
Submitted:
06 February 2024
Posted:
06 February 2024
You are already at the latest version
Abstract
To resolve problems in the dietary life of university athletes, education is essential for enabling athletes to change their own dietary behavior. The purpose of this research, it was decided to verify the effectiveness of sports nutrition education based on self-determination theory (SDT). Methods, the subjects were thirty-six male university rowers. A stratified randomized comparison test was conducted by student year (SDT group and control group). Sports nutrition education was held three times, via an Internet conferencing system. Furthermore, group work over social media was used for the SDT group. Four evaluations were carried out based on anthropometric measurements, brief-type self-administered diet history questionnaire (BDHQ),sports nutrition knowledge (SNK), and treatment self-regulation questionnaire (TSRQ). Results, for the intra-group factor "Protein," a significant difference was evident in the self-determination theory group (50.0±28.5, 78.6±28.1, 81.0±21.5, p<0.000, units: %), and there were significant differences between after and before, and between three months after and before (p=0.002, p=0.002). For BDHQ, significant differences were evident for green/yellow vegetables, fruits, and dairy between after and before for the self-determination theory group (159.1±74.2-126.7±70.6, p=0.009, 306.0±196.2-195.2±146.1, p=0.020, 257.0±147.0-183.3±167.9, p=0.040, units: g). In conclusion, sports nutrition education based on SDT improved dietary knowledge and increased dietary intake.
Keywords:
Sports nutrition knowledge
; Treatment self-regulation questionnaire
; Brief-type self-administered diet history questionnaire
; Intervention study
; Nutrition education
; Male Athletes
1. Introduction
1.1. Background
Rowing is a competition that requires both anaerobic and aerobic capacity. Although the competition lasts only 6-8 minutes, daily practice sessions are long. In addition, there are lightweight and heavyweight categories, which require different body weights and compositions, requiring individualized nutritional strategies and plans. Besides, Michael et al. reported that, there is an association between patterns of achievement-motivated behavior and performance with future success in rowing [1]. Karen et al. suggested that that a well-planned nutrition strategy that includes the careful timing and selection of appropriate foods and fluids helps to maximize training adaptations and, thus, should be an integral part of the athlete’s training program. And they also tell us that food choice is also influenced by physiological, social, psychological, and economic factors and varies both within and between individuals and populations, and they say that research is needed to investigate the motivations for athletes’ food choices [2].
Hamaguchi et al. reported that university students, because they tend to eat quick meals by buying takeaway foods or eating outside, “are less conscious about the importance of a well-balanced diet or cooking one’s own meals” [3]; they also pointed out that to raise awareness among university students, “we not only need to teach them nutritional knowledge but also to provide practical hands-on guidance” because “it is important for them to concretely understand and become aware of problematic areas from various directions by investigating information and problems related to food on their own and understanding their own dietary situation.” In addition, Akamatsu suggested that education on eating behavior is an important aspect of nutrition education that incorporates a perspective on eating behavior [4]. Jagim et al. reported a large discrepancy between the perceived amount of energy and nutritional intake and the actual intake” among university athletes [5]. These findings highlight the importance of sports nutrition education for university students.
Concerning nutrition education, Contento suggested that to facilitate changes in eating behavior, it is necessary to properly address various factors influencing or determining food choice and eating behavior and to use programs based on educational strategies, learned experience, and evidence [6]. In addition, a nutrition intervention protocol that incorporates a behavioral change model to boost motivation for the 5A’s (Ask, Advise, Assess, Assist, and Arrange) and motivational interviewing (MI) has been tested for adolescent athletes and has been reported to potentially promote changes in dietary behavior and inform nutrition strategies [7]. This 5A’s behavior-change model, which has also been tested in smoking cessation [8] and weight loss counseling [9], has been reported as an effective tool for behavioral counseling [10]. MI is a client-centered approach developed by Miller [11] that focuses on assisting subjects in planning and achieving autonomy to lead healthier and fulfilling lives. Regarding this motivation, it has been reported that Olympic medalists in judo “became intrinsically motivated by developing an interest in diet through a recognition that diet and athletic performance are linked” [12]. Therefore, research on nutrition education for athletes focusing on motivation has attracted a broad range of attention. The formation of athletes’ eating behaviors and assessment of dietary intake is very important because appropriate dietary intake improves athletes’ health and sports performance [13]. However, few studies have investigated deeper associations. Therefore, we focused on nutrition education research for athletes focusing on motivation.
This study examines this motivation in terms of intrinsic and extrinsic motivation and focuses on Ryan and Deci’s self-determination theory (SDT), which explains human behavior from the perspective of autonomy [14]. One of its subtheories, the Basic Psychological Needs Theory, involves three basic psychological needs–autonomy, competence, and relatedness–that lead to intrinsic motivation. This theory is employed in a wide range of areas, including health management and diet therapy, smoking cessation, dentistry, sports, physical activities, physical education, and work and organization.
Contento asserted that nutrition education helps students achieve motivation, self-control, and self-determination when it provides active feedback to the experience of autonomy (Autonomy) and situations where students feel responsible for acting with confidence (Competence), and provides support in the educator-student relationship (Relatedness) [6]. Markland et al. also suggested adopting the SDT perspective to deepen our understanding of the psychological processes involved in MI [15]. Furthermore, Patrick and Williams suggested that SDT and MI, although developed for different purposes and areas, have a great deal of conceptual overlap [16]. An SDT study on athletes reported that autonomy-supportive coaching strengthened the motivational orientation of behavior in high school and college athletes [17]. It has been reported that an SDT-informed intervention for young endurance athletes significantly increased knowledge but did not lead to changes in food intake [18]. In addition, motivation underlies feeding regulation, and the satisfaction and inhibition of basic psychological needs in SDT shows how disordered eating occurs and how a person can optimally regulate ongoing eating patterns [19]. Leblanc et al. suggest that nutrition education utilising self-determination theory appears to be particularly compatible with male [20]. The results of a meta-analysis by Ntoumanis et al. indicate that SDT-based interventions have a positive impact on health parameters [21]. However, although this type of intervention study focusing on male athletes is scarce.
1.2. Purpose
Against this background, we speculated that sports nutrition education, by incorporating SDT and creating opportunities to understand an individual’s own diet, might help students improve their food knowledge and improve and sustain their autonomous eating behavior. Therefore, the purpose of this study was to implement an SDT-informed sports-nutrition-education intervention and identify its effectiveness in inducing autonomous eating behaviors among male university athletes.
2. Materials and Methods
2.1. Experimental Design
The intervention period was six months, from June 13, 2021, to November 27, 2021. This study was a two-group randomized controlled trial.
Simona et al. reported that research on the effectiveness of nutrition education and behavior change interventions in athletes is lacking; therefore, additional studies of sufficient rigor (i.e., randomized controlled trials) are needed to demonstrate the benefits of nutrition counseling in athletes [22].
Individuals were assigned code names by the author, and the intervention group (SDT group) and the control group (hereafter referred to as the COT group) were randomly assigned according to grade level after the pre-survey. It used the RAND function in Excel to generate a random number and sort the members into two groups. The power calculations were based on the results from a prior study on nutrition knowledge [23]. In this study, the mean difference in knowledge between athletes and coaches was 8±9%, with athletes correct 73±9% and coaches correct 81±9%. Thus, we estimated that the change in knowledge scores achievable and beneficial to the participants was about 8%. (α = 0.05, desired power = 0.80). Based on this, we calculated that there should be 17 athletes in each group; with an expected dropout of 10%, we estimated that we needed at least 38 athletes.
2.2. Participants
The participants were defined as members of the University of Rowing Club in April 2021 who were training continuously, and exclusion criteria were those who had left the club, taken a leave of absence, or switched to coxswains. Thirty-six male athlete members and four staff members, including a coach, a coxswain, a new trainer coach, and a manager participated in the survey. The male athlete members were assigned to two groups 18 members in the SDT group and 18 in the COT group.
An explanatory meeting was held for the subjects two weeks before the study program began. An explanation of the study and a consent form were distributed to the participants who provided free and voluntary informed consent. For the consent of minors, we mailed an explanation of the study together with a consent form to their parents or guardians and asked them to give their consent by returning the completed forms to us in a self-addressed envelope. The participants were informed that they would not know which group they would be assigned to at the time of the briefing session. A preliminary survey was conducted on May 30th, two weeks before the program began. The overall study design is shown in Figure 1.
2.3. Intervention Program
2.3.1. Program Overview
This study created an intervention program centered on SDT that incorporated the elements of the 5As and MI. The aim of the SDT program was to enhance autonomy, leading to a change in intrinsic behavior, and it included the following elements: (1) Desire for Autonomy: A desire for self-determination of one’s own experiences and actions, and a sense of self-determination of one’s own actions; (2) Desire for Competence: A desire to effectively demonstrate one’s ability and competence, and the feeling of being able to demonstrate one’s abilities and talents; and (3) Desire for Relationships (relations and interactions): the desire to form good relatedness with others, to be cared for by significant others, and to contribute something to the benefit of others [14]. For the intervention program that incorporated elements of the 5A’s and MI, we also incorporated elements of the nutrition intervention protocol validated by Lee and Lim [7].
In this study, group sports-nutrition-education seminars were held once every four weeks for a total of three sessions using a web-conferencing system. Table S1 presents the overall flow of the program. The program time was 90 min for the SDT group and 60 min for the COT group. After the sports nutrition education seminar, information was shared once a week in small groups (four or five participants), including one manager for both groups, using an online communication tool. The content of the program was decided by two university faculty members specializing in physical education, sports management, coaching, and sports nutrition. One of the authors, a sports nutritionist, provided the guidance.
2.3.2. Sports-Nutrition-Education Seminars
Educational content and handouts were similar for both the SDT and COT groups, with the SDT group receiving an additional worksheet that included work on Autonomy, Competence, and Relatedness.
The common educational content for both groups was original and based on the content of the nutrition education session adopted by Lee and Lim [7]. In the first month, the Basic Nutrition Concept program included (1) the need for sports nutrition and how to use nutritional information, (2) nutrition and training, (3) regular eating habits, (4) body image, and (5) knowledge of sports nutrition (protein, carbohydrates, and water supplementation). In the second month, the Basic Food Skills program included (1) knowledge of sports nutrition (including supplements), (2) grocery shopping (ingredients and food selection), (3) cooking methods and food hygiene, (4) meal planning, and (5) eating out. In the third month, the Performance Enhancement program consisted of (1) planning light meals (recovery from fatigue and muscle pain), (2) meals before practice and games, (3) meals during practice and games, (4) meals after practice and games, (5) meals on the move, and (6) meals for various purposes (weight gain, weight loss, and weight maintenance). All participants were encouraged to participate in interactive communication through a web conferencing system.
The additional work performed by the SDT group was designed to promote autonomy based on (1) providing rational motivation for the participant’s activities, (2) understanding the participant’s feelings, and (3) giving the participant a choice of activities [24]. The participants then employed question-and-answer sessions and group discussions, and used a worksheet that allowed them to discover problems and issues from their own food profiles, their usual cooking, and light meals before and after practice and games. To enhance autonomy, support was provided by clearly communicating expectations and clarifying the process of achievement [25]. Concrete suggestions for improvement were provided before the worksheet was filled out. We ensured that this led to their usual eating habits by asking them to write down, in their own words, the areas for improvement and by actually taking action. The worksheets were collected after the sports nutrition education seminar and returned after checking their content. The checked content was used to send advice via e-mails. Sports, nutrition, and education seminars were held in the evenings after practice, and the participants attended seminars at the boatyard and from their homes.
2.3.3. Group Support Using Online Communication Tools
For the online communication tool, both groups shared one day’s worth of photographs of their meals once a week and were able to consult with the author about any questions they had.
In addition, for the SDT group, progress in the tasks was reported within the group based on worksheets completed at the monthly sports-nutrition-education seminars, allowing the groups to advise each other. The SDT group managers reported their progress to the authors each week, and the authors sent 12 advice e-mails to each group within two–three days of the report. This program was designed to link sports nutrition education with group support using online communication tools.
2.4. Survey and Measurement Instruments
The survey/measurement items included anthropometric measurements (height, weight, and body fat percentage), brief self-administered diet-history questionnaire (BDHQ), sports nutrition knowledge questionnaire (SNK) and treatment self-regulation questionnaire on the self-regulation of eating habits (TSRQ). The primary outcome were anthropometric measurements and BDHQ, the secondary outcome were SNK and TSRQ.
Anthropometric measurements were taken using equipment that estimates body composition using the Bioelectrical Impedance Analysis (BIA). The following seven points were standardized when measuring body weight and body fat percentage: (1) measurements were made two hours after eating; (2) urination and defecation were completed before measurement; (3) measurements immediately after exercise should be avoided; (4) measurements in the presence of dehydration or swelling should be avoided; (5) measurements at low temperatures or during hypothermia should be avoided; (6) measurements at high temperatures should be avoided; and (7) measurements immediately after bathing should be avoided. Anthropometric measurements were taken with a manager who was thoroughly familiar with this method.
Kobayashi et al. [26] developed the BDHQ, which retains the features of the self-administered dietary history questionnaire developed by Sasaki et al. [27] by simplifying its structure, responses, and data processing. We used the BDHQ to survey nutrient and other intakes in the previous month. The manager distributed the BDHQs and collected them within three days. The manager and authors checked for omissions and errors on the day of collection; if recompletion was required, the manager requested correction within a few days, and the resulting responses were collected once more.
The SNK was based on a questionnaire (40 questions) developed by Walsh et al. [28] and surveyed food knowledge categorized into five sections: (1) Training Schedule and Positioning with Training, (2) Eating and Hydration Habits and Awareness, (3) Attitudes Toward Nutrition Intake, (4) Nutrition Knowledge, and (5) Nutrition Information Sources and Nutrition Education that Might be Needed in the Future.
The TSRQ was developed by Ryan and Connell [29] to assess autonomous self-regulation, and was first used for health purposes by Williams et al. [30]. It is now widely used in behavioral change studies in medical settings. Subsequently, Levesque et al. validated the utility of healthy behaviors [31]. The TSRQ consists of a series of questions about why people engage in or attempt to engage in healthy behaviors, enter treatment for illness, change unhealthy behaviors, follow a treatment plan, or engage in other health-related behaviors (Center for Self-Determination Theory online) [32]. There were four types of TSRQ: smoking cessation, dietary modifications, regular exercise, and responsible drinking. In this study, we used a modified version of the diet. Furthermore, respondents were asked to respond to the questions by viewing their health as “health on the playing field.” The TSRQ was used after we reconfirmed its contents, which had been translated by a company specializing in translating research papers.
These surveys and measurements were conducted two weeks before the start of the program (before), immediately after program’s conclusion (immediately after), and three months after the program’s conclusion (after three months). During the program’s implementation period, the participants’ body composition in terms of height, weight, and body fat percentage was measured every four weeks, and anthropometric measurements and diet self-control were conducted every four weeks as a continuing evaluation for three months after the program ended.
2.5. Statistical Analysis Methods
The program was subjected to parametric tests before, immediately after, and after three months later. Anthropometric data were obtained as mean and standard deviation.
In this study, the nutrient intake of ten items and the nutrient intake by food group of 15 items were used in the BDHQ. The nutrients selected were "iron, vitamin D, calcium, and the antioxidant vitamin C," which are reported to be particularly important for athletes 33]. In addition, vitamin B1 and dietary fiber, which are easily deficient in the university’s rowing club, were selected.
The 14 SNK questions were divided into five items (Total Knowledge Score, Energy and Replenishment, Hydration, Supplements, and Protein), and the percentages of correct answers were analyzed for each item.
The TSRQ of 15 questions was divided into four items. The means of the responses to each question were calculated for three items: autonomous motivation, externally controlled motivation, and non-motivation. The fourth item, the Relative Autonomous Motivation Index, is calculated by subtracting the mean value of externally controlled reasons from that of autonomous reasons.
The results of the BDHQ, SNK, and TSRQ were expressed as means and standard deviations. Unpaired t-tests were used for pre-program group comparisons. Repeated two-way analysis of variance was used for between-group and within-group factors and the Bonferroni method was used for multiple comparison tests when significant differences were confirmed. The statistical significance level was set a 5%.
2.6. Ethical Considerations
The University of Tsukuba Research Ethics Committee reviewed the ethical considerations for conducting this study and approved it on May 20, 2021 (issue no. Tai 020-176). Statistical analysis software was IBM SPSS Statistics 28.0 for Windows.
3. Results
3.1. Participant flow and number of participants analyzed.
There were two left the club, one leave of absence, and two coxswain transfers, resulting in a total of 31 subjects for analysis:14 in the SDT group and 17 in the COT group.
3.2. Before-Group Differences
The results of the anthropometric measurements, SNK, and TSRQ are listed in Table S2. No significant differences were observed in any parameters between the SDT and COT groups. The BDHQ results are shown in Table S3. The SDT and COT groups had no significant differences in nutrient intake, but there were significant differences in meats (p = 0.043) and fat and oil (p = 0.004) intake by food group.
3.3. Anthropometric Measurements, Sports Nutritional Knowledge Questionnaire (SNK), and Treatment Self-Regulation Questionnaire (TSRQ)
Table S4 lists the results of the anthropometric measurements, SNK, and TSRQ. Between the SDT and COT groups, there were no significant differences in body weight, body-fat percentage, lean-body mass, or lean-body mass/m. There were no differences between the SDT and COT groups in intragroup factors for immediately after and before, after three months and before, or after three months and immediately after. There was no significant difference in the total SNK knowledge score between the SDT and COT groups in the between-groups factor. On the other hand, there was no significant difference in the main effect of time on the within-group factor (p = 0.004). The SDT group had a 78.6 ± 12.5% for before and 87.2 ± 7.5% for immediately after, whereas the COT group had a 75.6 ± 10.1% for before and 83.6 ± 8.3% for immediately after. Thereafter, there was a significant difference (p = 0.003) between immediately after and before in a subsequent multiple comparison test, with an increase in immediately after compared with before. In the between-group factor for protein, there was no significant difference between the SDT and COT groups. In contrast, there was a significant difference in the main effect of time on the within-group factor (p < 0.001).
In the SDT group, the results were 50.0 ± 28.5% for before, 78.6 ± 28.1% for immediately after, and 81.0 ± 21.5% for after three months. In the COT group, the results were 56.9 ± 22.9% for before, 72.5 ± 27.0% for immediately after, and 68.6 ± 24.9% for after three months. In the subsequent multiple comparison tests, there was a significant difference immediately after (p = 0.002), before and after three months and before (p = 0.002). There were no significant differences between or within the groups in terms of energy, supplementation, hydration, or supplements. There were no significant differences between the SDT and COT groups in the TSRQ autonomous motivation subscale, externally controlled motivation subscale, non-motivation subscale, or the Relative Autonomous Motivation index in terms of between-group and within-group factors.
3.4. Brief Dietary History Questionnaire (BDHQ)
The BDHQ results are presented in Table 1. In terms of between-group factors, there was no significant difference in carbohydrate intake between the SDT and COT groups. However, only the main effect of time was significant (p = 0.021), and a subsequent multiple comparison test revealed no significant difference. For the between-group factor, there was no significant difference in calcium between the SDT and COT groups. However, only the main effect of time was statistically significant (p = 0.026). Thereafter, subsequent multiple comparison tests showed no significant differences. Moreover, there were no significant differences in energy, protein, fat, iron, vitamin D, vitamin B1, vitamin C, or dietary fiber levels between or within groups.
There were no significant differences in the intake of green and yellow vegetables between the SDT and COT groups in terms of the intake of each food group and the between-group factors. However, the main effect of time on the within-group factors showed a significant difference (P = 0.009). The intake of green vegetables in the SDT group was 126.7 ± 70.6 g for before and 159.1 ± 74.2 g for immediately after, whereas in the COT group it was 99.8 ± 69.2 g for before and 159.9 ± 99.3 g for immediately after. A subsequent multiple comparison test revealed a significant difference (P = 0.009) immediately after and before. Fruits were not significantly different between the SDT and COT groups in terms of between-group factors. However, there was a significant difference in the main effect of time on within-group factors (p = 0.013).
In the SDT group, the intake of fruits was 195.2 ± 146.1 g for before and 306.0 ± 196.2 g for immediately after, whereas in the COT group, it was 133.2 ± 152.4 g for before and 215.3 ± 208.6 g for immediately after. Thereafter, multiple comparison tests showed a significant difference (p = 0.020) immediately after and before intervention.
There were no significant differences in the between-group factors for dairy products production between the SDT and COT groups. However, there was a significant difference in the main effect of time on within-group factors (p = 0.012). The intake of dairy products was 183.3 ± 167.9 g for before and 257.0 ± 147.0 g for immediately after in the SDT group, and 177.3 ± 93.3 g for before and 262.6 ± 134.4 g for immediately after in the COT group. A subsequent multiple comparison test revealed a significant difference (P = 0.040) immediately after and before.
There were no significant differences between or within the groups for cereals, potatoes, sugar and sweeteners, pulses, other vegetables, fish and shellfish, meats, eggs, fats and oils, confectioneries, beverages, or seasonings and spices.
4. Discussion
This study implemented SDT-informed sports nutrition education among male university rowing club with the goal of not only improving sports nutrition knowledge but also establishing an autonomous dietary environment. The results showed no differences between the two groups in terms of the anthropometric measurements, BDHQ, SNK and TSRQ. Thus, the effectiveness of education has not yet been demonstrated. However, anthropometric measurements included the summer months, when appetites are more likely to decrease, but weight and lean body mass did not decrease significantly. In an intervention program combining nutrition education and food environment intervention in a randomized controlled trial similar to this study, the authors reported that the main outcome, the BDHQ survey, confirmed changes in intake by food group [34]. In our study also, for the BDHQ results for intake by food group, from the time immediately before the intervention to the time immediately after it, green and yellow vegetables, fruits, and dairy products intake increased for both groups. In terms of food knowledge, the aggregate knowledge score from the SNK and the scores for protein items improved immediately after the intervention compared with those before the intervention and, with respect to protein items alone, remained higher for three months. However, the results indicated no significant differences between the two groups.
For intrinsic motivation, internalization, where a person integrates extrinsically motivated behaviors as their own, plays an important role, which requires the basic psychological needs of Autonomy, Competence, or Relatedness to be fulfilled [14]. Roth et al. [35] argued that autonomous motivation for learning is promoted by expanding support for autonomy. Based on these reports, in this study, support was provided to the SDT group so that the participants used a worksheet in the sports-nutrition-education seminars to review their everyday meals, write down areas for improvement in their own words, and link these exercises to actual actions. We attempted to strengthen this mechanism by providing group support using online communication tools. However, our results do not support the effectiveness of this mechanism. According to Murray et al., the factors that contribute to problematic cooking practices among university students include insufficient knowledge and skills in cooking, financial insecurity, inadequate information on healthy eating, and time and lifestyle constraints. Therefore, it is important to design an effective and strategic program to promote motivation [36]. In the case of university rowing clubs, some clubs provide meals in their dormitories, but if the environment is not conducive, they often cook their own meals. Therefore, specific suggestions were needed to create a food environment for university rowers. In this study, food choices and cooking methods were proposed to improve cooking skills at home. Therefore, this might explain why the effects were observed in both groups immediately after the intervention, leading to changes in eating behavior. Heikkilä et al. [18] reported that, in a study on SDT-informed nutrition-education intervention, administering the education three times significantly increased nutrition knowledge, but did not lead to changes in food intake. However, in the current study, the subjects in both groups established learning goals in a sports nutrition education seminar. This led not only to improved nutritional knowledge, but also to an increase in the food intake. The SDT group was asked to look at pictures of their own food, examine “the items that I’m missing” and set goals so that they would be intrinsically motivated. Such the program was unique, in that it was designed to use learning goals to make students “aware.” The approach based on the 5A’s and MI, which encouraged food selection, was effective, as we believe that it brought about such behaviors and practices in the SDT group.
All seminars were conducted using synchronous distance education and a web conferencing system. As this learning format was entirely new to the participants, we believe that it played a role in making it more difficult for the variances between the groups to manifest. In contrast, Liyun et al. reported that for knowledge acquisition, synchronous distance education was not significantly different from conventional education in terms of learning effectiveness, and the level of satisfaction was also high [37]. The adoption of synchronous distance education in this study led not only to knowledge, but also to action and practice in both groups. We can infer from this that the results demonstrate the effectiveness of synchronous distance education, regardless of the SDT-based approach.
Because intrinsic framing of goals produces effects such as deeper engagement in learning activities, better conceptual learning, and higher persistence at learning activities [38] and learning goals, in which individuals seek to increase their competence, promote challenge-seeking behaviors and a mastery-oriented response to failure [39], intrinsic framing of goals is likely to contribute to the subsequent continuation of specific habits. Therefore, considering the need for practical hands-on guidance, as discussed by Hamaguchi et al. [3], providing face-to-face nutrition education involving cooking practice and food tasting still leads to the creation of distinctive eating experiences: feeling the taste of food, thinking about how to achieve that taste, and discovering and being impressed by great food. This, in turn, might lead to the continuation of such experiences. In order to implement effective sports nutrition education, we would like to construct an ongoing program that can maintain the intrinsic motivation of athletes.
This study is limited in a number of dimensions. A randomized controlled trial administered within a single university rowing club by grade, we needed to guarantee the quality of the content and make it uniform to a certain extent between the two groups. Nutrition education had to be provided without significantly varying it between different subjects, and the manager and all other staff members had to treat all subjects similarly. In addition, because SDT and COT shared the same practice environment and ate in the same place, they inevitably interacted with one another and influenced each other. Within the club, athletes were mutually supportive, and the team’s group cohesiveness was high. The design of a controlled trial, “creating a COT group that does nothing,” might, therefore, have limitations in sports practice. In this study, the research design was developed without eliminating existing positive team practices. As Tanaka and Shigematsu [40] state, “rather than creating a control group that is not allowed to do anything, we should focus on having a sincere concern for the physically vulnerable people in front of us,” and we believe that researchers should pay attention to their research subjects and have flexible thinking and broad perspectives. Also, when was the survey, due to the COVID-19 pandemic, meals could not be provided within the team. To address this issue, both groups received assistance with meals immediately after the outbreak through an “emergency special donation” from the team alumni. We believe that this potentially had an uncontrollable influence on the variance between the SDT and COT groups. In addition, the SNK and TSRQ used expert-translated questionnaires, which have not been validated in our country and need to be validated. In the future, we would like to review the target population of the intervention, timing, research design such as questionnaires, and post-intervention follow-ups.
5. Conclusions
The results of this study demonstrate that SDT-informed sports nutrition education, through improvement in nutrition knowledge, can potentially lead to the practice and continuation of improved eating behaviors. These effects were clearly demonstrated by actual food intake. Therefore, body weight, one indicator of athlete health, was maintained, and lean body mass was not significantly reduced. Additionally, the provision of support designed to promote autonomy allowed us to discover that autonomy potentially facilitates intrinsic motivation. In developing a program utilizing SDT in a department that is student-driven, the cooperation of the student staff may lead to continued food awareness and eating behavior, which may affect the overall team’s bottom line. The program used in this study could potentially promote sports nutrition education.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, Table S1.Program Overview; Table S2. Between-group differences in anthropometric measurements, SNK and TSRQ (prior); Table S3. Between-group differences in BDHQ (prior); Table S4. Results of between-group and within-group factor analyses of anthropometrics, SNK, and TSRQ.
Author Contributions
Conceptualization, N.A., J.S. and M.O.; methodology, N.A., J.S. and M.O.; formal analysis, N.A., J.S., M.O. and T.T.; investigation, N.A.; resources, N.A.; data curation, N.A., J.S., M.O. and T.T.; writing—original draft preparation, N.A.; writing—review and editing, N.A., J.S. and M.O.; visualization, N.A., J.S. and M.O.; supervision, M.O.; project administration, N.A. and M.O.; funding acquisition, J.S. and M.O. All authors have read and agreed to the published version of the manuscript.
Funding
This study received no external funding.
Institutional Review Board Statement
The University of Tsukuba Research Ethics Committee reviewed and approved the ethical considerations for this study (issue no. Body 020-176) on 20 May 2021.
Informed Consent Statement
Informed consent was obtained from all participants involved in the study. We also express our sincere gratitude to the members of the university rowing club and their coaches for their long-term participation and for their great cooperation. We would also like to thank them for their cooperation in collecting valuable data.
Acknowledgments
N.E. expresses his deepest gratitude to his supervisor, Professor Mitsugu Ogata, for his guidance in this research. He would also like to express his sincere gratitude to Dr. Jun Seino for his careful and precise guidance and to Dr. Taishi Tsuji for his careful guidance and advice on statistical analysis.
Conflicts of Interest
The authors have no conflict of interest to declare.
References
- Michael, J.S.; Achim, C.; Claudia, Z. Patterns of achievement-motivated behavior and performance as predictors for future success in rowing: A person-oriented study. Int J Sports Sci Coach 2021, 16, 101–109. [Google Scholar]
- Karen, L.B.; Gary, S. A Review of Factors Influencing Athletes’ Food Choices. Sports Med 2015, 45, 1511–1522. [Google Scholar]
- Hamaguchi, I.; Adachi, T.; Ohkita, S.; Fukumoto, T.; Maeda, A.; Uchida, H.; Kitamoto, N.; Okuda, T. Relationship between the consciousness and behavior in dietary life of university students. J. Home Econ. Jpn. 2010, 61, 13–24. [Google Scholar]
- Akamatsu, R. Changing nutrition education’s focus on nutrition to on eating behavior: Basic and applied studies of coping strategies for temptations on weight management. Jpn. J. Behavioral Med. 2015, 21, 63–68. (in Japanese). [Google Scholar]
- Jagim, A.R.; Zabriskie, H.; Currier, B.; Harty, P.S.; Stecker, R.; Kerksick, C.M. Nutrient Status and perceptions of energy and macronutrient intake in a group of collegiate female lacrosse athletes. J. Int. Soc. Sports. Nutr. 2019, 16, 43. [Google Scholar] [CrossRef] [PubMed]
- Contento, I.R. Nutrition Education: Linking Research, Theory, and Practice; Jones & Bartlett Learning: Burlington, MA, USA, 2016. [Google Scholar]
- Lee, S.; Lim, H. Development of an Evidence-Based Nutritional Intervention. J Exerc Nutrition Biochem. 2019, 30, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Mak, Y.W.; Loke, A.Y.; Wong, F.K.Y. Nursing intervention practices for smoking cessation: A large survey in Hong Kong. Int. J. Environ. Res. Public Health 2018, 15, 1046. [Google Scholar] [CrossRef] [PubMed]
- Searight, H.R. Counseling patients in primary care: Evidence-based strategies. Am. Fam. Physician 2018, 98, 719–728. [Google Scholar] [PubMed]
- Whitlock, E.P.; Orleans, C.T.; Pender, N.; Allan, J. Evaluating primary care behavioral counseling interventions: An evidence-based approach. Am. J. Prev. Med. 2002, 22, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R. Motivational interviewing with problem drinkers. Behav. Cognitive Psychother. 1983, 11, 147–172. [Google Scholar] [CrossRef]
- Oshiba, Y.; Seino, J.; Ogata, M. Factors affecting changes in eating behavior of Japanese medalists in judo at the Rio Olympics. Jpn J. Phys. Educ. Health Sport Sci. 2020, 65, 705–721. [Google Scholar] [CrossRef]
- Kevin, I.M.; Erik, S. A Proposed Conceptual Sport Nutrition Approach for Athlete Development and Assessment: The Athlete Nutrition Development Approach. Sports Medicine - Open. 2022, 8, 142. [Google Scholar]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory Basic Psychological Needs in Motivation, Development, and Wellness; Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Markland, D.; Ryan, R.M.; Tobin, V.J.; Rollnick, S. Motivational interviewing and self-determination theory. J. Social Clin. Psychol. 2005, 24, 811–831. [Google Scholar] [CrossRef]
- Patrick, H.; Williams, G.C. Self-determination theory: Its application to health behavior and complementarity with motivational interviewing. Int. J. Behav. Nutr. Phys. Activity 2012, 9, 18. [Google Scholar] [CrossRef]
- Amorose, A.J.; Anderson-Butcher, D. Autonomy-supportive coaching and self-determined motivation in high school and college athletes: A test of self-determination theory. Psychol. Sport. Exerc 2007, 8, 654–670. [Google Scholar]
- Heikkilä, M.; Lehtovirta, M.; Autio, O.; Fogelholm, M.; Valve, R. The impact of nutrition education intervention with and without a mobile phone application on nutrition knowledge among young endurance athletes. Nutrients 2019, 11, nu11092249. [Google Scholar] [CrossRef]
- Joke, V.; Heather, P.; Maarten, V.; Pedro, J.T. Motivational dynamics of eating regulation: a self-determination theory perspective. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 21. [Google Scholar]
- Leblanc, V.; Bégin, C.; Hudon, A.M.; Royer, M.M.; Corneau, L.; Dodin, S.; Lemieux, S. Effects of a nutritional intervention program based on the self-determination theory and promoting the Mediterranean diet. Health Psychol. Open 2016, 3, 1. [Google Scholar] [CrossRef]
- Ntoumanis, N.; Ng, J.Y.Y.; Prestwich, A.; Quested, E.; Hancox, J.E.; Thøgersen-Ntoumani, C.; Deci, E.L.; Ryan, R.M.; Lonsdale, C.; Williams, G.C. A meta-analysis of self-determination theory-informed intervention studies in the health domain: effects on motivation, health behavior, physical, and psychological health. Health Psychol. Rev. 2021, 15, 214–244. [Google Scholar] [CrossRef]
- Simona, F.; Lenycia, D.C.L.N.; Monica, G.; Elisa, P.; Anna, T.; Paula, A.Q.; Cinzia, F. Nutritional counseling in athletes: A systematic review. Front Nutr. 2023, 10, 1250567. [Google Scholar]
- Heikkilä, M.; Valve, R.; Lehtovirta, M.; Fogelholm, M. Nutrition Knowledge Among Young Finnish Endurance Athletes and Their Coaches. Int J Sport Nutr Exerc Metab 2018, 28, 522–527. [Google Scholar] [CrossRef]
- Deci, E.L.; Eghrari, H.P.; Patrick, B.C.; Leone, D.R. Facilitating internalization: The self-determination theory perspective. J. Personality 1994, 62, 119–142. [Google Scholar] [CrossRef]
- Jang, H.; Reeve, J.; Deci, E.L. Engaging students in learning activities: It is not autonomy support or structure but autonomy support and structure. J. Educ. Psychol. 2010, 102, 588–600. [Google Scholar] [CrossRef]
- Kobayashi, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Public Health Nutr. 2011, 14, 1200–1211. [CrossRef]
- Sasaki, S.; Yanagibori, R.; Amano, K. Validity of a self-administered diet history questionnaire for assessment of sodium and potassium. Comparison with single 24-hour urinary excretion. Jpn. Circul. J. 1998, 62, 431–435. [Google Scholar] [CrossRef]
- Walsh, M.; Cartwright, L.; Corish, C.; Sugrue, S.; Wood-Martin, R. The body composition, nutritional knowledge, attitudes, behaviors and future education needs of senior schoolboy rugby players in Ireland. J. Sport Nutr. Exercise Metab. 2011, 21, 365–376. [Google Scholar] [CrossRef]
- Ryan, R.M.; Connell, J.P. Perceived locus of causality and internalization: Examining reasons for acting in two domains. J. Pers. Soc. Psychol. 1989, 57, 749–761. [Google Scholar] [CrossRef]
- Williams, G.C.; Grow, V.M.; Freedman, Z.; Ryan, R.M.; Deci, E.L. Motivational predictors of weight loss and weight-loss maintenance. J. Pers. Soc. Psychol. 1996, 70, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Levesque, C.S.; Williams, G.C.; Elliot, D.; Pickering, M.A.; Bodenhamer, B.; Finley, P.F. Validating the theoretical structure of the Treatment Self-Regulation Questionnaire (TSRQ) across three different health behaviors. Health Educ. Res. 2007, 22, 691–702. [Google Scholar] [CrossRef]
- Center for Self-Determination Theory (online) Health-Care Self-Determination Theory Questionnaire (HCSDTQ). Available online: https://selfdeterminationtheory.org/health-care-self-determination-theory-questionnaire/, (accessed on 12 September 2023).
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance. Med Sci Sports Exerc. 2016, 48, 543–568. [Google Scholar] [PubMed]
- Iriyama, Y.; Murayama, N. Effects of Worksite Nutrition Education and Environmental Interventionson Weight Control of Male Workers: A Randomized Controlled Trial. The Japanese journal of nutrition and dietetics. 2012, 70, 83–98. [Google Scholar] [CrossRef]
- Roth, G.; Assor, A.; Kanat, M.Y.; Kaplan, H. Autonomous motivation for teaching: How self-determined teaching may lead to self-determined learning. J. Educ. Psychol. 2007, 99, 761–774. [Google Scholar] [CrossRef]
- Murray, D.W.; Mahadevan, M.; Gatto, K.; O’Connor, K.; Fissinger, A.; Bailey, D.; Cassara, E. Culinary efficacy: An exploratory study of skills, confidence, and healthy cooking competencies among university students. Perspect Public Health 2016, 136, 143–151. [Google Scholar]
- Liyun, H.; Na, Y.; Lingling, X.; Fan, P.; Wei, L.; Qi, S.; Yuxiu, L.; Huijuan, Z.; Huabing, Z. Synchronous distance education vs traditional education for health science students: A systematic review and meta-analysis. Med. Educ. 2021, 55, 293–308. [Google Scholar]
- Vansteenkiste, M.; Lens, W.; Deci, E.L. Intrinsic versus extrinsic goal contents in self-determination theory: Another look at the quality of academic motivation. Educ. Psychol. 2006, 41, 19–31. [Google Scholar] [CrossRef]
- Elliott, E.S.; Dweck, C.S. Goals: An approach to motivation and achievement. J. Pers. Soc. Psychol. 1988, 54, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Shigematsu, R. A paradigm shift for designing health-related intervention studies in exercise science and physical education. Jpn. J. Phys. Fitness Sports Med. 2010, 59, 457–463. [Google Scholar] [CrossRef]
Figure 1.
Research Design.
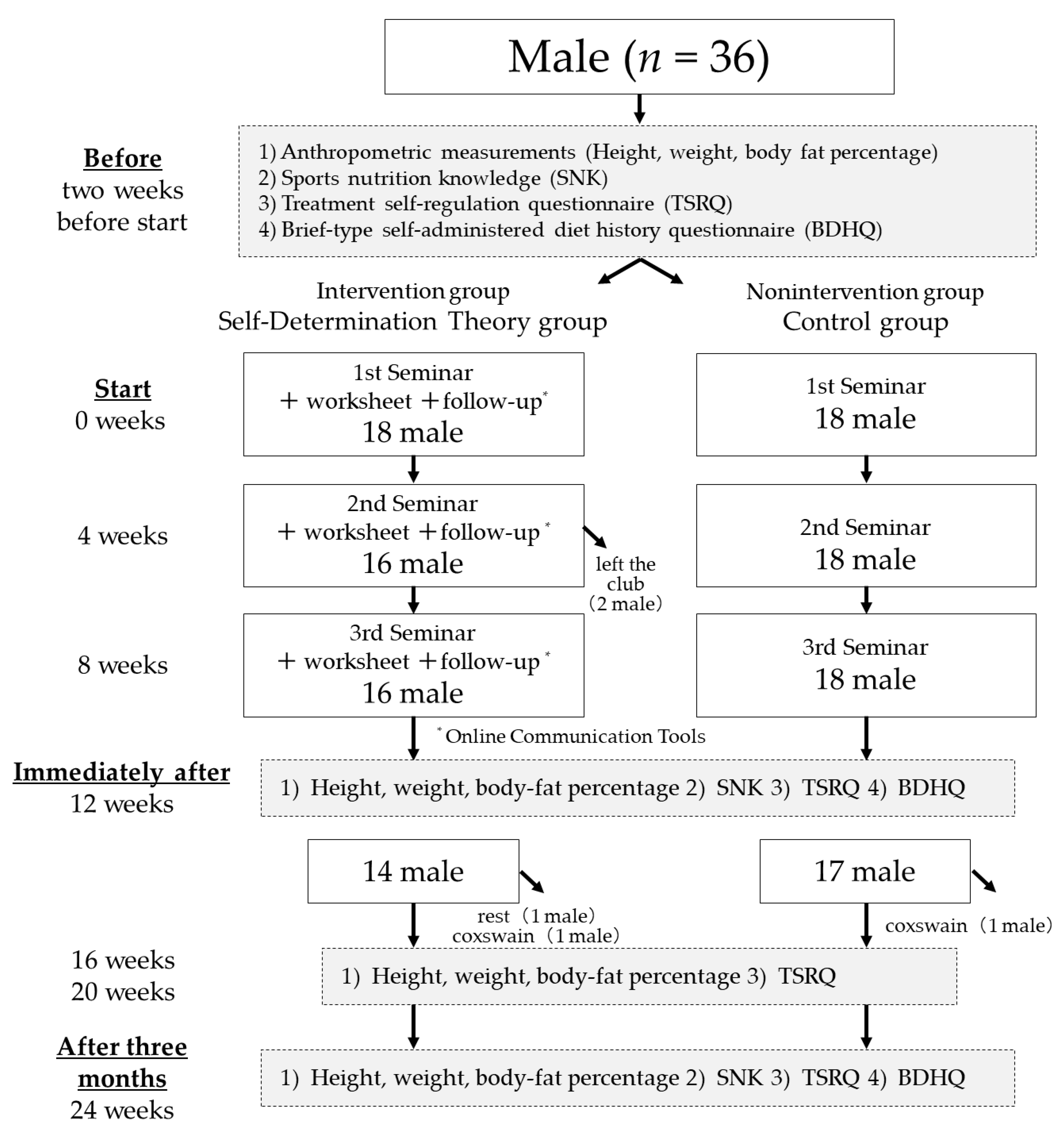

Table 1.
Results of between-group and within-group factor analysis of BDHQ.
| Grouping factor | Within-group factor | ||||||
|---|---|---|---|---|---|---|---|
| Reciprocal action Group × Time p † | Time Main Effects p † | Immediately after − Before p ‡ | After three months − Before p ‡ | After three months − Immediately after p ‡ | Multiple comparison test | ||
| BDHQ (Nutrient intake) | |||||||
| Energy (kcal) | 0.413 | 0.059 | |||||
| Protein (g) | 0.652 | 0.114 | |||||
| Fat (g) | 0.853 | 0.810 | |||||
| Carbohydrate (g) | 0.307 | 0.021 * | 0.059 | 0.090 | 1.000 | n.s | |
| Calcium (mg) | 0.939 | 0.026 * | 0.054 | 0.178 | 1.000 | n.s | |
| Iron (mg) | 0.757 | 0.056 | |||||
| Vitamin D (μg) | 0.314 | 0.059 | |||||
| Vitamin B1 (mg) | 0.832 | 0.080 | |||||
| Vitamin C (mg) | 0.854 | 0.050 | |||||
| Dietary fiber (g) | 0.967 | 0.295 | |||||
| BDHQ (Intake by food group) | |||||||
| Cereals (g) | 0.305 | 0.068 | |||||
| Potatoes (g) | 0.806 | 0.553 | |||||
| Sugar and sweeteners (g) | 0.864 | 0.051 | |||||
| Pulses (g) | 0.407 | 0.121 | |||||
| Green and yellow vegetables (g) | 0.450 | 0.009 * | 0.009 * | 0.204 | 0.735 | Before < Immediately After | |
| Other vegetables (g) | 0.769 | 0.435 | |||||
| Fruits (g) | 0.735 | 0.013 * | 0.020 * | 0.619 | 0.267 | Before < Immediately After | |
| Fish and shellfish (g) | 0.467 | 0.070 | |||||
| Meats (g) | 0.521 | 0.527 | |||||
| Eggs (g) | 0.973 | 0.871 | |||||
| Dairy products (g) | 0.657 | 0.012 * | 0.040 * | 0.770 | 0.076 | Before < Immediately After | |
| Fats and oils (g) | 0.252 | 0.322 | |||||
| Confectioneries(g) | 0.688 | 0.418 | |||||
| Beverages (g) | 0.713 | 0.052 | |||||
| Seasonings and spices (g) | 0.394 | 0.148 | |||||
* p < 0.05: Significant difference n.s: Not significant; † A two-way ANOVA was conducted on the between-group and within-group factors; ‡ Multiple comparison tests using the Bonferroni method were performed for before, after, after three months within-group factors; < less than,> more than; BDHQ: Brief-type self-administered diet history questionnaire.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



