.; Multhoff, G.; Atkinson, M.J.; Tapio, S. Activation of PPARα by Fenofibrate Attenuates the Effect of Local Heart High Dose Irradiation on the Mouse Cardiac Proteome. Biomedicines 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Turunen, M.; Peters, J.M.; Gonzalez, F.J.; Schedin, S.; Dallner, G. Influence of peroxisome proliferator-activated receptor alpha on ubiquinone biosynthesis. J Mol Biol 2000, 297, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Djujic, I.S.; Jozanov-Stankov, O.; Mandic, M.; Demajo, M.; Vrvic, M.M. Selenium content and distribution in rat tissues irradiated with gamma rays. Biological trace element research 1992, 33, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Knapp, F.F., Jr.; Goodman, M.M.; Callahan, A.P.; Kirsch, G. Radioiodinated 15-(p-iodophenyl)-3,3-dimethylpentadecanoic acid: a useful new agent to evaluate myocardial fatty acid uptake. J Nucl Med 1986, 27, 521–531. [Google Scholar] [PubMed]
- Ogata, M. [Myocardial uptake of 125I-BMIPP in rats treated with adriamycin]. Kaku Igaku 1989, 26, 69–76. [Google Scholar] [PubMed]
- Wakasugi, S.; Fischman, A.J.; Babich, J.W.; Callahan, R.J.; Elmaleh, D.R.; Wilkinson, R.; Strauss, H.W. Myocardial substrate utilization and left ventricular function in adriamycin cardiomyopathy. J Nucl Med 1993, 34, 1529–1535. [Google Scholar] [PubMed]
- Niitsu, N.; Yamazaki, J.; Umeda, M. [Clinical usefulness of 123I-BMIPP (beta-methyl iodophenyl pentadecanoic (acid) myocardial SPECT in patients with hematological malignancies with adriamycin-induced cardiomyopathy]. Gan To Kagaku Ryoho 1996, 23, 1793–1797. [Google Scholar] [PubMed]
- Piwnica-Worms, D.; Chiu, M.L.; Kronauge, J.F. Detection of adriamycin-induced cardiotoxicity in cultured heart cells with technetium 99m-SESTAMIBI. Cancer Chemother Pharmacol 1993, 32, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Takemura, G.; Fujiwara, H. Doxorubicin-induced cardiomyopathy from the cardiotoxic mechanisms to management. Prog Cardiovasc Dis 2007, 49, 330–352. [Google Scholar] [CrossRef]
- Inubushi, M.; Tadamura, E.; Kudoh, T.; Hattori, M.; Kubo, S.; Koshiji, T.; Nishimura, K.; Komeda, M.; Tamaki, N.; Konishi, J. Simultaneous assessment of myocardial free fatty acid utilization and left ventricular function using 123I-BMIPP-gated SPECT. J Nucl Med 1999, 40, 1840–1847. [Google Scholar] [PubMed]
- Saito, K.; Takeda, K.; Okamoto, S.; Okamoto, R.; Makino, K.; Tameda, Y.; Nomura, Y.; Maeda, H.; Ichihara, T.; Nakano, T. Detection of doxorubicin cardiotoxicity by using iodine-123 BMIPP early dynamic SPECT: quantitative evaluation of early abnormality of fatty acid metabolism with the Rutland method. J Nucl Cardiol 2000, 7, 553–561. [Google Scholar] [CrossRef]
- Saito, K.; Takeda, K.; Imanaka-Yoshida, K.; Imai, H.; Sekine, T.; Kamikura, Y. Assessment of fatty acid metabolism in taxan-induced myocardial damage with iodine-123 BMIPP SPECT: comparative study with myocardial perfusion, left ventricular function, and histopathological findings. Ann Nucl Med 2003, 17, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Sarocchi, M.; Bauckneht, M.; Arboscello, E.; Capitanio, S.; Marini, C.; Morbelli, S.; Miglino, M.; Congiu, A.G.; Ghigliotti, G.; Balbi, M.; et al. An increase in myocardial 18-fluorodeoxyglucose uptake is associated with left ventricular ejection fraction decline in Hodgkin lymphoma patients treated with anthracycline. J Transl Med 2018, 16, 295. [Google Scholar] [CrossRef] [PubMed]
- Bauckneht, M.; Pastorino, F.; Castellani, P.; Cossu, V.; Orengo, A.M.; Piccioli, P.; Emionite, L.; Capitanio, S.; Yosifov, N.; Bruno, S.; et al. Increased myocardial 18F-FDG uptake as a marker of Doxorubicin-induced oxidative stress. J Nucl Cardiol 2019, 27, 2183–2194. [Google Scholar] [CrossRef]
- Umezawa, R.; Takase, K.; Jingu, K.; Takanami, K.; Ota, H.; Kaneta, T.; Takeda, K.; Matsushita, H.; Ariga, H.; Takahashi, S.; Yamada, S. Evaluation of radiation-induced myocardial damage using iodine-123 β-methyl-iodophenyl pentadecanoic acid scintigraphy. J Radiat Res 2013, 54, 880–889. [Google Scholar] [CrossRef] [PubMed]
- Jingu, K.; Nemoto, K.; Kaneta, T.; Takai, Y.; Ichinose, A.; Ogawa, Y.; Yamada, S. [A case of high FDG-uptake into the myocardium after radiotherapy for esophageal cancer]. Nihon Igaku Hoshasen Gakkai Zasshi 2005, 65, 266–269. [Google Scholar] [PubMed]
- Jingu, K.; Nemoto, K.; Kaneta, T.; Oikawa, M.; Ogawa, Y.; Ariga, H.; Takeda, K.; Sakayauchi, T.; Fujimoto, K.; Narazaki, K.; et al. Temporal change in brain natriuretic Peptide after radiotherapy for thoracic esophageal cancer. Int J Radiat Oncol Biol Phys 2007, 69, 1417–1423. [Google Scholar] [CrossRef] [PubMed]
- Yan, R.; Song, J.; Wu, Z.; Guo, M.; Liu, J.; Li, J.; Hao, X.; Li, S. Detection of Myocardial Metabolic Abnormalities by 18F-FDG PET/CT and Corresponding Pathological Changes in Beagles with Local Heart Irradiation. Korean J Radiol 2015, 16, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Hayashi, D.; Yamazaki, T.; Mizuno, T.; Kanda, Y.; Komuro, I.; Kurabayashi, M.; Yamaoki, K.; Mitani, K.; Hirai, H.; et al. Elevated B-type natriuretic peptide levels after anthracycline administration. Am Heart J 1998, 136, 362–363. [Google Scholar] [CrossRef] [PubMed]
- Sandri, M.T.; Salvatici, M.; Cardinale, D.; Zorzino, L.; Passerini, R.; Lentati, P.; Leon, M.; Civelli, M.; Martinelli, G.; Cipolla, C.M. N-terminal pro-B-type natriuretic peptide after high-dose chemotherapy: a marker predictive of cardiac dysfunction? Clinical chemistry 2005, 51, 1405–1410. [Google Scholar] [CrossRef] [PubMed]
- Zaucha-Prażmo, A.; Sadurska, E.; Drabko, K.; Kowalczyk, J.R. Can we find a good biochemical marker of early cardiotoxicity in children treated with haematopoietic stem cell transplantation? Contemp Oncol (Pozn) 2016, 20, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Kuittinen, T.; Jantunen, E.; Vanninen, E.; Mussalo, H.; Vuolteenaho, O.; Ala-Kopsala, M.; Nousiainen, T.; Hartikainen, J. Cardiac effects within 3 months of BEAC high-dose therapy in non-Hodgkin's lymphoma patients undergoing autologous stem cell transplantation. European journal of haematology 2006, 77, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Upadhya, B.; Hegde, S.; Tannu, M.; Stacey, R.B.; Kalogeropoulos, A.; Schocken, D.D. Preventing new-onset heart failure: Intervening at stage A. Am J Prev Cardiol 2023, 16, 100609. [Google Scholar] [CrossRef] [PubMed]
- Kouloubinis, A.; Sofroniadou, S.; Panoulas, V.F.; Makaritsis, K.; Revela, I.; Karavolias, G.; Voudris, V.; Adamopoulos, S. The role of TNF-α, Fas/Fas ligand system and NT-proBNP in the early detection of asymptomatic left ventricular dysfunction in cancer patients treated with anthracyclines. Int J Cardiol Heart Vasc 2015, 6, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, L.; Hesham, D.; Abdel Hamid, M.; Youssef, G. The combined role of NT-proBNP and LV-GLS in the detection of early subtle chemotherapy-induced cardiotoxicity in breast cancer female patients. Egypt Heart J 2021, 73, 20. [Google Scholar] [CrossRef] [PubMed]
- Borde, C.; Kand, P.; Basu, S. Enhanced myocardial fluorodeoxyglucose uptake following Adriamycin-based therapy: Evidence of early chemotherapeutic cardiotoxicity? World J Radiol 2012, 4, 220–223. [Google Scholar] [CrossRef] [PubMed]
- Montravers, F.; McNamara, D.; Landman-Parker, J.; Grahek, D.; Kerrou, K.; Younsi, N.; Wioland, M.; Leverger, G.; Talbot, J.N. [18F]FDG in childhood lymphoma: clinical utility and impact on management. Eur J Nucl Med Mol Imaging 2002, 29, 1155–1165. [Google Scholar] [CrossRef] [PubMed]
- Kaste, S.C.; Howard, S.C.; McCarville, E.B.; Krasin, M.J.; Kogos, P.G.; Hudson, M.M. 18F-FDG-avid sites mimicking active disease in pediatric Hodgkin's. Pediatr Radiol 2005, 35, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.; Metser, U.; Avrahami, G.; Dvir, R.; Valdman, D.; Sira, L.B.; Sayar, D.; Burstein, Y.; Toren, A.; Yaniv, I.; Even-Sapir, E. Role of 18F-FDG PET/CT in staging and follow-up of lymphoma in pediatric and young adult patients. J Comput Assist Tomogr 2006, 30, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Jingu, K.; Kaneta, T.; Nemoto, K.; Ichinose, A.; Oikawa, M.; Takai, Y.; Ogawa, Y.; Nakata, E.; Sakayauchi, T.; Takai, K.; et al. The utility of 18F-fluorodeoxyglucose positron emission tomography for early diagnosis of radiation-induced myocardial damage. Int J Radiat Oncol Biol Phys 2006, 66, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Gorla, A.K.; Sood, A.; Prakash, G.; Parmar, M.; Mittal, B.R. Substantial Increase in Myocardial FDG Uptake on Interim PET/CT May Be an Early Sign of Adriamycin-Induced Cardiotoxicity. Clin Nucl Med 2016, 41, 462–463. [Google Scholar] [CrossRef] [PubMed]
- Bauckneht, M. Doxorubicin effect on myocardial metabolism: a translational 18F-FDG PET/CT approach. 2020. [Google Scholar] [CrossRef]
- Bauckneht, M.; Ferrarazzo, G.; Fiz, F.; Morbelli, S.; Sarocchi, M.; Pastorino, F.; Ghidella, A.; Pomposelli, E.; Miglino, M.; Ameri, P.; et al. Doxorubicin Effect on Myocardial Metabolism as a Prerequisite for Subsequent Development of Cardiac Toxicity: A Translational 18F-FDG PET/CT Observation. J Nucl Med 2017, 58, 1638–1645. [Google Scholar] [CrossRef] [PubMed]
- Bauckneht, M.; Cossu, V.; Miceli, A.; Donegani, M.; Capitanio, S.; Morbelli, S.; Marini, C.; Sambuceti, G. FDG-PET Imaging of Doxorubicin-Induced Cardiotoxicity: a New Window on an Old Problem. Current Cardiovascular Imaging Reports 2019, 12. [Google Scholar] [CrossRef]
- Haider, A.; Bengs, S.; Schade, K.; Wijnen, W.J.; Portmann, A.; Etter, D.; Fröhlich, S.; Warnock, G.I.; Treyer, V.; Burger, I.A.; et al. Myocardial 18F-FDG Uptake Pattern for Cardiovascular Risk Stratification in Patients Undergoing Oncologic PET/CT. J Clin Med 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Gherghe, M.; Lazar, A.M.; Mutuleanu, M.D.; Bordea, C.I.; Ionescu, S.; Mihaila, R.I.; Petroiu, C.; Stanciu, A.E. Evaluating Cardiotoxicity in Breast Cancer Patients Treated with HER2 Inhibitors: Could a Combination of Radionuclide Ventriculography and Cardiac Biomarkers Predict the Cardiac Impact? Cancers (Basel) 2022, 15. [Google Scholar] [CrossRef] [PubMed]
- Dourado, M.L.C.; Dompieri, L.T.; Leitao, G.M.; Mourato, F.A.; Santos, R.G.G.; Almeida Filho, P.J.; Markman Filho, B.; Melo, M.D.T.; Brandao, S.C.S. Aumento de Captação Cardíaca de 18F-FDG Induzida por Quimioterapia em Pacientes com Linfoma: Um Marcador Precoce de Cardiotoxicidade? Arq Bras Cardiol 2022, 118, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, C.T.; Rezende, M.F. Medicina de Precisão: A Tomografia por Emissão de Pósitrons com 18F-FDG pode Identificar Fenótipos de Cardiotoxicidade? Arq Bras Cardiol 2022, 119, 109–110. [Google Scholar] [CrossRef]
- Cadour, F.; Thuny, F.; Sourdon, J. New Insights in Early Detection of Anticancer Drug-Related Cardiotoxicity Using Perfusion and Metabolic Imaging. Front Cardiovasc Med 2022, 9, 813883. [Google Scholar] [CrossRef] [PubMed]
- Cannizzaro, M.T.; Inserra, M.C.; Passaniti, G.; Celona, A.; D'Angelo, T.; Romeo, P.; Basile, A. Role of advanced cardiovascular imaging in chemotherapy-induced cardiotoxicity. Heliyon 2023, 9, e15226. [Google Scholar] [CrossRef] [PubMed]
- Becker, M.M.C.; Arruda, G.F.A.; Berenguer, D.R.F.; Buril, R.O.; Cardinale, D.; Brandão, S.C.S. Anthracycline cardiotoxicity: current methods of diagnosis and possible role of (18)F-FDG PET/CT as a new biomarker. Cardiooncology 2023, 9, 17. [Google Scholar] [CrossRef] [PubMed]
- Moncayo, R.; Moncayo, H. Proof of concept of the WOMED model of benign thyroid disease: Restitution of thyroid morphology after correction of physical and psychological stressors and magnesium supplementation. BBA Clin 2015, 3, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Moncayo, R.; Moncayo, H. Applying a systems approach to thyroid physiology: looking at the whole with a mitochondrial perspective instead of just TSH values or why we should know more about mitochondria to understand metabolism. BBA Clin 2017, 7, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Moncayo, R.; Moncayo, H. Translating results from the WOMED model of benign thyroid disease to a practical approach to treat fatigue in COVID-19 patients based on combined supplementation with magnesium, selenium, and coenzyme Q10: a treatment strategy against fatigue. Cardiol Vasc Res 2020, 4, 1–4. Available online: https://scivisionpub.com/abstract-display.php?id=1443.
- Moncayo, R.; Moncayo, H.; Reisenzahn, J. Global view on the pathogenesis of benign thyroid disease based on historical, experimental, biochemical, and genetic data identifying the role of magnesium, selenium, coenzyme Q10 and iron in the context of the unfolded protein response and protein quality control of thyroglobulin. J Transl Genet Genom 2020, 4, 356–383. [Google Scholar] [CrossRef]
- Moncayo, R.; Moncayo, H. Practical Guidelines for Diagnosing and Treating Thyroid Disease Based on the WOMED Metabolic Model of Disease Focusing on Glycolysis and Coenzyme Q10 Deficiency—A Clinical Alternative to the 2021 Retired Clinical Practice Guidelines of the Endocrine Society. Diagnostics 2022, 12, 107. [Google Scholar] [CrossRef] [PubMed]
- Liparulo, I.; Bergamini, C.; Bortolus, M.; Calonghi, N.; Gasparre, G.; Kurelac, I.; Masin, L.; Rizzardi, N.; Rugolo, M.; Wang, W.; et al. Coenzyme Q biosynthesis inhibition induces HIF-1α stabilization and metabolic switch toward glycolysis. FEBS J 2021, 288, 1956–1974. [Google Scholar] [CrossRef] [PubMed]
- Moncayo, R.; Moncayo, H. From the thyroid to the heart. Global Journal of Medical Research 2023, 23, 1–36. [Google Scholar] [CrossRef]
- Davis, L.E.; Brown, C.E. Peripartum heart failure in a patient treated previously with doxorubicin. Obstet Gynecol 1988, 71, 506–508. [Google Scholar]
- Kyvernitakis, A.; Kyvernitakis, I.; Yang, A.; Albert, U.-S.; Schmidt, S.; Arabin, B. Can peripartum cardiomyopathy be caused by chemotherapy and radiation of breast cancer? Case Reports in Perinatal Medicine 2013, 2, 29–32. [Google Scholar] [CrossRef]
- Colović, N.; Seferović, P.; Plećić, M.; Vidović, A.; Suvajdzić, N.; Tomin, D. Peripartum cardiomyopathy in a patient treated for acute myeloid leukemia. Srp Arh Celok Lek 2016, 144, 77–80. [Google Scholar] [CrossRef]
- Chait-Rubinek, L.; Mariani, J.A.; Goroncy, N.; Herschtal, A.; Wheeler, G.C.; Dwyer, M.K.; Seymour, J.F.; Campbell, B.A. A Retrospective Evaluation of Risk of Peripartum Cardiac Dysfunction in Survivors of Childhood, Adolescent and Young Adult Malignancies. Cancers (Basel) 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Cowgill, J.A.; Francis, S.A.; Sawyer, D.B. Anthracycline and Peripartum Cardiomyopathies. Circulation research 2019, 124, 1633–1646. [Google Scholar] [CrossRef]
- Ritchie, C. Clinical Contributions to the Pathology, Diagnosis, and Treatment of Certain Chronic Diseases of the Heart. Edinb Med Surg J 1849, 72, 325–339. [Google Scholar] [PubMed]
- Porak, C. De l’influence reciproque de la grossesse et del maladies du Coeur [thesis]. Medical Faculty of Paris, France 1880. [Google Scholar]
- Gouley, B.A.; Mcmillan, T.M.; Bellet, S. Idiopathic myocardial degeneration associated with pregnancy and especially the puerperium. Am J Med Sci 1937, 19, 185–199. [Google Scholar] [CrossRef]
- Hull, E.; Hafkesbring, E. Toxic postpartal heart disease. New Orleans Med Surg J 1937, 89, 550–557. [Google Scholar]
- Hull, E.; Hidden, E. Postpartal heart failure. Southern Medical Journal 1938, 31, 265–270. [Google Scholar] [CrossRef]
- Demakis, J.G.; Rahimtoola, S.H. Peripartum cardiomyopathy. Circulation 1971, 44, 964–968. [Google Scholar] [CrossRef] [PubMed]
- Davidson, N.M.; Trevitt, L.; Parry, E.H. Perpartum cardiac failure. An explanation for the observed geographic distribution in Nigeria. Bull World Health Organ 1974, 51, 203–208. [Google Scholar] [PubMed]
- Ezem, B.U.; Otubu, J.A. A complication of a traditional puerperal practice in Nigeria. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics 1980, 18, 383–384. [Google Scholar] [CrossRef] [PubMed]
- Jha, N.; Jha, A.K. Peripartum cardiomyopathy. Heart Fail Rev 2021, 26, 781–797. [Google Scholar] [CrossRef] [PubMed]
- Cénac, A.; Simonoff, M.; Moretto, P.; Djibo, A. A low plasma selenium is a risk factor for peripartum cardiomyopathy. A comparative study in Sahelian Africa. Int J Cardiol 1992, 36, 57–59. [Google Scholar] [CrossRef] [PubMed]
- Cénac, A.; Djibo, A.; Djangnikpo, L. [Peripartum dilated cardiomyopathy. A model of multifactor disease?]. Rev Med Interne 1993, 14, 1033. [Google Scholar] [CrossRef] [PubMed]
- Cénac, A.; Simonoff, M.; Djibo, A. Nutritional status and plasma trace elements in peripartum cardiomyopathy. A comparative study in Niger. J Cardiovasc Risk 1996, 3, 483–487. [Google Scholar] [CrossRef] [PubMed]
- Cénac, A.; Sparfel, A.; Amiel-Lebigre, F.; Cleuziou, A.; Pennec, Y.; Le Goff, P.; Mottier, D. [Effect of stressful life events on clinical development of temporal arteritis and/or polymyalgia rheumatica]. Presse Med 2002, 31, 873–879. [Google Scholar] [PubMed]
- Cénac, A.; Touré, K.; Diarra, M.B.; Sergeant, C.; Jobic, Y.; Sanogo, K.; Dembele, M.; Fayol, V.; Simonoff, M. [Plasma selenium and peripartum cardiomyopathy in Bamako, Mali]. Med Trop (Mars) 2004, 64, 151–154. [Google Scholar] [PubMed]
- Karaye, K.M.; Yahaya, I.A.; Lindmark, K.; Henein, M.Y. Serum selenium and ceruloplasmin in nigerians with peripartum cardiomyopathy. International journal of molecular sciences 2015, 16, 7644–7654. [Google Scholar] [CrossRef]
- Vadhanavikit, S.; Ganther, H.E. Decreased ubiquinone levels in tissues of rats deficient in selenium. Biochem Biophys Res Commun 1993, 190, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Vadhanavikit, S.; Ganther, H.E. Selenium deficiency and decreased coenzyme Q levels. Molecular aspects of medicine 1994, 15 Suppl, s103–107. [Google Scholar] [CrossRef]
- Thet Thet, L.; Takeda, T.; Wu, J.; Fumikura, Y.; Iida, K.; Yamaguchi, I.; Itai, Y. Diffuse and marked breast uptake of both 123I-BMIPP and 99mTc-TF by myocardial scintigraphy. Ann Nucl Med 2000, 14, 315–318. [Google Scholar] [CrossRef]
- Ohtsuki, K.; Sugihara, H.; Umamoto, I.; Nakamura, T.; Nakagawa, T.; Nakagawa, M. Clinical evaluation of hypertrophic cardiomyopathy by myocardial scintigraphy using 123I-labelled 15-(p-iodophenyl)-3-R, S-methylpentadecanoic acid (123I-BMIPP). Nuclear medicine communications 1994, 15, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Yamada, H.; Oki, T.; Yamamoto, T.; Tanaka, H.; Tabata, T.; Wakatsuki, T.; Nomura, M.; Ito, S.; Thomas, J.D. Potential application of tissue Doppler imaging to assess regional left ventricular diastolic function in patients with hypertrophic cardiomyopathy: comparison with 123I-beta-methyl iodophenyl pentadecanoic acid myocardial scintigraphy. Clin Cardiol 2004, 27, 33–39. [Google Scholar] [CrossRef]
- Bello, N.; Rendon, I.S.H.; Arany, Z. The relationship between pre-eclampsia and peripartum cardiomyopathy: a systematic review and meta-analysis. J Am Coll Cardiol 2013, 62, 1715–1723. [Google Scholar] [CrossRef] [PubMed]
- Ersbøll, A.S.; Bojer, A.S.; Hauge, M.G.; Johansen, M.; Damm, P.; Gustafsson, F.; Vejlstrup, N.G. Long-Term Cardiac Function After Peripartum Cardiomyopathy and Preeclampsia: A Danish Nationwide, Clinical Follow-Up Study Using Maximal Exercise Testing and Cardiac Magnetic Resonance Imaging. Journal of the American Heart Association 2018, 7, e008991. [Google Scholar] [CrossRef] [PubMed]
- Masoomi, R.; Shah, Z.; Arany, Z.; Gupta, K. Peripartum cardiomyopathy: An epidemiologic study of early and late presentations. Pregnancy Hypertens 2018, 13, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Lindley, K.J. Heart Failure and Pregnancy: Thinking Beyond Peripartum Cardiomyopathy. J Card Fail 2021, 27, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.; Stout, M.J.; Rosenbloom, J.I.; Olsen, M.A.; Joynt Maddox, K.E.; Deych, E.; Davila-Roman, V.G.; Lindley, K.J. Preeclampsia Predicts Risk of Hospitalization for Heart Failure With Preserved Ejection Fraction. J Am Coll Cardiol 2021, 78, 2281–2290. [Google Scholar] [CrossRef]
- Rajapreyar, I.; Sinkey, R.; Pamboukian, S.V.; Tita, A. Did a shared thioredoxin-reductase gene mutation lead to maternal peripartum cardiomyopathy and fatal dilated cardiomyopathy in her son? A case report. Case Rep Womens Health 2020, 26, e00196. [Google Scholar] [CrossRef] [PubMed]
- Mustacich, D.; Powis, G. Thioredoxin reductase. The Biochemical journal 2000, 346 Pt 1, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Arbogast, S.; Ferreiro, A. Selenoproteins and protection against oxidative stress: selenoprotein N as a novel player at the crossroads of redox signaling and calcium homeostasis. Antioxidants & redox signaling 2010, 12, 893–904. [Google Scholar] [CrossRef]
- Bomer, N.; Grote Beverborg, N.; Hoes, M.F.; Streng, K.W.; Vermeer, M.; Dokter, M.M.; J, I.J.; Anker, S.D.; Cleland, J.G.F.; Hillege, H.L.; et al. Selenium and outcome in heart failure. Eur J Heart Fail 2019. [Google Scholar] [CrossRef] [PubMed]
- Narita, M.; Kurihara, T. Is I-123-beta-methyl-p-iodophenyl-methylpentadecanoic acid imaging useful to evaluate asymptomatic patients with hypertrophic cardiomyopathy? I-123 BMIPP imaging to evaluate asymptomatic hypertrophic cardiomyopathy. Int J Cardiovasc Imaging 2003, 19, 499–510. [Google Scholar] [CrossRef] [PubMed]
- Teran, E.; Racines-Orbe, M.; Vivero, S.; Escudero, C.; Molina, G.; Calle, A. Preeclampsia is associated with a decrease in plasma coenzyme Q10 levels. Free Radic Biol Med 2003, 35, 1453–1456. [Google Scholar] [CrossRef] [PubMed]
- Teran, E.; Chedraui, P.; Racines-Orbe, M.; Vivero, S.; Villena, F.; Duchicela, F.; Nacevilla, L.; Schwager, G.; Calle, A. Coenzyme Q10 levels in women with preeclampsia living at different altitudes. Biofactors 2008, 32, 185–190. [Google Scholar] [CrossRef]
- Teran, E.; Hernández, I.; Tana, L.; Teran, S.; Galaviz-Hernandez, C.; Sosa-Macías, M.; Molina, G.; Calle, A. Mitochondria and Coenzyme Q10 in the Pathogenesis of Preeclampsia. Front Physiol 2018, 9, 1561. [Google Scholar] [CrossRef] [PubMed]
- Marchi, S.; Patergnani, S.; Pinton, P. The endoplasmic reticulum-mitochondria connection: one touch, multiple functions. Biochim Biophys Acta 2014, 1837, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Pobezhimova, T.; Voinikov, V.; Varakina, N. Inactivation of complex I of the respiratory chain of maize mitochondria incubated in vitro by elevated temperature. Journal of Thermal Biology 1996, 21, 283–288. [Google Scholar] [CrossRef]
- Ludwig, P.; Bartels, M.; Schewe, T.; Rapoport, S. Selective inactivation of the NADH-ubiquinone segment of the respiratory chain of submitochondrial particles by endogenous free fatty acids during hyperthermia. FEBS Lett 1978, 95, 181–184. [Google Scholar] [CrossRef]
- Kommuru, T.R.; Ashraf, M.; Khan, M.A.; Reddy, I.K. Stability and bioequivalence studies of two marketed formulations of coenzyme Q10 in beagle dogs. Chem Pharm Bull (Tokyo) 1999, 47, 1024–1028. [Google Scholar] [CrossRef] [PubMed]
- Ide, T.; Tsutsui, H.; Kinugawa, S.; Utsumi, H.; Kang, D.; Hattori, N.; Uchida, K.; Arimura, K.; Egashira, K.; Takeshita, A. Mitochondrial electron transport complex I is a potential source of oxygen free radicals in the failing myocardium. Circulation research 1999, 85, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Zozina, V.I.; Covantev, S.; Goroshko, O.A.; Krasnykh, L.M.; Kukes, V.G. Coenzyme Q10 in Cardiovascular and Metabolic Diseases: Current State of the Problem. Curr Cardiol Rev 2018, 14, 164–174. [Google Scholar] [CrossRef] [PubMed]
- Seneş, M.; Erbay, A.R.; Yilmaz, F.M.; Topkaya, B.C.; Zengi, O.; Doğan, M.; Yücel, D. Coenzyme Q10 and high-sensitivity C-reactive protein in ischemic and idiopathic dilated cardiomyopathy. Clin Chem Lab Med 2008, 46, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Ranek, M.J.; Stachowski, M.J.; Kirk, J.A.; Willis, M.S. The role of heat shock proteins and co-chaperones in heart failure. Philos Trans R Soc Lond B Biol Sci 2018, 373. [Google Scholar] [CrossRef] [PubMed]
- Iguchi, M.; Littmann, A.E.; Chang, S.H.; Wester, L.A.; Knipper, J.S.; Shields, R.K. Heat stress and cardiovascular, hormonal, and heat shock proteins in humans. J Athl Train 2012, 47, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Burk, A.; Timpmann, S.; Kreegipuu, K.; Tamm, M.; Unt, E.; Ööpik, V. Effects of heat acclimation on endurance capacity and prolactin response to exercise in the heat. European journal of applied physiology 2012, 112, 4091–4101. [Google Scholar] [CrossRef] [PubMed]
- Stendig-Lindberg, G.; Moran, D.; Shapiro, Y. How significant is magnesium in thermoregulation? Journal of basic and clinical physiology and pharmacology 1998, 9, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.C.; Chien, W.C.; Chu, P.; Chung, C.H.; Lin, C.Y.; Tsai, S.H. The association between heat stroke and subsequent cardiovascular diseases. PLoS One 2019, 14, e0211386. [Google Scholar] [CrossRef] [PubMed]
- Nzvere, F.P.; Tariq, E.; Nishanth, K.; Arshid, A.; Cancarevic, I. Long-Term Cardiovascular Diseases of Heatstroke: A Delayed Pathophysiology Outcome. Cureus 2020, 12, e9595. [Google Scholar] [CrossRef] [PubMed]
- Dawson, D.W.; Pearce, S.F.; Zhong, R.; Silverstein, R.L.; Frazier, W.A.; Bouck, N.P. CD36 mediates the In vitro inhibitory effects of thrombospondin-1 on endothelial cells. J Cell Biol 1997, 138, 707–717. [Google Scholar] [CrossRef] [PubMed]
- Rac, M.; Kurzawski, G.; Safranow, K.; Rac, M.; Sagasz-Tysiewicz, D.; Krzystolik, A.; Poncyljusz, W.; Olszewska, M.; Dawid, G.; Chlubek, D. Association of CD36 gene polymorphisms with echo- and electrocardiographic parameters in patients with early onset coronary artery disease. Arch Med Sci 2013, 9, 640–650. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.M.; Kazantzis, M.; Wang, J.; Venkatraman, S.; Goncalves, R.L.; Quinlan, C.L.; Ng, R.; Jastroch, M.; Benjamin, D.I.; Nie, B.; et al. Dependence of brown adipose tissue function on CD36-mediated coenzyme Q uptake. Cell Rep 2015, 10, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Son, N.H.; Basu, D.; Samovski, D.; Pietka, T.A.; Peche, V.S.; Willecke, F.; Fang, X.; Yu, S.Q.; Scerbo, D.; Chang, H.R.; et al. Endothelial cell CD36 optimizes tissue fatty acid uptake. J Clin Invest 2018, 128, 4329–4342. [Google Scholar] [CrossRef] [PubMed]
- Daquinag, A.C.; Gao, Z.; Fussell, C.; Immaraj, L.; Pasqualini, R.; Arap, W.; Akimzhanov, A.M.; Febbraio, M.; Kolonin, M.G. Fatty acid mobilization from adipose tissue is mediated by CD36 posttranslational modifications and intracellular trafficking. JCI Insight 2021, 6. [Google Scholar] [CrossRef] [PubMed]
- Shu, H.; Peng, Y.; Hang, W.; Nie, J.; Zhou, N.; Wang, D.W. The role of CD36 in cardiovascular disease. Cardiovasc Res 2022, 118, 115–129. [Google Scholar] [CrossRef]
- Ahlbom, H. Castration by Roentgen Rays as An Auxiliary Treatment in the Radiotherapy of Cancer Mammae at Radiumhemmet, Stockholm. Acta Radiologica 1930, 11, 614–635. [Google Scholar] [CrossRef]
- Peck, W.S.; McGreer, J.T.; Kretzschmar, N.R.; Brown, W.E. Castration of the Female by Irradiation. Radiology 1940, 34, 176–186. [Google Scholar] [CrossRef]
- Brinkley, D.; Haybittle, J.L.; Murrell, D.S. The X-ray menopause in 267 cases. J Obstet Gynaecol Br Commonw 1963, 70, 1010–1015. [Google Scholar] [CrossRef] [PubMed]
- Brinkley, D.; Haybittle, J.L. The late effects of artificial menopause by X-radiation. Br J Radiol 1969, 42, 519–521. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.L.; Gray, R.J.; Solin, L.J.; Robert, N.J.; Martino, S.; Tripathy, D.; Ingle, J.N.; Wood, W.C. Efficacy of radiotherapy for ovarian ablation: results of a breast intergroup study. Cancer 2004, 101, 969–972. [Google Scholar] [CrossRef] [PubMed]
- Lushbaugh, C.C.; Casarett, G.W. The effects of gonadal irradiation in clinical radiation therapy: a review. Cancer 1976, 37, 1111–1125. [Google Scholar] [CrossRef] [PubMed]
- Wallace, W.H.; Shalet, S.M.; Crowne, E.C.; Morris-Jones, P.H.; Gattamaneni, H.R. Ovarian failure following abdominal irradiation in childhood: natural history and prognosis. Clin Oncol (R Coll Radiol) 1989, 1, 75–79. [Google Scholar] [CrossRef]
- Marcello, M.F.; Nuciforo, G.; Romeo, R.; Di Dino, G.; Russo, I.; Russo, A.; Palumbo, G.; Schilirò, G. Structural and ultrastructural study of the ovary in childhood leukemia after successful treatment. Cancer 1990, 66, 2099–2104. [Google Scholar] [CrossRef] [PubMed]
- Larsen, E.C.; Müller, J.; Schmiegelow, K.; Rechnitzer, C.; Andersen, A.N. Reduced ovarian function in long-term survivors of radiation- and chemotherapy-treated childhood cancer. The Journal of clinical endocrinology and metabolism 2003, 88, 5307–5314. [Google Scholar] [CrossRef] [PubMed]
- Chemaitilly, W.; Mertens, A.C.; Mitby, P.; Whitton, J.; Stovall, M.; Yasui, Y.; Robison, L.L.; Sklar, C.A. Acute ovarian failure in the childhood cancer survivor study. The Journal of clinical endocrinology and metabolism 2006, 91, 1723–1728. [Google Scholar] [CrossRef] [PubMed]
- Green, D.M.; Sklar, C.A.; Boice, J.D., Jr.; Mulvihill, J.J.; Whitton, J.A.; Stovall, M.; Yasui, Y. Ovarian failure and reproductive outcomes after childhood cancer treatment: results from the Childhood Cancer Survivor Study. J Clin Oncol 2009, 27, 2374–2381. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, E.; Shalet, S.M.; Blackledge, G.; Todd, I.; Crowther, D.; Beardwell, C.G. The effect of combination chemotherapy on ovarian function in women treated for Hodgkin's disease. Cancer 1983, 52, 988–993. [Google Scholar] [CrossRef] [PubMed]
- Meirow, D. Reproduction post-chemotherapy in young cancer patients. Mol Cell Endocrinol 2000, 169, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.M.; Whitton, J.A.; Ginsberg, J.P.; Green, D.M.; Leisenring, W.M.; Stovall, M.; Robison, L.L.; Armstrong, G.T.; Sklar, C.A. Nonsurgical premature menopause and reproductive implications in survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. Cancer 2018, 124, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- Armenian, S.H.; Hudson, M.M.; Mulder, R.L.; Chen, M.H.; Constine, L.S.; Dwyer, M.; Nathan, P.C.; Tissing, W.J.; Shankar, S.; Sieswerda, E.; et al. Recommendations for cardiomyopathy surveillance for survivors of childhood cancer: a report from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Oncol 2015, 16, e123–136. [Google Scholar] [CrossRef]
- van Dorp, W.; Mulder, R.L.; Kremer, L.C.; Hudson, M.M.; van den Heuvel-Eibrink, M.M.; van den Berg, M.H.; Levine, J.M.; van Dulmen-den Broeder, E.; di Iorgi, N.; Albanese, A.; et al. Recommendations for Premature Ovarian Insufficiency Surveillance for Female Survivors of Childhood, Adolescent, and Young Adult Cancer: A Report From the International Late Effects of Childhood Cancer Guideline Harmonization Group in Collaboration With the PanCareSurFup Consortium. J Clin Oncol 2016, 34, 3440–3450. [Google Scholar] [CrossRef] [PubMed]
- Zidan, A.; Sherief, L.M.; El-sheikh, A.; Saleh, S.H.; Shahbah, D.A.; Kamal, N.M.; Sherbiny, H.S.; Ahmad, H. NT-proBNP as early marker of subclinical late cardiotoxicity after doxorubicin therapy and mediastinal irradiation in childhood cancer survivors. Dis Markers 2015, 2015, 513219. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, K.; Sato, S.; Tanaka, Y.; Nakamura, A.; Fujisawa, A.; Yamamoto, Y.; Kashiba, M. Method for detecting CoQ10 incorporation in the mitochondrial respiratory chain supercomplex. J Clin Biochem Nutr 2023, 72, 207–214. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



