
Submitted:
06 February 2024
Posted:
07 February 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Abstract: Background: Patients with diabetes are particularly susceptible to COVID-19 infection, which can result in severe respiratory illness. Methods: This study conducted a comparative as-sessment of the impact of antiviral therapy using molnupiravir and favipiravir in COVID-19 pa-tients with underlying diabetes. A cohort of one hundred individuals infected with SARS-CoV-2, diagnosed with diabetes, and consecutively admitted, was included in the present study. These patients were treated with antivirals according to local guidelines: Group F (51 cases) was treated with favipiravir – 10 days and Group M (49 cases) was treated with molnupiravir – 5 days. Re-sults: In Group F, the average hospitalization was higher than in Group M (11.29±2.27 vs. 7.14±3.16, p
Keywords:
SARS-CoV-2
; favipiravir
; molnupiravir
; diabetes mellitus
; COVID-19
1. Introduction
COVID-19 is an infectious ailment characterized by its high level of contagion and pathogenicity [1]. This disease is attributed to the pandemic that emerged in recent years, with numerous confirmed infections and thousands of fatalities registered worldwide to date, and these numbers continue to rise.
The name "coronavirus" is derived from the microscopic appearance of the viral surface, which resembles a crown with spike glycoproteins. The tropism of the coronavirus is notably influenced by the spike (S) protein, which plays a critical role in virus infection by facilitating its attachment to the surface of host cells [2]. Structural and non-structural proteins are encoded by the viral genome [1]. Structural proteins ensure infectivity, viral attachment, morphological structure formation, and exocytosis [3,4,5], while non-structural proteins play a pivotal role in the processes of transcription and replication of the virus [6].
In December 2019, initial instances of severe pneumonia with undetermined origin emerged in China. Subsequent investigation revealed these cases to be attributed to the coronavirus known as severe acute respiratory syndrome 2 (SARS-CoV-2) [7]. The COVID-19 symptomatic display varies from typical symptoms of acute respiratory infection to a wide range of manifestations, due to both immediate and delayed complications. In a study published by Rodrigo R. et al. in November 2020, analyzing 152 publications and 41,409 COVID-19 patients, the most frequently reported symptoms were fever (56.66%), cough (54.52%), dyspnea (30.82%), asthenia (28.16%), dysphagia (14.41%), diarrhea (9.59%), productive cough (25.33%), myalgia (16.9%), headache (12.17%), neurological manifestations (20.82%), and chest pain (11.49%) [8].
Currently, there are specific vaccines for this infection and non-specific antiviral therapies. Numerous vaccines have been formulated and administered to restrain the proliferation of infection. However, mutations in the viral sequence have introduced several viral variants, posing challenges to these endeavors undertaken by the global healthcare system [9].
The treatment of SARS-CoV-2 infection includes combining antiviral therapy with other medications such as anticoagulants, antibiotics, monoclonal antibodies, immunomodulatory drugs, glucocorticoids, probiotics, diet therapy, and individualized rehabilitation program [10,11]. At present, there exists no authorized antiviral treatment specifically tailored for SARS-CoV-2 infection. However, certain antiviral drugs, such as remdesivir, have been approved and used for the management of COVID-19 [12]. Additionally, other antiviral drugs like favipiravir, molnupiravir, and nirmatrelvir/ritonavirare currently undergoing evaluation in clinical studies [13,14]. Nonetheless, no antiviral medication has been deemed both safe and efficacious for COVID-19 at present.
Favipiravir, originally designated as T-705, received its initial approval in 2014 by the Japanese Agency of Medical and Pharmaceutical Products as a treatment for influenza [15]. It has subsequently demonstrated its efficacy against ribonucleic acid (RNA) viruses such as Ebola virus, rhinoviruses, and respiratory syncytial virus [16]. Favipiravir operates as an RNA-dependent RNA polymerase (RdRp) inhibitor. Host enzymes convert it into T-705 ribofuranosyl 5'-triphosphate, functioning as a nucleotide analogue that discriminately impedes viral RdRp activity [17,18,19]. Studies have shown that patients with mild and moderate COVID-19 treated with favipiravir experienced a favorable clinical evolution and good tolerance compared to standard supportive therapy [20,21]. The most reported adverse effects of favipiravir include hyperuricemia, diarrhea, neutropenia, and hepatocytolysis syndrome [21].
In the last few years, molnupiravir has garnered significant interest due to its capacity to hinder SARS-CoV-2 replication, rapidly clear the virus, reduce viral load, and lead to rapid recovery in COVID-19 patients. Moreover, this oral active RdRp inhibitor is recognized for its favorable pharmacokinetic profile [20]. Molnupiravir is categorized as a prodrug, being the isopropyl ester of the ribonucleoside analogue β-D-N4-hydroxycytidine [18,22]. In vitro, evidence shows that molnupiravir is a potent inhibitor of SARS-CoV-2 replication, with an effective half-maximum concentration in the submicromolar range [23,24]. A study by Fischer W. et al., in 2021, on 202 molnupiravir-treated patients showed that the time required for viral RNA elimination was significantly reduced by 92.5% in patients treated with molnupiravir compared to 80.3% with placebo [25]. Molnupiravir has been shown to be safe and effective in reducing the risk of hospitalization and unfavorable outcomes in 50% of mild and moderate COVID-19 cases, particularly in patients with underlying risk factors (i.e., cardiovascular diseases, age > 60 years, diabetes mellitus) for adverse outcomes [26].
Both favipiravir and molnupiravir are antiviral medications that have been integrated into the therapeutic regimen for patients with COVID-19, including those grappling with the concurrent presence of diabetes mellitus. Substantive medical assessments have highlighted the potential efficacy of both antivirals, indicative of its ability to curtail recovery timelines and alleviate the severity of symptoms among individuals affected by COVID-19. Remarkably, emerging evidence has even suggested that favipiravir could enhance survival prospects for patients who encounter the more severe manifestations of the disease [20]. Moreover, it's worth noting that favipiravir has demonstrated commendable tolerability within the diabetic patient population, signifying its capability to be administered without inducing substantial fluctuations in blood glucose levels or other significant side effects. A systematic literature review conducted in 2021 by Singh A.K et al supports that molnupiravir demonstrates positive effects in patients with mild forms of COVID-19, while severe and moderate forms of the disease require further studies. [27].
Unfavorable outcomes in cases of SARS-CoV-2 infection are influenced by a range of significant risk factors. These factors encompass not only advanced age, particularly above 60 but also conditions such as obesity, cardiovascular diseases, chronic obstructive pulmonary disease, diabetes mellitus, and chronic kidney disease. Furthermore, individuals who have faced oncological conditions or undergone organ transplantation are also identified as particularly vulnerable to experiencing severe consequences in the context of COVID-19 infection. These risk factors collectively underscore the complex interplay of various health determinants in shaping the course and impact of SARS-CoV-2 infection [28].
Diabetes mellitus is a chronic disease that has reached an alarming number in recent years, and it triples the risk of hospitalization in the H1N1 influenza pandemic and the transfer to intensive care or unfavorable patient outcome [29,30]. Patients with diabetes exhibit notable concentrations of plasminogen, an enzyme that contributes to the breakdown of the SARS-CoV-2 spike protein. This process enhances the virus's capability to infiltrate cells, thereby amplifying its virulence and potential for infection [31]. Furthermore, diabetic patients have demonstrated elevated levels of proinflammatory biomarkers, including D-dimers, C-reactive protein (CRP), and interleukin-6, when compared to individuals without this medical condition. [32,33,34].
In general, the existing body of research has indicated that both favipiravir and molnupiravir hold promise as potential treatment options for individuals suffering from COVID-19. However, it's important to note that studies present differing viewpoints on the effectiveness of these antivirals [20,25,26,35]. Therefore, further investigation is essential to validate these findings and comprehensively understand the intricate safety and efficacy profiles of favipiravir and molnupiravir in managing COVID-19 patients with diabetes mellitus. Given the aforementioned context, the objective of this study was to evaluate the therapeutic effectiveness of antiviral interventions involving both favipiravir and molnupiravir within the population of adult patients concurrently dealing with COVID-19 and diabetes mellitus.
2. Materials and Methods
2.1. Study design
Between November 2021 and April 2022, a retrospective study was carried out at the Emergency County Clinical Hospital in Oradea, Romania and it included consecutively admitted diabetic patients with COVID-19.
Prior to initiating antiviral treatment and upon admission to the hospital, all patients were granted informed consent. The study was approved by the Ethics Committee of Medicine and the Faculty of Pharmacy, University of Oradea (Approval No. 31466/05.11.2020), and it followed the Code of Ethics of the World Medical Association (Declaration of Helsinki, 1967).
The initial cohort was selected according to the inclusion and exclusion criteria, Figure 1. The study's inclusion criteria encompassed:
- Being aged above 18 years;
- Pre-existing diagnosis of type II diabetes prior to inclusion in the study;
- Positive test for the identification of SARS-CoV-2 viral antigen or RNA;
- No history of previous antiviral therapy.
- The exclusion criteria from the study were:
- Pregnancy;
- Death before completing the antiviral treatment period;
- Absence from the 10-day follow-up appointment after hospital admission, within the hospital outpatient clinic.
- The need to change to another antiviral treatment.
Patients were treated with antivirals based on the available stock of molecules within the hospital during the observed period, and in accordance with the regional treatment guidelines valid during the studied period. The study participants were categorized into two distinct groups: Group F was treated with favipiravir, and Group M with molnupiravir. In Group F, the dosage of favipiravir was administered for 10 days, starting with a loading dose of 1600 mg twice a day (TID), followed by 600 mg TID. In Group M, molnupiravir was administered for 5 days, with a dose of 800 mg TID.
The COVID-GRAM risk score (Figure 2), a clinical risk assessment tool, was applied to all patients upon admission and at the end of antiviral therapy. The scoring system was developed to assess the clinical risk and prognostic outlook of COVID-19 patients admitted to the hospital. The scoring criteria encompassed a comprehensive set of parameters for evaluation. These factors include level of direct bilirubin, unconsciousness, neutrophil-lymphocyte ratio, age, pulmonary imaging changes, dyspnea, number of comorbidities (0-5), hemoptysis, level of lactate dehydrogenase (LDH), and cancer history. The score considered a range of comorbidities for assessment, including cerebral vascular disease, diabetes mellitus, chronic obstructive pulmonary disease, chronic heart disease, cancer, chronic kidney disease, hypertension, coronary heart disease, immunodeficiency, and hepatitis B, and was calculated using an online calculator [36,37].
2.2. Data Collection
The demographic data, incorporating age, sex, and place of origin, along with the history of past medical conditions, vaccination history against COVID-19 in the last 12 months (VHC), clinical data [stomatitis, diarrhea, abdominal pain, nausea, vomiting, dizziness, oxygen saturation (SpO2), BMI, period from onset to hospitalization (POH)], number of hospitalization days, and paraclinical investigations [complete blood count (CBC), ferritin, D-dimers, CRP, HbA1c, LDH, direct bilirubin, chest computed tomography (CCT)] were collected from the patient's medical records. Paraclinical investigations (ALAT, D-dimers), and the COVID-GRAM risk score were evaluated in two stages:
t0 = before starting the treatment with molnupiravir and favipiravir;
t1 = at the end of the antiviral treatment.
All patients had their CRP values measured upon admission (t0), at the end of antiviral treatment (t1: 5 days for M group, 10 days for F group), and on day 10 from admission, for patients from M group discharged before 10 days. Patients discharged before 10 days, were called in for a follow-up visit at the hospital's outpatient clinic, on day 10.
The collected data was encoded to ensure anonymity. The demographic data, past medical history, clinical data, and values of ferritin, LDH, and SpO2 were used to compare the severity of COVID-19 in the enrolled patients. At the point of hospitalization, all patients underwent CCT scans.
The diagnosis of COVID-19 was validated through either the detection of SARS-CoV-2 antigens (i.e., rapid test) or a single positive real-time polymerase chain reaction test, following the World Health Organization's (WHO) recommendations. In adherence to the guidelines provided by the WHO, specimens from the pharynx and oropharynx were collected and appropriately transported [38].
The patients' SpO2 was evaluated using a Human Pulse Oximeter (Human Accurate Bio-Medical Technology Co., Ltd, China).
Laboratory investigations, including CBC, direct bilirubin, HbA1c, D-dimers, ferritin, and LDH, were collected from venous blood samples using specific vacutainer tubes for each test. For the CBC, ethylenediaminetetraacetic acid (EDTA) was employed as an anticoagulant in the collection of venous blood samples using tubes. Upon collection, all samples were promptly transported to the hospital's laboratory for analysis. The CBC examination was carried out utilizing the Beckman Coulter 628134 UniCel DxH Hematology Analyzer 800 from Beckman Coulter International S.A., USA. Interpretation of reference values was tailored to the patient's age and gender. For the assessment of HbA1c levels, venous blood samples were obtained using vacutainer tubes with EDTA as an anticoagulant and were subsequently analyzed utilizing the ALINITY AC analyzer (Indonesia). The reference values were computed in accordance with the patient's gender and age.
To assess D-dimer levels, venous blood samples were collected in vacutainer tubes with 0.105 M sodium citrate and analyzed using the ALINITY AC analyzer (Indonesia). To determine the levels of ferritin, venous blood samples were acquired using vacutainer tubes without the inclusion of any anticoagulant agent and analyzed using the Alinity Abbott analyzer (Indonesia). To assess the blood transaminase level, venous blood samples were placed in tubes without anticoagulant. The measurement was performed using the Beckman Coulter AU5811 Chemistry analyzer, a device manufactured by Beckman Coulter International S.A. For the determination of CRP values, blood samples were collected in vacutainer tubes without anticoagulant, and the analysis was subsequently performed using Beckman Coulter AU5811. Reference values for the transaminase level were determined based on factors such as age, sex, and the specific assay employed, ensuring accurate interpretation of the results. All samples were collected during fasting and immediately transported to the hospital's laboratory for analysis.
2.3. Statistical analysis
The sample size of patients included in the study was calculated considering the total number of adult patients hospitalized during the observed period. To calculate the sample size, we considered the following variables:
- p: the probability of the phenomenon, where 0 ≤ p ≤ 1,
- q: the complementary probability, where q = 1 - p,
- t: the probability factor,
- Δx: the permissible margin of error,
- N: the population size.
To determine the sample size of cases, we used the following formula: n = t2pq/(Δx2 + t2pq /N). The formula is applicable to studies in which the observed characteristic is binary (in this case: the comparison between treatment with favipiravir and treatment with molnupiravir). The value of "n" is maximized when the product "pq" is at its maximum, which occurs when "p" and "q" are both equal to 0.5. A 95% probability corresponds to a "t" value of 1.96. An acceptable margin of error of 0.1 has been established. If "N" is large (over 10,000), the ratio "t2pq/N" can be neglected. In the case of an adult population hospitalized during the observed period of 1031 individuals, the minimum sample size is 96.
Statistical analysis was performed utilizing the Statistical Package for Social Sciences (SPSS), version 26, (IBM Corp., Armonk, New York, United States) [39]. The data were showcased through numeric values (N), proportions (%), means (M), and standard deviations (SD). Statistical significance (p-value) was computed utilizing the chi-squared test, Student's t-test, and log-rank test for Kaplan-Meier method.
3. Results
Throughout the study duration, 105 patients with both COVID-19 and diabetes mellitus fulfilled the inclusion criteria for the investigation. A total of 5 patients changed their antiviral treatment before completing the course and were subsequently excluded from the study. One hundred subjects completed the study, with 51 patients in Group F and 49 in Group M. Statistically significant differences were not observed in the demographic characteristics of the two groups (Table 1). The samples had a normal distribution [COVID-GRAM risk score (Group F, p = 0.057); (Group M, p = 0.064); (Shapiro-Wilk test)].
At the end of the treatment period (t1), the COVID-GRAM risk score exhibited a statistically significant decrease only within the M group compared to baseline (t0) (156.29±61.32; 160.59±59.41, p<0.001), (Figure 3).
F_0, starting time of the favipiravir; F_1, end time of the favipiravir; M_0, starting time of the molnupiravir; M_1, end time of the molnupiravir; P, value as determined by t-test.
Even though a minor decline in the count of high-risk patients for severe illness was noted in both groups, this decrease was not statistically significant (Table 2).
The number of patients who died after completing antiviral treatment but during the current hospitalization was markedly reduced in group M when compared to group F [2 (4.08%) vs. 9 (17.65%), p=0.034]. The patients who received treatment with molnupiravir stayed 4.15 days less in the hospital compared to those who received treatment with favipiravir (7.14±3.16; 11.29±2.27; p<0.001) (Figure 4).
The D-dimer values recorded in the two groups upon admission to hospital (t0) compared to at the end of antiviral treatment (t1) were less statistically significant only in the group treated with molnupiravir [group F (t0:1039.18 ± 801.80 ng/mL, t1: 987.31 ± 695.82 ng/mL, p=0.311); group M (t0:1106.02 ± 1439.30 ng/mL, t1: 754.69 ± 783.01 ng/mL, p=0.016)], (Figure 5).
The CRP values were statistically significantly lower at the end of the molnupiravir therapy compared to the decrease observed in the group that received treatment with favipiravir, [group F (t0: 93.02 ± 90.96 mg/L, t1: 87.47 ± 91.38 mg/L, p=0.088); group M (t0: 60.92 ± 73.41 mg/L, t1: 52.75 ± 65.40 mg/L, p<0.001)]. The number of patients with CRP normalization after 10 days from hospital admission was significantly different between the two groups [33 (67.35%) in the M group vs. 16 (31.37%%) in the F group, P<0.001]. (Figure 6).
Adverse reactions were statistically significantly more frequently reported in the group of patients treated with favipiravir (Table 3). Out of the clinical symptoms reported by subjects as having a negative impact during antiviral treatment, diarrhea was more commonly observed in the group that received favipiravir regime.
The ALAT values in the two groups did not show a statistically significant difference at the end point of the antiviral therapy [group M (38.17 ± 7.26) vs group F (39.87 ± 8.45), p=0.282, t-test].
4. Discussion
COVID-19 has become a major global challenge since 2019. The SARS-CoV-2 infection has affected millions of people, putting pressure on healthcare systems, causing suffering, and increasing the number of deaths in all communities. Antiviral therapy has been a crucial point in the fight against the pandemic.
The COVID-GRAM risk score, introduced for the first time in 2020, was employed to identify intensive care unit admissions, the need for mechanical ventilation, and mortality among hospitalized COVID-19 patients [36]. The score tracks a set of 10 independent factors that are typically used to monitor the progress of a hospitalized COVID-19 patient. At the conclusion of the treatment (t1), the COVID-GRAM risk score exhibited a statistically significant decrease in the M group when compared to its initial value (t0) (156.29±61.32; 160.59±59.41, p<0.001). Nonetheless, despite a slight reduction in the number of high-risk patients for severe illness in both groups, this decline did not reach statistical significance. In contrast to the F group, the M group experienced a significant reduction in the number of patients who passed away during the current hospitalization after completing antiviral treatment [M group: 2 (4.08%) vs F group: 9 (17.65%), p=0.034]. In a retrospective study involving a cohort of 26,554 COVID-19 patients in the United States, with at least one predictor of severe progression, published in 2023, Prajapati G. and colleagues reported that patients treated with molnupiravir required admission to intensive care in a low percentage of 0.3%, the need for oxygen therapy was recorded in 0.1% of patients, and those requiring invasive mechanical ventilation accounted for 0.1% [40]. Multiple studies explore the use of molnupiravir following the identification of the Omicron variants (November 2021) [41,42,43,44,45], using data from the United States, Israel, and Hong Kong, participants with risk factors for severe COVID-19. The majority of patients in the U.S. and Israeli studies were COVID-19 single-vaccinated. In the U.S. Veterans Health Administration study, on old patients (68-75 years), the hospitalization/death rate, within one month from the initiation of molnupiravir treatment was 4.5%. The one-month hospitalization/death rate for molnupiravir in the MOVe-OUT study was 6.8% [46]. In the PANORAMA study, the 28-day hospitalization/mortality rate with monopiravir was 1%, the same with usual care. But, in this particular study, the population did not include patients in the highest risk categories who are clinically particularly vulnerable. Specifically, the average age of participants was <60 years, one in three had no comorbidities, and the vast majority (94%) had been vaccinated with more than 2 doses of COVID-19 vaccine [47]. The PIONEER study examined 499 hospitalized COVID-19 patients and found no significant difference in 28-day mortality rate (10% in the favipiravir group vs. 14% in the standard care group) [48]. In the study by Al-Muhsen S. and colleagues, on 598 hospitalized patients with moderate/severe COVID-19, favipiravir was associated with longer hospital stays and a higher mortality rate compared to no favipiravir regimen [49]. In a meta-analysis of 2702 studies, Özlüşen B. and colleagues reported that there were no statistically significant differences in death rates or the need for mechanical ventilation between patients with severe/moderate forms of COVID-19 treated with favipiravir and those receiving standard care [50]. Our results align with the conclusions of medical studies conducted on moderate/severe forms of COVID-19 patients, older than 65 years, with risk factors for severe progression (such as diabetes, in this case), in predominantly unvaccinated individuals.
Infection with SARS-CoV-2 results in D-dimer levels that are twice as high as those seen in cases of community-acquired pneumonia [51]. Several studies have suggested an indirect link between D-dimer levels and a heightened risk of thrombosis, establishing D-dimer as a prognostic factor in COVID-19 patients [51,52,53,54]. This study has indicated that D-dimer values were lower after the conclusion of molnupiravir treatment when compared to the group receiving favipiravir treatment. In a study conducted by Pontolillo M. et al., which involved 100 individuals with mild to moderate COVID-19, the research findings indicated that D-dimer levels remained unaffected at both 7 and 10 days into the treatment with molnupiravir [55]. In a study led by Mutair A. et al., which involved 538 COVID-19 patients, with 50% of them receiving favipiravir and the other 50% undergoing different antiviral treatments, the results revealed that patients treated with favipiravir showed reduced D-dimer levels when compared to those who received alternative antiviral medications [56].
The hepatic synthesis of CRP is stimulated by interleukin-6, a pro-inflammatory cytokine in the context of tissue damage either traumatically or in a specific pathological process, practically, it is correlated with the magnitude of the inflammatory process. In a study conducted on 209 adult patients with non-severe COVID-19, Wang G. and colleagues argue that an increase in CRP by one unit is equivalent to a 5% increase in the risk of developing severe disease [57]. Our findings indicate a significant decrease in CRP values at the end of antiviral treatment in the group treated with molnupiravir. Furthermore, it is noteworthy that this reduction is faster, considering that the comparison was made at the end of the antiviral treatment period (which is 5 days for molnupiravir and 10 days for favipiravir), and the number of patients who had normal CRP values on day 10 of hospitalization was statistically significantly higher in group M. Our results align with those obtained by Johnson M.G. and colleagues, who assert in the MOVe-OUT trial that CRP values in adult COVID-19 patients treated with molnupiravir significantly improved statistically after the third day of antiviral treatment [58]. Pontolillo M. at all. state in a study conducted on 100 participants with COVID-19 a statistically significant improvement in CRP values at 7/10 days after the initiation of treatment with molnupiravir [55]. On the other hand, medical studies present conflicting results regarding the effect of favipiravir on CRP [59,60].
Adverse drug reactions can lead to treatment inefficiency either by necessitating its discontinuation due to its high severity or through patients' difficult adherence to the treatment or due to the drug interactions they may generate. In the present study, adverse reactions were observed in both groups of monitored patients, but their frequency was statistically significantly higher in the group that received favipiravir treatment. Furthermore, diarrhea was statistically significantly more frequently reported in this group. Currently, molnupiravir is authorized by the United States Food and Drug Administration (FDA) (the last from October 3, 2023) for the treatment of COVID-19 patients with mild to moderate forms and risk factors, and adverse reactions are under monitoring [61]. In a study conducted by Santi Laurini, G. and colleagues, based on adverse effects recorded in the FDA Adverse Event Reporting System regarding molnupiravir therapy, it is suggested that the most commonly reported complaints were of gastrointestinal nature (diarrhea, nausea) and cutaneous [62]. Adverse reactions following the administration of favipiravir, in the study conducted by Ergür F. and colleagues on a sample of 357 patients, were most frequently associated with hepatic impairment and gastrointestinal complaints (diarrhea, nausea, and abdominal pain) [63]. The results obtained by us align with current medical studies, but it seems that molnupiravir exhibits greater tolerance in comparison to favipiravir. Nevertheless, studies conducted over a more extended duration are necessary to substantiate this observation.
5. Conclusions
The present study suggests that molnupiravir could be a promising option in the treatment of hospitalized adult COVID-19 patients with diabetes, with positive results in terms of reducing the risk of severe complications, controlling inflammation, and tolerability. Reducing the length of hospitalization leads to a decrease in associated costs, especially for individuals over the age of 65 [64]. Considering the multitude of complications that COVID-19 can induce in both the immediate and extended periods, promptly halting viral replication during the illness is crucial for restoring the body's balance. However, it is essential to conduct further long-term investigations to support these findings and to assess the efficacy and safety of molnupiravir in managing COVID-19.
Author Contributions
Conceptualization, Andreea Fitero and Nicoleta Negrut; Data curation, Andreea Fitero and Paul Andrei Negru; Formal analysis, Andreea Fitero and Nicoleta Negruț; Investigation, Andreea Fitero, 0and Nicoleta Negrut; Methodology, Andreea Fitero, Delia Carmen Nistor Cseppento and Nicoleta Negruț; Resources, Andreea Fitero and Paul Andrei Negru; Software, Paul Andrei Negru and Nicoleta Negruț; Supervision, Delia Mirela Tit and Simona Gabriela Bungau; Validation, Delia Mirela Tit and Paul Andrei Negru; Visualization, Delia Carmen Nistor Cseppento and Delia Mirela Tit; Writing – original draft, Andreea Fitero, Nicoleta Negruț, Delia Mirela Tit and Andrei-Flavius Radu; Writing – review & editing, Simona Gabriela Bungau, Cristian Bustea and Andrei-Flavius Radu.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the Ethics Committee of Medicine and the Faculty of Pharmacy, University of Oradea (Approval No. 31466/05.11.2020), and it followed the Code of Ethics of the World Medical Association (Declaration of Helsinki, 1967).
Informed Consent Statement
All the patients signed an informed consent at their hospitalization.
Data Availability Statement
All data are registered at the Bihor County Clinical Hospital Oradea, Bihor County, Romania.
Acknowledgments
The authors express their gratitude to the University of Oradea, Oradea, Romania, for supporting the APC.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mittal, A.; Manjunath, K.; Ranjan, R.K.; Kaushik, S.; Kumar, S.; Verma, V. COVID-19 pandemic: Insights into structure, function, and hACE2 receptor recognition by SARS-CoV-2. PLoS Pathog. 2020, 16, e1008762. [Google Scholar] [CrossRef] [PubMed]
- Behl, T.; Kaur, I.; Aleya, L.; Sehgal, A.; Singh, S.; Sharma, N.; Bhatia, S.; Al-Harrasi, A.; Bungau, S. CD147-spike protein interaction in COVID-19: Get the ball rolling with a novel receptor and therapeutic target. Sci. Total Environ. 2022, 808, 152072. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, H.; Pöhlmann, S. Cellular entry of the SARS coronavirus. Trends Microbiol. 2004, 12, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Vennema, H.; Godeke, G.J.; Rossen, J.W.; Voorhout, W.F.; Horzinek, M.C.; Opstelten, D.J.; Rottier, P.J. Nucleocapsid-independent assembly of coronavirus-like particles by co-expression of viral envelope protein genes. EMBO J. 1996, 15, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Siu, Y.L.; Teoh, K.T.; Lo, J.; Chan, C.M.; Kien, F.; Escriou, N.; Tsao, S.W.; Nicholls, J.M.; Altmeyer, R.; Peiris, J.S.M.; et al. The M, E, and N structural proteins of the severe acute respiratory syndrome coronavirus are required for efficient assembly, trafficking, and release of virus-like particles. J. Virol. 2008, 82, 11318–11330. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Yan, L.; Huang, Y.; Liu, F.; Zhao, Y.; Cao, L.; Wang, T.; Sun, Q.; Ming, Z.; Zhang, L.; et al. Structure of the RNA-dependent RNA polymerase from COVID-19 virus. Science (80-.). 2020, 368, 779–782. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- da Rosa Mesquita, R.; Francelino Silva Junior, L.C.; Santos Santana, F.M.; Farias de Oliveira, T.; Campos Alcântara, R.; Monteiro Arnozo, G.; Rodrigues da Silva Filho, E.; Galdino Dos Santos, A.G.; Oliveira da Cunha, E.J.; Salgueiro de Aquino, S.H.; et al. Clinical manifestations of COVID-19 in the general population: systematic review. Wien. Klin. Wochenschr. 2021, 133, 377–382. [Google Scholar] [CrossRef]
- Behl, T.; Kaur, I.; Sehgal, A.; Singh, S.; Sharma, N.; Anwer, M.K.; Makeen, H.A.; Albratty, M.; Alhazmi, H.A.; Bhatia, S.; et al. There is nothing exempt from the peril of mutation – The Omicron spike. Biomed. Pharmacother. 2022, 148, 112756. [Google Scholar] [CrossRef]
- Nistor-Cseppento, C.D.; Moga, T.D.; Bungau, A.F.; Tit, D.M.; Negrut, N.; Pasca, B.; Bochis, C.F.; Ghitea, T.C.; Jurcau, A.; Purza, A.L.; et al. The Contribution of Diet Therapy and Probiotics in the Treatment of Sarcopenia Induced by Prolonged Immobilization Caused by the COVID-19 Pandemic. Nutrients 2022, 14, 4701. [Google Scholar] [CrossRef]
- Moga, T.D.; Nistor-Cseppento, C.D.; Bungau, S.G.; Tit, D.M.; Sabau, A.M.; Behl, T.; Nechifor, A.C.; Bungau, A.F.; Negrut, N. The Effects of the “Catabolic Crisis” on Patients’ Prolonged Immobility after COVID-19 Infection. Medicina (B. Aires). 2022, 58, 828. [Google Scholar] [CrossRef] [PubMed]
- Negrut, N.; Codrean, A.; Hodisan, I.; Bungau, S.; Tit, D.M.; Marin, R.; Behl, T.; Banica, F.; Diaconu, C.C.; Nistor-Cseppento, D.C. Efficiency of antiviral treatment in COVID-19. Exp. Ther. Med. 2021, 21, 648. [Google Scholar] [CrossRef] [PubMed]
- Eloy, P.; Le Grand, R.; Malvy, D.; Guedj, J. Combined treatment of molnupiravir and favipiravir against SARS-CoV-2 infection: One + zero equals two? EBioMedicine 2021, 74, 103663. [Google Scholar] [CrossRef] [PubMed]
- Najjar-Debbiny, R.; Gronich, N.; Weber, G.; Khoury, J.; Amar, M.; Stein, N.; Goldstein, L.H.; Saliba, W. Effectiveness of Paxlovid in Reducing Severe Coronavirus Disease 2019 and Mortality in High-Risk Patients. Clin. Infect. Dis. 2023, 76, e342–e349. [Google Scholar] [CrossRef] [PubMed]
- Negru, P.A.; Radu, A.-F.; Vesa, C.M.; Behl, T.; Abdel-Daim, M.M.; Nechifor, A.C.; Endres, L.; Stoicescu, M.; Pasca, B.; Tit, D.M.; et al. Therapeutic dilemmas in addressing SARS-CoV-2 infection: Favipiravir versus Remdesivir. Biomed. Pharmacother. 2022, 147, 112700. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Adhikari, N.K.J.; Kwon, H.Y.; Teo, K.; Siemieniuk, R.; Lamontagne, F.; Chan, A.; Mishra, S.; Murthy, S.; Kiiza, P.; et al. Anti-Ebola therapy for patients with Ebola virus disease: a systematic review. BMC Infect. Dis. 2019, 19, 376. [Google Scholar] [CrossRef] [PubMed]
- Baranovich, T.; Wong, S.-S.; Armstrong, J.; Marjuki, H.; Webby, R.J.; Webster, R.G.; Govorkova, E.A. T-705 (favipiravir) induces lethal mutagenesis in influenza A H1N1 viruses in vitro. J. Virol. 2013, 87, 3741–3751. [Google Scholar] [CrossRef] [PubMed]
- Jin, Z.; Smith, L.K.; Rajwanshi, V.K.; Kim, B.; Deval, J. The ambiguous base-pairing and high substrate efficiency of T-705 (Favipiravir) Ribofuranosyl 5’-triphosphate towards influenza A virus polymerase. PLoS One 2013, 8, e68347. [Google Scholar] [CrossRef]
- Vanderlinden, E.; Vrancken, B.; Van Houdt, J.; Rajwanshi, V.K.; Gillemot, S.; Andrei, G.; Lemey, P.; Naesens, L. Distinct Effects of T-705 (Favipiravir) and Ribavirin on Influenza Virus Replication and Viral RNA Synthesis. Antimicrob. Agents Chemother. 2016, 60, 6679–6691. [Google Scholar] [CrossRef]
- Udwadia, Z.F.; Singh, P.; Barkate, H.; Patil, S.; Rangwala, S.; Pendse, A.; Kadam, J.; Wu, W.; Caracta, C.F.; Tandon, M. Efficacy and safety of favipiravir, an oral RNA-dependent RNA polymerase inhibitor, in mild-to-moderate COVID-19: A randomized, comparative, open-label, multicenter, phase 3 clinical trial. Int. J. Infect. Dis. 2021, 103, 62–71. [Google Scholar] [CrossRef]
- Pilkington, V.; Pepperrell, T.; Hill, A. A review of the safety of favipiravir – a potential treatment in the COVID-19 pandemic? J. Virus Erad. 2020, 6, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Imran, M.; Kumar Arora, M.; Asdaq, S.M.B.; Khan, S.A.; Alaqel, S.I.; Alshammari, M.K.; Alshehri, M.M.; Alshrari, A.S.; Mateq Ali, A.; Al-Shammeri, A.M.; et al. Discovery, Development, and Patent Trends on Molnupiravir: A Prospective Oral Treatment for COVID-19. Molecules 2021, 26, 5795. [Google Scholar] [CrossRef] [PubMed]
- Menéndez-Arias, L. Decoding molnupiravir-induced mutagenesis in SARS-CoV-2. J. Biol. Chem. 2021, 297, 100867. [Google Scholar] [CrossRef] [PubMed]
- Agostini, M.L.; Pruijssers, A.J.; Chappell, J.D.; Gribble, J.; Lu, X.; Andres, E.L.; Bluemling, G.R.; Lockwood, M.A.; Sheahan, T.P.; Sims, A.C.; et al. Small-Molecule Antiviral β-d-N(4)-Hydroxycytidine Inhibits a Proofreading-Intact Coronavirus with a High Genetic Barrier to Resistance. J. Virol. 2019, 93, e01348-19. [Google Scholar] [CrossRef] [PubMed]
- Fischer, W.A. 2nd; Eron, J.J.J.; Holman, W.; Cohen, M.S.; Fang, L.; Szewczyk, L.J.; Sheahan, T.P.; Baric, R.; Mollan, K.R.; Wolfe, C.R.; et al. A phase 2a clinical trial of molnupiravir in patients with COVID-19 shows accelerated SARS-CoV-2 RNA clearance and elimination of infectious virus. Sci. Transl. Med. 2022, 14, eabl7430. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Covid-19: Molnupiravir reduces risk of hospital admission or death by 50% in patients at risk, MSD reports. BMJ 2021, 375, n2422. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Singh, A.; Singh, R.; Misra, A. Molnupiravir in COVID-19: A systematic review of literature. Diabetes Metab. Syndr. 2021, 15, 102329. [Google Scholar] [CrossRef]
- Fitero, A.; Bungau, S.G.; Tit, D.M.; Endres, L.; Khan, S.A.; Bungau, A.F.; Romanul, I.; Vesa, C.M.; Radu, A.-F.; Tarce, A.G.; et al. Comorbidities, Associated Diseases, and Risk Assessment in COVID-19—A Systematic Review. Int. J. Clin. Pract. 2022, 2022, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Allard, R.; Leclerc, P.; Tremblay, C.; Tannenbaum, T.-N. Diabetes and the severity of pandemic influenza A (H1N1) infection. Diabetes Care 2010, 33, 1491–1493. [Google Scholar] [CrossRef]
- Cortes Garcia, M.; Sierra Moros, M.J.; Santa-Olalla Peralta, P.; Hernandez-Barrera, V.; Jimenez-Garcia, R.; Pachon, I. Clinical characteristics and outcomes of diabetic patients who were hospitalised with 2009 pandemic influenza A H1N1 infection. J. Infect. 2012, 64, 218–224. [Google Scholar] [CrossRef]
- Gorricho, J.; Garjón, J.; Alonso, A.; Celaya, M.C.; Saiz, L.C.; Erviti, J.; López, A. Use of oral antidiabetic agents and risk of community-acquired pneumonia: a nested case-control study. Br. J. Clin. Pharmacol. 2017, 83, 2034–2044. [Google Scholar] [CrossRef]
- Zhang, W.; Xu, Y.-Z.; Liu, B.; Wu, R.; Yang, Y.-Y.; Xiao, X.-Q.; Zhang, X. Pioglitazone upregulates angiotensin converting enzyme 2 expression in insulin-sensitive tissues in rats with high-fat diet-induced nonalcoholic steatohepatitis. ScientificWorldJournal. 2014, 2014, 603409. [Google Scholar] [CrossRef] [PubMed]
- Behl, T.; Kumar, K.; Singh, S.; Sehgal, A.; Sachdeva, M.; Bhatia, S.; Al-Harrasi, A.; Buhas, C.; Teodora Judea-Pusta, C.; Negrut, N.; et al. Unveiling the role of polyphenols in diabetic retinopathy. J. Funct. Foods 2021, 85, 104608. [Google Scholar] [CrossRef]
- Popa, A.; Chereji, A.-I.; Dodu, M.A.; Chereji, I.; Fitero, A.; Daina, C.M.; Daina, L.G.; Badau, D.; Neculoiu, D.C.; Domnariu, C. The Impact of Changes regarding Working Circumstances during COVID-19 Pandemic upon Patients Evaluated for Thyroid Dysfunction. Int. J. Environ. Res. Public Health 2022, 19, 9856. [Google Scholar] [CrossRef] [PubMed]
- Vaezi, A.; Salmasi, M.; Soltaninejad, F.; Salahi, M.; Javanmard, S.H.; Amra, B. Favipiravir in the Treatment of Outpatient COVID-19: A Multicenter, Randomized, Triple-Blind, Placebo-Controlled Clinical Trial. Adv. Respir. Med. 2023, 91, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Intern. Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef] [PubMed]
- COVID-GRAM Critical Illness Risk Score. Available online: https://www.mdcalc.com/calc/10303/covid-gram-critical-illness-risk-score (accessed on 7 August 2023).
- World Health Organization. COVID-19 - Tests. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/media-resources/science-in-5/episode-14---covid-19---tests?gclid=Cj0KCQjwiIOmBhDjARIsAP6YhSUhh1k3L0EYckHvj8sW- lsJnYh7lAeUloiWlhJ9axHC3vnksU2z5VoaAijuEALw_wcB (accessed on 7 August 2023).
- Elliott, A.C.; Woodward, W.A. Statistical analysis quick reference guidebook : with SPSS examples, 1st ed.; Sage Publications: Thousand Oaks, CA, USA, 2007; ISBN 1-4129-2560-6. [Google Scholar]
- Prajapati, G.; Das, A.; Sun, Y.; Fonseca, E. Hospitalization Among Patients Treated With Molnupiravir: A Retrospective Study of Administrative Data. Clinical Therapeutics 2023. [Google Scholar] [CrossRef] [PubMed]
- Bajema, K.L.; Berry, K.; Streja, E.; Rajeevan, N.; Li, Y.; Yan, L.; Cunningham, F.; Hynes, D.M.; Rowneki, M.; Bohnert, A.; et al. Effectiveness of COVID-19 treatment with nirmatrelvir-ritonavir or molnupiravir among U.S. Veterans: target trial emulation studies with one-month and six-month outcomes. medRxiv 2022, 2022.2012.2005.22283134. [Google Scholar] [CrossRef]
- Gentry, C.A.; Nguyen, P.; Thind, S.K.; Kurdgelashvili, G.; Williams, R.J. Characteristics and outcomes of US Veterans at least 65 years of age at high risk of severe SARS-CoV-2 infection with or without receipt of oral antiviral agents. Journal of Infection 2023, 86, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Bowe, B.; Al-Aly, Z. Molnupiravir and risk of hospital admission or death in adults with covid-19: emulation of a randomized target trial using electronic health records. BMJ 2023, 380, e072705. [Google Scholar] [CrossRef]
- Najjar-Debbiny, R.; Gronich, N.; Weber, G.; Khoury, J.; Amar, M.; Stein, N.; Goldstein, L.H.; Saliba, W. Effectiveness of Molnupiravir in High-Risk Patients: A Propensity Score Matched Analysis. Clinical Infectious Diseases 2022, 76, 453–460. [Google Scholar] [CrossRef]
- Wai, A.K.-C.; Chan, C.Y.; Cheung, A.W.-L.; Wang, K.; Chan, S.C.-L.; Lee, T.T.-L.; Luk, L.Y.-F.; Yip, E.T.-F.; Ho, J.W.-K.; Tsui, O.W.-K.; et al. Association of Molnupiravir and Nirmatrelvir-Ritonavir with preventable mortality, hospital admissions and related avoidable healthcare system cost among high-risk patients with mild to moderate COVID-19. The Lancet Regional Health – Western Pacific 2023, 30. [Google Scholar] [CrossRef] [PubMed]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients. N Engl J Med 2022, 386, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.C.; Hobbs, F.D.R.; Gbinigie, O.A.; Rahman, N.M.; Hayward, G.; Richards, D.B.; Dorward, J.; Lowe, D.M.; Standing, J.F.; Breuer, J.; et al. Molnupiravir plus usual care versus usual care alone as early treatment for adults with COVID-19 at increased risk of adverse outcomes (PANORAMIC): an open-label, platform-adaptive randomised controlled trial. The Lancet 2023, 401, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.L.; Orton, C.M.; Grinsztejn, B.; Donaldson, G.C.; Crabtree Ramírez, B.; Tonkin, J.; Santos, B.R.; Cardoso, S.W.; Ritchie, A.I.; Conway, F.; et al. Favipiravir in patients hospitalised with COVID-19 (PIONEER trial): a multicentre, open-label, phase 3, randomised controlled trial of early intervention versus standard care. The Lancet Respiratory Medicine 2023, 11, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Al-Muhsen, S.; Al-Numair, N.S.; Saheb Sharif-Askari, N.; Basamh, R.; Alyounes, B.; Jabaan, A.; Saheb Sharif-Askari, F.; Alosaimi, M.F.; Alsohime, F.; Halwani, R.; et al. Favipiravir Effectiveness and Safety in Hospitalized Moderate-Severe COVID-19 Patients: Observational Prospective Multicenter Investigation in Saudi Arabia. Front Med (Lausanne) 2022, 9, 826247. [Google Scholar] [CrossRef] [PubMed]
- Özlüşen, B.; Kozan, Ş.; Akcan, R.E.; Kalender, M.; Yaprak, D.; Peltek, İ.B.; Keske, Ş.; Gönen, M.; Ergönül, Ö. Effectiveness of favipiravir in COVID-19: a live systematic review. European Journal of Clinical Microbiology & Infectious Diseases 2021, 40, 2575–2583. [Google Scholar] [CrossRef]
- Nemec, H.M.; Ferenczy, A.; Christie, B.D. 3rd; Ashley, D.W.; Montgomery, A. Correlation of D-dimer and Outcomes in COVID-19 Patients. Am. Surg. 2022, 88, 2115–2118. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Li, X.; Chen, J.; Ouyang, M.; Zhang, H.; Zhao, X.; Tang, L.; Luo, Q.; Xu, M.; Yang, L.; et al. Evaluation of variation in D-dimer levels among COVID-19 and bacterial pneumonia: a retrospective analysis. J. Thromb. Thrombolysis 2020, 50, 548–557. [Google Scholar] [CrossRef]
- Zhang, L.; Yan, X.; Fan, Q.; Liu, H.; Liu, X.; Liu, Z.; Zhang, Z. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19. J. Thromb. Haemost. 2020, 18, 1324–1329. [Google Scholar] [CrossRef]
- Hayıroğlu, M.İ.; Çınar, T.; Tekkeşin, A.İ. Fibrinogen and D-dimer variances and anticoagulation recommendations in Covid-19: current literature review. Rev. Assoc. Med. Bras. 2020, 66, 842–848. [Google Scholar] [CrossRef]
- Mutair, A. Al; Shamou, J.; Alhumaid, S.; Layqah, L.; Ahmed, G.Y.; Thoyaja, K.; Mohaini, M. Al; Almahmoud, S.; Barry, M.; Khan, A.; et al. Overview of clinical outcome and therapeutic effectiveness of Favipiravir in patients with COVID-19 admitted to intensive care unit, Riyadh, Saudi Arabia. J. Infect. Public Health 2022, 15, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Wu, C.; Zhang, Q.; Wu, F.; Yu, B.; Lv, J.; Li, Y.; Li, T.; Zhang, S.; Wu, C.; et al. C-Reactive Protein Level May Predict the Risk of COVID-19 Aggravation. Open Forum Infect Dis 2020, 7, ofaa153. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.G.; Puenpatom, A.; Moncada, P.A.; Burgess, L.; Duke, E.R.; Ohmagari, N.; Wolf, T.; Bassetti, M.; Bhagani, S.; Ghosn, J.; et al. Effect of Molnupiravir on Biomarkers, Respiratory Interventions, and Medical Services in COVID-19 : A Randomized, Placebo-Controlled Trial. Ann Intern Med 2022, 175, 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Pontolillo, M.; Ucciferri, C.; Borrelli, P.; Di Nicola, M.; Vecchiet, J.; Falasca, K. Molnupiravir as an Early Treatment for COVID-19: A Real Life Study. Pathogens 2022, 11, 1121. [Google Scholar] [CrossRef] [PubMed]
- Kurita, T.; Ishida, K.; Muranaka, E.; Sasazawa, H.; Mito, H.; Yano, Y.; Hase, R. A Favipiravir-induced Fever in a Patient with COVID-19. Intern Med 2020, 59, 2951–2953. [Google Scholar] [CrossRef]
- Bely, P. A.; Krasheninnikov, A. E.; Matveev, A. V.; Zaslavskaya, K. Y. FAVIPIRAVIR IN THE TREATMENT OF MILD CORONAVIRUS INFECTION: RESULTS OF A MULTICENTER OPEN-LABEL, POST-REGISTRATION, NON-INTERVENTIONAL STUDY. Eksperimental'naya i Klinicheskaya Farmakologiya 2023, 86, 18-27, covidwho-2312974. [Google Scholar]
- United States Food and Drug Administration. Title of Site. Available online: https://www.fda.gov/media/155053/download (accessed on 18 October 2023).
- Santi Laurini, G.; Montanaro, N.; Motola, D. Safety Profile of Molnupiravir in the Treatment of COVID-19: A Descriptive Study Based on FAERS Data. J Clin Med 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Ergür, F.; Yıldız, M.; Şener, M.U.; Kavurgacı, S.; Ozturk, A. Adverse effects associated with favipiravir in patients with COVID-19 pneumonia: a retrospective study. Sao Paulo Med J 2022, 140, 372–377. [Google Scholar] [CrossRef]
- Manole, F.; Marian, P.; Mekeres, G.M.; Voiţă-Mekereş, F. Systematic Review of the Effect of Aging on Health Costs. Archives of Pharmacy Practice 2023, 14, 58–61. [Google Scholar] [CrossRef]
Figure 1.
CONSORT flow diagram of the study. n, number; M, molnupiravir; F, favipiravir.
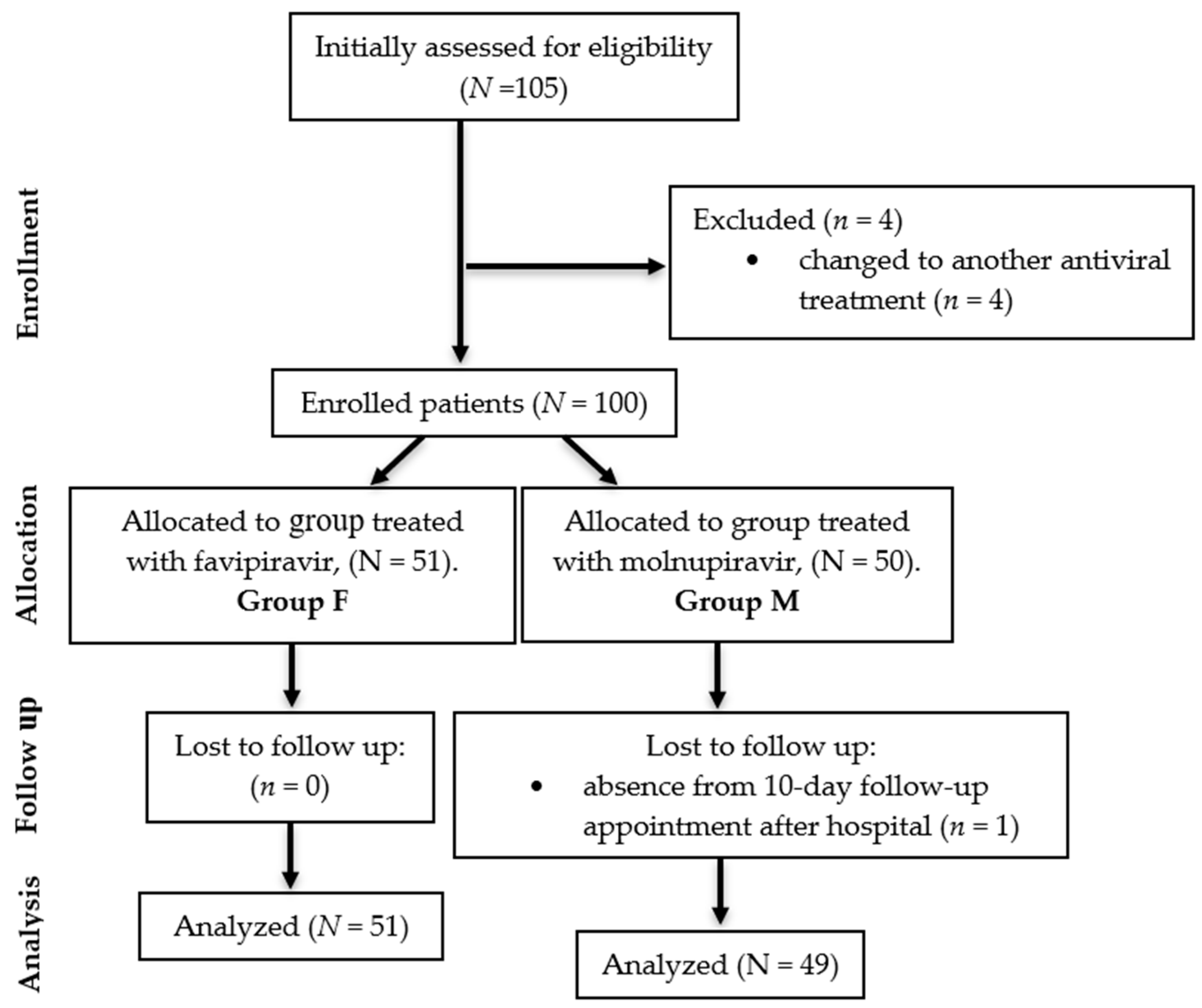
Figure 2.
COVID-GRAM Risk Score Organigram.
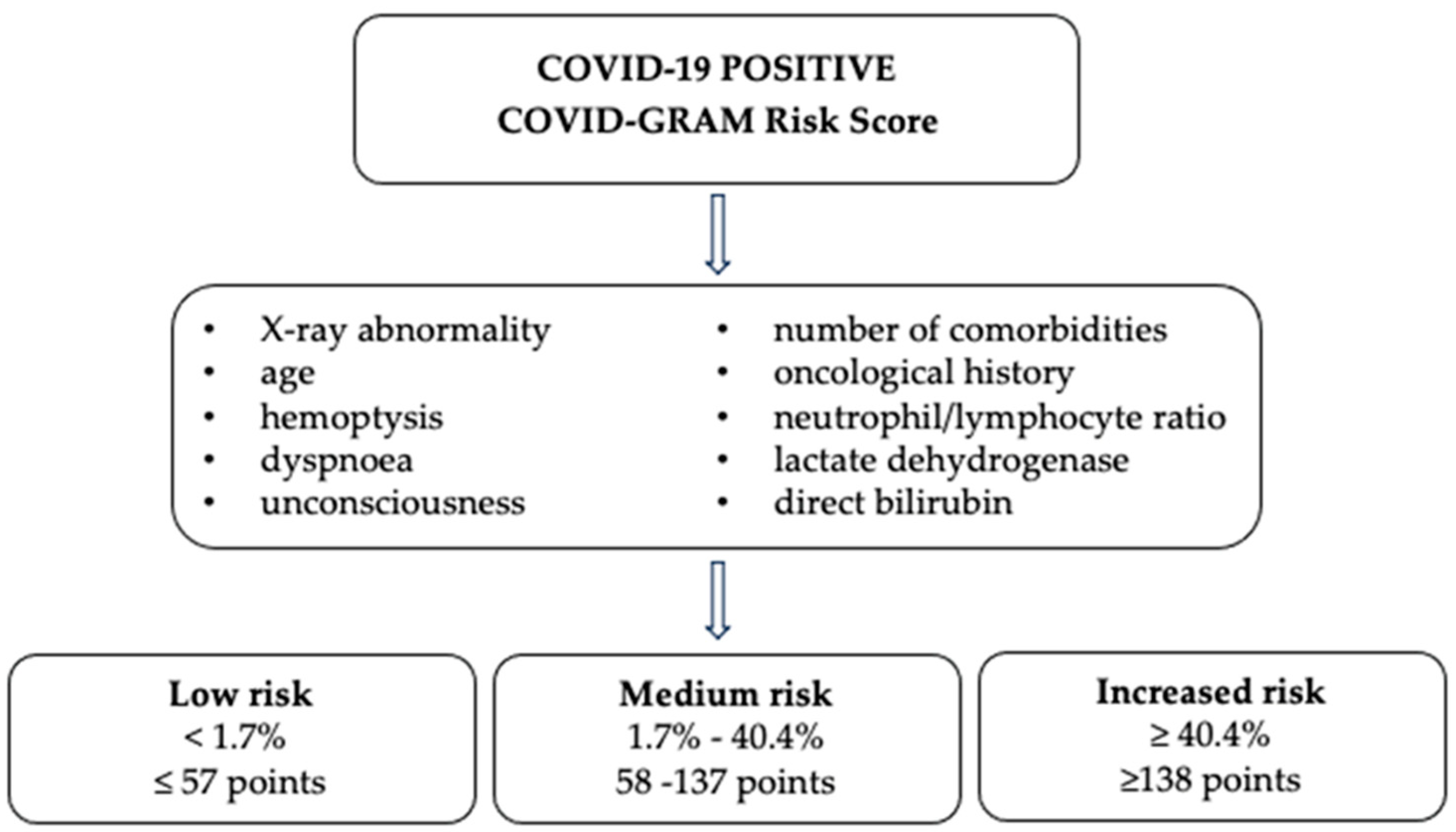
Figure 3.
COVID-GRAM risk score in groups F and M, at times t0 and t1.
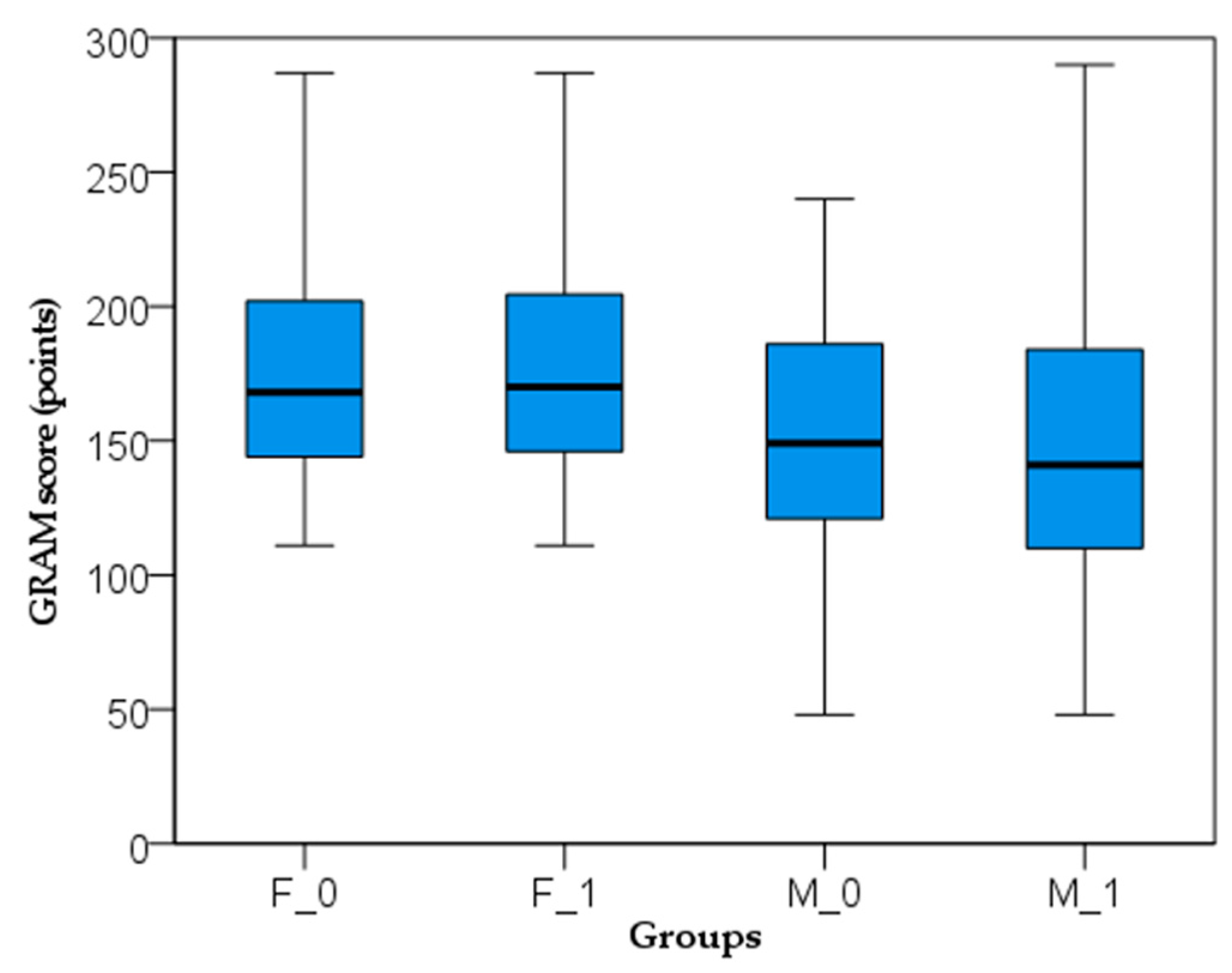
Figure 4.
Histogram of the hospitalization days. HD, hospitalization days; F, favipiravir; M, molnupiravir.
Figure 4.
Histogram of the hospitalization days. HD, hospitalization days; F, favipiravir; M, molnupiravir.
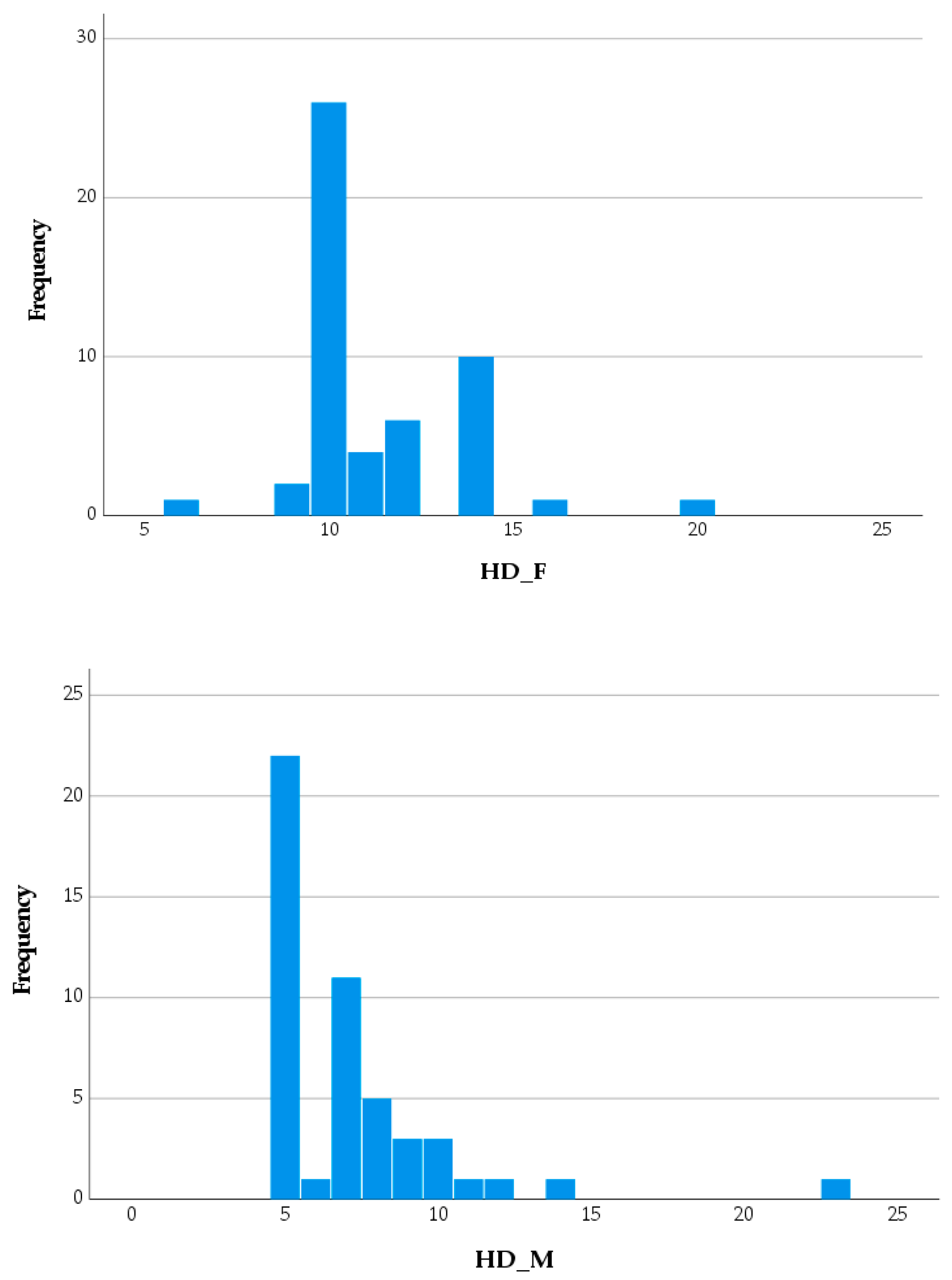
Figure 5.
D-dimer values in groups F and M, at times t0 and t1. F_0, starting time of the favipiravir; F_1, end time of the favipiravir; M_0, starting time of the molnupiravir; M_1, end time of the molnupiravir; P, value as determined by t-test.
Figure 5.
D-dimer values in groups F and M, at times t0 and t1. F_0, starting time of the favipiravir; F_1, end time of the favipiravir; M_0, starting time of the molnupiravir; M_1, end time of the molnupiravir; P, value as determined by t-test.

Figure 6.
Kaplan-Meier curves for time to normalization of CRP values. HD, hospitalization days; F, favipiravir; M, molnupiravir; *P=0.001, statistical significance according to log-rank test.
Figure 6.
Kaplan-Meier curves for time to normalization of CRP values. HD, hospitalization days; F, favipiravir; M, molnupiravir; *P=0.001, statistical significance according to log-rank test.
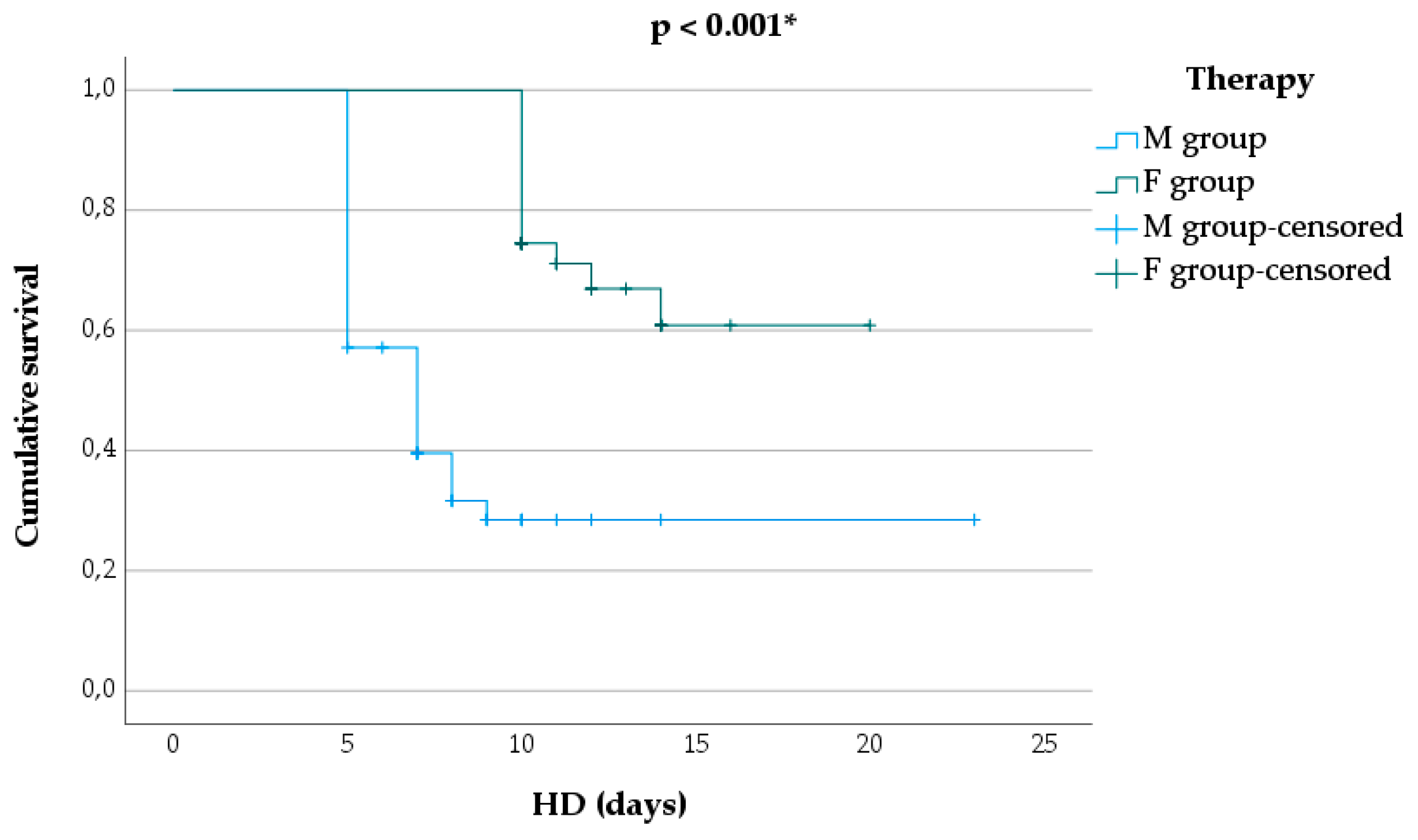

Table 1.
Characteristics of COVID-19 groups.
| Parameter | Group F (n=51) | Group M (n=49) | P-value |
|---|---|---|---|
| DD | |||
| Age, years, mean ± SD | 71.16 ± 12.50 | 65.84 ± 16.66 | 0.075a |
| Male gender, n (%) | 17 (33.33) | 22 (44.90) | 0.643b |
| Urban residence, n (%) | 16 (31.37) | 21 (42.86) | 0.411b |
| VHC, n (%) | 2 (3.92) | 1 (2.04) | 0.563b |
| Clinical data | |||
| Stomatitis, n (%) | 0 (0) | 1 (2) | 0.317b |
| Diarrhea, n (%) | 3 (5.88) | 4 (8.16) | 0.705b |
| Abdominal pain, n (%) | 4 (7.84) | 3 (6.12) | 0.705b |
| Nausea, n (%) | 6 (11.76) | 3(6.12) | 0.317b |
| Vomiting, n (%) | 3 (5.88) | 0 (0) | 0.083b |
| Dizziness, n (%) | 2 (3.92) | 1 (2) | 0.563b |
| SpO2, M ± SD | 92.29 ± 6.59 | 92.67 ± 7.14 | 0.783a |
| POH, M ± SD | 4.31 ± 1.35 | 4.55 ± 1.57 | 0.420a |
| BMI, M ± SD | 28.91 ± 3.98 | 28.26 ± 3.52 | 0.390a |
| PMH | |||
| CVC, n (%) | 40 (78.43) | 33 (67.35) | 0.412b |
| CKD, n (%) | 11 (21.57) | 12 (24.49) | 0.834b |
| N, n (%) | 2 (3.92) | 1 (2.04) | 0.563b |
| CPD, n (%) | 1 (1.96) | 2 (4.08) | 0.563b |
| CVD, n (%) | 8 (15.69) | 5 (10.20) | 0.692b |
| Hep B, n (%) | 1 (1.96) | 0 (0.00) | 0.317b |
| ID, n (%) | 1 (1.96) | 2 (4.08) | 0.563b |
| Paraclinical investigations, mean ± SD | |||
| Ferritin, (ng/mL) | 1314.06 ± 1266.20 | 843.53 ± 1160.23 | 0.061a |
| HbA1c, (mg%) | 7.24 ± 0.57 | 7.25 ± 0.65 | 0.924a |
| D-dimer, (ng/mL) | 1039.18 ± 801.80 | 1106.02 ±1439.30 | 0.776a |
| ALAT (mg%) | 33.78 ± 15.24 | 32.91±15.99 | 0.781a |
| CRP (mg/L) | 92.02 ± 90.96 | 60.92 ± 73.41 | 0.062a |
| COVID-GRAM risk score | 178.14 ± 43.78 | 160.59 ± 59.41 | 0.129a |
DD, graphic data; PMH, past medical history; BMI, body mass index; VHC, vaccination history against COVID-19 in the last 12 months; SpO2, oxygen saturation levels; CVC, cardio-vascular disease comorbidities; CKD, chronic kidney disease; N, neoplasm; CPD, chronic pulmonary disease; CVD, cerebral vascular disease; POH, period from onset to hospitalization; Hep B, hepatitis B; ID, immunodeficiency; ALAT, alanine aminotransferase; HbA1c, glycated hemoglobin; CRP, C-reactive protein; n, number; M, mean; SD, standard deviation; P, value as determined by a t-test or b Chi-square test.
Table 2.
The evolution of subjects based on the COVID-GRAM risk score.
| Risk of critical illness | t0 | t1 | P-value |
|---|---|---|---|
| Group F | |||
| Low, n (%) | 0 (0%) | 0 (0%) | - |
| Medium, n (%) | 9 (17.65%) | 10 (19.61%) | 0.818a |
| High, n (%) | 42 (82.35%) | 41 (80.39%) | 0.912a |
| Group M | |||
| Low, n (%) | 1 (2.04%) | 1 (2.04%) | 1.000a |
| Medium, n (%) | 19 (38.78%) | 22 (44.90%) | 0.639a |
| High, n (%) | 29 (59.18%) | 26 (53.06%) | 0.685a |
t0, starting time of the antiviral; t1, end time of the antiviral; F, favipiravir group; M, molnupiravir group; n, number; P, value as determined by a Chi-square test.
Table 3.
Adverse effects of subjects during antiviral treatment.
| Adverse effects, n (%) | M group | F group | P-valuea |
|---|---|---|---|
| Stomatitis | 8 (15.69) | 7 (14.29) | 0.796 |
| Diarrhea | 1 (1.96) | 9 (18.37) | 0.011 |
| Abdominal pain | 2 (3.92) | 3 (6.12) | 0.654 |
| Nausea | 8 (15.69) | 14 (28.57) | 0.2 |
| Vomiting | 1 (1.96) | 4 (8.16) | 0.179 |
| Dizziness | 5 (9.80) | 9 (18.37) | 0.285 |
| ALAT elevated | 1 (1.96) | 3 (4.08) | 0.317 |
| Total | 26 (50.98) | 48 (97.96) | 0.010 |
n, number; ALAT, alanine aminotransferase; P, value as determined by a Chi-square test. Significant P-values are noted in bold print.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



