
Submitted:
02 February 2024
Posted:
05 February 2024
You are already at the latest version
Abstract
Abstract: Background: The birthrate of Black preterm (BPT) infant is 65% higher than White preterm (WPT) infants with BPT mortality 2.3 times higher. The incidence of culture positive sepsis is as high as 41% in preterms. This study aimed to examine infections and mortality in BPTs and WPTs. Methods: We enrolled 362 preterms born < 32 weeks gestational age (GA) between 2019-2023 in 5 neonatal intensive care unit (NICU)s to study onset of infections, and dispositions; RedCap data were analyzed for descriptive statistics. Results: 226 BPTs (63.5%) and 107 WPTs (30.8%) enrolled, with 29 other than White or Black, 50.5% female, mean GA of 27.67 weeks and 986.74 grams birthweight. Of 426 suspected infections evaluated in enrolled infants, there were 7 infants with early onset sepsis (EOS) and 39 infants with late onset sepsis (LOS). The incidence of EOS was 1.9% overall, 2.2% in BPTs vs 0.9% in WPTs. LOS incidence was 10.8% overall, 11.9% in BPTs and 9.3% in WPTs. Both BPT and WPT infants had ~ 8% gram-positive LOS events and 3% gram-negative LOS events; however, 82% of all gram-negative LOS episodes occurred in BPTs. There were 27 urinary tract infections and 78% were in BPTs. Two cerebral spinal fluid cultures were positive in BPTs. Necrotizing enterocolitis was diagnosed in 5.8% of the sample, with an incidence of 6.1% in BPTs versus 4.7% in WPTs. Death occurred in 6.0% of the enrolled infants with the rate of death being slightly higher in BPTs (7.0%) versus WPTs (5.6%). Conclusions: BPTs had a higher rate of positive cultures, double the gram-negative infections, a much higher rate of urinary tract infec-tions and a higher rate of mortality than their WPT counterparts. This study emphasizes higher risk of morbidity and mortality for BPTs.
Keywords:
premature infant
; infection
; disparities
; mortality
; bacteria.
1. Introduction
Over 63,000 very preterm infants, those infants delivered before 32 weeks gestational age (GA), are born annually in the United States [1]. In 2020, the rate of preterm single births was almost 65% higher for Black mothers compared to White mothers [2]. For every 1000 preterm or low birthweight (i.e., birthweight <2500 grams) infants born, 25 more Black preterm (BPT) infants die compared to White preterm (WPT) infants [3] and survival without major morbidity is a significant problem [4]. Morbidity such as infection and/or necrotizing enterocolitis (NEC) can lead to extended hospitalizations or even death[5,6]. Moreover, there are significant racial and ethnic disparities in mortality rates. Compared to WPT infants, BPT infants have higher rates of fetal death and infant mortality during the first year of life [3], and compared to WPT infants, are at a higher risk of all neonatal morbidities [7]. The health of BPT infants is indistinguishably linked to the health of Black women who experience high levels of chronic stress over the life course due to structural racism that disproportionately exposes them to poverty, neighborhood disadvantage, and low educational attainment [8,9]. In a study of over 20,000 mothers and their infants, Black mothers compared to White mothers, had higher rates of diabetes (including pregestational and gestational), hypertension (including chronic and pregnancy-induced), chorioamnionitis, and premature rupture of membranes (PROM) [10]. Over a decade ago, the annual societal financial burden associated with preterm birth in the United States was found to be at least $26.2 billion [11]. Even though extremely preterm infants (i.e., those born before 28 weeks’ GA) account for only 6% of all preterm births, they account for 1/3 of all costs associated with preterm birth through 7 years of age which imposes a huge economic burden through early childhood. Black women and their families are placed at a large socioeconomic disadvantage upon the birth of a preterm infant, which may impact the family for generations [12]. Importantly, social determinants of health, or the conditions in which people are born, grow, live and work, have been linked to the incidence of sepsis in adults and may also be related to sepsis in preterm infants [13].
Neonatal sepsis occurs in up to 41% of very preterm infants while they are hospitalized in a neonatal intensive care unit (NICU) [14]. Infants may be born infected or acquire a nosocomial infection over their NICU hospitalization. Early onset sepsis (EOS), diagnosed within the first 72 hours after birth, is attributed to transference of a maternal infection when PROM or chorioamnionitis is present [15]. EOS confirmed by positive blood cultures is rare with an incidence of 1-4% [16], but EOS is frequently suspected due to high prevalence of maternal PROM and chorioamnionitis [17] and culture-negative EOS is often treated. Other risk factors for EOS are perinatal asphyxia, amniotic fluid meconium contamination, maternal urinary tract infection, and vaginal examinations [18]. Most often, Group B Streptococcus (GBS) and Escherichia coli (E. coli) are the bacteria associated with EOS. If the mother presents with signs of infection, or PROM, she is treated with antibiotics prior to delivery if there is time to do so before delivery, and the infant is treated with broad-spectrum antibiotics for 24-48 hours to monitor blood cultures for bacterial growth, if present.
Late onset sepsis (LOS) is usually diagnosed after the preterm infant reaches 72 hours of age, with the highest incidence between 10-22 days of life [19]. The incidence of LOS is highest for very preterm or very low birth weight infants and ranges from 12-50% [14,20]. Some of the common pathogens leading to a diagnosis of LOS are coagulase-negative Staphylococcus (CONS)[20,21] in > 50% of gram-positive cultures, Staphylococcus aureus (4-18%), and Enterococcus species (spp., 3-16%) [22]. Usual pathogens associated with gram-negative sepsis in very preterm infants are E. coli (3-13%), Klebsiella spp. (4-5%), Pseudomonas spp. (2-5%), Enterobacter spp. (2.5-21%), Serratia (0.8-2%) and Acinetobacter (0.1-2%) [22]. These type of infections can be frequent and occur several times during a NICU hospitalization, due to the vulnerability of preterm infants with depressed immune systems, and the frequency of contact with multiple hospital personnel, indwelling central lines, and respiratory treatment with apparatus that requires warming through fluids [15]. Signs of infection are often ambiguous and may include apnea and bradycardia, respiratory distress, thermal instability, feeding intolerance, lethargy, or infant clinically not at baseline per staff [15]. Evaluations to rule out and treat based on suspicion of LOS is less standardized than when the mother’s clinical obstetrical history prompts the clinician to rule out and conduct surveillance treatment for EOS, especially as clinicians attempt to scale back overuse of antibiotics [15].
LOS leads to increased morbidity and mortality, with the incidence increasing as the GA at birth decreases [22]. It is imperative researchers examine health disparities in the maternal-infant population so etiological pathways can be exposed, and potential interventions developed to lessen those disparities. This analysis aimed to examine disparities between Black and White mothers’ prenatal health and their preterm infants, with an emphasis on disparities in preterm morbidities including EOS, LOS, NEC, and bacteria present in the urinary tract, respiratory tract, and cerebral spinal fluid (CSF) as well as infant mortality between birth and NICU discharge/transfer/or death.
2. Materials and Methods
This study (protocol 00082482) was approved by the Medical University of South Carolina Institutional Review Board (IRB) with a Federal Wide Assurance #1888, as a multi-site study using a single IRB, and study procedures and documents were site approved by local site IRBs. The study is funded through National Institute of Health, National Institute of Nursing Research (R01NR017872) beginning 2018 through 2023. A detailed study protocol [23] is published. In this longitudinal, observational trial, 367 very preterm infants, or those infants born prior to 32 weeks’ GA were enrolled from 5 NICUs in North and South Carolina. The first infant enrolled at each site was considered a pilot infant and was not included in analysis. This study examined averaged daily central-peripheral temperature difference (CPTd) values over each infant’s first 28 days to determine if abnormal thermal gradients, or CPTd values of < 0⁰ C and/or > 2⁰ C were related to the onset of infection. [23] Body temperatures were measured every minute using a thermistor (disposable skin sensor, 499B, Cincinnati Sub Zero, Cincinnati, OH) attached to each infant’s abdominal/flank area, for central temperatures and one to the foot for peripheral temperatures. Temperatures were measured, stored, and downloaded from a research data logger (Squirrel SQ2010, Grant Instruments, Cambridge, England). Infants were enrolled within 6 hours of birth and included if at least 24 weeks’ but born prior to reaching 32 weeks’ GA by obstetrical dating, and if they weighed between 500 and 1500 grams at birth. Analyses related to temperature measures and the onset of infection are ongoing.
Infants were hospitalized in one of five hospitals, each with a level IV regional NICU servicing many counties from central and eastern North Carolina and central and coastal South Carolina. Each NICU has several attending neonatologists, and all NICUs had care teams consisting of nurses, respiratory therapists, neonatal nurse practitioners, and physicians. All NICUs have standards dictating the use of double walled incubators to care for their infants and infants are on cardio-pulmonary monitors. This study enrolled infants beginning in 2019, through the pandemic years of 2020-2021, and completed enrollment in December 2023. Although enrollment greatly decreased during the pandemic, most units continued to enroll infants and our experiences with this study during the pandemic are published [24].
All clinical context data were entered into a REDCap [25] database built for this study which included maternal obstetrical history and delivery details, infant morbidities, medical treatments, feedings, radiology reports, and disposition at discharge, transfer or death. Morbidity data included any suspected infection, type of cultures obtained, results, and treatment for infection. In all NICUs, standard of care is to respond to signs and symptoms of infection reported by an infant’s bedside nurse with laboratory testing to rule out infection and most often, broad-spectrum antibiotics are initiated for at least a 36 hour-time period while waiting for culture results. Signs that a preterm may have an infection include apnea and bradycardia, feeding intolerance, lethargy, temperature instability including hypothermia, and the need for respiratory support [15].
3. Results
Between June 2019 and December 2023, 367 infants met the inclusion criteria and were enrolled for study measures. The first infant at each NICU was excluded from analysis. The remaining sample totaled 362 infants. These infants were 63.5% Black (n=226), 30.8% White (n=107) and the remaining 29 infants were classified as American Indian, Asian, Hispanic, or other. Infants were 50.5% female and ranged between 24-32 weeks’ GA at birth, with a mean of 27.67 weeks (SD 2.09). Birthweight ranged from 500 to 1490 grams, with a mean of 986.74 (SD 259.39) grams. BPT infants averaged 970.03 grams at birth, (SD 257.11) and 27.68 (SD 2.08) weeks GA compared to WPT infants in this study with a mean birthweight of 1006.25 grams (SD 257.77) and 27.66 (SD 2.02) weeks GA. Overall mortality in this study was 6.0%, with that of BPT infants at 7.0% and WPT infants at 5.6%.
3.1. Maternal Morbidities
In this sample, there were no stark differences between delivery mode with 75.1% of Black mothers and 78.4% of White mothers being delivered of their preterm infant by caesarean section. Almost all mothers stated they had received prenatal care prior to delivery of their infant (97.8% Black women, 98.2% White women). More Black mothers cultured positive for GBS prior to delivery than White mothers (23.7% vs 18.6%) and similarly, more Black mothers were diagnosed with chorioamnionitis than White mothers (15.2% vs 9.8%). However, the incidence of PROM was approximately equal between Black and White mothers (32.6% vs 32.7%).
During pregnancy, Black women had preeclampsia less often than White women (31% vs 36.3%) but had twice the incidence of gestational diabetes compared to White women (7.7% vs 3.5%). Black women had a much higher incidence of cardiovascular disease prenatally (13.7% vs 4.4%), renal disease (0.8% vs 0), and a slightly higher incidence of diabetes (8.6% vs 7%).
3.2. Infant Infections
3.1.1. Early Onset Sepsis
In this sample, there were seven infants with confirmed, culture-positive early onset infection. Five BPT infants had EOS: three infants with E. Coli, one infant with E. Coli and S. capitus, and one infant with S. capitus; and one WPT infant with S. hominis. One infant of other race/ethnicity was diagnosed with Candida. See Figure 1. The incidence of EOS was 1.9% of the enrolled infants, with BPT infants having a 2.2% incidence and WPT infants having 0.9% incidence. All infants with EOS had a mean birthweight of 915.29 grams and GA of 26.4 weeks (see Table 1). All gram-negative infections occurred in BPT infants, with one of those infants dying at two days of age (female infant, birthweight of 670 grams and 25 weeks GA).
3.1.2. Late Onset Sepsis
LOS occurred in 10.8% of the enrolled infants, with 39 infants having a bacterial or fungal infection (see Figure 2) prior to discharge, transfer, or death. In total, there were 54 separate infections amongst the 39 infants, with some infants having multiple infections of the blood. LOS occurred in 11.9% of BPT infants versus 9.3% of WPT infants. Infants who acquired LOS were smaller at birth compared to infants who did not acquire LOS, with BPTs mean birthweight at 773.44 grams versus WPTs mean at 788.2 grams average. Their counterparts who did not acquire LOS: BPTs 996.7 grams versus WPT infants 1028.73 grams; however, disparities remain between the Black and White infants over these trends (see Table 1). Of all 27 BPT infants with LOS cases, there were 22 instances of infection with gram-positive bacteria and 9 instances of gram-negative bacteria. For the 10 WPT infants with LOS, there were 8 infections with gram-positive bacteria and 3 infections with gram-negative bacteria. Both BPT and WPT infants had ~ 8% gram-positive LOS and 3% gram-negative LOS; however, 82% of all gram-negative LOS episodes occurred in BPTs. Moreover, out of the 23 deaths that occurred in enrolled infants, 10 occurred in BPT infants diagnosed with infection. The six WPT infants who died had no positive blood cultures and died of NEC, cardio-pulmonary issues, or neurologic issues. There were 28 instances of Staphylococcus (capitus, epidermidis, haemolyticus, hominis) which may be recognized as normal skin flora or deemed to be contaminants. Other gram-positive LOS cases included 1 BPT infant with Enterococcus faecalis, 6 cases of S. Aureus in 5 BPT and 1 WPT infant, and 1 case of Streptococcus and 1 case of Stenotrophomonas, both in BPT infants. Additionally, there were 2 cases of Candida positive blood cultures, both in BPT infants and both in the same enrollment unit.
3.1.3. Urinary Tract Infections
Twenty-three infants, or 6.4% of the sample had positive urinary tract cultures in this study with 27 bacterial readings provided. This rate of urinary tract infections is similar to that found in other studies [26]. Of these, 78% were in BPT infants. Only four samples identified Staphylococcus contaminants: 5 gram-negative bacteria including Citrobacter, E. Coli, Enterobacter, Klebsiella, and Proteus mirabilis as well as Enterococcus faecalis in addition to contaminant Staphylococcus. Of note, three infants with urinary tract infections identified, also had NEC (two BPT and one WPT infants), and two of those infants, both BPTs, died.
3.1.4. Respiratory Tract Infections
Not all enrollment units use culturing of tracheal aspirates or nares as surveillance for respiratory tract infections as standard management; however, two NICUs reported one positive respiratory tract culture, one NICU reported three, and one NICU reported 14 positive respiratory cultures. Of the 19 infants with positive cultures, 12 were BPTs, 6 were WPTs, and 1 was other than Black or White. In addition to all bacteria cultured in urinary tract infections (listed above in section 3.1.3) including Stenotrophomonas and Proteus, there was one respiratory culture positive for adenovirus.
3.1.5. Cerebral Spinal Fluid Infections
There were two BPT infants diagnosed with positive CSF infections. A 570-gram male BPT infant born at 24 weeks’ GA, had a positive culture for Candida in the blood on day of life 5, CSF on day of life 7 with death at 12 days of age from multiorgan failure, coagulopathy, and metabolic acidosis due to sepsis. A BPT female infant born at 700 grams, 24 weeks GA had EOS with E. Coli and a CSF infection with Paenibacillus spp. on day of life 2. This infant was discharged home at 5 months of age, with an intraventricular hemorrhage of a left grade II and right grade I, with resolution by 2 months of age.
3.1.6. Necrotizing Enterocolitis
Infants were diagnosed with NEC in four out of five enrolling NICUs; NEC diagnosis was declared through abdominal radiographs surveying for pneumatosis and/or free air in the peritoneum. There were 21 NEC diagnoses assigned or 5.8% incidence, with 14 BPT, 5 WPT, and 2 other than Black or White infants with NEC. The incidence among BPT infants in this sample was 6.1% versus 4.7% in WPT infants. Overall, the incidence of mortality amongst the NEC cases was 47.6%, which was approximately the same between BPTs and WPTs. Of the NEC cases, seven infants also had co-occurrence of bacterial infections in blood, two of those infants had positive cultures in blood and urine, and one infant had positive blood and respiratory cultures. These bacteria in the blood included E. Coli, methicillin-resistant S. Aureus (MRSA), S. aureus, Serratia, Streptococcus and Candida, as well as three cultures with S. capitus. Urine bacteria included E. Coli, Enterococcus faecalis, and MRSA and one infant had Serratia in the blood and Serratia, S. aureus and Stenotrophomonas in the respiratory tract. Of the infants with NEC, there were 10 deaths including 6 BPT, 2 WPT, and 2 other than Black or White infants. Of the seven infants that had NEC with sepsis, five infants did not survive; all were BPT infants with gram-positive infections including two with only S. capitus which can be a contaminant.
4. Discussion
Study results from this observational trial of 362 preterm infants, born less than 32 weeks GA and less than 1500 grams birthweight reveals that disparities between NICU course, morbidity and mortality outcomes continue to exist between Black and White preterm infants. Our enrollment period took 55 months to meet our enrollment goal, due to the existence of the coronavirus disease outbreak in 2019, which caused a global pandemic beginning in March 2020 and into 2023. This study intended to observe infants for the onset of infection, and although enrollment began in 2019, our study is limited by reduced enrollment during many months and altered infection control procedures across several of our enrollment NICUs put in place due to the pandemic with reduced or no visitation, all of which is outlined in a previously published paper [24]. Despite enrollment during all of the pandemic months and beyond, our incidence of EOS (1.9%) is only slightly higher than that of studies prior to the pandemic [16] and like these studies, we found E. Coli to be the most prevalent cause for EOS. Our overall incidence of LOS (10.8%) is lower than recent trends [27] which may reflect the strict infection control procedures in many of our enrollment units during the pandemic. Masking, increased handwashing, and limited visitation may have decreased spread of nosocomial infections; although, this hypothesis has been studied and found to have no effect on hospital acquired infections [28,29] which highlights the need to be continuously vigilant to reduce LOS in preterms.
With EOS and LOS, BPT infants were at a higher risk of infection than their WPT counterparts. Although sepsis rates for very preterm infants are decreasing, studies are showing faster declines in rates of sepsis for BPT compared to WPT infants [10]; our study confirms rates of EOS, LOS, NEC, and morality remain higher for BPT infants compared to WPT infants, similar to Boghossian et al. [30]. It is interesting that in both the EOS and LOS comparison groups, BPT infants averaged a lower birthweight compared to WPT infants, which may place them at a slightly higher risk. Although the difference is 19.26 grams, the SD is only 0.6 different and the GA in both groups is approximately the same. Perhaps this difference reflects social determinants of health effects on the BPT infants’ group in this study compared to the WPT infants. Our enrollment NICUs were all North and South Carolina, evenly divided between urban and rural areas. Investigators have attempted to account for the difference in the preterm birthrate in Black individuals compared to their White counterparts, without definitive pathways [31]. Our enrollment was 63.5% Black versus 30.8% White, in the areas of NC and SC, which are both approximately 60% White individuals versus 25% Black individuals. Researchers also posit that the only plausible explanation for the differences in the preterm birth rate between Black and White individuals is racism, with biology, social determinants, immune response, and stress only contributing a small portion of the pathogenesis [32].
With this study, we see stark differences in the pathogens causing sepsis in BPT and WPT infants. BPT infants were more likely to be infected with gram-negative bacteria, which are associated with significant mortality [33]. Researchers have found non-White race as a risk factor for gram-negative infections [34]. In studies of central catheter-associated bloodstream infection events, Black patients are more likely to acquire an infection than White patients [35]. As with other studies [36], E. Coli was the most prevalent type of gram-negative bacteria associated with LOS, EOS and one of the bacterial meningitis cases in our cohort. Three of the deaths in this sample can also be attributed to E. Coli sepsis. Research is showing a strain of E. Coli is multi-drug resistant [37]. Clinicians now must monitor response to antibiotics and search for the right treatment to resistant E. Coli infections. Research shows that the proportion of extended spectrum beta-lactamase (ESBL)-producing strains of E. Coli is rising to the level of over 60% as recently as 2021 [36].
In our study, there were 28 instances of Staphylococcus (capitus, epidermidis, haemolyticus, hominis), which many clinicians deem to be normal skin flora or contaminants. However, in this cohort, four infants with these bacteria in their blood cultures died during this study, and in two cases, infants ONLY grew S. capitus from the blood culture and had NEC diagnosed prior to death. A research team from the United Kingdom conducted a retrospective study to determine if S. capitus infections lead to worse outcomes in very preterm infant but found no differences in mortality or outcomes with S. epidermidis, S. capitus, S. haemolyticus and S. warneri [38]. Researchers have also identified S. capitis strains that belong to NRCS-S clone subgroups, which may lead to virulent LOS and poor outcomes [39]. As in our study, CONs is a prevalent bacteria growing out of blood cultures [40] and in this study, 10 infants had S. capitus identified in their blood cultures; therefore, it may be difficult to discern if the CONs is a contaminant or infection that may lead to poor outcomes. More research is needed to investigate CON infections and their virulence so clinicians can manage this bacterium in the blood of fragile NICU patients effectively.
Researchers have identified the most common bacterial pathogens as Enterococcus spp. (20%), E. Coli (19%) and Klebsiella spp. (18%) in the urinary tract [26]. In our study, Proteous mirabilis caused a urinary tract infection in a 624-gram, male WPT infant and a concordant respiratory tract infection. This is a gram-negative bacteria can be found in the human intestines and is associated with urinary stones [41]. One urinary tract infection cultured mycoplasma and ureaplasma, which are bacteria common to the genital tract; ureaplasma was also identified in one respiratory tract infection. Researchers have linked ureaplasma with an increased incidence of bronchopulmonary dysplasia (BPD) [42].
In our study, local NICU standards dictated whether or not to culture tracheal aspirates. This practice has been debated for many years. The practice in this study yielded 19 positive cultures, with nine gram-negative pathogens. There was one 812-gram, 26 week GA, WPT male infant whose culture grew Serratia, S. aureus and Stenotrophomonas and developed NEC. Studies have shown an association between gram-negative bacteria in the tracheal aspirate and developing severe BPD in infants less than 26 weeks’ GA [43]. More research is needed to determine if respiratory cultures or tracheal aspirate cultures should and can be used in medical management of very preterm infants.
This sample had one case where a BPT female infant born at 700 grams was found to have Paenibacillus meningitis on the second day of life and yet, this infant went on to recover and was discharged home at 5 months of age. A review revealed Paenibacillus sepsis and meningitis to be rare in very preterm infants and most cases reported lead to increased mortality [44,45]. Of note, this BPT female had an EOS with E. Coli as well, for which she was treated with ampicillin, gentamicin, and erythromycin. Two days later, cefotaxime was added to the treatment. Three days later, when Paenicbacillus spp. was cultured from the CSF, antibiotics were changed to gentamicin and cefotaxime, with gentamicin discontinued the next day. The infant was treated with additional antibiotics ending at 3 weeks of age with no other incidence of infection.
The incidence of NEC in this study was within the current prevalence at 5.8% [46]. As with other studies [47], we found racial disparities amongst our NEC cases, with BPT infants having a higher incidence of NEC at 6.1% versus WPT infants at 4.7%. Researchers have found that smaller birthweight is a risk factor for NEC [48]. BPT infants in our study averaged a lower birthweight compared to WPT infant, with approximately the same mean GA. Other possible causes include social, cultural, education, economic and environmental factors according to Cuna et al. [47]. Our study was not constructed to evaluate factors for social determinants of health; however, future research could examine the interplay between social determinants and infections/NEC outcomes by race.
5. Conclusions
In our study of 362 very preterm infants, we have showed racial disparities exist in infection outcomes, NEC, and mortality from data gathered in five NICUs in North and South Carolina. The study shows incidence within published incident rates for EOS, LOS, and NEC with bacteria prevalent from the blood, urinary tract, trachea, and CSF comparable from studies across the United States. Importantly, BPT infants in this study dealt with many more gram-negative infections than their WPT infant peers, with lower body weights and their overall mortality rate was higher than the entire study sample and their WPT peers. Examining racial disparities across neonatal intensive care and health outcomes is urgent to decrease morbidity and mortality for BPT infants.
Author Contributions
Conceptualization, R.D.; methodology, R.D.; software, R.D. and K.E.; validation, R.D., K.E., and K. W. ; formal analysis, R. D.; investigation, W. C., K. F., V. I., H. S., K. E., and K. W.; resources, R. D. ; data curation, W. C., K. F., V. I., H. S., K. E., and K. W.; writing—original draft preparation, R. D.; writing—review and editing, K. E., W. C., K. F., V. I., H. S., and K. W.; visualization, R. D.; supervision, R. D.; project administration, R. D.; funding acquisition, R. D. All authors have read and agreed to the published version of the manuscript. Robin Dail: R.D.; Kayla Everhart, K. E.; Weili Chang, W. C.; Kimbereley Fisher, K. F.; Victor Iskersky, V. I.; Karen Warren, K. W.; Heidi Steflik, H. S.
Funding
This research was funded by National Institute of Health/National Institute of Nursing Research, grant number 1R01NR017872.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Medical University of South Carolina (protocol code 82482, initial date of approval November 6, 2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is being analyzed. Please contact Robin B. Dail, PhD, RN, FAAN @ rdail@mailbox.sc.edu to inquire about data access.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hamilton BE, Martin JA, Osterman MHS, Curtin SC, Mathews TJ, Statistics DoV. Births: Final Data for 2014. National Vital Statistics Reports. 2015, 64. [Google Scholar]
- Martin JA, OM. Exploring the decline in the singleton preterm birth rate in the United States, 2019–2020. Hyattsville, MD: Centers for Disease Control and Prevention (CDC), Statistics NCfH; 2022 2022.
- Matthews TJ, MacDorman MF, Thoma ME. Infant Mortality Statistics From the 2013 Period Linked Birth/Infant Death Data Set. National vital statistics reports. 2015, 64, 1–30. [Google Scholar]
- Fanaroff A, Hack M, Walsh M. The NICHD neonatal reseach network: changes in practic adn outcomes during the first 15 years. Seminars in Neonatology. 2003, 27, 281–287. [Google Scholar] [CrossRef]
- Ertugrul S, Aktar F, Yolbas I, Yilmaz A, Elbey B, Yildirim A, et al. Risk Factors for Health Care-Associated Bloodstream Infections in a Neonatal Intensive Care Unit. Iran J Pediatr. 2016, 26, e5213. [Google Scholar] [CrossRef]
- Kurek Eken M, Tuten A, Ozkaya E, Karatekin G, Karateke A. Major determinants of survival and length of stay in the neonatal intensive care unit of newborns from women with premature preterm rupture of membranes. The journal of maternal-fetal & neonatal medicine: the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstet. 2017, 30, 1972–1975. [Google Scholar]
- Janevic T, Zeitlin J, Auger N, Egorova NN, Hebert P, Balbierz A, et al. Association of Race/Ethnicity With Very Preterm Neonatal Morbidities. JAMA Pediatrics. 2018, 172, 1061. [Google Scholar] [CrossRef]
- Assari, S. Social Epidemiology of Perceived Discrimination in the United States: Role of Race, Educational Attainment, and Income. Int J Epidemiol Res. 2020, 7, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Millender E, Barile JP, J RB, Harris RM, De Faria L, Wong FY, et al. Associations between social determinants of health, perceived discrimination, and body mass index on symptoms of depression among young African American mothers. Arch Psychiatr Nurs. 2021, 35, 94–101. [Google Scholar] [CrossRef]
- Travers CP, Carlo WA, McDonald SA, Das A, Ambalavanan N, Bell EF, et al. Racial/Ethnic Disparities Among Extremely Preterm Infants in the United States From 2002 to 2016. JAMA network open. 2020, 3, e206757. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine Committee on Understanding Premature B, Assuring Healthy O. The National Academies Collection: Reports funded by National Institutes of Health. In: Behrman RE, Butler AS, editors. Preterm Birth: Causes, Consequences, and Prevention. Washington (DC): National Academies Press (US) Copyright © 2007, National Academy of Sciences.; 2007.
- Xu X, Grigorescu V, Siefert KA, Lori JR, Ransom SB. Cost of racial disparity in preterm birth: evidence from Michigan. J Health Care Poor Underserved. 2009, 20, 729–747. [Google Scholar] [CrossRef]
- Sheikh F, Douglas W, Catenacci V, Machon C, Fox-Robichaud AE. Social Determinants of Health Associated With the Development of Sepsis in Adults: A Scoping Review. Crit Care Explor. 2022, 4, e0731. [Google Scholar] [CrossRef] [PubMed]
- Greenberg RG, Kandefer S, Do BT, Smith PB, Stoll BJ, Bell EF, et al. Late-onset Sepsis in Extremely Premature Infants: 2000-2011. The Pediatric infectious disease journal. 2017, 36, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Cohen R, Romain O, Tauzin M, Gras-Leguen C, Raymond J, Butin M. Neonatal bacterial infections: Diagnosis, bacterial epidemiology and antibiotic treatment. Infect Dis Now. 2023, 53, 104793. [Google Scholar] [CrossRef]
- Stoll BJ, Puopolo KM, Hansen NI, Sánchez PJ, Bell EF, Carlo WA, et al. Early-Onset Neonatal Sepsis 2015 to 2017, the Rise of Escherichia coli, and the Need for Novel Prevention Strategies. JAMA Pediatr. 2020, 174, e200593. [Google Scholar] [CrossRef] [PubMed]
- Dey AC, Hossain MI, Afroze S, Dey SK, Mannan MA, Shahidullah M. A Survey on Current Practice of Management of Early Onset Neonatal Sepsis. Mymensingh Med J. 2016, 25, 243–247. [Google Scholar]
- Guo L, Han W, Su Y, Wang N, Chen X, Ma J, et al. Perinatal risk factors for neonatal early-onset sepsis: a meta-analysis of observational studies. The journal of maternal-fetal & neonatal medicine: the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstet. 2023, 36, 2259049. [Google Scholar] [CrossRef]
- Boghossian NS, Page GP, Bell EF, Stoll BJ, Murray JC, Cotten CM, et al. Late-onset sepsis in very low birth weight infants from singleton and multiple-gestation births. The Journal of pediatrics. 2013, 162, 1120–1124.e1. [Google Scholar] [CrossRef]
- Köstlin-Gille N, Härtel C, Haug C, Göpel W, Zemlin M, Müller A, et al. Epidemiology of Early and Late Onset Neonatal Sepsis in Very Low Birthweight Infants: Data From the German Neonatal Network. The Pediatric infectious disease journal. 2021, 40, 255–259. [Google Scholar] [CrossRef]
- Dong Y, Speer CP. Late-onset neonatal sepsis: recent developments. Archives of disease in childhood Fetal and neonatal edition. 2015, 100, F257–F263. [Google Scholar] [CrossRef]
- Coggins SA, Glaser K. Updates in Late-Onset Sepsis: Risk Assessment, Therapy, and Outcomes. Neoreviews. 2022, 23, 738–755. [Google Scholar] [CrossRef]
- Dail RB, Everhart KC, Hardin JW, Chang W, Kuehn D, Iskersky V, et al. Predicting Infection in Very Preterm Infants: A Study Protocol. Nursing research. 2021, 70, 142–149. [Google Scholar] [CrossRef]
- Nist MD, Casavant SG, Dail RB, Everhart KC, Sealschott S, Cong XS. Conducting Neonatal Intensive Care Unit Research During a Pandemic: Challenges and Lessons Learned. Nursing research. 2022, 71, 147–152. [Google Scholar] [CrossRef]
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of biomedical informatics. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Kilpatrick R, Boutzoukas AE, Chan E, Girgis V, Kinduelo V, Kwabia SA, et al. Urinary Tract Infection Epidemiology in NICUs in the United States. American journal of perinatology. 2023. [Google Scholar] [CrossRef]
- Horbar JD, Greenberg LT, Buzas JS, Ehret DEY, Soll RF, Edwards EM. Trends in Mortality and Morbidities for Infants Born 24 to 28 Weeks in the US: 1997-2021. Pediatrics. 2024, 153, e2023064153. [Google Scholar] [CrossRef] [PubMed]
- Tham N, Fazio T, Johnson D, Skandarajah A, Hayes IP. Hospital Acquired Infections in Surgical Patients: Impact of COVID-19-Related Infection Prevention Measures. World Journal of Surgery. 2022, 46, 1249–1258. [Google Scholar] [CrossRef]
- Abubakar U, Awaisu A, Khan AH, Alam K. Impact of COVID-19 Pandemic on Healthcare-Associated Infections: A Systematic Review and Meta-Analysis. Antibiotics. 2023, 12, 1600. [Google Scholar] [CrossRef]
- Boghossian NS, Geraci M, Lorch SA, Phibbs CS, Edwards EM, Horbar JD. Racial and Ethnic Differences Over Time in Outcomes of Infants Born Less Than 30 Weeks' Gestation. Pediatrics. 2019, 144, e20191106. [Google Scholar] [CrossRef] [PubMed]
- Manuck, TA. Racial and ethnic differences in preterm birth: A complex, multifactorial problem. Seminars in perinatology. 2017, 41, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Braveman P, Dominguez TP, Burke W, Dolan SM, Stevenson DK, Jackson FM, et al. Explaining the Black-White Disparity in Preterm Birth: A Consensus Statement From a Multi-Disciplinary Scientific Work Group Convened by the March of Dimes. Front Reprod Health. 2021, 3, 684207. [Google Scholar] [CrossRef]
- Wang W, Jiang T, Zhang W, Li C, Chen J, Xiang D, et al. Predictors of mortality in bloodstream infections caused by multidrug-resistant gram-negative bacteria: 4 years of collection. Am J Infect Control. 2017, 45, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Bock A, Hanson BM, Ruffin F, Parsons JB, Park LP, Sharma-Kuinkel B, et al. Clinical and Molecular Analyses of Recurrent Gram-Negative Bloodstream Infections. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2023, 76, e1285–e1293. [Google Scholar] [CrossRef] [PubMed]
- McGrath CL, Bettinger B, Stimpson M, Bell SL, Coker TR, Kronman MP, et al. Identifying and Mitigating Disparities in Central Line-Associated Bloodstream Infections in Minoritized Racial, Ethnic, and Language Groups. JAMA Pediatr. 2023, 177, 700–709. [Google Scholar] [CrossRef]
- Zhu M, Wang L, Zhuge Z, Li W, Zheng Y, Mai J, et al. Risk Factors Associated with Multi-Drug Resistance in Neonatal Sepsis Caused by Escherichia coli. Infect Drug Resist. 2023, 16, 2097–2106. [Google Scholar] [CrossRef]
- Malaure C, Geslain G, Birgy A, Bidet P, Poilane I, Allain M, et al. Early-Onset Infection Caused by Escherichia coli Sequence Type 1193 in Late Preterm and Full-Term Neonates. Emerg Infect Dis. 2024, 30, 20–28. [Google Scholar] [CrossRef]
- Yuan JM, Nugent C, Wilson A, Verlander NQ, Alexander E, Fleming P, et al. Clinical outcomes of Staphylococcus capitis isolation from neonates, England, 2015-2021: a retrospective case-control study. Archives of disease in childhood Fetal and neonatal edition. 2023.
- Chavignon M, Coignet L, Bonhomme M, Bergot M, Tristan A, Verhoeven P, et al. Environmental Persistence of Staphylococcus capitis NRCS-A in Neonatal Intensive Care Units: Role of Biofilm Formation, Desiccation, and Disinfectant Tolerance. Microbiol Spectr. 2022, 10, e0421522. [Google Scholar] [CrossRef]
- [A multicenter prospective cohort study of late-onset sepsis and its poor prognosis in very low birth weight infants]. Zhonghua Er Ke Za Zhi. 2023, 61, 228–234. [CrossRef]
- Szczerbiec D, Słaba M, Torzewska A. Substances Secreted by Lactobacillus spp. from the Urinary Tract Microbiota Play a Protective Role against Proteus mirabilis Infections and Their Complications. Int J Mol Sci. 2023, 25, 103. [Google Scholar] [CrossRef]
- Gobec K, Mukenauer R, Keše D, Erčulj V, Grosek Š, Perme T. Association between colonization of the respiratory tract with Ureaplasma species and bronchopulmonary dysplasia in newborns with extremely low gestational age: a retrospective study. Croat Med J. 2023, 64, 75–83. [Google Scholar] [CrossRef]
- Imanishi Y, Hirata K, Nozaki M, Mochizuki N, Hirano S, Wada K. The Association between Early Gram-Negative Bacteria in Tracheal Aspirate Cultures and Severe Bronchopulmonary Dysplasia among Extremely Preterm Infants Requiring Prolonged Ventilation. American journal of perinatology. 2023, 40, 1321–1327. [Google Scholar] [CrossRef]
- Hunt B, Rogers C, Blais RM, Adachi K, Sathyavagiswaran L. Paenibacillus Sepsis and Meningitis in a Premature Infant: A Case Report. Am J Forensic Med Pathol. 2021, 42, 96–98. [Google Scholar] [CrossRef] [PubMed]
- DeLeon SD, Welliver RC, Sr. Paenibacillus alvei Sepsis in a Neonate. The Pediatric infectious disease journal. 2016, 35, 358. [Google Scholar] [CrossRef] [PubMed]
- Hu X, Liang H, Li F, Zhang R, Zhu Y, Zhu X, et al. Necrotizing enterocolitis: current understanding of the prevention and management. Pediatr Surg Int. 2024, 40, 32. [Google Scholar] [CrossRef] [PubMed]
- Cuna A, Sampath V, Khashu M. Racial Disparities in Necrotizing Enterocolitis. Front Pediatr. 2021, 9, 633088. [Google Scholar] [CrossRef]
- Ree IM, Smits-Wintjens VE, Rijntjes-Jacobs EG, Pelsma IC, Steggerda SJ, Walther FJ, et al. Necrotizing enterocolitis in small-for-gestational-age neonates: a matched case-control study. Neonatology. 2014, 105, 74–78. [Google Scholar] [CrossRef]
Figure 1.
Early Onset Infections for 7 infants.
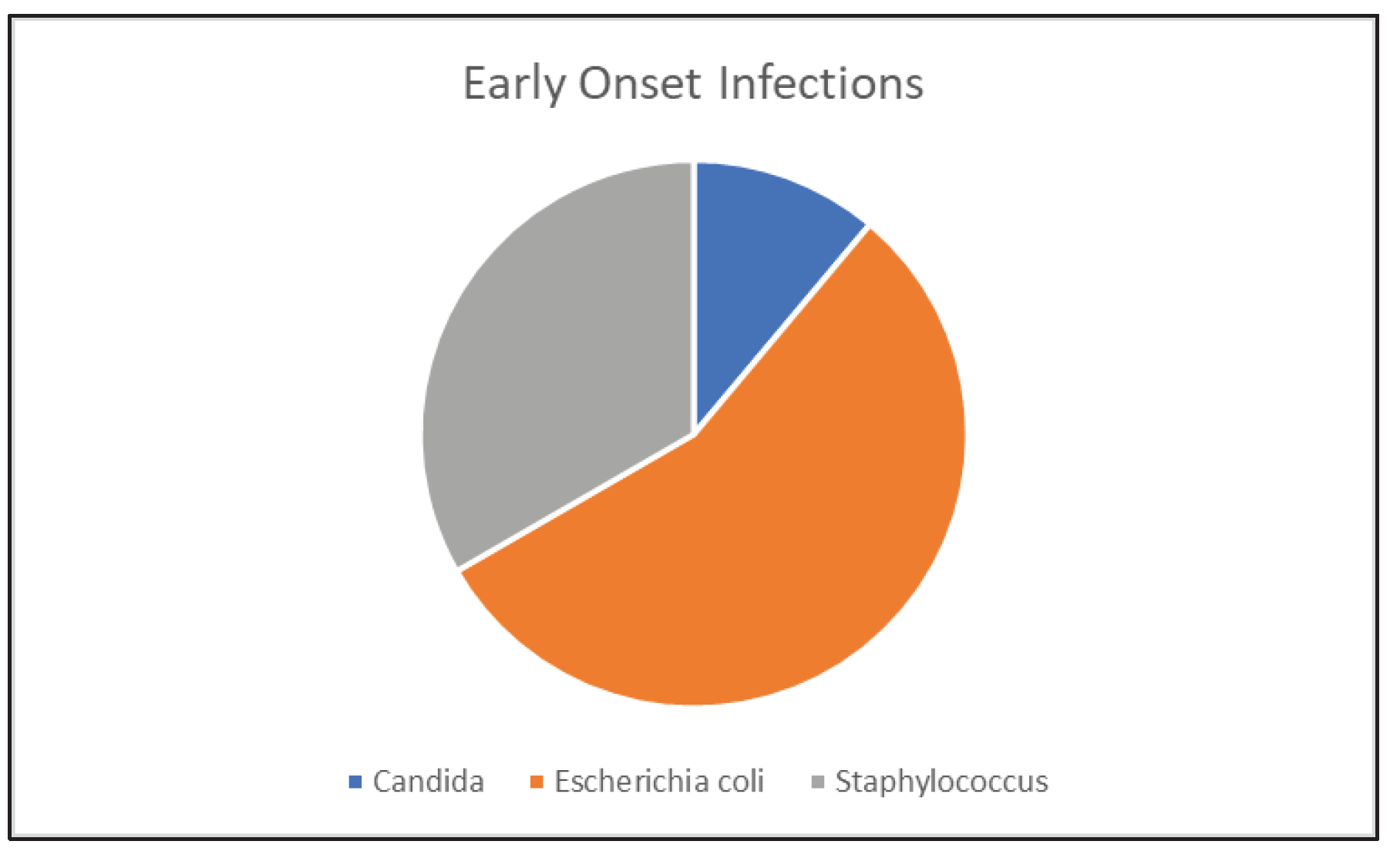
Figure 2.
Late Onset Infections for 39 infants. Footnote: Staphylococcus species: S. capitus, S. epidermidis, S. haemolyticus, S. hominis, normal flora, possible contaminants.
Figure 2.
Late Onset Infections for 39 infants. Footnote: Staphylococcus species: S. capitus, S. epidermidis, S. haemolyticus, S. hominis, normal flora, possible contaminants.
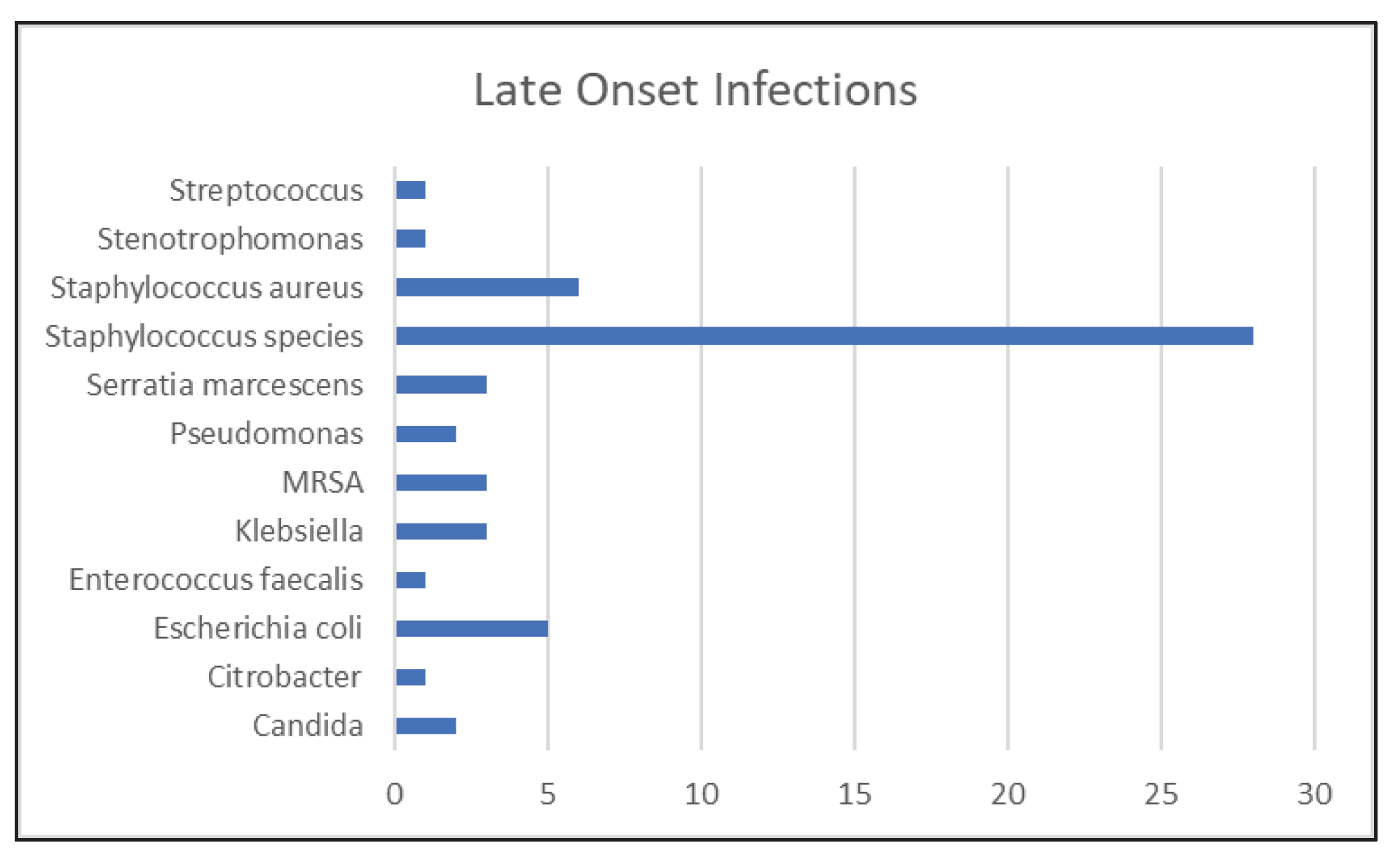

Table 1.
Demographics for Black and White Preterms with Positive Blood Cultures Key: BW: birthweight in grams; SD: standard deviation; GA: gestational age in weeks.
Table 1.
Demographics for Black and White Preterms with Positive Blood Cultures Key: BW: birthweight in grams; SD: standard deviation; GA: gestational age in weeks.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



