
Submitted:
04 February 2024
Posted:
05 February 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
This is a SARS-CoV-2 seroepidemiological study in pediatric population(0-16 years) during BA.5 Omicron predominance period in Athens metropolitan area. Serum samples were tested for SARS-CoV-2 nucleocapsid antibodies(Abs-N), representing natural infection during three sub-periods of BA.5 predominance: 01/05/2022-31/08/2022(period A), 01/09/2022-31/12/2022(period B) and July 2023(period C) and epidemiological data were collected. Additionally in period C Abs-N seronegative samples were tested for SARS-CoV-2 spike antibodies(Abs-S). A total of 878 children were tested (males:51.3%) with median age(IQR): 108(36-156) months and seropositivity during the 3 subperiods was: A:292/417(70%), B:288/356(80.9%), C:89/105(84.8%), P-value<0.001. SARS-CoV-2 seropositivity increased for from period A to C for 0-1-year (P-value: 0.044), 1-4 years (P-value: 0.028) and 6-12 years children (P-value: 0.003). Children 6-12y had the highest seroposi-tivity rates in all subperiods (A: 77.3%, B: 91.4% and C: 95.8%). A significant correlation of monthly SARS-CoV-2 median antibody titers with monthly seropositivity rates was detected (rs:0.812, P-value:0.008). During period C, an additional 12/105 (11.4%) Abs-S seropositive and Abs-N ser-onegative samples were detected and total seropositivity was estimated at 96.2% (101/105). The increased SARS-CoV-2 seropositivity detected in current seroepidemiology study illustrates a high exposure rate during BA.5 predominance period. These data could guide public health decisions regarding immunization strategies and protection measures.
Keywords:
SARS-CoV-2
; COVID-19
; Children
; BA.5 Omicron variant
; seroepidemiology
1. Introduction
The rapid evolution of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), causing coronavirus disease 2019 (COVID-19) pandemic, has resulted in distinct variants which are characterized by increased transmissibility, immune invasion strategies and replication advantages [1]. The number of laboratory-confirmed COVID-19 cases has significantly increased especially following the emergence of BA.1, BA.2, BA.4 and BA.5 Omicron sublineages [2].
SARS-CoV-2 confirmed cases in children younger than 18 years old have exceeded 16 million, according to American Academy of Pediatrics [3]. Although viral transmission rates have been documented in various activities, including educational settings, children are most typically infected by close contact with an infected family member within the same household[4].
Conventional approaches to acute disease surveillance fail to encompass the exact burden of COVID-19 due to factors such as asymptomatic, undetected, or unreported cases, especially in pediatric population, especially after Omicron emergence [3]. Early studies in 2020 support that SARS-CoV-2 asymptomatic infection ratio in children ranges between 15-40% [5]. A study from the United States in 2022 showed that SARS-CoV-2 asymptomatic infections in children during 2020 and 2021 reached 65% [6].
Despite the predominance of different SARS-CoV-2 sublienages, SARS-CoV-2 antibody detection remains the most accurate test for SARS-CoV-2 infection confirmation. Serologic tests have limited utility for acute SARS-CoV-2 infection diagnosis [7]. Antibody responses comprise the initial production of immunoglobulin M (IgM), which is subsequently followed by an increase in body circulation of IgA and IgG [8]. The presence of IgG antibodies is typically detectable 16–20 days following infection in the majority of patients [9]. A comprehensive analysis of 38 studies examining the accuracy of serologic testing in COVID-19 patients based on the duration of symptoms revealed that IgM antibodies were identified in 23% of cases within one week, 58% within two weeks, and 75% within three weeks. Similarly, IgG antibodies were detected in 30%, 66%, and 88% of cases, respectively [10]. SARS-CoV-2 IgG nucleocapsid protein antibodies are produced only after natural infection and are not produced after SARS-CoV-2 vaccination, while SARS-CoV-2 IgG spike protein antibodies are produced both after natural infection and vaccination, since SARS-CoV-2 spike protein in the major antigenic target of currently available SARS-CoV-2 vaccines [11]. Seroprevalence studies, based on SARS-CoV-2 natural infection antibodies, assist by determining a more accurate approach to COVID-19 proportion in pediatric population and offer valuable public health surveillance evidence [12].
SARS-CoV-2 seropositivity was prospectively investigated in Athens metropolitan area pediatric population by our research group and highlighted the increase of SARS-CoV-2 seropositivity in children from Wuhan strain (1.7%) to Alpha (12.7%), Delta (29.7%) and pre-BA.5 Omicron predominance periods (48.5%) [13,14]. In these studies, the possible role of sex, age, origin, hospitalization status and different hospital departments on SARS-CoV-2 natural infection seropositivity and antibody levels was evaluated. The predominance period of BA.5. Omicron sublineage in Europe, including Greece, was approximately initiated on May 2022 [15].
In current SARS-CoV-2 seroepidemiological study, we aim to investigate SARS-CoV-2 natural infection seropositivity and antibody levels during distinct BA.5 Omicron predominance subperiods and associate with epidemiological parameters.
2. Materials and Methods
2.1. Study Design and Participants
This is a prospective seroepidemiological study conducted at ‘'Aghia Sophia’’ Children's Hospital, the largest (750-bed) pediatric hospital in Greece and also a pediatric COVID-19 reference center for Athens metropolitan area. Subjects of the study were children 0-16 years old who were admitted to the hospital or presented to the emergency department for any reason other than confirmed SARS-CoV-2 infection.
To prospectively evaluate SARS-CoV-2 infection seropositivity and antibody levels, approximately 100 leftover sera per month were randomly collected from the Department of Biochemistry of ‘'Aghia Sophia’’ Children's Hospital. Serum samples were collected and stored at -70oC until laboratory analysis. Serum samples laboratory processes were performed anonymously using a unique individual identification code. When a child was readmitted to the hospital on multiple occasions during the study period and had positive antibody test results, only the initial positive result was included in the analysis. Children who were admitted to the Departments of Oncology, Bleeding Disorders, or β-Thalassemia were prospectively excluded from the study because of possible interference with antibody detection due to immunocompromised conditions or transfusions.
Demographic data of sex, age, origin (Greek, non-Greek), hospitalization status and hospital department [pediatric departments, emergency department, neonatal intensive care unit (NICU), pediatric intensive care unit (PICU), surgical departments (surgery, orthopedics, otorhinolaryngology, ophthalmology, urology, cardiothoracic surgery, neurosurgery and plastic surgery departments)] were also prospectively collected and included in analysis. Children of all ages were involved in the study and were classified as neonates and infants (0–1 year), toddlers (1–4 years), pre-school age children (4–6 years), school age children (6–12 years), and adolescents (12–16 years).
Due to high SARS-CoV-2 seropositivity rates detected in Athens in our last published seroepidemiology study by April 2022 [14], we decided to perform follow-up SARS-CoV-2 seroprevalence studies every six months. Thus, the research timeframe was divided into three subperiods which corresponded to the predominance of SARS-CoV-2 BA.5 variant in Greece; period A: 01/05/2022-31/08/2022, period B: 01/09/2022-31/12/2022 and period C: July 2023.
The study protocol was in accordance with the 1964 Declaration of Helsinki and was approved by the scientific and bioethics committee of “Aghia Sophia” Children's Hospital (No. 25609).
2.2. SARS-CoV-2 Antibody Detection
Serum samples were analyzed for total SARS-CoV-2 nucleocapsid protein antibodies (Abs-N) for all the study period using Elecsys® Anti-SARS-CoV-2 (Roche Diagnostics, Basel, Switzerland) reagent [values of ≥1 cut-off index (COI) are positive]. During the last subperiod (July 2023) all children who were negative for Abs-N were also analyzed for spike protein antibodies (Abs-S) using Anti-SARS-CoV-2 S (Roche Diagnostics, Basel, Switzerland) reagent (values ≥ 0.8 U/mL are positive). The Cobas e 411 immunoassay analyzer and reagents were used according to manufacturer's instructions. Elecsys® Anti-SARS-CoV-2 is an electrochemiluminescence immunoassay (ECLIA) that use a double antigen sandwich enzyme-linked immunosorbent test technology. The ECLIA method is a highly efficient approach, with an estimated sensitivity of 99.5% (14 days after symptoms appear) and a specificity of 99.8%.
2.3. Statistical Analysis
Statistical analysis was performed using Statistical Package for the Social Sciences SPSS version 25.0 (IBM Corp., Released 2017. IBM SPSS Statistics for Windows, Version 25.0. IBM Corp). Absolute and relative frequencies (%) were used for the description of qualitative variables. Median and interquartile range (IQR) were applied for quantitative variables after the assumption of normality was evaluated with kurtosis and skewness and verified with Kolmogorov–Smirnov and Shapiro–Wilk tests. X2 tests were applied to assess distinctions among qualitative variables. Differences between qualitative and quantitative variables involved the application of two nonparametric tests: the Wilcoxon rank sum test (qualitative with 2 categories) and the Kruskal–Wallis test (qualitative with >2 categories). Correlations between quantitative variables were accessed via the Spearman r correlation coefficient. A multiple linear regression model was performed in order to estimate the SARS-CoV-2 seropositive children antibody titers (quantitative dependent variable) taking into account the simultaneous interaction of study period, age, sex, origin and hospitalization (independent variables). Graphs were created using GraphPad Prism 10. Statistical significance was set at a P-value of <0.05 level.
3. Results
3.1. Study Population
Serum samples from 878 children with median age 96 (IQR= 36-156) months [462/878 (52.6%) were males] were collected and tested for SARS-CoV-2 Abs-N.: 417/878 (47.5%) period A, 356/878 (40.5%) in period B and 105/878 (12%) in period C. Among the 878 children, 140 (15.9%) were 0-1 year, 160 (18.2%) were 1-4 years, 77 (8.8%) were 4-6 years, 270 (30.8%) were 6-12 years and 231 (26.3%) were 12-16 years. In the study population, 671/878 (76.4%) were of Greek origin, 617/878 (70.3%) were hospitalized and the majority of them [477/878 (54.3%)] were hospitalized to the pediatric departments of the hospital. Detailed epidemiological characteristics of the study population for each study period are presented in Table 1.
During the study period, a total of 669/878 (76.2%) SARS-CoV-2 seropositive children were detected with median age (IQR) of 108 months (36-156 months). Among the 669 seropositive children, 343/669 (51.3%) were males, 502/669 (75%) were of Greek origin, 459/669 (68.6%) were hospitalized and 352/669 (52.6%) were hospitalized to the pediatric departments (Table 1).
3.2. Seropositivity per Subperiod and per Month
SARS-CoV-2 seropositivity significantly increased from 292/417 (70%) in period A to 288/356 (80.9%) in period B and 89/105 (84.8%) in period C (P-value< 0.001) (Table 1). SARS-CoV-2 seropositivity during each study month also varied significantly (P-value<0.001) and is presented in Figure 1. The highest seropositivity rate of the whole study period was detected in July 2023 (84.8%, 89/105) and the lowest was detected in June 2022 (61.2%, 60/98) (Figure 1). No statistically significant correlations were identified between SARS-CoV-2 monthly seropositivity rates and newly diagnosed COVID-19 confirmed cases per month in pediatric (rs: -0,209, P-value: 0,589) or total (rs: 0,092, P-value: 0,814) population of Greece, respectively ((data from European Centre for Disease Prevention and Control (ECDC) [16].
During period C, we additionally analyzed all SARS-CoV-2 Abs-N seronegative samples (n=16) for SARS-CoV-2 Abs-S and 12/16 (75%) were positive. Therefore, an additional 12/105 (11.4%) seropositive were detected and total seropositivity was estimated at 96.2% (101/105).
3.3. Seropositivity in Different Age Groups
SARS-CoV-2 seropositivity rates in the three study subperiods per age group varied significantly (P-value<0.001) and are presented in Table 1 and Figure 2.
SARS-CoV-2 seropositivity per age group significantly varied in period A (P-value<0.001) and period B (P-value<0.001), but no significant differences were detected in period C (P-value: 0.293). SARS-CoV-2 seropositivity rates progressively increased from period A to C for all age groups, except for 4-6 years (P-value: 0.249, Table 1) and 12-16 years children (P-value: 0.158, Table 1). Children 6-12 years had the highest seropositivity rates during the whole study period (84.4%, 228/270) and to all subsequent subperiods [A: 109/141 (77.3%), B: 96/105 (91.4%) and C: 23/24 (95.8%), respectively, P-value: 0.003]. Among age groups, the lowest SARS-CoV-2 seropositivity rates were detected in 0-1 year children for the whole study population (61.4%, 86/140) and during period A (50%, 26/52) and period B (64.1%, 41/64) and 4-6 years children had the lowest seropositivity in period C (71.4%, 10/14). 3 were 0-1 year, 3 were 1-4 years, 1 was 4-6 years, 2 were 6-12 years and 2 were 12-16 years. In May 2022, SARS-CoV-2 seropositivity rates per age group varied significantly [0-1 year: 5/16 (31.3%) vs 1-4 years: 13/22 (59.1%) vs 4-6 years: 2/3 (66.7%) vs 6-12 years: 16/21 (76.2%) vs 12-16 years: 28/40 (70%), P-value: 0.05]. In September 2022, SARS-CoV-2 seropositivity rates per age group also varied significantly [0-1 year: 8/15 (53.3%) vs 1-4 years: 15/21 (71.4%) vs 4-6 years: 8/9 (88.9%) vs 6-12 years: 25/27 (92.6%) vs 24/26 (92.3%), P-value: 0.008].Total SARS-CoV-2 seropositivity (Abs-S and Abs-N) in period C was estimated at 91.7% (22/24) in 0-1 year, 96.2% (25/26) in 1-4 years, 78.6% (11/14) in 4-6 years, 100% (24/24) in 6-12 years and 100% (17/17) in 12-16 years, respectively (P-value: 0.262).
3.4. Seropositivity and Sex, Origin, Hospitalization Status and Departments
No significant differences were detected between seropositive males and females (P-value: 0.152, Table 1). SARS-CoV-2 seropositivity rates significantly increased from periods A to C for both males (P-value: 0.028) and females (P-value: 0.002). Females had higher seropositivity rates than males in period C [(92%, 46/50) vs (78.2%, 43/55), respectively, P-value: 0.049] (Table 1). Seropositivity per sex was not significantly increased in period A (P-value: 0.411) and period B (P-value: 0.38) subperiods, but females had higher seropositivity rates than males in period C [(92%, 46/50) vs (78.2%, 43/55), respectively, P-value: 0.049] (Table 1). Seropositivity per month varied significantly for females (P-value <0.001) but not for males (P-value: 0.072). The highest SARS-CoV-2 monthly seropositivity rates were detected in November 2022 for males [44/52 (84.6%)] and in August 2022 for females [48/55 (87.3%)]. The lowest SARS-CoV-2 monthly seropositivity rates were detected in July 2022 for males [30/50 (60%)] and in May 2022 for females [27/48 (56.3%)]. In August 2022, SARS-CoV-2 seropositivity rates between males and females varied significantly [males: 27/41 (65.9%) vs females: 48/55 (87.3%), P-value:0.023]. No other significant differences in SARS-CoV-2 monthly seropositivity rates between males and females were detected. SARS-CoV-2 Abs-S seropositivity in period C was estimated at 92.7% (51/55) for males and 100% (50/50) for females (P-value: 0.118).
No significant differences were detected between seropositive Greek and non-Greek children (P-value: 0.083, Table 1) or each different study subperiod (summer 2022: P-value: 0.24, winter 2022: P-value: 0.099, July 2023: P-value: 0.724 Table 1). Seropositivity in Greek was significantly increased from periods A to C (P-value: 0.001) but not for non-Greek children (P-value: 0.102) (Table 1). Seropositivity per month varied significantly for Greek (P-value: 0.001) but not for non-Greek children (P-value: 0.092). The highest SARS-CoV-2 monthly seropositivity rates were detected in July 2023 for Greek [65/76 (85.5%)] and in September 2022 for non-Greek children [21/22 (95.5%)]. The lowest SARS-CoV-2 monthly seropositivity rates were detected in June 2022 for Greek [46/79 (58.2%)] and in May 2022 for non-Greek children [14/23 (60.9%)]. SARS-CoV-2 Abs-S seropositivity in period C was estimated at 98.7% (75/76) for Greek and 89.7% (26/29) for non-Greek children (P-value: 0.304).
SARS-CoV-2 seropositivity rates significantly increased from periods A to C for both hospitalized (P-value: 0.002) and non-hospitalized children (P-value: 0.023). Non-hospitalized children had significantly higher SARS-CoV-2 seropositivity rates compared to hospitalized children (80.5%, 210/261) vs (74.4%, 459/617) P-value: 0.05, Table 1). Monthly SARS-CoV-2 seropositivity rates differ significantly in hospitalized (P-value <0.001) but not in non-hospitalized children (P-value: 0.25). The highest SARS-CoV-2 monthly seropositivity rates were detected in July 2023 for hospitalized [68/79 (86.1%)] and in December 2022 for non-hospitalized children [8/9 (88.9%)]. The lowest SARS-CoV-2 monthly seropositivity rates were detected in June 2022 for hospitalized [35/64 (54.7%)] and in May 2022 for non-hospitalized children [21/29 (72.4%)]. SARS-CoV-2 Abs-S seropositivity in period C was estimated at 89.9% (71/79) for hospitalized and 88.5% (23/26) for non-hospitalized children (P-value: 0.57).
SARS-CoV-2 seropositivity rates significantly increased from periods A to C in general pediatric departments (P-value: 0.001). No significant differences were reported in among SARS-CoV-2 seropositivity in different hospital departments (P-value: 0.177, Table 1). Monthly SARS-CoV-2 seropositivity rates differ significantly in general pediatric departments (P-value: 0.001). SARS-CoV-2 Abs-S seropositivity in period C was estimated at 87.9% (58/66) in pediatrics departments, 100% (2/2) in NICU, 100% (3/3) in PICU, 8/8 in surgical departments and 0/0 in cardiology/neurology department, respectively (P-value: 0.659).
3.5. Antibody Titers per Age Group, Sex, Origin, Hospitalization Status and Department
SARS-CoV-2 median (IQR) Abs titers (MAbs) of 669 SARS-CoV-2 seropositive children was 31.1 COI (9.1-102.5 COI) and did not significantly vary among the three study subperiods [A: 35.52 COI (11.04-112.7 COI) vs B: 26.48 COI (7.87-97.28 COI) vs C: 27.91 COI (6.14-81.12 COI), P-value: 0.119] (Figure 3A) but varied significantly per month (P-value: 0.003). SARS-CoV-2 MAbs per month significantly correlate with SARS-CoV-2 monthly seropositivity rates (rs: 0.812, P-value: 0.008).
MAbs per age group were estimated at 20.63 COI (4.82–94.15 COI) in 0-1 years children, 43.5 COI (10.05–113.1 COI) in 1-4 years, 28.38 COI (6.7–108.8 COI) in 4-6 years, 29.29 COI (8.27–82.47 COI) in 6-12 years and 33.46 COI (11.42–119.1 COI) in 12-16 years (P-value: 0.08) (Figure 3B). MAbs did not correlate significantly with age either during the whole study period (rs: 0.064, P-value: 0.098) or in any of the study subperiods (Period A: rs: 0.057 and P-value: 0.336, Period B: rs: 0.023 and P-value: 0.696, Period C: rs: 0.125 and P-value: 0.243, respectively).
MAbs were detected significantly higher in non-Greek vs Greek children [39.58 COI (10.46-126.5 COI) vs 27.42 (8.4-93.31 COI), P-value: 0.031]. There were significant differences regarding MAbs among different departments of the hospital (P-value: 0.026). MAbs were higher in emergency deparment children compared to children in NICU [41.30 (9.08-113.5 COI) vs 6.07 (2.61-48.72 COI) P-value: 0.036] and higher in the surgical departments compared to NICU [41.50 (14.87-110.7 COI) vs 6.07 (2.61-48.72 COI) P-value: 0.017].
No significant differences were detected regarding MAbs per sex [27.22 COI (8.11-95.02 COI) in males vs 35.12 COI (10.18-109.88 COI) in females, P-value: 0.266] and per hospitalization status [27.87 COI (9.06-94.68 COI) in hospitalized vs 41.31 COI (9.07-113.5 COI) in non-hospitalized, P-value: 0.154].
3.6. Multiple Linear Regression Model by Study Period
Analysis of the data in all SARS-CoV-2 seropositive children (n=669) showed that the multiple linear regression model including study period, age, gender, ethnicity and hospitalization as independent variables was statistically significantly more effective in predicting SARS-CoV-2 natural disease antibody titers compared to monoparametric comparisons (ANOVA Test, P-value: 0.031). The results of the multiple linear regression analysis for the entire study are presented in Supplementary Table S1.
Based on the linear regression model for the whole study period (n=669 seropositive children), children of non-Greek origin are expected to have a 15.073 COI higher MAbs than children of Greek origin given that all other independent variables remain constant (P-value: 0.009, Supplementary Table S1).
4. Discussion
In the present study, we investigated SARS-CoV-2 seropositivity and antibody levels during BA.5 predominance period in Athens pediatric population taking into consideration epidemiological parameters. This is a follow-up study from previous investigations starting from the beginning of the pandemic (3/2020) showing a gradual increase in seropositivity rates in our area from 4% to 52.6% [13,14]. A further increase in SARS-CoV-2 Abs-N seropositivity during BA.5 predominance period from 62.7% in May 2022 to 84.8% in July 2023 was detected. SARS-CoV-2 seropositivity increased for all age groups, for both sexes, regardless of origin or hospitalization status, and in all different hospital departments, including emergency departments.
The prospective acquisition of routine leftover residual serum samples from the Biochemistry department presents a viable approach for assessing SARS-CoV-2 serosurveillance in children and provides the advantage of avoiding additional blood sampling for paediatric patients. All previous studies were based on the testing of routine leftover residual serum samples avoiding additional blood sampling for pediatric patients and has successfully been implemented in other seroprevalence studies as well [17,18,19].
SARS-CoV-2 seropositivity in our area does not substantially differ from reported seroepidemiological data from the USA, Latvia, Thailand, Guinea and Cameroon, indicating increased SARS-CoV-2 seropositivity during the BA.5 Omicron period [18,20,21,22]. No differences in SARS-CoV-2 seropositivity rates between sexes was detected which is also the finding of Greek National Public Health Organization COVID-19 Surveillance System and other similar studies [15], [17,18]. According to our previously published studies, SARS-CoV-2 seropositivity rates between sexes did not significantly differ either during Wuhan (females: 1.4% vs males: 1.4%), or Alpha (females: 14.6% vs males: 19.7%), or Delta (females: 32.8% vs males: 27.3%) or pre-BA.5 Omicron (females: 47.7% vs males: 49.2%) predominance periods, respectively [13,14].
In this study, SARS-CoV-2 infection seropositivity increased for all age groups and was higher especially for children 6-12 years and adolescents (12-16 years). Similar findings from CDC report that children 5-11 years old, from May to October 2022 in USA, had the highest SARS-CoV-2 natural infection seropositivity rates (93.5%) follower by 12-17 years (93%) [22]. According to our previously published studies, SARS-CoV-2 natural infection seropositivity rates in children 6-12 years gradually increased from 0% in Wuhan to 14.4% in Alpha, 27.8% in Delta and 56.5% in pre-BA.5 Omicron predominance periods [13,14]. Similarly, SARS-CoV-2 seropositivity rates in children 12-16 years increased from 0% in Wuhan to 16.9% in Alpha, 32.5% in Delta and 51.8% in pre-BA.5 Omicron predominance periods, respectively [13,14].
A SARS-CoV-2 seropositivity study in Latvia from May 2022 to July 2022 in 173 children showed that children 12-18 years had the highest seropositivity rates (94.3%) when compared to 5-11 years (90.9%) and <5 years (77.8%) [20]. These differences could possibly be attributed to different number of participants and age group stratification. These findings may be attributed to the increased exposure of school-age children in Omicron period and enhanced transmissibility of BA.5 subvariant.
According to a recent meta-analysis, SARS-CoV-2 seropositivity is higher in children of Asian and African regions [23]. These countries are also associated with increased migration rates to Greece over the last years. In the present study, children of non-Greek origin had similar seropositivity in contrast with the findings from our previously published data in 2021 and 2022 [13,14]. In our previously published studies, SARS-CoV-2 seropositivity rates significantly differed between Greek and non-Greek children during Wuhan (Greek: 1% vs non-Greek: 2.4%) and Alpha (Greek: 14.3% vs non-Greek: 25.6%) but not during Delta (Greek: 29.3% vs non-Greek: 31.5%) or pre-BA.5 Omicron (Greek: 48% vs non-Greek: 49.7%) predominance periods, respectively [13], [14]. However, in current study, children of non-Greek origin had higher antibody titers compared to Greek. This finding could possibly indicate increased exposure that leads to repeated infections among non-Greek underprivileged communities within Athens metropolitan area.
Due to high SARS-CoV-2 seropositivity rates for natural infection (Abs-N) in our area, we decided to perform follow-up SARS-CoV-2 seroprevalence studies every six months with additional Abs-S testing. From the additional testing, it was shown that even with negative Abs-N a significant percentage of population could have positive Abs-S representing either immunization or SARS-CoV-2 exposure. After detecting both antibodies, it was found that children 6-16 years had 100% SARS-CoV-2 seropositivity. According to CDC, these two pediatric age groups are associated with the highest seroprevalence rates (97.1% for school-age children and 98.9% for adolescents, respectively) and agree with the findings of our study [22]. In Greece, where approximately half of total country population has laboratory-confirmed COVID-19, SARS-CoV-2 vaccination rates with a complete primary series reach 75% in adults and children[24]. Waning Humoral immunity several months following SARS-CoV-2 infection [25] supports that SARS-CoV-2 vaccination is of vital importance to offer a surrogate of protection. Our data suggest that, in future seroepidemiological studies, both antibodies should be tested in Abs-N seronegative population.
In Winter 2022 BA.5 predominance period, non-hospitalized children were incommensurately affected by COVID-19 compared to hospitalized children regardless of different hospital departments. In contrast, hospitalized children in Greece were found to have higher seropositivity rates during Alpha and Delta periods [13,14]. Those differences could be explained as more children possibly visited the emergency department during Omicron for mild common cold symptoms due to SARS-CoV-2 reinfection but were not detected as SARS-CoV-2 positive at admission by molecular or rapid antigen testing. This hypothesis could also explain the increased antibody titers of non-hospitalized compared to hospitalized children also reported in our study. According to CDC, there is an increasing trend of emergency department visits due to COVID-19 diagnosis during 2023 for both children and adults [26]. Therefore, SARS-CoV-2 seroprevalence studies in different hospital departments, including emergency departments, could provide valuable epidemiological data or possibly guide hospital measures.
Limitations of present study include that it represents data from a specific area of Greece and not in a national level. In addition, Abs-N, representing natural infection, was analyzed for the total population and Abs-S, which could be also vaccine-induced, was additionally analyzed only for the last period of the study. The suggested multiple linear regression model for SARS-CoV-2 antibody titers was successful for antibody values measured only by a certain detection laboratory assay and should be interpreted cautiously if applied to other distinct assays. Therefore, the ultimate trajectory of bias arising from these factors remains uncertain. However, this is the third part of our department’s prospective longitudinal seroepidemiology and antibody levels study from the beginning of the pandemic involving the pediatric population of Athens metropolitan area and it is the largest in terms of duration (2020-2022) and total study population (approximately 5000 children 0-16 years old in total) in Greece.
5. Conclusions
To date, there is limited serosurveillance evidence in BA.5 Omicron period regarding SARS-CoV-2 disease in pediatric population. The increased SARS-CoV-2 seropositivity detected in current seroepidemiology study illustrates a high exposure rate during BA.5 predominance period. These data could guide public health decisions regarding immunization strategies and protection measures. Since monthly seropositivity rates attributed only to SARS-CoV-2 disease fail to reach 100% during 2022 and 2023, continuous surveillance of SARS-CoV-2 disease with the inclusion of other clinical and epidemiological factors is needed in order the COVID-19 in children to be better approached.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Multiple linear regression model analysis of 669 SARS-CoV-2 seropositive children for the whole study period (01/05/2022-31/12/2022 and July 2023) involving SARS-CoV-2 natural infection antibody titers as dependent variable and period, sex, age, origin and hospitalization status as independent variables. Statistically significant differences (P-value <0.05) are marked in bold.
Author Contributions
Conceptualization, A.M. and V.S.; methodology, A.M., V.S. and F.F.; validation, F.F., E.-B.T. and A.M.; formal analysis, F.F.; investigation, F.F. and E.-B.T.; data curation, F.F., M.-M.D. and Al.M.; writing—original draft preparation, F.F.; writing—review and editing, A.M. and V.S,; supervision, A.M..; project administration, A.M. and F.F. All authors have read and agreed to the published version of the manuscript.
Data Availability Statement
All relevant data are published within the paper.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- S. B. Jørgensen, K. S. B. Jørgensen, K. Nygård, O. Kacelnik, and K. Telle, “Secondary Attack Rates for Omicron and Delta Variants of SARS-CoV-2 in Norwegian Households,” JAMA, vol. 327, no. 16, pp. 1610–1611, Apr. 2022. [CrossRef]
- “Implications of the emergence and spread of the SARS-CoV-2 variants of concern BA.4 and BA.5 for the EU/EEA.” Accessed: Dec. 19, 2023. [Online]. Available: https://www.ecdc.europa.eu/en/news-events/implications-emergence-spread-sars-cov-2-variants-concern-ba4-and-ba5.
- “Children and COVID-19: State-Level Data Report.” Accessed: Dec. 19, 2023. [Online]. Available: https://www.aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/children-and-covid-19-state-level-data-report/?_ga=2.86856984.1216052961.1702976577-307753667.1702976577.
- G. T. Chua et al., “Clinical Characteristics and Transmission of COVID-19 in Children and Youths During 3 Waves of Outbreaks in Hong Kong,” JAMA Netw Open, vol. 4, no. 4, no. 5, 2021. 5. [CrossRef]
- R. M. Viner et al., “Systematic review of reviews of symptoms and signs of COVID-19 in children and adolescents,” Arch Dis Child, vol. 106, no. 8, pp. 802–807, Aug. [CrossRef]
- C. B. Forrest et al., “Severity of Acute COVID-19 in Children <18 Years Old March 2020 to December 2021,” Pediatrics, vol. 149, no. 4, Apr. 2022. 20 March. [CrossRef]
- C. MP et al., “Serodiagnostics for Severe Acute Respiratory Syndrome-Related Coronavirus 2 : A Narrative Review,” Ann Intern Med, vol. 173, no. 6, pp. 450–460, Sep. 2020. [CrossRef]
- T. Huang et al., “A systematic review of antibody mediated immunity to coronaviruses: kinetics, correlates of protection, and association with severity,” Nat Commun, vol. 11, no. 1, Dec. 2020. [CrossRef]
- X. Wang et al., “Neutralizing Antibody Responses to Severe Acute Respiratory Syndrome Coronavirus 2 in Coronavirus Disease 2019 Inpatients and Convalescent Patients,” Clinical Infectious Diseases, vol. 71, no. 10, pp. 2688–2694, Dec. 2020. [CrossRef]
- J. J. Deeks et al., “Antibody tests for identification of current and past infection with SARS-CoV-2,” Cochrane Database Syst Rev, vol. 6, no. 6, Jun. 2020. [CrossRef]
- F. Krammer, “SARS-CoV-2 vaccines in development,” 516 | Nature |, vol. 586, 2020. [CrossRef]
- E. I. Kritsotakis, “On the importance of population-based serological surveys of SARS-CoV-2 without overlooking their inherent uncertainties,” Public Health in Practice, vol. 1, Nov. 2020. [CrossRef]
- F. Filippatos et al., “Seroepidemiology of SARS-CoV-2 in pediatric population during a 16-month period prior to vaccination,” J Med Virol, vol. 94, no. 5, pp. 2174–2180, May 2022. 20 May. [CrossRef]
- F. Filippatos et al., “SARS-CoV-2 seroepidemiology in paediatric population during Delta and Omicron predominance,” Epidemiol Infect, vol. 150, Oct. 2022. [CrossRef]
- T. E. Tallei et al., “Update on the omicron sub-variants BA.4 and BA.5,” Rev Med Virol, vol. 33, no. 1, Jan. 2023. [CrossRef]
- “Download COVID-19 data sets.” Accessed: Jan. 25, 2024. [Online]. Available: https://www.ecdc.europa.eu/en/covid-19/data.
- F. Wachter et al., “Continuous monitoring of SARS-CoV-2 seroprevalence in children using residual blood samples from routine clinical chemistry,” Clin Chem Lab Med, vol. 60, no. 6, pp. 941–951, May 2022. 20 May. [CrossRef]
- N. Suntronwong et al., “SARS-CoV-2 infection- induced seroprevalence among children and associated risk factors during the pre- and omicron-dominant wave, from 21 through December 2022, Thailand: A longitudinal study,” PLoS One, vol. 18, no. 4, p. e0279147, Apr. 2023. 20 January. [CrossRef]
- N. Sarmento et al., “The use of residual serum samples to perform serological surveillance of severe acute respiratory syndrome coronavirus 2 in Dili and regional areas of Timor-Leste,” Trans R Soc Trop Med Hyg, vol. 117, no. 4, pp. 313–315, Apr. 2023. [CrossRef]
- K. Sapronova et al., “SARS-CoV-2 seroprevalence among children in Latvia: A cross-sectional study,” Medicine (United States), vol. 102, no. 6, Feb. 2023. [CrossRef]
- M. S. K. Diallo et al., “Large Diffusion of Severe Acute Respiratory Syndrome Coronavirus 2 After the Successive Epidemiological Waves, Including Omicron, in Guinea and Cameroon: Implications for Vaccine Strategies,” Open Forum Infect Dis, vol. 10, no. 5, May 2023. 20 May; 5. [CrossRef]
- “Nationwide Commercial Laboratory Seroprevalence Survey | Data | Centers for Disease Control and Prevention.” Accessed: Nov. 10, 2023. [Online]. Available: https://data.cdc.gov/Laboratory-Surveillance/Nationwide-Commercial-Laboratory-Seroprevalence-Su/d2tw-32xv.
- R. Naeimi et al., “SARS-CoV-2 seroprevalence in children worldwide: A systematic review and meta-analysis,” EClinicalMedicine, vol. 56, Feb. 2023. 2023. [CrossRef]
- “WHO Coronavirus (COVID-19) Dashboard | WHO Coronavirus (COVID-19) Dashboard With Vaccination Data.” Accessed: Dec. 19, 2023. [Online]. Available: https://covid19.who.int/.
- M. Stich et al., “Waning Immunity 14 Months After SARS-CoV-2 Infection,” Pediatrics, vol. 150, no. 5, Nov. 2022. [CrossRef]
- “CDC COVID Data Tracker: Trends in ED Visits.” Accessed: Jan. 25, 2024. [Online]. Available: https://covid.cdc.gov/covid-data-tracker/#ed-visits_separated_by_age_group.
Figure 1.
Monthly SARS-CoV-2 seropositivity rates for nucleocapsid antibodies from May 2022 to December 2022 and July 2023 for the whole study population.
Figure 1.
Monthly SARS-CoV-2 seropositivity rates for nucleocapsid antibodies from May 2022 to December 2022 and July 2023 for the whole study population.
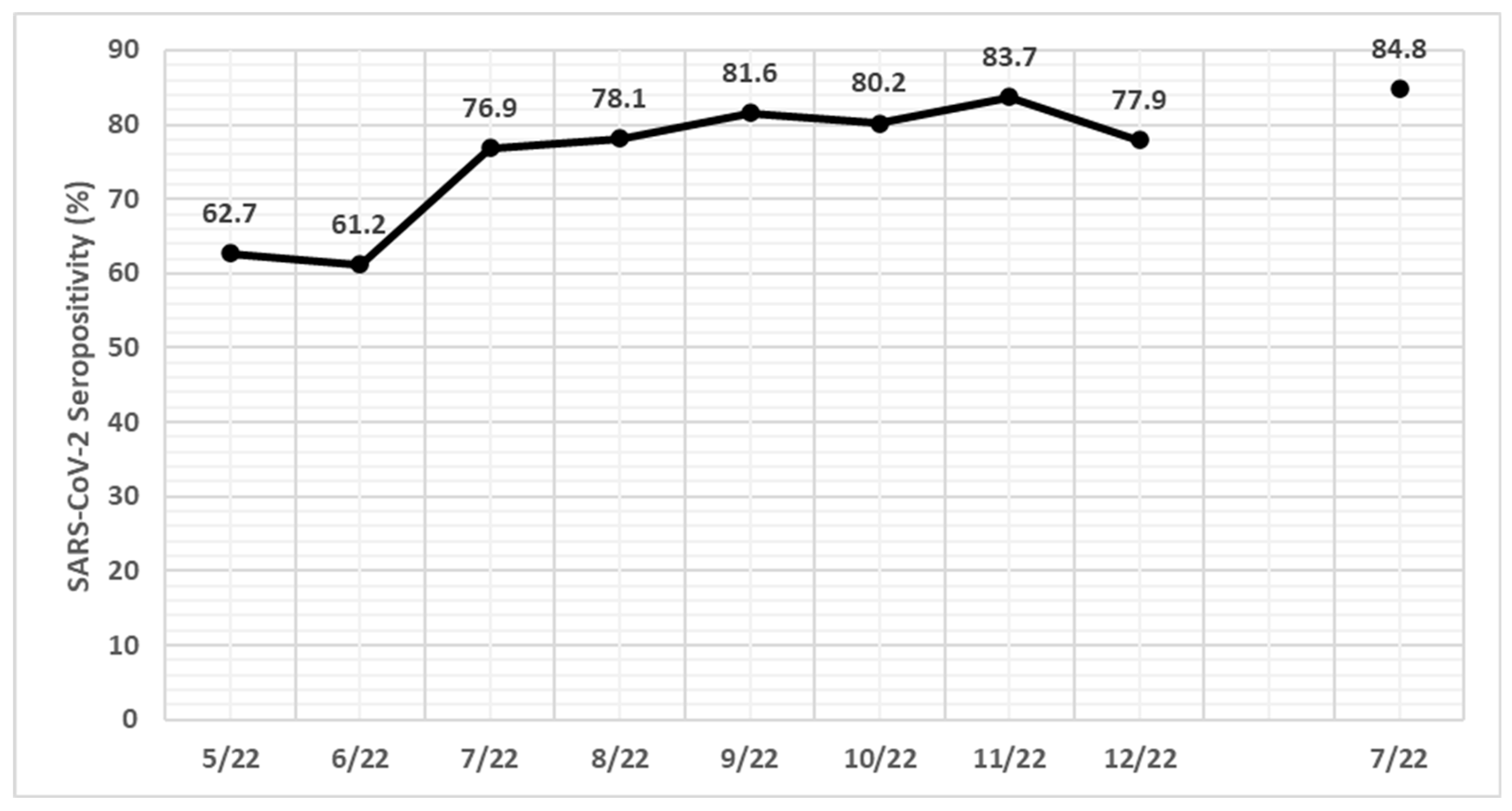
Figure 2.
SARS-CoV-2 seropositivity rates per study subperiod (Period A: 01/05/2022-31/08/2022, Period B: 01/09/2022-31/12/2022 and Period C: July 2023) for neonates-infants (0-1 year), toddlers (1-4 years), pre-school children (4-6 years), school age children (6-12 years) and adolescents (12-16 years). *: P-value<0.05, **: P-value<0.01.
Figure 2.
SARS-CoV-2 seropositivity rates per study subperiod (Period A: 01/05/2022-31/08/2022, Period B: 01/09/2022-31/12/2022 and Period C: July 2023) for neonates-infants (0-1 year), toddlers (1-4 years), pre-school children (4-6 years), school age children (6-12 years) and adolescents (12-16 years). *: P-value<0.05, **: P-value<0.01.
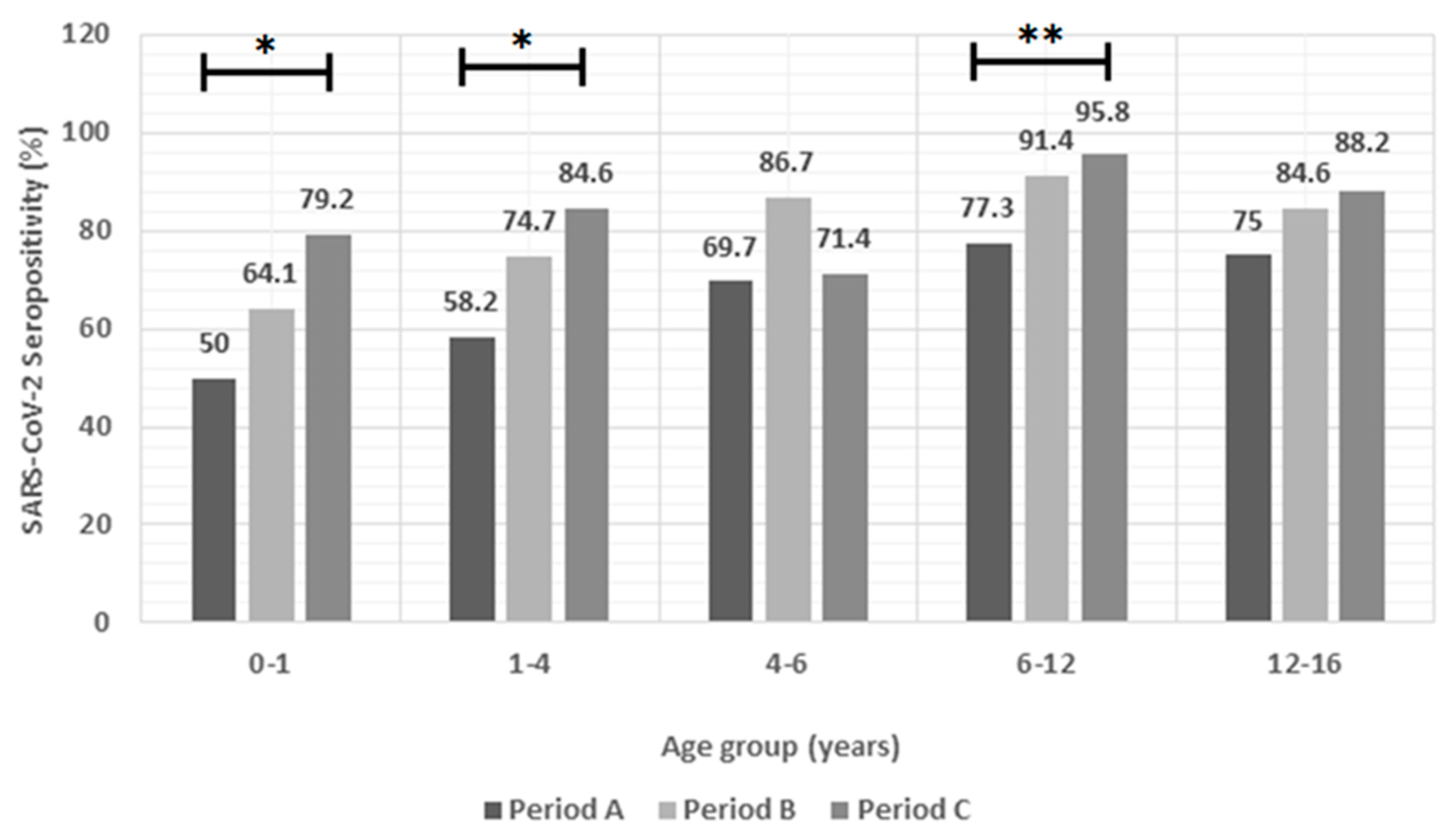
Figure 3.
Median antibody titers per study subperiod (Panel A) and per age group (0-1, 1-4, 4-6, 6-12, 12-16 years) (Panel B) of the 669 SARS-CoV-2 seropositive children in Athens Metropolitan area from Period A (01/05/2022-31/08/2022), Period B (01/09/2022-31/12/2022) and Period C (July 2023). Bold horizontal lines represent median antibody titer values and non-bold horizontal lines represent interquartile range (IQR) values. COI, cut-off index; Abs-N: antibodies for SARS-CoV-2 nucleocapsid protein.
Figure 3.
Median antibody titers per study subperiod (Panel A) and per age group (0-1, 1-4, 4-6, 6-12, 12-16 years) (Panel B) of the 669 SARS-CoV-2 seropositive children in Athens Metropolitan area from Period A (01/05/2022-31/08/2022), Period B (01/09/2022-31/12/2022) and Period C (July 2023). Bold horizontal lines represent median antibody titer values and non-bold horizontal lines represent interquartile range (IQR) values. COI, cut-off index; Abs-N: antibodies for SARS-CoV-2 nucleocapsid protein.
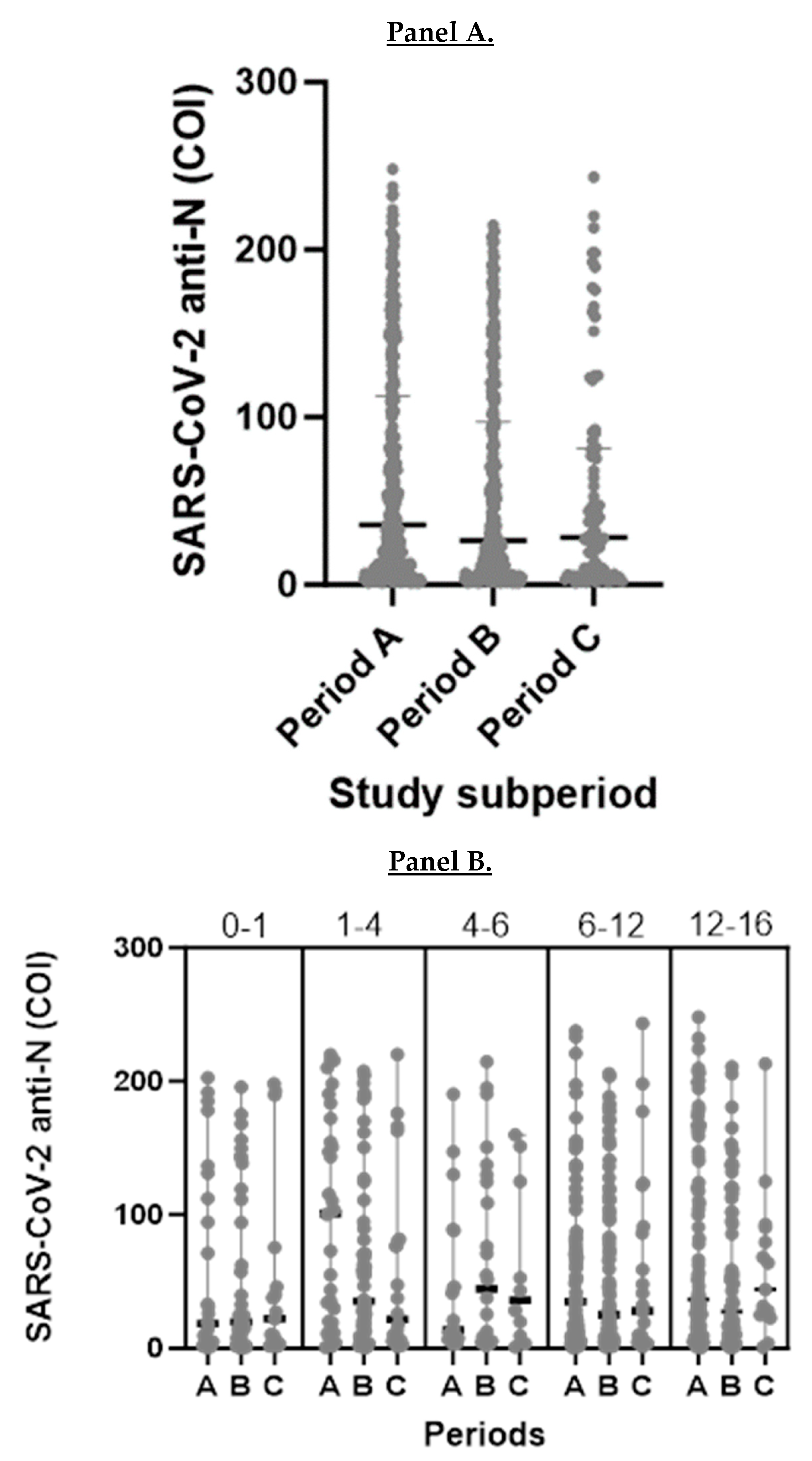

Table 1.
Distribution of the 878 children (SARS-CoV-2 seropositive: 669/878) who participated in the study over the course of the three distinct study subperiods (Period A: 01/05/2022-31/08/2022, Period B: 01/09/2022-31/12/2022 and Period C: July 2023) according to their demographic characteristics. Statistically significant differences (P-value <0.05) are marked in bold.
Table 1.
Distribution of the 878 children (SARS-CoV-2 seropositive: 669/878) who participated in the study over the course of the three distinct study subperiods (Period A: 01/05/2022-31/08/2022, Period B: 01/09/2022-31/12/2022 and Period C: July 2023) according to their demographic characteristics. Statistically significant differences (P-value <0.05) are marked in bold.
| Study period | |||||
|---|---|---|---|---|---|
| Total n(%) |
Period A n(%) |
Period B n(%) |
Period C n(%) |
P-value | |
| Total | 878 | 417 | 356 | 105 | |
| 669/878 (76.2) |
292/417 (70) |
288/356 (80.9) |
89/105 (84.8) |
<0.001 | |
| Sex | |||||
| Male | 343/462 (74.2) |
139/204 (68.1) | 161/203 (79.3) |
43/55 (78.2) |
0.028 |
| Female | 326/416 (78.4) |
153/213 (71.8) | 127/153 (83) |
46/50 (92) |
0.002 |
| P-value | 0.152 | 0.411 | 0.38 | 0.049 | |
| Age group (years) | |||||
| 0-1 | 86/140 (61.4) |
26/52 (50) |
41/64 (64.1) |
19/24 (79.2) |
0.044 |
| 1-4 | 113/160 (70.6) |
32/55 (58.2) |
59/79 (74.7) |
22/26 (84.6) |
0.028 |
| 4-6 | 59/77 (76.6) |
22/33 (69.7) |
26/30 (86.7) |
10/14 (71.4) |
0.249 |
| 6-12 | 228/270 (84.4) |
109/141 (77.3) | 96/105 (91.4) |
23/24 (95.8) |
0.003 |
| 12-16 | 189/231 (79.2) |
102/136 (75) |
66/78 (84.6) |
15/17 (88.2) |
0.158 |
| P-value | <0.001 | 0.001 | <0.001 | 0.293 | |
| Origin | |||||
| Greek | 502/671 (74.8) |
218/318 (68.6) | 219/277 (79.1) |
65/76 (85.5) |
0.001 |
| non-Greek | 167/207 (80.07) |
74/99 (74.7) |
69/79 (87.3) |
24/29 (82.8) |
0.102 |
| P-value | 0.083 | 0.24 | 0.099 | 0.724 | |
| Hospitalized | |||||
| Yes | 459/617 (74.4) |
199/291 (68.4) | 192/247 (77.7) |
68/79 (86.1) |
0.002 |
| No | 210/261 (80.5) |
93/126 (73.8) |
96/109 (88.1) |
21/26 (80.8) |
0.023 |
| P-value | 0.05 | 0.267 | 0.022 | 0.514 | |
| Department | |||||
| Pediatrics | 352/477 (73.8) |
145/219 (66.2) | 151/192 (78.6) |
56/66 (84.8) |
0.001 |
| NICU | 22/29 (75.9) |
11/14 (78.6) |
9/13 (69.2) |
2/2 (100) |
0.605 |
| PICU | 11/18 (61.1) |
5/10 (50) |
4/5 (80) |
2/3 (66.7) |
0.52 |
| Surgical | 51/66 (77.3) |
29/36 (80.6) |
14/22 (63.9) |
8/8 (100) |
0.086 |
| Cardiology-Neurology | 23/27 (85.2) |
9/12 (75) |
14/15 (93.3) |
0/0 (0) |
0.183 |
| P-value | 0.177 | 0.234 | 0.048 | 0.578 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



