
Submitted:
06 February 2024
Posted:
07 February 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Vaccination against the SARS-CoV2 virus has shown great promise in managing the spread and severity of Covid-19. While these vaccines were able to provide a favourable response in controlling the SARS-CoV2 infection, its use came with accompanying side effects. This systematic review aimed to determine the effectiveness of the different Covid-19 vaccine subtypes and discover the side effects associated with each vaccine elsewhere but specially in Trinidad and Tobago. For this systematic review, the keywords “Pfizer-BioNTech OR Moderna OR Oxford-AstraZeneca OR Janssen OR Sinopharm OR Novavax AND Covid-19 vaccine efficacy” and “Covid-19 vaccines AND Trinidad and Tobago” were researched under PubMed, MEDLINE and other internet sources through which other notable journals, and documents were discovered and searched similarly as outlined previously. In doing so, 65 relevant articles were included as part of this review. Of the studies examined, overall the vaccine with the greatest VE was found to be Pfizer-BioNTech (95%), followed by Moderna (94.1%), Novavax (89.7%), AstraZeneca (70.4%), Sinopharm (67%) and finally Janssen (66.9%). The use of Pfizer-BioNTech or Moderna was most efficacious in response to the different Covid-19 variants. Some side effects were common for all vaccine types however adverse effects were more commonly seen with vaccination by mRNA vaccines, Pfizer-BioNTech and Oxford-Astrazeneca. Researchers targeted individuals aged 18 and above residing in various geographical areas of TT, specifically focusing on those who had not received the COVID-19 vaccine and expressed hesitancy towards it. Convenience sampling was used to select the study participants, and formal in-depth virtual interviews were conducted on a one-to-one basis, employing a semi-structured questionnaire to guide the discussions. The interviews were meticulously recorded and transcribed, following the principles of reflexive thematic analysis, to distill key insights from the participants' responses. The study's findings, derived from the perspectives of 25 participants, illuminated a complex tapestry of reasons underlying vaccine hesitancy in Trinidad and Tobago. Notably, prominent themes emerged, including fear, doubts regarding vaccine efficacy, a perceived inadequacy of information, a sense of susceptibility to the virus, deep-seated mistrust, alternative herbal remedies, and religious reservations. Interestingly, the motivations expressed by these vaccine-hesitant individuals for potentially receiving the vaccine in the future were rooted in notions of necessity, an increased sense of susceptibility to the virus, a desire to reach a certain health benchmark, and a need for assurance regarding the vaccine's safety and effectiveness. This comprehensive exploration of vaccine hesitancy in TT provides valuable insights for public health officials and policymakers in crafting targeted strategies to address this critical issue within the local context. Conclusion: The findings of this study determined that vaccination against the SARS-CoV2 virus provided beneficial outcomes against infection, Covid-19 related hospitalizations, ICU admissions and mortality. While vaccination was deemed highly appropriate in managing the spread of the SARS-CoV2 virus and enhancing the outcomes in infected persons, the effectiveness of the different vaccine platforms indicated that certain vaccine platforms are preferential to others in different populations. In terms of vaccine efficacy, nucleic acid vaccines such as Pfizer-BioNTech and Moderna showed the greatest effectiveness while inactivated whole virus vaccines such as Sinopharm and viral vectors like Janssen had the least effectiveness. The side effects, joint/muscle soreness, pain at the injection site, shoulder pain, headaches, fever, chills, weakness, epistaxis, renal and certain cardiovascular events were common for all vaccine types. Adverse effects were more frequent and severe with the mRNA vaccines by Pfizer-BioNTech and Oxford-Astrazeneca than inactivated whole virus vaccines. The data collected in this research can be very useful to help individuals make a decision on which vaccine would be appropriate for them. More long-term studies are needed to better gauge the scope of side effects for each vaccine type.
Keywords:
Pfizer-BioNTech
; Modern
; Novavax
; AstraZeneca
; Sinopharm
; Janssen
; vaccine effectiveness (VE)
; COVID-19
; Trinidad and Tobago
1. Introduction
In light of the Covid-19 pandemic declared by the WHO in March 2020, many interventions were introduced to not only curb the spread of the SARS-CoV2 virus but provide protection against this fatal virus. One undertaking in establishing control of the spread and severity of this virus included vaccination [1].
Having utilised a variety of biomedical technologies, multiple vaccines were developed and have since undergone extensive testing in clinical trials. Many candidate vaccines have been highlighted with their main difference being the platform in which these vaccines would elicit an immune response. Each vaccine technology has its associated benefits and limitations. As vaccines became more readily available throughout the different platforms (whole virus, nucleic acid, viral vector, protein based), the immunogenic potential of each type became evident [2]. Across these platforms, some vaccines of interest included: Pfizer-BioNTech (BNT162b2), Moderna (mRNA-1273), Oxford-AstraZeneca (AZD1222), Janssen (Ad26.COV2.S), Sinopharm (BBIBP-CorV) and Novavax (NVX-CoV2373). The implementation of vaccination for the SARS-CoV2 virus demonstrated great promise across the world with studies showing how favourable vaccination has proven against this virus [3]. Vaccination has proved effective in protecting vaccinated populations from SARS-CoV2 infection and even in reducing the number of hospitalizations for acute cases of COVID-19 and limiting the extent of ICU admissions and death [4]. Vaccine effectiveness however is also subjective as it can be impacted by the rise of new and existing strains of the SARS-CoV2 virus [[5]]. While each aforementioned vaccine was associated with a different vaccine effectiveness, many side effects also accompanied their use.
Purpose of Study:
The aim of this study is to conduct a systematic review of the effectiveness of COVID-19 vaccines and vaccination issues in Trinidad and Tobago.
Research Questions:
What is the effectiveness of different COVID-19 vaccines based on a critical appraisal of existing literature?
Aims & Objectives of Research:
This paper aims to critically evaluate existing literature on the effectiveness and side effects of COVID-19 vaccines, and vaccination issues in Trinidad and Tobago.
The research objectives of this study are as follows:
- Conducting a systematic review of the effectiveness and side effects of COVID-19 vaccines.
- Identifying gaps in current scientific literature related to COVID-19 vaccination issues in Trinidad and Tobago.
2. Materials and Methods
Eligibility Criteria: Table 1 shows the eligibility/inclusion criteria for the study.
Exclusion Criteria
- Children under the aged 4 or below.
- Research that only provided abstracts and did not have full text available.
Information Sources
The databases utilised for this research included PubMed, and Medline along with other online resources. The search was conducted in September 2022. Some updates were done in 2023.
Search Strategy
Relevant keywords and terms were used to search the database PubMed and other online sources, in alignment with the study’s objectives.
Keywords used: “Pfizer-BioNTech OR Moderna OR Oxford-AstraZeneca OR Janssen OR Sinopharm OR Novavax AND Covid-19 vaccine efficacy”
Terms used: Covid-19 vaccines AND Trinidad and Tobago.
Selection Process
The selection process involved a manual review of titles and abstracts to identify studies/articles that met the inclusion criteria. All 21 reviewers participated in this task, using the search strategy outlined in Figure 1.
Process of Data Collection
Each study/report was evaluated by two independent reviewers to avoid bias and to determine if it met the inclusion criteria. In case of any disagreement between the two reviewers, a third reviewer was appointed to resolve the issue. This process was documented using a PRISMA (Preferred Reporting Items for Systematic Reviews & Meta-Analyses) flowchart (Refer to Figure 1).
Figure 1 shows the results of database search and screening. Studies were written in English, without date restrictions. The flow diagram summarizes the details of our protocol. After removing the duplicates, 150 studies were retrieved, and among those, 65 studies were selected for full-text screening, since they met the inclusion criteria.
3. Results and Discussions
3.1. Effectiveness of Covid-19 Vaccines
Vaccination against SARS-CoV2 has shown great promise over the last three years. Zheng et al found that in fully vaccinated populations, the vaccine effectiveness, VE, against SARS-CoV2 infection was on average 89.1%. Vaccinated populations exhibited lower rates of hospitalisation (VE: 97.2%), ICU admission (VE: 97.4%) and death (VE: 99%) [3].
As the pandemic progressed, many vaccine platforms were recommended for use among certain populations. The VE of different platforms such as nucleic acid vaccines (Pfizer-BioNTech, Moderna), viral vector vaccines (AstraZeneca, Janssen), whole virus (Sinopharm) and protein based (Novavax), are distinct due to the varying immunologic potential of each vaccine. Table 2 summarises the VE displayed by the aforementioned vaccines [6].
Table 2 compares the efficacy of the different types of vaccines used throughout the COVID-19 pandemic. The vaccines that showed the most effectiveness were the nucleic acid vaccines which included the Pfizer-BioNTech (BNT162b2), Moderna (mRNA-1273) followed by the Novavax (NVX-CoV2373). Alternatively, the viral vector vaccines such as the Astrazeneca (AZD1222), Janssen (Ad26.COV2.S) vaccines and inactivated viral vaccines such as the Sinopharm (BBIBP-CorV) did not show as much effectiveness when compared to the nucleic acid vaccines.
3.1.1. Pfizer-BioNTech
The Pfizer-BioNTech vaccine proved beneficial against SARS-CoV2 infection. This vaccine, which contains a nucleoside modified mRNA, induces the production of antibodies in response to the antigen associated spike protein [6]. It was found to lessen the risk of diagnosed SARS-CoV2 (RR 0.07, 95% CI: 0.05–0.13) as well as hospitalisation (RR 0.06, 95% CI: 0.03–0.12), and COVID-19 associated deaths (RR 0.04, 95% CI: 0.02–0.09) [7]. This implies that those vaccinated with this mRNA vaccine possess far greater immune protection than those who remain unvaccinated. In a study by Rotshild et al, Pfizer-BioNTech showed the highest probability for efficacy in symptomatic COVID-19 compared to 9 other vaccines [8].
While Pfizer-BioNTech’s effectiveness was supported on multiple accounts, it was seen that VE, while lower in patients over 75, as well as patients suffering from comorbidities like diabetes and hypertension, was still significant in comparison to other vaccines [9]. Another study discerned that VE of Pfizer-BioNTech among the elderly population was 60-70% following a single dose, while 2 doses provided 85-90% efficacy. Among this population, it was also seen that those vaccinated with the Pfizer-BioNTech, who were still infected with SARS-CoV2 post vaccination, experienced a significantly lower risk of hospital admission and morbidity, 44% and 51% respectively when compared to those remaining unvaccinated [10]. This highlights the definite effectiveness of this vaccine for use among elderly patients [11].
Moreover, the use of the PfizerBioNTech vaccine was found to provide high VE against symptomatic Covid-19 and severe infection in children aged 5-11 [12]. This indicates the suitability of this vaccine for yet another population, making it well suited for almost all age groups. Additionally, it was discovered that the VE of both the mRNA vaccines against hospitalisation for severe Covid-19 was well sustained, extending well into a 24 week period, even in patients who were considered high risk, such as those who are immunocompromised [13].
Pfizer’s VE against SARS-CoV2 infection decreased from 93.2% to 68.5% within a 6 month period. This signifies the importance of a booster being administered to maintain optimal protection from breakthrough infections [14]. This is endorsed by another study which investigated the impact of a third dose of Pfizer-BioNTech versus a placebo. They determined that doing so allowed for 95.3% efficacy against infection even after almost 10 months [15]. Furthermore, persons administered the Pfizer-BioNTech booster as part of a study done in Israel, exhibited not only a decrease in the rate of infection by 11.3, but persons experiencing severe illness due to SARS-CoV2 infection also declined, by a factor of 19.5 [16]. These common findings indicate that the VE of Pfizer-BioNTech is evident not just as a double dose vaccine, but in its administration as a booster.
Pfizer–BioNTech proved to have an efficacy of 92% and 83% against symptomatic cases of the alpha and delta variant respectively. Furthermore, it displayed 75% protection against the beta strain which was otherwise difficult to control with the implementation of other vaccines [17]. In comparison to other vaccines, Pfizer-BioNTech has the greatest effectiveness against both alpha and beta strains, following its full dose [18]. In response to the Omicron variant, while a double dose bore limited effectiveness, receiving a Pfizer–BioNTech booster enhanced the neutralising capability thus providing better protection against this potent strain [19]. This was supported in another study which determined that mRNA vaccines possessed the greatest vaccine efficacy against alpha, beta, gamma and delta variants as opposed to other vaccines [20].
3.1.2. Moderna
A study found that vaccination using the Moderna vaccine lowered laboratory-confirmed COVID-19 when compared to using no vaccine (VE: 94.1%; 95% CI: 0.89, 0.97). Additionally, they discerned that VE against COVID-19 associated hospitalizations was 89% (95% CI: 0.13, 0.99) in persons receiving two doses of the Moderna vaccine [21]. Similarly findings of another study conferred that effectiveness of Moderna against the incidence of infection was 69% following the first dose which then increased to 80% following the second dose [22]. This highlights the significance of adhering to the 2 dose regimen in order to achieve maximal immunity.
Further to this, it was discovered that Moderna’s VE was not only high, but long lasting when compared to other vaccines [23]. While protection from other vaccines of the same platform, exhibited a decrease in effectiveness 4 months post inoculation, Moderna did not, but instead displayed comparatively high levels of postvaccination anti-RBD antibodies [24].
Moreover, when examining the use of vaccines among the older US population, it was found those vaccinated with Moderna had a 14% lower risk of diagnosed COVID-19. In addition, receiving the Moderna vaccine was associated with greater immunogenicity and a reduction in morbidity [25]. Likewise, it was seen that the immune response via antibody production in patients receiving the Moderna vaccine was similar for both groups of younger and older patients [11].
It was established, in a study done on US veterans, characterised by dominance of the alpha variant, the administration of Moderna recorded lower events for SARS-CoV2 infection (4.52), ICU admission (0.26) and death (0.20) when compared to persons vaccinated with Pfizer-BioNTech, (SARS-CoV2 infection: 5.75, ICU admission: 0.36, death: 0.22) [26].
In response to the Omicron variant, the Moderna vaccine was responsible for a significant increase in neutralisation titers against this strain [27]. This finding provided precedence for the recent approval by the FDA, for the use of Moderna’s 2023-2024 formula which includes a monovalent component corresponding to the Omicron variant, XBB.1.5 of SARS-CoV2 [28].
With the emergence of the delta variant, Moderna was also useful. In a study done on nursing home residents, it was found that the use of mRNA vaccines, both Moderna and Pfizer-BioNTech shared identical levels of VE against the delta variant. While these vaccines had a VE of 74.7% prior to the delta wave, this declined to 53.1% as this variant became predominant in the US. To enhance the immune response, an additional dose of either of these mRNA vaccines has been postulated to establish a more protective response, especially against the delta variant [29]. This finding was supported in another study which discerned that the use of either of the mRNA vaccines coincided with less COVID-19 related hospitalizations and deaths in elderly patients [30].
3.1.3. Oxford-AstraZeneca
The AstraZeneca vaccine is a viral vector vaccine that has displayed a significantly lower efficacy, about 70%, when compared to other vaccines, namely Moderna, Pfizer-BioNTech and Novavax. This vaccine encodes the spike protein found on SARS-CoV2 allowing those inoculated with it to produce antibodies in response to the presence of this protein [6].
Its response to the SARS-CoV2 variants proved different for each strain. Most notably, a study found that even after having 2 doses of the AstraZeneca vaccine, it was not protective against infection by the beta variant, originating in South Africa, prompting its use to be curbed in this region [17]. This was consistent with the findings of another study which reported the protection provided by this vaccine against the beta strain was only 10% in participants in South Africa [6]. VE against the alpha strain, 70.4%, although greater than that of the delta variant was still comparatively lower than that provided by other vaccines [31]. The AstraZeneca vaccine also failed to provide a sufficient and effective response against the Omicron strain. It was found to have very minimal protection after two doses, thus it was suggested that supplementation with either Pfizer-BioNTech or Moderna boosters could assist in improving the immune response [19].
A study found that after a single dose of AstraZeneca, VE was 15% while other vaccines like Pfizer-BioNTech proved to be 31% effective after just one dose. In comparing the two aforementioned vaccines, another determination was that the incidence rate ratio for infection by SARS-CoV2 was much higher, 0.85 with AstraZeneca vaccination than Pfizer-BioNTech, 0.69 [32].
Another crucial finding was that AstraZeneca appeared more agreeable with older patients than younger individuals at first, however after receiving both doses, a similar level of immunogenicity was established across all age groups [17]. The use of AstraZeneca in the elderly population was once again supported, as a study done among persons aged 70-84, found that following AstraZeneca vaccination, these elderly patients had desirable antibody responses associated with low reactogenicity [11]. Further to this, a study done in Japan concluded that the respective antibody seroresponses following vaccination with AZD1222 were above 50% across all age groups examined (8-55, 56-69 and over 70 years) [33]. This level of seropositivity suggests that this vaccine is associated with great protection, however this may wane over time [34]. Thus, it can be inferred that the potency of humoral immunity elicited by this vaccine is strong and it also displays significant tolerance across different age groups.
While the mRNA vaccines displayed greater effectiveness when compared to this viral vector vaccine, there has been a higher efficacy against SARS-CoV2 infection than that seen by Sinopharm. In a study done where persons initially received two doses of Sinopharm, a booster was administered of either Sinopharm or AstraZeneca. The findings displayed that individuals receiving the AstraZeneca booster developed a stronger antibody and CD8+ T cell response and thus were better protected by the AstraZeneca vaccine [35].
3.1.4. Janssen
The Janssen vaccine utilises a viral vector (adenovirus type 26) that contains the gene encoding the spike protein which induces an antibody response against the SARS-CoV-2 virus. This single dose vaccine has demonstrated a VE of 66.9% [6]. Another study showed that its effectiveness against hospitalisations relating to COVID-19 infection was 93%. Additionally, they discerned that Janssen’s VE continued to increase post vaccination and showed little to no evidence of waning efficacy up to 15 weeks after vaccination. This is comparatively favourable to Janssen, as other vaccines displayed waning efficacy from as early as week 12 [36]. Furthermore, when examining Janssen vaccine as a booster, it was discovered that after receiving the recommended single dose, an additional booster further enhanced VE against SARS-CoV2 infection [37].
In a study comparing the cellular and humoral responses of different vaccines, it was found that antibody binding to Ad26.COV2.S and the production of neutralising antibodies increased overtime after vaccination with the Janssen vaccine. However, the neutralising antibody titers were still significantly lower than other vaccines (3.6-fold lower than Moderna, 2.4-fold lower than Pfizer-BioNtech) [38]. This was supported by a study done in Boston, which noted that by day 57, after receiving the Janssen vaccine, binding and neutralising antibodies were already identified in all recipients. This signifies that the Janssen vaccine is associated with rapid humoral and cellular immune responses [39]. However, despite this rapid response, the levels of anti-SARS-CoV-2 antibody after Janssen vaccination remains comparably lower than that of two dose regimens like Moderna and Pfizer-BioNTech [24].
When examined against the strains of SARS-CoV2, it was found that the VE against the Omicron variant was only 47% in patients receiving the Janssen vaccine as part of a study in Czech Republic. Furthermore, VE against the delta variant was also found to be low, 42% [40]. This was noted again when the delta strain surged across the US as the effectiveness of Janssen declined [37]. Compared to other vaccines, Janssen showed limited effectiveness in protection against the various strains alluding to its restricted immunogenic capabilities.
3.1.5. Sinopharm
The Sinopharm vaccine has shown an efficacy of 67% against SARS-CoV2 infection. This inactivated virus vaccine triggers the extensive production of neutralising antibodies in response to the antigen thus providing immune protection. In a study comparing the effectiveness of Sinopharm against other platforms, it was found that the risk of infection by this virus was higher in those who received the Sinopharm vaccine, 0.36, than that of those vaccinated with other vaccines such as the Pfizer-BioNTech whose risk, 0.22, was lower [4].
Furthermore, a study conducted among an elderly population in Faisalabad, Pakistan found that 14 days after a second dose of Sinopharm, individuals were less likely to develop symptomatic COVID-19 infections (94.3%). Additionally, they were less likely to require hospitalizations (60.5%) and 98.6% had a reduced risk of mortality [41].
Another potent discovery was that Sinopharm’s VE was associated with an evident decline post vaccination. The VE decreased from a maximum of 70% in its first month, to just above 20% by the 36 week mark [4]. This was supported by another study which indicated that while the immune response regulated by T cells was able to persist overtime, the antibody response began declining 3 months post vaccination [42].
The lower immunogenicity of the Sinopharm vaccine was again validated as studies found there to be lower levels of anti spike IgG in persons with this vaccine [42]. In comparing the effectiveness of Sinopharm to Pfizer-BioNTech, IgG titers were measured in groups following vaccination with either of these vaccines. It was concluded that while 99.3% of the Pfizer recipients had positive IgG titers, only 85.7% of the Sinopharm recipients achieved this. Furthermore, the mean IgG titre for Pfizer recipients (515.5 ± 1143.5 BAU/mL) was significantly greater than persons receiving the Sinopharm vaccine (170.0 ± 230.0 BAU/mL). Having lower titres, as seen in Sinopharm recipients, indicates less potent and effectual immunity against SARS-CoV2 infection [43].
Additionally, it was seen that the Sinopharm vaccine possesses lower immunogenic potential in comparison to other vaccines and as a result, persons receiving this vaccine were more likely to suffer from more severe SARS-CoV2 infection. It was inferred that even after two doses, patients were still unable to achieve immunologic memory, thus the need for a booster is crucial [35]. This was supported in another study done among healthcare workers, which recorded that those vaccinated with Sinopharm had the highest rate of reinfection with SARS-CoV2 following vaccination [44].
In a study done in Morocco however, it was found that while Sinopharm was proven effective in protecting against critical illness and need for hospitalisation in adults aged 20 to 60 (VE: 96%), it was only moderately effective among the older population (VE: 53%). This suggests the reduced need for ICU admission and ventilator support for patients infected with SARS-CoV2 after having received the Sinopharm vaccine. This research also proved that by administering a Sinopharm booster, there would be optimised protection despite age [45].
3.1.6. Novavax
In a study published by Dunkle et al., it was concluded that the NVX-CoV2373 vaccine was effective and safe for the prevention of the COVID-19 virus [46]. The Novavax vaccine is an adjuvanted, recombinant spike protein nanoparticle vaccine. In the PREVENT-19, phase 3 trial of the Novavax vaccine, results exhibited a well-tolerated and efficacious (VE: 90%) vaccine in the prevention of symptomatic COVID-19 [47]. In addition to this, it was established in another study that Novavax had a VE of 82.9% (95% CI: 50.49, 94.10) against the incidence of symptomatic Covid-19 in comparison to a placebo [48].
Furthermore, Marchese et al., highlighted that the strategic randomization scheme of PREVENT-19 resulted in equilibrium amongst the demographics possessed between both the placebo and the vaccine treatment groups. Over the course of this investigation, the predominant SARS-CoV2 variant was the alpha variant, with additional beta, epsilon, iota, and gamma variants in sporadic circulation [47]. The same authors reported that over the course of the analysis period, there were approximately 4 hospitalizations occurring with 0 among vaccine recipients and 4 among placebo recipients, yielding a post hoc VE against hospitalisation of 100% (95% CI: 28.8, 100) [47].
Additionally, in a study conducted by Heath et al in 2021, the Novavax vaccine was found to have VE of 86.3% (95% CI, 71.3 to 93.5) against the alpha variant and 96.4% (95% CI, 73.8 to 99.5) against non-alpha variants. The study was a randomised, placebo- controlled trial, and in the vaccine group 10 persons were infected with no hospitalisations or deaths whereas the placebo group saw 96 infections, with 5 being severe [40].
An analysis shows that Novavax exhibited remarkable efficacy in the prevention of COVID-19 related hospitalisation. Particularly, this study showed that the majority of those who required hospitalisation suffered with pre-existing medical conditions, such as diabetes, hyperlipidemia hypertension, and obesity (BMI > 30 kg/m2). Thus, Marchese inferred that these collective findings suggest that Novavax is effective in reducing the risk of hospitalisation due to COVID-19, specially in individuals with pre-existing comorbidities and higher BMIs [39].
3.2. Side Effects of COVID-19 vaccines
3.2.1. Local and systemic side effects
Local and systemic side effects are relatively common following vaccination and are often self-limiting and not affecting activities of daily living. The most common reported local side effect of the Pfizer vaccine was injection site pain (77.43%) followed by local swelling (33.57%).Fatigue was the most reported systemic side effect (43% ) followed by muscle pain, headache, joint pain, fever, itching, lymphadenopathy, nausea, dyspnea and diarrhea [49]
3.2.2. Neurological side effects
Reported neurological side effects associated with SARS-CoV-2 vaccinations were usually mild, and self-limiting. However some side effects were more severe resulting in ICU admission[50] and even death[51]. Covid-19 neurological side effects includes Guillain-Barre syndrome (GBS)[50,52], headaches[53], venous sinus thrombosis (VST)[54,55], transverse myelitis[56,57,58]. Another problems encounter with COVID-19 vaccination include facial nerve palsy[59,60], small fiber neuropathy[61], multiple sclerosis[62], autoimmune encephalitis[63] and ischemic strokes[64].
3.2.3. Myocarditis and Pericarditis
Vaccine-related myocarditis (VRM) is a rare complication of COVID-19 vaccines seen in 1,08 per 100 000 vaccinated persons[65,66]. Myocarditis and pericarditis have been rarely reported in patients receiving mRNA and Novavax vaccines [67]. The patients were predominantly young adolescent males suggesting a possible gender difference who complained of chest pain and were found to have elevated troponin and evidenced by MRI and ECG findings[68]. Table 3 summarises the main side effects of the COVID-19 vaccines.
3.3. COVID-19 Vaccination in Trinidad and Tobago.
Of the twelve vaccines approved by the WHO, eight were approved in Trinidad and Tobago: Spikevax, Comirnaty, Jcovden, Vaxevria, Covshield (AstraZeneca formulation), Covaxin, Covilo and CoronaVac. Jcovden, Covishield and Vaxzevria, the first referred to as the Johnson & Johnson vaccine and the latter two referred to as the AstraZeneca, were non- replicating viral vector vaccines. These vaccines contained the viral genetic material that was placed inside of another harmless virus, which was unable to replicate, hence the name, non-replicating viral vector [82]. The Oxford/AstraZeneca vaccine was the first vaccine brought to Trinidad and Tobago in late March 2021, almost a year after the first case which was diagnosed on March 12th, 2020. This was also about a month after being approved by the 33,600 doses were received through the COVID-19 Vaccines Global Access (COVAX) Facility as part of the initiative to increase COVID-19 vaccine accessibility and end the global pandemics.
Following this initial delivery, more vaccines were supplied to reach a total of 100,800 vaccines [82]. The Oxford/AstraZeneca was approved in 149 countries after 73 trials in 34 countries. Conversely, the Serum Institute of India’s Covishield vaccine of the same formulation was only approved in 49 countries after six trials in India [83]. The Johnson & Johnson vaccine was also approved in Trinidad and Tobago in June 2021, despite being approved by the WHO in March 2021 [84]. It was disseminated under the “One Shot and Done” initiative, as it only required one dose for the patient to be considered fully vaccinated, while other vaccines, like AstraZeneca, involved two doses [85].
Both Spikevax and Comirnaty, locally referred to as the Moderna and Pfizer vaccines, were messenger ribonucleic acid (mRNA) vaccines, meaning that they contained an mRNA sequence which encoded an antigen of the pathogen, which stimulated an immune response from the patient. This allows the adaptive immune system to recognise and defend itself against the actual Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) when it enters the body [84,86]. While this type of vaccine is newer than previous technology, the Pfizer and Moderna vaccines both showed a high efficacy in decreasing the risk of Long COVID, which refers to the development of signs, symptoms and conditions after the initial COVID infection [87]. Despite the Pfizer vaccine being the first vaccine approved by the WHO in December 2020; it was only approved for use in Trinidad and Tobago in August 2021, and at that time was the only vaccine approved by the World Health Organisation for children over age twelve [83].
Covaxin, Sinopharm and Sinovax vaccines were all inactivated whole virus vaccines [88]. This contrasts with the previous vaccines, which only contained a component of viral vaccines. The inactivated vaccines contained killed or inactivated copies of the virus, to introduce the immune system to a harmless version of the virus that cannot replicate and thus prompt a faster and more effective adaptive response [84,88]. The Sinopharm was the first of these inactivated viruses to be approved by the WHO and Trinidad and Tobago in May 2021, to meet the local demand for vaccines [89]. The Sinovac was next in June 2021 and lastly, Covaxin in November 2021 [84].
These vaccines were disseminated in Trinidad and Tobago through COVID-19 vaccine campaigns in which public advertisements were used to encourage citizens to take advantage of the free vaccines offered at designated vaccination centres. Overall, as of June 2023, Trinidad and Tobago had administered a total of 1.5 million vaccines, including multiple doses, out of a total population of 1.5 million. This has helped to decrease the incidence of COVID-19 in Trinidad and Tobago and assisted with the return to normal societal functioning [90]. It is essential to weigh these potential risks against the significant benefits of vaccination, which greatly reduce the risk of severe COVID-19 illness and death.
A study conducted in Trinidad and Tobago, assessed the safety of the ChAdOx1 nCoV-19 vaccine (Oxford–AstraZeneca) during the vaccination of healthcare workers during the National COVID-19 Vaccination Program in February 2021. Local and systemic side effects after receiving the first and second dose were reported via telephone questionnaire were gathered and analyzed. Among the participants, systemic side effects such as: body pain, fever, headache, chills, myalgia, nausea, and malaise seemed to be greatly diminished 48 hours after administration of the second dose, compared to the first dose. Additionally, analysis determined that there was an increased chance of younger recipients reporting systemic side effects, as compared to older recipients. Furthermore, it was found that females had a greater likelihood of experiencing fatigue, headache, and discomfort, and were more likely to report symptoms as compared to males, for both doses. This study have important implications for lowering vaccine hesitancy due to safety concerns [91].
“It was found that systemic and local side-effects after BNT162b2 and ChAdOx1 nCoV-19 vaccination occur at frequencies lower than reported in phase 3 trials. Both vaccines decrease the risk of SARS-CoV-2 infection after 12 days [92]”.
In May 2023, about 50% of individuals in Trinidad and Tobago had completed their COVID-19 vaccination regimen, falling short of the expected 63% who initially expressed willingness to get vaccinated before vaccines were available. Two studies on healthcare professionals in Trinidad and Tobago found that they had good COVID-19 knowledge, positive attitudes, and perceptions. Primary care workers in Trinidad and Tobago were hesitant to get vaccinated due to concerns about potential side effects, insufficient information, and the short duration of vaccine trials [93]. In February 2021, Trinidad and Tobago initiated its National COVID-19 Vaccination Program, with healthcare workers being among the initial recipients of the ChAdOx1 nCoV-19 vaccine (Oxford-AstraZeneca), which was the first COVID-19 vaccine to become available in the country [94]. Since then, Trinidad and Tobago COVID-19 vaccination program, initiated four different vaccines: Pfizer-BioNTech, Oxford/AstraZeneca, Johnson & Johnson, and Sinopharm [95]. Vaccines were made available to the public by several means: health centers, home visits (shut-in persons only) and community vaccination outreach activities [89] (How to Get the Vaccine and COVID-19 Vaccine Locations | Ministry of Health, n.d.). On August 25, 2021, Trinidad and Tobago's Ministry of Health authorized the administration of the Pfizer vaccine for expectant mothers in their second and third trimesters of pregnancy [95]. The Ministry of Health reported that as of May 02, 2023, its COVID-19 statistics showed 718,969 of the Trinidad and Tobago population has been fully vaccinated with 335 deaths from this category. The report also showed that citizens who were not fully vaccinated (encompass of 1st dose or no dose), had a mortality of 3665. During February and March 2021, previous to the commencement of the Ministry of Health of Trinidad and Tobago offering Covid-19 vaccination to its citizens, an article was released regarding the thorough preparation the Ministry of Health invested in order to have a problem free vaccination process. The article highlighted the utilization of the WHO and COVAX vaccination procedure guidelines by Trinidad and Tobago. This included the application of simulation exercises to normalize both patients and doctors of having the experience of giving and receiving the COVID-19 vaccine. Furthermore, it was revealed that some of the simulation exercises included doctors being trained to deal with vaccine hesitancy, walk in patients, patients who do not meet the vaccine recipient criteria as well as patients who may have allergic reactions to the vaccine. Nurses and other medical staff were guided on checking and inputting relevant information onto immunization cards and patient observation. The patient observation was necessary for thirty minutes post vaccination in order to identify and quickly assist patients who may develop a life threatening reaction to the vaccine. In conclusion, the article encapsulated all the efforts made by the Ministry of Health of Trinidad and Tobago in an attempt to have a successful vaccination roll out plan in order to help fight the COVID-19 pandemic [96].
An independent investigation sought to shed light on the sudden upsurge in COVID-19 cases from April 2021 onwards despite distribution of the vaccine to the local population, as well as an effort to trace and minimize spread of the virus which was praised by international committees. Some of the hypothesized factors included a lack of vaccines due to reliance on too few sources which were highly unreliable, which was coupled with a relaxation of COVID-19 measures, coincidentally at the beginning of the easter vacation period, resulting in a dramatic spike in infection rates. For context, as of May 2021, the twin island republic had procured 75 600 vaccines, with approximately half of those having been administered to citizens. This equated to only 3% of the estimated population of Trinidad and Tobago, with over 55% of vaccines being donated by other nations. In comparison, at the same period, fellow Caribbean nations were able to procure and vaccinate a much greater portion of their populations, which had directly negotiated and received their vaccines from the governments of the UK and India to name a few. Furthermore, Trinidad’s vaccine procurement strategy largely involved receiving vaccines from fellow Caribbean nations, which were unable to fully administer said vaccines prior to expiry, rather than receive these vaccines directly from the source/manufacturer. The study concluded that this vaccine procurement strategy, among other factors, left the government of Trinidad and Tobago largely unequipped to manage an exponential rise in COVID-19 cases due to the low availability of vaccines, and the small immunization rate amongst the population, with most of the nation’s vaccines having been received much later in the year, at which point the virus had run rampant [97].
In a study conducted in Trinidad and Tobago, reasons for COVID-19 vaccine hesitancy were explored. The study identified several factors contributing to hesitancy, including mistrust in institutions, doubts about the vaccine development process, reliability of information, complacency, and structural barriers to access. Participants also expressed concerns about adverse effects, safety during pregnancy, and effects on pre-existing medical conditions. Additionally, the study noted the influence of religiosity and herbal culture on vaccine uptake in this context. These findings contribute to understanding vaccine hesitancy and suggest areas for further research [93].
This study was focused on the effects of knowledge, attitudes, and perceptions of primary care health workers toward receiving the Oxford AstraZeneca vaccine in North Central, Trinidad. It explored the main contributors of hesitancy were due to inadequate clinical trial span and fear of adverse effects. Hesitancy towards vaccines stemmed from lack of information. This lack of information factor however was broken down between Health care professions, sex and marital status. This study highlighted that doctor had a higher perception and knowledge compared to other health care professions. Males also had a higher perception and attitude towards vaccination than females. Women were more skeptical towards the AstraZeneca vaccination like, safety, efficacy, and quality. Female candidates expressed concerns against the vaccine due to its effects on pregnancy, labor, and fertility. Marital status gave a positive correlation to single persons and the knowledge attitude towards the COVID-19 vaccine. Overall, this study expressed the various factors contributing to health care workers and their hesitancy towards AstraZeneca vaccination in Trinidad and Tobago. Overall, the COVID-19 vaccine uptake and acceptance rates were relatively low, 23.6% and 26.4%, respectively. This study can now increase beneficial strategies in information dissemination across the country [95].
The study examined the side effects of the ChAdOx1 nCov-19 vaccine and found that side effects varied significantly by gender and age, with females and younger individuals reporting more. However, side effects decreased significantly after the second dose. Four patients developed new-onset neurological diseases after vaccination, but due to the high prevalence of such diseases and the large number of vaccinations, establishing a causal relationship is challenging. Despite these rare adverse effects, the general safety profile of the vaccines was well established. Therefore, while it’s important to be aware of potential side effects, the benefits of vaccination outweigh the risks [98].
In December 2020, the Faculty of Medical Sciences' ad hoc committee on vaccinations (UWI-STA Committee on Vaccine Efficacy) conducted research and provided a critical evaluation of the existing evidence regarding the efficacy and safety of the COVID-19 vaccines, which have been authorized and made available to the general population. BioNTech/Pfizer (BNT162b2) and Moderna mRNA 1273 (both mRNA vaccines) were found to have efficacy of 95% and 86.4% respectively while the approved Oxford/Astra Zeneca (ChAdOx1 nCov-19) vaccine had an efficacy of 62.1%. Additionally, the Sinopharm vaccine (BBIBP-Cor vaccine) was reported to have an efficacy of 86%. It was also noted that these vaccines had good safety profiles. In addition, the research mentioned that the mRNA vaccines (BioNTech/Pfizer and Moderna) were linked to sporadic instances of anaphylactic-like reactions [99].
One of the main reasons the entire populace is not immunized against the COVID -19 virus is reluctance. Data on people's main vaccine worries were acquired using primary data collection techniques in research by the UWI-St Augustine Committee on COVID-19 Vaccine Hesitancy and Uptake. It was discovered that young individuals (ages 15 to 17) showed suspicion due to the speed at which the vaccinations were generated and the potential adverse consequences of the immunizations. Additionally, they held the view that people in good health who eat a balanced diet, lead active lifestyles, get enough sunlight, and live in overall good health are immune to the virus. Furthermore, older persons (25-40 years), were mainly concerned about the nature and efficacy of the vaccines, particularly the AstraZeneca vaccine. Additionally, immunocompromised patients (29-65) years with pre-existing comorbidities (such as cancer, hypertension, diabetes), explained that their hesitancy was due to the dissemination of false information from all media platforms. However, despite reluctance, the 2021 COVID-19 Vaccine Hesitancy Survey Report stated that 65% of respondents said they had been vaccinated, putting Trinidad and Tobago at the second highest percentage behind Barbados. Furthermore, it was shown that Sinopharm (used by 47%) and Oxford/AstraZeneca (used by 23%) were the two most popular brands [100].
4. Conclusion
“To combat the pandemic, vaccines for COVID-19 started developing at an exceptional rate. Many of them were approved for emergency use by different regulatory authorities like the Food and Drug Administration in the United States, the Medicines and Healthcare Products Regulatory Agency in the United Kingdom, and the European Medicines Agency after reviewing clinical efficacy data from phase 3 results, which subsequently led to mass vaccination worldwide [56].” This study concluded that immunization against the SARS-CoV2 virus yielded positive results in preventing infection, reducing Covid-19 related hospitalizations, ICU admissions, and mortality. Vaccination was found to be highly effective in controlling the spread of the SARS-CoV2 virus and improving outcomes in infected individuals. However, the efficacy of different vaccine platforms varied, suggesting that some vaccines may be more suitable for certain populations than others. Nucleic acid vaccines, such as Pfizer-BioNTech and Moderna, demonstrated the highest effectiveness, while inactivated whole virus vaccines like Sinopharm and viral vectors like Janssen were less effective. Common side effects across all vaccine types included joint/muscle soreness, shoulder pain, pain at the injection site, headaches, chills, weakness, fever, renal, epistaxis, and certain cardiovascular events. Adverse effects were more common and severe with the mRNA vaccines by Pfizer-BioNTech and Oxford-Astrazeneca than with inactivated whole virus vaccines. The information gathered in this study can assist individuals in deciding which vaccine is most suitable for them and inform the public about potential side effects. Further long-term studies are required to fully understand the range of side effects associated with each vaccine type. The global pandemic of COVID-19 has posed an unprecedented challenge to public health in Trinidad and Tobago and globally. After a strenuous three-year fight, the World Health Organization (WHO) announced that the pandemic no longer constituted a global health emergency. Nonetheless, vaccination continues to be a crucial part of the ongoing management strategy, particularly in areas where vaccine hesitancy is prevalent.
Table 4 shows a sumary of the aims/questions, type of study and results of the selected studies in the systematic review.
Author Contributions
Conceptualization, A.J.-V, D.G.; Sachin Soodeen (S.S.); methodology, All authors; software and statistical analysis, All authors; validation, All authors; and investigation, All authors; writing—original draft preparation, A.J.-V, K.R., Shaundell Solomon (S.S.), A.P., writing—review and editing, WIIS. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank the West Indian Immunology Society (WIIS) for support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Pormohammad, A.; Zarei, M.; Ghorbani, S.; Mohammadi, M.; Razizadeh, M.H.; Turner, D.L.; Turner, R.J. Efficacy and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Vaccines (Basel) 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Forni, G.; Mantovani, A.; COVID-19 Commission of Accademia Nazionale dei Lincei, Rome. COVID-19 Vaccines: Where We Stand and Challenges Ahead. Cell Death Differ. 2021, 28, 626–639. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Shao, W.; Chen, X.; Zhang, B.; Wang, G.; Zhang, W. Real-World Effectiveness of COVID-19 Vaccines: A Literature Review and Meta-Analysis. Int. J. Infect. Dis. 2022, 114, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Al-Momani, H.; Aldajah, K.; Alda’ajah, E.; ALjafar, Y.; Abushawer, Z. Effectiveness of Pfizer/BioNTech and Sinopharm COVID-19 Vaccines in Reducing Hospital Admissions in Prince Hamza Hospital, Jordan. Front Public Health 2022, 10, 1008521. [Google Scholar] [CrossRef] [PubMed]
- Hadj Hassine, I. Covid-19 Vaccines and Variants of Concern: A Review. Rev. Med. Virol. 2022, 32, e2313. [Google Scholar] [CrossRef] [PubMed]
- Francis, A.I.; Ghany, S.; Gilkes, T.; Umakanthan, S. Review of COVID-19 Vaccine Subtypes, Efficacy and Geographical Distributions. Postgrad. Med. J. 2022, 98, 389–394. [Google Scholar] [CrossRef] [PubMed]
- GRADE: Pfizer-BioNTech COVID-19 Vaccine Available online:. Available online: https://www.cdc.gov/vaccines/acip/recs/grade/covid-19-pfizer-biontech-vaccine.html (accessed on 7 November 2023).
- Rotshild, V.; Hirsh-Raccah, B.; Miskin, I.; Muszkat, M.; Matok, I. Comparing the Clinical Efficacy of COVID-19 Vaccines: A Systematic Review and Network Meta-Analysis. Sci. Rep. 2021, 11, 22777. [Google Scholar] [CrossRef] [PubMed]
- Saciuk, Y.; Kertes, J.; Mandel, M.; Hemo, B.; Shamir Stein, N.; Ekka Zohar, A. Pfizer-BioNTech Vaccine Effectiveness against Sars-Cov-2 Infection: Findings from a Large Observational Study in Israel. Prev. Med. 2022, 155, 106947. [Google Scholar] [CrossRef] [PubMed]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca Vaccines on Covid-19 Related Symptoms, Hospital Admissions, and Mortality in Older Adults in England: Test Negative Case-Control Study. BMJ 2021, 373, n1088. [Google Scholar] [CrossRef]
- Soiza, R.L.; Scicluna, C.; Thomson, E.C. Efficacy and Safety of COVID-19 Vaccines in Older People. Age Ageing 2021, 50, 279–283. [Google Scholar] [CrossRef]
- Piechotta, V.; Siemens, W.; Thielemann, I.; Toews, M.; Koch, J.; Vygen-Bonnet, S.; Kothari, K.; Grummich, K.; Braun, C.; Kapp, P.; et al. Safety and Effectiveness of Vaccines against COVID-19 in Children Aged 5-11 Years: A Systematic Review and Meta-Analysis. Lancet Child Adolesc Health 2023, 7, 379–391. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Self, W.H.; Naioti, E.A.; Ginde, A.A.; Douin, D.J.; Olson, S.M.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; Zepeski, A.; et al. Sustained Effectiveness of Pfizer-BioNTech and Moderna Vaccines Against COVID-19 Associated Hospitalizations Among Adults - United States, March-July 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1156–1162. [Google Scholar] [CrossRef]
- Elamin, M.Y.; Maslamani, Y.A.; Muaddi, M.A.; Alameer, A.A.; Alqassim, A.Y.; Doweri, A.A.; Zaylaee, M.M.; Rayani, H.Y.; Darraj, A.Y.; Hejri, Y.M.; et al. Real-World Effectiveness of COVID-19 Vaccines: A Retrospective Cohort Study of Vaccinated Individuals in Jazan, Saudi Arabia. J. Infect. Public Health 2023, 16, 1512–1517. [Google Scholar] [CrossRef]
- Moreira, E.D., Jr; Kitchin, N.; Xu, X.; Dychter, S.S.; Lockhart, S.; Gurtman, A.; Perez, J.L.; Zerbini, C.; Dever, M.E.; Jennings, T.W.; et al. Safety and Efficacy of a Third Dose of BNT162b2 Covid-19 Vaccine. N. Engl. J. Med. 2022, 386, 1910–1921. [Google Scholar] [CrossRef] [PubMed]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef]
- Chirico, F.; Teixeira da Silva, J.A.; Tsigaris, P.; Sharun, K. Safety & Effectiveness of COVID-19 Vaccines: A Narrative Review. Indian J. Med. Res. 2022, 155, 91–104. [Google Scholar]
- Mohammed, I.; Nauman, A.; Paul, P.; Ganesan, S.; Chen, K.-H.; Jalil, S.M.S.; Jaouni, S.H.; Kawas, H.; Khan, W.A.; Vattoth, A.L.; et al. The Efficacy and Effectiveness of the COVID-19 Vaccines in Reducing Infection, Severity, Hospitalization, and Mortality: A Systematic Review. Hum. Vaccin. Immunother. 2022, 18, 2027160. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. Covid-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Zeng, B.; Gao, L.; Zhou, Q.; Yu, K.; Sun, F. Effectiveness of COVID-19 Vaccines against SARS-CoV-2 Variants of Concern: A Systematic Review and Meta-Analysis. BMC Med. 2022, 20, 200. [Google Scholar] [CrossRef]
- GRADE: Moderna COVID-19 Vaccine Available online:. Available online: https://www.cdc.gov/vaccines/acip/recs/grade/covid-19-moderna-vaccine.html (accessed on 7 November 2023).
- Rahmani, K.; Shavaleh, R.; Forouhi, M.; Disfani, H.F.; Kamandi, M.; Oskooi, R.K.; Foogerdi, M.; Soltani, M.; Rahchamani, M.; Mohaddespour, M.; et al. The Effectiveness of COVID-19 Vaccines in Reducing the Incidence, Hospitalization, and Mortality from COVID-19: A Systematic Review and Meta-Analysis. Front Public Health 2022, 10, 873596. [Google Scholar] [CrossRef]
- Soheili, M.; Khateri, S.; Moradpour, F.; Mohammadzedeh, P.; Zareie, M.; Mortazavi, S.M.M.; Manifar, S.; Kohan, H.G.; Moradi, Y. The Efficacy and Effectiveness of COVID-19 Vaccines around the World: A Mini-Review and Meta-Analysis. Ann. Clin. Microbiol. Antimicrob. 2023, 22, 42. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Tenforde, M.W.; Rhoads, J.P.; Gaglani, M.; Ginde, A.A.; Douin, D.J.; Olson, S.M.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; et al. Comparative Effectiveness of Moderna, Pfizer-BioNTech, and Janssen (Johnson & Johnson) Vaccines in Preventing COVID-19 Hospitalizations Among Adults Without Immunocompromising Conditions - United States, March-August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1337–1343. [Google Scholar] [PubMed]
- Harris, D.A.; Hayes, K.N.; Zullo, A.R.; Mor, V.; Chachlani, P.; Deng, Y.; McCarthy, E.P.; Djibo, D.A.; McMahill-Walraven, C.N.; Gravenstein, S. Comparative Risks of Potential Adverse Events Following COVID-19 mRNA Vaccination Among Older US Adults. JAMA Netw Open 2023, 6, e2326852. [Google Scholar] [CrossRef] [PubMed]
- Dickerman, B.A.; Gerlovin, H.; Madenci, A.L.; Kurgansky, K.E.; Ferolito, B.R.; Figueroa Muñiz, M.J.; Gagnon, D.R.; Gaziano, J.M.; Cho, K.; Casas, J.P.; et al. Comparative Effectiveness of BNT162b2 and mRNA-1273 Vaccines in U.S. Veterans. N. Engl. J. Med. 2022, 386, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Doria-Rose, N.A.; Shen, X.; Schmidt, S.D.; O’Dell, S.; McDanal, C.; Feng, W.; Tong, J.; Eaton, A.; Maglinao, M.; Tang, H.; et al. Booster of mRNA-1273 Strengthens SARS-CoV-2 Omicron Neutralization. medRxiv 2021. [Google Scholar] [CrossRef] [PubMed]
- Center for Biologics Evaluation; Research Moderna COVID-19 Vaccine Available online:. Available online: https://www.fda.gov/vaccines-blood-biologics/coronavirus-covid-19-cber-regulated-biologics/moderna-covid-19-vaccine (accessed on 6 November 2023).
- Nanduri, S.; Pilishvili, T.; Derado, G.; Soe, M.M.; Dollard, P.; Wu, H.; Li, Q.; Bagchi, S.; Dubendris, H.; Link-Gelles, R.; et al. Effectiveness of Pfizer-BioNTech and Moderna Vaccines in Preventing SARS-CoV-2 Infection Among Nursing Home Residents Before and During Widespread Circulation of the SARS-CoV-2 B.1.617.2 (Delta) Variant - National Healthcare Safety Network, March 1-August 1, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1163–1166. [Google Scholar] [PubMed]
- Mazagatos, C.; Monge, S.; Olmedo, C.; Vega, L.; Gallego, P.; Martín-Merino, E.; Sierra, M.J.; Limia, A.; Larrauri, A.; Working Group for the surveillance and control of COVID-19 in Spain; et al. Effectiveness of mRNA COVID-19 Vaccines in Preventing SARS-CoV-2 Infections and COVID-19 Hospitalisations and Deaths in Elderly Long-Term Care Facility Residents, Spain, Weeks 53 2020 to 13 2021. Euro Surveill. 2021, 26. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.-J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 Vaccines for Their Characteristics, Efficacy and Effectiveness against SARS-CoV-2 and Variants of Concern: A Narrative Review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef]
- Kaura, A.; Trickey, A.; Shah, A.S.V.; Benedetto, U.; Glampson, B.; Mulla, A.; Mercuri, L.; Gautama, S.; Costelloe, C.E.; Goodman, I.; et al. Comparing the Longer-Term Effectiveness of a Single Dose of the Pfizer-BioNTech and Oxford-AstraZeneca COVID-19 Vaccines across the Age Spectrum. EClinicalMedicine 2022, 46, 101344. [Google Scholar] [CrossRef]
- Asano, M.; Okada, H.; Itoh, Y.; Hirata, H.; Ishikawa, K.; Yoshida, E.; Matsui, A.; Kelly, E.J.; Shoemaker, K.; Olsson, U.; et al. Immunogenicity and Safety of AZD1222 (ChAdOx1 nCoV-19) against SARS-CoV-2 in Japan: A Double-Blind, Randomized Controlled Phase 1/2 Trial. Int. J. Infect. Dis. 2022, 114, 165–174. [Google Scholar] [CrossRef]
- Harvey, R.A.; Rassen, J.A.; Kabelac, C.A.; Turenne, W.; Leonard, S.; Klesh, R.; Meyer, W.A., 3rd; Kaufman, H.W.; Anderson, S.; Cohen, O.; et al. Association of SARS-CoV-2 Seropositive Antibody Test With Risk of Future Infection. JAMA Intern. Med. 2021, 181, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Letafati, A.; Eyvazzadeh, N.; Gharehkhani, A.; Khorshidian, A.; Chalabiani, S.; Soufiani, E.K.; Khakpoor, N.; Shamsodini, B.; Beheshti, T.; Bavili Olyaei, R.T.; et al. Comparison of AstraZeneca and Sinopharm Vaccines as Boosters in Protection against COVID-19 Infection. Biologicals 2023, 82, 101668. [Google Scholar] [CrossRef] [PubMed]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef] [PubMed]
- Hardt, K.; Vandebosch, A.; Sadoff, J.; Le Gars, M.; Truyers, C.; Lowson, D.; Van Dromme, I.; Vingerhoets, J.; Kamphuis, T.; Scheper, G.; et al. Efficacy, Safety, and Immunogenicity of a Booster Regimen of Ad26.COV2.S Vaccine against COVID-19 (ENSEMBLE2): Results of a Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet Infect. Dis. 2022, 22, 1703–1715. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Mateus, J.; Coelho, C.H.; Dan, J.M.; Moderbacher, C.R.; Gálvez, R.I.; Cortes, F.H.; Grifoni, A.; Tarke, A.; Chang, J.; et al. Humoral and Cellular Immune Memory to Four COVID-19 Vaccines. Cell 2022, 185, 2434–2451. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, K.E.; Le Gars, M.; Sadoff, J.; de Groot, A.M.; Heerwegh, D.; Truyers, C.; Atyeo, C.; Loos, C.; Chandrashekar, A.; McMahan, K.; et al. Immunogenicity of the Ad26.COV2.S Vaccine for COVID-19. JAMA 2021, 325, 1535–1544. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Zhu, Y.; Chu, M. Role of COVID-19 Vaccines in SARS-CoV-2 Variants. Front. Immunol. 2022, 13, 898192. [Google Scholar] [CrossRef] [PubMed]
- Nadeem, I.; Ul Munamm, S.A.; Ur Rasool, M.; Fatimah, M.; Abu Bakar, M.; Rana, Z.K.; Khatana, U.F.; Jordon, L.; Saqlain, M.; Mahdi, N.; et al. Safety and Efficacy of Sinopharm Vaccine (BBIBP-CorV) in Elderly Population of Faisalabad District of Pakistan. Postgrad. Med. J. 2023, 99, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Chen, L.-Y.; Lu, Q.-B.; Cui, F. Vaccination with the Inactivated Vaccine (Sinopharm BBIBP-CorV) Ensures Protection against SARS-CoV-2 Related Disease. Vaccines (Basel) 2022, 10. [Google Scholar] [CrossRef]
- Alqassieh, R.; Suleiman, A.; Abu-Halaweh, S.; Santarisi, A.; Shatnawi, O.; Shdaifat, L.; Tarifi, A.; Al-Tamimi, M.; Al-Shudifat, A.-E.; Alsmadi, H.; et al. Pfizer-BioNTech and Sinopharm: A Comparative Study on Post-Vaccination Antibody Titers. Vaccines (Basel) 2021, 9. [Google Scholar] [CrossRef]
- Jamalidoust, M.; Eilami, O.; Ashkan, Z.; Ziyaeyan, M.; Aliabadi, N.; Habibi, M. The Rates and Symptoms of Natural and Breakthrough Infection Pre- and Post- Covid-19 Non-mRNA Vaccination at Various Peaks amongst Iranian Healthcare Workers. Virol. J. 2023, 20, 182. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Belayachi, J.; Yang, Y.; Fu, Q.; Rodewald, L.; Li, H.; Yan, B.; Wang, Y.; Shen, Y.; Yang, Q.; et al. Real-World Study of the Effectiveness of BBIBP-CorV (Sinopharm) COVID-19 Vaccine in the Kingdom of Morocco. BMC Public Health 2022, 22, 1584. [Google Scholar] [CrossRef] [PubMed]
- Dunkle, L.M.; Kotloff, K.L.; Gay, C.L.; Áñez, G.; Adelglass, J.M.; Barrat Hernández, A.Q.; Harper, W.L.; Duncanson, D.M.; McArthur, M.A.; Florescu, D.F.; et al. Efficacy and Safety of NVX-CoV2373 in Adults in the United States and Mexico. N. Engl. J. Med. 2022, 386, 531–543. [Google Scholar] [CrossRef] [PubMed]
- Marchese, A.M.; Zhou, X.; Kinol, J.; Underwood, E.; Woo, W.; McGarry, A.; Beyhaghi, H.; Áñez, G.; Toback, S.; Dunkle, L.M. NVX-CoV2373 Vaccine Efficacy against Hospitalization: A Post Hoc Analysis of the PREVENT-19 Phase 3, Randomized, Placebo-Controlled Trial. Vaccine 2023, 41, 3461–3466. [Google Scholar] [CrossRef] [PubMed]
- Graña, C.; Ghosn, L.; Evrenoglou, T.; Jarde, A.; Minozzi, S.; Bergman, H.; Buckley, B.S.; Probyn, K.; Villanueva, G.; Henschke, N.; et al. Efficacy and Safety of COVID-19 Vaccines. Cochrane Database Syst. Rev. 2022. [Google Scholar] [CrossRef] [PubMed]
- Dighriri, I.M.; Alhusayni, K.M.; Mobarki, A.Y.; Aljerary, I.S.; Alqurashi, K.A.; Aljuaid, F.A.; Alamri, K.A.; Mutwalli, A.A.; Maashi, N.A.; Aljohani, A.M.; et al. Pfizer-BioNTech COVID-19 Vaccine (BNT162b2) Side Effects: A Systematic Review. Cureus 2022, 14, e23526. [Google Scholar] [CrossRef] [PubMed]
- Finsterer, J.; Scorza, F.A.; Scorza, C.A. Post SARS-CoV-2 Vaccination Guillain-Barre Syndrome in 19 Patients. Clinics 2021, 76, e3286. [Google Scholar] [CrossRef] [PubMed]
- Wiedmann, M.; Skattør, T.; Stray-Pedersen, A.; Romundstad, L.; Antal, E.-A.; Marthinsen, P.B.; Sørvoll, I.H.; Leiknes Ernstsen, S.; Lund, C.G.; Holme, P.A.; et al. Vaccine Induced Immune Thrombotic Thrombocytopenia Causing a Severe Form of Cerebral Venous Thrombosis With High Fatality Rate: A Case Series. Front. Neurol. 2021, 12, 721146. [Google Scholar] [CrossRef] [PubMed]
- Introna, A.; Caputo, F.; Santoro, C.; Guerra, T.; Ucci, M.; Mezzapesa, D.M.; Trojano, M. Guillain-Barré Syndrome after AstraZeneca COVID-19-Vaccination: A Causal or Casual Association? Clin. Neurol. Neurosurg. 2021, 208, 106887. [Google Scholar] [CrossRef]
- Göbel, C.H.; Heinze, A.; Karstedt, S.; Morscheck, M.; Tashiro, L.; Cirkel, A.; Hamid, Q.; Halwani, R.; Temsah, M.-H.; Ziemann, M.; et al. Clinical Characteristics of Headache after Vaccination against COVID-19 (coronavirus SARS-CoV-2) with the BNT162b2 mRNA Vaccine: A Multicentre Observational Cohort Study. Brain Commun 2021, 3, fcab169. [Google Scholar] [CrossRef]
- García-Azorín, D.; Do, T.P.; Gantenbein, A.R.; Hansen, J.M.; Souza, M.N.P.; Obermann, M.; Pohl, H.; Schankin, C.J.; Schytz, H.W.; Sinclair, A.; et al. Delayed Headache after COVID-19 Vaccination: A Red Flag for Vaccine Induced Cerebral Venous Thrombosis. J. Headache Pain 2021, 22, 108. [Google Scholar] [CrossRef] [PubMed]
- Sharifian-Dorche, M.; Bahmanyar, M.; Sharifian-Dorche, A.; Mohammadi, P.; Nomovi, M.; Mowla, A. Vaccine-Induced Immune Thrombotic Thrombocytopenia and Cerebral Venous Sinus Thrombosis Post COVID-19 Vaccination; a Systematic Review. J. Neurol. Sci. 2021, 428, 117607. [Google Scholar] [CrossRef]
- Tahir, N.; Koorapati, G.; Prasad, S.; Jeelani, H.M.; Sherchan, R.; Shrestha, J.; Shayuk, M. SARS-CoV-2 Vaccination-Induced Transverse Myelitis. Cureus 2021, 13, e16624. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.-J.; Tseng, H.-P.; Lin, C.-L.; Shiu, J.-S.; Lee, M.-H.; Liu, C.-H. Acute Transverse Myelitis Following COVID-19 Vaccination. Vaccines (Basel) 2021, 9. [Google Scholar] [CrossRef]
- Notghi, A.A.; Atley, J.; Silva, M. Lessons of the Month 1: Longitudinal Extensive Transverse Myelitis Following AstraZeneca COVID-19 Vaccination. Clin. Med. 2021, 21, e535–e538. [Google Scholar] [CrossRef]
- Burrows, A.; Bartholomew, T.; Rudd, J.; Walker, D. Sequential Contralateral Facial Nerve Palsies Following COVID-19 Vaccination First and Second Doses. BMJ Case Rep. 2021, 14. [Google Scholar] [CrossRef]
- Patel, R.; Kaki, M.; Potluri, V.S.; Kahar, P.; Khanna, D. A Comprehensive Review of SARS-CoV-2 Vaccines: Pfizer, Moderna & Johnson & Johnson. Hum. Vaccin. Immunother. 2022, 18, 2002083. [Google Scholar] [PubMed]
- Watad, A.; De Marco, G.; Mahajna, H.; Druyan, A.; Eltity, M.; Hijazi, N.; Haddad, A.; Elias, M.; Zisman, D.; Naffaa, M.E.; et al. Immune-Mediated Disease Flares or New-Onset Disease in 27 Subjects Following mRNA/DNA SARS-CoV-2 Vaccination. Vaccines (Basel) 2021, 9. [Google Scholar] [CrossRef]
- Khayat-Khoei, M.; Bhattacharyya, S.; Katz, J.; Harrison, D.; Tauhid, S.; Bruso, P.; Houtchens, M.K.; Edwards, K.R.; Bakshi, R. COVID-19 mRNA Vaccination Leading to CNS Inflammation: A Case Series. J. Neurol. 2022, 269, 1093–1106. [Google Scholar] [CrossRef]
- Zuhorn, F.; Graf, T.; Klingebiel, R.; Schäbitz, W.-R.; Rogalewski, A. Postvaccinal Encephalitis after ChAdOx1 nCov-19. Ann. Neurol. 2021, 90, 506–511. [Google Scholar] [CrossRef]
- Corrêa, D.G.; Cañete, L.A.Q.; Dos Santos, G.A.C.; de Oliveira, R.V.; Brandão, C.O.; da Cruz, L.C.H., Jr. Neurological Symptoms and Neuroimaging Alterations Related with COVID-19 Vaccine: Cause or Coincidence? Clin. Imaging 2021, 80, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis With COVID-19 mRNA Vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.Y.; Kim, K.H.; Lee, N.; Cho, S.H.; Kim, S.Y.; Kim, E.K.; Park, J.-H.; Choi, E.-Y.; Choi, J.-O.; Park, H.; et al. COVID-19 Vaccination-Related Myocarditis: A Korean Nationwide Study. Eur. Heart J. 2023, 44, 2234–2243. [Google Scholar] [CrossRef] [PubMed]
- Hromić-Jahjefendić, A.; Sezer, A.; Aljabali, A.A.A.; Serrano-Aroca, Á.; Tambuwala, M.M.; Uversky, V.N.; Redwan, E.M.; Barh, D.; Lundstrom, K. COVID-19 Vaccines and Myocarditis: An Overview of Current Evidence. Biomedicines 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Abdeldayem, E.H.; Raief Mosaad, B.M.; Yassin, A.; Abdelrahman, A.S. Cardiac MRI in Patients with COVID-19 Infection. Eur. Radiol. 2023, 33, 3867–3877. [Google Scholar] [CrossRef] [PubMed]
- Haider, S.M.S.; Alvi, S.A.; Khan, H.; Majeed, R.; Syed, T.; Anwar, A.; Hashmi, A.A. Common Side Effects of Pfizer COVID-19 Vaccine: An Experience From Pakistan. Cureus 2023, 15, e40878. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, R.A.; Garout, R.M.; Wahid, S.; Ayub, F.; Firas ZinAlddin, L.M.; Sultan, I. A Survey on the Side Effects of Pfizer/BioNTech COVID-19 Vaccine Among Vaccinated Adults in Saudi Arabia. Cureus 2021, 13, e19222. [Google Scholar] [CrossRef] [PubMed]
- Abukhalil, A.D.; Shatat, S.S.; Abushehadeh, R.R.; Al-Shami, N. ’meh; Naseef, H.A.; Rabba, A. Side Effects of Pfizer/BioNTech (BNT162b2) COVID-19 Vaccine Reported by the Birzeit University Community. BMC Infect. Dis. 2023, 23, 5. [Google Scholar] [CrossRef] [PubMed]
- Oster, M.E.; Shay, D.K.; Su, J.R.; Gee, J.; Creech, C.B.; Broder, K.R.; Edwards, K.; Soslow, J.H.; Dendy, J.M.; Schlaudecker, E.; et al. Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021. JAMA 2022, 327, 331–340. [Google Scholar] [CrossRef]
- Akiyama, H.; Kakiuchi, S.; Rikitake, J.; Matsuba, H.; Sekinada, D.; Kozuki, Y.; Iwata, N. Immune Thrombocytopenia Associated with Pfizer-BioNTech’s BNT162b2 mRNA COVID-19 Vaccine. IDCases 2021, 25, e01245. [Google Scholar] [CrossRef]
- Ganesan, S.; Al Ketbi, L.M.B.; Al Kaabi, N.; Al Mansoori, M.; Al Maskari, N.N.; Al Shamsi, M.S.; Alderei, A.S.; El Eissaee, H.N.; Al Ketbi, R.M.; Al Shamsi, N.S.; et al. Vaccine Side Effects Following COVID-19 Vaccination Among the Residents of the UAE-An Observational Study. Front Public Health 2022, 10, 876336. [Google Scholar] [CrossRef] [PubMed]
- Khan, Z.; Pabani, U.K.; Gul, A.; Muhammad, S.A.; Yousif, Y.; Abumedian, M.; Elmahdi, O.; Gupta, A. COVID-19 Vaccine-Induced Myocarditis: A Systemic Review and Literature Search. Cureus 2022, 14, e27408. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.-J.; Cines, D.B.; Gernsheimer, T.; Kessler, C.; Michel, M.; Tarantino, M.D.; Semple, J.W.; Arnold, D.M.; Godeau, B.; Lambert, M.P.; et al. Thrombocytopenia Following Pfizer and Moderna SARS-CoV-2 Vaccination. Am. J. Hematol. 2021, 96, 534–537. [Google Scholar] [CrossRef]
- Desalegn, M.; Garoma, G.; Tamrat, H.; Desta, A.; Prakash, A. The Prevalence of AstraZeneca COVID-19 Vaccine Side Effects among Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital Health Workers. Cross Sectional Survey. PLoS One 2022, 17, e0265140. [Google Scholar] [CrossRef] [PubMed]
- Haider, T.; Ali, J.; Ali, S.M.; Iftikhar, A.S.; Siddiqui, A.A.; Khan, A.S.; Qamar, J.A.; Sohail, K.; Anwar, A.; Hashmi, A.A. Prevalence of Side Effects of the AstraZeneca COVID-19 Vaccine: A Multicenter Experience From Pakistan. Cureus 2023, 15, e46543. [Google Scholar] [CrossRef] [PubMed]
- Johnson & Johnson Updates, U.S. COVID-19 Vaccine Fact Sheet Available online:. Available online: https://www.jnj.com/johnson-johnson-updates-u-s-covid-19-vaccine-fact-sheet (accessed on 10 November 2023).
- Haider, T.; Abidi, S.R.Z.; Fatima, M.; Zafar, A.; Siddiqui, R.Q.U.; Khan, W.; Saeed, T.; Anwar, A.; Hashmi, A.A. The Prevalence of Side Effects of Sinopharm COVID-19 Vaccine: An Experience From Pakistan. Cureus 2023, 15, e38180. [Google Scholar] [CrossRef] [PubMed]
- Dadras, O.; Mehraeen, E.; Karimi, A.; Tantuoyir, M.M.; Afzalian, A.; Nazarian, N.; Mojdeganlou, H.; Mirzapour, P.; Shamsabadi, A.; Dashti, M.; et al. Safety and Adverse Events Related to Inactivated COVID-19 Vaccines and Novavax;a Systematic Review. Arch Acad Emerg Med 2022, 10, e54. [Google Scholar] [PubMed]
- Lindo, P. Health Ministry Begins “One Shot and Done” Initiative with J&J Vaccine - Trinidad and Tobago Newsday. Trinidad and Tobago Newsday 2021. [Google Scholar]
- Mar, 31 Trinidad and Tobago Receives the First COVID-19 Vaccines through the COVAX Facility Available online:. Available online: https://www.paho.org/en/news/31-3-2021-trinidad-and-tobago-receives-first-covid-19-vaccines-through-covax-facility (accessed on 7 November 2023).
- George, K. Tobago Parents Contacted for Pfizer Vaccine Approval. Trinidad and Tobago Newsday 2021. [Google Scholar]
- The Oxford/AstraZeneca (ChAdOx1-S [recombinant] Vaccine) COVID-19 Vaccine: What You Need to Know. Available online: https://www.who.int/news-room/feature-stories/detail/the-oxford-astrazeneca-covid-19-vaccine-what-you-need-to-know/ (accessed on 7 November 2023).
- Munavalli, G.G.; Guthridge, R.; Knutsen-Larson, S.; Brodsky, A.; Matthew, E.; Landau, M. COVID-19/SARS-CoV-2 Virus Spike Protein-Related Delayed Inflammatory Reaction to Hyaluronic Acid Dermal Fillers: A Challenging Clinical Conundrum in Diagnosis and Treatment. Arch. Dermatol. Res. 2022, 314, 1–15. [Google Scholar] [CrossRef]
- Wilson, S.-A. Trinidad and Tobago. In Politics of Identity in Small Plural Societies; Palgrave Macmillan US: New York, 2012; ISBN 9781349342426. [Google Scholar]
- Meo, S.A.; ElToukhy, R.A.; Meo, A.S.; Klonoff, D.C. Comparison of Biological, Pharmacological Characteristics, Indications, Contraindications, Efficacy, and Adverse Effects of Inactivated Whole-Virus COVID-19 Vaccines Sinopharm, CoronaVac, and Covaxin: An Observational Study. Vaccines (Basel) 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- What Is COVID-19. Available online: https://health.gov.tt/covid-19 (accessed on 7 November 2023).
- Individual; Family Health Pediatric COVID-19 Vaccination. Available online: https://www.health.state.mn.us/diseases/coronavirus/vaccine/peds.html (accessed on 8 November 2023).
- Rafeek, R.; Sa, B.; Smith, W. Vaccine Acceptance, Knowledge, Attitude and Practices Regarding the COVID-19 Pandemic: Cross-Sectional Study among Dentists in Trinidad and Tobago. Dent. J. 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- CDC COVID-19 Response Team. Food and Drug Administration Allergic Reactions Including Anaphylaxis After Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine - United States, December 14-23, 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Motilal, S.; Ward, D.; Mahabir, K.; Lopez, T.; Logan, R.; Maharaj, S.; Maloney, J.; Marson, M.; Marcelle, C. COVID-19 Vaccine Hesitancy in Trinidad and Tobago: A Qualitative Study. Cureus 2023, 15, e43171. [Google Scholar] [CrossRef] [PubMed]
- Gopaul, C.D.; Ventour, D.; Thomas, D. ChAdOx1 nCoV-19 Vaccine Side Effects among Healthcare Workers in Trinidad and Tobago. Vaccines (Basel) 2022, 10. [Google Scholar] [CrossRef]
- Khan, S.; Sohan, K.; Mohammed, Z.C.M.; Bachan, V. COVID-19 Vaccine Uptake, Acceptance, and Reasons for Vaccine Hesitancy: A Cross-Sectional Study among Pregnant Women in Trinidad, West Indies [Response To Letter]. Int. J. Womens Health 2023, 15, 621–622. [Google Scholar] [CrossRef]
- Simulating COVID-19 Vaccination in Trinidad and Tobago. Available online: https://www.who.int/news-room/feature-stories/detail/simulating-covid-19-vaccination-in-trinidad-and-tobago (accessed on 8 November 2023).
- COVID-19 Fortnightly Update - Tuesday May 02, 2023. Available online: https://health.gov.tt/covid-19-fortnightly-update-tuesday-may-02-2023 (accessed on 8 November 2023).
- Fernandes, J.; Jaggernauth, S.; Ramnarine, V.; Mohammed, S.R.; Khan, C.; Panday, A. Neurological Conditions Following COVID-19 Vaccinations: Chance or Association? Cureus 2022, 14, e21919. [Google Scholar] [CrossRef]
- Review of the Current Status of COVID-19 Vaccines v1.0.pdf. (accessed on 8 October 2023).
- COVID-19 Vaccines - Addressing Hesitancy 2021050302.pdf. (accessed on 15 September 2023).
Figure 1.
PRISMA Flow Chart showing identification & inclusion process of studies.
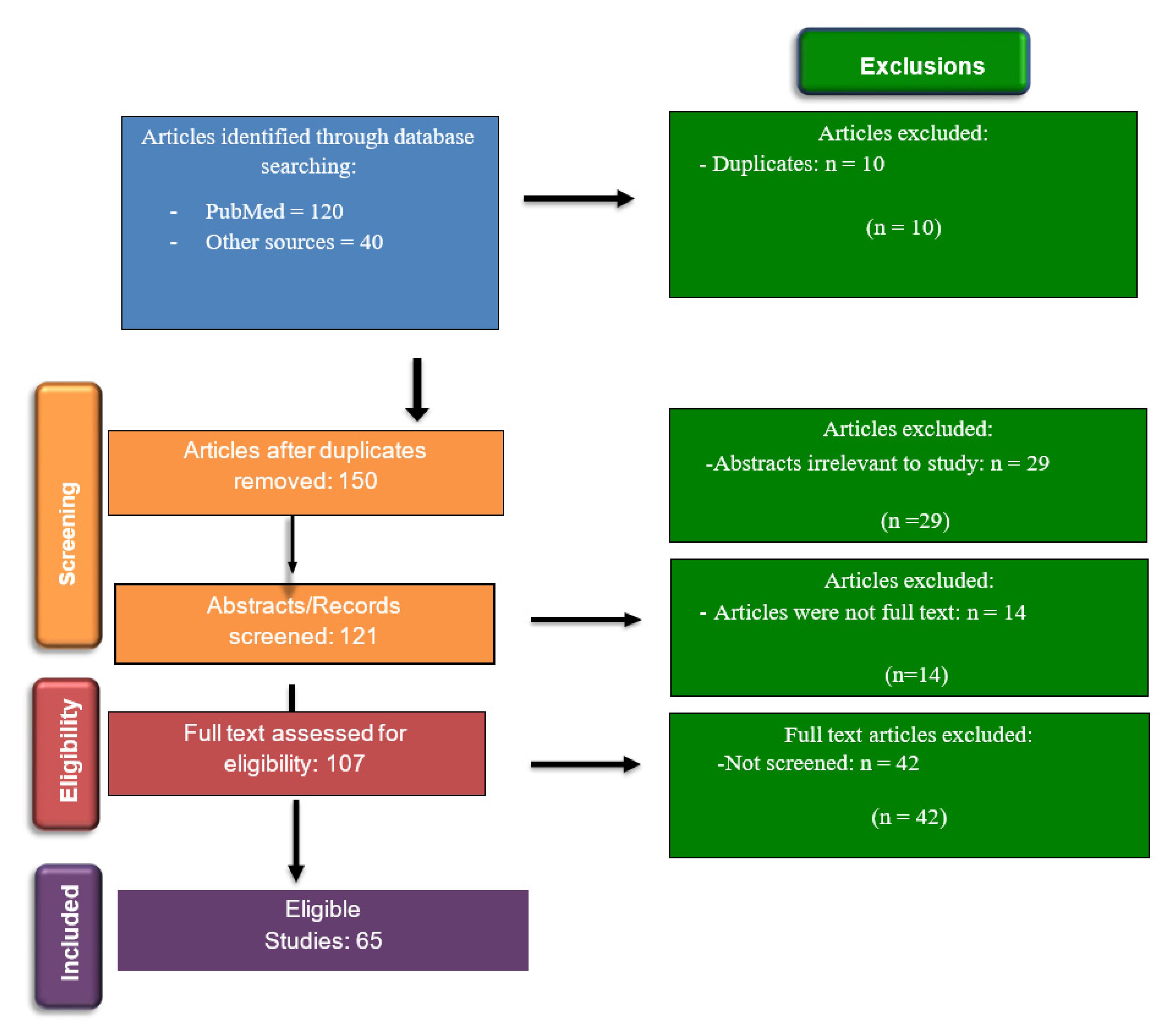

Table 1.
Showing Eligibility/Inclusion Criteria for study using PICOS format.
| Population | Intervention | Comparison | Outcome | Study Type |
| Aged 5-<80 years | Six COVID-19 vaccines including Pfizer-BioNTech, Moderna, Novavax, AstraZeneca, Sinopharm, and Janssen | Effectiveness and safety | Decreased morbidity and mortality COVID-19 vaccination in Trinidad and Tobago |
All Study Types |
Table 2.
Table comparing the vaccine effectiveness (VE) of different Covid-19 vaccines.
| Covid-19 Vaccines | Type of Vaccine | Vaccine Effectiveness, VE (%) |
|---|---|---|
|
Pfizer-BioNTech BNT162b2 |
Nucleic acid | 95 |
|
Moderna mRNA-1273 |
Nucleic acid | 94.1 |
|
Novavax NVX-CoV2373 |
Protein based | 89.7 |
|
AstraZeneca AZD1222 |
Viral vector | 70.4 |
|
Sinopharm BBIBP-CorV |
Whole virus (inactivated) | 67 |
|
Janssen Ad26.COV2.S |
Viral vector | 66.9 |
Table 3.
Side effects of the COVID-19 vaccines and references.
| Vaccines | Side effects | Source |
|---|---|---|
| Pfizer-BioNTech |
Common: Burning, pain and swelling at the injection site, fever, joint pain Rare: thrombocytopenia and myocarditis, |
[69,70] [71,72,73] |
| Moderna | Common: pain at the site of injection, fatigue, drowsiness, headache, joint/muscle pain. Rare: myocarditis |
[74] [75,76] |
| Oxford-AstraZeneca | Pain and swelling at the injection site, fever | [77,78] |
| Janssen | Injection site reactions: pain, redness of the skin, and swelling, fatigue, headache, nausea, muscle aches, and fever. | [79] |
| Sinopharm | Burning and pain at injection site , fever, fatigue | [80] |
| Novavax | Injection site pain and swelling, redness, and pruritus, fatigue, headaches |
[81] |
Table 4.
Showing overview of 65 eligible studies examining the effectiveness and safety of COVID-19 vaccines and vaccination issues in Trinidad and Tobago.
Table 4.
Showing overview of 65 eligible studies examining the effectiveness and safety of COVID-19 vaccines and vaccination issues in Trinidad and Tobago.
| Author/Year | Aim/Open questions | Type of Study/ Design | Results |
|---|---|---|---|
| Pormohammad et al, 2021 [1] | The current study systematically reviewed the clinical features of the vaccines in clinical trials to provide a better estimate of their efficacy, side effects and immunogenicity. | Systematic review | The adenovirus-vectored and mRNA-based vaccines showed the highest efficacy after first and second doses, respectively. The mRNA-based vaccines had the highest level of side effects reported. |
| Forni et al, 2021 [2] | Will the new vaccines be able to control the COVID-19 pandemic? |
Literature Review | Due to the novelty of the technologies adopted and short development time, these vaccines deploys several unresolved issues that will permit to clarify only on the passage of time. Technical problems connected with the production of billions of doses are imminent challenges. |
| Zheng et al, 2022 [3] | To estimate COVID-19 vaccine effectiveness (VE) against concerned outcomes. | Systematic review | The COVID-19 vaccines were highly protective. |
| Al-Momani et al, 2022 [4] | To establish the effectiveness of the COVID-19 vaccines in reducing hopitalization of patients in Jordan. | Prospective, Case-control Study |
The overall VE among the participants was 84% (95% Cl 79–88%). VE was higher for Pfizer vaccine recipients than for those who received the Sinopharm vaccine |
|
Hadj Hassine, 2022 [5] |
VE can be jeopardised by the rapid spread and emergence of SARS-CoV-2 variants of concern (VOCs)? | Literature Review |
Covid-19 vaccines have good neutralising activity against the Alpha strain, and a reduced effect on the Beta strain. |
| Francis et al, 2022 [6] | To discuss the most recent WHO-approved Covid-19 vaccine subtypes, and geographical scheduled updates. | Literature Review | As of 16 May 2021, the number of countries that have approved the use of the following vaccines is Oxford/AstraZeneca in 101, Pfizer in 85, Moderna in 46, and Janssen in 41. |
|
https://www.cdc.gov/vaccines/acip/recs/grade/covid-19-pfizer-biontech-vaccine.html 2021 [7] |
Should vaccination with Pfizer-BioNTech COVID-19 vaccine (2-doses, IM) be recommended for persons 16 years of age and older? |
Report | The pooled VE estimates from the observational studies (OS) demonstrated that the Pfizer-BioNTech vaccine reduced symptomatic COVID-19 when was compared to no vaccination. |
| Rotshild et al, 2021 [8] |
To compare the efficacy of COVID-19 vaccines to prevent severe disease in the adults and among the elderly. |
Systematic Review and Meta-analysis | BNT162b2 and mRNA-1273 vaccines were ranked with the highest probability of efficacy against symptomatic COVID-19. |
| Saciuk et al, 2022 [9] | To measure VE regarding infection, hospitalization and mortality from COVID-19 after adjusting for both person-specific risk variables and virus exposure. | Retrospective cohort study | Of 1,650,885; 28,042 became PCR positive during the study period, of whom 1047 were hospitalized and 164 died. |
| Lopez Bernal et al, 2021 [10] | To compare and diagnose a patient with XLA that presented with an initial diagnosis of THI and CVID. |
Test negative case-control study | Participants aged 80 years and older vaccinated with BNT162b2 before January 2021 had a higher probability of testing positive in the first nine days post-vaccination indicating a higher underlying risk of infection. |
| Soiza et al, 2021 [11] | To review of the main candidate vaccines focusing on the evidence of safety and efficacy in older adult population. | Review article | Pfizer and Moderna vaccine have announced high degrees of efficacy among the elderly. |
| Piechotta et al, 2023 [12] | To assess effectiveness of COVID-19 vaccines approved in the EU for children aged 5-11 years. | Systematic Review and Meta-Analysis | Vaccine effectiveness after two doses against omicron infections was 41,6%. |
| Tenforde et al, 2021 [13] | The duration of mRNA vaccine (Pfizer-BioNTech or Moderna) VE against COVID-19–associated hospitalizations was assessed among adults aged ≥18 years. | Cross- sectional study | VE against COVID-19– associated hospitalization was 86% 2–12 weeks and 84% 13–24 weeks from receipt of the second vaccine dose |
| Elamin et al, 2023 [14] | To assess effectiveness of how two doses of the Pfizer and Oxford-AstraZeneca vaccines were in preventing COVID-19 infection six months after administration. | Retrospectivecohort study | Enrolled 4458 participants in Jazan. The majority of them received the Pfizer vaccine. The results showed that the Pfizer and ASZ vaccine’s protection decreased from 93.2% and 90.2%, respectively, during the first three months, to 68.5% and 68.1% after a second six-month interval. |
| Moreira et al, 2022 [15] | To assess the BNT162b2 vaccine (Pfizer-BioNTech) safety and efficacy against Covid-19 starting 7 days after the third dose. | Clinical trial |
A total of 5081 participants received a third Pfizer-BioNTech dose and 5044 received placebo. Local and systemic events were generally of low grade. No new cases of pericarditis or myocarditis was reported. |
| Bar-On et al, 2021 [16] | To assess the efficacy of a third dose (booster) of the Pfizer-BioNTech in individuals aged 60 and older in Israel. | Prospective study. |
The rate of confirmed infection was lower in the booster group, which included 10.6 million person-days with 934 confirmed infections and 29 cases of severe illness, as compared the nonbooster group, which included approximately 5.2 million person-days with 4439 confirmed infections and 294 cases of severe illness. |
| Chirico et al, 2022 [17] | To examine the scientific literature on the efficacy, effectiveness and safety of COVID-19 vaccines and new SARS-CoV-2 strains. | Literature Review | For some vaccines including Janssen (Ad26.COV2.S), Covaxin (BBV152), Sinopharm (BBIBP-CorV), and Sinovac (CoronaVac), exist information available on their safety and immunogenicity from phase I and II, but evidence of their effectiveness is not clear. There were four serious issues among BNT162b2 participants in a clinical trial including right axillary lymphadenopathy, shoulder injury from vaccine administration, right leg paresthesia and paroxysmal ventricular arrhythmia. Moderna vaccine showed some mild and moderate side effects. A global concern is the highly transmissible Delta variant, which has become predominant worldwide. |
| Mohammed et al, 2022 [18] | To compare the efficacy and effectiveness of seven COVID-19 vaccines. | Systematic Review | The Pfizer/BioNTech vaccine had the highest effectiveness for the first dose of any vaccine against infection with B.1.1.7 variant, it was 70 (CI 55–85) at ≥21 days after vaccination. |
| Andrews et al, 2022 [19] | To explore concerns about the effectiveness of current vaccines against the omicron (B.1.1.529) variant. | Test-negative case-control design | A Pfizer/BioNTech or Moderna vaccine booster after either the ChAdOx1 nCoV-19 or Pfizer/BioNTech primary course substantially increased protection, which decreases over time. |
| Zeng et al, 2022 [20] | To provide a comprehensive overview of the effectiveness profile of COVID-19 vaccines against variants of concern (VOC). | Systematic Review and Meta-analysis | Eleven COVID-19 vaccines were included in this analysis. Full vaccination was protective against Alpha, Beta, Gamma, Delta, and Omicron variants, with VE of 88.0%, 73.0%, 63.0%, 77.8% and 55.9% respectively. Booster vaccinations were more effective against Delta and Omicron variants, with a vaccine efficacy of 95.5% and 80.8%, respectively. |
| https://www.cdc.gov/vaccines/acip/recs/grade/covid-19-moderna-vaccine.html; 2020 [21] | “Should vaccination with Moderna COVID-19 vaccine be recommended for persons 18 years of age and older during an Emergency Use Authorization?” | Report on a systematic review | Data were reviewed from two published Phase I studies, one Phase II randomized controlled trial and one Phase III randomized controlled trial using data provided by the sponsor and FDA. The Moderna COVID-19 vaccine has a VE of 94.1%. |
| Rahmani et al, 2022 [22] | “To evaluate the effectiveness of COVID-19 vaccines in reducing the incidence, hospitalization, and mortality from COVID-19”. | Systematic Review and Meta-analysis | The Pooled Vaccine Effectiveness (PVE) against SARS-COV 2 infection was in the first and second doses 71% and 87%, respectively; preventing hospitalization was 73% and 89%, respectively. Regarding the infection-related mortality was 68% and 92%, respectively. |
| Soheili et al, 2023 [23] | “To evaluate the efficacy and effectiveness of several COVID-19 vaccines, including AstraZeneca, Pfizer, Moderna, Bharat, and Johnson & Johnson, to better estimate their immunogenicity, benefits, or side effects”. | Meta-analysis | The total effectiveness of all COVID-19 vaccines after the first and second doses were 71% and 91%, respectively. The total efficacy of vaccines after the first and second doses was 81% and 71% |
| Self et al, 2021 [24] |
To assess VE of three COVID-19 vaccines (mRNA-1273 from Moderna, BNT162b2 from Pfizer-BioNTech and Ad26.COV2 from Janssen) in preventing COVID-19 hospitalization. | Case control study |
Among U.S. adults without immunocompromising conditions, vaccines effectiveness against COVID-19 hospitalization during March 11- August 15, 2021, was higher for the Moderna vaccine (93%) than the Pfizer/BioNTech vaccine (88%) and Janssen vaccine (71%). |
| Harris et al, 2023 [25] | “To compare the risk of adverse events between mRNA vaccines for COVID-19 (mRNA-1273 and BNT162b2) overall, by frailty level, and by prior history of the adverse events of interest”. | Cohort study | “In this study of 6 388 196 older US adults, a 4% lower risk of pulmonary embolism, a 2% lower risk of thromboembolic events, and a 14% lower risk of diagnosed COVID-19 were observed among those who received the mRNA-1273 vaccine compared with the BNT162b2 vaccine”. |
| Dickerman et al, 2022 [26] | To investigate he messenger RNA (mRNA)–based vaccines for their comparative effectiveness range of outcomes across diverse populations. | Cross- sectional study | “Recipients of the BNT162b2 vaccine had a 27% higher risk of documented SARS-CoV-2 infection and a 70% higher risk of hospitalization for Covid-19 than recipients of the mRNA-1273 vaccine over 24 weeks of follow-up in a period marked by alpha-variant predominance”. |
| Doria-Rose et al, 2021 [27] | To assess the potential risk of the Omicron variant to existing vaccines. | Prospective study | “Omicron was 49-84-fold less sensitive to neutralization than D614G and 5.3-6.2-fold less sensitive than Beta when assayed with serum samples obtained 4 weeks after 2 standard inoculations with 100 µg mRNA-1273”. |
| https://www.fda.gov/vaccines-blood-biologics/coronavirus-covid-19-cber-regulated-biologics/moderna-covid-19-vaccine; 2023 [28] | N/A | Technical Report | Ensuring that the correct volume of the Moderna vaccine is withdrawn from the vial to administered to children up to age 11. |
| Nanduri et al, 2021 [29] | To assess the VE of mRNA vaccines among nursing home residents in the US. |
Prospective study | “Two doses of mRNA vaccines were 74.7% effective against infection among nursing home residents early in the vaccination program (March-May 2021). During June-July 2021, when B.1.617.2 (Delta) variant circulation predominated, effectiveness declined significantly to 53.1%”. |
| Mazagatos et al, 2021 [30] | To estimate mRNA COVID-19 vaccine effectiveness for elderly in long-term care facilities (LTCF) in Spain. | Prospective study | COVID-19 mRNA vaccines including Moderna, were highly effective in preventing not only COVID-19 but also hospitalisations, and deaths in elderly LTCF. |
| Fiolet et al, 2022 [31] |
“To provide an up-to-date comparative analysis of the characteristics, adverse events, efficacy, effectiveness and impact of the variants of concern for 19 COVID-19 vaccines”. | Literature Review | All vaccines appear to be safe and effective tools to prevent severe COVID-19. |
| Kaura et al, 2022 [32] | “To compare compared the effectiveness of a single dose strategy of the Oxford-AstraZeneca or Pfizer-BioNTech vaccines against SARS-CoV-2 infection across all age groups and over an extended follow-up period”. | Observational cohort study | “534 infections were documented overall, of which 65 (11.9%) required hospitalization, and 29 (5.6%) resulted in death, during the period from 14 to 84 days”. |
| Asano el al, 2022 [33] | To evaluate the immunogenicity and safety of the AZD1222 (ChAdOx1 nCoV-19) vaccine in Japanese adults |
Randomized, double-blind trial |
“The AZD1222 (ChAdOx1 nCoV-19) vaccine is a replication-deficient simian adenovirus-vectored vaccine encoding the full-length SARS-CoV-2 spike protein.” “In a pooled analysis of four trials conducted in the UK (phase 1/2 and 2/3), Brazil (phase 3) and South Africa (phase 1/2), AZD1222 exhibited an acceptable safety profile and overall vaccine efficacy of 66.7% [95% confidence interval (CI) 57.4–74.0] against COVID-19 >14 days after the second dose.” |
| Harvey et al, 2021 [34] | “Can observational clinical data from commercial laboratories be used to evaluate the comparative risk of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection for individuals who are antibody positive vs those who are antibody negative?” | Observational descriptive cohort study |
“A total of 3 257 478 unique patients with an index antibody test were identified after excluding 132 patients with discordant antibody tests on the index day. Of these, 2 876 773 (88.3%) had a negative index antibody result (seronegatives), 378 606 (11.6%) had a positive index antibody result (seropositives), and 2099 (0.1%) had an inconclusive index antibody result (sero-uncertain).” Seropositive individuals were more likely to have symptoms or a diagnosis of COVID-19 than seronegative individuals. |
| Letafati et al, 2023 [35] | “To evaluate the role played by the type of the 3rd dose of vaccination by comparing the safety and efficacy of two common vaccination histories differing only in the 3rd received dose.” | Cross-sectional study | “Out of 346 cases with respiratory symptoms, 120 cases tested positive for SARS-CoV-2 and had received two doses of Sinopharm and a different booster dose of either AZD1222 (AstraZeneca) or BIBP (Sinopharm).” |
| Sadoff et al, 2021 [36] | To conduc an ongoing phase 3 trial (ENSEMBLE) to evaluate the safety and efficacy of a single dose of Ad26.COV2.S at 5×1010 viral particles for the prevention of Covid-19 and SARS-CoV-2 infection in adults. | Multicenter, randomized, double-blind, placebo-controlled, phase 3, pivotal trial. | “A total of 44,325 participants underwent randomization, of whom 43,783 received vaccine or placebo; the per-protocol population included 39,321 SARS-CoV-2–negative participants, of whom 19,630 received Ad26.COV2.S and 19,691 received placebo.” “With regard to severe–critical Covid-19, vaccine efficacy was 76.7% (adjusted 95% CI, 54.6 to 89.1) against disease with onset at least 14 days after administration and 85.4% (adjusted 95% CI, 54.2 to 96.9) against disease with onset at least 28 days after administration.” |
| Hardt et al, 2022 [37] | “To investigate the efficacy, safety, and immunogenicity of the Ad26.COV2.S vaccine (Janssen) as primary vaccination plus a booster dose.” | Randomised, double-blind, placebo-controlled, phase 3 trial | Vaccine efficacy was 75·2%. The booster vaccine exhibited an acceptable safety profile. “In these studies, both homologous and heterologous Ad26.COV2.S boosters had less effect on neutralising antibody titres than boosters of mRNA vaccines; both Ad26.COV2.S and mRNA boosters generally yielded lower titres against delta and omicron variants relative to the wild-type or reference strains.” |
| Zhang et al, 2022 [38] | To compare the development of immune memory in subjects who had received immunization with mRNA-1273, BNT162b2, Ad26.COV2.S, or NVX-CoV2373 vaccine. | Prospective study | “While neutralizing antibody kinetics were different between mRNA and viral vector vaccines, the CD4+ T cell response kinetics were similar.” |
| Stephenson et al, 2021 [39] | “To evaluate the immunogenicity of the Ad26.COV2.S vaccine in humans.” | Randomized, double-blind, placebo-controlled phase 1 clinical trial | By day 8 following immunization, binding antibodies were observed in 65% (13 of 20) of vaccine recipients. Binding and neutralizing antibodies continued to increase on days 29, 57, and 71. |
| Zhou et al, 2022 [40] |
“To provide references for subsequent vaccine development and clinical research.’ | Literature Review | All countries play a great role in vaccine research and development, and there are a variety of vaccines that have been listed through clinical trials. |
| Nadeem et al, 2023 [41] | “To assess the safety and efficacy of BBIBPP-CorV (Sinopharm) vaccine within the Pakistani adult population aged 60 or above.” | Retrospective study | Between 5 May 2021 and 31 July 2021, 3426 symptomatic individuals were PCR tested. The results displayed that BBIBPP-CorV (Sinopharm) vaccine 14 days after the second dose was efficient in reducing the risk of symptomatic infection (94.3%), hospitalisations (60.5%) and mortality by 98.6%, among vaccinated individuals with a significant p value of 0.001. |
| Wang et al, 2022 [42] | To review evidences of the safety, efficacy, and effectiveness of Sinopharm vaccine. | Literature Review | Clinical trials conducted during the first wave of the infection suggested BBIBP-CorV offered a good efficacy in preventing new death and infections related to SARS-CoV-2. The protective efficacy was 78.89 %. Vaccine efficacy was 78.07%, calculating the person-years of follow-up. Antibody response declined three months following BBIBP-CorV vaccination, while the T cell response persisted. |
| Alqassieh et al, 2021 [43] | To compare the specific antibody titers in subjects vaccinated with either the Sinopharm vaccine or the Pfizer-BioNTech COVID-19 vaccine. | Prospective observational cohort | The study showed that 99.3% recipients of the Pfizer-BioNTech vaccine had a positive IgG titers, while 85.7% recipients of Sinopharm had positive IgG (p < 0.001). |
| Jamalidoust et al, 2023 [44] | “To determine the rate of natural and breakthrough infection and related symptoms of Covid-19 amongst Iranian healthcare workers (HCWs) who were vaccinated by different non-mRNA-based vaccines at peak points.” | Cross-sectional study | “In total, 53% of the HCWs were exposed to SARS-CoV-2 infection between 1 and 5 times within two years after the current pandemic, while 20.7% and 32.3% experienced natural and breakthrough SARS-CoV-2 infection, respectively.” “This study compared the clinical differences between the two peaks of Omicron and Delta.” |
| Zhang et al, 2022 [45] | “To determine real-world BBIBP-CorV vaccine effectiveness (VE) against serious or critical hospitalization of individuals RT-PCR-positive for SARS-CoV-2 during the first five months of BBIBP-CorV use in Morocco.” | Retrospective cohort study | “Among hospitalized subjects, 52.1% were male and 61.1% were less than 60 years old.” “Unadjusted, unboosted full-series BBIBP-CorV vaccine effectiveness against serious or critical hospitalization was 90.2% (95%CI: 87.8—92.0%).” |
| Dunkle et al, 2022 [46] | To investigate the efficacy of NVX-CoV2373 (adjuvanted, recombinant spike protein nanoparticle vaccine) in the U.S. and Mexico. | Phase 3, randomized, observer-blinded, placebo-controlled trial. | In this study, the efficacy of NVX-CoV2373 vaccine was 90.4% and demonstrated to be efficient against COVID-19 infection as shown in the prevention of the disease in the United Kingdom and South Africa. |
| Marchese et al, 2023 [47] | To assess the NVX-CoV2373 vaccine efficacy against hospitalization. |
Phase 3, randomized, placebo-controlled trial |
The study showed that NVX-CoV2373 vaccine demonstrated a 100% efficacy rate against hospitalization. |
| Graña et al, 2022 [48] | To assess the efficacy and safety of COVID-19 vaccines against SARS-CoV-2. | Systematic Review | “The authors included and analyzed 41 RCTs assessing 12 different vaccines, including homologous and heterologous vaccine schedules and the effect of booster doses. Thirty-two RCTs were multicenter and five were multinational. The sample sizes of RCTs were 60 to 44,325 participants.” |
| Dighriri et al, 2022 [49] | To assess the Pfizer-BioNTech vaccine side effects. | Systematic Review | “The total number of participants in the 14 studies was 10,632 participants. Average of the most frequent side effects of 14 studies were injection site pain 77.34%, fatigue 43%, and muscle pain 39.67%.” |
| Finsterer et al, 2021 [50] | To summarize and discuss Guillain-Barré syndrome (GBS) as a side effect of SARS-CoV-2 vaccinations. | Review article | Nine articles reporting 18 patients with side effect of SARS-CoV-2 vaccinations such as GBS, ranging between 20- and 86-year-old, ten patients were female and nine patients were male. In all 19 patients, GBS developed after the first dose of the vaccines: Astra Zeneca vaccine (14 patients), the Pfizer vaccine (4 patients) and the Johnson & Johnson vaccine (one patient). The latency between vaccination and GBS onset ranged from 3h to 39 days. |
| Wiedmann et al, 2021 [51] | To reveal side effects of the ChAdOx1 nCoV-19 vaccine (Vaxzevria; COVID-19 vaccine AstraZeneca) in Norway at the beginning of the vaccination programme. | Case reports | In Norway, a total of 132 488 first doses of the ChAdOx1 nCoV-19 vaccine were administered mainly to health care workers until halted by the health authorities on March 11th, 2021. It was due to five cases of severe cerebral venous thrombosis (CVT), associated with thrombocytopenia and intra-cerebral hemorrhage. They have developed the problem within 2 weeks post-vaccination. One case with splanchnic vein thrombosis and thrombocytopenia were encountered in previously healthy health care worker after having received ChAdOx1 CoV-19 vaccine. |
| Introna et al, 2021 [52] | To report side effects of a COVID-19 vaccine. | Case reports | It was described a case of GBS following the first dose of Oxford/AstraZeneca COVID-19 vaccine with papilledema as atypical onset. |
| Göbel et al, 2021 [53] | “To examine in detail the clinical characteristics of headaches occurring after vaccination against COVID-19 with the BNT162b2 mRNA COVID-19 vaccine.” | Prospective observational cohort | “In 66.6% of the participants, headache occurs as a single episode. A bilateral location is indicated by 73.1% of the participants. This is most often found on the forehead (38.0%) and temples (32.1%). A pressing pain character is indicated by 49.2% and 40.7% report a dull pain character. The pain intensity is most often moderate (46.2%), severe (32.1%) or very severe (8.2%). The most common accompanying symptoms are fatigue (38.8%), exhaustion (25.7%) and muscle pain (23.4%).” |
| García-Azorín et al, 2021 [54] | To assess whether the existance of headache with higher probability of intracranial hemorrhage was linked. | Observational study with case-control design | The CVT-related clinical symptoms started earlier in patients with headache than in patients without headache. |
| Sharifian-Dorche et al, 2021 [55] | To systemically review the reported cases of cases of vaccine-induced immune thrombotic thrombocytopenia (VITT) and cerebral venous sinus thrombosis (CVST) following the COVID-19 vaccination. | Systematic Review | Two articles were found, which present 13 patients with VITT and CVST after Ad26.COV2 vaccine. Moreover, 12 articles, which present clinical features of 36 patients with VITT and CVST after the ChAdOx1 nCoV-19 vaccine were examined. |
| Tahir et al, 2021 [56] |
To report a case of Bell's palsy and transverse myelitis secondary to the Johnson and Johnson COVID-19 vaccine. | Case reports | The MRI showed a long segment of increased signal throughout the spinal cord extending at least from C2 up to the thoracic spine, suggestive of transverse myelitis after rule out other causes, with a history of 10 days Johnson and Johnson COVID-19 post-vaccination. |
| Gao et al, 2021 [57] |
To report an exceedingly rare case of longitudinally extensive transverse myelitis (LETM) that occurred shortly after vaccination with the Moderna COVID-19 (mRNA-1273) vaccine. | Case reports | “C-spine MRI revealed extensive intramedullary hyperintensity in the cervical cord at the C2–C5 levels on T2-weighted images, and at the C3 level with T1 ring enhancement of the cervical cord.” |
| Hromić-Jahjefendić et al, 2023 [67] | The objectives of this systematic review and meta-analysis are to find out how often myocarditis occurs after receiving the COVID-19 vaccine, as well as the risk factors and clinical repercussions of this condition. | Systematic Review and Meta-analysis | Myocarditis is one of the potential complications of the mRNA-based COVID-19 vaccines in adolescents and young adults. “The causal relationship between vaccination and myocarditis has been difficult to establish, and further research is required.” |
| Lindo P, 2021 [82] |
To report on the national vaccine deployment programme assisted by The Health Ministry of Trinidad and Tobago expanded through the implementation of a One Shot and Done initiative for the rollout of the Janssen (Johnson & Johnson) covid19 vaccine. | News report | “The vaccine will be made available to prisoners and staff, healthcare workers, and frontline workers, in addition to residents in coastal and rural communities.” |
| https://www.paho.org/en/news/31-3-2021-trinidad-and-tobago-receives-first-covid-19-vaccines-through-covax-facility; 2021 [83] | To report on the first arrival of COVID-19 vaccines to Trinidad and Tobago. | News report | “(PAHO/WHO)- Today, 30 March, 2021, Trinidad and Tobago received 33,600 doses of COVID-19 vaccines through the COVAX Facility, a global effort between the Coalition for Epidemic Preparedness Innovations (CEPI), Gavi, the Vaccine Alliance Gavi, UNICEF, the Pan American Health Organization (PAHO) and the World Health Organization (WHO).” |
| Rafeek et al, 2023 [91] | “To assess Trinidad and Tobago dentists' vaccine acceptance, knowledge, attitude and practices regarding the COVID-19 pandemic.” | Cross-sectional study | 153 dentists completed questionnaires giving a 46.2% response rate with a 5.8% margin of error and a confidence level of 95%. 7.2% of the respondents worked at the university, 86.9% at private practice, and 5.9% at government health centres. |
| Motilal et al, 2023 [93] | “To explore the reasons for COVID-19 vaccine hesitancy in Trinidad and Tobago.” | Qualitative study | From 25 participants' responses, the main themes for being vaccine-hesitant were inefficacy, fear, information inadequacy, mistrust, perceived susceptibility, religious hesitations, and herbal alternatives. Additionally, their motivations for receiving the vaccine in the future were surrounded by perceived susceptibility, themes of necessity, health benchmark, and assurance. |
| Gopaul et al, 2022 [94] | “This study examined the safety of this vaccine in terms of the systemic and local adverse events following immunization reported by healthcare worker recipients.” | Cross-sectional study | Among the 687 participants (female = 412; female = 275), prevalence of body pain, fever, chills, myalgia, nausea, headache, fatigue, malaise, and other systemic symptoms decreased significantly 48 h after given the second dose compared to the first dose. |
| Khan et al, 2023 [95] |
To discuss about the effectiveness and safety profile of each COVID-19 vaccine in pregnancy in Trinidad and Tobago. | Letter to the Editor | The Pfizer BioNTech vaccine was the only one approved by the Ministry of Health for use in the second and third trimesters. Lack of confidence in the vaccine attributed to little research of COVID-19 in pregnancy was the reason of vaccine hesitancy in the population of pregnant women in Trinidad and Tobago. |
|
https://www.who.int/news-room/feature-stories/detail/simulating-covid-19-vaccination-in-trinidad-and-tobago 2021 [96] |
To report on a simulation exercise to respond to the COVID-19 pandemy. | WHO news report | “Before the arrival of COVID-19 vaccines, Trinidad and Tobago used simulation exercises to prepare and train the health workforce for the roll-out. Simulation exercises help develop, assess and test the functional capabilities of emergency systems, procedures and mechanisms to respond to public health emergencies.” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



