
Submitted:
04 February 2024
Posted:
05 February 2024
You are already at the latest version
Abstract
Background. Implementing mammogram screening means that clinicians are seeing many breast cancers that will never develop metastases. The purpose of this study was to identify subgroups of breast cancer patients who did not present events related to long-term breast cancer mortality, taking into account diagnosis at breast screening, absence of palpability and axillary involvement, and genomic analysis with PAM50.
Patients and Methods. To identify them, a retrospective observational study was carried out selecting patients without palpable tumour, without axillary involvement, and a genomic analysis was performed with PAM50.
Results. The probability of distant metastasis-free interval (DMFI) of 337 patients was 0.92 (95% CI, 0.90-0.93) at 20 years and 0.96 (95% CI, 0.92-1.00) in 95 patients (28%) with available PAM50 tests. In 22 (23.15%) luminal A tumours and in 9 (9.47%) luminal B tumours smaller than 1 cm and in HER2 and basal type tumours there were no metastatic events (20-year DMFI of 1.00).
Conclusion. Patients with nonpalpable breast cancer found at screening with negative nodes are at very low risk. It is possible to identify subgroups without metastatic events by determining the intrinsic subtype and tumour size less than 1 cm. De-escalation of treatment should be considered.
Keywords:
Low-risk breast cancer
; Metastasis
; Observational study
; Screening
1. Introduction
The expansion in breast screening (mammogram) programmes has resulted in clinicians seeing a large number of very early-stage breast cancers [1]. Advertising emphasises the benefits of detecting these preclinical lesions because intuition tells us that early-stage treatment of breast cancer should facilitate treatment and cure [2].
Mammography, as an effective screening test for breast cancer, should not only increase the incidence of preclinical disease, but should also decrease the incidence of metastatic cancer and cancer-related mortality. Otherwise, early detection efforts may be uncovering a reservoir of non-progressive, or very slowly progressive, breast cancers that were not destined to cause symptoms for the rest of the woman's life, nor her death, a phenomenon known as overdiagnosis [3].
If cancer is detected, it is impossible to know who has been overdiagnosed, as it is not possible to know how it would have evolved in the absence of screening. However, from the point of view of the clinician caring for these patients with very early breast cancer detected on screening mammography, it would be essential to be able to identify those whose diagnosis will have no impact on mortality because this would allow their treatment to be de-escalated in some way. To do so, the first requirement would be to demonstrate that a particular patient, diagnosed with breast cancer, will not have metastases, or breast cancer-related death, for an extended period of time. Secondly, the clinical, pathological and genomic characteristics of their tumours should be analysed and, thirdly, a clinical trial should be designed to de-escalate the treatments.
National registry studies can identify patients with breast cancer without any loss in life expectancy [4] and patients with certain breast cancers may have even higher relative survival than the general population if the cancer is detected incidentally or by mammogram screening, and patients also adopt other healthy behaviours (the healthy-user effect) [5].
Within the group of women diagnosed in breast screening, tumour palpability at diagnosis [6], a parameter that leads us to classify it as preclinical cancer, is a prognostic variable that helps to select those with a lower risk of developing metastases and with lower mortality [6]. Another way to identify breast cancers without a clear impact on mortality is the genomic analysis of the breast tumour. In a large prospective study, patients with ultra-low genomic risk determined by 70-gene signature (Mammaprint) had the best prognosis, with a reduced risk of distant metastasis or breast cancer-related death [7]. PAM50 intrinsic subtypes were independently prognostic for long-term breast cancer survival [8].
The purpose of this study was to identify subgroups of breast cancer patients who did not present events related to long-term breast cancer mortality, taking into account diagnosis at breast screening, absence of palpability and axillary involvement, and genomic analysis with PAM50.
2. Materials and Methods
2.1. Study Design
A retrospective, observational study of breast cancer patients from a public or opportunistic mammogram screening programme, with non-palpable breast tumours and without axillary involvement, treated in the Medical Oncology departments of two university hospitals between 2001 and 2014, was carried out.
Data related to patients and treatment received were collected retrospectively from the clinical records of the Medical Oncology departments. The Spanish register of deaths (Índice Nacional de Defunciones) was consulted for vital status and patients’ date of death.
2.2. Inclusion and Exclusion Criteria
Women seen in the oncology clinic for breast carcinoma with the following characteristics: detected during the screening programme at the asymptomatic phase with non-palpable tumour and with no other signs or symptoms directly related to the tumour, such as skin retraction, bloody nipple discharge, or others, and with negative axillary nodes in diagnostic surgery. Tumours with histologic grade 1, 2 and 3, oestrogen and progesterone receptor positive and negative, HER2 negative and positive were permitted. Males and carcinomas in situ were excluded.
2.3. Data Analysis
Molecular analysis of gene expression of 50 genes allowed the tumour to be classified into one of 4 intrinsic subtypes: luminal A, luminal B, HER2-enriched and basal-like. Formalin-fixed, paraffin-embedded tumour tissue blocks and corresponding slides were obtained and reviewed by a pathologist who marked a representative area of the tumour. Tissue samples 1 mm in thickness were obtained from the area of the block corresponding to the marked slide. Two samples per box (or one sample if the primary tumour was less than 0.7 cm in diameter) were placed in plastic tubes with an identification number and sent to the reference laboratory. Tissue samples were deparaffinised and digested for RNA extraction. After assessment of their quality and concentration, the samples were processed and recorded in nCounter®. Samples were prepared with marker and capture probes, incubated in a thermocycler and transferred to the nCounter® preparation station. The reading was performed using a digital analyser. The analysis of the expression values was performed with the bioinformatics tool nSolver®.
The events collected were ipsilateral local recurrence after conserving surgery, postmastectomy local recurrence, regional lymph node recurrence, distant metastases, second primary invasive tumours (in ipsilateral or contralateral breast and other locations) and ipsilateral or contralateral breast carcinoma in situ. The dependent variable analysed was the distant metastasis-free interval (DMFI), defined as the interval between surgery and one of the following events: distant metastasis and death from breast cancer [9] (events related to breast cancer mortality).
A descriptive analysis of the variables related to patients, breast tumour and treatment (absolute and relative frequency, mean, median and standard deviation) was performed. For the comparison of qualitative variables, the chi-square test with Fisher's correction was applied and, for quantitative variables, the Student's t-test was used.
The Kaplan Meier method and the Log-Rank test for the comparison of survival curves were used to calculate survival. Cox regression with an independent variable was used to calculate the hazard ratio. SPSS version 21 was used for statistical analysis of the data. In the statistical analysis, p<0.05 was considered to indicate statistical significance.
3. Results
3.1. Patient Characteristics
Three hundred and thirty-seven patients met the inclusion and exclusion criteria. In 31 cases (9.20%) the immunohistochemical subtype was not available, 268 (79.50%) cases were hormone-sensitive, 23 (6.80%) were triple-negative and 15 (4.40%) were HER2. Of all of them, 96 (28.40%) intrinsic subtyping was available with PAM50 (57, 60% luminal A; 26, 27% luminal B; 6, 6.30% HER2; 7, 7.40% basal-like) (Figure 1). In one luminal A subtype patient the information on events and survival was not available.
The median age was 56 years, with a range between 38 and 71. Participation in the public screening programme was from the age of 45 up until 2013, and the presence of younger women in the study (65, 19.20% premenopausal) is explained as a result of opportunistic screening. All were referred from breast screening (302, 89.30% public and 36, 10.70% opportunistic). The vast majority had full functional capacity. Of the patients, 93.20% had no or few comorbidities. Most of the carcinomas (82.50%) were of the invasive ductal type, stage I (77.20%), with a median tumour size of 1.20 cm, mean histologic grade in half of the cases and a median Ki67 proliferative index of 12%. Oestrogen receptors were positive in 88.50% of tumours and progesterone receptors in 76%. Regarding HER2, 4.40% were positive.
Some 88.80% of the women underwent breast-conserving surgery and 68.60% underwent axillary lymph node-sparing surgery. Among the patients, 73.10% were treated with adjuvant hormone therapy for 5 years, and one third with 3-6 months of adjuvant chemotherapy.
Table 1 shows the patients’ characteristics.
3.2. Event Analysis
The median follow-up of patients was 142 months (1-249). During this time, 72 patients suffered an event (21.30%), which are shown in Table 2.
In the 22 patients with tumours of luminal intrinsic subtype A and size less than 1 cm, there were no events related to breast cancer mortality. In the 34 patients with tumours of luminal intrinsic subtype A and size greater than 1 cm, there were 2 events related to breast cancer mortality. Likewise, in the 9 patients with luminal intrinsic subtype B and size less than 1 cm, there were no events related to breast cancer mortality. Again, in the 17 patients with luminal B tumours and size greater than 1 cm, there was 1 event related to breast cancer mortality.
In the 6 patients with intrinsic HER2 subtype and in the 7 with basal-like subtype, no metastatic events occurred (Table 3).
3.3. Survival Analysis
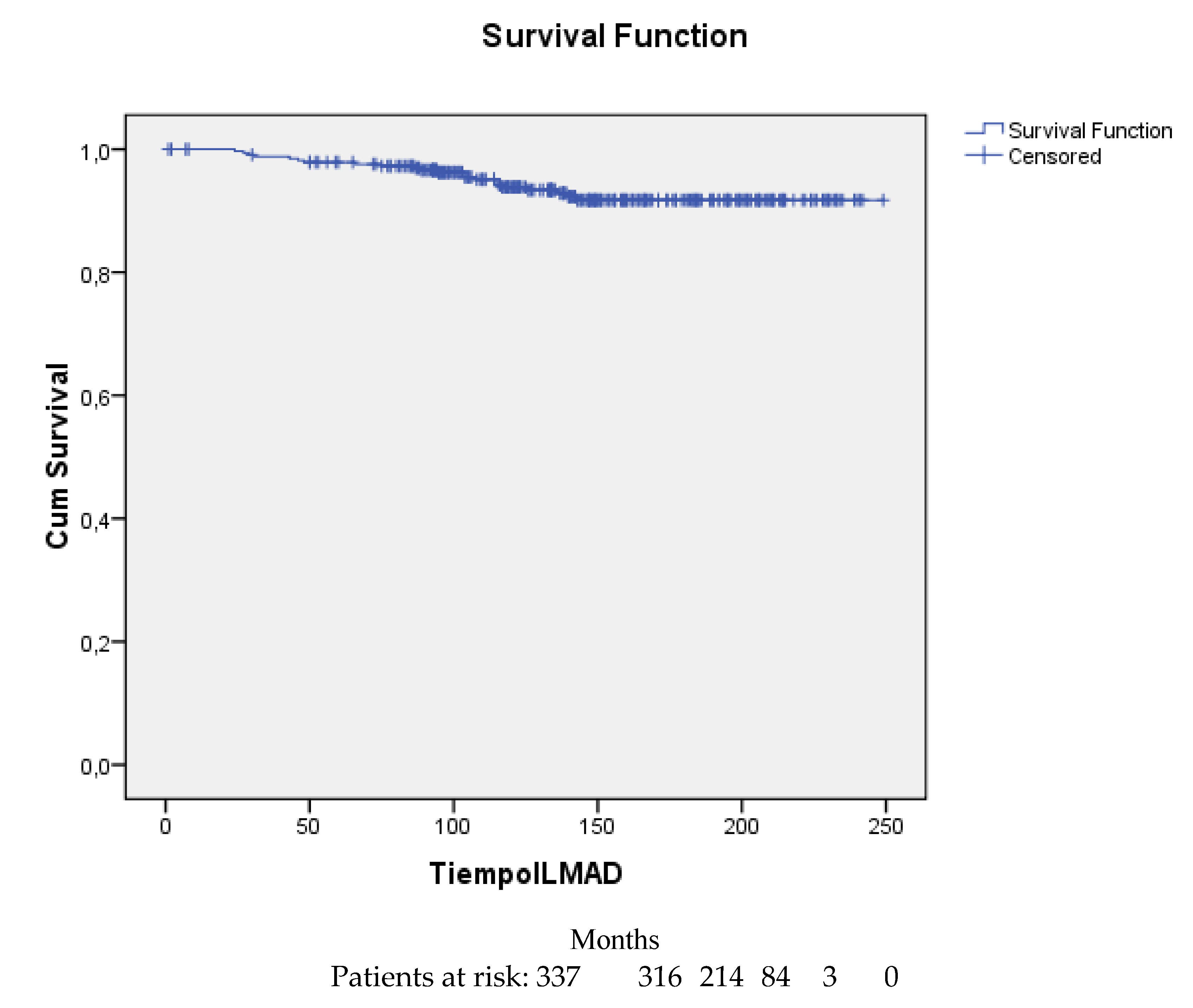
The distant metastasis-free interval probability at 5, 10, 15 and 20 years was 0.98 (95% CI, 0.96-0.99), 0.94 (95% CI, 0.91-0.97), 0.92 (95% CI, 0.90-0.93) and again 0.92 (95% CI, 0.90-0.93), respectively.
Figure 2 shows the distant metastasis-free probability curve.
Figure 2.
Distant metastasis-free interval probability curve for the 337 patients.
In the 95 patients with available intrinsic subtype determination the distant metastasis-free interval probability at 5 years was 1.00 and at 10 years, 15 years and 20 years was 0.96 (95% CI, 0.92-1.00).
Figure 3 shows the distant metastasis-free interval probability curve for the 95 patients with intrinsic subtype determined by PAM50.
4. Discussion
In this retrospective attempt to identify subgroups of breast cancer patients who did not present events related to long-term breast cancer mortality, taking into account diagnosis at breast screening, absence of palpable anomalies, and no axillary involvement, and genomic analysis with PAM50, we found that patients with luminal intrinsic subtypes A and B and tumours smaller than 1 cm (32.62%) never develop metastatic events. The low representation of HER2 (6.30%) and basal (7.30%) tumours also did not develop metastases. As has been shown before, patients with tumours smaller than 1 cm, with luminal A, HER2 and triple-negative subtypes on immunohistochemistry did not develop metastases [12].
Breast screening detects slow-growing cancers, the vast majority of which tend to be of the luminal subtype. In our study, the proportion of HER2 or basal-like breast cancers has been lower than the known proportion for all age groups [13,14]. Specifically, the age, represented by a low number of young women in our study, where the presentation of these aggressive tumour subtypes is more frequent, justifies this lower proportion of HER2 and basal tumours. Likewise, the aggressive behaviour of these rapidly growing tumour subtypes with a shorter preclinical detectable phase, justifies their lower frequency in our study as these tumours often emerge clinically between screening cycles [14]. HER2 and basal cancers detected by screening mammography are usually diagnosed at an earlier stage, and their prognosis was better than those detected by symptoms [15].
As we said in the introduction, the next step, once the subgroups of breast cancer patients who, having undergone standard treatment, will not develop metastases have been identified, would be to de-escalate the treatment. If we exclude progressive preclinical cancers [16] (HER2 and basal), the adjuvant systemic treatment of women with luminal tumours and tumours smaller than 1 cm is hormone therapy. De-escalating this treatment would be possible in this subgroup of patients because the effect of hormone therapy on the development of metastases is limited [17]. In fact, in the Mindact trial, which had an 8-year follow-up, the distant metastasis-free interval and overall survival of low-risk stage I patients treated with adjuvant hormone therapy was not statistically different from those who did not receive this treatment [17], using propensity score matching methodology to select a group of patients receiving hormone therapy and another not receiving hormone therapy. A drawback of refraining from using adjuvant hormonal therapy is that this treatment not only reduces distant relapses, but also locoregional recurrences and second contralateral or ipsilateral breast cancers [17]. As we have seen in the event analysis of our study, the number of locoregional recurrences and second primary breast tumours is similar to the number of metastases. The follow-up period of the Mindact trial of 8 years and that of our study of almost 12 years seem short due to the considerable risk of late recurrence of these luminal tumours, with recurrences up to 32 years after diagnosis [18]. For this reason, it is impractical to design a controlled clinical trial to answer research questions that require decades of follow-up and also require events that will almost never occur.
In fact, at present, de-escalation measures could already be applied in this patient population. For example, based on the SOUND non-inferiority trial [19], the results of which suggest that breast cancer patients with tumours of less than 2 cm and ultrasonographically negative axillary lymph nodes, can safely avoid any axillary surgery [19], the patients identified in our study could also be offered the choice to abstain from axillary surgery.
Likewise, women with luminal A tumours could also be offered abstinence from adjuvant radiotherapy after conserving surgery, based on the results of the LUMINA trial [20].
Finally, as we have seen [17], in patients with low-risk stage I breast cancer, the beneficial effect of hormone therapy on the distant metastasis-free interval is limited and has to be counterbalanced by its side effects [21], and should be discussed with these patients at very low risk of distant metastasis [17,21]. The Canadian LA LEAST trial compares 2 years of endocrine therapy in women over 50 years of age whose node-negative breast cancers are low risk according to the Prosigna score [22], also as a form of de-escalation. However, one must be very careful about combining several forms of de-escalation at the same time, for example, omitting radiotherapy and hormone therapy at the same time [23]. Just like for ductal carcinoma in situ [24], dose reduction of hormone therapy could be explored in this group of very low-risk patients. There are no data with dose reduction of aromatase inhibitors, but there are data with reduction to 5 mg per day of tamoxifen [24].
The strengths of this study include its large cohort of patients with long-term follow-up and reliable data based on individual medical records. However, this study suffered from biases, such as the low availability of material for the determination of the PAM50 genomic study and the biases associated with retrospective studies, such as selection bias.
5. Conclusion
Our study provides novel insights into the epidemiology of very low-risk breast cancer. Oncologists and other health care professionals should be aware that there are patients with breast cancer who will never metastasise, particularly women diagnosed on breast screening with non-palpable, luminal subtype tumours smaller than 1 cm and node negative. Our study advocates further research to optimise treatment de-escalation to prevent overtreatment.
Author Contributions
Conceptualization, Salvador Gámez-Casado and José Manuel Baena-Cañada; Data curation, Salvador Gámez-Casado, Lourdes Rodríguez-Pérez, Cristina Bandera-López, Andrés Mesas-Ruiz, Alicia Campini-Bermejo, Marta Bernal-Gómez, Manuel Zalabardo-Aguilar, Julio Calvete-Candenas, Gala Martínez-Bernal, Lidia Atienza-Cuevas, Marcial Garcia-Rojo, Encarnación Benítez-Rodríguez, Bella Pajares-Hachero, María José Bermejo-Pérez and José Manuel Baena-Cañada; Formal analysis, Manuel Zalabardo-Aguilar, Encarnación Benítez-Rodríguez and José Manuel Baena-Cañada; Funding acquisition, José Manuel Baena-Cañada; Investigation, Salvador Gámez-Casado, Lourdes Rodríguez-Pérez, Cristina Bandera-López, Andrés Mesas-Ruiz, Alicia Campini-Bermejo, Marta Bernal-Gómez, Manuel Zalabardo-Aguilar, Julio Calvete-Candenas, Gala Martínez-Bernal, Lidia Atienza-Cuevas, Marcial Garcia-Rojo, Encarnación Benítez-Rodríguez, Bella Pajares-Hachero, María José Bermejo-Pérez and José Manuel Baena-Cañada; Methodology, Salvador Gámez-Casado, Lourdes Rodríguez-Pérez, Cristina Bandera-López, Andrés Mesas-Ruiz, Alicia Campini-Bermejo, Marta Bernal-Gómez, Manuel Zalabardo-Aguilar, Julio Calvete-Candenas, Gala Martínez-Bernal, Lidia Atienza-Cuevas, Marcial Garcia-Rojo, Encarnación Benítez-Rodríguez, Bella Pajares-Hachero, María José Bermejo-Pérez and José Manuel Baena-Cañada; Project administration, José Manuel Baena-Cañada; Resources, José Manuel Baena-Cañada; Software, Salvador Gámez-Casado, Lourdes Rodríguez-Pérez, Cristina Bandera-López, Andrés Mesas-Ruiz, Alicia Campini-Bermejo, Marta Bernal-Gómez, Manuel Zalabardo-Aguilar, Julio Calvete-Candenas, Gala Martínez-Bernal, Lidia Atienza-Cuevas, Marcial Garcia-Rojo, Encarnación Benítez-Rodríguez, Bella Pajares-Hachero, María José Bermejo-Pérez and José Manuel Baena-Cañada; Supervision, Encarnación Benítez-Rodríguez and José Manuel Baena-Cañada; Validation, Salvador Gámez-Casado, Lourdes Rodríguez-Pérez, Cristina Bandera-López, Andrés Mesas-Ruiz, Alicia Campini-Bermejo, Julio Calvete-Candenas, Gala Martínez-Bernal, Lidia Atienza-Cuevas, Encarnación Benítez-Rodríguez, Bella Pajares-Hachero, María José Bermejo-Pérez and José Manuel Baena-Cañada; Visualization, Lourdes Rodríguez-Pérez, Cristina Bandera-López, Andrés Mesas-Ruiz, Alicia Campini-Bermejo, Marta Bernal-Gómez, Manuel Zalabardo-Aguilar, Gala Martínez-Bernal, Lidia Atienza-Cuevas, Marcial Garcia-Rojo, Encarnación Benítez-Rodríguez, Bella Pajares-Hachero, María José Bermejo-Pérez and José Manuel Baena-Cañada; Writing – original draft, José Manuel Baena-Cañada; Writing – review & editing, Salvador Gámez-Casado, Lourdes Rodríguez-Pérez, Cristina Bandera-López, Andrés Mesas-Ruiz, Alicia Campini-Bermejo, Marta Bernal-Gómez, Manuel Zalabardo-Aguilar, Julio Calvete-Candenas, Gala Martínez-Bernal, Lidia Atienza-Cuevas, Marcial Garcia-Rojo, Encarnación Benítez-Rodríguez, Bella Pajares-Hachero, María José Bermejo-Pérez and José Manuel Baena-Cañada.
Funding
This work was supported by Consejería de Salud y Consumo de la Junta de Andalucía [grant number PI-0346-2017]. The funding source had no role in the design of the study, in the collection, analysis and interpretation of the data, in the writing of the report, or in the decision to submit the article for publication.
Conflicts of Interest
Declarations of interest: none. This study was carried out in accordance with the ethical guidelines of the Declaration of Helsinki. All procedures were performed in compliance with relevant laws and institutional guidelines and have been approved by the Research Ethics Committee (04/17). Authorisation was obtained from the Research Ethics Committee for the exemption of informed consent in those patients who were deceased, those who could not be contacted or those who could not travel to the hospital centre.
References
- Srivastava S, Koay EJ, Borowsky AD, De Marzo AM, Ghosh S, Wagner PD, Kramer BS. Cancer overdiagnosis: a biological challenge and clinical dilemma. Nat Rev Cancer 2019; 19 (6): 349-358. [CrossRef]
- Woloshin S, Schwartz LM, Black WC, Kramer BS. Cancer screening campaigns--getting past uninformative persuasion. N Engl J Med 2012; 367 (18); 1677-1679. [CrossRef]
- Dunn BK, Woloshin S, Xie H, Kramer BS. Cancer overdiagnosis: a challenge in the era of screening. J Natl Cancer Cent 2022; 2 (4): 235-242. [CrossRef]
- Maas CCHM, van Klaveren D, Visser O, Merkx MAW, Lingsma HF, Lemmens VEPP, Dinmohamed AG. Number of life-years lost at the time of diagnosis and several years post-diagnosis in patients with solid malignancies: a population-based study in the Netherlands, 1989-2019. EClinicalMedicine 2023; 60:101994. [CrossRef]
- Marcadis AR, Marti JL, Ehdaie B, Hakimi A, Davies L, Morris LGT. Characterizing relative and disease-specific survival in early-stage cancers. JAMA Intern Med 2020; 180 (3): 461-463. [CrossRef]
- Brouckaert O, Schoneveld A, Truyers C, Kellen E, Van Ongeval C, Vergote I, et al. Breast cancer phenotype, nodal status and palpability may be useful in the detection of overdiagnosed screening-detected breast cancers. Ann Oncol 2013; 24: 1847-1852. 1852. [CrossRef]
- Lopes Cardozo JMN, Drukker CA, Rutgers EJT, Schmidt MK, Glas AM, Witteveen A, et al. Outcome of patients with an ultralow-risk 70-gene signature in the MINDACT Trial. J Clin Oncol 2022; 40: 1335-1345. [CrossRef]
- Pu M, Messer K, Davies SR, Vickery TL, Pittman E, Parker BA, et al. Research-based PAM50 signature and long-term breast cancer survival. Breast Cancer Res Treat 2020; 179 (1): 197-206. [CrossRef]
- Hudis CA, Barlow WE, Costantino JP, Gray RJ, Pritchard KI, Chapman JA, et al. Proposal for standardized definitions for efficacy end points in adjuvant breast cancer trials: The STEEP system. J Clin Oncol 2007; 25: 2127-2132. [CrossRef]
- Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, Carbone PP. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 1982; 5: 649-655.
- Charlson ME, Pompei P, Ales KL, MacKenzie CRA. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chron Dis 1987; 40: 373-383. [CrossRef]
- Baena-Cañada JM, Gámez-Casado S, Rodríguez-Pérez L, Bandera-López C, Mesas-Ruiz A, Campini-Bermejo A et al. Clinicopathological characteristics and survival results of patients with ultralow risk breast cancer. Med Clin (Barc) 2022; 159 (8): 351-358. [CrossRef]
- Bastien RR, Rodríguez-Lescure Á, Ebbert MT, Prat A, Munárriz B, Rowe L et al. PAM50 breast cancer subtyping by RT-qPCR and concordance with standard clinical molecular markers. BMC Med Genomics 2012; 5: 44. [CrossRef]
- Köninki K, Tanner M, Auvinen A, Isola J. HER-2 positive breast cancer: decreasing proportion but stable incidence in Finnish population from 1982 to 2005. Breast Cancer Res 2009; 11 (3): R37. [CrossRef]
- Alanko J, Tanner M, Vanninen R, Auvinen A, Isola J. Triple-negative and HER2-positive breast cancers found by mammography screening show excellent prognosis. Breast Cancer Res Treat 2021; 187 (1): 267-274. [CrossRef]
- Weyers W. Forward to the past-Oncology between underdiagnosis and overtreatment. Am J Dermatopathol 2016; 38: 517-528. [CrossRef]
- Lopes Cardozo JMN, Byng D, Drukker CA, Schmidt MK, Binuya MA, van 't Veer LJ, et al. Outcome without any adjuvant systemic treatment in stage I ER+/HER2- breast cancer patients included in the MINDACT trial. Ann Oncol 2022; 33 (3): 310-320. [CrossRef]
- Pedersen RN, Esen BÖ, Mellemkjær L, Christiansen P, Ejlertsen B, Lash TL et al. The incidence of breast cancer recurrence 10-32 years after primary diagnosis. J Natl Cancer Inst 2022; 114 (3): 391-399. [CrossRef]
- Gentilini OD, Botteri E, Sangalli C, Galimberti V, Porpiglia M, Agresti R et al. Sentinel lymph node biopsy vs no axillary surgery in patients with small breast cancer and negative results on ultrasonography of axillary lymph nodes: The SOUND randomized clinical trial. JAMA Oncol 2023; e233759. [CrossRef]
- Whelan TJ, Smith S, Parpia S, Fyles AW, Bane A, Liu FF et al. Omitting radiotherapy after breast-conserving surgery in luminal A breast cancer. N Engl J Med 2023; 389: 612-619. [CrossRef]
- Hu X, Walker MS, Stepanski E, Kaplan CM, Martin MY, Vidal GA, Schwartzberg LS, Graetz I. Racial differences in patient-reported symptoms and adherence to adjuvant endocrine therapy among women with early-stage, hormone receptor-positive breast cancer. JAMA Netw Open 2022; 5 (8): e2225485. [CrossRef]
- Sasada S, Kondo N, Hashimoto H, Takahashi Y, Terata K, Kida K et al. Prognostic impact of adjuvant endocrine therapy for oestrogen receptor-positive and HER2-negative T1a/bN0M0 breast cancer. Breast Cancer Res Treat 2023; 202: 473-483. [CrossRef]
- Pistilli B, Lohrisch C, Sheade J, Flemin, GF. Personalizing adjuvant endocrine therapy for early-stage hormone receptor positive breast cancer. American Society of Clinical Oncology Educational Book 2022; 42 (May 27, 2022) 60-72. [CrossRef]
- DeCensi A, Puntoni M, Guerrieri-Gonzaga A, Caviglia S, Avino F, Cortesi L, et al. Randomized placebo controlled trial of low-dose tamoxifen to prevent local and contralateral recurrence in breast intraepithelial neoplasia. J Clin Oncol 2019; 37: 1629-1637. [CrossRef]
Figure 1.
Flow chart of the stude.
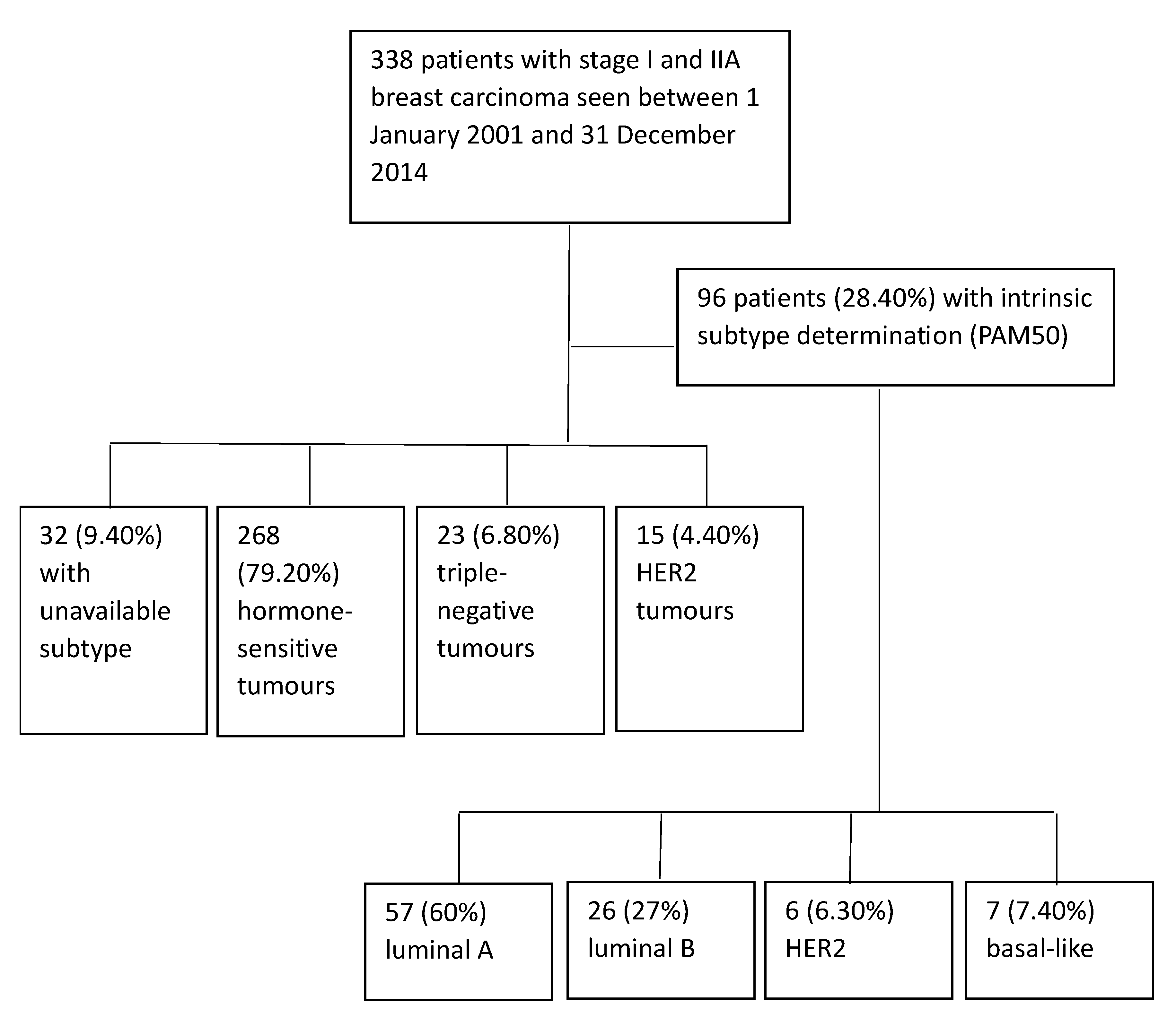
Figure 3.
Distant metastasis-free interval probability curve for 95 patients with intrinsic subgroup determination by PAM50.
Figure 3.
Distant metastasis-free interval probability curve for 95 patients with intrinsic subgroup determination by PAM50.
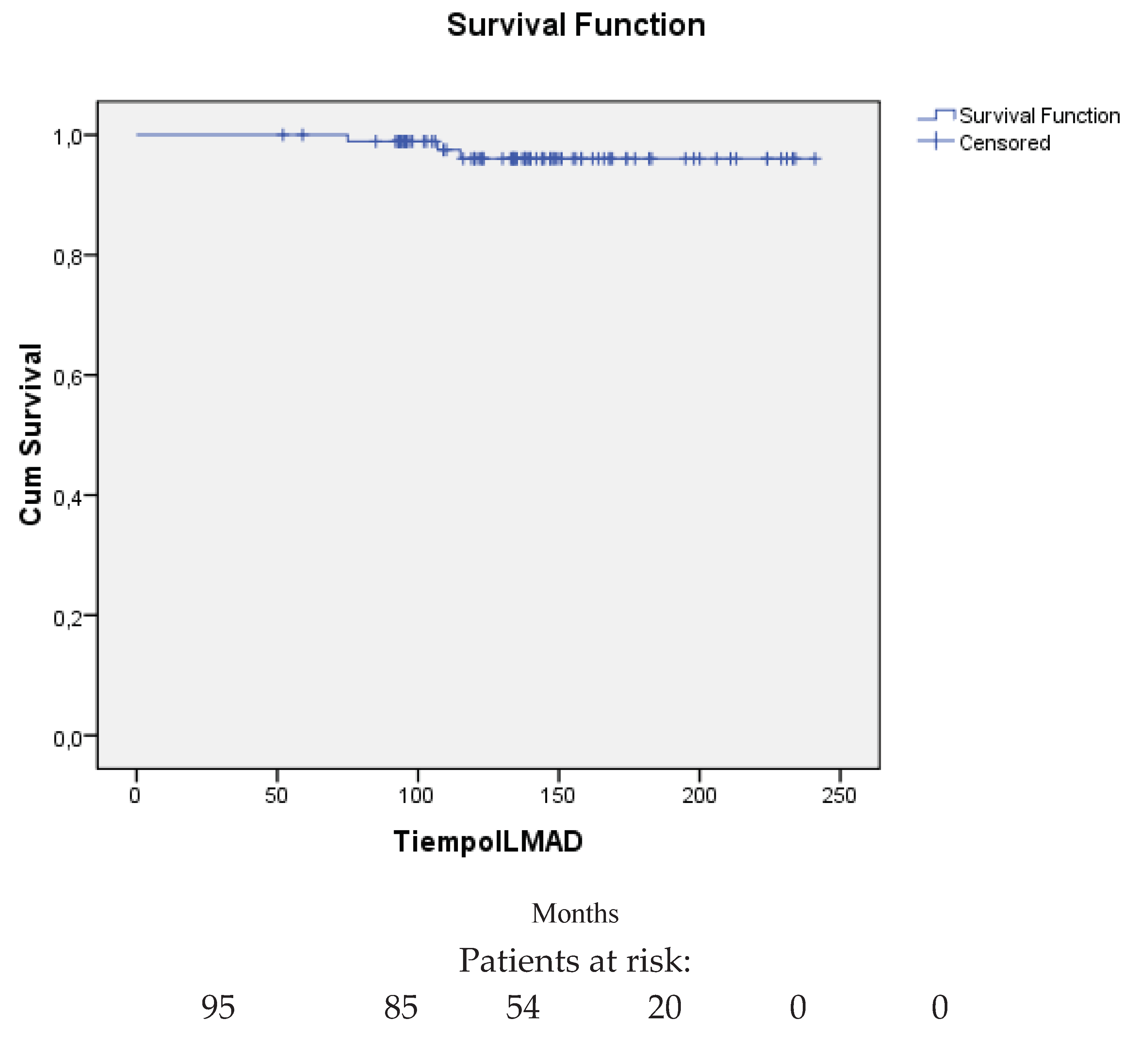

Table 1.
Characteristics of the 338 patients in the study.
| Characteristics of the 338 patients | N | % |
|---|---|---|
| Age, median (range) | 56 (38-71) | |
|
Functional capacity (ECOG)1 0 1 2 3 |
296 40 1 1 |
87.60 11.80 0.30 0.30 |
|
Comorbidity2 0 1 2 3 4 6 |
83 21 211 20 1 2 |
24.60 6.20 62.40 5.90 0.30 0.60 |
|
Menopause status Premenopausal Postmenopausal |
65 273 |
19.20 80.80 |
|
Breast screening mammogram Public Opportunistic |
302 36 |
89.30 10.70 |
|
Histological type Ductal Lobular Others |
279 21 38 |
82.50 6.20 11.20 |
|
Stage I IIA Unknown |
261 75 2 |
77.20 22.20 0.60 |
|
Tumour (pT) pT1mi pT1a pT1b pT1c pT2 Unknown |
8 21 101 161 44 3 |
2.40 6.20 29.90 47.60 13 0.90 |
| Tumour size (cm), median (range) | 1.20 (0.06-5) | |
|
Histological grade 1 2 3 Unknown |
106 167 49 16 |
31.40 49.40 14.50 4.70 |
| Ki67 proliferative index, median (range) | 12 (1-90) | |
|
Oestrogen receptors Positive Negative Unknown |
299 34 5 |
88.50 10.10 1.50 |
|
Progesterone receptors Positive Negative Unknown |
258 75 5 |
76.30 22.20 1.50 |
|
HER2 Positive Negative Unknown |
15 318 5 |
4.40 94.10 1.50 |
|
Breast surgery Conserving Mastectomy |
300 38 |
88.80 11.20 |
|
Axillary surgery Sentinel lymph node biopsy Axillary lymphadenectomy None |
232 98 8 |
68.60 29 2.40 |
|
Adjuvant systemic treatment Hormone therapy Chemotherapy Chemotherapy-hormone therapy None Unknown |
152 28 95 58 5 |
45 8.30 28.10 17.20 1.50 |
|
Hormone therapy Tamoxifen Aromatase inhibitor Tamoxifen-aromatase inhibitor Ovarian ablation |
106 59 76 2 |
43.60 24.30 31.30 0.80 |
|
Chemotherapy Anthracyclines Anthracyclines and taxanes Others |
67 37 20 |
54 29.80 16.10 |
Table 2.
Events in the 338 patients.
| Events | N | % |
|---|---|---|
|
Local recurrence After conserving surgery After mastectomy |
16 13 3 |
4.70 3.80 0.90 |
| Regional recurrence | 3 | 0.90 |
|
Metastasis Liver Bone Lung Central nervous system Skin Peritoneum Others |
18 6 5 5 2 1 1 2 |
5.30 1.80 1.50 1.50 0.60 0.30 0.30 0.60 |
|
Secondary invasive primaries Breast Ipsilateral Contralateral Non-breast Colorectal Ovarian Endometrial Pancreatic Lung Thyroid Bladder Vulva Carcinoid tumour Soft tissue sarcoma Non-Hodgkin’s lymphoma Multiple myeloma Oncocytoma |
31 10 3 7 21 4 3 3 2 1 1 1 1 1 1 1 1 1 |
9.30 3 0.90 2.10 6.30 1.20 0.90 0.90 0.60 0.30 0.30 0.30 0.30 0.30 0.30 0.30 0.30 0.30 |
|
Secondary non-invasive primaries Ductal carcinoma in situ of the ipsilateral breast Ductal carcinoma in situ of the contralateral breast |
7 5 2 |
2.10 1.50 0.60 |
|
Deaths From breast carcinoma From other causes Due to unknown causes |
30 16 12 2 |
9 4.80 3.60 0.60 |
Table 3.
Metastatic and non-metastatic events in relation to intrinsic subtype and tumour size less than or greater than 1 cm.
Table 3.
Metastatic and non-metastatic events in relation to intrinsic subtype and tumour size less than or greater than 1 cm.
| Intrinsic subtype and tumour size | N and % | Events (N and %) | Events not related to breast cancer mortality | Events related to breast cancer mortality |
|---|---|---|---|---|
| Luminal A | 56/95 (58.90%) | 9/56 (16.10%) | 7/56 (12.50%) | 2/56 (3.50%) |
| < 1 cm | 22 (39.30%) | 3/56 (5.30%) | 3/56 (5.30%) | 0/56 (0%) |
| > 1 cm | 34 (60.70%) | 6/56 (10.70%) | 4/56 (7.10%) | 2/56 (3.60%) |
| Luminal B | 26/95 (27.30%) | 6/26 (23%) | 5/26 (19.20%) | 1/26 (3.80%) |
| < 1 cm | 9 (34.60%) | 3/26 (11.50%) | 3/26 (11.50%) | 0/26 (0%) |
| > 1 cm | 17 (65.40%) | 3/26 (11.50%) | 2/26 (7.70%) | 1/26 (3.80%) |
| HER2 Enrichment | 6/95 (6.30%) | 1/6 (16.70%) | 1/6 (16.70%) | 0/6 (0%) |
| < 1 cm | 0 (0%) | |||
| > 1 cm | 6 (100%) | 1/6 (16.70%) | 1/6 (16,70%) | 0/6 (0%) |
| Basal like | 7/95 (7.30%) | 1/7 (14.30%) | 1/7 (14.30%) | 0/7 (0%) |
| < 1 cm | 4 (57.10%) | 0/7 (0%) | 0/7 (0%) | 0/7 (0%) |
| > 1 cm | 3 (42.90%) | 1/7 (14.30%) | 1/7 (14.30%) | 0/7 (0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



